factors affecting children's oral health: perceptions among latino parents
TRANSCRIPT

Factors affecting children’s oral health: perceptions amongLatino parentsjphd_287 82..89
Dharma E. Cortés, PhD1,2; Ludmila Réategui-Sharpe, MPH3; Avron Spiro, III, PhD3,4;Raul I. García, DMD, MMedSc3
1 Cambridge Health Alliance2 Harvard Medical School3 Department of Health Policy and Health Services Research, Boston University Henry M. Goldman School of Dental Medicine4 Department of Epidemiology, Boston University School of Public Health
Abstract
Objective: The objective of this study is to understand factors that influence the oralhealth-related behaviors of Latino children, as reported by their parents.Methods: Focus groups and in-depth interviews assessed parental perceptions,experiences, attributions, and beliefs regarding their children’s oral health. Guidingquestions focused on a) the participant’s child dental experiences; b) the impact ofdental problems on the child’s daily activities, emotions, self-esteem; c) parentalexperiences coping with child’s dental problems; and d) hygienic and dietary habits.Participants were purposively sampled from dental clinics and public schools with ahigh concentration of Latinos; 92 urban low-income Latino Spanish-speakingparents participated. Transcriptions of the audio files were thematically analyzedusing a grounded theory approach.Results: Parents’ explanations of their children’s dental experiences were catego-rized under the following themes: caries and diet, access to dental care, migrationexperiences, and routines.Conclusions: Findings revealed fundamental multilevel (i.e., individual/child,family, and community) factors that are important to consider for future interven-tions to reduce oral health disparities: behaviors leading to caries, parental knowl-edge about optimal oral health, access to sugary foods within the living environmentand to fluoridated water as well as barriers to oral health care such as lack of healthinsurance or limited health insurance coverage, among others.
Introduction
Oral health among Latino children
Despite two decades of efforts directed at eliminating ethnicand racial disparities, Latino children continue to have a highprevalence of caries and unmet oral treatment needs (1,2).National studies show that while the rates of dental caries aredeclining, Mexican American children have the highest per-centage of untreated caries compared with other ethnic/racialgroups (1). Latino children’s health disparities are importantbecause the percentage of Latino persons in the United Statescontinues to grow; Latinos are 16.3 percent of the total popu-lation in the United States and young children comprise a sig-nificant portion of this population (3).
Inadditiontoexperiencingdisproportionateratesof caries,Latino children are less likely to access dental care and otherpreventivemeasures (4).In2003,61percentof Latinochildrenhad at least one preventive dental visit in the past year, com-pared with 77 percent of White children and 66 percent ofBlack children (4). Limited access to dental services amongLatinos has been associated with lack of dental insurance,poverty, and low levels of education (5). A more recent studyfurther confirms a disproportionate oral disease burdenamong Latino children: Latino parents were four times aslikely to report their children’s oral health as fair or poor thannon-Latino White children and twice as likely to report thesame than parents of non-Latino Black children (6).
Qualitative studies conducted to understand oral healthdisparities in Latino children call for in-depth explorations of
Keywordsoral health; children; Latinos.
CorrespondenceDr. Dharma E. Cortés, Cambridge HealthAlliance/Harvard Medical School, Departmentof Psychiatry, 1493 Cambridge Street,Cambridge, MA 02139. Tel.: 617-905-9094;Fax: 617-503-2380; e-mail:[email protected]. Dharma E.Cortés is with Cambridge Health Alliance andHarvard Medical School. LudmilaRéategui-Sharpe is formerly with the BostonUniversity Henry M. Goldman School of DentalMedicine. Avron Spiro and Raul I. García arewith the Department of Health Policy andHealth Services Research, Boston UniversityHenry M. Goldman Schoolof Dental Medicine. Avron Spiro is withDepartment of Epidemiology, Boston UniversitySchool of Public Health.
Received: 6/24/2010; accepted: 8/18/2011.
doi: 10.1111/j.1752-7325.2011.00287.x
Journal of Public Health Dentistry . ISSN 0022-4006
82 Journal of Public Health Dentistry 72 (2012) 82–89 © 2011 American Association of Public Health Dentistry

beliefs that contribute to their suboptimal oral health out-comes. Butani et al. reviewed oral health-related culturalbeliefs from 1980 to 2006 and concluded that the majority ofstudies on ethnic/racial oral disparities are epidemiological innature and few focus on ideas and beliefs for specific popula-tions (7). Other studies that have qualitatively examinedLatino parental views on children’s oral health demonstratethe value of a qualitative approach to address knowledge gapsthat contribute to oral health disparities (8-10). Lopez DelValle et al. used focus groups to study beliefs, preferences, andbehaviors related to oral health and found that many Latinamothers were unaware of baby bottle tooth decay andthought that decay did not affect very young children (8). Twoqualitative studies with Spanish-speaking Mexican Americanmothers showed that the mothers recognized factors causingcaries, yet need comprehensive education on oral health(9,10).
Oral health among Latino children inMassachusetts
A recent statewide study conducted in Massachusetts amonga representative sample of kindergarteners, third and sixthgraders found that Latino children fare worse than non-Latino White children (11). Latino kindergarteners were 1.8times more likely than non-Latino white kindergarteners tohave untreated caries (41 percent); furthermore, 58 percent ofLatino third graders and 49 percent of sixth graders haveuntreated caries, rates that are 1.6 times more likely than theirnon-Latino White counterparts (11). Thus, although Massa-chusetts has achieved some Healthy People 2010 oral healthgoals of reducing the proportion of children aged six to eightwith dental caries and untreated decay, ethnic-related oraldisparities remain (11). The purpose of this study, conductedby the Northeast Center for Research to Evaluate and Elimi-nate Dental Disparities, was to examine the role of social andpsychological factors as potential sources of disparities in oralhealth.
Methods
Design
This qualitative study used focus groups and interviews withLatino parents or caregivers in schools and dental clinics ingreater Boston. The Boston University Institutional ReviewBoard and the schools approved the study; all participantsprovided written informed consent for their participation.
Procedures
Focus groups (in schools and clinics) and in-depth interviews(conducted only in clinics) assessed parental perceptions,
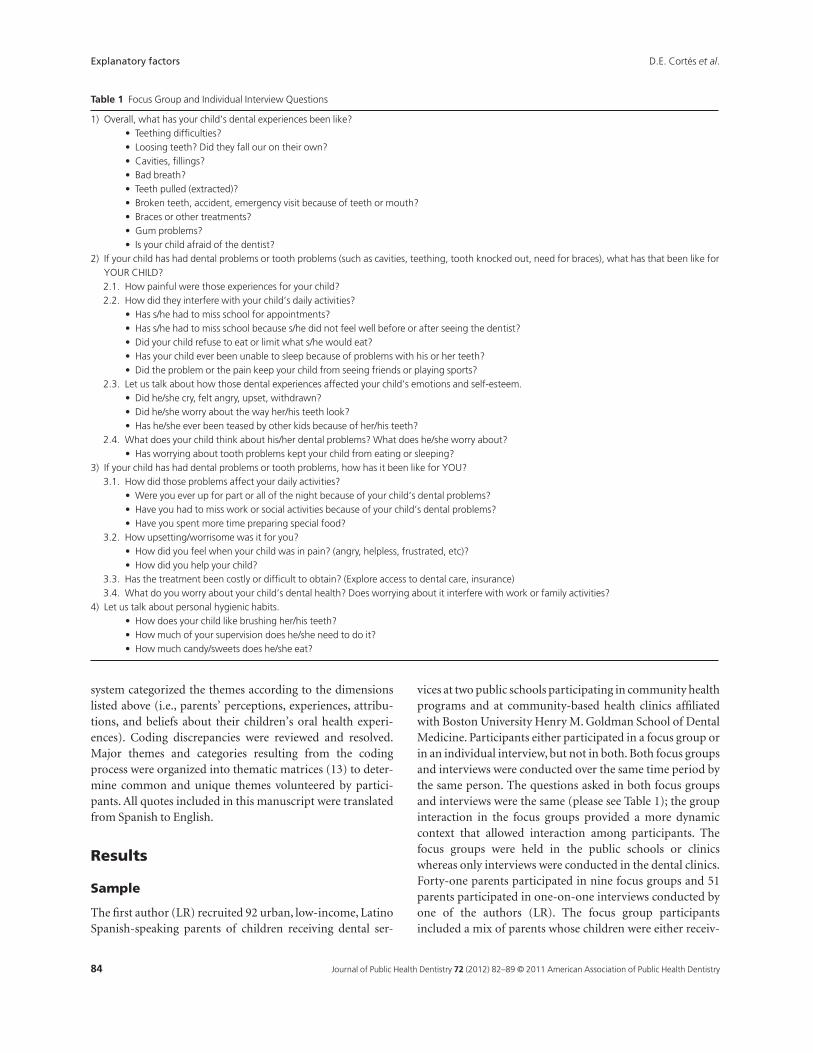
experiences, attributions, and beliefs regarding their chil-dren’s oral health. Questions focused on a) the participant’schild dental experiences; b) the impact of dental problemson the child’s daily activities, emotions, and self-esteem;c) parental experiences coping with child’s dental problems;and d) hygienic and dietary habits. Focus groups and inter-views followed the guide shown in Table 1; however, at theend of each session, the interviewer invited participants todiscuss topics not covered by the guide.
Sample recruitment
The study recruited Latino parents from different countries oforigin, regardless of immigration status (i.e., documented orundocumented), from two dental clinics and several publicschools with a high concentration of Latinos. In the clinics,Spanish-speaking Latino parents and caregivers (i.e., grand-parents) who brought children for a dental appointment wereapproached in person and invited to participate in an inter-view or focus group. In the public schools, classroom teachersgave invitation letters to parents through the children. Theletter, written in English and Spanish, instructed parents toreturn the tear-away portion of the letter with their contactinformation if they wanted to participate. One investigator(LR) contacted parents to confirm eligibility criteria: a)Spanish as primary language; b) Hispanic/Latino self-identification; and c) having children between ages 6 and 14;and arranged the focus group meetings. Only clinic partici-pants chose to participate in interviews because they could beconducted immediately after agreeing to participate in thestudy. All participants received $25 as incentive as a token ofappreciation.
Analytic procedure
The first two authors (native Spanish speakers) analyzedtranscriptions of the audio files in Spanish. They used agrounded theory approach (with NVIVO 7 software, QSRInternational, Doncaster,Victoria,Australia) to guide the the-matic analyses of interviews and the focus groups (12).
The goal of the analyses was to uncover parents’ per-ceptions, experiences, attributions, and beliefs about theirchildren’s oral health experiences. The grounded theoryapproach allowed authors to uncover and developempirically-based explanations of factors influencing oralhealth-related beliefs and practices among Latino parents inMassachusetts; this knowledge will inform interventionsdesigned to reduce oral health disparities.
The first two authors first read the transcripts to obtain ageneral view of the topics discussed during the interviews.Then, each of them, working independently, identified thewords and phrases that represented both broad categoriesand specific themes expressed by participants. The coding
D.E. Cortés et al. Explanatory factors
83Journal of Public Health Dentistry 72 (2012) 82–89 © 2011 American Association of Public Health Dentistry
system categorized the themes according to the dimensionslisted above (i.e., parents’ perceptions, experiences, attribu-tions, and beliefs about their children’s oral health experi-ences). Coding discrepancies were reviewed and resolved.Major themes and categories resulting from the codingprocess were organized into thematic matrices (13) to deter-mine common and unique themes volunteered by partici-pants. All quotes included in this manuscript were translatedfrom Spanish to English.
Results
Sample
The first author (LR) recruited 92 urban, low-income, LatinoSpanish-speaking parents of children receiving dental ser-
vices at two public schools participating in community healthprograms and at community-based health clinics affiliatedwith Boston University Henry M. Goldman School of DentalMedicine. Participants either participated in a focus group orin an individual interview, but not in both. Both focus groupsand interviews were conducted over the same time period bythe same person. The questions asked in both focus groupsand interviews were the same (please see Table 1); the groupinteraction in the focus groups provided a more dynamiccontext that allowed interaction among participants. Thefocus groups were held in the public schools or clinicswhereas only interviews were conducted in the dental clinics.Forty-one parents participated in nine focus groups and 51parents participated in one-on-one interviews conducted byone of the authors (LR). The focus group participantsincluded a mix of parents whose children were either receiv-
Table 1 Focus Group and Individual Interview Questions
1) Overall, what has your child’s dental experiences been like?• Teething difficulties?• Loosing teeth? Did they fall our on their own?• Cavities, fillings?• Bad breath?• Teeth pulled (extracted)?• Broken teeth, accident, emergency visit because of teeth or mouth?• Braces or other treatments?• Gum problems?• Is your child afraid of the dentist?
2) If your child has had dental problems or tooth problems (such as cavities, teething, tooth knocked out, need for braces), what has that been like forYOUR CHILD?2.1. How painful were those experiences for your child?2.2. How did they interfere with your child’s daily activities?
• Has s/he had to miss school for appointments?• Has s/he had to miss school because s/he did not feel well before or after seeing the dentist?• Did your child refuse to eat or limit what s/he would eat?• Has your child ever been unable to sleep because of problems with his or her teeth?• Did the problem or the pain keep your child from seeing friends or playing sports?
2.3. Let us talk about how those dental experiences affected your child’s emotions and self-esteem.• Did he/she cry, felt angry, upset, withdrawn?• Did he/she worry about the way her/his teeth look?• Has he/she ever been teased by other kids because of her/his teeth?
2.4. What does your child think about his/her dental problems? What does he/she worry about?• Has worrying about tooth problems kept your child from eating or sleeping?
3) If your child has had dental problems or tooth problems, how has it been like for YOU?3.1. How did those problems affect your daily activities?
• Were you ever up for part or all of the night because of your child’s dental problems?• Have you had to miss work or social activities because of your child’s dental problems?• Have you spent more time preparing special food?
3.2. How upsetting/worrisome was it for you?• How did you feel when your child was in pain? (angry, helpless, frustrated, etc)?• How did you help your child?
3.3. Has the treatment been costly or difficult to obtain? (Explore access to dental care, insurance)3.4. What do you worry about your child’s dental health? Does worrying about it interfere with work or family activities?
4) Let us talk about personal hygienic habits.• How does your child like brushing her/his teeth?• How much of your supervision does he/she need to do it?• How much candy/sweets does he/she eat?
Explanatory factors D.E. Cortés et al.
84 Journal of Public Health Dentistry 72 (2012) 82–89 © 2011 American Association of Public Health Dentistry

ing dental services or not. The number of participants in thefocus groups ranged from a low of two to a high of eight par-ticipants.
The countries of origin of parents were Puerto Rico (28percent), Dominican Republic (20 percent), Honduras (13percent), El Salvador (13 percent), Colombia (12 percent),Guatemala (5 percent), Mexico (4 percent), United States (3percent), and Costa Rica (1 percent). About half (51 percent)of participants’ children were born in the United States; only3 percent of the parents were US born. Most participants (85percent) were women, and about 60-70 percent of the partici-pants were undocumented. The mean age of parents was 32.4years old and the mean number of years living in the UnitedStates was 12.7 (range 4-33 years). Three percent of parentsreported some college or technical studies, 66 percentreported receiving a high school diploma/General Equiva-lency Diploma, and 31 percent reported less than high schoolgraduation. In an effort to facilitate participant opennesswith the interviewer/focus group leader, no additional demo-graphic data were collected.
Findings
The coding process generated more than 60 unique codes,topics included the questions asked (i.e., how oral healthproblems impacted both parents and children; tooth prob-lems that lead to experiencing pain, loss of sleep; emotionalproblems related to oral health problems). Although thesequestions were specifically focused to generate descriptivenarratives of the nature and experience of pediatric dentalproblems, the resulting narratives gravitated toward the chal-lenges Latino parents face when they seek dental care, acommon result while conducting qualitative research.
The unique codes generated were organized under second-level thematic categories that parents used to explain theirchildren’s oral health status and experiences. And, althoughthe focus groups and interviews included aspects other thanoral health experiences, the findings presented here focusexclusively on what parents related to their children’s dentalexperiences. Caries and diet, access to dental care, migrationexperiences (including perceptions of discrimination), androutines were the themes that parents linked to their chil-dren’s oral health status. Findings are summarized below bythe thematic categories generated from the analyses.
Caries and diet
Most parents reported that their children had caries in boththeir primary and permanent teeth. One mother reportedthat her child had caries in 11 of her 22 teeth. Parents attrib-uted the presence of caries to eating candies, poor nutritionand dental hygiene practices. In contrast to children in theircountries of origin, parents reported that children in the
United States have more access to both money and candies;thus it is difficult for parents to restrain their children’s accessto sugary food:
. . . it is a problem in this country, there is way too muchcandy available and the kids have access to candies. I thinkthat (candy) is the thing that is affecting them the most.Here (in the United States), there is a reason to eat candies(Halloween, Christmas, St. Valentine’s Day). My childcame from the Dominican Republic with only one cavityand in about 2 years, she has gotten 14, 17 caries . . . fromeating candies.
Another parent said,“I think that part of the cause is candies,chocolate. I am not sure, but I’ve heard that, and also notbrushing your teeth correctly, that can lead to caries.” Onlyone mother attributed the presence of caries in “temporary”(primary or baby) teeth to putting her child to bed whilefeeding from a bottle of milk. However, she reported that thereason she knew this was because her child’s dentist explainedit to her.
Other parents made the connection between candies andinadequate oral hygiene. They pointed out that eating toomuch candy, combined with lack of proper dental hygiene,leads to caries. Most parents face the challenge of making surethat their children practice good oral hygiene. One parentindicated, “They (kids) eat too much candy and they do notbrush their teeth very well. For as long as they are little, youmake sure to take them to the bathroom, you brush theirteeth, but when they reach 10 and 11 years of age, you have tolet them do it on their own.”
Other nutritional aspects that parents linked to caries werelack of milk intake and too much junk food. One parent indi-cated, “Sometimes I think that is lack of milk . . . because she(daughter) used to drink a lot of milk, but as she grew, shestopped drinking milk.”
Migration experiences
Narratives related to migration experiences were salient;many parents compared dental services available in theircountries of origin versus those available in the United States.Parents rated the quality of the dental care services in theUnited States higher than in their countries of origin. Whenasked whether her child had caries in Honduras, a motherresponded, “Yes, he had them, but there you do not checktheir teeth. Here (United States), they do that in school.”Other parents echoed the role of schools in their children’soral health and dental care, “Here, one pays attention (todental care) because the school tells you about it.”None of theparents mentioned the use of dental sealants as one of the ser-vices that their children have received in the United States.
One mother described the quality of dental procedures inher country of origin,“Before I came, I took her to the dentistin Santo Domingo. They turned a simple problem into a very
D.E. Cortés et al. Explanatory factors
85Journal of Public Health Dentistry 72 (2012) 82–89 © 2011 American Association of Public Health Dentistry

bad one, damaged her teeth, and sent her for a root canal. Thedentist here (United States) found out that the (root) canalwas not done completely, it was not done properly.”
Socioeconomic status is an important factor influencingaccess to dental services in their countries of origin. Referringto her country of origin, a mother said, “Where I come from,there are two social classes: poor and high, because the middleclass disappeared. The middle class is now poor. Parents havea hard time taking care of their children, and that affectsparents and children alike. Sometimes they have to extract alltheir teeth because parents cannot afford dental care. Theycould have saved their teeth, but dental care is expensive.”
Perceptions of discrimination
Embedded in their migration experiences, some parentsviewed the selectivity in allocating health insurance coverageas a form of discrimination. “Not everyone can getMassHealth (Medicaid). If they are not citizens they cannotget it, and that is like discrimination, because I think that allkids should get medical care whether they are citizens or not.Maybe not the adults, but the children should have greaterprotections in order to grow with healthy teeth, and if they donot have health insurance, how is this going to be achievedbecause everything here is so expensive and hard to get?”
Although parents’ reports seemed to indicate that theywere fairly satisfied with their children’s access to dental care,they also noted other instances in which they felt discrimi-nated against. For example, one parent said, “In any part ofthe world, Latinos are discriminated against, but more here(United States). In all the states there is a little bit (of discrimi-nation), you know, and I think that they take care of youbecause they are forced to do it. They do it because they haveto do it not because you necessarily deserve the service.”Another mother interpreted as discrimination what appearedto be unhelpful staff attitudes, “As Latinos, I don’t think theyhelp us get more access. They tell you “go here” but they don’tsay “I’m going to make an appointment for you to go to thisplace.” You know, they just give you the “run around.” Forother people I see, you know, they say,“Oh, you need this? I’llset you an appointment so you get it done.” And it’s reallyhard. They just give it to other people that they assume havemore access to it. So you have to keep moving around, askingquestions to find out what you can do, what they can give you,what they can provide you and your kids.”
Access to dental care
Parents indicated that having dental insurance coverage isessential to good dental care and healthy teeth. However, thechallenges many of them face as they navigate a complexhealth insurance system are sources of great concern amongthem. In this regard, some parents have experienced situa-
tions in which their children’s dental insurance does notprovide certain benefits. One mother said, “Right now theykeep cutting (coverage). How are the kids going to get theirteeth fixed? That’s the scariest part, not having insurance andto have to get their teeth fixed; and then not being able to takethem to the place you want. Right now my daughter and him(son) need braces, and that’s one of my worries (not havinginsurance coverage). They’re growing up and they are notgetting confident in themselves, they’re being shy, are not ableto smile. Their teeth are not looking the way they want themto look.”
Another mother emphasized her children’s dental insur-ance’s limited coverage, “It does not cover everything. Look,my daughter has problems. When she was 14, they sent her tohave a root canal. I took her to the clinic and they told me thatthe insurance (Medicaid) did not cover that. She had Medic-aid and another health insurance plan, and I was very con-cerned because I thought she had full coverage.” Thissituation is of great concern to this mother because sheworries about the long-term consequences of poor oralhealth: “This upsets me a lot, my daughter’s teeth condition,because I know how valuable it is to have healthy teeth. I knowhow valuable a tooth is. So, when I see her with so manycaries, and that she needs a root canal and all that, I worry alot. It looks ugly when you are missing teeth and it affectsevery other area (of your life), because if there is a bad tooth,that could affect other body organs, and that worries me alot.”
In addition to limited insurance coverage, parents alsoreport appointment scheduling as a barrier to access. A fre-quent complaint of parents was that they have too long towait before they can bring the child to an appointment.Another obstacle for parents is conflict with work schedules.Many parents take time off from work to bring their child to adental appointment, and when they have more than one childit is hard for them to take them to different appointmentsinstead of bringing them all on the same day. Most parentsindicated that missing work involves a reduction in salarywages; and for most parents who do not own a car, publictransportation adds another level of challenge to make it tothe dentist office.
Another mother compared the dental services received inthe United States versus the ones received in her country oforigin, by saying, “In Santo Domingo, they did not do theX-rays, they did here and all the services he (her son) got here.It’s easier to get the service here.” Another parent added,“There are more services here because it’s paid for, the gov-ernment helps. It is different there (country of origin). Thereyou have to pay. It is very difficult (to get the service) and isexpensive. There, dental services are expensive. People therego to the dentist when a tooth hurts, to pull out a tooth, notlike here, where they do treatment, like for example, a rootcanal to see if they can save the tooth.”
Explanatory factors D.E. Cortés et al.
86 Journal of Public Health Dentistry 72 (2012) 82–89 © 2011 American Association of Public Health Dentistry

According to participants, having health insurance in theUnited States eases access to dental care; however, mostparents did not have health insurance coverage. Most chil-dren received their health insurance coverage through thestate’s Children Health Insurance Program. One parentindicated, “His (son’s) health insurance covers everything.However, as you know, it is very hard for parents because, atleast in my case, I do not have dental insurance. I applied for“free care” in this clinic, but I was not eligible. But thank God,he (son) is eligible until age 18 or maybe until age 21, I think.”One mother reported the same situation by saying, “Kids arecompletely covered, but adults are not.”
Routines
When talking about their children’s oral health problems,such as caries, parents indicated that establishing a routinehelps making sure that their children practice good oralhygiene. However, they also reported challenges trying toachieve this. One parent said, “They (children) do not have ahabit of brushing their teeth. I have to be on top of my twoyounger kids because they usually fall asleep before theybrush their teeth. Sometimes, you do not have the time (tosupervise them) and they have already fallen asleep, and youdo not want to wake them up. At least that is what happens inmy case.”
Another parent said, “you have to encourage them to do it(brush their teeth). You have to get them the kind of brushthat they like, the toothpaste that they like, you know. That ispretty basic when it’s hard to make kids to brush their teeth.The most important thing is for them to develop the habit,before they go to bed, because if a child does not develop thehabit at a very young age, he will grow up and will not brushhis teeth.”
One parent suggested that tooth brushing becomes a partof a child’s routine, “Kids need to be reminded most of thetime. You have to tell them to brush their teeth beforebedtime, and they do not do it out of laziness. It is tedious andkids do not like it. They have to be encouraged. There aremany ways to encourage them. You could buy toothpaste thatcomes in many different forms; encourage them with theirfavorite cartoon characters.” One mother indicated that it isimportant to teach her child to brush his teeth after everymeal and after eating candy.
Discussion
This qualitative study provided first-person accounts of per-ceptions of pediatric oral health and dental care among asample of Spanish-speaking Latino parents in Massachusetts,most of whom are immigrants. Findings shed light on issuesimportant to consider for interventions to reduce oral healthdisparities, and on the interrelated nature of social determi-
nants of oral health (14), such as personal and contextualfactors that may influence the efforts that immigrant parentstake to address the dental care needs of their children. UsingFisher-Owens et al.’s multilevel conceptual model, whichtakes into account levels of influence on oral health outcomescoming from the individual, family, and community (15), wepresent potential directions that could be taken to developinterventions to address oral health disparities amongLatinos in light of our findings.
Migration experience emerged as a pervasive factor relatedto their children’s oral health. On the one hand, parents per-ceived that living in the United States leads to an increase inthe incidence of caries in children by virtue of access to sugaryfoods. On the other hand, living in the United States facilitatesaccess to dental care. This raises the question of whether theincrease in caries that parents perceive might be a result ofbetter access to dental care in the United States comparedwith their countries of origin, which leads to a greater detec-tion of caries, rather than more caries, per se. Fisher-Owens’model calls for interventions that address community-,family-, and individual- /child-level influences. At the com-munity level, there is the need to assess access to sugary foodswithin the living environment as well as whether childrenreside in fluoridated areas. At the family level, it would beimportant to address health behaviors and practices, whichcould be counter to optimal oral health, as some of the find-ings presented here suggest. Finally, at the child level, diet,use of dental care, and health behaviors and practices couldbe modified using child- and family-focused educationalapproaches.
The role of routines in proper dental hygiene offers greatpotential for influencing changes in health behaviors andpractices. Parents reported that children need to be remindedabout brushing their teeth after meals, after eating candy, andbefore bedtime. Some parents described routines that theyestablished to develop enduring habits in their children.Using social marketing, routines could be supported by mass-media messages directed to parents and children. Finally, therole of sealants in the prevention of caries, a theme absentfrom the narratives, offers opportunities for educationalinterventions. Educational interventions need to be availablein Spanish to be able to influence behavioral changes amongparents similar to those who participated in this studybecause evidence suggests that Spanish speakers are morelikely to report fair or poor condition of their teeth (16).
An important child-level influence that emerged from thisstudy – also noted by Fisher-Owens’ conceptual model – is therole that health insurance plays in connecting children withdental care. Parents observed that in most instances the chil-dren were the only members in the family who enjoy the ben-efits of dental insurance coverage. Most parents in this studydid not have health insurance coverage; we suspect (but pur-posefully we did not ask) that one of the reasons is ineligibility
D.E. Cortés et al. Explanatory factors
87Journal of Public Health Dentistry 72 (2012) 82–89 © 2011 American Association of Public Health Dentistry

because of immigration status. Even when children haveinsurance, some parents complained that the coverage usuallyleftoutservices suchasrootcanalsandorthodontic treatment.Parents whose children needed services that were not coveredby their health insurance expressed a great deal of concernabout the impact that unattended oral health problems haveon their children’s overall health and quality of life. Soon afterthe data for this study were collected, a law was passed in Mas-sachusetts that requires that residents who can afford healthinsuranceobtain it.Thegoalof thisbill is toachievenearlyuni-versal health insurance, while at the same time providing cov-erage to those who cannot afford it.Two important parts of thebill thatarerelevant tothepopulationweincludedinthisstudyare a) the increase in Medicaid eligibility to children in familiesearning up to 300 percent of the Federal Poverty Level and b)the bill’s aim at reducing racial and ethnic health disparities byrequiring hospitals to collect and report on health care datarelated to race, ethnicity, and language. In addition, the billredirects a portion of the public funds used to provide “freecare” through hospitals to subsidize care for the uninsured.While98percentof Massachusetts residentshavehealth insur-ance,Latinoswith lowEnglishproficiencyareatamuchhigherrisk of being uninsured and lacking access to care than othergroups (17).
Another factor, embedded in the community-level influ-ence stratum, was perceived discrimination. Some parentsfelt being treated as second-class citizens, as they sought helpand information to procure the dental care their childrenneed. This finding reveals that navigating the US health caresystem requires more than just health insurance coverage. Itrequires knowledge and personal agency, including health lit-eracy, which has been found to have multidimensionalimpact on children’s oral health outcomes (18).
Other community-level factors that surfaced as importantissues affecting Latino children’s access to dental care wereparental hardship in the form of lost wages (when parentsneed to take unpaid time off from their jobs to take their chil-dren to their dental appointments) and transportation diffi-culties. While these obstacles have been documented in theliterature (19), interventions to address them are required.
Increasing health literacy and self-efficacy, by teachingparents how to navigate both the health insurance and healthcare systems, could reduce the frustration they experiencebecause of ill-informed expectations about health insurancebenefits and coverage. Schools appeared to be an optimalconduit through which parents new to this country couldlearn about the importance of procuring preventive dentalcare for their children, as evidenced by a study that examinedthe influence of school-based oral health education on fami-lies’ daily health practices (20). School-based dental pro-grams could become the link between parents who have littleexperience with dental care and a complex health insurancesystem that many parents fail to understand.
Acknowledgments
The authors would like to acknowledge Dr. Judith A. Jonesand Carolyn J. Wehler for their assistance during the develop-ment of this manuscript and their valuable feedback.
The work presented in this original research report is sup-ported by National Institute of Dental and CraniofacialResearch Grant Numbers U54 DE014264, K24 DE018211,and K24 DE00419.
References
1. U.S. Department of Health and Human Services (HHS). Oralhealth in America: a report of the surgeon general. (NIH Pub.No.00-4713). Rockville, MD: HHS, National Institutes ofHealth, National Institute of Dental and CraniofacialResearch; 2000.
2. United States General Accounting Office (GAO). Oral health:dental disease is a chronic problem among low-income popula-tions. (Pub. No. HEHS-00-72). Washington, DC: GAO; 2000.
3. Passel JS, Cohn DV, López MH. Census 2010: 50 millionLatinos. Hispanics account for more than half of nation’s growthin past decade. Washington, DC: Pew Hispanic Center; 2011.
4. U.S. Department of Health and Human Services, HealthResources and Services Administration, Maternal and ChildHealth Bureau. The oral health of children: a portrait of statesand the nation 2005. The National Survey of Children’s Health2003. Rockville, MD: U.S. Department of Health and HumanServices; 2005.
5. Garcia R. Addressing oral health disparities in diversepopulations. J Am Dent Assoc. 2005;136:1210-2.
6. Dietrich T, Culler C, Garcia RI, Henshaw MM. Racial andethnic disparities in children’s oral health: the national surveyof children’s health. J Am Dent Assoc. 2008;139:1507-17.
7. Butani Y, Weintraub JA, Barker JC. Oral health-relatedcultural beliefs for four racial/ethnic groups: assessment ofthe literature. BMC Oral Health. 2008;8:1-13.
8. Lopez Del Valle LM, Riedy CA, Weinstein P. Rural PuertoRican women’s views on children’s oral health: a qualitativecommunity-based study. J Dent Child. 2005;7:61-6.
9. Hoeft KS, Masterson EE, Barker JC. Mexican Americanmothers’ initiation and understanding of home oral hygienefor young children. Pediatr Dent. 2009;31:395-404.
10. Hoeft KS, Barker JC, Masterson EE. Urban Mexican-American mothers’ beliefs about caries etiology in children.Community Dent Oral Epidemiol. 2010;38:244-55.
11. White BA, Monopoli MP, Souza BS. Catalyst Institute. Theoral health of Massachusetts’ children. January, 2008.
12. Glaser B, Strauss A. The discovery of grounded theory: strategiesfor qualitative research. Chicago: Aldine Publishing Co; 1967.
13. Strauss AL. Qualitative analysis for social scientists. Cambridge[Cambridgeshire]; New York: Cambridge University Press;1987.
14. Spencer N. Social, economic, and political determinants ofchild health. Pediatrics. 2003;112:704-6.
Explanatory factors D.E. Cortés et al.
88 Journal of Public Health Dentistry 72 (2012) 82–89 © 2011 American Association of Public Health Dentistry

15. Fisher-Owens SA, Gansky SA, Platt LJ, Weintraub JA,Soobader MJ, Bramlett MD Newacheck PW. Influences onchildren’s oral health: a conceptual model. Pediatrics.2007;120:e510-20.
16. Telford C, Coulter I, Murray L. Exploring socioeconomicdisparities in self-reported oral health among adolescents inCalifornia. J Am Dent Assoc. 2011;142(1):70-8.
17. Maxwell JH, Cortés DE, Schneider K, Graves A, Rosman B.Massachusetts health care reform reduces disparities. HealthAffairs. 2011;30(8):1-10.
18. Vann WF, Lee JW, Baker D, Divaris K. Oral health literacyamong female caregivers: impact on oral health outcomes inearly childhood. J Dent Res. 2010;89(12):1395-400.
19. Flores G, Vega LR. Barriers to health care access for Latinochildren: a review. Fam Med. 1998;30:196-205.
20. Garbin C, Garbin A, Dos Santos K, Lima D. Oral healtheducation in schools: promoting health agents. Int J DentHyg. 2009;7(3):212-6.
D.E. Cortés et al. Explanatory factors
89Journal of Public Health Dentistry 72 (2012) 82–89 © 2011 American Association of Public Health Dentistry