factor viia for emergent warfarin reversal david pavlik, pharm.d. clinical specialist –...
TRANSCRIPT

Factor VIIa for
Emergent Warfarin Reversal
David Pavlik, Pharm.D.Clinical Specialist – Trauma/Critical Care
Allegheny General HospitalPittsburgh, PA
PSHP Annual Assembly – October 1st, 2008
Disclosures / Conflict of Interest
• None
ObjectivesObjectives• Review warfarin-related pharmacology Review warfarin-related pharmacology • Evaluate available options for warfarin reversalEvaluate available options for warfarin reversal• Evaluate Factor VIIa pharmacology and Evaluate Factor VIIa pharmacology and
pharamcokineticspharamcokinetics• Summarize Factor VIIa literature for warfarin reversalSummarize Factor VIIa literature for warfarin reversal• Compare PCC to rVIIa for warfarin reversalCompare PCC to rVIIa for warfarin reversal
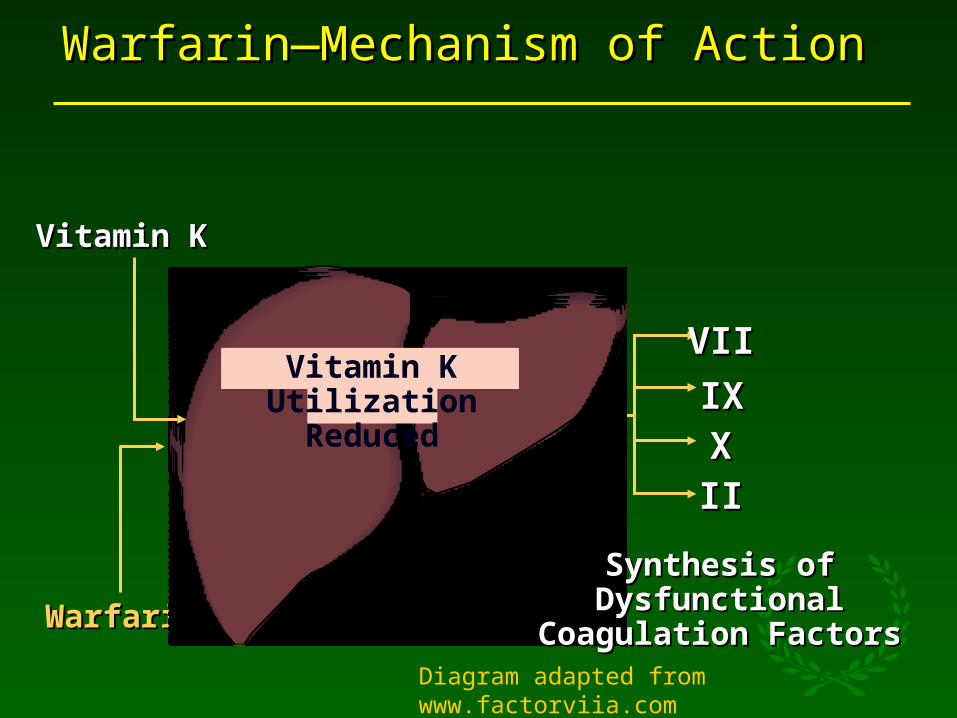
Warfarin—Mechanism of ActionWarfarin—Mechanism of Action
Vitamin KVitamin K
WarfarinWarfarin
Synthesis of Dysfunctional Synthesis of Dysfunctional Coagulation FactorsCoagulation Factors
VIIVII
IXIXXXIIII
Vitamin K Utilization Reduced
Diagram adapted from www.factorviia.com
Vitamin KVitamin K
• Required for prolonged reversal of warfarin
• Order in most cases of severe warfarin-related bleeding

Warfarin Related BleedingWarfarin Related Bleeding

ACCP – Serious/Life Threatening Bleed
• Hold Warfarin• Vitamin K
• Fresh Frozen Plasma OR• Prothrombin Complex OR• Factor VIIa
Ansell et al. CHEST 2008;133:160S

Fresh Frozen Plasma (FFP)• Volume Concerns
• INR = 2.5 then dose ~1600mL or 4-6 Units• INR > 5 then dose ~2800mL or 8-10 Units
• Infusion Time
• Factor concentrations variable• Delays in obtaining product
Aguilar M et al Mayo Clin Proc 2007; 82(1):82-92
Schulman et al N Engl J Med 2003; 349;675-83
Factor VIIa - Indications
• Hemophilia A or B with Inhibitors to Factors VIII or IX
• 90 mcg/kg every 2 hours as needed
• Factor VII deficiency• 15-30 mcg/kg every 4-6 hours as needed

Factor VIIa Off-Label
• Massive Transfusion• Trauma• Cardiothoracic Surgery
• Coagulopathy• Liver Disease/Transplant• Hematologic Disorders• Warfarin

TF-Bearing CellTF-Bearing Cell
VaVaTFTF VIIaVIIa XaXa
XX IIIIIIaIIa VIII/vWFVIII/vWF
VIIIaVIIIa
VV VaVa
PlateletPlatelet
TFTFIXIX
IXaIXa
Activated PlateletActivated Platelet
Coagulation PathwayCoagulation Pathway
XX
XaXaVIIIaVIIIaIXaIXa
Adapted from: Hoffman et al. Adapted from: Hoffman et al. Blood Coagul FibrinolysisBlood Coagul Fibrinolysis 1998;9(suppl 1):S61. 1998;9(suppl 1):S61.
VIIaVIIa
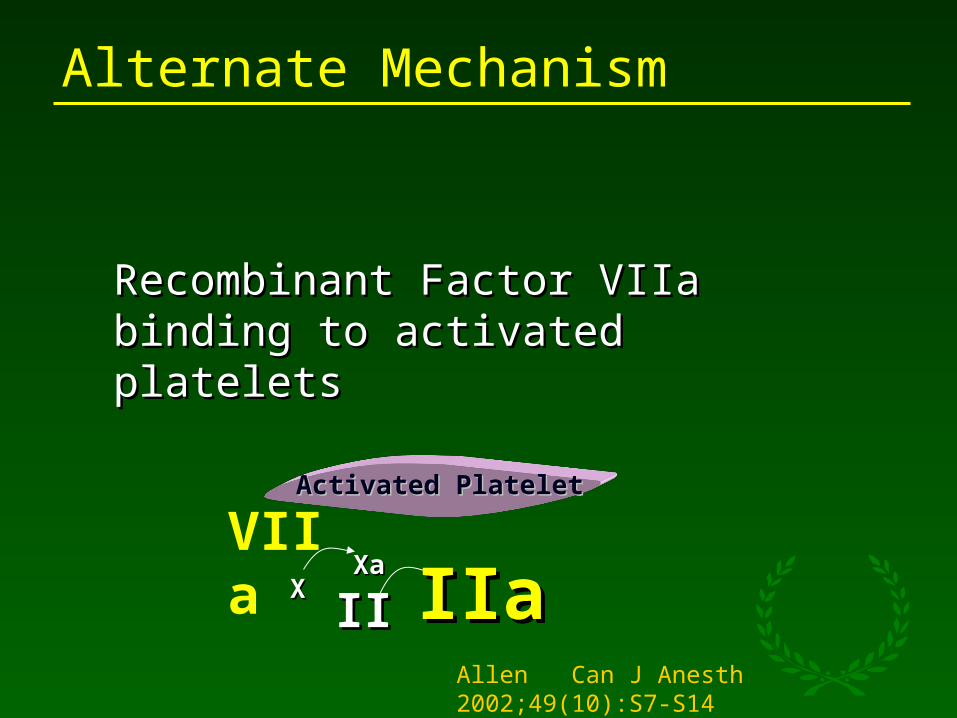
Alternate Mechanism
Activated PlateletActivated Platelet
XXXaXa
IIaIIaIIII
Recombinant Factor VIIaRecombinant Factor VIIabinding to activated plateletsbinding to activated platelets
Allen Can J Anesth 2002;49(10):S7-S14
VIIa

Factor VIIa - Kinetics
• Onset• 10-20 minutes
• Infusion volume <10mL
• Half-Life• 2.5 hours
• Recombinant Product

CCostost
Agent Cost
Fresh Frozen Plasma (4-6 Units) $300-500
Prothrombin Complex 2000 Units $1020-1620
Prothrombin Complex 3000 Units $1530-2430
Factor VIIa 1-2mg (~15-20mcg/kg) $1100-2200
Factor VIIa 3-4mg (~40mcg/kg) $3300-4500
Factor VIIa 6-7mg (~90mcg/kg) $6500-8000
Deveras et al.
• Reported 13 patients on warfarin• Doses
• 12-90 mcg/kg• 8 with 1.2mg (12-25 mcg/kg)
• Indications• Supratherapeutic INR/High risk of bleed• Rapid reversal required• Invasive procedures• Bleeding
Deveras Ann Int Med 2002; 137:884-888

Deveras - Low-Dose rFVIIa
Patient Indication Dose
mcg/kg (mg)
Pre-INR Post-INR
55F Bleeding 20 (1.2) 13.9 5.6
41M Procedure 14 (1.2) 3.4 1.7
56M Bleeding 14 (1.2) 5.8 2.9
38M High Risk 15 (1.2) 6.2 2.1
74M Procedure 12 (1.2) 2.6 1.6
73F Procedure 17 (1.2) 1.9 0.7
44M High Risk 15 (1.2) 11.9 3.2
81F High Risk 25 (1.2) 8.9 3.2

ICH on Warfarin
Author N Adjunct Agents Dose(mcg/kg)
Outcome
Sorenson 7 FFP in 5/7Platelets in 1/7Vitamin K in 6/7
10-40 Hemostasis
Lin 4 FFP in 4/4 16-22 1 Death3 Recover
Veschev 1 Not stated 120 Death
Dutton 9 Not stated 36-152 5 Death4 Discharged
Freeman 7 FFP + Vit K in 8/9 15-90 2 Death5 GCS=3

Dager et al.• 16 warfarin patients with major bleeding
• 12 CNS bleeding/Neurosurgery• 3 Retroperitoneal bleeding• 1 emergent reversal for bleeding during
laparotomy
• Fixed dose of 1.2 mg• Mean = 16 mcg/kg (11-25mcg/kg)
• All received FFP• 13/16 received Vitamin K
Dager et al. Pharmacotherapy 2006;26(8):1091-98
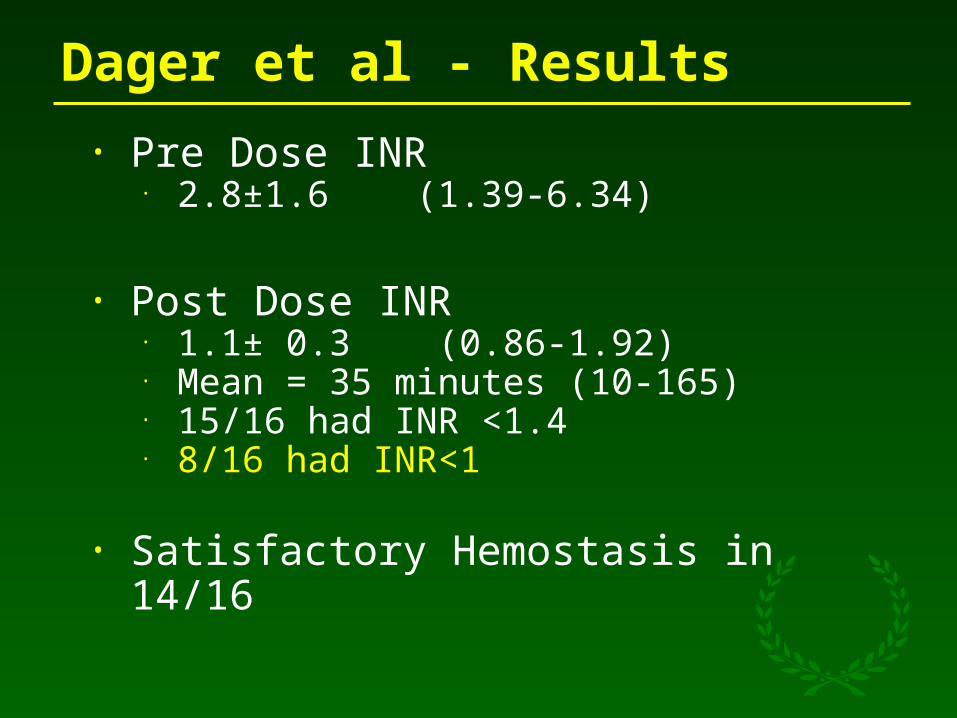
Dager et al - Results
• Pre Dose INR• 2.8±1.6 (1.39-6.34)
• Post Dose INR• 1.1± 0.3 (0.86-1.92)• Mean = 35 minutes (10-165)• 15/16 had INR <1.4• 8/16 had INR<1
• Satisfactory Hemostasis in 14/16
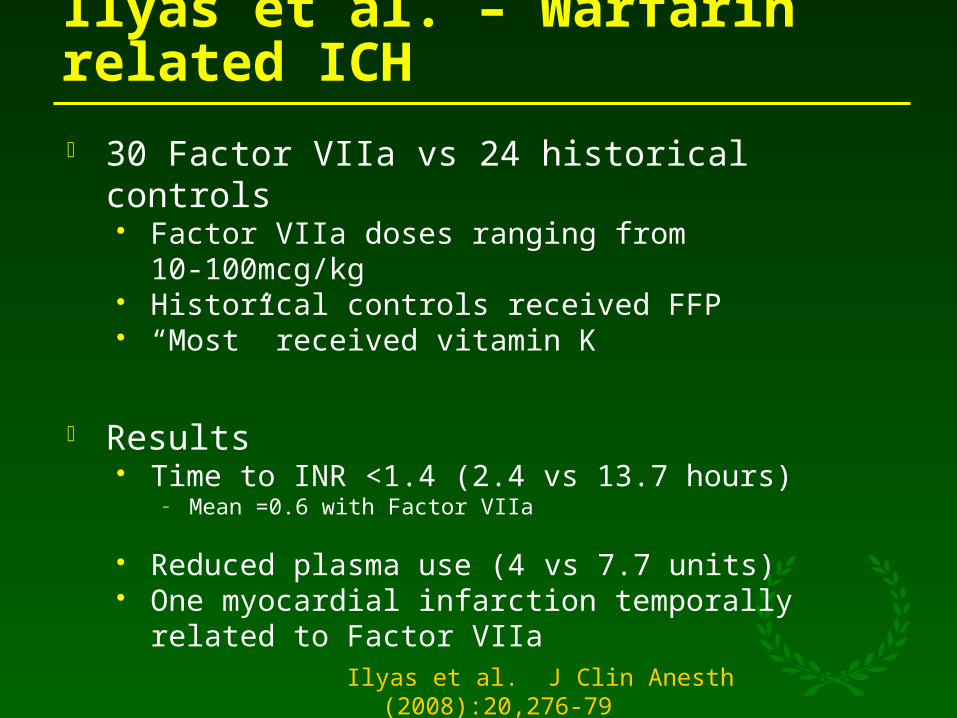
Ilyas et al. – Warfarin related ICH
30 Factor VIIa vs 24 historical controls Factor VIIa doses ranging from 10-100mcg/kg Historical controls received FFP “Most” received vitamin K
Results Time to INR <1.4 (2.4 vs 13.7 hours)
– Mean =0.6 with Factor VIIa
Reduced plasma use (4 vs 7.7 units) One myocardial infarction temporally related to
Factor VIIa
Ilyas et al. J Clin Anesth (2008):20,276-79

Ilyas et al.

Thrombotic Events - Factor VIIaThrombotic Events - Factor VIIa
Hemophlia 1-2 %
Trauma Study 3-6 %
ICH Study
Arterial Events
9-10%
9 vs 4%
CT Surgery 16 %
Warfarin Reversal ??
Levi Crit Care Med 2005;33(4):883 Boffard J Trauma 2005;59:8-18
Mayer N Eng J Med 2008; 358:2127 Karkouti Transfusion 2005;45:26-34.
PCC Disadvantages
• Extended half-lives• Factor II (60hrs)• Factor X (30hrs)
• Availability
• Viral Transmission
• Optimal dose/methodology unclearSorenson et al. Blood Coagl Fibrinolysis 2003 12:469-77
Aguilar M et al Mayo Clin Proc 2007; 82(1):82-92
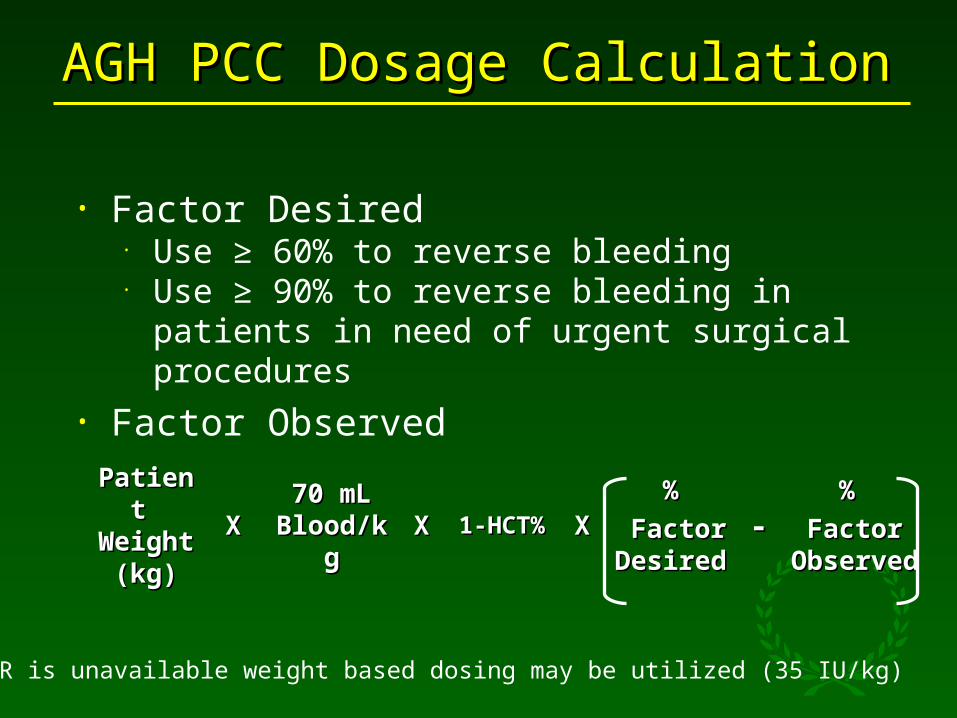
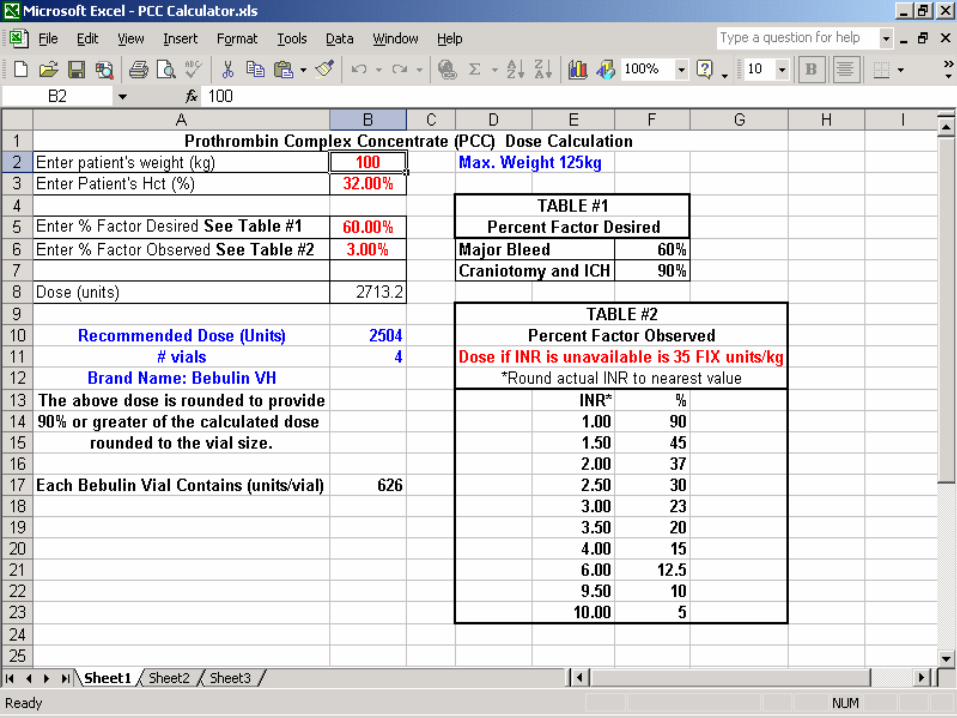
AGH PCC Dosage CalculationAGH PCC Dosage Calculation
• Factor Desired• Use ≥ 60% to reverse bleeding• Use ≥ 90% to reverse bleeding in patients in need
of urgent surgical procedures
• Factor Observed
Patient Patient Weight Weight
(kg)(kg)XX
70 mL 70 mL Blood/kgBlood/kg XX 1-HCT%1-HCT% XX
%%
Factor Factor DesiredDesired
--% %
Factor Factor ObservedObserved
*If INR is unavailable weight based dosing may be utilized (35 IU/kg)

Factor ObservedFactor ObservedINRINR Factor %Factor %
1.01.0 9090
1.51.5 4545
2.02.0 3737
2.52.5 3030
3.03.0 2323
3.53.5 2020
4.04.0 1515
6.06.0 12.512.5
9.59.5 1010
10.010.0 55

So easy Korczynski can do it!

AGH PCC Dosage CalculationAGH PCC Dosage Calculation Weight (kg)Weight (kg) Hematocrit %Hematocrit % Factor DesiredFactor Desired
Level of factors needed to be replacedLevel of factors needed to be replaced Use ≥ 60% to reverse bleedingUse ≥ 60% to reverse bleeding Use ≥ 90% to reverse bleeding in patients in need of urgent Use ≥ 90% to reverse bleeding in patients in need of urgent
surgical proceduressurgical procedures Factor ObservedFactor Observed
Using reported INR and Factor Observed TableUsing reported INR and Factor Observed Table
Patient Patient Weight Weight
(kg)(kg)XX
70 mL 70 mL Blood/kgBlood/kg XX 1-HCT% 1-HCT%
%%
Factor Factor DesiredDesired
--% %
Factor Factor ObservedObserved
*If INR is unavailable weight based dosing may be utilized (35 IU/kg)
X
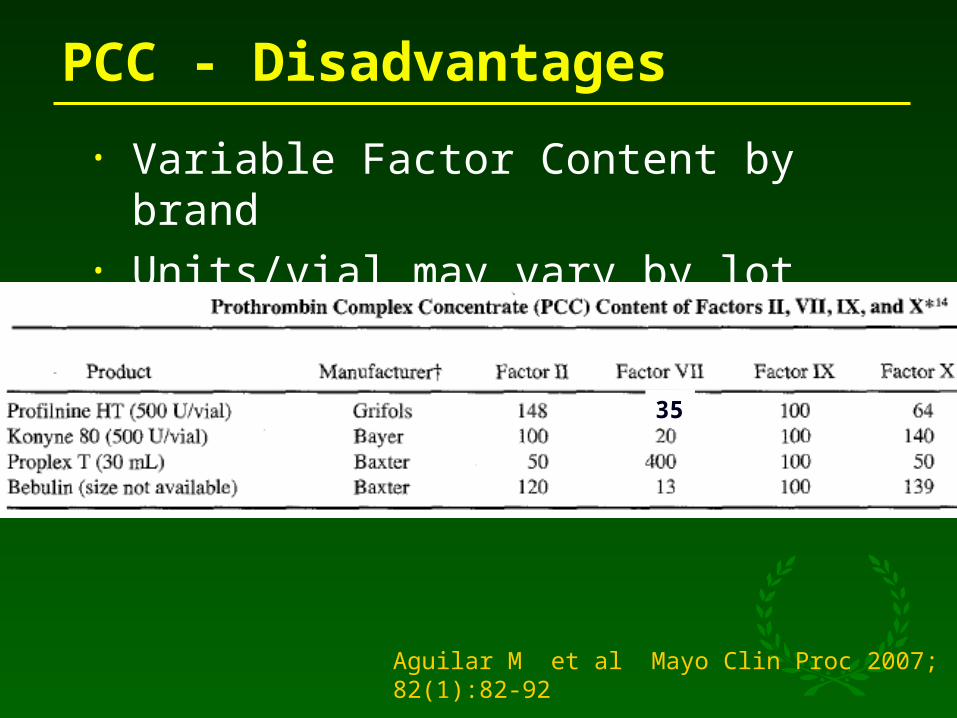
PCC - Disadvantages
• Variable Factor Content by brand• Units/vial may vary by lot
Aguilar M et al Mayo Clin Proc 2007; 82(1):82-92
35

Conclusions
• Factor VIIa is an option for emergent warfarin reversal
• Optimal use not fully defined• Dose• Monitoring
• Large scale clinical trials are lacking

Prothrombin Complex Concentrates (PCC)for
Emergent Warfarin Reversal
Michael Korczynski Pharm.D.Clinical Specialist – Ambulatory Care
Allegheny General HospitalPittsburgh, PA
PSHP Annual Assembly – October 1st, 2008
DisclosuresDisclosures• NoneNone

ObjectivesObjectives• Review of warfarin-related bleeding riskReview of warfarin-related bleeding risk• Evaluate available options for warfarin reversalEvaluate available options for warfarin reversal• Examine PCC CharacteristicsExamine PCC Characteristics• Summarize PCC literatureSummarize PCC literature• Compare PCC to rVIIa for warfarin reversalCompare PCC to rVIIa for warfarin reversal

Warfarin and bleeding riskWarfarin and bleeding risk• Most common complication is bleedingMost common complication is bleeding
• Incidence can range from 5-50%Incidence can range from 5-50%• Related to intensity of anticoagulationRelated to intensity of anticoagulation• Risk factorsRisk factors
• Age > 65 yearsAge > 65 years• Age > 75 years with concomitant afib/ICHAge > 75 years with concomitant afib/ICH• History of GI bleedingHistory of GI bleeding• Comorbid disease states:Comorbid disease states:
• Hypertension Hypertension • Cerebrovascular diseaseCerebrovascular disease• Serious heart disease Serious heart disease • Renal insufficiencyRenal insufficiency
Am Fam Physician. 1999 Feb 1;59(3):635-46

Warfarin and Intracranial Hemorrhage (ICH)Warfarin and Intracranial Hemorrhage (ICH)
• Overall increases the risk of ICH 2-5xOverall increases the risk of ICH 2-5x• Depends on anticoagulation intensityDepends on anticoagulation intensity• Estimated to account for about 3500 ICHs annuallyEstimated to account for about 3500 ICHs annually• ~ 5 % of all non-traumatic ICH episodes ICH in the US~ 5 % of all non-traumatic ICH episodes ICH in the US• Spontaneous ICH among 70-year-olds averages 0.15 % Spontaneous ICH among 70-year-olds averages 0.15 %
per yearper year• Those closely monitored on warfarin (INR of 2- 3), risk Those closely monitored on warfarin (INR of 2- 3), risk
of ICH increases to 0.3 to 0.8 percent/yearof ICH increases to 0.3 to 0.8 percent/year
.
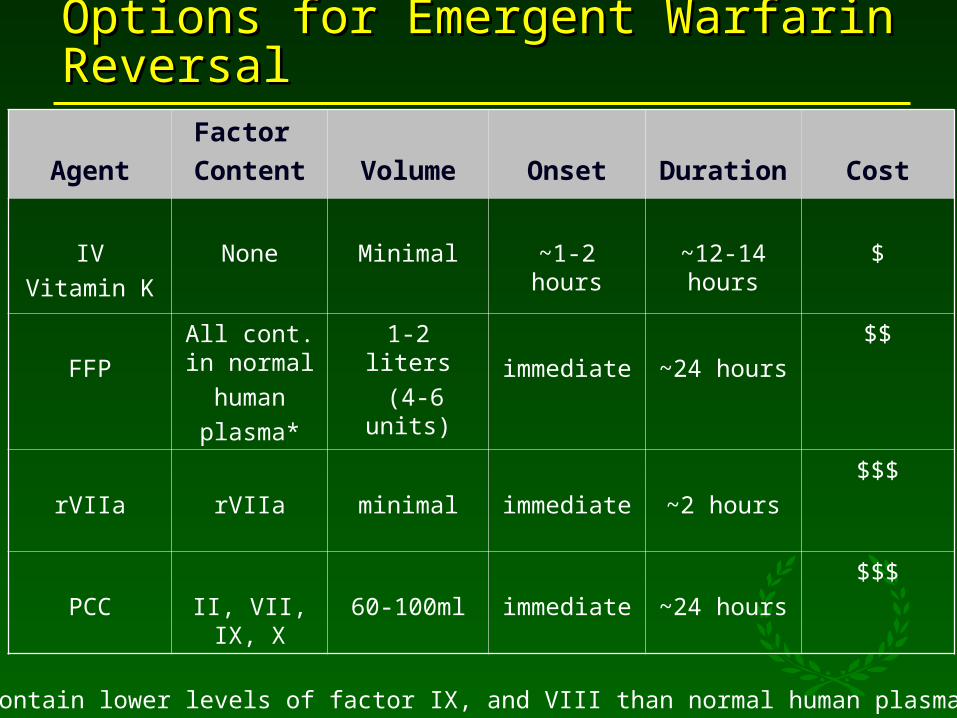
Options for Emergent Warfarin ReversalOptions for Emergent Warfarin Reversal
Agent
Factor
Content Volume Onset Duration Cost
IV
Vitamin K
None Minimal ~1-2 hours ~12-14 hours
$
FFP
All cont. in normal
human
plasma*
1-2 liters
(4-6 units) immediate ~24 hours
$$
rVIIa rVIIa minimal immediate ~2 hours
$$$
PCC II, VII, IX, X 60-100ml immediate ~24 hours
$$$
*may contain lower levels of factor IX, and VIII than normal human plasma
PCCPCC
• Pooled-plasma product from live donorsPooled-plasma product from live donors• Contains vitamin K dependent clotting Contains vitamin K dependent clotting
factors II, VII, IX, and Xfactors II, VII, IX, and X• FDA approved for the prevention and FDA approved for the prevention and
control of hemorrhagic episodes in control of hemorrhagic episodes in hemophilia B patientshemophilia B patients
• Literature reports for warfarin reversalLiterature reports for warfarin reversal
Baxter, Bebulin VH® (Package Insert)
New Product?New Product?
• Around since the early 1990’sAround since the early 1990’s• Concern of viral transmission Concern of viral transmission • More sophisticated purification More sophisticated purification
processes have reduced viral riskprocesses have reduced viral risk• Effective in correcting the INR and Effective in correcting the INR and
stopping bleedingstopping bleeding• Must be combined with Vitamin KMust be combined with Vitamin K

Bebulin VH®Bebulin VH®
• Vapor heat treated• Unit content differs between lots • Contains lyophilized powder and diluent• Must be refrigerated prior to mixing• Use within 3 hours of reconstitution• Infuse at ≤ 3ml/min
Product Factor II
Factor VII
Factor IX
Factor X
Bebulin VH 120 13 100 139
Baxter, Bebulin VH® (Package Insert)

Why PCC?Why PCC?
• PCC contains in clotting factors:PCC contains in clotting factors:• II (prothrombin), VII, IX, and X.II (prothrombin), VII, IX, and X.
• Warfarin depletes clotting factors:Warfarin depletes clotting factors:• II (prothrombin), VII, IX, and XII (prothrombin), VII, IX, and X
• Quick onset of action (15-30 minutes)Quick onset of action (15-30 minutes)• Long duration of action (~24 hours)Long duration of action (~24 hours)• Factor VIIa does not supplement all Factor VIIa does not supplement all
coagulation factors coagulation factors • Short half-life (~2.5 hours) Short half-life (~2.5 hours)
• CHEST GuidelinesCHEST Guidelines
General Usage ConsiderationsGeneral Usage Considerations
• Patients and families may object to PCC (a Patients and families may object to PCC (a pooled plasma product) or rVIIa on religious pooled plasma product) or rVIIa on religious grounds. grounds.
• PCC should only be used if traditional PCC should only be used if traditional modalities to correct warfarin related modalities to correct warfarin related bleeding are insufficient to work in a timely bleeding are insufficient to work in a timely mannermanner
• Patients at high risk for thrombosisPatients at high risk for thrombosis• Active ischemic diseaseActive ischemic disease• Mechanical heart valvesMechanical heart valves• Antiphospholipid antibody syndrome (APLS)Antiphospholipid antibody syndrome (APLS)

PCC CharacteristicsPCC Characteristics
Pros
Rapid reversal of INRRapid reversal of INR
Standardized coagulation factor Standardized coagulation factor componentscomponents
Limited volumeLimited volume
One-time dosingOne-time dosing
↓↓ risk of virus transmissionrisk of virus transmission
Cons
Limited dataLimited data
Cost (~$500/vial)Cost (~$500/vial)
Potential thrombosis riskPotential thrombosis risk
Lack of consensus on dosingLack of consensus on dosing

ACCP Management of Elevated INRsACCP Management of Elevated INRs
Life-Threatening Bleeding
Hold warfarinHold warfarin
Give FFP, PCC, or rVIIaGive FFP, PCC, or rVIIa
Supplement with vitamin K Supplement with vitamin K (10mg by slow IV infusion)(10mg by slow IV infusion)
Repeat, if necessary, Repeat, if necessary, depending on INRdepending on INR
Serious Bleeding at any elevation of INR
Hold warfarinHold warfarin
Vitamin K (10 mg by slow IV Vitamin K (10 mg by slow IV infusion); can be repeated infusion); can be repeated q12h q12h
Supplemented with FFP, PCC, Supplemented with FFP, PCC, or rVIIa, depending on the or rVIIa, depending on the urgency of the situationurgency of the situation
CHEST 2008

Literature ReviewLiterature Review
• Use for warfarin reversal has been Use for warfarin reversal has been documented:documented:
• Small prospective and retrospective Small prospective and retrospective studiesstudies
• Case reportsCase reports• Primary objective of most studies was to Primary objective of most studies was to
determine the efficacy of PCC based on INR determine the efficacy of PCC based on INR reversalreversal
• Various dosing regimens have be utilizedVarious dosing regimens have be utilized
Throb Res. 2005:115(6):455-9
Ann Hematol. 2003:8(2):121-3
Br J Haematol. 2002:116(3):619-24
Hematology 2001: 115:998-1001
Literature ReviewLiterature Review
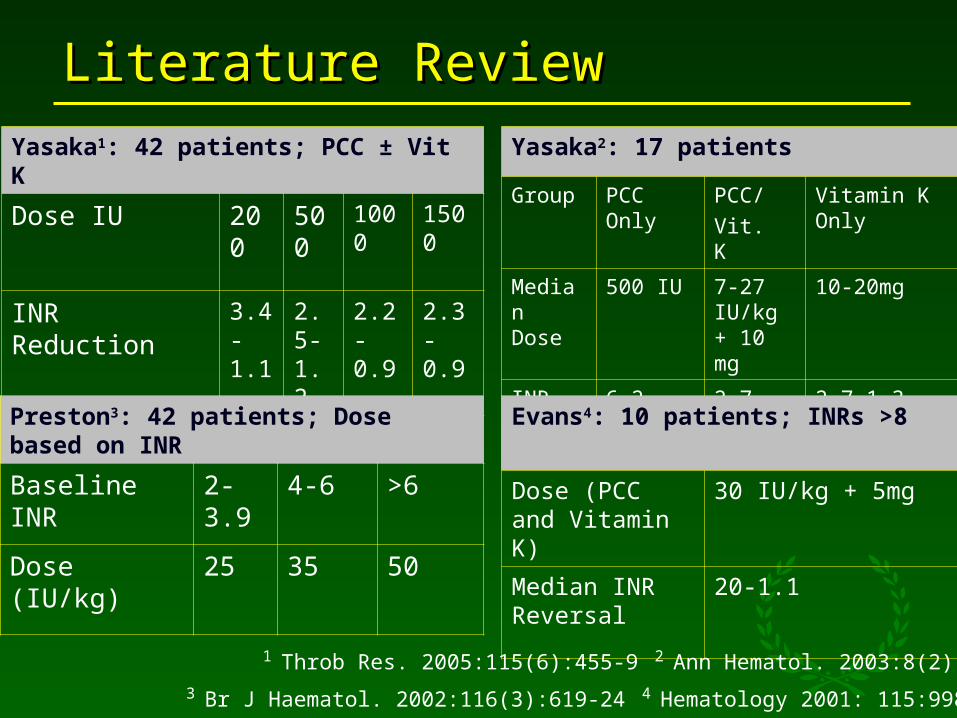
Yasaka1: 42 patients; PCC ± Vit K
Dose IU 200 500
1000
1500
INR Reduction 3.4-1.1
2.5-1.2
2.2-0.9
2.3-0.9
Yasaka2: 17 patients
Group PCC Only
PCC/
Vit. K
Vitamin K Only
Median Dose
500 IU 7-27 IU/kg + 10 mg
10-20mg
INR Reduction
6.2-2.1 2.7-1.1 2.7-1.3
Preston3: 42 patients; Dose based on INR
Baseline INR 2-3.9 4-6 >6
Dose (IU/kg) 25 35 50
Evans4: 10 patients; INRs >8
Dose (PCC and Vitamin K)
30 IU/kg + 5mg
Median INR Reversal
20-1.1
1 Throb Res. 2005:115(6):455-9 2 Ann Hematol. 2003:8(2):121-33 Br J Haematol. 2002:116(3):619-24 4 Hematology 2001: 115:998-1001

Literature ReviewLiterature ReviewLorenz1: 8 patients; PCC only fixed dose
Dose IUDose IU 36003600
INR INR ReductionReduction 3.4-1.33.4-1.3
Reiss2: 56 patients; PCC only weight-based
Dose IU/kgDose IU/kg 41.141.1/kg
INR INR
ReductionReduction 2.8-1.12.8-1.1
Lankiewicz3: 88 patients; PCC only weight-based
Dose IU Dose IU 25-50/kg25-50/kg
INR INR ReductionReduction 3.8-1.33.8-1.3
1 Blood Coagul Fibrinolysis. 2007 Sep;18(6):565-70 2 Thromb Res. 2007;121(1):9-16 3 J Thromb Haemost. 2006 May;4(5):967-70 4 J Thromb Haemost. 2008 Apr;6(4):622-31
Pabinger4: 43 patients; dosed based on weight and INR
Baseline INRBaseline INR 2-3.92-3.9 4-64-6 >6>6
Dose (IU/kg)Dose (IU/kg) 2525 3535 5050

PCC AdvantagesPCC Advantages
• Known factor contentKnown factor content• Low volumeLow volume• Contains factors II, VII, IX, XContains factors II, VII, IX, X• Rapid administrationRapid administration• Long duration of effect (~24 hours)Long duration of effect (~24 hours)• Only one dose requiredOnly one dose required
• Average dose: $1500Average dose: $1500• Dosing optionsDosing options
• Fixed dosingFixed dosing• Weight/INR Weight/INR • Factor replacementFactor replacement

PCC ConcernsPCC Concerns
• Risk of thrombosisRisk of thrombosis• Low risk of virus transmissionLow risk of virus transmission
• Hepatitis CHepatitis C• ParvovirusParvovirus
• Infusion reactionsInfusion reactions• CostCost
• $1500/dose$1500/dose
rVIIa CharacteristicsrVIIa Characteristics
• Contains only factor rVIIaContains only factor rVIIa• Short half-life (~2.5 hours)Short half-life (~2.5 hours)• May require multiple doses ($$$)May require multiple doses ($$$)
• 1mg = ~$11001mg = ~$1100• Limited literature support for warfarin reversalLimited literature support for warfarin reversal• No consistent approach to dosingNo consistent approach to dosing

Factor VIIa - Dose vs. Duration
– 5-20 mcg/kg– Duration ~4-8hrs– Cost~$1,100-2,200
– 40-80 mcg/kg– Duration ~10-12 hrs– Cost~$3,300-6,600
– 120-320mcg/kg– Duration ~18-20 hrs– Cost ~$9,900-25,600
Girard et al. Thromb Hemost 1998;80:109-13
Placebo

PCC vs rVIIaPCC vs rVIIa • In vivo rat and in vitro human modelsIn vivo rat and in vitro human models • Compared recovery of endogenous thrombin Compared recovery of endogenous thrombin
generationgeneration• Rats received phenprocoumon Rats received phenprocoumon • Humans received warfarinHumans received warfarin• Plasma samples from warfarin-treated individualsPlasma samples from warfarin-treated individuals
• INR values of 2.1-6.7INR values of 2.1-6.7• Treatments evaluated using prothrombin time (PT) Treatments evaluated using prothrombin time (PT)
and thrombin generation measurementand thrombin generation measurement• PCC and rFVIIa reverse warfarin anticoagulation PCC and rFVIIa reverse warfarin anticoagulation
based on PTbased on PT• Only PCC restored overall thrombin generation Only PCC restored overall thrombin generation
Tanaka KA, et al. Thromb Res. 2008;122(1):117-23

Antifibrinolytic ActivityAntifibrinolytic Activity
• PCC and rVIIa added to plasma PCC and rVIIa added to plasma samples of warfarin-treated patientssamples of warfarin-treated patients
• PCC was more effective in increasing PCC was more effective in increasing thrombin compared to rVIIathrombin compared to rVIIa
• Warfarin activity dependent on reduced Warfarin activity dependent on reduced prothrombin activityprothrombin activity rather than factor VII
• Thrombin activity measured by Thrombinoscope system
Taketomi et al. Blood Coagul Fibrinolysis. 2008 Jan;19(1):106-8.Taketomi et al. Blood Coagul Fibrinolysis. 2008 Jan;19(1):106-8.

Risk of Adverse EventsRisk of Adverse Events
• All patients on warfarin have inherent risk of All patients on warfarin have inherent risk of thrombosisthrombosis
• Low risk of virus transmission with PCCLow risk of virus transmission with PCC• Use in emergent/life-threatening situationsUse in emergent/life-threatening situations• Cost/benefit analysisCost/benefit analysis• Is rapid correction necessary?Is rapid correction necessary?• Monitor for signs/symptoms of PE, DVT, MI, Monitor for signs/symptoms of PE, DVT, MI,
strokestroke

PCC Ordering ProtocolPCC Ordering Protocol• First doses MUST be ordered under the approval of an First doses MUST be ordered under the approval of an
attending physician for warfarin reversal ONLY. attending physician for warfarin reversal ONLY. • First doses require subsequent consultation with the First doses require subsequent consultation with the
Hematology attending on-call.Hematology attending on-call.• Only one dose will be ordered at a timeOnly one dose will be ordered at a time• One dose should be sufficientOne dose should be sufficient• If a second is requested, then consultation with the If a second is requested, then consultation with the
hematology/anticoagulation service is required.hematology/anticoagulation service is required.• Doses will be rounded to the nearest vial size. Vial size Doses will be rounded to the nearest vial size. Vial size
can vary from depending on product and lot availabilitycan vary from depending on product and lot availability • All patients must receive Vitamin K 10 mg IV mixed in All patients must receive Vitamin K 10 mg IV mixed in
50mL NSS via slow infusion (over 30 minutes) along with 50mL NSS via slow infusion (over 30 minutes) along with PCCPCC

PCC Ordering ProtocolPCC Ordering Protocol
• Criteria for use:Criteria for use:• INR ≥ 2.5 INR ≥ 2.5 • Serious or life-threatening bleeding Serious or life-threatening bleeding
• Immediate reversal of warfarinImmediate reversal of warfarin• Immediate reversal of warfarin prior to an urgent Immediate reversal of warfarin prior to an urgent
neurosurgical procedureneurosurgical procedure• If above criteria not met PCC should not If above criteria not met PCC should not
be dispensedbe dispensed

AGH PCC Dosage CalculationAGH PCC Dosage Calculation Weight (kg)Weight (kg) Hematocrit %Hematocrit % Factor DesiredFactor Desired
Level of factors needed to be replacedLevel of factors needed to be replaced Use ≥ 60% to reverse bleedingUse ≥ 60% to reverse bleeding Use ≥ 90% to reverse bleeding in patients in need of urgent Use ≥ 90% to reverse bleeding in patients in need of urgent
surgical proceduressurgical procedures Factor ObservedFactor Observed
Using reported INR and Factor Observed TableUsing reported INR and Factor Observed Table
Patient Patient Weight Weight
(kg)(kg)XX
70 mL 70 mL Blood/kgBlood/kg XX 1-HCT% 1-HCT%
%%
Factor Factor DesiredDesired
--% %
Factor Factor ObservedObserved
*If INR is unavailable weight based dosing may be utilized (35 IU/kg)
X
PCC CalculatorPCC Calculator

PCC- Conclusions
• Emerging literature advocating PCC use in emergent warfarin reversal
• Dosing methods available:• Fixed dosing• Weight based dosing• Factor replacement dosing
• Large scale clinical trials lacking
Final Thoughts
Factor VIIa- possible uses for warfarin
• Emergent reversal• Serious/Life threatening bleeding• Reversal for emergent surgery
• Patients unable to receive blood products
• Other factor shortage• PCC, FFP
• At risk for circulatory overload

Factor VIIa - Dosing
• INR <4*• 15-20mcg/kg
• INR >4*• 40mcg/kg
*INR may not represent full factor repletion
• Standard therapy• FFP• Vitamin K
• Consider omission of Factor VIIa if FFP can be given in a timely fashion
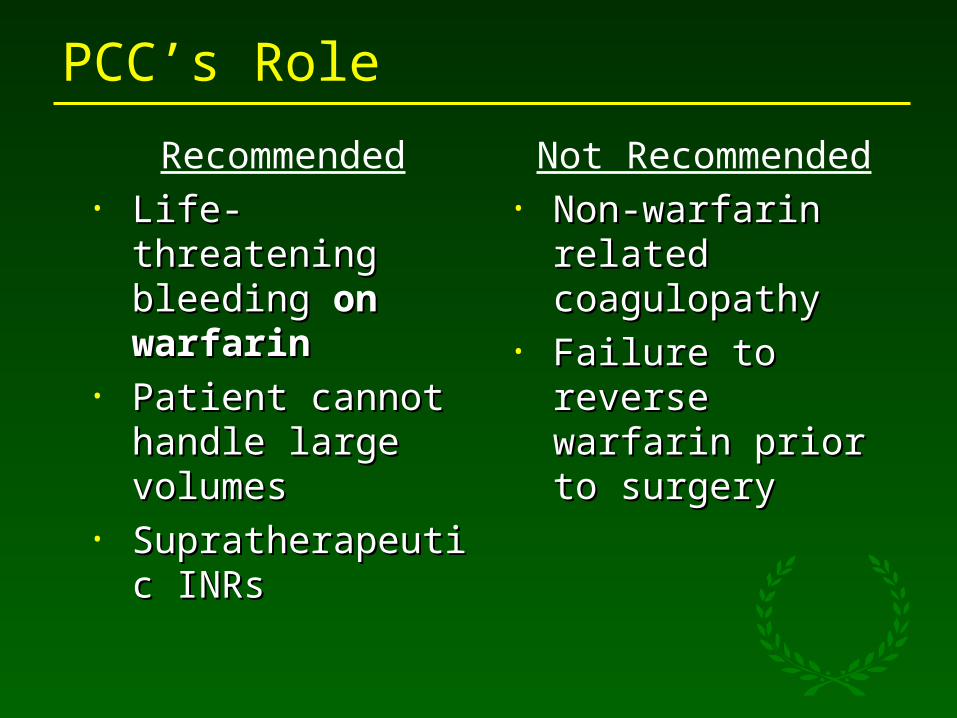
PCC’s Role
Recommended• Life-threatening Life-threatening
bleeding bleeding on on warfarinwarfarin
• Patient cannot Patient cannot handle large handle large volumes volumes
• Supratherapeutic Supratherapeutic INRsINRs
Not Recommended• Non-warfarin related Non-warfarin related
coagulopathycoagulopathy• Failure to reverse Failure to reverse
warfarin prior to warfarin prior to surgerysurgery
PCC/Factor VIIa - where NOT to use
• Active/recent ischemia or thrombosis• Hypercoaguable state
• APLS• Non-coagulopathic bleeding
• Spontaneous ICH• Minor bleeding• Elective Procedures• Overlapping DIC/Sepsis ?• Liver failure (PCC)
Mayer et al. N Engl J Med 2008;358:2127
Broderick et al. Stroke 2007;38:2001
Prothrombin Complex Concentrates (PCC)and Factor VIIa for
Emergent Warfarin Reversal
Michael Korczynski Pharm.D.Clinical Specialist – Ambulatory Care
David Pavlik, Pharm.D.Clinical Specialist- Trauma/Critical Care
Allegheny General HospitalPittsburgh, PA