final open mole pdf
TRANSCRIPT
8/8/2019 Final Open Mole PDF
http://slidepdf.com/reader/full/final-open-mole-pdf 1/27
O R I G I N A L P A P E R
Trauma and Humanitarian Translation in Liberia:
The Tale of Open Mole
Sharon Alane Abramowitz
Published online: 17 April 2010Ó Springer Science+Business Media, LLC 2010
Abstract The focus of this paper is the intercultural process through which Open
Mole and trauma-related mental illnesses are brought together in the postconflict
mental health encounter. In this paper, I explore the historical dimension of this
process by reviewing the history of Open Mole, and the ways in which it has been
interpreted, acted on, and objectified by external observers over the last half-
century. Moving into Liberia’s recent war and postconflict period, I examine the
process by which Open Mole is transformed from a culture-bound disorder into alocal idiom of trauma, and how it has become a gateway diagnosis of PTSD-related
mental illnesses, and consider how it is produced as an objectified experience of
psychiatric disorder in clinical humanitarian contexts. By studying how Open Mole
is transformed in the humanitarian encounter, I address the structure and teleology
of the humanitarian encounter and challenge some of the foundational assumptions
about cultural sensitivity and community-based mental health care in postconflict
settings that are prevalent in scholarship and practice today.
Keywords LiberiaÁ
TraumaÁ
Open MoleÁ
Transcultural psychiatryÁ
Culture-bound syndromes Á Idiom of distress Á Community-based mental health Á
Humanitarian intervention
Introduction
The Tale of Open Mole is a story of Liberian suffering in dialogue with
humanitarian agencies’ understandings of local experience around a single local
S. A. Abramowitz (&)
Department of Anthropology, Harvard University, William James Hall No. 302, 33 Kirkland Street,
Cambridge, MA 02138, USA
e-mail: [email protected]
123
Cult Med Psychiatry (2010) 34:353–379
DOI 10.1007/s11013-010-9172-0

8/8/2019 Final Open Mole PDF
http://slidepdf.com/reader/full/final-open-mole-pdf 2/27
idiom of distress—an Open Mole, or ‘‘hole in the head’’ (sunken fontanelle),
occurring in adults, along with symptoms of pain, dizziness, headache, confusion,
social withdrawal and occasional fugue states—that is prevalent in rural commu-
nities and across ethnic groups in contemporary Liberia. In this paper, I study how
nongovernmental organizations (NGOs) integrate local categories of somatizeddistress into their operational diagnoses of trauma-related mental illness and
transform social reality through interventions. I present the historical dimension of
this process by reviewing Open Mole’s history, etiology and interventions. I
demonstrate the process by which Open Mole is transformed from a culture-bound
disorder into a local idiom of trauma, and from a local idiom of trauma into an
object of clinical psychiatry. I go on to examine how this process of transformation
occurs by studying the ‘‘dialogic’’ encounter between international NGO ‘‘local
practitioners’’ and ‘clients,’ and use Open Mole to examine how ‘‘culturally
sensitive’’ mental health programs and ‘‘community-based’’ trauma-healing initia-tives yield unintended outcomes.
Culturally sensitive, community-based mental health care is now a widely
idealized model for postconflict mental health and psychosocial intervention [Inter-
Agency Standing Committee (IASC) 2007; Weiss et al. 2003]. Through ‘‘The Tale
of Open Mole,’’ a local idiom of distress with a long social history in Liberia, I track
the trajectory of semiotic movement around a cultural idiom—specifically, the
movement around Open Mole—as it is transformed from a culture-bound form of
somatic illness, to an ‘idiom of distress’ with transcultural psychiatric interpreta-
tions, to a gateway diagnosis for PTSD and a host of other trauma-related mentalhealth and psychiatric disorders at Healthworkers International (HI), an interna-
tional medical humanitarian NGO. I demonstrate how cultural meanings
surrounding mental illness and trauma are strategically integrated into global
programs, thereby transforming the meanings of local idioms into a ‘‘pidgin
psychiatry’’ that transforms original ontologies into different, but legible and
perceptible phenomena that fit within humanitarian epistemologies. The goal of this
paper is to show how meanings of mental illness, trauma and local idioms of distress
are ‘‘appropriated and translated’’ (Merry 2006) in clinical encounters and come to
take on an ‘emanating’ transformation of social definitions and conventions.
Research Setting
The civil war in Liberia (1990–2003) earned an international reputation for the
chaos it inspired in every part of social, moral, religious, political and economic life,
and earned Liberia a dubious reputation as an exemplary model of a ‘‘failed state.’’
The conflict itself lacked an ideological foundation and was known internationally
for its endless splintering factions, the ruthless greed and murderousness of Charles
Taylor and other faction leaders, ‘‘blood diamonds’’ and ‘‘blood timber,’’
widespread rape, displacement, child soldiering and dismemberment and cannibal-
ism (Ellis 1999; International Crisis Group 2004; Moran and Anne Pitcher 2004;
Renner et al. 2002; Sawyer 2005). Between 1990 and 2003, nearly 200,000 people
were killed in warfare—approximately 10 percent of the country’s total population.
354 Cult Med Psychiatry (2010) 34:353–379
123

8/8/2019 Final Open Mole PDF
http://slidepdf.com/reader/full/final-open-mole-pdf 3/27
Population displacement occurred on a massive scale within and outside Liberia’s
borders, leading to the flight and repatriation of more than 1 million Liberian
citizens several times and contributing to the spillover of violence into neighboring
states (Sierra Leone, Guinea and Cote d’Ivoire). At the local level in Liberia, the
extent to which violence reached into the lives of every village, hamlet andtownship is palpable.
By the conclusion of the conflict, few standing structures remained in most
communities. Villages virtually inaccessible to major markets were reached by rebels
and burned to the ground. Tens of thousands of Liberians spent years foraging in the
rainforest and avoiding settled areas, which were usually controlled by one faction or
another. Rape occurred so widely that it became a taken-for-granted part of everyday
life. However, since Charles Taylor’s resignation and departure in 2003, the end of the
Liberian civil war, and the intervention of the United Nations Mission in Liberia
(UNMIL), a massive international effort has been under way to reconstruct the countryof Liberia. New institutions, buildings, roads and bridges are slowly being rebuilt.
Children and adults are returning to school, there has been a successful Presidential
election, and the country is starting to report positive economic growth. Liberians are
seeking jobs, night school education, university enrollment, computer training and job
training programs amid an economic environment of nearly 80 percent formal
unemployment. As one Liberian student said, ‘‘During the war, we all had to sleep on
the floor. Now, we are just trying to get our mattresses, and then get our mattresses off
of the floor. Small small, we are trying to rebuild.’’
Tens of thousands of Liberians are attempting to manage the emotional,psychological and somatic consequences of past violence and present vulnerability
while struggling to take back their lives and country from the enduring violence of
the Liberian civil war. Some are doing so through art, theater, socializing and telling
stories to friends and family. Thousands are simply trying to forget, to ‘‘put the past
behind us. Now is a time of forgiveness.’’ Thousands of youth and adults cannot let
go, and cling to the lifestyles, social arrangements, drugs and crime they became
habituated to during the war. This article focuses on a small subset of the population
using psychiatric interventions as a way to find peace and resolve the trauma of war,
which has been re-interpreted by the HI Psych Team through the local idiom of
distress called ‘‘Open Mole.’’ HI is the sole provider of outpatient psychiatric care
outside of Monrovia, Liberia’s capitol city.
Methods
This investigation took place during dissertation research investigating psychosocial
interventions, mental health and psychiatric care, and individual and collective
trauma in the context of Liberia’s postconflict transition (Abramowitz 2009). I
conducted this investigation at a major medical NGO, given the pseudonym
‘‘Healthworkers International,’’1 which is working in several counties in Liberia.
Data collection included an array of ethnographic methods, including participant
1 This study’s findings were provided to HI in an internal report at the conclusion of field research.
Cult Med Psychiatry (2010) 34:353–379 355
123
8/8/2019 Final Open Mole PDF
http://slidepdf.com/reader/full/final-open-mole-pdf 4/27
observation of HI-patient clinical consultations, formal and informal interviews with
Open Mole sufferers, traditional healers, and health-care providers. I also analyzed
medical records during two field visits in December 2006 and February 2007 and
participated in community outreach activities, ‘traditional women’s’ groups, and
ex-combatant psychosocial follow-up in seven of HI’s beneficiary communities. Bythe conclusion of my research, I collected 40 clinical case narratives from HI Psych
Team patient visits and considerable qualitative data on the Psych Team’s activities,
operations, and clinical procedures.
What is Open Mole?
Across Liberia, a single unified characteristic defines Open Mole. Open Mole is
understood to be a soft spot in the center of the skull similar to the soft areas in aninfant’s unformed skull, or the sunken fontanel associated with infant dehydration
(Kezala et al. 1989). However, in contrast to the infant skeletal development
processes and the dehydration-induced softening with which the Western medical
literature is familiar, Open Mole is understood to be an acquired disease state that
can occur to adults who experience a sudden fright or shock or who endure chronic
adversity and stress. While its defining symptom is the soft spot on top of the skull,
Open Mole is commonly associated with many symptoms, including: severe
headache, neck pain, back pain, fatigue, weakness, nightmares, troubled sleep,
loss of appetite and social withdrawal (see Table 1 for a comprehensive list of Open Mole symptoms). Many additional symptoms are believed to accompany
Open Mole, but there is little consensus among Liberians about Open Mole’s
ethnophysiology.
The etiology of Open Mole is heterogeneous. Although a belief in the existence
of Open Mole exists across geographical boundaries2 (Bender and Ewbank 2004)
and ethnic groupings,3 it is contested among Liberians on a number of indicators.
Some understand Open Mole to be contagious, while others believe that it is not.
Some believe that Open Mole is caused by tampering with dangerous spiritual
forces, practicing witchcraft or having a dangerous nightmare, while others believe
that it can be caused by sharing a hairbrush or a headscarf, getting caught in the rain
or sitting in the sun too long. Some believed that Open Mole is caused by
committing an act of wrongdoing (like violence, theft or sorcery), while others
believed that Open Mole is a victim’s affliction, carried by those who have had
wrong done to them.
Traditional healers’ medical examination for Open Mole consists of a perfunc-
tory study of the sufferer’s head and a brief recounting of symptoms. The healer
then prepares a paste of herbs and leaves, shaves a small space on the top of the
sufferer’s head, applies the paste and bandages the head tightly. This remedy is
2 Sources cited in this paper document reports of Open Mole across diverse population centers, including
Zorzor, Gbarnga, Beh Town, Gbama Town, Gohgan Town and Bopalu.3 Reports in this paper include Open Mole complaints coming from women from Bassa, Gola, Loma,
Kpelle and Kissi ethnic groups.
356 Cult Med Psychiatry (2010) 34:353–379
123
8/8/2019 Final Open Mole PDF
http://slidepdf.com/reader/full/final-open-mole-pdf 5/27
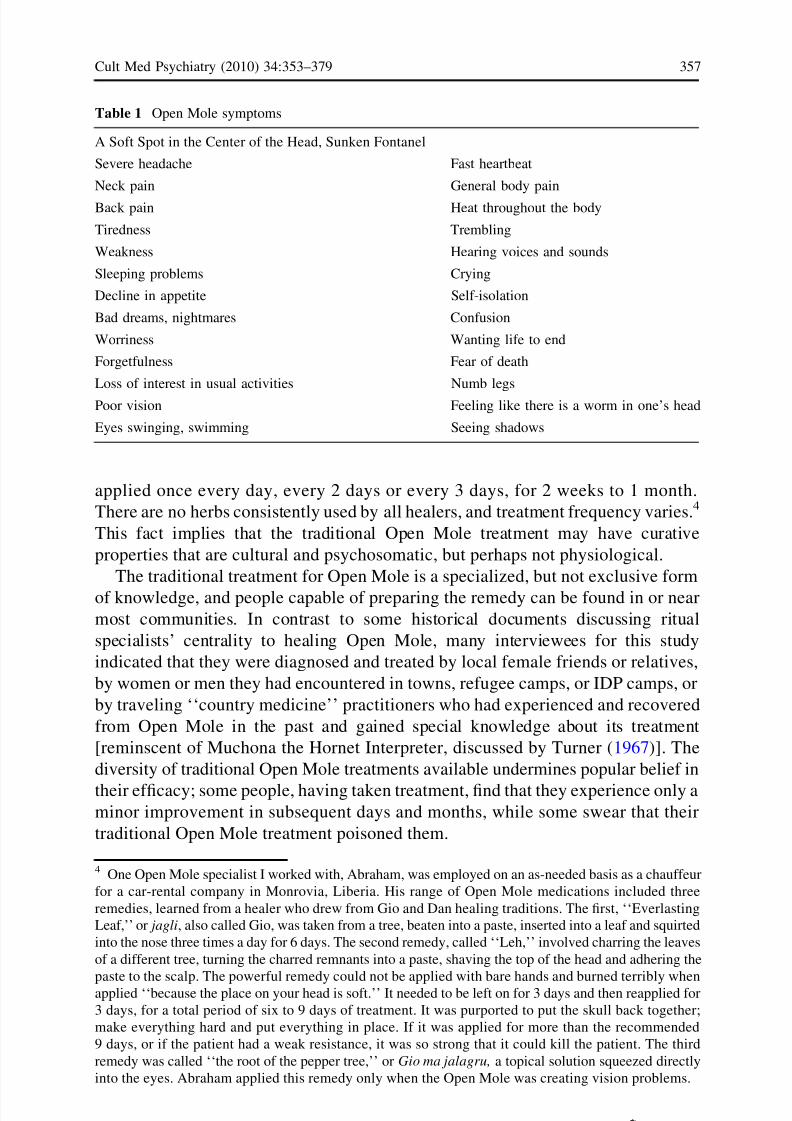
applied once every day, every 2 days or every 3 days, for 2 weeks to 1 month.
There are no herbs consistently used by all healers, and treatment frequency varies.4
This fact implies that the traditional Open Mole treatment may have curative
properties that are cultural and psychosomatic, but perhaps not physiological.
The traditional treatment for Open Mole is a specialized, but not exclusive form
of knowledge, and people capable of preparing the remedy can be found in or near
most communities. In contrast to some historical documents discussing ritual
specialists’ centrality to healing Open Mole, many interviewees for this study
indicated that they were diagnosed and treated by local female friends or relatives,
by women or men they had encountered in towns, refugee camps, or IDP camps, or
by traveling ‘‘country medicine’’ practitioners who had experienced and recovered
from Open Mole in the past and gained special knowledge about its treatment
[reminscent of Muchona the Hornet Interpreter, discussed by Turner (1967)]. The
diversity of traditional Open Mole treatments available undermines popular belief in
their efficacy; some people, having taken treatment, find that they experience only aminor improvement in subsequent days and months, while some swear that their
traditional Open Mole treatment poisoned them.
Table 1 Open Mole symptoms
A Soft Spot in the Center of the Head, Sunken Fontanel
Severe headache Fast heartbeat
Neck pain General body pain
Back pain Heat throughout the body
Tiredness Trembling
Weakness Hearing voices and sounds
Sleeping problems Crying
Decline in appetite Self-isolation
Bad dreams, nightmares Confusion
Worriness Wanting life to end
Forgetfulness Fear of death
Loss of interest in usual activities Numb legs
Poor vision Feeling like there is a worm in one’s head
Eyes swinging, swimming Seeing shadows
4 One Open Mole specialist I worked with, Abraham, was employed on an as-needed basis as a chauffeur
for a car-rental company in Monrovia, Liberia. His range of Open Mole medications included three
remedies, learned from a healer who drew from Gio and Dan healing traditions. The first, ‘‘Everlasting
Leaf,’’ or jagli, also called Gio, was taken from a tree, beaten into a paste, inserted into a leaf and squirted
into the nose three times a day for 6 days. The second remedy, called ‘‘Leh,’’ involved charring the leaves
of a different tree, turning the charred remnants into a paste, shaving the top of the head and adhering the
paste to the scalp. The powerful remedy could not be applied with bare hands and burned terribly whenapplied ‘‘because the place on your head is soft.’’ It needed to be left on for 3 days and then reapplied for
3 days, for a total period of six to 9 days of treatment. It was purported to put the skull back together;
make everything hard and put everything in place. If it was applied for more than the recommended
9 days, or if the patient had a weak resistance, it was so strong that it could kill the patient. The third
remedy was called ‘‘the root of the pepper tree,’’ or Gio ma jalagru, a topical solution squeezed directly
into the eyes. Abraham applied this remedy only when the Open Mole was creating vision problems.
Cult Med Psychiatry (2010) 34:353–379 357
123

8/8/2019 Final Open Mole PDF
http://slidepdf.com/reader/full/final-open-mole-pdf 6/27
To understand the disparate interpretations and treatments of Open Mole in
traditional medicine, it is important to understand that the course of the Liberian
Civil War has led to a radical disruption in traditional medical systems’ ability to
reproduce itself. Whereas, in the past, there may have been coherence among
etiology, symptoms and treatments, in the present, traditional medical knowledge isfractured, incomplete and ad hoc. Open Mole treatments, however, extend beyond
the domain of ‘‘traditional medicine.’’ Most sufferers of Open Mole use an array of
strategies to manage Open Mole. Liberians self-medicate widely for Open-Mole-
like symptoms of ‘‘worriness’’—or constant preoccupation with one’s past, present
and future troubles, ‘‘headache,’’ ‘‘blood pressure’’ and ‘‘can’t sleep,’’ using widely
available drugs like diazepam (Valium), sleeping pills, ‘ayurvedic’ sedatives and
‘Chinese medicines’ from Indian and Chinese pharmaceutical companies that have
been smuggled into urban and rural markets.5 They also turn to alcohol and
marijuana to manage Open Mole’s effects. Additionally, Liberians depend on anarray of social strategies to escape Open Mole. They attend church to try to pray the
Open Mole away, they pray privately, they visit with friends and relatives in search
of advice and support and, occasionally, they withdraw from society altogether.
Social interventions are rarely reported to be effective.
The History of Open Mole
There are few previous mentions of Open Mole in the scholarly literature onLiberia, although the references available demonstrate Open Mole’s continued
undulation between psychiatric and somatic interpretations. Bearing remarkable
similarity to the symptom presentations of Open Mole today, Poindexter’s (1953a,
b) epidemiological study of the Gola more than a half-century ago found many
reports of Open Mole and recorded its somatic manifestations:
There is a combination of symptoms among certain native African tribes
referred to as the ‘‘Open Mole’’ of the adult. Medical schools, medical journals
and standard medical texts either do not mention the condition or do not
recognize it as an entity. The ‘Open Mole,’ ‘Craw Craw’ and a few otherconditions referred to by the natives as definite diseases do not have known
specific etiologies… The cases of ‘Open Mole’ in this study present a certain
similarity of symptoms and physical findings. These were all adults with
widened sagittal sutures and easily felt pulsations in the anterior fontanelle
regions. All of them showed elevated blood pressures. Some showed signs of
increased intra-cranial pressure such as pupil changes, hyperactivity of the
peripheral reflexes, rigidity of the neck, etc. There were areas of tenderness
over the head or face. Headache was a common symptom to all. The Hahn
tests and malaria smears were negative except in one case. This appears to be asyndrome worthy of further study (Poindexter 1953b).
5 I was able to purchase off-license remedies for ‘worriness,’ ‘can’t sleep’ and ‘thinking too much’ from
markets at most of the communities I visited with the HI Psych Team.
358 Cult Med Psychiatry (2010) 34:353–379
123

8/8/2019 Final Open Mole PDF
http://slidepdf.com/reader/full/final-open-mole-pdf 7/27
By 1968, however, Open Mole had come to be interpreted as a mental illness by
foreign observers, although the presentation of symptoms remained essentially the
same. Dr. Ronald Wintrob of McGill University, who had served for two years as
the only psychiatrist in Liberia and as the director of its sole psychiatric unit, the
Catherine Mills Rehabilitation Center, described Open Mole in an article entitled‘‘Sexual Guilt and Culturally Sanctioned Delusions in Liberia, West Africa.’’ His
goal was to demonstrate in two case studies the clinical presentation of symptoms of
depression, which ‘‘become rapidly obscured by the development of agitation and
paranoid thinking … with the elaboration of a delusional system focused on
fantasies [culturally sanctioned delusions; sic] of snakes and genii.’’ (Wintrob
1968).
Wintrob’s interpretation of Open Mole is offered through a classical transcultural
psychological perspective that provides a fascinating contrast to the current state of
the field. He describes the story of a woman in her mid-20’s who is admitted to the(now destroyed) psychiatric hospital in Monrovia in a state of agitation, with
severely disorganized thinking and overactive behavior. He describes her biography
of social marginality, conflict-ridden relationships and an absence of familial
support, and describes her ‘‘descent’’ into a life of bar-cruising and prostitution. Her
symptoms began during her failure to conceive a child with a new husband. Wintrob
(1968) narrates the beginning of her Open Mole with the following story:
About 4 weeks prior to admission, she began to experience fugue-like
confusional states and episodes of irritability in which she would ‘‘just cuss
the people out’’ who lived in the surrounding houses. She suspected thatsomeone had witched her by putting ‘‘medicine’’ in her food ‘‘to spoil my
belly…’’ Three days prior to admission she had suddenly wakened following a
dream in which a huge black snake wound around her body and was
suffocating her. The next morning, she thought she saw the same snake in the
river, with its tail sticking up out of the water. The snake wound around her
and ordered her to bring a human sacrifice. She replied that she had nobody
she could offer and ran home in a panic. Thereafter she was confused and
restless, complained of her eyes turning, of headache, and of ‘‘Open Mole’’
(fontanelle.) Agitation increased rapidly. She would shout, ‘‘My heart want to jump out. Everything be turning before my eyes. Snake be coming all around
me. The people make me plenty crazy—oh!’’ She slept poorly, overturned
furniture, dumped food on the floor, tore her clothes, and fought with anyone
who tried to restrain her (Wintrob 1968).
Wintrob interpreted her spiritual interpretation of a snake as symptoms of
psychosis while continuing an ongoing regime of medications. He attributed her
Open Mole to denied and repressed guilt feelings about sexual behavior, fear of
imminent rejection by her husband, aggressive impulses and ‘‘fantasies of reparation
such as sacrifice .…
Massive ego regression followed. The culturally sanctioned
delusions in this case appeared to be primarily superego delusions.’’ The Bassa
woman, however, understood Open Mole to be caused by her neighbors through
sorcery, or ‘‘African sign.’’ Following local Bassa interpretations of Open Mole, the
Bassa woman’s visions resonated with a regional belief in the power of ‘‘Mami
Cult Med Psychiatry (2010) 34:353–379 359
123
8/8/2019 Final Open Mole PDF
http://slidepdf.com/reader/full/final-open-mole-pdf 8/27
Wata’’ (Drewal 1988, 2008; Frank 1995). We see here how Open Mole’s etiology,
symptoms and moral terms are very much mediated by the professional framework
of the clinical beholder.
In 1975, M. Wheeler observes that Open Mole, identified in treatment at a
hospital in Zorzor, indicated dehydration in children and mental illness in adults. Henoted that in children, Open Mole occurred as a result of dehydration and required
the application of local or commercial topical medicines. For adults, however, Open
Mole assumed a different profile. Wheeler (1975) wrote:
Basically any adult who is ill-at-ease with his environment, anxious,
depressed, or even frankly psychotic is examined by a country doctor, who
often finds a soft spot somewhere on the head of the patient. This is
pathognomonic of open mole. Treatment consists of various salves, plus what
is apparently some form of counseling by the country doctor, and seems to be
surprisingly successful.
By the late 1980s, Kezala and his colleagues (1989) were again studying Open
Mole solely as a physiological problem of sunken fontanel in children, but Open
Mole was alive in Liberia’s psychiatric legacy and remerged just a few years later.
Hales (1996) study of Liberian beliefs about mental illness reported that her study
population—Liberian nursing students and their elder relatives—believed that Open
Mole was an inherited mental illness that was passed ‘‘down the line’’ through the
mother’s side, either from the mother herself or from an ancestor who had been ‘‘so
offensive to the spirits that the whole lineage was punished with mental illness.’’Hales wrote:
The generally accepted belief is that people with excessive symptoms of
anxiety have a congenital opening at the junction of their fontanels, which
provides an entry for evil spirits.… A person with ‘‘open mole’’ is generally
treated for his or her anxiety by talking to a zoe, who then determines the
source of the anxiety. The nursing goal of helping clients to examine sources
of their own anxiety was compared to this kind of ‘talk therapy.’
The ethnophysiology of Open Mole among Liberian populations is clearly
diverse and, therefore, difficult to generalize. Open Mole has resonance with
previously studied somatized mental illnesses widely known among West African
populations (Kirmayer 1984; Makanjuola 1987), including Brain Fag (Prince 1960)
and other illnesses like Nigerian ode ori, innu, and were ironu (Patel 1995). Open
Mole resembles Brain Fag in that pain and burning in the neck and at the crown of
the head is the somatic complaint:
This may be described as pain the back of the neck and over the occiput,
frontal headache, burning sensations over the scalp (‘‘as if pepper had been
rubbed into it’’), a burning sensation in the centre of the head, ‘‘like a piece of red hot iron’’, a feeling of waves passing over the scalp, a feeling of vacancy in
the head, etc. (Prince 1960).
There are accompanied symptoms, including headache, alteration in vision and
onset of weakness and fatigue, associated with mental exertion (for Liberians,
360 Cult Med Psychiatry (2010) 34:353–379
123
8/8/2019 Final Open Mole PDF
http://slidepdf.com/reader/full/final-open-mole-pdf 9/27
‘‘stress and worriness’’ constitutes the mental exertion, while for Prince’s students, it
was exams and coursework). Compellingly, Patel (1995) wrote ‘‘…The soul and
spirit is concerned with mental life and emotions, and some authors suggest that
illnesses of the ‘spirit’ and of the ‘soul’ are probably analogous to mental illness.
The somatic localization of the soul and mind is in the head, chest, and/orabdominal regions.’’ Although there is no direct correlation between Open Mole and
other African mental illnesses, the parallel is suggestive. Significantly, however,
Kirmayer and Young (1998) remarked that the classification of Brain Fag and other
somatized illnesses are in fact Western constructions, rather than local idioms of
distress. As we shall see, this problem of classification has important relevance for
the interpretation of Open Mole by humanitarian agencies.
Healthworkers International
Open Mole was first brought to my attention in October 2006 by the general
coordinator of HI–Liberia while I conducted an institutional inventory of mental
health and psychosocial services across Liberia. HI is a fairly typical medical
humanitarian NGO that provides emergency and preventive health services to rural
and urban populations through mobile outreach teams, community-based clinical
work and inpatient hospital care (e.g., Medecins Sans Frontiers, MERLIN, and
IMC). HI provides approximately 30–60 percent of the medical care in the counties
they serve, and has been doing so since 2003. Similarly to most other medical NGOsoperating in Liberia today, the HI mobile medical unit travels into surrounding
counties providing primary health care, health care referrals, free medication and
public education about health issues ranging from infant and maternal health to
HIV/AIDS. They also operate hospitals in regional centers and are relevant on the
national health scene—they participate actively in policy discussions, coordination
efforts and international conferences about the future of medicine and health care in
Liberia.
HI is unusual, however, in that, in the absence of donor support for mental health
care in Liberia, it has taken the initiative to muster funding and resources from their
own coffers to provide psychiatric care, psychological counseling and psychiatric
medications to rural populations. They provide salary, training, supervision,
transport and resources (medical, logistical, pharmaceutical) to a ‘‘Psych Team’’
consisting of two psychiatric nurses and five psychological assistants/counselors. An
on-the-ground expatriate hired for a 6-month period of volunteer service supervises
the Psych Team, but due to recruitment issues, HI has had some difficulty ensuring
continuity of supervision. At times, the Psych Team has been managed by a
psychiatric nurse, while at other times the Psych Team has been run by a
psychologist with a psychoanalytic orientation, leading to a lack of consistency in
processes of prioritization in training and service delivery. The expatriate’s skill set
has been dictated by the availability of European volunteers, more than the needs of
the Psych Team, and during my period of research, the Psych Team had been
without direct extended supervision for a 6- to 9-month period. During these
extended gaps of supervision, the Psych Team receives long-distance supervision
Cult Med Psychiatry (2010) 34:353–379 361
123
8/8/2019 Final Open Mole PDF
http://slidepdf.com/reader/full/final-open-mole-pdf 10/27
and technical oversight (several short-term visits each year to provide training,
supported by phone supervision on an approximately weekly or biweekly basis) by a
European psychiatrist.
HI’s investment in mental health is truly remarkable in that key decision makers
at HI headquarters in Europe materially support their conviction that psychologicaland psychiatric care constitute fundamental human rights and are of central
importance in Liberia’s postconflict reconstruction. By the onset of their work in
Liberia, mental health care had fallen into disfavor in humanitarian donor networks,
and it was nearly impossible to attain any funding for clinically based psychiatric
care in Liberia6 from traditional donor groups like ECHO, USAID, UNDP, or the
myriad bilateral and multilateral agencies funding Liberia’s postconflict recon-
struction.7 Even more remarkably, in the continued absence of funding lines, HI’s
European leadership has sustained the political will to continue to advocate for
mental health care in the absence of new funding opportunities.Although HI’s initial foray into mental health in Liberia began with some ex-
combatant rehabilitation projects during 2003–2005, the Psych Team’s responsi-
bilities have expanded dramatically. The Psych Team’s principal responsibilities
include clinical psychiatric consultations in an outpatient setting, diagnosing
psychiatric disorders, and prescribing psychiatric medication to people suffering
from PTSD, depression, anxiety, episodes of psychosis, and schizophrenia. To build
a mental health education and outreach capacity, the Psych Team organizes
‘traditional women’s groups’ in the communities they serve, where they bring
together ‘traditional’ women—local female residents in rural communities—andconduct group therapy in a quasi-educational format. They then turn these groups
into local outlets for outreach and clinical referral.
Postconflict Mental Health: Intervention Debates
For the last 20 years, scholars and practitioners have debated the diagnosis and
treatment of posttraumatic stress disorder (PTSD), and the appropriateness of PTSD
counseling and psychosocial intervention in postconflict settings. Within this
debate, considerable psychiatric, psychological, medical and anthropological
discourse has been dedicated to debating problems of validity, utility, cross-cultural
sensitivity, the rights of the mentally ill and the practical conditions of normal
suffering and response in postconflict contexts. The locus of disagreement around
mental health care in postconflict settings revolves around rapid mental health and
psychosocial interventions for PTSD (Van Ommeren et al. 2005). Psychiatrists and
medical anthropologists tend to agree with the following assertions: severe cases of
acute and chronic PTSD exist; PTSD can destroy health, lives and social worlds;
and PTSD and other trauma-related mental illnesses require medical and counseling
interventions (Baingana et al. 2005; de Jong et al. 2003; International Federation of
Red Cross, Red Crescent Societies 2009; Salama et al. 2004). Advocates for
6 The only other organization in Liberia providing psychiatric care is also self-funding its own efforts.7 I discuss this phenomenon in a publication in progress.
362 Cult Med Psychiatry (2010) 34:353–379
123

8/8/2019 Final Open Mole PDF
http://slidepdf.com/reader/full/final-open-mole-pdf 11/27
psychosocial intervention argue that experiences and memories of violence have
important implications for the possibility of reconstruction in postconflict settings;
impeding civil society reconstruction efforts, preventing the reintegration of
ex-combatants in community life and damaging family, societal and political
dynamics for years and decades to follow (Reno 2004; Sawyer 2005; UNMIL 2005).However, scholars and practitioners disagree over attempts to address these
issues in postconflict settings. Important critiques assert that the Western-based
PTSD diagnosis may be an inappropriate framework with which to understand non-
Western, conflict-related experience, and individual resiliency, and community
resources. It is argued, moreover, that the PTSD framework may be incapable of
engaging local biomedical experience, integrating local explanatory models, and
working with locally understood illness trajectories to create appropriate treatment
options (Bracken et al. 1995; Summerfield 1995). In contrast, advocates for the
provision of mental health care, including treatment for PTSD, argue that thosesuffering from established severe mental illness are vulnerable to harm, violence,
abandonment, stigma, sickness and neglect (Desjarlais et al. 1995; Silove et al.
2000). Via de facto inclusion, this debate has also come to encompass the treatment
of disorders frequently associated with PTSD comorbidity, including depression,
anxiety, and drug and alcohol abuse that often implicitly fall into this category of
debate.
Academics and practitioners are making efforts to move beyond the debate by
tackling these issues through interdisciplinary study (Kirmayer et al. 2008), policy
recommendations for a diversity of minimum standards [Inter-Agency StandingCommittee (IASC) 2007; Psychosocial Working Group 2003] and the adoption of a
holistic approach to humanitarian practice, exemplified by the ‘‘black box’’ term
psychosocial. In comparison to underfunded psychiatric interventions and now-
controversial trauma healing activities, psychosocial interventions that place a
premium on ‘‘community-based interventions’’ have become the norm in postcon-
flict settings. Under the label psychosocial, a consensus has emerged around the
goal of providing population-based mental health services that are based on a public
health framework, with the key characteristics of being ‘‘affordable, effective,
acceptable, and culturally valid interventions at the community level (Banatvala and
Zwi 2000).’’
A central tenet of the public health approach to postconflict mental health is that
the structure of intervention is crucially important for ensuring that short-term
mental health interventions are transformed into positive long-term outcomes for
efficacy and institutional development (Baingana and Bannon 2004; Baingana et al.
2005; Inter-Agency Standing Committee (IASC) 2007; Mollica et al. 2004). de Jong
and Komproe explain it best when they state that public, community-based mental
health programs fulfill six crucial functions: (1) they use contextual approaches that
integrate the social worlds of the patients into a locally relevant framework for
managing trauma, (2) they integrate competing academic perspectives on mental
health and social welfare through service delivery structures, (3) they facilitate
interventions that encompass all of the complex determinants of mental illness, (4)
they empower ‘‘natural’’ social support systems already in place at the local level,
(5) they strengthen social cohesion and social capital and (6) they create ‘‘a cascade
Cult Med Psychiatry (2010) 34:353–379 363
123

8/8/2019 Final Open Mole PDF
http://slidepdf.com/reader/full/final-open-mole-pdf 12/27
of training and supervision on different levels.’’ In doing so, de Jong and Komproe
(2002) argue that community-based mental health programs
can train hundreds of professionals and paraprofessionals and thousands of
community leaders in tailored training programmes. Such large-scale buildingof a human-resource capacity allows the community to restore the social fabric
that is disrupted or destroyed by the ongoing cycles of violence in many parts
of the world.
The community-based mental health care model is hypothesized to have greater
sensitivity to local culture, to be more able to demonstrate cultural competency, to
use local outreach more effectively and to emphasize community participation in
the development of healing networks of care. Mollica et al. (2004) argue for the
immediate provision of support for ‘‘de-facto mental health system[-]primary health
care practitioners, traditional healers, and local and international relief workers[who] use culturally validated and scientifically established mental health
interventions throughout the system.’’ This follows a recent move in the global
health literature to regard violence as a public health (vs. a political or sociological)
problem, which might be addressed through public health frameworks of
intervention and treatment (Krug et al. 2002; Pedersen 2002).
Open Mole at Healthworkers International
HI learned about Open Mole during their work on ex-combatant rehabilitation from
2004 to 2005, when local patients began to report the problem in early clinic
encounters. At this time, HI’s expatriate psychologist, the key figure responsible for
training the Psych Team, decided on a dualistic approach to the problem of Open
Mole. Like Wintrob and Hales decades before, she determined that Open Mole was
a psychosomatic displacement onto the body of anxiety, depression and psycho-
logical trauma. The psychologist numerated and catalogued the causes for this
psychosomatic displacement in an internal report to HI officials—sufferers of
mental illness who displaced anxiety, depression and trauma onto their bodies were
somatizing pain as a result of their difficulty mourning the loss of husbands or
children, maltreatment, neglect, domestic violence and economic difficulties, as
well as changes in status. (The case of Garmah (below), a woman who mourned the
death of her husband and bemoaned her economic vulnerability and self-reliance,
poses an excellent model for this narrative interpretation.) According to the
psychologist, Liberians may have believed that they suffered from Open Mole, but
in fact, they were suffering from psychological distress.
The first move in translating the idiom of Open Mole into humanitarian practice
was to isolate Open Mole as a culturally specific idiom of distress that was also an
empty signifier; Open Mole needed to become a disease stripped of ontological
meaning. Toward this end, the psychologist worked actively to train Psych Team
members and local outreach workers in rural communities that Open Mole was a
displacement of something else; that it was a misapprehension of the true cause of
suffering. Open Mole was reduced to an idiom of complaint, rather than an actual
364 Cult Med Psychiatry (2010) 34:353–379
123

8/8/2019 Final Open Mole PDF
http://slidepdf.com/reader/full/final-open-mole-pdf 13/27
complaint with an ontologically valid status that was recognized in the clinical
encounter as a generalized phenomenology of psychosomatic (and possibly
biomedical) experience (in contradiction to the biomedical findings of Poindexter
and the biomedical implications of Wheeler and Kezala).
The second move was to create the lexical pairing of Open Mole with locallyuntranslatable Western psychiatric disorders like depression, anxiety and PTSD—
Open Mole’s comorbid disorders—in HI’s framework. This was accomplished in a
most accidental and well-intentioned way. To integrate cultural awareness and
sensitivity into the mental health framework of the HI Psych Team, an early
decision was made to adopt the Open Mole illness classification into its working
operations. In HI medical records, complaints of Open Mole and diagnoses of
psychiatric distress are reported as follows: Open Mole—with anxiety, Open
Mole—with depression, Open Mole—with schizophrenia and Open Mole—with
psychosis. The diagnosis of Open Mole is made on the basis of the patient’snarrative and is reviewed and reconsidered occasionally in subsequent patient
counseling sessions. Treatment programs involve long-term prescriptions of
antidepressants, antianxiety agents, and antipsychotics including fluoxetine,
amitriptyline, alprazolam and haloperidol. As resources and supply paths are
limited, the Psych Team has few other psychoactive medications available for their
clinical work. This repertoire of medications is called on to satisfy most treatment
needs.
This process of humanitarian translation seems to have emerged as a result of an
epidemiological fallacy of generalization. Because HI’s Psych Team’s patientpopulation worked in overwhelmingly Kpelle and Loma areas, the majority of Open
Mole complaints came from Kpelle and Loma patients, leading HI’s expatriate
leadership to erroneously conclude that Open Mole is an idiom of suffering with
Kpelle and Loma cultural specificity, rather than a somatic complaint with
countrywide presence and relevance. Issues of marginality may have been at stake
as well—of all Open Mole complaints, internal HI reports found that 80 percent of
complainants were women, and 20 percent were men. According to my informants,
women have been more predisposed to Open Mole than men for as long as Open
Mole has existed. As one informant stated, ‘‘Women are weaker than men. They
can’t understand that everyone must die. But men understand this, and that is why
they will not develop Open Mole.’’
What does this mean for a cultural psychiatry of trauma? Open Mole is a puzzle
that is ‘‘good to think with’’ about the intersections of PTSD, idioms of distress and
transcultural psychiatry in postconflict settings. It poses a clear case of a local idiom
of distress that had been appropriated into a clinical setting, resulting in an increase
in rural patients seeking psychiatric treatment, leading to the translation of an
indigenous illness (or idiom of distress) into a biomedical diagnosis requiring
psychopharmaceutical intervention. However, what the local ontology of trauma is
remains unclear. Here, I think it is important to point out that, for there to be a local
ontology, there needs to be some coherence around what constitutes ‘‘the local.’’
The very recent and radical, long-term disruption of the war has disrupted many of
the ways of ‘‘being’’ local in Liberia—it has very much eroded a sense of shared
identity and experience. Consequently, in Liberia, the local ontology of trauma is
Cult Med Psychiatry (2010) 34:353–379 365
123
8/8/2019 Final Open Mole PDF
http://slidepdf.com/reader/full/final-open-mole-pdf 14/27

8/8/2019 Final Open Mole PDF
http://slidepdf.com/reader/full/final-open-mole-pdf 15/27
and a general sense of fear. Symptoms of severe depression such as sadness,
generalized pain, despair and suicidal thoughts ( N = 5–7) seemed to cohere around
the middle of the chart, and patients reported symptoms of psychosis very rarely
( N = 2–3).
However, as HI has engaged with the illness category of Open Mole, the meaning
of open mole has undergone a gradual shift among the populations receiving HI
medical and Psych Team services. Open Mole has lost all practical meaning as an
expression of embodied suffering through its defining symptom, the sunken
fontanelle. Although it was understood elsewhere as a childhood illness, an
Table 2 Frequencies of
symptoms among 40 clinical
cases presenting with the
primary symptom of Open Mole
Symptom No. of cases
Headache 20
Fast heartbeat 20
Insomnia/difficulty sleeping 16
Worriness 15
Loss of appetite/weight loss 13
Nightmares 11
General sense of fear 9
Eyes swinging 8
Weakness 8
Cries a lot 7
Social withdrawal 7
Trembling 7
Neck pain 7
Generalized body pain 7
Confusion/disorientation 6
Sadness 6
Didn’t understand life/what life held
for me/thoughts of ending life
5
Heat in body 5
Flashbacks 4
Fatigue 4Poor memory/forgetfulness 3
Hearing voices 3
Running into the bush 3
Aggressive behavior 2
Chest pain 2
Hallucinations 2
Feeling of insects or worms crawling
in body or head
2
Poor concentration 1Back pain 1
Cult Med Psychiatry (2010) 34:353–379 367
123
8/8/2019 Final Open Mole PDF
http://slidepdf.com/reader/full/final-open-mole-pdf 16/27
aggravated response to bereavement or catastrophic life events or a consequence of
African sign (sorcery), Open Mole has come to be understood at HI as a symbol of
long-term suffering that is the consequence of war-related hardships, deaths, losses
and postconflict worries, vulnerabilities and fears. This seems to be a self-fulfilling
process—after all, the long history and the pervasive violence of the Liberian civilwar have translated directly into the nearly universal presence of traumatic war
histories in patients’ lives and autobiographies. In a process of overdetermined
causal associations, HI patients link their complaints of Open Mole to the deaths of
husbands and children, family conflict, stunted life chances and deaths and illnesses
of sisters and wives. (Some examples of stories heard in initial clinical encounters of
Open Mole complaints are listed in Table 3.) Therefore, at HI, nearly all narratives
of Open Mole are told as histories of trauma. Again, following Kirmayer and Young
(1998), somatized symptoms are reproduced as a Western construction, rather than a
local construction.Open Mole narratives, in their initial rendering, are diverse, unsystematic and
nonlinear. They emphasize the somatic, de-emphasize the patient’s personal history
and freely combine problems as divergent as headaches, backaches, insomnia and
hearing voices into systematic rubrics for diagnosis. A presentation of Open Mole
suffering is fed through an interpretive process yielding the outcome of an
identifiable psychiatric diagnosis and course of treatment. Patients initiate the
clinical encounter with a complaint, then request medication, and Psych Team
members and the clinical questionnaire coach them through the clinical process.
While patients give an account of their symptoms and their narrative, the PsychTeam members jot down notes about the patient’s physical and behavioral
presentation, speech and complaints. Most of the time, family interviews and
medical histories are unavailable. Medication is not prescribed for a period of
3–6 weeks, while HI counselors attempt to counsel patients on a weekly basis
through relationship issues that may be causing them distress. If, at the conclusion of
three clinical interviews, patients’ symptoms have not abated, HI personnel proffer a
diagnosis and begin to prescribe prescription psychiatric medication. Sometimes, HI
psychology assistants are able to avoid prescribing medication altogether and
manage clients’ symptoms through counseling interventions, including family and
marital counseling, referrals to other social support networks and individual therapy.
Of the 40 patients I studied, 9 were diagnosed with Open Mole, undifferentiated
by further diagnosis. Eleven were diagnosed with Open Mole/Anxiety, five were
diagnosed with Open Mole/Depression and five were diagnosed with Open Mole/
PTSD. Five patients were diagnosed simply as ‘‘Severe Depression,’’ one patient
was diagnosed as psychotic and no diagnosis was administered for seven patients.9
In an ideal environment, psychiatric diagnostic procedures would include the
production of an extended psychiatric narrative that included multiple modes of
assessment, an extended case history, family interviews and ongoing observation.
But in practice at HI, the reality of assessment practice involved a relatively brief
9 Figures include four cases of comorbid diagnoses, including two cases of Open Mole with PTSD/Open
Mole with depression, one case of Open Mole with PTSD/Open Mole with anxiety, and one case of Open
Mole with anxiety/Open Mole with depression.
368 Cult Med Psychiatry (2010) 34:353–379
123

8/8/2019 Final Open Mole PDF
http://slidepdf.com/reader/full/final-open-mole-pdf 17/27
interview, a single standardized questionnaire and a framework for ‘‘checking in’’
that was monotonously repeated week after week for drug distributions. In this
grossly simplified process, Open Mole serves an indexical function for the PsychTeam, who must curate from the Open Mole narrative a clinically acceptable
outcome. Open Mole narratives signify variants of psychosis, schizophrenia,
depression, anxiety and PTSD, but the Psych Team must listen to the patient’s
experience narrative to isolate the specific diagnosis of Open Mole that the
interview will generate.
As Table 3 suggests, in diagnoses, process of interpretation and translation can
be ad hoc. From the data collected, there appears to be no direct association between
diagnosis and treatment. A narrative reference to hearing voices or seeing visions
may yield a diagnosis of depression and a treatment protocol of fluoxetine, while awoman who experiences flashbacks of her husband’s murder during the war may be
advised to return for counseling if she is diagnosed with Open Mole/PTSD, or she
may be prescribed a low dosage of haloperidol for her flashbacks, with may be
diagnosed as Open Mole/anxiety. Fluoxetine or alprazolam is routinely prescribed
Table 3 Open Mole narratives and diagnoses
Narrative Diagnosis and treatment
‘‘A’’ heard the story about the brutal butchery of her son
on the Guinean border. She immediately ‘‘went off inher head’’ and ran into the bush, and ever since then
has never been quite right.
Dx: Open Mole/psychosis
Rx: Haloperidol
‘‘B’s’’ Open Mole developed when the war came to her
village in 1991. She heard gunshots. From that point,
she developed Open Mole, manifested by a headache,
she developed many different kinds of forms of
suffering and she’s never been quite right since.
Dx: Open Mole/PTSD
Rx: Counseling
‘‘C’s’’ Open Mole is resulting from a conflict with her
husband in the present. He wants her to leave her
church and join the Seventh Day Adventist Church,
but she prayed and gave devotion at her own churchthroughout the war, and she doesn’t want to leave. He
is making palaver (conflict). She is suffering from a
headache, worriness, fast heartbeat and bad dreams.
Dx: Open Mole/depression
Rx: Fluoxetine
‘‘D’s’’ Open Mole began in 1993, when ULIMO killed
her boyfriend during a raid, while D was pregnant.
Her worriness caused her to have an abortion, and she
treated her Open Mole with traditional remedies.
Dx: Open Mole/anxiety
Rx: Haloperidol
‘‘E’s’’ Open Mole began in 1991, when she saw her
nephew murdered at the crossroads in Salala. Her
sister has died, and her son has lost his mind. She
feels sad, cries and gets confused. She has terriblenightmares of the war.
Dx: Open Mole/anxiety, Open
Mole/depression
Rx: Paroxetine
‘‘F’’ developed Open Mole in 1987 after having a dream
with a series of foreboding portents and symbols.
After that, she began to experience terrible
headaches.
Dx: Open Mole with depression
Rx: Fluoxetine
Cult Med Psychiatry (2010) 34:353–379 369
123

8/8/2019 Final Open Mole PDF
http://slidepdf.com/reader/full/final-open-mole-pdf 18/27
for symptoms associated with depression, and amitriptyline is also used for
depression when alprazolam seems to have little effect. Haloperidol is prescribed
quite often when there are symptoms of possible psychosis, including ‘going off
one’s mind’ or running into the bush, but it also may be prescribed for other
symptoms, including flashbacks, hearing voices, being confused or disoriented,
socially isolating oneself and demonstrating uncontrollable anger. See Table 4 for a
listing of frequencies of medications diagnosed at HI.
Although HI mandates a three-visit waiting period for counseling before the
distribution of medication, most patients are given medication if they return after
three counseling sessions. Once they are put on a medication regimen, counseling
largely disappears from their clinical consultation encounters, and courses of
medication continue indefinitely. As an exponentially increasing number of OpenMole cases create greater time constraints on the already overburdened Psych Team
staff, clinical interview days in some communities have come to resemble refugee
camp ‘‘distributions’’ (of medication, rather than food and goods), rather than
extended opportunities for counseling and ‘talking.’ Under the pressure of time and
patient load, the Psych Team changes diagnoses and issues psychiatric treatments on
an ad hoc basis, in an effort to ‘do something’ to help the sufferer. With persistence,
a patient can wear the Psych Team down into changing a diagnosis of ‘‘Open Mole
with PTSD’’ to a diagnosis of ‘‘Open Mole with anxiety,’’ earning them the
privilege of being medicated.The Psych Team constantly reiterated that the medications HI offers are expected
to ameliorate symptoms, not to act as remedies. Despite this, it was often unclear
(possibly due to a reporting bias created by the clinical context) whether or not
patients understood or believed that their treatment plans are palliatives, not cures.
Nearly 100 percent of the patients who were asked reported to HI Psych Team
members that their symptoms had improved. This was clearly true for psychotic
patients, for some of the patients being treated for severe depression and for some of
the patients being treated for PTSD, but few patients receiving care for Open Mole/
anxiety seemed meaningfully relieved by their courses of medication. Sometimes, Ihad a sense during clinical interviews that minor improvements in appetite or
insomnia were offered as evidence of the patient’s belief in the drug’s efficacy, and
as part of an entreaty for continued treatment. Many patients, however, seemed to be
biding their time for the drugs to ‘‘kick in’’ or ‘‘take effect.’’
Table 4 Frequencies of
medications diagnosed among
40 HI patients
a Due to periodic supply issues,
paroxetine and fluoxetine were
used interchangeably
Medication No. of cases
Haloperidol 9
Counseling 9
Paroxetinea
7
Fluoxetinea 5
None 5
Amitriptyline 3
Cyamezine or diazepam 2
370 Cult Med Psychiatry (2010) 34:353–379
123

8/8/2019 Final Open Mole PDF
http://slidepdf.com/reader/full/final-open-mole-pdf 19/27
The Dialogic of Intervention: Three Case Studies
The locus of interaction between humanitarian organizations and local clients was
the clinical interview, and it was in the context of the ‘‘dialogic’’ (Bakhtin and
Holquist 1981) of the interview that meanings, values and medicines weretransacted. Despite the cultural sensitivity and localization of Open Mole Treatment,
at HI, the meaning, diagnosis, narratives, interpretations and treatments of Open
Mole were all unclear, situationally negotiated and imprecise to local Liberian
patients and to the mental health workers. In the dialogic of the intervention, the
Psych Team was the partner in communication most invested in the shifting of
categories—in managing the switch of Open Mole from culture-bound syndrome to
idiom of trauma. The patients were the partners most invested in obtaining the end
goal of medication, to permanently resolve their symptoms of sufering. In the
context of this dialogic, the relationship between ‘‘talk’’ and ‘‘medicine’’ was oftenconfusing to mental health workers and patients, with the ‘‘talk’’ component of care
leading to contention between patients and workers and the ‘‘medicine’’ component
of care yielding questionable medical outcomes.
But first, let us observe a few typical Open Mole cases. Case 1, Garmah’s case,
illustrates the typical client profile, mode of interventions and trajectory of treatment
frequently found among complainants of Open Mole.
Case 1: Garmah
On a hot day in Liberia’s dry season of 2006–2007, I sat at a round, roughhewn
wooden table in a small, blue-painted clinic room in a northern Liberian county with
three members of HI’s Psych Team. Two female mental health workers were
headed to the market to track down ex-combatants who had participated in the
postconflict rehabilitation program facilitated by the NGO several years earlier. One
male mental health worker headed over to the palaver hut to work on mother and
child attachment issues with women in the local community. I remained in the
breezeless clinic room with the last two mental health workers—a social worker and
a psychiatric nurse—to observe weekly psychiatric clinic consultations. The videoclub shack in the yard outside blasted out the clattering sounds of filmic gunfire
from a Chuck Norris movie.
HI mental health workers received Garmah into their examination room. Garmah
is a sad, quiet, 40-year old widow and mother of nine children (two deceased) who
lived off of a subsistence farm near a local industrial settlement. She is a long-term
patient of HI with a standing diagnosis of Open Mole with PTSD and depression,
and her treatment course had alternated between paroxetine and fluoxetine,
depending on supply availability. Garmah reported her psychiatric narrative thus: In
1990, a traumatic event took place in her presence. Her records reported a traumaticevent: President Samuel Doe killed her husband just before the onset of the conflict.
At this time, she began to experience the symptoms noted in HI’s diagnostic
interview documents: ‘‘worriness,’’ poor vision, severe headaches and weakness in
her neck—all of which culminated in the development of Open Mole. Initially, an
Cult Med Psychiatry (2010) 34:353–379 371
123
8/8/2019 Final Open Mole PDF
http://slidepdf.com/reader/full/final-open-mole-pdf 20/27
herbalist named Kebbe, on Kerry Street in Monrovia, where she had sought refuge
during the war, treated her. Kebbe’s treatment provided some salve, but ultimately
the Open Mole returned, along with Garmah’s constant ‘‘worriness’’ over the death
of her husband, and the persistent realization that, in his absence, no one would help
her support her children in the present or in years to come. She was solely reliant onthe small business that she made from her garden. Garmah had been receiving
psychiatric treatment with HI for over a year, and on the day I met her, she
complained of a severe headache, pain in her neck and a poor appetite. Of particular
relevance to the HI mental health team was Garmah’s reports of severe headaches,
bad dreams, nightmares and ‘‘worriness.’’ Since the beginning of Garmah’s
treatment with fluoxetine, she reported that her nightmares had ceased. Many of her
other symptoms continued to persist. The Psych Team issued her a new supply of
fluoxetine and reminded her of her next scheduled appointment.
Case Study 2: Margaret
Margaret is a tiny, thin, elderly widow with a broad smile and thick, gnarled fingers.
She has three living children, and several children who have died. Margaret started
having signs of open mole during the war, at the time that she lost her oldest son, in
1991. In her own words, ‘‘Open Mole fell on her at the time of the war,’’ and she
‘‘went off and ran into the bush.’’ She was treated with country medicine and
recovered. In 1993, she lost her husband to illness, and her Open Mole returned.
Since then, she has suffered from headaches, heat in the body, fast heartbeat,flashbacks of her son’s death and an ongoing fear of death. She worries a great deal
about her Open Mole, and she is also quite worried about the deaths of her husband
and son. HI diagnosed Margaret with Open Mole, PTSD variety. She has
consistently sought country medicine treatment since 1993, sometimes going to
great lengths to find country medicine specialists, but nothing has worked.
When I met Margaret, she complained of weariness, insomnia, her eyes
swimming, headache, flashbacks and dreams of her late son and husband. After 1
month of observation, her diagnosis was changed to Open Mole with anxiety
features and depression, which made it possible for HI’s psychiatric nurse to start
prescribing medication: She is now on a regimen of 1.25 mg of haloperidol/day—a
standard prescription for Open Mole sufferers with anxiety features.10 Since
treatment, there has been some change, but not much. She continues to have
flashbacks and dreams.
At the time of her clinical interview, John, the psychiatric nurse, was eager to
demonstrate the HI Psych Team’s counseling skills, and illustrate their prioritization
of ‘‘talk therapy’’ over pharmaceutical intervention. For my benefit, he started trying
to counsel her about her psychological symptoms, which surprised Margaret. First,
he asked her, ‘‘Do you have the feeling that you are going to die?’’ ‘‘Yes,’’ she said.
He replied, ‘‘Everyone is going to die.’’ In an aside to me, John interpreted her silent
10 By comparison, in the United States, haloperidol is used to manage symptoms of psychosis,
schizophrenia, hyperactivity, aggression and delirium, but not PTSD, depression or anxiety. In clinical
care in the United States, the typical dosage of haloperidol is 1–5 mg (up to 10 mg) every four to 8 h,
about five to eight times the incredibly low dosage that Margaret is receiving.
372 Cult Med Psychiatry (2010) 34:353–379
123

8/8/2019 Final Open Mole PDF
http://slidepdf.com/reader/full/final-open-mole-pdf 21/27
suffering to mean that this woman, a Methodist, fears that, because her son died an
unnatural death, she will not see him when she dies. She did not seem much
comforted by his counsel, though it was done in exemplary therapeutic tone.
John’s harsh message of, ‘‘Get over it. You need to let it go, forget about it. Stop
crying. Everyone dies. Death is natural’’ was paradoxical: It was delivered in theempathic, low-voiced tone of the Western-trained therapeutic intervention but had a
distinctly nonempathic message. John’s message reveals intense, culturally
embedded expectations surrounding the emotional management of grief and
bereavement. Death in Liberia is—and perhaps always has been—intensely public.
It occupies a large space in the public sphere in funerals, in radio and newspaper
obituaries, with town criers and in mourning activities. Mourning and bereavement,
however, are not allowed to occupy a limitless space in the public domain. Grief,
fear, worry and despair are expected to be carefully managed—and many people,
particularly women, cannot meet these expectations. And it appears as though OpenMole is the consequence. In Margaret’s case, her inability to meet social
expectations of emotional management is now being medicated with a very low
dosage of antipsychotic medication, and she is feeling slightly better. But she is still
afraid of the consequences, for her and for her son, of her son’s unnatural death.
Case Study 3: Nowa
The first client this day sat down quietly at the wooden table, and Florence and Sita
began the paperwork while Nowa presented her case for the second week in a row.She reported that she could not sleep because her heart was racing and reminded the
mental health team that they had prescribed some small green and yellow tablets—
fluoxetine—the week before. She said that she believed that she had Open Mole—
she felt like she was carrying a heavy load all the time, she felt pain throughout her
body and, with her fast heartbeat, she could not sleep at night. Nowa’s friend, who
had accompanied her to the clinic and was seated on a bench outside, had told her
about Open Mole. Since taking the medication, the pain in her body had been
somewhat relieved, but she continued to suffer. The Psych Team told her that they
would review her case after three consultations and suggested that perhaps she did
not need medication. ‘‘Maybe we can just sit and discuss. Maybe you know how it
started. Most people believe in the tablet, but we don’t do that with Open Mole.
Maybe we will just sit and talk.’’ She left the clinic room with a new week’s supply
of fluoxetine, and little talking had transpired. Nowa had failed to activate the
lexical trigger for obtaining Open Mole treatment and was directed to an alternative
course of conflict resolution.
The HI Psych Team had noticed an ever-expanding number of patients
demanding rural-based psychiatric care, and they were having a difficult time
meeting the demand. It seemed that Open Mole was on the move, that it had
acquired a life of its own through its appropriation into HI’s clinical context. To
understand this fact, it is of crucial importance to recognize that HI’s Open Mole
patients believed that the medication being dispensed at HI was for the treatment
and resolution of Open Mole. At HI, Open Mole treatment has been coupled with
other services, including general psychiatric treatment, medical care, ex-combatant
Cult Med Psychiatry (2010) 34:353–379 373
123
8/8/2019 Final Open Mole PDF
http://slidepdf.com/reader/full/final-open-mole-pdf 22/27
outreach, traditional women’s groups and mother–child groups. Through this
extension of services, a kind of social marketing effort, or ‘‘snowball’’ recruitment,
has been under way to bring local communities into the scope of Open Mole
treatment. Unfortunately, the operative marketing message in these recruitment
processes is that HI is giving out medication to heal Open Mole, rather than theintended message: HI can help resolve your suffering through therapy, and we will
use medicine as a temporary measure. This is perilous, because it has created a
situation in which Liberian sufferers of widely prevalent form of psychosomatic
distress are learning help-seeking behaviors that will gain them access to potent
psychiatric medications, in the belief that they will be ‘cured.’ Moreover, some of
these medications have serious side effects, such as haldol’s extrapyramidal side
effects, and there are physical consequences of intermingling different forms of
antidepressant medications.
Garmah, Nowa and Margaret’s case studies point us toward the other half of theintervention dyad: the knowledge, interpretive frameworks and subjectivities of
HI’s Liberian Psych Team members. The Psych Team members are the crucial
lynchpin in the constitution of HI’s Open Mole interventions as community-based,
local and ‘‘culturally relevant.’’ Nearly all HI’s Psych Team members remembered
childhoods filled with Open Mole as a widespread event in their families and
communities. However, in their dual adult statuses as educated Liberians and NGO
workers, they often personally doubted and publicly renounced the legitimacy of
these Open Mole experiences. They overlay their early accounts of Open Mole with
critical commentaries about tradition, superstition and ignorance among Liberians,and their narratives often concluded with a testament to their greater insight and
knowledge as a result of their NGO training and education.
Psych Team ambivalence about Open Mole was bound up with their ambivalent
status as local employees and cultural interlocutors of an international humanitarian
medical organization. Psych Team members were deeply involved with their
postconflict statuses as professional health workers for a prominent international
medical NGO. As health workers, they held salaried positions that gave them
precious middle-class status, stability and respectability in a fraught and unstable
postconflict environment. But their ambivalence toward their work was more than
just the product of social status concerns. The Psych Team members’ postconflict
identities were deeply enmeshed in their own self-perceptions as healers and helpers
(Abramowitz 2010). Their confidence in their work, their skills and their knowledge
sets were bound in complex ways with their individual relationships with past and
present expatriate supervisors. From the expatriate psychologist who founded the
Psych Team, they were intensely trained to ‘see’ the psychological consequences of
war exposure and experiences and have been taught to counsel victims and
perpetrators of violence with sensitivity and care. From their distant supervision by
a European psychiatrist, they have been trained to adhere strictly to the clinical
questionnaire, to interpret physical symptoms through a psychiatric lens and to
situate their observations in a framework of diagnosis and treatment.
However, Psych Team members too believed in the ontological validity of Open
Mole. All of the Psych Team members recounted pre-HI memories, experiences and
knowledge of Open Mole—stories that they narrated timidly in clinical settings but
374 Cult Med Psychiatry (2010) 34:353–379
123

8/8/2019 Final Open Mole PDF
http://slidepdf.com/reader/full/final-open-mole-pdf 23/27
told more vociferously in informal environments. Psych Team members explained
the illness course of Open Mole as follows: ‘‘If they [Open Mole sufferers] run away
from their troubles, the problem will be left behind; but in reality, the problem
would stay. They would just go crazy. Most Open Mole leads to a mental disorder.’’
For the mental health workers, Open Mole is real and makes a causal contribution tomental illness, and patients are being treated with psychiatric medications to avert
full-blown mental illness. This interpretation contrasts strikingly with the intent of
expatriates, who had intended that Open Mole would function as a culturally
sensitive symbolic code for mental illness, which the Psych Team decodes to
provide trauma-related mental health treatment.
Conclusion: Toward a Pidgin Psychiatry?
Psych Team members continue to diagnose, counsel and medicate for Open Mole in
hundreds of clinical encounters, but despite their role in structuring these
encounters, they are unable to significantly alter the course of the intervention by
inserting their community-based , local knowledge into the power-laden process of
the clinical encounter. This fact must force us to fundamentally reconsider what we
mean by ‘‘community-based,’’ ‘‘cultural sensitivity’’ and ‘‘local healing systems.’’
Are healing systems locally relevant simply by virute of inserting local idiomatic
language and employing local staff fluent in local languages? Or does local
relevance require more than the criteria set forth by de Jong and Komproe, relatedearlier in this paper?
Local relevance, to my mind, requires some degree of epidemiological validity
grounded in an ethnographically informed psychiatric epidemiology that is carefully
linked up with an ontology of suffering. But from the humanitarian perspective, the
central office of HI International regarded the Psych Team project as a paragon of
success for its demonstration of cultural relevance and community-based human-
itarian mental health care. It boasted a rural mobile outreach team that brought
clinical psychiatric care into inaccessible communities. Liberian nationals—middle-
class Liberians who spoke local dialects, were trained in psychiatric diagnosis and
treatment, and had social origins in the service area—staffed the program. It was
culturally sensitive—it had integrated a local idiom of distress, ‘‘Open Mole,’’ into
the HI diagnostic framework, and clinical interviews routinely used Open Mole as a
framework for taking case histories and prescribing remedies. Clinical supervision
was available, and the Psych Team was trained to emphasize that ‘‘talk’’ was
preferred to ‘‘medicine’’ in each of their consultations. In addition, the HI Psych
Team conducted outreach services, community education initiatives and client
follow-up to ensure that their services were understood, locally relevant and
effective. On nearly every count, it was a model of postconflict mental health care in
humanitarian intervention.
And so we must ask, Why Open Mole? What work did Open Mole do for HI’s
practice of humanitarian intervention? For HI, Open Mole worked as more than an
idiom of distress. The classification of Open Mole itself has created a space for the
application of modern psychiatric classification systems in rural schema of language
Cult Med Psychiatry (2010) 34:353–379 375
123
8/8/2019 Final Open Mole PDF
http://slidepdf.com/reader/full/final-open-mole-pdf 24/27
and meaning. It functions as a lexical switching point, a sign at the intersection of
systems of meaning in which communications around pain and suffering take on
meaning that is decipherable to the other in the moment of communicative
encounter. What emerges from the clinical encounter around Open Mole is a kind of
‘‘pidgin psychiatry.’’ By pidgin psychiatry, I reference a process of communicationtaking place in the context of an intercultural encounter that is replete with the
fractures and harsh edges of communication. Open Mole is the center of a linguistic
compromise around an encounter meant to manage suffering and healing, across
which multiple forms of social goods, meanings and medicines are transacted.
Open Mole is intrinsically situated in a humanitarian cultural logic in which
‘‘cultural relevance’’ operates more as an ideology than as an outcomes-oriented
approach to clinical intervention. The HI Psych Team members are the unwitting
gatekeepers of this communication and act as cultural mediators between the NGO
and the patients. The next step forward for the medical anthropology of conflictsettings is to examine the linguistic and clinical interactions of internationally
employed ‘‘local healers,’’ to complicate our all-too-routine differentiation of
medical healing systems into ‘‘the global’’ and ‘‘the local.’’ Local employees
constitute the crucial gatekeepers to paradigms of care. An ethnographic study of
their roles, and their subjective interpretations of their labor, can have a great deal of
value for the future of mental health research in postconflict and development
settings.
Myriad forces outside the dialogic of the clinical interview—local medical
histories, NGO mandates and bureaucratic problems with training and supervi-sion—shaped, constrained and limited the clinical encounter around Open Mole
between HI patient and HI staff. In this way, Open Mole had a local history and a
clinical structure that continued to have a life of its own outside the medical
encounter, even as HI attempted to appropriate the local idiom into its system of
medical translation. In this way, Open Mole challenged the best intentions of
policymakers’ and program designers’ efforts to keep mental health local, culturally
sensitive and relevant. On a policy level, transnational comparative survey work can
and should be conducted to assess the efficacy of appropriating local idioms into
systems of medical translation and the feedback impact it has on the quality of
clinical care provided.
Despite the great efforts made toward cultural sensitivity, HI has remained
culturally insensitive to the powerful symbolic meanings and interpretations of ‘‘the
tablet’’ and Western medicine in local populations. In Liberia, there is a widespread
but indiscriminate belief in rural populations that ‘‘the tablet’’ is a cure-all for most
forms of illness. The problem of overmedication, inappropriate medication practices
and abuse of pharmaceuticals is widely known among public health practitioners.
However, HI should be commended for its commitment to providing high-quality
community-based psychiatric and psychological care to needy populations. They are
presently the only NGO in Liberia providing this service and are providing real and
much needed relief to sufferers of debilitating illnesses and diseases. But HI’s
efforts to integrate local idioms of distress into their diagnostic practice, though
noteworthy, have a confusing logic and uncertain consequences for patients and for
376 Cult Med Psychiatry (2010) 34:353–379
123

8/8/2019 Final Open Mole PDF
http://slidepdf.com/reader/full/final-open-mole-pdf 25/27
staff, posing potent questions for the practice of cultural sensitivity and community-
based mental health in postconflict settings.
Research Limitations
During my research at HI, I was strictly limited to a participant-observer role at the
clinic. Because I lacked permission to interrupt the clinical encounter (except on an
ad hoc basis) to collect additional information about the patients’ experiences, or to
administer a standardized questionnaire to investigate patient symptoms, I was
unable to collect standardized data on Open Mole symptoms and illness trajectories.
It has therefore been impossible to apply statistical analysis to my Open Mole
findings. The data presented are therefore to be understood as opportunistic,
nonrandom, and specific to the fieldwork situation. Additionally, due to concernsabout confidentiality, I could not gain permission to conduct external interviews
with HI patients, to obtain interview material regarding their understandings and
interpretations of Open Mole. However, I conducted external interviews with Open
Mole sufferers and Open Mole traditional healers outside of the HI clinical
framework to fill in gaps in qualitative data.
Unlike other papers in this issue, my methods of data collection prohibited an
exhaustive examination of each individual case, and I could not administer
formalized surveys or intervene in clinical interviews. Consequently, I was unable
to assess whether or not cases met DSM-V criteria for PTSD, schizophrenia,depression and anxiety diagnoses. As a result, the public health implications of these
findings remain uncertain.
References
Abramowitz, Sharon Alane
2009 Psychosocial Liberia: Managing Suffering in Post-conflict Life. Cambridge, MA: Harvard
University.
2010 Moral Missionaries: ‘Being’ Traumatized and ‘Doing’ Psychosocial Work in Liberia’s Post-Conflict Reconstruction. In Legacies of Violence: Symptom, Memory, and Intervention in the
Aftermath of Mass Trauma. A. Hinton and D. Hinton, eds.
Baingana, F., I. Bannon, and R. Thomas
2005 Mental Health and Conflicts. Conceptual Framework and Approaches. Health, Nutrition and
Population (HNP) Discussion Paper. Washington, DC: World Bank.
Baingana, Florence, and Ian Bannon
2004 Integrating Mental Health and Psychosocial Interventions into World Bank Lending for Conflict-
Affected Populations: A Toolkit Health Nutrition and Population, Conflict Prevention &
Reconstruction. Washington, DC: World Bank.
Bakhtin, M.M., and Michael Holquist
1981 The Dialogic Imagination: Four Essays. Austin: University of Texas Press.
Banatvala, N., and A.B. Zwi2000 Conflict and Health: Public Health and Humanitarian Interventions: Developing the Evidence
Base. British Medical Journal 321(7253): 101–105.
Bender, D.E., and D. Ewbank
2004 The Focus Group as a Tool for Health Research: Issues in Design and Analysis. Health
Transition Review 4(1): 63–79.
Cult Med Psychiatry (2010) 34:353–379 377
123

8/8/2019 Final Open Mole PDF
http://slidepdf.com/reader/full/final-open-mole-pdf 26/27
Bourdieu, Pierre
1977 Outline of a Theory of Practice. Cambridge: Cambridge University Press.
Bracken, P.J., J.E. Giller, and D. Summerfield
1995 Psychological Responses to War and Atrocity: The Limitations of Current Concepts. Social
Science & Medicine 40(8): 1073–1082.
de Jong, J.T.V.M., and I.H. Komproe2002 Closing the Gap Between Psychiatric Epidemiology and Mental Health in Post-Conflict
Situations. Lancet 359(9320): 1793–1794.
de Jong, J.T.V.M., I.H. Komproe, and M. Van Ommeren
2003 Common Mental Disorders in Postconflict Settings. Lancet 361(9375): 2128–2130.
Desjarlais, R., et al.
1995 World Mental Health: Problems and Priorities in Low-Income Countries. New York: Oxford
University Press.
Drewal, H.J.
1988 Performing the Other: Mami Wata Worship in Africa. TDR 32(2): 160–185.
2008 Mami Wata: Arts for Water Spirits in Africa and its Diasporas: Exhibition Preview. African Arts
4(2): 60–83.
Ellis, Stephen
1999 The Mask of Anarchy: The Destruction of Liberia and the Religious Dimension of an African
Civil War. New York: New York University Press.
Frank, B.
1995 Permitted and Prohibited Wealth: Commodity-Possessing Spirits, Economic Morals, and the
Goddess Mami Wata in West Africa. Ethnology 34(4): 331–346.
Hales, Ann
1996 West African Beliefs about Mental Illness. Perspectives in Psychiatric Care 32(2): 23–29.
Inter-Agency Standing Committee (IASC)
2007 IASC Guidelines on Mental Health and Psychosocial Support in Emergency Settings. Geneva:
IASC.
International Crisis Group2004 Liberia and Sierra Leone: Rebuilding Failed States. In Crisis Group Africa Report. Washington,
DC: International Crisis Group.
International Federation of Red Cross, Red Crescent Societies
2009 Psychosocial Interventions: A Handbook. Copenhagen, Denmark: IFRC.
Kezala, W.S., C.K. Ampadu, and R.J. Macauley
1989 Study of the Knowledge, Attitudes, and Practices of Parents on Open Mole in Children.
Monrovia, LR: Cuttington University College, International Development Research Centre.
Kirmayer, L.J.
1984 Culture, Affect and Somatization. Transcultural Psychiatry 21(159): 159–188.
Kirmayer, Laurence J.M.D., and Allan Young
1998 Culture and Somatization: Clinical, Epidemiological, and Ethnographic Perspectives. Psycho-
somatic Medicine July/August 60(4): 420–430.Kirmayer, Laurence J., Robert Lemelson, and Mark Barad
2008 Understanding Trauma: Integrating Biological, Clinical, and Cultural Perspectives. Cambridge:
Cambridge University Press.
Krug, E.G., et al.
2002 The World Report on Violence and Health. Lancet 360(9339): 1083–1088.
Makanjuola, R.O.A.
1987 Ode Oriı: A Culture-Bound Disorder with Prominent Somatic Features in Yoruba Nigerian
Patients. Acta Psychiatr Scand 75(3): 231–236.
Merry, Sally Engle
2006 Human Rights and Gender Violence: Translating International Law into Local Justice. Chicago:
University of Chicago Press.Mollica, R.F., et al.
2004 Mental Health in Complex Emergencies. Lancet 364(9450): 2058–2067.
Moran, Mary H., and M. Anne Pitcher
2004 The ‘Basket Case’ and the ‘Poster Child’: Explaining the End of Civil Conflicts in Liberia and
Mozambique. Third World Quarterly 25(3): 501–519.
378 Cult Med Psychiatry (2010) 34:353–379
123
8/8/2019 Final Open Mole PDF
http://slidepdf.com/reader/full/final-open-mole-pdf 27/27
Patel, V.
1995 Explanatory Models of Mental Illness in Sub-Saharan Africa. Social Science & Medicine 40(9):
1291–1298.
Pedersen, D.
2002 Political Violence, Ethnic Conflict, and Contemporary Wars: Broad Implications for Health and
Social Well-Being. Social Science & Medicine 55(2): 175–190.Poindexter, H.A.
1953a An Analytical Study of 45,000 Consecutive Admissions to a Clinic in Monrovia, Liberia, West
Africa. Journal of the National Medical Association 45(5): 345–349.
1953b Epidemiological Survey among the Gola Tribe in Liberia. American Journal of Tropical
Medicine and Hygiene 2(1): 30–38.
Prince, R.
1960 The ‘‘Brain Fag’’ Syndrome in Nigerian Students. British Journal of Psychiatry 106(443): 559–
570.
Psychosocial Working Group
2003 Psychosocial Intervention in Complex Emergencies: A Conceptual Framework. Oxford: Refugee
Studies Center.
Renner, Michael, Thomas Prugh, and Worldwatch Institute
2002 The Anatomy of Resource Wars. Washington, DC: Worldwatch Institute.
Reno, William
2004 Reconstructing Peace in Liberia. In Durable Peace: Challenges for Peacebuilding in Africa.
T.M.A. Ali and R.O. Matthews, eds., pp. 115–141. Toronto: University of Toronto Press.
Salama, P, et al.
2004 Lessons Learned from Complex Emergencies Over Past Decade. Lancet 364(9447): 1801–1813.
Sawyer, Amos
2005 Beyond Plunder: Toward Democratic Governance in Liberia. Boulder, CO: Lynne Rienner.
Silove, D., S. Ekblad, and R. Mollica
2000 The Rights of the Severely Mentally Ill in Post-Conflict Societies. Lancet 355(9214): 1548–
1549.Summerfield, Derek
1995 Addressing Human Response to War and Atrocity. In Beyond Trauma: Cultural and Societal
Dynamics. C.F.R. Kleber and B. Gersons, eds. New York: Plenum Books.
Turner, V.W.
1967 The Forest of Symbols: Aspects of Ndembu Ritual. Ithaca, NY: Cornell University Press.
UNMIL
2005 Status of Restoration of State Authority and Recovery in Liberia. C.A. Section: United Nations
Mission in Liberia.
Van Ommeren, M., S. Saxena, and B. Saraceno
2005 Mental and Social Health During and After Acute Emergencies: Emerging Consensus? Bulletin
of the World Health Organization 83: 71–75.
Weiss, M.G., et al.2003 Mental Health in the Aftermath of Disasters: Consensus and Controversy. Journal of Nervous
and Mental Disease 191(9): 611–615.
Wheeler, M.
1975 Travel Notes: A Liberian Medical Experience. Yale Journal of Biology and Medicine 48(5): 439.
Wintrob, R.M.
1968 Sexual Guilt and Culturally Sanctioned Delusions in Liberia, West Africa. American Journal of
Psychiatry 125(1): 89.
Cult Med Psychiatry (2010) 34:353–379 379