fetal growth geneticmaternalplacental fetus healthy newborn & appr- size normal circumstances...
TRANSCRIPT

INTRAUTERINE GROWTH RESTRICTION: RISK FACTORS AND PATHOGENESIS
Joserizal Serudji

Introduction
FETAL GROWTH
genetic
maternalplacental
FETUSHEALTHY NEWBORN
& APPR- SIZENormal circumstances
InheritanceGrowth
potential
Introduction

Growth potential
Environ-ment
Ability to reach optimal birth weight
Introduction
Introduction
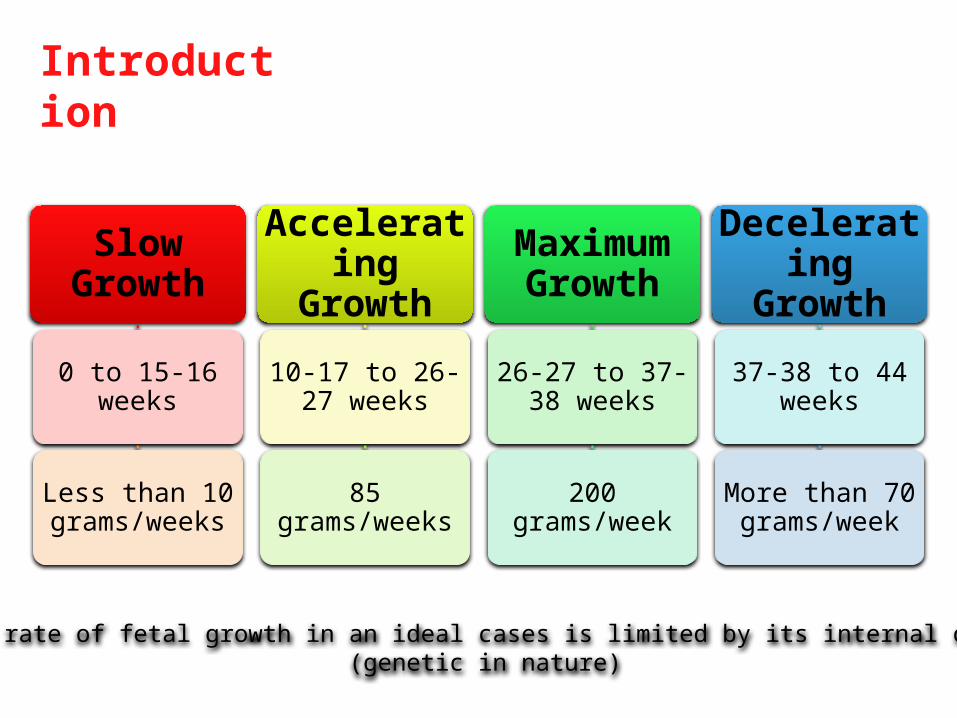
Slow Growth
0 to 15-16 weeks
Less than 10 grams/weeks
Accelerating Growth
10-17 to 26-27 weeks
85 grams/weeks
Maximum Growth
26-27 to 37-38 weeks
200 grams/week
Decelerating Growth
37-38 to 44 weeks
More than 70 grams/week
The normal rate of fetal growth in an ideal cases is limited by its internal constraints (genetic in nature)

Introduction

Introduction
Oxygen
Glucose
Amino
Acids
Fetal requirement

Introduction
Oxygen
Glucose
Amino Acids
Simple Diffusion
Facilitated Diffusion
Active Transport
Chemical energy (ATP)
Synthesis of lypids, glycogen, nucleoti des and
other molecules
Synthesis of protein

• Persistent decrease in availability of any of these substrates limit the ability of the fetus to reach its growth potential
• Persistent and severe substrate deficiency threaten the ability of the fetus to survive
• So many factors associated with reducing substrates supplies to the fetus
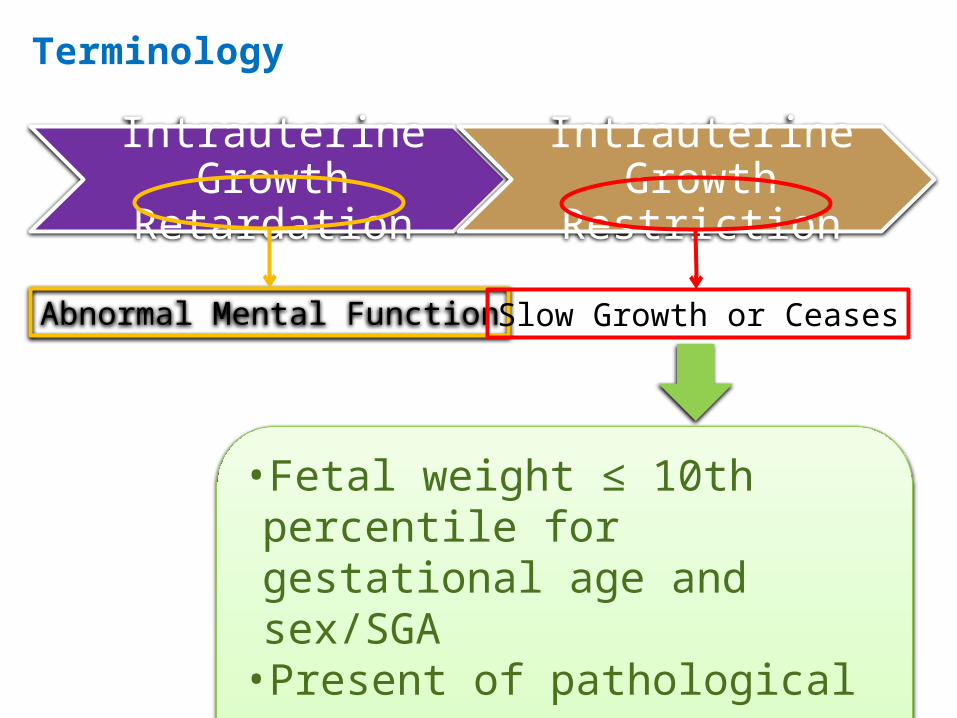
Terminology
Intrauterine Growth Retardation
Intrauterine Growth Restriction
Abnormal Mental Function Slow Growth or Ceases
•Fetal weight ≤ 10th percentile for gestational age and sex/SGA•Present of pathological process

SGA is defined as birth weight:• At 10th or less percentile, or• At 5th or less percentile, or• At 3rd or less percentile, or• 2 SDs below the mean for gestational age
The lower cut-off incidence and morbidity and mortality

Cut-off 10th percentile:
• SGA : 3—7 %• IUGR: 3 quarter (failed to achieve its potential
growth)• Non-IUGR: 1 quarters (constitutionally small)

Risk factorsIUGR occurs when gas exchange and nutrient delivery
to the fetus are not sufficientThe process occur primariliy because of:• Maternal disease causing decreased oxygen-carrying
capacity• A dysfunctional oxygen delivery system secondary to
maternal vascular desease• Placental damage resulting from maternal diseaseMany factors: fetoplacental fac tors and maternal
factors

Risk Factors
Constitutionally small mother• Small women have smaller baby• Reduced intrauterine growth of mother reduced intrauterine
growth of her children• Environment more important than genetic contribution
Poor maternal weight gain and nutrition• Lack of weight gain in the second trimester associated with
fetal growth restriction
Social deprivation• Associated to lifestyle factors such as smoking, alcohol or other
substances abuse and poor nutrition

Risk Factors
Fetal infections• Viral, bacterial, protozoon, and spirochaetal implicated on
fetal growth restriction• CMV direct cytolysis and loss functional cells• Rubella vascular deficiency• Another infection affect fetal growth : hepatitis A and B,
Listeriosis, TB, Syphilis, Toxoplasmosis and Congenital Malaria
Congenital malformations• More severe malformation more likely fetus to be small• Espescially with chromosomal abnormalities or serious
cardiovascular malformations

Risk Factors
Chromosomal abnormalities• Autosomal trisomies related togrowth restriction• Trisomy 18, 13 and 21• Not seen in Turner or Klinefelter Syndrome
Trisomi 16• Patches of trisomy 16 confined placental mosaicism
placental insufficiency fetal growth restriction
Primary disorders of cartilage and bone• Osteogenesis imperfecta• Various chondrodystrophies

Risk Factors
Chemical teratogens• Anticonvulsants (phenitoin, trimethadione)• Cigarette• Narcotics• Alcohol• Cocaine
Vascular disease• Chronic vascular disease especially when further complicated by
superimposed preeclampsia
Chronic renal disease• Renal disease maybe accompanied by restricted fetal growth

Risk Factors
Chronic hypoxia• Women in high altitude• Cyanotic heart disease
Maternal anemia• Anemia does not cause growth restriction (in most
cases)• Except : • sickle cell disease• inherited anemia with serious maternal disease• deficient total blood volume early in pregnancy

Risk Factors
Placental and cord abnormalities• Chronic partial placental separation• Extensive infarction• Chorioangioma• Marginal insertion of the cord• Velamentous insertion of the cord
Multiple fetuses• Two or more fetuses more likely complicated by
diminished growth of one or both fetuses compared with normal singleton

Risk Factors
Antiphospholipid antibody syndrome• Two classes of antiphospholipid antibodies :
• Anticardiolipin antibodies• Lupus anticoagulant
• Pathophysiological mechanism maternal platelet aggregation & placental thrombosis
Extrauterine pregnancy• Fetus gestated outside uterus is usually growth
restricted• Also some maternal uterine malformations

Pathogenesis & Categories
• There are standards and averages in weight according to gestational age (weeks)
• Using a fetal growth curve derived from one population and applyng to another over- or underestimation of true incidence of SGA
• A population of smaller individual will have smaller babies the difference lies in genetic growth potential

Normal intrauterine growth pattern:• 1st stage: 4—20 weeks gestation, rapid cell division and
multiplication (hyperplasia)• 2nd stage: 20—28/32 weeks gestation, cell division
(hyperplasia) and cells increase in size (hypertrophy)• 3rd stage: 28/32—40 weeks gestation, rapid increase in cell
size, rapid accumulation of fat, muscle and connective tissue
95% offetal weight gain occurs during the last 20 weeksIf development and weight gain is disturbed or
interrupted restricted growth

Fetal weight below tenth percentile
Pathological process present
IUGR
Increased Risk of Perinatal Mortality & Morbidity
Pathogenesis & Categories

IUGR
First StageHyperplactic Stage
Symmetric
Stage 2Hyperplastic and
Hypertrophic Stage
Stage 3Hypertrophic Stage
Asymmetric
Pathogenesis & Categories

Pathogenesis & Categories

Pathogenesis & Categories
Symmetrical Growth Restriction• Growth inhibition during first stage undersized
fetus with fewer cells but normal size• Weight, head and length < 10th percentile
proportionally small• Condition associated include genetic
(constitutional, chromosomal and single gene defect, deletion disorders and inborn error of metabolism), congenital anomalies, intrauterine infections, and therapeutic iradiation

Pathogenesis & Categories
Asymmetrical Growth Restriction• Growth inhibition during stage 2 and 3
decreased of cell size and fetal weight with less effect on total cell number fetal length and fetal head circumference
• Implies fetus who is undernourished and directing most of its energy to maintainaning growth of vital organs such as brain and heart at the expensive of the liver, muscle and fat role of brain sparing effect (redistribution mechanism)

Pathogenesis & Categories
Asymmetrical Growth Restriction• Normal head but small abdominal
circumference, scrawny limbs and thinned skin• Condition associated include uteroplacental
insufficiency (chronis hypertension or preeclampsia), chronis renal disease, cyanotic heart disease, hemoglobinopathies, placental infarcs, abruptio placenta, multiple gestation, velamentous insertion, cirmcumvallate placenta and high altitude

Perinatal Complication
Antepartum Complications
• Stillbirth• Oligohydramnios• Intrapartum fetal
acidosis

Perinatal Complication
Neonatal Complications
• Meconium aspiration syndrome• Persistent fetal circulation• Hypoxic-ischemic encephalopathy• Hypoglicemia• Hypocalcemia• Hyperviscosity syndrome• Deficient temperature controle

Conclusion
IUGR is a part of SGA with present of pathological process
Growth restricted fetus have a great chance to suffer from many prenatal and/or neonatal complications
Many factors should be recognized
Impaired substrates supply may reduce cellular process resulting in symmetrical or asymmetrical IUGR

Take home message
The most important thing in efforts to comprehensively overcome IUGR
issues is the early detection of its risk factor(s), -- eg. Premarital, preconception, or as early as
possible in pregnancy

THANK YOU