facilitators and barriers to health care access amongst
TRANSCRIPT

Facilitators and Barriers to Health Care Access Amongst people using Image and Performance
Enhancing Drugs in Wales
Findings & Outcomes
report

About Public Health Wales Public Health Wales exists to protect and improve health and wellbeing and reduce health ine-qualities for people in Wales. We work locally, nationally and internationally, with our partners and communities. The Substance Misuse Programme works to address both the current and emerging public health threats in Wales and in line with the overarching strategic objective to ‘reduce health inequalities, and prevent or reduce communicable and non-communicable disease, wider harms and premature death related to drugs and alcohol’.
Substance Misuse ProgrammePublic Health WalesNumber 2 Capital QuarterTyndall StreetCardiff CF10 4BZTel: 02920104496
www.publichealthwales.org/substancemisuse
About Public Health Institute
The Public Health Institute at Liverpool John Moores University specialises in applied research addressing health issues at all levels from policy development to service delivery. Public Health In-stitute is committed to a multidisciplinary approach to public health and works in partnership with health services, local authorities, judicial bodies, environmental services and community groups.
Influencing health service design and delivery, as well as health related policy, the Public Health Institute’s research has been at the forefront of the development of multi-agency strategies to pro-mote and protect public health.
Public Health InstituteLiverpool John Moores University3rd Floor Exchange StationTithebarn StreetLiverpool L2 2QP
https://www.ljmu.ac.uk/research/centres-and-institutes/public-health-institute
Acknowledgements: The research team and Public Health Wales would like to thank all those that contributed to this work.
Research Team: Public Health Wales: Josie Smith, Dean Acreman, Gareth Morgan.Public Health Institute, Liverpool John Moores University: Prof Vivian Hope, Dr Conan Leavy.
Suggested citation: V Hope, C Leavy, G Morgan, D Acreman, D Turner and J Smith. Facilitators and barriers to health care access amongst people using image and performance enhancing drugs in Wales: Findings & Outcomes Report. Public Health Wales, 2020

Contents
1 Executive summary 1 1.1 Key findings 1 1.2 Recommendations 1
2 Introduction 3 2.1 Background & context 3 2.2 The study 5
3 Method & Participants 6 3.1 Interviews with people using anabolic-androgenic steroids 7 3.2 Interviews with those providing services 7 3.3 Evidence Gathering & Synthesis Event 7
4 Findings and observations 9 4.1 Motivations, knowledge and information 9 4.2 Identity, stigma, and service engagement 14 4.3 Service delivery, practices and policy 18 4.4 Suggested recommendations for service improvement 25 4.5 Consensus on preliminary recommendations for service improvement and development 26
5 Conclusions & Recommendations 29
6 References 30

Building on the national surveys of image and performance enhancing drug use undertaken in both 2015 and 2016 (available at: www.ipedinfo.co.uk), a qualitative research project was undertaken in Wales to explore the barriers and facilitators to health care access amongst people using anabolic-androgenic steroids (AAS) and other image and performance enhancing drugs (IPEDs). The aim of this research was to identify low cost (<£5k) or no cost service improvements and interventions to encourage early engagement with health and related services by people using IPEDs in order to reduce health harms, be they physical, psychological and/or social. This study utilised data and ideas gathered through semi-structured qualitative interviews with individuals using anabolic–androgenic steroids and those providing community-based health and related services that should be accessed by this group and an Evidence Gathering and Synthesis Event which involved a wide range of stakeholders. Ideas for services improvements identified through these activities were then synthesised into a number of recommendations.
Whilst this work was undertaken in Wales, in light of the findings from the previous IPED surveys and extensive engagement with this population across England, Scotland and Wales, the findings and recommendations are considered to be generalizable to the wider UK population using AAS and other image and performance enhancing drugs.
Within this study reported durations of AAS use varied from a couple of years to several decades and motivations for use were varied and often changed over time. However, it was often perceived by individuals that their motivating factors were often undervalued or misunderstood by health professionals, with little credit being given to other lifestyle commitments e.g. diet and training. All participants using AAS had experienced or witnessed harmful side effects linked in part or fully to AAS use, however the majority of participants minimised the health risks. Concerns were raised by all participants groups regarding the availability and accessibility of evidence based information for both people who use AAS and other IPEDs and frontline professionals.
Most participants perceived their AAS use to be problematic in terms of incurring social risk, many felt judged by friends, family, work colleagues, and health care services. This negatively impacted on their willingness to disclose AAS use to health professionals and to seek appropriate healthcare. Facilitators to service engagement included non-judgemental and knowledgeable staff who were willing to acknowledge participants’ own expertise and offer targeted services.
It was widely recognised by all that there was a growing use of online technologies by individuals using AAS as a method in obtaining injecting paraphernalia and accessing metabolic testing. Such services were commonly viewed as more convenient and accessible when compared to traditional methods, and highlighted the importance for wider outreach and engagement services.
1
1.1 Key findings
1 Executive Summary

2
a.
b.
c.
d.
e.
f.
Government bodies, academic institutions and health services to provide resources and undertake a review with the aim of developing the evidence base on the use of online technologies (including social media) to facilitate effective health service engagement and e-clinics. This work should include online advice and triage clinics targeted towards young people using AAS currently not engaged with existing services
Public health bodies, community substance misuse leads and commissioners to develop best prac-tice guidance on the implementation of effective assertive outreach services and adaptation of health and social care settings to optimise on-site engagement
In collaboration with registered professional bodies (including; RCGP, RCN, RCPsych, GPhC), public health bodies to develop value-based ‘AAS for healthcare professionals’ training and knowledge shar-ing opportunities (including e-learning and GP cluster events). Products to be embedded as a core training programmes within NHS Trusts/Health Boards and community health services.
Adopting a ‘whole person’ approach, substance misuse commissioning boards to undertake a bienni-al comprehensive network mapping and gap analysis exercise of local health and social care services accessible to individuals using AAS. The mapping and gap analysis exercise should include:• Substance misuse and harm reduction• Physical health, mental health and wellbeing• Diet, nutrition, exercise and training advice • Sports injury• Sexual health and wellbeing
This work should lead to the development of a local/regional service directory for dissemination via outreach services, local health and social care expert AAS fora and establishment of dedicated AAS health and well-being clinic sessions within existing services
Public health bodies and AAS leads to produce the following essential documents:• A ‘What to expect’ document developed for distribution across gyms/fitness venues aimed at owners, managers and staff on working with AAS outreach services• Collation of all local/regional AAS health and social care directories for inclusion on national websites e.g. IPEDInfo.co.uk• A written statement on the implications and importance of AAS disclosure during a medical consultation or treatment
Public health bodies in collaboration with UK wide academic institutions to undertake research to establish a robust prevalence estimate of AAS use and evidence of harms associated with use.
1.2 Recomendations
Evidence suggests there has been a rise in non-prescribed use and injection of image and performance enhancing drugs (IPEDs), particularly anabolic-androgenic steroids (AAS) and associated drugs, in the United Kingdom over recent decades. In particular, the estimated number of 16 to 59 year olds reporting lifetime use of anabolic steroids in the Crime Survey for England and Wales has increased from 194,000 in 2005/06 to 271,000 in 2015/16.1. The survey is likely to be unreliable for rare events like anabolic steroid use and so it may under-estimate the extent of their use; however, data from needle and syringe programmes also indicate that use of IPEDs is likely to be increasing. 2.
The motivations for using AAS and other associated IPEDs are varied, and these and the other drivers of use have probably changed over time. Among longer established groups of people using AAS and associated drugs, such as bodybuilders and strength athletes, who have been most studied, being “bigger, stronger” is typically the rationale. However, there are a wide range of issues impacting on use and a more complex picture of interrelated factors associated with body image, masculinity, psychological well-being and early influences has emerged.3. 4. 5.
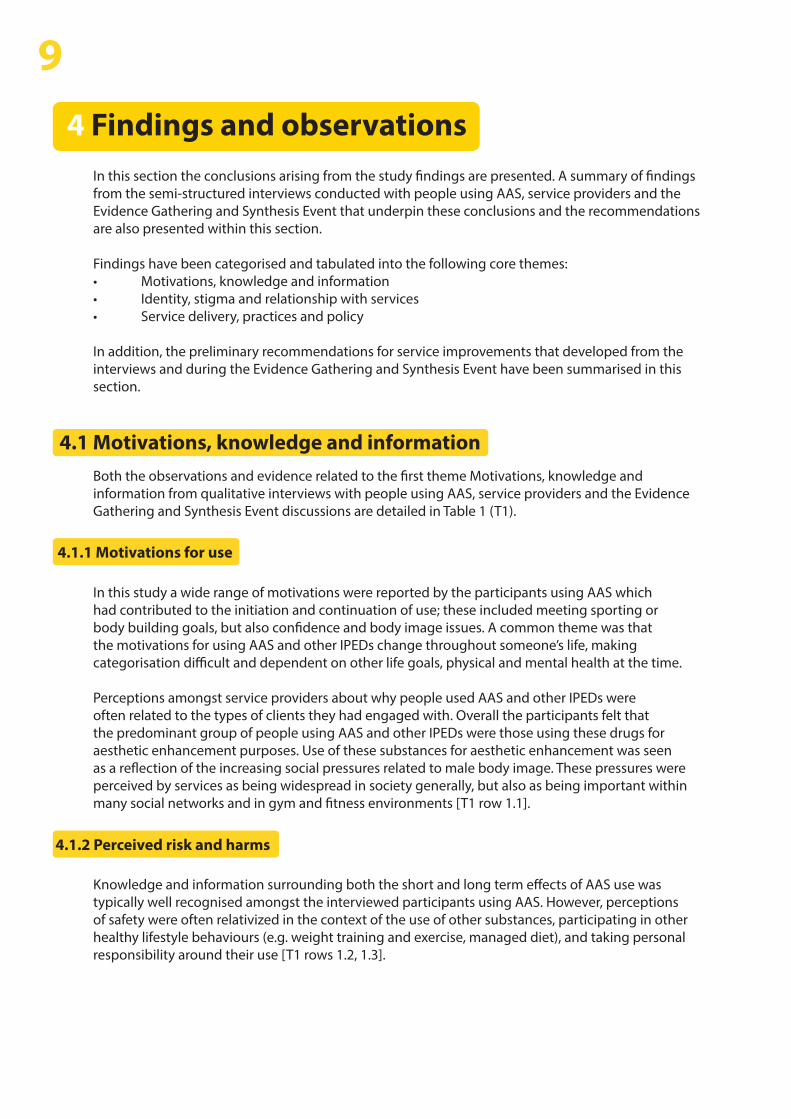
The use of IPEDs, including AAS, for aesthetic purposes probably represents the most common driver of their use in the UK.6. Recent work to develop typologies of AAS use has identified four broad types of people using these drugs: the expert, the athlete, the wellbeing, and the YOLO (You Only Live Once) types (Figure 1).7. 8. Though these groupings are likely to need further refinement, they illustrate the heterogeneity of those using AAS and associated IPEDs.
There are a diverse range of IPEDs that are being used, these include, “fat burners”, tanning agents and a range of hormonal products designed to assist or accelerate physical or physiological changes, as well as AAS. Whilst some of these substances are recognised medical preparations, some are sold as ‘research chemicals’ with little or no clinical testing.10. These drugs are frequently sourced illicitly. Evidence from testing of seized products shows a significant proportion are counterfeit or home produced, and as such; are of highly variable quality, may contain substances other than those reported on the label, have varying dose strengths, or have a high bacterial load; all of which can contribute to potential serious health risks and harms.
A number of potential health risks have been identified with the use and injection of AAS and other associated IPEDs. Many well established harms of AAS are comparatively minor (e.g. acne), however other harms include more severe physical (e.g. cardiovascular disease, damage to the liver) and psychological (e.g. mood changes, increased aggression) problems.9. 10. 11. Many IPEDs, including AAS, can be injected, and so their use can lead to health issues that result from poor or unhygienic injection practice, including soft-tissue damage and infections.12. 13. 14.
A lot of people I train with I know wouldn’t want to go to A&E or wouldn’t want to go to their doctor and they wouldn’t want any record of them using steroids. (DA01)
3
“”
2 Introduction
2.1 Background & context

A TYPOLOGY OFMALE STEROID USERS
AND THEIR RISKSEffectivenessEffectivenessLOW HIGH
Ris
ks
Risks
HIG
H
THE YOLO TYPE THE ATHLETE TYPE
THE EXPERT TYPETHE WELL-BEING TYPE
LOW
Design: Human Enhancement Drugs Network, Birmingham City University, Public Health Institute (LJMU) and Aalborg Antidoping (Aalborg Municipality, DK)
Reference: Christiansen, Vinther & Liokaftos. 2016. Drugs: Education, Prevention and Policy, 1-11.
More information is available at www.humanenhancementdrugs.com
A TYPOLOGY OFMALE STEROID USERS
AND THEIR RISKSEffectivenessEffectivenessLOW HIGH
Ris
ks
Risks
LOW
HIG
H
THE YOLO TYPE
THE WELL-BEING TYPE THE EXPERT TYPE
Motivated by impatience, curiosity and influence from peers and authoritative role models.
Focus on asserting his masculinity (e.g. impressing girls and advancing upwards in the male hierarchy).
Little to no concern about side effects and towards general health
Aims at immediate benefits.
Low level of ‘steroid knowledge’ - based on lore and advice from ‘gym rats’
Risk-taking lifestyle (e.g. recreational drug use andis more likely to end up in fights than the other types)
Little concern about diet, training and recovery
Motivated by vanity and/or wishes for restoration or rejuvenation
Focus on well-being, moderation and peer recognition (e.g. during summertime)
Considers side effects and wants to play it safe
Aims at slight improvements
Medium level of knowledge – based on own experience, online fora and other users
Wants to improve his quality of life and has a relaxed take on nutrition
Focus on healthy living and are typically older
Motivated by competitive aspirations
Focus on performance(e.g., skills, size, and definition).
Concerned with side effects but willing to run health risks in order to fulfil sporting ambitions.
Aims at maximising benefits by combining different steroids (stacking) with other performance and image enhancing drugs (polypharmacy)
Medium to high level of knowledge – based on medical assistance and experience from his sporting community.
Plans training and diet according to season – avoids recreational drugs.
Dedicated to the athlete life style
Motivated by lay scientific curiosity and a fascination with pharmacological performance enhancement.
Focus on muscularity, learning and knowledge sharing.
Very concerned with side effects and wants to play it safe
Aims at optimising benefits with a perceived sensible drug regimen
High level of knowledge – based on various sources including scientific papers
Values health and monitors his body systematically (e.g. in collaboration with physician)
Offers advice on harm reduction to others and seeks recognition as a source of expertise on steroids.
Design: Human Enhancement Drugs Network, Birmingham City University, Public Health Institute (LJMU) and Aalborg Antidoping (Aalborg Municipality, DK)
Reference: Christiansen, Vinther & Liokaftos. 2016. Drugs: Education, Prevention and Policy, 1-11.
More information is available at www.humanenhancementdrugs.com
Figure 1: A typology of men using anabolic-androgenic steroids and their risk by Christiansen, Vinther & Liokaftos (2016)
Whilst it is clear that there are harms associated with the use of AAS and associated IPEDs (figure 2), the uptake of healthcare and prevention services related to these is often poor.15. Data indicates that people who use these drugs will often choose to either wait for symptoms to go away or self-medicate with ‘natural remedies’, over the counter medication, or diverted pharmaceuticals.16. 17.
18. For example, findings from the recent national IPED Info survey* indicated that more than half waited for symptoms of side-effects to go away on their own without seeking medical help/advice, and a third self-medicated.6. In part, this reluctance to use healthcare services is probably due people being cautious about disclosing their use of AAS and other IPEDs to professionals, and so using peers for advice on use, preventing harm and managing any side-effects.19.
Furthermore, people who use AAS and other IPEDs may not perceive themselves as a ‘drug user’, as they are not using psychoactive drugs including cocaine or heroin,20. and so may not access specialist drug services and harm reduction interventions such as needle and syringe programmes. Recent studies indicate that the levels of blood borne viral infections among those injecting IPEDs are higher than among the general population 21. and that worryingly many of these infections remain undiagnosed.22. Thus, there is a need to improve access to health and prevention services for this group.23.
People who use AAS and other IPEDs can experience a range of preventable acute and chronic health problems due to the effects of the substances they use on their bodies. These potential harms could be reduced through regular metabolic testing and prompt health care seeking in response to symptoms of a possible problem. The little available evidence indicates that regular metabolic testing is limited, and typically done privately, and those using IPEDs may not always recognise symptoms or readily access health services in response to these.
In addition to the harms associated with the use of AAS and other IPEDs, evidence indicates a range of additional risk behaviours common amongst some of those using these drugs including sexual risk taking (Figure 2), which may result in sexually transmitted infections, psychoactive drug use and high alcohol consumption levels.6.
>
4
* Available at: http://www.ipedinfo.co.uk/resources/downloads/2016%20National%20IPED%20Info%20Survey%20report%20FINAL.pdf
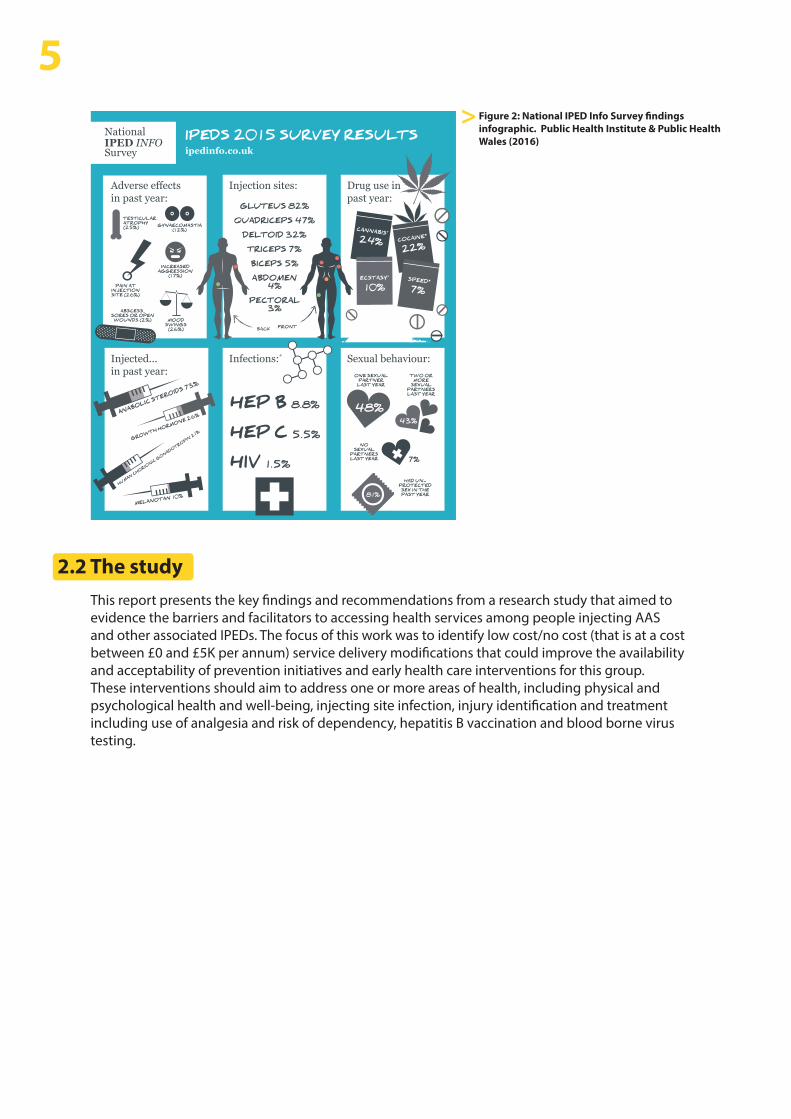
Figure 2: National IPED Info Survey findings infographic. Public Health Institute & Public Health Wales (2016)
To take part in our 2016 survey visit www.ipedinfo.co.uk or ask:
Survey closes December 1st 2016.
* Statistics taken from Hope, VD et al. Prevalence of, and risk factors for, HIV, hepatitis B and C infections among men who inject image and performance enhancing drugs: a cross-sectional study. BMJ pen 2013; 3:e003207.
Injected... in past year:
ANABOLIC STEROIDS 73%
GROWTH HORMONE 26%
MELANOTAN 10%
HUMAN CHORIONIC GONADOTROPIN 21%
Sexual behaviour:
81%
48%
ONE SEXUAL PARTNER
LAST YEAR
43%
TWO OR MORE
SEXUAL PARTNERS LAST YEAR
7%
NO SEXUAL
PARTNERS LAST YEAR
HAD UN- PROTECTED
SEX IN THE PAST YEAR
Infections:*
HEP B 8.8%
HEP C 5.5%
HIV 1.5%
Adverse effects in past year:
TESTICULAR ATROPHY (25%)
PAIN AT INJECTION SITE (26%)
GYNAECOMASTIA (12%)
INCREASED AGGRESSION
(17%)
MOOD SWINGS
(26%)
ABSCESS, SORES OR OPEN
WOUNDS (2%)
Drug use in past year:
CANNABIS+
24%
ECSTASY+
10%
COCAINE*
22%
SPEED* 7%
Injection sites:
GLUTEUS 82%QUADRICEPS 47%
DELTOID 32%TRICEPS 7%BICEPS 5%ABDOMEN
4%PECTORAL
3%
FRONTBACK
IPEDS 2015 SURVEY RESULTSipedinfo.co.uk
This report presents the key findings and recommendations from a research study that aimed to evidence the barriers and facilitators to accessing health services among people injecting AAS and other associated IPEDs. The focus of this work was to identify low cost/no cost (that is at a cost between £0 and £5K per annum) service delivery modifications that could improve the availability and acceptability of prevention initiatives and early health care interventions for this group. These interventions should aim to address one or more areas of health, including physical and psychological health and well-being, injecting site infection, injury identification and treatment including use of analgesia and risk of dependency, hepatitis B vaccination and blood borne virus testing.
>
5
2.2 The study

This study utilised three data collection activities involving people from across Wales.
Two sets of semi-structured qualitative interviews explored understandings of the harms associated with using AAS and other associated IPEDs, and the barriers and facilitators to accessing health services, involving:a. Individuals using anabolic–androgenic steroidsb. Individuals providing community-based health and related services that should be accessed by this group.
An Evidence Gathering and Synthesis Event which involved a wide range of stakeholders including providers of a range of NHS primary and secondary care services
Recruitment for the two sets of interviews took place in a number of selected local areas across Wales. Though these were pragmatically selected, they were geographically diverse reflecting a mix of urban and more rural settings. Participants in the Evidence Gathering and Synthesis Event were from across Wales. This study was approved by LJMU Research Ethics Committee.
The semi-structured interviews with men aged 18 years or over who were using AAS were conducted face-to-face. Participants were recruited from three regions in Wales; North East Wales, South and South East Wales Valleys, and Cardiff. The recruitment approach aimed to include participants who were using AAS for: ‘occupational’ reasons, those engaged in amateur competitive sport, and those whose use was for aesthetic purposes.
Participants were recruited in each area through individuals working in community settings and in specialist gyms who come into contact with people who are using AAS. These individuals acted as ‘gatekeepers’ introducing possible participants to a researcher and/or facilitated the study researcher’s access to recruitment settings. Interviews were undertaken between autumn of 2017 and summer of 2018, and were usually audio recorded, where the participant didn’t want to be recorded detailed field-notes were made. All participants provided written consent before being interviewed, and could opt out of the study at any point. The interviews were undertaken by trained researchers in a private safe space, convenient for the interviewee and lasted between 30 and 75 minutes. An agreed topic guide was followed during the interviews that explored their use AAS and other IPEDs, their knowledge and experience of harms related to use of these and health service engagement.
A total of 17 participants were recruited from three regions in Wales; North East Wales (5), South and South East Wales Valleys and Cardiff (12). There ages ranged from 20 years to 53 years old. The participants report durations of AAS use that varied from a couple of years to several decades.
All of the participants were men, and they included people who were using AAS for ‘occupational’ reasons, those engaged in amateur competitive sport, and those whose use of anabolic–androgenic steroids was for aesthetic purposes. Of the interviews, 13 were audio recorded and detailed field-notes were made for the four who declined to be recorded.
63 Method & Participants
1.
2.
3.1 Interviews with people using anabolic–androgenic steroids (AAS)
3.1.1 The participants

Semi-structured interviews were undertaken with invited individuals who were employed in, or led, community-based health, social care or related services that were being, or could have been, accessed by people who use AAS. These interviews lasted between 30 and 45 minutes, and were conducted either face-to-face or, when this was not practical, by telephone.
A list of relevant service providers was accessed through Public Health Wales and service directories. Those identified were initially emailed information about the study. Agreement to participate and the arrangements for interview was then established via telephone. All participants provided written consent before their interview, and were able to opt out of the study at any point.
The interviews were conducted by a trained researcher in a private and safe environment, usually at the person’s place of work. Semi-structured interviews were then completed following an agreed topic guide which explored: their role in current service provision, their knowledge of the use of AAS and other IPEDs, and their understandings of possible barriers and facilitators to service access.
The interviews were digitally recorded, and the researcher took additional field notes as needed to support the interview process. The recordings themselves were used in the analyses, alongside interview notes.
Interviews were completed with eight service providers during the autumn of 2017 and the winter of 2018. Participants worked in a range of settings including, needle and syringe programmes, drug use related outreach, community pharmacists, and professionals involved in the provision of community based sport and fitness related healthcare. All were currently working in roles that involved direct contact with people using IPEDs, and had been in their current role for at least several years.
The Evidence Gathering and Synthesis Event for the study was held in Cardiff on the 7th November 2018. It brought together a range of people including those from healthcare, public health, and the drug use fields, with people who had experience of using AAS and gym owners. Its overall aim was to explore options for service delivery developments that could improve the uptake of health services by those using AAS and other IPEDs for acute health issues; the prevention of health problems; and providing harm reduction interventions. The focus was on practical and low cost ideas for service delivery developments.
The day operated under the ‘Chatham House Rule’ to encourage frank and open discussion. Participates didn’t have name badges and they were not provided with a list of fellow participants.
The Evidence Gathering Event was structured on the COM-B behaviour change model. The first part of the day involved structured mixed groups discussions to explore issues impacting on service uptake using the following four questions:
Question 1: Can you identify, explain and discuss lifestyle factors or behaviours that may influence early engagement amongst IPED users for physical, psychological and social/relationship issues?
Question 2: Can you identify, explain and discuss social and environmental factors that may influence early engagement amongst IPED users for physical, psychological and social/relationship issues?
73.2 Interviews with those providing services
3.2.1 The participants
3.3 Evidence Gathering & Synthesis Event

8Question 3: Can you identify, explain and discuss policy and practices (of providers) that may influence early engagement amongst IPED users for physical, psychological and social/relationship issues? Question 4: Can you identify, explain and discuss access and quality issues within existing health and related services that may influence early engagement amongst IPED users for physical, psychological and social/relationship issues?
The discussion in each group was led by an experienced facilitator and a scribe took detailed notes, and as needed asked the group to validate the recording of key points. After the groups session all participants came together for an interactive feedback session to allow reflection on the groups’ discussions.
After lunch the key findings from the two sets of interviews undertaken as part of this study (see sections 3.1 and 3.2 above) were then presented and then discussed. Service delivery developments that were generated from both the interviews and during the group work in the morning were then developed by the study team into a set of suggested outline options for service delivery developments and improvements. The participants were then asked to vote on whether they supported each of these using an anonymous interactive smart phone application. The voting choices for each of the suggested options were: ‘Strongly Agree’, ‘Agree’, ‘Disagree’, or ‘Strongly Disagree’.
In this section the conclusions arising from the study findings are presented. A summary of findings from the semi-structured interviews conducted with people using AAS, service providers and the Evidence Gathering and Synthesis Event that underpin these conclusions and the recommendations are also presented within this section.
Findings have been categorised and tabulated into the following core themes: • Motivations, knowledge and information • Identity, stigma and relationship with services• Service delivery, practices and policy
In addition, the preliminary recommendations for service improvements that developed from the interviews and during the Evidence Gathering and Synthesis Event have been summarised in this section.
Both the observations and evidence related to the first theme Motivations, knowledge and information from qualitative interviews with people using AAS, service providers and the Evidence Gathering and Synthesis Event discussions are detailed in Table 1 (T1).
In this study a wide range of motivations were reported by the participants using AAS which had contributed to the initiation and continuation of use; these included meeting sporting or body building goals, but also confidence and body image issues. A common theme was that the motivations for using AAS and other IPEDs change throughout someone’s life, making categorisation difficult and dependent on other life goals, physical and mental health at the time.
Perceptions amongst service providers about why people used AAS and other IPEDs were often related to the types of clients they had engaged with. Overall the participants felt that the predominant group of people using AAS and other IPEDs were those using these drugs for aesthetic enhancement purposes. Use of these substances for aesthetic enhancement was seen as a reflection of the increasing social pressures related to male body image. These pressures were perceived by services as being widespread in society generally, but also as being important within many social networks and in gym and fitness environments [T1 row 1.1].
Knowledge and information surrounding both the short and long term effects of AAS use was typically well recognised amongst the interviewed participants using AAS. However, perceptions of safety were often relativized in the context of the use of other substances, participating in other healthy lifestyle behaviours (e.g. weight training and exercise, managed diet), and taking personal responsibility around their use [T1 rows 1.2, 1.3].
94 Findings and observations
4.1 Motivations, knowledge and information
4.1.1 Motivations for use
4.1.2 Perceived risk and harms

Amongst service providers, the accessibility of reliable and appropriate knowledge and information related to the use and effects of AAS and other IPEDs by those using or thinking about use, was another common theme [1.2]. There were concerns that many people using these drugs relied on internet forums, websites, their peers, and their ‘dealers’ for information about what to use and how to use AAS and other IPEDs. Information from these sources, though sometimes robust, is often incomplete, and sometimes inaccurate and misleading. Furthermore, sexual health risks and risk of blood borne viral infection were often underestimated. It was felt making access to reliable, neutral and scientifically based information was seen as an important area for action. Such information is available on a number of websites, though these sites may need some further development to ensure they are up-to-date, engaging and accessible. It was suggested that better signposting of people to these reliable sources of information using a range of means would be useful.
All interviewed participants using AAS had experienced or witnessed harmful effects linked in part or fully to the use of AAS. Whilst the potential impact of such side effects were recognised by most, in some cases impact was trivialised or disregarded [T1 row 1.4]. In the main, the management of side effects varied depending on its perceived nature by the individual. For example, effects perceived as cosmetic in nature (e.g. gynecomastia, acne, testicular atrophy) tended to be self-treated, whereas most felt they would seek medical advice for more serious side-effects that involved major organs [T1 row 1.5]. Discussions between service users and service providers surrounding side-effects often related to cosmetic and acute health effects rather than long term impacts associated with use. Concerns were raised within all participant groups about the levels of knowledge and understanding of the use of AAS and other IPEDs amongst those delivering services that are, or should be, being used by people using AAS and other IPEDs. There were particular concerns in relation to those staff working in pharmacies providing needle and syringe programmes, due to the high staff turnover and limited time for training, and also amongst primary care providers. It was suggested training should be available through easy to access routes, such as, online courses including refresher training. The training should cover approaches to effective engagement with this group, in addition to providing understandings of the reasons for, and nature of, AAS and other IPED use.
For Table 1 - see overleaf.
10

11Ta
ble
1: S
umm
ary
obse
rvat
ions
and
evi
denc
e re
lati
ng to
Mot
ivat
ions
, Kno
wle
dge
and
Info
rmat
ion
take
n fr
om q
ualit
ativ
e in
terv
iew
s w
ith
part
icip
ants
usi
ng A
AS,
ser
vice
pro
vide
rs a
nd E
vide
nce
Gat
heri
ng a
nd S
ynth
esis
Eve
nt d
iscu
ssio
ns.
No.
1.1
1.2
Them
e
Mot
ivat
ions
for u
se
Perc
eive
d ris
k an
d ha
rms
Obs
erva
tion
Soci
al/s
ocie
tal m
otiv
atio
nSe
rvic
e pr
ovid
ers
perc
eive
d th
at u
se o
f AA
S an
d ot
her I
PED
s ha
d pr
obab
ly b
ecom
e m
ore
com
mon
ov
er th
e la
st d
ecad
e or
so.
Use
of t
hese
sub
stan
ces
for a
esth
etic
enh
ance
men
t was
see
n as
a re
flect
ion
of
the
incr
easi
ng s
ocia
l pre
ssur
es re
late
d to
mal
e bo
dy
imag
e. T
hese
pre
ssur
es w
ere
perc
eive
d by
ser
vice
pr
ovid
ers
as b
eing
wid
espr
ead
in s
ocie
ty g
ener
ally
, bu
t als
o as
bei
ng im
port
ant w
ithin
man
y so
cial
ne
twor
ks a
nd in
gym
and
fitn
ess
envi
ronm
ents
.
Oth
er p
erce
ived
driv
ers
held
by
prof
essi
onal
bod
ies
and
serv
ice
prov
ider
s in
clud
ed p
sych
o-so
cial
issu
es,
incl
udin
g lo
w s
elf-
este
em, b
ody
dysm
orph
ia,
occu
patio
nal e
xpec
tatio
ns
Perc
epti
ons
of ri
skM
ost p
artic
ipan
ts u
sing
AA
S w
hen
aske
d ab
out
how
saf
e th
ey th
ough
t AA
S us
e w
as m
inim
ised
the
heal
th ri
sks,
but
ack
now
ledg
ed th
e im
port
ance
of
see
king
adv
ice
and
exer
cisi
ng p
erso
nal
resp
onsi
bilit
y. M
any
stat
ed th
at A
AS
use
coul
d be
sa
fe p
rovi
ding
the
corr
ect p
roto
cols
wer
e us
ed.
How
ever
, defi
nitio
ns s
urro
undi
ng s
uch
prot
ocol
s va
ried
.
Conc
erns
wer
e ra
ised
am
ongs
t the
ser
vice
pro
vide
rs
and
evid
ence
gat
herin
g ev
ent s
urro
undi
ng th
e so
urce
and
orig
in o
f inf
orm
atio
n ob
tain
ed b
y in
divi
dual
s us
ing
AA
S. W
ith m
any
obse
rvin
g in
form
atio
n ha
ving
bee
n ob
tain
ed fr
om n
on-o
ffici
al
onlin
e so
urce
s, fo
rum
s an
d pe
ers.
As
such
kno
wle
dge
abou
t the
long
er te
rm h
arm
s, th
e sa
fety
of i
llici
tly-
obta
ined
AA
S an
d ot
her I
PED
s, or
wha
t was
‘saf
e’ us
age
of th
ese
drug
s am
ong
thos
e us
ing
them
was
va
riabl
e. F
urth
erm
ore,
thos
e us
ing
AA
S an
d ot
her
IPED
s te
nded
to u
nder
estim
ate
thei
r sex
ual h
ealth
ris
ks a
nd ri
sk o
f blo
od b
orne
vira
l inf
ectio
n, s
uch
as,
HIV
and
hep
atiti
s C.
Part
icip
ant
Part
icip
ants
usi
ng A
AS
Part
icip
ants
usi
ng A
AS
Serv
ice
Prov
ider
Serv
ice
Prov
ider
Serv
ice
Prov
ider
Part
icip
ants
usi
ng A
AS
Part
icip
ants
usi
ng A
AS
Part
icip
ants
usi
ng A
AS
Part
icip
ants
usi
ng A
AS
Part
icip
ants
usi
ng A
AS
Evid
ence
gat
herin
g ev
ent
Evid
ence
“Erm
, I’d
be
lyin
g if
I sai
d it
was
n’t a
n ae
sthe
tic a
spec
t to
it, I’d
be
lyin
g if
I sai
d th
at.”
(DA
07)
“Er,
wel
l with
box
ing,
I mig
ht sa
y it’
s to
get fi
t, er
m, b
ut m
ore
vani
ty
real
ly.”
(DA
08)
“... i
t is a
bout
bod
y im
age,
it is
pee
r pre
ssur
e, w
antin
g to
look
goo
d,
wan
t to
have
bet
ter m
uscl
es th
an so
meo
ne e
lse
at th
e gy
m...”
(G
M08
)
“aes
thet
ic re
ason
s [ar
e th
e m
ost c
omm
on],
it’s t
he p
ress
ure
in te
rms
of m
ale
body
imag
e ha
s defi
nite
ly I w
ould
say
has d
ram
atic
ally
in
crea
sed
in th
e la
st o
ne o
r tw
o de
cade
s, ce
rtai
nly
now
ver
y m
uch
mor
e pr
essu
re fo
r men
to lo
ok a
cert
ain
way
, go
to g
yms,
and
enga
ge w
ith a
t lea
st so
me
elem
ent o
f hea
lth a
nd fi
tnes
s, th
ey a
re
sayi
ng th
at fi
t is t
he n
ew ri
ch; I
thin
k th
at is
the
larg
est p
opul
atio
n ta
king
it, t
o lo
ok a
cert
ain
way
”. (G
M05
)
“Mal
es n
ow m
ore
awar
e of
the
body
shap
e“. (
GM
04)
“I th
ink
the
side
effe
cts a
re p
oten
tially
ove
r egg
ed. I
t’s o
nly
thos
e us
ing
huge
dos
es, o
ver l
ots o
f cyc
les a
nd se
vera
l yea
rs, w
ho te
nd to
su
ffer.”
(D
A10
)
“Fro
m m
y ex
perie
nce,
I hav
e fo
und
them
to b
e ve
ry sa
fe to
be
hone
st. T
he o
nly
thin
g th
at is
eve
r in
ques
tion
is so
urce
and
lab
and
legi
timac
y.” (D
A07
)
“I th
ink
as lo
ng a
s you
’re n
ot a
busi
ng it
... I’
m b
lasé
abo
ut it
, inj
ectin
g st
eroi
ds, i
t doe
sn’t
even
ent
er m
y he
ad, t
he ri
sks.”
(C0
1)
“I th
ink
it ca
n be
as s
afe
as a
nyth
ing,
to b
e ho
nest
, if i
t’s u
sed
corr
ectly
.” (D
A02
)
“I th
ink
if it’
s don
e co
rrec
tly a
nd y
ou’v
e go
t the
righ
t sor
t of a
dvic
e -
it’s s
afe.”
(D
A06
)
Sour
ces
of in
form
atio
n w
ere
typi
cally
onl
ine,
and
oft
en b
ased
on
anec
dote
s, or
lite
ratu
re s
umm
arie
s, an
d fr
om n
on-o
ffici
al s
ourc
es.
The
inte
rnet
was
per
ceiv
ed a
s th
e m
ain
sour
ce o
f inf
orm
atio
n,
with
inte
rnet
sea
rche
s an
d fo
rum
s us
ed to
see
wha
t oth
ers
are
usin
g. S
ome
peop
le a
lso
sour
ced
deta
il ab
out w
here
and
how
co
mpo
unds
are
mad
e, in
clud
ing
qual
ity o
f pro
duct
ion.
Peo
ple
are
inte
rest
ed in
wha
t wor
ks, w
hat d
oesn
’t w
ork,
inte
rpre
tatio
n of
blo
od te
sts,
wha
t sup
plem
ents
to ta
ke, e
tc.,
but q
ualit
y of
in
form
atio
n ac
cess
ed o
nlin
e ab
out t
hese
is n
ot a
ssur
ed.
>

12N
o.
1.3
1.4
1.5
Them
e
Perc
eive
d ris
k an
d ha
rms
Perc
eive
d ris
k an
d ha
rms
Perc
eive
d ris
k an
d ha
rms
Obs
erva
tion
Rela
tivi
zed
risk
taki
ngA
mon
gst t
hose
usi
ng A
AS,
the
risk
from
AA
S us
e w
as o
ften
rela
tiviz
ed to
oth
er fo
rms
of d
rug
use
and
as s
uch
perc
eive
d as
saf
e.
Min
imis
ing
the
impa
ct
All
part
icip
ants
usi
ng A
AS
had
expe
rien
ced
or
witn
esse
d ha
rmfu
l effe
cts
linke
d in
par
t or f
ully
to
the
use
of A
AS
or o
ther
IPED
S. F
or th
e m
ost
part
, par
ticip
ants
thou
ght t
hey
wer
e se
nsib
le a
nd
mod
est i
n th
eir u
se, a
nd th
at it
was
oth
er p
eopl
e w
ho ‘a
buse
d’ A
AS
and
who
ther
efor
e su
ffere
d th
e m
ore
seve
re c
onse
quen
ces.
How
ever
, in
som
e ca
ses
clos
er s
crut
iny
iden
tified
inci
denc
es w
here
th
e im
pact
of s
ide
effec
ts w
ere
dow
n pl
ayed
or
disr
egar
ded.
Cons
ider
ed ri
sk ta
king
O
vera
ll, p
artic
ipan
ts u
sing
AA
S do
wnp
laye
d ri
sks,
em
phas
ised
thei
r ow
n ra
tiona
l use
and
m
inim
ised
thei
r exp
erie
nces
of h
arm
s. M
ore
seve
re
cons
eque
nces
of A
AS
use
wer
e ac
know
ledg
ed
impl
icitl
y or
exp
licitl
y an
d ge
nera
lly a
scri
bed
to
‘mis
use’
by
youn
ger,
irre
spon
sibl
e or
less
edu
cate
d us
ers.
Serv
ice
prov
ider
s al
l not
ed th
at th
e pe
ople
usi
ng A
AS
and
othe
r IPE
Ds
also
dow
n pl
ayed
risk
s as
soci
ated
w
ith th
e us
e of
thes
e dr
ugs.
This
was
rela
ted
to a
cu
ltura
l per
spec
tive
that
see
s th
e us
e of
IPED
s as
be
ing
rela
ted
to b
eing
in ‘g
ood
heal
th’ a
nd ‘fi
t’.
It w
as o
bser
ved
that
sev
eral
par
ticip
ants
usi
ng
AA
S lis
ted
a nu
mbe
r of m
inor
or a
ccep
tabl
e si
de-
effec
ts w
hich
wer
e vi
ewed
as
cosm
etic
(inc
ludi
ng
gyne
com
astia
, acn
e, b
oils
) and
wou
ld ty
pica
lly b
e ig
nore
d or
sel
f-tr
eate
d.
Inte
rest
ingl
y, a
mon
gst s
ome
serv
ice
prov
ider
s it
was
fe
lt an
y se
rvic
e us
er c
once
rns
abou
t the
har
ms
that
m
ight
aris
e fr
om u
se o
f AA
S an
d ot
her I
PED
s w
as
mai
nly
focu
sed
on th
e ac
ute
harm
s pa
rtic
ular
ly th
at
can
have
an
aest
hetic
effe
ct, s
uch
as, g
ynec
omas
tia,
acne
, moo
d, a
nd a
bsce
sses
.
Part
icip
ant
Part
icip
ants
usi
ng A
AS
Part
icip
ants
usi
ng A
AS
Part
icip
ants
usi
ng A
AS
Part
icip
ants
usi
ng A
AS
Part
icip
ants
usi
ng A
AS
Part
icip
ants
usi
ng A
AS
Serv
ice
Prov
ider
Serv
ice
Prov
ider
Evid
ence
“I th
ink
it ca
n be
use
d at
a sa
fe le
vel,
like
any
drug
, lik
e al
coho
l, lik
e to
bacc
o…
I thi
nk it
’s ve
ry sa
fe to
be
hone
st, s
afer
than
recr
eatio
nal d
rugs
.”
(C01
)
“Did
n’t h
ave
any
dam
agin
g eff
ects
.” (C
O3)
Sub
sequ
ently
he
wen
t on
to d
escr
ibe
bein
g ho
spita
lised
for a
car
diac
eve
nt a
ttrib
uted
at
leas
t in
part
to h
is u
se o
f AA
S. T
his
prom
pted
him
to g
ive
up
taki
ng A
AS
afte
r tw
o de
cade
s of
use
.
“I do
n’t r
eally
find
I get
bad
side
effe
cts i
n re
gard
to m
ysel
f.” (
DA
08).
But l
ater
reco
unte
d ha
ving
an
oper
atio
n ou
tsid
e th
e U
K to
trea
t hi
s gy
neco
mas
tia a
nd a
lso
stom
ach
pain
s, pa
infu
l tes
ticle
s, an
ab
sces
s re
quiri
ng d
rain
ing
and
“rea
lly b
ad m
enta
l pro
blem
s”
(DA
08) w
hen
he c
ame
off A
AS.
“In re
gard
to, a
s you
say,
thin
gs li
ke m
y liv
er, m
y ki
dney
s, th
ings
lik
e th
at, t
hen,
y’k
now
, defi
nite
ly, d
efini
tely
, go
to th
e do
ctor
s. W
ith
thin
gs li
ke a
s I d
id w
ith g
ynec
omas
tia a
nd th
ings
like
that
, I’d
try
and
trea
t the
m m
ysel
f. Th
e m
ore
visu
al st
uff, I
try
and
do m
ysel
f.” (
DA
08)
“If I w
as h
avin
g he
art i
ssue
s for
exa
mpl
e, o
r I w
as h
avin
g so
me
sort
of
kid
ney
issu
es, t
hen
yeah
, no,
I wou
ld g
o to
the
GP
‘cos a
t the
end
of
the
day,
whi
le I w
ould
n’t b
e ha
ppy
beca
use
I kno
w w
hat t
heir
resp
onse
wou
ld b
e (‘W
ell,
it’s s
elf-i
nflic
ted’
) the
y st
ill h
ave
a du
ty o
f ca
re to
trea
t me
... a
t the
end
of t
he d
ay m
y he
alth
is u
ltim
atel
y so
rt
of a
bit
mor
e im
port
ant t
han
my
prid
e.” (
DA
07)
“I’m
not
conc
erne
d ab
out a
ny si
de e
ffect
s rea
lly, n
one
of m
y pe
ers
have
exp
erie
nced
any
thin
g an
d I k
now
guy
s in
thei
r 50’
s and
60’
s w
ho w
ere
usin
g ba
ck in
the
1980
’s. I
supp
ose
from
the
ones
you
he
ar a
bout
any
thin
g to
do
with
my
hear
t con
cern
s me.
I’m
doi
ng
this
to b
e at
my
best
and
not
to m
ess m
y he
art u
p. B
ut I’m
confi
dent
in
wha
t I’m
doi
ng. I
hav
en’t
had
any
bloo
d pr
essu
re o
r oth
er te
sts.
I ca
n’t r
emem
ber t
hat l
ast t
ime
I wen
t to
a G
P to
be
fair.
” (D
A11
)
“[so
me]
peo
ple
will
say
I bou
ght t
hem
off
the
inte
rnet
... [
They
will
sa
y] ‘y
eah
I don
’t re
ally
kno
w w
hat I
am
taki
ng’...
as l
ong
as th
ey ca
n ge
t the
end
resu
lts, i
t doe
sn’t
put t
hem
off
at a
ll” (
GM
03)
“The
ben
efits
of h
avin
g a
mor
e m
uscu
lar b
ody,
and
bei
ng b
ette
r th
an so
meo
ne in
the
gym
, is w
orth
som
e of
the
side
-effe
cts w
hich
th
ey p
ossi
bly
don’
t bel
ieve
will
hap
pen
to th
em“
(GM
08)
Tabl
e 1
Cont
inue
d ov
erle
af.

13Pa
rtic
ipan
t
Serv
ice
Prov
ider
Serv
ice
Prov
ider
Serv
ice
Prov
ider
Evid
ence
gat
herin
g ev
ent
Evid
ence
gat
herin
g ev
ent
Evid
ence
“...th
eir c
once
rns a
re m
ore
cosm
etic
, siz
e of
test
icle
s, gy
neco
mas
tia,
acne
, tho
se so
rt o
f thi
ngs.
“ (G
M01
)
“I th
ink,
they
kno
w a
bout
the
risks
, but
they
cho
ose
not t
o, [p
ause
] th
ink
abou
t the
long
term
cons
eque
nces
, bec
ause
it e
asie
r not
to
thin
k ab
out i
t” (
GM
03)
“The
re is
a la
rge
belie
f – a
nd th
is is
real
ly p
reva
lent
in th
e co
mm
unity
–
that
, yes
I hav
e ta
ken
ster
oids
and
ther
e ar
e so
me
risks
, but
I don
’t sm
oke,
I don
’t dr
ink,
and
I exe
rcis
e ev
ery-
day,
unl
ike
my
peer
s, so
th
eref
ore
I am
hea
lthie
r.” (
GM
05
Man
y pe
ople
who
use
ana
bolic
–and
roge
nic
ster
oids
and
oth
er
IPED
s w
ere
perc
eive
d by
the
part
icip
ants
to b
e aw
are
that
ther
e ar
e po
tent
ial h
arm
s, bu
t als
o to
thin
k th
at th
ey ‘w
on’t
happ
en to
m
e’. H
owev
er, t
he p
artic
ipan
ts p
erce
ived
that
if s
omeo
ne h
ad
a m
ajor
or s
igni
fican
t hea
lth e
ffect
it w
ould
mak
e th
em s
eek
heal
thca
re, b
ut m
inor
one
s w
ould
pro
babl
y no
t.
Will
ingn
ess
to s
elf-m
edic
ate
prob
lem
s w
as fe
lt to
be
com
mon
am
ongs
t peo
ple
usin
g an
abol
ic–a
ndro
geni
c st
eroi
ds a
nd o
ther
IP
EDs
as m
any
alre
ady
try
to s
elf-m
anag
e th
e co
mm
on s
ide-
effec
ts o
f use
.
Tabl
e 1
Cont
inue
d fr
om p
revi
ous
page
.

In this study a wide range of motivations were reported by the participants using AAS which had contributed to the initiation and continuation of use; these included meeting sporting or body building goals, but also confidence and body image issues. A common theme was that the motivations for using AAS and other IPEDs change throughout someone’s life, making categorisation difficult and dependent on other life goals, physical and mental health at the time.
The observations and evidence related to the second theme Identity, stigma and service engagement from qualitative interviews with participants using AAS, service providers and Evidence Gathering and Synthesis Event discussions are summarised in Table 2 (T2).
It was clear from both the interviews with people using AAS and those delivering services, as well as from the evidence gathering event, that issues related to stigma, particularly embarrassment, about the use of AAS and other IPEDs was an important issue for people using these drugs [T2 rows 2.1, 2.3]. People using AAS and other IPEDs were concerned about disclosing their use of these drugs, this was often related to being concerned about people judging them and being stigmatised because of their use of these drugs. A key consequence of this was a reluctance to engage with services, particularly if these services, or some service staff, were felt to be unknowledgeable or perceived as potentially being judgemental.
Further exploration of the embarrassment experienced by participants using AAS, observed that such feelings tended to manifest themselves during specific points within their AAS using career. In most cases, this was at the point of needing to seek health care advice due to realised health and wellbeing concerns linked to their AAS use. Such individuals described themselves as educated and knowledgeable around potential side effects and yet had made a confident decision to use. However, where they had found themselves in a situation where their use had resulted in them suffering from adverse effects it was at this point participants said they felt/would feel embarrassed [T2 row 2.3].
The findings indicate that service engagement strategies for this group will probably be most effective if they focus on ensuring staff have an understanding of the reasons and drivers for the use of AAS and other IPEDs [T2 row 2.2]. Individuals interviewed who were using AAS claimed that they often felt that their motivations for use were misunderstood, seen as a way of “cutting corners”, and little acknowledgment was placed on the diet and training regimes that accompany use. It was felt that staff who have some understanding of the reasons as to why people use these drugs will offer a more empathetic, non-judgemental and understanding service.
144.2 Identity, stigma, and service engagement
For Table 2 - see overleaf.

>15Ta
ble
2: S
umm
ary
obse
rvat
ions
and
evi
denc
e re
lati
ng to
Iden
tity
, Sti
gma
and
Serv
ice
Enga
gem
ent t
aken
from
qua
litat
ive
inte
rvie
ws
wit
h pa
rtic
ipan
ts u
sing
AA
S, s
ervi
ce p
rovi
ders
and
Evi
denc
e G
athe
ring
and
Syn
thes
is E
vent
dis
cuss
ions
No.
2.1
Them
e
Iden
tity
man
agem
ent
and
rela
tions
hip
with
se
rvic
es
Obs
erva
tion
Soci
al ri
sk ta
king
M
any
of th
e pa
rtic
ipan
ts u
sing
AA
S pe
rcei
ved
thei
r us
e to
be
prob
lem
atic
, if n
ot fo
r the
ir h
ealth
, the
n in
term
s of
incu
rrin
g so
cial
risk
. Suc
h in
divi
dual
s fe
lt ju
dged
– b
y fr
iend
s, fa
mily
, wor
k co
lleag
ues,
ph
arm
acis
ts, G
Ps, a
nd h
ospi
tal s
taff.
Thi
s im
pact
ed
on th
eir w
illin
gnes
s to
dis
clos
e A
AS
use
to h
ealth
pr
ofes
sion
als
or to
see
k tr
eatm
ent f
or h
ealth
pr
oble
ms
(eith
er A
AS
or n
on-a
nabo
lic–a
ndro
geni
c st
eroi
d re
late
d).
It w
as c
lear
that
som
e pa
rtic
ipan
ts u
sing
AA
S ha
d ex
peri
ence
d so
cial
risk
taki
ng A
AS,
suc
h as
be
ing
rega
rded
as
a ch
eat,
a dr
ug d
eale
r, or
a d
rug
addi
ct, a
nd th
ere
was
a w
idel
y sh
ared
feel
ing
that
he
alth
pro
fess
iona
ls d
isap
prov
ed o
f AA
S an
d ot
her
IPED
s an
d he
ld p
eopl
e w
ho u
sed
them
per
sona
lly
culp
able
for t
heir
sym
ptom
s.
Part
icip
ants
usi
ng A
AS
reco
unte
d oc
casi
ons
whe
n th
ey h
ad a
ltere
d th
eir b
ehav
iour
to a
void
fe
elin
g ju
dged
. And
a n
umbe
r of p
artic
ipan
ts fe
lt pa
rtic
ular
ly s
tigm
atis
ed b
y he
alth
pro
fess
iona
ls.
This
con
tras
ts s
tron
gly
with
oth
er s
ocia
l en
viro
nmen
ts w
here
AA
S an
d ot
her I
PED
use
is
acce
pted
and
whe
re th
e ex
pert
ise
to u
se th
em
to m
ake
‘gai
ns’ i
s re
spec
ted.
As
one
resp
onde
nt
expl
aine
d, h
e co
uld
wal
k in
to a
ny g
ym in
the
wor
ld
and
“It’s
like
bei
ng in
the
Mas
ons.”
Part
icip
ant
Part
icip
ants
usi
ng A
AS
Part
icip
ants
usi
ng A
AS
Part
icip
ants
usi
ng A
AS
Part
icip
ants
usi
ng A
AS
Part
icip
ants
usi
ng A
AS
Part
icip
ants
usi
ng A
AS
Part
icip
ants
usi
ng A
AS
Evid
ence
“I ru
n a
busi
ness
, so
if so
meb
ody
seen
me
in th
ere.
.. y
ou g
et c
lass
ed
as a
dru
g de
aler
.” (C
O3)
“I kn
ow st
eroi
ds a
re fr
owne
d up
on a
nd th
ey’re
not
exa
ctly
lega
l.”
(DA
06)
“A lo
t of p
eopl
e ou
t the
re d
isap
prov
e an
d m
ake
it qu
ite c
lear
they
di
sapp
rove
esp
ecia
lly w
ith a
lot o
f spo
rts g
over
ning
bod
ies..
. the
re’s
a bi
g cr
ack
dow
n ac
ross
eve
ry sp
ort a
t the
min
ute.
I th
ink
they
[p
eopl
e us
ing
anab
olic
–and
roge
nic
ster
oids
] don
’t w
ant p
eopl
e kn
owin
g th
at th
ey’re
doi
ng it
, tha
t the
y’re
che
atin
g I g
uess
... t
hey
hide
it, n
ot o
nly
from
thei
r GP,
but
they
’re p
roba
bly
wor
ried
that
fa
mily
, frie
nds a
nd lo
ves o
nes a
re g
oing
to fi
nd o
ut.”
(DA
06)
“I th
ink
ther
e’s q
uite
a st
igm
a at
tach
ed to
ster
oid
user
s. I k
now
pe
ople
who
’ve
been
to h
ealth
care
pro
fess
iona
ls, b
een
to th
eir d
octo
r, be
en to
A&E
, and
they
feel
ost
raci
sed,
whe
re fo
r abu
sers
like
her
oin
addi
cts,
are
trea
ted
whe
re th
e ad
dict
ion
is co
nsid
ered
an
illne
ss.
Ster
oid
user
s ...
I th
ink
are
trea
ted
like
it’s s
elf-i
nflic
ted,
like
they
’ve
brou
ght i
t on
them
selv
es a
nd th
ey’v
e on
ly g
ot th
emse
lves
to b
lam
e.
I thi
nk p
eopl
e do
look
dow
n on
ster
oid
user
s.” (
DA
01)
“I’m
not
telli
ng m
y do
ctor
I’m o
n th
e ge
ar. I
thin
k m
edic
al p
eopl
e te
nd to
look
dow
n on
you
if y
ou a
re. I
t’s y
our f
ault
you’
re in
her
e [h
ospi
tal].
..” (C
03)
“You
’re n
ot ju
dged
by
the
harm
redu
ctio
n te
am. W
here
as if
you
go
to a
che
mis
t, yo
u’re
just
a d
rug
addi
ct...
the
y do
n’t w
ant t
o kn
ow...
G
oing
to A
&E ..
. the
y re
ally
do
frow
n on
the
fact
that
you
’ve
done
it...
I t
hink
they
look
at y
ou w
orse
than
like
the
hero
in u
ser..
. Som
ebod
y w
ho ta
kes s
tero
ids i
s bot
here
d w
hat s
omeb
ody
thin
ks ..
. peo
ple
who
do
bod
y bu
ildin
g ha
ve u
sual
ly g
ot lo
w se
lf-es
teem
any
way
, tha
t’s
why
they
star
t doi
ng it
in th
e fir
st p
lace
.” (C
01)
“You
see,
the
dang
er is
... it
is a
ll un
derg
roun
d...
I thi
nk m
edic
al
peop
le te
nd to
look
dow
n on
you
if y
ou a
re [u
sing
ana
bolic
–an
drog
enic
ste
roid
s]. I
t’s y
our f
ault
you’
re in
her
e. Y
ou k
now
, whe
n I
was
in h
ospi
tal I
did
n’t g
et th
at fa
ct, b
ut I e
ven
said
to m
y co
nsul
tant
: I k
now
I pro
babl
y br
ough
t mys
elf i
n he
re. I
hol
d m
y ha
nds u
p,
y’kn
ow, a
nd n
ot m
any
peop
le w
ould
say
that
, but
I adm
itted
it.”
(C
03)

16Ta
ble
2 co
ntin
ued.
Tabl
e 2
cont
inue
d ov
erle
af.
No.
2.2
Them
e
Iden
tity
man
agem
ent
and
rela
tions
hip
with
se
rvic
es
Obs
erva
tion
Mis
unde
rsto
od/u
nder
valu
ed m
otiv
atio
nsA
num
ber o
f par
ticip
ants
usi
ng A
AS
felt
that
he
alth
pro
fess
iona
ls o
ften
mis
unde
rsto
od p
eopl
e’s
reas
ons
for u
sing
AA
S an
d ot
her I
PED
s an
d/or
did
no
t cre
dit p
eopl
e w
ho u
se A
AS
for e
xper
tise
in
achi
evin
g sp
ortin
g or
aes
thet
ic g
oals
. Co
mm
ents
mad
e du
ring
the
serv
ice
prov
ider
in
terv
iew
s su
ppor
ted
this
bel
ief,
whe
re m
any
repo
rted
that
the
peop
le th
ey s
aw w
ho w
ere
usin
g,
or th
inki
ng a
bout
usi
ng, A
AS
and
othe
r IPE
Ds,
wer
e do
ing
so b
ecau
se th
ey w
ante
d to
get
a q
uick
er
resu
lt. T
hat i
s, th
ey w
ante
d to
impr
ove
thei
r bod
ies’
appe
aran
ce m
ore
quic
kly
or w
ith le
ss e
ffort
.
Part
icip
ant
Part
icip
ants
usi
ng A
AS
Part
icip
ants
usi
ng A
AS
Part
icip
ants
usi
ng A
AS
Serv
ice
Prov
ider
Serv
ice
Prov
ider
Part
icip
ants
usi
ng A
AS
Evid
ence
gat
herin
g ev
ent
Evid
ence
“To
be th
e be
st I c
an e
very
day
. I w
ant t
o be
the
stro
nges
t I ca
n, th
e fit
test
I can
and
in th
e be
st sh
ape
I can
.” (D
A11
)
“I th
ink
it’s b
asic
ally
dow
n to
stig
ma.
It’s
stig
ma
and
a la
ck o
f un
ders
tand
ing
or a
lack
of k
now
ledg
e on
a G
P’s p
art c
oz th
ey ju
st
thin
k yo
u do
it a
nd y
ou w
anna
be
bigg
er, f
aste
r, st
rong
er, a
s big
as
you
can
get a
nd, y
ou k
now
, the
y do
n’t t
ake
it in
to a
ccou
nt th
at so
me
peop
le w
ho c
hoos
e th
at li
fest
yle,
don
’t ch
oose
it li
ghtly
and
they
will
do
it a
nd th
ey w
ill h
ave
ultim
ate
com
mitm
ent t
o it
– th
ey ca
n te
ll yo
u ev
eryt
hing
they
eat
, the
y tr
ack
all t
heir
mac
ros,
ever
ythi
ng is
ca
lcul
ated
, the
ir tim
ings
, the
ir st
acks
, y’k
now
, whe
n th
ey g
o in
to P
C,
they
kno
w e
very
thin
g ab
out i
t and
they
’ve
com
mitt
ed so
muc
h tim
e bu
t the
n th
ey ca
n ju
st g
et p
oo-p
ooed
by
a do
ctor
goi
ng, ‘s
tero
id u
ser,
out y
ou g
o.”
(DA
07)
“I th
ink
othe
r peo
ple’s
per
cept
ions
of s
omeo
ne w
ho u
ses
perf
orm
ance
enh
anci
ng d
rugs
is th
ey a
re, y
ou k
now
, 225
pou
nds,
an
arse
hole
, coz
they
’ve
got s
uch
ange
r pro
blem
s. I t
hink
oth
er p
eopl
e’s
perc
eptio
ns a
re w
here
the
issu
es li
es. I
’m n
ot e
mba
rras
sed
- it’s
just
ot
her p
eopl
e th
ink,
they
exp
ect y
ou to
be
like
som
e ra
ge m
onst
er a
nd
that
you
’re g
oing
to b
e hu
ge.”
(DA
07)
“bec
ause
I thi
nk w
e ar
e na
tion
of q
uick
fix,
we
wan
t eve
ryth
ing
now
, w
ant i
t tod
ay”
(GM
03)
“Peo
ple
wan
ting
to c
ut co
rner
s” (
GM
04)
“A lo
t of p
eopl
e I t
rain
with
I kno
w w
ould
n’t w
ant t
o go
to A
&E o
r w
ould
n’t w
ant t
o go
to th
eir d
octo
r and
they
wou
ldn’
t wan
t any
re
cord
of t
hem
usi
ng st
eroi
ds.”
(DA
01)
It w
as n
oted
that
som
e pe
ople
saw
the
use
of A
AS
and
othe
r IP
EDs
as a
‘qui
ck fi
x’ to
get
ting
a be
tter
bod
y or
bei
ng fi
tter
.
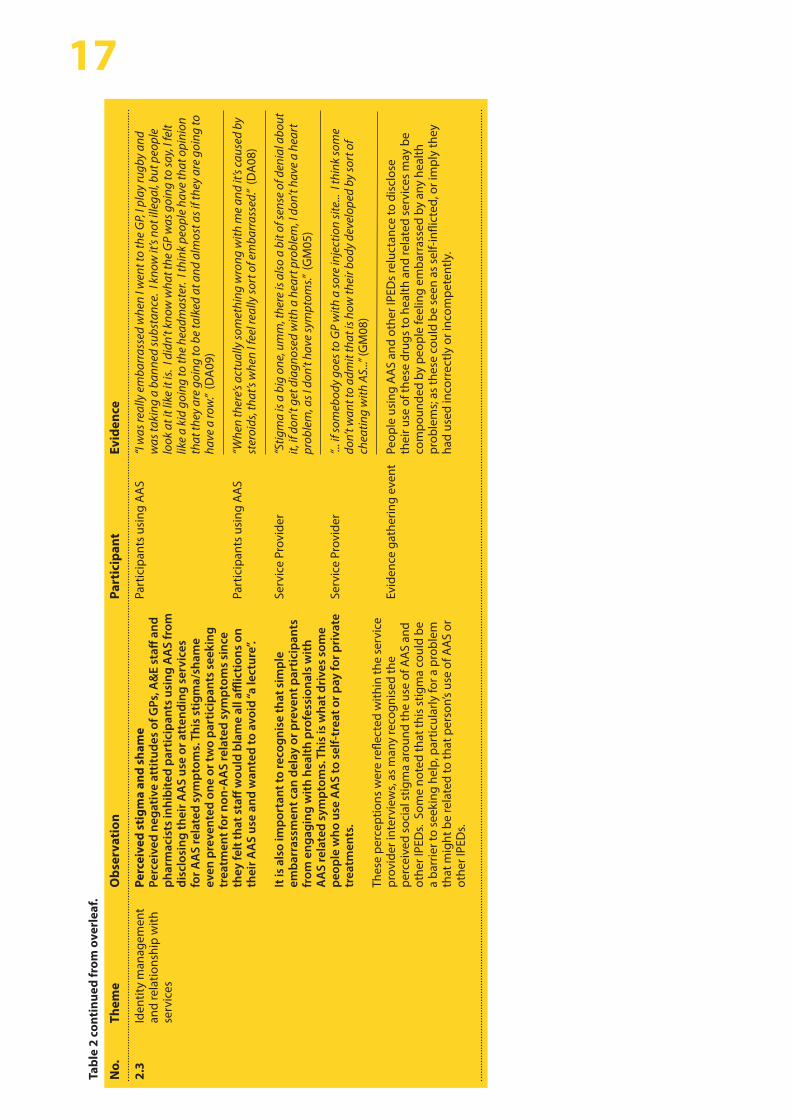
17Ta
ble
2 co
ntin
ued
from
ove
rlea
f.
No.
2.3
Them
e
Iden
tity
man
agem
ent
and
rela
tions
hip
with
se
rvic
es
Obs
erva
tion
Perc
eive
d st
igm
a an
d sh
ame
Perc
eive
d ne
gativ
e at
titud
es o
f GPs
, A&
E st
aff a
nd
phar
mac
ists
inhi
bite
d pa
rtic
ipan
ts u
sing
AA
S fr
om
disc
losi
ng th
eir A
AS
use
or a
tten
ding
ser
vice
s fo
r AA
S re
late
d sy
mpt
oms.
Thi
s st
igm
a/sh
ame
even
pre
vent
ed o
ne o
r tw
o pa
rtic
ipan
ts s
eeki
ng
trea
tmen
t for
non
-AA
S re
late
d sy
mpt
oms
sinc
e th
ey fe
lt th
at s
taff
wou
ld b
lam
e al
l affl
ictio
ns o
n th
eir A
AS
use
and
wan
ted
to a
void
“a le
ctur
e”.
It is
als
o im
port
ant t
o re
cogn
ise
that
sim
ple
emba
rras
smen
t can
del
ay o
r pre
vent
par
ticip
ants
fr
om e
ngag
ing
with
hea
lth p
rofe
ssio
nals
with
A
AS
rela
ted
sym
ptom
s. T
his
is w
hat d
rive
s so
me
peop
le w
ho u
se A
AS
to s
elf-
trea
t or p
ay fo
r pri
vate
tr
eatm
ents
.
Thes
e pe
rcep
tions
wer
e re
flect
ed w
ithin
the
serv
ice
prov
ider
inte
rvie
ws,
as m
any
reco
gnis
ed th
e pe
rcei
ved
soci
al s
tigm
a ar
ound
the
use
of A
AS
and
othe
r IPE
Ds.
Som
e no
ted
that
this
stig
ma
coul
d be
a
barr
ier t
o se
ekin
g he
lp, p
artic
ular
ly fo
r a p
robl
em
that
mig
ht b
e re
late
d to
that
per
son’
s us
e of
AA
S or
ot
her I
PED
s.
Part
icip
ant
Part
icip
ants
usi
ng A
AS
Part
icip
ants
usi
ng A
AS
Serv
ice
Prov
ider
Serv
ice
Prov
ider
Evid
ence
gat
herin
g ev
ent
Evid
ence
“I w
as re
ally
em
barr
asse
d w
hen
I wen
t to
the
GP,
I pla
y ru
gby
and
was
taki
ng a
ban
ned
subs
tanc
e. I
know
it’s
not i
llega
l, bu
t peo
ple
look
at i
t lik
e it
is. I
didn
’t kn
ow w
hat t
he G
P w
as g
oing
to sa
y, I f
elt
like
a ki
d go
ing
to th
e he
adm
aste
r. I t
hink
peo
ple
have
that
opi
nion
th
at th
ey a
re g
oing
to b
e ta
lked
at a
nd a
lmos
t as i
f the
y ar
e go
ing
to
have
a ro
w.”
(DA
09)
“Whe
n th
ere’s
act
ually
som
ethi
ng w
rong
with
me
and
it’s c
ause
d by
st
eroi
ds, t
hat’s
whe
n I f
eel r
eally
sort
of e
mba
rras
sed.
” (D
A08
)
“Stig
ma
is a
big
one
, um
m, t
here
is a
lso
a bi
t of s
ense
of d
enia
l abo
ut
it, if
don
’t ge
t dia
gnos
ed w
ith a
hea
rt p
robl
em, I
don
’t ha
ve a
hea
rt
prob
lem
, as I
don
’t ha
ve sy
mpt
oms.”
(G
M05
)
“... i
f som
ebod
y go
es to
GP
with
a so
re in
ject
ion
site
... I
thin
k so
me
don’
t wan
t to
adm
it th
at is
how
thei
r bod
y de
velo
ped
by so
rt o
f ch
eatin
g w
ith A
S...”
(GM
08)
Peop
le u
sing
AA
S an
d ot
her I
PED
s re
luct
ance
to d
iscl
ose
thei
r use
of t
hese
dru
gs to
hea
lth a
nd re
late
d se
rvic
es m
ay b
e co
mpo
unde
d by
peo
ple
feel
ing
emba
rras
sed
by a
ny h
ealth
pr
oble
ms;
as
thes
e co
uld
be s
een
as s
elf-i
nflic
ted,
or i
mpl
y th
ey
had
used
inco
rrec
tly o
r inc
ompe
tent
ly.

The observations and evidence related to the third theme Service delivery, practices and policy taken from qualitative interviews with participants using AAS, service providers and Evidence Gathering and Synthesis Event discussions are detailed in Table 3 (T3).
A range of issues related to service accessibility and acceptability were noted, including service opening times, service locations, and the environments in which services were provided. For many of the participants interviewed who were using AAS, the topic of confidentiality and the fear of their use of AAS and other IPEDs being recorded within medical records and notes was seen as a significant barrier in engaging with healthcare services [T3 row 3.1]. Their concerns ranged from the fear of being judged at a later date to medical records being passed to employers occupational health departments. This has led to a number of approaches being adopted amongst those individuals including; self-treatment of minor side effects, use of online services to access blood testing and injecting paraphernalia [T3 row 3.3]. There were varying opinions on whether co-provision of services for those using AAS and other IPEDs alongside those for people using psychoactive drugs was appropriate [T3 row 3.2]. Provision of stand-alone services with separate infrastructure is likely to be costly, and probably not sustainable where these would be delivering similar interventions to those provided to people using psychoactive drugs, such as, the provision of clean sterile injecting equipment through needle and syringe programmes. However, in relation to more specialist services focused on IPED specific issues, standalone services may be more practical if these were hosted within generic services. The form and practicalities of such services needs further examination, but the recent development of such a service in Newport, Gwent provides a possible model. The development of such service requires further exploration of a range of delivery models, for example, shared care systems with GPs and e-clinics. Such methods could facilitate ease of access to specialist services across Wales, particularly in rural areas.
The resultant problems with engagement was a very common concern raised repeatedly during the study. Participants suggested various approaches that could be used to improve engagement with services; however, the provision of services by informed, empathetic, and non-judgemental staff was seen as being key to improving engagement [T3 row 3.4]. Some participants indicated that service staff were sometimes overly concerned about not having a complete understanding of the nature of the drugs involved and their use; however, in many settings such knowledge is not necessary to engage with this group. For example, in needle and syringe programmes focusing on harm reduction and practical messages related to injection technique could be an effective approach to engagement. In relation to engaging clients about testing for sexually transmitted and blood borne viral infections, discussions focused around sexual risks are probably a more appropriate and effective approach, than discussions related to risk of infection transmission through injecting.
The use of outreach approaches to access people using AAS and other IPEDs, or who might be thinking about using these drugs, in gyms and other fitness venues was felt to be particularly important; however, there are a number of barriers to this, in particular gaining the support of the venue owners [T3 row 3.3]. Such outreach activities may be particularly effective if they involve credible messengers and peers in their delivery.
18
4.3 Service delivery, practices and policy
4.3.1 Barriers and facilitators to service engagement
For Table 3 - see overleaf.
The provision of more generic well-being services – either through outreach or in fixed sites – focusing on health, wellbeing and fitness, particularly if targeted at young people, may have a role preventing use and supporting other approaches to fitness, such as, diet and training, as well as reducing harm among those who go on to use AAS and other IPEDs.
Related to this, there was concern among those providing services about the lack of access to metabolic testing and treatment interventions for those using AAS and other IPEDs, as currently there are no approved treatment interventions [T3 row 3.5]. Concerns about the provision of, and access to, care for mental health issues for those using IPEDs was very common among the participants. Mental health issues may underpin the use of AAS and other IPEDs for some people, and so being able to address these issues is an important aspect of an effective response.
From a policy perspective, service providers and evidence gathering event attendees were particularly concerned about the lack of guidance in relation to providing services to those who use IPEDs, and the related lack of clear and well-defined care and referral pathways for them [T3 row 3.7]. It was suggested this needs to be addressed through development of guidelines on appropriate responses to the use of AAS and other IPEDs for health and wellbeing service providers. There was also support for the provision of guidance to the operators of gyms and fitness venues so as to support outreach, harm reduction interventions, and early identification of those who are experiencing problems related to their use of AASs or other IPEDs.
19
4.3.2 Policy issues

>20
Tabl
e 3:
Sum
mar
y ob
serv
atio
ns a
nd e
vide
nce
rela
ting
to S
ervi
ce D
eliv
ery,
Pra
ctic
es a
nd P
olic
y ta
ken
from
qua
litat
ive
inte
rvie
ws
wit
h pa
rtic
ipan
ts u
sing
AA
S, s
ervi
ce p
rovi
ders
and
Evi
denc
e G
athe
ring
and
Syn
thes
is E
vent
dis
cuss
ions
No.
3.1
Them
e
Barr
iers
to s
ervi
ce
enga
gem
ent
Obs
erva
tion
Avo
idin
g do
cum
enta
tion
on
med
ical
reco
rds
Furt
her t
o th
e co
mm
ents
rela
ted
to th
e st
igm
a of
us
ing
IPED
s, m
any
part
icip
ants
usi
ng A
AS
desc
ribed
th
eir r
eluc
tanc
e to
eng
age
in h
ealth
care
ser
vice
s or
dis
clos
e us
e as
a w
ay o
f pre
vent
ing
it be
ing
docu
men
ted
on th
eir m
edic
al re
cord
s. It
was
felt
that
by
doin
g so
it w
ould
pre
vent
futu
re n
egat
ive
repe
rcus
sion
s.
Such
fear
s an
d be
liefs
wer
e al
so re
cogn
ised
as
part
of
the
serv
ice
prov
ider
inte
rvie
ws.
They
add
ed th
at
in s
ome
case
s th
is s
tem
med
from
con
cern
s th
at
heal
th re
cord
s co
uld
be tr
ansf
erre
d to
occ
upat
iona
l he
alth
ser
vice
s an
d eff
ect c
urre
nt a
nd/o
r fut
ure
empl
oym
ent.
Part
icip
ant
Part
icip
ants
usi
ng A
AS
Part
icip
ants
usi
ng A
AS
Serv
ice
Prov
ider
Serv
ice
Prov
ider
Serv
ice
Prov
ider
Evid
ence
gat
herin
g ev
ent
Evid
ence
gat
herin
g ev
ent
Evid
ence
“I pa
id a
nd h
ad [m
y bl
ood
test
s] se
nt o
ff be
caus
e I d
idn’
t wan
t tha
t go
ing
dow
n as
a n
egat
ive
on m
y m
edic
al re
cord
, sam
e as
a lo
t of
peop
le I k
now
bec
ause
of t
he st
igm
a in
volv
ed. T
hey
just
go
thro
ugh
your
med
ical
reco
rds g
oing
, ‘Ah,
I see
you
’ve
been
taki
ng st
eroi
ds.’
It’s j
ust t
he n
egat
ive
stig
ma
and
the
lack
of u
nder
stan
ding
.” (D
A07
)
“I w
ould
n’t w
ant a
nyth
ing
writ
ten
dow
n on
any
reco
rd w
ith m
y na
me
that
I use
ster
oids
. The
re’s
so m
uch
nega
tivity
... I
know
peo
ple
who
are
so fr
ight
ened
to g
o to
a n
eedl
e ex
chan
ge in
case
they
get
se
en...
I do
n’t t
hink
peo
ple
wan
t to
risk
othe
rs k
now
ing
outs
ide
of th
e gy
m fr
ater
nity
.” (D
A01
)
“Abs
olut
ely
will
not
talk
abo
ut it
eith
er b
ecau
se u
sing
IPED
s tha
t are
ill
egal
and
fear
repe
rcus
sion
s of t
hat,
and
also
alo
ng w
ith IP
EDs t
hey
are
usin
g ot
her i
llega
l sub
stan
ces,
so a
bsol
utel
y w
on’t
talk
bec
ause
of
fear
it m
ight
get
out
“ (G
M05
)
“[In
rela
tion
to u
sing
GPs
] the
re is
real
conc
ern
as w
ell a
bout
co
nfide
ntia
lity
and
thin
gs b
eing
on
med
ical
reco
rds a
nd th
ose
sort
of
thin
gs b
ecau
se th
ey a
lot o
f peo
ple
do h
ave
high
pow
ered
jobs
...“
(GM
01)
“Fea
r of i
t goi
ng o
n th
eir m
edic
al re
cord
s, of
bei
ng ju
dged
.” (G
M02
)
Ass
essm
ents
for n
ew c
lient
s, in
clud
ing
the
need
to g
ive
pers
onal
id
entifi
catio
n da
ta, w
ith m
any
of th
ose
usin
g A
AS
and
othe
r IP
EDs
bein
g ve
ry w
ary
abou
t giv
ing
out a
ny s
uch
info
rmat
ion.
Th
is w
as p
art o
f wid
er c
once
rn a
bout
con
fiden
tially
and
the
lack
of
priv
acy.
Priv
acy
issu
es in
clud
ed c
once
rns
abou
t bei
ng s
een
in a
ne
edle
and
syr
inge
pro
gram
me,
and
abo
ut c
onfid
entia
lity
whe
n at
tend
ing
prim
ary
care
bei
ng c
ompr
omis
ed b
y th
e nu
mbe
r of
staff
who
cou
ld a
cces
s m
edic
al re
cord
s.
Cont
actin
g a
prim
ary
or s
econ
dary
hea
lthca
re s
ervi
ce a
bout
a
heal
th p
robl
em w
ould
requ
ire d
iscl
osur
e of
thei
r use
of a
nabo
lic–
andr
ogen
ic s
tero
ids
and
othe
r IPE
Ds,
resu
lting
in c
once
rns
abou
t th
e co
nseq
uenc
es, s
uch
as in
form
atio
n ab
out t
heir
use
goin
g on
med
ical
reco
rds.
This
was
see
n by
par
ticip
ants
as
bein
g a
part
icul
arly
impo
rtan
t iss
ue w
here
ther
e w
ere
occu
patio
nal
reas
ons
for u
se.
Tabl
e 3
cont
inue
d ov
erle
af.

21Ta
ble
3 co
ntin
ued.
No.
3.2
Them
e
Barr
iers
to s
ervi
ce
enga
gem
ent
Obs
erva
tion
Perc
epti
ons
surr
ound
ing
‘dru
g us
e’ a
nd
plac
emen
t of s
ervi
ces
Se
rvic
e pr
ovid
ers
note
d th
at th
ose
peop
le th
at th
ey
saw
who
wer
e us
ing
AA
S an
d ot
her I
PED
s do
not
se
e th
eir u
se o
f the
se d
rugs
as
bein
g ‘d
rug
use’.
The
y al
l not
ed th
at p
eopl
e us
ing
IPED
s sa
w th
emse
lves
as
bei
ng d
iffer
ent f
rom
peo
ple
usin
g dr
ugs
for t
heir
psyc
hoac
tive
effec
ts.
They
wer
e al
so c
once
rned
abo
ut th
e ap
prop
riate
ness
of
gen
eric
sub
stan
ce u
se s
ervi
ces,
such
as
need
le
and
syrin
ge p
rogr
amm
es, t
o th
ose
usin
g A
AS
and
othe
r IPE
Ds,
part
icul
arly
as
this
gro
up o
ften
sa
w th
emse
lves
as
bein
g di
ffere
nt to
thos
e us
ing
psyc
hoac
tive
drug
s an
d di
d no
t wan
t to
use
the
sam
e se
rvic
es a
s th
em.
Thes
e at
titud
es w
here
mir
rore
d du
ring
the
inte
rvie
ws
with
the
part
icip
ants
usi
ng A
AS,
with
m
any
ackn
owle
dgin
g it
was
diffi
cult
atte
ndin
g se
rvic
es w
here
they
felt
they
wer
e vi
ewed
as
a ‘d
rug
user
’.
Part
icip
ant
Serv
ice
Prov
ider
Serv
ice
Prov
ider
Part
icip
ants
usi
ng A
AS
Part
icip
ants
usi
ng A
AS
Part
icip
ants
usi
ng A
AS
Part
icip
ants
usi
ng A
AS
Serv
ice
Prov
ider
Serv
ice
Prov
ider
Evid
ence
“[th
ey] d
on’t
see
them
selv
es a
s dru
g us
ers”
(G
M03
)
“the
y vi
ew th
e su
bsta
nce
they
are
usi
ng a
s not
in sa
me
leag
ue a
s so
meo
ne u
sing
opi
ates
.” (G
M07
)
“I’ve
alw
ays f
elt t
here
’s a
bit o
f a n
egat
ive
attit
ude
tow
ards
ster
oid
user
s... I
kno
w p
eopl
e w
ho a
re so
frig
hten
ed to
go
to a
nee
dle
exch
ange
in ca
se th
ey g
et se
en, i
f the
y ca
me
away
with
ten
syrin
ges
they
wou
ld re
-use
them
.” (D
A01
)
“I di
dn’t
know
abo
ut sp
ecia
list e
xcha
nges
. I w
ould
n’t g
o an
yway
as
whe
n I g
o to
the
Chem
ist i
t’s a
pub
lic p
rem
ise/
serv
ice
and
I cou
ld
be g
oing
ther
e fo
r any
thin
g. G
oing
to o
ne o
f tho
se p
lace
s [ne
edle
ex
chan
ge] w
ould
put
me
in th
at ty
pe o
f box
, wou
ldn’
t it?
By
box,
I m
ean
drug
use
r.” (
DA
10)
“I w
ent t
o a
loca
l dru
g se
rvic
e an
d sp
oke
to so
meo
ne in
the
need
le
exch
ange
– th
at w
as h
ard
as I k
now
it’s
a pl
ace
whe
re ju
nkie
s go,
an
d th
e m
ain
door
look
s out
ont
o th
e m
ain
road
.” (D
A09
)
”You
kno
w w
hen
I use
d to
go
to in
to th
e dr
ug p
lace
s [ne
edle
and
sy
ringe
pro
gram
me]
to g
et m
y ne
edle
s... t
here
wer
e he
roin
add
icts
in
ther
e, th
ere
wer
e co
cain
e ad
dict
s... I
alw
ays t
houg
ht to
mys
elf,
y’kn
ow, I
’m n
ot w
here
you
are
– I’v
e go
t my
own
min
d, I k
now
wha
t I’m
doi
ng. I
t doe
sn’t
take
me
into
ano
ther
wor
ld b
asic
ally
. I’m
still
in
the
real
wor
ld, e
ven
thou
gh I’m
doi
ng th
at.”
(C03
)
“... a
lot o
f AAS
use
rs d
on’t
like
com
ing
in [t
o th
e ne
edle
and
syrin
ge
prog
ram
me]
whe
n th
ere
are
othe
r use
rs...
like
her
oin
user
s, be
caus
e th
ey th
ink
they
hav
en’t
got a
pro
blem
... t
hey
don’
t rea
lly co
me
in
and
have
a c
hat,
if yo
u kn
ow w
hat I
mea
n, li
tera
lly ju
st co
me
in a
nd
ask
for w
hat t
hey
wan
t and
go“
(G
M08
)
“IPED
use
rs d
on’t
like
goin
g to
NSP
... t
hey
see
them
selv
es a
s... w
e ar
e he
alth
y, w
e ar
e lo
okin
g af
ter o
ur h
ealth
, we
are
heal
th co
nsci
ous;
they
[oth
er N
SP u
sers
] are
not
” (G
M05
)

22
Tabl
e 3
cont
inue
d ov
erle
af.
Tabl
e 3
cont
inue
d.
No.
3.3
3.4
Them
e
Barr
iers
to s
ervi
ce
enga
gem
ent
Faci
litat
ors
to s
ervi
ce
enga
gem
ent
Obs
erva
tion
Acc
essi
bilit
y of
ser
vice
s an
d on
line
alte
rnat
ives
Man
y se
rvic
e pr
ovid
ers
repo
rted
con
cern
s ab
out
the
open
ing
hour
s of
ser
vice
s, su
ch a
s ne
edle
and
sy
ringe
pro
gram
mes
, as
thos
e us
ing
AA
S an
d ot
her
IPED
s w
ere
typi
cally
em
ploy
ed.
From
the
inte
rvie
ws
with
bot
h se
rvic
e pr
ovid
ers
and
part
icip
ants
usi
ng A
AS
it w
as c
lear
that
util
isat
ion
of
onlin
e se
rvic
es fo
r obt
aini
ng in
ject
ing
para
pher
nalia
an
d un
dert
akin
g m
etab
olic
test
ing
wer
e bo
th
com
mon
pla
ce. S
uch
serv
ices
wer
e vi
ewed
as
mor
e co
nven
ient
and
acc
essi
ble
whe
n co
mpa
red
to
trad
ition
al m
etho
ds o
f ser
vice
del
iver
y. T
his
refle
cts
the
issu
es w
ith a
ccep
tabi
lity
and
avai
labi
lity
of th
e ne
edle
and
syr
inge
pro
gram
mes
whe
re th
e sa
me
equi
pmen
t can
be
obta
ined
for f
ree.
Thro
ugho
ut d
iscu
ssio
ns d
urin
g th
e ev
iden
ce
gath
erin
g ev
ent i
t was
not
ed th
at o
utre
ach
serv
ices
ha
ve h
ad p
ositi
ve o
utco
mes
whe
re ra
ppor
t and
a
rela
tions
hip
has
been
mad
e w
ith g
ym o
wne
rs a
nd
clie
ntel
e.
Non
-judg
men
tal a
nd in
form
ed a
ppro
ach
Am
ongs
t the
par
ticip
ants
usi
ng A
AS,
key
fa
cilit
ator
s to
ser
vice
eng
agem
ent i
nclu
ded
non-
judg
emen
tal a
nd k
now
ledg
eabl
e st
aff w
ho
wer
e w
illin
g to
eng
age
in d
ialo
gue.
Fur
ther
mor
e,
reve
rsin
g th
e cl
imat
e of
dis
appr
oval
whi
ch p
eopl
e w
ho u
se A
AS
felt
surr
ound
ed fr
ont l
ine
serv
ices
w
as th
e m
ost p
rom
inen
t top
ic o
f con
vers
atio
n.
Serv
ice
prov
ider
s re
cogn
ised
that
sta
ff sk
ill s
et w
ithin
se
rvic
es c
ould
lim
it eff
ectiv
e se
rvic
e pr
ovis
ion.
H
owev
er, m
any
of th
e pa
rtic
ipan
ts in
this
con
text
w
ere
over
ly fo
cuse
d on
wha
t the
y pe
rcei
ved
to b
e th
eirs
, and
thei
r col
leag
ues,
limite
d kn
owle
dge
abou
t the
dru
gs b
eing
use
d. E
ven
thou
gh fo
r man
y th
is s
houl
d no
t hav
e im
pact
ed o
n en
gage
men
t ar
ound
issu
es re
late
d to
saf
e in
ject
ion
prac
tice,
se
xual
risk
, and
mot
ivat
ion
for u
se.
Part
icip
ant
Serv
ice
Prov
ider
Part
icip
ants
usi
ng A
AS
Part
icip
ants
usi
ng A
AS
Evid
ence
gat
herin
g ev
ent
Part
icip
ants
usi
ng A
AS
Part
icip
ants
usi
ng A
AS
Serv
ice
Prov
ider
Evid
ence
In re
latio
n to
acc
essi
ng n
eedl
e an
d sy
ringe
pro
gram
mes
: “...
the
y ar
e bu
ying
it [n
eedl
es a
nd s
yrin
ges]
onl
ine,
and
they
don
’t w
ant
to h
ave
to g
o in
to a
nee
dle
exch
ange
, and
they
don
’t w
ant t
o w
ait,
and
they
don
’t w
ant t
he st
igm
a; a
s wel
l it q
uite
rare
to co
me
acro
ss
som
eone
who
kno
wns
a si
gnifi
cant
am
ount
abo
ut th
em...“
(G
M01
)
“I kn
ow p
eopl
e w
ho b
uy a
ll th
eir e
quip
men
t onl
ine.
.. T
hey
buy
it on
line
for c
onve
nien
ce. Y
ou k
now
, you
coul
d ar
gue,
wel
l you
coul
d go
to a
pha
rmac
y. Y
eah,
I cou
ld g
o to
a p
harm
acy
on a
Sat
urda
y an
d Su
nday
whe
n it’
s ful
l of p
eopl
e. D
on’t
wan
t tha
t. It
’s ba
d en
ough
that
peo
ple
will
turn
aro
und
and
go ‘U
uugh
’. Li
ke I s
aid
it’s
such
a st
igm
a.”
(DA
07)
“I pa
id a
nd h
ad [m
y bl
ood
test
s] se
nt o
ff be
caus
e I d
idn’
t wan
t tha
t go
ing
dow
n as
a n
egat
ive
on m
y m
edic
al re
cord
, sam
e as
a lo
t of
peop
le I k
now
bec
ause
of t
he st
igm
a in
volv
ed.”
(DA
07)
Serv
ices
wer
e pe
rcei
ved
as ty
pica
lly n
ot b
eing
ope
n at
tim
es
whi
ch a
re c
onve
nien
t for
thos
e w
ho w
ere
wor
king
or i
n ed
ucat
ion,
and
that
ther
e w
as a
nee
d fo
r var
iabl
e op
enin
g tim
es
for h
ealth
ser
vice
s, in
clud
ing
need
le a
nd s
yrin
ge s
ervi
ces,
with
so
me
indi
catin
g th
is c
an re
sult
in b
ette
r tak
e-up
.
“I th
ink
a be
tter
und
erst
andi
ng, e
duca
tion.
If a
doc
tor h
ad a
bet
ter
unde
rsta
ndin
g, I t
hink
you
wou
ld g
et a
bet
ter u
ptak
e. I
can
wal
k in
to a
ny o
f the
gym
s...
boys
will
com
e up
to m
e lik
e an
d ha
ve
the
mos
t ope
n co
nver
satio
ns w
ith m
e...
Out
of t
he b
lue,
that
’s th
e co
nver
satio
ns th
at h
appe
ns in
gym
s.” (
DA
07)
“If a
cent
re h
ad sp
ecifi
c se
ssio
n fo
r ste
roid
use
rs, t
hen
you
wou
ld
know
who
was
goi
ng to
be
behi
nd th
e do
or a
nd th
ey w
ould
be
roug
hly
awar
e of
why
you
wer
e th
ere
with
out y
ou h
avin
g to
star
t w
ith, ‘A
nd it
’s be
caus
e I u
se st
eroi
ds’.
I don
’t kn
ow w
here
you
’d o
ut it
th
ough
as I
thin
k pe
ople
wou
ldn’
t wan
t to
be se
en w
alki
ng in
, may
be
on a
n in
dust
rial e
stat
e.” (
DA
09)
“A lo
t of i
t is t
ime,
in th
at w
hen
they
com
e in
for e
quip
men
t the
y ju
st
kind
of w
ant t
o be
in a
nd o
ut th
e do
n’t w
ant t
o be
han
ging
... a
nd
may
be
priv
acy
as w
ell..
. and
then
from
our
poi
nt v
iew
wou
ld b
e co
nfide
nce
to st
art t
he co
nver
satio
n, to
kno
w th
at w
hat y
ou w
ere
sayi
ng w
as ri
ght a
nd th
at y
ou w
ere
givi
ng g
ood
advi
ce...
” (G
M06
)
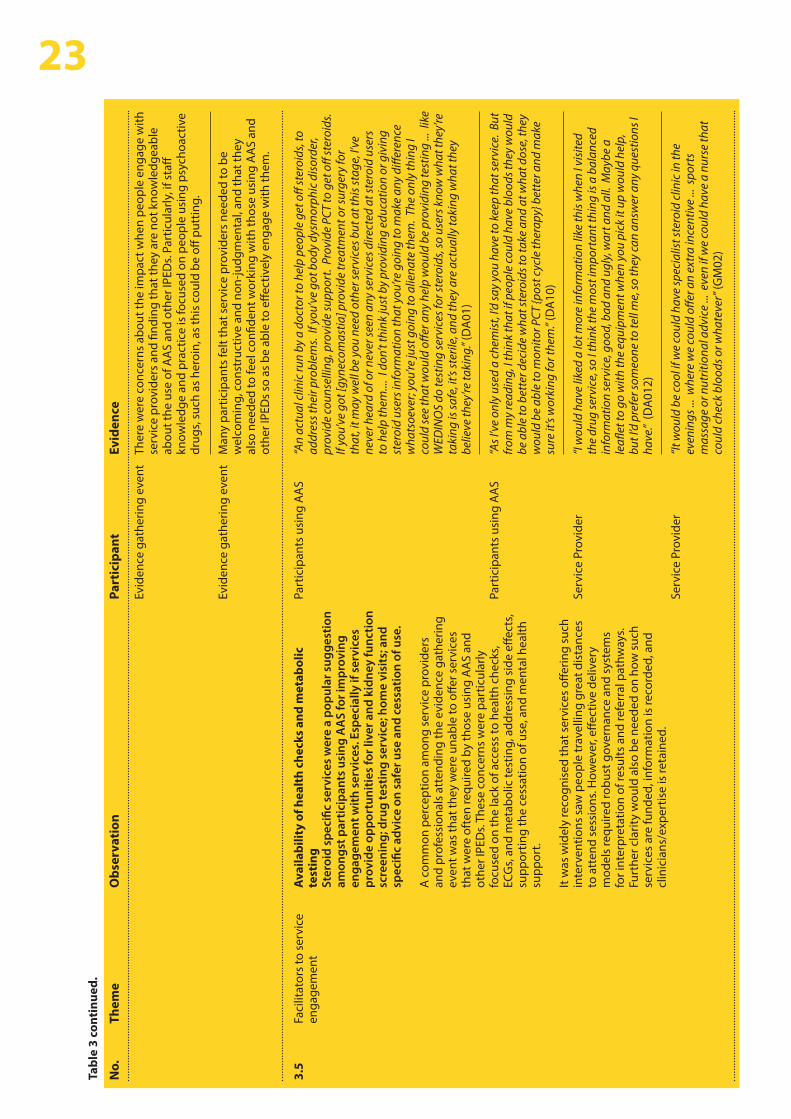
23Ta
ble
3 co
ntin
ued.
No.
3.5
Them
e
Faci
litat
ors
to s
ervi
ce
enga
gem
ent
Obs
erva
tion
Ava
ilabi
lity
of h
ealt
h ch
ecks
and
met
abol
ic
test
ing
Ster
oid
spec
ific
serv
ices
wer
e a
popu
lar s
ugge
stio
n am
ongs
t par
ticip
ants
usi
ng A
AS
for i
mpr
ovin
g en
gage
men
t with
ser
vice
s. E
spec
ially
if s
ervi
ces
prov
ide
oppo
rtun
ities
for l
iver
and
kid
ney
func
tion
scre
enin
g; d
rug
test
ing
serv
ice;
hom
e vi
sits
; and
sp
ecifi
c ad
vice
on
safe
r use
and
ces
satio
n of
use
. A
com
mon
per
cept
ion
amon
g se
rvic
e pr
ovid
ers
and
prof
essi
onal
s at
tend
ing
the
evid
ence
gat
herin
g ev
ent w
as th
at th
ey w
ere
unab
le to
offe
r ser
vice
s th
at w
ere
ofte
n re
quire
d by
thos
e us
ing
AA
S an
d ot
her I
PED
s. Th
ese
conc
erns
wer
e pa
rtic
ular
ly
focu
sed
on th
e la
ck o
f acc
ess
to h
ealth
che
cks,
ECG
s, an
d m
etab
olic
test
ing,
add
ress
ing
side
effe
cts,
supp
ortin
g th
e ce
ssat
ion
of u
se, a
nd m
enta
l hea
lth
supp
ort.
It w
as w
idel
y re
cogn
ised
that
ser
vice
s off
erin
g su
ch
inte
rven
tions
saw
peo
ple
trav
ellin
g gr
eat d
ista
nces
to
att
end
sess
ions
. How
ever
, effe
ctiv
e de
liver
y m
odel
s re
quire
d ro
bust
gov
erna
nce
and
syst
ems
for i
nter
pret
atio
n of
resu
lts a
nd re
ferr
al p
athw
ays.
Furt
her c
larit
y w
ould
als
o be
nee
ded
on h
ow s
uch
serv
ices
are
fund
ed, i
nfor
mat
ion
is re
cord
ed, a
nd
clin
icia
ns/e
xper
tise
is re
tain
ed.
Part
icip
ant
Evid
ence
gat
herin
g ev
ent
Evid
ence
gat
herin
g ev
ent
Part
icip
ants
usi
ng A
AS
Part
icip
ants
usi
ng A
AS
Serv
ice
Prov
ider
Serv
ice
Prov
ider
Evid
ence
Ther
e w
ere
conc
erns
abo
ut th
e im
pact
whe
n pe
ople
eng
age
with
se
rvic
e pr
ovid
ers
and
findi
ng th
at th
ey a
re n
ot k
now
ledg
eabl
e ab
out t
he u
se o
f AA
S an
d ot
her I
PED
s. Pa
rtic
ular
ly, i
f sta
ff kn
owle
dge
and
prac
tice
is fo
cuse
d on
peo
ple
usin
g ps
ycho
activ
e dr
ugs,
such
as
hero
in, a
s th
is c
ould
be
off p
uttin
g.
Man
y pa
rtic
ipan
ts fe
lt th
at s
ervi
ce p
rovi
ders
nee
ded
to b
e w
elco
min
g, c
onst
ruct
ive
and
non-
judg
men
tal,
and
that
they
al
so n
eede
d to
feel
con
fiden
t wor
king
with
thos
e us
ing
AA
S an
d ot
her I
PED
s so
as
be a
ble
to e
ffect
ivel
y en
gage
with
them
.
“An
actu
al c
linic
run
by a
doc
tor t
o he
lp p
eopl
e ge
t off
ster
oids
, to
addr
ess t
heir
prob
lem
s. If
you
’ve
got b
ody
dysm
orph
ic d
isor
der,
prov
ide
coun
selli
ng, p
rovi
de su
ppor
t. P
rovi
de P
CT to
get
off
ster
oids
. If
you’
ve g
ot [g
ynec
omas
tia] p
rovi
de tr
eatm
ent o
r sur
gery
for
that
, it m
ay w
ell b
e yo
u ne
ed o
ther
serv
ices
but
at t
his s
tage
, I’v
e ne
ver h
eard
of o
r nev
er se
en a
ny se
rvic
es d
irect
ed a
t ste
roid
use
rs
to h
elp
them
.... I
don
’t th
ink
just
by
prov
idin
g ed
ucat
ion
or g
ivin
g st
eroi
d us
ers i
nfor
mat
ion
that
you
’re g
oing
to m
ake
any
diffe
renc
e w
hats
oeve
r; yo
u’re
just
goi
ng to
alie
nate
them
. The
onl
y th
ing
I co
uld
see
that
wou
ld o
ffer a
ny h
elp
wou
ld b
e pr
ovid
ing
test
ing
... li
ke
WED
INO
S do
test
ing
serv
ices
for s
tero
ids,
so u
sers
kno
w w
hat t
hey’
re
taki
ng is
safe
, it’s
ster
ile, a
nd th
ey a
re a
ctua
lly ta
king
wha
t the
y be
lieve
they
’re ta
king
.” (D
A01
)
“As I
’ve
only
use
d a
chem
ist,
I’d sa
y yo
u ha
ve to
kee
p th
at se
rvic
e. B
ut
from
my
read
ing,
I thi
nk th
at if
peo
ple
coul
d ha
ve b
lood
s the
y w
ould
be
abl
e to
bet
ter d
ecid
e w
hat s
tero
ids t
o ta
ke a
nd a
t wha
t dos
e, th
ey
wou
ld b
e ab
le to
mon
itor P
CT {p
ost c
ycle
ther
apy}
bet
ter a
nd m
ake
sure
it’s
wor
king
for t
hem
.” (D
A10
)
“I w
ould
hav
e lik
ed a
lot m
ore
info
rmat
ion
like
this
whe
n I v
isite
d th
e dr
ug se
rvic
e, so
I thi
nk th
e m
ost i
mpo
rtan
t thi
ng is
a b
alan
ced
info
rmat
ion
serv
ice,
goo
d, b
ad a
nd u
gly,
war
t and
all.
May
be a
le
aflet
to g
o w
ith th
e eq
uipm
ent w
hen
you
pick
it u
p w
ould
hel
p,
but I
’d p
refe
r som
eone
to te
ll m
e, so
they
can
answ
er a
ny q
uest
ions
I ha
ve.”
(DA
012)
“It w
ould
be
cool
if w
e co
uld
have
spec
ialis
t ste
roid
clin
ic in
the
even
ings
... w
here
we
coul
d off
er a
n ex
tra
ince
ntiv
e ...
spo
rts
mas
sage
or n
utrit
iona
l adv
ice
... e
ven
if w
e co
uld
have
a n
urse
that
co
uld
chec
k bl
oods
or w
hate
ver”
(GM
02)

24Ta
ble
3 co
ntin
ued.
No.
3.6
3.7
Them
e
Polic
y is
sues
Polic
y is
sues
Obs
erva
tion
Ava
ilabi
lity
of c
linic
al g
uide
lines
Dur
ing
disc
ussi
ons
that
took
pla
ce d
urin
g th
e ev
iden
ce g
athe
ring
even
t man
y hi
ghlig
hted
that
w
hils
t the
re is
will
ingn
ess
to e
xplo
re a
nd d
evel
op
pack
ages
of c
linic
al s
uppo
rt fo
r ind
ivid
uals
usi
ng A
AS
and
othe
r IPE
Ds,
the
avai
labi
lity
of c
linic
al g
uide
lines
re
late
d to
this
topi
c is
cur
rent
ly v
ery
limite
d.
Com
peti
ng o
rgan
isat
iona
l age
ndas
Prof
essi
onal
s at
tend
ing
the
evid
ence
gat
herin
g ev
ent r
ecog
nise
d co
mpe
ting
agen
das
betw
een
orga
nisa
tions
whi
ch c
an re
sult
in in
cons
iste
ncie
s in
ap
proa
ch. T
he d
ispa
rity
betw
een
the
harm
redu
ctio
n ap
proa
ches
ado
pted
by
heal
th s
ervi
ces’
vers
us th
e ab
stin
ence
app
roac
h he
ld b
y sp
ortin
g bo
dies
was
us
ed a
s an
exa
mpl
e to
illu
stra
te th
is p
oint
.
Part
icip
ant
Evid
ence
gat
herin
g ev
ent
Evid
ence
gat
herin
g ev
ent
Evid
ence
Med
ical
pro
fess
iona
l’s re
spon
ses
may
be
limite
d by
thei
r kn
owle
dge
abou
t AA
S an
d ot
her I
PED
s. Th
is c
an b
e pr
oble
mat
ic
as h
avin
g ba
sic
know
ledg
e is
impo
rtan
t to
deliv
erin
g an
effe
ctiv
e re
spon
se to
peo
ple
usin
g A
AS
and
othe
r IPE
Ds
whe
n th
ey s
eek
help
. It w
as fe
lt by
man
y pa
rtic
ipan
ts th
at in
add
ition
to im
prov
ed
trai
ning
, hea
lth a
nd s
ocia
l car
e pr
ovid
ers
need
ed s
ome
form
al
guid
ance
on
AA
S an
d ot
her I
PED
s.
Som
e pa
rtic
ipan
ts fe
lt th
ere
was
a n
eed
for m
ore
focu
s on
this
is
sue
at h
ighe
r lev
els.
The
lack
of a
join
ed u
p ap
proa
ch e
lsew
here
in
the
UK
was
see
n as
a b
arrie
r, as
this
can
resu
lt in
inco
nsis
tent
ap
proa
ches
and
mes
sage
s, w
hich
can
then
hav
e ne
gativ
e im
pact
s on
ove
rall
confi
denc
e in
ser
vice
pro
visi
on. C
ross
-bor
der
patie
nts
have
repo
rted
that
the
use
of A
AS
and
othe
r IPE
Ds
is le
ss
in th
e op
en in
Eng
land
than
it is
in W
ales
. Se
rvic
e pr
ovis
ion
and
qual
ity v
arie
s by
loca
tion,
oft
en re
flect
ing
diffe
ring
agen
das.

Throughout the course of the interviews with participants using AAS, service providers, and the Evidence Gathering and Synthesis Event a range of recommendations for service improvements were suggested for wider discussion and consideration. These are summarised below.
• Making it easier for those using AAS and other IPEDs to access reliable and accurate information. Information needs to be modern and relevant, appropriately targeted and engaging and available in a range of formats • Improve staff skill set through engagement skills training specific to working with those who use AAS and other IPEDs, or who are thinking about doing so • E-learning, particularly for pharmacy counter staff on key issues related to the use of AAS and other IPEDs and engaging with those who use these drugs • Better training of, and engagement with, primary care staff particularly GPs. If GPs engaged effectively with those using AAS and other IPEDs, then they could provide a route to accessing metabolic testing and psychiatric interventions, as well as responding to concerns about acute and chronic harms.
Development of specialist care services • Development of clear healthcare guidelines for providing services to those using AAS and other IPEDs• The provision of more specialist services for those using AAS and other IPEDs was suggested. In particular doctor led specialist clinics for those using these drugs. It was suggested that this could be a virtual specialist GP led clinic with shared care agreements• To develop awareness of, and improve responses to, the use of AAS and other IPEDs it was suggested that GPs with specialist interest and knowledge meet quarterly within cluster protected education time (CPET) meetings – so that they could receive training from GP to GP.
Development of existing harm reduction services • Aim to make service offer appear more engaging to those using AAS and other IPEDs. Engagement should be about offering something that those using AAS and other IPEDs want – such as providing advice on diet or fitness, or access to metabolic testing – and using this to draw people into services so that other interventions can also be delivered• Focusing interactions in generic settings, such as needle and syringe programmes, on injecting, sexual, alcohol and ‘lifestyle’ risks rather than the drug(s) being used • Making existing services more acceptable and accessible to those using AAS and other IPEDs, this could include changes to opening hours, offer of specialist sessions, or a more careful approach to providing broad based drug services as well as improving outreach.
Developing other professional networks
• Closer working between services, with clear ‘care’ pathways for those using AAS and other IPEDs • Improving access to mental health support for those using AAS and other IPEDs through a range of routes • Closer working with Sexual Health Services in relation to testing for sexually transmitted infections and blood borne virus and for access to vaccinations. This should include awareness raising among staff of Sexual Health Services to support them in identifying those using AAS and other IPEDs. This will provide opportunities within these services for referral and advice provision related to use of IPEDs.
254.4 Suggested recommendations for service improvement
Education and awareness raising

26Community and peer to peer approaches • The development of a common document for use by all gyms with ‘dos and don’ts’ for responsible, safer use of supplements, AAS and other IPEDs. With use of this enforced, i.e. gym licenses mandate on displaying harm reduction information• Increasing engagement of those using AAS and other IPEDs with services through the use of social media and outreach into gyms• Develop a peer based network to provide information and harm reduction to those using AAS and other IPEDs – as well chosen peers would be seen as credible messengers • One respondent suggested consideration be given to co-payment for metabolic testing when this was used for physiological monitoring during periods of use. The co-payment would cover only the actual cost of the test advice and interpretation provided by NHS. However, this approach could be problematic in relation to equity of service access.
The suggestions and ideas for possible service developments and improvements that arose either during the two sets of semi-structured interviews or during the discussions that took place during the morning of the Evidence Gathering and Synthesis Event were collated and compared.
These suggestions were condensed and presented to those attending the Evidence Gathering and Synthesis Event for feedback. To explore consensus for each service improvement and development options, the participants used an anonymous online voting app to indicate if they either “Strongly Agreed”, “Agree”, “Disagree”, or “Strongly Disagree” with each option. The number of participants voting on each suggestion varied slightly, with between 25 and 28 valid votes per option. See Figure 3 for voting outcomes for each service improvement and development recommendation.
The proportion indicating agreement (that is voting for either Strongly Agree or Agree) with the development and improvement options ranged from 20% to 100%. There were only two options with less than 60% agreement. There were four options where agreement was between 60% and 70%, and eight with 100% agreement. The option with least support – with only 20% indicating agreement – was “Co-payment for metabolic testing for monitoring health”. There would seem to be little support for this option, and for taking this idea further at this time.
Eight options in total had 100% agreement, and considering this high level of support these service development and improvement options should therefore be considered for further development and implementation.
4.5 Consensus on preliminary recommendations for service improvement and development

0% 20% 40% 60% 80% 100%
Development and wider promotion of awareness raising products in various formats including information leaflets, QR
code business cards provided in a range of environments and in online packs; signposting to credible online info.
Practitioners need to focus on wider health and well-being issues including psychological health as intervention, NOT soley on the drugs.
Development of e-learning module on IPEDs for Primary and Secondary Care services including GPs, Pharmacy
Development of General Practitioner to General Practitioner IPED training model within cluster.
Produce short film on how to engage with individuals using IPEDs.
Dedicated needle and syringe programme staff in all needle and syringe programme sites including pharmacy with increased
flexible opening hours.
Improved networking and communication between and within service types (all needle and syringe programmes, all IPED health and allied
professionals/services etc); development of local forums.
Establish consistant targeted and tailored health and well-being outreach services (including needle and syringe programmes)
co-delivered by health care services and peer champions.
Establish an IPED user group to scope and design an interactive app (eg - cycle and training diaries) to promote engagement.
Development of targeted/specialist services which aims to address wider well-being including: fitness, diet and
supplementation - perhaps tie in with reducing obesity and other public health programmes.
The development of a virtual General practitioner or IPED clinic available online - utilising contemporary digital health approaches.
Figure 3: Extent of consensus with the service development and improvement recommendations generated: result of voting during Evidence Gathering and Synthesis day
Strongly Agree Agree Disagree Strongly Disagree
>
27
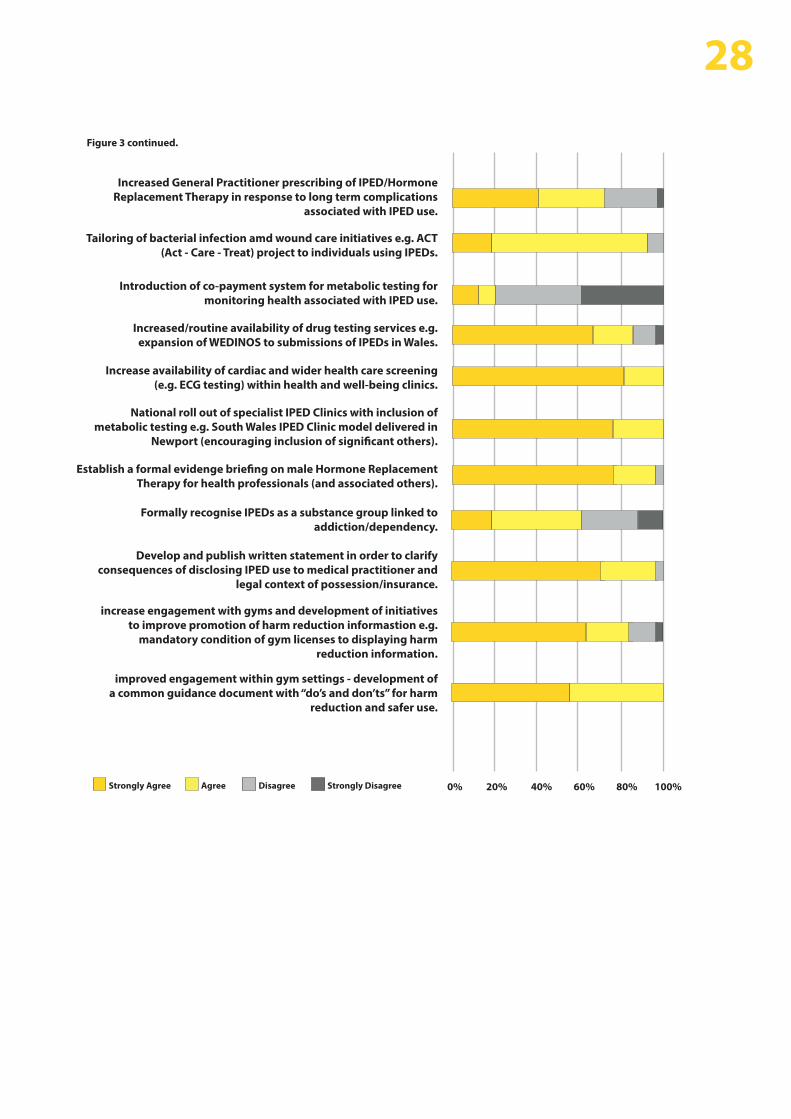
0% 20% 40% 60% 80% 100%
Increased General Practitioner prescribing of IPED/Hormone Replacement Therapy in response to long term complications
associated with IPED use.
Tailoring of bacterial infection amd wound care initiatives e.g. ACT (Act - Care - Treat) project to individuals using IPEDs.
Introduction of co-payment system for metabolic testing for monitoring health associated with IPED use.
Increased/routine availability of drug testing services e.g. expansion of WEDINOS to submissions of IPEDs in Wales.
Increase availability of cardiac and wider health care screening (e.g. ECG testing) within health and well-being clinics.
National roll out of specialist IPED Clinics with inclusion of metabolic testing e.g. South Wales IPED Clinic model delivered in
Newport (encouraging inclusion of significant others).
Establish a formal evidenge briefing on male Hormone Replacement Therapy for health professionals (and associated others).
Formally recognise IPEDs as a substance group linked to addiction/dependency.
Develop and publish written statement in order to clarify consequences of disclosing IPED use to medical practitioner and
legal context of possession/insurance.
increase engagement with gyms and development of initiatives to improve promotion of harm reduction informastion e.g.
mandatory condition of gym licenses to displaying harm reduction information.
improved engagement within gym settings - development of a common guidance document with “do’s and don’ts” for harm
reduction and safer use.
Figure 3 continued.
28
Strongly Agree Agree Disagree Strongly Disagree

The following recommendations draw upon data generated and collated as part of this study. However, they are principally informed by the ideas generated and voted on at the end of the Evidence Gathering and Synthesis Event. The following recommendations are based on those options that had widespread support throughout this project:
Government bodies, academic institutions and health services to provide resources and undertake a review with the aim of developing the evidence base on the use of online technologies (including social media) to facilitate effective health service engagement and e-clinics. This work should include online advice and triage clinics targeted towards young people using AAS currently not engaged with existing services
Public health bodies, community substance misuse leads and commissioners to develop best practice guidance on the implementation of effective assertive outreach services and adaptation of health and social care settings to optimise on-site engagement
In collaboration with registered professional bodies (including; RCGP, RCN, RCPsych, GPhC), public health bodies to develop value-based ‘AAS for healthcare professionals’ training and knowledge sharing opportunities (including e-learning and GP cluster events). Products to be embedded as a core training programmes within NHS Trusts/Health Boards and community health services
Adopting a ‘whole person’ approach, substance misuse commissioning boards to undertake a biennial comprehensive network mapping and gap analysis exercise of local health and social care services accessible to individuals using AAS. The mapping and gap analysis exercise should include:• Substance misuse and harm reduction• Physical health, mental health and wellbeing• Diet, nutrition, exercise and training advice • Sports injury• Sexual health and wellbeing
This work should lead to the development of a local/regional service directory for dissemination via outreach services, local health and social care expert AAS fora and establishment of dedicated AAS health and well-being clinic sessions within existing services
Public health bodies and AAS leads to produce the following essential documents:• A ‘What to expect’ document developed for distribution across gyms/fitness venues aimed at owners, managers and staff on working with AAS outreach services• Collation of all local/regional AAS health and social care directories for inclusion on national websites e.g. IPEDInfo.co.uk• A written statement on the implications and importance of AAS disclosure during a medical consultation or treatment
Public health bodies in collaboration with UK wide academic institutions to undertake research to establish a robust prevalence estimate of AAS use and evidence of harms associated with use.
295 Conclusions & Recommendations
a.
b.
c.
d.
e.
f.
1. Home Office. Drug misuse: Findings from the 2015/16 Crime Survey for England and Wales: data tables, 2016. Home Office: London2. McVeigh J., Begley E., Anabolic steroids in the UK: an increasing issue for public health. Drugs: Education, Prevention and Policy, 2016: p. 1-8.3. Hanely S., G., Coomber R. The risk environment of anabolic-androgenic steroid users in the UK: Examining motivations, practices and accounts of use. Int J Drug Policy, 2017. 40, 35-434. Kimergård A. A qualitative study of anabolic steroid use amongst gym users in the United Kingdom: motives, beliefs and experiences. Journal of Substance Use, 2015. 20, 288-294.5. Tod D., Edwards C., Cranswick I. Muscle dysmorphia: current insights. Psychology Research and Behavior Management, 2016. 9, 179-1886. Begley E., McVeigh J., Hope VD. Image and Performance Enhancing Drugs: 2016 National Survey Results. Public Health Institute LJMU and Public Health Wales7. Christiansen AV., Vinther AS., Liokaftos D. ‘Outline of a typology of men’s use of anabolic androgenic steroids in fitness and strength training environments’. Drugs: Education, Prevention and Policy, 2017 vol. 24, no. 3, pp. 295-305.8. Zahnow R., McVeigh J., Bates G., Hope V., Kean J., Campbell J., Smith J. Identifying a typology of men who use anabolic androgenic steroids (AAS). Int J Drug Policy, 2018. May;55:105-112.9. Pope H.G., et al., Adverse Health Consequences of Performance-Enhancing Drugs: An Endocrine Society Scientific Statement. Endocrine Reviews, 2014. 35(3): p. 341-37510. Zahnow R., et al., Adverse Effects, Health Service Engagement, and Service Satisfaction Among Anabolic Androgenic Steroid Users. Contemporary Drug Problems, 2017. 44(1): p. 69-83.11. Kanayama G., et al., Treatment of anabolic-androgenic steroid dependence: Emerging evidence and its implications. Drug and Alcohol Dependence, 2010. 109(1-3): p. 6-13.12. Hope VD., McVeigh J., Marongiu A., Evans-Brown M., Smith J., Kimergard A., Ncube F. Injection site infections and i njuries in men who inject image- and performance-enhancing drugs: prevalence, risks factors, and healthcare seeking. Epidemiology and Infection, 2015. 143(1): 132-14013. Day C.A., Topp L., Iversen J., Maher L., Collaboration of Australian Blood-borne virus prevalence and risk among steroid injectors: results from the Australian Needle and Syringe Program Survey. Drug Alcohol Rev, 2008. 27, 559-56114. Hope V.D., McVeigh J., Marongiu A., Evans-Brown M., Smith J., Kimergard A., Croxford S., Beynon CM., Parry JV., Bellis MA., Ncube F. Prevalence of, and risk factors for, HIV, hepatitis B and C infections among men who inject image and performance enhancing drugs: a cross-sectional study. BMJ Open 3, 2013. e00320715. Zahnow R., et al., Adverse Effects, Health Service Engagement, and Service Satisfaction Among Anabolic Androgenic Steroid Users. Contemporary Drug Problems, 2017. 44(1): p. 69-83.16. Graham MR., Ryan P., Baker JS., Davies B., Thomas NE., Cooper SM., Evans P., Easmon S., Walker CJ., Kickman AT. Counterfeiting in performance and image enhancing drugs. Drug Testing and Analysis 2009. 135-142. Doi: 10.1002/dta.3017. Kimergård A., McVeigh J., Knutsson S., Breindahl T., Stensballe A. Online marketing of syntheticpeptide hormones: Poor manufacturing, user safety, and challenges to public health. Drug Testingand Analysis, 2014a. 6(4): 396-398. doi:10.1002/dta.163618. Kimergard A., Breindahl T., Hindersson P., McVeigh J. The composition of anabolic steroids from the illicit market is largely unknown: implications for clinical case reports. QJM-An International Journal of Medicine, 2017. 107(7): 597-598. doi:10.1093/qjmed/19. Richardson A., Antonopoulos GA. Anabolic-androgenic steroids (AAS) users on AAS use: Negative effects, ‘code of silence’, and implications for forensic and medical professionals. J Forensic Leg Med, 2019. Sep 18;68:10187120. Underwood M. The unintended consequences of emphasising blood-borne virus in research on, and services for, people who inject image and performance enhancing drugs: A commentary based on enhanced bodybuilder perspectives. Int J Drug Policy, 2019. May;67:19-2321. Hope V.D., et al. Risk of HIV and Hepatitis B and C Over Time Among Men Who Inject Image and Performance Enhancing Drugs in England and Wales: Results From Cross-Sectional Prevalence Surveys, 1992-2013. Journal of Acquired Immune Deficiency Syndromes, 2016. 71(3): p. 331-33722. Hope VD., McVeigh J., Smith J., Glass R., Njoroge J., Tanner C., Parry JV., Ncube F., Desai M. Low levels of hepatitis C diagnosis and testing uptake among people who inject image and performance enhancing drugs in England and Wales, 2012-15. Drug Alcohol Depend, 2017. Jul 18;179:83-86.23. Bates G., Jones L., and McVeigh J. Update of NICE Guidance PH18 on ‘Needle and syringe programmes’. PIEDs Review, 2013. Liverpool John Moores University: Centre for Public Health.24. Michie S., van Stralen MM., West R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implementation Science, 2011. 6:42.
306 References


Facilitators and Barriers to Health Care Access Amongst people using Image and
Performance Enhancing Drugs in Wales
Findings & Outcomes report 2020
Facilitators and Barriers to Health Care Access Amongst people using Image and
Performance Enhancing Drugs in Wales
Findings & Outcomes report 2020