factors associated with cancer
TRANSCRIPT
3.Factors Associated With Cancer

Contents
Associated WithVarious%actors. . ......,.108
FIGURE
Figure No. Page18. Relative Risks of Esophageal Cancer in
Relation to the Daily Consumption ofAlcohol and Tobacco . . . . . . . . . . . . . . . . . . 75

Factors Associated With Cancer
A select committee of the World Health Orga-nization (WHO) broadly defined environmen-tally caused cancers as those in which extrinsicfactors are responsible (364):
These include all environmental carcinogens(whether identified or not) as well as “modifyingfactors” that favor neoplasia of apparently in-trinsic origin (e. g., hormonal imbalances, die-tary deficiencies, and metabolic defects).
This overarching picture of “environment”contrasts sharply with the more usual use of theword “environment .“ Common usage is re-stricted to what is seen as the purview of the En-vironmental Protection Agency (EPA): air,water, and soil.
GENETICS AND ENVIRONMENT
Environment, as used in this assessment, ex-cludes genetic factors. Genetic makeup does,however, play a role in determining the prob-ability of an individual developing cancer.Knudson (201) classifies all individuals as fallinginto four groups, according to the participationof heredity and environment in the possibledevelopment of cancer:
1.
2.
3.
4.
genetic predisposition to cancer even inthe absence of environmental variation;predisposition imposed by environmentalvariation in the absence of genetic varia-tion;predisposition imposed by both geneticand environmental factors; andneither genetic nor environmental predis-position.
The first category represents individuals witha genetic defect who have an extremely highprobability of developing one or more particu-lar cancers, regardless of environmental factors.Retinoblastoma, a malignancy of the retina, is a
The WHO committee expressed its belief that“the majority of cancers are caused by, or theircausation modified by extrinsic factors” (364).This view represents a general consensus amongcancer researchers, and lays the foundation forthe theory that the majority of cancers arepreventable. Individuals have gone further thanthe WHO committee, and have used figures of60 to 90 percent for the proportion of cancersthat are potentially preventable (31,115,164,165,166,368). These and other estimates havebeen erroneously cited as if they referred only toman-caused pollution or even more narrowly,only to manmade chemicals, in the “envi-ronment. ” In this report, “environment” is usedto describe the gamut of exposures and behav-iors that are associated with cancer.
childhood cancer which develops in about 95percent of those with the genetic predisposition.Several other childhood tumors—neuroblas-toma and Wilms’ tumor of the kidney—fall intothis category. In adults, polyposis of the colon,an inherited condition, often leads to coloncancer; another hereditary syndrome is charac-terized by high susceptibility to cancers of thecolon and endometrium, and other inheritedconditions are associated with other cancersites. Fortunately, these conditions are relative-ly rare and are involved in probably 1 to 2 per-cent of all cancer. Categories 2 and 4 representcancers which are not dependent on geneticsusceptibility.
A well-understood example of the third cat-egory is xeroderma pigmentosum, a genetic con-dition involving a defect in deoxyribonucleicacid (DNA) repair mechanisms. Affected indi-viduals exposed to ultraviolet light, a compo-nent of sunlight, develop skin tumors, as well asother skin abnormalities and some internal
65
66 ● Technologies for Determining Cancer Risks From the Environment
tumors. However, if sunlight is avoided entire-ly, these individuals will not develop tumors.Both environmental and hereditary predispos-ing factors must be present for clinical manifes-tation of the disease.
Xeroderma pigmentosum is rare, but the oc-currence of many common cancers have a ge-netic component as well. One of potentiallylarge importance is an apparent relationship be-tween genetically controlled responses to ciga-
rette smoke carcinogens (197) and the probabil-ity of developing lung cancer.
Daughters of breast cancer patients have ahigher risk of developing breast cancer thanwomen without this family history, thoughmany other factors affect the probability of thecancer occurring. Individuals with deeply pig-mented skin have a lower risk of skin cancer in-duced by sunlight. (The above discussion drawsheavily on Knudson (201).)
MULTISTAGE DEVELOPMENT OF CANCER
Cancer epidemiology and experimental car-cinogenesis have established that the carcino-genic process is multifactor in its causation andmultistage in its development (302).
Multifactored causality means that severalagents, environmental and genetic, may be in-volved in cancer occurrence. The multistep de-velopment of cancer is pictured as involving atleast two steps which must occur in sequence inthe cell that is eventually to develop into a tu-mor. The two steps are generally called “initi-ation” and “promotion,” and more generalterms are “early” and “late” events.
Some substances, “complete carcinogens, ”function both as initiators and promoters.Other substances are known to behave only aseither initiators or promoters.
Initiation is seen as occurring in response toan external stimulus and produces a cell that is“latently premalignant” (302). The initiationevent is generally thought to be a mutationalchange in the cell’s genetic material, but the
SHARED RESPONSIBILITY
Attribution of the risk of cancer to specific,single causes is the exception rather than therule. Genetic factors affecting individual sus-ceptibility are frequently part of the interaction.Of more relevance to this assessment are envi-ronmental agents which interact with each otherto produce carcinogenic effects.
change is unexpressed and causes no detectablechange in the cell’s growth pattern. Initiatedcells can remain as such for at least a large seg-ment of the animal’s life without being re-moved, destroyed, or otherwise harmed in anymeasurable way (116).
In laboratory experiments, exposure of an ini-tiated cell to another substance, a promoter,converts the cell to an “irreversible malignancy”(302). Promoters convert only initiated cells totumor cells and have no lasting effect on nonini-tiated cells. The long latency period between ex-posure to carcinogens and the manifestation ofdisease may represent the time necessary for theoccurrence of a promotional event.
The importance of initiation and promotion(or early and late events in carcinogenicity) inhumans is that interference in either one mightreduce cancer’s toll. Radman and Kinsella (302)draw attention to the possibility of identifyingsubstances which can inhibit the activities ofeither initiators or promoters.
There is clear evidence that smoking actssynergistically with some other factors. Syn-ergism in this context means that the number ofcancers resulting from exposure to two agents isgreater than the sum of cancers that would beexpected from the two exposures individually.Smoking interacts with ionizing radiation to

Ch. 3—Factors Associated With Cancer ● 67
produce cancer of the lung; and with alcohol toproduce cancer of the esophagus. One of thebest known synergisms is the interaction oftobacco and asbestos.
Asbestos and Smoking
In 1979, the Surgeon General stated (286):
Asbestos provides one of the most dramaticexamples of adverse health effects resulting frominteraction between the smoking of tobaccoproducts and an agent used in the workplace.
Exposure to asbestos is one of the most exten-sively studied occupational health hazards, andone which continues to attract the efforts of epi-demiologists, in part because of its interactionwith smoking, Indisputable evidence links as-bestos to lung cancers and to rare cancer types,mesotheliomas of the pleura and the perito-neum. Smokers exposed to asbestos, especiallythose exposed at high levels, have a much great-er probability of developing lung cancers thaneither smokers not exposed to asbestos, or non-smokers exposed to asbestos. Rates for meso-theliomas, on the other hand, are similar forsmokers and nonsmokers exposed to asbestos.
Hammond, Selikoff, and Seidman (156) haveanalyzed mortality data from a large group ofU.S. male asbestos insulation workers. Com-putations were carried out comparing the in-sulation workers to a control group of malesfrom a large cohort assembled by the AmericanCancer Society (ACS). Table 10 presents the re-sults of the analysis, supporting the existence ofstrong synergism between smoking and expo-sure to asbestos in the production of lung can-cer. As the authors explain, if the two exposures
were acting independently in this cohort, onewould predict the following (156):
. . . the lung cancer death rate of asbestosworkers with a history of cigarette smokingshould be very close to the sum of the followingthree numbers: 11.3 (the rate for the “no,no”group), 47.1 (the mortality difference for the“yes, no” group), and 111.3 (the mortality dif-ference for the “no, yes” group). The sum comesto 169.7 lung cancer deaths per 100,000 man-years . . . . In contrast, the observed lung can-cer death rate of the “yes, yes” group was 601.6per 100,000 man-years. The difference (601.6 –169.)7 = 431.9 lung cancer deaths per 100,000man-years, was presumably due to a synergisticeffect in men with both of the two types of ex-posure . . , .
Another measure, in addition to the mortalitydifference, is the mortality ratio, which in thiscase is the lung cancer death rate in each of thefour exposure groups, divided by the lungcancer death rate in the group of nonsmokerswho were not exposed to asbestos (group 1).The mortality ratio for exposure to both agents,53.24, is much higher than would be expectedfrom the additive effects of cigarette smokingalone (mortality ratio = 10.85) and asbestos ex-posure alone (mortality ratio = 5.17). The ef-fects appear to be multiplicative.
Attribution of Risk
In the case of smoking and asbestos, and inother cases where two or a variety of factors in-teract to produce some cases of cancers, thedisease may be prevented by interventions inany of the factors. Shared responsibility, how-ever, complicates the attribution of risk to a
Table 10.—Age-Standardized Lung Cancer Death Ratesa for Cigarette Smoking and/or Occupational Exposureto Asbestos Dust Compared With No Smoking and NO Occupational Exposure to Asbestos Dust
Exposure to History of Mortality MortalityGroup asbestos? cigarette smoking Death rate difference ratio
Control No No 11.3 0.0 1.00Asbestos workers Yes No 58.4 + 47.1 5.17Control No Yes 122.6 + 111.3 10.85Asbestos workers Yes Yes 601.6 + 590.3 53.24
aRat,s ~~r 100000 man. YearS standardized for age on tfle distribution Of tfle man-years of all the asbestos workers. Number Of lUn9 cancer deaths b=ed on death Certlfl-cate information.
SOURCE: Hammond, Sellkoff, and Seldman (156)

68 ● Technologies for Determining Cancer Risks From the Environment
particular factor. Adding up the numbers ofcases that might be prevented by various indi-vidual measures taken separately may producea total number of “preventable” cancers largerthan the number that actually occurs. An exam-ple of this concept, presented in table 11, isbased on Lloyd’s (214) analysis of the asbestosinsulation worker mortality data describedabove. He estimated the percentage reduction inlung cancer mortality that would accrue byeliminating smoking cigarettes alone to be 88.5percent, and by eliminating exposure toasbestos alone to be 79.6 percent. By eliminat-ing both exposures, the total reduction would be97.8 percent, and not the sum of the individualreductions, which would amount to a whopping168.1 percent. The multifactorial nature of
Table 1 1.—Estimates of Percentage Reduction inLung Cancer Mortality in Asbestos Workers by
Elimination of Exposure to Cigarettesand to Asbestos
Percentage reduction fromStatus current rate
Current. . . . . . . . . . . . . . . . . . . . 0.0Eliminate smoking only . . . . . . 88.5Eliminate asbestos only. . . . . . 79.6Eliminate smoking andasbestos. . . . . . . . . . . . . . . . . . 97.8
SOURCE: Lloyd (214).
cancer means that it is impossible a present aneat balance sheet adding up to 100 percent thatindicates the proportion of all cancers that canbe attributed to factors X, Y, and Z.
ESTIMATES OF THE AMOUNTS OF CANCER ASSOCIATED WITHENVIRONMENTAL FACTORS
Diverse methods have been used to produceestimates of the amounts of cancer associatedwith various exposures and behaviors. Themethods are variously described as rangingfrom “seat of the pants, ” to “top of the head,” tofigures based on more quantified inputs. Evi-dence for associations between various “factors”and cancer ranges from very strong to veryweak. There is no relationship between thestrength of the association and the estimatedmagnitude of the amount of cancer associatedwith a factor. For instance, the strongest asso-ciations include those ‘between smoking tobaccoand respiratory cancers, between asbestos andcancer of the lung and other sites, and betweenionizing radiation and cancer at many sites.While each of the three associations is strong,the percentage of cancer associated with each isdifferent. Smoking is associated with more than20 percent of cancer, asbestos with between 3and 18 percent, and natural background radia-tion, with less than 1 to 3 percent.
The importance of a factor, as measured bythe magnitude of the proportion of cancer withwhich it is associated, is one starting point fordeciding on the development of preventive strat-
egies. However, a large proportion, by itselfdoes not give any indication of the practicalityor availability of strategies. If all factors wereequally well understood, and preventive strat-egies equally available, one would choose to gofor big reductions. Under real conditions, strat-egies that can be implemented receive pref-erence.
Most numerical estimates of associations arebased on cancers occurring today or in the lastfew years. Therefore, they are not predictors ofcarcinogenic activity today, but reflections ofcarcinogenic activity in the past, possibly 20 to50 years ago. A few authors have attempted torelate today’s carcinogenic risk to future cancersand these are also cited.
All factors discussed here have not been” in-vestigated equally in the scientific community,either because of perceived differences in rela-tive importance, or because of difficulty in ob-taining meaningful results. Therefore, it has notbeen possible for “equal” evidence to be pre-sented for each factor in this assessment. Evi-dence for carcinogenicity in humans from goodepidemiologic studies is given more weight thanare animal data.

Ch. 3—Factors Associated With Cancer ● 69
The remainder of this chapter discusses whatis known about the contributions of the follow-ing factors to cancer incidence and mortality:tobacco, alcohol, diet, occupation, pollution,consumer products, medical drugs and radia-tion, sexual development, reproductive patternsand sexual practices, natural radiation, infec-tion, and other or unknown associations. Cur-rent thinking, with some historical background,is presented for the major elements of each fac-tor, and attempts are made to mention studiesgiving quantified estimates of the importance ofvarious factors. 1
I Discussion of the factors draws heavily on a contract report bySir Richard Doll and Richard Pete, who were charged with review-ing existing literature about the quantified estimates of cancer cau-sation. They also made their own estimates, which are cited in thisassessment. Doll and Pete’s report, in its entirety, is published inthe ]ournul of National Cancer lm-titute (93).
TOBACCO
Diseases related to the smoking of tobacco in-clude lung cancer and cancer at other sites, cor-onary heart disease and stroke, chronic bronchi-tis and emphysema, and many other diseases,including peptic ulcers (157). Tobacco smoking“is the single most important preventable en-vironmental factor contributing to illness,disability, and death in the United States” (286).WHO (365) states:
Smoking-related diseases are such importantcauses of disability and premature death in de-veloping countries that the control of cigarettesmoking could do more to improve health andprolong life in these countries than any single ac-tion in the whole field of preventive medicine.
The harmful effects of tobacco are greaterwhen it is smoked as cigarettes than when con-sumed in other forms. This may be because acidcigarette smoke is less irritating than thealkaline smoke from pipes and cigars and, there-fore, more easily inhaled. However, tobaccoconsumption in any form appears to be accom-panied by adverse effects, most recently demon-strated in a study showing that long-time snuffdippers experience a highly increased risk oforal cancer (363).
The categories used are not necessarily “natu-ral” assemblages, nor are they the only possiblegroupings of the components. The discussion ofeach factor includes a description of importantinclusions and exclusions. For instance, the“diet” section looks at all “foodstuffs,” includingnaturally occurring and added contaminants.Drinking water, which is discussed under “pol-lution, ” and “alcohol,” which is treated as a fac-tor unto itself, are excluded from diet.
All of the estimates considered in preparingthe following discussion of factors are listed intable 19, at the end of this chapter. Only “bestestimates, ” either point estimates or intervals, aspresented by each author are included in the ta-ble. The primary references should be consultedfor acceptable ranges and/or confidence limits,exact data sources and methods, and caveats.
Tobacco is known to contribute more heavilyto the number of cancer deaths than any othersingle substance.. The relationship of cigarettesmoking and cancer was first suggested in the1920’s. During the 1950’s, results from many ep-idemiologic studies confirmed this association(287). Many carcinogens have been identified incigarette smoke, and the differences consistentlyobserved between rates of lung cancer amongregular cigarette smokers and lifetime non-smokers is so extreme that it is not likely to bean artifact of the epidemiologic method (287):
The 1964 Surgeon General’s Report reachedthe following conclusion: ‘Cigarette smoking iscausally related to lung cancer in men . . . Thedata for women, though less extensive, point inthe same direction. ’
Today, cigarette smoking is regarded as the ma-jor cause of lung cancer in both males and fe-males and is largely responsible for the recentrapid rise in female lung cancer rates. The 1980Surgeon General’s report, The Health Conse-quences of Smoking For Women, states (287):
. . . the first signs of an epidemic of smoking-relateddisease among women are now appearing.

70 ● Technologies for Determining Cancer Risks From the Environment
It has been predicted that by the early 1980’s,the age-adjusted female lung cancer death ratewill surpass the breast cancer rate, which istoday’s leading cause of cancer death in women.The Surgeon General’s 1980 report estimates(287):
. . . smoking will contribute to 43 percent of themale and 18 percent of the female newly diag-nosed cancer cases in the United States in 1980and to 51 percent of the male and 26 percent ofthe female cancer deaths.The principal impact of tobacco smoking is
on the incidence of cancer of the lung althoughcancer at many other body sites, includinglarynx, oral cavity, esophagus, urinary bladder,kidney, and pancreas are also associated (287).By late middle age, the risk of developing lungcancer is more than 10 to 15 times greater incigarette smokers than in lifelong nonsmokers(152). Present evidence indicates that the effectof smoking on the development of lung cancer isaffected by number of years smoked, age whensmoking began, the number of cigarettes smok-ed per day, the degree of inhalation, and thecomposition of the cigarette.
Studies have shown that discontinuing smok-ing decreases the risk of developing lung cancer.Ten to fifteen years following cessation ofsmoking, an ex-smoker’s risk of dying of lungcancer decreases to a level only about two timeshigher than the risk for lifelong nonsmokers(286). This phenomenon is nicely illustrated bydata in table 12 from an epidemiologic study ofBritish doctors (92).
Higginson and Muir (166) attributed 30 per-cent of male and 7 percent of female cancersfrom 1968 through 1972 in the Birmingham andWest Midland region of England to tobacco.They specifically ascribed 80 to 85 percent oflung cancers to smoking. Wynder and Gori(368) estimated that 28 percent of male and 8percent of female 1976 cancer deaths in theUnited States can be attributed to smoking.Their estimate is based on calculating the per-cent difference between U.S. mortality rates andthe lowest reported worldwide mortality ratesfor each site and by considering specific case-control studies.
Table 12.—Lung Cancer Mortality Ratiosin Ex.Cigarette Smokers, by Number of
Years Stopped Smoking
MortalityYears stopped smoking ratio
Still smoking. . . . . . . . . . . . . . . . . . . . . . . . . . . 15.81-4 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . “16.@5-9 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5.910-14 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5.315+ . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2.0Nonsmokers . . . . . . . . . . . . . . . . . . . . . . . . . . . 1.0
aThe higher mortality ratios observed in the 1-4 year Category after quittin9compared to those continuing smoking is believed to be due 10 thoseindividuals who quit smoking because of illness,
SOURCE: Doll and Peto (93).
Enstrom (100) reported:
If all Americans did not smoke, the mortalityreduction that would occur has been estimatedto be 80,000 lung cancer deaths plus 22,000other cancer deaths of the “1978 total of 390,000cancer deaths—a reduction of 26 percent.
Data from a representative sample of non-smokers derived from a 1966–68 National Mor-tality Survey indicated that this group had atotal cancer rate which was 24 percent less thanthat of all U.S. whites (100).
Numerous estimates have been made of thecontribution of tobacco to the overall cancerrate. Most have taken advantage of concurrentepidemiologic cohort studies, in which largenumbers of people are queried about theirsmoking habits at the initiation of the study andthen followed to determine their causes ofdeaths. The largest such study involved 1 mil-lion Americans who were self-identified assmokers or nonsmokers in 1959 and whose sub-sequent mortality was monitored by ACS. Themagnitude of the excess risk observed forwomen in the ACS population was less than formen. The difference is thought to be due towomen having smoked fewer cigarettes per day,inhaling less deeply, and being more likely tosmoke cigarettes with reduced tar and nicotine(153). In addition, women are less frequently ex-posed to occupational hazards, including thosethat may act additively or synergistically withtobacco to cause cancer.
Several researchers have evaluated data fromthe ACS study population. Doll and Peto (93)
Ch. 3—Factors Associated With Cancer ● 71
computed mortality rates from the ACS studygroup and estimated that between 25 and 40percent of 1978 American cancer deaths, with abest estimate of 30 percent (94,782 or 43 percentmale; 27,266 or 15 percent female), could be at-tributed to tobacco smoking. Their computationmethod assumes that the male and female age-specific cancer death rates observed among theACS nonsmokers, between 1960 and 1972,would have applied to the entire country had noone smoked.
Hammond and Seidman (155) estimated thatfrom 25 to 35 percent of cancer mortality in theU.S. male population and 5 to 10 percent in thefemale population are “mainly due to smokingof tobacco products and cigarettes. ” Enstrom(100) calculated a 38-percent reduction in thetotal cancer rate in the “never smoked regular-ly” group as compared with all U.S. whites.These estimates from ACS data do not greatlydiffer and the reported differences can be ex-plained by the different methodological ap-proaches and assumptions used. Hammond andSeidman (155) assumed that the age-specificdistribution of smoking habits in the ACS groupwas similar to the country as a whole and reliedon mortality rates computed for individualsclassified as smokers in 1959, many of whomare known to have quit the habit by 1967. In theapproach taken by Doll and Peto (93), it wasunnecessary to speculate on the smoking habitsof the general population and instead of using
mortality rates for smokers, they relied on can-cer rates in the nonsmoking group. The specificsof Enstrom’s (100) calculations were not given.
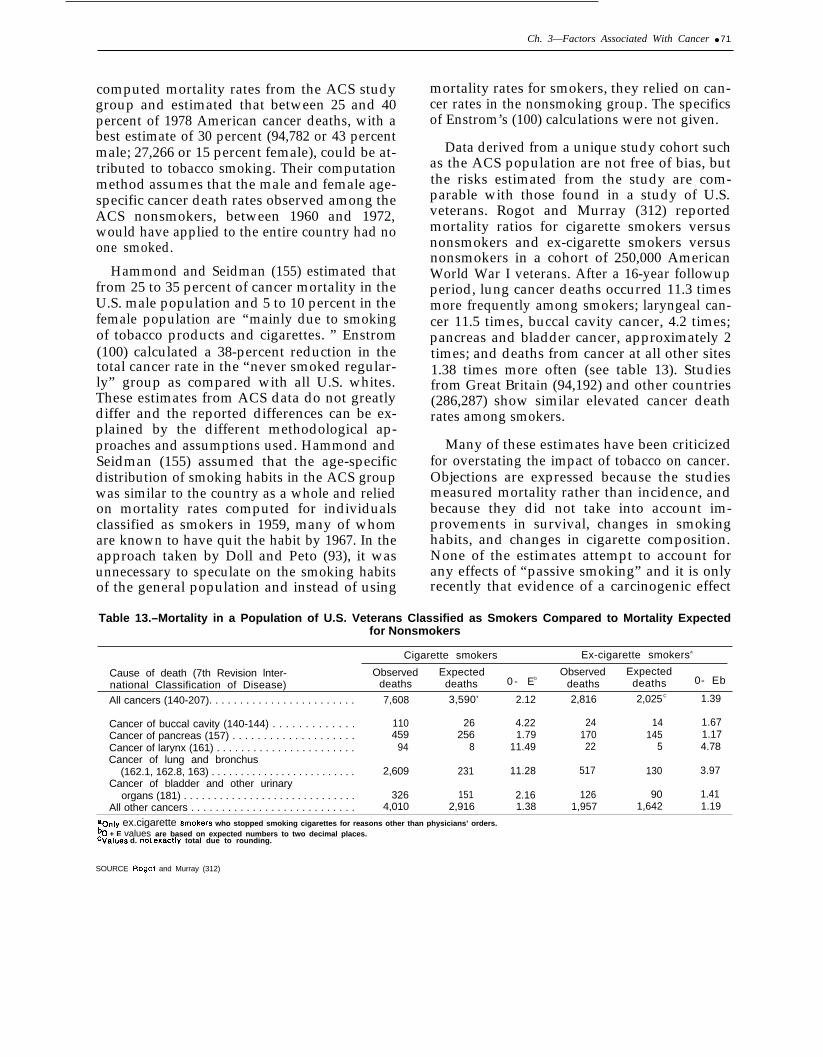
Data derived from a unique study cohort suchas the ACS population are not free of bias, butthe risks estimated from the study are com-parable with those found in a study of U.S.veterans. Rogot and Murray (312) reportedmortality ratios for cigarette smokers versusnonsmokers and ex-cigarette smokers versusnonsmokers in a cohort of 250,000 AmericanWorld War I veterans. After a 16-year followupperiod, lung cancer deaths occurred 11.3 timesmore frequently among smokers; laryngeal can-cer 11.5 times, buccal cavity cancer, 4.2 times;pancreas and bladder cancer, approximately 2times; and deaths from cancer at all other sites1.38 times more often (see table 13). Studiesfrom Great Britain (94,192) and other countries(286,287) show similar elevated cancer deathrates among smokers.
Many of these estimates have been criticizedfor overstating the impact of tobacco on cancer.Objections are expressed because the studiesmeasured mortality rather than incidence, andbecause they did not take into account im-provements in survival, changes in smokinghabits, and changes in cigarette composition.None of the estimates attempt to account forany effects of “passive smoking” and it is onlyrecently that evidence of a carcinogenic effect
Table 13.–Mortality in a Population of U.S. Veterans Classified as Smokers Compared to Mortality Expectedfor Nonsmokers
Cigarette smokers Ex-cigarette smokersa
Cause of death (7th Revision lnter- Observed Expected Observed Expectednational Classification of Disease) deaths deaths 0 - Eb
deaths deaths 0- Eb
All cancers (140-207). . . . . . . . . . . . . . . . . . . . . . . . 7,608 3,590’ 2.12 2,816 2,025C 1.39
Cancer of buccal cavity (140-144) . . . . . . . . . . . . . 110 26 4.22 24 14 1.67Cancer of pancreas (157) . . . . . . . . . . . . . . . . . . . . 459 256 1.79 170 145 1.17Cancer of larynx (161) . . . . . . . . . . . . . . . . . . . . . . . 94 8 11.49 22 5 4.78Cancer of lung and bronchus
(162.1, 162.8, 163) . . . . . . . . . . . . . . . . . . . . . . . . . 2,609 231 11.28 517 130 3.97Cancer of bladder and other urinary
organs (181) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 326 151 2.16 126 90 1.41All other cancers . . . . . . . . . . . . . . . . . . . . . . . . . . . 4,010 2,916 1.38 1,957 1,642 1.19
aonly ex.cigarette Smokers who stopped smoking cigarettes for reasons other than physicians’ orders.% + E values are based on expected numbers to two decimal places.cvalues d. not exactly total due to rounding.
SOURCE Rogot and Murray (312)

.
72 . Technologies for Determining Cancer Risks From the Environment
from such exposure has been documented.Hirayama (167) reported an approximately two-fold increased risk of developing lung canceramong nonsmoking wives of cigarette smokers.The effects may even be greater; a fourfold ex-cess was estimated by Doll and Peto (93), whoconsidered lifelong exposure, as would be thecase with children.
A more precise estimate of the proportion ofcancer associated with tobacco smoking re-quires a more exhaustive study of lung cancer.Such an effort might be desirable because of theimportance of lung cancer to overall cancerrates. As American lung cancer death rates con-tinue to rise, the estimate of the percentage ofcancer deaths caused by tobacco will likewiseincrease. The future course of lung cancer ratesdepends largely on patterns of cigarette con-sumption and possibly on changes in tar andnicotine yields. The latter point may be par-ticularly important in light of the large numbersof smokers who have switched to lower tar andnicotine cigarettes.
There is some evidence to indicate that low-tar/nicotine cigarettes may have a lesser car-cinogenic risk (6,153,157,287). The tar and nic-otine yield is believed to be a function both ofthe tar/nicotine content of the tobacco and thenumber of puffs taken (202). Therefore, a reduc-ed risk is dependent on the smoker’s behavior aswell as the cigarette itself. The decreased riskfrom a “less hazardous” cigarette may besomewhat offset by an increase in the number ofcigarettes smoked. Reports indicate that withthe increased production of low-tar/nicotinecigarettes, there has been an increase in thenumber of cigarettes consumed per currentsmoker (286). It is also unknown whetherchemicals newly added to cigarettes andchanges in the composition of the gaseous phasewill have health consequences.
The extent to which the increase in male andfemale lung cancer rates over the last few dec-ades can be accounted for by tobacco is de-bated. Doll and Peto (93) argue that the increasewithin the last century can almost totally be ex-plained by cigarette smoking, while others,
Schneiderman (321) and the Toxic SubstancesStrategy Committee (345) included, contendthat additional factors are responsible. (For amore complete discussion, see ch. 2.)
Examination of cigarette-consumption pat-terns in this country leads to speculations aboutfuture cancer statistics at tobacco-related sites.The proportion of adult men smoking cigaretteshas declined from 51 to 37 percent during theperiod 1965 to 1978 (287). There has also been aslowdown in the rate of initiation of smokingamong adolescent males. The decreases began atthe time of release of the first Surgeon General’sreport in 1964, and the widespread discussion ofthe dangers of smoking that followed (287).This information demonstrates that worthwhiledecreases in cigarette consumption can takeplace even without radical Government inter-vention, chiefly by increasing public awarenessof the hazards of smoking. The proportion ofadult women who smoke remained virtuallyconstant at around 32 percent between 1965 and1976, and has since started declining slightly.Unfortunately, the rate of smoking initiationamong young women has not declined (287).
Changes in smoking habits that should lowerrisks are believed to have already influencedlung cancer rates. The rate of increase in lungcancer among men under 65 years of age hasslowed during the last decade (see table 8 andfig. 10). Recent female mortality statistics arealso promising, for they indicate that femalelung cancer rates in the 30- to 4&year age groupare steady or decreasing. There is reason tohope that with continued reductions in exposureto the harmful components of cigarettes, the de-creases will follow through to older age groups.
Public health laws exclude tobacco from reg-ulatory action because smoking tobacco isviewed as a personal decision, and one in whichCongress has decided not to intervene. TheGovernment limits its responsibility to inform-ing smokers and potential smokers of thehazards of cigarettes, conducting behavioralstudies on ways of affecting smoking habits,and supporting research on low-tar/nicotinecigarettes.

Ch. 3—Factors Associated With Cancer ● 73
ALCOHOL
Alcohol is considered next because of the in-teraction between tobacco smoking and alcohol-related cancers. The National Institute on Alco-hol Abuse and Alcoholism (NIAAA) (257) esti-mated that approximately one-third of adultAmericans drink alcoholic beverages at leastonce a week and another third do not drink soregularly but drink primarily on special occa-sions. In addition, NIAAA estimated that thereare 9.3 to 10 million “problem drinkers, ” in-cluding alcoholics, in the adult population.Alcohol consumption is influenced by numerouspersonal characteristics including sex, age,education, socioeconomic status, occupation,residence, ethnicity, and religious affiliation.
Alcohol’s association with cancer was firstsuspected around the turn of the century. To-day, as is the case with tobacco, there is in-disputable evidence that alcohol consumptionincreases the risk of developing cancer atvarious body sites. The 1978 Department ofHealth, Education, and Welfare (DHEW) re-port, Alcohol and Health (257), states:
In comparison to the general population,heavy consumers of alcohol always show amarked excess of mortality from cancers of themouth and pharynx, larynx, esophagus, liver,and lung. In the United States, these cancersrange from 6.1 to 27.9 percent of the total in-cidence of all cancer recorded in those locationswhere there are cancer registries.
Epidemiologic studies have demonstrated thatcancers are more common in men employed intrades that encourage the consumption of largeamounts of alcohol. A recent study showed thatDanish brewery workers have a higher risk ofdeveloping cancer then the general population(193). Clinical evidence suggests that con-sumption of alcohol at levels sufficient to causecirrhosis of the liver also increases the incidenceof liver cancer (257).
Researchers have tried to determine whetherthe association between alcoholic drink andcancer is due to the alcohol itself or to otherchemicals found in spirits, wines, and beers(348). Pure grain alcohol (ethanol) has not been
shown to be carcinogenic in animal bioassays(93,277); however, both pure ethanol and meth-anol, a contaminant of many alcoholic bever-ages, are mutagenic in bacteria (160,277). Addi-tionally, many alcoholic drinks are found to bemutagenic. The resuIts from such experimentsdo not yet lead to firm conclusions, but it maybe that components of alcoholic beverages aswell as alcohol itself are related to increasedcancer risk. Some evidence suggests that the riskof cancer is greatest when alcohol is consumedas spirits and that the apple-based drinks con-sumed in Northwest France are particularlyharmful (93). However, the carcinogenic effectof alcoholic beverages is largely independent ofthe form in which it is drunk. In addition to adirect effect, alcohol may also exert a carcino-genic effect by facilitating contact between ex-trinsic carcinogenic chemicals and the contentsof the stem cells that line the upper digestivetract and larynx.
Epidemiologic evidence supports the viewthat excessive alcohol consumption increasesthe risk of developing cancers of the mouth (ex-cluding lip), larynx, and esophagus and thatalcohol acts additively and even synergisticallywith tobacco in the pathogenesis of cancers ofthe upper digestive tract (257,367).
Most estimates of the percentage of cancerassociated with alcohol fall in the 3- to 5-percentrange. From data presented by Schottenfeld(233), alcohol appears to be associated with 4 to5 percent of 1978 U.S. cancer deaths; Wynderand Gori (368) estimated 4 percent male and 1percent female 1976 U.S. cancer incidence; andHigginson and Muir (166) estimated 5 percentmale and 3 percent female 1968–1972 cancers inthe Birmingham and West Midland region ofEngland.
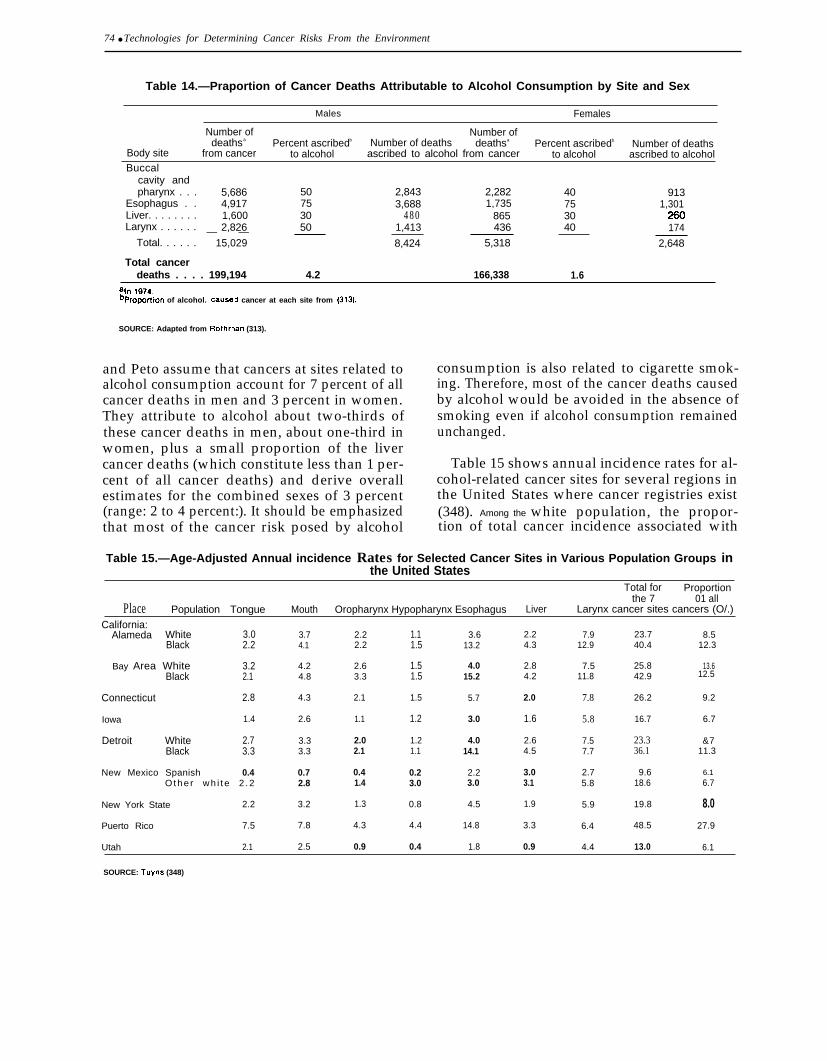
Rothman (313) (see table 14) and Doll and
Peto (93) estimated that 3 percent of U.S. cancermortality is related to alcohol. Rothman’scalculations are based on attributing a propor-tion of 1974 cancer deaths at each alcohol-related body site to alcohol consumption. Doll
!30-4’31 o - 81 - 6
74 ● Technologies for Determining Cancer Risks From the Environment
Table 14.—Praportion of Cancer Deaths Attributable to Alcohol Consumption by Site and Sex
Males Females
Number of Number ofdeathsa Percent ascribedb Number of deaths deathsa Percent ascribedb Number of deaths
Body site from cancer to alcohol ascribed to alcohol from cancer to alcohol ascribed to alcoholBuccal
cavity andpharynx . . . 5,686 50 2,843 2,282 40 913
Esophagus . . 4,917 75 3,688 1,735 75 1,301Liver. . . . . . . . 1,600 30 480 865 30Larynx . . . . . . 2,826 50 1,413 436 40 174— —
Total. . . . . . 15,029 8,424 5,318 2,648
Total cancerdeaths . . . . 199,194 4.2 166,338 1.6
aln 1974.bpropo~lon of alcohol. cause~ cancer at each site from (313).
SOURCE: Adapted from Rothman (313).
and Peto assume that cancers at sites related toalcohol consumption account for 7 percent of allcancer deaths in men and 3 percent in women.They attribute to alcohol about two-thirds ofthese cancer deaths in men, about one-third inwomen, plus a small proportion of the livercancer deaths (which constitute less than 1 per-cent of all cancer deaths) and derive overallestimates for the combined sexes of 3 percent(range: 2 to 4 percent:). It should be emphasizedthat most of the cancer risk posed by alcohol
consumption is also related to cigarette smok-ing. Therefore, most of the cancer deaths causedby alcohol would be avoided in the absence ofsmoking even if alcohol consumption remainedunchanged.
Table 15 shows annual incidence rates for al-cohol-related cancer sites for several regions inthe United States where cancer registries exist(348). Among the white population, the propor-tion of total cancer incidence associated with
Table 15.—Age-Adjusted Annual incidence Rates for Selected Cancer Sites in Various Population Groups inthe United States
Total for Proportionthe 7 01 all
Place Population Tongue Mouth Oropharynx Hypopharynx Esophagus Liver Larynx cancer sites cancers (O/.)
California:Alameda White 3.0
Black 2.23.6
13.23.74.1
2.22.2
1.11.5
2.24.3
7.912.9
23.740.4
8.512.3
13.612.5
Bay Area White 3.2Black 2.1
4.24.8
2.63.3
2.1
1.51.5
4.015.2
2.84.2
7.511.8
25.842.9
Connecticut 2.8 4.3 1.5 5.7 2.0 7.8 26.2 9.2
Iowa 1.4 2.6 1.1 1.2 3.0 1.6 5.8 16.7 6.7
Detroit White 2.7Black 3.3
3.33.3
2.02.1
1.21.1
4.014.1
2.64.5
7.57.7
23.336.1
&711.3
New Mexico Spanish 0.4Othe r wh i t e 2 .2
0.72.8
0.41.4
0.23.0
2.23.0
3.03.1
2.75.8
9.618.6
6.16.7
New York State 2.2 3.2 1.3 0.8 4.5 1.9 5.9 19.8 8.0
Puerto Rico 7.5 7.8 4.3 4.4 14.8 3.3
0.9
6.4 48.5 27.9
Utah 2.1 2.5 0.9 0.4 1.8 4.4 13.0 6.1
SOURCE: Tuyns (348)
Ch. 3—Factors Associated With Cancer ● 75
alcohol varies from 6.1 to 9.1 percent butreaches 11.3 to 12.5 percent among blacks. Thehighest proportion, 27.9 percent, is foundamong people living in Puerto Rico. It should benoted that these data refer only to those cancersfor which an obvious association with alcoholconsumption has been demonstrated.
Estimating the proportion of cancer at-tributable to alcohol alone is hindered by thedifficulty of obtaining accurate data on theamount of alcohol consumed. Results of studiesmust also be interpreted with caution in view ofthe fact that individuals who do not drink areoften distinguished by behavioral characteristicsvery different from those seen in drinkers, manyof which may affect cancer incidence.
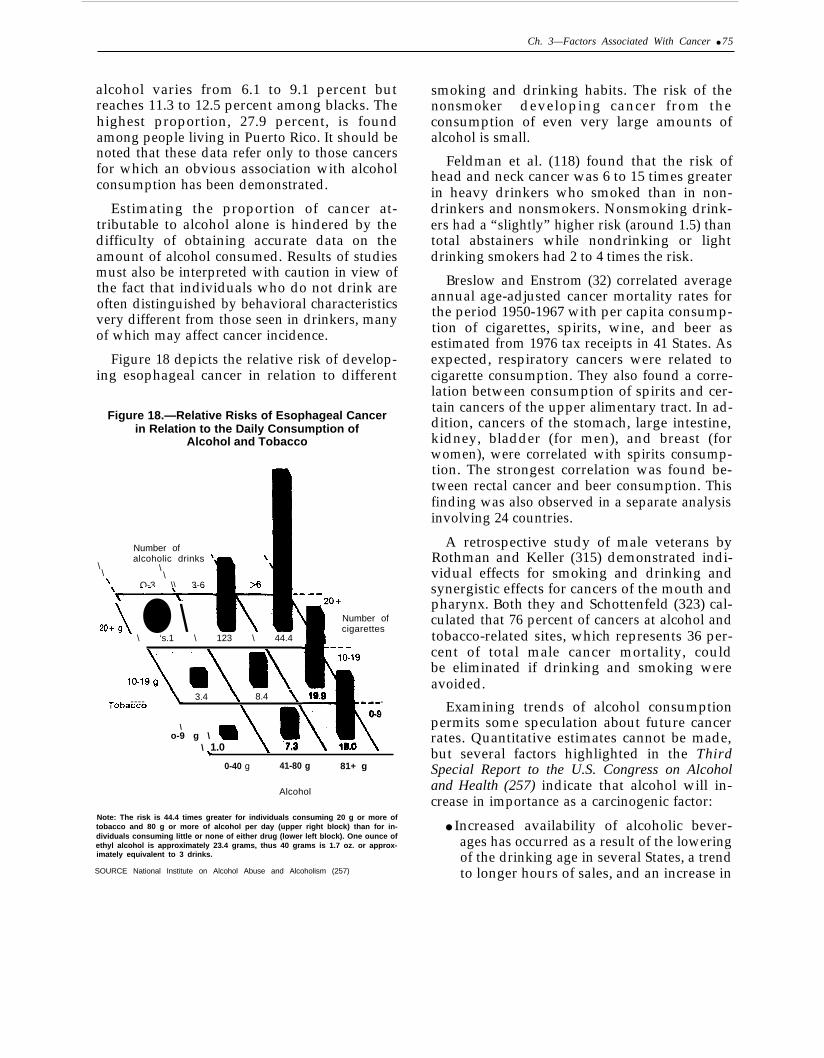
Figure 18 depicts the relative risk of develop-ing esophageal cancer in relation to different
Figure 18.—Relative Risks of Esophageal Cancerin Relation to the Daily Consumption of
Alcohol and Tobacco
Number ofalcoholic drinks ‘~ \
\\ \
\\ O-3 \\ 3-6‘~
20+A ● \\ ‘s.1 \ 123 \ 44.4
\Number ofcigarettes
---10-19
3.4 8.4 19.9*.L ---- 1
10-k 9/ Ii\I uoa~~v
\
%
- - -
\u\
0-9
m\ 1.0 7.3 tao
o-9 g \ ‘
\ .0-40 g 41-80 g 81+ g
Alcohol
Note: The risk is 44.4 times greater for individuals consuming 20 g or more oftobacco and 80 g or more of alcohol per day (upper right block) than for in-dividuals consuming little or none of either drug (lower left block). One ounce ofethyl alcohol is approximately 23.4 grams, thus 40 grams is 1.7 oz. or approx-imately equivalent to 3 drinks.
SOURCE National Institute on Alcohol Abuse and Alcoholism (257)
smoking and drinking habits. The risk of thenonsmoker developing cancer from theconsumption of even very large amounts ofalcohol is small.
Feldman et al. (118) found that the risk ofhead and neck cancer was 6 to 15 times greaterin heavy drinkers who smoked than in non-drinkers and nonsmokers. Nonsmoking drink-ers had a “slightly” higher risk (around 1.5) thantotal abstainers while nondrinking or lightdrinking smokers had 2 to 4 times the risk.
Breslow and Enstrom (32) correlated averageannual age-adjusted cancer mortality rates forthe period 1950-1967 with per capita consump-tion of cigarettes, spirits, wine, and beer asestimated from 1976 tax receipts in 41 States. Asexpected, respiratory cancers were related tocigarette consumption. They also found a corre-lation between consumption of spirits and cer-tain cancers of the upper alimentary tract. In ad-dition, cancers of the stomach, large intestine,kidney, bladder (for men), and breast (forwomen), were correlated with spirits consump-tion. The strongest correlation was found be-tween rectal cancer and beer consumption. Thisfinding was also observed in a separate analysisinvolving 24 countries.
A retrospective study of male veterans byRothman and Keller (315) demonstrated indi-vidual effects for smoking and drinking andsynergistic effects for cancers of the mouth andpharynx. Both they and Schottenfeld (323) cal-culated that 76 percent of cancers at alcohol andtobacco-related sites, which represents 36 per-cent of total male cancer mortality, couldbe eliminated if drinking and smoking wereavoided.
Examining trends of alcohol consumptionpermits some speculation about future cancerrates. Quantitative estimates cannot be made,but several factors highlighted in the ThirdSpecial Report to the U.S. Congress on Alcoholand Health (257) indicate that alcohol will in-crease in importance as a carcinogenic factor:
● Increased availability of alcoholic bever-ages has occurred as a result of the loweringof the drinking age in several States, a trendto longer hours of sales, and an increase in

76 ● Technologies for Determining Cancer Risks From the Environment
●
●
●
the number of retail outlets. (Recently, sev-eral States have raised drinking ages. )Around 1960, total per capita sales of ab-solute ethanol began to rise significantlyregistering a 30-percent gain between 1961and 1971. Since 1971, there has been vir-tually no change in per capita sales. The ef-fect of the overall increase may not yethave fully manifested itself in cancer rates.There is particular concern over increasedalcohol consumption in youths. This isheightened by the observation that earlydrinking behavior predicts drinking habitsin later life.The proportion of high school studentswho reported ever having been drunk in-creased dramatically from 19 percentbefore 1966 to 4.5 percent between 1966 and1975. The proportion reporting being in-toxicated at least once a month rose from
DIET
Introduction
Studying the relationship of diet and health isa continued source of frustration and excite-ment. Food affects all body functions and comesinto direct contact with the digestive system andindirect contact with all other organs. Cancerrates for digestive sites vary considerablyaround the world and have prompted studies ofdiet’s role in cancer causation.
As discussed here, diet encompasses thoseitems ingested as food, including substancesadded to food, those produced during normalcooking, storage, and digestion, but excludingdrinking water and alcohol (discussed in thischapter under Air and Water Pollution a n dAlcohol, respectively).
The amounts and balance of the major com-ponents of diet are generally believed to beresponsible for the lion’s share of diet-relatedcancers. Deficiencies or excesses of micro-elements, and the presence of additives or con-taminants, are probably less important. Thevarious means by which diet may influence the
10 percent before 1966 to 19 percent be-tween 1966 and 1975.
The importance of alcohol as a health hazardis not limited to its association with a relativelysmall percentage of cancer. Estimates of the an-nual number of deaths related to alcohol rangefrom 37,000 to 205,000. Cirrhosis of the liver,the seventh leading cause of death in the UnitedStates, was responsible for 30,066 deaths in1978. As an contributory cause of homicides,suicides, and accidents, alcohol’s toll is evengreater. The Institute of Medicine (178) recentlycompleted a study of alcoholism and relatedproblems and indicated several opportunitiesfor research. These included further research onalcohol metabolism, development of appro-priate animal models, and further effortsthrough epidemiologic studies to explore thelink between alcohol and its adverse health con-sequences.
development of cancer are listed in table 16.Diet also plays a role in the treatment of cancerillustrating the pervasive role of diet withrespect to all aspects of the disease.
Unfortunately, dietary studies are plaguedwith methodological problems and conflictingevidence exists for almost every specific ques-tion that has been investigated. The overallassociation of cancer with diet exists but there isno reliable indication of exactly what dietarychanges would be of major importance in reduc-ing cancer incidence and mortality.
The strongest positive associations identifiedthrough correlations of dietary patterns andcancer rates are those between total fat intake,particularly animal fat consumption and can-cers of the breast and endometrium; and be-tween total protein intake and cancer of the co-lon. The most dramatic change observed in adiet-related cancer site has been the reduction inincidence and mortality from stomach cancer.In the United States, the 1950 age-adjustedmortality rate from stomach cancer was 24.4/100,000 for males and 13.1/100,000 for females

Ch. 3—Factors Associated With Cancer ● 77
Table 16.—Some Currently Attractive Hypothetical or Actual Waysin Which Diet May Affect the Incidence of Cancer
Possible ways or means Example a
Ingest ion of powerful, direct-acting carcinogens or t heir Carcinogens in natural foodstuffs (plant products)precursors Carcinogens produced in cooking
Carcinogens produced in stored food by microorganisms(bacterial and fungal)
Affecting the formation of carcinogens in t he body Providing substrates for the formation of carcinogens in thebody (e.g., nit rites, nitrates, secondary amines)
Altering intake or excretion of cholesterol and bile acids (andhence the production of carcinogenic metabolizes in thebowel)
Altering the bacterial flora of the bowel (and hence the capaci-ty to form carcinogenic metabolizes)
Affecting transport, activation, or deactivationof carcinogens
Altering concentration in, or duration of contract with, fecesAltering transport of carcinogens to stem cellsInduction or inhibition of enzymes (which affect carcinogenmetabolism or catabolism)
Deactivation, or prevention of formation, of short-lived in-tracellular species (e.g., by use of selenium, vitamin E, orotherwise trapping free radicals; by use of b-carotene orotherwise quenching singlet oxygen; by use of other antiox-idant)
Affecting “promotion” of cells (that are alreadyinitiated) b
Vitamin A deficiency (clinical or subclinical)Retinol [Binding Protein] (hormonal and other factors deter-
mine blood RBP, though vitamin A intake may not affect itmuch)
Otherwise affecting stemcell differentiation (carotenoids?determinants of lipid “profile”?)
Overnutrition Age at menarcheAdipose-t issue-derived estrogensOther effects
aThere may be considerable overlap between many of the efltrleS In this tablebor, more ~enerally, affecting the ~robablllty that a partially transformed stem cell will become fully transformed and Will proliferate successfully Into Cancer
SOURCE Doll and Peto (93)
while in 1977 the rate was 8.8/100,000 for malesand 4.0/100,000 for females. This decrease hasoccurred in many other countries, includingthose with high initial rates, such as Japan andIceland, and those with lower initial rates, suchas Canada and New Zealand. The factors be-lieved to have contributed to these decreases in-clude: reduction in use of salt and pickling,lower consumption of smoked foods, and in-creased use of refrigeration, increased con-sumption of milk, green vegetables, fruit, andantioxidants (237).
In general, as a result of increased intake ofcalories, proteins, and certain other nutrients,Americans have been growing taller and reach-ing sexual maturation earlier. A great improve-ment in the Nation’s health has resulted fromthis change, but increased risk for certain cancersites may accompany the improvement. For ex-
ample, earlier sexual maturation in women isassociated with higher risk of breast cancer laterin life, though as yet, no increases in breastcancer has been attributed directly to improvednutrition (see Sexual Development, Reproduc-tive Patterns, and Sexual Practices for a morecomplete discussion of this topic).
Many estimates of the importance of diet tocancer have been put forth. Doll and Peto (93)estimated that altering dietary practices mayreduce cancer by as much as 35 percent (stom-ach and large bowel cancer by 90 percent; en-dometrium, gallbladder, pancreas, and breastby 50 percent; lung, larynx, bladder, cervix,mouth, pharynx, and esophagus by 20 percent;others by 10 percent). The great uncertainty ofthis estimate is indicated by the range of 10 to 70percent which they attach to their estimate.Wynder and Gori (368) estimate, by calculating

78 ● Technologies for Determining Cancer Risks From the Environment
the percent difference between U.S. mortalityrates and the lowest rates reported worldwideand by considering specific case-control studies,that an even larger proportion of cancer, ap-proximately 40 percent in males and 60 percentin females, could be attributable to diet.
In testimony before the Subcommittee onNutrition of the Senate Committee on Agri-culture, Nutrition, and Forestry, Dr. ArthurUpton (353), then-Director of the National Can-cer Institute (NCI), succinctly discussed the ex-tent of involvement of diet and cancer when hestated:
Despite the impression that cancers are linked withdietary patterns and the inability to pinpoint specificdietary carcinogens, scientists generally agree thatfactors in diet and nutrition-including drinkingwater contaminants—appear to be related to a largenumber of human cancers, perhaps approaching 50percent.
Dietary Intake
Fat/Meat Intake
Examination of cancer rates in different coun-tries show positive correlations between coloncancer and consumption of meat and animalprotein and between cancer of the breast and en-dometrium with total fat consumption (17).These cancers are common in the United States,Canada, and Western Europe and rarerthroughout the developing world.
The most widely held theory is that fat in thediet has a promotional effect on the devel-opment of cancer. One suggested mechanism isthat fats affect hormone levels. Several cancers,including breast, ovarian, and endometrial are,in turn, influenced by hormones. This associa-tion of dietary fat with higher cancer rates is,however, not found uniformly. Breast and col-orectal cancers are not uncommon among vege-tarians, and the observed incidence in SeventhDay Adventists who are largely vegetarian, ismatched by the same incidence in Mormonswho eat meat (293). This finding and the factthat meat intake among Mormons is not mark-edly lower than among the general population isoften cited as a rebuttal to the meat/fat cancercausation hypothesis. These interpretations
should be viewed cautiously for the studies maynot have been adequate to reflect any promo-tional effect in these low risk groups who areless exposed to many other types of carcino-genic stimuli, such as, cigarettes and alcohol,than is the general population. Additionalstudies in this area are needed.
More and more, studies have focused onspecific types of fat. Evidence suggests that dietswith a high ratio of polyunsaturated fats (main-ly of vegetable origin) to saturated fats (mainlyof animal origin) may increase the risk of can-cer. Paradoxically, this type of diet is recom-mended to lower the risk of heart disease. Re-sults from epidemiological studies (98,290) andanimal trials (53,305) have been inconsistentand confusing, and have shown different effectson different cancer sites. In rats, polyun-saturated fats need be only a small proportionof a total high fat intake to promote breasttumor incidence. If the animal model is ap-plicable to humans, virtually all high-fat dietswill exert a promotional effect (52).
Serum cholesterol has been investigated inmany studies as a risk factor for variouscancers. Serum levels are directly affected by in-take of cholesterol and fat. A diet with a lowsaturated fat to polyunsaturated fat ratiodecreases the amount of ingested cholesterolthat will appear in the serum. The discoverythat the stools of colorectal cancer patients con-tain an abnormally high proportion of acidsteroids, derived from bile salts, and cho-lesterol, supports the hypothesis that certaintypes of fat play a role in the production of col-orectal cancer.
A recent epidemiologic study found an asso-ciation between high-density lipoproteins andcancer risk (199). On the other hand, in a pro-spective epidemiologic study of heart disease inFramingham, Mass., serum cholesterol levelswere inversely associated with the incidence ofcolon cancer and other sites in men. Men withthe lowest serum cholesterol levels experienceda colon cancer rate which was three times higherthan men with the higher cholesterol levels(361). A similar negative association was re-ported in data from the Paris Prospective Studyof Coronary Heart Disease (45).

Ch. 3—Factors Associated With Cancer ● 79
The hypothesis that dietary cholesterol playsa direct role in the production of colon cancer issupported by some animal studies. For instance,the addition of cholesterol to the diet of rats on acholesterol-free liquid diet, had a promotionaleffect and cholesterol enhanced the carcinogeniceffect of a known carcinogen (1,2 dimethyl-hydrazine).
Fiber Intake
Burkitt (40) observed that several intestinaldiseases that are common in developed coun-tries are rare in rural Africa where unprocessedfood is consumed, and the stools tend to be soft,bulky, and frequent. It is suggested that dietaryfiber may reduce colorectal cancer by decreas-ing the time stools remain in the bowel, by in-creasing bulk (thereby decreasing the concentra-tion of carcinogens in stool), or by perhapsaltering the distribution of bacteria, some ofwhich may produce or destroy carcinogenic me-tabolizes.
The effects of fiber on cancer incidence haveattracted much interest but remain problemati-cal. As in the case of fats, dietary fiber is a termwhich covers a multitude of different sub-stances, each of which may have different influ-ences on carcinogenesis. The methods by whichtypes of fiber are chemically characterized arestill in a primitive state, and analyses of thecomposition of dietary fiber in many foods islacking. Despite the drawbacks, some associa-tions have emerged. A close inverse correlationhas been found between the pentose fiber con-tent of the diet and mortality from colon cancerin part of the United Kingdom (93). No correla-tion was shown with any other fiber types, orwith dietary fiber as a whole.
Elements and Vitamins
Several metals and vitamins are linked withcancer development. They can either act as car-cinogens themselves or they may biologicallycompete with other dietary constituents toenhance or suppress a cancerous response.
An iron-deficient syndrome was shown to beassociated with a high risk of developing can-cers of the pharyngeal and esophageal mucosa
in northern Scandinavia. The incidence ofgastric cancer is found to be 4 to 5 times higherin countries where iron deficiency is prevalentthan in the United States (356).
Selenium, an effective antioxidant, is oftenfound at higher levels in plants, milk, or humanblood in sections of the United States with lowcancer rates. Selenium deficiency in rats con-sistently increases the carcinogenic effect ofknown chemical carcinogens, particularly inanimals fed on high polyunsaturated fat diets(190). Supplementation with selenium abovedietary requirements decreases tumor yield inanimals on both low- and high-polyunsaturatedfat diets (188).
Stocks and Davies (24) found that a high zinc-copper ratio in soils was associated withelevated rates of human stomach cancer whileStrain et al. (24) reported an association ofelevated cancer rates with low zinc-copperratios. Marginal zinc deficiency is associatedwith increased esophageal cancer in animals(122) and esophageal cancer patients had lowerlevels of zinc in their blood, hair, and tumortissue than controls in a study of Chinese men(211). Zinc deficiency may interact synergisti-cally with alcohol to enhance esophageal car-cinogenesis (135).
The overall relationship between cancer andvitamins is not well understood. Vitamin C hasbeen shown to reduce carcinogen formation inexperimental animals (359), and this activitymay be important in reducing cancer occur-rence. Vitamin A (retinol) has been more ex-haustively studied than any other vitamin (forreview see 292) and it has been suggested thatvitamin A, or, more particularly, its vegetableprecursor, beta-carotene, may decrease the sus-ceptibility of a variety of epithelial tissues to thedevelopment of cancer. Retinol (or its analogsretinoic acid and various retinoids) has beenrepeatedly demonstrated to diminish the risk ofexperimentally induced cancer in laboratoryanimals (93). These results are particularly in-triguing because the protective effect is observedeven when these substances are fed long afterthe animal is treated with an initiating car-cinogen, and the vitamin and its analogs appearto be effective at a wide variety of sites.

80 ● Technologies for Determining Cancer Risks From the Environment
People with a history of consuming aboveaverage amounts of provitamin A (beta-caro-tene) have a slightly lower incidence of severaldifferent types of cancer than people who give ahistory of consuming less. Beta-carotene isfound in carrots, green leafy vegetables and inred palm oil which is used for cooking in manytropical countries. Further epidemiologic studiesare now in progress in areas where red palm oilis habitually used. The role of beta-carotene incancer prevention is still uncertain and this par-ticular hypothesis has been mentioned to illus-trate the potential importance of diet.
Local deficiency of folate (a B-complex vita-min) has been demonstrated in the abnormalcervical tissue of some women taking oral con-traceptives. The observed abnormalities areoften precursors of cervical cancer. Supplemen-tation with folic acid in these women can re-verse the abnormality and appears to preventprogression to carcinoma (41). Deficiencies oflipotropes (choline, methionine, and folic acid)increased the susceptibility of animals to avariety of environment carcinogens in severalstudies (311).
Dietary Balance
Studies in laboratory animals have shownthat altering gross aspects of diet can have sub-stantial impact on the risk of an animal de-veloping cancer. Jose (195) reviewed several re-ports which demonstrate that restricting calorieintake without modifying the proportion of theindividual constituents reduces the incidence ofspontaneous tumors and of a variety of cancersproduced by exposure to known carcinogens.Not only did calorie restriction result in de-creased incidence of tumors, but it also delayedthe time of appearance of tumors, and whentumors appeared, they grew and metastasizedmore slowly. The life spans of animals onrestricted diets were often increased up to 50percent compared to normally fed controls.However, decreased calorie intake, when ac-companied by inadequate protein intake makeslaboratory animals more susceptible to manyenvironmental carcinogens (47).
A suspected association between obesity andthe risk of cancer was strengthened in an epi-
demiologic study conducted by ACS which fol-lowed 750,000 people from 1959 to 1972 (207).Overall cancer mortality was found elevated forthose individuals who were more than 40 per-cent heavier than average. Mortality from can-cers of the colon and rectum were increasedamong men while mortality from cancers of thegallbladder and biliary passages, breast, cervix,endometrium, and ovary were increased amongwomen. The meaning to be attached to the re-sults is not entirely clear since weight is asso-ciated with a variety of social and behavioralcharacteristics that affect the risk of cancer inother ways, including smoking habits and socio-economic status. Another concern is that diag-nosing cancers may be more difficult in obeseindividuals, and cancers may generally be moreadvanced when they are detected.
In addition to the quantity and compositionof food, the timing of intake has also beenshown to be important. For example, Roe andTucker (cited in 93) randomized mice with ahigh spontaneous incidence of mammary tu-mors, between continuous feeding, in which themice were fed 6 g of food each day, which theyconsumed in frequent small amounts, and inter-mittent feeding, in which food was limited to 5 gper day which was eaten at once. No clear dif-ference in longevity was observed, but nonfatalspontaneous mammary tumors arose in 64 per-cent of the continuously fed mice and in only 8percent of those fed intermittently.
Immune function in both humans and ani-mals can be severely compromised by deficien-cies of certain dietary nutrients—in particular,protein, methionine, choline, folate, vitaminB12, vitamin A, zinc, and pyridoxine (147). Defi-ciencies in certain of these nutrients, with a con-comitant depression of immune system functionhave been demonstrated in animals and are sus-pected of increasing the susceptibility of de-veloping certain cancers (356).
Naturally Occurring Carcinogensand Precursors
Along with the major components, thousandsof chemical substances occur in small quantitiesin foods. Most naturally occurring carcinogens

Ch. 3—Factors Associated With Cancer ● 81
and mutagens are of plant origin, but an impor-tant class, nitrates and nitrites, occurs in bothplants and animals.
Nitrates and Nitrites
Nitrate and nitrite salts naturally occur invegetables, fish, and meat, are added to food fortheir preservative properties (see Additives p.82), and are present in pesticide and drugresidues in food (127). They react with otherchemicals in the body to produce N-nitro-samines and N-nitrosamides. N-nitrosaminesare among the most powerful chemical car-cinogens in laboratory animals, producing tu-mors at a variety of sites including liver, kidney,lungs, esophagus, bladder, pancreas, trachea,nasal cavities, and peripheral nervous system(221). Experimentally, vitamin C has beenshown to inhibit the formation of nitrosamines(359).
Epidemiological evidence linking nitrites andnitrates to cancer is fragmentary. Evidence for arelationship between gastric cancer and the ni-trite content of the diet is not wholly consistent.It is notable that vegetables, which are usuallythe main source of dietary nitrates, appear toprotect against the development of the disease,possibly because of their vitamin C content (93).On present knowledge, the possible contribu-tion of dietary nitrates and secondary amines tothe production of cancer is uncertain.
Other Substances
Cycasin in the cycad nut, safrole in sassafras,pyrrolizidine alkaloids in some plants, and ex-tracts of coltsfoot and bracken fern are a fewnaturally occurring compounds which exhibitcarcinogenic properties in animals. Onlybracken fern has been demonstrated to causecancer in man. Bracken fern is commonly eatenin Japan, and Japanese who eat it daily havethree times the risk of developing cancer of theesophagus as Japanese who do not eat it at all(93). It has been postulated that the high bowelcancer rates in Scotland may be due to the inges-tion of cattle fed on bracken fern or the leachingof the carcinogenic components into water orfood (24). Range-fed cattle and sheep may pass
pyrrolizidine alkaloids along to humans in theirmeat and milk (215).
Certain plant-derived preparations are asso-ciated with cancer. Extracts of some plants usedto make herbal infusions, for use as home rem-edies, tonics or beverages, are carcinogenic inanimals, and their tannin-containing fractionsare particularly active. Some population groupswho use these products have high rates ofesophageal cancer, suggesting an association(297). Perhaps of greater concern, because of itswidespread use, coffee has been associated withhuman bladder (24) and pancreatic cancer (220),but whether the associations are causal is notyet known. Studies in animal cell cultures haveshown caffeine, a constituent of both coffee andtea, to potentate the effect of carcinogenicsubstances (96).
Mutagenic substances have also been iden-tified in cruciferous plants (cabbage, broccoli,etc.), from cereal grains, and some grazingrange plants in the Southwestern United States(MacGregor, 1980). Other not-yet-identifiedcarcinogens and mutagens may occur naturallyin food, but on present evidence, naturally oc-curring carcinogens are not regarded as an im-portant cause of cancer in the United States (93).
Carcinogens and Precursors Producedby Cooking
Another possible source of carcinogens istheir production in cooking. Humans are the on-ly animals that cook their food, and it has beenknown for many years that carcinogenic chem-icals such as benzo(a)pyrene (B(a)P) and otherpolycyclic hydrocarbons are produced whenmeat or fish is broiled or smoked or when foodis fried in fat which has been used repeatedly,Sugimura et al. (336) demonstrated that broilingalso produces powerful mutagens that cannot beaccounted for by the production of B(a)P alone.Few people eat more broiled foods than Ameri-cans and while the declining stomach cancerrate provides some assurance that cancer at thatsite is not related to broiled food, the possibilityremains that colorectal cancer, which has notdecreased materially, might be related, Recent

evidence has shown that mutagens can in fact beproduced by cooking at relatively low tempera-tures (100-200C) (93).
Contaminants
Natural Contaminants
A less obvious source of carcinogenic activityand one that was overlooked altogether until theearly 1960’s, is the production of carcinogens bymicro-organisms in stored food. Aflatoxin, aproduct of the fungus Aspergillus flavus, is themost powerful liver carcinogen known for someanimal species. In addition, human liver cellscontain the enzymes necessary to produce themetabolic products that appear to be responsi-ble for its activity. l-here is evidence for believ-ing that aflatoxin is a major factor in the pro-duction of liver cancer in certain tropical coun-tries where it is a contaminant of carbohydratefoods, particularly grains and nuts. The in-cidence rates of primary liver cancer in differentparts of Africa are approximately proportionalto the amount of aflatoxin in the diet (212).
Liver cancer occurs more commonly in peoplewho are chronically infected with hepatitis Bvirus and it seems probable that where aflatoxinis present in the diet, both aflatoxin and hepa-titis B virus contribute to the risk of liver cancer,each multiplying the other’s effects.
In the United States, primary cancer of theliver is a rare disease accounting for less than 1percent of cancer deaths (2,796 deaths in 1978).The amount of aflatoxin in the American diet issmall and is only one among several other possi-ble causes of liver cancer. In the American con-text, the chief importance of the discovery of thedangers of aflatoxin is that it raises the possibili-ty that other as yet unrecognized mycotoxins infood may be carcinogenic. Recently, there hasbeen some evidence to suggest that a fungusmay contribute to the high incidence of esoph-ageal cancer in parts of China by increasing thenitrite content of contaminated food (209).
Environmental Contaminants
In late 1979, OTA (284) examined both reg-ulatory approaches and monitoring strategies
for coping with contaminated food. A widevariety of industrial products ranging fromheavy metals and pesticide residues, to sub-stances that leach out of packaging, such aspolyinyl chloride, can pollute food. Organiccompounds are felt to pose the greatest potentialfor environmental food contamination based onthe number, volume, and toxicity of organicsmanufactured in the United States.
Polycyclic aromatic hydrocarbons (PAH) arefound widely in all types of foods, sometimes atthe same level which can be present in charcoal-broiled meats and smoked ham, i.e., up to 15 ugB(a)P/kg net weight. Some shellfish and finfishfrom polluted waters have been reported to con-tain up to 1,000 ug B(a) P/kg. The importance ofingested B(a)P in cancer induction is uncertain.Epidemiologically, no relationship has been es-tablished, and when cancer is produced experi-mentally in laboratory animals, it either affectsan organ not represented in man or occurs by amechanism that does not appear relevant (93).
Some chlorinated hydrocarbons that wereused as pesticides (e.g., DDT, aldrin, dieldrin)produce liver tumors (hepatomas) in mice, andsome have been shown to be carcinogenic inother species. These compounds accumulate inhuman fat, but no increase in liver tumors ap-pears to have accompanied their introductionand use. However, the latent period is notknown, and the possibility exists that effectsmay be seen some years from now. Pesticideresidues in the form of secondary amines mayconstitute a hazard if the formation of nitros-amines in the stomach proves to be a cause ofcancer in man.
Many other chemicals fall into this categoryof environmental contaminants. The extent towhich these have contributed to the productionof human cancers is difficult to evaluate, butbelieved to be small (328).
Additives
Chemicals are used to preserve food and giveit color, flavor, and consistency. Food dyeswere among the first chemicals investigated be-cause of their structural similarities to acceptedchemical carcinogens (24). Consumption of

Ch. 3–Factors Associated With Cancer ● 83
chemicals by consumers who are unaware oftheir presence is partially responsible for thefood safety laws. The laws require that newlyintroduced direct food additives be carefullyscreened in the laboratory before they may beused.
Some definitely carcinogenic chemicals,which have now been withdrawn from foods,were used for a time before their carcinogenicityin animals was discovered. These include butteryellow, thiourea, and a food preservative usedin Japan. The number of cancers, if any, whichthese additives produced is unknown. Doll andPeto (93) estimated an attribution of less than 1percent of total cancer mortality to food ad-ditives.
Of the many food additives presently used inthe United States, three require special consider-ation: the artificial sweeteners cyclamates andsaccharin, butylated hydroxytoluene (BHT),and nitrites and nitrates.
Cyclamates were shown to produce bladdercancer in animals (24) and were removed fromcommerce in 1969. OTA (282) reviewed datathat show saccharin caused cancer of the blad-der in rats in two circumstances: 1) instraightforward feeding studies when given overtwo generations, and 2) when given followingthe administration of a powerful carcinogen.OTA also reported positive and negative resultsfrom a number of short-term tests. Therefore,some evidence supports the conclusion that sac-charin causes cancer in defined conditions. Thehuman evidence that has been collected over thelast few years fails to distinguish clearly be-tween saccharin and cyclamates, but it is morerelevant to the former as the use of saccharinbegan earlier (in 1902) and has continuedlonger. An increase in incidence or mortalityfrom bladder cancer could not be attributed tothe introduction of saccharin (16).
One epidemiologic study (175) showed thatingestion of artificial sweeteners by males in-creased their relative risk of bladder cancer to1.6. (The incidence of bladder cancer amongmen who did not consume saccharin was takenas relative risk equal to 1.0; saccharin users hada risk 60-percent higher). The results reported inthe study were consistent with those from the
laboratory. In both cases cancer occurred in thebladder in males.
Subsequent epidemiologic studies have failedto confirm the relative risk of 1,6. The largecase-control study of bladder cancer in theUnited States conducted by NCI revealed rel-ative risks of 0.99 for males and 1.01 for femalesamong users of artificial sweeteners in any form(174). However, Wilson (362) points out thatone projection from animal studies suggests thatonly about 500 bladder cancer cases annuallyare to be expected from saccharin consumptionin the United States (see also 282). The relativerisk represented by 500 cases could not havebeen detected in the case-control study.
Doll and Peto (93) reviewed five case-controlstudies which examined saccharin consumptionand bladder cancer. With the exception of Howeet al. (175), the relative risks in all the experi-
ments lie very close to 1.0; some slightly higher;some lower. They conclude that the “humanevidence could hardly be more null, ” at least forcancer of the bladder, which was the anatomicsite affected by saccharin in rats (93).
BHT has been used extensively as an antioxi-dant for many years. It is not carcinogenic byitself, but has been reported to enhance the pro-duction of lung tumors by urethan in mice (93).Conversely, its antioxidant effect is found to in-hibit the formation of active carcinogens in thelaboratory (93), and similar effects might be ex-pected to occur in vivo. It has been postulatedthat its use— and perhaps that of the more wide-ly used butylated hydroxyanisole—have con-tributed to the decline in mortality from stom-ach cancer (24).
Nitrites have been used to preserve meat sincethe last century (also see above). According toShubik (328), nitrites added to food Constitutesonly 10 percent of the total nitrite reaching thestomach in vegetables and saliva. However, ifthe formation of nitrosamines and nitrosamidesin the intestinal tract proves to be of practicalimportance, dietary nitrite may play a role incancer formation. The National Research Coun-cil’s Panel on Nitrates (cited in 93) was unable toreach any conclusions about their quantitativeeffect, but advised that reasonable measures be

taken to minimize human exposure to N-nitrosocompounds, including the restriction of theamounts of nitrate and nitrite added to meatproducts.
There is great uncertainty regarding the con-tribution of the compounds discussed above tothe formation of cancer. The possibility also ex-ists that other additives might have detrimentaleffects.
Diet Summary
Dietary components discussed above, andmany others, are currently the subjects of inten-sive research, from which some results shouldbe known within the next few years. The out-comes may show diet to be a factor in determin-ing cancer occurrence at many sites, particularlythe stomach, large bowel, endometrium, gall-bladder, and in tropical countries, the liver.Diet may also be shown to affect the incidence
OCCUPATIONAL EXPOSURES
The last several years have seen a heated dis-cussion concerning the contribution of occu-pational exposures to cancer in the UnitedStates. Since the formation of the OccupationalSafety and Health Administration (OSHA) in1970, 20 regulations have been promulgated andtwo more proposed relating to suspect carci-nogenic factors in the workplace. Labor unionsand public interest groups have criticized OSHAfor moving slowly, while industry and theirtrade associations claim unnecessary irrationalregulation and undue expense. In an effort toimplement a comprehensive and rational policyfor the regulation of carcinogens in the work-place, OSHA held 2 months of hearings in 1978which attracted the participation of laborunions, environmental groups and spawned amajor new trade association, the American In-dustrial Health Council (AIHC). Subsequently,OSHA promulgated “a general policy for theidentification and regulation of physical andchemical substances that pose a potential oc-cupational carcinogenic risk to humans”(278,279).
of cancers of the breast and pancreas, and,through the antipromoting effects of retinoids,to reduce incidence of epithelial cancers in manyother tissues. If these or other hypotheses areproven, practicable means of dietary modifica-tions may eventually be identified to reduce can-cer rates.
Cairns (43) draws attention to the probabledifficulty of changing cancer incidence even if adirect link is shown between a diet constituentand cancer incidence:
Cancer of the lung is due to a pleasant andhighly addictive habit, cancer of the large in-testine and breast are most common in affluentcountries and so are presumably associated withsome desirable habit, such as a diet high in ani-mal fats, that the rich nations can afford and theothers cannot . . . . These are signs, therefore,that the campaign to prevent cancer may comeinto some conflict with people’s immediatedesires.
The first recognized industrial cancer wasidentified by Percival Pott, a British surgeon,who observed that scrotal cancer occurred morefrequently in men who had been employed aschimney sweeps as boys. This led to the iden-tification of soot as the first chemical and oc-cupational carcinogen. In the ensuing years,many other groups of workers have been foundto suffer from occupationally induced cancer.For the purpose of this assessment, occupationalexposure is defined as exposure to a substanceor physical agent through any route during thecourse of employment.
The workplace setting has proved to be thesingle most productive source of information inthe discovery of carcinogenic substances. This isbecause of the defined populations involved andhigher exposures which can be more easilymonitored and identified. Table 17 lists carcino-gens and processes found in the workplacewhich are associated with increased cancer risk.Occupations known to produce an elevated riskof cancer, though the specific agents responsible
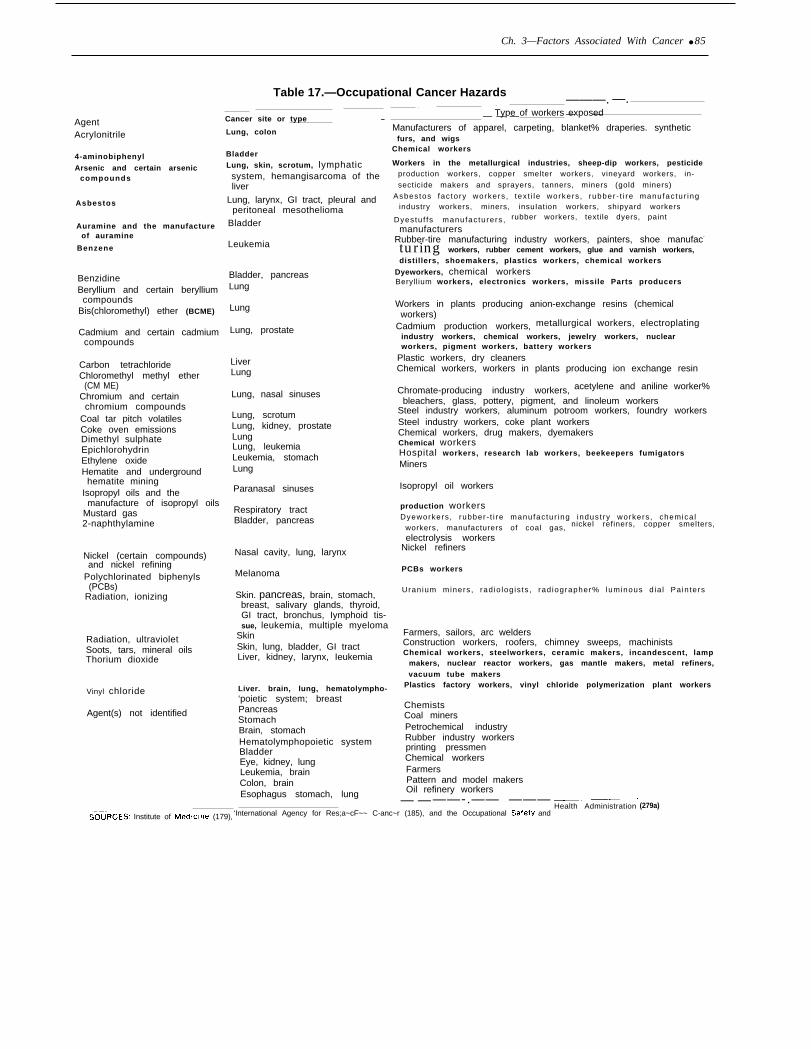
Ch. 3—Factors Associated With Cancer ● 85
Table 17.—Occupational Cancer Hazards
AgentAcrylonitrile
4-aminobiphenyl
Arsenic and certain arseniccompounds
Asbestos
Auramine and the manufactureof auramine
Benzene
BenzidineBeryllium and certain berylliumcompounds
Bis(chloromethyl) ether (BCME)
Cadmium and certain cadmiumcompounds
Carbon tetrachlorideChloromethyl methyl ether
(CM ME)Chromium and certain
chromium compoundsCoal tar pitch volatilesCoke oven emissionsDimethyl sulphateEpichlorohydrinEthylene oxideHematite and underground
hematite miningIsopropyl oils and themanufacture of isopropyl oils
Mustard gas2-naphthylamine
Nickel (certain compounds)and nickel refining
Polychlorinated biphenyls(PCBs)
Radiation, ionizing
Radiation, ultravioletSoots, tars, mineral oilsThorium dioxide
Vinyl chloride
Agent(s) not identified
Cancer site or type —
Lung, colon
BladderLung, skin, scrotum, lymphaticsystem, hemangisarcoma of theliver
Lung, larynx, GI tract, pleural andperitoneal mesothelioma
Bladder
Leukemia
Bladder, pancreasLung
Lung
Lung, prostate
LiverLung
Lung, nasal sinuses
Lung, scrotumLung, kidney, prostateLungLung, leukemiaLeukemia, stomachLung
Paranasal sinuses
Respiratory tractBladder, pancreas
Nasal cavity, lung, larynx
Melanoma
Skin. pancreas, brain, stomach,breast, salivary glands, thyroid,GI tract, bronchus, Iymphoid tis-
———. —.— A .
— .
Type of workers exposed— —— — —Manufacturers of apparel, carpeting, blanket% draperies. synthetic
furs, and wigsChemical workers
Workers in the metallurgical industries, sheep-dip workers, pesticideproduction workers, copper smelter workers, vineyard workers, in-
secticide makers and sprayers, tanners, miners (gold miners)
Asbestos fac tory workers , tex t i le workers , rubber - t i re manufac tur ingindustry workers, miners, insuIation workers, shipyard workers
Dyestu f fs manufac turers , rubber workers, textile dyers, paint
manufacturersRubber-tire manufacturing industry workers, painters, shoe manufac-
turing workers, rubber cement workers, glue and varnish workers,distillers, shoemakers, plastics workers, chemical workers
Dyeworkers, chemical workersBeryllium workers, electronics workers, missile Parts producers
Workers in plants producing anion-exchange resins (chemicalworkers)
Cadmium production workers, metallurgical workers, electroplatingindustry workers, chemical workers, jewelry workers, nuclearworkers, pigment workers, battery workers
Plastic workers, dry cleanersChemical workers, workers in plants producing ion exchange resin
Chromate-producing industry workers, acetylene and aniline worker%
bleachers, glass, pottery, pigment, and linoleum workersSteel industry workers, aluminum potroom workers, foundry workersSteel industry workers, coke plant workersChemical workers, drug makers, dyemakersChemical workersHospital workers, research lab workers, beekeepers fumigators
Miners
Isopropyl oil workers
production workersDyeworkers , rubber - t i re manufac tur ing indust ry workers , chemica l
workers, manufacturers of coal gas, nickel refiners, copper smelters,
electrolysis workersNickel refiners
PCBs workers
Uranium miners , rad io log is ts , rad iographer% luminous d ia l Pa in ters
SOUFiCES; Institute of Med!clne (179),
sue, leukemia, multiple myelomaSkin Farmers, sailors, arc welders
Skin, lung, bladder, GI tract Construction workers, roofers, chimney sweeps, machinists
Liver, kidney, larynx, Ieukemia Chemical workers, steelworkers, ceramic makers, incandescent, lampmakers, nuclear reactor workers, gas mantle makers, metal refiners,vacuum tube makers
Liver. brain, lung, hematolympho- Plastics factory workers, vinyl chloride polymerization plant workers
‘poietic system; breastPancreasStomachBrain, stomachHematolymphopoietic systemBladderEye, kidney, lungLeukemia, brainColon, brainEsophagus stomach, lung
ChemistsCoal minersPetrochemical industryRubber industry workersprinting pressmenChemical workersFarmersPattern and model makersOil refinery workers
— — ——-.—— ———‘International Agency for Res;a~cF~~ C-anc~r (185), and the Occupational SafetY and
————Health Administration (279a)

86 ● Technologies for Determining Cancer Risks From the Environment
have not yet been identified, are also included.Many of these exposures represent substantialhazards, and it is likely that other human car-cinogens exist which have not yet been detectedin the workplace. This may be because theadded cancer risk is small in comparison toother causes of cancer, because only a fewworkers have been exposed, or simply because ahazard has not been suspected and therefore notlooked for. Besides the substances listed, manyother industrial chemicals have been found tocause cancer in laboratory animals. It must alsobe borne in mind that human cancer seldom de-velops until one or more decades after exposureto a carcinogen, and thus it is too early to ascer-tain whether chemicals introduced into industryduring the last few decades will affect cancerrates.
Epidemiologically demonstrating an in-creased risk of developing cancer from an oc-cupational exposure generally involves resultsfrom examining large numbers of exposed peo-ple, the existence of relatively large risks, orsometimes a rare cancer, which facilitates draw-ing associations. Even then, years may passbefore a hazard is identified. As the workplacechanges, workers will be exposed to additionalsubstances, some of which may turn out to becarcinogenic.
Estimating the proportion of today’s cancersthat can be attributed to occupational hazards isdifficult. Determining how many future cancersmay arise from past and present occupationalexposures is even more speculative. As with allstudies of carcinogenesis, the latent periodmakes it extremely problematic to associate aparticular occupational exposure with an in-creased cancer risk. Individuals frequentlychange jobs which can result in exposure tonumerous substances, several of which may in-teract with each other either to promote or to in-hibit tumor formation. With rapidly changingtechnologies, new exposures emerge whileothers cease. Often, the available information isbased on studies which have inadequate ex-posure information. Exposure data are generallypoor because they are usually not collected untila hazard is recognized, or at least suspected.OSHA requires monitoring only for some of thesubstances which it regulates. Oftentimes em-
ployees, and even in some cases employers, areunaware of specific chemical exposures.
Certain occupational diseases are difficult todiagnose and this can lead to underreporting, asexemplified by recent letters to the New EnglandJournal of Medicine concerning the inability ofboard-certified pathologists to identify cases ofasbestosis (1,318). Studies can be designed toobtain exposure data and continuously monitorworkers’ health, but they are expensive. Eventhough no system has yet been adopted togather these types of information, such an ap-proach may be feasible in some industries.
Many estimates have been made of the per-centage of human cancers associated with occu-pational exposures, most ranging from 1 to 10percent. In most instances the bases for theseestimates are not presented and the estimatesthemselves appear little more than informedguesses. Since epidemiologic studies do notalways follow individuals for their full lifetimes,calculated risks may be underestimates. Themagnitude of a detected risk is dependent uponthe time elapsed between exposure and the timeindividuals are studied.
Higginson and Muir (165) estimated the im-pact of environmental factors in human cancer.They stated:
Although occupational cancers recognized sofar provide some of the most satisfactory datafor identifying external agents, the absolutenumber of cancers due to occupational expo-sures would appear to be relatively small, prob-ably 1 to 3 percent of all cancers.
Wynder and Gori (368) estimated the percentof 1976 cancer incidence in the United States at-tributable to occupation, From their summaryfigure, it appears that they estimated that thefraction of cancers attributable to occupationalfactors was 4 percent for men and 2 percent forwomen. Their explanation for these estimates isas follows:
The data presently available are, at best, edu-cated estimates of the relationship betweenspecific cancers and specific occupationalgroups. Cole et al.2 (1972) suggested that 20%
2P. Hoover, R. Cole, and G. H. Friedell, “Occupation and Can-cer of the Lower Urinary Tract, ” Cancer 29: 1250-60, 1972.

Ch, 3–Factors Associated With Cancer 87
of bladder cancers occurring in males in theBoston area are related to occupational ex-posure. In certain counties of New Jersey, the in-creased risk for this cancer appeared to be highamong workers in certain chemical industries.General estimates of the percentage of all humancancers related to occupational exposure rangebetween 1 and 10 percent.
Cole (62) estimated slightly higher figures forworkplace-caused cancer:
My estimates are less than 15 percent for menand less than 5 percent for women. These ratherlow figures emphasize that we are not dealingwith a single major public health problem.Rather, we are dealing with a series of modestproblems which are, however, of great impor-tance in the specific industries where they occur,
Cole does not describe the data used to derivethe estimate.
Higginson and Muir (166), in a later studyestimated that 6 percent of male cancers, skincancer included, in the Birmingham and WestMidland region of England in 1968 through1972, could be attributed to occupational ex-posures. Their paper describes some of the in-formation considered.
Fox and Adelstein (126) reviewed 1970-72British vital statistics and found that 12 percentof the differences in cancer mortality among dif-ferent occupational classifications could be ex-plained by variations associated with work andthe remaining 88 percent by lifestyle factors.They describe their estimate as an “over-simplified calculation, ignoring interactions be-tween direct and indirect influences . . . clearlyvery crude. ”
Recently, a different approach was used togenerate an estimate of workplace cancers by 10distinguished research workers of NCI, the Na-tional Institute of Environmental Health Sci-ences, and the National Institute for Occupa-tional Safety and Health (82). The report calcu-lated the proportion of cancers “for the nearterm and future, ” from quantitative estimates ofrisk and the numbers of workers exposed to sixknown carcinogens—asbestos, arsenic, ben-zene, chromium, nickel oxides, and petroleumfractions. This paper (82) concludes:
Reasonable projections of the future conse-quences of past exposure to established carcino-gens suggest that . . . occupationally relatedcancers may comprise as much as 20% or moreof total cancer mortality. Asbestos alone willprobably contribute up to 13-18% and the data(relating to five other carcinogens) suggest atleast 10-2070 more.
The total of occupationally related cancers fromthose six exposures is then 23 to 38 percent ofthe overall cancer total, to which must pre-sumably be added the effects of other occupa-tional carcinogens not included in the calcula-tion. This report has been widely misquoted asan assessment of the contribution of occupa-tional exposures to present cancer rates and isfrequently discussed and criticized because ofthe magnitude of the estimates and their diver-gence from previous estimates.
While this report has not been submitted forpublication, it has been widely circulated andreviewed (c f., 9,93,332,345). The two reviewsthat have been published are discussed below.
Toxic Substances Strategy Committee(TSSC) Review
TSSC (345) identified several methodologicalaspects which might have caused the HEW (82)paper to overestimate or to underestimate thecontribution of occupational factors to the over-all cancer rate.
Overestimating
1.
2.
3.
The number of cases of lung cancer asso-ciated with asbestos may have been over-estimated by attributing all cases of lung can-cer among asbestos workers to asbestos ex-posure.Exposures to the examined carcinogens wereprobably higher in the past than they havebeen recently.Estimates of the number of workers exposedmay have been too high since: a) workerswho were employed in more than one of thesix industries, a likely possibility in thechromium and nickel industries, might havebeen counted twice, and b) estimates of the

88 ● Technologies for Determining Cancer Risks From the Environment
number of exposed persons still alive and thusat risk may be exaggerated. This is particular-ly so with regard to the asbestos industry.
Underestimating
1. The six industries examined are not the onlyones believed to have carcinogens in theworkplace.
2. Epidemiologic data on which the estimatesare based do not reflect total lifetime risk.
3. Identifying unexposed groups to use for com-parison is difficult and the comparison groupused may be at a higher risk then the least ex-posed members of the population.
The TSSC report concludes (345):
Because it is difficult to quantify the impact ofall these factors, one cannot tell whether the fac-tors which lead to overestimation and thosewhich lead to underestimation balance eachother out.
Doll and Peto Review
Doll and Peto (93) examined the calculationsin the OSHA paper and in their view, the esti-mates:
. . . could not be regarded as having any validi-ty, primarily because the implicit assumptionwas made that the industrial conditions that hadbeen recognized as giving rise to gross hazards ofoccupational cancer were typical of the condi-tion to which 11.9 million workers in the UnitedStates were currently exposed.
Doll and Peto (93) used a different approachto estimate the proportion of cancers associated
AIR AND WATER POLLUTION
Determining the health effects of pollution isdifficult, particularly from low-level chronic ex-posures. The absolute risk from each pollutantis likely to be low and the resulting disease maynot appear for many decades, as is the case withcancer. Direct measurement of the incrementalrisk from these pollutants using epidemiologicmethods, against the background of more po-tent carcinogens, for instance tobacco, presents
with occupational exposures. Rather than focus-ing on individual occupational hazards, theybased their assessment on the contribution ofoccupational factors to individual cancer sitesand arrived at an estimate of approximately 4percent with an acceptable range from 2 to 10percent.
Lung cancers caused by asbestos contributethe largest proportion to the estimates madeboth by Doll and Peto (93) and by HEW (82).Hogan and Heel (171) have completed a carefulanalysis of asbestos and cancer and concludethat it may be associated with as much as 3(range: 1.4 to 4.4) percent of all cancers now orlikely in the near future. This inference is con-siderably less than the 13 to 18 percent es-timated by HEW (82).
Occupational Exposure Summary
Despite all of the arguments that have sur-rounded the estimates of workplace associatedcancers, almost every estimate fits comfortablyin the range of 10 & 5 percent. Uncertaintiesabout unknown carcinogens confound the esti-mates. Regardless of the exact number ofcancers associated with the workplace, the iden-tification of causes is most important. Preven-tive measures can reduce exposures only toidentified risks. Recently, an unusual number ofmelanomas in a nuclear research installation(89) and of brain tumors among oil industryworkers (55) have triggered further studies.These examples emphasize the value of work-place monitoring.
extreme methodological problems. There isoften little variation between individuals in thetype and extent of exposure to pervasive pollut-ants, and where measurable differences do exist,confounding variables often hinder adequatelydemonstrating an effect or the lack of one. It istherefore often necessary to rely on indirectsources of evidence that a pollutant is carcino-genic: short-term laboratory experiments that

Ch. 3—Factors Associated With Cancer ● 89
demonstrate mutagenicity or other toxic effects,animal bioassays, and epidemiologic data de-rived from groups exposed to high levels of pol-lutant chemicals. The latter are often obtainedin special situations, usually occupational,where people are exposed to much largeramounts than the general public.
Air Pollution
Air pollution is primarily a problem of majorcities but it can move in and out of differentareas and affect everyone. The Census Bureau(35) estimates that over 70 percent of the U.S.population lives in urban centers and that thisnumber is increasing with each passing year.The amount and type of air pollution in a givenregion changes not only with the time of day,but from day to day and year to year, makingmeaningful measurement difficult. Air pollutioncan be generally classified as a secondary en-vironmental stressor, aggravating existing dis-ease conditions or increasing the risk of diseasein those predisposed to ill health (326).
A variety of carcinogenic substances has beenidentified in air—e. g., asbestos, arsenic, PAH—and EPA has promulgated several regulationsunder section 112 of the Clean Air Act to limitexposure to these substances. Table 17 (see Oc-cupational Exposures) lists several recognizedoccupational carcinogens which may escapeinto the atmosphere in the course of industrialactivity and constitute a potential cancerhazard.
Morbidity and mortality due to chronic ob-structive lung disease—asthma, bronchitis, andemphysema —are probably the most importantlong-term health effects of air pollution. Urbanareas generally have a higher death rate fromchronic obstructive lung disease and lung cancerthan more rural environments (54,205). Thishas been used as the basis for suggesting that at-mospheric pollution is an etiologic factor in thedevelopment of cancer. However, like many ap-parently simple observations, this one isplagued by conflicting and confounding factors.Individuals residing in urban centers generallyhave smoking, drinking, and eating habits dif-ferent from their rural counterparts, and their
risk of infection and exposures to industrial en-vironments also varies. In addition, urban areastend to have more accurate death certificationand disease diagnosis which might bias collectedstatistics. Epidemiologic studies that examinethe health effects of air pollution must deal withthese factors.
Many airborne carcinogens are believed to in-teract synergistically with tobacco and occupa-tional exposures. Since cigarette smoking is thepredominant cause of lung cancer, it is a pri-mary suspect for explaining the observed ur-ban/rural gradient. There have been numerousattempts to disentangle the health effects ofsmoking from environmental pollution. Unfor-tunately, many studies have compared broadcategories of smoking habits, such as “smokers”versus “nonsmokers” or “never smoked” versus“ever smoked” which reduces the probability ofdiscerning any effects. More specific catego-ries —e.g., taking into account number of yearssmoked, age at which smoking began, numberof cigarettes smoked per day—are necessary toevaluate any urban/rural variation. In addition,other important differences may exist in smok-ing habits between urban and rural dwellers, forinstance, in the tar and nicotine content, inhala-tion habits, and other factors contributing todifferences in effective dose of carcinogenreceived (see Tobacco). Most studies concen-trating on nonsmokers have failed to demon-strate, or found only a slight difference, in lungcancer rates between nonsmokers in urban andrural environs, suggesting that airborne carcino-gens by themselves can be responsible for only asmall portion of the disease. Several have sug-gested that the effects of smoking a givenamount may be greater in urban than ruralareas (for review, see 91).
One of the most extensive investigations intothe effects of air pollution is a cohort study con-ducted by ACS. Data concerning men withoutknown carcinogenic occupational exposure pro-duced “little or no support to the hypothesis thaturban air pollution has an important effect onlung cancer death rates” (154). When lungcancer rates for men with occupational exposurewere compared to those for men without occu-
2 ,_+ ~ 1 - - 1? 1 - -

90 ● Technologies for Determining Cancer Risks From the Environment
pational exposures, the authors found a relativedifference of 26 percent in large metropolitanareas, 18 percent in smaller metropolitan areas,and 7 percent in nonmetropolitan areas. Thesedifferences, as Hammond and Garfinkel sug-gest, may be due to different types of occupa-tional exposures in the different areas. How-ever, an alternative explanation is that thehigher ratio of lung cancer maybe due to an at-tribute of the place of residence, air pollutionbeing one possible factor. In a reevaluation ofthese data, it was estimated that approximately10 percent of lung cancer in the ACS populationcould be attributed to an “urban effect” after ac-counting for smoking and occupation (61).Studies which concentrate on nonsmokers or thenonoccupationally exposed do not permit in-vestigating any interactive effects.
Another method for estimating the influenceof pollution on the cancer rate is to extrapolatefrom instances of high exposure. Occupationalstudies that include measurements of the con-centration of carcinogens in the respired air areespecially useful for this purpose. Measure-ments of the concentration of B(a)P are fre-quently used because it appears to be a good in-dicator of the concentration of PAH. However,it should be noted that B(a)P is not a perfect in-dicator of PAH in air, nor does it accuratelyreflect the carcinogenic potential of total airpollution. For instance, some non-PAH frac-tions of air pollution are as active as PAH incausing changes in cell cultures, which is ameasure related to carcinogenicity (294).
Pike and his colleagues (294) concluded that 1ng B(a)P per m3 in city air causes 0.4/100,000extra cases of lung cancer per year. In 1977, aninternational symposium at the Karolinska In-stitute in Stockholm, reached a similar conclu-sion (54):
. . . combustion products of fossil fuels in am-bient air, probably acting together with cigarettesmoke, have been responsible for cases of lungcancer in large urban areas, the numbers pro-duced being of the order of 5 to 10 cases per100,000 males per year . . . The actual rate willvary from place to place . . . depending uponlocal conditions.
These estimates must be used with caution sincethey are directly dependent on the concentrationof the different air pollutants, many of whichhave been changing over time. In 1959, BaPconcentrations ranged from 1 ng/m3 to approxi-mately 60 ng/m3; most nonurban areas hadlevels below 1 ng/m3. Recent monitoring byEPA found that the average concentration ofB(a)P in 26 urban areas decreased from approxi-mately 4 ng/m3 in the late 1960’s to 0.5 ng/m3 in1977 (70). Doll and Peto (93) estimated that thecurrent contribution of atmospheric B(a)P andassociated combustion products to the produc-tion of lung cancer is unlikely to account formore than 1 percent of future cases of lungcancer.
Similar calculations have been made for othercarcinogenic substances including airborne arse-nic and asbestos (93). These suggest that con-tributions to the overall cancer rate from theseagents should be small. Higher levels of pollut-ants and therefore greater risk may exist aroundparticular sources of pollution as exhibited bythe significantly increased mortality from lungcancer found in residents of counties with cop-per, lead, or zinc smelters or refineries (28). Theamount of asbestos commonly present in urbanair is 1,000 to 10,000 times less than the moststringent occupational regulations, although thegeneral public is exposed continuously to thislow level. At present, there is no evidence to in-dicate that the risk to the general public fromthese sources is measurable.
Also included under the heading of atmos-pheric pollution is the effect on the general pop-ulation of mining and milling of uranium andother radioactive ores and of radioactive falloutdue to testing of nuclear weapons. The HEW In-teragency Task Force on the Health Effects ofIonizing Radiation (182) estimated that for 1978the U.S. population collective dose was 1 mil-lion to 1.6 million person-rem. Based on the riskestimates derived from the linear model of theNAS Committee on the Biological Effects ofIonizing Radiation (BEIR) III (158 to 403 excesscancer deaths per million persons from contin-uous lifetime exposure to 1 rad/yr) one can es-timate that atmospheric radiation accounts for

Ch. 3—Factors Associated With Cancer ● 91
an upper limit of 645 fatal cancers per year. Thelower limit of risk can be considered to ap-proach zero.
The other class of atmospheric agents givenconsiderable attention because of a potential ef-fect on cancer rates are the chlorofluoro-carbons. Chlorofluorocarbons, used extensivelyas refrigerants and aerosol propellants, persistin the atmosphere and, it is argued, eventuallyreach the stratosphere where they react withozone, reduce its concentration, and hence per-mit more ultraviolet light to reach the surface ofthe Earth. This occurrence would result in an in-crease in the incidence of skin cancer, includingmelanoma. The issues involved, which are com-plex and based on a number of unprovedassumptions about physical and chemical proc-esses, have been reviewed by the NationalAcademy of Sciences (NAS) (70,264). Theyfound that if global release of chlorofluoro-carbons were to continue at 1977 rates, theozone concentration would eventually declineby 16.5 percent, with a reduction of about 8 per-cent by the year 2030 (70). A 16-percent ozonedepletion is predicted to eventually causeseveral thousand more cases of melanoma eachyear in the United States and several hundredthousand more cases of other less serious skincancers (70). This is approximately the sameorder of magnitude predicted by Urbach (354).The present contribution of chlorofluorocar-bons to overall cancer incidence is likely to bemuch less.
Until recently, air pollution was a problembelieved to be limited to outside air or dirtyworkplaces. Several studies have found that in-door air pollution may be a more serious healthhazard than outdoor air pollution (140). It hasbeen shown that a single smoker can pollute in-door air with around 1-1.5 ng/m3 B(a)P (260).NAS was asked by EPA to examine the vari-ables which are contributing to indoor air pollu-tion, their sources, and possible health hazards.To date, this issue has not been looked at in asystematic way though many people spend alarge percentage of their time in the indoor en-vironment. The General Accounting Office(140) suggested that the Clean Air Act beamended to provide EPA the responsibility and
necessary authority to address indoor air pollu-tion in the nonworkplace.
In sum, determining the proportion of thetotal cancer rate attributable to air pollution isnot possible with the available data. In moststudies, air pollution and smoking are seen asinteractive in cancer production. Whatever thecorrect percentage of cancer associated with airpollution, most researchers in this area believethat it is small. Doll and Peto (93) estimated that2 percent of cancer mortality, representing ap-proximately 8,000 cancer deaths, can be at-tributed to industrial pollution of air, water,and food, principally accounted for by the un-certain effects of combustion products of fossilfuels in urban air. This relatively small per-centage does not mean that efforts to control airpollutants should be minimized. Air pollution isresponsible for many serious detrimental healtheffects other than cancer and uncontrolled pol-lution might someday be found to impact moredramatically on cancer rates. Greater attentionshould be directed at discerning whether atmos-pheric pollutants act as initiating and/or pro-moting agents. If air pollution is acting as a sec-ondary stressor, then its role as a promoter mayprove to be most important.
Drinking Water Pollution
The extent to which water pollution is acausative agent for cancer is even less certainand more debated than is the role of air pollu-tion. The passage of the Safe Drinking WaterAct, Public Law 93-523, December 1974, wasprompted by the recognition that organic andinorganic chemicals, including substances iden-tified as known or suspect carcinogens and mu-tagens were present in drinking waters. Thesources for these contaminants are numerous:industrial pollution, agricultural runoff, leach-ate from waste disposal sites, and of particularrecent interest, byproducts of the disinfection ofdrinking water.
In the mid 1970’s, EPA set up various pro-grams, such as the National Organics Recon-naissance Survey, to evaluate the nature and ex-tent of organics in drinking water. Primary em-

92 ● Technololgies for Determining Cancer Risks From the Environment
phasis was on detecting a class of organics, thetrihalomethanes, formed during water treat-ment with chlorine and believed to be the mostubiquitous group of organics found in drinkingwater. Levels have been found to range frombelow 1 ug/liter to above 300 ug/liter. TheFederal Government has recently sought toreduce exposure to trihalomethanes by pro-mulgating a regulation establishing a “max-imum contaminant level” of 100 ug/liter totaltrihalomethanes for all community water sys-tems serving 10,000 persons or more that add adisinfectant in the treatment of their water(107).
Much attention has been centered on the rel-atively high concentrations of synthetic organ-ics found in untreated drinking water fromground water sources in certain areas of theUnited States. The extent to which these water-borne pollutants contribute to human carcino-genesis has been evaluated by the examinationof both laboratory and epidemiologic data.Many of these studies were reviewed by theNAS Safe Drinking Water Committee (266,270)as mandated by the Congress. (These reportsstand as references for many issues concerningthe health effects of drinking water con-taminants. )
The numerous epidemiologic studies thathave examined the association between drinkingwater and cancer have been of varying reliabili-ty and have taken many forms. These studiessuggest an association between constituents indrinking water and cancer mortality (169).However, the degree and extent of the associa-tion is disputed. NAS discussed and evaluated10 of the studies which focused on the relation-ship of trihalomethanes and cancer mortality.All but one of the studies were found to demon-strate a statistical association between exposureand excess cancer rate, but excess cancer at nosingle anatomical site was associated with ex-posure. The epidemiologic analyses do not havethe extrapolation difficulties of animal ex-periments, but they are plagued by confoundingvariables such as exposures to other sources ofcarcinogenic stimuli, including smoking, whichwere generally not accounted for. Many of thestudies utilized the cancer deaths rates of a
region and related them to the water quality ofthat region. The difficulty with this approach istwofold: 1) an individual’s place of death maydiffer considerably from where that personresided during most of his water-drinking life,and 2) the data on water quality are extremelylimited, often reflecting the water quality ofonly one water source in a region.
Prior to 1970, about 100 different organiccompounds has been identified in water (169).In the past, organic pollutants were measuredby crude, nonspecific methods such as biochem-ical oxygen demand and total organic content.Today, analytical techniques permit detectionof chemicals in minute quantities, and many arefound in concentrations of parts per trillion.NAS (270) found that over 700 volatile organiccompounds contaminate U.S. drinking water.Volatile substances make up only 10 percent ofthe total organic content of water and approx-imately 90 percent of this component has beenidentified and quantified. On the other hand,only 5 to 10 percent of the nonvolatile constit-uents of drinking water have been characterized(266). As technology improves and detectionmethods become more sensitive, an ever-in-creasing number of compounds may be detectedin drinking water.
In a report for the Council on EnvironmentalQuality, Crump and Guess (74) reviewed five ofthe recent case-control studies on cancer riskassociated with drinking water quality in thiscountry. While inadequacies were identified ineach of the studies (74):
. . . increased risks . . . are large enough to beof concern yet small enough to be very difficultto separate from confounding risks associatedwith other environmental factors.
Rectal cancer risk ratios for chlorinated v. un-chlorinated water were found to range from1.13 to 1.93. In three of the studies the riskratios were statistically significant. Statisticallysignificant risk ratios were also found in three ofthe studies for colon cancer and in two studiesfor bladder cancer. Although the studies did notindicate a consistently increasing cancer riskwith increasing exposure to organic contam-inants, one study did show such a relationship

Ch. 3—Factors Associated With Cancer ● 93
for rectal cancer and another was suggestive forcolon cancer.
Crump and Guess made crude estimates ofthe possible range of carcinogenic risks fromconsuming ground water (from wells) contain-ing various levels of synthetic organic chem-icals. They computed an upper risk limit of 7.5x 10-4 or about one case per 1,300 persons
from consuming water from a hypothetical wellcontaining the highest detected concentrationsof commonly found contaminants. Levels towhich most Americans are exposed are typicallymuch lower. The estimate is based on summingthe individual upper limits on human risk de-rived by a procedure which tends to produce ex-aggerated estimates of human risk. On the otherhand, only risks from chemicals known to bepresent in the wells and for which positive car-cinogenicity data exist, were considered in theestimate (74). Crump and Guess also computedan upper limit on the lifetime total cancer riskassociated with an average concentration ofchloroform to be 1.8 x 10 -4 or about one caseper 5,000 persons. The actual risk is probablymuch lower.
The NAS Safe Drinking Water Committeelists 19 carcinogens and 3 suspected carcinogensidentified in or thought to be in drinking water(266). NAS estimated the 95-percent upper con-fidence limit of cancer risks to humans fromlifetime exposure to water containing 1 ug/1 ofeach of these compounds. These estimates aredisplayed in table 18 and are compared with riskestimates computed by EPA’s Carcinogen As-sessment Group. It is interesting to note that inmany cases a tenfold to hundredfold differenceexists between the two estimates. These differ-ences are due to the use of different extrapola-tion models and the use of point rather than in-terval estimates.
The problem of evaluating the effects of mul-tiple exposures is acutely relevant to water-borne pollutants because of the multitude ofcompounds found in drinking water. Bioassayshave rarely attempted evaluation of synergisticor antagonistic effects. Therefore, these esti-mates may not accurately reflect the human car-cinogenic risk from these compounds.
Table 18.—Concentration of Drinking WaterContaminants and Calculated Excess Cancer Risk
NAS a CAGb
1 0 -6 1 0 -6
Ug/lc Ug/lc
Acrylonitrile . . . . . . . . . . . . . . . .Arsenic . . . . . . . . . . . . . . . . . . . .Benzene . . . . . . . . . . . . . . . . . . .Benzo (a) pyrene. . . . . . . . . . . . .Beryllium . . . . . . . . . . . . . . . . . .Bis (2-chloroethyl) ether . . . . . .Carbon tetrachloride. . . . . . . . .Chlordane. . . . . . . . . . . . . . . . . .Chloroform . . . . . . . . . . . . . . . . .DDT . . . . . . . . . . . . . . . . . . . . . . .1,2-Dichloroethane . . . . . . . . . .1,1-Dichloroethylene . . . . . . . . .Dieldrin . . . . . . . . . . . . . . . . . . . .Ethylenedibromide . . . . . . . . . .ETU . . . . . . . . . . . . . . . . . . . . . . .Heptachlor . . . . . . . . . . . . . . . . .Hexachlorobutadiene . . . . . . . .Hexachlorobenzene . . . . . . . . .N-nitrosodimethylamine. . . . . .Kepone . . . . . . . . . . . . . . . . . . . .Lindane. . . . . . . . . . . . . . . . . . . .PCB . . . . . . . . . . . . . . . . . . . . . . .PCNB . . . . . . . . . . . . . . . . . . . . .TCDD . . . . . . . . . . . . . . . . . . . . . .Tetrachloroethylene . . . . . . . . .Trichloroethylene . . . . . . . . . . .Vinyl chloride . . . . . . . . . . . . . . .
0.77————
0.839.090.0560.590.0831.4
—0.0040.110.460.024
—0.034
—0.0230.1080.327.14
—0.719.092.13
0.0340.0043.0
—0.02
—0.0860.0120.48
—1.46
.28—
0.0022—
2.41.4
—0.0052
————
5.0 x 10-’0.825.8
106.0astandardized to 1O-S risks from Natfonal Academy of Sciences, Drinking Waterand Health (266) for consumption of 1 I/water/day
bReca[culated to exclude aquatic food Intake from Cancer Assessment Group,
Arnbent Water (Jua//ty Cr/ter/a (104) Standardized to 1 I/water/day IntakecAverage adult water consumption IS 2 I/day.
SOURCE Office of Technology Assessment
As more chemicals are tested, additional sub-stances found in drinking water will be shownto be carcinogenic. Two substances identified indrinking water, toxaphene and 1,2 dichloro-ethane, not considered carcinogenic by NAS in1977, have since been shown by NCI to be car-cinogenic in animals. Two additional com-pounds, bromodichloromethane and chlorodi-bromomethane, found in most drinking watersystems surveyed by EPA, have not been appro-priately tested for carcinogenic properties buthave been shown to be mutagenic in the Amestest (169). In 1978, NCI (203) published a list of23 recognized or suspected carcinogens, 30mutagens and 11 tumor promoters which havebeen found in American drinking water.
Turning from the organics to inorganic, sev-eral studies have attempted to correlate levels of
94 ● Technologies for Determining Cancer Risks From the Environment
carcinogenic trace metals in water supplies, withcancer rates. Associations of high levels of arse-nic in drinking water with cancer of the skin andother sites were found in Taiwan and Argentina(203,370). Berg and Burbank (25) comparedconcentrations of eight carcinogenic metals inwater supplies with State cancer mortality rates.They found strong correlations with cadmiumconcentrations and cancer mortality; no signifi-cant correlations with iron, cobalt, and chro-mium; a low but not biologically interpretablelevel of significance with nickel and arsenic; andsome correlations with lead and berylliumwhich correspond to known biological ac-tivities.
Asbestos, an established human carcinogen,is also of some concern since it has been foundto contaminate water supply systems. No rela-tionship between asbestos in drinking water andcancer has been found but available data arevery limited.
Experimental and epidemiologic data providesome evidence that a carcinogenic hazard existsfrom drinking water contaminants, but does notpermit adequate quantification. Most attention
CONSUMER PRODUCTS
Consumer products are a class of agents thatare so numerous that it is only possible to echothe uncertainty with which pollutants were dis-cussed in the previous section. Detergents andother surfactants, hair dyes and other cos-metics, solid or foam plastics, paints, dyes,polishes, solvents, fabrics, and even the proc-essed paper and the printer’s ink in this reportare but a few. It is likely that some of theseproducts are already causing, unnoticed, a num-ber of today’s cancers, and it is quite possiblethat after prolonged exposure substantial risksmight be detected in the future.
The difficulty in assessing cancers associatedwith exposure to consumer products is that thedose is usually low, and the exposed populationtends to be very large. An adequate assessmentof the carcinogenic effect of a consumer productmight require a study of a million people,
on quantifying risk estimates from waterbornecarcinogens has focused on chloroform, since italone has consistently generated dose-responsedata sufficient for extrapolating human risk. Anad hoc study group of the EPA’s Hazardous Ma-terial’s Advisory Committee (158) estimated therisk as follows:
The level of risk, estimated from considera-tion of the worst case [Miami, 311 ppb] and forthe expected cancer site for chloroform (theliver), might be extrapolated to account for upto 40% of the observed liver cancer incidence.
The results of a large NCI case-control studywhich is examining possible relationships be-tween water quality and bladder cancer are ex-pected in 1981. Information was obtained inthat study on a wide range of demographic andexposure factors and a data bank on water qual-ity was created for more than 1,000 utilitiesserving many of the people in the study. Thatinformation will hopefully permit linking an in-dividual’s risk factors with disease state. In ad-dition, a case-control interview study to investi-gate relationships between drinking water andcolorectal cancer is being conducted (74).
whereas a study of only 1,000 workers might beadequate in an occupational setting. Further,while occupational exposure to a carcinogen isfrequently limited to a group of relativelyhealthy workers, consumer exposure includessubpopulation groups usually considered to be“at high risk, ” such as infants, small children,the elderly, and the infirm,
For most consumer products, available lab-oratory and human evidence is insufficient todetermine whether they pose a cancer risk. Themagnitude of the potential health hazard be-comes apparent when one begins to examinepopulation exposure to different consumerproducts. In 1973, U.S. production of aerosolproducts was estimated at 2.9 billion units. Arecent Consumer Product Safety Commission(CPSC) study indicated that manufacturers re-moved trichloroethylene (TCE), a widely used

Ch. 3—Factors Associated With Cancer ● 95
solvent in aerosol formulations, from consumeraerosol product formulas after TCE was shownto be carcinogenic in tests at NCI (117). The ex-tent to which aerosol products containing TCEhas impacted on today’s cancer rates or howmany future cancers will result from past ex-posures is difficult to evaluate.
Attempts at quantifying potential adverse ef-fects associated with consumer exposure to car-cinogens are relatively new. In 1977, CPSC es-timated that exposure of children to TRIS-treated clothing could result in an excess risk ofcancer of up to 180 cases per million exposures.Other examples of estimated consumer risk in-clude up to 2,000 lifetime excess respiratory can-cer deaths per million persons exposed to
MEDICAL DRUGS AND RADIATION
Medical practices have resulted in some dev-astating health crises, from the fatal puerperalfevers of the 19th century maternity wards tothe millions who were exposed in utero to dieth-ylstilbestrol (DES) and are now experiencing avariety of adverse health effects, including atleast one type of cancer. Only drugs which havebeen associated with cancer in humans will bediscussed in detail, but limited or inconclusiveevidence exists for many others, and still othershave not been investigated (see table 19).
The production of cancer, although alwaysan undesirable side effect, is not necessarily abar to the use of a drug if the risk of cancerdevelopment is materially less than the medicalgains brought about by the treatment—e.g., bythe use of alkylating agents, immunosuppres-sive drugs and radiotherapy in the treatment ofcancer. The risks in some cases are known, aswith some cancer chemotherapy agents, butmore often are not suspected. Detection of dis-proportionate adverse effects through case re-ports and epidemiologic studies have caused theabandonment of certain agents and treatmentsfor particular uses, for instance, inorganictrivalent arsenic, chlornaphazine, DES duringpregnancy, and the radioactive agents thoriumand thorotrast.
asbestos-containing patching compounds; paintstripper containing 52 percent benzene may pre-sent an excess risk of death from leukemia of upto 50 per million people exposed; and people liv-ing in a residence insulated with urea-formalde-hyde foam may beat an excess cancer risk of upto 290 per million people exposed (117).
At this time it is impossible to assess the con-tribution of consumer products to the overallcancer rate. Many industrial products have beenintroduced so recently that even if they do provehazardous their effects would not yet be ap-parent. Doll and Peto (93) attribute “less than 1percent” of all cancer deaths to such products,but stress that there is too much ignorance forcomplacency to be justified.
The causal link between in utero exposure toDES, a synthetic estrogen, and subsequent de-velopment of a rare type of vaginal cancer in fe-males (and possibly testicular cancer in males)about 20 years later is a well-publicized exampleof unsuspected risk. Between 4 million and 6million Americans (mothers, daughters, sons)were exposed to DES since about 1945 (258) inefforts to prevent spontaneous abortions. Aslater became evident, DES was an ineffectivetherapy (90).
In this case, in spite of the long latency be-tween in utero exposure and cancer develop-ment two or three decades later, the connectionwas made between exposure and disease. Thefacilitating factor in this case was the near non-existence of the cancer type in the general pop-ulation at the ages in which the disease wasseen. However, had the effect been a small ex-cess of a common cancer, it is doubtful that theassociation would have been uncovered. Sincethe original association was uncovered, otherpossible adverse effects have been suspected inDES mothers, daughters and sons.
In cases of agents for which some risk isknown or suspected, the use of the agent is con-tinued under controlled conditions, in the belief
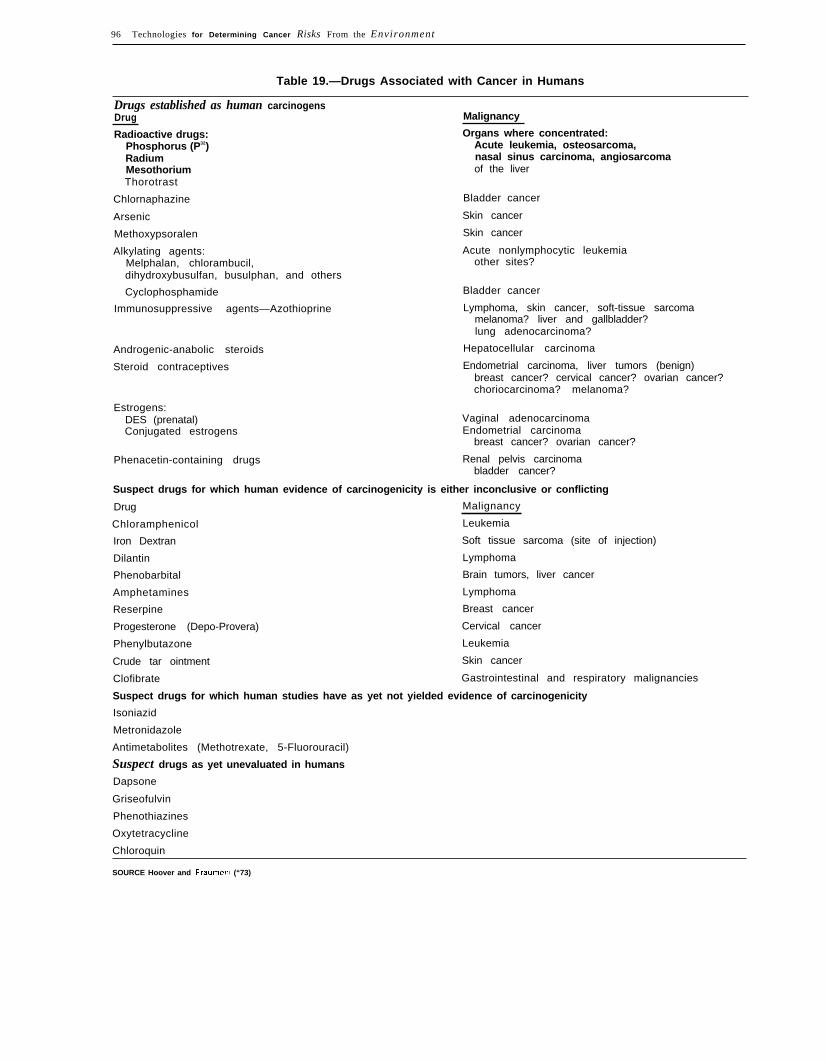
96 Technologies for Determining Cancer Risks From the Environment
Table 19.—Drugs Associated with Cancer in Humans
Drugs established as human carcinogensDrug Malignancy
Radioactive drugs: Organs where concentrated:Phosphorus (P32) Acute leukemia, osteosarcoma,Radium nasal sinus carcinoma, angiosarcomaMesothorium of the liverThorotrast
Chlornaphazine Bladder cancer
Arsenic Skin cancer
Methoxypsoralen Skin cancer
Alkylating agents: Acute nonlymphocytic leukemiaMelphalan, chlorambucil, other sites?dihydroxybusulfan, busulphan, and others
Cyclophosphamide Bladder cancer
Immunosuppressive agents—Azothioprine Lymphoma, skin cancer, soft-tissue sarcomamelanoma? liver and gallbladder?lung adenocarcinoma?
Androgenic-anabolic steroids Hepatocellular carcinoma
Steroid contraceptives Endometrial carcinoma, liver tumors (benign)breast cancer? cervical cancer? ovarian cancer?choriocarcinoma? melanoma?
Estrogens:DES (prenatal) Vaginal adenocarcinomaConjugated estrogens Endometrial carcinoma
breast cancer? ovarian cancer?
Phenacetin-containing drugs Renal pelvis carcinomabladder cancer?
Suspect drugs for which human evidence of carcinogenicity is either inconclusive or conflicting
Drug Malignancy
Chloramphenicol Leukemia
Iron Dextran Soft tissue sarcoma (site of injection)
Dilantin Lymphoma
Phenobarbital Brain tumors, liver cancer
Amphetamines Lymphoma
Reserpine Breast cancer
Progesterone (Depo-Provera) Cervical cancer
Phenylbutazone Leukemia
Crude tar ointment Skin cancer
Clofibrate Gastrointestinal and respiratory malignancies
Suspect drugs for which human studies have as yet not yielded evidence of carcinogenicity
Isoniazid
Metronidazole
Antimetabolites (Methotrexate, 5-Fluorouracil)
Suspect drugs as yet unevaluated in humans
Dapsone
Griseofulvin
Phenothiazines
Oxytetracycline
Chloroquin
SOURCE Hoover and Fraumenl (“73)

Ch, 3—Factors Associated With Cancer ● 97
that the benefit will prove to outweigh theharm. Many of the known hazardous drugs areused in the treatment of relatively uncommonserious conditions and the sum of the cancerscaused by them can amount to no more than afew score throughout the entire country eachyear. However, some drugs, including oral con-traceptives, and estrogens are or have been usedextensively. These and the medical use of ioniz-ing radiation, also known to be carcinogenic,are discussed below.
Oral Contraceptives
Oral contraceptives are taken by over 80 mil-lion healthy women the world over (366), spur-ring international concern about possible healtheffects, Not surprisingly, the possibility of in-creased cancer risk after long-term use and along latent period has been the focus of majorepidemiologic efforts.
The evidence to date has clearly implicatedone type of sequential oral contraceptive (anestrogen and a progestin taken separately dur-ing the first and second halves of the monthlycycle), the use of which has been abandoned,with some cases of endometrial cancer in youngwomen. Conversely, there is some evidence thatusers of combination type oral contraceptives(an estrogen and a progestin taken together inthe same pill) may be at slightly lower risk forendometrial cancer (360).
In animal tests, both breast and liver cancershave been induced by components of oral con-traceptives. A small number of benign livertumors in humans have been associated withcertain types of oral contraceptives, and thoughnot cancers in the usual sense, they can causefatal internal hemorrhage. No controlled studyhas yet evaluated the possible risk of malignantliver tumors (173).
Studies of breast cancer in oral contraceptiveusers have thus far yielded no clear-cut evidencefor either increased or decreased risk, exceptperhaps some increase for women already athigh risk (see p. 99, Sexual Development,Reproductive Patterns, and Sexual Practices fora full discussion of risk factors). Cervical cancer
also has been studied extensively with no con-sistent findings.
There is some evidence to suggest that oralcontraceptives may reduce the risk of ovariancancer. The reduction may be related to loweredlevels of ovulatory activity, since high levelshave been associated with an increased risk ofovarian cancer.
Because oral contraceptives have been part ofthe American lifestyle for a relatively shortperiod, large numbers of users have not reachedold age, the period of greatest cancer risk. Untilsuch time, perhaps within the decade, the full ef-fects cannot be known. Even then, because thereare many types of oral contraceptives, some ofwhich already have been shown to have differ-ent effects, and because formulations anddosage levels have changed significantly overtime, risks identified for that first cohort maynot apply to today’s users. Overall, evaluatingthe evidence available at this time, oral con-traceptives do not appear to be a major cause ofcancer, but do require continued epidemiologicattention.
Menopausal Estrogens
The use of “replacement estrogens” to relievemenopausal symptoms became widespread inthe 1960’s. A sharp rise in the incidence of en-dometrial cancer followed through the mid-1970’s in what has been termed “one of thelargest epidemics of iatrogenic disease , . . inthis country” (194). A cause-and-effect relation-ship was established through epidemiologicstudies, precipitating a decline in the use of theseagents. Shortly after the levels of use dropped,incidence began to fall toward previous levels,and the “epidemic” appears to be largely over.Fortunately, these endometrial cancers have arelatively good prognosis, and while morbidityincreased sharply, mortality attributable to es-trogen therapy has not paralleled the incidencetrend. Estrogen therapy is still prescribed forsome women, generally for shorter periods oftime than previously. Used in this way, the riskof endometrial cancer appears much lower,though some cases may still occur, but the ben-

98 ● Technologies for Determinin g Cancer Risks From the Environment
efits of therapy are thought to outweigh theresidual risk.
Evidence has been accumulating that breastcancer risk may be increased by menopausal es-trogen therapy (173), particularl y a m o n gwomen who develop benign breast disease whiletaking estrogens (93). Unlike the case of endo-metrial cancer and estrogen therapy, where in-creased and decreased risk follow closely thetemporal pattern of usage, change in breast can-cer risk appears to require many years to mani-fest itself.
Other associations between menopausal es-trogens and cancer have been suggested. TheBoston Collaborative Drug Surveillance Pro-gram (30) reported increased gallbladder dis-ease, which is a strong risk factor for cancer ofthe gallbladder, among women who had estro-gen therapy. Some studies have suggested an in-creased risk of ovarian cancer; others a de-creased risk of some reproductive-site cancers(173). Because of these uncertainties and thelong latent periods associated with many can-cers, continued long-term followup is requiredto determine if associations exist, and if so, themagnitude of the risks.
Other Drugs of Known Carcinogenicity
Certain alkylating agents, a class of drugsused primarily in the treatment of cancer, havebeen convincingly associated with acute non-lymphocytic leukemia, known to have a rela-tively short latent period, and one agent in par-ticular, cyclophosphamide, with bladder can-cer. As survival improves for some treated can-cers, increases may be seen in some other solidtumors, which generally have longer latentperiods than leukemia.
Immunosuppressive agents, used widely intransplant patients, greatly increase the risk oflymphoma, and result in moderate increases intumors at several other sites. The sites whichshow an increase are similar to those encoun-tered with genetically determined immune defi-ciency syndromes and other conditions associ-ated with immunodeficiency.
The initial report of a program designed toscreen large numbers of commonly used drugs
for carcinogenicity has recently appeared (133).The followup period has been only 4 years, and53 possible associations have been identified,some with increased risk and some with decreas-ed risk of cancer. Until a longer followup periodhas elapsed, no conclusions of causality can bereached. The importance of this type of surveil-lance mechanism lies in its long-term utility, inidentifying carcinogens and generatinghypotheses.
The Interagency Task Force on the Health Ef-fects of Ionizing Radiation (182) estimated thatthe collective dose of radiation received by theU.S. population for medical purposes, mainlydiagnostic, amounts to about 18 million person-rem per year. Using the linear model from BEIRIII (268), which produces a conservatively high
estimate, the risk of all types of cancer rangesfrom 158 to 403 fatal cancers per million person-rem. Applying these values to the total popula-tion yields an estimate of between 2,844 and7,254 fatal cancers per year. Using the least con-servative model, the lower risk estimate ap-proached zero. However, some of the medicallyassociated radiation would have been receivedby people with an expectation of life that wastoo short for any significant chance of devel-oping radiation-induced cancer (because of ill-ness or age) and the total effect may be some-what less.
Although well over half of the total popula-tion receives some medical radiation, the mostsusceptible members of the population—unbornfetuses—are of particular concern. Stewart,et al. (333) in England and MacMahon (216) inthe United States first identified a risk tochildren who had been exposed in utero, whichhas been corroborated by numerous studiessince. There is also evidence that the risk ofchildhood cancer is increased by X-rays of themother even before pregnancy (327), suggestingthat both germ cell (in this case, ovum) muta-tions as well as somatic (in the cells of thedeveloping child) may be important.
Pelvimetry, a radiographic examination usedto determine the pelvic dimensions of themother and the fetal headsize, is the majorsource of ionizing radiation to fetuses. It has

Ch. 3–Factors Associated With Cancer ● 99
been estimated that in recent years, 6 percent(about 200,000/yr) of all births have receivedroutine pelvimetry, and rates are much higher insome places (46,198). The Food and Drug Ad-ministration (FDA) panel on X-ray pelvimetry,in a statement adopted by the American Collegeof Radiology concluded that, “Pelvimetry is notusually necessary or helpful in making the deci-sion to perform a cesarean section. ” A similarstatement approved by the American College ofObstetricians and Gynecologists states that: “X-ray pelvimetry provides little additional in-formation to physicians involved in the man-agement of labor and delivery. ” Both groupsrecommend that pelvimetry be limited to indi-vidual cases meeting specific criteria forusefulness, and should not be used as a routineexamination (39). Although the actual numbersof childhood cancers caused by medical radia-tion may be modest, the number could easily bereduced by reductions in irradiation at least dur-ing and probably prior to pregnancy.
Unnecessary and unproductive radiation isnot limited to pelvimetry. The Bureau of Radio-
logical Health (FDA) has addressed this issue bybeginning to prepare a series of documents ad-dressing patient selection, conduct of examina-tions, and interpretation of results in radio-graphic procedures (38).
Doll and Peto (93) have estimated that about1 percent of 1977 cancer deaths probably are at-tributable to medical practice. They go on tosay that the number of ways in which drugsmight in principle increase or decrease cancer in-cidence rates is almost limitless.
Higginson and Muir (163) attributed about 1percent of all cancers in the Birmingham andWest Midland region of England (1968-72) toiatrogenic causes. They note that the wide-spread use of estrogen therapy in the UnitedStates mightU.S. women.that about 4cidence wasmones.
indicate a higher proportion forWynder and Gori (368) estimatedpercent of 1976 U.S. cancer un-associated with exogenous hor-
SEXUAL DEVELOPMENT, REPRODUCTIVE PATTERNS,AND SEXUAL PRACTICES
Sexual development and reproductive pat-terns affect the development of a number ofcancers, affecting females to a greater degreethan males. The course of sexual developmentitself may be heavily influenced by such factorsas diet and body composition (fat-to-lean ratio),and reproductive patterns are often influencedby economic and social conditions. Reproduc-tive and dietary factors might well interactmultiplicatively in the production of thesecancers and there will be overlap between whatis preventable through diet and through repro-ductive factors. Doll and Peto (93) have esti-mated that about 7 percent (6 percent frombreast, ovarian, and endometrial cancers and 1percent from cervical cancer) of all cancersmight be prevented by measures affecting themechanisms of reproduction and sexual factors.
Some evidence is consistent with cervicalcancer in women being associated with infec-
tious agents and less certain evidence associat-ing other genitourinary cancers with infection.If this is true, some cancer-causing agents maybe transmitted as venereal diseases.
Cancers of the Breast, Ovary,and Endometrium
The probability that environmental factorscontribute heavily to cancer of the breast, en-dometrium, and ovary is supported by interna-tional comparisons and studies of migrants. Thehighest rates are found in white women in theUnited States and Western Europe and the low-est among Asian women (see table 20) (184).Lifestyle differences, particularly in diet andreproductive patterns, are probably importantcontributors to the rate differences. Migrantstudies in the United States have shown that the

100 ● Technologies for Determining Cancer Risks From the Environment
Table 20.–Selected International Age-Standardized incidence per 100,000for Cancers of the Breast, Corpus Uteri, Cervix Uteri, Ovary, Prostate,
Testis and Penis
Females
Breast Corpus uteri Cervix uteri Ovary
Oxford, United Kingdom . . . . . . . . . . . . . 54.5 9.4 11.4 11.7Alameda County, Calif., blacks. . . . . . . . 56.6 13.6 28.0 10.3Alameda County, Calif., whites. . . . . . . . 76.1 33.3 12.3 13.5Osaka, tJapan . . . . . . . . . . . . . . . . . . . . . . 12.1 0.9 16.2 2.8Ibadan, Nigeria . . . . . . . . . . . . . . . . . . . . . 15.3 1.6 21.6 7.0
Males
Prostate Testis Penis
Oxford, United Kingdom . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19.2 2.6 0.7Alameda County, Calif., blacks . . . . . . . . . . . . . . . . . . . . . . . 75.0 0.5Alameda County, Calif., whites . . . . . . . . . . . . . . . . . . . . . . . 40.4 4.4 0.6Osaka, Japan . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2.7 0.7 0.5Ibadan, Nigeria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10.0 0.1 0.2
SOURCE Data from International Agency for Research on Cancer (184)
initially lower rates for Mexican-Americans(234) move toward the higher rates for whites inthe United States after a generation or two,owing to shifts in lifestyle toward those of theAmerican population,
ACS (6) estimates that 110,000 women in theUnited States will develop breast cancer in 1981,and that 37,000 women will die from the dis-ease. Breast, the leading site of cancer death inwomen today, will account for approximately19 percent of all female cancer deaths in 1981. Ahost of studies has established a set of factorsthat characterize women at high risk for breastcancer (219). Age, geographic area of residence,age at first childbirth, age at menarche (begin-ning of menstrual function), age at menopause(cessation of menstrual function), history ofbenign breast disease, and familial history ofbreast cancer are the major predictors.
International comparisons of breast cancerrisk by age has provided the basis for hy-potheses which have been examined in furtherepidemiologic studies. In areas where incidenceis high (e.g., North America and Western Eur-ope) the rate increases throughout life, oftenwith a break, where incidence decreases or atleast ceases to rise, at about 50 to 55 years ofage, after which it increases steeply once again.In areas of low incidence (e.g., most areas ofAsia and Africa), rates increase through middle
age, decreasing after about age 50. Intermediatepatterns occur in areas of intermediate incidence(e.g., Southern Europe and South America)(219).
One basic hypothesis following from thestudy of age-specific rates is that breast cancer isbest described as two diseases: one occurringpremenopausally and the other postmeno-pausally, each with different causes. De Waard(79) presents some additional arguments fromepidemiologic research favoring this hypothesis.Paffenbarger, Kampert, and Chang (289) haverecently added weight to the arguments againstthe hypothesis, based on a large case-controlstudy of breast cancer, concluding that overallthe evidence supports a “common cause subjectto modifying influences” for all breast cancer.The weight of evidence does not yet allow con-cluding whether breast cancer should be de-scribed as one disease or two.
Age at first childbirth is a strong predictor.Giving birth to the first child after age 30, orhaving no children at all place one at a greaterrisk than giving birth to the first child before age20 (238). A pregnancy must go to full term forany protective effect. It is widely believed thatthe first stimulus to lactation, whether or notbreast feeding is carried out, may be the factorof consequence. Miller and Bulbrook (238),reporting on a meeting of the Multi-Disciplinary

Ch. 3–Factors Associated With Cancer 101
Project on Breast Cancer of the InternationalUnion against Cancer, speculate:
A population that achieved a 5-year reductionin age at first delivery might achieve a 30-per-cent reduction in incidence of breast cancer.
An analysis of population-based cancer mor-tality rates (27) supports the correlation be-tween nulliparity and higher rates. The datasuggest that, if the current pattern continues, thedecreasing fertility trends of the 1960’s and1970’s may foretell increased breast cancer ratesfor women in this decade.
Age at menarche has also been shown to havesome degree of predictive value in nearly allbreast cancer studies, with a lower age indi-cating a higher risk. Tulinius et al., (346) in theirstudy of Icelandic women, found a “slight in-fluence” remaining after adjustment for parityand age at first pregnancy. Henderson et al.(162) found that women with menarche beforeage 13 had 1-1/2 times the breast cancer risk of awoman with later menarche.
Age at menarche, itself, maybe influenced byenvironmental factors, notably nutrition. Pop-ulation-based data reveal a steady decline in theage at menarche for American women, thoughtto be attributable to improved nutritional status(238). The effect of this on future breast cancerrates is uncertain. Early studies in rats cor-related body size, more than age, with onset ofmenarche (121). Similarly, observations in hu-mans, including a recent look at menarche anddisturbances in the menstrual cycle of balletdancers (134), provide evidence that lean bodymass is related to later menarche. Later age atmenopause brings increased risk. Women withnatural menopause after age 55 have abouttwice the risk of developing breast cancer as dowomen with natural menopause before age 45(219).
Breast cancer risk has a strong familial com-ponent that has not been entirely explained bylifestyle similarities among relatives. First-de-gree (sisters, mothers and daughters) and sec-ond-degree (nieces and aunts) relatives ofwomen with breast cancer have two to threetimes the risk of the general population. Rel-atives of women with bilateral breast cancer are
at higher risk, and are more likely to be diag-nosed at an earlier age and to develop bilateraldisease than are relatives of women with uni-lateral disease (15).
Gray, Henderson, and Pike (144) looked atthe higher rate of breast cancer in U.S. whitewomen compared with U.S. black women.They found that the relationship between blackand white rates is not constant. Below age 40,black women have higher rates than whites,while after age 45, black rates were 20 to 30 per-cent lower than those for whites. This can beonly partially explained by differences in age atmenarche, but a full explanation has not beendemonstrated.
Cancers of the endometrium and ovary shareat least two important risk factors with breastcancer. They are all associated with high-fatdiets and women who have not borne childrenare at an increased risk for all three types com-pared to women who have borne children. Oc-currence of either breast or ovarian cancer in-creases the risk of a cancer developing at theother site. Breast cancer also increases the riskof future endometrial cancer (324). Ovarianhormonal activity may be the influencing factorin alI of these sites.
Cancer of the Cervix
There is a striking association between cancerof the uterine cervix and the number of sexualpartners a woman has had. The death rate forthis cancer among nuns is much lower than it isfor the general population (129), suggesting theinvolvement of a venereally transmitted agent.A possible candidate is a virus (Herpes simplextype II) which has been found in associationwith both cervical cancer and other cervical cellabnormalities (244). Some study results supportthis hypothesis, but the data are considered onlysuggestive at this point, and no conclusion ofcausality can be drawn.
The number of deaths from cervical cancer(ACS projects 7,200 in 1981) has decreased andcontinues to decline, partially due to the morewidespread use of cervical screening (6). Basedon the assumption that the majority of cervical

102 ● Technologies for Determining Cancer Risks From the Environment
cancers are caused by infective processes, Dolland Peto (93) estimate that prevention or treat-ment of infection might reduce total cancer mor-tality by 1 percent.
Cancers of Male Reproductive Organs
International comparison and a study ofUgandan men has shown a correlation of higherrates of penile cancer in areas where circumci-sion is not generally practiced and where penilehygiene is poor (163),
Age-standardized incidence rates for prostatecancer vary between about 3/100,000 in Japanand 40/100,000 in U.S. whites, to a high ofabout 75/100,000 for some U.S. blacks (184),suggesting an environmental etiology. Feminella
NATURAL RADIATION
One would like to think that at least MotherNature would not place a carcinogenic burdenon the people of this planet. This unfortunatelyis not the case. Several types of natural radia-tion cause concern regarding carcinogenicity,the most important of which, ultraviolet radia-tion and ionizing radiation, were among thefirst factors recognized as human carcinogens.
Ultraviolet Radiation
Ultraviolet radiation (or ultraviolet light) isassociated with some lip cancers, with a largeproportion of squamous-cell carcinomas and isthe principal cause of basal-cell carcinoma ofthe face and neck in light-skinned people. Theevidence for the association includes prevalenceon sun-exposed areas, increased incidence inlightly pigmented people, and increased inci-dence with greater insolation and greater timeoutdoors. Basal-cell carcinomas account forover 75 percent of all skin cancers, but appro-priate treatment cures about 95 percent (159).The squamous- and basal-cell carcinomas arereferred to as nonmelanoma skin cancer.Approximately 400,000 cases occur annually–as many cancers as occur at all other sites com-bined (66). Fortunately, most are not fatal.
and Lattimer (119) found an increase in cervicalcarcinomas among wives of cases. A common,perhaps viral, etiology is suggested; however itis not substantiated by some population-basedrates, for instance, a lower rate of prostaticcancer and a higher rate of cervical cancer oc-curs among Mexican-Americans as compared toU.S. blacks (163).
Testicular cancer is highly associated with ab-normalities of sexual development, particularlycryptorchidism (failure of the testes to descendinto the scrotum) (208). Cancer occurs in 11 to15 percent of undescended testes (s). The associ-ation may be direct or a third factor, perhapsendocrinological,both conditions.
may predispose individuals to
NCI conducted a nonmelanoma skin cancersurvey in eight locations in the United Statesduring the period 1977-78, as mandated by theClean Air Act Amendments of 1977. Men werefound to be at greater risk of cancer than werewomen. The average age-adjusted incidencerate for white males was 310/100,000 and forwhite females 172/100,000 (250). An increase of15 to 20 percent was reported in incidence ascompared to the rate estimated from the ThirdNational Cancer Survey (TNCS). This increasemay be due, in large part, to changes in clothingstyles and greater exposure to sunlight than wascustomary years ago.
Ultraviolet radiation has also been associatedwith the far more serious skin cancer, malignantmelanoma. However, the data are less convinc-ing since the distribution of cancers on the bodydoes not directly correspond to the degree of ex-posure. In 1978, there were approximately 6,000deaths from malignant melanoma in the UnitedStates. ACS (6) estimates that there will be14,300 new cases and 6,700 deaths from mela-noma in 1981. Melanoma is the leading cause ofdeath from all diseases of the skin and is unques-tionably increasing in frequency.
Incidence and mortality rates from skin can-cer in different countries correlate fairly closely

Ch. 3—Factors Associated With Cancer ● 103
with the intensity of ultraviolet radiation. Thedisease is most prevalent in people receivinglarge amounts of sunlight, and it is a recognizedoccupational hazard for individuals workingoutdoors. The maps prepared by Mason, et al.(223), which depict average age-adjusted cancermortality rates on a county-by-county basis,convincingly demonstrate higher risk of skincancer in the Southeast United States. TNCSfound the annual incidence rate for nonmela-noma skin cancer to be 539/100,000 in theDallas-Fort Worth, Tex., area as compared to174/100,000 in Iowa.
An individual’s risk of developing skin canceris strongly influenced by genetic makeup. Ahigher risk exists for those with phenotypiccharacteristics such as fair complexion, light eyeand hair color, and poor ability to tan. By con-trast, skin cancer is very rare in deeply pig-mented populations. In addition, several dif-ferent types of chemicals can augment the carci-nogenic properties of ultraviolet radiation, in-cluding some used as medications and in cos-metics.
As discussed in the Air Pollution section, theuse of chlorofluorocarbons has been restrictedin the United States because of the belief thatthey may react in the stratosphere to reduce thethickness of the ozone layer and cause an in-crease in ultraviolet radiation reaching the sur-face of the Earth. NAS (70) estimated thatglobal release of chlorofluorocarbons at 1977rates could result in several hundred thousandadditional cases of nonmelanoma skin cancerand several thousand melanomas in the nextcentury. (For additional information on thepossible carcinogenic impact from release ofchlorofluorocarbons, see Air Pollution. )
Higginson and Muir (166) estimated that 10percent of male and female cancers in the Bir-mingham and West Midland region of Englandcould be attributed to sunlight. Doll and Peto(93) attribute 90 percent of lip cancers (in con-junction with smoking), 50 percent or more ofmelanomas, as well as 80 percent of other skincancers to ultraviolet radiation. This accountsfor between 1 and 2 percent of all cancer deathsif these proportions are applied to 1978 U.S.cancer deaths.
Ionizing Radiation
About half of the average U.S. exposure toionizing radiation comes from natural sources.Of the remainder, most comes from diagnosticmedical exposures, and smaller amounts comefrom medical therapy, occupational exposures,and from radioactive pollutants. (Those ex-posures are discussed in Medical Drugs and Ra-diation, Occupation, and Air Pollution, respec-tively. ) Cosmic rays and the minute amounts ofradioactive isotopes that occur in our bodiesand in all natural materials are the majorsources of natural background radiation.
The quantitative dose-response relationshipbetween cancer and low-level ionizing radiationhas been the cause of much debate. Until 30years ago, it was commonly assumed that ioniz-ing radiation did not cause cancer unless the ex-posures were high enough to cause clinicallydetectable damage to the irradiated tissue. Thisassumption is now known to be false, althoughthe dose-response relationship at low levels isstill not known with certainty.
Organs and tissues differ in their susceptibili-ty to carcinogenic effects induced by radiation.Leukemia was the first form of cancer associatedwith exposure to ionizing radiation, but we nowknow that cancer may be induced by radiationin many tissues of the human body and that therisk of inducing solid tumors exceeds that of leu-kemia (268). The major cancer sites affected arethe breast in women and the thyroid, lung, anddigestive organs in both sexes. Solid tumorshave a longer latency period (10 to more than 30years) than the few years before the excess riskfor leukemia manifests itself. The total cancerrisk from radiation is greater for women thanmen, principally because of the contribution ofbreast cancer.
More information is available on the dose-response relationship between radiation andcancer than any other, but there is still muchcontroversy over the appropriate extrapolationmodel to use for estimating the cancer risk fromionizing radiation. In July 1980, NAS officiallyreleased BEIR III (268). The estimates for therisks from ionizing radiation used by BEIR 111were derived principally from human experi-

104 ● Technologies for Determining Cancer Risks From the Enviromnent
ences with much higher doses than most peoplereceive. The most important of these are datafrom populations exposed to atomic blasts inHiroshima and Nagasaki, patients exposed totherapeutic radiation, and various occupationalgroups such as uranium miners and radiumwatch dial painters. Disagreement persists in thefield of radiation carcinogenesis over the appro-priateness of these high-exposure populationsfor estimating low-level risks.
The development and release of the BEIR 111report illustrates the diverging and changingopinions concerning the appropriate methodol-ogy for extrapolating from the measured effectsof high doses of ionizing radiation to the mostprobable effects of low doses. A draft of theBEIR 111 report was released for public commentin May 1979 but was retracted when it waslearned that a majority of the committee sup-ported a model different from the one presented.
Some members of the committee felt that forlow doses, a linear model overestimated the riskand a pure quadratic model, which estimates alower risk, could be used as a lower bound.However, others felt that the linear model wasmore accurate. Because of this disagreement, aconsensus panel was assembled and it adoptedthe linear-quadratic model: the pure quadraticmodel produces the lowest estimate, the linearthe highest, and the linear-quadratic estimatesan intermediate risk. Depending on which mod-el is used, estimates of mortality from all formsof cancer will differ by about one order of mag-nitude.
The committee also could not agree on wheth-er the cancer risk from radiation would have anadditive or multiplicative effect on the generalcancer rate. Throughout the report, excess riskis given as both an absolute (additive) and as arelative risk. The relative approach assumesthat the excess risk increases gradually and con-tinuously, proportional to the spontaneous risk,which increases with age for nearly all cancers.The absolute approach assumes a constant num-ber of additional cancers throughout life.
The BEIR III report (268) makes various at-tempts at estimating cancer risk from different
types of exposure but does not quantify the riskfrom low-dose radiation:
. . . the degree of risk is so low that it cannot beobserved directly and there is great uncertaintyas to the dose-response function most appro-priate for extrapolating in the low-dose region.
It further states:
It is by no means clear whether dose rates ofgamma or x radiation of about 100 mrads/yr arein any way detrimental to exposed people . . .
For the purpose of this assessment, the risksderived for continuous lifetime exposure to 1rad/yr of low-dose (gamma or X-ray) radiationis the most relevant, though it is an order ofmagnitude higher than average natural back-ground radiation. Table 21 displays both abso-lute and relative risk estimates generated byBEIR III.
The BEIR III report estimated that the averagewhole body dose of natural background radia-tion in the United States is approximately 100mrem/yr. The dose of radiation received varieswith altitude and geographical location. Using afigure of 220 million Americans, one can esti-mate that the population as a whole would beexposed to 22 million person-rem of back-ground radiation.3 Although BEIR III did not at-tempt to estimate the risk of cancer induced bylow-dose radiation, it would not be incorrect tocompute an upper limit of risk from the linearmodel since this is the only model whichassumes that dose and effect are proportional.Using the range of risk estimates, 158-403 ex-cess cancer deaths per million persons per rad,yields estimates of 3,476 and 8,866 cancerdeaths per year attributable to backgroundradiation. These figures represent between 0.9and 2.2 percent of all cancer deaths, and arecomparable with 3-percent estimates by Doll
31n 1972, EPA estimated that the average dose of natural back-ground radiation for a person living in the United States is 130mrem. Based on this estimate, the Interagency Task Force on theHealth Effects of Ionizing Radiation estimated that the U.S. pop-ulation is exposed to 20 million person-rem, but this is in error be-cause dividing 20 million person-rem by 130 mrem produces aquotient of 154 million people. The population is nearer 22omillion.

Ch. 3–Factors Associated With Cancer ● 105
and Peto (93) and Jablon and Bailar (191). The zero, in keeping with risks derived from otherlower estimate can be considered to approach models, including the quadratic model.
Table 21 .—Estimates of Excess Cancer Mortality From Continuous Exposureto 1 Rad/Year of Low-Level (background-type) Radiation by Three Dose-Response
Models and Two Risk Projection Models
Estimates of excess annual cancer mortality from continuous exposure to 1 rad/yearof low-level (background-type) radiation (excess deaths/million exposed and percentage of
normal expectation of cancer deaths)
Risk projection model
Dose-response model Absolute Relative
Normal expectation ofcancer deaths 167,300 167,300
Linear quadratic Excess deaths: number 4,751 12,920Percent of normal 2.8 7.7
Linear Excess deaths: number 11,250 30,520Percent of normal 6.7 18.2
Quadratic Excess deaths a a
aNot calculated because estimates very close to zero
Estimates of excess lifetime cancer mortality from continuous exposure to 1 rad/yearof low-level (background-type) radiation (excess deaths/million exposed)
Dose-response m o d e lRisk projection model
Absolute Relative
Linear quadratic 67 182Linear 158 403Quadratic — —
SOURCE: Tables adapted from (270)
INFECTION
Infection, particularly viral infection, haslong been thought to be a cause of cancer. Thisidea is partially based on the observation thatneoplasms appear in many animal species fol-lowing viral infections, and specific animaltumor viruses have been convincingly identi-fied. However, epidemiologic evidence indicatesthat cancer is not a contagious disease. Peoplewho come into close contact with cancer pa-tients, such as nurses, doctors, and spouses ofpatients, are at no higher risk of developing thedisease than others. Reports are occasionallypublished of the occurrence of an unusuallylarge number of cases of rare cancers, but suchclusters can be expected to occur periodically bychance. It is more plausible that certain virusesexist which are important in the development of
some types of cancer, but that they are wide-spread in the community. It is probably not thevirus itself, but a variety of other factors whichdetermine whether the virus will lead to the de-velopment of the disease. These may includegenetic and hormonal factors, chemical carcino-gens, and defective immune mechanisms, whichappear to exert an effect in only a small propor-tion of those exposed.
The strongest evidence implicating a viral in-fection in human cancer causation concernsEpstein-Barr virus (EBV) and hepatitis B virus,believed responsible for several cancer typeswhich are relatively rare in the United States.Epstein-Barr is a herpesvirus which is stronglyassociated with Burkitt’s lymphoma and naso-

106 ● Technologies for Determining Cancer Risks From the Environment
pharyngeal carcinoma (93,304). EBV occursubiquitously and is known to be the specificcause of infectious mononucleosis. It is postu-lated that the viral DNA integrates into the ge-netic material of a human stem cell and that cellbecomes the parent of a malignant clone. Epi-demiologic data and the detection of Epstein-Barr viral DNA in lymphoma cells supports theassociation between the virus and these twocancers. The association with nasopharyngealcarcinoma, found in the Far East, is not sostrong as with Burkitt’s Iymphoma, which oc-curs mainly in children in central Africa andNew Guinea. Nasopharyngeal carcinoma is be-lieved to involve a stronger genetic component,since Chinese migrating to the United Stateshave a much higher incidence of the disease thanU.S. whites and blacks, but the rate is lowerthan among Chinese remaining in the Far East(128). The unusual geographical distributionsuggests that the virus may act as a cocarcino-gen and that additional factors, such asimmunosuppression as a result of malaria, maybe involved.
Hepatitis B virus is associated with chronicliver infection which often advances to hepa-tocarcinoma. A greater prevalence of activehepatitis B infection has been demonstrated inpatients with primary hepatocellular carcinomaas compared with matched controls and the gen-eral population (304). The virus is believed to bethe initiating agent, but promoting agents suchas aflatoxin may be important cofactors (304).Two other herpesviruses are suspected of beingassociated with cancer: herpes simplex virustype 2 with cervical cancer, and less closely,cytomegalovirus with prostatic and cervicalcancers.
The vast majority of human cancers are notcharacterized by the presence of viral DNA inthe genetic material of cells. This may, ofcourse, be because the methods currently usedto detect the presence of a virus are not suffi-ciently sensitive, or it may be that viruses arenot often associated with cancer.
Doll and Peto (93) suggest that viral infectionmay eventually be shown to be an essential fac-tor in the production of some cancers:
●
●
●
●
If
cancer of the uterine cervix—women withmultiple partners are at high risk (see Sex-ual Development, Reproductive Patterns,and Sexual Practices);cancer of the penis—wives of penis cancerpatients are at high risk for cancer of theuterine cervix;acute lymphatic leukemia in children—dis-ease may recur in donor cells after a mar-row transplant; andreticulosarcoma —occasional appearanceshortly after receiving doses of immuno-suppressive drugs.
all of the above cancers depended on viralinfection, the proportion of cancers attributableto infection would be about 4 percent (93). Theproportion may be considerably larger if, likediet, infectious agents act by indirect means tocontribute to the production of cancers. Virusesmay promote the development of cancer bycausing tissue death, thereby stimulating thedivision of stem cells and sensitizing them to theaction of chemical carcinogens. It is possible forinstance, that this is the mechanism wherebyhepatitis B virus is associated with the develop-ment of liver cancer.
Infection with bacteria or parasites may alsocontribute to the production of cancer. The Dietsection discusses the possible role of intestinalbacteria in producing or destroying carcino-genic metabolizes in the large bowel and ofsalivary duct bacteria in converting nitrates intonitrites and hence facilitating the formation ofN-nitroso compounds in vivo. Bacterial infec-tion associated with the development of chronicbronchitis has been thought to increase the riskof lung cancer in cigarette smokers (93), pos-sibly by impairing the efficiency of the mecha-nism for clearing the bronchi and hence permit-ting more prolonged contact between inspiredcarcinogens and the bronchial stem cells. Asimilar role for infection may also explain theassociation between ulcerative colitis and col-orectal cancer, and that between schistosomi-asis, a parasitic infection of the bladder com-mon in parts of Africa, and the development ofbladder cancer.
Ch. 3–Factors Associated With Ca/leer ● 107
The examples cited are unlikely to be the onlyways in which infection affects the risk of de-veloping cancer; but even if they were, the rangeof estimates for its contribution to the overallcancer rate would be large. Rapp (304) specu-lated that if herpesviruses are eventually shownto be involved in all cancers of the male andfemale genitourinary systems, then those withactive venereal disease would have a 1 per70-100 risk of developing the disease:
This estimate is based on the number of newgenitourinary cancer cases per year in the UnitedStates (100,000 for females and 70,000 for males)in a population containing about 14 million ac-tive cases . . . of venereal disease due to herpes-viruses.
If one applies this reasoning to 1978 U.S. cancerdeaths, approximately 15 percent of all cancer
mortality would be associated with infection.This estimate is extremely tentative—there ismuch more certainty around the associationwith cervical cancer than other genital sites.Doll and Peto (93) suggested a figure about 10percent as a very uncertain best estimate, withina very wide range of acceptable estimates, of theproportion of cancer deaths attributable to in-fection, distributed as follows:
. . . 5% perhaps attributable to the action ofviruses and a token figure of 5% to allow for thepossible role of other infective agents in deter-mining the conditions under which cancer is pro-duced in vivo. The likely role of infectiousagents in the etiology of cancer of the uterinecervix provides a lower limit of at least 1%, butwe can at present make no useful guess at the up-per limit.
OTHER OR UNKNOWN ASSOCIATIONS
Two basic classes of “other” associations willbe considered:
1. Associations with cancers which as yet re-main unidentified, but which, when eluci-dated, will most likely fall into categoriesthat have been discussed in this chapter.
2. Associations of agents or exposures withcancers of the future. These may havebeen introduced recently, but have not yetproduced cancers, or may be introducedin the future.
Causes of Cancers Occurring Today
The agents associated with and/or responsi-ble for many of today’s cancers have not beenidentified. For example, although cancers of thebreast, colon, rectum, and stomach are associ-ated in some way with dietary factors, a causalrelationship has not been found for cancers atthose sites. Additionally the incidence of somecancers, myelomatosis and non-Hodgkins lym-phoma, for example, appear to be increasingbut no evidence associates those cancers witheven a broad category of factors.
The search for environmental factors asso-ciated with cancer will undoubtedly continue.Observed differences in rates between popula-tions, within countries, and through inter-national comparisons will result in advancingnew hypotheses and promoting further studies.
Some suggested associations that were notdiscussed above are likely to be further in-vestigated, but currently few data exist aboutthem. Biological factors, like immunologic con-trol, may normally limit the onset of disease,and a breakdown of this mechanism which maybe brought on by an environmental agent, couldincrease the propensity for cancer development.Similarly, psychological factors such as stressmay create an internal milieu suitable for tumorgrowth. There is some animal evidence to sup-port this hypothesis but it is limited. Studies ofpatients in mental hospitals are not supportiveof an increased risk (93). Psychological stressdoes have a recognized role in causing people tosmoke, drink, overeat, and take part in otherharmful activities which may directly or indi-rectly increase their risk of cancer.
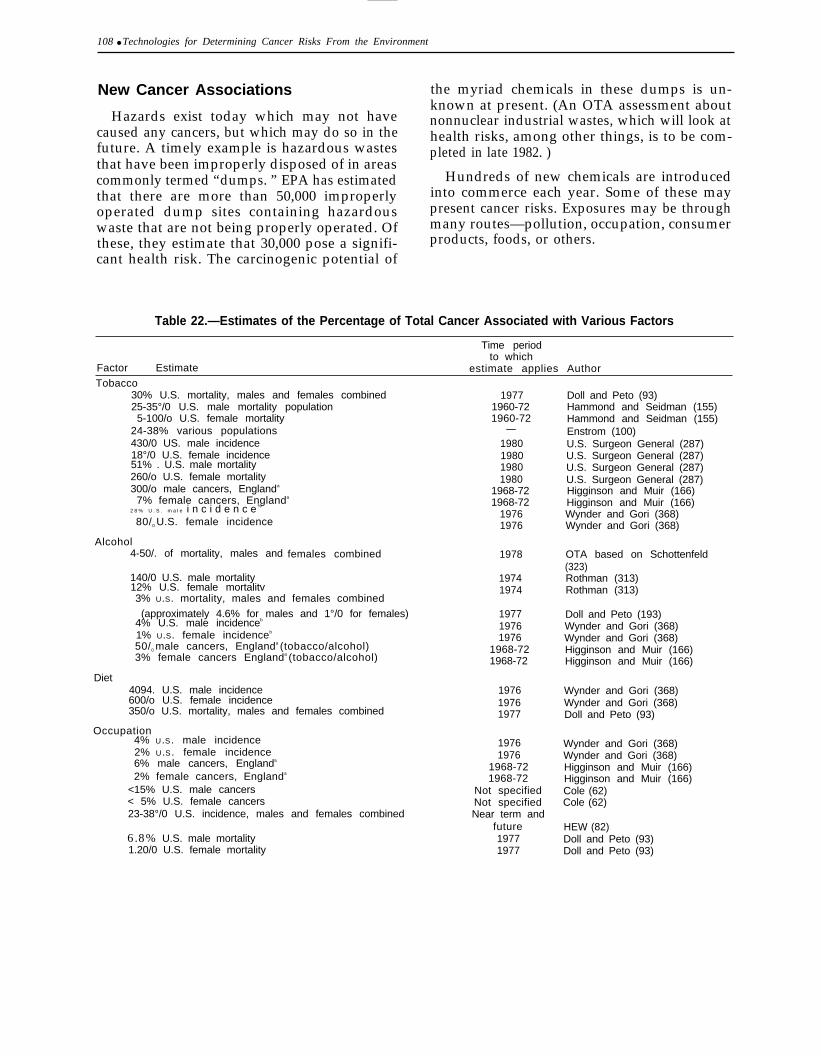
108 ● Technologies for Determining Cancer Risks From the Environment
New Cancer Associations
Hazards exist today which may not havecaused any cancers, but which may do so in thefuture. A timely example is hazardous wastesthat have been improperly disposed of in areascommonly termed “dumps. ” EPA has estimatedthat there are more than 50,000 improperlyoperated dump sites containing hazardouswaste that are not being properly operated. Ofthese, they estimate that 30,000 pose a signifi-cant health risk. The carcinogenic potential of
the myriad chemicals in these dumps is un-known at present. (An OTA assessment aboutnonnuclear industrial wastes, which will look athealth risks, among other things, is to be com-pleted in late 1982. )
Hundreds of new chemicals are introducedinto commerce each year. Some of these maypresent cancer risks. Exposures may be throughmany routes—pollution, occupation, consumerproducts, foods, or others.
Table 22.—Estimates of the Percentage of Total Cancer Associated with Various Factors
Time periodto which
Factor Estimate estimate applies AuthorTobacco
30% U.S. mortality, males and females combined25-35°/0 U.S. male mortality population5-100/o U.S. female mortality
24-38% various populations430/0 US. male incidence18°/0 U.S. female incidence51% . U.S. male mortality260/o U.S. female mortality300/o male cancers, Englanda
7% female cancers, Englanda
19771960-721960-72
—1980198019801980
1968-721968-72
2 8 % U . S . m a l e i n c i d e n c e %
80/0 U.S. female incidence
Alcohol4-50/. of mortality, males and
140/0 U.S. male mortality12% U.S. female mortalitv
19761976
females combined 1978
19741974
3% U.S. mortality, males and females combined
(approximately 4.6% for males and 1°/0 for females)4% U.S. male incidenceb
1% U.S. female incidenceb
50/0 male cancers, Englanda (tobacco/alcohol)3% female cancers Englanda (tobacco/alcohol)
Diet4094. U.S. male incidence600/o U.S. female incidence350/o U.S. mortality, males and females combined
Occupation4% U.S . male incidence2% U.S . female incidence6% male cancers, Englanda
2% female cancers, Englanda
<15% U.S. male cancers< 5% U.S. female cancers23-38°/0 U.S. incidence, males and females combined
6.8% U.S. male mortality1.20/0 U.S. female mortality
197719761976
1968-721968-72
197619761977
19761976
1968-721968-72
Not specifiedNot specifiedNear term and
future19771977
Doll and Peto (93)Hammond and Seidman (155)Hammond and Seidman (155)Enstrom (100)U.S. Surgeon General (287)U.S. Surgeon General (287)U.S. Surgeon General (287)U.S. Surgeon General (287)Higginson and Muir (166)Higginson and Muir (166)Wynder and Gori (368)Wynder and Gori (368)
OTA based on Schottenfeld(323)Rothman (313)Rothman (313)
Doll and Peto (193)Wynder and Gori (368)Wynder and Gori (368)Higginson and Muir (166)Higginson and Muir (166)
Wynder and Gori (368)Wynder and Gori (368)Doll and Peto (93)
Wynder and Gori (368)Wynder and Gori (368)Higginson and Muir (166)Higginson and Muir (166)Cole (62)Cole (62)
HEW (82)Doll and Peto (93)Doll and Peto (93)
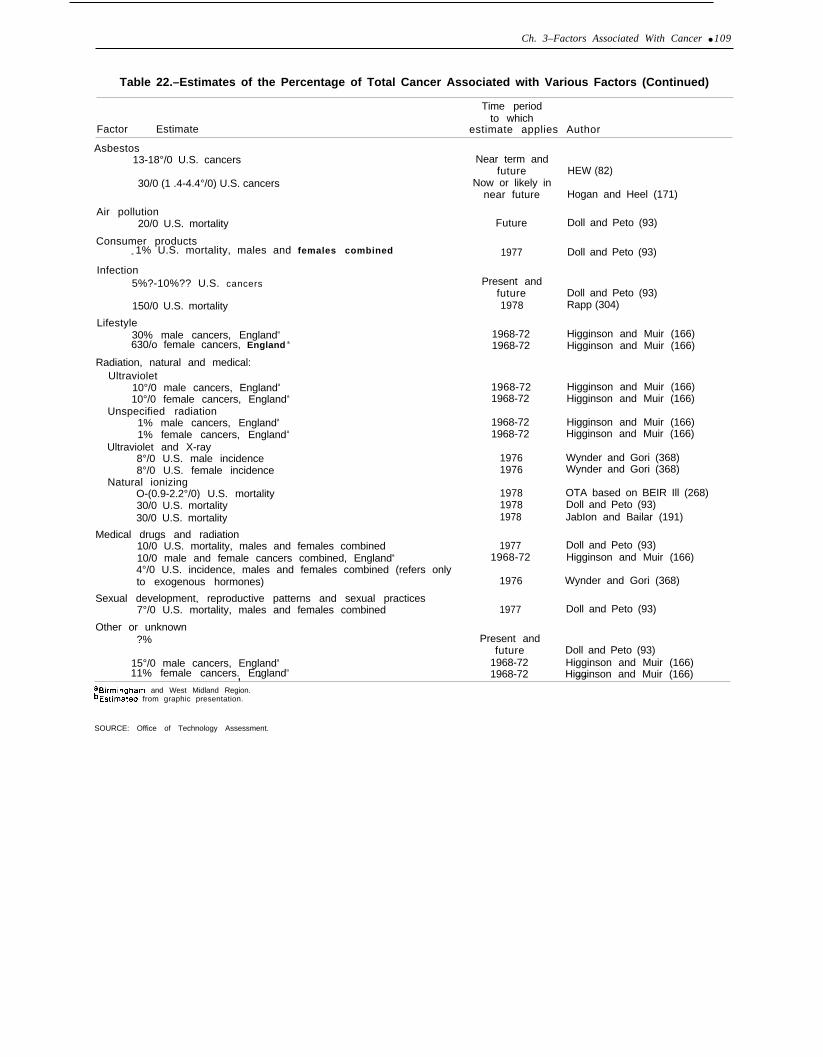
Ch. 3–Factors Associated With Cancer ● 109
Table 22.–Estimates of the Percentage of Total Cancer Associated with Various Factors (Continued)
Time periodto which
Factor Estimate estimate applies Author
Asbestos13-18°/0 U.S. cancers
30/0 (1 .4-4.4°/0) U.S. cancers
Air pollution20/0 U.S. mortality
Consumer products< 1% U.S. mortality, males and females combined
Infection5%?-10%?? U.S. cancers
150/0 U.S. mortality
Lifestyle30% male cancers, Englanda
630/o female cancers, England a
Radiation, natural and medical:Ultraviolet
10°/0 male cancers, Englanda
10°/0 female cancers, Englanda
Unspecified radiation1% male cancers, Englanda
1% female cancers, Englanda
Ultraviolet and X-ray8°/0 U.S. male incidence8°/0 U.S. female incidence
Natural ionizingO-(0.9-2.2°/0) U.S. mortality30/0 U.S. mortality30/0 U.S. mortality
Medical drugs and radiation10/0 U.S. mortality, males and females combined10/0 male and female cancers combined, Englanda
4°/0 U.S. incidence, males and females combined (refers onlyto exogenous hormones)
Sexual development, reproductive patterns and sexual practices7°/0 U.S. mortality, males and females combined
Other or unknown?%
15°/0 male cancers, Englanda
11% female cancers. Englanda
Near term andfuture
Now or likely innear future
Future
1977
Present andfuture1978
1968-721968-72
1968-721968-72
1968-721968-72
19761976
197819781978
19771968-72
1976
1977
Present andfuture
1968-721968-72
HEW (82)
Hogan and Heel (171)
Doll and Peto (93)
Doll and Peto (93)
Doll and Peto (93)Rapp (304)
Higginson and Muir (166)Higginson and Muir (166)
Higginson and Muir (166)Higginson and Muir (166)
Higginson and Muir (166)Higginson and Muir (166)
Wynder and Gori (368)Wynder and Gori (368)
OTA based on BEIR Ill (268)Doll and Peto (93)JabIon and Bailar (191)
Doll and Peto (93)Higginson and Muir (166)
Wynder and Gori (368)
Doll and Peto (93)
Doll and Peto (93)Higginson and Muir (166)Higginson and Muir (166), - - -
aBlrmlngham and West Midland Region.bEstimated from graphic presentation.
SOURCE: Office of Technology Assessment.