fabrication of flurbiprofen transdermal patch using...
TRANSCRIPT

Acta Poloniae Pharmaceutica ñ Drug Research, Vol. 74 No. 4 pp. 1187ñ1201, 2017 ISSN 0001-6837Polish Pharmaceutical Society
Transdermal drug delivery system is designedin a way that it must deliver drug at predeterminedand controlled rate for systemic effect. This shouldalso maintain the plasma drug concentrationbetween minimum effective and minimum toxiclevel over a desired period of time (1). The oralroute is an attractive site for the delivery of the drugsbut faces several barriers like intestinal and or hepat-ic first pass elimination, high variance in bioavail-ability due to variable conditions of gastrointestinaltract, difficulty in long term and rate regulatedabsorption, and impossibility of arbitrary drug inputand its interruption. Such problems of oral routes ofdelivery can be solved by using the transdermaladministration of drugs due to low metabolic activi-ty of the skin when compared with that of the gas-trointestinal tract and liver.
The physicochemical properties of the drug arevery important in the penetration of drugs throughskin. Stratum corneum being a barrier allows onlysmall amount of drug which could reach the sys-temic circulation making this route favorable onlyfor lipophilic drugs (2). For a drug to permeatethrough skin, it must have high but balanced valueof partition coefficient, because the stratumcorneum offers much more resistance to hydrophiliccompounds for diffusion comparatively to the cellu-lar layers beneath it (3). Dermis layer is a significantbarrier to the lipophilic compounds. Materials hav-ing partition coefficient greater than 400 are restrict-ed by dermis but can be absorbed through the stra-
tum corneum. Similarly, the molecular weight ofdrug and daily dose should be low to achieve thera-peutic drug concentration because the drug has topass through tight junctions of skin (4).
Drug permeation through skin is very slow andto reach steady state requires lag time of several hour(5). It is impossible to achieve therapeutic effectivedrug concentrations in blood without enhancing skinpermeation (2). In order to facilitate drug diffusionacross skin, penetration enhancers are commonlyused. After partitioning into stratum corneum, pene-tration enhancers modify the skin properties, themechanism of which is attributed to the disorderingthe stratum corneum lipid structure (6). The use ofpenetration enhancers is a long-standing and widelyused approach to increase transdermal and topicaldrug delivery. Various natural oils are used as pene-tration enhancers. Lack of information on the com-position and utilization of new natural compoundshas created a considerable concern in exploring inno-vative resources to get safe and efficient active andinactive entities of pharmaceutical interest (7).
The Silybum marianum (Milk Thistle) belongsto family Asteraceae (compositae) (annul or bienni-al herb) (8), abundantly available as weed in KhyberPakhtoon Khwah and in some areas of Punjab,Pakistan on unutilized barren ground. It is the safestoil and has extensively been used in EuropeanTraditional Medicines since long, particularly in thetreatment of various liver diseases. The seeds yield26-39% fixed oil that is rich in polyunsaturated fatty
FABRICATION OF FLURBIPROFEN TRANSDERMAL PATCH USING MILKTHISTLE OIL AS PERMEATION ENHANCER
MUHAMMAD AKHLAQ1, ZEESHAN DANISH2*, KAMRAN KHAN1, ABID HUSSAIN3, MAHVISH AJAZ3, JUNAID QURESHI4, GHULAM RAZAQUE6, AAMIR JALIL5,
NAUMAN UL HAQ6 and HAMID SAEED2
1Faculty of Pharmacy, Gomal University, Dera Ismael Khan, Pakistan2University College of Pharmacy, University of the Punjab, Lahore, Pakistan
3Faculty of Medical and Health Sciences, University of Poonch, Rawlakot, Pakistan4Fculty of Pharmacy, Bahaudin Zakariya University, Multan, Pakistan
5Department of Pharmacy, Comsats Institute of Information Technology, Abbottabad, PakistanFaculty of Pharmacy, University of Balochsitan, Quetta, Pakistan
1187
* Corresponding author: e-mail: [email protected]; phone number: 00923214041222

1188 MUHAMMAD AKHLAQ et al.
acids. The other constituents of oil are free fatty acids,compesterol, stigmasterol, mono, di and triglycerides.The defatted seed contains an excellent quality andquantity of proteins, ranging from 20-24% containingamino acids such as aspartic acid, glycine, cystine andglutamic acid. The seed of Silybum marianum is apotential source of dietary oil and protein, an excel-lent source of unsaturated fatty acid i.e., linoleic acid(64.59%) and oleic acid (23.59%) which is of greatmedicinal significance (9, 10).
The study aims to design a typical zero orderrelease transdermal patch using indigenous crudemilk thistle oil extracted from the seeds of Silybummarianum collected locally from Mansehra andAbbottabad districts, KPK, Pakistan as natural pen-etration enhancers. The said formulation would helpthe patient to overcome the burden of repeated dos-ing frequencies and would ultimately help to get thebetter compliance. It would also help utilize thelocal plants to get various valuable natural com-pounds of pharmaceutical interest.
MATERIALS AND METHODS
Materials used in the present study include:flurbiprofen received as a gift from GlobalPharmaceuticals, Pakistan, Silybum marianum seedscollected locally from the surroundings of Mansehra
and Abbottabad districts in the province of KPK,Pakistan. Potassium dihydrogen phosphate(KH2PO4), sodium hydroxide (NaOH), hydrochloricacid (HCl), ethanol and chloroform were purchasedfrom Merck Germany, Olive oil (OLO) fromMarhaba Pvt Ltd., Pakistan, polyvinyl alcohol(PVA) from Sigma Aldrich (Germany), ethyl cellu-lose ether derivative polymer EthocelÆ Premium 10FP (EC) and di N-butyl phthalate were purchasedfrom Dow Chemical Co., Midland, USA. All chem-icals and reagents used in the experiments were ofmolecular biology grade.
Extraction of milk thistle oil (MTO)
Fully ripened seeds of Silybum marianum werecollected from Mansehra and Abbottabad districts,KPK, Pakistan. The seeds were dried in sunlightduring the month of August. After drying, the seedswere cleaned and grinded using a common electricgrinder model (Panasonic, BH 925P, Japan). Theground samples were stored in air tight containers ina cold dark room at temperature 25OC.
The oil was extracted using a Soxhlet extrac-tion apparatus (PyrexÆ, Sigma-Aldrich, USA) usingn-hexane as a solvent. The solvent was removedwith a rotary evaporator (Tokyo Rikakai Co, Ltd, N,No. 4030414) at 40OC and later in an oven at 50OC.The oil samples were stored in cool dry dark place at25OC for further experimental use (11).
Preparation of transdermal patch
Backing membrane of polyvinyl alcohol(PVA) 4% (w/v solution of PVA) (Sigma Aldrich,Germany) was prepared in distilled water. The mix-ture was heated under constant stirring at 80OC untila clear solution was obtained. The solution was thencooled to room temperature and was placed on theSonicator (Elma D 78224, Germany) for 2 min toremove any entrapped air bubbles. About 12 mL ofthis solution was finally poured into Petri dishes (ofabout 20 cm2 area) and was dried at room tempera-ture in open air. Drug polymer dispersions was pre-pared by dissolving the drug (2 mg) and polymers(160 mg) (EC : PVP, 3 : 1) in solvent system(ethanol QS 10 mL) with continuous stirring at 300rpm on the magnetic stirrer. Later, Di-n-butyl phtha-late (15% w/w of polymer) was added to the solu-tion as a plasticizer. Finally, the prepared solution(containing drug-polymer-plasticizers) was pouredinto a Petri dish containing the backing membrane.The solvent was allowed to evaporate under ambientconditions for 24 h. The Petri dish was covered witha funnel to control the rate of evaporation.Penetration enhancers (each 5%) milk thistle oil and
Table 1. Detailed composition table of flurbiprofen controlledrelease transdermal patches formulated with different concentra-tions of natural penetration enhancers (milk thistle oil and oliveoil).
FormulationPermeation Enhancers (w/w)
MTO/OLO
MT1 1%
MT2 2%
MT3 3%
MT4 4%
MT5 5%
MT10 10%
OL1 1%
OL2 2%
OL3 3%
OL4 4%
OL5 5%
OL10 10%
Control 0%
Flurbiprofen 1% w/w, Di-n-butyl phthalate 15% w/w of polymer,Ethanol QS 10 ml , Polymer (mg) EC:PVA 3:1

Fabrication of flurbiprofen transdermal patch using milk thistle oil... 1189
olive oil (w/w of the polymer) were finally added(see Table 1). After complete drying, the film wasremoved from the Petri dish and cut into squarepatches (3.14 cm2) (12).
Physicochemical evaluation of patches
Physicochemical evaluations of all the patcheswere performed in following order:
Physical appearance, thickness and weight unifor-mity
The patches were examined visually forappearance, color, homogeneity, smoothness andtransparency. Thickness was determined at threedifferent points in triplicates. The weight waschecked by randomly selecting 10 patches andweighing in triplicates; the average was calculatedand tabulated.
Moisture content, % moisture uptake and moistureloss
The test patch formulations were marked,weighed accurately and kept in a desiccators usingsilica maintained at room temperature for about 24h. Percent moisture content was calculated usingequation 1:
Wf ñ Wi% moisture uptake = ñññññññññ × 100 (1)Wi
Percent moisture uptake was calculated byselecting three patches randomly and weighingaccurately. The selected patches were then placed ina desiccator at room temperature. To maintain thehumidity, saturated solution of aluminium chloridewas placed in the desiccator. After three days thepatches were taken out from the desiccator and wereweighed again. Percent moisture uptake was calcu-lated using equation 1.
To determine the % moisture loss, three samplepatches were randomly selected, weighed andplaced in desiccator at 37OC. To maintain dry condi-tion anhydrous calcium chloride was also placed.After three days the patches were taken out from thedesiccator and were weighed again. The average %moisture loss was calculated using equation 2 (13):
Wi ñ Wf% moisture loss = ñññññññññ × 100 (2)Wi
Folding endurance, tensile strength, and percentelongation
The folding endurance for test patches wasdetermined by swiftly folding patch at the samepoint till it broke. The number of times a patch canbe folded at the same point without breaking definesthe value of the folding endurance.
The mechanical properties were assessed bytensile strength and percent elongation of the patch.The fixed pulley arrangement was used to determinethe tensile strength and % elongation. The initiallength of the patch strip was determined with a com-mon scale. One end of the patch was fixed and theother end of the patch was tied to a thread passingover a pulley. The hanging end of the thread wasattached to a pan. Weight was gradually added to thepan until the patch was broken and the weight wasnoted. A pointer on the thread was used to measurethe elongation of the patch. Finally, the tensilestrength (in kg/cm2) of the patch was measured usingequation 3:
FTensile strength = ñññññññññññ × 100 (3)
a∑b (1 + L/I)where, F = force required breaking the patch; a =width (cm) of the patch, b = thickness (cm) of thepatch, L = length of the film (cm) and I = elongation(cm) of the film just before the patch is broken.Percent elongation of the patches was determinedusing equation 4:
Lf ñ Li% elongation = ñññññññññ × 100 (4)Li
where, Lf = final length just before the patch is bro-ken. Li = initial length.
Drug contents
The drug contents were determined by placingthe patches in 100 mL phosphate buffer pH 7.4 in avolumetric flask and sonicated for about 8 h. After son-ication, the solution was filtered and the drug contentswere determined spectrophotometrically at 247 nm.
Differential scanning calorimetery (DSC)
The physicochemical compatibility of flur-biprofen drug and excipients was investigated bydifferential scanning calorimetric (DSC) analysis,using a DSC instrument (Mettler Toledo DSC 822e,Greifensee, Switzerland) with a thermal analysisdata station system, computer and a plotter interface.The instrument was calibrated with indium as stan-dard over a temperature range 100-350OC, at heatingrate 10OC/min using nitrogen as purge gas at flowrate 50 mL/min. The samples were heated (50-300OC) at a constant scanning speed of 10OC/min insealed aluminium pan size (1cm diameter).
Fourier transform infrared (FTIR)
FTIR was used to study possible interaction offlurbiprofen and excipients. FTIR (FT-IR Spectrumspectrophotometer, Perkin Elmer, UK) was used inthis study. Approximately 10 mg sample was placedon a previously cleaned diamond surface plate,

1190 MUHAMMAD AKHLAQ et al.
enough pressure was applied and absorptionpattern was recorded over a wavelength range500 to 4000 cm-1.
X-ray diffraction (XRD)
The samples were analyzed, using X-raydiffractometer, Phillips PW1830 powder dif-fractometer (Phillips, Eindhoven, Netherland),using nickel-filtered CuKα, 30 kV and 20 mAvoltage and current, respectively. The spectrawere taken in the range of 0-20O and the time foreach run was kept at 1O/min.
Scanning electron microscopy (SEM)
Surface morphology of the drug were ana-lyzed by photomicrographs of flurbiprofenusing SEM (SEM; Joel JSM-5910, Japan). Forsuch purpose physical mixtures and solid dis-persions in ethanol were used to scrutinize thesurface morphology of the drug, physical mix-tures and solid dispersions. A suitable amountof sample was mounted on a metal stub usingdouble sided adhesive tape and was coated withcold for conductivity. The micrographs wereobtained at 10-50 µm to view the clear mor-phology.
Skin irritation assay
Skin irritation studies were performedaccording to Draize patch test for optimizedpatch (14). Fifteen healthy male rabbits weredivided into five groups each comprising ofthree rabbits. Group-I was tagged as normaland was kept without any treatment. Group-IIreceived marketed adhesive tape (NichiporeSurgical tape, Japan) and was tagged as controlgroup. Test transdermal flurbiprofen patcheswere applied to Group-III, while the blankpatches (without drug) to Group-IV. Standardirritant formalin (0.8% v/v aqueous solution)was applied to Group-V. The experiment wascarried out for 7 days and application siteswere graded according to visual scoring scale,by the same person. The erythema and edemawere scored as follows: 0 for none, 1 for slight,2 for well defined, 3 for moderate and 4 forscar formation and severe erythema andedema.
Skin preparation, invitro permeation and
release kinetics
The skin from rabbit abdominal regionwas carefully removed by surgery after anes-thesia. The adhering fats were removed by dip-
Tab
le 2
. Phy
sica
l par
amet
ers
and
perc
ent d
rug
cont
ent o
f th
e pr
epar
ed f
lurb
ipro
fen
tran
sder
mal
pat
ches
con
tain
ing
milk
this
tle o
il as
pen
etra
tion
enha
ncer
, val
ues
wer
e ta
ken
in tr
iplic
ate,
the
mea
ns a
nd s
tand
ard
devi
atio
ns w
ere
calc
ulat
ed (
n =
±3).
Form
ulat
ion
Dru
g W
eigh
t T
hick
ness
Fo
ldin
g %
Moi
stur
e %
Moi
stur
e H
ardn
ess
Ten
sile
str
engt
hco
nten
t(m
g)(m
m)
endu
ranc
eab
sorb
ance
loss
(N)
kg/c
m2
MT
110
2.4
± 0.
1374
.43
± 0.
033
0.40
± 0
.006
204
±1.5
59.
38 ±
1.1
47.
8 ±
1.30
250
± 2.
1712
.22
MT
299
.69
± 0.
1981
.38
± 0.
029
0.39
± 0
.002
231
± 2.
1210
.70
± 0.
57.
1 ±
0.13
238
± 2.
2210
.09
MT
398
.34
± 0.
1171
.54
± 0.
047
0.39
± 0
.005
243
± 2.
229.
84 ±
0.8
6.4
± 0.
3224
8 ±
3.11
11.1
6
MT
498
.98
± 0.
1773
.17
± 0.
043
0.38
± 0
.001
200
± 0.
918.
54 ±
1.1
47.
4 ±
0.46
291
± 2.
1911
.21
MT
597
.91
± 0.
1276
.28
± 0.
021
0.37
± 0
.003
230
± 1.
098.
35 ±
1.2
37.
0 ±
0.54
240
± 3.
2810
.11
MT
1010
0.7
± 0.
1369
.13
± 0.
027
0.41
± 0
.008
232
± 3.
219.
72 ±
1.0
37.
7 ±
1.20
211
± 2.
2712
.15
OL
197
.21
± 0.
1182
.20
± 0.
032
0.42
± 0
.004
211
± 0.
199.
33 ±
0.5
6.5
± 0.
2123
9 ±
2.22
11.1
3
OL
299
.93
± 0.
1268
.62
± 0.
041
0.39
± 0
.004
210
± 3.
2210
.15
± 0.
76.
5 ±
0.39
246
± 3.
129.
86
OL
398
.76
± 0.
2082
.17
± 0.
043
0.37
± 0
.007
201
± 1.
1111
.13
± 1.
137.
2 ±
0.89
298
± 2.
3911
.28
OL
499
.08
± 0.
0270
.41
± 0.
041
0.39
± 0
.001
241
± 2.
108.
99 ±
1.8
7.1
± 0.
1323
6 ±
2.49
9.03
OL
598
.34
± 0.
1171
.54
± 0.
047
0.39
± 0
.004
243
± 1.
119.
90 ±
0.8
6.5
± 0.
3224
9 ±
3.12
11.1
3
OL
1010
0.6
± 0.
2369
.13
± 0.
029
0.41
± 0
.007
232
± 0.
999.
72 ±
1.1
37.
7 ±
1.21
211
± 2.
1712
.14

Fabrication of flurbiprofen transdermal patch using milk thistle oil... 1191
ping the skin in hot water for a while and then teas-ing the epidermis from the dermis. The skin wasthen washed with distilled water and was stored at -20OC till further use. Franz diffusion cell (FDC)(surface area 176 ± 0.34 mm2) apparatus was used toevaluate the permeation of the drugs from the patch-es across the rabbit skin. The prepared rabbit skinwas allowed to hydrate for 1 h before the experi-ment. The skin was placed in between the donor andreceptor compartment of (FDC) with the stratumcorneum of the skin facing the donor compartment.Then, the patch having an area of 3.14 cm2 wasplaced on the skin with the drug releasing surface ofthe patch facing the stratum corneum of the skin.The receptor compartment was filled with the phos-phate buffer pH 7.4. The receptor fluid was main-tained at 32 ± 0.5OC by means of water circulating inthe water jacket around the receptor compartmentand the medium was stirred with a magnetic bead.Two ml samples were taken from the receptor fluidat the time intervals of 0.5, 1, 1.5, 2, 4, 8, 12, 16, 20
and 24 h and an equal volume of fresh receptor fluidwas added to receptor compartment to maintain thefluid volume. The samples were then analyzed spec-trophotometrically at 247 nm. The drug permeatedper cm2 of patch was calculated and plotted againsttime and the flux was calculated as drug permeatedper cm2 per hour (14).
Invivo studies and pharmacokinetic analysis
For pharmacokinetic studies (15), the rabbitswere divided into three groups, each group contain-ing four rabbits. The rabbits were kept in cages withhusk bedding. On the next day, early in the morning,flurbiprofen reference tablet (50 mg) was given oral-ly through a feeding tube by making a solution indistilled water to group-I. The blood samples (3 mL)were collected at 0, 0.5, 1, 2, 3, 4 and 8 h after drugadministration. The sparse hairs on the back of theanimal were shaved carefully without damaging thestratum corneum with an electrical clipper one daybefore the scheduled experiment. The application
Figure 1. DSC thermograms of pure flurbiprofen drug, patch formulation (drug-polymer dispersions in ethanol) and drug-polymer physi-cal mixture

1192 MUHAMMAD AKHLAQ et al.
area was swept with dry cotton. The flurbiprofenpatch was applied on back of rabbit (group-II) patchand the attachment was sustained for 24 h. Theblood samples were taken at 0, 0.5, 1, 2, 3, 4, 6, 8,12, 16, and 24 h. The placebo transdermal formula-tion was given to group-II rabbits which acted ascontrol group. The blood samples were taken regu-larly up to 24 h.
The centrifuged tubes containing sodiumheparin (as anticoagulant) (Vacutainer, BD) wereused for collecting blood samples of 3 mL at speci-fied time intervals via an in-dwelling cannulaplaced in the marginal ear vein of rabbits followingadministration of test and reference formulations.
The blood samples collected were centrifuged for15 min at 3500 rpm and the plasma was transferredto new glass tubes and kept frozen at -20OC untilanalysis.
Acetonitrile (2 mL) was added to plasma sam-ple (1 mL) in order to precipitate the proteins. Thissuspension was vortexed for 60 s, centrifuged for 5min at 3500 rpm and supernatant was transferred toanother Eppendorf (propylene) tube. The clearsupernatant was evaporated to dryness under nitro-gen flux, dissolved in 80 µL of mobile phase and 20µL of it was injected into the injection port ofreversed-phase HPLC (Perkin Elmer series 200,USA). Briefly, the HPLC system comprised of an
Figure 2. FTIR spectra of pure flurbiprofen, drug-polymer physical mixture, drug-polymer dispersion in ethanol (patch formulation)
Figure 3. X-ray diffraction pattern of pure flurbiprofen, drug-polymer physical mixture, drug-polymer dispersion in ethanol (patch formu-lation)

Fabrication of flurbiprofen transdermal patch using milk thistle oil... 1193
HPLC (Perkin Elmer series 200, USA) with binarypump solvent delivery system, reverse phase C-18(ODS Hypersil, 4.6 × 250 mm, 5 µm) stainless steelanalytical column (Thermo Electron Corporation,UK) fitted with a refillable guard column,UV/Visible wave length detector, integrator NCI900, degasser and ChemStation software.
Following the injection 20 µL of plasma solu-tion to a 20 µL sample loop in injection port using50 µL syringe chromatographic peaks were record-ed at λ 247 nm. The solvent used were degassedwith the help of sonicator (Elma D 78224, Germany)before operation of HPLC and the pH of the mobilewas adjusted by pH meter (Inolab Series, Germany).Mobile phase consisted of a mixture of acetonitrileand ammonium acetate buffer 0.01 M with pH 3.4adjusted by glacial acetic acid (60 : 40, v/v).Optimum flow rate was 1.5 mL/min. The mobilephase prepared was filtered through the 0.45 µLmembrane filter (Sartorius, Germany) and was thendegassed by ultra-sonication.
In case of in vivo studies different pharmacoki-netic parameters such as Cmax (peak plasma concen-
tration), Tmax (time to reach maximum plasma con-centration and AUC (area under the plasma concen-tration time curve) were determined. Plasma con-centration data were used to calculate the peak plas-ma concentration Cmax and time of its occurrenceTmax.
Statistical analysis
A p value < 0.05 was considered to be statisti-cally significant using t-test. The data were collect-ed in triplicates and expressed as the mean ± stan-dard deviation.
RESULTS
Physicochemical evaluation of patches
The patches were subjected for evaluation ofdifferent physicochemical properties (see Table 2).Morphologically all the test patches were found tobe consistent, clear, non-sticky and smooth inappearance. The thickness and weight rangedbetween 0.37 ± 0.003 to 0.42 ± 0.004 mm and668.62 ± 0.041 to 82.20 ± 0.032 mg, respectively.
Figure 4. Photomicrographs of flurbiprofen (A1 and A2), flurbiprofen physical mixture (B1 and B2) and flurbiprofen solid dispersions (C1-C4) using scanning Electron Microscopy (SEM)

1194 MUHAMMAD AKHLAQ et al.
Percent moisture absorbance and percent moistureloss were found to be 8.35 ± 1.23 to 11.13 ± 1.13and 6.4 ± 0.32 to 7.8 ± 1.3, respectively. Foldingendurance and drug content ranged from 200 to 243and 97.21 ± 0.11 to 102.4 ± 0.13, respectively, whilethe tensile strength was found to be ranging from9.03 to 12.22 kg/cm2.
Differential scanning calorimetery (DSC)
DSC thermograms of pure flurbiprofen, drug-polymer physical mixture and drug-polymer disper-sions are presented in Figure 1. All of the thermo-grams displayed a characteristic endothermic peakat ~117OC which corresponds to the melting of flur-biprofen. The melting peak demonstrated a negligi-ble shift to low temperature following inclusion ofexcipients; this might be attributed to the presenceof moisture or the solvent in the patch matrix. Thefact that melting peak of flurbiprofen was persist-ently observed at 117OC demonstrates that the drugremains intact in the patches (16).
Fourier transform infrared (FTIR) absorption
spectroscopy
FT-IR spectra of pure flurbiprofen, its physicalmixture and drug polymer dispersions were taken tostudy any possible chemical interaction betweendrug and polymer (see Fig. 2). Pure flurbiprofenshowed a sharp characteristic peak at 1695.82/cm-1
which corresponds to the carboxyl acid (COOH)present in drug molecule. Other smaller peaks foundin the region 1000-1700/cm-1 are the indication ofbenzene ring in drug molecule. As the sharp charac-teristic peaks of flurbiprofen did not showed anystretching or bending in physical mixture or patchformulation suggesting no interaction between thedrug and excipients.
X-ray diffraction (XRD)
X-ray diffraction results of flurbiprofen areshown in Figure 3 where drug polymer physicalmixture and drug polymer solid dispersions were
measured in θ angle from 0 to 50O. Due to crystallinenature of flurbiprofen drug, x-ray diffraction patternshowed sharp characteristic peaks for flurbiprofenpowder at 20 degree which are slightly shifted tolower diffraction in patch formulation containingpolymeric excipient and ethanol. The minor changesin the peaks might be attributed to the reduction inparticle size of flurbiprofen drug in the physicalmixture or drug-polymer dispersions. The XRD datasuggest that the crystallinity of flurbiprofen is leastinfluenced by the formulation components.
Scanning electron microscopy
The photomicrographs of SEM have shownthat the flurbiprofen (Fig. 4, A1-A2) occur as crys-talline solid (22.5 to 294.59 µm in size) that arelonger than wide and have smooth surfaces. Whilein physical mixture, the geometry of particles is notchanged (see Fig. 4, B1-B2). The solid dispersion ofdrug with polymers in ethanol, on the other hand(Fig. 4, C1-C4) show that the crystalline surfaces ofdrug particles are damaged and they lose their geo-metric shape and adhere to the surface of excipients.
Skin irritation studies
No noticeable sign of erythema or edema wasfound on the rabbit skin for any group throughoutstudy period. The skin irritation score (erythema andedema) with test formulations was found to be up to1.50 ± 0.00 (see Table 3). Standard irritant formalinproduced severe erythema and edema when used onthe rabbitís skin in Group-V i.e., 3.06 ± 0.19, 3.22 ±0.48, respectively. According to the Draize test,score of less than 2.0 ± 0.00 is considered negative.
In vitro permeation studies
Figs. 5-8 show the permeation profiles of flur-biprofen through synthetic membrane and rabbitskin with and without different concentrations ofMTO and OLO used as penetration enhancers intransdermal patches. The flux, permeability coeffi-cient (Kp), lag time (Tlag) and enhancement ratio
Table 3. Results of skin irritation studies on albino rabbit's skin.
Formulation CodingVisual Observation
Erythema Edema
Group 1 0.00 ± 0.00 0.00 ± 0.00
Group 2 0.96 ± 0.61* 1.07 ± 0.87*
Group 3 1.26 ± 0.77* 1.12 ± 0.39*
Group 4 1.01 ± 0.28* 0.89 ± 0.67*
Group 5 3.06 ± 0.19 3.22 ± 0.48
Visual observation are expressed as the mean ± SD, n = 3; *Significant compared to formaline (p < 0.05).

Fabrication of flurbiprofen transdermal patch using milk thistle oil... 1195
Figure 7. Cumulative amount of flurbiprofen patch permeation containing different concentration of olive oil as enhancer across synthet-ic membrane, the mean ± SD (n = 3).
Figure 5. Cumulative amount of flurbiprofen patch permeation containing different concentration of milk thistle oil as enhancer across syn-thetic membrane, the mean ± SD (n = 3).
Figure 6. Cumulative amount of flurbiprofen patch permeation containing different concentration of milk thistle oil as enhancer across rab-bit skin, the mean ± SD (n = 3).

1196 MUHAMMAD AKHLAQ et al.
(ER) are shown in Table 4. The maximum flux wasachieved for flurbiprofen transdermal patch with10% MTO (w/w) used as penetration enhancer giv-ing the best permeability coefficient and ER. Thepermeation rate, permeability coefficient, and ER ofthe control formulation was found to be 12.25 ±0.20, 0.199 ± 0.003 and 1.0 through synthetic mem-brane and 15.33 ± 0.21, 0.250 ± 0.002 and 1.0through rabbit skin. The formulation containing10% MTO as enhancer exhibited the parameters as53.75 ± 1.71, 0.839 ± 0.002 and 4.09 through syn-thetic membrane and 77.15 ± 2.14, 1.771 ± 0.001and 7.27 through rabbit skin, respectively. Similarly,
the skin permeation parameters for olive oil used aspermeation enhancer were found to be 50.53 ± 2.74,0.784 ± 0.002 and 4.34 for synthetic membrane,while 66.03 ± 3.14, 2.08 ± 0.001 and 2.86 for rabbitskin as flux, permeability coefficient (Kp) and ER,respectively.
Ex vivo permeation through different natural
skins
Since human skin may not be available for ex-vivo permeation studies. It might be important toselect suitable animal skin model to conduct ex-vivotransdermal evaluation. The current study allows
Figure 8. Cumulative amount of flurbiprofen patch permeation containing different concentration of olive oil as enhancer across rabbit skin,the mean ± SD (n = 3).
Figure 9. Cumulative amount of flurbiprofen patch permeation containing different concentration of olive oil as enhancer across rabbit skin,the mean ± SD (n = 3).
Fabrication of flurbiprofen transdermal patch using milk thistle oil... 1197
comparing rabbit, mice, pig, sheep and dogís skinsusing flurbiprofen transdermal patch formulatedwith MTO as natural permeation enhancer. It wasobserved that flurbiprofen permeation using differ-ent skins flux was increased in the order dog < sheep< mice < pig < rabbit when 10% MTO was used andwas found to be 50.32 ± 2.32 < 57.34 ± 1.87 < 60.62± 0.98 < 67.21 ± 1.54 < 70.55 ± 2.11 < 77.15 ± 2.14,respectively (see Figure 9).
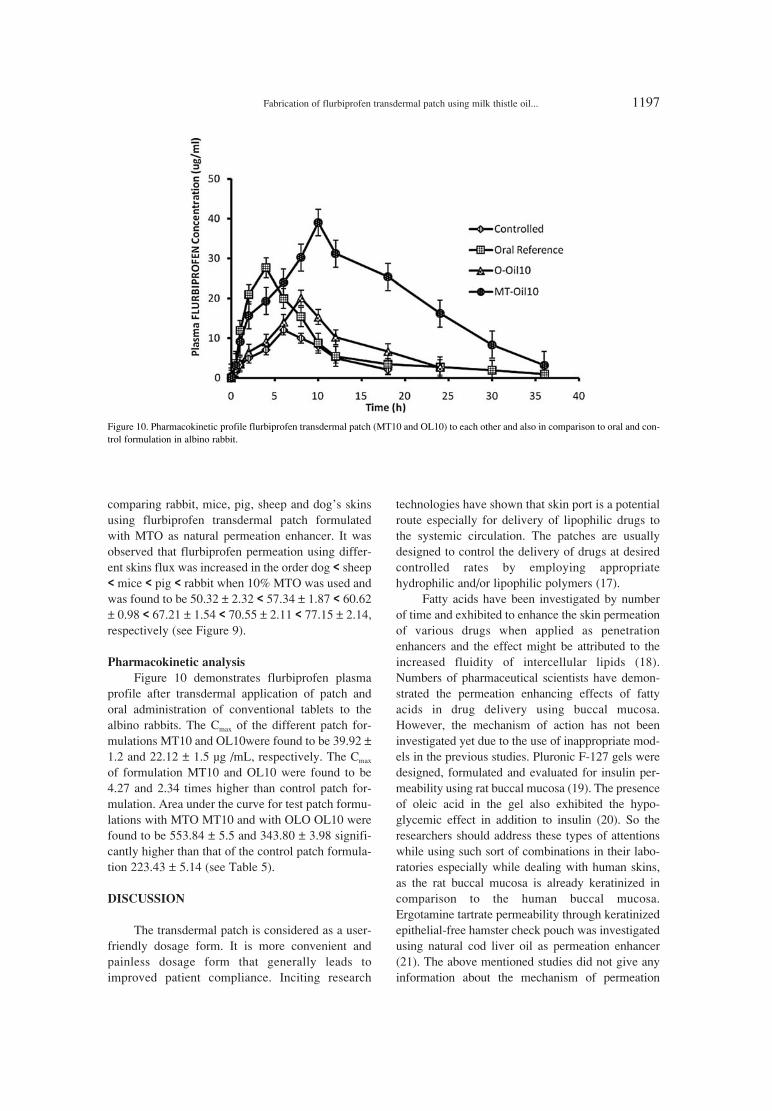
Pharmacokinetic analysis
Figure 10 demonstrates flurbiprofen plasmaprofile after transdermal application of patch andoral administration of conventional tablets to thealbino rabbits. The Cmax of the different patch for-mulations MT10 and OL10were found to be 39.92 ±1.2 and 22.12 ± 1.5 µg /mL, respectively. The Cmax
of formulation MT10 and OL10 were found to be4.27 and 2.34 times higher than control patch for-mulation. Area under the curve for test patch formu-lations with MTO MT10 and with OLO OL10 werefound to be 553.84 ± 5.5 and 343.80 ± 3.98 signifi-cantly higher than that of the control patch formula-tion 223.43 ± 5.14 (see Table 5).
DISCUSSION
The transdermal patch is considered as a user-friendly dosage form. It is more convenient andpainless dosage form that generally leads toimproved patient compliance. Inciting research
technologies have shown that skin port is a potentialroute especially for delivery of lipophilic drugs tothe systemic circulation. The patches are usuallydesigned to control the delivery of drugs at desiredcontrolled rates by employing appropriatehydrophilic and/or lipophilic polymers (17).
Fatty acids have been investigated by numberof time and exhibited to enhance the skin permeationof various drugs when applied as penetrationenhancers and the effect might be attributed to theincreased fluidity of intercellular lipids (18).Numbers of pharmaceutical scientists have demon-strated the permeation enhancing effects of fattyacids in drug delivery using buccal mucosa.However, the mechanism of action has not beeninvestigated yet due to the use of inappropriate mod-els in the previous studies. Pluronic F-127 gels weredesigned, formulated and evaluated for insulin per-meability using rat buccal mucosa (19). The presenceof oleic acid in the gel also exhibited the hypo-glycemic effect in addition to insulin (20). So theresearchers should address these types of attentionswhile using such sort of combinations in their labo-ratories especially while dealing with human skins,as the rat buccal mucosa is already keratinized incomparison to the human buccal mucosa.Ergotamine tartrate permeability through keratinizedepithelial-free hamster check pouch was investigatedusing natural cod liver oil as permeation enhancer(21). The above mentioned studies did not give anyinformation about the mechanism of permeation
Figure 10. Pharmacokinetic profile flurbiprofen transdermal patch (MT10 and OL10) to each other and also in comparison to oral and con-trol formulation in albino rabbit.

1198 MUHAMMAD AKHLAQ et al.
Tab
le 4
. Ski
n pe
rmea
tion
para
met
ers
for
flur
bipr
ofen
tran
sder
mal
pat
ch f
orm
ulat
ed w
ith m
ilk th
istle
oil
and
oliv
e oi
l as
perm
eatio
n en
hanc
er u
sing
syn
thet
ic m
embr
ane
and
rabb
it sk
in. T
he v
alue
s ar
e ta
ken
in tr
ip-
licat
e, th
e m
ean
and
stan
dard
dev
iatio
ns w
ere
calc
ulat
ed.
Synt
hetic
mem
bran
eR
abbi
t ski
n
Form
ulat
ion
Flux
(µg
/cm
2 ∑h)
Kp
(cm
/h)
ER
Tla
g(h
) Fl
ux (
µg /c
m2 ∑h
)K
p(c
m/h
) E
RT
lag
(h)
± SD
± SD
± SD
± SD
± SD
± SD
Con
trol
12.2
5 ±
0.20
0.19
9 ±
0.00
31.
003.
66 ±
0.0
0115
.33
± 0.
210.
250
± 0.
002
1.00
5.08
± 0
.001
Milk
this
tle o
il
MT
-Oil1
13.2
3 ±
0.31
0.20
3 ±
0.00
20.
972.
04 ±
0.0
0215
.29
±1.0
10.
242
± 0.
002
0.89
84.
23 ±
0.0
01
MT
-O
il216
.72
± 1.
080.
277
± 00
011.
382.
33 ±
0.0
0137
.39
± 2.
330.
792
± 0.
001
3.03
86.
09 ±
0.0
02
MT
-O
il320
.41
± 0.
430.
391
± 0.
001
1.92
2.61
± 0
.001
33.3
1 ±
0.21
0.74
4 ±
0.00
42.
795
3.22
± 0
.003
MT
-O
il423
.31
± 1.
150.
471
± 0.
002
2.33
2.11
± 0
.002
51.0
4 ±
2.04
1.17
5 ±
0.00
14.
484.
26 ±
0.0
02
MT
-O
il525
.61
± 1.
170.
598
± 0.
001
2.93
1.61
± 0
.003
58.1
± 1
.01
1.56
2 ±
0.00
15.
914.
11 ±
0.0
05
MT
-O
il10
53.7
5 ±
1.71
0.83
9 ±
0.00
24.
091.
55 ±
0.0
0577
.15
± 2.
141.
771
± 0.
001
7.27
3.14
± 0
.016
Oliv
e oi
l
O-O
il118
.673
± 0.
010.
196
± 0.
001
0.87
7.72
± 0
.001
26.6
7 ±
1.51
0.85
9 ±
0.00
11.
188.
32 ±
0.0
03
O-O
il277
.47
± 2.
130.
254
± 0.
001*
3.76
4.81
± 0
.001
83.7
78 ±
1.4
32.
71 ±
0.0
06*
3.73
4.33
± 0
.006
O-O
il344
.08
± 3.
951.
321
± 0.
005
2.29
5.52
± 0
.009
51.1
67 ±
2.1
51.
649
± 0.
003
2.27
7.22
± 0
.009
O-O
il444
.53
± 2.
740.
411
± 0.
002*
3.11
4.34
± 0
.001
46.0
3 ±
3.32
2.03
± 0
.001
*2.
864.
65 ±
0.0
03
O-O
il537
.741
± 1
.91
0.48
8 ±
0.00
1*2.
076.
33 ±
0.0
0538
.181
± 2
.01
1.21
7 ±
0.00
61.
687.
65 ±
0.0
02
O-O
il10
50.5
3 ±
2.74
0.78
4 ±
0.00
2*3.
194.
34 ±
0.0
0166
.03
±3.1
42.
08 ±
0.0
01*
2.86
4.65
± 0
.003

Fabrication of flurbiprofen transdermal patch using milk thistle oil... 1199
through skin. In another report published on in vitropermeability of propranolol using oleic acid as per-meability enhancer using porcine buccal epithelialmembrane, it was just assumed that oleic acid mighthave permeation enhancing effect attributed to thelipid-fluidizing effect of fatty acid. However, themechanism by which drug permeation is enhancedthrough skin port has never been instigated and dis-cussed so far.
Most researchers used co-solvents and solubi-lizing agents along with penetration enhancers intheir studies while determining the penetrationeffect (22-24). Our study aimed at finding out thepotential of these fatty acids as pure compoundswithout using co-solvents. Although this techniquehas been found to be used in volatile transdermalsprays (25) and topical gels as well (26). The resultsof this study imply three conclusions, first as pene-tration enhancers fatty acids in liquid state (OLA,LA) showed high efficiency in comparison to thosefatty acids which are in solid state (SDA, TDA).Thus high melting point fatty acids show low pene-tration enhancement effect and are less effectivethan liquid fatty acids in formulations for topicalapplications (27). The second implication of thestudy points towards the existence of a linear rela-tionship between the solubility and permeationenhancement (28). The solubility of the enhancer inlipids of SC is a important factor for penetration offatty acid enhancers, effectively. Third, as thedecreasing lipophilicity of penetration enhancerscould indicate the decreased duration of theenhancement. The consequent enhancement effectcannot be maintained as with decreasing lipophilic-ity of enhancer (18).
The techniques used in the current study mightallow the overall drug release through patch matrixvia appropriate choice of polymers and their combi-nations utilizing different diffusion pathways to getoverall desired steady state and release pattern bothin vitro in vivo. The cumulative amount of flurbipro-fen drug released per cm2 from different drug deliv-ery systems of varied ratios of EC and PVP exhibit-ed a variable release patterns (see Figs. 5-8). The
drug release pattern in most of the controlled/sus-tained release devices is mostly governed by the dif-fusion and erosion mechanism. Since, the patchmatrix formulated with compatible polymers comesinto contact with the solvent system, the fluid isabsorbed into the patch matrix initiating drug as wellas polymer chain dissolution process in the matrix(15). The satisfactory folding endurance of patchrevealed that the formulated patch might be able tomaintain their reliability with general skin foldingduring handling and would be able to endure thecracks and ruptures (12). The flatness study mightindicate that the patch formulation has the same striplength before and after the cuts. Moisture content inthe formulation was related to ratios of EC and PVP.Low moisture uptake by the polymer matrix gives100% flatness to the patch and might maintainsmooth and uniform surface when applied onto skin.The tensile strength of the patch, a critical productattribute, is impacted by the concentration of poly-mer, plasticizer and polyethylene. The flux dependsupon the presence of penetration/permeationenhancers.
Formulations containing high concentration ofpolymer show a greater tensile strength than thecounterparts fabricated with low concentrations.Similar behavior was observed with the plasticizer,however the impact of plasticizer concentration is toa lower extent than the one recorded with polymer.The presence of the plasticizer also contributed inthe production of smooth, uniform and flexiblepatches throughout. Its existence also prevents thecracking of the film by imparting it the flexibilityand desirable mechanical properties. Similarly, theconcentration of the PE has a relatively small posi-tive correlation with the tensile strength (29). All thepatches were found to have agreeable flexibility evi-denced by getting high values of tensile strengthsand % elongation. Uniform and homogenous distri-bution of drug in the patches is necessary to ensureuniform sustained delivery of the drug from thepatches. Furthermore, no significant changes in thephysicochemical properties and drug contents of theformulated patches were observed during the stabil-
Table 5. Pharmacokinetic parameters of flurbiprofen after transdermal application and oral administration in albino rabbits, the mean (± S.D).
FormulationCmax Tmax AUC0-α Relative Half-life t1/2 MRT 0-48 Clearance
(µg/mL) (h) (µg.h/mL) bioavailability (h) (h) (mL/min)
Oral 26.44 ± 2.11 1.00 77.78 ± 3.72 - 5.33 ± 0.13 7.21 ± 0.88 0.34 ± 0.32
Plain (control) 09.43 ± 0.62 6.0 223.43 ± 5.14 2.87 9.33 ± 0.07 14.29 ± 1.87 0.07 ± 0.01
MT10 39.92 ± 1.2 8.0 553.84 ± 8.3 7.12 10.88 ± 0.01 15.89 ± 2.1 0.09 ± 0.02
OL10 22.12 ±1.5 6.0 343.80 ± 3.98 4.42 11.22 ± 0.05 16.11 ± 1.34 0.04 ± 0.03

1200 MUHAMMAD AKHLAQ et al.
ity studies of the patches for a period of threemonths, thus ensuring the stability of the formulatedpatches.
The profiles of permeation enhancers showingdissimilar slopes are evident where the MTO andOLO concentration increases gradually from 1-10percent. After twelve hours, formulations containing5.0% MTO and OLO have shown significantly high-er permeated (mg/cm2) cumulative amount of flur-biprofen through porcine skins with full thickness (p< 0.01 > or 10% (p < 0.001)) in contrast to controlformulations. Still, no significant difference wasfound between the thickness of two formulations con-taining 5.0% and 10.0% OLO, respectively (p >0.05). The calculated flux (J) values of flurbiprofenfrom downwards slopes of steady state (linear) por-tion of in vitro permeation curves are shown in Table4. As it is evident, the flux (J) is increased with theincrease in concentrations of MTO and OLO. Theonly formulation containing 10.0% OLO (w/w) wasfound to be statistically different (p < 0.001) fromcontrol. A 2.4 times higher value for flurbiprofen flux(J) was found through the skin for this percentage.Thus the formulations having OLO concentrations of2-5% showed statistically significant and varied val-ues of fluxes (J) in comparison to formulation of 10%OLO. A diffusion model can also be interpreted formthe values of permeated flurbiprofen values (mg/cm2)in Table 4, presenting a linear correlation (r). Thusrendering the proposed mechanism of MTO as pene-tration enhancer compatible with this observation i.e.,the diffusion of the compound is facilitated by theincreased SC permeability. Another suggested mech-anism for MTO penetration is the phase separationbetween lamellar solids and fluids (1). The efficiencyof MTO and OLO has been proven from highlyhydrophilic than lipophilic compounds (ethan-ol/water < 0), which supports our rationale for usingthese compounds to enhance delivery of highlyhydrophilic flurbiprofen through skin (23).
The potential formulations could be identifiedfrom the suggested in vitro models. It can be inferredstatistically from this model that 5.0-10.0% facili-tates the penetration of flurbiprofen in the skin, thusincreasing its availability quantitatively in the tissueand to the deeper layers. This happens due to theenhancement effect of the oil, which interacts withthe lipids or cellular membranes of SC.
Olive oil has been widely used to enhance thetransdermal permeation of drug molecules. Thiscompound acts by disordering the highly packed SCintercellular domains lipid. Another possible mech-anism for the action of olive oil is lamellar solidsfluid phase separation. When applied together with
ethanol, olive oil is also believed to cause SC lipidsextraction. In our study, we demonstrated that oliveoil not only affects the SC lipids, but also influencesthe viable cells in the epidermis responsible for theskin immune function (29).
CONCLUSION
Flurbiprofen transdermal patch was successful-ly prepared and in vitro ex vivo and in vivo studieswere performed using milk thistle oil as unique per-meation enhancer. This compound was testedagainst artificial membrane, rabbit, rat, pig dog andhuman skin. The physicochemical parameters and invitro drug permeation data showed that the formula-tion containing 5-10% milk thistle oil exhibitedenhanced drug release; hence the one with 10% per-meation enhancer was further selected for in vivostudies using rabbit as optimized animal model forfurther pharmacokinetics evaluation. It was con-cluded that the patch formulated with flurbiprofen inthe current study using indigenous extracted milkthistle oil could serve as a potential formulation fortransdermal delivery.
Acknowledgment
Thanks to global pharmaceuticals for provid-ing gift samples of drug.
REFERENCES
1. Prow T.W., Grice J.E., Lin L.L., Faye R., ButlerM. et al.: Adv. Drug Del. Rev. 63, (2011).
2. Naik A., Kalia Y.N., Guy R.H.: Pharm. Sci.Tech. Tod. 3, 318 (2000).
3. Ko P.T., Lee I.C., Chen M.C., Tsai S.W.: J. Tai.Inst. Chem. Eng. 51, 1 (2015).
4. Zakrewsky M., Kumar S., Mitragotri S.: J.Control. Rel. (2015).
5. Denet A.R., Vanbever R., PrÈat V.: Adv. DrugDel. Rev. 56, 659 (2004).
6. Prausnitz M.R., Langer, R.: Nat. Biotech. 26,1261 (2008).
7. Prausnitz M.R., Mitragotri S., Langer R.: Nat.Rev. Drug. Discov. 3, 115 (2004).
8. Vairo Cavalli S., Silva S.V., Cimino C.,Malcata F.X., Priolo N.: Food Chem. 106, 997(2008).
9. Takase M., Chen Y., Liu H., Zhao T., Yang L.,Wu X.: Ultra. Sonochem. 21, 1752 (2014).
10. Passerini N., Perissutti B., Albertini B.,Franceschinis E., Lenaz D., Hasa D. et al.:Phytomedicine 19, 160 (2012).

Fabrication of flurbiprofen transdermal patch using milk thistle oil... 1201
11. «elik H.T., G¸r¸ M.: J. Supercritic. Fluids 100,105 (2015).
12. Jung E., Lee E.Y., Choi H.K., Ban S.J., ChoiS.H. et al.: Int. J. Pharm. 487, 49 (2015).
13. Suksaeree J., Charoenchai L., Madaka F.,Monton C., Sakunpak A. et al.: Asian J. Pharm.Sci. 10, 341 (2015).
14. Kanikkannan N., Singh M.: Int. J. Pharm. 248,219 (2002).
15. Charoo N.A., Anwer A., Kohli K., Pillai K.K.,Rahman Z.: Pharm. Dev. Tech. 10, 343 (2005).
16. Zhang L., Zhang Q., Wang X., Zhang W., LinC. et al.: Int. J. Pharm. 492, 40 (2015).
17. Ren C., Fang L., Ling L., Wang Q., Liu S. et al.:Int. J. Pharm. 370, 129 (2009).
18. Chen Y., Quan P., Liu X., Wang M., Fang L.:Asian J. Pharm. Sci. 9, 51 (2014).
19. Morishita M., Barichello J.M., Takayama K.,Chiba Y., Tokiwa S., Nagai T.: Int. J. Pharm.212, 289 (2001).
20. Khafagy E.S., Morishita M., Onuki Y.,Takayama K.: Adv. Drug Deliv. Rev. 59, 1521(2007).
21. Tsutsumi K., Obata Y., Nagai T., Loftsson T.,Takayama K.: Int. J. Pharm. 238, 161 (2002).
22. Sadekar S., Thiagarajan G., Bartlett K.,Hubbard D., Ray A. et al.: Int. J. Pharm. 456,175 (2013).
23. Babu R.J., Pandit J.K.: Int. J. Pharm. 288, 325(2005).
24. Suhonen T.M., Pirskanen L., R‰is‰nen M.,Kosonen K., Rytting J.H. et al.: J. Control. Rel.43, 251 (1997).
25. Oliveira G., Hadgraft J., Lane M.E.: Int. J.Pharm. 435, 38 (2012).
26. Das B., Nayak A.K., Nanda U.: Int. J. Biol.Macromol. 62, 514 (2013).
27. Stott P.W., Williams A.C., Barry B.W.: Int. J.Pharm. 219, 161 (2001).
28. Welling S.R.H., Clemmensen L.K.H., BuckleyS.T., Hovgaard L., Brockhoff P.B., RefsgaardH.H.F.: Eur. J. Pharm. Biopharm. 94, 152(2015).
290. Abid H., Gul M.K., Syed U.J., Shefaat U.S.,Kifayatullah S. et al.: Pak. J. Pharm. Sci. 25,
365-369 (2012).
Received: 3. 067. 2016