f amilial h yperlipidemias julia creider, pgy4 endocrine
TRANSCRIPT

FAMILIAL HYPERLIPIDEMIASJulia Creider, PGY4 Endocrine

OBJECTIVES
Review lipid and lipoprotein classification and nomenclature
Understand the pathways of cholesterol biosynthesis and metabolism
Review primary disorders of hyper- and hypolipidemia Low-Density Lipoprotein (LDL) Triglycerides (TG) High-Density Lipoprotein (HDL)

LIPIDS
Group of naturally occurring molecules Biologically important lipids
Free cholesterol Cholesterol esters (CE) Triglycerides (TG) Phospholipids Fat soluble vitamins (A, D, E, and K)
Main biological functions include Storing energy Signaling Structural components of cell membranes

LIPOPROTEINS
Large macromolecular complexes that transport hydrophobic lipids surrounded by hydrophilic phospholipids and proteins

LIPOPROTEINS
Type Site of Origin Major Lipids Major Apolipoprotiens
Chylomicrons (CM)
Intestine 85% TG B48, A1, AIV
CM Remnant Intestine 60% TG, 20% C B48, E
VLDL Liver 55% TG, 20% C B100, E, C1, CII, CIII
IDL From VLDL 35% C, 25% TG B100, E
LDL From IDL 60% C, 5% TG B100
HDL Liver, intestine, plasma
25% PL, 20% C, 5% TG (50% protein)
A1, AII, C1, CII, CIII, E
Lp(a) Liver 60% C, 5% TG B100, (a)

LIPOPROTEINS
Lp(a)

APOLIPOPROTEINS
Protein component of lipoproteins Function
Activate enzymes important to lipid metabolism Act as ligands for cell surface receptors

Apolipoprotein Site of Synthesis Major Functions
ApoA-1 Liver, intestineStructural protein of HDLCofactor for LCATLigand for ABCA-1 and SR-B1
ApoA-II Liver Inhibits apo-E binding to receptors
ApoA-IV IntestineActivator of LCATFacilitates lipid secretion from intestine
ApoA-V Liver Activator of LPL lipolysis
ApoB-100 Liver Protein for VLDL, IDL, LDL
ApoB-48 Intestine Protein for CMs
ApoC-1 LiverModulates apo-E mediated binding of remnantsActivate LCAT
ApoC-II Liver Cofactor for LPL
ApoC-III LiverRemnant binding to receptorsInhibitor of LPL
ApoELiver, brain, skin,
spleen, testesLigand for LDL & remnant receptorReverse cholesterol transport
Apo(a) Liver Unknown

RECEPTORS
Low-Density Lipoprotein Receptor (LDLR) Present on cells throughout the body Mediates uptake of cholesterol-rich lipoproteins Requires specific proteins on lipoprotein surface
ApoB-100 (LDL) ApoE (CM remnants, VLDL, IDL, and HDL)
Number of LDLR on cell surface is tightly regulated by intracellular cholesterol content
Low-Density Lipoprotein Receptor-Related Protein (LRP) Aka Remnant receptor Binds with high affinity to ApoE (CM remnants, VLDL) Does not bind LDL

IMPORTANT ENZYMES
Lipoprotein Lipase (LPL) Bound to capillary endothelial cells Mediates hydrolysis of TGs to release FFA from
CMs and VLDL Requires ApoC-II as cofactor Activated by ApoA-V Inhibited by ApoC-III Activated by insulin in adipocytes Activated by glucagon and adrenaline in muscle
and myocardial tissues
IMPORTANT ENZYMES
Hepatic Lipase (HL) Hydrolyzes TGs in final processing of CM
remnants Completes processing of IDL to LDL Facilitates interaction of remnant lipoproteins
with LRP for internalization by hepatocytes Participates in conversion of HDL2 back to HDL3

WHAT HAPPENS WHEN YOU EAT? (1)
Brush boarder of epithelial cells of small intestine (duodenum and proximal jejunum) synthesize CMs from dietary fat and cholesterol
CMs enter mesenteric lymph and are absorbed into general circulation by the thoracic duct
Newly synthesized CMs have: ApoB-48 ApoA-1 ApoA-IV
They acquire ApoE and C-apolipoproteins (primarily from HDL)

WHAT HAPPENS WHEN YOU EAT? (2)
LPL catalyzes release of FFAs from CM TG’s and converts them to CM remnants
FFAs are: Stored in adipose tissue Oxidized as energy source Reutilized in hepatic lipoprotien TG synthesis (VLDL)
Hepatic lipase helps in final preparation of CMs for uptake by hepatocytes
CM remnants are rapidly cleared by the liver by either LDL or LRP receptors, mediated by ApoE
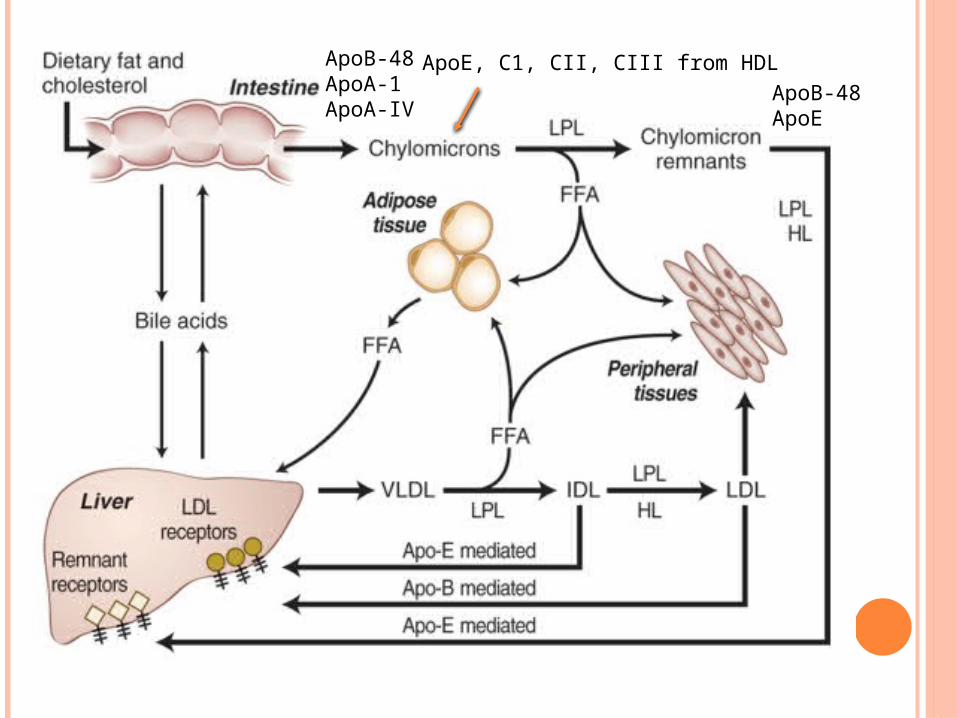
ApoB-48ApoA-1ApoA-IV
ApoE, C1, CII, CIII from HDLApoB-48ApoE

VLDL
Synthesized by the liver Production stimulated by increased delivery of FFA
to hepatocytes Microsomal triglyceride transfer protein (MTP)
Transfers TG and PL to nascent ApoB containing lipoproteins (ApoB-100, and B48)
Deficiency of MTP causes Abetalipoproteinemia VLDL triglycerides are hydrolyzed by LPL and HL Converted to smaller particles that are
increasingly rich in cholesterol

IDL
Metabolic product of VLDL catabolism by LPL Primary proteins are ApoE and ApoB-100 Fate:
Further processed by LPL and HL to LDL Removed from plasma by the LDLR (uptake
mediated by ApoE

LDL
50% of VLDL makes it to LDL
70% of total plasma cholesterol is in LDL
Major apolipoprotein is ApoB-100
Uptake by the LDLR is mediated by ApoB-100
Delivers cholesterol to cells

B100, E, C1, CII, CIII B100, E B100

LIPID DISORDERS
Previously classified according to Fredrickson phenotype
Categorized by type of lipoprotein particle that accumulated in the blood
Does not include HDL Not take into account cause Not distinguish between primary and secondary
causes

FREDRICKSON PHENOTYPES
Phenotype Lipoprotein Lipid Elevation
Type I CMs TG
Type IIa LDL TC
Type IIb LDL and VLDL TC and TG
Type III IDL TC and TG
Type IV VLDL TG
Type V VLDL and CMs TC and TG

PRIMARY DISORDERS OF HYPERLIPIDEMIA
Increased Cholesterol
Increased Cholesterol and Triglycerides
Increased Triglycerides

PRIMARY DISORDERS OF HYPERLIPIDEMIA
Increased Cholesterol Familial Hypercholesterolemia (FH) Familial Defective Apolipoprotein B100 (FDB) Autosomal Recessive Hypercholesterolemia (ARH) Sitosterolemia Polygenic Hypercholesterolemia

FAMILIAL HYPERCHOLESTEROLEMIA (FH)
Autosomal dominant Caused by mutation in LDL receptor gene
>900 described mutations Markedly elevated LDL (>95%ile) Heterozygous 1 in 500, homozygous 1 in 106
60-80, 000 Canadians French Canadian, Christian Lebanese, Dutch
South Afrikaners ~5% of men with MI age < 60
High Risk of CAD if untreated > 60% men, > 30% women by age 60
Katz P. 2014. Lipid metabolism & clinical lipid disorders.

WHEN TO CONSIDER FH
Very high LDL (typically > 5.0 mmol/L) Personal history of early cardiovascular
disease Typical physical findings:
Xanthelasmas Arcus cornealis Tendon xanthomas
Family history: Early cardiovascular disease Marked hyperlipidemia

XANTHALASMAS

ARCUS CORNEALIS

TENDON XANTHOMAS

HOMOZYGOUS FH Very rare, 1 in 106
Marked hypercholesterolemia from birth TC 15 – 25 mmol/L, LDL 14 - 25 mmol/L
Symptomatic CHD < 10 years of age, MI as
young as 18 months If untreated, usually die
in 20’s of CHD Xanthomas,
xanthelasma early in life
Tuberous xanthomasKatz P. 2014. Lipid metabolism & clinical lipid disorders.

SCREENING FOR FH
1. Targeted screening to identify FH index cases with at least 1 feature:
Personal or family history of clinical stigmata or premature CVD
Family history of significant hypercholesterolemia
2. Cascade screening to detect affected members
Opportunistic screening should be done around time of cardiovascular event
Canadian-specific cascade screening www.fhcanada.net
CCS: Position Statement on FH. 2014

FH DIAGNOSIS
Homozygous Suspect in child with TC > 12.9 or xanthomas
Heterozygotes Primarily clinical diagnosis Family history very important Standard criteria have been suggested:
Simon-Broome Criteria Dutch Lipid Clinic Criteria
If family member has known FH and mutation can do cascade testing in family members
Yuan G et al. 2006. CMAJ 17(8):1124

Yuan G et al. 2006. CMAJ 17(8):1124

FH DIAGNOSIS
Yuan G et al. 2006. CMAJ 17(8):1124

WHEN TO DO GENETIC TESTING?
Cases of diagnostic uncertainty Unavailable family history Borderline lipid levels Screened as possible or probable FH Will change management
CCS: Position Statement on FH. 2014

TREATMENT OF FH
Global risk factor assessment and management HTN, DM, smoking, obesity
Homozygotes – plasmapharesis or LDL apheresis
Heterozygotes – statins +/- other agents Ezetimibe, bile acid sequestrants, niacin Newer agents PSCK9 monoclonal antibodies
Treatment goal is at least a 50% reduction in LDL or less than 2.0 mmol/L
Feldman D et al. 2015. CurrAtherosclerRep 17(1):473.

TREATMENT OF FH
Feldman D et al. 2015. CurrAtherosclerRep 17(1):473.

CHOLESTEROL BIOSYNTHESIS
Cholesterol is either absorbed from diet or synthesized by cells in the body
3 molecules of acetate are condensed to form 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA)
HMG-CoA is converted to mevalonic acid by HMG-CoA reductase ➔ RATE LIMITING STEP
Feedback regulation: intracellular cholesterol ➔ HMG-CoA reductase Cholesterol deficiency ➔ upregulate enzyme

ENTEROHEPATIC CIRCULATION
Either excreted as free cholesterol (FC) in bile or converted to bile acids (BA)
50% of FC and 97% of secreted BA are reabsorbed
Reabsorbed cholesterol and BA regulate de novo cholesterol and bile acid synthesis in the liver
7-αHydroxylase RATE LIMITING STEP in BA synthesis Feedback regulation by recirculating BA Closely coupled to HMG-CoA reductase
activity

Niacin:
1. Direct inhibition of DGAT2
2. Decrease lipolysis and FFA influx to liver
3. Increase ApoB catabolism
Statins: inhibit HMG CoA reductasedecrease cholesterolupregulate LDL-R expressionincreased clearance of LDL-C
Bile acid sequestrants:Decrease FC/BA reabsorptionEzetimibe:inhibit intestinal absorption
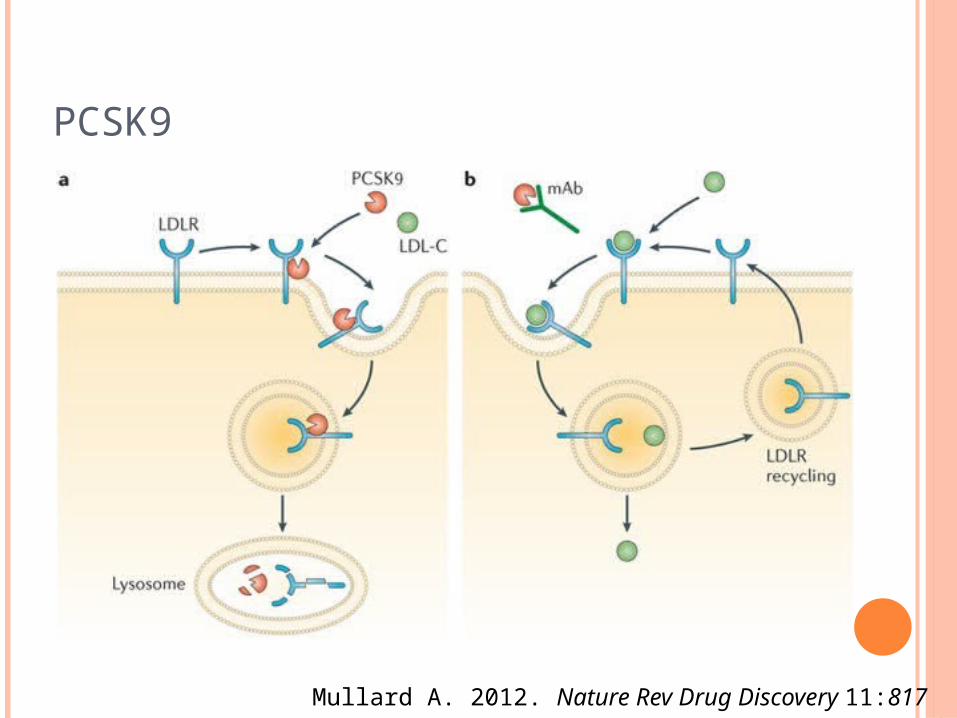
PCSK9
Mullard A. 2012. Nature Rev Drug Discovery 11:817
FAMILIAL DEFECTIVE APOLIPOPROTEIN B100
Mutation in ApoB-100 that impairs its ability to bind to the LDL receptor
Single mutation accounts for almost all cases Substitution of glutamine for arginine at aa3500
Phenotypically similar to FH Isolated elevated LDL Tendon xanthomas and xanthelasma Premature CVD
Generally less severe Clear remnant particles through LDL receptor via ApoE
Kronenberg HM et al. Williams Textbook of Endocrinology. 12th Ed

AUTOSOMAL RECESSIVE HYPERCHOLESTEROLEMIA
Mutation in ARH which encodes LDLR adaptor protein 1
Mediates endocytosis of LDL receptor in hepatocyte cells
Very rare – described in Sardinia, Lebanon
✕
Soutar A. 2010. IUBMB Life. 62(2):125.

SITOSTEROLEMIA
Very rare autosomal recessive Mutations in Adenosine triphosphate binding
cassette transporter (ABCG) 5 or 8 Function to remove passively absorbed plant
sterols Leads to elevations of sitosterol and
campesterol Presentation:
Xanthomas Premature CHD Arthralgias, hemolysis, thrombocytopenia
Requires liquid or gas chromatography to identify
Treatment – restriction of dietary plant sterols and ezetimibe
Othman R et al. 2013. Atherosclerosis. 231(2):291.

POLYGENIC HYPERCHOLESTEROLEMIA
A cholesterol value > 95th percentile for population
Exclude other primary genetic causes by absence of tendon xanthomas and family history in ≤ 10% of first degree relatives
Katz P. 2014. Lipid metabolism & clinical lipid disorders.

PRIMARY DISORDERS OF HYPERLIPIDEMIA
Increased Cholesterol and Triglyceride Familial Combined Hyperlipidemia Familial Dysbetalipoproteinemia

FAMILIAL COMBINED HYPERLIPIDEMIA (FCH)
Autosomal dominant Common disorder (5-7%) Unknown genetic cause, likely multiple genes Overproduction of ApoB ➔ ⇧ VLDL, LDL or
both Moderate elevations of cholesterol or TG or
both Predominant lipid abnormality can vary
among affected family member or a single person over time
Kronenberg HM et al. Williams Textbook of Endocrinology. 12th Ed

FAMILIAL COMBINED HYPERLIPIDEMIA (FCH)
Clinically Overlapping features of metabolic syndrome
Insulin resistance Obesity Hyperuricemia Low HDL
No xanthomas Increased susceptibility to CHD
11% of male survivors of MI < age 60
Treatment Lifestyle – diet, exercise, weight loss Pharmacotherapy – targeted at specific lipid
abnormality
Kronenberg HM et al. Williams Textbook of Endocrinology. 12th Ed
FAMILIAL DYSBETALIPOPROTEINEMIA/TYPE III HYPERLIPOPROTEINEMIA
Mutations in ApoE Results in impaired binding of ApoE to lipoprotein
receptors and accumulations of remnant particles (CM remnants and IDL)
Moderate to severe ⇧ TG and TC LDL reduced (cleared by LDL receptor via ApoB-
100)
Marais A et al. 2014.CritRevClinLabSci. 51(1):46.

ApoB-48ApoE
B100, E B100
×
×

FAMILIAL DYSBETALIPOPROTEINEMIA/TYPE III HYPERLIPOPROTEINEMIA
Typically autosomal recessive (rarely dominant) 1 in 10, 000 Majority are homozygous of ApoE-2 genotype ~ 1% population is ApoE2/E2, only 0.01% have type
III Requires 2nd exacerbating metabolic factor Hypothyroidism, menopause, alcohol, diabetes
Premature vascular disease (including PVD) Treatment
Treat exacerbating factor Diet Fibrates +/- statins
Marais A et al. 2014.CritRevClinLabSci. 51(1):46.
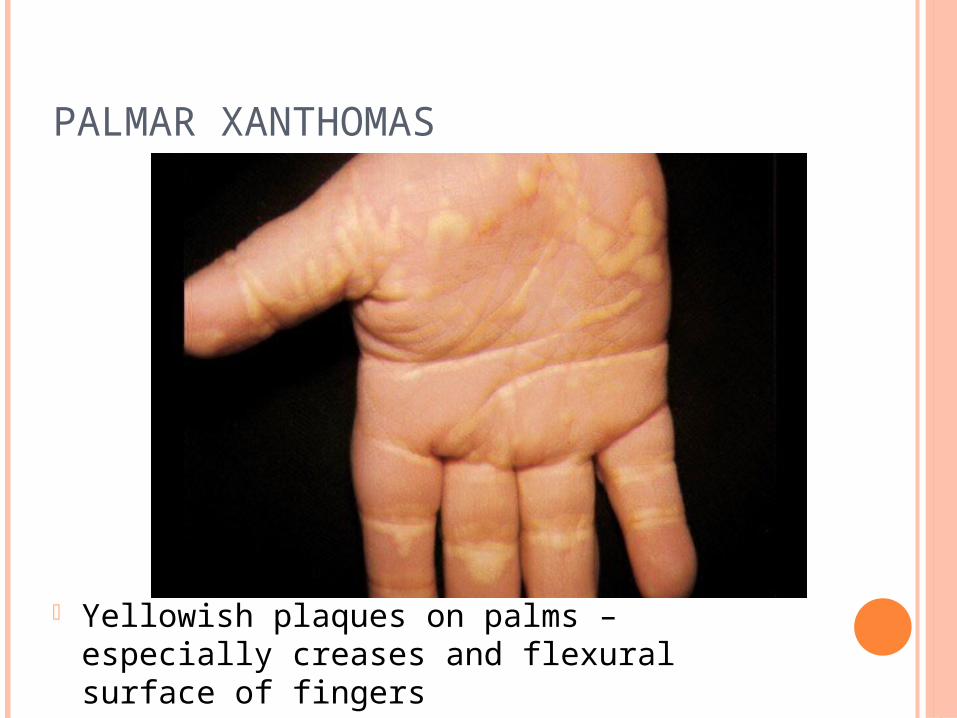
PALMAR XANTHOMAS
Yellowish plaques on palms – especially creases and flexural surface of fingers

PRIMARY DISORDERS OF HYPERLIPIDEMIA
Increased Triglceride Lipoprotein Lipase Deficiency Apolipoprotein CII Deficiency Familial hypertriglyceridemia

LIPOPROTEIN LIPASE DEFICIENCY
Autosomal recessive Mutation in the LPL gene
Absence or inactivation of LPL protein Impaired clearance of TG-rich lipoproteins from
plasma Accumulation of CMs and VLDL
Chylomicronemia Syndrome Marked hypertriglyceridemia (TG >22.6 mmol/L) Recurrent abdominal pain /pancreatitis
Rahalkar A et al. 2009.Can J Physiol Pharmacol. 87(3):151.

LIPOPROTEIN LIPASE DEFICIENCY
Usually present in infancy or childhood Clinically
Eruptive xanthomas Lipemia retinalis Hepatosplenomegaly Neurological manifestations Dyspnea
Biochemically Lipemic plasma Pseudohyponatremia
Treatment – diet, fibrates
Rahalkar A et al. 2009.Can J Physiol Pharmacol. 87(3):151.

ERUPTIVE XANTHOMA

LIPEMIA RETINALIS

LIPEMIC PLASMA

APOLIPOPROTEIN CII DEFICIENCY
Rare autosomal recessive disorder (< 1 in 106)
ApoC-II necessary cofactor for LPL activity Chylomicronemic syndrome similar to LPL
deficiency Severely elevated TG Lipemic serum Recurrent pancreatitis/abdominal pain Eruptive xanthmoas and lipemia retinalis
Absent ApoC-II on electrophoresis Treatment – diet, fibrates
Katz P. 2014. Lipid metabolism & clinical lipid disorders.

FAMILIAL HYPERTRIGLYCERIDEMIA
Overproduction of VLDL with near normal ApoB production Typically TG 2.3-5.6 Normal LDL Often low HDL
Must be present in half of 1st degree relatives to diagnose
Eruptive xanthomas usually not present Obesity, insulin resistance common
Exacerbating factors – hypothyroid, estrogen therapy, alcohol
Uncertain if increase CHD risk
Katz P. 2014. Lipid metabolism & clinical lipid disorders.

HIGH-DENSITY LIPOPROTEIN (HDL)
Redistribution of lipids among lipoproteins and cells by REVERSE CHOLESTEROL TRANSPORT: HDL acquires cholesterol from cells and transports it
to other cells that require cholesterol or to the liver for excretion
ORIGIN OF HDL
1. Liver makes ApoA-I phspholipid disc (nascent, pre-beta HDL)
2. Small intestine directly synthesizes small ApoA-I containing HDL particles
3. Derived from surface material (ApoA-I and PL) that comes from CM and VLDL during lipolysis by LPL


ACQUISITION OF CHOLESTEROL BY HDL
1. Aqueous transfer from cells Free cholesterol moves by passive desorption from
high concentration in membranes of cells with excess cholesterol to low concentration on HDL surface
2. Transport by a cell-surface binding proteins SR-B1 – transfers CEs through hydrophilic channel ABCA1
Binds ApoA-1 or a pre-beta HDL disc to the cell membrane and facilitates transfer of FC and PL from cell to HDL precursor
ATP binding cassette transporters (ABCG1 and ABCG4) stimulate cholesterol efflux to mature HDL (HDL2 and HDL3)

MATURATION OF HDL
Nascent HDL particles (ApoA-I phospholipid discs) are excellent acceptors of excess cholesterol from cells or other lipoproteins
Lecithin-cholesterol acyltransferase (LCAT) Converts free cholesterol to cholesterol esters (CEs) LCAT is activated by ApoA-I
CEs are more hydrophobic, turn disc ➔ sphere (HDL3)
HDL3 accepts and esterifies free cholesterol increases in size ➔ HDL2


FATE OF HDL2
1. Reconverted to HDL3 by hepatic lipase
2. Exchange CE for TG with VLDL, IDL, LDL and remnants via CETP which are then indirectly delivered to the liver and taken up by remnant receptor (MAJOR)
3. Via SR-B1 receptor deposit CEs directly to liver, adrenal, gonads
4. Is further enriched with CE and acquires ApoE becoming HDL1 thereby allowing interaction with LDL receptor allowing excretion of cholesterol by the liver (MINOR)

PRIMARY DISORDERS OF HDL METABOLISM
DisorderMutant Gene
AD vs AR Frequency HDL Corneal
opacification
Early vascular disease
Familial Hypo-alphalipoproteinemia Unknown AD ~1/400 0.5-0.8 No Yes
Familial ApoA-I and ApoC-II deficiency
ApoA-I or ApoC-II AR Rare <0.1 Yes Yes
ApoA-I Milano ApoA-I AD Rare ~0.3 No No
LCAT deficiency LCAT AR Rare <0.3 Yes Yes
Fish-eye disease LCAT AR Rare <0.3 Yes No
Tangier disease ABCA1 AR Rare <0.1 Yes Yes
CETP deficiency CETP AR Rare >2.6 No No
Katz P. 2014. Lipid metabolism & clinical lipid disorders.

FAMILIAL HYPOALPHALIPOPROTEINEMIA
HDL < 10% in men (<0.77 mmol/L), < 15% in women (<1.04 mmol/L)
Normal LDL and TG Increased risk of premature CHD No characteristic findings Often family history
Katz P. 2014. Lipid metabolism & clinical lipid disorders.

APOLIPOPROTEIN A1 MUTATIONS
Mutations in ApoA-I results in poor LCAT activation
HDL < 0.3 Corneal opacities Increased CHD ApoA-I Milano
rare variant of ApoA-I Autosomal dominant Low HDL Not associated with premature CHD
Katz P. 2014. Lipid metabolism & clinical lipid disorders.

LCAT DEFICIENCY
Decreased esterification of cholesterol to cholesterol esters in HDL particles
Free cholesterol accumulates on lipoprotein particles and in peripheral tissues
Features Corneal opacities Normochromic anemia Renal failure Decreased HDL Increased free cholesterol
Saeedi R et al. 2014. Clin Biochem. Aug:Epub
FISH-EYE DISEASE
Variant of LCAT deficiency Phenotype is less severe
Able to esterfy cholesterol on ApoB-containing lipoproteins just not HDL
Low HDL Corneal opacities No anemia, renal disease, or premature CHD
Katz P. 2014. Lipid metabolism & clinical lipid disorders.

TANGIER DISEASE
Mutations in ABCA1 Loss of cholesterol efflux from cells such as
macrophages ➔ massive accumulation of CEs Hypolipidemia
Decreases in plasma HDL and LDL Features
Orange tonsils Corneal opacities Hepatosplenomegaly Peripheral neuropathy Premature CHD
Kolovou G et al. 2006. Curr Med Chem. 13(7):771.

CHOLESTERYL ESTER TRANSFER PROTEIN (CETP) DEFICIENCY
Diminished CETP activity Decreased transfer of CE from HDL to
ApoB containing lipoproteins (VLDL, IDL, LDL)
HDL increased More common in Japanese population Homozygotes have marked elevation of
HDL (> 2.6 mmol/L) Effect on CHD risk is unclear
Katz P. 2014. Lipid metabolism & clinical lipid disorders.

OBJECTIVES
Review lipid and lipoprotein classification and nomenclature
Understand the pathways of cholesterol biosynthesis and metabolism
Review primary disorders of hyper- and hypolipidemia Low-Density Lipoprotein (LDL) Triglycerides (TG) High-Density Lipoprotein (HDL)

QUESTIONS?
REFERENCES CCS: Position Statement on FH. 2014 Feldman D et al. 2015. CurrAtherosclerRep 17(1):473. Katz P. 2014. Lipid metabolism & clinical lipid disorders.
CSEM. Kolovou G et al. 2006. Curr Med Chem. 13(7):771. Kronenberg HM et al. Williams Textbook of
Endocrinology. 12th Ed Marais A et al. 2014.CritRevClinLabSci. 51(1):46. Mullard A. 2012. Nature Rev Drug Discovery 11:817. Othman R et al. 2013. Atherosclerosis. 231(2):291. Rahalkar A et al. 2009.Can J Physiol Pharmacol.
87(3):151. Saeedi R et al. 2014. Clin Biochem. Aug:Epub. Soutar A. 2010. IUBMB Life. 62(2):125. Yuan G et al. 2006. CMAJ 17(8):1124.