february 16, 2017 - idaho medicaid pharmacy program | … pain reliever for most state medicaid...
TRANSCRIPT
February 16, 2017
1

Ongoing Reviews
Narcotic Prescribing Improvement Project
Top 150 Utilizers
Top 150 Narcotic Utilizers 2013-2016 and Treatment of Opioid Induced Constipation
Methadone
Buprenorphine and benzodiazepine concomitant use
Opioid and benzodiazepine concomitant use
Hepatitis C Update
Foster kids
Second-Generation Antipsychotic Use in children < 6 years old2

February 16, 2017
3

Medicaid DUR
February 16, 2017
4

Opioid Induced Constipation
Frequent use of opioids can lead to constipation
Increased amount of time for stool to travel through the gastric system
Decrease longitudinal propulsive peristalsis in the intestines
Opioids can cause gastroparesis
Opioids reduce digestive secretions and decrease the urge to defecate
Additional factors
Inadequate fiber/fluid intake
Lack of physical activity
Diabetes, spinal cord compression, excessive calcium, or kidney problems 5

Opioid Induced Constipation
Idaho Medicaid was asked about the frequency of emergency room visits for abdominal pain due to opioid induced constipation.
Difficult to gather medical billing information and data to determine if emergency room visits for abdominal pain are related to opioid induced constipation.
Pharmacy data can determine prescribing patterns for medications to treat or prevent opioid induced constipation.
Obtained the top 150 narcotic utilizers and determined the number of patients and claims for the treatment/prevention of opioid induced constipation.
6

Opioid Induced Constipation
Review of top 150 narcotic utilizers
Total number of patients prescribed an agent for constipation
21 patients
Male= 7 Female=14
6 patients were prescribed more than 1 agent.
7

Opioid Induced Constipation
8

Opioid Induced Constipation
Conclusions
Majority of patients from the top 150 narcotic utilizers are not treated for opioid induced constipation.
21 patients (14%) have active prescription history for agents to treat constipation.
Multiple factors can be involved in constipation including diet, exercise, and comorbid illnesses.
Limitations to data collection for Medical admissions to the emergency room and diagnosis to determine opioid induced constipation prevalence in Medicaid population.
9

Ongoing Review
February 16, 2017
10

MethadoneGrowing Public Health Concern
More than 16,500 people in the United States die each year from opioid-related prescription drug overdoses.
Methadone is responsible for nearly 1/3 of these deaths but accounts for only 2% of opioid pain reliever prescription.
Centers for Disease Control and Prevention. “Opioids Drive Continued Increase in Drug Overdose Deaths” (2013). http://www.cdc.gov/media/relases/2013/p0220_drug_overdose_deaths.html.
11

MethadonePreferred pain reliever for most state Medicaid programs.
Idaho Medicaid removed Methadone preferred status October 2015.
Prior authorization required.
Informed methadone providers of implementation of methadone prior authorization and requested tapering off of methadone.
12

MethadoneMethadone Prior Authorization Request Forms
Methadone, Initial Request
States initial criteria for review:
Failure of all alternative long acting narcotic agents.
Electrocardiogram (QTc interval documentation).
Pain score and functionality documentation.
Other active concurrent opioids (immediate release).
Documentation of failure/intolerance to non-opioid or opioid agents.
13

Methadone Methadone, Reauthorization
Emphasizes monitoring and recommends dose tapering: Electrocardiogram (QTc interval annual review).
Doses greater than 40 mg/day will require documentation of medical necessity and clinical reason why dose reduction cannot be employed.
History of failure/intolerance to non-opioid or other opioid agents.
Only prescribers who are familiar with methadone’s titration and risks, or those who are able to consult with a pain specialist or clinical pharmacist, should prescribe or make changes to methadone treatment.
Work in progress.
14
MethadoneReview of Methadone drug utilization after changing to non-preferred agent.
Calendar Quarters Reviewed:
4th Quarter 2015 (Oct-Dec)
2nd Quarter of 2016 (Apr-Jun)
3rd Quarter of 2016 (Jul-Sept)
4th Quarter of 2016 (Oct-Dec)
15

Methadone
16

Methadone
17

Methadone
18

MethadonePatients taking more than 40 mg/day
Average #tablets/day=7
Range: 5-17 tablets/day (50 mg-160 mg/day)
Morphine Equivalents Daily (MED)*
30 mg-240
40 mg=320
50 mg=500
60 mg=600
70 mg=840
130 mg=1560*Opioid Dose Calculator: http://www.agencymeddirectors.wa.gov/opioiddosing.asp
(Washington State Agency Medical Directors' Group)19

MethadoneIn conclusion:
Methadone utilization has decreased since incorporation of non-preferred status and prior authorization requirements.
Total providers, total patients, and total claims have decreased.
No change noted with percentage of patients on greater than 40 mg/day of methadone.
20

Methadone Questions/Comments??
21

February 16, 2017
22

Buprenorphine and benzodiazepine concomitant use
23
Suboxone Package Insert
Buprenorphine in combination with benzodiazepines or other CNS depressants including alcohol has been associated with significant respiratory depression and death.
Patients should be warned of the potential of self-administration of benzodiazepines or other depressants while under treatment with Suboxone.

Buprenorphine and benzodiazepine concomitant use
24
Payment block went in to effect 1/6/16 requiring prior authorization for payment for either buprenorphine or benzodiazepine with overlapping days of service.

Buprenorphine and benzodiazepine concomitant use
25
PMP Interconnect Search
Nineteen States now on the list (must select each individual state to search) –including Idaho
Alaska Massachusetts North Dakota
Arizona Michigan Ohio
Colorado Minnesota Rhode Island
Illinois Mississippi South Carolina
Indiana Nevada Texas
Kansas New Mexico Utah

Buprenorphine and benzodiazepine concomitant use
26
New Federal Regulations Increase Limit Rule to 275 Buprenorphine Patients
Effective Date: 8/08/2016

Buprenorphine and benzodiazepine concomitant use
27
Physicians who have prescribed buprenorphine to 100 patients for at least one year can now apply to increase their patient limits to 275 under new federal regulations.
To be considered for the higher limit, complete the Online Request for Patient Limit Increase. SAMHSA reviews applications within 45 days of receipt.
Document Citation: 81 FR 44711

Buprenorphine and benzodiazepine concomitant use
28
FOR IMMEDIATE RELEASENovember 16, 2016
Contact: HHS Press [email protected]
HHS takes additional steps to expand access to opioid treatment The U.S. Department of Health and Human Services (HHS) is taking additional steps to
address the U.S. opioid epidemic by further expanding access to medication-assisted treatment (MAT) for opioid use disorders.
Administered by the Substance Abuse and Mental Health Services Administration (SAMHSA), today’s announcement enables nurse practitioners (NPs) and physician assistants (PAs) to immediately begin taking the 24 hours of required training to prescribe the opioid use disorder treatment, buprenorphine.

Buprenorphine and benzodiazepine concomitant use
29
NPs and PAs who complete the required training and seek to prescribe buprenorphine for up to 30 patients will be able to apply to do so beginning in early 2017. Previously, only physicians could prescribe buprenorphine. Once NPs and PAs receive their waiver they can begin prescribing buprenorphine immediately.
HHS also is announcing its intent to initiate rulemaking to allow NPs and PAs who have prescribed at the 30 patient limit for one year, to apply for a waiver to prescribe buprenorphine for up to 100 patients.

Buprenorphine and benzodiazepine concomitant use
30
NPs and PAs prescribing buprenorphine for treatment of opioid abuse in Idaho
What still needs to happen:
The new language has to be added to the federal controlled substances act (DEA).
There is no time estimate yet on when this will happen.
Personal communication – Idaho Board of Pharmacy – January 19, 2017

Buprenorphine and benzodiazepine concomitant use
31
200 201 210 223 222 211 212 223241 251 265 265 267
301
342
26 27 23 2036 31 20 31 35 40 46 32 28 21
40
0
50
100
150
200
250
300
350
400
2/1/13 -4/30/13
6/1/13 -8/31/13
9/1/13 -11/30/13
12/1/13 -2/28/14
3/1/14 -5/31/14
6/1/14 -8/31/14
9/1/14 -11/30/14
12/1/14 -2/28/15
3/1/15 -5/31/15
4/1/15 -8/31/15
9/1/15 -11/30/2015
12/1/15 -2/29/16
3/1/16 -5/31/16
6/1/16 -8/31/16
9/1/16 -11/30/16
Total # of participants on oral buprenorphine
Participants who paid cash for an opioid while on oral buprenorphine

Buprenorphine and benzodiazepine concomitant use
32
251 265265 267
301342
57 65 5955 55 60
40 46 32 28 2140
20 19 10 7 120
100
200
300
400
6/1/15 - 8/31/15 9/1/15 - 11/30/15 12/1/15 - 2/29/16 3/1/16 - 5/31/16 6/1/16 - 8/31/16 9/1/16 - 11/30/16
buprenorphine patients
concomitant benzo while on buprenorphine
cash paying opioids while on buprenorphine
cash paying opioids AND concomitant benzo while on buprenorphine
Buprenorphine and benzodiazepine concomitant use
33
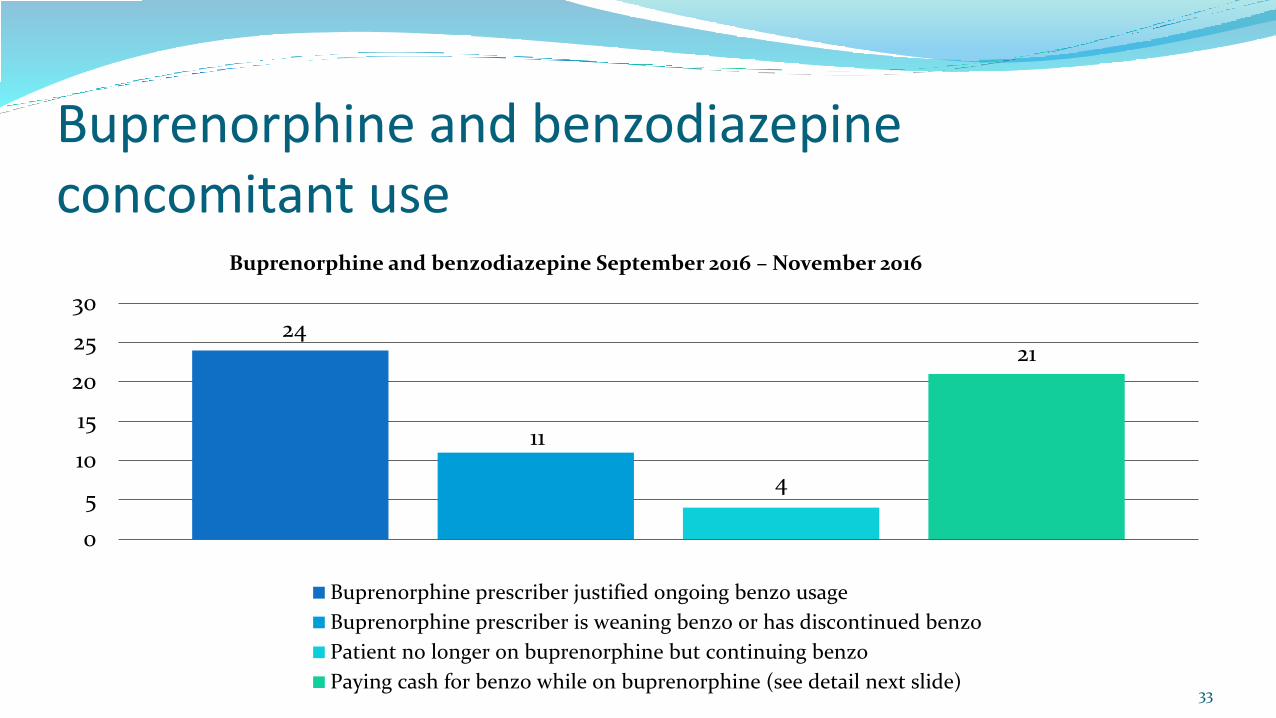
24
11
4
21
0
5
10
15
20
25
30
Buprenorphine and benzodiazepine September 2016 – November 2016
Buprenorphine prescriber justified ongoing benzo usage
Buprenorphine prescriber is weaning benzo or has discontinued benzo
Patient no longer on buprenorphine but continuing benzo
Paying cash for benzo while on buprenorphine (see detail next slide)

Buprenorphine and benzodiazepine concomitant use
34
15
1
5
0
2
4
6
8
10
12
14
16
Detail on patients paying cash for benzo while on buprenorphine but no PA submitted
MD aware/ok with it
Patient told to discontinue benzo
Procedural (1 - 4 tablets), 1x fill

Buprenorphine and benzodiazepine concomitant use
35
Questions/Comments ??

Chris Johnson PharmD
Mark England PharmD
36

Opioid and benzodiazepine concomitant use
37
FDA is requiring boxed warnings for all opioid analgesics and benzodiazepines with information about the serious risks associated with concomitant use of opioids and benzodiazepines.
Part of the FDA Opioid Action Plan to combat the growing epidemic of opioid abuse, dependence and overdose in the United States.

Opioid and benzodiazepine concomitant use
38
Diazepam Package Insert:
Concomitant use of benzodiazepines and opioids may result in profound sedation, respiratory depression, coma, or death. Reserve use for patients for whom alternative therapies are inadequate and limit use to lowest possible dose and shortest possible duration. Monitor for signs or symptoms of respiratory depression and sedation
Oxycodone Package Insert:
Concomitant use of benzodiazepines and opioids may result in profound sedation, respiratory depression, coma, and death. Reserve concomitant prescribing for patients with inadequate alternative treatment options. Limit dosages and durations to the minimum required and follow patients for signs and symptoms of respiratory depression and sedation

Opioid and benzodiazepine concomitant use
39
Included in packet is the FDA Drug Safety Communication and FDB response.
ProDUR report ran for 1/2017 for DR/DR between LA/SA Opioids and Benzos and LA/SA Opioids and Sleep Drugs;Tranquilizers
5,236 claims
1,925 unique recipients

Opioid and benzodiazepine concomitant use
40
Utilizing Magellan Rx First IQ Data and pulling for dates of 11/1/2016 –1/31/2017:

Opioid and benzodiazepine concomitant use
41
Discussion on Concomitant Benzodiazepines and Opiates
How to proceed ?

February 16, 2017
4th Quarter 2016
(Calendar Year)
42

Hepatitis-C DUR
43

Hepatitis-C DUR
44

Hepatitis-C DUR
45

Hepatitis-C DUR
46

Hepatitis-C DUR
47
Hepatitis-C DUR
48

Hepatitis-C DUR
49

Hepatitis-C DUR
50

Hepatitis-C DUR
51

Hepatitis-C DUR
52

Hepatitis-C DUR
53

Hepatitis-C DUR
54

Hepatitis-C DUR
Total: $1,510,841 55

Hepatitis-C DUR Questions/Comments??
56

February 16, 2017
57

February 16, 2017
58

Current Interventions/Outcomes Studies
Codeine and Tramadol Use in Children
Low dose quetiapine
Ophthalmic Antibiotic/Steroid Combinations
59

February 16, 2017
60

Codeine Use in Children
AAP Report Says Codeine Too Risky for Kids, Urges Restrictions on Use 9/19/16
The American Academy of Pediatrics is urging parents and health providers to stop giving codeine to children, calling for more education about its risks and restrictions on its use in patients under age 18. A new AAP clinical report in the October 2016 issue of Pediatrics, Codeine: Time to Say `No’, cites continued use of the drug in pediatric settings despite growing evidence linking the common painkiller to life-threatening or fatal breathing reactions.
61
Codeine Use in Children
AAP Report Says Codeine Too Risky for Kids, Urges Restrictions on Use 9/19/16
According to the AAP report, it still is commonly prescribed to children after surgical procedures such as tonsil and adenoid removal. More than 800,000 patients under age 11 were prescribed codeine between 2007 and 2011, according to one study cited in the AAP report. Otolaryngologists were the most frequent prescribers of codeine/acetaminophen liquid formulations (19.6 percent), followed by dentists (13.3 percent), pediatricians (12.7 percent) and general practice/family physicians (10.1 percent).
62

Codeine Use in Children
Excerpts from Codeine: Time to Say No
Codeine is a prodrug that has limited affinity for the µ-opioid receptor and no analgesic effects. After an oral dose, the majority of codeine undergoes hepatic glucuronidation or N-demethylation to inactive metabolites. The analgesic properties result from hepatic metabolism and conversion of the parent compound (codeine) to morphine and the active metabolite morphine-6-glucuronide. The conversion from codeine to morphine is regulated by the cytochrome P450 2D6 (CYP2D6) enzyme system.
63

Codeine Use in Children
Excerpts from Codeine: Time to Say No
The activity of CYP2D6 varies significantly as a function of genetic polymorphisms. Poor metabolizers initially received the greatest attention because of codeine’s lack of efficacy in such patients. As our understanding of the influence of genetic variations on pharmacokinetics has improved, attention has become more focused on individuals who are ultrarapid metabolizers secondary to gene duplications. This latter group has ≥2 copies of the CYP2D6 gene, which can result in an enzyme activity score ≥3, indicating a very high level of enzyme activity. The result in these patients is the production of large amounts of morphine that can cause respiratory depression or apnea, even after normal therapeutic doses of oral codeine.
64
Codeine Use in Children
Excerpts from Codeine: Time to Say NoIn the last 5 years, various organizations and regulatory bodies have promulgated warnings regarding adverse responses associated with codeine, as follows:
1. March 2011: The World Health Organization deleted codeine from its list of essential medications for children because of concerns that its “efficacy and safety were questionable in an unpredictable portion of the pediatric population.”
2. August 2012: The US Food and Drug Administration (FDA) issued a safety alert regarding the use of codeine in children after tonsillectomy, adenoidectomy, or adenotonsillectomy.
3. February 2013: An update from the FDA added a “black box warning” to the drug label of codeine and codeine-containing preparations. The warning advises health care professionals “to prescribe an alternative analgesic [to codeine] for postoperative pain control in children undergoing tonsillectomy and/or adenoidectomy.” A contraindication was added to restrict codeine use in such patients. The “Warnings/Precautions,” “Pediatric Use,” and “Patient Counseling Information” sections of the label were also updated.
65

Codeine Use in Children
Excerpts from Codeine: Time to Say No
4. June 2013: The European Medicines Agency issued a report recommending the restriction of codeine for the treatment of pain to children older than 12 years as well as a contraindication to its use in children younger than 18 years undergoing tonsillectomy and/or adenoidectomy. In addition, it recommended against codeine use in breastfeeding women.
5. June 2013: Health Canada announced that it had reviewed the safety of prescription pain and cough medications containing codeine and recommended against their use in children younger than 12 years.
6. March 2015: The European Medicines Agency completed a review of the use of codeine for cough and cold and recommended against its use in children younger than 12 years as well as children and adolescents between 12 and 18 years who have problems with breathing.
66

Codeine Use in Children
Paid oral codeine claims for Idaho Medicaid participants – Age < 18 years
August 1 – October 31, 2016
287 claims
274 unique patients (13 patients with two paid claims)
$3723 in paid claims to pharmacies
Safety issue – not a cost issue !!
67

Codeine Use in Children
68
0-6 years, 2, 1%
7-11 years, 65, 24%
12-15 years, 129, 47%
16-17 years, 78, 28%
Paid claims for Idaho Medicaid participants – Age < 18 years August 1 - October 31, 2016

Codeine Use in Children
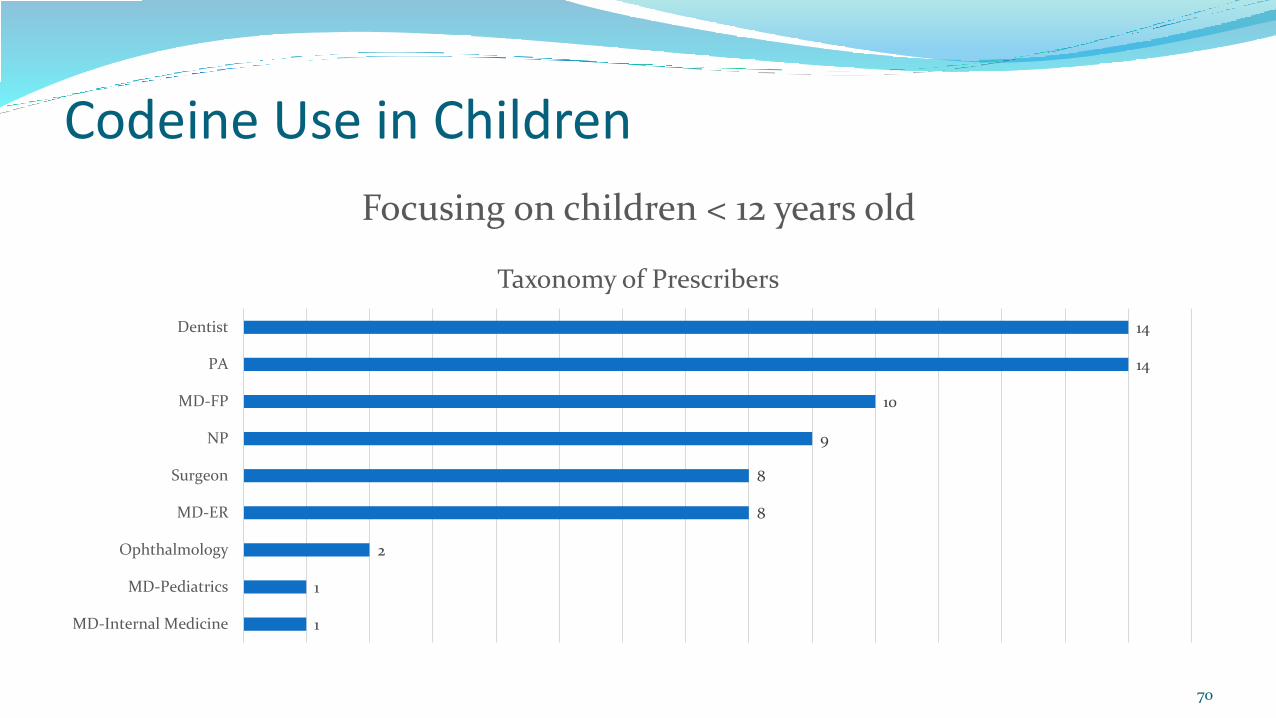
Focusing on children < 12 years old:
68 paid claims for 67 unique patients
58 prescribers (one prescriber with 3 paid claims and 9 prescribers with 2 paid claims)
69
Codeine Use in Children
14
14
10
9
8
8
2
1
1
Dentist
PA
MD-FP
NP
Surgeon
MD-ER
Ophthalmology
MD-Pediatrics
MD-Internal Medicine
Focusing on children < 12 years old
Taxonomy of Prescribers
70

Codeine Use in Children
71
Discussion on how to proceed
Currently codeine/acetaminophen products are a preferred agent and pay at the pharmacy with prior authorization not needed.
Possible option: Institute age limits that would require an age override prior authorization with medical necessity justification for use (e.g. under 12 years old or under 18 years old).

Tramadol Use in Children
72
Ultram (tramadol) Package Insert
The safety and efficacy of Ultram in patients under 16 years of age have not been established. The use of Ultram in the pediatric population is not recommended.
FDA Drug Safety Communication – 9/21/15
FDA Evaluating Risks of Using Tramadol in Children Aged 17 and Younger:
The FDA is investigating the use of the pain medicine tramadol in children aged 17 years and younger, because of the rare but serious risk of slowed or difficult breathing.

Tramadol Use in Children
73
Mechanism of Action
Tramadol is a centrally acting synthetic opioid analgesic. Although its mode of action is not completely understood, at least two complementary mechanisms appear applicable: binding of parent and M1 metabolite to μ-opioid receptors and weak inhibition of re-uptake of norepinephrine and serotonin.
Opioid activity is due to both low affinity binding of the parent compound and higher affinity binding of the O-demethylated metabolite M1 to μ-opioid receptors. In animal models, M1 is up to 6 times more potent than tramadol in producing analgesia and 200 times more potent in μ-opioid binding.
Tramadol Use in Children
74
Metabolism
Tramadol is extensively metabolized after oral administration by a number of pathways, including CYP2D6 and CYP3A4, as well as by conjugation of parent and metabolites. Approximately 30% of the dose is excreted in the urine as unchanged drug, whereas 60% of the dose is excreted as metabolites. The remainder is excreted either as unidentified or as unextractable metabolites. The major metabolic pathways appear to be N- and O-demethylation and glucuronidation or sulfation in the liver. One metabolite (O-desmethyltramadol, denoted M1) is pharmacologically active in animal models. Formation of M1 is dependent on CYP2D6 and as such is subject to inhibition, which may affect the therapeutic response.
Tramadol Use in Children
75
Pharmacogenomics
Approximately 7% of the population has reduced activity of the CYP2D6 isoenzyme of cytochrome P-450. These individuals are "poor metabolizers". Based on a population PK analysis of Phase I studies in healthy subjects, concentrations of tramadol were approximately 20% higher in "poor metabolizers" versus "extensive metabolizers", while M1 concentrations were 40% lower.
Tramadol Use in Children
76
Serotonin Syndrome Risk
The development of a potentially life-threatening serotonin syndrome may occur with the use of tramadol products, including ULTRAM®, particularly with concomitant use of serotonergic drugs such as SSRIs, SNRIs, TCAs, MAOIs, and triptans, with drugs which impair metabolism of serotonin (including MAOIs), and with drugs which impair metabolism of tramadol (CYP2D6 and CYP3A4 inhibitors). This may occur within the recommended dose.
Serotonin syndrome may include mental-status changes (e.g., agitation, hallucinations, coma), autonomic instability (e.g., tachycardia, labile blood pressure, hyperthermia), neuromuscular aberrations (e.g., hyperreflexia, incoordination) and/or gastrointestinal symptoms (e.g., nausea, vomiting, diarrhea).

Tramadol Use in Children
77
Paid oral tramadol (includes tramadol/acetaminophen) claims for Idaho Medicaid participants – Age < 18 years
November 1, 2015 – October 31, 2016
1158 claims
803 unique patients
$12,688 in paid claims to pharmacies

Tramadol Use in Children
78
0-6 years, 0, 0% 7-11 years, 68, 6%
12-15 years, 554, 48%
16-17 years, 536, 46%
Paid oral tramadol (includes tramadol/acetaminophen) claims for Idaho Medicaid participants – Age < 18 years
November 1, 2015 – October 31, 2016

Tramadol Use in Children
15
14
12
9
8
3
2
1
1
1
1
1
0
0
0
Surgeon
PA
MD-FP
MD-ER
MD-Pediatrics
OB
Urology
Dentist
Podiatry
Student
Medical Examiner
other
MD-Internal Medicine
NP
Ophthalmology
Taxonomy of Prescribers
79

Tramadol Use in Children
80
Discussion on how to proceed
Currently tramadol and tramadol/acetaminophen are preferred agents and pay at the pharmacy with prior authorization not needed for patients ≥ 10 years of age.
Possible option: Institute age limits that would require an age override prior authorization with medical necessity justification for use (e.g. under 18 years old).

February 16, 2017
81

Low dose quetiapine
82
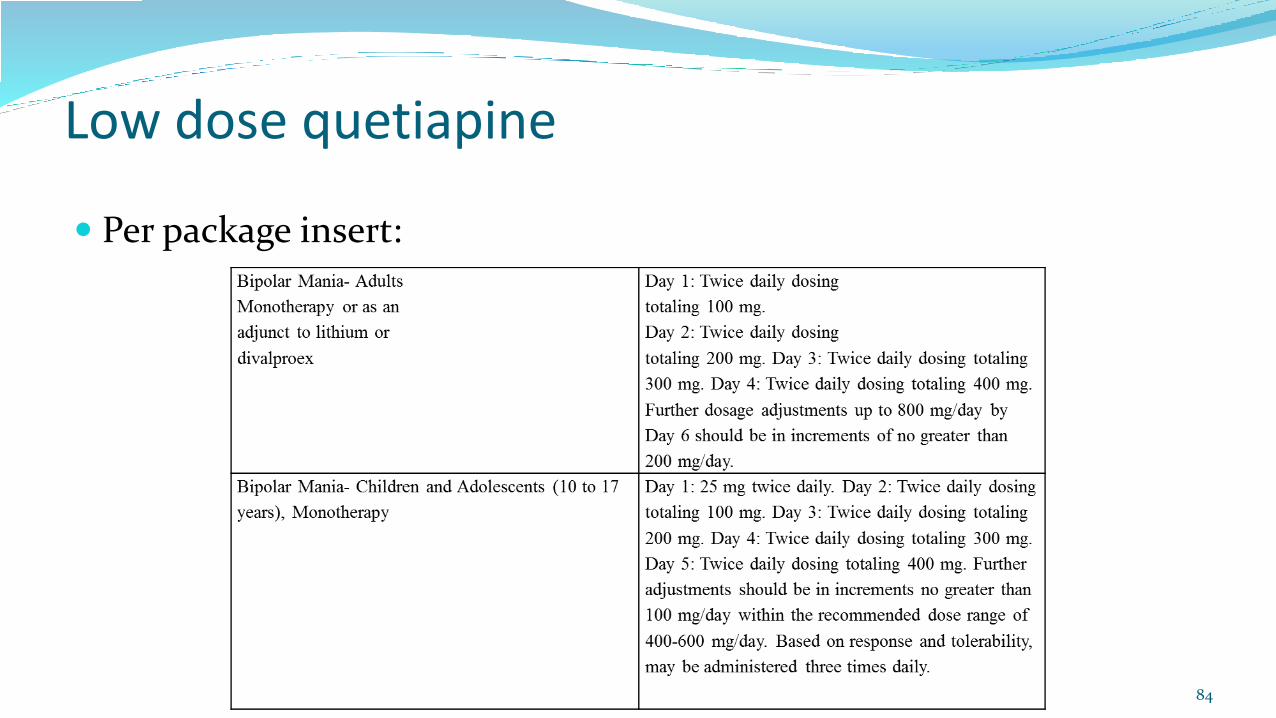
Per package insert:

Low dose quetiapine
83
Per package insert:
Low dose quetiapine
84
Per package insert:

Low dose quetiapine
85
Concern – Likely that low dose quetiapine (especially doses < 100mg/day) is being used off-label as a sedative-hypnotic as these doses are not therapeutic for treatment of either bipolar disease or schizophrenia.

Low dose quetiapine
86
Paid claims for quetiapine 25mg and 50mg tablets between 11/1/16 – 12/31/16
Children < 18 years
218 patients
372 claims
Adults ≥ 18 years
472 patients
819 claims
The majority of these patients are filling prescriptions for the 25mg and 50mg strengths monthly and for at least 30 tablets so these tablet strengths are NOT being used for initial dose titration.

Low dose quetiapine
87
176
42
Paid claims for quetiapine 25mg and 50mg tablets for children < 18 years between 11/1/16 – 12/31/16
Only on 25mg and 50mg tablets On 25mg and/or 50mg tablets plus larger strength tablet

Low dose quetiapine
88
48
4
78
2116
72
0
10
20
30
40
50
60
70
80
90
25mg 37.5mg 50mg 75mg 100mg 150mg 200mg
Nu
mb
er o
f p
atie
nts
Daily dose
Paid claims for quetiapine 25mg and 50mg tablets for children < 18 years between 11/1/16 – 12/31/16

Low dose quetiapine
89
Discussion on how to proceed next
Limiting 25mg and 50mg tablets to 6/month which is the maximum amount needed to titrate up to a minimally therapeutic dose per package insert dosing.
Concerns – will affect hundreds of current patients; staffing issues to handle phone calls and PA requests
Grandfather current patients ?
Send out educational DUR letter ?
February 16, 2017
90

Ophthalmic Antibiotic/Steroid Combinations
91
Paid claims between 9/1/16 – 11/30/16
DUR review requested by P&T Committee to look at taxonomy of prescriber of pediatric patients
Concern: Risk of cataract formation, glaucoma, or worsening infection, especially with long-term use.

Ophthalmic Antibiotic/Steroid Combinations
92
Risks Associated with Use of Ophthalmic Steroids
Prolonged use: risk for increased intraocular pressure (glaucoma) and secondary infections.
Micromedex Solutions – online database accessed 12/22/16
Cataracts can develop in patients with uveitis as a result of chronic ocular inflammation or secondary to the chronic use of steroids.
American Academy of Pediatrics
Pediatric Cataracts: An Overview
Nov 11, 2015

Ophthalmic Antibiotic/Steroid Combinations
93
< 18 years of age, 169, 64%
>= 18 years of age, 96, 36%
Paid claims between 9/1/16 – 11/30/16

Ophthalmic Antibiotic/Steroid Combinations
94
19
7
11
10
5
3
8
10
5
12
7
13
15
7
8
19
7
3
0
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
# of recipients
Age
of
reci
pie
nt
Breakdown by age
Ophthalmic Antibiotic/Steroid Combinations
95
Patients with more than one paid claim for an ophthalmic steroid
Of the 169 paid claims for patients < 18 years, 8 patients had 2 claims each during the 9/1/16 – 11/30/16.
Reviewed these 8 patients’ profiles and none of them had more than 2 paid claims for an ophthalmic steroid looking back for 2 years.

Ophthalmic Antibiotic/Steroid Combinations
96
Prescribed by ophthalmologist/optometrist, 7,
87%
Prescribed by surgeon, 1, 13%
Patients with more than one paid claim for an ophthalmic steroid

Ophthalmic Antibiotic/Steroid Combinations
97
108
18 159 6 5 3 5
0
20
40
60
80
100
120
# o
f p
resc
rib
ers
Taxonomy of prescribers

Ophthalmic Antibiotic/Steroid Combinations
98
Discussion
Majority of prescriptions were done by ophthalmologist/optometrists.
Can limit to one fill/60 days (or any other number of days) without prior authorization required.

Study Proposals for Upcoming Quarters:
99
Multiple dosage forms of quetiapine prescribed concomitantly
Paroxetine Use in Children
Temazepam – No Longer a Preferred Sedative
Paroxetine Use in Children
100
The P&T Committee in November 2016 expressed concern about the usage of paroxetine in children < 18 years old due to both lack of efficacy and incidence of side effects.

Paroxetine Use in Children
101
FDA Statement Regarding Anti-Depressant Paxil for Children
June 19, 2003
Three well-controlled trials in pediatric patients with MDD failed to show that the drug was more effective than placebo.
The Food and Drug Administration (FDA) said today it is reviewing reports of a possible increased risk of suicidal thinking and suicide attempts in children and adolescents under the age of 18 treated with the drug Paxil for major depressive disorder (MDD).
Paroxetine Use in Children
102
FDA Statement Regarding Anti-Depressant Paxil for Children
June 19, 2003
The FDA is recommending that Paxil not be used in children and adolescents for the treatment of MDD. There is currently no evidence that Paxil is effective in children or adolescents with MDD, and Paxil is not currently approved for use in children and adolescents. Other approved treatment options are available for depression in children.
The UK Department of Health issued a Press Release on June 10, 2003 stating that paroxetine (brand name Seroxat in the UK) must not be used to treat children and teenagers under the age of 18 years for depressive illness because UK authorities have concluded that there is an increase in the rate of self harm and potentially suicidal behavior in this age group, when paroxetine is used for depressive illness.

Paroxetine Use in Children
103
FDA Statement Regarding Anti-Depressant Paxil for Children
June 19, 2003
FDA advises that caretakers of pediatric patients already receiving treatment with Paxil for MDD talk to their doctor before stopping use of the drug. Patients should not discontinue use of Paxil without first consulting their physicians, and it is important that Paxil not be abruptly discontinued.

Paroxetine Use in Children
104
Current package insert for Paxil:
Pediatric Use: Safety and effectiveness in the pediatric population have not been established (see BOX WARNING and WARNINGS: Clinical Worsening and Suicide Risk). Three placebo-controlled trials in 752 pediatric patients with MDD have been conducted with PAXIL, and the data were not sufficient to support a claim for use in pediatric patients. Anyone considering the use of PAXIL in a child or adolescent must balance the potential risks with the clinical need.

Paroxetine Use in Children
105
Current package insert for Paxil:
In placebo-controlled clinical trials conducted with pediatric patients, the following adverse events were reported in at least 2% of pediatric patients treated with PAXIL and occurred at a rate at least twice that for pediatric patients receiving placebo: emotional lability (including self-harm, suicidal thoughts, attempted suicide, crying, and mood fluctuations), hostility, decreased appetite, tremor, sweating, hyperkinesia, and agitation.

Paroxetine Use in Children
106
Currently prior authorization is not required for patients > 6 years old.
Paid claims for paroxetine (both immediate release and extended release) in children < 18 years between 7/1/16 – 12/31/16: 86 patients identified.

Paroxetine Use in Children
107
10
2
5 56
16
2625
0
5
10
15
20
25
30
9 10 11 12 13 14 15 16 17
# o
f p
atie
nts
Age of patient
Breakdown by age (n=86)
Paroxetine Use in Children
108
Of the 86 patients with paid claims between 7/1/16 – 12/31/16, only 46 of them had paid claims between 11/1/16 – 12/31/16 showing a discontinuation rate of 47%.
Paroxetine Use in Children
109
Next steps for next quarter:
1. Change minimum age at which prior authorization is not needed for new patients as paroxetine immediate release is a preferred antidepressant to 18 years
2. Send out DUR letter to current patients on paroxetine who are < 18 years
a) Include educational information on efficacy and safety concerns
b) Who to include – e.g. exclude patients that are already 17 ?
c) Timeframe to implement change for current patients – e.g. 60 days to respond to DUR letter
Temazepam – No Longer a Preferred Sedative
110
Per Idaho Medicaid’s Pharmacy & Therapeutics Committee recommendation, temazepam 15mg and 30mg capsules have switched from preferred to non-preferred status effective 1-18-17. The other strengths of temazepam are already non-preferred.
The current preferred agents are zolpidem immediate release (unchanged for years) and Rozerem (ramelteon). The P&T Committee wanted to have a non-controlled sedative available as a preferred agent that would not require prior authorization.
Temazepam – No Longer a Preferred Sedative
111
Current patients who have a paid claim between 9-1-16 and 12-31-16 were identified:
398 unique recipients with 1203 paid claims
Many patients are filling their prescription monthly with 30 capsules monthly being the most common quantity.

Temazepam – No Longer a Preferred Sedative
112
Next steps for next quarter:
Send out DUR letter to current temazepam patients
Emphasize concerns about safety and efficacy of a long-term benzodiazepine, especially if the patient is concurrently on an opioid.
Prescriber will need to fill out a prior authorization form if they want the patient to continue on temazepam, including medical necessity justification, reason an alternative sedative cannot be used, and screening for substance abuse.
How long should we grandfather current patients ?

Prospective DUR Report
113
History Errors:
• DD – drug-to-drug
• PG – drug to pregnancy
• TD – therapeutic duplication
• ER – early refill
• MC – drug-to-disease
Non-History Errors:
• PA – drug-to-age
• HD – high dose
• LD – low dose
• SX – drug-to-gender

Prospective DUR Report
114

DUR Board Meeting February 16, 2017
115

Next Meeting April 20, 2017
116