extra-corporal shockwave lithotripsy - for urolithiasis dr. chan shu yin eddie urology division,...
TRANSCRIPT

Extra-corporal Shockwave Lithotripsy- for Urolithiasis
Dr. Chan Shu Yin EddieDr. Chan Shu Yin EddieUrology Division, Department of Urology Division, Department of SurgerySurgeryPYNEHPYNEH

Agenda
History and basic principle of ESWL
Challenges and Complications of ESWL
Take home messages

ESWLESWL
Easy, simple, thing thatnothing need to learn
REALLY???REALLY???


History of ESWL
1951 SW for treatment of brain tumours 1971 in-vitro disintegration of kidney stones 1974 in-vivo trials 10/1983 1st ESWL machine HM3 installed 1984 FDA approval 1991 1st ESWL machine in HA hospital

Components of ESWL Machine
Generator & focusing system Electrohydraulic Electromagnetic Piezoelectric
Coupling mechanism Water Bath Semi-water Bath Water Cushion
Localization system Fluoroscopy vs. Ultra-sonography

HM3 machine

The New Generation ESWL Machine Principles of shockwave generation Focusing system Coupling Localization
Aim as low cost, pain-free application, multifunctional use and easy handling

Lithostar
“The cellular phone… was introduced in 1984, the same year as the Dornier HM3 lithotriptor, an equally revolutionary device from a medical technology perspective. Cellular phone initially weighted in excess of 2 pounds…weigh as little as 2 ounces today.
The last 15 years of lithotriptor technology have been a disappointment.”
Dr. J. Lingeman
ESWL – Challenges
When to use ESWL?
Management of post-ESWL complications

Case 1
Good case for ESWL?
BMI = 49

Ureteric Stone
Rate of spontaneous passage
ESWL is unnecessary for small uncomplicated ureteric stones
≤ 5mm 5 – 10 mm
% proximal ureteric
29 – 98 % 10 – 53 %
% distal ureteric 71 – 98 % 25 – 53 %
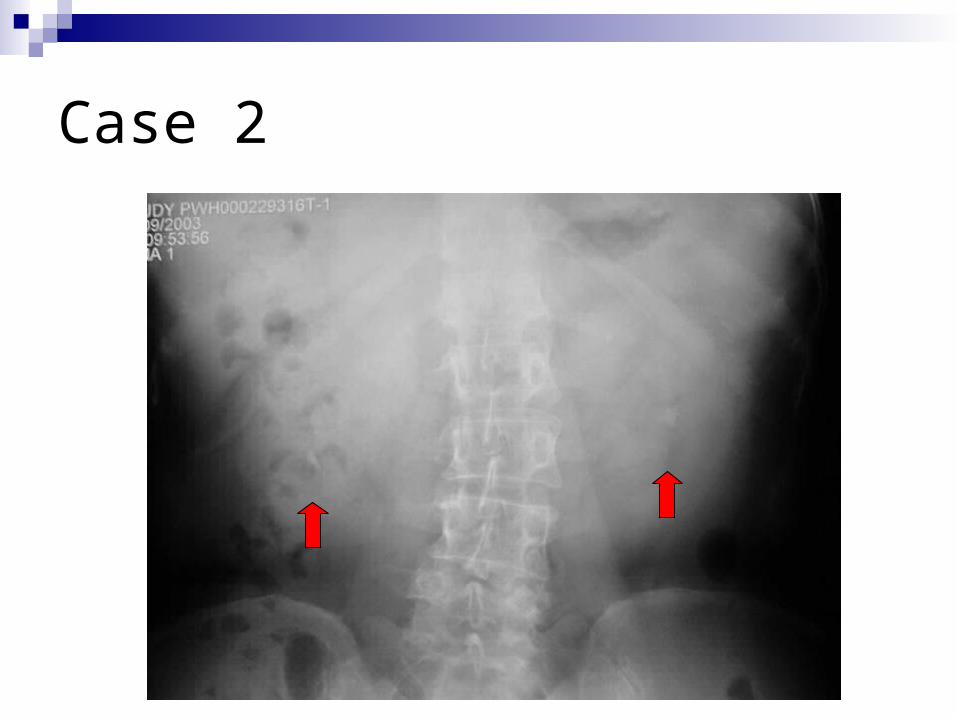
Case 2
ESWL vs. Observation: Outcome for small asymptomatic calyceal stone <15mm 228 patients
200 available for FU, mean 2.2 yr (1-5 yr)
SWL 28% stone-free 15% additional Rx OBS 17% stone-free 21% additional Rx
p = 0.06 p=0.27
No difference in outcome
Bristol Urological Institutes, BJU 2001;87,1-8

ESWL - Complications
Complications of anaesthesia or sedation / antibiotics
1% clinical significant haematoma 5-25% pain due to stone fragments
passage 2-6% stone obstruction – steinstrasse Hypertension – unknown long-term effects

Perinephric Haematoma

Perinephric Haematoma Occurrence
Radiologically 20-25% Clinical significant - < 1% Risk factors
HT Uncontrolled coagulopathy NSAID Obesity UTI Bilateral treatment Lithotriptor model – larger peak pressure and smaller focal
zone

Case 3
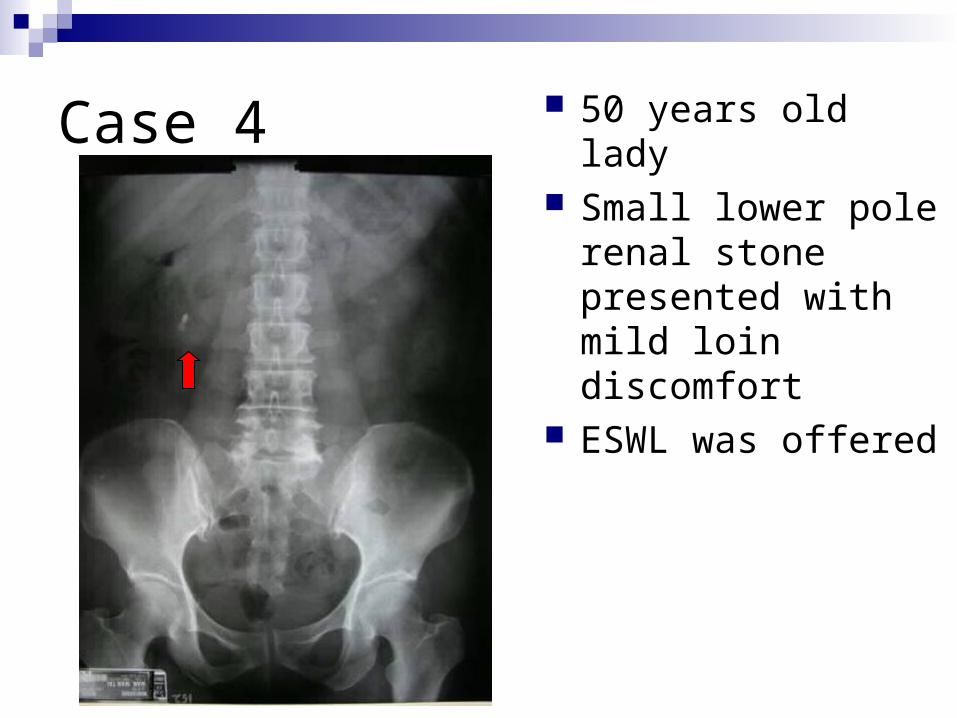
Case 4 50 years old lady Small lower pole renal
stone presented with mild loin discomfort
ESWL was offered
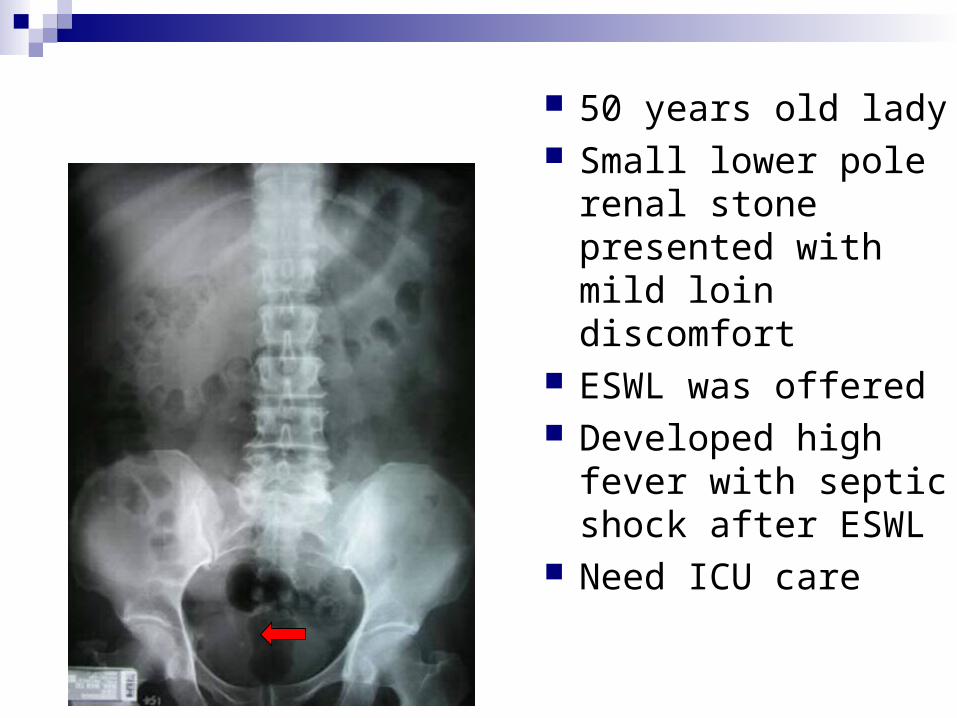
50 years old lady Small lower pole renal
stone presented with mild loin discomfort
ESWL was offered Developed high fever
with septic shock after ESWL
Need ICU care
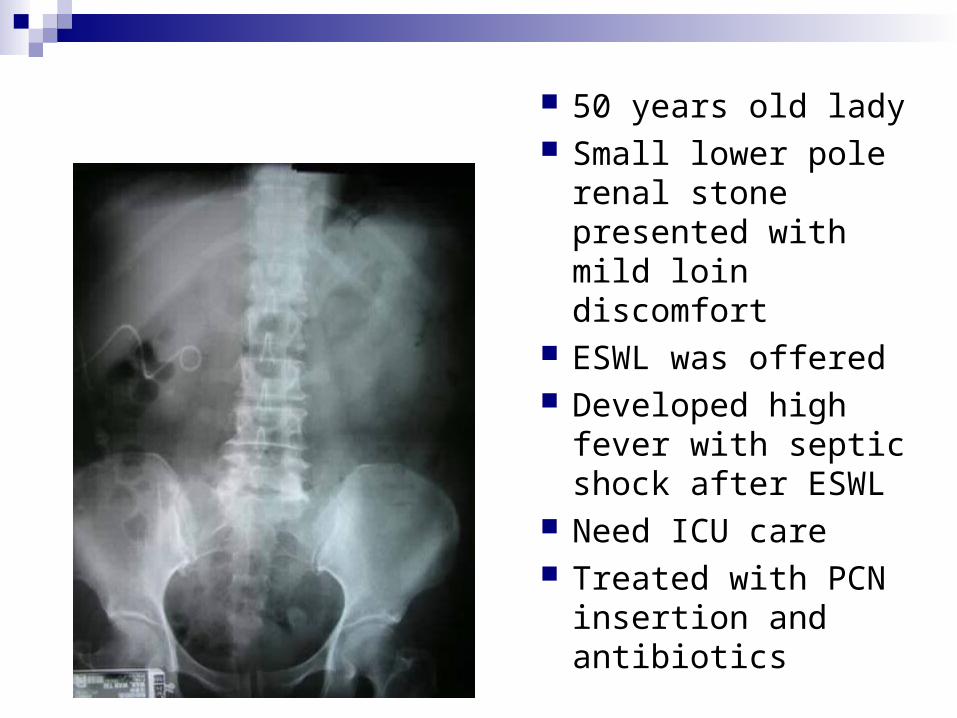
50 years old lady Small lower pole renal
stone presented with mild loin discomfort
ESWL was offered Developed high fever
with septic shock after ESWL
Need ICU care Treated with PCN
insertion and antibiotics

Take Home messages
Stone management can be difficult. ESWL should not be considered as a treatment modality in isolation and must not be abused.
Complications of ESWL are not very common but may lead to major morbidity.
Complications can be silent and delayed in picking up