farmakologi umum2.ppt
TRANSCRIPT

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 1/51
1
Pharmacology:Pharmacokinetics : what the body does tothe drug (absorption, distribution,biotransformation, and excretion)Pharmacodynamics : what the drug does tothe body

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 2/51
2

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 3/51

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 4/51
4
Passive membrane transport is directlyproportional to:
Drug concentration gradient across themembrane.Lipid: water partition coefficient.Cell surface areaDifferences in pH

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 5/51
5
Lipid Mucosal Barrier
pH = 1.4
pH = 7.4
Gastric Juice
Plasma
HA[1] [1000] [1001]
Total
[HA]+[A] A - + H +
HA[1] [1000]
A - + H +[1001]
HA A-
+ H+
pK
a=
4.4Weak acid nonionized ionized

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 6/51
6
Active membrane transport:
Requirement for energy. Against electro-concentration gradient.Saturability.Selectivity.Inhibited by cotransported compounds.

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 7/51

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 8/51
8
Transporter proteins (TP):
There are two major TP superfamilies: 1) ABC (ATPbinding cassete); 2) SLC (Solute carriers).The SLC type of transporter mediate either uptake orefflux, whereas ABC transporters mediate only
unidirectional efflux.Most ABC proteins are primary active transporters,which rely on ATP hydrolysis to actively pump theirsubstrates across. Among the best known transporter inthe ABC superfamily is P glycoprotein (P-gp, also termedby MDR1, encoded by ABCC7).It is an important effluxtransporter in hepatocyte, brain capillaries, andenterocyte.

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 9/51
9
Transporter Proteins (TP):
SLC superfamily includes genes that encodefacilitated transporters and ion-coupled secondaryactive transporters that reside in various cellmembrane.Many serve as drug targets or in drug absorptionand disposition. Widely recognized transportersinclude the serotonin and dopamine transporters.Drug transporters operate in pharmacokinetic andpharmacodynamic pathways, including pathwaysinvolved in both therapeutic and adverse effects.
8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 10/51

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 11/51
11
Administration
A knowledge of the advantages anddisadvantages of the different routes is ofprimary importance in deciding the choice ofadministration: oral, sublingual, suppository,inhalation, local, topical, intravenous,intramuscular, subcutan, etc.

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 12/51
12
Bio-availability (1)
The rate & the amount of administereddrug reaches the systemic circulation intactThe rate depends on pharmaceuticalfactors and GI absorption, the extentdepends on the extent of absorption andthe extent of pre-systemic metabolism

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 13/51
13
Bio-availability (2)
Dosage form of a drug from differentmanufacturers sometimes differed in theirbioavailabilityRectal solution, but not suppositoryformulation, is absorbed better than oralformulation, and the potential for first pass-
metabolism is less potential
8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 14/51
14
Distribution (1)
Unbound drug is distributed into interstitial andcellular fluidsThe rate and the extent of a drug distributedinto extra vascular fluids depend onphysiological factors, physiochemical properties,and the extend of its binding to plasma proteinsTwo phases of distribution: faster and slowerLipid solubility is an important determinant oftissue uptake

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 15/51
15
Distribution (2)
Highly bound drug will yield an increase inunbound fraction in cases or renalimpairment, the last trimester of
pregnancy, displacement by other drugsand saturability of protein bindingBBB restricts the entry of drugs into CFSand CNS extra cellular spaceTermination drug effect may also resultfrom redistribution

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 16/51
16
Distribution of drugs into and out of CNS
It is unique because functional barriers are presentBrain capillary endothelial cells have continuous tight
junctionThe unique precapillary cells also contribute to BBB
At the choroid plexus a similar barrier is also present.The lipid solubility and the unbound of the drug isdeterminant of its uptake by the brainEfflux carrier is another important factor in functional
BBBDrugs also exit CNS along the flow of CFS through villi

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 17/51
17
Placental Transfer
Drug may cause congenital anomaliesLipid solubility, extend of plasma binding, anddegree of ionization are determinant of the transfer
Fetal plasma is slightly more acidic (pH 7.0-7.2), sothat ion trapping of basic drugs occurP-glycoprotein is present in placentaThe view that placenta is an absolute barrier isinaccurate

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 18/51
18
Plasma Proteins (1)
Acidic drugs are bound to albuminBasic drugs are bound to acid glycoproteinThe binding is usually reversible
Drugs bound to plasma is determined by conc.,affinity, and number of binding sitesPlasma binding is saturable processWithin the therapeutic ranges the unbound fraction
is relatively constant.Hypoalbuminemia results in reduced binding
8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 19/51
19
Plasma Protein (2)
Elevated levels of acid glycoprotein enhance bindingof basic drugsDrugs with similar physicochemical properties cancompete each other
Only unbound drug is in equilibrium acrossmembranesUnbound drug in intracellular water is the same asthat in plasma.Binding also limits glomerular filtration of the drug.

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 20/51
20
Fat as Reservoir
Lipid soluble drugs are stored in the neutral fatIn obese the fat content may be as high as 50% ofbody weight
Fat serves as an important reservoir for lipid solubledrugs. For example, 70% thiopental may be presentin body fat 3 hours after administration.Muscles, bones, and plasma proteins can serve as
drug reservoirs

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 21/51
21
Redistribution
From its site of action into other tissuesMay terminate drug effectThiopental is a good example

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 22/51
22
Biotransformation (1)
To generate more polar, inactive metabolites that arereadily excreted from the bodyClassified as phase I and Phase II reactions. Phase Iresults in the loss of pharmacological activity; phaseII lead to conjugate with endogenous compounds.Conjugates are highly polar, inactive, and rapidlyexcreted. Phase I is in ER: phase II is cytosolic.There are three major types of biotransformationreactions: oxidative, hydrolysis, and conjugation.
Cytochrome P450 1,2, and 3 families (GYP1, CYP2,and CYP3) are responsible for the oxidativemetabolism of numerous drugs

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 23/51
8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 24/51
24
Biotransformation (3)
Glucoronidation is quantitatively the most importantconjugation reation.UDP-glucoronyl transferases catalyze the tranfer of anactivated glucoronic acid molecule to form glucoronide
conjugates.The increased water solubility of the glucoronideconjugates promotes their renal elimination.Most phase II reactions are cytosolic, but UDP-glucoronyl tranferases are microsomal enzymes.
Acetylated metabolites often are less water soluble, thatprolongs their elimination from the body.

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 25/51
25
Factors affecting drug biotransformation(1)
A hallmark of drug metabolism is large variability. A combination of genetic, environmental, andphysiological factors are involved in regulation ofdrug biotransformation.The most important factors are geneticallydetermined polymorphism in drug oxidations andconjugations, concomitant use of other drugs,pollutants and chemicals, disease, and age. These
factors can decrease efficacy, prolong effects, orincrease toxicity.

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 26/51
26
Factors affecting drug biotransformation(2)
A number of genetic polymorphisms are exist: poor,intermediate, extensive, or ultrarapid metabolizer.
A polymorphism also occurs in N-acetyl transferaseGreater likelihood of type α side effects in poormetabolizer.Drugs and pollutants can induce the synthesis or inhibitthe action of CYP450 protein. Many CYP450 inducerscan also induce phase II biotransformation. Inhibitiondrug biotransformation enzymes results in elevated drugblood levels, prolonged pharmacological effects, and anincreased incidence of drug toxicity.
8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 27/51
27
Factors affecting drug biotransformation(3)
Impairment of liver function can alter hepatic drugbiotransformation.Decreases in hepatic blood flow can decrease thebiotransformation of drugs with high extraction ratio.In the elderly, metabolic capacity is reduced.Drug metabolizing enzymes develop early in fetal life, but thelevel even lower following 2-4 weeks postpartum.Induction of certain metabolizing enzymes occurs in the secondand third semester.Oral contraceptives are potent inhibitor of CYP450
8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 28/51
8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 29/51
29
Biliary, Fecal, and OtherExcretion
Organic anions including glucoronides, andorganic cations are actively transported by P-glycoprotein into bile. These metabolites may beexcreted in the feces; but more commonly theyare reabsorbed into the blood and ultimatelyexcreted in the urine.Drugs in breast milk are sources of unwanted
effects in nursing infant. Milk is more acidic,basic compounds may be slightly concentrated.

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 30/51
30
Pharmacodynamics
Is the study of the mechanism of action, thebiochemical and physiological effects ofdrugs, and the relationship between
concentration and effect

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 31/51

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 32/51
32

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 33/51
33
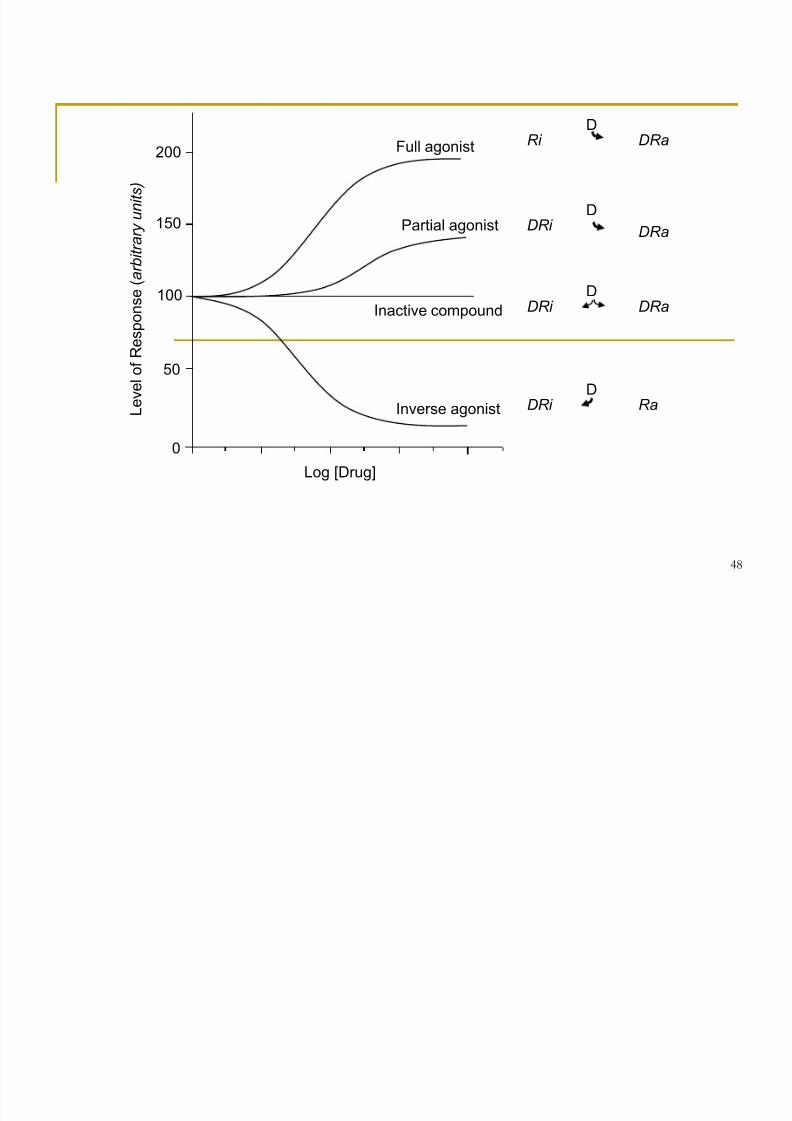
Drug Receptors
Proteins form the most important class of receptors. They serveas receptor for endogenous regulatory ligands.Many drugs act selectively on such physiological factorsDrugs that bind to physiological receptor and mimic the effect ofthe endogenous regulatory compounds are termed agonist.
Drugs that bind to receptors but do not mimic the effect ofendogenous agonist are termed antagonist .Drugs that are partly as effective as agonist are termed partialagonist.Drugs that stabilize the receptor from conformational changesare termed negative antagonist or inverse agonist.
8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 34/51

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 35/51
35
Physiological Function of Receptors
The function of physiological receptors consist of bindingappropriate ligand and, in response, propagating its regulatorysignals in the target cell.The regulatory actions of a receptor may be exerted directly onits cellular target, effector protein, or may be conveyed byintermediary cellular molecules, tranducers.The receptor, its cellular target, and any intermediary cellularmolecules are referred as receptor-effector system or signaltransduction pathway.The receptor act catalytically and hence are biochemical signal
amplifiers.

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 36/51
36
Structural and Functional Families ofPhysiological Receptors
Members of various classes of receptors and manyof the associated transducer and effector proteinhave been purified, and their mechanism of actionare understood in considerable biochemical detail.Receptors, transducers, and effectors can beexpressed via molecular genetic strategies andstudied in cultured cells. Alternatively, they can be
expressed in large amounts in cell of bacteria oryeast to facilitate their purification.
8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 37/51
37
Structural and Functional Families ofPhysiological Receptors (2)1. Receptor protein kinases (tyrosine phosphatase,
adenyl cyclase).2. Ion channels (nicotinic cholinergic, GABA)3. G-protein coupled receptors (for biologic amines,
eicosanoids, peptide hormones)4. Transcription factors (for steroid, thyroid, vit D,
retinoids) that regulate the the transcription ofspecific genes.
5. Cytoplasmic messengers (cyclic AMP, Ca ++).

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 38/51
38

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 39/51
39

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 40/51
40
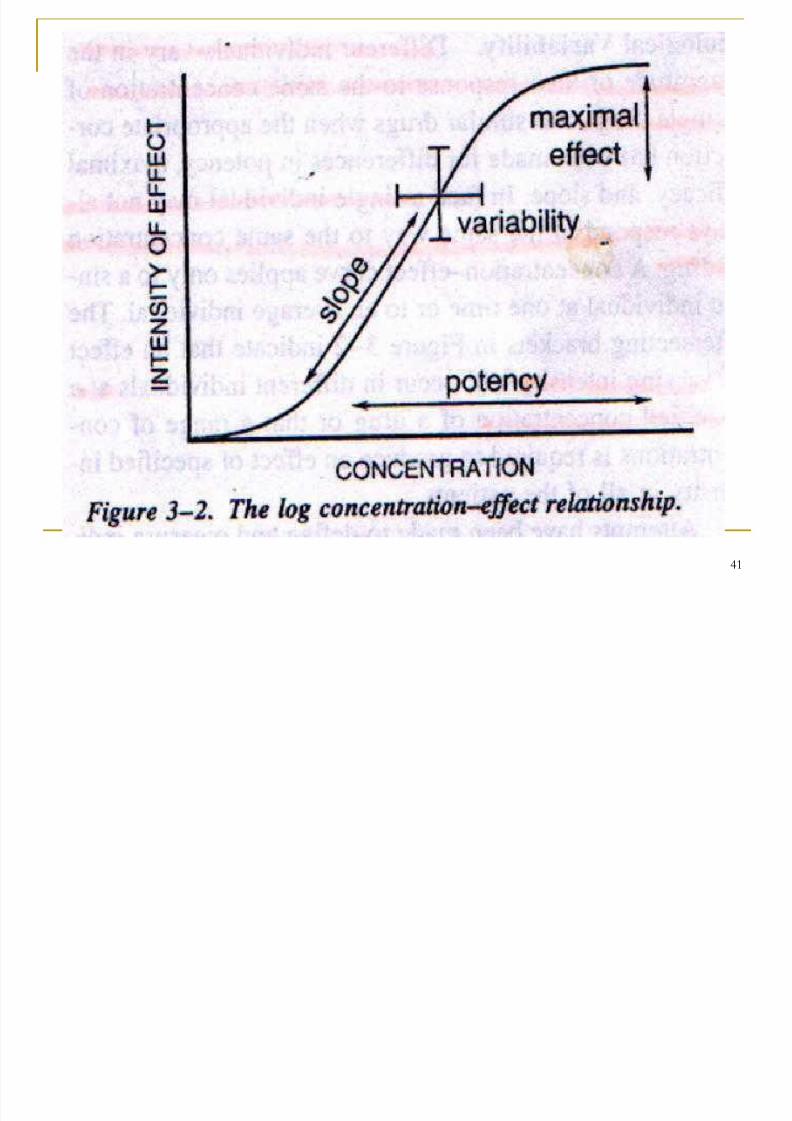
Quantitative Pharmacodynamics
The dose-response curve (DRC) depicts theobserved effect as a function of drug concentrationin the receptor. A dose-response curve is typified bya maximal asymptote value when all receptor siteswere occupied.
A DRC is plotted with the log concentration. A DRC has three basic properties: threshold, slope,and maximal asymptote.
A drug does two things to receptor: bind and changetheir behavior. Binding is governed by affinity;changing is governed by efficacy.
8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 41/51
41
8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 42/51
42
Receptor Occupancy Theory (1)
Ka A + R AR Stimulus Response
Response = receptor x efficacy x receptoroccupancy number(binding)
Efficacy=intrinsic activity= the power of the drug toinduce response.

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 43/51
43
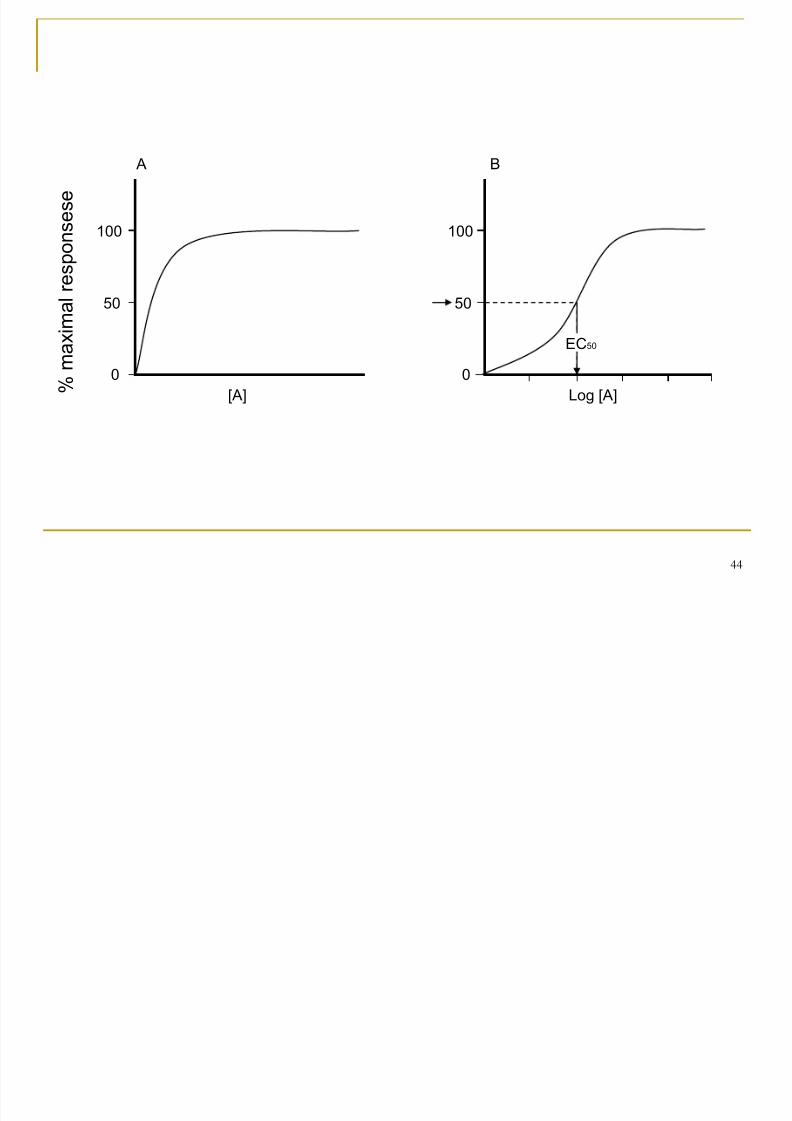
Receptor Occupancy Theory (2)
Stimulus is the initial effect of drug upon thereceptor itself.Stimulus is then transduced by the system to
yield observed response. Affinity is increased by the increase of K a .The fraction of receptors occupied by thedrug is determined by the concentration thedrug and K a .
8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 44/51
44
% m
a x i m a
l r e s p o n s e s e
[A] Log [A]
50
0
100
50
0
100
A B
EC 50
8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 45/51
45
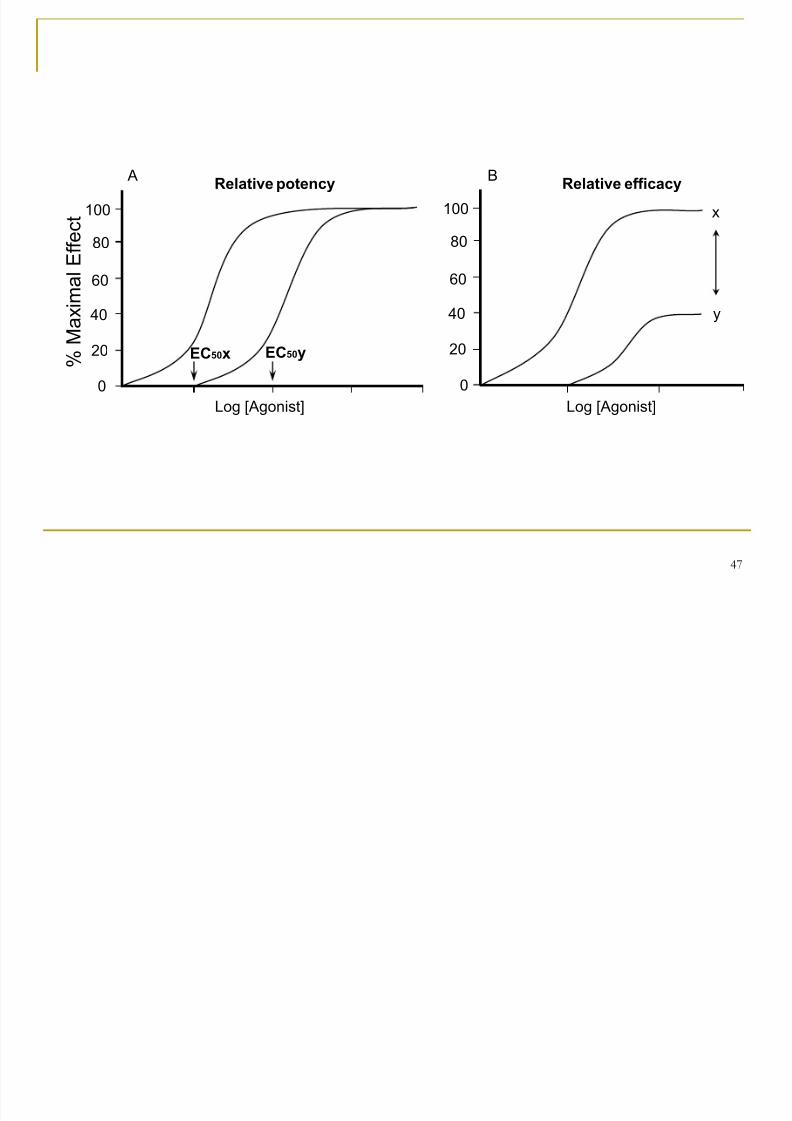
Quantifying Agonism
Drugs have two observed properties in biologicalsystems, i.e. potency and magnitude of effects,when a biological response is produced.
Potency is controlled by four factors: two relate tothe receptors (density and efficacy of the stimulusresponse), and the other two relate to the drug-receptor interaction (affinity and efficacy).

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 46/51
8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 47/51
47
% M
a x i m a
l E f f e c t
Log [Agonist] Log [Agonist]
40
0
80
A B
20
60
100
Relative potency
40
0
80
20
60
100
Relative efficacy
EC 50 x EC 50 y
x
y
8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 48/51
48
Full agonist
Partial agonist
Inactive compound
Inverse agonist
Ri
DRi
DRi
DRi
DRa
DRa
DRa
Ra
D
D
D
D
200
150
100
50
0
Log [Drug]
L e v e
l o f R e s p o n s e ( a r b
i t r a r y u n
i t s )

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 49/51
49

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 50/51
50

8/10/2019 Farmakologi Umum2.ppt
http://slidepdf.com/reader/full/farmakologi-umum2ppt 51/51