expansion of a regional st-segment elevation myocardial
TRANSCRIPT
GrangerAluko, B. Hadley Wilson, Robert J. Applegate, Greg Mears, Claire C. Corbett and Christopher B.
James G. Jollis, Hussein R. Al-Khalidi, Lisa Monk, Mayme L. Roettig, J. Lee Garvey, Akinyele O.Expansion of a Regional ST-Segment Elevation Myocardial Infarction System to an Entire State
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2012 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation published online June 4, 2012;Circulation.
http://circ.ahajournals.org/content/early/2012/05/31/CIRCULATIONAHA.111.068049World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org/content/suppl/2012/05/31/CIRCULATIONAHA.111.068049.DC1.htmlData Supplement (unedited) at:
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Circulation Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on June 4, 2012http://circ.ahajournals.org/Downloaded from
DOI: 10.1161/CIRCULATIONAHA.111.068049
1
Expansion of a Regional ST-Segment Elevation Myocardial
Infarction System to an Entire State
Running title: Jollis et al.; Expansion of regional STEMI System to entire state
James G. Jollis, MD1; Hussein R. Al-Khalidi, PhD1; Lisa Monk, RN, MSN1;
Mayme L. Roettig, RN, MSN1; J. Lee Garvey, MD3; Akinyele O. Aluko, MD2;
B. Hadley Wilson, MD4; Robert J. Applegate, MD5; Greg Mears, MD6; Claire C. Corbett,
MMS7; Christopher B. Granger, MD1 on behalf of the Race Investigators
1Duke Clinical Research Institute, Duke University, Durham; 2Dept of Cardiology, Presbyterian Hospital; 3Depts of Emergency Medicine, 4Cardiology, Carolinas Medical Center, Charlotte; 5Wake Forest Health Sciences University Winston-Salem; 6EMS Performance Improvement Center, University of North Carolina at Chapel Hill, Chapel Hill; 7New Hanover Regional
Medical Center, Wilmington, NC
Correspondence:
James G. Jollis, MD
Duke Clinical Research Institute
Duke University
Box 3254 DUMC
Durham, NC 27710
Tel: 919-684-4015
Fax: 919-668-3575
E-mail: [email protected]
Journal Subject Codes: [4] Acute myocardial infarction; [100] Health policy and outcome research
B. Hadley Wilson, MD ; Robert J. Applegate, MD ; Greg Mears, MD ; Clairee C CC. . CoCorbrbetett,t,
MMS7; Christopher B. Granger, MD1 on behalf of the Race Investigagaatotoorss
1DuDukeke C CClilininicacc l ReReReses arch Institute, Duke Univerrsisiitytyty, Durham; 2Dept oof f f CaCC rdiology, PresbyterianHoHoHospspitalall;;; 33DDDeptpttss ofo Emergency Medicine, 4Caardrdr iioologygy, Carolinanan s MeMeM ddidical Center, Charlotte; 5WWWake Fororresesestt t HeHeH alalalththth S S Scicicienenencececesss UnUnU ivivivererersisitytyty W W Wininssstooon-SSSalalalememem; ; ; 6EMEMEMS S S PePePerfrfrfoormamaancncnce e e ImImImprprprovovovemememenenent CeC nter, Univiverrrsiityty oof f NoNoortrtthh CaCaarroro ilinanaa at ChChChapeeel HHilllll,l, C C Chhhapppel HHiill; 77NeNeNew w HaHHanonovvverr r RRReggigionnall
MeMedidid ccall Cenntnteer, , WiWiW lmlmmininingtgtoonon,, NCC
CoCorrrresespopondndenencece::
by guest on June 4, 2012http://circ.ahajournals.org/Downloaded from

DOI: 10.1161/CIRCULATIONAHA.111.068049
2
Abstract:
Background - Despite national guidelines calling for timely coronary artery reperfusion,
treatment is often delayed, particularly for patients requiring inter-hospital transfer.
Methods and Results - 119 North Carolina hospitals developed coordinated plans to rapidly treat
patients with ST segment elevation myocardial infarction (STEMI) according to presentation:
walk-in, ambulance, or hospital transfer. 6841 patients with STEMI (3907 directly presenting to
21 percutaneous coronary intervention (PCI) hospitals, 2933 transferred from 98 non-PCI
hospitals were treated between July 2008 and December 2009 (age 59 years, 30% women, 19%
uninsured, chest pain duration 91 minutes, shock 9.2%). The rate of patients not receiving
reperfusion fell from 5.4% to 4.0% (P=0.04). Treatment times for hospital transfer patients
substantially improved. First hospital door to device for hospitals that adopted a “transfer for
PCI” reperfusion strategy fell from 117 minutes to 103 minutes (P=0.0008), while times at
hospitals with a mixed strategy of transfer or fibrinolysis fell from 195 minutes to 138 minutes
(P=0.002). Median door to device times for patients presenting directly to PCI hospitals fell
from 64 to 59 minutes (P<0.001). EMS-transported patients were most likely to reach door to
device goals with 91% treated within 90 minutes and 52% being treated with 60 minutes.
Patients treated within guideline goals had a mortality of 2.2% compared to 5.7% for those
exceeding guideline recommendations (P<0.001)
Conclusions - By extending regional coordination to an entire state, rapid diagnosis and
treatment of STEMI has become an established standard of care independent of health care
setting or geographic location.
Key words: acute myocardial infarction
y p p p p
PCI” reperfusion strategy fell from 117 minutes to 103 minutes (P=0.0008), whhilillee tititimemeess s atatat
hospitals with a mixed strategy of transfer or fibrinolysis fell from 195 minutes to 138 minutes
P=0.002). Median door to device times for patients presenting directlyy to PCI hospitals fell
frfromomom 6 64 4 too 555999 miminunutetes (P(P<00.0010 ).). EMEMS-transpspororttteddd patitienents wererree e moostst l liikely y toto reachch dooo r to
ddedevvivicec goals wwititith hh 9191% %% trtrreaeaateteted d d wiwithththinini 99900 miinununutes anannd 525252% % bebebeiingngg ttrereatateede wwittthh h 6060 m mminininututtesss..
PaPaatitieenentsts treatatatedede w wwiitthihinnn gguguidideelelininne e gogooalala ss hhaad d aaa mmomortrtalalitityy y ofof 2 2..2%% % ccompmpmpararreddd too o 55.5.7%7% ffooror t thohohosese
exceeedediing g gug iddele inne e rerecommmmenendadatitions (P(P<0<0.0.00101) )
Conclusionnss s -- ByByBy e extxxtenenenddingngng rrregegioioionanaall cococoorordididinananatitit onono t tooo ann ee entntntiririre ee ststatte,e,e rr rapapapididid dddiaiagnggnosososisisis aaand
by guest on June 4, 2012http://circ.ahajournals.org/Downloaded from
DOI: 10.1161/CIRCULATIONAHA.111.068049
3
Introduction
The ideal treatment of ST segment elevation myocardial infarction (STEMI) involves early
diagnosis followed by rapid reperfusion therapy.1-5 Such treatment becomes more challenging
when the activities of diagnosis and reperfusion span multiple, loosely connected hospitals and
emergency medical services (EMS). To overcome these barriers and provide ideal reperfusion as
a uniform standard of care regardless of health care setting or geographic location, we
established coordinated regional care across the entire state of North Carolina.6-8 Specifically, we
aimed to determine whether expanding our STEMI system to all hospitals and EMS agencies in
North Carolina on a voluntary and “grass roots” basis would improve the rate and speed of
myocardial reperfusion. According to protocols established in the Regional Approach to
Cardiovascular Emergencies (RACE) project, we implemented processes to expedite care in 119
hospitals across a state with a population of 9.4 million residents and area of 53,000 square
miles.9 Hospitals adopted synchronized strategies to expedite reperfusion for patients presenting
by EMS, hospital transfer, and “walk-in.”
Methods
Our work was approved by the IRB at Duke University. Data Use Agreements for a HIPAA
defined limited data set were established with all primary percutaneous coronary intervention
(PCI) hospitals. We implemented our system by building on a model established in prior work
and by using the principles outlined in the American Heart Association Mission: Lifeline and the
American College of Cardiology D2B programs. 9-12 First, we developed leadership composed of
a state director, hospital system coordinators, and nursing, EMS, and physician leaders from
multiple institutions across the state (see Supplemental Material). This leadership team
myocardial reperfusion. According to protocols established in the Regional Apprprroaaachchh t ttoo o
Cardiovascular Emergencies (RACE) project, we implemented processes to expedite care in 119
hoospspspitititalalalss acacacrorooss aaa s s stat te with a population of 9.4 mmmillllion residents aaand aaarerereaa of 53,000 square
mmileees.s 9 Hospittalallsss aadopoppteted dd syssyncncnchrhrononniizizeedd sstratttegggies tooo exxxppepedidiitee rrepeppeerrfufusiisiononn ffooror pppatatieieentntts s pppresesesenenntiinnng
byby E E EMMSMS,, , hohohosspspititaalal tttraransnnsfefeer,r, anndnd ““ “wawawallklk-i-iin.n.””
by guest on June 4, 2012http://circ.ahajournals.org/Downloaded from
DOI: 10.1161/CIRCULATIONAHA.111.068049
4
conferred in weekly conference calls and numerous regional and state meetings. Next, we
instituted the Acute Coronary Treatment and Intervention Outcomes Network Registry -- Get
With The Guidelines (AR-G) as our main data collection instrument, requesting that all
participating primary percutaneous coronary intervention (PCI) hospitals participate and
contribute to state-system reports.13 These data were maintained by the leadership team and were
used to monitor and report treatment rates and times to individual hospitals, benchmarked to
state performance. The AR-G registry at PCI hospitals represented the majority of STEMI
patients in the state eligible for reperfusion during the study period, as 95% of patients treated at
non-PCI hospitals were transferred to PCI hospitals prior to discharge.9
Once leadership and data systems were established, we organized all 21 PCI hospitals in
the state with on-site surgery to serve as regional primary PCI centers (10 in the initial RACE
intervention, 11 additional for the state-wide intervention).9 These hospitals agreed to collect and
share ARG data, fund or co-fund a hospital STEMI system coordinator, accept all STEMI
patients regardless of bed availability on a 24 hour 7 day per week basis, allow for
catheterization laboratory activation by a single call from emergency physicians or trained
paramedics without the need for cardiology consultation, have the catheterization laboratory
available within 30 minutes including the presence of an interventional cardiologists at the start
of the procedure, establish a single treatment regimen agreed upon by all physicians, and provide
immediate and regular feedback to the emergency physicians and paramedics who initiated the
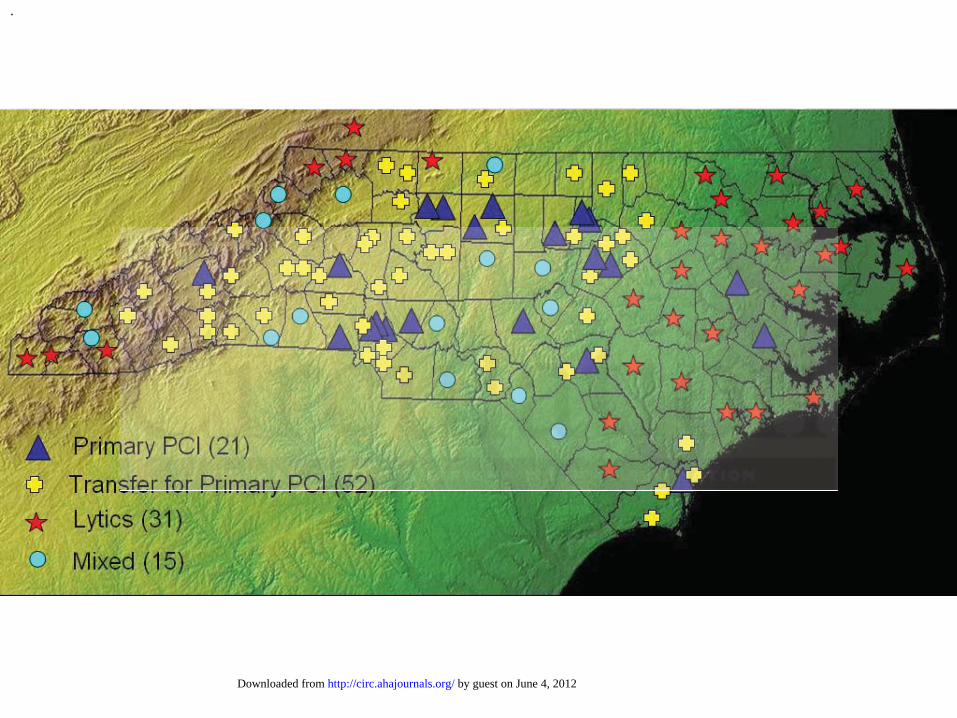
procedure. The 98 non-PCI centers (55 in the initial RACE intervention, 43 additional for the
state-wide intervention) designated themselves according to their reperfusion strategy for
patients presenting with STEMI: routine transfer for primary PCI, routine fibrinolytic therapy, or
a mixed strategy that consisted of transfer for primary PCI when transportation was readily
Once leadership and data systems were established, we organized all 21 PPPCICII h hhososospipipitatatalslsls i in
he state with on-site surgery to serve as regional primary PCI centers (10 in the initial RACE
nnteteervrvrvenenentititiononon, 11 a aaddddditional for the state-wide inttererervveention).9 Thesse e e hospsppitititala s agreed to collect and
hhharrare e ARG daatata,, fufuundndd orr r cococo-f-ffunuund d a aa hohoh spspiital SSTTTEMMMII syyststs emem cooooorrddiinnatatororr, acacccecepptpt aallllll S SSTETETEMIMIMI
papatititienenntstst rregegegaraardldleesss ofof bbeeded a avavaaililabababilililititityy ononon aa a 2224 hhhououur 77 ddaday yy pepeper wewew ekekek b b basasiis, , alallololoww w fofoorr r
catheterizatioon n n lalal boboborarar totot ryryr aaactctctivivi aaatititiononon b by y y a a sisisingngnglelee cccalalall l frfromomm eeemememergrgrgenene cycycy p pphyhyhysisisicicic ananans s s ororor t t trarar ined
by guest on June 4, 2012http://circ.ahajournals.org/Downloaded from
DOI: 10.1161/CIRCULATIONAHA.111.068049
5
available (Figure 1).
Supported by the primary PCI facilities, system coordinators and their leadership
approached every hospital and EMS within their referral region to establish a single plan to
rapidly diagnose and reperfuse patients with an acute STEMI according to national time
standards and guidelines. Emergency departments were encouraged to ascertain whether patients
had potential symptoms prior to registration, designate an area and personnel to perform ECG
within 10 minutes of arrival, and choose a reperfusion plan according to local consensus and
resources that involved either primary PCI or fibrinolysis. Hospitals that selected fibrinolysis
also developed plans for rapid primary PCI for patients with contraindications. For hospitals
served by more than one primary PCI center, all PCI centers were represented in planning
meetings. Under the guidance of the North Carolina Office of EMS, emergency medical systems
were encouraged to obtain an ECG for every patient with potential STEMI symptoms, interpret
the ECG and communicate the findings of a possible STEMI to receiving hospitals, divert to PCI
centers if first medical contact to device could reliably be achieved within 90 minutes or patients
were ineligible for fibrinolysis, and provide a standard method for the EMS time data to be
available to receiving hospital personnel.
The final step of our intervention involved multiple levels of communication between
hospitals and EMS regarding system performance, immediately after PCI, within 24 hours of a
myocardial infarction admission, and in regularly scheduled hospital, EMS, regional, and state
meetings. During these meetings, we shared best practices, reviewed treatment intervals (derived
from symptom onset, first medical contact, door time, ECG time, departure time, catheterization
lab time, device time, needle time), outcomes (deaths, complications, hospital and angiography
findings) and opportunities for system improvement. Additional description of our intervention
erved by more than one primary PCI center, all PCI centers were represented inn pplalaannnninining g g
meetings. Under the guidance of the North Carolina Office of EMS, emergency medical systems
wewererere e eenncncouououraraagedd d tototo obtain an ECG for every paatititienenent with potentiialala STETEEMMMI symptoms, interpret
hhhe EECG and cocommmmmmununniccatatateee thththeee fifinndndinini gggs oof aa a ppossiibiblle STSTSTEMEMMII toto rreecceieivivivinngg hhosososppititalalals,s, d d divivivererertt totoo PPPCI
ceentntnterererss s ifif f ffiririrstsst m mededdicicaall ccconontaactctc tttooo d d deevevicicce cococouuuld dd rerer lliliaabblylyy bbbeee aacachihihievevveddd wwwititthiin n 909090 mmmininnutututeses oor r papattitienenntsddd
were ineligiblbllee e fofof rr r fififibrbrrininnolllysysysisii , ananand d prpp ovovovididide e e a a a ststtananandadadardrdr mmmetetethohohod d d fofofor thththee e EMEMEMS S S titimememe d ddatatataa a to be
by guest on June 4, 2012http://circ.ahajournals.org/Downloaded from
DOI: 10.1161/CIRCULATIONAHA.111.068049
6
can be found in the RACE Operations Manual
[http://www.nccacc.org/RACE/RACEOperationsManualOct.09.pdf].
Statistical Analysis
Descriptive statistics for continuous and categorical variables were described as median (inter-
quartile rage) and number (percentage), respectively. Patient characteristics and process
measures were compared using Wilcoxon rank-sum test for 2 groups comparison (Kruskal-
Wallis test for more than 2 groups comparison) and chi-square tests as appropriate. The
Cochran-Armitage test for trend was used to assess changes in rates over time. To consider
whether changes in treatment time varied by hospital, mixed-effects model analyses were
conducted with PCI hospitals as a random effect. Performance data were compared in three
month intervals from July 2008 through December 2009 stratified according to treatment and
presentation to PCI hospital (fibrinolysis or primary PCI; presentation to PCI hospital by
transfer, self, or EMS).
For the PCI hospitals, the objectives of the RACE intervention were to reduce door-to-
device times for directly presenting patients and first medical contact to device for EMS
transported patients. For non-PCI hospitals, the objectives of RACE were to reduce the door-in
to door-out times and first door to device times for patients who were transferred to undergo PCI
elsewhere and door-to-needle times for those receiving fibrinolysis. For both hospital settings,
we also aimed to increase the rate of reperfusion among eligible patients. In cases where the first
ECG did not have diagnostic ST elevation, door or first medical contact time was reset to the
first diagnostic ECG. All tests were conducted at the 0.05 significance level. All patients with
ischemic symptoms lasting greater than 10 minutes within 24 hours prior to arrival and an ECG
with diagnostic ST segment elevation were included in the analyses. Statistical analyses were
conducted with PCI hospitals as a random effect. Performance data were compararrededd inn n thththrereree e e
month intervals from July 2008 through December 2009 stratified according to treatment and
prresessenenentatatatititiononon t t to PCPCPCI I hospital (fibrinolysis or primamamaryyy PCI; presentataatit onn t ttoo o PCI hospital by r
rrannnsfs er, self, oror EE MSMSMS).))
FFororr t t thehhe P PCICII hhooospipipitatalss, , ththheee obobobjjececctiiiveveves ss offf t t thehee RRRAACACEEE inininteteervrvr enene tititionono w wwerere ee totoo r r ededducuuce e dododooror-t-tto---
device timess f ffororor d ddiririrecece tltlt y y y prprresesesenenentititingngn p ppatattieiei ntntn ss s aaandndnd f ffirirrststt m medededicicicalala cccononontaaactctct t t to o o dededeviviv cecee fffororor E EEMSMM
by guest on June 4, 2012http://circ.ahajournals.org/Downloaded from
DOI: 10.1161/CIRCULATIONAHA.111.068049
7
carried out using SAS version 9.2 (SAS Institute INC, Cary, NC).
Results
Between July 2008 and December 2009, 6,841 patients presented with acute ST elevation
myocardial infarction including 3,907 patients who presented directly (57%) and 2,933 patients
who were transferred to PCI hospitals (43%). (Table 1) The median age of the cohort was 59
years (interquartile range 51-69), 30% of patients were women, and 15% were either black or of
Latino ethnicity. Nineteen percent of patients had no insurance and 7% were covered by
Medicaid. Median duration of chest pain from onset to ECG was 91 minutes, 20% of patients
had prior myocardial infarction or PCI, and shock was present on admission for 9% of patients.
By medical record review, 86% of patients were felt to be reperfusion candidates and STEMI
was apparent on the initial ECG for 89% of patients.
Means of transport to the first facility was by EMS for 55% of patients and walk-in for
43% of patients. Over the course of the study, there was an increase in the percentage of patients
presenting by EMS to PCI hospitals, from 70 to 75% (P=0.04). The inverse pattern and trend
were seen at non-PCI hospitals, where EMS presentation fell from 35 to 30% (P= 0.10). During
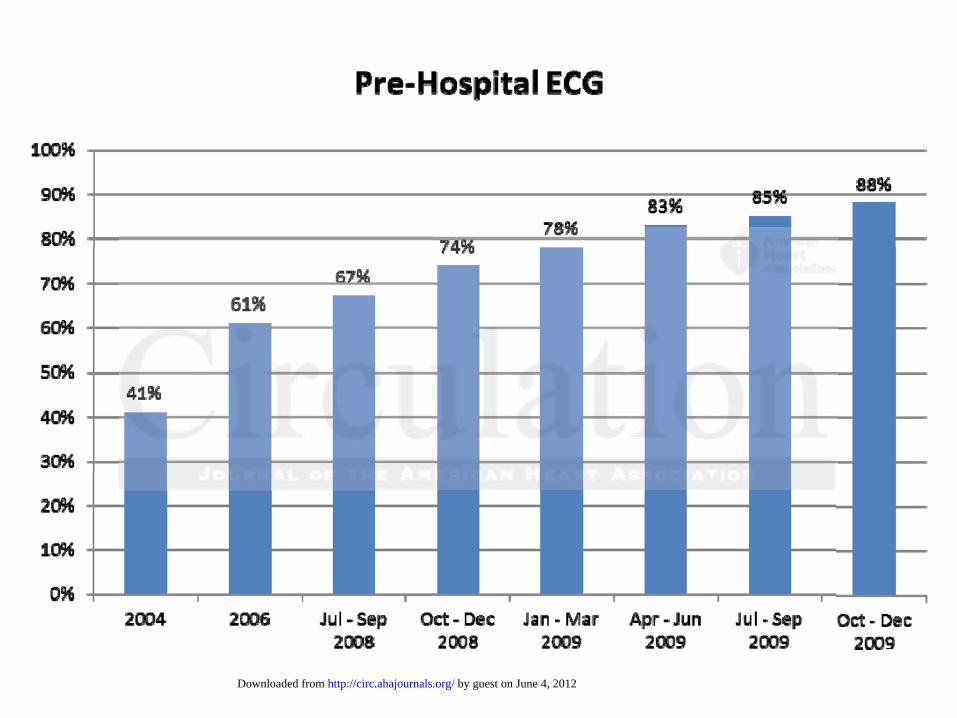
the final quarter of data collection, pre-hospital ECGs were identified for 88% of patients
presenting to PCI centers via EMS and for 32% of patients presenting to non-PCI centers
(P<0.0001). (Figure 2)
Treatment rates and times
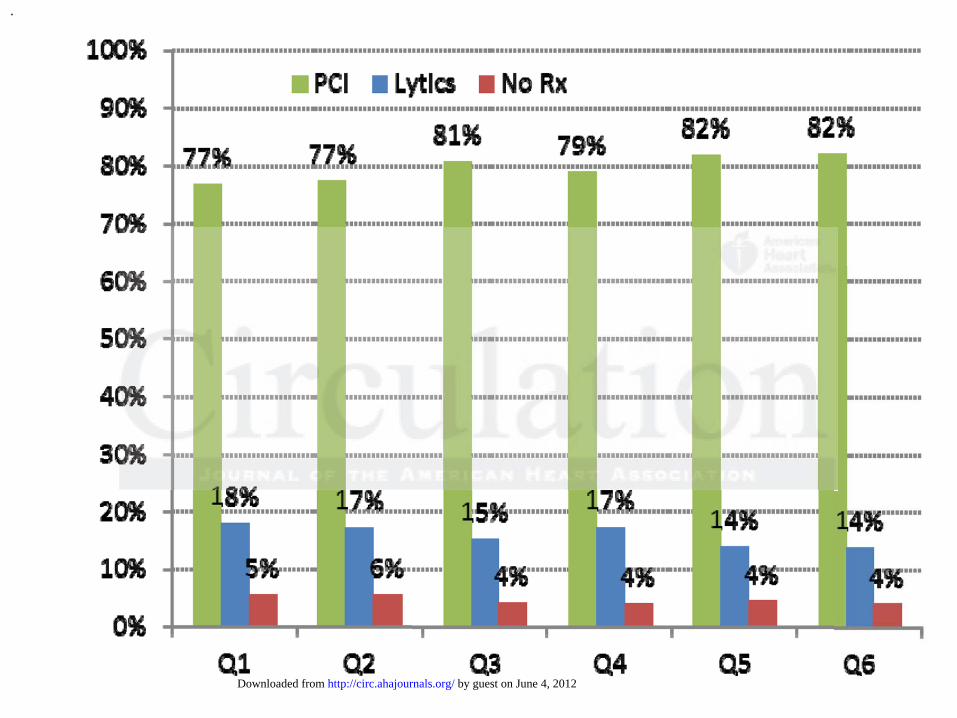
Among the 5,888 eligible patients, the rate of patients not receiving reperfusion fell from 5.4% to
4.0% (P=0.04) largely attributable to a 4% absolute decline in eligible untreated patients at non-
PCI hospitals (P<0.01) (Figure 3). During the same period, primary PCI as reperfusion mode
had prior myocardial infarction or PCI, and shock was present on admission for 9%9%9% of f f papapatititienenentsts.
By medical record review, 86% of patients were felt to be reperfusion candidates and STEMI
wawas s s apapapppaparererentntnt on n thththe e initial ECG for 89% of patieieentntn ss.
Means s ofofof ttraransnsspooortrtrt t t too o thththe e fifif rsrsrst t fafaccilittyy wwass bbyy EMEMEMS S fofoor r 5555%%% ofoff ppaaatieientntntss anannd d d wwawalklkl -i-i-in n fofof rrr
4333% % % ofofof p ppatattieieientnts.s. OOvOverer ttheheh coouoursrsseee ofofof tthhehe ssstututudydydy, , , ththt eereree e wwwasss ananan iincncncrreeasasase e e ininn tthhhe e pepepercrcr enenntataagege off f papaattieenents
presenting by y y EMEMEMS S S totot P PPCICI h hhososo pipipitatatalslss,, frrromomom 7 7 70 0 tototo 757575% % % (PPP=0=00.0.0.04)4)4).. ThThhe e e inininveveversrsrse e papapattttttererern n n ana d trend
by guest on June 4, 2012http://circ.ahajournals.org/Downloaded from
DOI: 10.1161/CIRCULATIONAHA.111.068049
8
increased from 52% to 66% in non-PCI hospitals with a corresponding decrease in fibrinolysis
from 41% to 31% of eligible patients. For patients presenting directly to PCI hospitals, primary
PCI remained stable at 95%, with only 17 patients being treated with fibrinolysis during the
study period. These patients either received fibrinolysis pre-hospital or when a significant delay
to catheterization laboratory availability was anticipated due to simultaneously presenting
patients.
Corresponding with guideline goals, treatment times of interest included door to device
for patients undergoing primary PCI, first medical contact to device for patients presenting to
PCI hospitals by EMS, first hospital door to device for patients transferred between hospitals,
and door to needle for patients treated with fibrinolysis. Over the study period, median door to
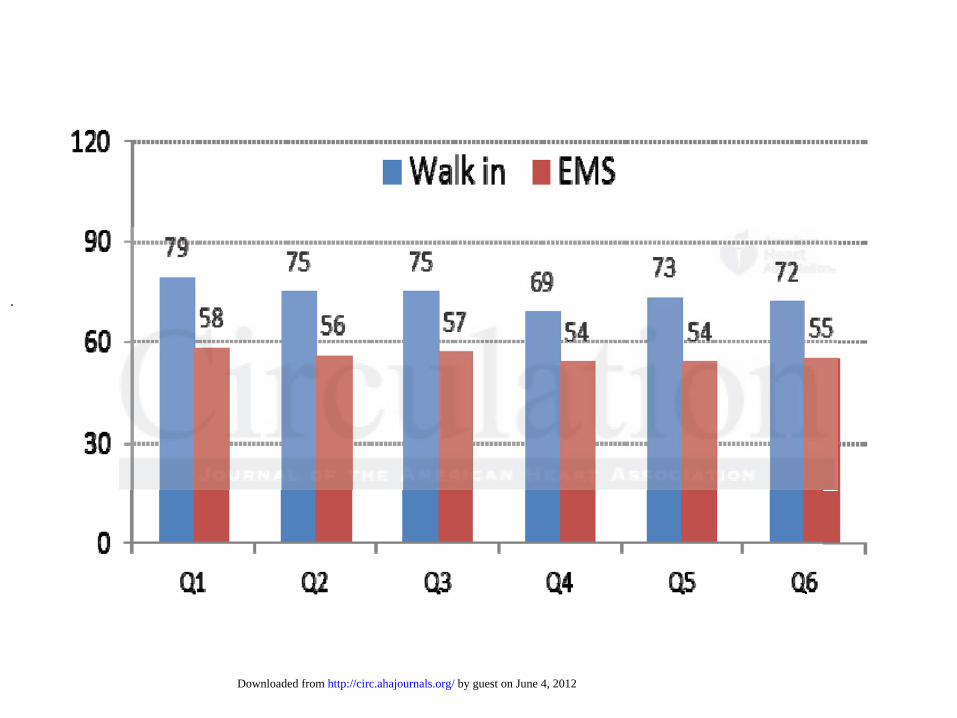
device times for patients presenting directly to PCI hospitals fell modestly from 64 to 59 minutes
(P<0.001) with improvements in both self presenting patients from 79 to 73 minutes (P=0.01)
and EMS transported patients from 58 to 55 minutes (P=0.06) (Figure 4). The proportion of
directly presenting patients who underwent PCI within 90 minutes increased from 83% to 89%.
For patients transported directly to PCI hospitals by EMS, pre-hospital ECG rates
increased from 67% to 88% during the intervention. This improvement was accompanied by a
decline in median time from first medical contact to device from 103 to 91 minutes (P<0.0001),
with 50% of patients being treated within 90 minutes by the last quarter. The transport
component of this time interval remained stable at a median of 35 minutes (interquartile range
25, 49) from first medical contact to hospital door. The percentage of patients receiving device
activation within 90 minutes of first medical contact increased from 36% to 50% (P=0.0002).
Patients transported by EMS were most likely to reach door to device goals, with 91%
undergoing device activation within 90 minutes of hospital arrival and 52% being treated with 60
and door to needle for patients treated with fibrinolysis. Over the study period, mmmedidid anann d ddoooooor r r toto
device times for patients presenting directly to PCI hospitals fell modestly from 64 to 59 minutes
PP<0<0<0.0.0.0010101) )) wiwiwitth iimpmpmprrovements in both self presenennttit nnng patients fromomm 79 9 tototo 73 minutes (P=0.01)
anndd d EME S trannspspoorortted dd papaatititienenentststs f ffroromm m 5858 tooo 555 mmminuuuteees (P=P=P=0.0.060606) ) ((FFFiggugurere 4 4)). ThThThe e prprropopporortit oonon o oof
didirereectcttlylyly ppprereesesesentntininng g g papattieenentsts wwwhohoo unununddederwrwwenenentt t PCPCCI I I wwwitththinnn 999000 mimiminunun ttetes ss ininincrcrreaaasesed dd frfrfromomm 8 883%3%% ttto o 89899%%.%.
For papapatitit enene tststs t ttraraansnsn popoortrtrtedede d ddiriri ececectly y y totoo P PPCCCI I I hohohospspspititi alalss s bybyby EEEMSMSMS, prprpre-e-e hohohospspspititi alall E E ECGCGCG r rrata es
by guest on June 4, 2012http://circ.ahajournals.org/Downloaded from
DOI: 10.1161/CIRCULATIONAHA.111.068049
9
minutes by the end of the study.
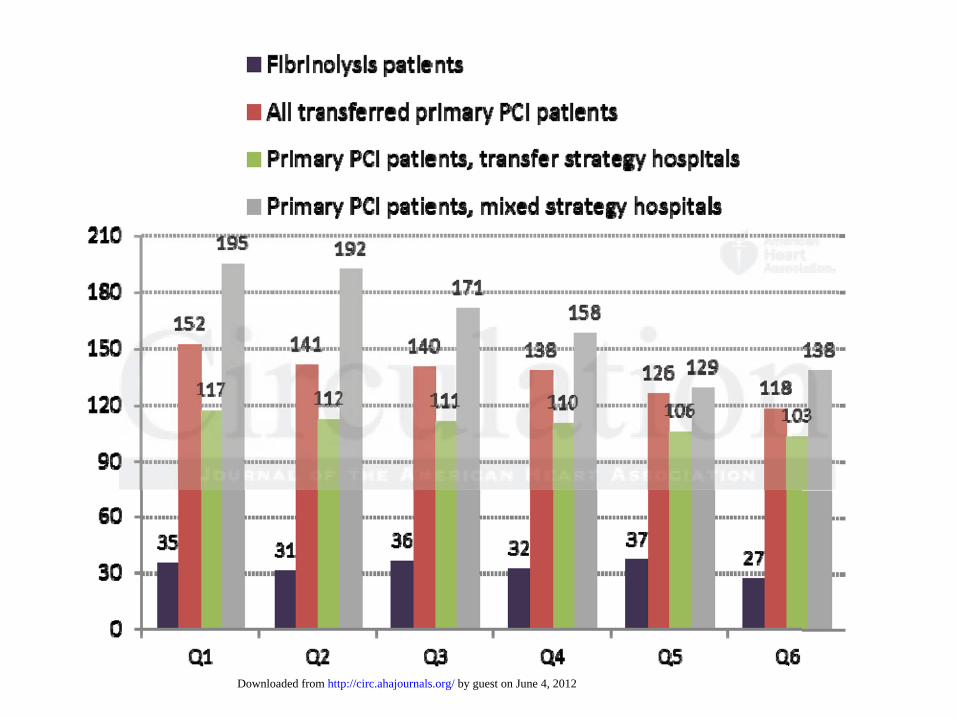
Treatment times for patients transferred between hospitals for primary PCI significantly
improved (Figure 5). The median time from first hospital door to device activation for 1,175
patients transferred from hospitals that adopted a “transfer for PCI” strategy (52 hospitals) fell
from 117 minutes to 103 minutes (P=0.0008) with 39% patients being treated within the 90
minute goal by the end of the intervention. A time interval of focus for these transferred patients
involved first hospital “door in door out” time, improving from 44 to 39 minutes. The 474
patients transferred from hospitals with a “mixed” strategy of transfer and fibrinolysis (15
hospitals) had substantially longer treatment time with first door to device falling from 195
minutes to 138 minutes by the end of the study (P=0.002). Treatment time varied substantially
by transfer distance expressed as drive times according to standard mapping software
[http://www.mapquest.com access October 21, 2010] Median first door to device time for
hospitals within 30 minutes was 94 minutes, 134 minutes for hospitals between 31 and 45
minutes drive time, and 192 minutes for hospitals exceeding 45 minutes drive time. Mixed
strategy hospitals had a 21 minute longer median drive time compared to transfer for PCI
strategy hospitals. Among the 903 patients treated with fibrinolysis prior to transfer, door to
needle did not significantly improve with median times of 35 minutes and 27 minutes in the first
and last quarters of the study (P=0.27) with 48% being treated within 30 minutes during the
entire study period. When treatment time analyses were stratified according to patients treated at
the initial RACE intervention hospitals or hospitals added for the full state intervention, the
findings were similar for both subgroups of patients. When treatment times were further
considered in mixed-effects models with PCI hospital as a random effect, the models were
significant, indicating that some hospitals had significantly greater improvement than others
minutes to 138 minutes by the end of the study (P=0.002). Treatment time varieieedd d suss bsbsbstatatantntntiaiaialllly y
by transfer distance expressed as drive times according to standard mapping software
hhtttttp:p:p://////wwwwwww.ww mmamapqpqpquueuest.com access October 21, 2020201100] Median firrststs dooooorr r tto device time for
hhohosppspitals withhinin 3 000 mimiminuuuteetess s wawawas s 949494 mmiininuuutess,, 11134 miminuuutetees s fofoforr hohospspitalallss bbeetwtwweeeeen n 313131 aaandndnd 4445 55
mimiinunun tetetess drdriviviveee titimememe, , , anannd d 19192 mimiminununutetetess fofoor r hohohossspitititaaalslss e excxceeeee dididinngng 4445 5 mimiminununutetees drdrivivive e titit mememe.. MMiMixexex dd d
trategy hospipipitatatalsls h hhadada a a 2 1 1 mimiminuuutttee e loloongnggererer m m mededediaiaann n drdrd ivivi e tititimememe c c omomompapaarerered dd tototo t t trararansnssfefefer r r fofoforr r PCI
by guest on June 4, 2012http://circ.ahajournals.org/Downloaded from
DOI: 10.1161/CIRCULATIONAHA.111.068049
10
(P<0.01).
Outcomes
Patients treated within times suggested by guidelines had a mortality of 2.2% compared to 5.7%
for patients whose treatment time exceeded guideline recommendations (P=0.001) Overall in-
hospital mortality was 5.7% (95% confidence interval 5.2 – 6.3%) during the study period
including 5.9% during the first half of the intervention and 5.5% during the second half (P=NS).
Other clinical outcomes, bleeding, stroke, hemorrhagic stroke, congestive heart failure, and
shock did not significantly vary over the study period.
Discussion
The RACE system is the largest state-wide ST elevation myocardial infarction system ever
implemented in the United States. Our intervention demonstrates that systematic barriers in
timely reperfusion can be overcome with a broadly organized voluntary effort to fill leadership
gaps in the health care. These gaps primarily exist between competing institutions and between
health care entities that function in separate and distinct systems. By building consensus among
all primary PCI hospitals in the state, we were able to convince the majority of emergency
departments and EMS systems to adopt uniform and coordinated processes for rapid diagnosis
and treatment. This universal approach allowed us to establish and embed a standard of care
independent of health care setting or geographic location of the patient. By the end of our
intervention, our protocols were adopted by state regulation for all EMS agencies, and all PCI
hospitals voluntarily agreed to continue sharing data and support regional care.
http://www.ncems.org/pdf/OverviewEMSTriageandDestinationPlan.pdf
The findings identify some remarkable changes in patterns of care and improvements in
Discussion
The RACE system is the largest state-wide ST elevation myocardial infarction system ever
mmplplplememmenennteteteddd in ttthehehe U nited States. Our intervenntititiononn demonstrates s s tht atat sysysysts ematic barriers in
iiimeemelyl reperfuusisiiononon ccanann bbbee ovovovererercocomememe w witithh a bbrbroooadlllyy orgagaganinizzzedd d vovooluuuntntararyy efeffofofortrtrt tto o fifif llllll l lleeadededersrshihihipp
gagapspsps iiinn n ththe ee hehehealalththh cccarareee. ThThessse e gagagapspsps p pririimamamariririllly eeexixix ssst bbetettweweweenenen cccomomompepepetititingngg innsnstitiitutut tititiononns s aananddd bbebetwtwweeeen
health care enenntitit titit eseses t tthahahat t fuf ncncnctititiononn i inn n seses papaarararatetete a aandndnd d ddisisstititincnctt t sysysystststememems.s.s. ByByBy b b buiuiuildldldinini g g g cococonsnsnsenenensus amongg
by guest on June 4, 2012http://circ.ahajournals.org/Downloaded from
DOI: 10.1161/CIRCULATIONAHA.111.068049
11
performance measures. Notable achievements of the RACE system include a historically low
rate of eligible but untreated of 4.0% and exceptionally fast coronary intervention for patients
presenting directly to PCI facilities with 89% being treated within 90 minutes and 52% treated
within 60 minutes. These results achieved across all 21 PCI hospitals in the state are comparable
to those achieved by 10 select systems that reported on EMS transported patients alone by Rokos
and colleagues of 86% within 90 minutes and 50% within 60 minutes.3
At the same time, this work highlights areas that need further consideration in
formulating STEMI treatment guidelines and building systems of care. Two particular areas of
interest include EMS transported patients and patient transferred between hospitals for primary
PCI. In 2007, the American College of Cardiology / American Heart Association STEMI
guidelines first directed device activation to occur within 90 minutes of “first medical contact”
rather than hospital door for patients initially treated by emergency personnel, defined as the
time that the EMS crew arrives at the “scene” of the patient.14 By adding scene time and
transport time to the 90 minute goal, this guideline effectively raised the bar on primary PCI and
made hospitals and emergency medical services jointly accountable for patient treatment. This
work describes the first broad application of this new standard with 50% of patients treated
within 90 minutes of first medical contact (or EMS arrival on scene) by the end of our study.
Time from scene arrival to hospital door consumed a median of 36 minutes of the 90 minute goal
including 15 minute scene time and 21 minute transport time. Our findings indicate that
incremental improvements in all processes of care will allow a majority of EMS transported
patients to meet this goal. These improvements should include universal adoption of
catheterization laboratory activation by paramedics as a standard of care (median time savings 17
minutes). The 28 minute median hospital door to laboratory arrival time for EMS transported
PCI. In 2007, the American College of Cardiology / American Heart Associatioonnn STSTS EMEMEMI II
guidelines first directed device activation to occur within 90 minutes of “first medical contact”
aaththhererer tt thhahannn hohohosppitititaalal d oor for patients initially treaeaeatetet dd by emergencycyc pererrsososonnn el, defined as the
iiimeeme t hat the EMEMMS crreeww aarrrrrriviviveeses aat t ththhe e “s“scceneee”” of ttthhee paatatiieientntt.14 14 1 BByy aadddddininingg scscenenene e titimememe a a nndn
rranannspspspororo tt titiimemem ttoo thhhe e 99090 mmmini uutute gogogoalalal, , ththhisss g g guuiuidedeelilil nnne eefffefectctctivivivelely y y raraaissededed tthhehe bbararr o o n n n prprprimimmararry PCPCIII aanand
made hospitaalslsls a aandndnd eeemememergrgenenencycyc mmmedededicici alall s s erererviviv cececes s s jojojoininintltly y acacaccococounununtatatablblee e fofofor r r papapatititienennt tt trtrtreaeaeatmtmtment. This
by guest on June 4, 2012http://circ.ahajournals.org/Downloaded from
DOI: 10.1161/CIRCULATIONAHA.111.068049
12
patients also indicates potential for a further improvement in hospital processes such as pre-
registration of patients, proceeding directly to the catheterization laboratory when available, and
cross training laboratory, emergency department, and intensive care unit personnel to cover
emergent STEMI patients.
To our knowledge the 39% of patients undergoing primary PCI within 90 minutes of first
hospital door in “transfer strategy” hospitals represents the highest rate reported in a multicenter
study. For comparison, 15% of patients requiring hospital transfer in Massachusetts State were
treated within 90 minutes in 2008, the latest year data are available, and the AR-G registry
reported 24% of patients transferred for PCI in the fourth quarter of 2009 had device times
within 90 minutes of first door.14 The AR-G registry involved a select group of approximately
220 hospitals that were submitting data and this national benchmark likely reflects above average
performance. The treatment times in RACE for transferred patients also compare favorably to
selected single center or single region reports from Abbot Northwestern of 32%, Mayo Clinic of
12%, and Springfield, Illinois Stat Heart of 12%. 1, 2, 5 With national guidelines for inter-hospital
transfer continuing to call for device activation within 90 minutes of first medical contact as a
“systems goal,” our inability to reach this goal in a majority of patients despite focused efforts
raises questions regarding the feasibility of achieving this benchmark on a broad scale.15 First
door to device time varied as a function of inter-hospital drive time, from 93 minutes for
hospitals within 30 minutes, 117 minutes for 31 to 45 minute drive times, and 121 minutes for
hospitals beyond 45 minutes drive time. Patients transported by air were not treated faster, with
median first door to device times of 125 minutes for hospitals in the 31 to 45 drive time range,
and 138 minutes for hospitals beyond 45 minute drive times. Thus, treatment by the 90 minute
goal for hospitals located beyond the 30 minute drive time appears less likely to occur for the
within 90 minutes of first door.14 The AR-G registry involved a select group of apappprrroxxximimimatatatelelely y
220 hospitals that were submitting data and this national benchmark likely reflects above average
peerfrffororormmamancncnce.e Thehehe t t trer atment times in RACE for trtrtranannsferred patienntstt alslsso oo ccompare favorably to
eeleeectc ed single e cceennnterer oor r r sisisingngnglelele rregeggioioon n rerepporttts frommm AAbbbbbootot N NNoororththwwesesteterrrn oof f 323232%,%, M MMayaya ooo ClClClinninicic o f
1222%,%,%, a a andnd S SSprprp ininggfgfieieeldld,,, Illllilinnoisisis S SStatatattt HeHeH aarart tt ofofof 12%2%2%. . 1, 22, 55 WW Wititith hh nananatitioononalalal g guuuiddedeliliinenen s ss fofoorr r iininteteer---hohospsspitittal
ransfer contitinununuining g g totot ccalaa l fofofor r r deeeviviv cecee a ctctctivivvatatatioioion n n wiwiw thththinini 9990 00 mimiminununutetetes s ofofof fffiririrststst m m mededdicicicalalal c ccononontact as a
by guest on June 4, 2012http://circ.ahajournals.org/Downloaded from
DOI: 10.1161/CIRCULATIONAHA.111.068049
13
majority of patients using current processes. Our work supports the extension of the standard to
120 minutes in order to have relevance for the majority of patients undergoing hospital transfer
for primary PCI.16
Mortality
While there are trends toward lower STEMI mortality in North Carolina since the initiation of
our regional system, our study lacked adequate sample size to reliably identify mortality
differences. Pathological, imaging, and clinical data support a strong relationship between
earlier treatment, less myocardial necrosis and lower mortality, and we believe the significant
time improvements in coronary reperfusion resulting from our intervention represent an
important improvement of myocardial infarction care in North Carolina.17-19 Observations from
our RACE data also support timely treatment according to a 2.2% mortality for those receiving
reperfusion according to overall guideline time goals compare to a 5.7% mortality for those
treated beyond recommended time intervals (P<0.001).
Limitations
This study relied on the voluntary submission of data to the AR-G registry, a system that lacks
any mechanism for auditing. Thus, it is possible that some of the observed improvements in
performance and outcome may have been due to self reporting. The extent to which our data
elements overlapped with door to device and needle measures in CMS Hospital Compare, a
subset of our data were subject to random audit, providing some impetus for accurate reporting.20
Our study design did not allow us to determine whether changes in care were directly attributable
to the RACE interventions or whether they occurred independently of the project. During the
corresponding time period from Q3 2008 to Q4 2009, the 220 hospitals submitting data to AR-G
had improved median door to device times for directly presenting patients from 66 to 62 minutes
mportant improvement of myocardial infarction care in North Carolina.17-19 Obsbsserrrvavav tititiononons ss frfrfromom
our RACE data also support timely treatment according to a 2.2% mortality for those receiving
eepepeperfrfrfuususioioionn n aacccoordrdrdining to overall guideline time gogogoaalls compare to a aa 5.77% % % mom rtality for those
rreaaateted beyondd rrecececommmemeendndndededd tttimime ee inini tteerrvvalss (PPP<00.0.0001).).).
LiLiimimimitatatatitiononns s s
This study relellieieied d d ononon t t hehehe v olololunununtaaaryryry s sububu mimim ssssssioioon n n ofofo d ddatatataaa to o o thththe ee ARARAR-G-G rrregegegisisstrtrraa y,y,y, a a sssysysystetetem m m tht at lacks
by guest on June 4, 2012http://circ.ahajournals.org/Downloaded from
DOI: 10.1161/CIRCULATIONAHA.111.068049
14
compared to 64 to 59 minutes in our study, and 120 to 113 minutes for transferred patients
compared to 152 to 118 minutes in RACE. Thus, the improvements in our system were of a
similar magnitude to those seen for all AR-G hospitals for directly presenting patients, and
appear to be substantially larger for transferred patients. As hospitals participating in AR-G
represent a select group focused on improving treatment times among the 1200 to 1400 hospitals
in the United States that perform primary PCI, we believe that the improvements in North
Carolina, particularly among transferred patients, likely reflect the effect of our system.
Conclusions
A uniform and comprehensive approach to organizing STEMI care across an entire state on a
voluntary basis resulted in marked improvements in timely coronary artery reperfusion. Patients
presenting directly to PCI hospitals received the fastest treatment, while those requiring inter-
hospital transfer showed the greatest improvements in treatment time. By extending our
organization to an entire state, rapid diagnosis and treatment of STEMI has become an embedded
standard of care independent of health care setting or geographic location.
Funding Sources: Unrestricted grants from Phillips, Sanofi Aventis, Medtronic Foundation. Phillips, Sanofi Aventis, and the Medtronic Foundation had no role in the design and conduct ofthe study, analysis and interpretation of the data, or in the preparation, review, or approval of the manuscript
Conflict of Interest Disclosures: Jollis received research grants from Phillips, Sanofi Aventis, Medtronic Foundation and The Medicines Company. He also acted as a consultant for United Healthcare and Blue Cross Blue Shield North Carolina. Granger received research grants from Astellas, Medtronic Foundation, Astra Zeneca, Merck, Boehringer Ingelheim, Bristol-Myers Squibb, The Medicines Company, GlaxoSmithKline, and Sanofi Aventis. He also acted as a consultant for Boehringer Ingelheim, Sanofi Aventis, Astra Zeneca, Bristol-Myers Squibb, GlaxoSmithKline, Roche, Novarti, and The Medicines Company. Applegate acted as a consultant for Abbott, St. Jude, and Terumo Medical Corporation. Wilson acted as a consultant for Boston Scientific. Garvey acted as a consultant for Abbott Vascular.
A uniform and comprehensive approach to organizing STEMI care across an enntitiiree staaatetete o o on n n a a
voluntary basis resulted in marked improvements in timely coronaryd artery reperfusion. Patients
prresessenenentititingngg d d diririrecctltltlyy y tot PCI hospitals received the ee fafaf ssstest treatment,t,, w hihilelele t those requiring inter-
hhohosppspital transfefer r shhhowowwededd tt thehehe g ggrrereatattesesest t immmpprovvvemmmennntss in ttrrereatattmemmentnt tiimme.e BBBy y exexextetendnddininng g oouourr r
orrgagaganininizazaz titiononon t to o aaan eentntiiree e ststatte,e,e rrrapapapididid d diiaiagngngnosososisss a a andndd tttrer atata mememennnt oooff SSSTETETEMMIMI hhhasas b bbecececomommee e anann eembmbm edededdded dff
tandard of cacaarerere i indndndepepepenenendeeentntnt o of f f hehehealalaltht cacacarerere s ssetetettitit ngngng o oorr r geeeogogograraraphphphicicic locococatatatioioion.n.n
by guest on June 4, 2012http://circ.ahajournals.org/Downloaded from
DOI: 10.1161/CIRCULATIONAHA.111.068049
15
References:
1. Henry TD, Sharkey SW, Burke MN, Chavez IJ, Graham KJ, Henry CR, Lips DL, Madison JD, Menssen KM, Mooney MR, Newell MC, Pedersen WR, Poulose AK, Traverse JH, Unger BT, Wang YL, Larson DM. A regional system to provide timely access to percutaneous coronary intervention for ST-elevation myocardial infarction. Circulation. 2007;116:721-728.
2. Ting HH, Rihal CS, Gersh BJ, Haro LH, Bjerke CM, Lennon RJ, Lim CC, Bresnahan JF, Jaffe AS, Holmes DR, Bell MR. Regional systems of care to optimize timeliness of reperfusion therapy for ST-elevation myocardial infarction: the Mayo Clinic STEMI protocol. Circulation.2007;116:729-736.
3. Rokos IC, French WF, Koenig WJ, Stratton SJ, Nighswonger B, Strunk B, Jewell J, Mahmud E, Dunford JV, Hokanson J, Smith SW, Baran KW, Swor R, Berman A, Wilson BH, Aluko AO, Gross BW, Rostykus PS, Salvucci A, Dev, V, McNally B, Manoukian SV, King SB III. Integration of pre-hospital electrocardiograms and ST-elevation myocardial infarction receiving center (SRC) networks: impact on door-to-balloon times across 10 independent regions. J Am Coll Cardiol Intv. 2009;2:339-346.
4. Le May MR, So DY, Dionne R, Glover CA, Froeschi MPV, Wells GA, Davies RF, Sherrard HL, Maloney J, Marquis JF, O’Brien ER, Trickett J, Poirier P, Ryan SC, Ha A, Joseph PG Labinaz M. A citywide protocol for primary PCI in ST-segment elevation myocardial infarction. N Engl J Med. 2008;358:231-240.
5. Aguirre FV, Varghese JJ, Kelley MP, Lam W, Lucore CL, Gill JB, Page L, Turner L, Davis C, Mikell FL; Stat Heart Investigators. Rural interhospital transfer of ST-elevation myocardial infarction patients for percutaneous coronary revascularization: the Stat Heart Program. Circulation. 2008;117:1145-1152.
6. Boersma E, Maas AC, Deckers JW, Simoons ML. Early thrombolytic treatment in acute myocardial infarction. Lancet. 1996;348:771
7. Pinto DS, Kirtane AJ, Nallamothu BK, Murphy SA, Dohen DJ, Laham RJ, Cutlip DE, Bates ER, Frederick PD, Miller DP, Carrozza JP Jr, Antman EM, Cannon CP, Gibson CM. Hospital delays in reperfusion for ST-elevation myocardial infarction: implications when selecting a reperfusion strategy. Circulation. 2006;114:2019-2025.
8. Gersh BJ, Stone GW, White HD, Holmes DR. Pharmacological facilitation of primary percutaneous coronary intervention for acute myocardial infarction: is the slope of the curve the shape of the future?. JAMA. 2005;293:979-986.
9. Jollis JG, Roettig ML, Aluko AO, Antrom KJ, Applegate RJ, Babb JD, Berger PB, Bohle DJ, Fletcher SM, Garvey JL, Hathaway WR, Hoekstra JW, Kelly RV, Maddox WT, Shiber JR, Valeri FS, Watling BA, Wilson BH, Granger CB. Implementation of a statewide system for coronary reperfusion for ST-segment elevation myocardial infarction. JAMA. 2007;298:2371-2380.
Coll Cardiol Intv. 2009;2:339-346.
4. Le May MR, So DY, Dionne R, Glover CA, Froeschi MPV, Wells GA, Davieses RR RFFF, SSSheheherrrrrrarrarddd HL, Maloney J, Marquis JF, O’Brien ER, Trickett J, Poirier P, Ryan SC, Ha A, Joseph PG Labinaz M. A citywywide protocol for primary PCI in ST-segment elevation myocardial infarction.N N EnEnEnglglgl JJ J M M Mededed. 220000008;8 358:231-240.
5.. AAAgug irre FV,V V VVaarrghghheeseee JJJJJJ, , KeKeK lllleyeyey MMP,P, Lammm W, LLuucoooreree C CCL,L,, GGiilill JBB, PaPaPagege LLL, , TuTurnrnr erere L L L, DaDaDaviviv ss s CMMMikkekell FL; SStat t HeHeHeart Innnveststtigggata oro s.s. R R ururaal innnteeerhoosppipitaaall l trtrtranannsfffer ooff f ST--eelleevaaatiionon mmmyoyoocacaardddialnnfafafarcrcctititionon p p patatatieienntts foforr peeercrcutttanana eeeououous ss cocoorororonananarryry rrreveve aaascccullalariririzazazatttiooon:n:n t tthehee S S Stataat HHeHeaarart tt PrPrP ogogogrrarammm.
Circcululattioionn. 200080 ;1;11717:114145-11115252.
66 BBoeoersrsmama EE MaMaasas AACC DDececkekersrs JJWW SSimimoooonsns MLML EaEarlrlyy ththrorombmbololytyticic ttrereatatmementnt iinn acacututee
by guest on June 4, 2012http://circ.ahajournals.org/Downloaded from
DOI: 10.1161/CIRCULATIONAHA.111.068049
16
10. Bradley EH, Herrin J, Wang Y-F, Barton BA, Webster TR, Mattera JA, Roumanis SA, Curtis JP, Nallamothu BK, Magid DJ, McNamara RL, Parkosewich J, Loeb JM, Krumholz HM. Strategies for reducing the door-to-balloon time in acute myocardial infarction. N Engl J Med.2006;355:2308-2320.
11. Krumholz HM, Bradley EH, Nallamothu BK, Ting HH, Batchelor WB, Kline-Rogers E, Stern AF, Byrd JR, Brush JE Jr. A campaign to improve the timeliness of primary percutaneous coronary intervention: Door-to-Balloon: An Alliance for Quality. JACC Cardiovasc Interv.2008;1:97-104.
12. Jacobs AK, Antman EM, Faxon DP, Gregory T, Solis P. Development of systems of care for ST-elevation myocardial infarction patients: executive summary. Circulation. 2007;116:217-230.
13.http://www.ncdr.com/WebNCDR/NCDRDocuments/ACTION_v2_CodersDictionary_2.2.pdf
14. Antman EM, Hand M, Armstrong PW, Bates ER, Green LA, Halasyamani LK, Hochman JS, Krumholz HM, Lamas GA, Mullany CJ, Pearle DL, Sloan MA, Smith SC Jr, 2004 Writing Committee Members; Antman EM, Anbe DT, Armstrong PW, Bates, ER, Green LA, Hand M, Hochman JS Krumholz HM, Kushner FG, Lamas GA, Mullany CJ, Ornato JP, Pearle DL, Sloan MA, Smith SC Jr, Task Force Members: Jacobs AK, Adams CD, Anderson JL, Buller CE, Creager MA, Ettinger SM, Halperin JL, Hunt SA, Krumholz HM, Kushner FG, Lytle BW, Nishimura R, Page RL, Riegel B, Tarkington LG, Yancy CW l. 2007 Focused update of the ACC/AHA 2004 Guidelines for the Management of Patients With ST-Elevation Myocardial Infarction. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2008;117:296-329.
15.http://www.cardiosource.org/~/media/Files/Science%20and%20Quality/NCDR/Slidesets/ACTIONGWTG%20ResultsQ309_Q210.ashx Accessed 12/18/2010.
16. Levine GN, Bates ER, Blankenship JC, Bailey SR, Bittl JA, Cercek B, Chambers CE, Ellis SG, Guyton RA, Hollenberg SM, Khot UN, Lange RA, Mauri L, Mehran R, Moussa ID, Mukherjee D, Nallamothu BK, Ting HH. 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Circulation. 2011;124:e574-651.
17. Reimer KA, Jennings RB. The "wavefront phenomenon" of myocardial ischemic cell death. II. Transmural progression of necrosis within the framework of ischemic bed size (myocardium at risk) and collateral flow. Lab Invest. 1979;40:633-44.
18. De Luca G, Suryapranata H, Ottervanger JP, Antman EM. Time delay to treatment and mortality in primary angioplasty for acute myocardial infarction: every minute of delay counts. Circulation. 2004;109:1223-5.
19. Hedström E, Engblom H, Frogner F, Åström-Olsson K, Öhlin H, Jovinge S, Arheden H. Infarct evolution in man studied in patients with first-time coronary occlusion in comparison to
Committee Members; Antman EM, Anbe DT, Armstrong PW, Bates, ER, Green LLA,A,A H Hanand d M,M Hochman JS Krumholz HM, Kushner FG, Lamas GA, Mullany CJ, Ornato JP, PePeearrrlle DD DL,L,L, SS Slolloana MA, Smith SC Jr, Task Force Members: Jacobs AK, Adams CD, Anderson JL, BBulululleleler r CECECE, Creager MA, Ettinger SM, Halperin JL, Hunt SA, Krumholz HM, Kushner FG, Lytle BW, Nishimura R,, Pagage RL, Riegel B, Tarkington LG,G Yancy CW l. 2007 Focused update of the ACACCC/C/C/AHAHAHA A A 20202 0444 G GGuiu delines for the Managementntnt ooff Patients Withthh S T-T-ElElEleve ation Myocardial nnnfafaarrrctit on. A A A reepopoportrtr oof f ththt ee e AmAmA ererericicicanana C Colollelegegeg o off CCCarrrdiolologogogy/y/y/AmAmmereericicanan H HHeeartrt A AAssssssococo iaiatitiononon TTTasasask k ff
FForccrce on Practcticicee GuGuGuididi elelelininineseses. CCiCircrccuululaattiooon. 2220008;1111177:229966-6-332299.9.
1555.h.h.httttttp:p:p:////wwwwwww.w.cacaardrddioiosssouururcce.o.oorgrgg///~/~/~/memmedddia/a/a/FiFiFillles/s/s/ScScScieiencnce%e%e%202020annnd%d%d%20200QuQuQuallitity/y//NCNCNCDRDRR//S/Slilidededesesetstss/AAACTIONONGWGWTGT %2%20RResesultssQ3Q 0909_QQ212 0.asshxhx AAccccese sed d 1212/1/18/8/2020100.
1616 LeLevivinene GGNN BBatateses EERR BBlalanknkenenshshipip JJCC BBaiaileleyy SSRR BBitittltl JJAA CCerercecekk BB CChahambmbererss CECE ElElliliss
by guest on June 4, 2012http://circ.ahajournals.org/Downloaded from
DOI: 10.1161/CIRCULATIONAHA.111.068049
17
different species - implications for assessment of myocardial salvage. J Cardiovasc Magn Reson.2009;11:38.
20. http://www.hospitalcompare.hhs.gov Accessed 12/18/2010.
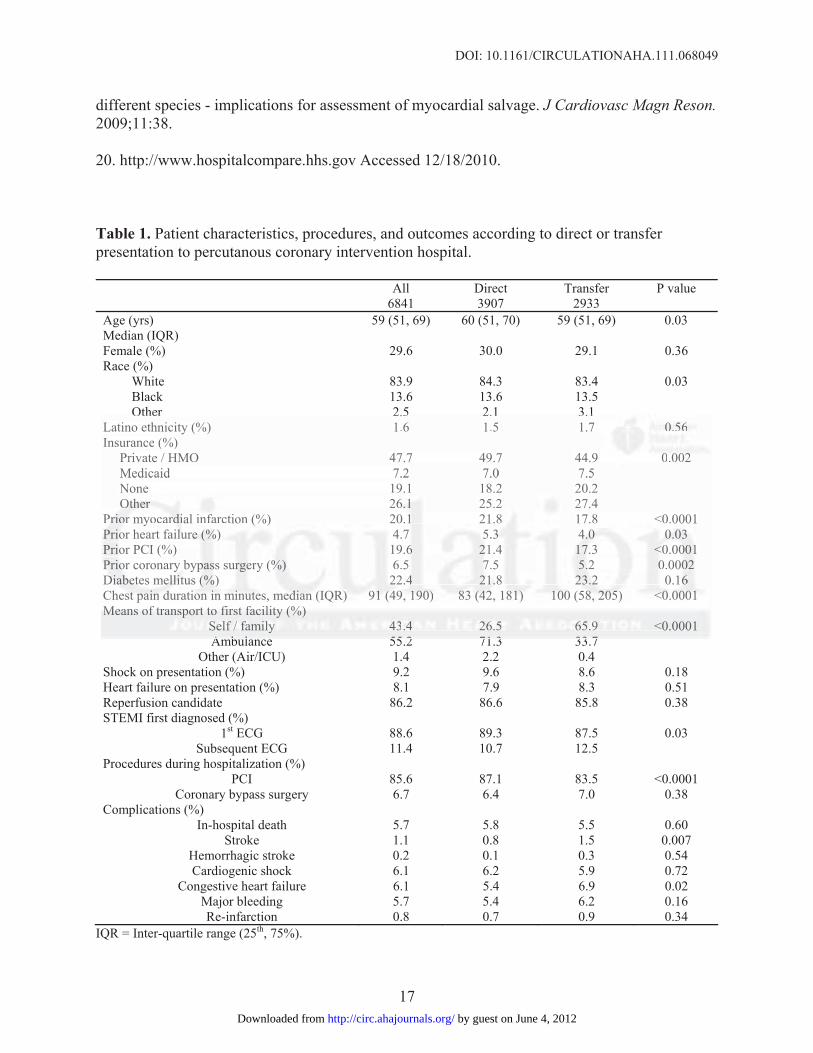
Table 1. Patient characteristics, procedures, and outcomes according to direct or transfer presentation to percutanous coronary intervention hospital.
All Direct Transfer P value 6841 3907 2933 Age (yrs) Median (IQR)
59 (51, 69) 60 (51, 70) 59 (51, 69) 0.03
Female (%) 29.6 30.0 29.1 0.36 Race (%)
White 83.9 84.3 83.4 0.03 Black 13.6 13.6 13.5 Other 2.5 2.1 3.1
Latino ethnicity (%) 1.6 1.5 1.7 0.56 Insurance (%)
Private / HMO 47.7 49.7 44.9 0.002 Medicaid 7.2 7.0 7.5 None 19.1 18.2 20.2 Other 26.1 25.2 27.4
Prior myocardial infarction (%) 20.1 21.8 17.8 <0.0001 Prior heart failure (%) 4.7 5.3 4.0 0.03 Prior PCI (%) 19.6 21.4 17.3 <0.0001 Prior coronary bypass surgery (%) 6.5 7.5 5.2 0.0002 Diabetes mellitus (%) 22.4 21.8 23.2 0.16 Chest pain duration in minutes, median (IQR) 91 (49, 190) 83 (42, 181) 100 (58, 205) <0.0001 Means of transport to first facility (%)
Self / family 43.4 26.5 65.9 <0.0001 Ambulance 55.2 71.3 33.7
Other (Air/ICU) 1.4 2.2 0.4 Shock on presentation (%) 9.2 9.6 8.6 0.18 Heart failure on presentation (%) 8.1 7.9 8.3 0.51 Reperfusion candidate 86.2 86.6 85.8 0.38 STEMI first diagnosed (%)
1st ECG 88.6 89.3 87.5 0.03 Subsequent ECG 11.4 10.7 12.5
Procedures during hospitalization (%) PCI 85.6 87.1 83.5 <0.0001
Coronary bypass surgery 6.7 6.4 7.0 0.38 Complications (%)
In-hospital death 5.7 5.8 5.5 0.60 Stroke 1.1 0.8 1.5 0.007
Hemorrhagic stroke 0.2 0.1 0.3 0.54 Cardiogenic shock 6.1 6.2 5.9 0.72
Congestive heart failure 6.1 5.4 6.9 0.02 Major bleeding 5.7 5.4 6.2 0.16 Re-infarction 0.8 0.7 0.9 0.34
IQR = Inter-quartile range (25th, 75%).
Other 2.5 2.1 3.1Latino ethnicity (%) 1.6 1.5 1.7 0.0.0 565656 Insurance (%)
Private / HMO 47.7 49.7 44.9 00 0.00202 Medicaid 7.2 7.0 7.5None 19.1 18.2 20.2 OtOtOtheheherrr 2666 1.1.1 25.2 27.4
PrPrrioioiorrr mym occararddidial iinfnfararctc ion n (%(%) ) 2020.1.1 21.8 177.88 < 0.0 0001 PPPriooor r heart faailillururee e (%(%(%)) 4.4 7 5.5.3 3 3 4.4.4.0 0 0 00.0.030303 PPriioor r PCI (%) 19.66 2221.4 4 17117.3.3 < <<0.0.000000111 PPrP iooor r coronaryryy b yppassss suurrgeeery (%(%%) ) 6.5 777.5 5..22 00.000202 DiDiDiabababetete eses mmelelellililitutus s (%(%(%) ) 2222.4.44 2221.1.1.8 8 2223.2.2.2 0 0.1.166 ChChesest tt papapaininin d d duru atatioioi nn iinin m miinin tututeses, memedididiananan ( (IQQR)R)) 91911 (( (44949,, 1919190)0)0) 8 883 3 (4(4(422,2, 11818181)) ) 1010100 0 0 (558,88, 2 2 2050505)) <0<0<0.0.0000000011 1 MeMeMeananansss ofofof tt trararansnsnspopoportrtrt tt tooo fififirsrsrsttt fafafacicicilililitytyty (( (%)%)%)
SeSeSelflflf / // f ffamaamilillyy y 434343.4.44 2226.6.6 5 55 65656 .9.99 <0.0001 A bb ll 55 2 71 3 33 7
by guest on June 4, 2012http://circ.ahajournals.org/Downloaded from
DOI: 10.1161/CIRCULATIONAHA.111.068049
18
Figure Legends:
Figure 1. North Carolina hospitals according to reperfusion strategy.
Figure 2. Pre-hospital ECG for patients presenting directly to PCI hospitals by EMS.
Figure 3. Reperfusion treatment by quarter, all eligible patients. P=0.04 for trend.
Figure 4. Hospital door to device times for patients presenting directly to PCI hospitals by
arrival mode and quarter, median times. For trend, walk in P=0.01, EMS transported P=0.06.
Figure 5. Reperfusion times for patients presenting to hospitals without PCI facilities by quarter,
median times. Door to needle times for patients treated with fibrinolysis. First hospital door to
device time for patients transferred for PCI. For transferred patients, treatment times are
presented according to hospital reperfusion strategy. For lytic P=0.27, transfer strategy
P=0.0008, mixed strategy P=0.002.
arrival mode and quarter, median times. For trend, walk in P=0.01, EMS transpoorrrtededd PPP=0=0=0.0.006.6.6.
Fiigugugurerere 55 5. ReReReppperfrffusususioi n times for patients presentttinininggg to hospitals wwwiti hooututut P PCI facilities by quarter,
mmeddidian times. D DDoooor r toto nnneeeeedldldle e e titimmemesss fofoor patiiiennnts ttrreeateed d wiwiththt ff ibibrrinnonolylysiss ss. F FFiririrstst hhhososo pipipitataal dododooroor ttto
dedeviviv cecece t t imimee e fofofor r pppattitienentts ttraransssfefeferrrrrrededed ff fororr P P PCICICI.. . FoFoFor r tttraananssffererrrerereddd papapatitienenntststs, , trtrreaaatmtmmenenentt t titimememes s aaaree e
presented acccocoordrdrdininng g g totoo h hhossspipipitatat l rererepepeperfrr usususioioon n n stststrararateteegygygy. . F Fororor l llytytyticicic P P P=0=00.2.2.27,7,7 t ttrararansnsnsfefeer rr stststrararatetetegygg
by guest on June 4, 2012http://circ.ahajournals.org/Downloaded from
Supplemental Material
RACE Investigators
State Project Leader
Lisa Monk, RN, MSN
Central Organizing Committee
Christopher B. Granger, MD
James G. Jollis, MD
Mayme Lou Roettig, RN, MSN
EMS Regional Coordinators
Claire Corbett, MMS, NREMT-P
Scott Starnes, NREMT-P
Nurse System Coordinators
Tracey Blevins, RN, BSN, MBA
Harriet Buss, RN, BSN, MSHA
Joanne Cary, BS, RN, CN,
Frank Castelblanco, RN, ADN, BA
Bridget Harding, RN, MSN
Cheryl Henderson, RN,BSN
Michelle Keasling, RN, MSN
Robyn Keller, RN, BSN
by guest on June 4, 2012http://circ.ahajournals.org/Downloaded from
Jan Matthews, RN,
Jeannie Moore, RN, BSN
Linda Newton, RN, MSN
Heather Norman, MHA, RN, BSN
Gloria Paul, RN, MSN
Mary Printz, RN, MSN, FNC
Susan Rouse, RN, BSN
Betsy Russell, RN
Stephanie Starling, BSN, RN, MHA
Jennifer Sarafin, RN, MSN
Amanda Thompson, RN, BSN, MHA
April Traxler, RN, BSN
Annette Winkler, RN, MSN
Other Systems Coordinators
Keith Pendergrass, RRT, RCP
Cathy Rabb, RRT, RCP
David Reich RCIS, BS
Charles H. Wilson, MD
Interventional Cardiology Leaders
Akinyele O. Aluko, MD
Robert J. Applegate, MD
Joseph D. Babb, MD
Christopher C. Barber, MD
by guest on June 4, 2012http://circ.ahajournals.org/Downloaded from
Bruce R. Brodie, MD
Brian P. Hearon, MD
R. Lee Jobe, MD
Kevin R. Kruse, MD
Michael R. Komada, MD
William T. Maddox, MD
Robert B. Preli, MD
Steven C. Rohrbeck, MD
John R. Sinden, MD
Patrick J. Simpson, MD
George A. Stouffer, III, MD
Thomas D. Stuckey, MD
Mark A. Thompson, MD
F. Scott Valeri, MD
John A. Williams, III, MD
B. Hadley Wilson, MD
Emergency Medicine Leaders
Robert L. Beaton, MD
Joshua N. Cochrane, MD
Sidney M. Fletcher, MD
J. Lee Garvey, MD
Penny Jo Hamilton-Gaertner, MD
Matthew R. Harmody, MD
James W. Hoekstra, MD
by guest on June 4, 2012http://circ.ahajournals.org/Downloaded from
Paul E. Horton, MD
Jonathan D. Kelly, MD
Scott T. Miekley, MD
R. Darrell Nelson, MD
Brad A. Watling, MD
Randall N. Willard, MD
Emergency Medical Service Leaders
David Cuddeback, NREMT-P
Greg Mears, MD
J. Brent Myers, MD
Drexdal R. Pratt
Dwayne R. Young, BS, REMTP
by guest on June 4, 2012http://circ.ahajournals.org/Downloaded from