eye health knowledge of early childhood and classroom
TRANSCRIPT
Turk J Public Health 2019;17(2):169-182 Available online at: http://dergipark.gov.tr/tjph doi: 10.20518/tjph.429035
Research Article
Copyright holder Turkish Journal of Public Health
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This is an open Access article which can be used if cited properly.
Turk J Public Health 2019;17(2) 169
Eye health knowledge of early childhood and classroom education departments’ students: A
descriptive study from Turkey Mohammad Haris Abdianwall a, Bahar Güçiz Doğan b
a MD, Clinical Ophthalmologist, MSc, PhD., Hacettepe University Institute of Public Health, Ankara, Turkey
b Prof, MSc, PhD., Hacettepe University Faculty of Medicine, Dept. of Public Health, Ankara, Turkey
Submitted date: 01.05.2018, Accepted date: 25.02.2019
Abstract
Objective: The aim of this study was to determine the knowledge of students and increase awareness regarding eye health in an Education Faculty in Ankara, Turkey. Method: The population of this descriptive study (n=330; response rate 76.1%) was third and fourth year students of Early Childhood Education (n=130) and Classroom Education (n=200) Departments in 2016-2017 Spring Semester. Data were collected via a structured, pre-tested, self-administered 34-question questionnaire. Ethical permission was obtained from Hacettepe University Non-Interventional Clinical Research Ethics Board as well as verbal consent of the students. Data were analyzed using SPSS version 21.0; descriptive statistics were presented with numbers and percentages; Chi-square test was used to detect the difference between categorical variables; the level of significance was considered as p-value <0.05. Results: Of the students, 89.2% were female and 64.9% were from the Classroom Education Department. The majority of the participants knew the situations with high probability of eye trauma, causes of visual impairment, indicators of visual impairment and recommendations for prevention of eye health. However, a considerable number did not know suitable practices about characteristics of disordered eyes and first aid for eye trauma. Conclusion: In conclusion, knowledge of the students was not satisfactory in general and developing the eye health education program in the curriculum was recommended.
Key words: Knowledge, eye health, early childhood education, classroom education, students.
Corresponding Author: Mohammad Haris Abdianwall, Hacettepe University Institute of Public Health, 06100, Ankara, Turkey, E-mail: [email protected], Tel: +90.507.545 1008
Eye health knowledge
Turk J Public Health 2019;17(2) 170
Eğitim Fakültesi Okul Öncesi ve Sınıf Eğitimi Bölümleri öğrencilerinin göz sağlığı
konusundaki bilgileri:
Türkiye’den tanımlayıcı tipte bir çalışma
Özet
Amaç: Bu çalışma, Ankara’da bulunan bir üniversitenin Eğitim Fakültesi Okul Öncesi ve Sınıf Eğitimi Bölümleri üçüncü ve dördüncü sınıf öğrencilerinin göz sağlığı konusundaki bilgilerini saptamak ve öğrencilerin konu hakkındaki farkındalıklarını artırmak amacıyla planlanmış ve uygulanmıştır. Yöntem: Tanımlayıcı bir epidemiyolojik araştırma olan çalışmaya adı geçen fakültede 2016-2017 Bahar Döneminde okuyan Okul Öncesi Eğitimi Bölümü’nden 130, Sınıf Eğitimi Bölümü’nden 200 olmak üzere toplam 330 kişi katılmıştır (yanıtlama yüzdesi %76.1). Veriler yapılandırılmış, ön testi yapılmış, kendi kendine doldurma şeklinde uygulanan 34 soruluk bir anket formu ile toplanmıştır. Veri toplama öncesi Hacettepe Girişimsel Olmayan Klinik Araştırmalar Etik Kurulu izni ve katılımcıların sözlü onamları alınmıştır. Veriler SPSS 21.0 kullanılarak analiz edilmiş, tanımlayıcı istatistikler sayı ve yüzdeler olarak gösterilmiştir. Kategorik değişkenler arasında gözlenen farkların anlamlı olup olmadığını değerlendirmek için Ki-kare testi kullanılmış, anlamlılık düzeyi olarak p değeri <0.05 kabul edilmiştir. Bulgular: Araştırmaya katılan öğrencilerin %89.2’si kadındır; %64.9’u Sınıf Eğitimi Bölümü’nde okumaktadır. Katılımcıların büyük bölümü göz travması olma olasılığı olan durumları, görme bozukluğu nedenlerini ve göz sağlığını korumak için önerilenleri bilmektedirler. Ancak kayda değer bir bölümünün bozuk gözün özelliklerini ve gözde bir travma durumunda ilk yardım önlemlerini bilmedikleri belirlenmiştir. Sonuç: Sonuç olarak, genel olarak öğrencilerin göz sağlığı konusundaki bilgileri tatmin edici düzeyde değildir; öğretim programı içinde göz sağlığına ilişkin bir eğitim programının geliştirilmesi önerilmiştir.
Anahtar kelimeler: Bilgi, göz sağlığı, okul öncesi eğitim, sınıf eğitimi, öğrenci
Introduction
Worldwide, 285 million people are estimated to be visually impaired, 39 million are blind and 246 have low vision. Of these people, 19 million are children below the age of 15; 12 million are visually impaired because of uncorrected refractive error, which is easily diagnosed and corrected, and 1.4 million are irreversibly blind and need visual rehabilitation interventions.1,2 Almost three-quarters of the blind children live in the poorest regions of Asia and Africa.3 Childhood blindness refers to a group of diseases and conditions occurring in childhood, which, if not treated at a proper time, may result in
severe visual impairment or blindness which are likely to be untreatable in later life3. In low-income countries, the prevalence of childhood blindness may be as high as 1.5 per 1000 children, while in high-income countries, it is around 0.3 per 1000 children.4,5 Emotional, social and economic impacts of childhood blindness to the child, family and society is more than adult onset blindness as blind children have a lifetime of blindness ahead of them.4
In high income countries, the causes of blindness were determined as lesions of the optic nerve and higher visual pathways, while in low income countries, corneal scarring from

Eye health knowledge
Turk J Public Health 2019;17(2) 171
measles, vitamin A deficiency, and the use of harmful traditional eye remedies along with ophthalmia neonatorum, and rubella cataract are the major causes. At the same time, retinopathy of prematurity is an important cause in middle-income countries. Other significant causes in all countries are congenital abnormalities, such as cataract, glaucoma, and hereditary retinal dystrophies.4
A study which was conducted in Izmir-Turkey indicated that in 69.6% of the patients, the causes of visual impairment were considered either preventable or treatable, including cataract, retinopathy of prematurity (ROP), genetic disorders, and uncorrected refractive error(s).6 The prevalence of uncorrected refractive error(s) was found to be between 12.2% and 50.1% in various studies conducted within the scope of school health screening in Ankara, the capital city of Turkey from 2000 to 2017.7-13 Ocular trauma is, on the other hand, a leading cause of non-congenital unilateral blindness among children under 20 years old in this country.14
Interventions are available for most causes of childhood blindness. These are most effective if carried out together with school health programs, having positive externalities for not only the children but also their families and communities.15 Educational achievement, quality of life, social interactions and economic productivity are closely associated with school health programs including eye health. In order to fully benefit from education, students’ health is fundamental and must be guaranteed in school settings. Health education allows them to acquire knowledge, attitudes and practices necessary for a healthy life. School eye health programs should be comprehensive and based on the local and regional prevalent common eye conditions and diseases16.
The prevalence of uncorrected refractive error is high in different parts of Turkey and school screenings were found to be the most cost-effective program for the detection and treatment of uncorrected refractive error among school children17.
Therefore, school eye health programs are required to be undertaken in schools. In the schools, teachers are playing more significant roles in detection and referral of students with probable eye problems as well as monitoring spectacle use. In order to perform these roles correctly and timely, teachers must obtain these abilities (knowledge and skills) during their undergraduate training and keep them updated through their professional lives. Therefore, this study was designed to determine the eye health knowledge of the third and fourth grade students of Early Childhood and Classroom Education Departments in an Education Faculty of a University in Ankara, Turkey and increase awareness among them about eye health.
Material and Method
This descriptive study was carried out at Early Childhood and Classroom Education Departments of an Education Faculty located in the capital city of Turkey, Ankara.
The universe consisted of third and fourth year students (n=330) studying in Early Childhood and Classroom Education Departments of a university in 2016-2017, Spring Semester. In the Early Childhood Education Department, n= 130 students were studying (72; 55.4% were studying in third class and 58; 44.6% in fourth class). In the Classroom Education Department, there were 200 students (90; 45.0% were in third class and 110; 55.0% in fourth class). It was aimed to reach the entire universe n=330; however, 251 students (76.1%) participated, 88(67.7%) from Early Childhood Education and 163 (81.5%) from Classroom Education students.
The data were collected via a structured, pre-tested, self-administered questionnaire developed by the researchers in which questions related to some socio-demographic characteristics and questions for assessing the knowledge of the participants in reference to eye health of the children in school were included (34 questions in total). The first 12 (35.3%) questions were related to

Eye health knowledge
Turk J Public Health 2019;17(2) 172
socio-demographic characteristics of the students including their parent’s professions and income. These questions were either multiple choice or open ended in type. The remaining 22 (64.7%) questions were related to eye health and these questions were true-false, open ended and multiple choice.
The survey forms were distributed to the students at the relevant lecture time with the attendance of the researcher. Ethical permission was obtained from Non-Interventional Clinical Researches Ethical Board of Hacettepe University, and permission for data collection was obtained from the Directorate of the Education Faculty. Moreover, the aim and objectives of the study and the procedure were explained to the students before the distribution of the questionnaires, and verbal consent was obtained. Participation in the study was voluntary.
Data were analyzed by using IBM SPSS Statistics 21.0 software program. Descriptive statistics of the variables were presented with numbers (n) and percentages (%). Chi square test was used to observe the difference between categorical variables. The findings were presented in marginal and contingency tables; p-value less than 0.05 considered as statistically significant.
Results
Of the participants, 224 (89.2%) were female; 163 (64.9%) were Classroom and 88 (35.1%) were Early Childhood Department students. Among Classroom Education participants (n=163), 59.5% were in fourth grade; 85.9% were female; 96.9% had at least one sibling; 1.8% were currently married; 63.8% had employed fathers and 11.0% had employed mothers. The related figures for the Early Childhood Education students (n=88) were 40.9%; 95.5%; 96.6%; 2.3%; 54.5%, and 12.5%, respectively.
Five participants (2.0%) reported that they had experienced eye trauma and 4.4%
(n= 11) stated that they had witnessed a person nearby sustain an eye trauma. Regarding the objects that caused trauma in the eye, ‘oil’, ‘pencil’, ‘ball’, ‘knife’, ‘elbow’, ‘garbage’, ‘hot particles of iron’, ‘fist’, ‘stone’, and “bullet of toy gun” have been mentioned by the participants in different proportions.
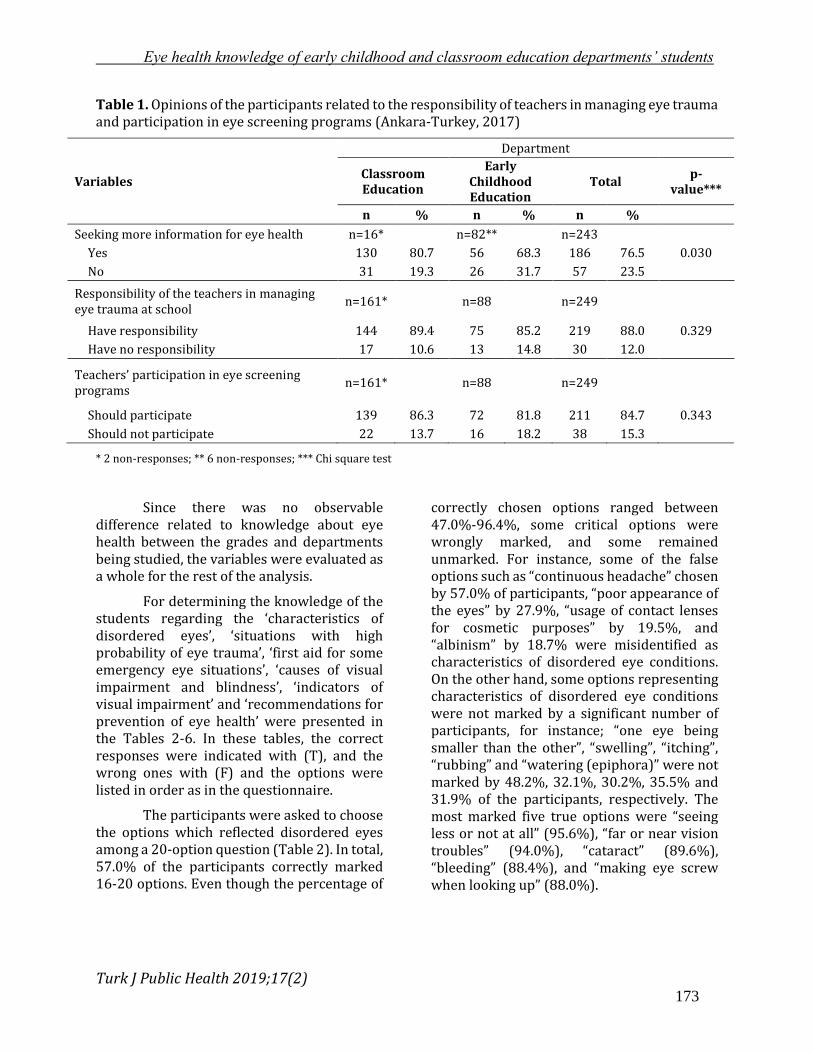
Of the participants, 76.5% reported that they need more information regarding eye health; the proportion was higher among participants from Classroom Education (80.7%) than Early Childhood Education (68.3%) (p=0.030) (Table 1). In response to the type of information, 33.6% demanded information about eye health and injuries, 32.8% about first aid in eye trauma or injury, 11.7% about eye diseases and 10.2% about general health.
84.7% of the participants thought that teachers were responsible for managing the eye trauma of the children occurred at school and this proportion was similarly distributed among Classroom Education (89.4%) and Early Childhood Education (85.2%) students (p=0.329). In response to the type of responsibility, 75.7% of the participants mentioned “first aid” and “transferring the child to the nearest health care center”, 8.1% “prevention of eye trauma and injury”, and 8.1% “giving information related to eye trauma to the students”. The need for the participation of teachers in eye screening programs was reported by 84.7% of the participants (86.3% in Classroom Education students and 81.8% Early Childhood Students; p=0.343). Reasons stated by 22 students who thought that teachers should not be required to participate in eye screening programs were: ‘teachers are not health personnel’ (50.0%), ‘teachers do not have enough information’ (47.4%) and ‘there is high work burden on the teachers’ (2.6%).
Eye health knowledge of early childhood and classroom education departments’ students
Turk J Public Health 2019;17(2) 173
Table 1. Opinions of the participants related to the responsibility of teachers in managing eye trauma and participation in eye screening programs (Ankara-Turkey, 2017)
Department
Variables Classroom Education
Early Childhood Education
Total p-
value***
n % n % n %
Seeking more information for eye health n=16* n=82** n=243
Yes 130 80.7 56 68.3 186 76.5 0.030
No 31 19.3 26 31.7 57 23.5
Responsibility of the teachers in managing eye trauma at school
n=161* n=88 n=249
Have responsibility 144 89.4 75 85.2 219 88.0 0.329
Have no responsibility 17 10.6 13 14.8 30 12.0
Teachers’ participation in eye screening programs
n=161* n=88 n=249
Should participate 139 86.3 72 81.8 211 84.7 0.343
Should not participate 22 13.7 16 18.2 38 15.3
* 2 non-responses; ** 6 non-responses; *** Chi square test
Since there was no observable difference related to knowledge about eye health between the grades and departments being studied, the variables were evaluated as a whole for the rest of the analysis.
For determining the knowledge of the students regarding the ‘characteristics of disordered eyes’, ‘situations with high probability of eye trauma’, ‘first aid for some emergency eye situations’, ‘causes of visual impairment and blindness’, ‘indicators of visual impairment’ and ‘recommendations for prevention of eye health’ were presented in the Tables 2-6. In these tables, the correct responses were indicated with (T), and the wrong ones with (F) and the options were listed in order as in the questionnaire.
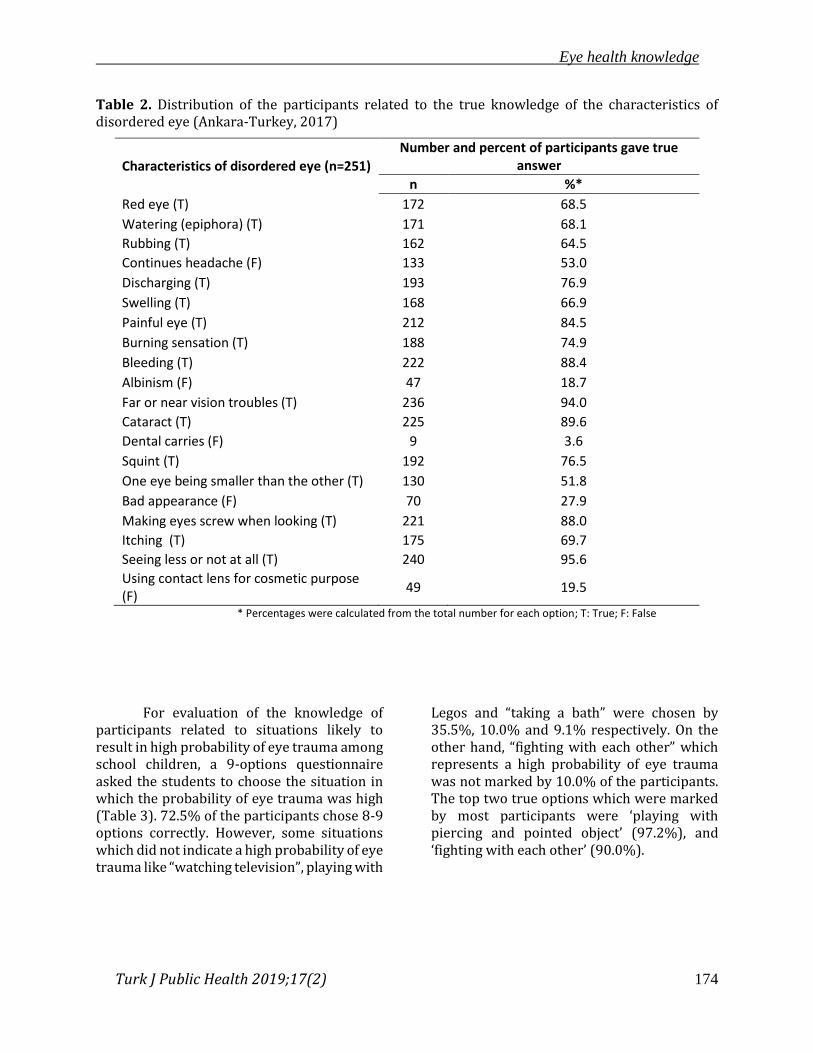
The participants were asked to choose the options which reflected disordered eyes among a 20-option question (Table 2). In total, 57.0% of the participants correctly marked 16-20 options. Even though the percentage of
correctly chosen options ranged between 47.0%-96.4%, some critical options were wrongly marked, and some remained unmarked. For instance, some of the false options such as “continuous headache” chosen by 57.0% of participants, “poor appearance of the eyes” by 27.9%, “usage of contact lenses for cosmetic purposes” by 19.5%, and “albinism” by 18.7% were misidentified as characteristics of disordered eye conditions. On the other hand, some options representing characteristics of disordered eye conditions were not marked by a significant number of participants, for instance; “one eye being smaller than the other”, “swelling”, “itching”, “rubbing” and “watering (epiphora)” were not marked by 48.2%, 32.1%, 30.2%, 35.5% and 31.9% of the participants, respectively. The most marked five true options were “seeing less or not at all” (95.6%), “far or near vision troubles” (94.0%), “cataract” (89.6%), “bleeding” (88.4%), and “making eye screw when looking up” (88.0%).
Eye health knowledge
Turk J Public Health 2019;17(2) 174
Table 2. Distribution of the participants related to the true knowledge of the characteristics of disordered eye (Ankara-Turkey, 2017)
Characteristics of disordered eye (n=251)
Number and percent of participants gave true answer
n %*
Red eye (T) 172 68.5
Watering (epiphora) (T) 171 68.1
Rubbing (T) 162 64.5
Continues headache (F) 133 53.0
Discharging (T) 193 76.9
Swelling (T) 168 66.9
Painful eye (T) 212 84.5
Burning sensation (T) 188 74.9
Bleeding (T) 222 88.4
Albinism (F) 47 18.7
Far or near vision troubles (T) 236 94.0
Cataract (T) 225 89.6
Dental carries (F) 9 3.6
Squint (T) 192 76.5
One eye being smaller than the other (T) 130 51.8
Bad appearance (F) 70 27.9
Making eyes screw when looking (T) 221 88.0
Itching (T) 175 69.7
Seeing less or not at all (T) 240 95.6
Using contact lens for cosmetic purpose (F)
49 19.5
* Percentages were calculated from the total number for each option; T: True; F: False
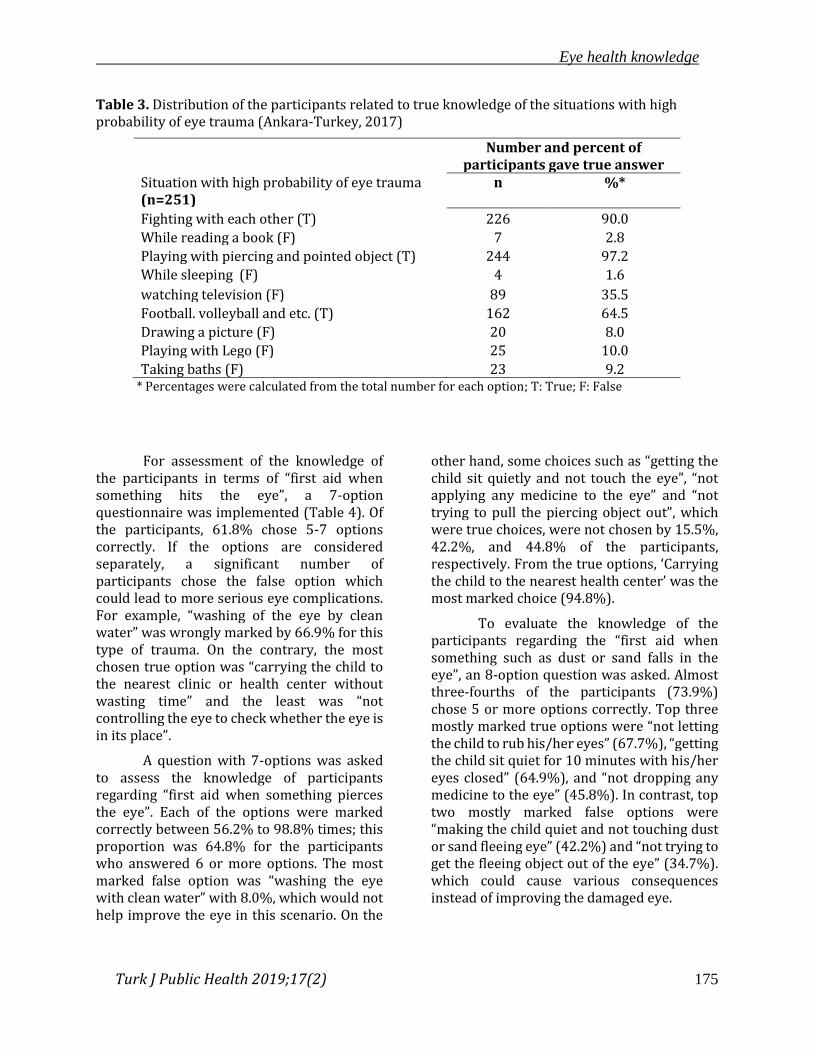
For evaluation of the knowledge of participants related to situations likely to result in high probability of eye trauma among school children, a 9-options questionnaire asked the students to choose the situation in which the probability of eye trauma was high (Table 3). 72.5% of the participants chose 8-9 options correctly. However, some situations which did not indicate a high probability of eye trauma like “watching television”, playing with
Legos and “taking a bath” were chosen by 35.5%, 10.0% and 9.1% respectively. On the other hand, “fighting with each other” which represents a high probability of eye trauma was not marked by 10.0% of the participants. The top two true options which were marked by most participants were ‘playing with piercing and pointed object’ (97.2%), and ‘fighting with each other’ (90.0%).
Eye health knowledge
Turk J Public Health 2019;17(2) 175
Table 3. Distribution of the participants related to true knowledge of the situations with high probability of eye trauma (Ankara-Turkey, 2017)
Situation with high probability of eye trauma (n=251)
Number and percent of participants gave true answer
n
%*
Fighting with each other (T) 226 90.0
While reading a book (F) 7 2.8
Playing with piercing and pointed object (T) 244 97.2
While sleeping (F) 4 1.6
watching television (F) 89 35.5
Football. volleyball and etc. (T) 162 64.5
Drawing a picture (F) 20 8.0
Playing with Lego (F) 25 10.0
Taking baths (F) 23 9.2 * Percentages were calculated from the total number for each option; T: True; F: False
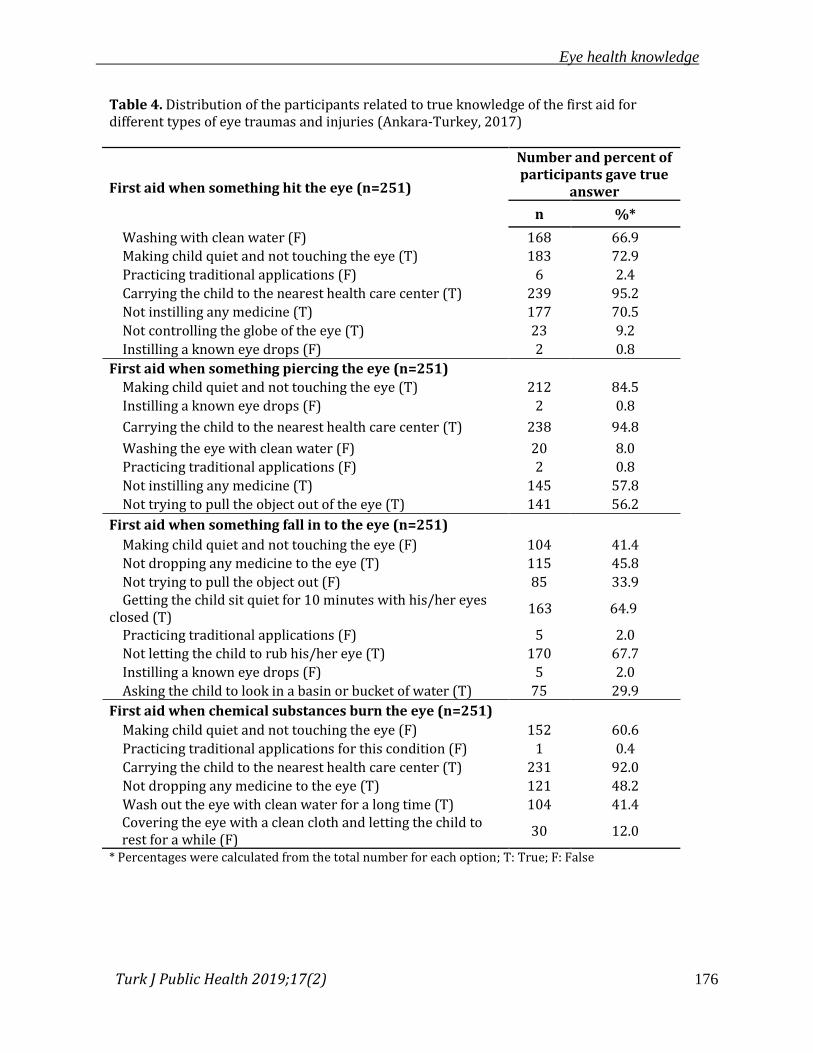
For assessment of the knowledge of the participants in terms of “first aid when something hits the eye”, a 7-option questionnaire was implemented (Table 4). Of the participants, 61.8% chose 5-7 options correctly. If the options are considered separately, a significant number of participants chose the false option which could lead to more serious eye complications. For example, “washing of the eye by clean water” was wrongly marked by 66.9% for this type of trauma. On the contrary, the most chosen true option was “carrying the child to the nearest clinic or health center without wasting time” and the least was “not controlling the eye to check whether the eye is in its place”.
A question with 7-options was asked to assess the knowledge of participants regarding “first aid when something pierces the eye”. Each of the options were marked correctly between 56.2% to 98.8% times; this proportion was 64.8% for the participants who answered 6 or more options. The most marked false option was “washing the eye with clean water” with 8.0%, which would not help improve the eye in this scenario. On the
other hand, some choices such as “getting the child sit quietly and not touch the eye”, “not applying any medicine to the eye” and “not trying to pull the piercing object out”, which were true choices, were not chosen by 15.5%, 42.2%, and 44.8% of the participants, respectively. From the true options, ‘Carrying the child to the nearest health center’ was the most marked choice (94.8%).
To evaluate the knowledge of the participants regarding the “first aid when something such as dust or sand falls in the eye”, an 8-option question was asked. Almost three-fourths of the participants (73.9%) chose 5 or more options correctly. Top three mostly marked true options were “not letting the child to rub his/her eyes” (67.7%), “getting the child sit quiet for 10 minutes with his/her eyes closed” (64.9%), and “not dropping any medicine to the eye” (45.8%). In contrast, top two mostly marked false options were “making the child quiet and not touching dust or sand fleeing eye” (42.2%) and “not trying to get the fleeing object out of the eye” (34.7%). which could cause various consequences instead of improving the damaged eye.
Eye health knowledge
Turk J Public Health 2019;17(2) 176
Table 4. Distribution of the participants related to true knowledge of the first aid for different types of eye traumas and injuries (Ankara-Turkey, 2017)
First aid when something hit the eye (n=251)
Number and percent of participants gave true
answer
n %*
Washing with clean water (F) 168 66.9
Making child quiet and not touching the eye (T) 183 72.9
Practicing traditional applications (F) 6 2.4
Carrying the child to the nearest health care center (T) 239 95.2
Not instilling any medicine (T) 177 70.5
Not controlling the globe of the eye (T) 23 9.2
Instilling a known eye drops (F) 2 0.8
First aid when something piercing the eye (n=251)
Making child quiet and not touching the eye (T) 212 84.5
Instilling a known eye drops (F) 2 0.8
Carrying the child to the nearest health care center (T) 238 94.8
Washing the eye with clean water (F) 20 8.0
Practicing traditional applications (F) 2 0.8
Not instilling any medicine (T) 145 57.8
Not trying to pull the object out of the eye (T) 141 56.2
First aid when something fall in to the eye (n=251)
Making child quiet and not touching the eye (F) 104 41.4
Not dropping any medicine to the eye (T) 115 45.8
Not trying to pull the object out (F) 85 33.9 Getting the child sit quiet for 10 minutes with his/her eyes
closed (T) 163 64.9
Practicing traditional applications (F) 5 2.0
Not letting the child to rub his/her eye (T) 170 67.7
Instilling a known eye drops (F) 5 2.0
Asking the child to look in a basin or bucket of water (T) 75 29.9
First aid when chemical substances burn the eye (n=251)
Making child quiet and not touching the eye (F) 152 60.6
Practicing traditional applications for this condition (F) 1 0.4
Carrying the child to the nearest health care center (T) 231 92.0
Not dropping any medicine to the eye (T) 121 48.2
Wash out the eye with clean water for a long time (T) 104 41.4 Covering the eye with a clean cloth and letting the child to rest for a while (F)
30 12.0
* Percentages were calculated from the total number for each option; T: True; F: False

Eye health knowledge
Turk J Public Health 2019;17(2) 177
A question that contained 6 options was asked in order to determine knowledge of the participants related to “first aid when chemical substances burn the eye”. From 39.2% to 99.2% options were chosen correctly. “Not dropping any medicine in the damaged eye” and “washing the eye by clean water for a long period of time” which were true practices for helping to improve eye burnt with chemical substances were not chosen by 51.8% and 58.6% of the participants, respectively. On the other hand, two mostly marked false options were “making the child quiet and not touching the damaged eye” marked (60.8%) and “closing his/her eyes with a clean cloth and letting the child rest for a while” (11.4%). ‘Carrying the child to the nearest health care center’ was the mostly chosen true options which was marked by 92.0% of the participants.
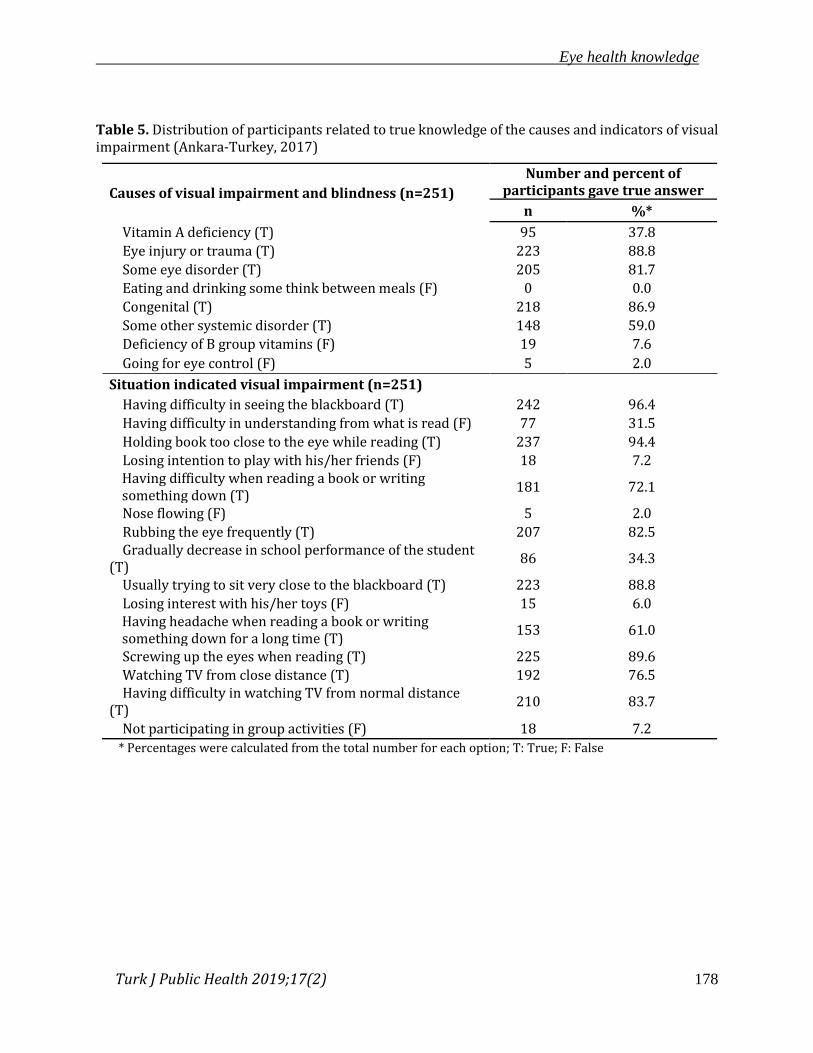
For understanding the knowledge of the participants related to the causes of visual impairment or blindness” among school children, an 8-option question was asked (Table 5). Correctly responded options ranged from 37.8% to 100.0%; 96.4% of the participants marked 4 or more options correctly. “Eye trauma and injury”, “congenital”, and “eye diseases” were the most commonly chosen true options marked correctly by 88.8%, 86.9% and 81.7%, respectively. On the other hand, ‘vitamin A deficiency’ and ‘some systemic diseases’, which were the true options, were not marked by a certain number of participants (62.2% and 41.0% respectively).
For determining the knowledge of participants about situations which indicated visual impairment among school children, a
question containing 15 options was asked. Participants marked each option from 34.3% to 97.2%. All participants chose 5 or more options correctly while only 27.3% of the participants marked 14 or more options correctly. 72.0% of the participants marked eight from ten true options. The options of “having difficulty in seeing the blackboard”, “holding books too close to the eye while reading”, “screwing up the eyes when reading”, “usually trying to sit very close to the blackboard in class” and “rubbing eyes frequently” were the five mostly marked true options by 96.4%, 94.4%, 89.6%, 88.8% and 82.5%, respectively. The option of “having difficulty in understanding from what is read” was the most marked false option with 31.5%.
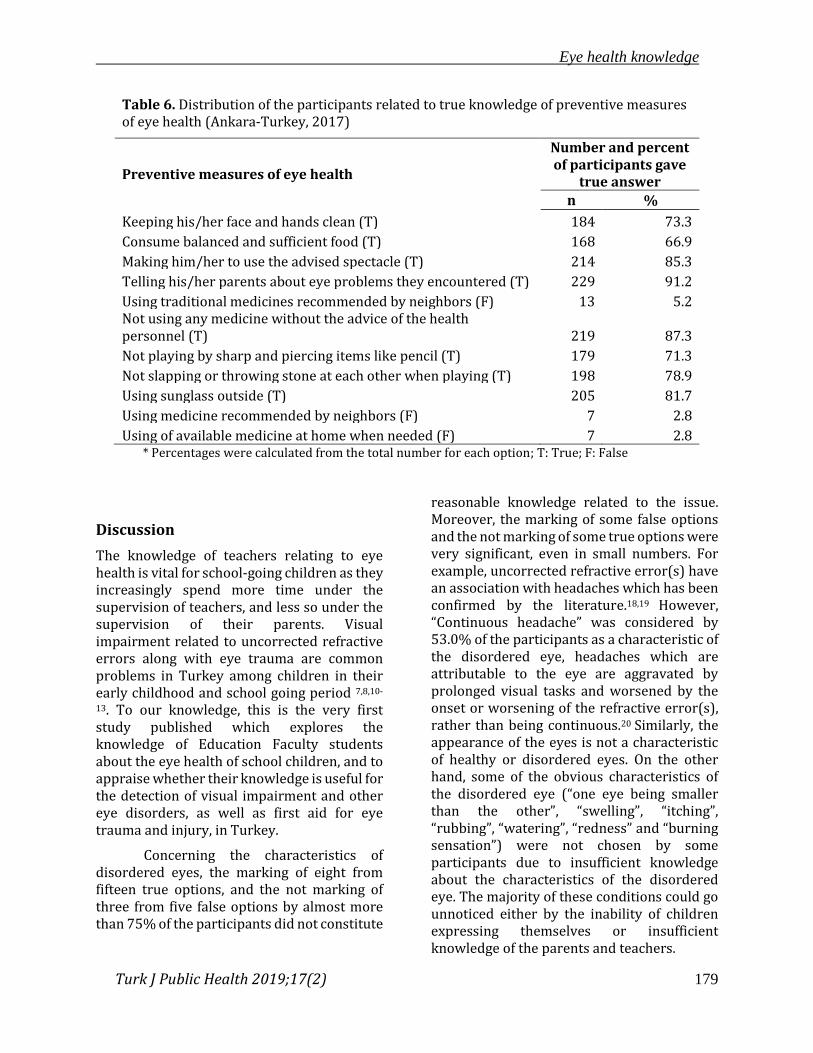
For the assessment of the knowledge of the participants relating to “eye health protection”, an 11-option question was asked (Table 6). Participants correctly responded to each option variously, from 66.9% to 97.2%. In total, seven from eight true options were chosen by approximately more than 70% of the participants. The top mostly marked true options were “telling his/her parents about eye problems” ( 91.2%), “recommending not to use any medicine without the advice of the health personnel” (87.3%), “making him/her to use the advised spectacle” (85.3%), “recommending the use of sunglasses outside” (81.7%) and “not slapping or throwing stones at each other when playing” (78.9%). However, even though it was chosen by a small proportion of the participants (5.2%), the mostly marked false choice was “using traditional medicines recommended by neighbors”.
Eye health knowledge
Turk J Public Health 2019;17(2) 178
Table 5. Distribution of participants related to true knowledge of the causes and indicators of visual impairment (Ankara-Turkey, 2017)
Causes of visual impairment and blindness (n=251)
Number and percent of participants gave true answer
n %*
Vitamin A deficiency (T) 95 37.8
Eye injury or trauma (T) 223 88.8
Some eye disorder (T) 205 81.7
Eating and drinking some think between meals (F) 0 0.0
Congenital (T) 218 86.9
Some other systemic disorder (T) 148 59.0
Deficiency of B group vitamins (F) 19 7.6
Going for eye control (F) 5 2.0
Situation indicated visual impairment (n=251)
Having difficulty in seeing the blackboard (T) 242 96.4
Having difficulty in understanding from what is read (F) 77 31.5
Holding book too close to the eye while reading (T) 237 94.4
Losing intention to play with his/her friends (F) 18 7.2 Having difficulty when reading a book or writing something down (T)
181 72.1
Nose flowing (F) 5 2.0
Rubbing the eye frequently (T) 207 82.5 Gradually decrease in school performance of the student
(T) 86 34.3
Usually trying to sit very close to the blackboard (T) 223 88.8
Losing interest with his/her toys (F) 15 6.0 Having headache when reading a book or writing something down for a long time (T)
153 61.0
Screwing up the eyes when reading (T) 225 89.6
Watching TV from close distance (T) 192 76.5 Having difficulty in watching TV from normal distance
(T) 210 83.7
Not participating in group activities (F) 18 7.2
* Percentages were calculated from the total number for each option; T: True; F: False
Eye health knowledge
Turk J Public Health 2019;17(2) 179
Table 6. Distribution of the participants related to true knowledge of preventive measures of eye health (Ankara-Turkey, 2017)
Preventive measures of eye health
Number and percent of participants gave
true answer
n %
Keeping his/her face and hands clean (T) 184 73.3
Consume balanced and sufficient food (T) 168 66.9
Making him/her to use the advised spectacle (T) 214 85.3
Telling his/her parents about eye problems they encountered (T) 229 91.2
Using traditional medicines recommended by neighbors (F) 13 5.2 Not using any medicine without the advice of the health personnel (T) 219 87.3
Not playing by sharp and piercing items like pencil (T) 179 71.3
Not slapping or throwing stone at each other when playing (T) 198 78.9
Using sunglass outside (T) 205 81.7
Using medicine recommended by neighbors (F) 7 2.8
Using of available medicine at home when needed (F) 7 2.8 * Percentages were calculated from the total number for each option; T: True; F: False
Discussion
The knowledge of teachers relating to eye health is vital for school-going children as they increasingly spend more time under the supervision of teachers, and less so under the supervision of their parents. Visual impairment related to uncorrected refractive errors along with eye trauma are common problems in Turkey among children in their early childhood and school going period 7,8,10-
13. To our knowledge, this is the very first study published which explores the knowledge of Education Faculty students about the eye health of school children, and to appraise whether their knowledge is useful for the detection of visual impairment and other eye disorders, as well as first aid for eye trauma and injury, in Turkey.
Concerning the characteristics of disordered eyes, the marking of eight from fifteen true options, and the not marking of three from five false options by almost more than 75% of the participants did not constitute
reasonable knowledge related to the issue. Moreover, the marking of some false options and the not marking of some true options were very significant, even in small numbers. For example, uncorrected refractive error(s) have an association with headaches which has been confirmed by the literature.18,19 However, “Continuous headache” was considered by 53.0% of the participants as a characteristic of the disordered eye, headaches which are attributable to the eye are aggravated by prolonged visual tasks and worsened by the onset or worsening of the refractive error(s), rather than being continuous.20 Similarly, the appearance of the eyes is not a characteristic of healthy or disordered eyes. On the other hand, some of the obvious characteristics of the disordered eye (“one eye being smaller than the other”, “swelling”, “itching”, “rubbing”, “watering”, “redness” and “burning sensation”) were not chosen by some participants due to insufficient knowledge about the characteristics of the disordered eye. The majority of these conditions could go unnoticed either by the inability of children expressing themselves or insufficient knowledge of the parents and teachers.
Eye health knowledge
Turk J Public Health 2019;17(2) 180
Related to knowledge about situations with high probability of eye trauma, approximately 90% of the participants marked two of three true options and did not marked five of the six false options. This shows that the knowledge of the participants in this arena was satisfactory although some options like “fighting with each other” was not considered by a small number of participants as conditions with high probability of eye trauma.
The most common first aids for different conditions were ‘Carrying the child to the nearest health center without losing time’ and ‘not controlling the eye to see whether the eye is in its place’21,22 for when something hitting the eye; ‘covering the eye with clean cloth so as to not induce any pressure on the globe of the eye’ and ‘referring the child to the eye specialist’23-25for piercing or penetrating injury; ‘washing out the eye’ and ‘not letting the child to rub his/her eye(s)’21,22,26 for fleeing of dust and sand into the eye; ‘immediate and profuse irrigation of the eye(s) with any source of clean water at the site of injury’21,22,24,25 for burning of the eye by chemical substances. Not choosing of the above-mentioned true choices, which show the correct behavior and on the contrary, choosing of some false options which might cause serious complications when the eye(s) is exposed to trauma or injury were indicating that the knowledge of the participants in terms of the first aid was not satisfactory.
The understanding of the participants with regard to causes of visual impairment indicated to be not satisfactory although three of the five true options were marked by approximately more than 80% of the participants. Because some systemic disorders (endocrine and/or metabolic diseases, inflammatory and immune response processes, etc.27) and vitamin A deficiency 28,29 which affect the eye and cause visual impairment and blindness among children were ignored by a significant number of participants.
It was found that the knowledge of the participants relevant to situations with high probability of eye trauma, causes of visual impairment, indicators of visual impairment and recommendations for prevention of eye health were reasonable as most of the true and false options were known by the majority of the participants. At the same time, knowledge of participants about characteristics of disordered eyes, first aid for all types of eye trauma and knowledge related to causes of visual impairment were not found to be satisfactory. A considerable number of participants did not know suitable practices, which could either let the problems go undetected and cause serious complications or exacerbate any dangerous situation. This could be due to the fact that more than half of the participants (57.8%) obtained eye health information from their personal experience, social media and community rather than from formal education. The deficiency of knowledge discovered was in compliance with the requirements of participants, as the majority of them demanded more information regarding first aid for eye trauma and injury, eye health and eye diseases.
Three in four participants required more information related to eye health (eye health, eye trauma or injuries and first aid for eye trauma or injury) and nine in ten participants mentioned teachers as responsible in management of eye trauma and participation of the teachers in school screening program. Considering that the knowledge of teachers is going to be more effective in primary prevention, and early diagnosis and treatment of visual impairment causing conditions among school children, this explanation is clearly highlighting the appropriateness and applicability of the school eye health programs.
The data collection coincided with the pre-examination period in the calendar. It caused an increase in the absentee rate of the students, which was the limitation of the study.
Eye health knowledge
Turk J Public Health 2019;17(2) 181
In conclusion, even though some of the issues related to eye health were known by most of the participants, the knowledge of Early Childhood and Classroom Education Department’s students were not satisfactory in general. Developing an “eye health education program” focusing mainly on first aid for eye traumas, common eye diseases (especially refractive errors) and the characteristics of disordered eyes is recommended by this study. Furthermore, this education should be made to be a part of the curriculum of undergraduate education, and courses that improve health literacy on children's health along with workshops and seminars for candidate teachers are recommended.
References
1. World Health Organization. Visual impairment and blindness: WHO; 2016. Available from: http://www.who.int/mediacentre/factsheets/fs282/en/. Accessed October 5, 2016.
2. World Health Organization. Global Data on Visual impairments and Blindness 2010 2016. Available from: http://www.who.int/blindness/GLOBALDATAFINALforweb.pdf. Accessed October 5, 2016.
3. World Health Organization. Priority eye diseases. Available from: http://www.who.int/blindness/causes/priority/en/index3.html. Accessed October 4, 2016.
4. Gilbert C, Foster A. Childhood blindness in the context of VISION 2020--the right to sight. Bull World Health Organ. 2001;79(3):227-32.
5. Gilbert CE, Anderton L, Dandona L, Foster A. Prevalence of visual impairment in children: a review of available data. Ophthalmic Epidemiol. 1999;6(1):73-82.
6. Cetin E, Yaman A, Berk AT. Etiology of childhood blindness in Izmir, Turkey. Eur J Ophthalmol. 2004;14(6):531-7.
7. Sağlık Bakanlığı Sağlık Araştırmaları Genel Müdürlüğü. Ankara İli’nde İlkokul 1.
Sınıf Öğrencilerinde Gözde Kırma Kusurları Sıklığının Tespit Edilmesi Araştırması 2013. Available from: http://www.sagem.gov.tr/Gozde_Kirma_Kusurlari_Raporu_04_03_2014.pdf. Accessed April 14, 2017.
8. Akyol N SE, Aslan L, Oğuzöncül F, Dinç E. Elazığ İl Merkezinde Ambliyopi ve Ambliyojenik Faktörlerin Prevalansı Üzerine Bir Çalışma. T Klin J Ophthalmol 2000, 9:77-82. 2000.
9. Yaramış N KN. Nevşehir İl Merkezinde İlköğretim Çağındaki Çocuklarda
Göz Hastalıklarının Tespit Edilmesinde Hemşirenin Rolü. Sağlık Bilimleri Dergisi (Journal of Health Sciences) 2005; 14 (Ek Sayı:Hemşirelik Özel Sayısı) 45-53. 2005.
10. Azizoğlu S, Crewther SG, Şerefhan F, Barutchu A, Göker S, Junghans BM. Evidence for the need for vision screening of school children in Turkey. BMC Ophthalmology. 2017;17(1):230.
11. Cumurcu T, Düz C, Gündüz A, Doğanay S. The prevalence and distribution of refractive errors in elementary school children in area of Malatya. Annals of Medical Research (İnönü Üniversitesi Tıp Fakültesi Dergisi), Ann Med Res 2011;18(3):145-8.
12. Caca I, Cingu AK, Sahin A, Ari S, Dursun ME, Dag U, et al. Amblyopia and refractive errors among school-aged children with low socioeconomic status in southeastern Turkey. J Pediatr Ophthalmol Strabismus. 2013;50(1):37-43.
13. Gursoy H, Basmak H, Yaz Y, Colak E. Vision screening in children entering school: Eskisehir, Turkey. Ophthalmic Epidemiol. 2013;20(4):232-8.
14. Aritürk N, Sahin M, Oge I, Erkan D, Süllü Y. The evaluation of ocular trauma in children between ages 0-12. Turk J Pediatr. 1999;41(1):43-52.
15. International Agency for Prevention of Blindness. School Health Programme Advocacy Paper | International Agency for the Prevention of Blindness [Available from:
Eye health knowledge
Turk J Public Health 2019;17(2) 182
http://www.iapb.org/resources/school-health-programme-advocacy-paper. Accessed March 30, 2017.
16. Yasmin S, Minto H, Chan VF. School eye health -giubg betibd refractuve errirs, Community Eye Health.2015;28(89):14-5. yazım hataları var!!!
17. Frick KD, Riva-Clement L, Shankar MB. Screening for refractive error and fitting with spectacles in rural and urban India: Cost-effectiveness. Ophthalmic Epidemiol. 2009;16(6):378-87.
18. Gil‐Gouveia R, Martins I. Headaches associated with refractive errors: myth or reality? J Headache Pain. 2002;42(4):256-62.
19. Akinci A, Güven A, Degerliyurt A, Kibar E, Mutlu M, Citirik M. The correlation between headache and refractive errors. Journal of AAPOS. 2008;12(3):290-3.
20. Headache Classification Subcommittee of the International Headache Society. The International Classification of Headache Disorders. Cephalalgia An International Journal of Headache. 2018; 38(1) (9):1–211
21. Nichols BD. Ocular Trauma: Emergency Care and Management. Canadian Family Physician. 1986;32:1466-71.
22. Mutie D, Mwangi N. Managing eye injuries. Community Eye Health. 2015;28(91):48-9.
23. Hepler L. First aid care for eye injuries: Healthline; Dec 5, 2016. Available from: https://www.healthline.com/health/first-aid/eye-care. Accessed May 4, 2018.
24. Pramanik S, Doan A, Oetting TA. Assessment and Management of Ocular Trauma Ophthalmology and Visual Sciences. Available from: https://webeye.ophth.uiowa.edu/eyeforum/tutorials/trauma.htm. Accessed May 4, 2018.
25. Lecuona K. Assessing and managing eye injuries. Community Eye Health. 2005;18(55):101-4.
26. Francis V and Wiafe B. The Healthy Eyes Activity Book - A Health Teaching Book for Primary Schools. 2nd Edition. International Center for Eye Health-Sight and Life ISBN 1-90-2541-21-9 2007. 2017.
27. Pinazo-Durán MD, Zanón-Moreno V, García-Medina JJ, Arévalo JF, Gallego-Pinazo R, Nucci C. Eclectic Ocular Comorbidities and Systemic Diseases with Eye Involvement: A Review. Biomed Res Int. 2016;2016:6215745.
28. Shrestha JB, Gnyawali S, Upadhyay MP. Causes of Blindness and Visual Impairment among Students in Integrated Schools for the Blind in Nepal. Ophthalmic Epidemiol. 2012;19(6):401-6.
29. Rahi JS, Sripathi S, Gilbert CE, Foster A. Childhood blindness due to vitamin A deficiency in India: regional variations. Arch Dis Child. 1995;72(4):330-3