fda introductory comments · marketing approval prior to demonstration of ... switch to...
TRANSCRIPT

FDA Introductory Comments
NDA 210303: Plazomicin Sulfate Injection
Antimicrobial Drugs Advisory Committee MeetingMay 02, 2018
Sumati Nambiar MD MPHDirector, Division of Anti‐Infective Products
FDA

2
Introduction• NDA 210303: Plazomicin sulfate injection• Applicant: Achaogen Inc. • Qualified Infectious Disease Product (QIDP) designation for:
– Complicated Urinary Tract Infections (cUTI) – Catheter‐related Bloodstream Infections (BSI)– Hospital‐Acquired Bacterial Pneumonia (HABP), Ventilator‐Associated Bacterial
Pneumonia (VABP)– Complicated Intra‐Abdominal Infections
• Breakthrough therapy designation for:– Treatment of BSI caused by certain Enterobacteriaceae in patients who have
limited or no alternative treatment options
• The Applicant requested review of the BSI indication under section 506(h) of the Federal Food, Drug and Cosmetic Act (FD&C Act)
• NDA granted priority review as the product has QIDP designationwww.fda.gov
3
Proposed Indications• As a single agent in patients aged 18 years or older for the treatment
of complicated urinary tract infections (cUTIs), including pyelonephritis, caused by the following susceptible microorganism(s): Escherichia coli (including cases with concurrent bacteremia), Klebsiella pneumoniae, Proteus spp (including Proteus mirabilis and Proteus vulgaris), and Enterobacter cloacae
• For patients aged 18 years or older for the treatment of bloodstream infections (BSIs) caused by the following susceptible microorganism(s): Klebsiella pneumoniae and Escherichia coli
As only limited clinical safety and efficacy data for plazomicin are currently available, plazomicin should be reserved for use in patients who have limited or no alternative treatment options (both indications)
4
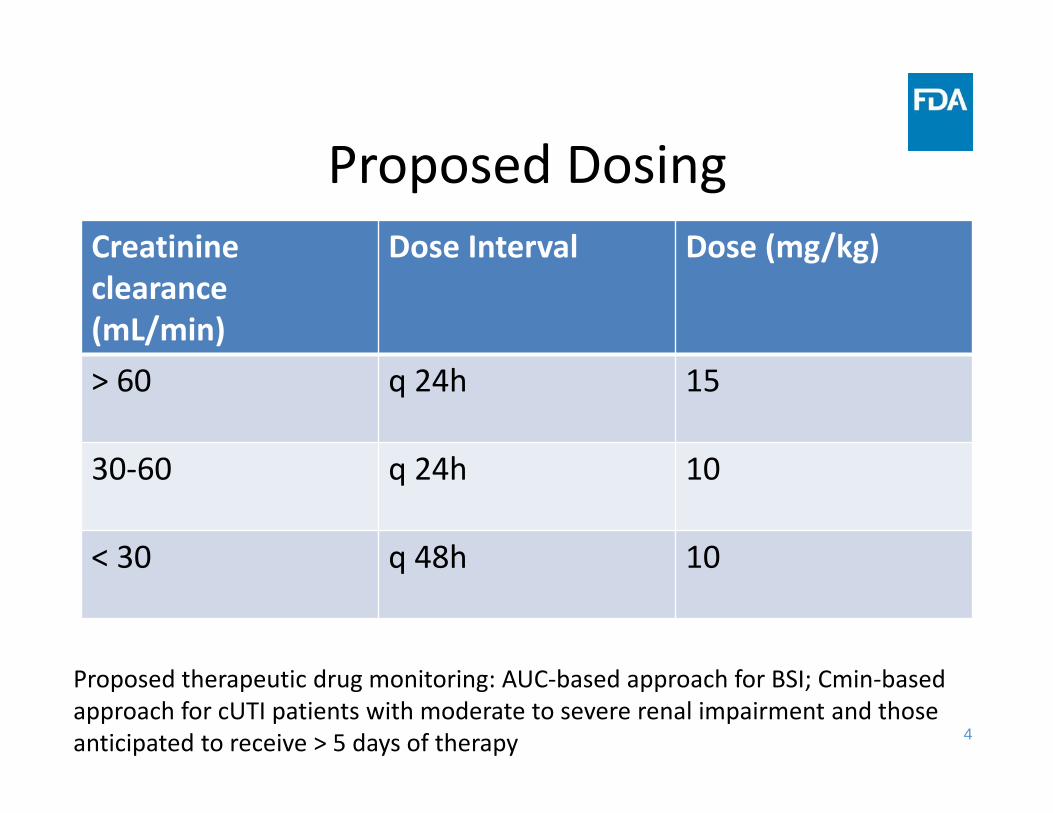
Proposed DosingCreatinineclearance (mL/min)
Dose Interval Dose (mg/kg)
> 60 q 24h 15
30‐60 q 24h 10
< 30 q 48h 10
Proposed therapeutic drug monitoring: AUC‐based approach for BSI; Cmin‐based approach for cUTI patients with moderate to severe renal impairment and those anticipated to receive > 5 days of therapy

5
21st Century Cures Act• Signed into law on December 13, 2016• Title III, Subtitle E – Antimicrobial Innovation and Stewardship– Section 3044. Susceptibility test interpretive criteria for microorganisms; antimicrobial susceptibility testing devices
– Section 3041. Antimicrobial Resistance Monitoring– Section 3042. Limited Population Pathway for antibacterial and antifungal drugs (LPAD)
https://www.congress.gov/114/bills/hr34/BILLS‐114hr34enr.pdf
6
LPAD: Requirements• The drug is intended to treat a serious or life‐threatening infection in a limited population of patients with unmet needs
• Standards for approval under 505(c) and (d) or standards for licensure under 351 of Public Health Service Act are met
• Written request from the Sponsor that the drug be approved as a limited population drug
7
Standards for Approval
• Sponsor must provide substantial evidence of effectiveness for the drug’s intended use and sufficient information to conclude that it is safe for use under conditions prescribed, recommended, or suggested in the proposed labeling
• Safe and effective – Substantial evidence of effectiveness for treatment of the
proposed indication – Benefits for proposed population outweigh risks
• Substantial evidence requires evidence consisting of adequate and well‐controlled investigations (21 CFR 314.126)– FDA may consider “data from one adequate and well‐controlled
clinical investigation and confirmatory evidence” to constitute substantial evidence (section 505(d) of the FD&C Act)
8
Standards for Approval• Acceptance of greater uncertainty or higher risk in patients with serious diseases and with an unmet need is an appropriate approach to the risk‐benefit assessment
• Flexibility in FDA regulations does not mean marketing approval prior to demonstration of substantial evidence of effectiveness
21 CFR 312 subpart E
9
LPAD: Additional Requirements• Labeling: To indicate that safety and effectiveness has only been demonstrated with respect to a limited population– All advertising and labeling will include “Limited Population” in a prominent manner, and
– The prescribing information will contain the statement “This drug is indicated for use in a limited and specific population of patients”
• Promotional Materials: – Pre‐submission of promotional materials at least 30 days prior to dissemination of such materials
10
Development Program• Six phase 1 studies including a lung penetration study, a thorough QT study and a renal impairment study
• One phase 2 (Study ACHN‐490‐002) and one phase 3 trial in adults with cUTI/acute pyelonephritis (Study ACHN‐490‐009)
• One phase 3 trial in adults with BSI or HABP/VABP (Study ACHN‐490‐007)
11
Phase 2 cUTI Trial: Study 002• Two plazomicin doses, 10 mg/kg and 15 mg/kg were
evaluated; levofloxacin was the comparator• Plazomicin administered for 5 days; no oral switch allowed • Patients with creatinine clearance < 60 mL/min were
excluded• Primary endpoint: Microbiologic eradication at Test of Cure
(TOC) visit• Results: In the MITT population, microbiologic eradication
rates were 50% (6/12) in the 10 mg/kg group, 60.8% (31/51) in the 15 mg/kg group, and 58.6% (17/29) in the levofloxacin group
MITT‐Modified Intent To Treat
12
Phase 3 cUTI Trial: Study 009• Randomized, double‐blind noninferiority (NI) trial
comparing plazomicin to meropenem• Trial design generally consistent with the cUTI guidance• After a minimum of 4 days of blinded IV therapy, option to
switch to open‐label oral levofloxacin for an additional 3 to 6 days
• Co‐primary endpoints: Composite of microbiologic eradication and clinical cure rate in the microbiological modified intent‐to‐treat (mMITT) population at the Day 5 and TOC visits
• Pre‐specified NI margin of 15%* • Dose adjustment was based on creatinine clearance;
Therapeutic drug monitoring (TDM) was not performed *to be reserved for use in patients who have limited or no alternative treatment optionshttps://www.fda.gov/downloads/Drugs/.../Guidances/ucm070981.pdf
13
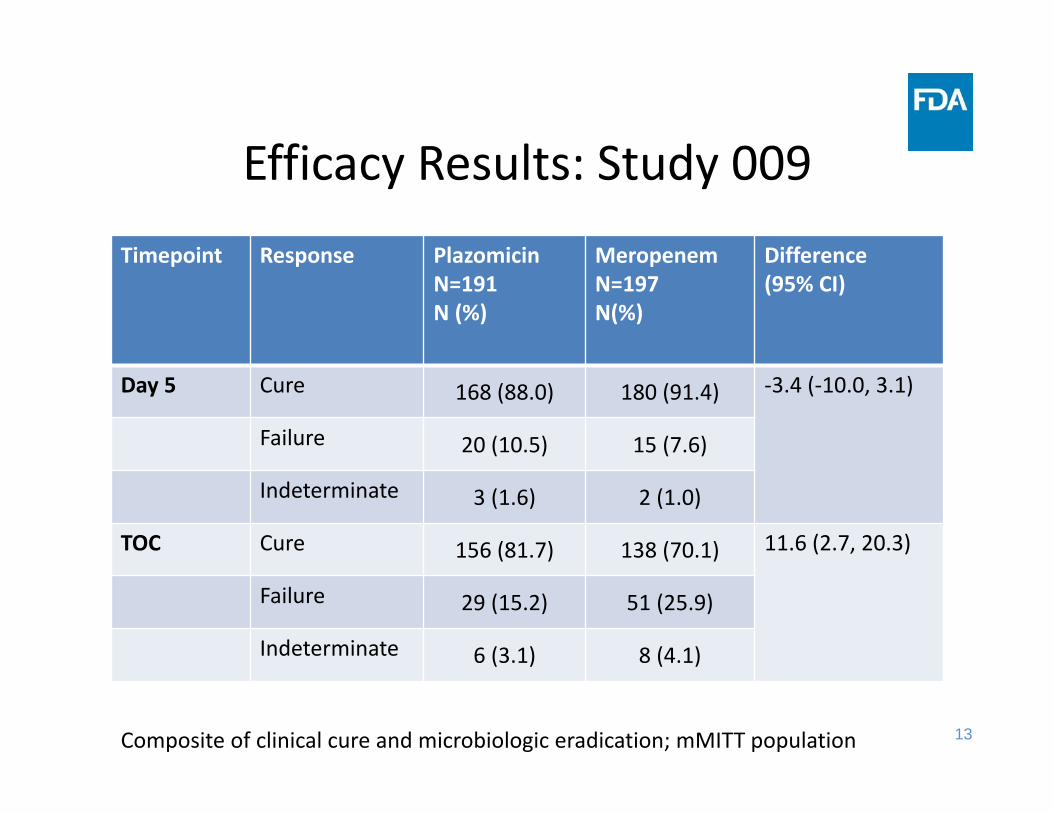
Efficacy Results: Study 009Timepoint Response Plazomicin
N=191N (%)
MeropenemN=197N(%)
Difference(95% CI)
Day 5 Cure 168 (88.0) 180 (91.4) ‐3.4 (‐10.0, 3.1)
Failure 20 (10.5) 15 (7.6)
Indeterminate 3 (1.6) 2 (1.0)
TOC Cure 156 (81.7) 138 (70.1) 11.6 (2.7, 20.3)
Failure 29 (15.2) 51 (25.9)
Indeterminate 6 (3.1) 8 (4.1)
Composite of clinical cure and microbiologic eradication; mMITT population
14
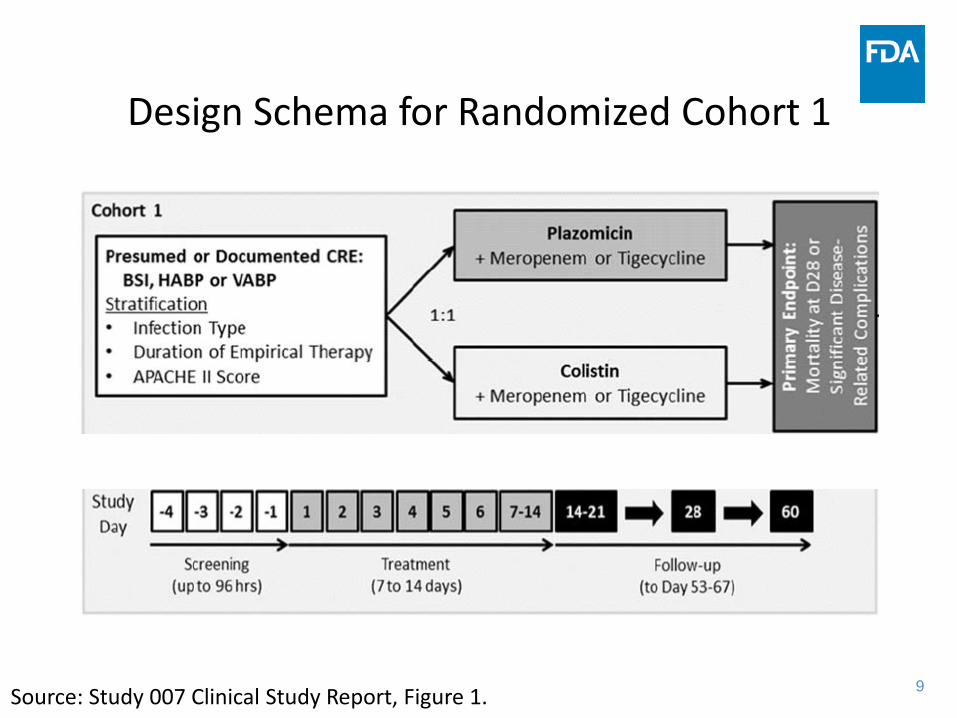
Phase 3 BSI, HABP/VABP Trial: Study 007• Randomized, open‐label, superiority trial comparing plazomicin to colistin in
patients with BSI or HABP/VABP due to carbapenem‐resistant Enterobacteriaceae (CRE)
• In both arms of the trial, patients could receive concomitant tigecycline or meropenem based on susceptibility of the baseline organism
• Original primary efficacy endpoint was 28‐day all‐cause mortality (ACM)• Primary analysis population:
– Microbiological modified intent‐to‐treat (mMITT) population: Randomized patients who received at least one dose of study drug and had a CRE isolated from an acceptable study‐qualifying baseline specimen
• Originally planned sample size: 286 patients with confirmed CRE• Statistical significance level:
– one‐sided α = 0.05 – the usual two‐sided p‐value would only need to be <0.10 instead of <0.05

15
Study 007• Protocol amendments:
– Primary efficacy endpoint changed from Day 28 ACM to composite of Day 28 ACM or significant disease‐related complications (SDRCs)*
– Second amendment, uncontrolled Cohort 2 created to include patients not eligible for randomization
• Study was stopped after two years due to difficulty in enrolling• Final sample size in the randomized cohort was 37 in the
primary analysis population• Statistical analysis plan was finalized after enrollment was
completed, but before unblinding results; no formal hypothesis testing was to be performed
*new or worsening acute respiratory distress syndrome, a new lung abscess, empyema, onset of septic shock, persistent CRE bacteremia, or a new CRE bacteremia

16
Study 007• The initial dose and dosing interval were adjusted based on the baseline estimated creatinine clearance (CLcr), or by the type of renal replacement for those on continuous renal replacement therapy
• Subsequent doses were adjusted as needed, based on TDM, using measured plazomicin plasma concentrations and dose adjustment equations

17
Study 007: Clinical Outcomes (BSI, HABP/VABP, mMITT Population)
Endpoint Colistin (n = 20)
Plazomicin(n = 17)
Difference Exact 90% CI one‐sided exact p‐value
28‐day all‐cause mortality or
SDRCs
10 (50%)
4 (24%)
26% ‐1% to 51% 0.09
28‐day all‐causemortality
8(40%)
2(12%)
28% 1% to 52% 0.06

18
Study 007: Outcomes by Subgroups(mMITT Population)
Day 28 all‐cause mortality or SDRCs
Colistin Plazomicin Difference Exact 90% CI One‐sided exact p‐value
Overall(BSI, HABP/VABP)
10/20 (50%)
4/17 (24%)
26% ‐1% to 51% 0.09
BSI 8/15(53%)
2/14(14%)
39% 9% to 66% 0.03
HABP/VABP 2/5(40%)
2/3 (67%)
19
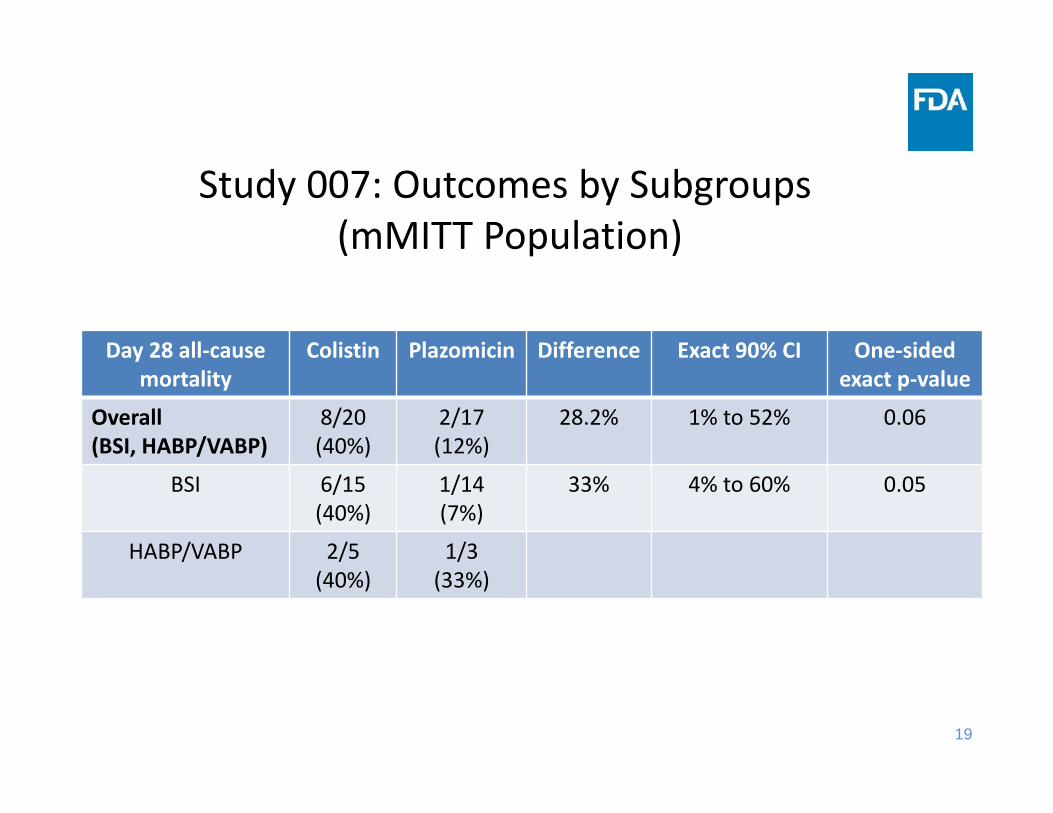
Study 007: Outcomes by Subgroups(mMITT Population)
Day 28 all‐cause mortality
Colistin Plazomicin Difference Exact 90% CI One‐sided exact p‐value
Overall(BSI, HABP/VABP)
8/20 (40%)
2/17 (12%)
28.2% 1% to 52% 0.06
BSI 6/15(40%)
1/14(7%)
33% 4% to 60% 0.05
HABP/VABP 2/5(40%)
1/3 (33%)
20
Safety Assessment• Primary safety assessment is based on the Phase 3 cUTI trial; supportive evidence from the Phase 2 cUTI trial
• Safety from Study 007 was assessed separately due to differences between the trials, e.g., duration of treatment, patient population, concomitant medications
• Safety of plazomicin is consistent with the aminoglycoside class; signal for nephrotoxicity; potential for ototoxicity cannot be ruled out
21
Outline for the Day• Presentations by the Applicant• Presentations by the FDAEfficacy:
cUTI: Hengrui Sun, DrPH BSI, HABP/VABP: Daniel Rubin, PhD and Shrimant Mishra, MD MPH
Safety: Shrimant Mishra MD MPH Clinical Pharmacology:
cUTI: Luning Zhuang, PhD BSI: Kunyi Wu, PharmD
• Clarifying questions• Lunch• Open public hearing• Questions for the committee
21
22
Question 1• Has the Applicant provided substantial evidence of the safety and effectiveness of plazomicin for the treatment of complicated urinary tract infections in patients with limited or no treatment options?– If yes, please provide any recommendations for labeling.
– If no, please discuss additional studies/analyses that are needed.
22

23
Question 2• Has the Applicant provided substantial evidence of the safety and effectiveness of plazomicin for the treatment of bloodstream infections in patients with limited or no treatment options?– If yes, please provide any recommendations for labeling.
– If no, please discuss additional studies/analyses that are needed.
23
Presentation of Clinical Efficacy for cUTI
Antimicrobial Drugs Advisory Committee MeetingMay 2, 2018
Hengrui Sun, DrPHStatistical Reviewer
Division of Biometrics IV, Office of Biostatistics, Office of Translational Sciences, CDER, FDA
2
Outline
• Study 009 design• Disposition, demographics, and baseline characteristics
• Efficacy results• Summary

3
Study Design
Source: Study 009 Protocol version A1, Figure 1
Note: EOIV = End-of-IV (within 24 hours of last dose of IV study drug); TOC = Test of cure (Day 17 ± 2 days); LFU = Late follow-up (Day 24 – 32)
4
Statistical Methods
• Co‐primary efficacy endpoints: microbiological eradication and clinical cure rate – at Day 5 (or EOIV)– at TOC
• Primary analysis population:microbiological modified intent‐to‐treat (mMITT) population
• Non‐inferiority (NI) margin: ‐15%• Analysis method: Difference in the cure rate (plazomicin – meropenem) and 95% CI (continuity corrected Z‐statistics) were calculated

5
Disposition, mMITT Population Plazomicin (N=191)
Meropenem(N=197)
Completed Study 189 (99%) 194 (98.5%)Prematurely Discontinued Study 2 (1%) 3 (1.5%)Lost to Follow‐up 1 (0.5%) 1 (0.5%)Withdrawal of Consent 1 (0.5%) 2 (1%)
Completed Study Treatment 183 (95.8%) 187 (94.9%)Prematurely Discontinued Study Drug (IV or Oral) 8 (4.2%) 10 (5.1%)Prematurely Discontinued IV Study DrugAdverse Event 1 (0.5%) 5 (2.5%)Lack of Study Qualifying Pre‐treatment Baseline Urine Culture 1 (0.5%) 1 (0.5%)Withdrawal of Consent 1 (0.5%)CLCR<30mL/min 1 (0.5%)Investigator Decision 2 (1%)
Prematurely Discontinued Oral Study DrugAdverse Event 2 (1%) 2 (1%)Pathogen Resistant to Levofloxacin 1 (0.5%)Lost to Follow‐up 1 (0.5%)
Note: A total of 609 patients were randomized to the study
6
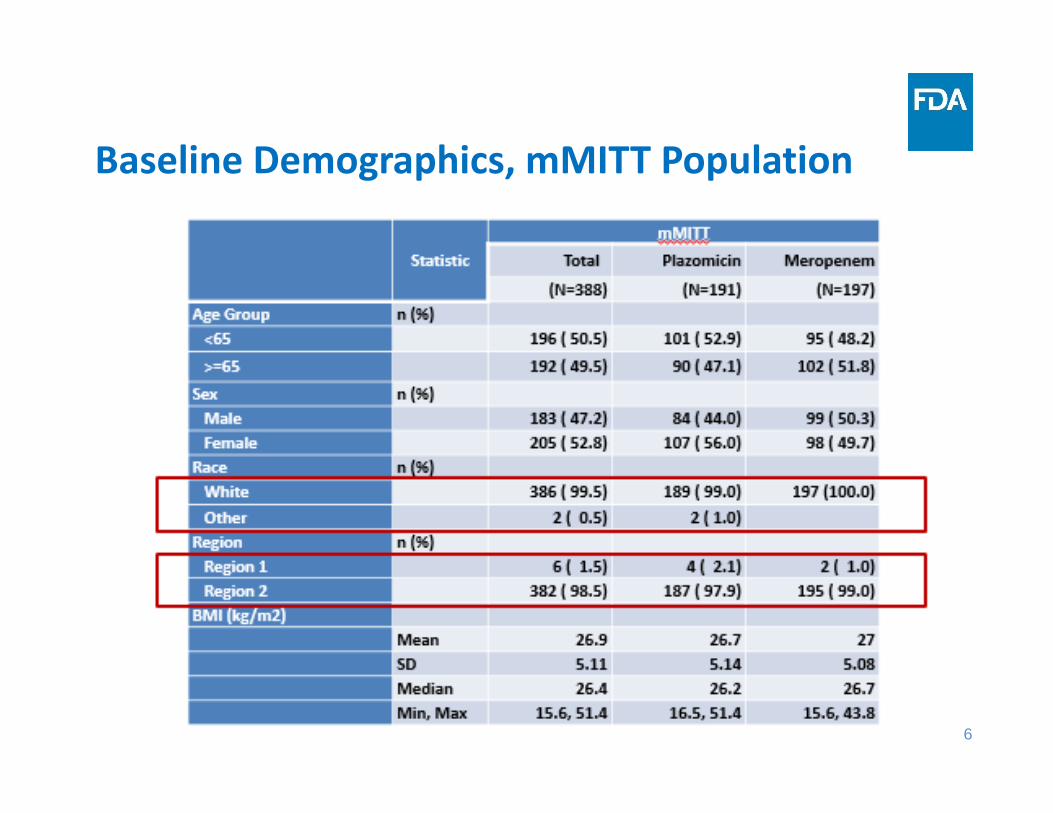
Baseline Demographics, mMITT Population
7
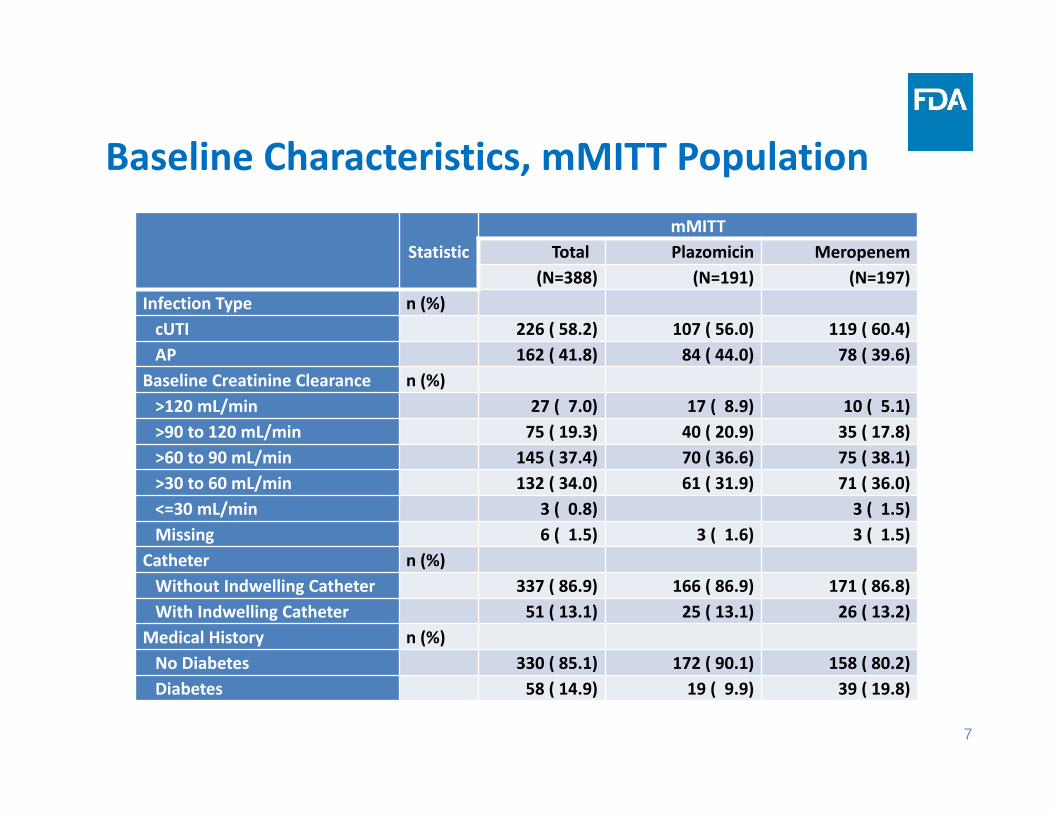
Baseline Characteristics, mMITT Population
StatisticmMITT
Total Plazomicin Meropenem(N=388) (N=191) (N=197)
Infection Type n (%)cUTI 226 ( 58.2) 107 ( 56.0) 119 ( 60.4)AP 162 ( 41.8) 84 ( 44.0) 78 ( 39.6)
Baseline Creatinine Clearance n (%)>120 mL/min 27 ( 7.0) 17 ( 8.9) 10 ( 5.1)>90 to 120 mL/min 75 ( 19.3) 40 ( 20.9) 35 ( 17.8)>60 to 90 mL/min 145 ( 37.4) 70 ( 36.6) 75 ( 38.1)>30 to 60 mL/min 132 ( 34.0) 61 ( 31.9) 71 ( 36.0)<=30 mL/min 3 ( 0.8) 3 ( 1.5)Missing 6 ( 1.5) 3 ( 1.6) 3 ( 1.5)
Catheter n (%)Without Indwelling Catheter 337 ( 86.9) 166 ( 86.9) 171 ( 86.8)With Indwelling Catheter 51 ( 13.1) 25 ( 13.1) 26 ( 13.2)
Medical History n (%)No Diabetes 330 ( 85.1) 172 ( 90.1) 158 ( 80.2)Diabetes 58 ( 14.9) 19 ( 9.9) 39 ( 19.8)
8
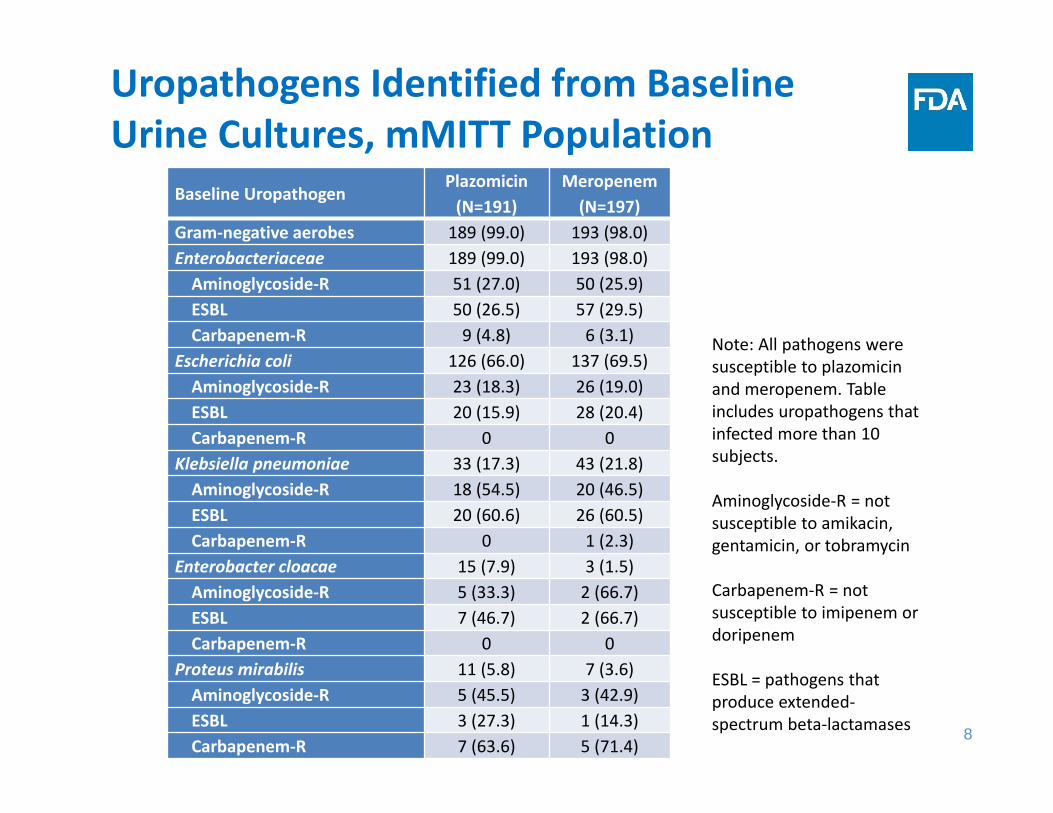
Uropathogens Identified from Baseline Urine Cultures, mMITT Population
Baseline UropathogenPlazomicin (N=191)
Meropenem (N=197)
Gram‐negative aerobes 189 (99.0) 193 (98.0)Enterobacteriaceae 189 (99.0) 193 (98.0)Aminoglycoside‐R 51 (27.0) 50 (25.9)ESBL 50 (26.5) 57 (29.5)Carbapenem‐R 9 (4.8) 6 (3.1)
Escherichia coli 126 (66.0) 137 (69.5)Aminoglycoside‐R 23 (18.3) 26 (19.0)ESBL 20 (15.9) 28 (20.4)Carbapenem‐R 0 0
Klebsiella pneumoniae 33 (17.3) 43 (21.8)Aminoglycoside‐R 18 (54.5) 20 (46.5)ESBL 20 (60.6) 26 (60.5)Carbapenem‐R 0 1 (2.3)
Enterobacter cloacae 15 (7.9) 3 (1.5)Aminoglycoside‐R 5 (33.3) 2 (66.7)ESBL 7 (46.7) 2 (66.7)Carbapenem‐R 0 0
Proteus mirabilis 11 (5.8) 7 (3.6)Aminoglycoside‐R 5 (45.5) 3 (42.9)ESBL 3 (27.3) 1 (14.3)Carbapenem‐R 7 (63.6) 5 (71.4)
Note: All pathogens were susceptible to plazomicinand meropenem. Table includes uropathogens that infected more than 10 subjects.
Aminoglycoside‐R = not susceptible to amikacin, gentamicin, or tobramycin
Carbapenem‐R = not susceptible to imipenem or doripenem
ESBL = pathogens that produce extended‐spectrum beta‐lactamases

9
Proportion of Subjects Administered IV Drug Only or Oral Drug Following IV
mMITT populationPlazomicin (N=191)
Meropenem(N=197)
IV only 37 (19.4%) 46 (23.4%)
IV then oral
Oral Levofloxacin 128 (67%) 121 (61.4%)
Other Approved Oral 26 (13.6%) 30 (15.2%)
10
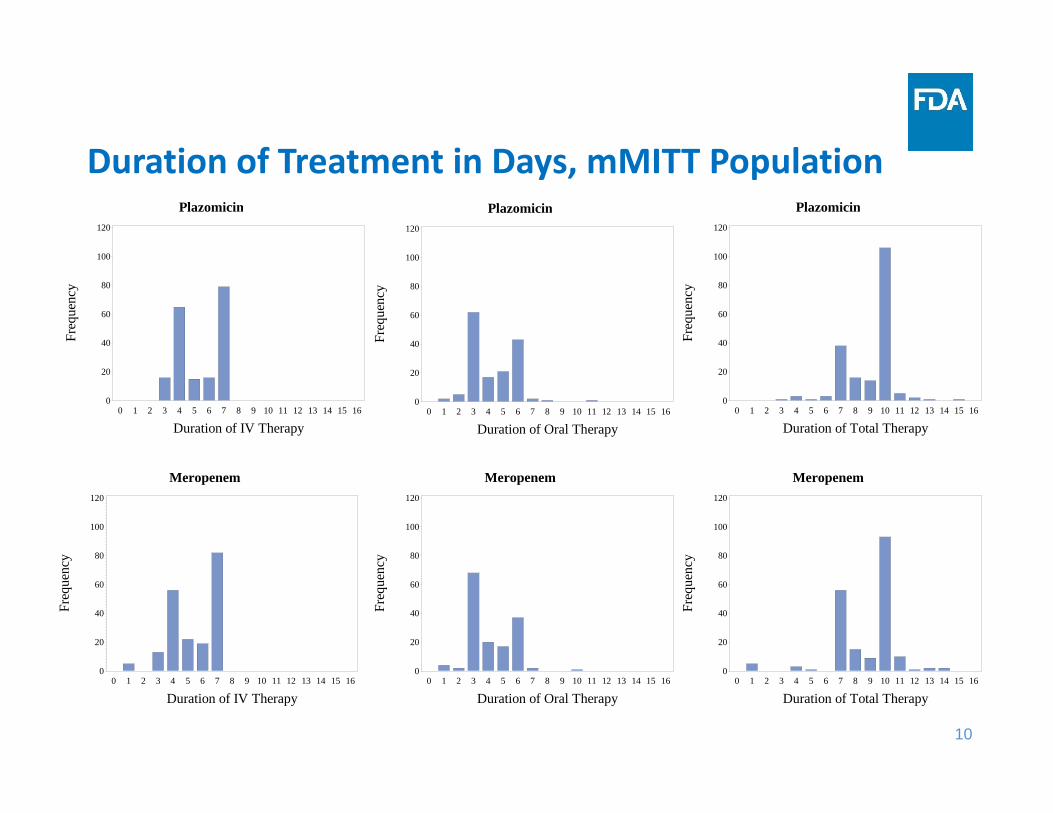
Duration of Treatment in Days, mMITT PopulationPlazomicin
Freq
uenc
y
0
20
40
60
80
100
120
Duration of IV Therapy0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
Meropenem
Freq
uenc
y
0
20
40
60
80
100
120
Duration of IV Therapy0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
Plazomicin
Freq
uenc
y 0
20
40
60
80
100
120
Duration of Oral Therapy0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
Meropenem
Freq
uenc
y
0
20
40
60
80
100
120
Duration of Oral Therapy0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
Plazomicin
Freq
uenc
y
0
20
40
60
80
100
120
Duration of Total Therapy0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
Meropenem
Freq
uenc
y 0
20
40
60
80
100
120
Duration of Total Therapy0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
11
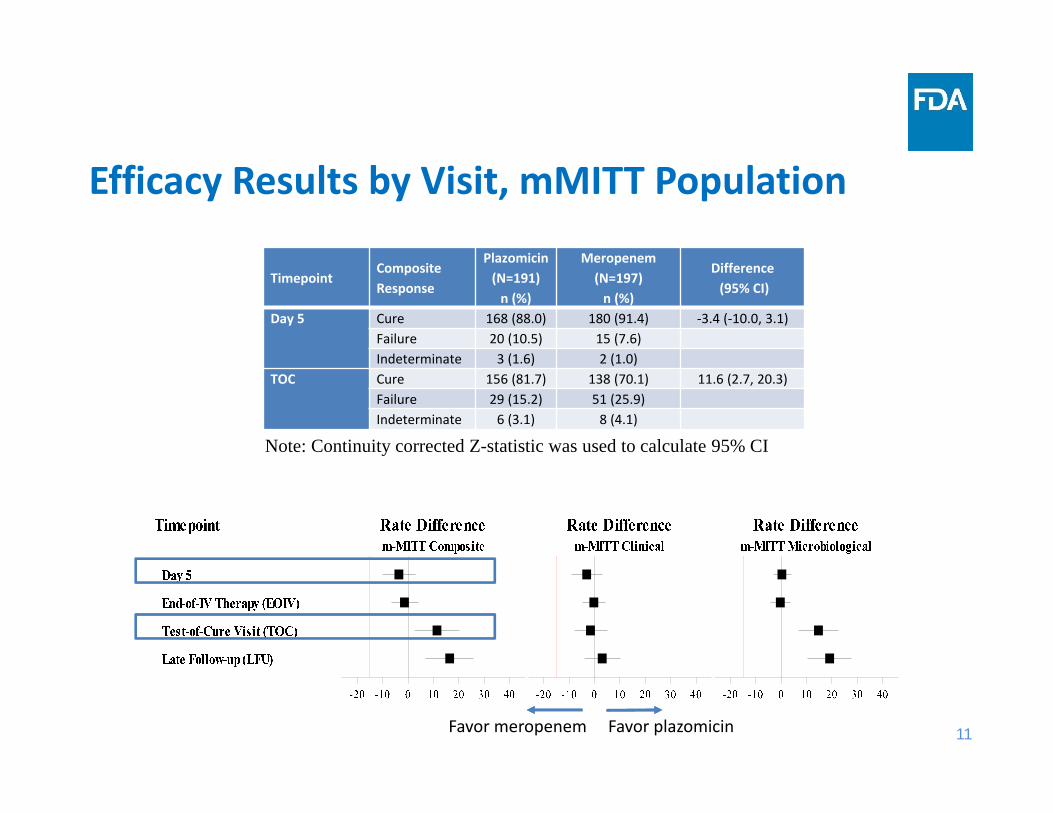
Efficacy Results by Visit, mMITT Population
TimepointComposite Response
Plazomicin(N=191)n (%)
Meropenem(N=197)n (%)
Difference(95% CI)
Day 5 Cure 168 (88.0) 180 (91.4) ‐3.4 (‐10.0, 3.1)Failure 20 (10.5) 15 (7.6)Indeterminate 3 (1.6) 2 (1.0)
TOC Cure 156 (81.7) 138 (70.1) 11.6 (2.7, 20.3)Failure 29 (15.2) 51 (25.9)Indeterminate 6 (3.1) 8 (4.1)
Note: Continuity corrected Z-statistic was used to calculate 95% CI
Favor plazomicinFavor meropenem
12
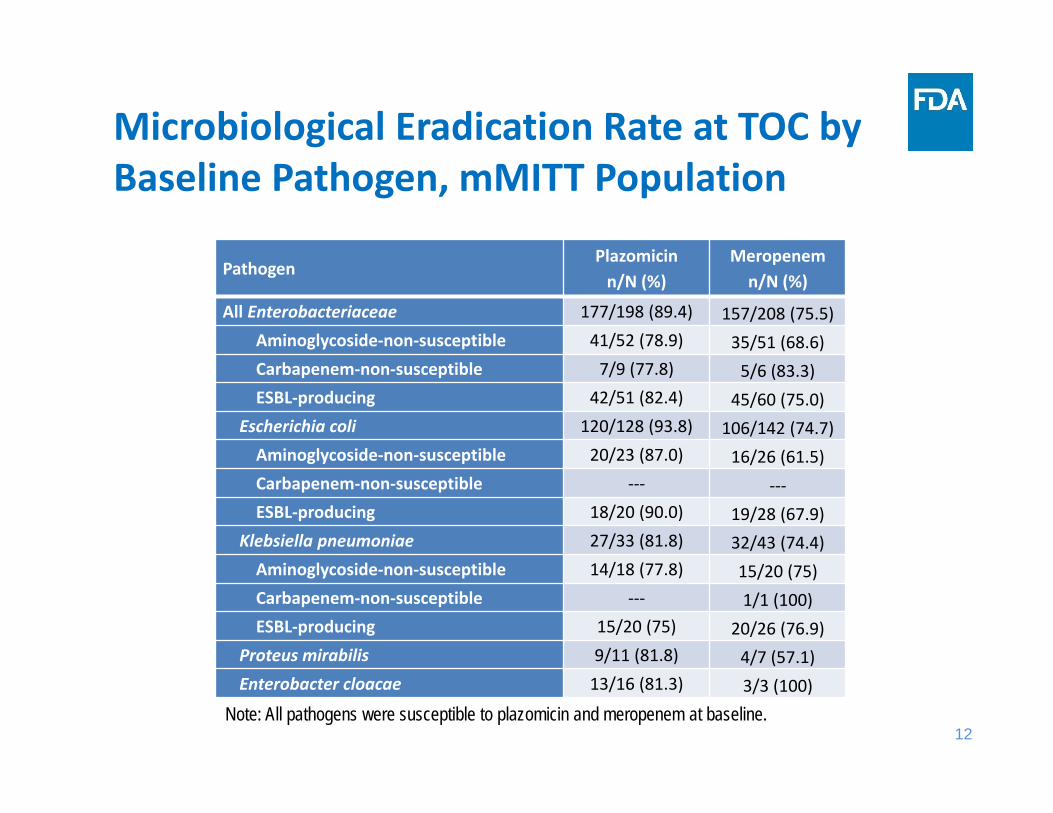
Microbiological Eradication Rate at TOC by Baseline Pathogen, mMITT Population
PathogenPlazomicinn/N (%)
Meropenemn/N (%)
All Enterobacteriaceae 177/198 (89.4) 157/208 (75.5)Aminoglycoside‐non‐susceptible 41/52 (78.9) 35/51 (68.6)Carbapenem‐non‐susceptible 7/9 (77.8) 5/6 (83.3)ESBL‐producing 42/51 (82.4) 45/60 (75.0)
Escherichia coli 120/128 (93.8) 106/142 (74.7)Aminoglycoside‐non‐susceptible 20/23 (87.0) 16/26 (61.5)Carbapenem‐non‐susceptible ‐‐‐ ‐‐‐ESBL‐producing 18/20 (90.0) 19/28 (67.9)
Klebsiella pneumoniae 27/33 (81.8) 32/43 (74.4)Aminoglycoside‐non‐susceptible 14/18 (77.8) 15/20 (75)Carbapenem‐non‐susceptible ‐‐‐ 1/1 (100)ESBL‐producing 15/20 (75) 20/26 (76.9)
Proteus mirabilis 9/11 (81.8) 4/7 (57.1)Enterobacter cloacae 13/16 (81.3) 3/3 (100)
Note: All pathogens were susceptible to plazomicin and meropenem at baseline.
13
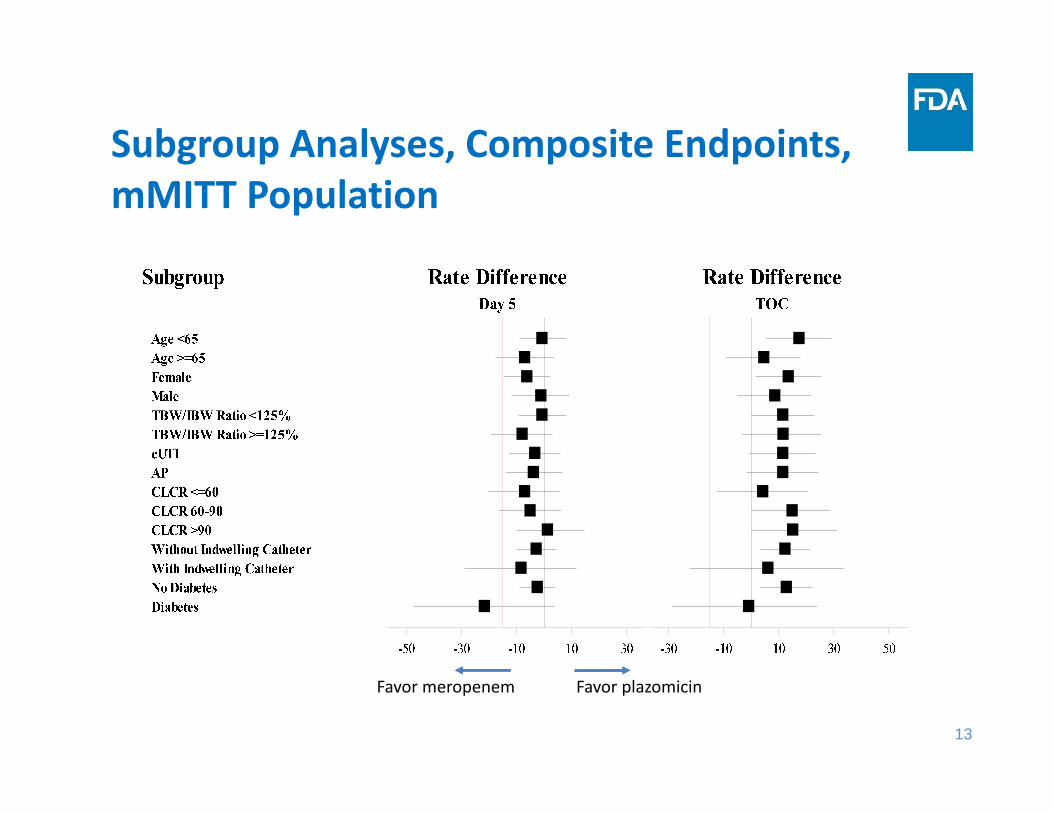
Subgroup Analyses, Composite Endpoints, mMITT Population
Favor plazomicinFavor meropenem
14
Efficacy Summary
• Plazomicin was non‐inferior to meropenem based on the pre‐specified NI margin of ‐15%.
• The efficacy findings were robust to the handling of indeterminate data
• Study was primarily conducted in Eastern European countries and white patients.

Presentation of Efficacy for Bloodstream Infections
Antimicrobial Drugs Advisory Committee MeetingMay 2, 2018
Daniel Rubin, PhDStatistical Reviewer
Division of Biometrics IV, Office of Biostatistics, Office of Translational Sciences, CDER, FDA
2
Outline
• Study 007 design and results
• Statistical issues limiting superiority conclusions
• Alternate analysis and consideration of noninferiority
• Summary
3
Original Study Design
• Randomized, open-label, comparison of plazomicin versus colistin for treatment of bloodstream infections (BSI) or hospital-acquired or ventilator-associated bacterial pneumonia (HABP/VABP) due to carbapenem-resistant Enterobacteriaceae (CRE), with meropenem minimum inhibitory concentrations ≥4 µg/mL
• Superiority trial
• Original primary efficacy endpoint: Day 28 all-cause mortality
• Secondary efficacy endpoints: – Clinical response at the test of cure visit 7 ± 2 days after the end of therapy– Day 14 all-cause mortality– Time-to-death through Day 28
4
Original Study Design• Primary analysis population:
– Microbiological modified intent-to-treat (mMITT) population of randomized patients who received at least one dose of study drug and had a CRE isolated from an acceptable study-qualifying baseline specimen
• Originally planned sample size: 286 patients with confirmed CRE infections
• Statistical significance level:– One-sided α = 0.05 – Thus, the usual two-sided p-value would only need to be <0.10 instead of <0.05
• FDA agreed to this statistical testing approach for the following reasons:– The high cost of failing to detect a superior therapy in an unmet need setting– A study demonstrating superiority to the colistin active comparator at this level
would likely provide strong evidence of superiority to a hypothetical placebo
5
Original Study Design
• FDA agreed to several features of the trial because this was a superiority design:– Inclusion of patients with either BSI or HABP/VABP– Enrollment of patients with positive CRE cultures anytime in the 96 hours
before randomization, even if subsequent baseline cultures were negative– Prior antibacterial therapy for up to 72 hours– Concomitant meropenem or tigecycline for the entire 7-14 day duration of
therapy. Tigecycline was to be used if the meropenem minimum inhibitory concentration was >8 µg/mL or when meropenem was contraindicated.
– Although known colistin-resistance was an exclusion criterion, patients could be in the primary analysis population if resistance to the baseline pathogen was identified after enrollment
– Intent-to-treat analysis approach did not consider study drug discontinuations
6
Protocol Amendments• First protocol amendment:
– Changed the primary efficacy endpoint from Day 28 all-cause mortality to the composite of Day 28 all-cause mortality or significant disease-related complications (SDRCs)
– SDRCs could include new or worsening acute respiratory distress syndrome, a new lung abscess, a new empyema, a new onset of septic shock, persistent CRE bacteremia, or a new CRE bacteremia
• Second protocol amendment:– Established uncontrolled Cohort 2 so that patients ineligible for randomization
could obtain plazomicin. Included patients with cUTI, APACHE II score <15, polymicrobial infections, and colistin-resistant infections
– However, the primary efficacy analysis was to be based only on patients from randomized Cohort 1, and uncontrolled Cohort 2 would be separately analyzed
7
Enrollment Challenges
• Study halted after two years due to slow enrollment
• Final sample size of n = 37 patients in the primary analysis population of the randomized cohort
• Much smaller than the originally planned sample size of n = 286 patients

8
Statistical Analysis Plan
• Finalized after enrollment had completed, but before unblinding results
• “While the protocol-specified primary and secondary endpoints will be analyzed and traditional statistical inference measures such as p-values and/or confidence intervals will be included for descriptive purposes, no formal hypothesis testing is to be performed in this limited sample size.”
• Final primary endpoint and original primary endpoint to be presented in parallel
• Descriptive presentations to use 90% confidence intervals and one-sided p-values
9
Design Schema for Randomized Cohort 1
Source: Study 007 Clinical Study Report, Figure 1.

10
Disposition for Study 007
Source: Study 007 Clinical Study Report, Figure 4.
11
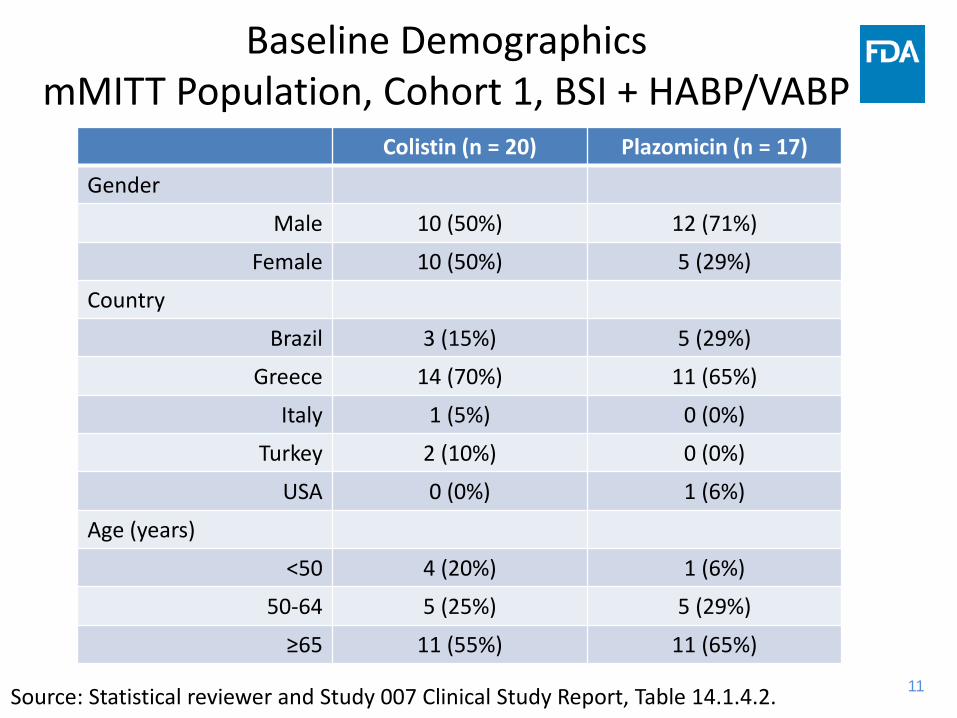
Baseline DemographicsmMITT Population, Cohort 1, BSI + HABP/VABP
Colistin (n = 20) Plazomicin (n = 17)
Gender
Male 10 (50%) 12 (71%)
Female 10 (50%) 5 (29%)
Country
Brazil 3 (15%) 5 (29%)
Greece 14 (70%) 11 (65%)
Italy 1 (5%) 0 (0%)
Turkey 2 (10%) 0 (0%)
USA 0 (0%) 1 (6%)
Age (years)
<50 4 (20%) 1 (6%)
50-64 5 (25%) 5 (29%)
≥65 11 (55%) 11 (65%)
Source: Statistical reviewer and Study 007 Clinical Study Report, Table 14.1.4.2.
12
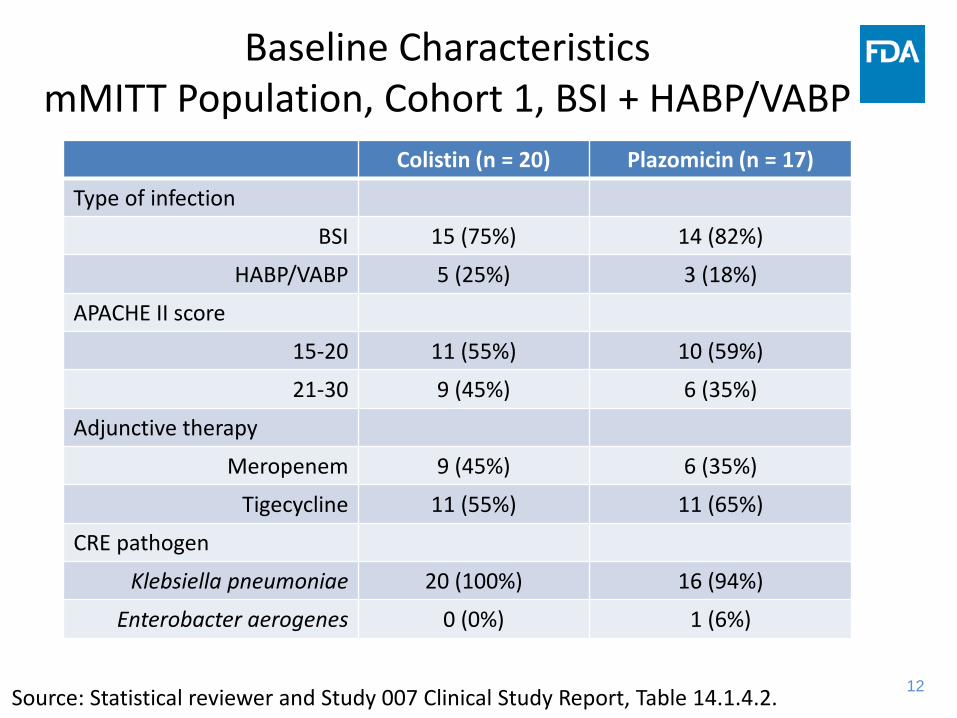
Baseline CharacteristicsmMITT Population, Cohort 1, BSI + HABP/VABP
Colistin (n = 20) Plazomicin (n = 17)
Type of infection
BSI 15 (75%) 14 (82%)
HABP/VABP 5 (25%) 3 (18%)
APACHE II score
15-20 11 (55%) 10 (59%)
21-30 9 (45%) 6 (35%)
Adjunctive therapy
Meropenem 9 (45%) 6 (35%)
Tigecycline 11 (55%) 11 (65%)
CRE pathogen
Klebsiella pneumoniae 20 (100%) 16 (94%)
Enterobacter aerogenes 0 (0%) 1 (6%)
Source: Statistical reviewer and Study 007 Clinical Study Report, Table 14.1.4.2.
13
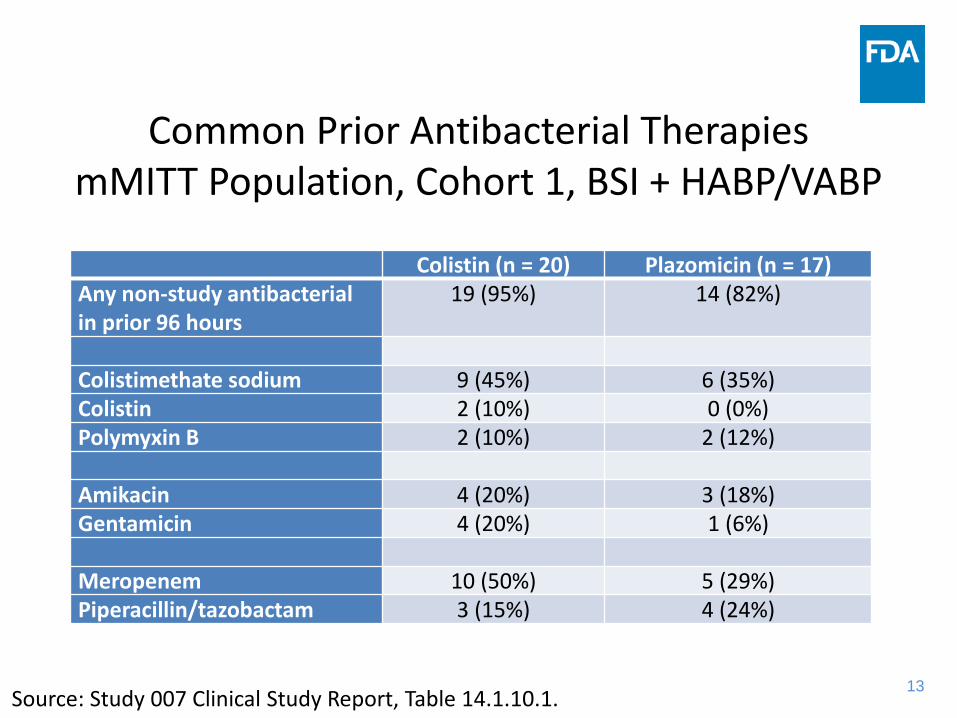
Common Prior Antibacterial TherapiesmMITT Population, Cohort 1, BSI + HABP/VABP
Colistin (n = 20) Plazomicin (n = 17)Any non-study antibacterial in prior 96 hours
19 (95%) 14 (82%)
Colistimethate sodium 9 (45%) 6 (35%)Colistin 2 (10%) 0 (0%)Polymyxin B 2 (10%) 2 (12%)
Amikacin 4 (20%) 3 (18%)Gentamicin 4 (20%) 1 (6%)
Meropenem 10 (50%) 5 (29%)Piperacillin/tazobactam 3 (15%) 4 (24%)
Source: Study 007 Clinical Study Report, Table 14.1.10.1.

14
Original and Final Primary EndpointsmMITT Population, Cohort 1, BSI + HABP/VABP
Day 28 endpoint Colistin (n = 20)
Plazomicin(n = 17)
Difference Exact 90% CI One-sided exact p-value
All-cause mortality or SDRCs
10 (50%)
4 (24%)
26% -1% to 51% 0.09
All-cause mortality 8(40%)
2(12%)
28% 1% to 52% 0.06
Two patients in each treatment group survived with a failure triggered by an SDRC: • In the colistin group 2 patients had persistent bacteremia• In the plazomicin group 1 patient had persistent bacteremia and 1 had septic shock
Source: Study 007 Clinical Study Report, Table 31.
15
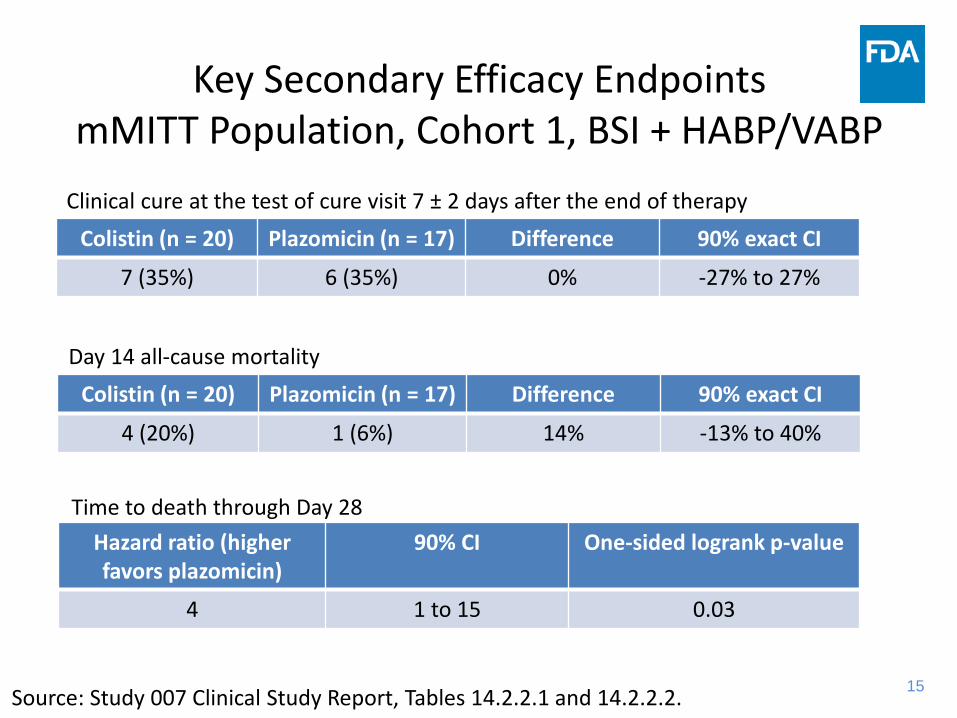
Key Secondary Efficacy EndpointsmMITT Population, Cohort 1, BSI + HABP/VABP
Colistin (n = 20) Plazomicin (n = 17) Difference 90% exact CI
7 (35%) 6 (35%) 0% -27% to 27%
Clinical cure at the test of cure visit 7 ± 2 days after the end of therapy
Day 14 all-cause mortalityColistin (n = 20) Plazomicin (n = 17) Difference 90% exact CI
4 (20%) 1 (6%) 14% -13% to 40%
Time to death through Day 28Hazard ratio (higher favors plazomicin)
90% CI One-sided logrank p-value
4 1 to 15 0.03
Source: Study 007 Clinical Study Report, Tables 14.2.2.1 and 14.2.2.2.

16
Results by Infection TypemMITT Population, Cohort 1
Day 28 all-cause mortality or SDRCs
Colistin Plazomicin Difference Exact 90% CI One-sided exact p-value
Entire mMITT 10/20 (50%)
4/17 (24%)
26% -1% to 51% 0.09
BSI 8/15(53%)
2/14(14%)
39% 9% to 66% 0.03
HABP/VABP 2/5(40%)
2/3 (67%)
Day 28 all-cause mortality
Colistin Plazomicin Difference Exact 90% CI One-sided exact p-value
Entire mMITT 8/20(40%)
2/17(12%)
28.2% 1% to 52% 0.06
BSI 6/15(40%)
1/14(7%)
33% 4% to 60% 0.05
HABP/VABP 2/5 (40%)
1/3 (33%)
Source: Study 007 Clinical Study Report, Table 32.
17
Statistical Issues Limiting Superiority Conclusions in Cohort 1
• Very small sample size substantial uncertainty for plazomicin treatment effect
• The statistical analysis plan specified use of only descriptive statistics
• Statistical superiority would not have been achieved for the final or original primary endpoint at the protocol-specified one-sided α = 0.05 significance level
• Uncertainty was expressed using 90% confidence intervals rather than the wider traditionally used 95% confidence intervals
• Possible multiplicity issues when considering two primary endpoints and results and the BSI subgroup. Focusing on particularly favorable results (e.g., mortality benefit in BSI) could unduly favor plazomicin.
18
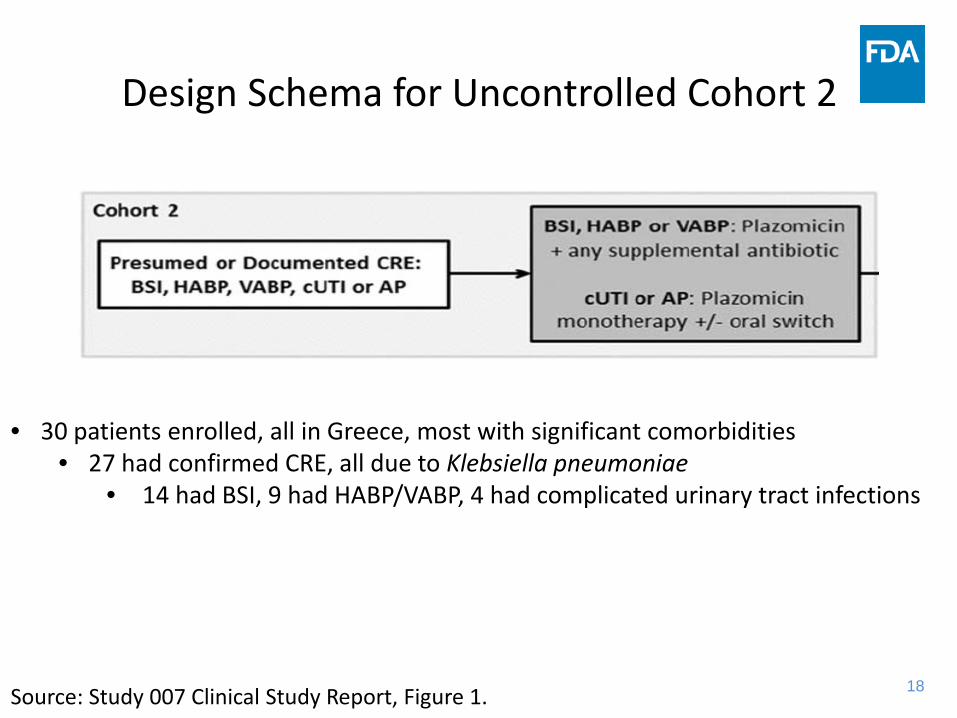
Design Schema for Uncontrolled Cohort 2
Source: Study 007 Clinical Study Report, Figure 1.
• 30 patients enrolled, all in Greece, most with significant comorbidities• 27 had confirmed CRE, all due to Klebsiella pneumoniae
• 14 had BSI, 9 had HABP/VABP, 4 had complicated urinary tract infections
19
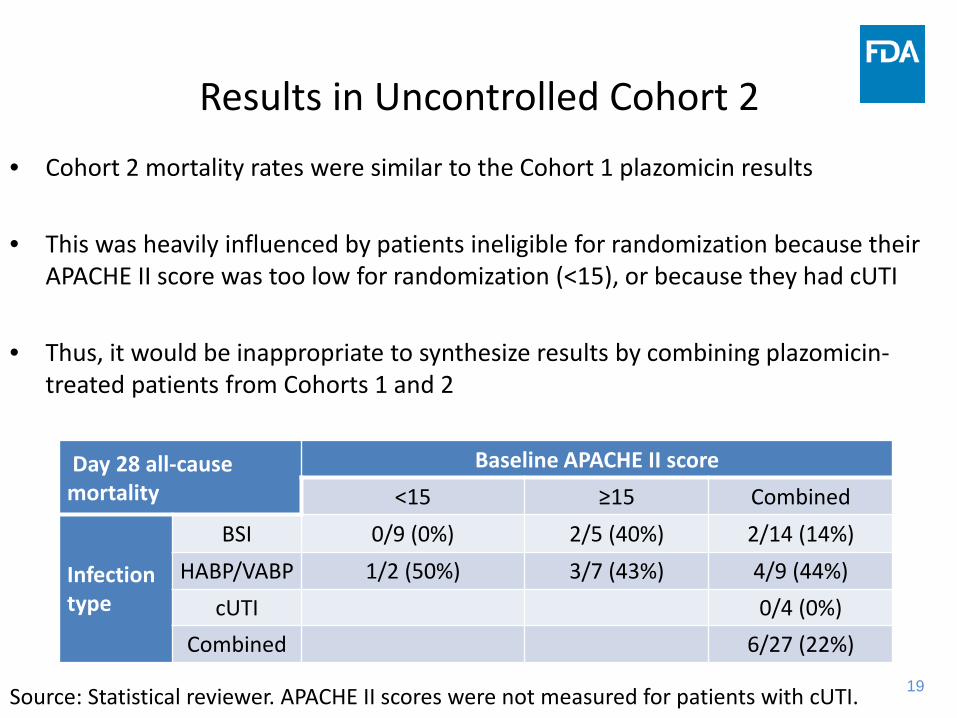
Results in Uncontrolled Cohort 2• Cohort 2 mortality rates were similar to the Cohort 1 plazomicin results
• This was heavily influenced by patients ineligible for randomization because their APACHE II score was too low for randomization (<15), or because they had cUTI
• Thus, it would be inappropriate to synthesize results by combining plazomicin-treated patients from Cohorts 1 and 2
Day 28 all-cause mortality in Cohort 2, mMITT populationDay 28 all-cause mortality
Baseline APACHE II score<15 ≥15 Combined
Infection type
BSI 0/9 (0%) 2/5 (40%) 2/14 (14%)HABP/VABP 1/2 (50%) 3/7 (43%) 4/9 (44%)
cUTI 0/4 (0%)Combined 6/27 (22%)
Source: Statistical reviewer. APACHE II scores were not measured for patients with cUTI.
20
Statistical Reviewer’s Analytic Choices
• Focus on randomized Cohort 1 and the entire mMITT primary analysis population:– Included 29 BSI patients and 8 HABP/VABP patients with CRE infections
• Focus on the primary endpoint from the final protocol amendment: – Day 28 all-cause mortality or SDRCs
• Focus on exact 95% confidence intervals– The FDA’s acceptance of 90% confidence intervals was due to the original superiority design
• Rationale: – This is the closest one can come to having the statistical protection of pre-specification– This a mortality-driven endpoint in a BSI-driven study population
• Drawbacks to this analysis:– SDRC events based on persistent bacteremia may be less meaningful than mortality events– The applicant is only seeking a BSI indication and not a HABP/VABP indication– Possible to envision more efficient analyses (e.g., time-to-event data, ordinal endpoints,
covariate adjustment)
21
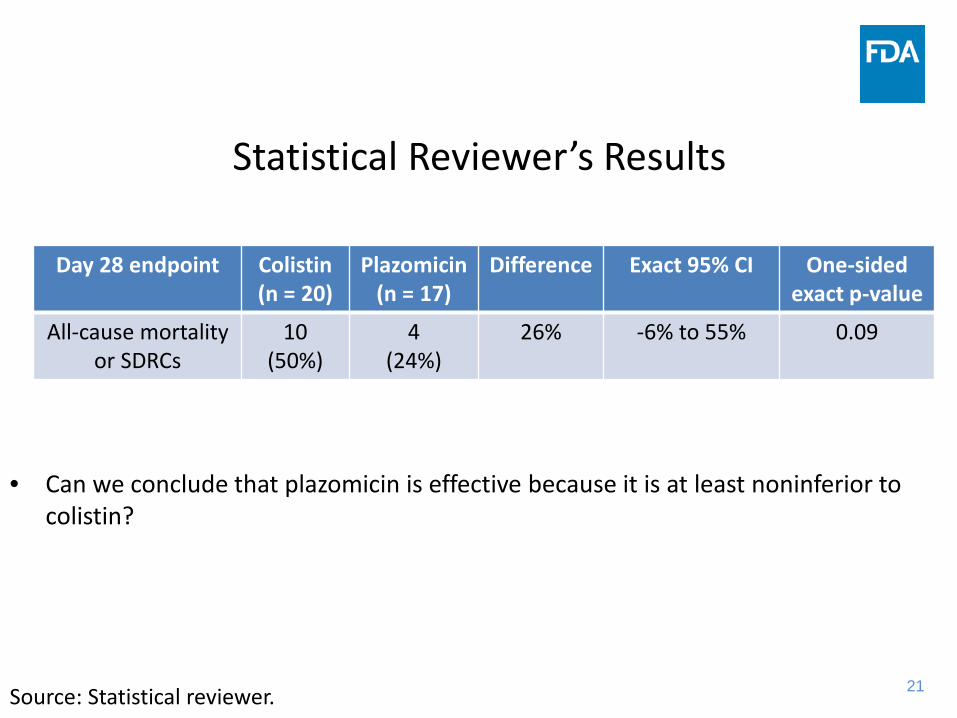
Statistical Reviewer’s Results
Day 28 endpoint Colistin (n = 20)
Plazomicin(n = 17)
Difference Exact 95% CI One-sided exact p-value
All-cause mortality or SDRCs
10 (50%)
4 (24%)
26% -6% to 55% 0.09
Source: Statistical reviewer.
• Can we conclude that plazomicin is effective because it is at least noninferior to colistin?

22
Why Might Noninferiority be Considered?
• The lower confidence limit of -6% for the (colistin – plazomicin) difference was based on conservative choices, in that other choices for the endpoint, analysis population, and confidence interval would have been more favorable to plazomicin
• Noninferiority could still in principle imply a favorable benefit-to-risk profile, if a very small efficacy decrement is counterbalanced by much better safety than colistin. However, any nontrivial increase in mortality risk would likely offset improved rates of reversible nephrotoxicity.
23
Limitations of Noninferiority Analysis
• An efficacy conclusion based on noninferiority would require reasonable confidence in there being a large (colistin – hypothetical placebo) effect in the setting of this study
• There are limited data with which to quantify the efficacy of colistin
• Pre-specification of the noninferiority margin is preferable from a regulatory practice standpoint, but is not a statistical multiplicity issue
• Several design features were agreed to when planning a superiority trial, but which may have impacted the magnitude of the (colistin – hypothetical placebo) effect, such the degree of allowed prior and concomitant antibacterial therapy
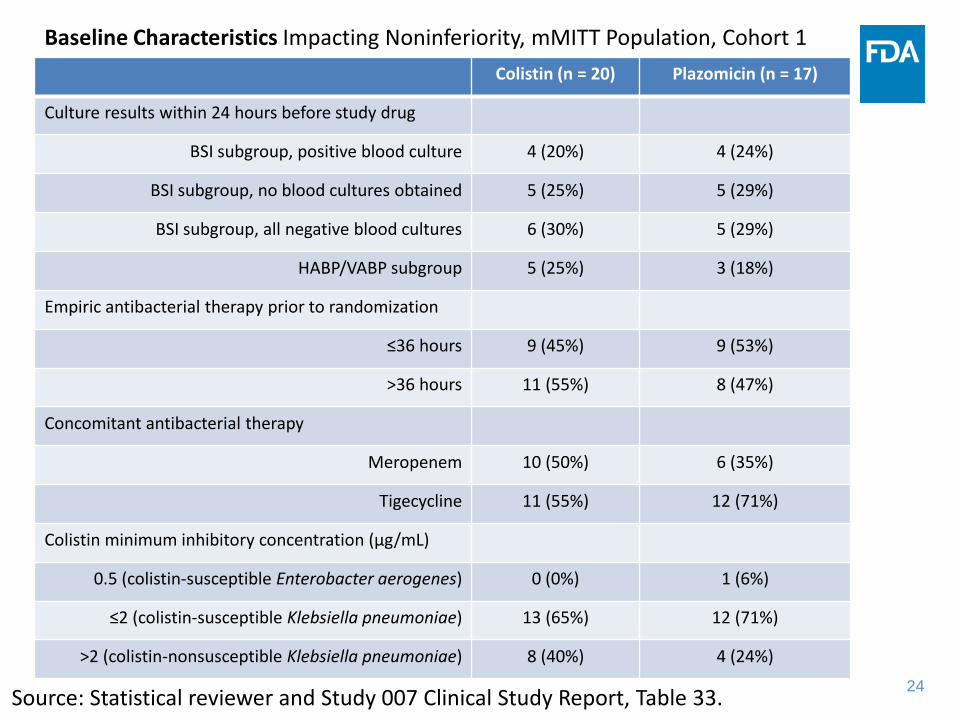
24Source: Statistical reviewer and Study 007 Clinical Study Report, Table 33.
Colistin (n = 20) Plazomicin (n = 17)
Culture results within 24 hours before study drug
BSI subgroup, positive blood culture 4 (20%) 4 (24%)
BSI subgroup, no blood cultures obtained 5 (25%) 5 (29%)
BSI subgroup, all negative blood cultures 6 (30%) 5 (29%)
HABP/VABP subgroup 5 (25%) 3 (18%)
Empiric antibacterial therapy prior to randomization
≤36 hours 9 (45%) 9 (53%)
>36 hours 11 (55%) 8 (47%)
Concomitant antibacterial therapy
Meropenem 10 (50%) 6 (35%)
Tigecycline 11 (55%) 12 (71%)
Colistin minimum inhibitory concentration (µg/mL)
0.5 (colistin-susceptible Enterobacter aerogenes) 0 (0%) 1 (6%)
≤2 (colistin-susceptible Klebsiella pneumoniae) 13 (65%) 12 (71%)
>2 (colistin-nonsusceptible Klebsiella pneumoniae) 8 (40%) 4 (24%)
Baseline Characteristics Impacting Noninferiority, mMITT Population, Cohort 1
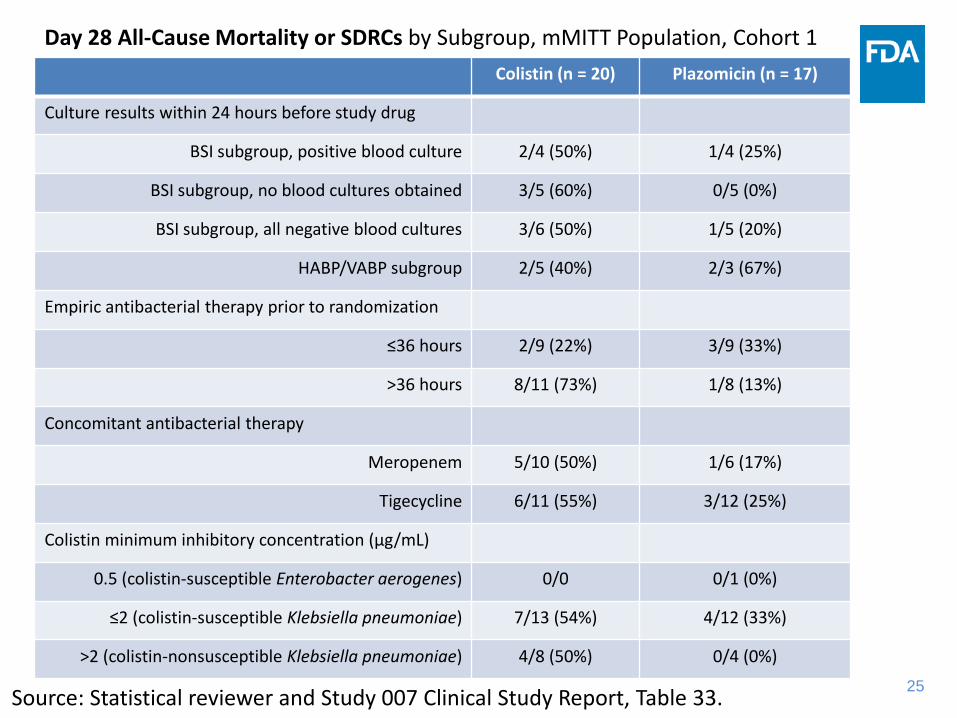
25Source: Statistical reviewer and Study 007 Clinical Study Report, Table 33.
Colistin (n = 20) Plazomicin (n = 17)
Culture results within 24 hours before study drug
BSI subgroup, positive blood culture 2/4 (50%) 1/4 (25%)
BSI subgroup, no blood cultures obtained 3/5 (60%) 0/5 (0%)
BSI subgroup, all negative blood cultures 3/6 (50%) 1/5 (20%)
HABP/VABP subgroup 2/5 (40%) 2/3 (67%)
Empiric antibacterial therapy prior to randomization
≤36 hours 2/9 (22%) 3/9 (33%)
>36 hours 8/11 (73%) 1/8 (13%)
Concomitant antibacterial therapy
Meropenem 5/10 (50%) 1/6 (17%)
Tigecycline 6/11 (55%) 3/12 (25%)
Colistin minimum inhibitory concentration (µg/mL)
0.5 (colistin-susceptible Enterobacter aerogenes) 0/0 0/1 (0%)
≤2 (colistin-susceptible Klebsiella pneumoniae) 7/13 (54%) 4/12 (33%)
>2 (colistin-nonsusceptible Klebsiella pneumoniae) 4/8 (50%) 0/4 (0%)
Day 28 All-Cause Mortality or SDRCs by Subgroup, mMITT Population, Cohort 1

26
Nonadherence• Two plazomicin group BSI patients discontinued therapy on Day 1 due to
microbiological findings, switched to regimens that included polymyxins, and were counted as successes for the plazomicin group for both primary endpoints
• Two colistin group patients also had very early therapy discontinuations. Both died and were considered failures for the colistin group.
• Results for the original and amended primary endpoint if excluding the plazomicin group patients with Day 1 therapy discontinuations, mMITT population, Cohort 1
Day 28 endpoint Colistin (n = 20)
Plazomicin(n = 15)
Difference Exact 95% CI One-sided exact p-value
All-cause mortality or SDRCs
10 (50%)
4(27%)
23% -11% to 54% 0.15
All-cause mortality 8(40%)
2(13%)
27% -6% to 57% 0.09
Source: Statistical reviewer

27
Efficacy Summary
• Numerical trends favored plazomicin compared to colistin
• There are statistical limitations to concluding that plazomicin has superior efficacy
• A conservative analysis is to focus on the primary endpoint and analysis population from the final protocol, using 95% confidence intervals. This provides evidence that the (plazomicin - colistin) difference in rates of Day 28 all-cause mortality or SDRCs is not larger than 6%. However, noninferiority assessments are complicated by design features agreed to when planning a superiority trial.
Bloodstream Infection (BSI) Efficacy-Clinical Review
Shrimant Mishra, MD MPHMedical Officer, DAIP
2
Clinical Efficacy Review• Case Report Form (CRF) review of all BSI cases in
Cohort 1 (29 cases)– blood culture records– presence of lines; dates of line removal– source workup– dates of study drug administration– prior drug therapy– classification as success/failure

3
Uncertainty Regarding Primary Bacteremias
• Protocol definitions for defining source of bacteremia – primary, secondary, central-line associated– eCRF pages to document source
• No standardized procedure for source determination– Bacteremias defined as primary despite limited workup– Two Examples
• Subject with femoral line in; qualifying culture was a peripheral culture (one set) with none taken from femoral line
• Subject with K. pneumoniae from catheter and peripheral cultures at baseline but still called primary bacteremia (differing resistance patterns CRE vs. non-CRE)

4
Protocol Definition of BSI Source
- Study 007 Protocol
5
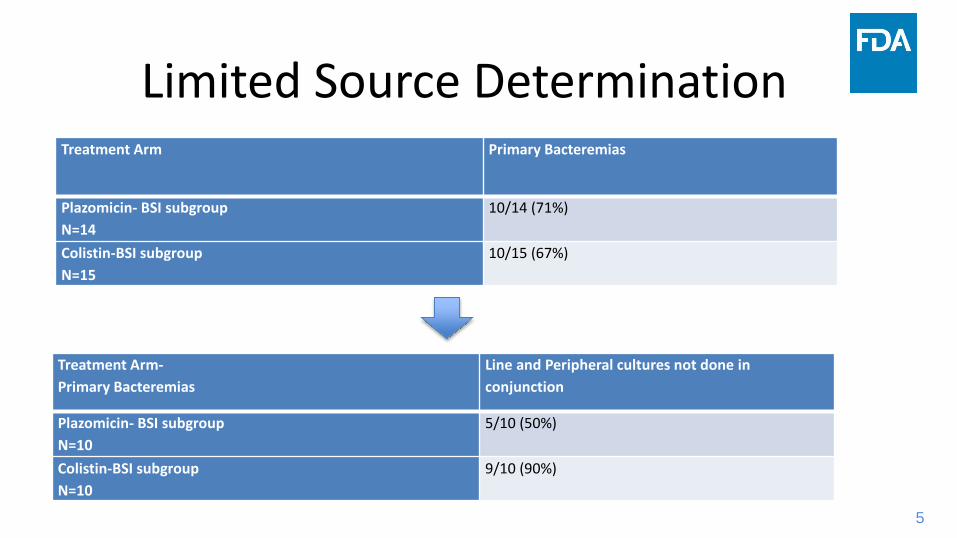
Limited Source DeterminationTreatment Arm Primary Bacteremias
Plazomicin- BSI subgroupN=14
10/14 (71%)
Colistin-BSI subgroupN=15
10/15 (67%)
Treatment Arm-Primary Bacteremias
Line and Peripheral cultures not done in conjunction
Plazomicin- BSI subgroupN=10
5/10 (50%)
Colistin-BSI subgroupN=10
9/10 (90%)

6
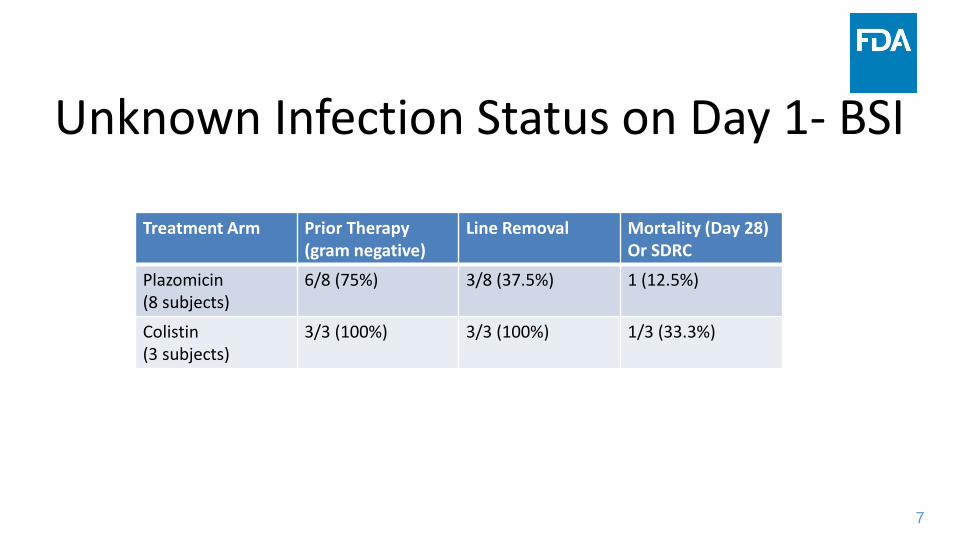
Uncertain Diagnosis of Bacteremia at Baseline
• In several subjects there was uncertainty regarding the diagnosis of bacteremia on Day 1
• BSI CRFs evaluated in Cohort 1– 8/14 (57%) plazomicin and 3/15 (20%) colistin subjects had negative/no cultures at the
time of starting treatment and remained culture negative for baseline CRE pathogen throughout the rest of study
– Only 4 subjects in each arm that had positive cultures within 24 hrs. of baseline
• Were these subjects essentially adequately treated already? – Prior therapy (gram negative therapy including colistin, meropenem,
tigecycline, aminoglycoside)– Line removed/replaced around Day 1
7
Unknown Infection Status on Day 1- BSI
Treatment Arm Prior Therapy (gram negative)
Line Removal Mortality (Day 28)Or SDRC
Plazomicin(8 subjects)
6/8 (75%) 3/8 (37.5%) 1 (12.5%)
Colistin(3 subjects)
3/3 (100%) 3/3 (100%) 1/3 (33.3%)
8
Efficacy Summary• Numerical trends favored plazomicin compared to colistin
• There are statistical limitations to concluding that plazomicin has superior efficacy
• A conservative analysis is to focus on the primary endpoint and analysis population from the final protocol, using 95% confidence intervals. This provides evidence that the (plazomicin - colistin) difference in rates of Day 28 all-cause mortality or SDRCs is not larger than 6%. However, noninferiority assessments are complicated by design features agreed to when planning a superiority trial.
1
Plazomicin
Overview of Clinical Safety
Shrimant Mishra, MD, MPHMedical Officer
Division of Anti-Infective Products
Antimicrobial Drugs Advisory Committee MeetingMay 2, 2018
1
2
Plazomicin: Overview of Clinical Safety
Summary of Drug ExposureSafety Population Subject DemographicsMajor Safety Results
DeathsSerious Adverse Events
Treatment Emergent Adverse Events Drug Class Associated Adverse Events of Interest
NephrotoxicityOtotoxicity
Conclusions
Outline
2
3
Clinical Development Program6 phase 1 studies
– QT, study in renal impairment, PK/safety– 2 studies received after NDA submission (mass balance, metformin drug
interaction)1 phase 2 study
– complicated urinary tract infections (cUTI)2 phase 3 studies
– cUTI and bloodstream infection (BSI)
Focus is on phase 2 and 3 safety findings, primarily in cUTI
3
4
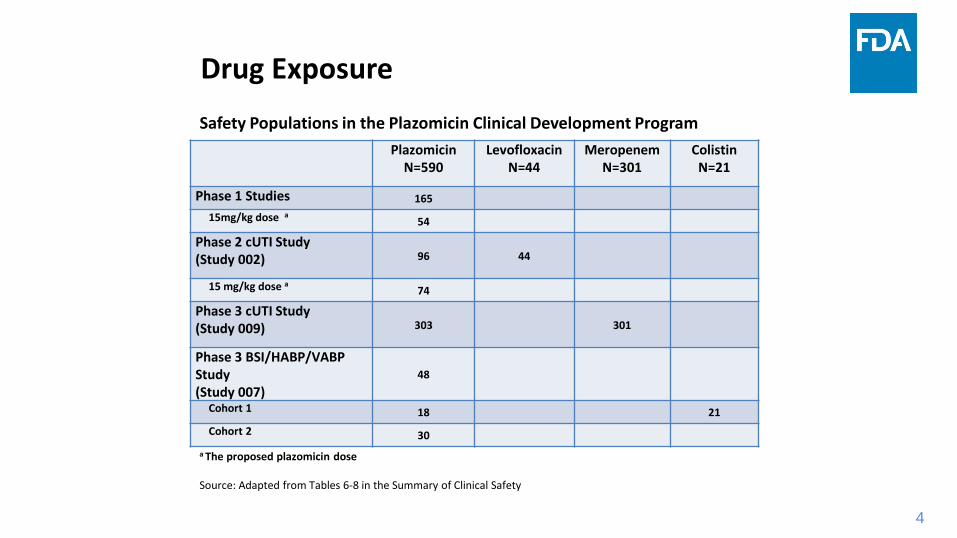
Drug ExposureSafety Populations in the Plazomicin Clinical Development Program
4
PlazomicinN=590
LevofloxacinN=44
MeropenemN=301
ColistinN=21
Phase 1 Studies 16515mg/kg dose a 54
Phase 2 cUTI Study (Study 002) 96 44
15 mg/kg dose a 74
Phase 3 cUTI Study (Study 009) 303 301
Phase 3 BSI/HABP/VABP Study (Study 007)
48
Cohort 1 18 21 Cohort 2 30
a The proposed plazomicin dose
Source: Adapted from Tables 6-8 in the Summary of Clinical Safety

5
Drug Exposure
Primary Safety Analysis Population: Subjects from phase 2 and 3 cUTI trials who received the proposed dose of 15 mg/kg plazomicin
- Median duration of treatment was 5 days in the plazomicin and comparator arms.
- No subject received greater than 7 days of therapy.
- Less than 15% of subjects in any arm received fewer than 4 days of therapy.
5
6
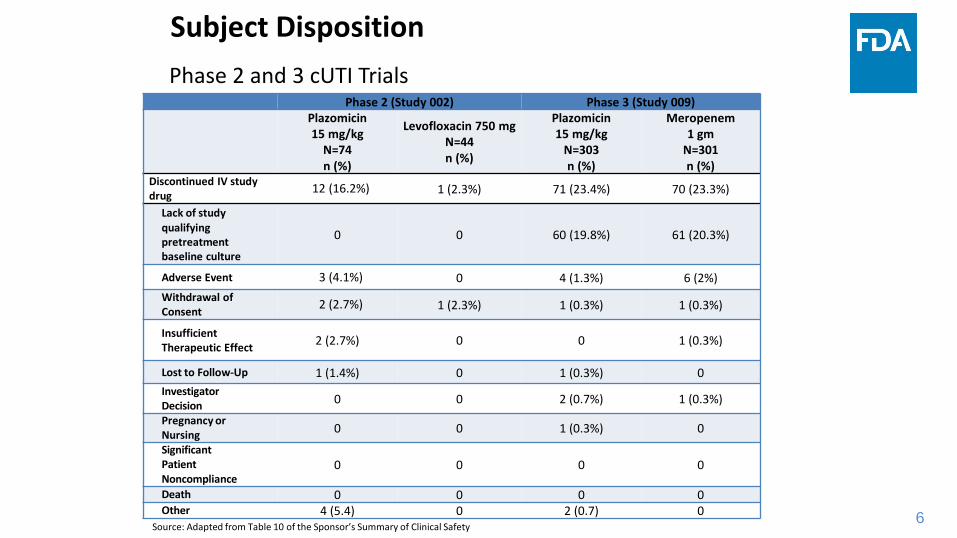
Subject DispositionPhase 2 and 3 cUTI Trials
6
Phase 2 (Study 002) Phase 3 (Study 009)Plazomicin15 mg/kg
N=74 n (%)
Levofloxacin 750 mgN=44 n (%)
Plazomicin15 mg/kg
N=303 n (%)
Meropenem 1 gm
N=301 n (%)
Discontinued IV studydrug 12 (16.2%) 1 (2.3%) 71 (23.4%) 70 (23.3%)
Lack of studyqualifying pretreatment baseline culture
0 0 60 (19.8%) 61 (20.3%)
Adverse Event 3 (4.1%) 0 4 (1.3%) 6 (2%)Withdrawal of Consent 2 (2.7%) 1 (2.3%) 1 (0.3%) 1 (0.3%)
InsufficientTherapeutic Effect 2 (2.7%) 0 0 1 (0.3%)
Lost to Follow-Up 1 (1.4%) 0 1 (0.3%) 0InvestigatorDecision 0 0 2 (0.7%) 1 (0.3%)
Pregnancy orNursing 0 0 1 (0.3%) 0
SignificantPatient Noncompliance
0 0 0 0
Death 0 0 0 0Other 4 (5.4) 0 2 (0.7) 0
Source: Adapted from Table 10 of the Sponsor’s Summary of Clinical Safety
7
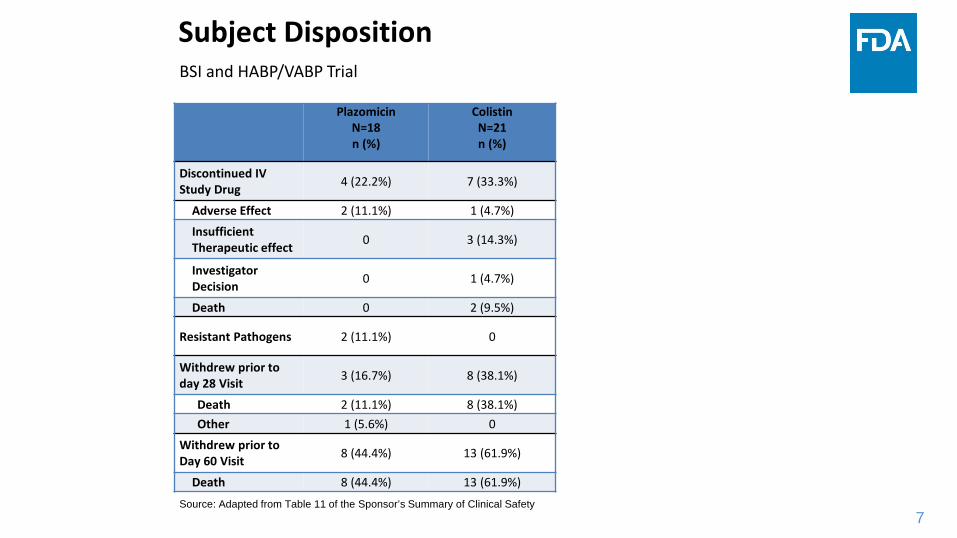
Subject DispositionBSI and HABP/VABP Trial
7Source: Adapted from Table 11 of the Sponsor’s Summary of Clinical Safety
PlazomicinN=18n (%)
ColistinN=21n (%)
Discontinued IV Study Drug 4 (22.2%) 7 (33.3%)
Adverse Effect 2 (11.1%) 1 (4.7%)
Insufficient Therapeutic effect 0 3 (14.3%)
Investigator Decision 0 1 (4.7%)
Death 0 2 (9.5%)
Resistant Pathogens 2 (11.1%) 0
Withdrew prior to day 28 Visit 3 (16.7%) 8 (38.1%)
Death 2 (11.1%) 8 (38.1%)Other 1 (5.6%) 0
Withdrew prior to Day 60 Visit 8 (44.4%) 13 (61.9%)
Death 8 (44.4%) 13 (61.9%)
8
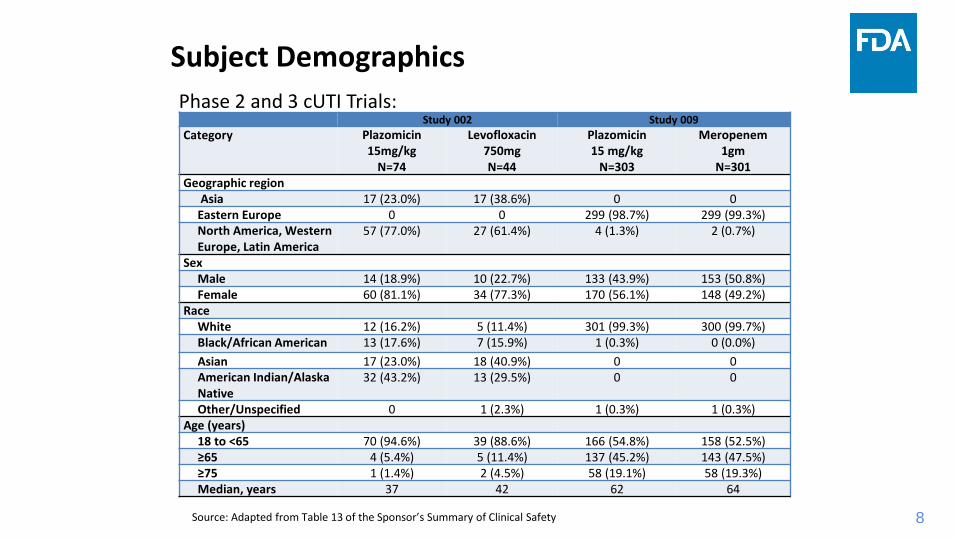
Subject DemographicsPhase 2 and 3 cUTI Trials:
8
Study 002 Study 009Category Plazomicin
15mg/kgN=74
Levofloxacin750mgN=44
Plazomicin15 mg/kg
N=303
Meropenem1gm
N=301Geographic region
Asia 17 (23.0%) 17 (38.6%) 0 0Eastern Europe 0 0 299 (98.7%) 299 (99.3%)North America, Western Europe, Latin America
57 (77.0%) 27 (61.4%) 4 (1.3%) 2 (0.7%)
SexMale 14 (18.9%) 10 (22.7%) 133 (43.9%) 153 (50.8%)Female 60 (81.1%) 34 (77.3%) 170 (56.1%) 148 (49.2%)
RaceWhite 12 (16.2%) 5 (11.4%) 301 (99.3%) 300 (99.7%)Black/African American 13 (17.6%) 7 (15.9%) 1 (0.3%) 0 (0.0%)Asian 17 (23.0%) 18 (40.9%) 0 0American Indian/Alaska Native
32 (43.2%) 13 (29.5%) 0 0
Other/Unspecified 0 1 (2.3%) 1 (0.3%) 1 (0.3%)Age (years)
18 to <65 70 (94.6%) 39 (88.6%) 166 (54.8%) 158 (52.5%)≥65 4 (5.4%) 5 (11.4%) 137 (45.2%) 143 (47.5%)≥75 1 (1.4%) 2 (4.5%) 58 (19.1%) 58 (19.3%)Median, years 37 42 62 64
Source: Adapted from Table 13 of the Sponsor’s Summary of Clinical Safety

9
Subject DemographicsPhase 2 and 3 cUTI Trials:
9
Study 002 Study 009Category Plazomicin
15mg/kgN=74
Levofloxacin750mgN=44
Plazomicin15 mg/kg
N=303
Meropenem1gm
N=301Infection Type
cUTI 33 (44.6%) 20 (45.5%) 177 (58.4%) 179 (59.5%)AP 41 (55.4%) 24 (54.5%) 126 (41.6%) 122 (40.5%)
Baseline CrCl (ml/min)>120 8 (10.8%) 6 (13.6% ) 28 (9.2%) 19 (6.3%)>90-120 26 (35.1%) 11 (25.0%) 65 (21.5%) 62 (20.6%)>60-90 23 (31.1%) 16 (36.4%) 115 (38.0%) 111 (36.9%)>30-60 15 (20.3%) 6 (13.6%) 91 (30.0%) 103 (34.2%)≤30 0 2 (4.5%) 1 (0.3%) 3 (1.0%)Missing 2 (2.7%) 3 (6.8%) 3 (1.0%) 3 (1.0%)
Source: Adapted from Table 13 of the Sponsor’s Summary of Clinical Safety

10
DeathsPhase 2 and 3 cUTI Trials:
One reported death involved a 63-year-old White woman who was admitted for pyelonephritis. She received one dose of plazomicin and then was discontinued from study drug due to acute kidney injury (switched to piperacillin-tazobactam and then meropenem).
At the time of discontinuation, she was found to have metastatic uterine cancer with possible involvement of the lungs and liver.
Renal function declined and she underwent hemodialysis. On Day 17 she refused further hemodialysis and died the following day.
The subject had significant comorbidities, but a causal relationship with plazomicincannot be fully excluded due to its nephrotoxic effects.
10

11
DeathsBSI and HABP/VABP Trial Cohort 1 (Study 007):
11
Subjects with Fatal SAE (Day 60)Plazomicin
N=18n (%)
ColistinN= 21n (%)
Total 8 (44.4%) 13 (61.9%)Septic Shock 3 (16.7%) 5 (23.8%)Cardiac Arrest 1 (5.6%) 1 (4.8%)Cardiorespiratory arrest 1 (5.6%) 0Lung Infection 1 (5.6%) 0Pneumonia 1 (5.6%) 0Pneumonitis chemical 1 (5.6%) 0Multiorgan dysfunction syndrome 0 1 (4.8%)
Pneumonia aspiration 0 1 (4.8%)Bladder Cancer 0 1 (4.8%)Cerebral ischemia 0 1 (4.8%)Pulmonary embolism 0 1 (4.8%)Sepsis 0 2 (9.5%)
Source: Adapted from Table 25 of the Sponsor’s Summary of Clinical Safety
12
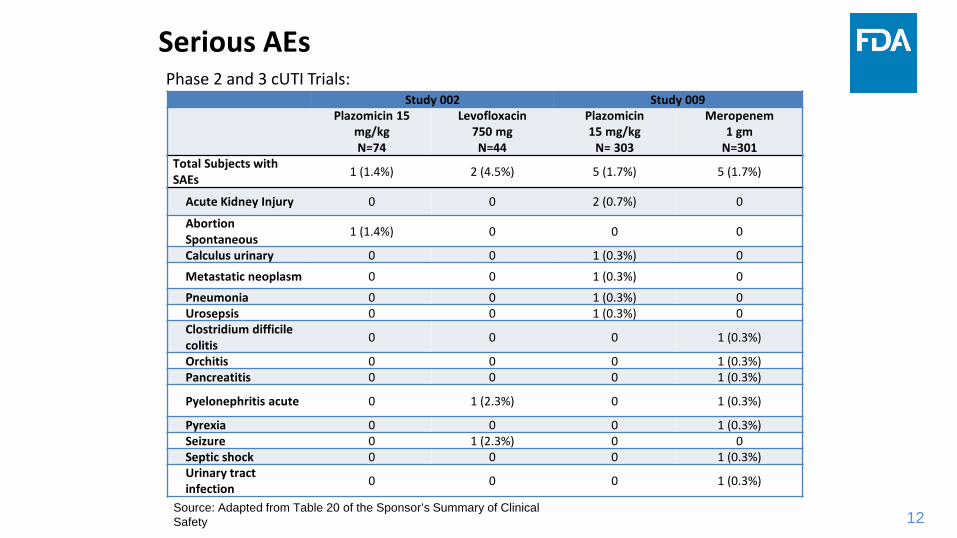
Serious AEsPhase 2 and 3 cUTI Trials:
12
Study 002 Study 009Plazomicin 15
mg/kgN=74
Levofloxacin750 mgN=44
Plazomicin15 mg/kg
N= 303
Meropenem1 gm
N=301Total Subjects with SAEs 1 (1.4%) 2 (4.5%) 5 (1.7%) 5 (1.7%)
Acute Kidney Injury 0 0 2 (0.7%) 0
Abortion Spontaneous 1 (1.4%) 0 0 0
Calculus urinary 0 0 1 (0.3%) 0
Metastatic neoplasm 0 0 1 (0.3%) 0
Pneumonia 0 0 1 (0.3%) 0Urosepsis 0 0 1 (0.3%) 0Clostridium difficile colitis 0 0 0 1 (0.3%)
Orchitis 0 0 0 1 (0.3%)Pancreatitis 0 0 0 1 (0.3%)
Pyelonephritis acute 0 1 (2.3%) 0 1 (0.3%)
Pyrexia 0 0 0 1 (0.3%)Seizure 0 1 (2.3%) 0 0Septic shock 0 0 0 1 (0.3%)Urinary tract infection 0 0 0 1 (0.3%)
Source: Adapted from Table 20 of the Sponsor’s Summary of Clinical Safety

13
Treatment Emergent Adverse Events Related to Plazomicin (Phase 3 cUTI Study)
13
PlazomicinN=303n (%)
MeropenemN= 301n (%)
Subjects with TEAEs related IV study drug
18 (5.9%) 16 (5.3%)
Diarrhea 3 (1.0%) 4 (1.3%)Headache 2 (0.7%) 2 (0.7%)Blood Creatinine Increased 2 (0.7%) 0
Vomiting 1 (0.3%) 1 (0.3%Nausea 1 (0.3%) 1 (0.3%)Renal Failure 1 (0.3%) 1 (0.3%)Hypoacusis 1 (0.3%) 0Stomatitis 1 (0.3%) 0Infusion site phlebitis 1 (0.3%) 0Injection site erythema 1 (0.3%) 0Creatinine renal clearance decreased
1 (0.3%) 0
Acute Kidney Injury 1 (0.3%) 0Renal impairment 1 (0.3%) 0Dyspnea 1 (0.3%) 0Rash papular 1 (0.3%) 0Hypertension 1 (0.3%) 0
Note: Not all related TEAEs are shown for meropenem
Source: Adapted from Table 49 of the Sponsor’s Summary of Clinical Safety

14
Treatment Emergent Adverse Events Related to Plazomicin, BSI and HABP/VABP Trial Cohort 1
14
Source: Adapted from Table 24 of the Sponsor’s Summary of Clinical Safety
Subjects with TEAEs related to IV study drug
PlazomicinN= 18n (%)
ColistinN= 21n (%)
Total 5 (27.8%) 9 (42.9%)Acute Kidney Injury 2 (11.1%) 4 (19.0%)Renal Impairment 1 (5.6%) 0
Blood Creatinine Increase 0 3 (14.3%)
Systemic Candida 1 (5.6%) 0Vomiting 1 (5.6%) 1 (4.8%)Anemia 1 (5.6%) 0Paresthesia 0 1 (4.8%)Gait Disturbance 0 1 (4.8%)Hypoaesthesia Oral 0 1 (4.8%)
15
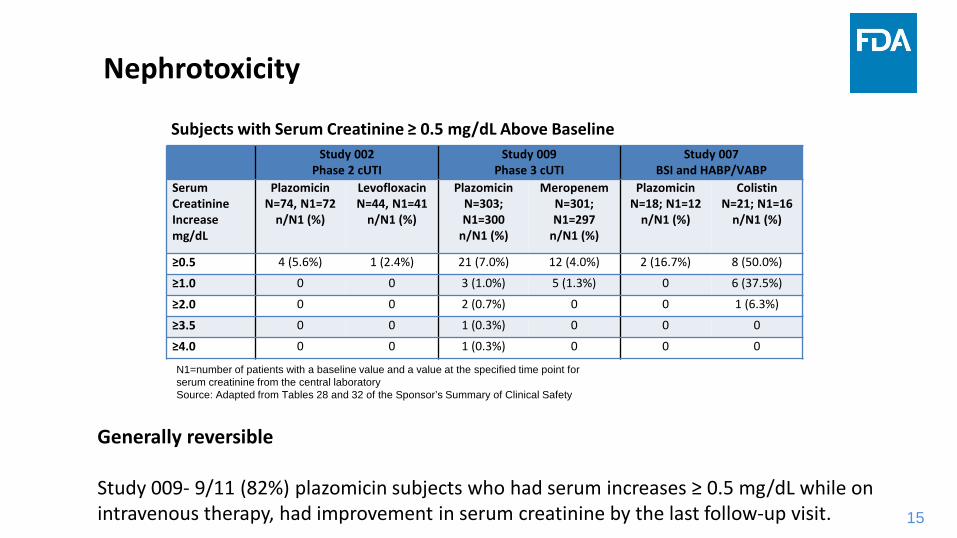
Nephrotoxicity
Subjects with Serum Creatinine ≥ 0.5 mg/dL Above Baseline
Generally reversible
Study 009- 9/11 (82%) plazomicin subjects who had serum increases ≥ 0.5 mg/dL while on intravenous therapy, had improvement in serum creatinine by the last follow-up visit. 15
Study 002Phase 2 cUTI
Study 009Phase 3 cUTI
Study 007BSI and HABP/VABP
Serum Creatinine Increasemg/dL
PlazomicinN=74, N1=72
n/N1 (%)
LevofloxacinN=44, N1=41
n/N1 (%)
PlazomicinN=303; N1=300
n/N1 (%)
MeropenemN=301; N1=297
n/N1 (%)
PlazomicinN=18; N1=12
n/N1 (%)
ColistinN=21; N1=16
n/N1 (%)
≥0.5 4 (5.6%) 1 (2.4%) 21 (7.0%) 12 (4.0%) 2 (16.7%) 8 (50.0%)
≥1.0 0 0 3 (1.0%) 5 (1.3%) 0 6 (37.5%)
≥2.0 0 0 2 (0.7%) 0 0 1 (6.3%)
≥3.5 0 0 1 (0.3%) 0 0 0
≥4.0 0 0 1 (0.3%) 0 0 0
N1=number of patients with a baseline value and a value at the specified time point for serum creatinine from the central laboratorySource: Adapted from Tables 28 and 32 of the Sponsor’s Summary of Clinical Safety
16
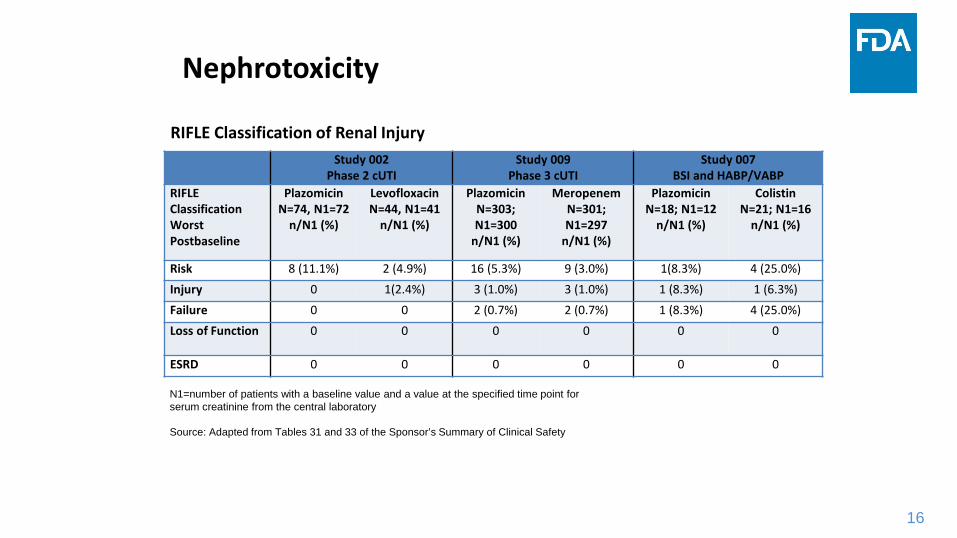
Nephrotoxicity
RIFLE Classification of Renal Injury
16
Study 002Phase 2 cUTI
Study 009Phase 3 cUTI
Study 007BSI and HABP/VABP
RIFLE Classification Worst Postbaseline
PlazomicinN=74, N1=72
n/N1 (%)
LevofloxacinN=44, N1=41
n/N1 (%)
PlazomicinN=303; N1=300
n/N1 (%)
MeropenemN=301; N1=297
n/N1 (%)
PlazomicinN=18; N1=12
n/N1 (%)
ColistinN=21; N1=16
n/N1 (%)
Risk 8 (11.1%) 2 (4.9%) 16 (5.3%) 9 (3.0%) 1(8.3%) 4 (25.0%)Injury 0 1(2.4%) 3 (1.0%) 3 (1.0%) 1 (8.3%) 1 (6.3%)Failure 0 0 2 (0.7%) 2 (0.7%) 1 (8.3%) 4 (25.0%)Loss of Function 0 0 0 0 0 0
ESRD 0 0 0 0 0 0
N1=number of patients with a baseline value and a value at the specified time point for serum creatinine from the central laboratory
Source: Adapted from Tables 31 and 33 of the Sponsor’s Summary of Clinical Safety
17
Ototoxicity
Phase 2 and 3 cUTI Trials:
Three reports of adverse events associated with cochlear or vestibular function- Reports of hypoacusis, tinnitus, and vertigo. These events were somewhat
atypical for aminoglycoside-related ototoxicity in that the hypoacusis and vertigo events resolved and the tinnitus event was unilateral.
Laboratory testing: Pure tone audiometry was performed in the phase 1 and phase 2 studies
- Four out of 182 plazomicin-exposed subjects had findings of possible drug-related ototoxicity.
17
Phase 1 Studies:- Five reports of transient tinnitus following a single dose of plazomicin
- One of the five subjects also reported transient nystagmus - One subject had an abnormal vestibular function test

18
SummarySafety Findings
The data from the plazomicin clinical trials presents a safety profile that is generally consistent with an aminoglycoside class drug.
The main safety signal observed was nephrotoxicity typical of an aminoglycoside and generally associated with reversibility.
No clear comparison of plazomicin’s nephrotoxic potential relative to colistin’snephrotoxic potential can be made due to the small sample size of the CRE study 007; however, there was a trend suggesting less nephrotoxicity for plazomicin.
Overt ototoxicity due to plazomicin was not identified given the limited duration of treatment. There is no definitive evidence that plazomicin does not have the potential for aminoglycoside-associated ototoxicity.
18

1
Therapeutic Drug Monitoring (TDM) for Plazomicin in cUTI Patients
Luning (Ada) Zhuang, Ph.D.Office of Clinical Pharmacology
FDA
www.fda.gov
Antimicrobial Drugs Advisory Committee Meeting May 2, 2018

2
Plazomicin Pharmacokinetics (PK) Highlights
www.fda.gov
• Distribution– Mainly distributed in extracellular space– Plasma protein binding is approximately 20%
• Metabolism– Minimal metabolism
• Elimination– Predominantly eliminated by the kidneys, CL≈CLrenal≈GFR*fu– Half-life is ~3.5 hours
3
TDM in cUTI Patients• TDM using Cmin ≥2 μg/mL during first 48 hours is proposed by Applicant
• Cmin-based TDM was NOT used in cUTI patients in either Phase 2 or 3 studies (Study 002 and 009)
• Dose was adjusted daily based on creatinine clearance (CLcr) in the Phase 3 study.
– Nephrotoxicity, defined as ΔScr≥0.5 mg/dL from baseline, occurred in 22 cUTI patients (22 out of 367)
– Nephrotoxicity occurred after 10 days (≥ 3 days after stopping the therapy) in 9 cUTIpatients (9 out of 22)

4
Evaluation of Risks for NephrotoxicityMost nephrotoxicity occurred in cUTI patients with renal impairment (CLcr >30 to 90 mL/min) from Phase 2 and 3 studies
Arm% Nephrotoxicity (n/N)
CLcr >30 to 90 mL/min CLcr >90 mL/min
Plazomicin 8.6% (21/244) 0.8% (1/123)
Active Control* 4.1% (10/243) 3.1% (3/97)
*Meropenem or levofloxacin
• Only one patient with CLcr >90 mL/min had nephrotoxicity, exposure-response (E-R) analysis cannot be conducted (N=123). Lower nephrotoxicity compared to active control
• A significant E-R relationship between estimated C1st,min and nephrotoxicity was identified in patients with CLcr >30 to 90 mL/min (N=244) C1st, min was used as PK measure as Cmin did not change
substantially during treatment Cmin values were estimated by population PK model
C1st, min (µg/mL)In
cide
nce
of N
ephr
otox
icity

5
C1st,min Thresholds for Nephrotoxicity• C1st, min of 3 µg/mL is predicted to be the critical threshold associated with high
nephrotoxicity incidence for cUTI patients with CLcr >30 to 90 mL/min– Classification and Regression Tree (CART) analysis
• Nephrotoxicity incidence is ~10% for patients with C1st, min ranging from 2 to 3 μg/mL and higher than 30% for patients with C1st, min ≥3 μg/mL
C1st,min range (µg/mL) % Nephrotoxicity (n/N)
≥ 4 40.0% (6/15)
≥ 3 – 4 30.8% (4/13)
≥ 2 – 3 9.8% (4/41)
≥ 1 – 2 5.0% (4/80)
<1 3.2% (3/95)
Total 8.6% (21/244)
C1st,min <2.995
0.051N=216
0.086N=244
0.357N=28
CLcr >30 to 90 mL/min
6
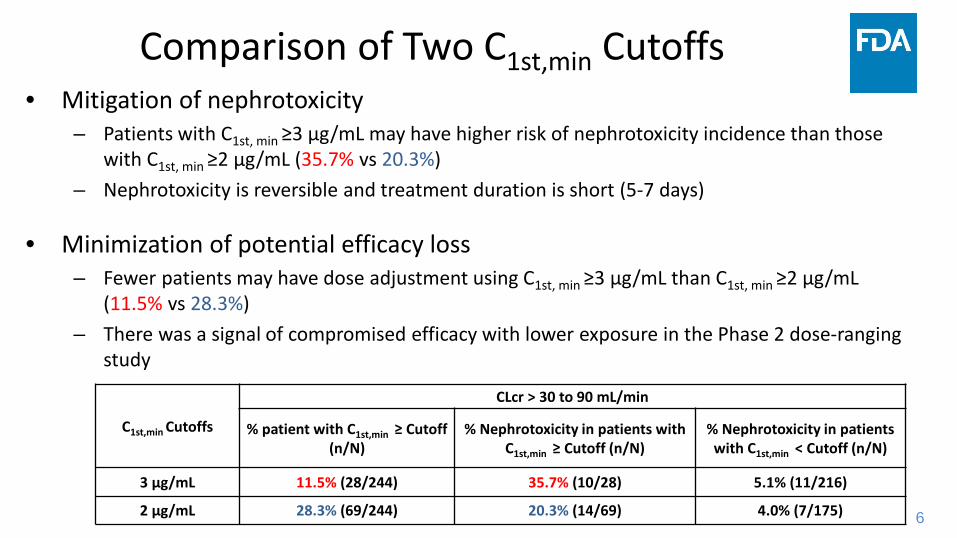
Comparison of Two C1st,min Cutoffs• Mitigation of nephrotoxicity
– Patients with C1st, min ≥3 µg/mL may have higher risk of nephrotoxicity incidence than those with C1st, min ≥2 µg/mL (35.7% vs 20.3%)
– Nephrotoxicity is reversible and treatment duration is short (5-7 days)
• Minimization of potential efficacy loss– Fewer patients may have dose adjustment using C1st, min ≥3 µg/mL than C1st, min ≥2 µg/mL
(11.5% vs 28.3%)– There was a signal of compromised efficacy with lower exposure in the Phase 2 dose-ranging
study
C1st,min Cutoffs
CLcr > 30 to 90 mL/min
% patient with C1st,min ≥ Cutoff(n/N)
% Nephrotoxicity in patients with C1st,min ≥ Cutoff (n/N)
% Nephrotoxicity in patients with C1st,min < Cutoff (n/N)
3 μg/mL 11.5% (28/244) 35.7% (10/28) 5.1% (11/216)
2 μg/mL 28.3% (69/244) 20.3% (14/69) 4.0% (7/175)

7
Comparison of Two C1st,min Cutoffs• C1st,min ≥3 μg/mL provides a high specificity while C1st,min ≥2 μg/mL provides a
good sensitivity in cUTI patients with CLcr >30 to 90 mL/min– Specificity: the percentage of patients without nephrotoxicity who can be correctly classified
as no dose adjustment is needed. – Sensitivity: the percentage of patients with nephrotoxicity who can be correctly classified as
dose adjustment is needed
– C1st, min ≥3 µg/mL is an option if efficacy loss is a major concern for TDM while C1st, min ≥2 µg/mL is an option if safety is a major concern for TDM
C1st,min Cutoffs Sensitivity Specificity
3 μg/mL 48% 92%
2 μg/mL 67% 75%
8
Dose Adjustment in cUTI Patients
• More than one dose adjustment may not be clinically feasible for the cUTI patients with a short treatment duration (5-7 days)
– Concentration values will be available at 24 to 36 hours after blood samples are collected.
• One dose adjustment by increasing dosing interval to 1.5 fold (36 hours) for cUTI patients with CLcr >30 to 90 mL/min
– 92% patients may have Cmin<2 μg/mL or 97% patients may have Cmin<3 μg/mL after one dose adjustment based on simulation
9
Dosing Strategy in Patients with CLcr >15 to 30 mL/min
• Uncertainty and unmet medical need– Safety and efficacy data are limited (N=1 cUTI patient)– Expected higher risk of nephrotoxicity compared to that in mild or moderate renal
impairment patients (CLcr > 30 to 90 mL/min) – Limited treatment options for this patient population
– Approaches– Leveraging the finding and knowledge from patients with CLcr >30 mL/min– Proposed dosing regimen is every 48 hours; TDM should be evaluated
10
Summary• TDM may not be needed to mitigate the nephrotoxicity in cUTI patients with
CLcr >90 mL/min– Lower nephrotoxicity incidence compared to the active control
• Cmin-based TDM can potentially mitigate the nephrotoxicity in cUTI patients with CLcr >30 to 90 mL/min
– C1st, min ≥3 μg/mL if efficacy loss is a concern for TDM– C1st, min ≥2 μg/mL if safety is a major concern for TDM
• TDM should be further evaluated in cUTI patients with CLcr >15 to 30 mL/min– Limited efficacy and safety information


Kunyi Wu, PharmDOffice of Clinical Pharmacology
OTS, CDER, FDA
Therapeutic Drug Monitoring (TDM) for Plazomicin in Patients with Bloodstream Infection (BSI)
Antimicrobial Drugs Advisory Committee MeetingMay 2, 2018
2
AUC0-24 – Based TDM in BSI patients
• The target AUC0-24 range in Study 007 was 210 – 315 μg*h/mL.
• The TDM range was pre-determined based on ±20% of the mean AUC 0-24 (i.e., 262 μg*h/mL) in Phase 2 cUTI patients with normal renal function receiving 15 mg/kg/day plazomicin.
• In Study 007– Doses were adjusted on Day 3, Day 6 (± 1 day), and Day 10 (± 1 day) based on
the estimated AUC0-24 on Day 1, Day 4 (± 1 day) and Day 8 (± 1 day), respectively, in order to maintain the AUC 0-24 in the target range.
– Doses were also adjusted based on renal function and physician’s clinical judgement in the course of the treatment.
www.fda.gov
3
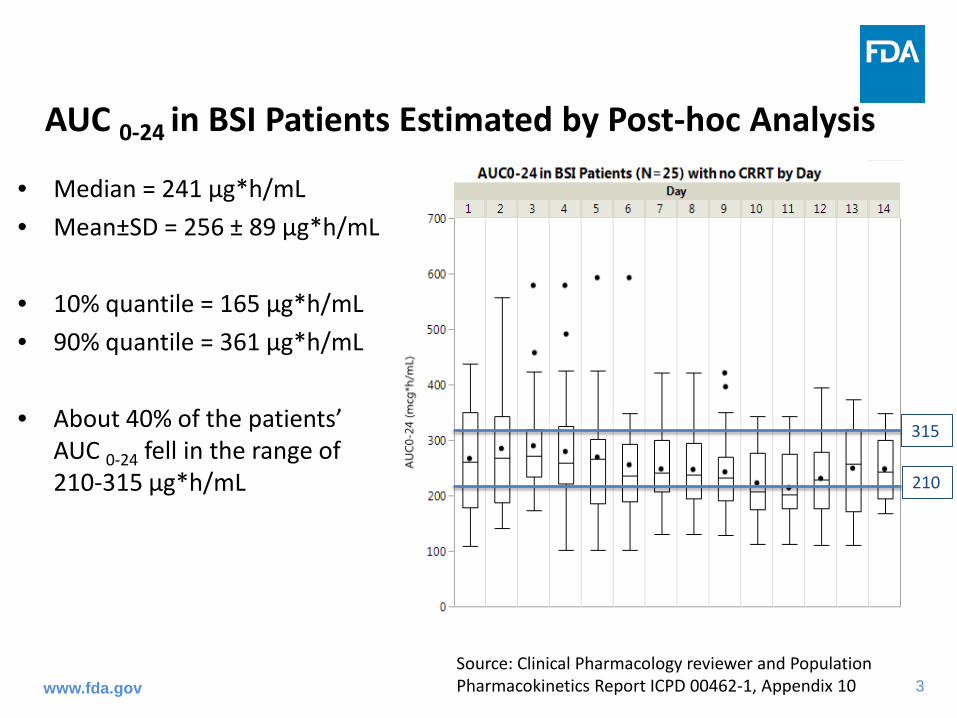
AUC 0-24 in BSI Patients Estimated by Post-hoc Analysis
• Median = 241 µg*h/mL• Mean±SD = 256 ± 89 µg*h/mL
• 10% quantile = 165 µg*h/mL • 90% quantile = 361 µg*h/mL
• About 40% of the patients’ AUC 0-24 fell in the range of 210-315 μg*h/mL
315
210
Source: Clinical Pharmacology reviewer and Population Pharmacokinetics Report ICPD 00462-1, Appendix 10www.fda.gov

4
Individual Patient’s AUC 0-24 Fluctuated Over the Course of the Treatment
• Most patients received more than one dose adjustment during the treatment.
• Large AUC 0-24 variability was observed despite TDM and renal function based dose adjustment.
315
210
Source: Clinical Pharmacology reviewer and Population Pharmacokinetics Report ICPD 00462-1, Appendix 10

5
Difficulties in Evaluation of the TDM Range in BSI Patients
• No exposure-response (E-R) analyses can be performed for either efficacy or safety. – Limited number of patients were in Study 007.
• Evaluation of the clinical utility of TDM is not possible. – No BSI patients received plazomicin treatment without TDM.– Due to the AUC fluctuation, most patients’ AUC only fell in the target
TDM range periodically.
www.fda.gov

6
Evaluation of the Lower Bound of the TDM Range in BSI Patients Based on PK/PD Targets from a Neutropenic Murine Thigh Model
• Plazomicin antibacterial activity is related to AUC 0-24/ MIC. • PK/PD Target was determined based on 17 Enterobacteriaceae strains using a
neutropenic murine thigh model.
PK/PD Target (AUC0-24/MIC)
AUC0-24 (μg·h/mL) required to attain the PK/PD target valuesMIC = 4 μg/mL
Median for bacterial stasis
= 24 9675th percentile
for bacterial stasis = 39 156
www.fda.gov

7
Evaluation of the Upper Bound of the TDM Range Based on the Observed Nephrotoxicity in Study 007
• Nephrotoxicity is defined as serum creatinine increase of 0.5 mg/dL or greater from baseline.
• In cUTI patients, increase in incidence of nephrotoxicity was related to increased exposure.
• Higher AUC is expected to result in higher incidence of nephrotoxicity. Upper bound AUC may be helpful to limit the incidence of nephrotoxicity.
• In Study 007– About 30% patients in plazomicin arm (Cohort 1 & 2) experienced
nephrotoxicity – About 50% patients in colistin arm experienced nephrotoxicity
www.fda.gov
8
Summary• AUC0-24 – based TDM range in BSI patients:
– The proposed lower bound (i.e., 210 μg*h/mL) is sufficient to attain the PK/PD target for bacterial stasis against Enterobacteriaceae for MIC up to 4 μg/mL .
– The proposed upper bound (i.e., 315 μg*h/mL) is questionable due to 30% incidence of nephrotoxicity.
• Consideration should be given to the tolerability of this risk of nephrotoxicity in patients who have limited or no alternative treatment options.
– The clinical utility of TDM in BSI patients has not been demonstrated.
www.fda.gov

9
Thank You!
www.fda.gov
1
Back up Slides Shown
5
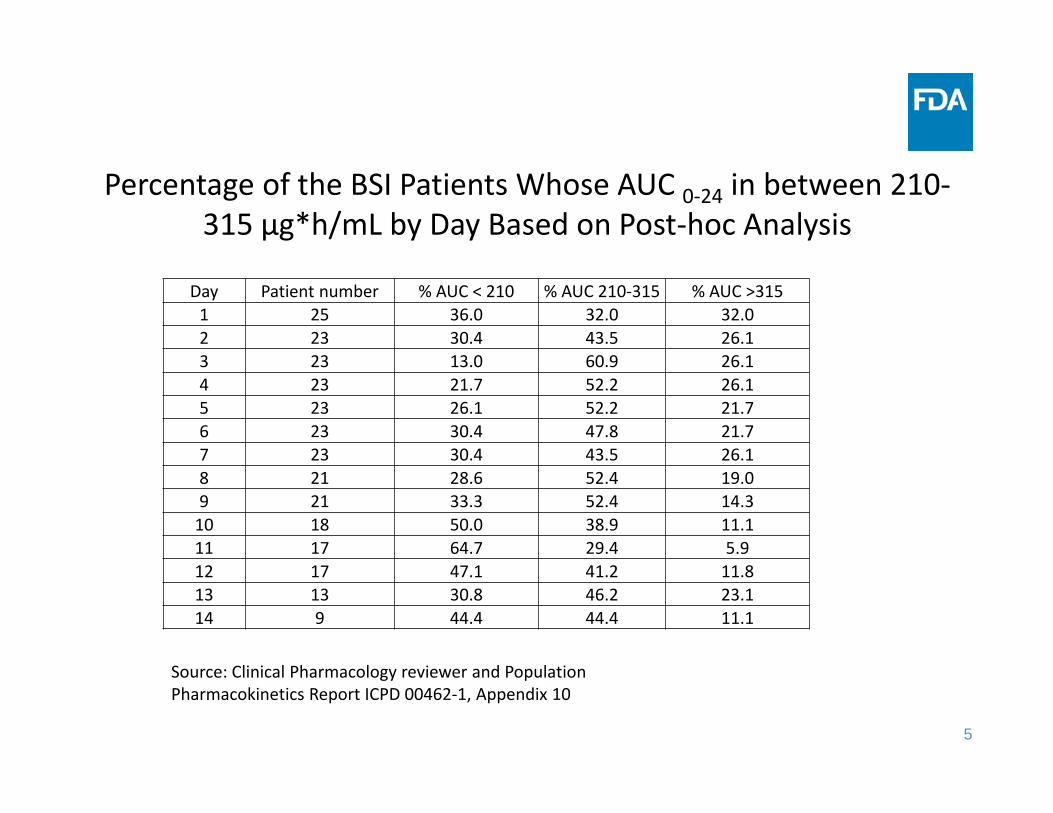
Percentage of the BSI Patients Whose AUC 0‐24 in between 210‐315 μg*h/mL by Day Based on Post‐hoc Analysis
Source: Clinical Pharmacology reviewer and Population Pharmacokinetics Report ICPD 00462‐1, Appendix 10
Day Patient number % AUC < 210 % AUC 210‐315 % AUC >3151 25 36.0 32.0 32.02 23 30.4 43.5 26.13 23 13.0 60.9 26.14 23 21.7 52.2 26.15 23 26.1 52.2 21.76 23 30.4 47.8 21.77 23 30.4 43.5 26.18 21 28.6 52.4 19.09 21 33.3 52.4 14.310 18 50.0 38.9 11.111 17 64.7 29.4 5.912 17 47.1 41.2 11.813 13 30.8 46.2 23.114 9 44.4 44.4 11.1
6
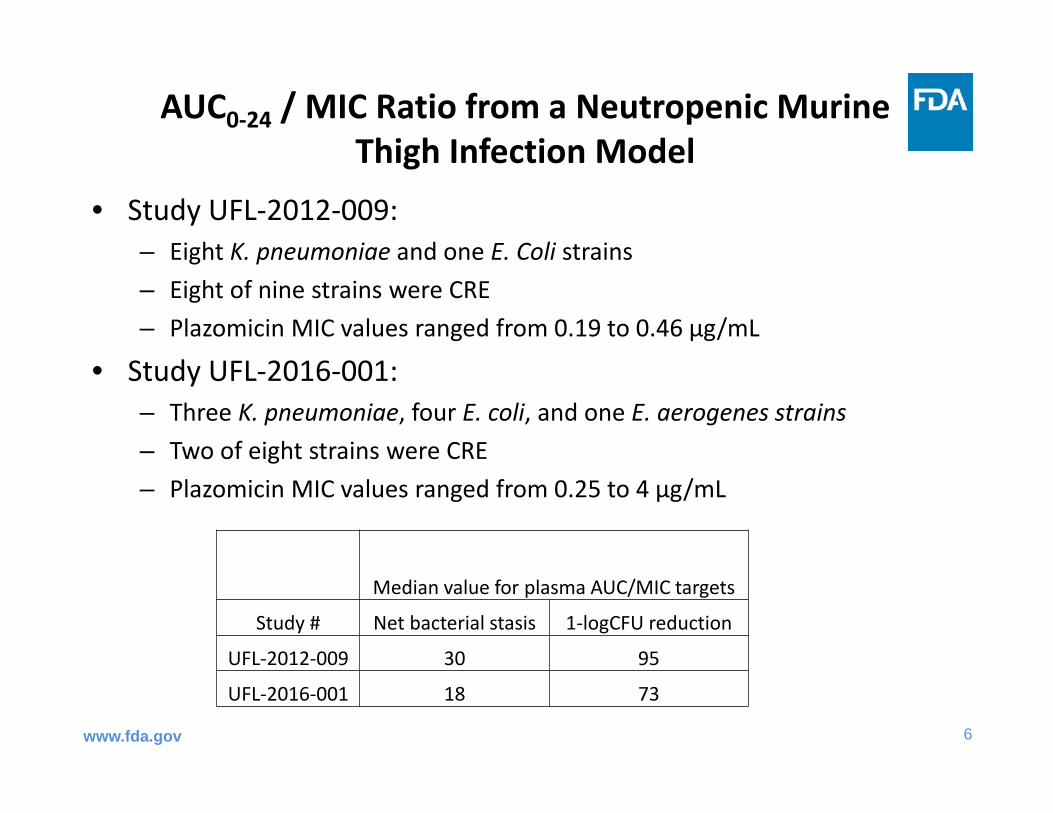
AUC0‐24 / MIC Ratio from a Neutropenic Murine Thigh Infection Model
• Study UFL‐2012‐009: – Eight K. pneumoniae and one E. Coli strains– Eight of nine strains were CRE– Plazomicin MIC values ranged from 0.19 to 0.46 μg/mL
• Study UFL‐2016‐001: – Three K. pneumoniae, four E. coli, and one E. aerogenes strains– Two of eight strains were CRE – Plazomicin MIC values ranged from 0.25 to 4 μg/mL
www.fda.gov
Median value for plasma AUC/MIC targets
Study # Net bacterial stasis 1‐logCFU reduction
UFL‐2012‐009 30 95
UFL‐2016‐001 18 73
7
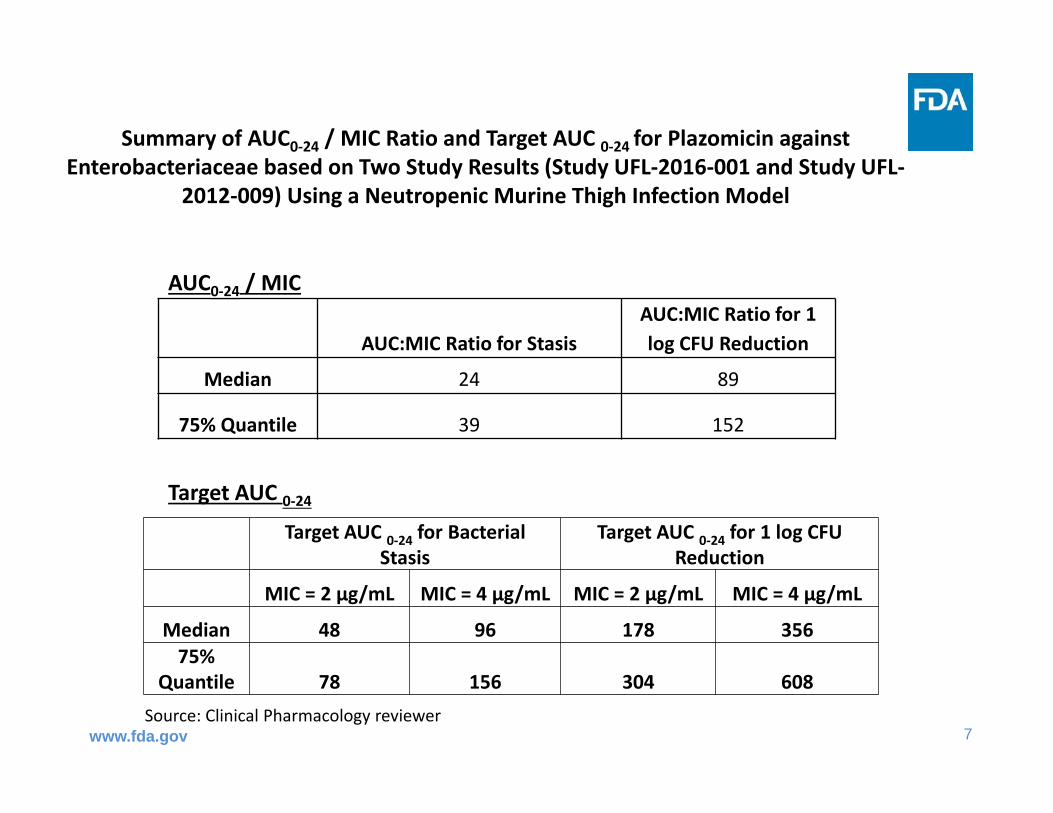
Summary of AUC0‐24 / MIC Ratio and Target AUC 0‐24 for Plazomicin against Enterobacteriaceae based on Two Study Results (Study UFL‐2016‐001 and Study UFL‐
2012‐009) Using a Neutropenic Murine Thigh Infection Model
www.fda.gov
AUC:MIC Ratio for StasisAUC:MIC Ratio for 1 log CFU Reduction
Median 24 89
75% Quantile 39 152
AUC0‐24 / MIC
Target AUC 0‐24Target AUC 0‐24 for Bacterial
Stasis Target AUC 0‐24 for 1 log CFU
Reduction
MIC = 2 μg/mL MIC = 4 μg/mL MIC = 2 μg/mL MIC = 4 μg/mL
Median 48 96 178 35675%
Quantile 78 156 304 608Source: Clinical Pharmacology reviewer