fda arthritis advisory committee meeting fda opening remarks · patients from p2 and p3 studies:...
TRANSCRIPT

FDA Arthritis Advisory Committee MeetingFDA Opening Remarks
NDA 207924: Baricitinib for the treatment of adult patients with moderately to severely active rheumatoid arthritis who have
inadequate response to methotrexate
Nikolay P. Nikolov, M.D.Clinical Team Leader
Division of Pulmonary, Allergy, and Rheumatology ProductsU.S. Food and Drug Administration
April 23, 2018

2
Baricitinib
• Applicant: Eli Lilly & Co.• New Molecular Entity (NME)• Second in class for rheumatoid arthritis (RA)• Small molecule, Janus Kinase (JAK) inhibitor for oral
administration

3
Proposed Usage• Indication and Usage
– “Treatment of adult patients with moderately to severely active rheumatoid arthritis (RA) who have had an inadequate response or are intolerant to methotrexate (MTX).”
• Dosage and Administration– “The recommended dose is 2 mg once daily. For patients with an inadequate
response or intolerance to more than one disease modifying anti-rheumatic drug (DMARD), a dose of 4 mg once daily is recommended.
– Dose tapering to 2 mg once daily may be considered for patients who have achieved sustained control of disease activity with 4 mg once daily.”

4
Clinical Program: Phase 2 StudiesStudy Patient
population Study design
Treatment arm Patients per arm
Primary endpoint
JADC cDMARD-IR R, DB, PC Baricitinib 4 mgBaricitinib 7 mgBaricitinib 10 mgPBO
32323231
ACR20 at Week 12
JADA cDMARD-IR R, DB, PC Baricitinib 1 mgBaricitinib 2 mgBaricitinib 4 mgBaricitinib 8 mgPBO
4952525098
ACR20 at Week 12
JADN cDMARD-IR R, DB, PC Baricitinib 1 mgBaricitinib 2 mgBaricitinib 4 mgBaricitinib 8 mgPBO
2424242449
ACR20 at Week 12
cDMARD=conventional DMARD; IR=inadequate response; R=randomized; DB=double-blind; PC=placebo controlled; ACR=American College of Rheumatology; PG=parallel group; PBO=placebo

5
Clinical Program: Phase 3 StudiesStudy Patient
populationStudy design Treatment arms Patients
per arm Major endpoints
JADV MTX-IR R, DB, PC and AC52 weeks
Baricitinib 4 mg + MTXAdalimumab 40 mg QOW+ MTXPBO + MTX (→ Baricitinib 4 at Week 24)
Rescue to Bari 4 mg, starting at Week 16
488330487
ACR20, HAQ-DI atWeek 12mTSS at Week 24
JADX cDMARD-IR R, DB, PC24 weeks
Baricitinib 2 mg + cDMARDBaricitinib 4 mg + cDMARDPBO + cDMARD
Rescue to Baricitinib 4 mg, starting at Week 16
229227228
ACR20, HAQ-DI at Week 12
JADW TNF-IR R, DB, PC24 weeks
Baricitinib 2 mg + cDMARDBaricitinib 4 mg + cDMARDPBO + cDMARD
Rescue to Baricitinib 4 mg, starting at Week 16
174177178
ACR20, HAQ-DI at Week 12
JADZ Treatment naïve/early RA
R, DB, ACMTX titrated up to 20 mg weekly52 weeks
MTX Baricitinib 4 mgBaricitinib 4 mg + MTX
Rescue to Baricitinib 4 + MTX mg, starting at Week 24
213160215
ACR20, HAQ-DI at Week 24
JADY Patients from P2 and P3 studies
LTERW
Baricitinib 2 mg (patients from JADX and JADW)Baricitinib 4 mg
2539 SafetyEfficacy
MTX=methotrexate; AC=active controlled; IR=inadequate response; TNF=tumor necrosis factor; QOW=every other week; P2=phase 2; P3=phase 3

6
Clinical Program: Phase 3 StudiesStudy Patient
populationStudy design Treatment arms Patients
per arm Major endpoints
JADV MTX-IR R, DB, PC and AC52 weeks
Baricitinib 4 mg + MTXAdalimumab 40 mg QOW+ MTXPBO + MTX (→ Baricitinib 4 at Week 24)
Rescue to Bari 4 mg, starting at Week 16
488330487
ACR20, HAQ-DI atWeek 12mTSS at Week 24
JADX cDMARD-IR R, DB, PC24 weeks
Baricitinib 2 mg + cDMARDBaricitinib 4 mg + cDMARDPBO + cDMARD
Rescue to Baricitinib 4 mg, starting at Week 16
229227228
ACR20, HAQ-DI at Week 12
JADW TNF-IR R, DB, PC24 weeks
Baricitinib 2 mg + cDMARDBaricitinib 4 mg + cDMARDPBO + cDMARD
Rescue to Baricitinib 4 mg, starting at Week 16
174177178
ACR20, HAQ-DI at Week 12
JADZ Treatment naïve/early RA
R, DB, ACMTX titrated up to 20 mg weekly52 weeks
MTX Baricitinib 4 mgBaricitinib 4 mg + MTX
Rescue to Baricitinib 4 + MTX mg, starting at Week 24
213160215
ACR20, HAQ-DI at Week 24
JADY Patients from P2 and P3 studies
LTERW
Baricitinib 2 mg (patients from JADX and JADW)Baricitinib 4 mg
2539 SafetyEfficacy
MTX=methotrexate; AC=active controlled; IR=inadequate response; TNF=tumor necrosis factor; QOW=every other week; P2=phase 2; P3=phase 3

7
Clinical Program: Phase 3 StudiesStudy Patient
populationStudy design Treatment arms Patients
per arm Major endpoints
JADV MTX-IR R, DB, PC and AC52 weeks
Baricitinib 4 mg + MTXAdalimumab 40 mg QOW+ MTXPBO + MTX (→ Baricitinib 4 at Week 24)
Rescue to Bari 4 mg, starting at Week 16
488330487
ACR20, HAQ-DI atWeek 12mTSS at Week 24
JADX cDMARD-IR R, DB, PC24 weeks
Baricitinib 2 mg + cDMARDBaricitinib 4 mg + cDMARDPBO + cDMARD
Rescue to Baricitinib 4 mg, starting at Week 16
229227228
ACR20, HAQ-DI at Week 12
JADW TNF-IR R, DB, PC24 weeks
Baricitinib 2 mg + cDMARDBaricitinib 4 mg + cDMARDPBO + cDMARD
Rescue to Baricitinib 4 mg, starting at Week 16
174177178
ACR20, HAQ-DI at Week 12
JADZ Treatment naïve/early RA
R, DB, ACMTX titrated up to 20 mg weekly52 weeks
MTX Baricitinib 4 mgBaricitinib 4 mg + MTX
Rescue to Baricitinib 4 + MTX mg, starting at Week 24
213160215
ACR20, HAQ-DI at Week 24
JADY Patients from P2 and P3 studies
LTERW
Baricitinib 2 mg (patients from JADX and JADW)Baricitinib 4 mg
2539 SafetyEfficacy
MTX=methotrexate; AC=active controlled; IR=inadequate response; TNF=tumor necrosis factor; QOW=every other week; P2=phase 2; P3=phase 3

8
Efficacy Considerations• Both baricitinib doses, 2 mg and 4 mg once daily, are effective in reducing
signs and symptoms and improving physical function in patients with RA versus placebo– Higher ACR20, 50, 70 response rates versus placebo– Improvement in Health Assessment Questionnaire-Disability Index (HAQ-DI)
compared to placebo– Data not consistent in showing a meaningful benefit of 4 mg over the 2 mg dose
• Radiographic response– The data for 4 mg dose are robust– Some uncertainty about 2 mg dose, studied in only one study as an exploratory
endpoint

9
Safety Considerations• Serious infections, including H. zoster, opportunistic infections and
tuberculosis• Malignancy, including lymphoma and other malignancies• Thrombosis, both venous and arterial• Laboratory Abnormalities (often dose-dependent)
– Decrease in neutrophils and hemoglobin– Platelet elevations– Lipid elevations– Liver test elevations

10
Safety Data Limitations• Limited placebo-controlled data
– Duration of baricitinib versus placebo controlled data pre-escape was limited to 16 weeks
• Overall safety exposure data limited for baricitinib 2 mg vs 4 mg– Four of the seven phase 2 and 3 clinical studies included 2 mg and 4 mg baricitinib dose
arms – Patient escape/cross-overs
• Patients on placebo were switched or escaped to 4 mg of baricitinib• Patients who escaped from 2 mg baricitinib were placed on 4 mg of baricitinib• Patients who were eligible for escape from 4 mg of baricitinib remained on 4 mg of baricitinib
– Patients in study JADY who had a pre-defined response* to 4 mg of baricitinib were eligible to be randomized to 2 mg vs 4 mg of baricitinib
*CDAI≤10 for 3 months in study JADY or CDAI≤2.8 from study JADZ; patients originating from study JADA were not eligible

11
Benefits• Superior efficacy of both baricitinib
doses compared to placebo:– Signs and symptoms – Physical function – No consistent meaningful benefit of 4
mg over 2 mg• Radiographic response:
– Data for 4 mg dose are robust– Some uncertainty about 2 mg dose,
studied in only one study as an exploratory endpoint
Risks
• Serious infections• Herpes zoster, opportunistic
infections and TB• Malignancies• Thrombosis
– Both arterial and venous
• Laboratory abnormalities– Many dose-dependent, including
platelet elevations
Benefit-Risk Considerations

12
Regulatory History: Original Submission• Original NDA was submitted on January 14, 2016
– Indication: “Moderately to severely active rheumatoid arthritis (RA).”– Dosage and Administration: Proposed dose was 4 mg once daily, with an added notation
that “for some patients a dose of 2 mg once daily may be acceptable.”
• Review clock was extended by three months for review of new safety analyses• Complete Response action on April 12, 2017
– An imbalance in thrombotic events in the baricitinib RA program with potential thrombotic risk with use of baricitinib in RA
– Inadequate safety exposure for 2 mg of baricitinib– Not consistent findings to conclude greater efficacy with 4 mg over 2 mg– Lower doses of baricitinib should be considered for use in RA as there was evidence that
lower doses may be effective for treatment of RA– Cases consistent with drug-induced liver injury were observed with baricitinib use and need
to be described

13
Regulatory History: Re-submission• Re-submission on December 04, 2017• A revised proposal
– Indication and Usage: “Moderately to severely active RA who have had an inadequate response or are intolerant to methotrexate (MTX).”
– Warnings and Precautions: Warning about the potential risk of thrombosis– Dosage and Administration: “Proposed dose is 2 mg once daily. For patients with an inadequate
response or intolerance to more than one DMARD, a dose of 4 mg once daily is recommended. Dose tapering to 2 mg once daily may be considered for patients who have achieved sustained control of disease activity with 4 mg once daily.”
• Information provided in the re-submission– Updated analyses of accumulated safety (cut-off date, April 01, 2017 vs. August 01, 2015)– Epidemiological data comparing rates of VTE/PE from retrospective cohorts to those from the
prospective baricitinib studies in RA– Post-hoc efficacy analyses in patients who had failed more than one DMARD to support the new
dosing recommendations

14
Discussion Points and Voting Questions1. DISCUSSION: Discuss the efficacy data for baricitinib for the treatment of
adult patients with moderately to severely active rheumatoid arthritis who have had an inadequate response or are intolerant to methotrexate (MTX). Include a discussion of the 2 mg and 4 mg doses of baricitinib and whether available data support a benefit of one dose over the other.

15
Discussion Points and Voting Questions2. VOTE: Do the data provide substantial evidence of the efficacy of baricitinib
2 mg once daily for the treatment of adult patients with moderately to severely active rheumatoid arthritis who have had an inadequate response or are intolerant to methotrexate (MTX)?– If no, what data are needed?
3. VOTE: Do the data provide substantial evidence of the efficacy of baricitinib 4 mg once daily for the treatment of adult patients with moderately to severely active rheumatoid arthritis who have had an inadequate response or are intolerant to methotrexate (MTX)?– If no, what data are needed?

16
Discussion Points and Voting Questions4. DISCUSSION: Discuss the safety data for baricitinib for the treatment of
adult patients with moderately to severely active rheumatoid arthritis who have had an inadequate response or are intolerant to methotrexate (MTX) Include a discussion of the following issues:
a) Adequacy of safety database for the 2 mg dose of baricitinibb) Safety issues of interest and whether data suggest a dose response
– Thromboembolic events– Malignancy– Serious infections, opportunistic infections, herpes zoster, tuberculosis– Abnormal laboratory parameters, specifically platelet count elevations
c) Overall safety profile of the 2 mg dose and the 4 mg dose, and whether the data are more favorable for one dose versus the other.

17
Discussion Points and Voting Questions5. VOTE: Are the safety data adequate to support approval of baricitinib 2 mg
once daily for the treatment of adult patients with moderately to severely active rheumatoid arthritis who have had an inadequate response or are intolerant to methotrexate (MTX)?– If no, what data are needed?
6. VOTE: Are the safety data adequate to support approval of baricitinib 4 mg once daily for the treatment of adult patients with moderately to severely active rheumatoid arthritis who have had an inadequate response or are intolerant to methotrexate (MTX)?– If no, what data are needed?

18
Discussion Points and Voting Questions7. VOTE: Is the benefit-risk profile adequate to support approval of baricitinib
2 mg once daily for the proposed indication of the treatment of adult patients with moderately to severely active rheumatoid arthritis who have had an inadequate response or are intolerant to methotrexate (MTX)?– If no, what data are needed?
8. VOTE: Is the benefit-risk profile adequate to support approval of baricitinib 4 mg once daily for the proposed indication of the treatment of adult patients with moderately to severely active rheumatoid arthritis who have had an inadequate response or are intolerant to methotrexate (MTX)?– If no, what data are needed?


Robert Abugov, Ph.D.Acting Biostatistics Team Leader
Division of Biometrics IIU.S. Food and Drug Administration
April 23, 2018
FDA Arthritis Advisory Committee MeetingEfficacy of Baricitinib
NDA 207924: Baricitinib for the treatment of adult patients with moderately to severely active rheumatoid arthritis who have
inadequate response to methotrexate

2
Proposed Usage in Re-submission• Indication and Usage:
– “Treatment of adult patients with moderately to severely active rheumatoid arthritis (RA) who have had an inadequate response or are intolerant to methotrexate (MTX).”
• Dosage and Administration:– “The recommended dose is 2 mg once daily. For patients with an inadequate
response or intolerance to more than one disease modifying anti-rheumatic drug (DMARD), a dose of 4 mg once daily is recommended.
– Dose tapering to 2 mg once daily may be considered for patients who have achieved sustained control of disease activity with 4 mg once daily.”

3
Presentation Outline• Efficacy Compared to Control
– Clinical Response– Physical Function– Radiographic Response
• Efficacy of Baricitinib 4 mg Compared to 2 mg– Individual Phase 3 Studies– Integrated Analyses of Multiple Studies– Subgroup Analyses
• Efficacy Conclusions

4
Presentation Outline• Efficacy Compared to Control
– Clinical Response– Physical Function– Radiographic Response
• Efficacy of Baricitinib 4 mg Compared to 2 mg– Individual Phase 3 Studies– Integrated Analyses of Multiple Studies– Subgroup Analyses
• Efficacy Conclusions

5
Confirmatory Phase 3 StudiesStudy Patients Design Treatments N Major
EndpointsJADV MTX-IR R, DB, PC and AC
52 weeksB4 + MTXA QOW+ MTXPBO + MTX (→ 4 at Week 24)
Rescue to B4, starting at Week 16
488330487
W12 ACR20, HAQ-DI, DAS28
W24 mTSSJADX cDMARD-IR R, DB, PC
24 weeksB2 + cDMARDB4 + cDMARDPBO + cDMARD
Rescue to B4, starting at Week 16
229227228
W12 ACR20, HAQ-DI, DAS28
JADW TNF-IR R, DB, PC24 weeks
B2 + cDMARDB4 + cDMARDPBO + cDMARD
Rescue to B4, starting at Week 16
174177178
W12 ACR20, HAQ-DI, DAS28
JADZ Treatment naïve/early RA
R, DB, ACMTX titrated up to 20 mg weekly52 weeks
MTX B4B4 + MTX
Rescue to B4 + MTX starting at Week 24
213160215
W24 ACR20, HAQ-DI, DAS28
B4=baricitinib 4 mg PO QD, B2=baricitinib 2 mg PO QD, A=adalimumab 40 mg QOW, MTX=methotrexate, R=randomized, DB=double-blind, PC=placebo-controlled, AC=active-controlled, IR=inadequate response, TNF=tumor necrosis factor, QOW=every other week, W12=week 12, W24=week 24, ACR20=American College of Rheumatology 20% improvement, HAQ-DI=Health Assessment Questionnaire-Disability Index, DAS28=Disease Activity Score 28 Joints, mTSS=modified Total Sharp Score, PO=per orem, QD=each day

6
ACR20 Response in Phase 3 StudiesStudy
% Responders Odds Ratio (p-value)B4 B2 PBO B4:PBO B2:PBO
At Week 12JADV 70% -- 40% 3.6 (<0.001) -JADW 55% 49% 27% 3.4 (<0.001) 2.7 (0.001)JADX 62% 66% 39% 2.5 (<0.001) 3.0 (<0.001)
At Week 24B4+MTX B4 MTX (B4+MTX):MTX B4:MTX
JADZ 78% 77% 62% 2.2 (0.001) 2.0 (0.003)
ACR20=American College of Rheumatology 20% improvement; B2, B4=baricitinib 2 mg, 4 mg; PBO=placebo; MTX=methotrexate

7
Change from Baseline in DAS28Study
Mean Change in DAS28 Difference (p-value)B4 B2 PBO B4-PBO B2-PBO
At Week 12JADV -2.19 -0.96 -1.23 (.001) -JADW -1.79 -1.49 -0.83 -0.95 (.001) -0.66 (.001)JADX -1.92 -1.83 -1.08 -0.84 (.001) -0.75 (.001)
At Week 24B4+MTX B4 MTX (B4+MTX)-MTX B4-MTX
JADZ -2.84 -2.75 -2.06 -0.78 (.001) -0.69 (.001)
DAS28=Disease Activity Score for 28 joints; B2, B4=baricitinib 2 mg, 4 mg; PBO=placebo; MTX=methotrexate

8
Change from Baseline in HAQ-DI Study Mean Change in HAQ-DI Score Difference (p-value)
B4 B2 PBO B4-PBO B2-PBOAt Week 12JADV -0.66 -- -0.34 -0.32 (<.001) -JADW -0.41 -0.37 -0.17 -0.24 (<.001) -0.20 (<.001)JADX -0.56 -0.57 -0.36 -0.19 (<.001) -0.21 (<.001)
At Week 24B4+MTX B4 MTX (B4+MTX)-MTX B4-MTX
JADZ -1.03 -1.04 -0.74 -0.29 (<.001) -0.30 (<.001)
HAQ-DI=Health Assessment Questionnaire-Disability Index; B2, B4=baricitinib 2 mg, 4 mg; PBO=placebo; MTX=methotrexate

9
Presentation Outline• Efficacy Compared to Control
– Clinical Response– Physical Function– Radiographic Response
• Efficacy of Baricitinib 4 mg Compared to 2 mg– Individual Phase 3 Studies– Integrated Analyses of Multiple Studies– Subgroup Analyses
• Efficacy Conclusions

10
Radiographic Response in JADVMean Change in mTSS (n) Difference (p-value)
B4 A PBO B4-PBO A-PBOAt Week 24Linear extrapolation
0.41(470)
0.33(312)
0.90(452)
-0.49 (<.001) -0.56 (<.001)
All observed data 0.36 (424)
0.29 (280)
0.79 (363)
-0.44 (<.001) -0.51 (<.001)
mTSS=modified total sharp score; B4=baricitinib 4 mg; PBO=placebo; A=adalimumab; n=number of values included in analysis
• No radiographic progression• 70% - PBO • 82% - A• 81% - B4

11
Radiographic Response in JADXMean Change in mTSS (n) Difference (p-value)
B4 B2 PBO B4-PBO B2-PBOAt Week 24Linear extrapolation
0.15(198)
0.33(208)
0.70(190)
-0.55 (0.003) -0.38 (0.04)
All observed data 0.19(184)
0.34(188)
0.49(167)
-0.30 (0.03) -0.15 (0.3)
mTSS=modified total sharp score; B2, B4=baricitinib 2 mg, 4 mg; PBO=placebo; n=number of values included in analysis
• No radiographic progression• 76% - PBO • 71% - B2 • 80% - B4

12
Efficacy of Baricitinib 4 mg versus Adalimumab in JADV
Endpoint Treatment Baricitinib 4 mg vs. Adalimumab
B4 A PBO Odds Ratio (p-value)
Difference (p-value)
ACR20 Response, Week 12
70% 61% 40% 1.5 (.01)
Mean Change inDAS28, Week 12
-2.19 -1.91 -0.96 -0.28 (<.001)
Mean Change in mTSS, Week 24
0.36 0.30 0.80 0.07 (.6)
B4=baricitinib 4 mg; A=adalimumab; PBO=placebo

13
Conclusion: Efficacy of Baricitinib
• Clinical Response– Both baricitinib 2 mg and 4 mg are effective
• Physical Function– Both baricitinib 2 mg and 4 mg are effective
• Radiographic Response– 4 mg effective– Some uncertainty about effectiveness of 2 mg

14
Presentation Outline• Efficacy Compared to Control
– Clinical Response– Physical Function– Radiographic Response
• Efficacy of Baricitinib 4 mg Compared to 2 mg– Individual Phase 3 Studies– Integrated Analyses of Multiple Studies– Subgroup Analyses
• Efficacy Conclusions

15
JADW at Week 12: All RandomizedEndpoint B4
N=177B2
N=174PBO
N=176Baricitinib 4 mg vs. 2 mg(95% confidence interval)
ACR20 55% 49% 27% Odds Ratio: 1.3 (0.8, 2.0)ACR50 5% 2% 2% 2.2 (0.7, 7.4)ACR70 28% 20% 8% 1.5 (0.9, 2.5)
∆ DAS28 -1.95 -1.59 -0.85 Difference: -0.36 (-0.64, -0.08)
∆ HAQ-DI -0.41 -0.37 -0.17 -0.03 (-0.14, 0.07)
ACR20, 50, 70=American College of Rheumatology 20%, 50%, 70% improvement; DAS28=disease activity score 28 joints; HAQ-DI=Health Assessment Questionnaire-Disability Index; B2, B4=baricitinib 2 mg, 4 mg; PBO=placebo; ∆=mean change

16
JADX at Week 12: All RandomizedEndpoint B4
N=227B2
N=229PBO
N=228Baricitinib 4 mg vs. 2 mg(95% confidence interval)
ACR20 62% 66% 39% Odds Ratio: 0.8 (0.6, 1.2)ACR50 33% 34% 13% 1.0 (0.7, 1.5)ACR70 18% 18% 3% 1.0 (0.7, 1.7)
∆ DAS28 -1.92 -1.83 -1.08 Difference: -0.09 (-0.31, 0.13)∆ HAQ-DI -0.56 -0.57 -0.36 0.01 (-0.08, 0.11)
ACR20, 50, 70=American College of Rheumatology 20%, 50%, 70% improvement; DAS28=disease activity score 28 joints; HAQ-DI=Health Assessment Questionnaire-Disability Index; B2, B4=baricitinib 2 mg, 4 mg; PBO=placebo; ∆=mean change

17
Presentation Outline• Efficacy Compared to Control
– Clinical Response– Physical Function– Radiographic Response
• Efficacy of Baricitinib 4 mg Compared to 2 mg– Individual Phase 3 Studies– Integrated Analyses of Multiple Studies– Subgroup Analyses
• Efficacy Conclusions
18
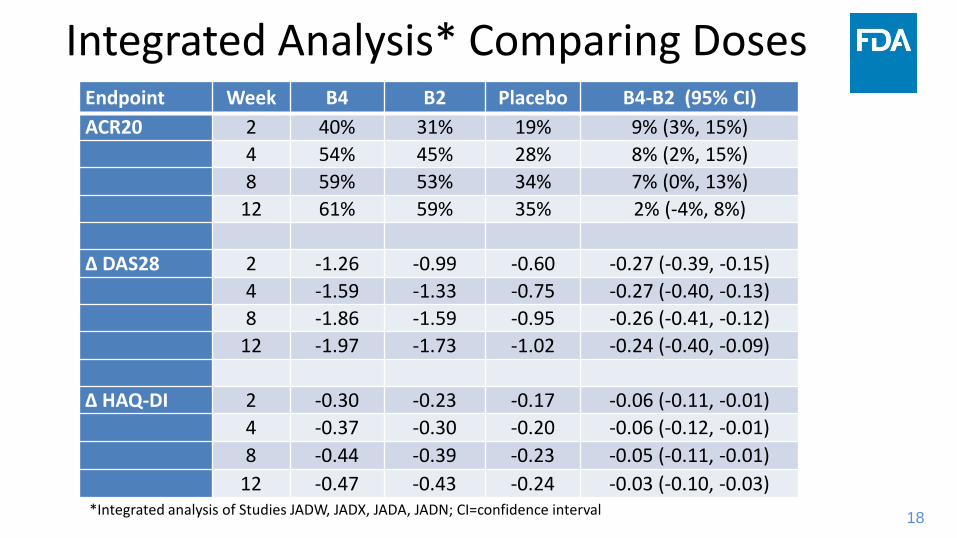
Integrated Analysis* Comparing Doses Endpoint Week B4 B2 Placebo B4-B2 (95% CI)ACR20 2 40% 31% 19% 9% (3%, 15%)
4 54% 45% 28% 8% (2%, 15%)8 59% 53% 34% 7% (0%, 13%)
12 61% 59% 35% 2% (-4%, 8%)
∆ DAS28 2 -1.26 -0.99 -0.60 -0.27 (-0.39, -0.15)4 -1.59 -1.33 -0.75 -0.27 (-0.40, -0.13)8 -1.86 -1.59 -0.95 -0.26 (-0.41, -0.12)
12 -1.97 -1.73 -1.02 -0.24 (-0.40, -0.09)
∆ HAQ-DI 2 -0.30 -0.23 -0.17 -0.06 (-0.11, -0.01)4 -0.37 -0.30 -0.20 -0.06 (-0.12, -0.01)8 -0.44 -0.39 -0.23 -0.05 (-0.11, -0.01)
12 -0.47 -0.43 -0.24 -0.03 (-0.10, -0.03)*Integrated analysis of Studies JADW, JADX, JADA, JADN; CI=confidence interval

19
Conclusion: Comparison of Doses
• Likely some small differences in efficacy between baricitinib 4 mg and 2 mg– May trend downward over time– Estimated differences small
• e.g., 2% difference in ACR20 response at Week 12– Confidence intervals rule out differences as large
as commonly used estimates of minimal clinically important differences for DAS28 and HAQ-DI

20
Presentation Outline• Efficacy Compared to Control
– Clinical Response– Physical Function– Radiographic Response
• Efficacy of Baricitinib 4 mg Compared to 2 mg– Individual Phase 3 Studies– Integrated Analyses of Multiple Studies– Subgroup Analyses
• Efficacy Conclusions

21
JADX at Week 12: At least Two Prior DMARD SubgroupEndpoint B4
N=227B2
N=229PBO
N=228Baricitinib 4 mg vs. 2 mg(95% confidence interval)
ACR20 64% 63% 44% Odds Ratio: 1.0 (0.6, 1.8)ACR50 36% 30% 15% 1.4 (0.8, 2.4)ACR70 17% 16% 5% 1.2 (0.6, 2.4)
∆ DAS28 -1.92 -1.83 -1.08 Difference: -0.27 (-0.56, 0.03)∆ HAQ-DI -0.56 -0.57 -0.36 0.01 (-0.08, 0.11)ACR20, 50, 70=American College of Rheumatology 20%, 50%, 70% improvement; DAS28=disease activity score 28 joints; HAQ-DI=Health Assessment Questionnaire-Disability Index; B2, B4=baricitinib 2 mg, 4 mg; PBO=placebo; ∆=mean change

22
JADX at Week 12: Less than Two Prior DMARD Subgroup
Endpoint B4N=99
B2N=107
PBON=97
Baricitinib 4 mg vs. 2 mg(95% confidence interval)
ACR20 59% 69% 34% Odds Ratio: 0.6 (0.4, 1.1)ACR50 30% 38% 9% 0.6 (0.4, 1.2)ACR70 19% 21% 1% 0.8 (0.4, 1.7)
∆ DAS28 -1.80 -1.94 -1.01 Difference: 0.14 (-0.20, 0.48)∆ HAQ-DI -0.59 -0.64 -0.37 0.05 (-0.10, 0.19)ACR20, 50, 70=American College of Rheumatology 20%, 50%, 70% improvement; DAS28=disease activity score 28 joints; HAQ-DI=Health Assessment Questionnaire-Disability Index; B2, B4=baricitinib 2 mg, 4 mg; PBO=placebo; ∆=mean change

23
Conclusion: Subgroup Analyses
• Results do not change conclusions about efficacy comparison between doses- Motivated in part by post hoc subgroup analyses- Statistical significance between doses lacking
and differences consistently small- Lack of evidence of interaction- Same methodology in complementary
population suggests implausible conclusions

24
Presentation Outline• Efficacy Compared to Control
– Clinical Response– Physical Function– Radiographic Response
• Efficacy of Baricitinib 4 mg versus 2 mg– Individual Phase 3 Studies– Integrated Analyses of Multiple Studies– Subgroup Analyses
• Efficacy Conclusions

25
Efficacy Conclusions: Baricitinib
• Both doses effective – Clinical response – Improvement in physical function
• Efficacy differences between 4 and 2 mg small• Subgroup analyses do not change conclusions


Raj Nair, M.D.Clinical Reviewer
Division of Pulmonary, Allergy, and Rheumatology ProductsU.S. Food and Drug Administration
April 23, 2018
FDA Arthritis Advisory Committee MeetingSafety of Baricitinib
NDA 207924: Baricitinib for the treatment of adult patients with moderately to severely active rheumatoid arthritis who have
inadequate response to methotrexate

2
Overview of Baricitinib Safety• Immunosuppressive
– Serious infections leading to hospitalization or death – Tuberculosis and bacterial, invasive fungal, viral (herpes zoster), and other
opportunistic infections– Malignancies, including lymphoma and other malignancies
• Laboratory Abnormalities– Decrease in neutrophil counts and hemoglobin– Platelet elevations– Lipids elevations– Liver test elevations
• Thrombosis

3
Focus of Safety PresentationAdverse Events• Deaths • Serious Adverse Events (SAEs)• Adverse events of special interest
– Malignancy– Serious infections– Herpes zoster– Opportunistic infections and TB– MACE– Thrombosis
• Arterial events• DVT/PE
Laboratory Parameters• Hematologic parameters
– Platelet elevations
• Lipid elevations• Liver test elevations
TB=tuberculosis; MACE=major adverse cardiovascular events; DVT=deep vein thrombosis; PE=pulmonary embolism

4
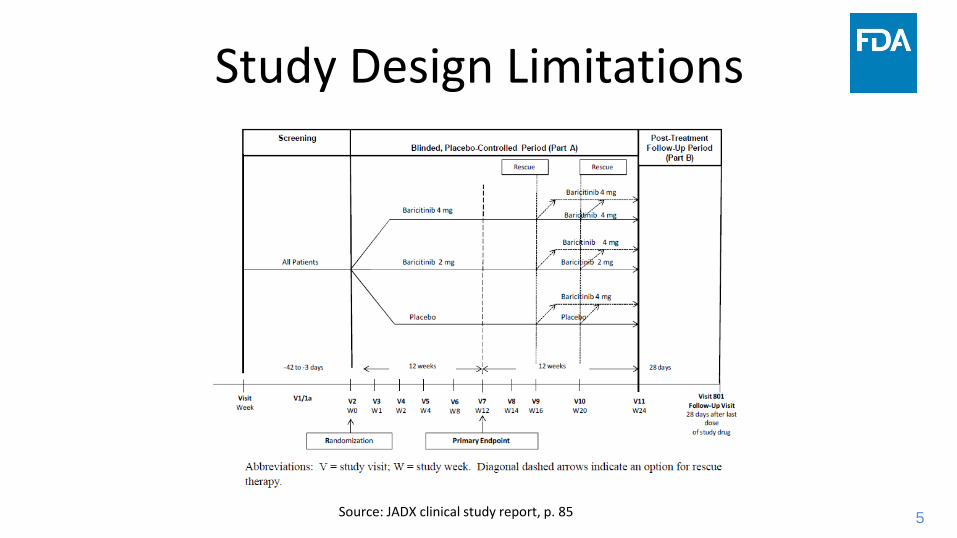
Safety Data Limitations• Limited placebo-controlled data
– Duration of baricitinib versus placebo controlled data pre-escape was limited to 16 weeks
• Overall safety exposure data limited for baricitinib 2 mg vs 4 mg– Four of the seven phase 2 and 3 clinical studies included 2 mg and 4 mg baricitinib dose
arms – Patient escape/cross-overs
• Patients on placebo were escaped to 4 mg of baricitinib• Patients who escaped from 2 mg baricitinib were placed on 4 mg of baricitinib• Patients who met escape criteria on 4 mg of baricitinib remained on 4 mg of baricitinib
– Patients in study JADY who had a pre-defined response* to 4 mg of baricitinib were eligible to be randomized to 2 mg vs. 4 mg of baricitinib
*CDAI≤10 for 3 months in study JADY or CDAI≤2.8 from study JADZ; patients originating from study JADA were not eligible
5
Study Design Limitations
Source: JADX clinical study report, p. 85

6
Study Design Limitations
Source: JADX clinical study report, p. 85

7
Study Design Limitations
Source: JADX clinical study report, p. 85

8
Safety Evaluation of Adverse Events

9
Safety Evaluation of Adverse Events

10
Safety Evaluation of Adverse Events

11
Safety Evaluation of Adverse Events

12
Safety Evaluation of Adverse Events

13
Safety Evaluation of Adverse Events

14
Safety Evaluation: Study Cohorts
• 0-16 weeks– 16-week pooled data from JADC, JADN, JADA/Y, JADV/Y, JADW/Y, JADX/Y– Comparisons: BARI 2 vs BARI 4, BARI 2/4 vs placebo
• 0-52 weeks– Comparisons: BARI 2 vs BARI 4
• >52 weeks– BARI 2 vs BARI 4

15
Presentation of Adverse Events
0-16 weeks: Studies JADA, JADC, JADN, JADV, JADW, and JADX0-52 and >52 weeks: JADA/Y, JADC, JADN, JADV/Y, JADX/Y, JADW/YIRD=incidence rate difference; CI=confidence interval; BARI=baricitinib; N=number of subjects; PYE=patient year exposure; n=number of patients with event; PY=patient year
IRD (95 % CI)
PlaceboN=1070
BARI 2N=479
BARI 4N=997
BARI 2/4N=1476
BARI 2/4 vs Placebo
BARI 4 vs BARI 2
0-16 weeks
PYE XX XX XX XX
n (rate/100 PY) n (rate) n (rate) n (rate) n (rate) IRD (95 % CI) IRD (95 % CI)
0-52 weeks
PYE XX XX XX
n (rate/100 PY) n (rate) n (rate) n (rate) IRD (95 % CI)
>52 weeks
PYE XX XX XX
n (rate/100 PY) n (rate) n (rate) n (rate) IRD (95 % CI)

16
Presentation of Adverse Events
0-16 weeks: Studies JADA, JADC, JADN, JADV, JADW, and JADX0-52 and >52 weeks: JADA/Y, JADC, JADN, JADV/Y, JADX/Y, JADW/YIRD=incidence rate difference; CI=confidence interval; BARI=baricitinib; N=number of subjects; PYE=patient year exposure; n=number of patients with event; PY=patient year
IRD (95 % CI)
PlaceboN=1070
BARI 2N=479
BARI 4N=997
BARI 2/4N=1476
BARI 2/4 vs Placebo
BARI 4 vs BARI 2
0-16 weeks
PYE XX XX XX XX
n (rate/100 PY) n (rate) n (rate) n (rate) n (rate)
0-52 weeks
PYE
n (rate/100 PY)
>52 weeks
PYE
n (rate/100 PY)

17
Presentation of Adverse Events
0-16 weeks: Studies JADA, JADC, JADN, JADV, JADW, and JADX0-52 and >52 weeks: JADA/Y, JADC, JADN, JADV/Y, JADX/Y, JADW/YIRD=incidence rate difference; CI=confidence interval; BARI=baricitinib; N=number of subjects; PYE=patient year exposure; n=number of patients with event; PY=patient year
IRD (95 % CI)
PlaceboN=1070
BARI 2N=479
BARI 4N=997
BARI 2/4N=1476
BARI 2/4 vs Placebo
BARI 4 vs BARI 2
0-16 weeks
PYE
n (rate/100 PY) IRD (95 % CI) IRD (95 % CI)
0-52 weeks
PYE
n (rate/100 PY)
>52 weeks
PYE
n (rate/100 PY)

18
Presentation of Adverse Events
0-16 weeks: Studies JADA, JADC, JADN, JADV, JADW, and JADX0-52 and >52 weeks: JADA/Y, JADC, JADN, JADV/Y, JADX/Y, JADW/YIRD=incidence rate difference; CI=confidence interval; BARI=baricitinib; N=number of subjects; PYE=patient year exposure; n=number of patients with event; PY=patient year
IRD (95 % CI)
PlaceboN=1070
BARI 2N=479
BARI 4N=997
BARI 2/4N=1476
BARI 2/4 vs Placebo
BARI 4 vs BARI 2
0-16 weeks
PYE
n (rate/100 PY)
0-52 weeks
PYE XX XX XX
n (rate/100 PY) n (rate) n (rate) n (rate)
>52 weeks
PYE XX XX XX
n (rate/100 PY) n (rate) n (rate) n (rate)

19
Presentation of Adverse Events
0-16 weeks: Studies JADA, JADC, JADN, JADV, JADW, and JADX0-52 and >52 weeks: JADA/Y, JADC, JADN, JADV/Y, JADX/Y, JADW/YIRD=incidence rate difference; CI=confidence interval; BARI=baricitinib; N=number of subjects; PYE=patient year exposure; n=number of patients with event; PY=patient year
IRD (95 % CI)
PlaceboN=1070
BARI 2N=479
BARI 4N=997
BARI 2/4N=1476
BARI 2/4 vs Placebo
BARI 4 vs BARI 2
0-16 weeks
PYE
n (rate/100 PY)
0-52 weeks
PYE
n (rate/100 PY) IRD (95 % CI)
>52 weeks
PYE
n (rate/100 PY) IRD (95 % CI)

20
Exposures
0-16 weeks: Studies JADA, JADC, JADN, JADV, JADW, and JADX0-52 and >52 weeks: JADA/Y, JADC, JADN, JADV/Y, JADX/Y, JADW/YIRD=incidence rate difference; CI=confidence interval; BARI=baricitinib; N=number of subjects; PYE=patient year exposure; n=number of patients with event; PY=patient year
IRD (95 % CI)
PlaceboN=1070
BARI 2N=479
BARI 4N=997
BARI 2/4N=1476
BARI 2/4 vs Placebo
BARI 4 vs BARI 2
0-16 weeks
PYE 308 140 298 438
n (rate/100 PY)
0-52 weeks
PYE 336 904 1318
n (rate/100 PY)
>52 weeks
PYE 155 653 1215
n (rate/100 PY)

21
Death
0-16 weeks: Studies JADA, JADC, JADN, JADV, JADW, and JADX0-52 and >52 weeks: JADA/Y, JADC, JADN, JADV/Y, JADX/Y, JADW/YIRD=incidence rate difference; CI=confidence interval; BARI=baricitinib; N=number of subjects; PYE=patient year exposure; n=number of patients with event; PY=patient year
IRD (95 % CI)
PlaceboN=1070
BARI 2N=479
BARI 4N=997
BARI 2/4N=1476
BARI 2/4 vs Placebo
BARI 4 vs BARI 2
0-16 weeks
PYE 308 140 298 438
n (rate/100 PY) 2 (0.6) 0 1 (0.3) 1 (0.2) -0.6 (-1.7, 0.5) 0.7 (-0.7, 2.1)
0-52 weeks
PYE 336 904 1318
n (rate/100 PY) 0 4 (0.4) 4 (0.3) 0.5 (-0.2, 1.2)
>52 weeks
PYE 155 653 1215
n (rate/100 PY) 1 (0.6) 2 (0.3) 4 (0.3) -0.6 (-1.8, 0.6)

22
Serious Adverse Events
0-16 weeks: Studies JADA, JADC, JADN, JADV, JADW, and JADX0-52 and >52 weeks: JADA/Y, JADC, JADN, JADV/Y, JADX/Y, JADW/YIRD=incidence rate difference; CI=confidence interval; BARI=baricitinib; N=number of subjects; PYE=patient year exposure; n=number of patients with event; PY=patient year
IRD (95 % CI)
PlaceboN=1070
BARI 2N=479
BARI 4N=997
BARI 2/4N=1476
BARI 2/4 vs Placebo
BARI 4 vs BARI 2
0-16 weeks
PYE 308 140 298 438
n (rate/100 PY) 41 (13) 16 (11.4) 43 (14.4) 59 (13.5) 0 (-5.5, 5.4) 6.1 (-2.8, 15)
0-52 weeks
PYE 336 904 1318
n (rate/100 PY) 40 (11.9) 113 (12.5) 164 (12.4) 3.2 (-2.2, 8.6)
>52 weeks
PYE 155 653 1215
n (rate/100 PY) 12 (7.7) 75 (11.5) 123 (10.1) 6.4 (0.2, 12.6)*

23
Malignancies Excluding NMSC
0-16 weeks: Studies JADA, JADC, JADN, JADV, JADW, and JADX0-52 and >52 weeks: JADA/Y, JADC, JADN, JADV/Y, JADX/Y, JADW/YIRD=incidence rate difference; CI=confidence interval; BARI=baricitinib; N=number of subjects; PYE=patient year exposure; n=number of patients with event; PY=patient year
IRD (95 % CI)
PlaceboN=1070
BARI 2N=479
BARI 4N=997
BARI 2/4N=1476
BARI 2/4 vs Placebo
BARI 4 vs BARI 2
0-16 weeks
PYE 308 140 298 438
n (rate/100 PY) 0 1 (0.7) 1 (0.3) 2 (0.5) 0.5 (-0.2, 1.1) 2.8 (-2.4, 7.9)
0-52 weeks
PYE 336 904 1318
n (rate/100 PY) 2 (0.6) 6 (0.7) 8 (0.6) 0 (-1.1, 1.1)
>52 weeks
PYE 155 653 1215
n (rate/100 PY) 0 4 (0.6) 9 (0.7) 1.1 (-0.2, 2.3)

24
Serious Infections
0-16 weeks: Studies JADA, JADC, JADN, JADV, JADW, and JADX0-52 and >52 weeks: JADA/Y, JADC, JADN, JADV/Y, JADX/Y, JADW/YIRD=incidence rate difference; CI=confidence interval; BARI=baricitinib; N=number of subjects; PYE=patient year exposure; n=number of patients with event; PY=patient year
IRD (95 % CI)
PlaceboN=1070
BARI 2N=479
BARI 4N=997
BARI 2/4N=1476
BARI 2/4 vs Placebo
BARI 4 vs BARI 2
0-16 weeks
PYE 308 140 298 438
n (rate/100 PY) 13 (4.2) 6 (4.3) 12 (4.1) 18 (4.1) -0.4 (-3.5, 2.7) 1.3 (-3.9, 6.6)
0-52 weeks
PYE 336 904 1318
n (rate/100 PY) 14 (4.2) 32 (3.5) 50 (3.8) 0.7 (-2.4, 3.7)
>52 weeks
PYE 155 653 1215
n (rate/100 PY) 4 (2.6) 20 (3.1) 35 (2.9) 1.3 (-2.2, 4.8)

25
Herpes Zoster
0-16 weeks: Studies JADA, JADC, JADN, JADV, JADW, and JADX0-52 and >52 weeks: JADA/Y, JADC, JADN, JADV/Y, JADX/Y, JADW/Y; >52 week data from resubmissionIRD=incidence rate difference; CI=confidence interval; BARI=baricitinib; N=number of subjects; PYE=patient year exposure; n=number of patients with event; PY=patient year
IRD (95 % CI)
PlaceboN=1070
BARI 2N=479
BARI 4N=997
BARI 2/4N=1476
BARI 2/4 vs Placebo
BARI 4 vs BARI 2
0-16 weeks
PYE 308 140 298 438
n (rate/100 PY) 4 (1.3) 5 (3.6) 15 (5) 20 (4.6) 3 (0.6, 5.3)* 2.8 (-2.4, 7.9)
0-52 weeks
PYE 336 904 1318
n (rate/100 PY) 11 (3.3) 29 (3.2) 48 (3.6) 0.4 (-2.2, 3)
>52 weeks
PYE 155 653 1215
n (rate/100 PY) 6 (2.1) 44 (3.7) 87 (3.7) 0.7 (-1.5, 2.9)

26
Opportunistic Infections
0-16 weeks: Studies JADA, JADC, JADN, JADV, JADW, and JADX0-52 and >52 weeks: JADA/Y, JADC, JADN, JADV/Y, JADX/Y, JADW/Y; >52 week data from resubmissionIRD=incidence rate difference; CI=confidence interval; BARI=baricitinib; N=number of subjects; PYE=patient year exposure; n=number of patients with event; PY=patient year
IRD (95 % CI)
PlaceboN=1070
BARI 2N=479
BARI 4N=997
BARI 2/4N=1476
BARI 2/4 vs Placebo
BARI 4 vs BARI 2
0-16 weeks
PYE 308 140 298 438
n (rate/100 PY) 2 (0.6) 0 2 (0.7) 2 (0.5) -0.2 (-1.4, 1.0) 0.7 (-0.7, 2.1)
0-52 weeks
PYE 336 904 1318
n (rate/100 PY) 1 (0.3) 5 (0.6) 6 (0.5) 0 (-0.8, 0.7)
>52 weeks
PYE 155 653 1215
n (rate/100 PY) 1 (0.4) 8 (0.7) 13 (0.6) -0.1 (-0.9, 0.7)

27
Tuberculosis
0-16 weeks: Studies JADA, JADC, JADN, JADV, JADW, and JADX0-52 and >52 weeks: JADA/Y, JADC, JADN, JADV/Y, JADX/Y, JADW/Y; >52 week data from resubmissionIRD=incidence rate difference; CI=confidence interval; BARI=baricitinib; N=number of subjects; PYE=patient year exposure; n=number of patients with event; PY=patient year
IRD (95 % CI)
PlaceboN=1070
BARI 2N=479
BARI 4N=997
BARI 2/4N=1476
BARI 2/4 vs Placebo
BARI 4 vs BARI 2
0-16 weeks
PYE 308 140 298 438
n (rate/100 PY) 0 0 0 0 -- --
0-52 weeks
PYE 336 904 1318
n (rate/100 PY) 0 1 (0.1) 1 (0.1) 0.3(-0.2, 0.8)
>52 weeks
PYE 155 653 1215
n (rate/100 PY) 0 5 (0.4) 6 (0.3) 1.1 (0.1, 2)*

28
Major Adverse Cardiovascular Events
0-16 weeks: Studies JADV, JADW, and JADX0-52 and >52 weeks: JADV/Y, JADX/Y, JADW/YIRD=incidence rate difference; CI=confidence interval; BARI=baricitinib; N=number of subjects; PYE=patient year exposure; n=number of patients with event; PY=patient year
IRD (95 % CI)
PlaceboN=1070
BARI 2N=479
BARI 4N=997
BARI 2/4N=1476
BARI 2/4 vs Placebo
BARI 4 vs BARI 2
0-16 weeks
PYE 267 123 273 396
n (rate/100 PY) 2 (0.8) 0 2 (0.7) 2 (0.5) -0 (-1.5, 1.4) 1.6 (-0.6, 3.8)
0-52 weeks
PYE 305 825 1189
n (rate/100 PY) 1 (0.3) 4 (0.5) 5 (0.4) 0.2 (-0.8, 1.2)
>52 weeks
PYE 155 575 1092
n (rate/100 PY) 0 4 (0.7) 7 (0.6) 1 (-0.1, 2.1)

29
Overall Thrombosis
0-16 weeks: Studies JADA, JADC, JADN, JADV, JADW, and JADX0-52 and >52 weeks: JADA/Y, JADC, JADN, JADV/Y, JADX/Y, JADW/YIRD=incidence rate difference; CI=confidence interval; BARI=baricitinib; N=number of subjects; PYE=patient year exposure; n=number of patients with event; PY=patient year
IRD (95 % CI)
PlaceboN=1070
BARI 2N=479
BARI 4N=997
BARI 2/4N=1476
BARI 2/4 vs Placebo
BARI 4 vs BARI 2
0-16 weeks
PYE 308 140 298 438
n (rate/100 PY) 1 (0.3) 2 (1.4) 7 (2.4) 9 (2.1) 1.6 (0.1, 3.1)* 1.4 (-2, 4.8)
0-52 weeks
PYE 336 904 1318
n (rate/100 PY) 5 (1.5) 10 (1.1) 16 (1.2) -0.4 (-2.1, 1.2)
>52 weeks
PYE 155 653 1215
n (rate/100 PY) 1 (0.4) 14 (1.2) 21 (0.9) 1.7 (0.3, 3.1)*

30
Arterial Thrombosis
0-16 weeks: Studies JADA, JADC, JADN, JADV, JADW, and JADX0-52 and >52 weeks: JADA/Y, JADC, JADN, JADV/Y, JADX/Y, JADW/YIRD=incidence rate difference; CI=confidence interval; BARI=baricitinib; N=number of subjects; PYE=patient year exposure; n=number of patients with event; PY=patient year
IRD (95 % CI)
PlaceboN=1070
BARI 2N=479
BARI 4N=997
BARI 2/4N=1476
BARI 2/4 vs Placebo
BARI 4 vs BARI 2
0-16 weeks
PYE 308 140 298 438
n (rate/100 PY) 1 (0.3) 2 (1.4) 2 (0.7) 4 (0.9) 0.4 (-0.7, 1.4) 0 (-2.8, 2.7)
0-52 weeks
PYE 336 904 1318
n (rate/100 PY) 3 (0.9) 3 (0.3) 6 (0.5) -0.4 (-1.6, 0.8)
>52 weeks
PYE 155 653 1215
n (rate/100 PY) 0 8 (0.7) 11 (0.5) 1.2 (0.3, 2.2)*

31
Venous Thrombosis
0-16 weeks: Studies JADA, JADC, JADN, JADV, JADW, and JADX0-52 and >52 weeks: JADA/Y, JADC, JADN, JADV/Y, JADX/Y, JADW/YIRD=incidence rate difference; CI=confidence interval; BARI=baricitinib; N=number of subjects; PYE=patient year exposure; n=number of patients with event; PY=patient year
IRD (95 % CI)
PlaceboN=1070
BARI 2N=479
BARI 4N=997
BARI 2/4N=1476
BARI 2/4 vs Placebo
BARI 4 vs BARI 2
0-16 weeks
PYE 308 140 298 438
n (rate/100 PY) 0 0 5 (1.7) 5 (1.1) 1.2 (0.1, 2.3)* 1.4 (-0.6, 3.4)
0-52 weeks
PYE 336 904 1318
n (rate/100 PY) 2 (0.6) 7 (0.8) 10 (0.8) 0 (-0.8, 0.3)
>52 weeks
PYE 155 653 1215
n (rate/100 PY) 1 (0.4) 7 (0.6) 11 (0.5) 0.5 (-0.6, 1.5)

32
JADV: 24 Week Safety Summary
TEAE=treatment emergent adverse event

33
JADZ: 24 Week Safety Summary

34
LABORATORY ABNORMALITIES

35
Laboratory Abnormalities
*mean change from baseline in combined phase 3 studies (JADX, JADW, JADV, JADZ)g=gram; dL=deciliter; µL=microliter
0-16 weeks, mean change* Placebo BARI 2 mg BARI 4 mg
Number of patients 892 403 1265
Hematologic Changes
Hemoglobin (g/dL) -0.20 -0.30 -0.26
Neutrophil (thousand cells/µL) 0.10 -0.60 -1.09
Lymphocyte (thousand cells/µL) -0.01 0.11 0.15Platelets (109/L) 2 16 17

36
Platelet Elevations: JADX & JADW

37
Platelet Elevations: JADX & JADW
1Number (%) of patients with platelet counts greater than 600 109/L. Seven (7) patients with their platelet counts greater than 600 109/L at baseline are excluded2Number (%) of patients with platelet counts greater than 450 109/L. Sixty seven (67) patients with their platelet counts greater than 450 109/L at baseline are excludedFrom phase 3 studies that included both 2 mg and 4 mg baricitinib study arms with data to week 24; patient data censored with change in treatment arm

38
Platelet Elevations: Phase 2 Studies
Data up to Week 13

39
Lipid Elevations
*mean change from baseline in combined phase 3 studies (JADX, JADW, JADV, JADZ)LDL=low density lipoprotein; HDL=high density lipoprotein

40
Liver Test Elevations
*mean change from baseline in combined phase 3 studies (JADX, JADW, JADV, JADZ)ALT=alanine aminotransferase; AST=aspartate aminotransferase; IU=international unit; L=liter; mg=milligram

41
Safety Conclusions• Serious infection, including opportunistic infections and tuberculosis• Herpes zoster• Malignancy• Thrombosis, both venous and arterial• Laboratory Abnormalities (often dose-dependent)
– Decreased neutrophil counts and hemoglobin– Platelet count elevations– Lipid elevations– Liver test elevations


Matthew Whittaker, Ph.D.Non-Clinical Reviewer
Division of Pulmonary, Allergy, and Rheumatology ProductsU.S. Food and Drug Administration
April 23, 2018
FDA Arthritis Advisory Committee MeetingPotential Biological Mechanisms for Baricitinib-induced Increase in Platelets
NDA 207924: Baricitinib for the treatment of adult patients with moderately to severely active rheumatoid arthritis who have
inadequate response to methotrexate

2
Janus Kinase (JAK) Enzyme Function
Clark et al. (2014) J. Med. Chem. 57, 5023-5038

3
In Vitro Selectivity of BaricitinibCell-free isolated enzyme assay Cell-based assay (human peripheral blood mononuclear cells)
JAK1 JAK2 JAK3 TYK2 JAK1/2 JAK1/3 JAK1/TYK2 JAK2/JAK2 JAK2/TYK2IC50 (nM) 5.9 5.7 >400 53 IC50 (nM) 32.8 55.4 71.6 NA 69.0
Selectivityvs. JAK3 >68 >70 - >7.5 Selectivity vs.
JAK1/JAK3 1.7 - 0.8 NA 0.8
Apparent selectivity of baricitinib (BARI) for JAK1 & JAK2 over JAK3, TYK2 Decreased inhibitory activity JAK3: intended to limit immune-suppressive effects seen with pan-JAK
inhibitors
Cell-free isolated enzyme assay Cell-based assay (human whole blood)
JAK1 JAK2 JAK3 TYK2JAK1/2 or JAK1/TYK2 JAK1/3 JAK1/TYK2 JAK2/JAK2 JAK2/TYK2 JAK2/TYK2
IC50 (nM) 4.0 6.6 787.0 61.0 IC50 (nM) 21.1 259 28.7 87.8 149 81.9
Selectivityvs. JAK3 197 119 - 13
Selectivityvs.
JAK1/JAK312.3 - 9.0 2.9 1.7 3.2
Clark et al. (2014) J Med Chem. 57, 5023 – 5038

4
Platelet Count: JADX & JADW

5
Kile, B. (2015) Nature Medicine. 21: 11 – 12.
Megakaryopoiesis
Thrombopoietin (TPO): glycoprotein hormone produced in liver
Acts at the TPO receptor (Mpl) to mediate expansion & differentiation of Hematopoietic stem cells (HSCs) → megakaryocyte progenitors (pro-MKs) → MKs → platelets (PLTs)
Mpl expressed on HSCs, pro-MKs, MKs, PLTs Mpl associates with JAK2 Geddis, A. (2010) Seminars in Hematology.
47: 212-219

6
JAK2 and Platelet Homeostasis Based on Meyer et al. Blood (2014); Ng et al. PNAS (2014)
T
T
T
TP
P T
P
T
LIVERT
BONE MARROW
HSC PRO-MK MK
Proliferation & expansion
Mpl MplMpl
TT
T TT
P
TT
PP
P
TPO
JAK2
Internalize & Degrade
TPO
Mpl
JAK2
= TPO= Platelet= JAK2
TP
P
P
P
TT
TT
T
T
P
T
Meyer S et al. (2014) Blood. 124: 2280 – 2284Skoda (2014) Blood. 124: 2168.Ng A. et al. (2014) PNAS. 111, 5884-5889.
T
P
Blood vessels
Blood vesselsHow might BARI increase platelets in RA patients?

7
Baricitinib-Induced Platelet IncreaseT
T
T
TP
P T
P
T
LIVERT
BONE MARROW
HSC PRO-MK MK
Mpl MplMpl
TT
T TT
P
TT
PP
P
TPO
JAK2
Internalize & Degrade
TPO
Mpl
JAK2
= TPO= Platelet= JAK2
TP
P
P
P
TT
TT
T
T
P
T
Meyer S et al. (2014) Blood. 124: 2280 – 2284Skoda (2014) Blood. 124: 2168.Ng A. et al. (2014) PNAS. 111, 5884-5889.
T
P
Blood vessels
BARIT
TTT
TT
T
T
T
TT
TBlood vesselsP
P
P
P
P
P
P
P
P
P
P
Proliferation & expansion

8
Initiation of BARI treatmento At clinical doses, BARI is present at a concentration that is:
• Sufficient to inhibit Mpl-mediated TPO clearance by platelets, BUT• Not sufficient to completely inhibit Mpl-mediated signal transduction in HSC/progenitor cells in
bone marrowo ↑ circulating TPO can stimulate expansion of HSC/progenitor cells that retain Mpl functiono Platelet population reaches maximum at ~ 2 weeks
2 weeks – 8 weeks of dosingo Increased platelet population: sufficient to overcome BARI inhibitory effect on TPO removal–
circulating TPO levels decline o Stimulus for platelet production is attenuated – platelet production is reduced – resetting to a new
equilibrium
Long-term BARI treatmento New equilibrium is achieved: Platelets are chronically elevated vs. placeboo Circulating TPO levels are chronically elevated via BARI inhibition of Mpl-associated JAK2 in platelets –
BARI levels in bone marrow are not sufficient to completely mitigate the effects of elevated TPO on HSC/progenitor cells
Potential Effects on Platelet Homeostasis

9
Evidence from the published literature provides a mechanistic framework for the observed BARI-induced increase in platelet countso Extent of platelet production is defined by TPO activation of Mpl in
HSC/progenitor cells in bone marrowo Circulating TPO levels are controlled by Mpl-mediated removal in mature
plateletso Mpl function is mediated by the activity of JAK2o BARI inhibition of JAK2 alters platelet homeostasis
• Differential inhibition of JAK2 associated with Mpl in platelets vs. stem/progenitor cell population could enhance platelet production
• BARI effects on biological processes associated with platelet removal cannot be ruled out
Conclusions


FDA Arthritis Advisory Committee MeetingEpidemiology Safety Study Review
NDA 207924: Baricitinib for the treatment of adult patients with moderately to severely active rheumatoid arthritis who have
inadequate response to methotrexate
Veronica V. Sansing-Foster, PhD, MSEpidemiologist
Division of Epidemiology II (DEPI-II)U.S. Food and Drug Administration
April 23, 2018

2
Baricitinib Resubmission
• January 15, 2016: Applicant submitted NDA 207924 for baricitinib – During the 24-week randomized placebo-controlled period of the Phase 2/3 studies, 6
patients with baricitinib 4-mg (n=997) reported venous thromboembolism (VTE) events (deep vein thrombosis [DVT] and pulmonary embolism [PE])
– No events in the baricitinib 2-mg (n=479) and placebo arms (n=1070)
• April 12, 2017: FDA issued a Complete Response letter due to the unfavorable benefit-risk given the potential risk of thrombosis
• December 4, 2017: Applicant resubmitted the application with the pooled incidence rates (IR) for all patients exposed to baricitinib (ALL BARI RA) – VTE IRs for baricitinib from clinical studies were compared to VTE IRs for DMARDs from
applicant’s observational study

3
Observational Safety Study Methods• Design: Retrospective, observational, descriptive study
• Data Sources: IMEDS/Sentinel and Truven Marketscan/Medicare
• Study inclusion criteria: RA, ≥ 18 yrs old, no prior VTE
• Exposure: csDMARDs (including MTX) and bDMARDs
• Outcomes: VTE, including DVT and PE
• Follow-up/Censoring: Outcome, death, plan disenrollment, drug discontinuation, starting another drug, or end of study
• Analysis: Incidence rate (IR) per 100 PY for DMARDs vs. pooled IRs per 100 PY for baricitinibfrom clinical trials; stratified by age, calendar year, and gender

4
Study Groups (Data Source)
VTEIR (95% CI)
Baricitinib (ALL BARI RA)
0.53 (0.38, 0.71)
DMARDs (Truven – Def. 1)
0.68 (0.65, 0.71)
DMARDs (Truven – Def. 2)
1.05 (1.01, 1.09)
DMARDs (Truven – Def. 3)
1.63 (1.58, 1.69)
DMARDs (IMEDS)
1.34 (1.24, 1.44)
Results: VTE Incidence Rates per 100 PY by Study Groups
* DEFINITION 1: diagnostic code + anticoagulant w/in 31 days of VTE, DVT, PEDEFINITION 2: inpatient diag. code for venous or PE or phlebitis and thrombophlebitis or DVT or outpatient diagnostic code + anticoagulant w/in 31 ds of VTE DEFINITION 3: diagnostic code for venous embolism or phlebitis and thrombophlebitis or DVT in inpatient, outpatient or emergency department care setting
ǂ The mid-P exact test 95% confidence intervals have been calculated by the DEPI-II reviewer using Open Epi Software.

5
Study Groups (Data Source)
DVTIR (95% CI)
Baricitinib (ALL BARI RA)
0.38(0.25, 0.54)
DMARDs (Truven – Def. 1)
0.55 (0.52, 0.58) ǂ
DMARDs (Truven – Def. 2)
0.84 (0.80, 0.87) ǂ
DMARDs (Truven – Def. 3)
1.36 (1.31, 1.40) ǂ
DMARDs (IMEDS)
1.97 (1.85, 2.09)
Results: DVT & PE Incidence Rates per 100 PY by Study Groups
* DEFINITION 1: diagnostic code + anticoagulant w/in 31 days of VTE, DVT, PEDEFINITION 2: inpatient diag. code for venous or PE or phlebitis and thrombophlebitis or DVT or outpatient diagnostic code + anticoagulant w/in 31 ds of VTE DEFINITION 3: diag. code for venous embolism or phlebitis and thrombophlebitis or DVT in an inpatient, outpatient or emergency department care setting
ǂ The mid-P exact test 95% confidence intervals have been calculated by the DEPI-II reviewer using Open Epi Software.

6
Study Groups (Data Source)
DVTIR (95% CI)
PEIR (95% CI)
Baricitinib (ALL BARI RA)
0.38(0.25, 0.54)
0.24(0.14, 0.37)
DMARDs (Truven – Def. 1)
0.55 (0.52, 0.58) ǂ
0.26 (0.24, 0.28) ǂ
DMARDs (Truven – Def. 2)
0.84 (0.80, 0.87) ǂ
0.38 (0.36, 0.41) ǂ
DMARDs (Truven – Def. 3)
1.36 (1.31, 1.40) ǂ
0.46 (0.43, 0.49) ǂ
DMARDs (IMEDS)
1.97 (1.85, 2.09)
0.77 (0.70, 0.84)
Results: DVT & PE Incidence Rates per 100 PY by Study Groups
* DEFINITION 1: diagnostic code + anticoagulant w/in 31 days of VTE, DVT, PEDEFINITION 2: inpatient diag. code for venous or PE or phlebitis and thrombophlebitis or DVT or outpatient diagnostic code + anticoagulant w/in 31 ds of VTE DEFINITION 3: diag. code for venous embolism or phlebitis and thrombophlebitis or DVT in an inpatient, outpatient or emergency department care setting
ǂ The mid-P exact test 95% confidence intervals have been calculated by the DEPI-II reviewer using Open Epi Software.

7
Applicant’s Conclusion
• All rates from the baricitinib patients were lower than or within the lower range of the VTE rates observed in the RA population treated with DMARDs
• The study’s conclusions were not altered by:– Age-stratified rates– bDMARD and csDMARD rates

8
FDA Concerns
• The overall study designs and populations compared by the applicant are fundamentally different and aim to address different objectives
– Clinical studies aim to address efficacy, and sometimes safety, in a clinical setting
– Observational studies aim to address safety in a “real world” setting

9
FDA Concerns
ConcernBaricitinib
Clinical Data Example
DMARDObservational Data Example
Different patient populations US and Non-USpatients
US patients

10
FDA Concerns
ConcernBaricitinib
Clinical Data Example
DMARDObservational Data Example
Different patient populations US and Non-USpatients
US patients
Different inclusion and exclusion criteria Past DMARD use Incident DMARD use

11
FDA Concerns
ConcernBaricitinib
Clinical Data Example
DMARD Observational Data Example
Different patient populations US and Non-USpatients
US patients
Different inclusion and exclusion criteria Past DMARD use Incident DMARD use
Different collection methods for medical history, RA, and baseline drug exposure
Drug exposure captured at baseline
Drug exposure captured 3 mos. before baseline

12
FDA Concerns
ConcernBaricitinib
Clinical Data Example
DMARDObservational Data Example
Different patient populations US and Non-US patients
US patients
Different inclusion and exclusion criteria Past DMARD use Incident DMARD use
Different collection methods for medical history, RA, and baseline drug exposure
Drug exposure captured at baseline
Drug exposure captured 3 mos. before baseline
Patients with baseline anticoagulant use for prior VTE were included
Stratified rates cannot be compared

13
The VTE rates from the baricitinib clinical trials should not be
compared to those of DMARD users in the IMEDS/Truven data
to conclude that baricitinib
is less safe, as safe as, or safer than DMARDs
FDA Conclusion

14
FDA Acknowledgements
Dr. Efe EworukeDr. Saharat Patanavanich
Nichelle RashidDr. Lockwood Taylor
Dr. Joel WeissfeldDr. Judith Zander


Raj Nair, M.D.Clinical Reviewer
Division of Pulmonary, Allergy, and Rheumatology ProductsU.S. Food and Drug Administration
April 23, 2018
FDA Arthritis Advisory Committee MeetingBenefit Risk Considerations
NDA 207924: Baricitinib for the treatment of adult patients with moderately to severely active rheumatoid arthritis who have
inadequate response to methotrexate

2
Benefits• Both baricitinib 2 mg and 4 mg once daily doses are effective in reducing
signs and symptoms and improving physical function in patients with RA versus placebo
– Higher ACR20, 50, 70 response rates versus placebo – Improvement in Health Assessment Questionnaire-Disability Index (HAQ-DI) compared to
placebo– Data not consistent in showing a meaningful benefit of 4 mg over the 2 mg dose
• Radiographic response– The data for 4 mg dose are robust– Some uncertainty about 2 mg dose, studied in only one study as an exploratory endpoint

3
Risks• Safety consistent with an immunosuppressant and MOA
– Serious and sometimes fatal infections– Opportunistic infections and TB– Herpes zoster– Malignancies – Thrombosis, including arterial and venous thromboses
• Laboratory abnormalities (often dose-dependent)– Decreases in neutrophil counts and hemoglobin– Platelet count elevations– Lipid elevations– Liver test elevations

4
Baricitinib for RABenefits • Superior efficacy of both
baricitinib doses compared to placebo:
– Signs and symptoms – Physical function – No consistent meaningful benefit of 4
mg over 2 mg
• Radiographic response:– Data for 4 mg dose are robust– Some uncertainty about 2 mg dose,
studied in only one study as an exploratory endpoint
Risks • Serious infections• Herpes zoster, opportunistic
infections and TB• Malignancies• Thrombosis
– Both arterial and venous
• Laboratory abnormalities– Many dose-dependent, including
platelet elevations


FDA Arthritis Advisory Committee MeetingCharge to the Committee
NDA 207924: Baricitinib for the treatment of adult patients with moderately to severely active rheumatoid arthritis who have
inadequate response to methotrexate
Nikolay P. Nikolov, M.D.Clinical Team Leader
Division of Pulmonary, Allergy, and Rheumatology ProductsU.S. Food and Drug Administration
April 23, 2018

2
Efficacy Considerations• Both baricitinib 2 mg and 4 mg once daily doses are effective in reducing
signs and symptoms and improving physical function in patients with RA versus placebo– Higher ACR20, 50, 70 response rates versus placebo at week 12 and week 24– Improvement in Health Assessment Questionnaire-Disability Index (HAQ-DI)
compared to placebo– Data not consistent in showing a meaningful benefit of 4 mg over the 2 mg dose
• Radiographic response– The data for 4 mg dose are robust– Some uncertainty about 2 mg dose, studied in only one study as an exploratory
endpoint

3
Safety Considerations• Safety findings
– Serious infection, including H. zoster, opportunistic infections and tuberculosis
– Malignancy– Thrombosis, both venous and arterial– Laboratory abnormalities (often dose-dependent)
• Safety data limitations– Limited controlled comparisons– Overall safety exposure data limited for baricitinib 2 mg vs 4 mg

4
Benefits• Superior efficacy of both
baricitinib doses compared to placebo
– Signs and symptoms – Physical function – No consistent meaningful benefit of 4 mg
over 2 mg
• Radiographic response– Data for 4 mg dose are robust– Some uncertainty about 2 mg dose,
studied in only one study as an exploratory endpoint
Risks• Serious infections• Herpes zoster, opportunistic
infections and TB• Malignancies• Thrombosis
– Both arterial and venous
• Laboratory abnormalities– Many dose-dependent, including
thrombocytosis
Benefit-Risk Considerations

5
• “FDA will approve an application after it determines that the drug meets the statutory standards for safety and effectiveness, manufacturing and controls, and labeling.”
Approval of an Application21 CFR 314.105 (c)

6
• (b)(5) “…substantial evidence consisting of adequate and well-controlled investigations…that the drug product will have the effect it purports or is represented to have under the conditions of use prescribed, recommended, or suggested in the proposed labeling.”
Efficacy Standard21 CFR 314.125
Refusal to Approve an Application

7
(b)(2) “…do not include adequate tests by all methods reasonably applicable to show whether or not the drug is safe for use under the conditions prescribed, recommended, or suggested in its proposed labeling.”
(b)(3) “The results of the test show that the drug is unsafe for use under the conditions prescribed, recommended, or suggested in its proposed labeling or the results do not show that the drug product is safe for use under those conditions.”
(b)(4) “There is insufficient information about the drug to determine whether the product is safe for use under the conditions prescribed, recommended, or suggested in its proposed labeling.”
Safety Standard21 CFR 314.125
Refusal to Approve an Application

8
Discussion Points and Voting Questions
1. DISCUSSION: Discuss the efficacy data for baricitinib for the treatment of adult patients with moderately to severely active rheumatoid arthritis who have had an inadequate response or are intolerant to methotrexate (MTX). Include a discussion of the 2 mg and 4 mg doses of baricitinib and whether available data support a benefit of one dose over the other.

9
Discussion Points and Voting Questions
2. VOTE: Do the data provide substantial evidence of the efficacy of baricitinib 2 mg once daily for the treatment of adult patients with moderately to severely active rheumatoid arthritis who have had an inadequate response or are intolerant to methotrexate (MTX)?– If no, what data are needed?
3. VOTE: Do the data provide substantial evidence of the efficacy of baricitinib 4 mg once daily for the treatment of adult patients with moderately to severely active rheumatoid arthritis who have had an inadequate response or are intolerant to methotrexate (MTX)?– If no, what data are needed?

10
Discussion Points and Voting Questions
4. DISCUSSION: Discuss the safety data for baricitinib for the treatment of adult patients with moderately to severely active rheumatoid arthritis who have had an inadequate response or are intolerant to methotrexate (MTX) Include a discussion of the following issues:
a) Adequacy of safety database for the 2 mg dose of baricitinibb) Safety issues of interest and whether data suggest a dose response
– Thromboembolic events– Malignancy– Serious infections, opportunistic infections, herpes zoster, tuberculosis– Abnormal laboratory parameters, specifically platelet count elevations
c) Overall safety profile of the 2 mg dose and the 4 mg dose, and whether the data are more favorable for one dose versus the other.

11
Discussion Points and Voting Questions5. VOTE: Are the safety data adequate to support approval of baricitinib 2 mg
once daily for the treatment of adult patients with moderately to severely active rheumatoid arthritis who have had an inadequate response or are intolerant to methotrexate (MTX)?– If no, what data are needed?
6. VOTE: Are the safety data adequate to support approval of baricitinib 4 mg once daily for the treatment of adult patients with moderately to severely active rheumatoid arthritis who have had an inadequate response or are intolerant to methotrexate (MTX)?– If no, what data are needed?

12
Discussion Points and Voting Questions7. VOTE: Is the benefit-risk profile adequate to support approval of baricitinib
2 mg once daily for the proposed indication of the treatment of adult patients with moderately to severely active rheumatoid arthritis who have had an inadequate response or are intolerant to methotrexate (MTX)?– If no, what data are needed?
8. VOTE: Is the benefit-risk profile adequate to support approval of baricitinib 4 mg once daily for the proposed indication of the treatment of adult patients with moderately to severely active rheumatoid arthritis who have had an inadequate response or are intolerant to methotrexate (MTX)?– If no, what data are needed?
