facing the challenges of hypertension in children...
TRANSCRIPT

Facing The Challenges Of HypertensionIn Children and Adolescents
Julie R. Ingelfinger, M.D.
Professor of Pediatrics, Harvard Medical School
Senior Consultant in Pediatric Nephrology, MassGeneral Hospital for Children at MGH
Deputy Editor, the New England Journal of Medicine
I have no relevant disclosures

Challenges in Pediatric Hypertension
• Defining, detecting and recognizing hypertension
• Intervening by minimizing predisposing factors
• Finding better ways to predict and assess target-organ damage
• Investigating the feasibility of individualized approaches for management
• Improving Health Provider Education and Interpretation of Guidelines and Their Application
• Funding and Execution of major clinical trials in children and adolescents

Challenges in Pediatric Hypertension
“Hypertension is the leading cause of death worldwide. Globally and locally there has been an increase in hypertension in children, adolescents and young adults.
“In South Africa, the first decade of the millennium saw a doubling of the prevalence rate among adolescents and young adults aged 15 - 24 years.
“This increase suggests that an explosion of cerebrovascular disease, cardiovascular disease and chronic kidney disease can be expected in the forthcoming decades. “
Mangena P, Saban S, Hlabyago KE, Rayner B. An Approach to the young hypertensive patient. S Afr Med J 2016; 106: 36-8.

Challenges in Pediatric Hypertension
• Defining, detecting and recognizing hypertension
• Decreasing predisposing factors
• Finding better ways to predict and assess target-organ damage
• Investigating the feasibility of individualized approaches for management
• Improving Health Provider Education and Interpretation of Guidelines and Their Application
• Funding and Execution of major clinical trials in children and adolescents

How to DEFINE Pediatric Hypertension
• Definitions are, to date, epidemiological
• Prior pediatric HTN guidelines issued in the US by NHLBI in 1977, 1987, 1996 and 2004
• Increase in interest in childhood HTN since 2004 Fourth Report– 3.5% of children have HTN; another 10-11% have elevated BP
• Increase in prevalence due to obesity
– High BP in childhood increases the risk for adult HTN and cardiovascular disease
– Even youth with HTN have evidence of accelerated vascular aging


New Guidelines in US– Recent Guidelines in Europe
• Rigorous evidence-based methodology
• Revised definitions of blood pressure categories; alignment with AHA/ACC GL
• New normative BP tables based on BPs from normal-weight children
• Simplified screening table

New US GuidelinesMajor Changes From the Fourth Report
• Emphasis on use of 24-hr ABPM to confirm HTN diagnosis
• Revised recommendations for performance of echocardiography
• Lower treatment goals for primary HTN; ABPM goal for CKD

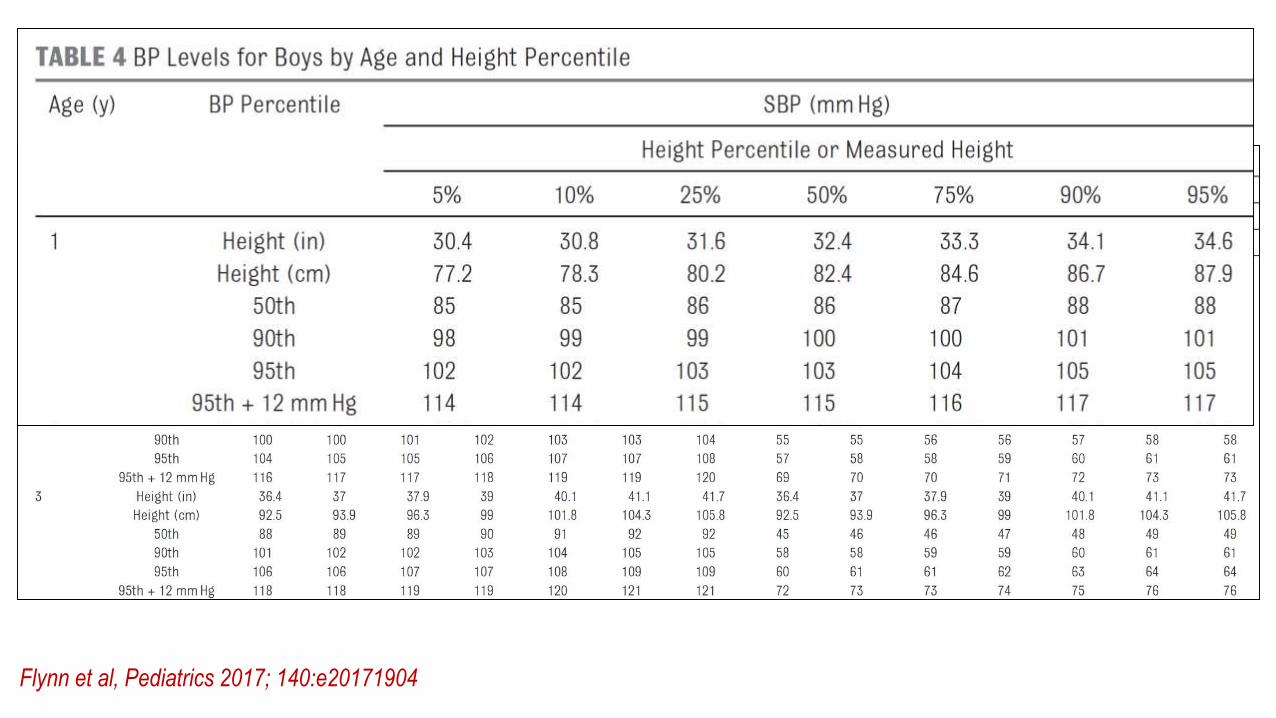
Definition of HTN (1-18y)
Flynn et al, Pediatrics 2017; 140:e20171904

New BP Tables
Flynn et al, Pediatrics 2017; 140:e20171904
New BP Tables
Flynn et al, Pediatrics 2017; 140:e20171904

New BP Tables
Flynn et al, Pediatrics 2017; 140:e20171904
New BP Tables
Flynn et al, Pediatrics 2017; 140:e20171904

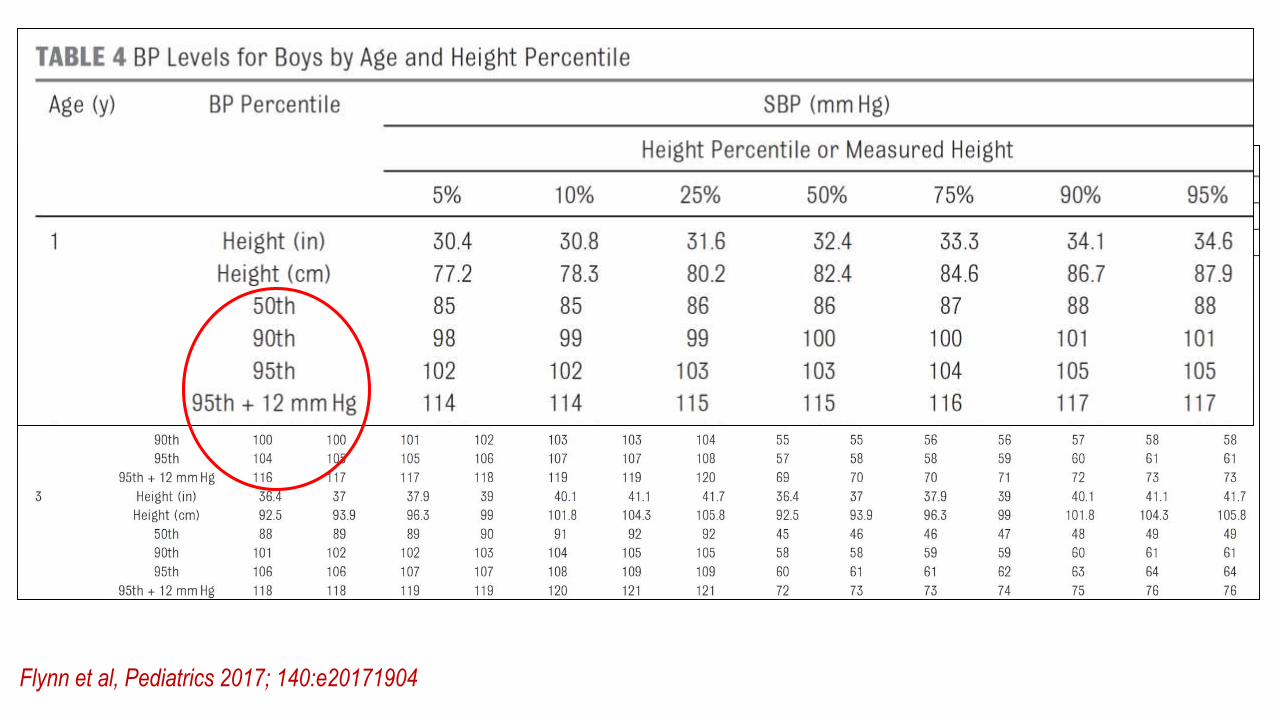
Simplified BP Table
• Full BP tables are complicated• Leads to under-recognition of
childhood HTN
• Simplified BP table created for use in initial screening of BP values• Based on 90th percentile BP values
for children at 5th height percentile
Flynn et al, Pediatrics 2017; 140:e20171904

Simplified BP Table
• Full BP tables are complicated• Leads to under-recognition of
childhood HTN
• Simplified BP table created for use in initial screening of BP values• Based on 90th percentile BP values
for children at 5th height percentile
Flynn et al, Pediatrics 2017; 140:e20171904

Despite Guidelines, Hypertension Recognition is Poor!
• In the presence of elevated BP, majority of practitioners do not recognize or report it.
• Hansen et al. reported underdiagnosis of Htn in children and adolescents in 2007 (JAMA 298:22-29).
• Beacher et al. 29,000 patients (2-17 years), among those with > 3 elevated BP measurements, only 215 were identified as having an elevated BP. (J Pediatr 2015; 166: 1233-9).
• WE HAVE A PROBLEM!!

Predicted probability of recognition of elevated SBP according to SBP level and weight status.
Tammy M. Brady et al. Pediatrics 2010;125:e1286-e1293
©2010 by American Academy of Pediatrics

Ward RL. J Commun Health 2016; 41: 258-264

WHAT THIS STUDY ADDS: In this 20-site, cluster-randomized trial, we demonstrated how an innovative electronic health record—linked, clinical decision support tool can increase hypertension recognition and promote guideline-adherent clinical care.
Kharbanda EO, Asche SE, Sinaiko AR, et al. Clinical Decision Support for Recognition and Management of Hypertension: A Randomized Trial. Pediatrics. 2018;141(2): e20172954
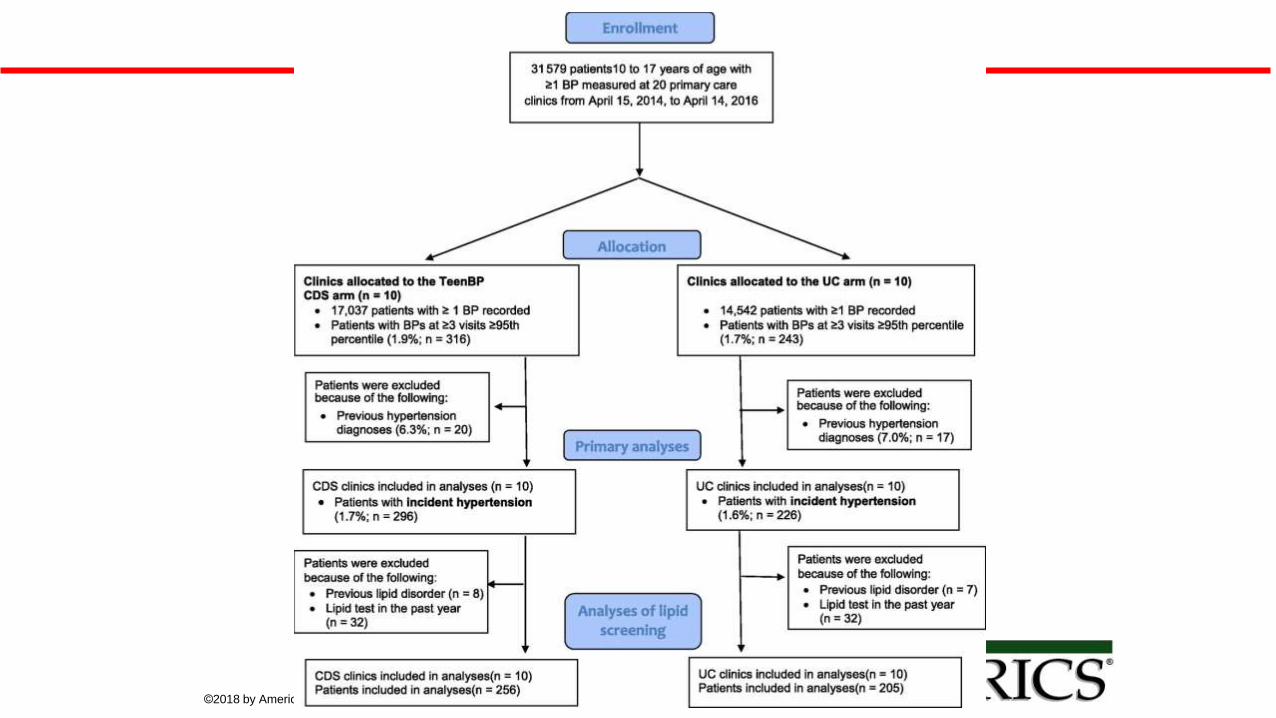
Summary of clinic and patient eligibility.
Elyse O. Kharbanda et al. Pediatrics 2018;141:e20172954
©2018 by American Academy of Pediatrics

TeenBP CDS. %tile, percentile.
Elyse O. Kharbanda et al. Pediatrics 2018;141:e20172954
©2018 by American Academy of Pediatrics

Kharbanda EO, Asche SE, Sinaiko AR, et al. ClinicalDecision Support for Recognition and Management ofHypertension: A Randomized Trial. Pediatrics. 2018;141(2):e20172954

Pollack AH, Flynn JT. Pediatrics 2018; 141:pii: e20173756
“There are likely many contributing factors that lead to the underrecognition of pediatric hypertension, but the fact that clinicians providing care to children and adolescents do not have a simple, single BP value to reference creates significant complexity for what should be a relatively straightforward problem.”
You Can’t Treat a Problem if You Don’t Recognize ItAri H. Pollack, Joseph T. Flynn
Worldwide– Recognition is Problematic
• Resourced areas– same issues as in US
• Under-resourced areas– competing issues• Not only difficulty in recognizing
• Difficulty in obtaining measurements
• Implications—• In the face of a worldwide obesity epidemic, the recognition of hypertension
is lagging.
• Identification of hypertension renders intervention possible.

Challenges in Pediatric Hypertension
• Defining, detecting and recognizing hypertension
• Intervening by minimizing predisposing factors
• Finding better ways to predict and assess target-organ damage
• Investigating the feasibility of individualized approaches for management
• Improving Health Provider Education and Interpretation of Guidelines and Their Application
• Funding and Execution of major clinical trials in children and adolescents

Obesity Epidemic Co-Morbidities

Obesity- Children 5-19 Years of Age
• overweight is BMI-for-age greater than 1 standard deviation above the WHO Growth Reference median; and
• obesity is greater than 2 standard deviations above the WHO Growth Reference median.
http://www.who.int/mediacentre/factsheets/fs311/en/
Weight Status Category Percentile Range
Underweight Less than the 5th percentile
Normal or Healthy Weight 5th percentile to less than the 85th percentile
Overweight 85th to less than the 95th percentile
Obese 95th percentile or greater

Obesity in Childhood and Adolescence in the USA– CDC Data

Co-Morbidities of Obesity in Children and Adolescents
• Pathophysiology:• Dyslipidemia• Inflammation• Mitochondrial abnormalities
• Metabolic syndrome and insulin resistance
• Sleep apnea and asthma
• Fatty liver- NAFLD
• Gallstones and GERD
• Joint and other orthopedic problems and risk
• Psychological issues
• Kidney and vascular risks evident early

Nutrients that may promote insulin resistance and fat mass accumulation:
Fructose (sucrose, HFCS)Purine-rich foods (meat, seafood)Beer, EtOH
Nutrients that may oppose nsulin resistance and fat mass accumulation:
Plant food (berries, vegetables, fruit)Nuts (especially walnuts)Marine lipids (omega-3 FA)
Gut microbiota NutritionArtificial sweeteners, probiotics, prebiotics, FFA, abx
Genetics Epigenetics Lifestyle Physical Activity
Appetite Transcriptional regulation Epigenetics
OBESITY Metabolic disease
FFA receptorsTransgenerational impact ofIntrauterine nutrition (methyl-rich food, genistein)
MC4R hypomethylation PPARƳ hypomethylationPGC1α hypomethylation
Insulin resistanceInflammation
FTO, MC4R, TMEM18
- +
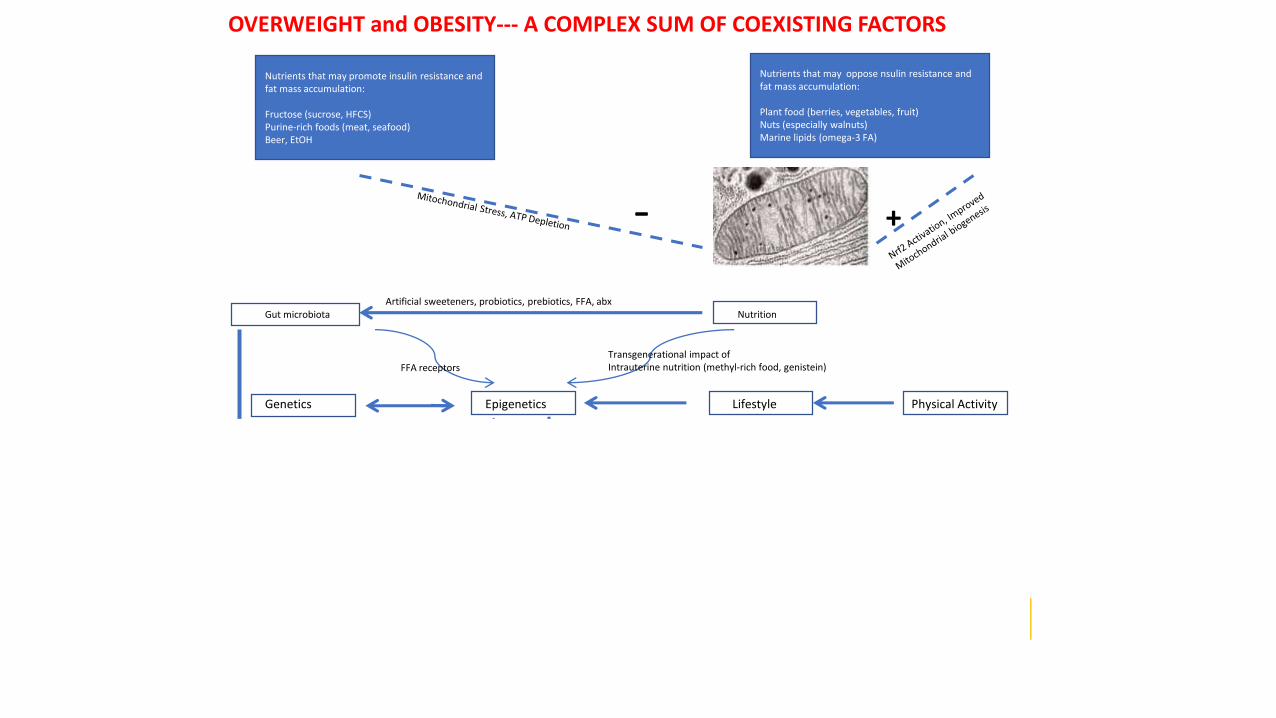
OVERWEIGHT and OBESITY--- A COMPLEX SUM OF COEXISTING FACTORS

Nutrients that may promote insulin resistance and fat mass accumulation:
Fructose (sucrose, HFCS)Purine-rich foods (meat, seafood)Beer, EtOH
Nutrients that may oppose nsulin resistance and fat mass accumulation:
Plant food (berries, vegetables, fruit)Nuts (especially walnuts)Marine lipids (omega-3 FA)
Gut microbiota NutritionArtificial sweeteners, probiotics, prebiotics, FFA, abx
Genetics Epigenetics Lifestyle Physical Activity
Appetite Transcriptional regulation Epigenetics
OBESITY Metabolic disease
FFA receptorsTransgenerational impact ofIntrauterine nutrition (methyl-rich food, genistein)
MC4R hypomethylation PPARƳ hypomethylationPGC1α hypomethylation
Insulin resistanceInflammation
FTO, MC4R, TMEM18
- +
OVERWEIGHT and OBESITY--- A COMPLEX SUM OF COEXISTING FACTORS

Nutrients that may promote insulin resistance and fat mass accumulation:
Fructose (sucrose, HFCS)Purine-rich foods (meat, seafood)Beer, EtOH
Nutrients that may oppose nsulin resistance and fat mass accumulation:
Plant food (berries, vegetables, fruit)Nuts (especially walnuts)Marine lipids (omega-3 FA)
Gut microbiota NutritionArtificial sweeteners, probiotics, prebiotics, FFA, abx
Genetics Epigenetics Lifestyle Physical Activity
Appetite Transcriptional regulation Epigenetics
OBESITY Metabolic disease
FFA receptorsTransgenerational impact ofIntrauterine nutrition (methyl-rich food, genistein)
MC4R hypomethylation PPARƳ hypomethylationPGC1α hypomethylation
Insulin resistanceInflammation
FTO, MC4R, TMEM18
- +
OVERWEIGHT and OBESITY--- A COMPLEX SUM OF COEXISTING FACTORS
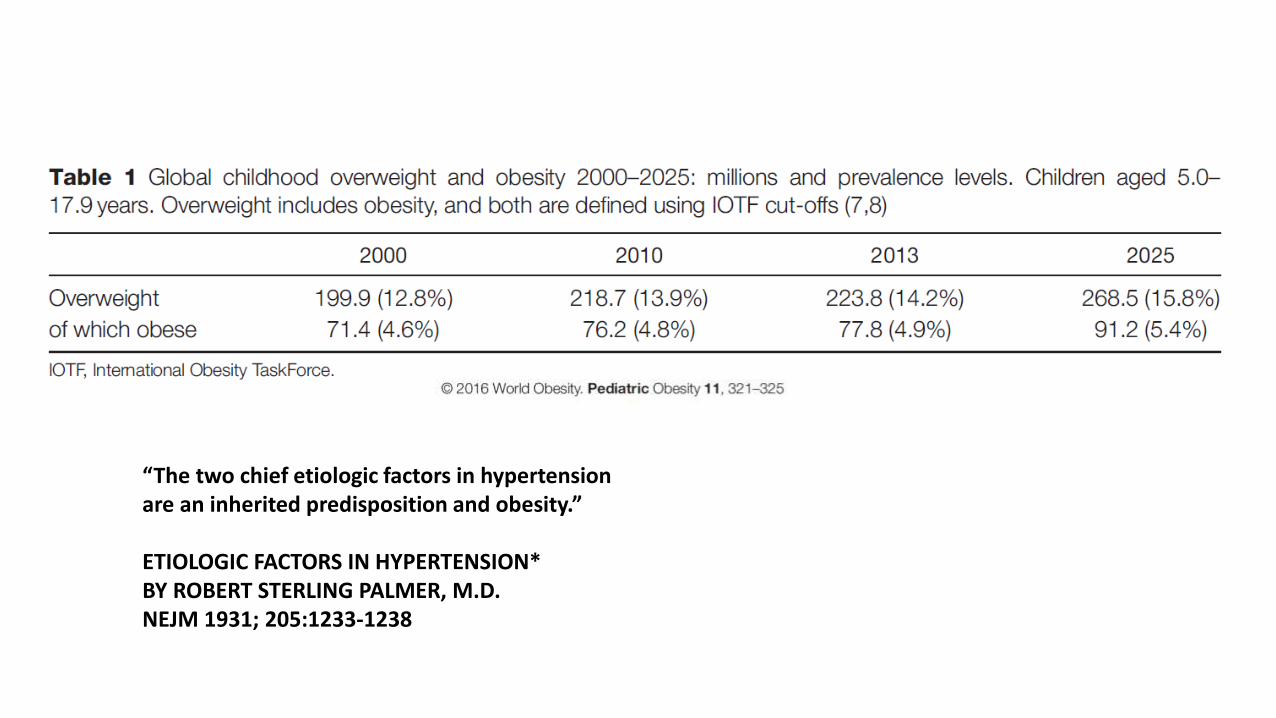
“The two chief etiologic factors in hypertensionare an inherited predisposition and obesity.”
ETIOLOGIC FACTORS IN HYPERTENSION*BY ROBERT STERLING PALMER, M.D.NEJM 1931; 205:1233-1238

Kaplan-Meier Curves for Premature Death
Franks PW et al. N Engl J Med 2010;362:485-493
Franks et al. N Engl J MedVolume 362(6):485-493
February 11, 2010

Nehus et al. KI 2017; 91: 451-458

Treatment of Pediatric Obesity
Crocker and Yanovski, Ped Clin N America
Other Predisposing Factors
• Salt intake?
• Uric acid levels
• Dyslipidemia
• Lack of conditioning
Challenges in Pediatric Hypertension
• Detecting and recognizing hypertension
• Decreasing predisposing factors
• Finding better ways to predict and assess target-organ damage
• Investigating the feasibility of individualized approaches for management
• Improving Health Provider Education and Interpretation of Guidelines and Their Application
• Funding and Execution of major clinical trials in children and adolescents

• 145 participants• At 5 years, both BW and current weight were determinants of blood pressure and metabolic parameters• As participants got older, the impact of body size increased. Higher BW and maternal obesity increased the risk of becoming obese at 5 years while this was reduced if breastfeeding. • Maternal obesity was the only factor associated with becoming obese at 10 years. • Twenty-two children at 10 years had insulin values ≥15 U/L. Participants with insulin values ≥15 U/L showed significant higher values of office systolic blood pressure, triglycerides, and uric acid and lower values of high-density lipoprotein than did those with normal insulin values. Highest weight gain from 5 to 10 years and lowest BW were the main determinants of high insulin levels. • In conclusion, although BW was a proxy of the events during fetal life and projected its influence later, the influence of gaining weight was a key determinant in the risk to develop obesity and metabolic abnormalities.145

*P <0.04 MH vs. NT; Mitsnefes 2010 JASH
LVH by BP Classification
0
5
10
15
20
25
30
35
Pre
va
len
e o
f L
VH
(%
)
Normotensive Masked HTN Confirmed HTN
*
Figure 1

20
25
30
35
40
45
Normal PreHTN HTN
20
25
30
35
40
45
Low Mid High
Increased LVM Across the BP Spectrum
Figure 4
*P<0.05 for Normal<PreHTN<HTN; Urbina J Clin Htn 2011;
*P<0.001 for L<M<H; Falkner 2013 JPeds.
LV
MI
(g/m
2.7
)Urbina* Falkner*

Increased PWV With Pre-HTN & HTN
P<0.05 for *Normal<PreHTN<HTN; Urbina J Clin Htn 2011.
*
4
4.5
5
5.5
6
6.5
7
7.5
PW
V (
m/s
ec)
Normal PreHTN HTN
Normal PreHTN HTN
Figure 5

35
40
45
50
55T
est
Sco
re
BRI MI GEC
Normal HTN
*P<0.03; Lande 2003 J Peds
Diminished Neuro-Cognitive Function in Youth with HTN
* *
Figure 1
*

Shah, Daniels, Urbina 2011 Diabetologia
Diastolic DysfunctionRelated to Obesity & Metabolic Control
Lean
Obese
T2DM
Figure 4

Challenges in Pediatric Hypertension
• Detecting and recognizing hypertension
• Intervening by minimizing predisposing factors
• Finding better ways to predict and assess target-organ damage
• Investigating the feasibility of individualized approaches for management
• Improving Health Provider Education and Interpretation of Guidelines and Their Application
• Funding and Execution of major clinical trials in children and adolescents

HOW TO PREVENT THESE
EFFECTS
Intermedica-inc.com

Will a Biology-Based PathwayApproachLead to Individualized Approach?
49
Design Studies to Examine

Symbol Gene Name Pathway Associated miRNAs
ADRB1 adrenoceptor beta 1 Symp NS23, 30, 125a, 133a
NPY neuropeptide Y Symp NS30
AGTangiotensinogen (serpin peptidase
inhibitor, clade A, member 8)RAAS
31
REN renin RAAS145
ACE angiotensin I converting enzyme RAAS 133a, 145
CYP11B1cytochrome P450, family 11, subfamily B,
polypeptide 1Aldosterone
24
HSD11B2 hydroxysteroid (11-beta) dehydrogenase 2 Aldosterone 101, 125a, 133a
NPPA natriuretic peptide A Na reabs kidney133
SCNN1Asodium channel, non-voltage-gated 1 alpha
subunitNa reabs kidney
143
EDN1 endothelin 1Vasoconstriction
(NOS) 125
NOS3 nitric oxide synthase 3 (endothelial cell) Vasoconstriction (NOS)21
DRD2 dopamine receptor D2 Heart125a, 133a, 143, 145, 146, 181
GNB3guanine nucleotide binding protein (G
protein), beta polypeptide 3Heart
101, 125a, 133a, 143, 145, 146
MYH9 myosin, heavy chain 9, non-muscle Heart125a, 133a, 145, 146, 181

Impact: Identifying novel therapeutic targets
•Traditional genetic studies identify risk variants while miRNA & methylation profiles allows identification of dynamic factors associated with TOD risk.
•miRNA expression and methylation are potential targets for pharmacologic interventions.
• Identifying miRNA and methylation differences associated with TOD risk is a critical step in developing novel therapeutic interventions.

Innovation: Gene-environment interface and potential for reverse translation
•Few data exist on epigenetic changes and modifying miRNAs related to HTN and LVH- promoting genes in youth.
•Opportunity to evaluate epigenetic changes and modifying miRNA related to other forms of TOD in youth.
•Set the stage for reverse translation to better understand mechanism of TOD.

• Focus & Future Directions:
• Candidate genes- molecular determinants in development of both HTN & TOD selected -each connected by a common pathway.
• Pathway analyses supported the need to consider bothBP & TOD genes in LVH may occur in youth.
• Future studies to delineate mechanistic underpinnings include gene, epigene and miRNA sequencing, metabolomics and molecular patterns of injury*.
* Samples saved for future studies.

Hypertension and Chronic Renal Disease:
Hemodynamic Abnormalities
Mean BPTotal Systemic
Vascular Resistance= X
Increased Cardiac Output Intravascular Volume
Glomerular filtration Sodium excretion Extracellular Fluid Renal Nerve ActivityMyocardial Performance
Adrenergic Activity
IncreasedVasoconstriction Adrenergic Stimuli Angiotensin II Endothelin Endothelium-derived
Contracting Factors Thromboxane
CardiacOutput
DecreasedVasodilation Prostacyclin Nitric oxide EDHF*
Textor SC. Atlas of Diseases of the Kidney.
*Endothelium-derived Hyperpolarizing Factors
www.hypertensiononline.org

Factors Controlling Blood Pressure
• Acetylcholine
• Angiotensin II
• Endothelium-derived contracting factor
• Kinins
• Neuropeptides (neurotensin, NPY, substance P)
• Nitric oxide
• Oxytocin
• Prostanoids (Prostaglandins, HETEs, leukotrienes, thromboxanes
• Serotonin
• Vasopressin (antidiuretic hormone)

Looking for Individual Factors….
Yu-D-H. J Clin Invest 2014;124:3708-3712.

Pivotal Role of ROS in Stimulus-Induced EC and VSMC Growth, Survival, and Apoptosis
PDGF, Thrombin, Norepinephrine, Ang II, TNF, Ox-LDL, High Glucose, VEGF
ROS
Arachidonate Metabolism
Mitochondrial ElectronTransport Chain
CytochromeP450
NOX-1 Oxidase
Xanthine Oxidase
Growth or Hypertrophy
Survival Apoptosis
Caspases NF-B Akt ERKs JNKs
SAPKs
p38MAPK
Potential Targetsof ROS
Sources of ROS
Growth/DeathSurvival Signals
www.hypertensiononline.org
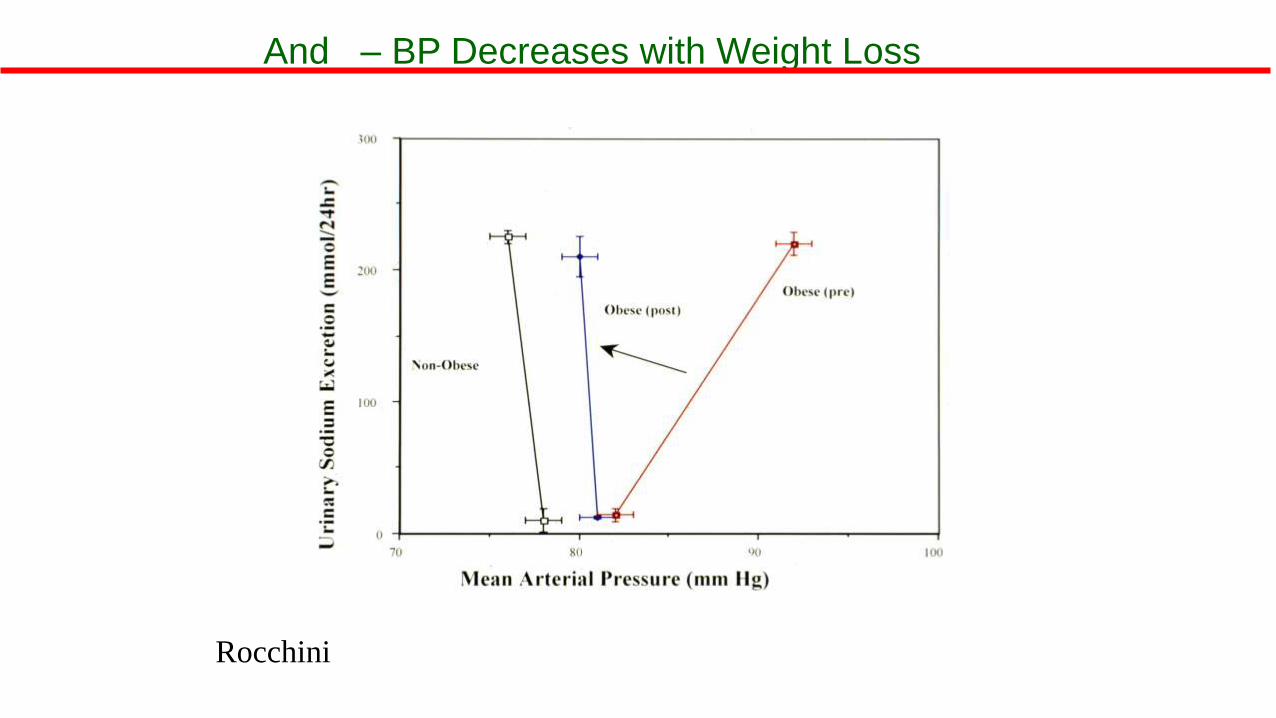
Rocchini
And – BP Decreases with Weight Loss

Delineating mechanisms may be the
key to prevention
Intermedica-inc.com

Challenges in Pediatric Hypertension
• Detecting and recognizing hypertension
• Intervening by minimizing predisposing factors
• Finding better ways to predict and assess target-organ damage
• Investigating the feasibility of individualized approaches for management
• Improving Health Provider Education and Interpretation of Guidelines and Their Application
• Funding and Execution of major clinical trials in children and adolescents

Flynn et al, Pediatrics 2017; 140:e20171904
KAS 1: BP Measurement Frequency

Flynn et al, Pediatrics 2017; 140:e20171904
KAS 1: BP Measurement Frequency

KAS 2: BP Measurement Frequency
• BP should be checked in all children and adolescents ≥3 y of age at every health care encounter if they have obesity, are taking medications known to increase BP, have renal disease, a history of aortic arch obstruction or coarctation, or diabetes.
Flynn et al, Pediatrics 2017; 140:e20171904

Repeat High BP Measurements
•BP in childhood may vary considerably between visits and even during the same visit• Many potential etiologies for isolated elevated BP in children
and adolescents
•Therefore the clinician should:• Repeat high BP readings at a visit • Obtain multiple measurements over time before diagnosing
HTN

KAS 3: Diagnosis of Hypertension
Flynn et al, Pediatrics 2017; 140:e20171904
• Trained health care professionals in the office setting should make a diagnosis of HTN if a child or adolescent has auscultatory confirmed BP readings ≥95th percentile* at 3 different visits.
*≥130/80 in adolescents ≥13 years old

BP Measurement & Classification
Flynn et al, Pediatrics 2017; 140:e20171904

Patient Evaluation & Management by BP LevelBP Category(see Table 3)
BP Screening Schedule
Lifestyle Counseling
(Weight, Nutrition)
Check Upper and
Lower Extremity
BP
ABPMDiagnostic Evaluation
Initiate Treatment
Consider Sub-
specialty Referral
Normal Annual X
Elevated BP
Initial measurement X
Second measurement: Repeat in 6 months X X
Third measurement: Repeat in 6 months X X X X
Stage 1 HTN
Initial measurement X
Second measurement: Repeat in 1-2 weeks X X
Third measurement: Repeat in 3 months X X X X X
Stage 2 HTN
Initial measurement X X
Second measurement: Repeat/refer to specialty carewithin 1 week
X X X X X
Flynn et al, Pediatrics 2017; 140:e20171904

Patient Evaluation & Management by BP LevelBP Category(see Table 3)
BP Screening Schedule
Lifestyle Counseling
(Weight, Nutrition)
Check Upper and
Lower Extremity
BP
ABPMDiagnostic Evaluation
Initiate Treatment
Consider Sub-
specialty Referral
Normal Annual X
Elevated BP
Initial measurement X
Second measurement: Repeat in 6 months X X
Third measurement: Repeat in 6 months X X X X
Stage 1 HTN
Initial measurement X
Second measurement: Repeat in 1-2 weeks X X
Third measurement: Repeat in 3 months X X X X X
Stage 2 HTN
Initial measurement X X
Second measurement: Repeat/refer to specialty carewithin 1 week
X X X X X
Flynn et al, Pediatrics 2017; 140:e20171904

Patient Evaluation & Management by BP LevelBP Category(see Table 3)
BP Screening Schedule
Lifestyle Counseling
(Weight, Nutrition)
Check Upper and
Lower Extremity
BP
ABPMDiagnostic Evaluation
Initiate Treatment
Consider Sub-
specialty Referral
Normal Annual X
Elevated BP
Initial measurement X
Second measurement: Repeat in 6 months X X
Third measurement: Repeat in 6 months X X X X
Stage 1 HTN
Initial measurement X
Second measurement: Repeat in 1-2 weeks X X
Third measurement: Repeat in 3 months X X X X X
Stage 2 HTN
Initial measurement X X
Second measurement: Repeat/refer to specialty carewithin 1 week
X X X X X
Flynn et al, Pediatrics 2017; 140:e20171904

Patient Evaluation & Management by BP LevelBP Category(see Table 3)
BP Screening Schedule
Lifestyle Counseling
(Weight, Nutrition)
Check Upper and
Lower Extremity
BP
ABPMDiagnostic Evaluation
Initiate Treatment
Consider Sub-
specialty Referral
Normal Annual X
Elevated BP
Initial measurement X
Second measurement: Repeat in 6 months X X
Third measurement: Repeat in 6 months X X X X
Stage 1 HTN
Initial measurement X
Second measurement: Repeat in 1-2 weeks X X
Third measurement: Repeat in 3 months X X X X X
Stage 2 HTN
Initial measurement X X
Second measurement: Repeat/refer to specialty carewithin 1 week
X X X X X
Flynn et al, Pediatrics 2017; 140:e20171904

Oscillometric vs Auscultatory BP
• Pediatric normative BP values are based on auscultation
• Despite this, oscillometric devices commonly used in many healthcare settings• Several perceived benefits
• Known inaccuracies

KAS 5: Oscillometric vs Auscultatory BP
•Oscillometric devices may be used for BP screening in children and adolescents. When doing so, providers should use a device that has been validated in the pediatric age group. If elevated BP is suspected on the basis of oscillometric readings, confirmatory measurements should be obtained by auscultation.
Flynn et al, Pediatrics 2017; 140:e20171904
Ambulatory BP Monitoring
• Use of ABPM in pediatric age group increasing
• Normative data tables available based on age, sex, height
• Consensus guidelines for interpretation available*
• Mentioned as ‘useful’ but not endorsed in 2004 Fourth Report
Flynn et al, Hypertension 2014; 63:1116

BP Patterns by cBP & ABPAmbulatory BP Office BP
Normal BP Normal Normal
Sustained HTN Elevated Elevated
White Coat HTN Normal Elevated
Masked HTN Elevated Normal

Ambulatory BP Monitoring
• New data available regarding• Frequency of WCH, Masked HTN
• Associations with hypertensive TOD
• Application in high-risk populations: CKD, DM, aortic coarctation, solid organ transplantation
• Cost-effectiveness in pediatric HTN evaluation

KAS 6: ABPM to Confirm HTN
Flynn et al, Pediatrics 2017; 140:e20171904
• ABPM should be performed for confirmation of HTN in children and adolescents with office BP measurements in the elevated BP category for 1 year or more or with stage 1 HTN over 3 clinic visits.
ABPM Procedure and WCH
• KAS 8: ABPM should be performed by using a standardized approach (see Table 13) with monitors that have been validated in a pediatric population, and studies should be interpreted by using pediatric normative data.
• KAS 9: Children and adolescents with suspected WCH should undergo ABPM. Diagnosis is based on the presence of mean SBP and DBP <95th percentile and SBP and DBP load <25%.
Flynn et al, Pediatrics 2017; 140:e20171904

KAS 7: ABPM in High-Risk Conditions
•Routine performance of ABPM should be strongly considered in children and adolescents with high-risk conditions to assess HTN severity and determine if abnormal circadian BP patterns are present, which may indicate increased risk for target organ damage.
Flynn et al, Pediatrics 2017; 140:e20171904

Table 12: High Risk Conditions
Flynn et al, Pediatrics 2017; 140:e20171904

Home BP Measurement
• Pediatric studies do not show that BP measurements obtained in settings other than the office or by ABPM are sufficiently reliable to establish a diagnosis of HTN
• Practical concerns:• Little normative data
• Only a few devices validated for children
• Cuff sizes limited
• No consensus about how many measurements across what period of time needed to evaluate BP

KAS 10: Home BP Measurement
• Home BP monitoring should not be used to diagnose HTN, MH, or WCH but may be a useful adjunct to office and ambulatory BP measurement after HTN has been diagnosed.
Flynn et al, Pediatrics 2017; 140:e20171904

Challenges in Pediatric Hypertension
• Detecting and recognizing hypertension
• Decreasing predisposing factors
• Finding better ways to predict and assess target-organ damage
• Investigating the feasibility of individualized approaches for management
• Improving Health Provider Education and Interpretation of Guidelines and Their Application
• Funding and Execution of major clinical trials in children and adolescents

Funding and Carrying Out Studies
• Collaboration– on a worldwide level
• Training and coordination of training
• Constant change and methodology to address
• Studies of national history
• Interventional studies require collaboration and trialists

THANK YOU!
Questions?

Definition of HTN in Neonates and Infants (0-1 y)
•Many factors affect BP in neonates, making it hard to precisely define HTN
•BP values for neonates 26-44 weeks post-menstrual age have been compiled and may be used to identify neonates with high BP
•2nd TF Report BP curves should still be used for infants 1-12 months of age

Predicted probability of recognition of elevated SBP according to SBP level and age.
Tammy M. Brady et al. Pediatrics 2010;125:e1286-e1293
©2010 by American Academy of Pediatrics

• Data regarding the association of ABP and TOD in youth are limited.
Sorof et al., Hypertension. 2002 Apr; 39(4) 903-8.

www.nhlbi.nih.gov

Skinner AC et al. N Engl J Med 2015;373:1307-1317.
Prevalence of Cardiometabolic Risk Factors by Weight Status.


Imbalance in Factors Affecting Vascular Tone and Structure
Nephron destruction and
renal failure
Vascular tone and structure
EDHF= endothelium-derived hyperpolarizing factors
ROS= reactive oxygen species
EDCF= endothelium-derived constricting factors www.hypertensiononline.org

Yiu VW, Dluhy RG, Lifton RP, Guay-Woodford LM. Low peripheral plasma renin activity
as a critical marker in pediatric hypertension. Pediatr Nephrol 1997;11: 343-346.

Hall et al., Circ. Res. 2015;116:991-1006.