experimental study of paraplegia caused by spinal tumors...
TRANSCRIPT

The Spine Journal 4 (2004) 675–680
Experimental study of paraplegia caused by spinal tumors: an animalmodel of spinal tumors created by transplantation of VX2 carcinoma
Masahito Takahashi, MD*, Jun Ogawa, MD, Yoshiaki Kinoshita, MD,Motoki Takakura, MD, Kazuo Mochizuki, MD, Kazuhiko Satomi, MD
Department of Orthopaedic Surgery, School of Medicine, Kyorin University, 6-20-2 Shinkawa Mitaka-shi, Tokyo 181-8611, Japan
Received 13 October 2003; accepted 3 June 2004
Abstract BACKGROUND: Little is known about the mechanism of the paraplegia produced by metastaticspinal tumors, although the quality of life of patients with paraplegia caused by malignant tumorsdepends to a great extent on treatment of the paraplegia. We previously established an experimentalmodel of malignant femoral tumors by transplanting VX2 carcinoma into the femur, and we havereported the efficacy of chemical embolic therapy, radiotherapy and hyperthermal therapy in treatingthe tumors in the model.PURPOSE: The purpose of the present study was to establish an animal model of metastatic spinaltumors by transplanting VX2 carcinoma into a pedicle and to analyze the mechanism of the paraplegiaproduced by metastatic spinal tumors.STUDY DESIGN: An experimental study.METHODS: VX2 carcinoma that had been successively transplanted to the thigh muscles ofJapanese White rabbits in the Department of Orthopaedic Surgery of Kyorin University Schoolof Medicine was used. The third lumbar vertebra of 37 healthy rabbits was exposed, and apiece of VX2 carcinoma was transplanted into a hole created in the pedicle with an air drill aftertransplantation. The animals were examined every other day. As soon as paraplegia developed, theanimals were sacrificed, and the axial localization of the tumor was evaluated based on the surgicalstaging of the spinal tumor (SSST classification by Tomita). Roentgenographic, histological andangiographic studies were also performed.RESULTS: Twenty-two rabbits (60%) had paraplegia at the time of the final examination. Seventeenof them had complete paraplegia, and the other five had incomplete paraplegia. The average intervaluntil incomplete paraplegia developed was 18.4�4.3 days, and the average interval until completeparaplegia developed was 30.0�4.3 days. The average proportion of the diameter of the spinalcanal occupied by the tumor was 37.2�4.9% in the incomplete cases, and 70.6% in the complete cases.The radiographs revealed an osteolytic area in the pedicle and posterior border of the third lumbarvertebra in the rabbits with complete paraplegia, but no osteolytic areas were detected in the rabbitswith incomplete paraplegia. According to the SSST classification, the lesions of all of the rabbits withparaplegia were classified as stage IV. Pathological studies revealed that the spinal cord generallyexhibited degenerative change, especially at the site of tumor compression. No tumor cells hadinvaded the spinal cord. Microangiography showed a marked reduction in blood vessels in the graymatter of the spinal cord in the complete paraplegia in comparison with incomplete paraplegia.CONCLUSION: Our method succeeded in establishing a model of metastatic spinal tumors,because the natural history of the disease, including the anatomical location of the tumors and theimaging findings, was similar to the natural history in clinical cases. This model was useful for
FDA device/drug status: not applicable.Nothing of value received from a commercial entity related to this
research.
1529-9430/04/$ – see front matter � 2004 Elsevier Inc. All rights reserved.doi:10.1016/j.spinee.2004.06.006
* Corresponding author. Department of Orthopaedic Surgery, Schoolof Medicine, Kyorin University, 6-20-2 Shinkawa Mitaka-shi, Tokyo 181-8611, Japan. Tel.: 81-422-47-5511; fax: 81-422-48-4206.
E-mail address: [email protected] (M. Takahashi)

M. Takahashi et al. / The Spine Journal 4 (2004) 675–680676
elucidating the pathogenetic mechanism of the paraplegia caused by metastatic spinal tumors.
� 2004 Elsevier Inc. All rights reserved.
Keywords: Experimental animal model; Metastatic spinal tumors; Paraplegia; Microangiography
Introduction
The paraplegia caused by metastatic spinal tumors prog-resses rapidly and often fails to improve after decompressivesurgery [1]. However, there have been hardly any reportson basic research on the paraplegia caused by metastaticspinal tumors. Sato [2] transplanted pieces of MRMT-1breast carcinoma to the third or fourth lumbar vertebra ofrats and reported that paraplegia developed in 64% of them.Fujita et al. [3] injected neoplastic cells into the left ventricleof the heart in mice and reported the development ofmultiple spinal metastases in every animal.
We produced a rabbit model of femoral sarcoma by trans-planting VX2 carcinoma into the femur and have reportedthe results of chemotherapy and thermotherapy [4–6]. VX2carcinoma is a squamous cell carcinoma and is a malignanttumor specific to the rabbits [7]. It is characterized by pulmo-nary metastasis and has been successively transplanted to thethigh muscles of Japanese White rabbits in the Departmentof Orthopaedic Surgery of Kyorin University School ofMedicine since 1995.
In the present study we used this technique to produce amodel of metastatic spinal tumors in rabbits, and we assessedthe natural course of the disease and the pathogenesis ofthe paraplegia.
Materials and methods
The animals used were 37 Japanese White rabbits (maturemale) 3 to 4 months of age and weighing 2.7 to 3.0 kg.
VX2 carcinoma successively transplanted to the thighmuscles of Japanese White rabbits in the Department ofOrthopaedic Surgery of Kyorin University School of Medi-cine was used. The VX2 carcinoma tissue was minced whiledripping physiological saline on it, and then passed througha metal filter (mesh size, 0.25 mm2). The filtrate was centri-fuged at 500 to 800 cycles/minute for 5 minutes, and afterremoving the supernatant, the concentration of the suspen-sion was 2×108 tumor cells/ml.
Under intravenous pentobarbital anesthesia (1.0 to 1.5mg), the left pedicle of the third lumbar vertebra was exposedby a posterior approach. A hole 2 mm in diameter and 2mm deep was then made in the pedicle with an air drill, andafter transplanting a piece of VX2 carcinoma (1×1×1 mm,2×105 tumor cells) into it, the hole was immediately sealedwith bone wax. After transplantation, we confirmed that allthe rabbits were capable of running satisfactorily.
We monitored the animals daily for hind limb muscleweakness for 6 weeks after transplantation. The animalswere classified according to the system of Kato et al. [8] into
three stages. Animals that could run were classified as thenormal group. Animals that could stand but not run wereclassified as the incomplete paraplegia group, and animalsthat could not even stand were classified as the completeparaplegia group (Table 1).
Fuji X-ray film was used to obtain radiographic imagesof the spine centered on the transplanted VX2 under thefollowing conditions: voltage, 48 kV; current, 100 mA; focallength, 55 cm and acquisition time, 0.1 second.
For histological examination, the spine around the tumorwas removed from animals that had developed completeor incomplete paraplegia, and cross sections were prepared.The axial localization of the tumor was evaluated based on thesurgical staging of the spinal tumor (SSST classification byTomita) [9], which classifies the extent of spinal tumors intofour stages: Stage I, intracorporeal or intralaminar; Stage II,pedicular and/or epidural extension; Stage III, anteroposter-ior development and Stage IV, paraspinal development. Theproportion of the diameter of the spinal canal occupied bytumor was calculated by using NIH Image software. Afterfixing the cross sections in 10% formalin solution for 1week, paraffin sections were prepared and stained with he-matoxylin eosin and Kluver and Barrera stain [10].
Microangiography was performed after complete or in-complete paraplegia had developed [11–13]. Under intrave-nous anesthesia, paraplegic rabbits were perfused withnormal saline (500 ml) and heparin (5,000 U), and the femo-ral artery was dissected free. The perfusion was continueduntil the solution draining freely from the cut end of thevessels turned white. After perfusion, 10 g of liquid gelatinto which 100 cc of India ink had been added was injected intothe inferior vena cava. The specimen was then removed andplaced in 10% formalin solution for 1 week.
Results
Spontaneous progression, classification of motor loss
Complete paraplegia or incomplete paraplegia developedin 22 (60%) of the 37 rabbits. Seventeen rabbits had complete
Table 1Stage of weakness
Stage Definition
Normal Animal is able to run.Incomplete paraplegia Animal can stand but is unable to walk.Complete paraplegia Animal cannot stand and there is only
a slight movement of the legs.No movement is observed.
M. Takahashi et al. / The Spine Journal 4 (2004) 675–680 677
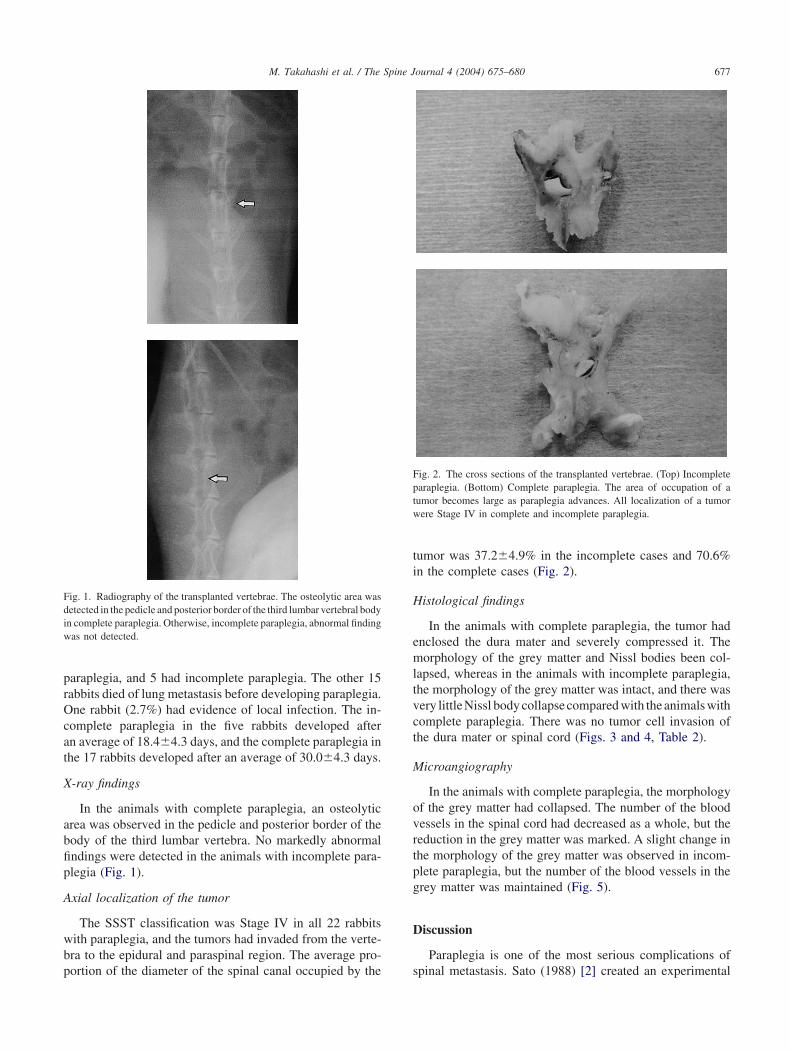
Fig. 1. Radiography of the transplanted vertebrae. The osteolytic area wasdetected in the pedicle and posterior border of the third lumbar vertebral bodyin complete paraplegia. Otherwise, incomplete paraplegia, abnormal findingwas not detected.
paraplegia, and 5 had incomplete paraplegia. The other 15rabbits died of lung metastasis before developing paraplegia.One rabbit (2.7%) had evidence of local infection. The in-complete paraplegia in the five rabbits developed afteran average of 18.4�4.3 days, and the complete paraplegia inthe 17 rabbits developed after an average of 30.0�4.3 days.
X-ray findings
In the animals with complete paraplegia, an osteolyticarea was observed in the pedicle and posterior border of thebody of the third lumbar vertebra. No markedly abnormalfindings were detected in the animals with incomplete para-plegia (Fig. 1).
Axial localization of the tumor
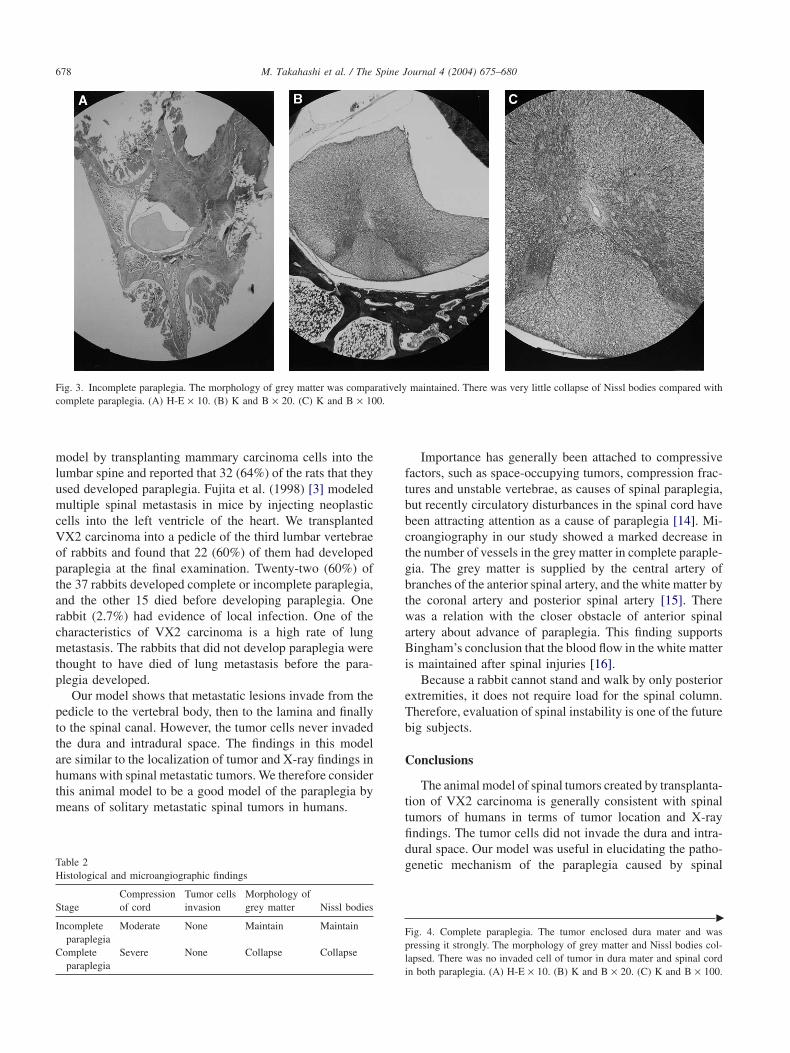
The SSST classification was Stage IV in all 22 rabbitswith paraplegia, and the tumors had invaded from the verte-bra to the epidural and paraspinal region. The average pro-portion of the diameter of the spinal canal occupied by the
Fig. 2. The cross sections of the transplanted vertebrae. (Top) Incompleteparaplegia. (Bottom) Complete paraplegia. The area of occupation of atumor becomes large as paraplegia advances. All localization of a tumorwere Stage IV in complete and incomplete paraplegia.
tumor was 37.2�4.9% in the incomplete cases and 70.6%in the complete cases (Fig. 2).
Histological findings
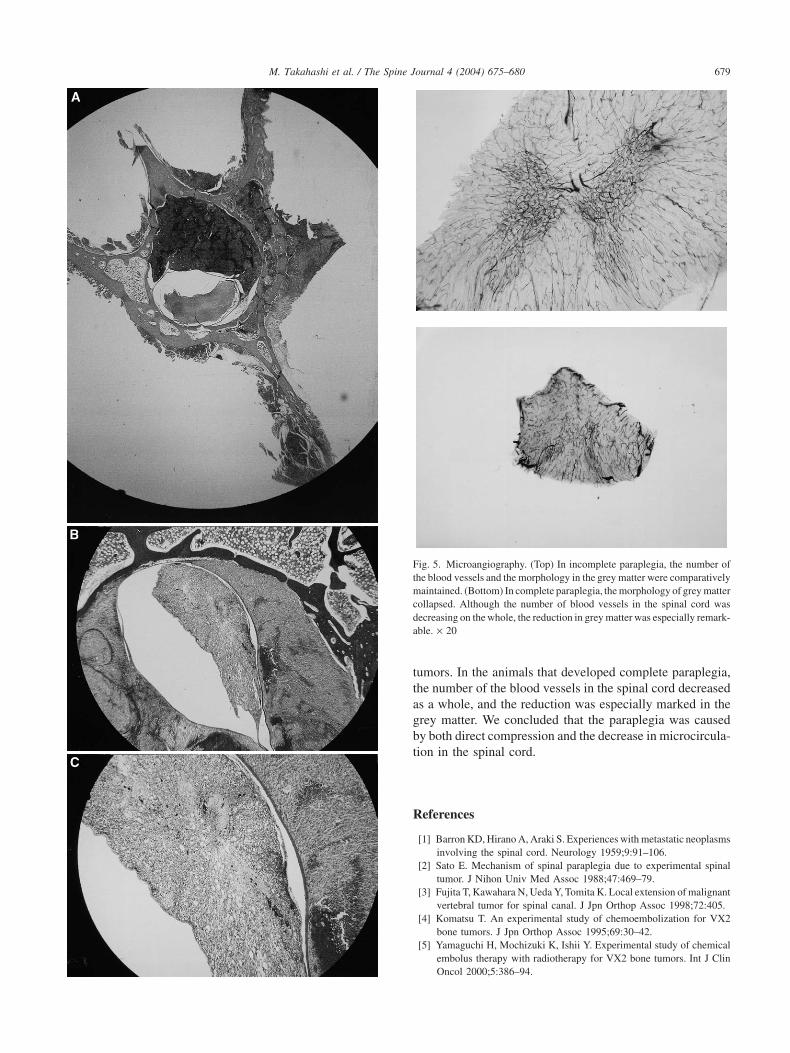
In the animals with complete paraplegia, the tumor hadenclosed the dura mater and severely compressed it. Themorphology of the grey matter and Nissl bodies been col-lapsed, whereas in the animals with incomplete paraplegia,the morphology of the grey matter was intact, and there wasvery littleNissl body collapsecompared with the animals withcomplete paraplegia. There was no tumor cell invasion ofthe dura mater or spinal cord (Figs. 3 and 4, Table 2).
Microangiography
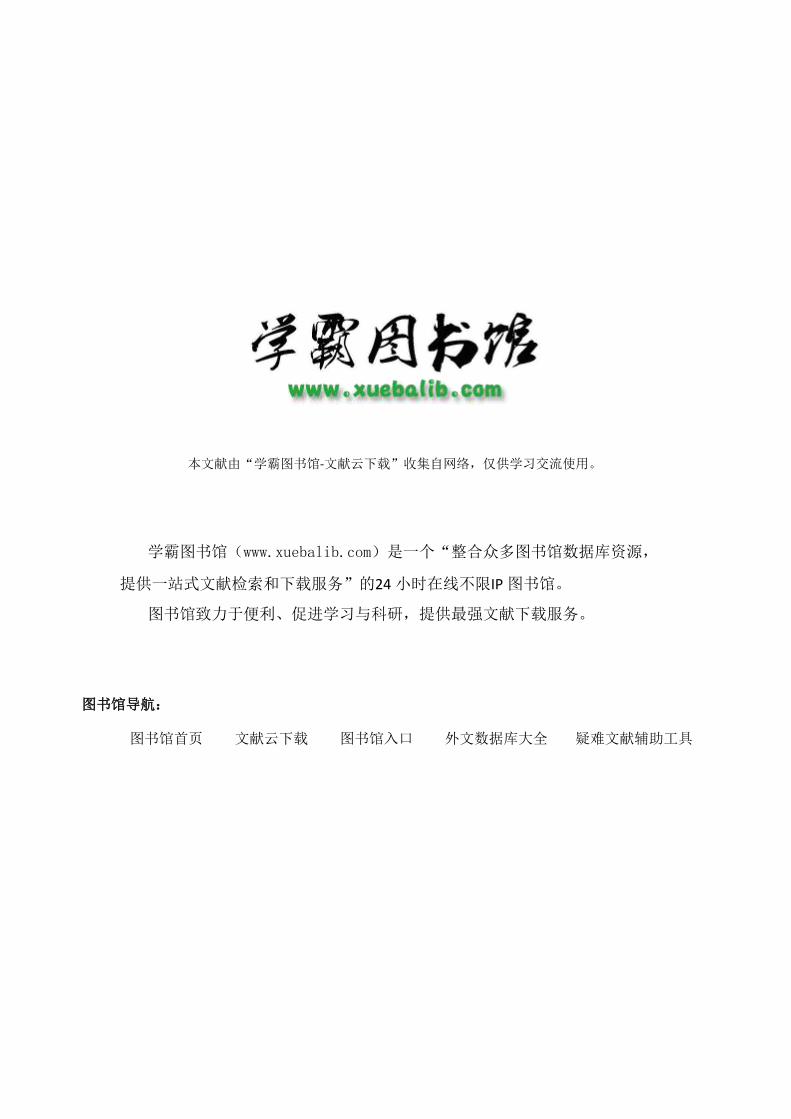
In the animals with complete paraplegia, the morphologyof the grey matter had collapsed. The number of the bloodvessels in the spinal cord had decreased as a whole, but thereduction in the grey matter was marked. A slight change inthe morphology of the grey matter was observed in incom-plete paraplegia, but the number of the blood vessels in thegrey matter was maintained (Fig. 5).
Discussion
Paraplegia is one of the most serious complications ofspinal metastasis. Sato (1988) [2] created an experimental
M. Takahashi et al. / The Spine Journal 4 (2004) 675–680678
Fig. 3. Incomplete paraplegia. The morphology of grey matter was comparatively maintained. There was very little collapse of Nissl bodies compared withcomplete paraplegia. (A) H-E × 10. (B) K and B × 20. (C) K and B × 100.
model by transplanting mammary carcinoma cells into thelumbar spine and reported that 32 (64%) of the rats that theyused developed paraplegia. Fujita et al. (1998) [3] modeledmultiple spinal metastasis in mice by injecting neoplasticcells into the left ventricle of the heart. We transplantedVX2 carcinoma into a pedicle of the third lumbar vertebraeof rabbits and found that 22 (60%) of them had developedparaplegia at the final examination. Twenty-two (60%) ofthe 37 rabbits developed complete or incomplete paraplegia,and the other 15 died before developing paraplegia. Onerabbit (2.7%) had evidence of local infection. One of thecharacteristics of VX2 carcinoma is a high rate of lungmetastasis. The rabbits that did not develop paraplegia werethought to have died of lung metastasis before the para-plegia developed.
Our model shows that metastatic lesions invade from thepedicle to the vertebral body, then to the lamina and finallyto the spinal canal. However, the tumor cells never invadedthe dura and intradural space. The findings in this modelare similar to the localization of tumor and X-ray findings inhumans with spinal metastatic tumors. We therefore considerthis animal model to be a good model of the paraplegia bymeans of solitary metastatic spinal tumors in humans.
Table 2Histological and microangiographic findings
Compression Tumor cells Morphology ofStage of cord invasion grey matter Nissl bodies
Incomplete Moderate None Maintain Maintainparaplegia
Complete Severe None Collapse Collapseparaplegia
Importance has generally been attached to compressivefactors, such as space-occupying tumors, compression frac-tures and unstable vertebrae, as causes of spinal paraplegia,but recently circulatory disturbances in the spinal cord havebeen attracting attention as a cause of paraplegia [14]. Mi-croangiography in our study showed a marked decrease inthe number of vessels in the grey matter in complete paraple-gia. The grey matter is supplied by the central artery ofbranches of the anterior spinal artery, and the white matter bythe coronal artery and posterior spinal artery [15]. Therewas a relation with the closer obstacle of anterior spinalartery about advance of paraplegia. This finding supportsBingham’s conclusion that the blood flow in the white matteris maintained after spinal injuries [16].
Because a rabbit cannot stand and walk by only posteriorextremities, it does not require load for the spinal column.Therefore, evaluation of spinal instability is one of the futurebig subjects.
Conclusions
The animal model of spinal tumors created by transplanta-tion of VX2 carcinoma is generally consistent with spinaltumors of humans in terms of tumor location and X-rayfindings. The tumor cells did not invade the dura and intra-dural space. Our model was useful in elucidating the patho-genetic mechanism of the paraplegia caused by spinal
�
Fig. 4. Complete paraplegia. The tumor enclosed dura mater and waspressing it strongly. The morphology of grey matter and Nissl bodies col-lapsed. There was no invaded cell of tumor in dura mater and spinal cordin both paraplegia. (A) H-E × 10. (B) K and B × 20. (C) K and B × 100.
M. Takahashi et al. / The Spine Journal 4 (2004) 675–680 679
Fig. 5. Microangiography. (Top) In incomplete paraplegia, the number ofthe blood vessels and the morphology in the grey matter were comparativelymaintained. (Bottom) In complete paraplegia, the morphology of grey mattercollapsed. Although the number of blood vessels in the spinal cord wasdecreasing on the whole, the reduction in grey matter was especially remark-able. × 20
tumors. In the animals that developed complete paraplegia,the number of the blood vessels in the spinal cord decreasedas a whole, and the reduction was especially marked in thegrey matter. We concluded that the paraplegia was causedby both direct compression and the decrease in microcircula-tion in the spinal cord.
References
[1] Barron KD, Hirano A, Araki S. Experiences with metastatic neoplasmsinvolving the spinal cord. Neurology 1959;9:91–106.
[2] Sato E. Mechanism of spinal paraplegia due to experimental spinaltumor. J Nihon Univ Med Assoc 1988;47:469–79.
[3] Fujita T, Kawahara N, Ueda Y, Tomita K. Local extension of malignantvertebral tumor for spinal canal. J Jpn Orthop Assoc 1998;72:405.
[4] Komatsu T. An experimental study of chemoembolization for VX2bone tumors. J Jpn Orthop Assoc 1995;69:30–42.
[5] Yamaguchi H, Mochizuki K, Ishii Y. Experimental study of chemicalembolus therapy with radiotherapy for VX2 bone tumors. Int J ClinOncol 2000;5:386–94.

M. Takahashi et al. / The Spine Journal 4 (2004) 675–680680
[6] Hirata I. Chemical embolus therapy combined with hyperthermia forVX2 bone tumors in rabbits. J Kyorin Med Soc 2001;32:409–15.
[7] Wang HM, Crank S, Oliver G, Galasko CS. The effect of methotrexte-loaded bone cement on local destruction by the VX2 tumor. J Bone JointSurg (Br) 1996;78:14–7.
[8] Kato A, Ushio Y, Hayakawa T, Yamada K, Ikeda H, Mogami H.Circulatory disturbance of the spinal cord with epidural neoplasmin rats. J Neurosurg 1985;63:260–5.
[9] Tomita K, Kawahara N. Surgical treatment of spinal metastasis—withspecial emphasis to posterior total spondylectomy. Rinsyo Seikei Geka1992;27:481–90.
[10] Kluver H, Barrera E. A method for the combined staining of cells andfibers in the nervous system. J Neuropath Exp Neurol 1953;12:400–6.
Fifty YearsAgo in Spine
Results of experiments by Tarlov et al.[1,2], published in 1953 and 1954, in which spinal cordinjury in dogs was produced by acute and gradual pro-gression and outcomes correlated with duration of the
[11] Tanaka H, Kurokawa T, Seki H. Microangiogram injected with Indiaink and scanning electron microscope study of corrosion casts ofcapillary vessels. Seikeigeka 1980;31:929–34.
[12] Onur O, Spira M, Levy B. Microangiography: a detailed techniqueof perfusion. J Surg Res 1980;29:406–13.
[13] Kotani M, Tanaka J. Postmortem microangiographic studies on acuteandchroniccervical cord injuries. JYonagoMed Assoc 1983;34:511–8.
[14] Muroya M, Sakou T, Gotoh M, Nakamura T. Three autopsy cases ofmetastatic spinal tumor complicated by complete spinal paraplegia.Spine and spinal cord 1993;3:257–60.
[15] Goto N, Ito J, Shiraishi N. Anatomy of the spinal vascular system.Spine and spinal cord 1993;6:35–9.
[16] Bingham WG. Blood flow in normal and injured monkey spinalcord. J Neurosurg 1975;43:162–71.
compression, contributed to understanding of mecha-nisms of spinal cord injury from trauma and from 1
spondylosis. 1
References 1
[1] Tarlov IM, Klinger H, Vitale S. Spinal cord compression studies: I. 1Experimental techniques to produce acute and gradual compres- 1sion. Arch Neurol Psychiatry 1953;70:813–9. 1
[2] Tarlov IM, Klinger H. Spinal cord compression studies: II. Time 1limits for recovery after acute compression in dogs. Arch Neurol 1Psychiatry 1954;71:271–90. 1
本文献由“学霸图书馆-文献云下载”收集自网络,仅供学习交流使用。
学霸图书馆(www.xuebalib.com)是一个“整合众多图书馆数据库资源,
提供一站式文献检索和下载服务”的24 小时在线不限IP
图书馆。
图书馆致力于便利、促进学习与科研,提供最强文献下载服务。
图书馆导航:
图书馆首页 文献云下载 图书馆入口 外文数据库大全 疑难文献辅助工具