fat necrosis simulating breast malignancy following
TRANSCRIPT

Fat necrosis is a relatively common benign diseasethat can be the result of trauma (iatrogenic or noniatro-genic) or may have an idiopathic cause (1). Reductionmammoplasty also invokes extensive soft tissue injuryand this occasionally leads to fat necrosis. Fat necrosis isoften depicted on mammography as characteristicround calcifications with lucent centers (oil cysts) or asdense amorphous solid calcifications (2). On occasion,however, fat necrosis may have atypical imaging andphysical examination features that are indistinguishablefrom malignancy (3). We report a case of fat necrosissimulating malignancy by mammography and ultra-
sonography, which developed in the breast following re-duction mammoplasty.
Case Report
A 63-year-old woman was referred to our hospital dueto an abnormal density on a screening mammogram.The patient had received bilateral reduction mammo-plasty 10 months previously. The mammogram takenbefore the mammoplasty showed almost entirely fattybreasts without focal mass or clustered microcalcifica-tions. She has been receiving estrogen therapy for 2years. The mammogram taken on referral revealed anirregular high density with a spiculated margin in theleft upper inner quadrant (Fig. 1). Ultrasonographyshowed a 1.5 cm sized, ill-defined, and irregular hypoe-choic lesion with posterior acoustic shadowing at the 10o’clock position in the left breast, 3 cm away from thenipple (Fig. 2). Because of this suspicious imaging find-ing, ultrasonography-guided core biopsy using a 14-
J Korean Radiol Soc 2004;51:573-576
─ 573 ─
Fat Necrosis Simulating Breast Malignancy FollowingReduction Mammoplasty: A Case Report1
Yeong Mi Park, M.D., Eun Kyung Kim, M.D.2
1Department of Diagnostic Radiology, Busan Paik Hospital, InjeUniversity College of Medicine
2Department of Diagnostic Radiology, Severance Hospital, YonseiUniversity College of MedicineReceived July 23, 2004 ; Accepted September 16, 2004Address reprint requests to : Yeong Mi Park, M.D., Department ofDiagnostic Radiology, Busan Paik Hospital, Inje University College ofMedicine, 614-735, Gaekum-dong, Busanjin-gu, Busan, Korea.Tel. 82-51-896-6579 Fax. 82-51-896-1085 E-mail: [email protected]
Fat necrosis is well depicted on imaging by characteristic findings such as oil cysts.However it may be rarely indistinguishable from carcinoma clinically and radiological-ly, and require biopsy for diagnosis. We report a case of fat necrosis simulating malig-nancy following reduction mammoplasty. The screening mammogram of a 63-year-oldwoman, who had received bilateral reduction mammoplasties 10 months previously,showed an irregular high-density lesion with a spiculated margin in the upper innerquadrant of the left breast. Ultrasonography revealed a 1.5 cm sized, ill-defined, and ir-regular hypoechoic lesion with posterior acoustic shadowing. The confirm diagnosiswas fat necrosis, by ultrasonography-guided core needle biopsy. On the 6-month fol-low-up ultrasonography, the lesion was found to have decreased in size.
Index words : RadiographyFat, necrosis

gauge needle was performed (Fig. 3). A microscopic ex-amination showed aggregates of fat with dense fibrosisand inflammatory cells, suggestive of fat necrosis (Fig.4). There was no evidence of malignant cells. On the 6-month follow-up ultrasonogram, the lesion was found tohave decreased in size (Fig. 5).
Discussion
Reduction mammoplasty is increasing in popularity,and is usually performed for bilateral macromastia orfor symmetry after mastectomy and breast reconstruc-tion. Reduction mammoplasty involves elevating thenipple and resecting the skin and glandular tissue fromthe inferior aspect of the breast (4). The procedure cre-ates scars, fibrotic tissue and alterations in the involvedtissue, such as architectural distortion, hematomas, neo-calcifications, or skin thickening that may in some casesmimic a pathologic condition (5). Fat necrosis after re-duction mammoplasty has been reported in up to 10%-20% of cases (5, 6). Fat necrosis is of clinical concern be-cause it is difficult to distinguish from carcinoma onboth physical examination and radiologic images.
The process of fat necrosis results from aseptic saponi-fication of fat by blood and tissue lipases (7). These le-sions may contain both oily fat and hemorrhagic orserosanguineous fluid within the same compartment, asin oil cysts, which result in a fat-fluid layer effect (1).
This can be seen most often in the periareolar and in-ferior portions of the breast, where most surgical dissec-
tion occurs. Our patient, however, revealed fat necrosisin upper inner quadrant of the breast. Dissection for flapraising disrupts blood vessels and causes fat necrosis (8).Mandrekas et al suggested that the use of electrocauteryduring breast reduction might be a main cause of fatnecrosis (9).
Mammographic features associated with fat necrosisrange from lipid cyst to findings suspicious of malignan-cy (3). Oil cysts have been described as the most charac-
Yeong Mi Park, et al : Fat Necrosis Simulating Breast Malignancy Following Reduction Mammoplasty
─ 574 ─
Fig. 2. Ultrasonogram of the left breast revealing a 1.5 cmsized, ill-defined, and irregular hypoechoic lesion with posteri-or shadowing (arrows) in the 10 o’clock position in the leftbreast, 3 cm away from the nipple.
A B
Fig. 1. A, B. Mediolateral oblique (A)and craniocaudal (B) mammogramsshowing irregular high density with aspiculated border in the left upper in-ner quadrant (arrows).
teristic lesion associated with fat necrosis (6, 9). Fatnecrosis uncommonly manifests as focally clustered,pleomorphic microcalcifications that are mammographi-cally indistinguishable from those of malignancy (3). Italso appears as an ill defined or spiculated area of in-creased opacity where fibrosis predominates and pro-duces a desmoplastic response similar to that seen inscirrhous carcinoma (10), and should be included in thedifferential diagnosis of a spiculated mass in addition tocarcinoma, radial scar, and postbiopsy change (3).
By ultrasonography, small anechoic, well-defined sub-cutaneous lesions, which release a yellow oily fluid onaspiration, represent the oil cysts that are found in typi-cal fat necrosis (9). Soo et al (1) demonstrated a wide
range of the sonographic features of fat necrosis, whichincluded cystic, complex, and solid appearing masseswith circumscribed or ill-defined margins, often associ-ated with distortions of the normal sonographic archi-tecture. Moreover, distortion of parenchyma may beconfused with scarring in postsurgical cases (1, 9).
Short-term follow-up with imaging and physical exam-ination rather than immediate biopsy has been recom-mended, because within a year after reduction mammo-plasty parenchymal distortion and skin thickening sub-side and the breast achieves a new baseline appearance(9). Nevertheless, if a lesion has a suspicious imaging ap-pearance, a biopsy is necessary for confirmation.
The radiologist should be aware of imaging findings offat necrosis mimicking malignancy following reductionmammoplasty. Although breast imagings reveal suspi-cious findings in patients that have received reductionmammoplasty, a result of fat necrosis on needle biopsymay be acceptable, and short-term follow up (at 6months) with imaging rather than surgical interventionis recommended.
References
1. Soo MS, Kornguth PJ, Hertzberg BS. Fat necrosis in the breast:sonographic features. Radiology 1998;206:261-269
2. Mendelson EB. Evaluation of the postoperative breast. Radiol ClinNorth Am 1992;30:107-138
3. Hogge JP, Robinson RE, Magnant CM, Zuurbier RA. The mammo-
J Korean Radiol Soc 2004;51:573-576
─ 575 ─
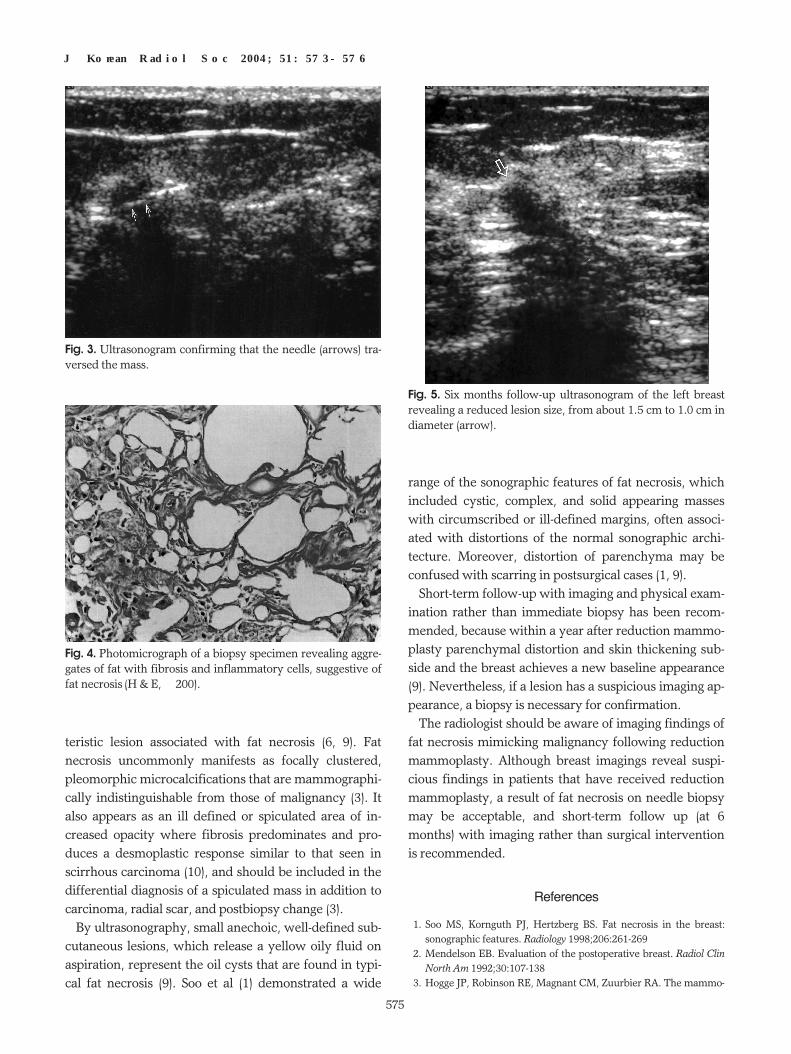
Fig. 5. Six months follow-up ultrasonogram of the left breastrevealing a reduced lesion size, from about 1.5 cm to 1.0 cm indiameter (arrow).
Fig. 3. Ultrasonogram confirming that the needle (arrows) tra-versed the mass.
Fig. 4. Photomicrograph of a biopsy specimen revealing aggre-gates of fat with fibrosis and inflammatory cells, suggestive offat necrosis (H & E, ×200).

graphic spectrum of fat necrosis of the breast. Radiographics 1995;15:1347-1356
4. Miller CL, Feig SA, Fos JW4th. Mammographic changes after re-duction mammoplasty. AJR Am J Roentgenol 1987;149:35-38
5. Miller JA, Festa S, Goldstein M. Benign fat necrosis simulating bi-lateral breast malignancy after reduction mammoplasty. SouthMed J 1998;91:765-767
6. Danikas D, Theodorou SV, Kokkalis G, Vasiou K, KyriakopoulouK. Mammographic findings following reduction mammoplasty.Aesthetic Plast Surg 2001;25:283-285
7. Frates MC, Homer MJ, Robert NJ, Smith TJ. Noniatrogenic breast
trauma. Breast Dis 1992;5:11-198. Mitnick JS, Roses DF, Harris MN, Colen SR. Calcifications of the
breast after reduction mammoplasty. Surg Gynecol Obstet 1990;171:409-412
9. Mandrekas AD, Assimakopoulos GI, Mastorakos DP, Pantzalis K.Fat necrosis following breast reduction. Br J Plast Surg 1994;47:560-562
10. Bassett LW, Gold RH, Cove HC. Mammographic spectrum oftraumatic fat necrosis: the fallibility of “pathognomonic”signs ofcarcinoma. AJR Am J Roentgenol 1978;130:119-122
Yeong Mi Park, et al : Fat Necrosis Simulating Breast Malignancy Following Reduction Mammoplasty
─ 576 ─
대한영상의학회지 2004;51:573-576
악성종양과 유사한 소견을 보인 유방축소술후 생긴 지방괴사: 증례 보고1
1인제대학교 의과대학 부산백병원 영상의학과학교실2연세대학교 의과대학 세브란스병원 영상의학과학교실
박 영 미·김 은 경2
지방괴사는 대부분 유성낭종과 같은 특징적인 영상소견을 보이지만 드물게 악성종양과 유사한 임상 및 영상소견
을 보일 수 있으며, 이 경우 감별진단을 위해 조직검사가 불가피하다. 저자들은 유방축소술 후 유방에서 발생한 악
성종양과 유사한 영상소견을 보인 지방괴사를 보고하고자 한다. 10개월 전 유방축소술을 받은 63세 여자환자의 유
방촬영술에서 좌측 유방의 상내측에 불규칙한 모양의 침상경계를 가진 고음영의 병소가 발견되었다. 유방초음파검
사상 1.5 cm 직경의, 경계가 불명확하고 불규칙한 모양을 보이며 후방음영감쇄가 동반된 악성종양의 소견을 보였
다. 초음파유도하조직검사를 시행하여 지방괴사로 진단되었으며, 6개월 후 초음파검사에서 크기가 줄어든 소견을
보였다.