fire service consultation medical... · the replies to this consultation will inform the final...
TRANSCRIPT

Draft Medical Guidelines for theFire and Rescue Service:
A consultation document
July 2004


Draft Medical Guidelines for theFire and Rescue Service:
A consultation document
July 2004
July 2004
Office of the Deputy Prime Minister: London

Office of the Deputy Prime MinisterEland HouseBressenden PlaceLondon SW1E 5DUTelephone 020 7944 4400Website: www.odpm.gov.uk
© Queen’s Printer and Controller of Her Majesty’s Stationery Office 2004.
Copyright in the typographical arrangement rests with the Crown.
This publication, excluding logos, may be reproduced free of charge in any format or medium for research, private study or for internalcirculation within an organisation. This is subject to it being reproduced accurately and not used in a misleading context. The material mustbe acknowledged as Crown copyright and the title of the publication specified.
For any other use of this material, please write to HMSO Licensing,St Clements House, 2-16 Colegate, Norwich NR3 1BQ Fax: 01603 723000or e-mail: [email protected]
Further copies of this report are available from:ODPM PublicationsPO Box 236WetherbyWest YorkshireLS23 7NBTel: 0870 1226 236Fax: 0870 1226 237Textphone: 0870 1207 405E-mail: [email protected]
This document is also available on the ODPM website: www.odpm.gov.uk/fire/consult
Printed in the UK on material containing 75% post-consumer waste and 25% ECF pulp (cover),and 100% post-consumer waste (text).
July 2004
Reference No. 04FPD02342

v
Gill McManusHR Modernisation BranchFire and Rescue Service DirectorateOffice of the Deputy Prime MinisterFire Service Effectiveness DivisionZone 16A Portland HouseStag PlaceLondon SW1E 5LP
Direct line: 020 7944 8640Fax: 020 7944 [email protected]
Web site: www.odpm.gov.uk
July 2004
DISABILITY DISCRIMINATION ACT 1995:
CONSULTATION ON DRAFT MEDICAL GUIDELINES FOR THE FIRE ANDRESCUE SERVICE
This consultation document invites your comments on the enclosed draft Fire andRescue Service Occupational Medical Guidelines by 10 September 2004.
1. The Disability Discrimination Act 1995 (DDA) currently exempts firefighting from itsemployment provisions. On 1 October 2004 that exemption will be removed and the Actwill be extended to include the fire and rescue service.
2. In preparation for the legislative change, the Office of the Deputy Prime Minister(ODPM) commissioned Optimal Performance Ltd to conduct research into the medicalcriteria for selection and retention and examine the basis on which medical assessmentsare made.
3. Historically, the approach to determining occupational medical standards within the fireand rescue service has been shaped by the view that candidates must be capable of fittinginto the job, as perceived by service professionals and stakeholders, rather than objectivelyassess how the role could be shaped around the individual.
4. The research project was commissioned to deliver robust, legally defensible guidelinesappropriate to identified roles within the service. The new occupational medical guidancewill assist the medical advisers and occupational health practitioners to guide seniormanagers in reaching informed, evidence-based decisions when considering new applicantsto the service and deciding on the course of action to take when existing staff developmedical conditions which may constitute a disability.

vi
5. As part of the project, consideration has been given to the impact of the requirementsof the DDA on the Firefighters’ Pension Scheme (FPS). At present, the provisions ofFirefighters’ Pension Scheme (FPS) expect all firefighters to be fully capable of engaging infirefighting. However, the FPS is being amended so that whilst access to the Scheme will beopen only to a person recruited to fight fires, continued membership will be available tothose whose roles no longer include operational firefighting and who are no longer fit forsuch duties.
6. From 1 October decisions about recruitment and retention will need to be based far moreon assessment of the individual against a series of guidelines, rather than the current relianceplaced by the fire and rescue service on prescriptive pass/fail criteria. The purpose of the newoccupational medical guidance is to assist the medical advisers and occupational healthpractitioners to guide senior managers in reaching informed, evidence-based decisions.
7. The evidence concerns both the requirements of the various roles within the fire andrescue service (see ‘Job Analysis’ chapter and appendices) and current medical thinking onthe nature of particular medical conditions and their effect on the ability of the individual toperform the role (see Chapters 3-11). Together these two sources of information can be usedto assess the viability of an appointment of a potential employee, or retention of a currentemployee, and the likely extent of adjustments to the role and workplace that may berequired to accommodate the individual concerned.
8. The attached draft guidelines were developed with input from a steering group comprisedof service stakeholders and Disability Rights Commission.
9. Consultees are invited to:
• identify any specific aspects of the guidance about which they have concerns,
• provide any supporting evidence which they consider would be useful, and
• suggest amendments that might improve the document as an assessment tool for itsprimary users (medical advisers and senior managers).
10. A Regulatory Impact Assessment has not been conducted. This is because we believethat the guidelines do not impose new or additional costs on fire and rescue authorities.
11. Comments on the draft guidelines should be submitted to ODPM by 10 September 2004.Our aim is to ensure that the guidance document will be available to all fire and rescueservices before the impending change to legislation takes place. Therefore an eight weekperiod of consultation has been agreed.
12. The consultation document on the draft medical guidelines can be accessed from thewebsite at www.odpm.gov.uk/fire/consult and comments can be sent by e-mail [email protected]

vii
13. Any enquiries about this consultation document should be directed to:
Name: Bernadette Ogunrinde Telephone: 0207 944 6832E-mail: [email protected]: HR Modernisation Branch
Fire Service Effectiveness DivisionFire & Rescue Service DirectorateOffice of the Deputy Prime Minister Zone 16A, Portland HouseStag PlaceLondon SW1E 5LP
14. After the deadline date of 10 September 2004 we will analyse the responses to theconsultation and produce a feedback document within 3 months of the deadline date whichsummarises the:
• received responses and comments;
• any amendments to the draft guidelines as a result of the consultation.
15. The replies to this consultation will inform the final version of the medical guidelines.
16. A list of individuals and organisations who have been invited to comment on the draftguidelines can be found at Annex A attached. However, the list is not exhaustive.
17. Please note that responses, including the names and addresses of respondents, will bemade available to anyone who asks for them unless confidentiality is specifically requested ordisclosure would prejudice third parties.
Gill McManus

Fire and Rescue Service: Draft Medical Guidelines – June 2004
viii
Anglian Polytechnic University
Association of Local Authority MedicalAdvisers (ALAMA)
Avon & Somerset Constabulary
BMI Health Services
British Deaf Association
British Dyslexia Association
Bristol City Council
Business in the Community
Chief Fire Officers’ Association (CFOA)
Chief Executive, County Councils
Clerk to the Fire and Civil DefenceAuthorities
Clerk to the Combined Fire and RescueAuthorities
City of London Police
City University, London
Clinical Science Centre for Research& Education
Commission for Racial Equality
Diabetes UK
Disabled Living Foundation
Disability Information Scotland
Disability Matters Ltd
Disability Rights Commission
Employers’ Forum on Disability
Epilepsy Action
Equal Opportunities Commission
Essex County Council
Fire Brigades' Union
Fire Officers’ Association (FOA)
Fire Service College
Fire Services National Benevolent Fund
Hearing Concern
International Register of Firefighters withDiabetes (UK)
Isle of Wight NHS Trust
Local Government Association
London Fire and Emergency PlanningAuthority
MENCAP
MIND (Mental Health Charity)
Ministry of Defence
National Hospital for Neurology &Neurosurgery
RADAR (Royal Association for Disabilityand Rehabilitation)
Retained Firefighters Union
Royal College of Nursing
Royal National Institute for the Blind
Royal National Institute for the Deaf
Scottish Executive Justice Department
Scottish Fire Service Inspectorate
Shaw Trust
Walton Centre for Neurology andNeurosurgery
Working Fit Ltd
Dr M Baggaley
Mr David Campbell
Dr Tim Carter
Prof David Chadwick
Dr C Chisholm
Dr Stephen Coles
Dr P Cullinan
Mr J K O'Dowd
Mr DS Gartry
Dr Ian Gemmell
Dr G Gill
Air Commodore R T G Merry QHS, FRCP
Dr Susan A Robson (2)
Captain Rintoul RN FRCS
Dr Tony Steele-Perkins
Prof Simon Shorvon
ANNEX A
LIST OF INDIVIDUALS AND ORGANISATIONS WHO HAVE BEEN INVITEDTO COMMENT ON THE DRAFT MEDICAL GUIDELINES FOR RECRUITMENTAND RETENTION IN THE FIRE AND RESCUE SERVICE

ix
The Consultation Criteria
1. The Government has adopted a code of practice on consultations. The criteria belowapply to all UK national public consultations consisting of a document in electronic orprinted form.
I. Consult widely throughout the process, allowing a minimum of 12 weeks forwritten consultation at least once during the development of the policy.
II. Be clear about what your proposals are, who may be affected, what questions arebeing asked and the timescale for responses.
III. Ensure that your consultation is clear, concise and widely accessible.IV. Give feedback regarding the responses received and how the consultation process
influenced the policy.V. Monitor your department’s effectiveness at consultation, including through the use
of a designated consultation co-ordinator.VI. Ensure your consultation follows better regulation best practice, including carrying
out a Regulatory Impact Assessment if appropriate.
2. The code does not have legal force but is regarded as binding on UK departments andtheir agencies unless Ministers conclude that exceptional circumstances requires adeparture from it. The full consultation code may be viewed at:www.cabinet office.gov.uk/regulation/Consultation/Introduction.htm.
3. If you are not satisfied that this consultation has followed the above criteria, or you haveany other observations about ways of improving the consultation process, then pleasecontact:David PlantODPM Consultation Co-ordinatorRoom 3.1926 WhitehallLondonSW1A 2WH; e-mail: [email protected]

x
Draft Medical Guidelines for the Fire andRescue Service: A consultation document
CONTENTS
CHAPTER 1
Introduction and the legal position of fire service medical standards
CHAPTER 2
Job analysis of Fire and Rescue Service roles
CHAPTER 3
Cardiovascular problems
CHAPTER 4
Respiratory problems
CHAPTER 5
Problems with the nervous system and special senses
CHAPTER 6
Mental health problems
CHAPTER 7
Musculoskeletal problems
CHAPTER 8
Endocrine disorders
CHAPTER 9
Gastro-intestinal disorders
CHAPTER 10
Skin problems
CHAPTER 11
The pregnant firefighter

APPENDIX 1
Summary of Results for Firefighters from Occupational Guidelines Questionnaire
APPENDIX 2
Summary of Results for Crew Manager from Occupational Guidelines Questionnaire
APPENDIX 3
Summary of Results for Watch Manager from Occupational Guidelines Questionnaire
APPENDIX 4
Summary of Results for Station Manager from Occupational Guidelines Questionnaire
APPENDIX 5
Summary of Results for Group Manager from Occupational Guidelines Questionnaire
APPENDIX 6
Summary of Results for Area Manager from Occupational Guidelines Questionnaire
APPENDIX 7
Summary of Results for Brigade Manager from Occupational Guidelines Questionnaire
APPENDIX 8
Summary of Results for Control Operator from Occupational Guidelines Questionnaire
APPENDIX 9
Summary of Results for Control Supervisor from Occupational Guidelines Questionnaire
APPENDIX 10
Summary of Results for Control Watch Manager from OccupationalGuidelines Questionnaire

APPENDIX 11
Summary of Results for Control Operations Manager from OccupationalGuidelines Questionnaire
APPENDIX 12
Summary of Results for Fire Safety Officer from Occupational Guidelines Questionnaire
APPENDIX 13
Summary of Results for Fire Safety Manager from Occupational Guidelines Questionnaire
APPENDIX 14
Summary of Results for Fire Safety Advisor/Engineer from OccupationalGuidelines Questionnaire
APPENDIX 15
Summary of Results for Fire Investigator from Occupational Guidelines Questionnaire
APPENDIX 16
Summary of Results for Technical Support from Occupational Guidelines Questionnaire
APPENDIX 17
Summary of Results for Trainer from Occupational Guidelines Questionnaire
APPENDIX 18
Summary of Results for Training Manager from Occupational Guidelines Questionnaire
xii

xiii

CHAPTER 1
Introduction and the legalposition of fire servicemedical standards


CHAPTER 1Introduction and the legal position offire service medical standards
CONTENTS
INTRODUCTION 1-3
JOB ANALYSIS 1-4
PURPOSE OF STANDARDS 1-5
LEGAL BASIS OF STANDARDS AND GUIDANCE 1-6
OTHER RELEVANT LEGISLATION 1-7
Health and Safety at Work etc Act 1974 (HSW Act) 1-7The Management of Health & Safety at Work Regulations 1999 1-9Sex Discrimination Act 1975 1-10Firemen’s Pension Scheme Order (FPSO) 1992 and relevant Case Law 1-11Employment Rights Act (ERA) 1996 1-11Maternity and parental leave etc Regulations 1999 1-11Common law 1-11
THE DISABILITY DISCRIMINATION ACT 1995 1-12
Who decides? 1-12Definition of disability 1-12Direct and indirect discrimination 1-14Conflict with other legislation 1-14Reasonable adjustments 1-14Disability related discrimination 1-15When does the DDA not apply? 1-15
INDIVIDUAL VARIATION 1-16
RISK ASSESSMENT 1-16
TOLERANCE OF SYMPTOMS 1-17
1-1

Fire and Rescue Service: Draft Medical Guidelines – June 2004
1-2
REASONABLE ADJUSTMENTS 1-17
CAN RISK BE ACCEPTED? 1-17
REFERENCES 1-19
ANNEX A
– Summary of legislation applying to Fire Service medical advisers 1-21– Summary of the Fire Service circulars and letters 1-23
AUTHORS:
Dr Ian Gemmell MB ChB MSc MA(Law) MFOM, Consultant OccupationalPhysician, Employment Medical Services Ltd.
Dr Tony Williams MFOM, Consultant Occupational Physician, Working Fit Ltd.
Dr Mark Rayson PhD MA BSc MErg, Consultant Occupational Physiologist,Optimal Performance Ltd., Bristol.

Introduction and the legal position of fire service medical standards
1-3
Introduction
The Fire Services Act of 1947 brought the various local fire services under one commonlegislative basis. A series of regulations have since been issued as statutory instruments, andthese have outlined the requirement for assessment by ‘a duly qualified MedicalPractitioner’. As a Medical Adviser to the Fire Service you are therefore providing adviceto meet a statutory requirement.
This requirement has been very general. The Medical Adviser must be satisfied that ‘theapplicant has not any physical abnormality and is not suffering from any disease thatwould in either case be likely to incapacitate him/her temporarily or permanently for theperformance of the said duties’. A series of specific regulations have been added, andremoved over time, addressing particular medical conditions and physical attributes.Currently there is a requirement to assess grip and back strength, to assess lung function bymeasuring FEV1 and FVC, and to assess general fitness and aerobic capacity as measured bya step test.
Specific medical conditions were first prohibited following the Godber Report of 1968 andfurther medical conditions were added in recommendations by a Joint Working Party in1988. Although few of these recommendations were incorporated into statutoryinstruments, they formed the basis of an expanded series of recommendations produced bythe Association of Local Authority Medical Advisers (ALAMA). This publication,‘Medical Aspects of Fitness for Firefighting’ was never completed, although chapters wereadded through the 1990s and others updated.
These recommendations were straightforward and didactic, addressing a number ofconditions with advice to ‘accept’, ‘accept with caution’, ‘reject’ or ‘retire’. Therecommendations were produced by experienced occupational physicians working inconjunction with expert clinicians in each field and based on available evidence at thetime. Much of the evidence was not referenced in the guidelines.
The extension of the Disability Discrimination Act 1995 to apply to uniformed Servicesincluding the Fire Service from October 2004 has required a new perspective for theALAMA guidelines. A ‘blanket’ view of medical conditions is no longer appropriate; eachindividual applicant or employee must be assessed on their own merit, with an individualrisk assessment of the proposed role being conducted by the Medical Adviser. Theresulting decision based on this advice is specific to the individual and role. While theultimate decision on employment will be for Management, the advice provided by theMedical Adviser will play a key role.
To enable Medical Advisers to conduct an appropriate risk assessment, the Office of theDeputy Prime Minister commissioned a review of the ALAMA guidelines and a high leveljob analysis to identify the work demands of individual roles within the UK Fire andRescue Service. This review has addressed a number of common medical conditions andhas incorporated the current available evidence relevant to employment.
The job analysis (refer to Chapter 2) has identified the importance and frequency ofactivities required of the eighteen identified roles within the Service. This allows MedicalAdvisers to perform an objective assessment of physical and psychological abilities ofindividuals against the requirements of the role. It also allows both Medical Advisers and

Fire and Rescue Service: Draft Medical Guidelines – June 2004
1-4
management to identify any potential adjustments to roles. Management can then meetthe requirements of the Disability Discrimination Act by determining whether theseadjustments are reasonable when set against the common and essential tasks of each role.
Medical Advisers are expected to make individual decisions by combining medicalevidence with the requirements of the role. There are some general guidelines to helpprovide an overall view of the risk associated with these conditions. Specific aspects ofrelevant legislation are outlined below. These all form key aspects of the risk assessmentprocess which is itself enshrined in legislation.
Job analysis
Eighteen discrete roles were suggested by the Integrated Personal Development System(IPDS) within the Service. Following development and piloting, 4000 questionnaires weredistributed to all 58 Services in the United Kingdom. 1057 usable returns were receivedrepresenting a response rate of 26.4%.
Chapter 2 describes the frequency with which the listed activities and tasks are reportedlyperformed by the job incumbents in a typical year for each of the 18 roles, and theimportance attached to being able to fulfil these possible requirements to be effective intheir role. One worked example of the firefighter role is provided in detail. Thecorresponding data for all of the roles are summarised in tables in Appendices 1-18.
The four clusters of roles proposed by IPDS were revisited using statistical techniques toinvestigate for commonality across six ‘activity categories’. These six categories were foundto comprise one ‘physical’ component and one ‘psycho-social’ component. The physicalcomponent included ‘movements performed’, ‘strength tasks’, ‘environments encountered’,and the ‘wearing of SCBA’. The psycho-social component comprised ‘addressing groups’and ‘operational pressure’. These are listed in the table below:
Activity Categories Constituent Activities and Tasks
Movement Sprinting; Running; Jogging; Walking; Climbing stairs; Climbing ladders;Crawling; Jumping; Hammering; Digging
Strength Lifting more than 5kg, 10kg, 20kg, 40kg; Carrying more than 5kg, 10kg,20kg, 40kg; Pushing/pulling more than 5kg, 10kg, 40kg
Environment Fire compartment temperatures above 100oC; Elevated temperatures (30-100oC); Freezing temperatures (sub-zero); Dust; Overcrowding;Open spaces; Height; Enclosed spaces; Total darkness; Partial darkness;Working in water; Working under water; Handling hazardous substances;Smoke; High humidity
Addressing Groups Addressing groups of people
Operational Pressure Dealing with traumatised victims; Dealing with traumatised others (e.g. relatives, public); Making critical decisions quickly
SCBA Using SCBA

Introduction and the legal position of fire service medical standards
1-5
Four revised clusters of roles were formed on the basis of the statistical analysis, referred toas ‘operational’, ‘management/safety’, ‘control’ and ‘trainer’ roles. The revised clusters arelisted below:
Management/ Station ManagerSafety roles Group Manager
Area ManagerBrigade ManagerControl Ops ManagerFire Safety OfficerFire Safety ManagerFire Safety Adv/EngFire InvestigatorTechnical SupportTraining Manager
Operational roles FirefighterCrew ManagerWatch Manager
Control roles Control Operator ControlSupervisor ControlWatch Manager
Training roles Trainer
The requirement for each of the revised clustered roles to perform each of the activitycategories is described in Chapter 2 and is summarised in the table below. The detailunderpinning these high level classifications is provided in Appendices 1-19.
Summary requirement of revised clustered roles:
Purpose of standards
Standards are inevitably prescriptive as they are intended to standardise and ensureuniformity. They also simplify assessment where advisers are not required to have a deepunderstanding of an issue. This, in many circumstances, is an advantage. In thesecircumstances Medical Advisers do not necessarily require extensive training inoccupational medicine, and there can be an assumption that recruiting is safe when risk isminimised. Rather than knowing what they are getting, Management knows exactly whatthey are not getting as recruits, and who should be retired on grounds of ill health.
Management will be primarily concerned with operational efficiency. Firefighters must befit enough to perform their physically demanding job whenever required to do so. Theymust generally be able to withstand rotating shifts and work with periods of intenseactivity punctuated by periods of inactivity. The process of identifying and maintaining anefficient workforce must be cost-effective, and within this is a requirement to ensure thatfirefighters will remain operationally fit for as long as is reasonable to be cost-effective. Inessence, firefighters must start fit, stay fit, and be safe at work. Management must ensurerecruitment and retention is fair and meets all the relevant legislation for employment lawand Health and Safety Law.
Clustered Movement Strength Environment Address Op. SCBARoles Gps Pressure
Operational high high high high very high very high
Managers/Safety low low low very high moderate low
Control none none none moderate high none
Trainers moderate low moderate very high moderate high

Fire and Rescue Service: Draft Medical Guidelines – June 2004
1-6
Physical fitness promotes good health (see Chapter 3) and is protective againstmusculoskeletal injury1 incurred in manual jobs. It is essentially a management issue (but itlinks with the Health & Safety at Work Act), and is defined as a capability requirement tomeet specific job-related standards. These were the subject of a number of projectscommissioned to ensure that standards for selection reflect the requirements of the job(e.g. development and validation of national point of entry selection (PES) tests). MedicalAdvisers must familiarise themselves with these standards as they form part of the medicalrisk assessment.
The main risks for firefighters, and concerns for management, are
injury to the individual or to others
sickness absence
ill-health retirement
While a set of prescriptive standards can minimise the risk of injury and reduce sicknessabsence, it is likely to prevent many individuals from joining who in fact are capable ofworking safely as firefighters with acceptable levels of sickness absence or risk. Prescriptivestandards also lead to excessive ill-health retirement of individuals who remain capable ofworking safely and effectively in some Fire Service roles.
Social and legal policy is moving away from general prescriptive medical standards infavour of individually based assessments:
Risk awareness is increasing in line with a willingness to seek compensationand redress
Employment rights and equal opportunities provisions have expanded, and theDisability Discrimination Act will apply to the Fire and Rescue Service from Oct 2004
Tight budgets and the pressure to strive for optimum efficiency in the public sectorhave led to critical focus on pensions appeals with new, tighter procedures
Old standards are no longer acceptable and a more flexible, intelligent approach toindividual cases is now required.
While all decisions on recruitment, redeployment and retirement are for Management tomake, they need good medical advice. There is an increasing need for an intelligentapproach to interpretation of the effect of the various Fire and Rescue Service roles onhealth, and the effect of the health of employees on these roles.
Legal basis of standards and guidance
Criminal law overrides all other instruments, and therefore Health and Safety issues areparamount. Civil law, including employment law, comes next. Official guidance such asthe Health and Safety Executive Codes of Practice should be followed unless analternative approach is supported by evidence and best practice; however they are notlegally binding, whereas Regulations may be. Standards and guidance lie relatively low inthe order of precedence.

Introduction and the legal position of fire service medical standards
1-7
The medical guidance in this publication represents expert interpretation of availableevidence. Where there is no other official statute or guidance it should form the basis ofdecision-making unless there is an appropriate reason for taking an alternative view. It isimportant to understand that Medical Advisers must not take management decisions.Management guidance published in Fire and Rescue Service Circulars (previously issued asFire Service Circulars and ‘Dear Chief Fire Officer’ or ‘Dear Chief Officer’ letters) shouldtherefore take precedence over this publication, and Medical Advisers must familiarisethemselves with all of these sources of guidance.
Legislation underpins all that Medical Advisers do, and it is therefore essential thatguidelines are evidence based and robust enough to stand up in a court of law. Theirproduction must therefore follow general principles behind modern medical practice.Where evidence is clear and authoritative it should provide the basis for decision making.Where there is limited evidence, then consultation and consensus among practitionersshould be sought. This process must also follow the principles of continuing professionaldevelopment to ensure that the guidance is current, and the practitioner must make everyeffort to stay up to date with new developments that will inevitably be a year or moreahead of published guidance.
It must also be acknowledged that most cases are complex, and require extrapolation fromseveral bodies of evidence. This process can only be done by the practitioner who knowsthe firefighter, understands local issues and can make a decision that balances local Serviceneeds, resources and options with the firefighter’s overall physical and mental capabilities.
The table at Annex A summarises the relevant sources of material relating to legislationavailable at the time of publication. Medical Advisers should ensure they have access to allthese publications.
Other relevant legislation
Medical Advisers will be expected to have an understanding of the law in relation tohealth and employment, including anti-discrimination law. There are a number ofexcellent reference books, guidance notes and codes of practice. Only a very brief overviewis included here.
Health and Safety at Work etc Act 1974 (HSW Act)
The Health and Safety at Work Act 1974 is an enabling Act under which a number ofvery important regulations have been introduced. It is criminal law and so flouting it mayresult in prosecution. It is written in a rather generic manner, however s.2 of the Actstates:
‘It shall be the duty of every employer to ensure, so far as is reasonably practicable, thehealth, safety and welfare at work of all employees.’
This is as prescriptive as the Act gets and this is known as the absolute duty of care.Although the Act is rather generic in its provisions, responsibility remains firmly withthe employer.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
1-8
The Act does not specifically include medical assessment, nor does it require risk to becompletely eliminated – it does require risk to be reduced ‘as far as is reasonablypracticable’, recognising that ‘reasonably practicable’ includes:
‘taking into account the degree of risk balanced against the time, trouble, cost and physicaldifficulty of implementing control measures’2.
This matrix of considerations includes the likelihood of the event occurring and theconsequence of failure.
But what of offers by individuals to waive the employer’s liability? Crucially, the employee’schoice is of secondary importance as the s.2 employer’s liability cannot be waived. Caselaw(Withers v Perry Chain Co Ltd) has often been cited in this respect when the Court ofAppeal held:
‘There was no legal duty on an employer to refuse to employ an adult employee on work hewas willing to do because the employer thought it was not in the employee’s best interests ...If there was a risk, it was for the employee to weigh it against the desirability or necessity ofthe employment.’3
But if such caselaw was allowed to prevail, employers might encourage workers to overlookhealth and safety matters or even ask them to sign statements accepting full liability. Tworecent cases have clarified the position:
In Page v Freight Hire Ltd the Employment Appeals Tribunal held that the matters to beconsidered when determining whether a course of action was justified included theseriousness of the risk being guarded against, the steps reasonably necessary to eliminate it,and, in suitable cases only, the wishes of the employee affected.4
In Coxall v Goodyear5 a tyre fabricator developed occupational asthma. The company andthe individual employee were advised by their occupational physician to change his jobbut no changes to his work were implemented. The manager claimed not to have receivedthe memo and the applicant wished to remain employed in that capacity. Eventually hislung deterioration necessitated ill-health retirement and the company was found to benegligent.
The defence cited Withers in that Mr Coxall had not ‘chased up’ the Management and hadnot pressed for a job change, implying that he accepted the risks of the job. They arguedthe employer had discharged its statutory duty to control the risks of fume exposure and sothey were not liable for the ill health. However, Lord Justice Brown disagreed and held that:
“The principal consideration in determining whether any particular case fell within theWithers principle was the actual nature and extent of the known risk. Cases wouldundoubtedly arise when, despite the employee’s desire to remain at work, notwithstanding hisrecognition of the risk he ran, the employer would nevertheless be under a duty in law todismiss him for his own good so as to protect him.”

Introduction and the legal position of fire service medical standards
1-9
Therefore using the risk matrix of consequence vs. likelihood; if the risk is slight, theWithers principle will apply, but where the consequence is disability or death, it will not.As the Lord Justice Brown put it:
“a lot has happened in 40 years since Withers, not least COSHH (Regs).”
Although in general this is a matter for the employer, a Medical Adviser is expected toassist in risk assessment. For example a Medical Adviser is much better placed to estimatethe onset of symptomatic lung deterioration or the risk of a person with epilepsy collapsingat a critical time.
The Management of Health & Safety at Work Regulations 1999
The ‘Management Regulations’ were first issued in 1992 and were amended significantly in19996. They ‘put meat on the bones’ of the HSW Act and are published as a collection of6 booklets. They explain the employer’s position in relation to the absolute duty providedfor in s.2 and provide guidance on conducting a risk assessment:
Regulation 6 states:
‘Every employer shall ... appoint one or more competent persons to assist him in undertakingthe measures he needs to take to comply with the requirements and prohibitions imposed uponhim by the relevant statutory provision’.
and guidance is given with regard to how to assess competence. In relation to the qualityof the risk assessment and how comprehensive it must be, Regulation 3 gives the generalrequirements:
Every employer shall make a suitable and sufficient assessment of:
the risks to the health and safety of (his) employees whilst they are at work
the risks to the health and safety of persons not in his employment
Every employer shall:
review the risk assessment if there is reason to suspect it is no longer valid or if therehas been a significant change
record the significant findings of the assessment and identify any group of employeesas being especially at risk
and paragraphs 9 and 17 of the Approved Code of Practice (ACOP) provide furtherguidance:
‘Trivial risks can usually be ignored as can risks arising from routine activities – unless thework compounds those risks ... the level of detail in the risk assessment should be broadlyproportionate to the risk.’
As pre-existing health will affect the ability to do the job and may affect the predispositionto subsequent ill health and the possibility of endangering others, the pre-employmentmedical assessment is a critical part of the risk assessment for that particular individual inthe proposed occupation.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
1-10
There are specific health and safety obligations on employers to assess risk where there arewomen of childbearing age at work7. It is a statutory requirement to review the individualrisk assessment for a female employee on learning that she is pregnant – as this represents achange in circumstances as defined under Regulation 6 of the Management Regulations.Failure to conduct a risk assessment is not only a criminal offence under the HSW Act butis also a civil offence under the Sex Discrimination Act 19758. Employers may have toalter working conditions, hours of work or offer suitable alternative work. If none isavailable a suspension on maternity grounds (on full pay) becomes necessary in order toavoid risk to her or the unborn child9.
Sex Discrimination Act 1975
This Act makes it unlawful to treat a person less favourably on grounds of sex, althoughthe European Court extended this to include gender reassignment and sexual orientation10.
Examples of selection criteria which may be discriminatory include minimum heights andrunning speeds that are set at a level which disfavours one group to a disproportionatedegree, if those conditions are not routinely met in the job. If the standards are directlyrelevant to the employment and are routinely met, they are deemed to be justified unlesssimple adjustments can be made.
In addition, it is unlawful under the Sex Discrimination Act to employ unjustifiablepractices which cause detriment to a considerably larger proportion of women than men.Conditions may be justifiable if they are shown to be necessary provided they reflect thetask in hand, but if the detriment is their health, then this is evidence of failure to complywith the requirements of the HSW Act 197411.
Selection tests may be role related ‘gender free’ tests which represent the actual task – suchas the ability to roll out a fire hose, or ‘gender fair’ surrogate tests which requiremeasurement and extrapolation and where standardization across genders would generateerrors – an example is the Chester step test where a 12” step is used for men and a 10” stepis used for women.
The Sex Discrimination Act states that:
‘Nothing ... shall render unlawful any act done by a person in relation to a woman if ... itwas necessary for that person to do it in order to comply with a requirement of a relevantstatutory provision (within the meaning of Part 1 of the HSW Act) and it was done by thatperson for the purpose of the protection of the woman in question.’12
High levels of physical fitness are required among Fire Fighters because of the physicalnature of the role and the protection which underlying fitness gives. This reflects thehealth and safety requirements for the role and so, provided the standards reflect the tasksto be met, they will be lawful.

Introduction and the legal position of fire service medical standards
1-11
Firemen’s Pension Scheme Order (FPSO) 1992 and relevant Case Law
As with any other ill-health retirement scheme, it is the wording of the scheme that isimportant, not what the Medical Adviser feels is morally right. If the firefighter meets therequirements for incapacity defined in the FPSO they are entitled to an ill-healthretirement pension, however this decision is one for Management, based on the advice ofthe Medical Adviser.
There is relevant case law that Medical Advisers should know. A number of these cases,with notes, are listed on the ODPM website13.
Employment Rights Act (ERA) 1996
This enabling Act includes the following rights (covered in detail in subsequentRegulations):
The right not to be unfairly dismissed
The right to maternity leave and other maternity related rights
Maternity and parental leave etc Regulations 1999
These contain the detail of the rights to maternity and parental leave outlined in theEmployment Rights Act 1996 (ERA). They also prescribe the circumstances in which adismissal will be automatically unfair for the purposes of the ERA if the dismissal is for areason related to pregnancy, childbirth, maternity leave, parental leave, or time off fordependants.
Most employees have the right to take up to 4 weeks unpaid parental leave per child(usually <5 yrs) in any one calendar year provided they have given their employer 21 daysnotice and the employer has agreed. They are also entitled to take reasonable periods oftime off work at short notice to deal with an emergency involving a dependant. Thedetermination of what is and what is not reasonable is for Management to determine andadvise the employee accordingly.
Common Law
The English and Scottish legal systems have evolved in such a way that Statutes are passedby Parliament but interpreted by Judges. Common or Case Law is the term given to thesejudgments and such law guides us in everything we do.
The Roben’s Committee brought together much established common law and entwined it intheir recommendations which later became the Health and Safety at Work etc. Act 1974. Byso doing, the common law duty of care was enshrined in law as s.2 of the HSW Act.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
1-12
The principle of common law duty of care in the work place dates back to the late 19thcentury where the standards applied related to reasonable and prudent employers14. Ofinterest however is that employers have an increased duty of care to a worker with a knownpredisposition to illness or injury. For example a one eyed worker deserves greater eyeprotection than a worker with binocular vision, because the consequences of an accidentare magnified15. A similar situation was found in Smith v Leech Brain & Co. Ltd16 where the‘egg-shell skull’ principle was applied. Both these cases have led to the dual approach torisk assessment – the generic risks of the job and the individual characteristics of theemployee.
It is the principle of identifying foreseeable harm and taking steps to prevent theoccurrence which underlies the common law duty of care. Although the principle wasenshrined in the HSW Act, the Act affords no liability under civil law, although asuccessful prosecution under it would assist a civil claim for negligence.
Therefore, the application of medical standards for roles with a significant safety risk is ademonstration of the individual risk assessment being applied. If a disability is discovered,it is for the Medical Adviser to assess the degree of disability and its impact on theindividual and his/her colleagues in normal conditions and under adverse conditions.Having made that assessment, it is for Management to determine the course of action.
The Disability Discrimination Act 1995
Knowledge of the requirements of the Disability Discrimination Act 1995 (DDA) Parts Iand II is a key responsibility for Medical Advisers. The contents of the Act are brieflydiscussed below, but this is intended as a reminder only. Medical Advisers must obtainofficial guidance documentation17.
Who decides?
Part 2 of the DDA contains provisions for ensuring equality of access to employment fordisabled people. Actions against employers are heard predominantly in EmploymentTribunals. Officially, only the Tribunal can interpret the Act and decide which conditionsapply, under what circumstances, what is or is not reasonable adjustment and thereforewhen discrimination has occurred. Medical Advisers play a crucial role in advisingemployers on whether a condition is likely to meet the criteria (set out in Part I of the Act)to be counted as a disability under the Act.
Definition of disability
Disability can be defined in many different ways. The Disability Discrimination Actdefines disability as:
A physical or mental impairment which has an effect on:
his or her ability to carry out normal day-to-day activities.

Introduction and the legal position of fire service medical standards
1-13
That effect must be:
Substantial (that is, more than minor or trivial)
Adverse
Long term (that is, it has lasted or is likely to last for at least a year, or for the rest ofthe person’s life if they are not likely to live longer than a year).
The definition includes mobility and sensory impairment and hidden impairments such asmental health issues, learning disabilities, and conditions that are controlled bymedication but would otherwise be considered disabilities, such as epilepsy or diabetes.
‘Normal’ does not include activities such as sports, or physical requirements of some worksuch as the ability of a policeman to chase a thief, or a postman to walk five miles with aheavy bag, or a musician to play an instrument.
Day-to-day activities are fully explained in the Approved Code of Practice and Guidanceon defining disability. In brief, disability is covered in eight areas:
Mobility – the ability to travel as a passenger in a car or on public transport, walk a shortdistance at a reasonable pace, climb stairs.
Manual Dexterity – using hands and fingers with precision, pick things up, use a standardkeyboard.
Physical Co-ordination – pouring water from kettle to cup, feeding themselves, walkingunaided.
Continence – infrequent loss of bowel control, loss of bladder control asleep once a month,frequent day-time minor faecal or urinary incontinence.
Ability to lift, carry or otherwise move everyday objects – carrying a shopping bag,carrying a tray of cups steadily, moving a chair.
Speech, hearing or eyesight – very slow speech, inability to ask specific questions to clarifyinstructions, inability to hear normal speech in a moderately noisy environment or a voiceon the telephone, failing the standard driving eyesight test, inability to read ordinarynewsprint, total inability to distinguish colours.
Memory or ability to concentrate, learn or understand – any form of epilepsy, inability toremember names of close friends, inability to write a cheque.
Perception of the risk of physical danger – inability to feel very hot or very cold,persistent inability to cross a road safely.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
1-14
Direct and indirect discrimination
This Act makes it unlawful to treat a disabled person less favourably than others for areason which relates solely to their disability. This is called ‘direct discrimination’ andcannot be justified.
Indirect Discrimination relates to circumstances where an employer may treat a disabledperson less favourably because of specific job requirements that may either make ithazardous to that person or others, or that they simply would not be able to achieve. It isessential in these circumstances that the employer has determined that there are nopossible ‘reasonable adjustments’ that can be made. The key issues that might justifydiscrimination are:
‘Standards, criteria, administrative methods, work practices or procedures that adverselyaffect a disabled person’.18
The most common examples are statutory requirements for vehicle licensing andconsiderations under the Health & Safety at Work Act.
Conflict with other legislation
It should not be forgotten that the Health & Safety at Work Act is criminal legislationand therefore the employer’s first duty is to uphold the HSW Act before applyingprinciples of civil legislation. Sometimes this may bring two (or more) Acts into apparentconflict, however the criminal legislation takes precedence and case law supports theprinciple of individual risk assessment in disability cases19. In such cases, if thediscrimination can be so justified, then it is likely to be lawful.
Discrimination can only be justified, for example under Safety legislation, if expresslycovered. For example under the Road Traffic Act 1988 individuals with insulin-dependentdiabetes are not allowed Group 2 licences. Where that specific condition is not expresslycovered, Safety can only be used as justification if the employer can demonstrate that therisk would be too great for that particular individual in that specific employment role. Thisis a narrow definition, and it is for the employer to prove his case on safety grounds ratherthan the employee having to prove discrimination.
The Medical Adviser should provide advice based on clinical findings, supported bycurrent and reasonable medical evidence. It is recommended that the Bolitho20 rather thanBolam21 principle should be followed; it is insufficient to demonstrate just that a reasonablebody of medical opinion supports a view, but this view should also be proved to be logical.Provided the advice is appropriate and the reasoning not irrational, then the decision islikely to be considered reasonable and justified.
Reasonable adjustments
The DDA requires employers to make reasonable adjustments to facilitate the employmentof disabled people. The Medical Adviser can suggest adjustments to be considered in lightof the clinical findings and knowledge of the condition. They may include varying thehours of work, meal times, locations of work, allowing for additional time off for acutesickness or hospital appointments, allowing for slower performance, or providing additionalsupport or equipment.

Introduction and the legal position of fire service medical standards
1-15
Adjustments to equipment are important to consider, such as adaptations tocommunications equipment for those with hearing impairment, or adjustments to clothing,harnesses or personal protective equipment to allow for individual musculoskeletal or skinconditions.
It is for the employer to consider whether the adjustments are reasonable or not – and todefend that decision to a Tribunal if necessary. The onus lies with the employer ratherthan the employee to disprove discrimination. Failure to make reasonable adjustmentscannot be justified except where the employer can demonstrate he was not informed bythe employee that reasonable adjustments were required, or could not reasonably beexpected to know22 23. This places a responsibility on the Medical Advisor to ensure therelevant information is passed to the Service as knowledge by an Occupational Physicianacting on behalf of the Service is deemed to be knowledge by the employer5. It also placesa responsibility on the employer to postpone any adverse decision for a reasonable period oftime whilst awaiting confirmation of a diagnosis or definitive treatment24 25.
Long term changes which affect the number of hours at work or productivity maynecessitate a review of the contract of employment. Adjustments which require specialistequipment may attract grants from charitable concerns or schemes such as Access toWork. Access to Work can pay other costs related to employment besides provision ofspecialist equipment. These should all be considered before cost is consideredunreasonable.
Disability related discrimination
If a disabled employee suffers a penalty for performing less well than a non-disabledemployee because of their disability, it is called ‘disability related discrimination’. If theemployer cannot justify this treatment or has not considered reasonable adjustments toreduce the effects of the disability, on for example productivity, it is discrimination. Anexample in practice could concern the appointment of a clerical officer. One has arthritisand cannot type; the second is trained and able to type. The second applicant isappointed. If typing was crucial to the job then the appointment is justified. If not, directdiscrimination may have occurred.
This can also apply to attendance warnings for excessive sickness absence. Employers areencouraged to consider discounting some or all absences directly related to the specifieddisability before contemplating action26. It is for the employer to determine what level ofleniency would be reasonable for the business.
When does the DDA not apply
Employers may ask a Medical Advisor whether the DDA applies to an individual. It isimportant to distinguish whether the individual’s medical condition meets the threecriteria of long term, substantial impairment of day to day activities. Day to day activitiesare everyday activities including commuting and do not necessarily include work relatedactivities or indeed activities related to that specific form of work. This is to avoid acondition meeting the act’s definition in one job but not in another27.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
1-16
The DDA is unlikely to apply to an individual with arthritis who takes frequent sick leavefor colds and flu as the poor attendance record is unrelated to the disability. The DDA isequally unlikely to apply to an individual who cannot stand in one place for 2 hours –such as at a conveyor belt – because such activity cannot be considered to be a normal dayto day activity.28
In this way, difficulty climbing stairs does meet the DDA criteria for disability butdifficulty climbing a ladder does not because it is not a normal day to day activity – andthere are additional H&S concerns anyway.
Individual variation
Individuals with the same diagnosis may differ considerably in the severity of theircondition and how it affects their day to day lives. Employers frequently ask anOccupational Physician whether a condition ‘is a DDA one’, yet two people with forexample Crohn’s disease, may have different severities of disease so that one suffers littleadverse effect whilst the other suffers a substantial adverse effect. The answer therefore liesin the subjective assessment of the condition’s impact on normal day to day activities.
Motivation, level of education and the degree of family support can lead to very differentpresentations for the same condition. It therefore follows that Medical Advisers willprovide Services with different advice for different individuals with the same condition.This is not as confusing as first thought – the DDA is all about individual assessment.
Risk assessment
The probability of clinical outcome and knowledge of the work and the workplace formthe cornerstones of risk advice by Occupational Physicians. Service Medical Advisors musthave knowledge of Service tasks and be expected to take the lead in providing the medicaladvice in the process of risk assessment. Advice from General Practitioners or indeedhospital specialists with no formal training in occupational medicine has, on occasion,been dismissed by Tribunals as unqualified or inappropriate29. While clinical informationfrom GPs and specialists is essential to the risk assessment process, care should be taken inthe use of reports when these clinicians have also provided advice on capability related toemployment.
Where workplace risk assessment is being applied, Management take the lead on the basisthat they have a greater depth of understanding of the role and the requirements of thejob. Medical Advisers should limit their advice to factors specific to the medical process.
An example of this co-operation may be a firefighter who has a lower back condition andwho has difficulty wearing a BA set for an extended period of time. Management would beexpected to estimate the typical amount of time a firefighter spends wearing a BA set eachtime and the cumulative period over a month and the medical advisor may then commenton whether this would be within the capabilities of the individual or whether it mightaggravate the condition.
Also, current safety practices, such as use of safety harnesses, or working in pairs ratherthan alone, are fundamental to risk assessments. Medical Advisers must avoid makingassumptions about the workplace when assessing risk.

Introduction and the legal position of fire service medical standards
1-17
Tolerance of symptoms
Both symptoms and signs are subjective. Medical Advisors must be careful to ask correctand detailed questions in order to determine the limit of the medical condition. Anunlimited list of symptoms may raise suspicions. Similarly, careful examination and the useof repeatable measures are important in the clinical assessment. Objective measures such asmuscle wasting or loss of spinal reflexes are preferable to subjective reports which may relymore heavily on illness behaviour or secondary gain. However, it is equally important toidentify those with a significant condition but a high ‘pain threshold’.
Reasonable adjustments
Recruiting and retaining individuals with temporary or permanent disabilities or medicalconditions may require Management action. This can either be ‘reasonable adjustments’ toaspects of work or the workplace that either reduce risk or improve capability, orinvestment in treatment and rehabilitation. Circumstances will inevitably differ betweenservices. Shift patterns, balance of work (urban vs. rural etc.) and numbers involved maydiffer significantly, with associated differences in financial support available. It maytherefore be possible to recruit or retain individuals in some Services, or some areas withinone Service, but not in others.
These are decisions for Management; however Medical Advisers may be required to assistin decision making.
Where there is an opportunity to outlay resources on enabling options, Medical Advisersshould consider risk, and advise Management not on the basis of clinical need (which is anissue for the general practitioner and the NHS) but on the basis of likelihood of successfuloutcome. For example privately funded knee arthroscopy may be supported while total hipreplacement may not be supported.
Can Risk be accepted?
Risks cannot always be eliminated, a principle accepted within the Health and Safety atWork Act. Management will need to take a view on an accepted level of residual risk.Medical Advisers will need to be able to express risk in appropriate terms to enableManagement to make decisions on the acceptability of risk. There will also be varyinglevels of acceptability depending on whether the risk is to life, a limited effect on health,or to property. The principles of Withers3 and Coxall5 outlined above should be applied.
Where there is a limited effect, then the financial aspects of risk versus cost of reducing oreliminating the risk will be relevant.
In general, where members of the public or other firefighters are at risk, the level has to bekept as low as possible. If in doubt, the risk levels acceptable for Group 2 drivers in theDVLA guidance are a useful comparator.
Where the risk is solely to the individual themselves, then a higher level of risk is generallyacceptable. In these circumstances there has to be a balance between the risks of an effecton health including ill-health retirement, balanced against the benefits of remaining inwork and the choice of the individual to continue in work and accept the risk.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
1-18
Management cannot devolve the risk to the individual and will always retainresponsibility, but can legally defend acceptance of a higher level of risk where there is anappropriate balance between risk and benefit.
Even more importantly, Medical Advisers must distinguish between risk of ill-healthdeveloping as a result of work versus the risk of ill-health developing at work but notbecause of work. Thus if a person with epilepsy chose to work alone where the sole riskwas the same as the risk they would accept living alone at home, this would be consideredreasonable. If an employee in a sedentary role with advanced coronary artery disease choseto work, with a high risk of a coronary event while at work, this would be acceptableprovided work did not foreseeably precipitate that event.
Finally there is the actuarial risk of reduction in performance, increased sickness absence,or of ill-health unrelated to work that nevertheless precipitates ill-health retirement.Advice of this nature must be clearly separated from advice on risk affecting health andsafety at work or because of work. The DDA applies to such actuarial calculations, when‘reasonable adjustments’ may be applied but blanket rejection from the pension scheme isunlikely to be acceptable.
There are several factors that may be considered:
The cost of sickness absence
The cost of training against loss of performance
The cost of medical support or assessment
The cost of ill-health retirement or injury awards
The opportunities for redeployment
Political pressure to avoid ill-health retirement or reduce sickness absence.

Introduction and the legal position of fire service medical standards
1-19
References
1 Hunt A. Musculoskeletal fitness: the keystone in overall well-being and injuryprevention. Clin Orthop. 2003; Apr; 409: 96–105.
2 Para 23 to A Guide to the Health and Safety at Work etc Act 1974. HSC. ISBN 0 7176 04411.
3 Withers v Perry Chain Co Ltd. [1961]1 All ER 82 CA.
4 Page v Freight Hire (Tank Haulage) Ltd [1981] ICR 299 EAT.
5 Coxall v Goodyear [2002] EWCA Civ 1010; [2002] TLR 335 CA.
6 Para 17 to Management of Health & Safety at Work Regulations SI 1999 No. 3242. ISBN 0717624889.
7 European Directive on Pregnant Workers (SI No. 2865), Council Directive 92/85/EEC.
8 Hardman v Mallon (T/A Orchard Lodge Nursing Home) [2002] IRLR 517 EAT.
9 Employment Rights Act 1996. ss.66-68.
10 Grant v South West Trains (Case C-249/96) [1998] IRLR 206, ECJ.
11 Gemmell IMM. ‘Injuries amongst female army recruits: a conflict of legislation’ J R Soc Med 2002; 95: 23–7.
12 The Sex Discrimination Act 1975. s 51(1c)(ii).
13 www.odpm.gov.uk.
14 Smith v Baker & Sons [1891] AC 325 HL.
15 Paris v Stepney Borough Council [1951] AC 367, [1951] All Er 81 HL.
16 Smith v Leech Brain & Co. Ltd. [1961] 3 AER 1159; [1962] 2 QB 405.
17 Approved Codes of Practice for the Disability Discrimination Act, available through theDisability Rights Commission and online at www.drc-gb.org: Guidance on matters to betaken into account in determining questions relating to the definition of disability.HMSO 1996.
18 HC Deb Standing Committee E, col 142.
19 Jones v The Post Office. [2001] IRLR 384 CA.
20 Bolitho v City & Hackney Health Authority [1997] 4 All ER 771.
21 Bolam v Friern Hospital Management Committee [1957] 1 WLR 582.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
1-20
22 Disability Discrimination Act 1995 s.6(6).
23 O’Neill v Symm & Co Ltd [1998] IRLR 233, EAT.
24 Baynton v Saurus General Engineers Ltd [1999] IRLR 604, EAT.
25 HJ Heinz v Kenrick [2000] ICR 491, EAT.
26 Clark v TDG Ltd t/a Novacold [1999] IRLR 318 CA.
27 Abadeh v British Telecommunications PLC [2001] IRLR 23, EAT.
28 Cook v Kitchen Range Foods Ltd [1957] 1501064/97, IT.
29 Holmes v Whittingham & Porter Ltd [1997] 1802799/97, IT.

Annex A to Chapter 1
1-21
Summary of legislation applying to Fire Servicemedical advisers
Common Law Duty of Care
Fire Services Act 1947 as amended 1959
Health and Safety at Work etc. Act 1974
Sex Discrimination Act 1975
Disability Discrimination Act 1995
Employment Rights Act 1996
Fire Service (Appointments & Promotion) Regulations & Amendments
Statutory Instrument No 436 1978
Statutory Instrument No 2235 1988
Statutory Instrument No 959 1997
Management of Health and Safety at Work Regulations 1999
Maternal and Parental Leave etc. Regulations 1999
Firemen's Pension Scheme Order 1992 (SI 1992/129)As amended by:
The Firemen’s Pensions (Provision of Information Regulations) 1997 (SI 1997/1829)
The Firemen’s Pension Scheme (Amendment) Order 1997 (SI 1997/2309)
The Firemen’s Pension Scheme (Amendment No 2) Order 1997 (SI 1997/2851)
The Firemen’s Pension Scheme (Amendment) Order 1998 (SI 1998/1010)
The Firemen’s Pension Scheme (Pension Sharing) Order 2001 (SI 2001/3691)
Godber Report, endorsed by FSC 41/70
1988 Joint Working Party Report, endorsed by FSC 1/89
Fire Service Circulars and DCFO Letters:
FSC 8/1991 Step Test
DCOL 3/1995 Visual Standards and Diabetics
DCFO 2/1996 Chester Step Test
FSC 9/1996 Visual Standards
DCOL 9/1996 Age Limit
FSC 5/1997 Height requirements for Fire Service recruitment
DCFO 8/1997 Fitness and strength recruitment tests

Fire and Rescue Service: Draft Medical Guidelines – June 2004
1-22

Annex A to Chapter 1
1-23
Summary of the Fire Service circulars and letters
The recommendations of the Godber Report and the Joint Working Party (JWP) reporthave been largely superseded by more recent guidance. The 1988 JWP recommended useof the step test with a minimum VO2 max of 45 ml/kg/min or greater.
Fire Service Circular 8/1991 recommended introduction of occupational health schemesfor Fire Brigades.
Dear Chief Fire Officer Letter 3/1995 allowed serving firefighters to wear glasses in order tomeet acuity standards and allowed optometrists as well as ophthalmologists to conducteyesight tests on recruits. It also removed the operational bar on the employment ofinsulin-dependent diabetics for firefighting.
Dear Chief Fire Officer Letter 2/1996 recommended the use of the Chester step test multi-stage protocol instead of the Fire Service step test single stage protocol.
Fire Service Circular 9/1996 confirms most of the recommendations of the City Universityreport on visual acuity and colour vision. The visual standards were thus revised inrecommendations (rather than statute) from the Central Fire Brigades Advisory Councils.
Dear Chief Officer Letter 9/1996 removed the upper age limit for recruitment to whole-time service while retaining the aerobic fitness standard required.
Fire Service Circular 5/1997 removed the height requirements for Fire Service recruitment.
Dear Chief Officer Letter 8/1997 confirms the standards for grip and leg & back strength,and the use of the Chester step test.
Fire Services (Appointment and Promotion) Regulations 1997 remain current as the latestlegislative standards. They require:
• minimum grip and back strengths, ie dominant hand 35kg, subordinate hand 33kg;back pull test 117 kg.
• the assessment of ability to undertake firefighting duties by a duly qualified medicalpractitioner, including assessment of:
– lung function by the measurement of FEV1 and FVC;
– an assessment of general fitness level, including aerobic capacity as measured by astep test.
• that a duly qualified medical practitioner must be satisfied that the applicant does nothave any physical abnormality and is not suffering from any disease that would ineither case be likely to incapacitate him/her temporarily or permanently for theperformance of their duties.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
1-24

CHAPTER 2
Job analysis of Fire and RescueService roles


CHAPTER 2Job analysis of Fire and RescueService roles
CONTENTS
INTRODUCTION 2-3
OBJECTIVES AND APPROACH 2-3
THE QUESTIONNAIRE 2-4
STATISTICAL ANALYSIS 2-6
RESULTS 2-8
OVERVIEW OF REQUIREMENTS OF REVISED ROLE CLUSTERS 2-23
SUMMARY AND CONCLUDING REMARKS 2-26
AUTHOR
Dr Mark Rayson PhD MA BSc MErg, Occupational Physiologist, OptimalPerformance Ltd., Bristol.
2-1

2-2

Job analysis of Fire and Rescue Service roles
2-3
Introduction
The roles and responsibilities of the UK Fire and Rescue Service and the personnel whoserve the Service are changing dramatically. These changes were highlighted by the BainReview1 published at the end of 2002 and by the government’s White Paper entitled OurFire and Rescue Service in June 20032. The White Paper announced a whole raft ofchanges based upon risk assessment and management, ranging from the refocusing of theService on fire prevention to the explicit targeting of resources to combat the risks topublic safety from both natural and terrorist-related incidents.
Essential to the process of individual risk assessment is the requirement to have objectiveinformation on the physical and psychological demands of the various roles within theService. In the context of assessing fitness for employment, core objectives of the DDA areindividual and competent assessments, full consideration of enabling options and the needfor any discrimination to be justified by management.
This chapter summarises the findings from a high-level job analysis conducted to supportthe interpretation and implementation of the revised Medical Guidelines. The intention isthat this chapter and the supporting appendices be used as a resource manual for MedicalAdvisers and Management to improve their understanding of the occupationalrequirements of given roles within the UK Fire and Rescue Service and to inform theirrecommendations and decision making.
Objectives and Approach
Objectives
The aim of this chapter is to provide an evidence base of the core requirements associatedwith specified roles in the UK Fire and Rescue Service. This database can be used byMedical Advisers and by Management to assist decision making regarding reasonableadjustments that might be made to accommodate the needs of personnel protected by theDDA, and ultimately whether to retain or release from employment individuals who areno longer able to perform their role safely or adequately.
Approach
Early discussions with the Integrated Personal Development System (IPDS) group at theFire Service College (FSC) lead to the consolidation of 18 discrete roles within the UKFire and Rescue Service. These roles summarised in Table 1, which were provisionallyendorsed by ODPM, fell within 4 clusters comprising Operational roles on the fire-ground,Management roles, Fire Control and Fire Safety roles. All results in this chapter arepresented for these 18 individual roles. However, the clustering of roles was re-evaluatedand revised clusters were formed.
1 Bain (2002). The Bain Review.
2 TSO (2003). Our Fire and Rescue Service Cm 5808.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2-4
Table 1: Draft IPDS role clusters
Management/ Station Managerroles Group Manager
Area ManagerBrigade ManagerControl Watch ManagerControl Ops ManagerFire Safety ManagerTechnical SupportTraining Manager
Operational roles FirefighterCrew ManagerWatch ManagerFire InvestigatorTrainer
Control roles Control OperatorControl Supervisor
Fire Safety roles Fire Safety OfficerFire Safety Advisor/Eng
The Questionnaire
The IPDS group also helped with the drafting and piloting of the questionnaire in twoways. First, they were able to identify potential core requirements of the various roles. Thisinformation was used to supplement an established job analysis questionnaire used byOptimal Performance Ltd (OPL) with other employment groups. Second, IPDS conveneda series of evening workshops at the FSC which served to pilot the draft questionnaire andto discuss additions and refinements to the draft version. The result was the OccupationalGuidelines Questionnaire shown at Appendix 19.
This questionnaire was despatched via the ODPM with a cover letter by OPL on 4 December2003 to all Services. Human Resource Managers were identified as the most suitable pointof contact within Services and named HR Managers were targeted. Approximately 70questionnaires were sent to each Service. The HR Manager was asked to select randomlypersonnel from each role, distribute the questionnaires to those individuals, and collate theresponses within the fortnight. The questionnaires were completed and returnedanonymously. HR Managers were asked to collate the responses and despatch them toOPL. The timeline for responses being tight, combined with the intervening Christmasperiod, resulted in the deadline for responses being extended to 9 January 2004.
The 4-page questionnaire shown at Appendix 19 contains only 13 questions, thoughquestions 6 to 13 contained up to 35 items, each of which required a response. Questions 1to 5 provide basic demographic data which serve both to describe the population sampledand identify to which role respondents belonged. Categorical data were preferred by theODPM to these demographic questions to help protect the identity of respondents. Forexample, age categories were selected rather than asking respondents their age directly;and similarly for years of service. The remaining Questions 6 to 13 also involvedcategorical responses; for example respondents indicated how many times they performedcertain activities in a typical year, with response options ranging from ‘not at all’ to ‘manytimes per day’. Further detail of each question is provided below.
Question 6 enquired how frequently respondents performed certain activities in a typicalyear. Respondents were asked to focus on their Fire & Rescue Service duties and to excludeactivities performed during training or leisure time. The activities were subdivided into:
• Movements (sprinting, running, jogging, walking, climbing stairs, climbing ladders,crawling, jumping, hammering, digging)
• Strength tasks (lifting, carrying, pushing/pulling more than 5, 10, 20 and 40 kg)

Job analysis of Fire and Rescue Service roles
2-5
• Static postures (standing, sitting, squatting, kneeling)
• Dynamic flexibility requirements (bending at waist, reaching, stooping,turning/twisting)
• Object activities (catching, throwing, fine dexterity such as writing and mousecontrol, assembling equipment, and foot control such as driving).
Question 7 repeated all of the activities listed at Question 6 and asked respondents toindicate how important performance of these activities was to the effective performance oftheir role. Possible answers ranged from ‘critical’ to ‘unimportant’, with ‘not applicable’ asa further option.
Questions 8 and 9 asked similar questions to Questions 6 and 7 respectively – howfrequently respondents performed additional activities in a typical year and how critical orimportant they considered performance of these tasks to be. The same options for answerswere available as for Questions 6 and 7. These questions focussed on:
• Tasks (handling hoses, handling unconscious casualties, handling ladders, operatingcutting equipment, driving vehicles, climbing ladders, dealing with traumatisedvictims, dealing with traumatised others, addressing groups of people, filling in formsor completing paperwork, making critical decisions quickly, dealing with the media,working on a computer, communicating over the telephone)
• Environments encountered (fire compartment temperatures >100oC, elevatedtemperatures (30-100oC), freezing temperatures, dust, overcrowding, open spaces,height, enclosed spaces, total darkness, partial darkness, working in water, workingunder water, handling hazardous substances, smoke, high humidity)
• Equipment used (fire protective Personal Protective Equipment, Self ContainedBreathing Apparatus, Extended Duration Breathing Apparatus, vibrating equipment,computer, telephone, hand-held radio).
Question 10 enquired about Near Vision Tasks required for role – 41 vision tasks werelisted and respondents indicated if these tasks were a requirement for their role. Question11 asked about Distance Vision Tasks – 22 tasks were listed. Many of the Near andDistance Vision Tasks were taken from the Visual Task Analysis performed by CityUniversity3. Other tasks were added following the pilot work and the discussion groupsconvened at the FSC. A full list of these vision tasks may be found at Questions 10 and 11of the questionnaire shown at Appendix 19.
Question 12 listed 13 Hearing Tasks (distress signal unit, warning whistle, radio, fireground orders, evacuation signals/alarms, telephone, traffic, vibraphone, pager, normalverbal communication with and without background noise, hand clapping, cries of help)and asked respondents to indicate whether they were a requirement of their role. Question13 asked about the relevance of other senses to performance of the role, including touch,smell and taste.
3 Aids to Vision of the Fireground. Final Report by Fireground Vision Research Unit, Department ofOptometry and Visual Science, City University, London, 1 May 1996.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2-6
Statistical Analysis
Due to the nature of the data (i.e. categorical rather than continuous) and its volume (thenumber of items, the number of roles and the number of questionnaires returned), we haveelected to provide summary data in this chapter using the following statistical techniques:
• the number of responses (N)
• the median response (a measure of central location; the value that half the responsesfall above and half below)
• the mode or modal response (the most frequently occurring response)
• frequency distributions (the percentage of the sample that provides a given response).
We have also elected to provide diagrams and commentary supporting the data for onesingle role only (that of Firefighter), with the data for all roles provided in summary tablesin the Appendices. The activities associated with the revised clusters of roles are alsodescribed in the section entitled Overview of Requirements of revised Role Clusters. TheContents page lists where these data may be found. For example, the responses fromControl Operators may be found at Appendix 8, while those of Fire Investigators arelocated at Appendix 15. The expectation on the part of the likely users of this report (HRManagers, Medical Advisers) is that the straightforward nature of these descriptive data inthe Appendices will be readily understandable once an example has been provided.
In order to confirm and/or improve the four clusters of roles proposed by IPDS sixcategories of activities were selected for further analysis. These categories of activities weretermed Movement, Strength, Environment, Addressing Groups, Operational Pressure, andSCBA. The components of each of these categories are provided in Table 2.
Scores for each category of activity for each of the 18 roles were calculated from theresponses to the questions about frequency and importance of the relevant tasks andactivities. The tasks were scored on frequency by six possible categories of response from‘not at all’ (scored as 0), increasing by increments of one, to ‘many times per day’ (scoredas 5). The tasks were scored on importance, from ‘not applicable’ (0) to ‘critical’ (5). Thefrequency and importance scores were then multiplied to produce an overall score for eachActivity Category ranging from 0 to 25, known as the Activity Category Score.
A cluster analysis was then performed. The purpose of a cluster analysis is to classify (inour case) Fire and Rescue Service roles into relatively homogeneous groups assuming thegroups are initially not known. The procedure uses an agglomerative hierarchical methodthat begins with all observations (roles) being separate, each forming its own cluster. Inthe first step, the two observations closest together are joined. In the next step, either athird observation joins the first two or two other observations join together into a differentcluster (based on the Euclidean Distance least squares). This process continues until allclusters are joined into one. It is for the expert to decide how many groups are logical forthat particular data set.

Job analysis of Fire and Rescue Service roles
2-7
An exploratory factor analysis was also conducted to investigate the dimensionality of thesix Activity Categories.
Scope and Limitations
This study set out to conduct a high-level job analysis via questionnaire to identify the corerequirements associated with each role defined by IPDS. It encompassed seeking theopinions of job incumbents about their own roles only. For some roles the number ofresponses was small and caution is advised in drawing conclusions where the number ofresponses was less than 20, as was the case in 3 of the 18 roles.
To cluster and draw high-level conclusions about the requirements of the various rolessome sub-sections of the data have been used selectively, in agreement with representativesfrom the Steering Group. For example, indices of movement, material handling andoperational pressure were used together with 3 other Activity Categories as they weredeemed to be the most appropriate. Use of alternative sub-sections of data, for exampleabout hearing and vision, may have lead to different clusters.
A key component of the DDA is the requirement for individual assessment of individuals,both of their potential disability and the role they are required to perform. To use thisevidence base effectively and appropriately, the reader should refer to the detailed analysesof data presented in the appendices and not rely solely on the summary data presented inthe main sections of this chapter.
Table 2: Activity Categories and their constituent questions
Activity Categories Constituent Activities and Tasks
Movement Sprinting, Running, Jogging, Walking, Climbing stairs, Climbing ladders,Crawling, Jumping, Hammering, Digging
Strength Lifting more than 5kg, 10kg, 20kg, 40kg Carrying more than 5kg, 10kg,20kg, 40kg Pushing/pulling more than 5kg, 10kg, 40kg
Environment Fire compartment temperatures above 100˚C, Elevated temperatures (30-100oC), Freezing temperatures (sub-zero), Dust, Overcrowding, Openspaces, Height, Enclosed spaces, Total darkness, Partial darkness,Working in water, Working under water, Handling hazardous substances,Smoke, High humidity
Addressing Groups Addressing groups of people
Operational Pressure Dealing with traumatised victims, Dealing with traumatised others (e.g.relatives, public), Making critical decisions quickly
SCBA Using Self Contained Breathing Apparatus

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2-8
Results
Overall Response Rate
From 4000 questionnaires that were issued, 1122 were returned by 9 January 2004providing a response rate of 28.05%. 1057 of the 1122 were usable: 65 were ‘spoiled’ by therespondents indicating more than 1 role on question 1 thereby preventing the inclusion oftheir data. Responses were received from all 58 Services.
Response by Role
Table 3 summarises the age and number of years served, the ratio of male to female andfulltime to retained, and the number of responses received per role.
Overall (shown in the bottom row) the median age of the sample was 40-49 years and themedian ‘years of experience’ was 20-24 years. 80% of respondents were male, 20% werefemale. 98% were fulltime; the remaining 2% were retained.
As might be anticipated the more junior roles within each cluster of roles tended to beboth younger and have less years of service compared to the more senior roles. Mendominated most roles and clusters of roles, except for the Control Roles where womendominated. The majority of respondents to all roles were fulltime. Crew Manager was theonly role to have more than 10% retained.
Table 3: Description of respondents
Role Median Median Male: Fulltime: Numberage years of female retained
service
Firefighter 30-39 0-4 95:5% 96:4% 129
Crew Manager 30-39 10-14 96:4% 89:11% 73
Watch Manager 30-49 15-19 99:1% 92:8% 80
Station Manager 40-49 20-24 98:2% 98:2% 92
Group Manager 40-49 25+ 100:0% 100:0% 105
Area Manager 40-49 25+ 100:0% 100:0% 77
Brigade Manager 40-49 25+ 100:0% 100:0% 58
Control Operator 30-39 0-4 10:90% 99:1% 84
Control Supervisor 40-49 15-19 17:83% 100:0% 64
Control Watch Manager 40-49 25+ 27:73% 100:0% 82
Control Operations Manager 40-49 25+ 39:61% 96:4% 28
Fire Safety Officer 40-49 25+ 98:2% 100:0% 63
Fire Safety Manager 40-49 25+ 97:3% 100:0% 29
Fire Safety Advisor/Engineer 40-49 25+ 100:0% 100:0% 6
Fire Investigator 40-49 20+ 100:0% 100:0% 10
Technical Support 40-49 25+ 89:11% 100:0% 19
Trainer 30-39 10-14 97:3% 100:0% 36
Training Manager 40-49 15-19 100:0% 100:0% 22
Overall 40-49 20-24 80:20% 98:2% 1,057

Job analysis of Fire and Rescue Service roles
2-9
Firefighter Role: a worked example
DemographicsThere were 129 responses on the Firefighter role. 95% of respondents were male; 5% werefemale. 96% were fulltime; 4% were retained.
The age distribution of the sample of Firefighters is shown in Figure 1. The most frequently(modal) reported age category was 30-39 years (40%), followed by 20-29 years (33%), 40-49 years (22%), and 50+ (5%). None was less than 20 years.
Years of service are shown in Figure 2. The most frequently reported category was 0-4 years(39%), then 5-9 years (22%), 10-14 and 25+ years (12%), 15-19 years (8%) and 20-24years (7%). The median category was 5-9 years.
Figure 2: Years of Service of Firefighter sample
Figure 1: Age distribution of Firefighter sample
0
5
10
15
20
25
30
35
40
45
Age category
freq
uen
cy (
%)
20-2918-19 30-39 40-49 50+
0
5
10
15
20
25
30
35
40
45
Years of service
freq
uen
cy (
%)
5-90-4 10-14 15-19 20-24 25+

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2-10
Frequency of Activities performed Figure 3 shows the frequency response to the first part of Question 6 regarding Movementsperformed in a typical year. It shows little consistency or consensus of response to many ofthe movements. For example, while ~25% of firefighters report that they Sprint once perweek on average, another 20% report that they never Sprint. Walking and Climbing stairsare exceptions where the overwhelming majority of Firefighters report performing themovement ‘many times per day’. ‘Once per month’ is the modal and median response toCrawling, Jumping, Hammering and Digging.
Figure 4 shows the frequency response to Strength tasks performed in a typical year, wherethe loads Lifted (L), Carried (C), Pushed/Pulled (P) are indicated. The modal response forLoads greater than 5 kg and 10 kg lifted, carried, pushed/pulled is ‘many times per day’.Handling loads of greater than 20 kg is most frequently reported as occurring ‘once perday’, while handling loads of greater than 40 kg is reported most frequently occurring ‘onceper week’. A wide range of responses is again reported to any given strength task.
Figure 4: Frequency response of Firefighters to Material Handling Tasks
Figure 3: Frequency response of Firefighters to Movements performed
0
10
Sprint Run Jog Walk ClimbStairs
ClimbLadder
Crawl Jump Hammer Dig
20
30
40
50
60
70
80
90
100
not at all once per year once per month once per week once per day many times per day
freq
uen
cy (
%)
0
10
20
30
40
50
60
70
not at all once per year once per month once per week once per day many times per day
freq
uen
cy (
%)
L>5K
G
L>10
KG
L>20
KG
L>40
KG
C>5KG
C>10KG
C>20KG
C>40KG
P>5K
G
P>10
KG
P>20
KG
P>40
KG

Job analysis of Fire and Rescue Service roles
2-11
Figure 5 shows the frequency responses to the remaining activities listed at Question 6,including static postures, dynamic flexibility requirements and catching activities. The majorityof Firefighters indicated that they stand, sit, bend, reach, stoop, turn, use fine dexterity and footcontrol ‘many times per day’. Squatting and kneeling are typically reported either ‘once perday’ or ‘many times per day’; while lying, catching and throwing show a more varied response.
Figure 6 shows the responses to the first part of Question 8 concerning the frequency withwhich Firefighters perform a variety of operational tasks. There is a huge range of responsesto almost all questions, ranging from the majority indicating that they use the telephone‘many times per day’ to the majority indicating that they never deal with the media. Thetasks that are reported as being performed most frequently include using the telephone,driving a vehicle and handling hoses, with around 40-50% of Firefighters indicating thesetasks are performed ‘many times per day’. By contrast, handling unconscious casualties,dealing with traumatised victims, traumatised others, addressing groups and dealing withthe media are reported as being typically performed ‘once per month’ or less.
Figure 6: Frequency response of Firefighters to Operational Tasks
Figure 5: Frequency response of Firefighters to Static Postures, Dynamic
Flexibility Requirements and Object Activities
0
10
stand sit squat kneel lie bend reach stoop turn catch throw finedexterity
footcontrol
20
30
40
50
60
70
80
90
100
not at all once per year once per month once per week once per day many times per day
freq
uen
cy (
%)
0
60
50
40
30
20
10
hand
le ho
se
hand
le ca
sualt
y
hand
le lad
der
cut e
quip
drive
vehic
le
climb l
adde
r
traum
a vict
im
traum
a oth
ers
addr
ess g
roup
s
pape
rwor
k
make d
ecisio
ns
deal
with m
edia
opera
te PC
use p
hone
not at all once per year once per month once per week once per day many times per day
freq
uen
cy (
%)

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2-12
Figure 7 shows the frequency response to various environments encountered during thecourse of the Firefighters’ Service duties. Typically, Firefighters report being exposed to manyof the environments ‘once per month’ – these include temperatures above 100˚C, between30 and 100˚C, dust, overcrowding, open space, enclosed space, total darkness, smoke andhigh humidity. Less frequent exposures are reported for sub-zero temperatures, working inwater and handling hazardous substances. Working under water appears to be rare, with 75%indicating that they are never exposed to this environment. Working at height and workingin partial darkness have intermediate responses, typically ‘once per week’ or ‘once per day’.
Figure 8 indicates the frequency with which Firefighters report using the listed items ofequipment. The majority of Firefighters indicated that PPE (Personal ProtectiveEquipment), the telephone and hand-held radio are used ‘many times per day’. While useof SDBA (Standard Duration Breathing Apparatus) varies between once per month forsome and many times per day for others, EDBA (Extended Duration Breathing Apparatus)is not used at all by the majority. The frequency of use of vibrating equipment varieswidely. Computers are used by the majority at least ‘once per day’.
Figure 8: Frequency response of Firefighters to equipment used
Figure 7: Frequency response of Firefighters to Environments encountered
0
80
70
60
50
40
30
20
10
>100
deg C
30-1
00 de
g C
<0 de
g C dust
overc
rowdin
g
open
spac
e
heigh
t
encl
spac
e
total
dark
parti
al da
rk
in wate
r
unde
r wate
r
HAZMAT
smok
e
humidi
ty
not at all once per year once per month once per week once per day many times per day
freq
uen
cy (
%)
0SCBAPPE vibrating
equipmentEDBA PC phone radio
80
70
60
50
40
30
20
10
not at all once per year once per month once per week once per day many times per day
freq
uen
cy (
%)

Job analysis of Fire and Rescue Service roles
2-13
Near VisionFigure 9 shows the frequency of the dichotomous response (‘yes’ or ‘no’ as a requirementfor role) of Firefighters to the list of 41 Near Vision Tasks with which they were presented.These tasks are shown by number in the questionnaire at Appendix 19. A detailed visualtask analysis has been conducted on many of these items and the visual acuity required toperform them has been previously reported (City University, 1996). The visual standardsrequired to perform these tasks may therefore be determined by cross reference to the CityUniversity Report.
Affirmative response rates to these 41 questions varied between 33% and 91%. Thehighest affirmative responses were to generic items of equipment such as reading the clockon the BA Control Board, the turnout sheet and maps. Unsurprisingly, the visionrequirements that were least frequently reported were to brand-specific items of equipment,such as reading the BA graduations and the needle position on the Siebe Gorman SCBA.Clearly many Services do not own this brand of equipment. That is not to say that thegeneric task is not a requirement of the role.
Distance VisionFigure 10 indicates the extent to which the 22 Distance Vision Tasks presented (seeAppendix 19 for a listing) are perceived as a requirement for the Firefighter role.Affirmative responses varied between 54% and 93%, with the highest response to readingstreet names (black letters on a white background), road traffic signs (Stop, Give Way,One Way), chemical warning signs, vehicle lights, and fire safety and exit signs. Clearly,the majority of Firefighters considered all of the tasks listed to be a requirement for role.As for the Near Vision Tasks the vision requirements of many of these Distance VisionTasks may be found in the City University Report (1996).
Figure 9: Near Vision Tasks reported by Firefighters as a role requirement
Yes No
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 410
10
20
30
40
50
60
70
80
90
100
freq
uen
cy (
%)

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2-14
HearingFigure 11 indicates the degree to which the listed Hearing Tasks were perceived to beimportant by Firefighters. Affirmative response rates ranged from 56% to 95% – themajority of Firefighters thereby deeming all of the Hearing Tasks listed to be a requirementfor their role. Response rates were 90% and higher for all tasks except for the vibraphone(57%), pager (56%) and hand clapping (86%). Clearly, use of a vibraphone and pager isnot ubiquitous.
Figure 11: Hearing Tasks reported by Firefighters as a role requirement
Figure 10: Distance Vision Tasks reported by Firefighters as a role requirement
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 220
10
20
30
40
50
60
70
80
90
100
freq
uen
cy (
%)
Yes No
0
10
20
30
40
50
60
70
80
90
100
freq
uen
cy (
%)
Yes No
DSU
g whis
tlerad
io
nd or
ders
ac si
gnals
telep
hone
traffi
c
brap
hone
page
r
ms no b
gn
with bg
n
d clapp
ing
es of
help

Job analysis of Fire and Rescue Service roles
2-15
Other SensesFigure 12 shows Firefighters’ responses to the three other senses listed (touch, smell, taste).The overwhelming majority considered touch and smell to be a requirement, while amarginal majority (53%) considering taste to be.
Importance of Activities performed Figure 13 shows the respondents’ ratings regarding the importance of performing the listedmovements (listed at Question 6 and 7 on the questionnaire at Appendix 19) to theeffective performance of their role. The modal response to Sprinting, Running and Joggingwas ‘important’ (as was the median response except to Jogging which was ‘veryimportant’), though a similar number felt these movements were more (i.e. ‘critical’ or‘very important’) and less (‘not very important’, ‘unimportant’) important. Walking andClimbing stairs and ladders were seen as ‘critical’ by the majority of respondents. Theability to Crawl was also rated as ‘important’ or higher by the majority. By contrast,Jumping, Hammering and Digging received a more varied rating, with between 15 and30% of respondents indicating that these movements were ‘not very important’ through to‘critical’. In all three activities the median response was ‘important’.
Figure 12: Other Senses reported by Firefighters as a role requirement
0
10
20
touch smell taste
30
40
50
60
70
80
90
100
freq
uen
cy (
%)
Yes No

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2-16
Figure 14 indicates the perceived importance attributed to Lifting, Carrying, Pushing/Pullingobjects among Firefighters. The modal response to all forms of Material Handlingirrespective of load handled was ‘critical’, with a somewhat diminishing response to greaterloads. The median response to all these items was either ‘critical’ or ‘very important’. Evenwith the heaviest loads (> 40 kg) only 15% or less of Firefighters regarded the activity asless than ‘important’. Clearly, Material Handling is seen as a frequent and very importantor critical aspect of the role for the majority of Firefighters.
Figure 14: Degree of importance attributed to Material Handling activities
Figure 13: Degree of importance attributed to ability to perform Movements
0
10
20
30
40
50
60
70
freq
uen
cy (
%)
critical very important important not very important unimportant not applicable
Sprint Run Jog Walk ClimbStairs
ClimbLadder
Crawl Jump Hammer Dig
0
60
50
40
30
20
10
freq
uen
cy (
%)
critical very important important not very important unimportant not applicable
L>5K
G
L>10
KG
L>20
KG
L>40
KG
C>5KG
C>10KG
C>20KG
C>40KG
P>5K
G
P>10
KG
P>20
KG
P>40
KG

Job analysis of Fire and Rescue Service roles
2-17
Figure 15 shows the perceived importance attributed to static postures, dynamic flexibilityrequirements and object activities. The modal response to all activities except Catchingwas ‘critical’, though the median response to the majority was ‘very important’. Less than25% of Firefighters considered any of these tasks to be less than ‘important’ – i.e. 75%considered all activities listed as ‘important’, ‘very important’ or ‘critical’.
Figure 16 shows the Firefighters’ perceived importance of being capable of performing thesame series of tasks previously shown in Figure 6. The majority felt that it was ‘critical’ totheir role to handle hoses, handle unconscious casualties, handle ladders, operate cuttingequipment, drive a vehicle, climb ladders, deal with traumatised victims and others, andmake critical decisions quickly. Of the remaining tasks, the modal and median responsewas ‘important’. It appears that all of these tasks are perceived to be ‘important’ or ‘critical’to the majority of Firefighters.
Figure 16: Degree of importance attributed to the ability to perform operational
tasks
Figure 15: Degree of importance attributed to Static Postures, Dynamic
Flexibility Requirements and Object Activities
0
60
50
40
30
20
10
freq
uen
cy (
%)
critical very important important not very important unimportant not applicable
stand sit squat kneel lie bend reach stoop turn catch throw finedexterity
footcontrol
0
80
70
60
50
40
30
20
10
freq
uen
cy (
%)
hand
le ho
se
hand
le ca
sualt
y
hand
le lad
der
cut e
quip
drive
vehic
le
climb l
adde
r
traum
a vict
im
traum
a oth
ers
addr
ess g
roup
s
pape
rwor
k
make d
ecisio
ns
deal
with m
edia
opera
te PC
use p
hone
critical very important important not very important unimportant not applicable

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2-18
Figure 17 indicates the Firefighters’ perceived importance of being able to operate in thevarious Environments described previously in Figure 7. The modal response to allenvironments listed was ‘critical’. The median response to many environments was also‘critical’, though to some environments was ‘very important’, and to one environment(operating under water) was ‘important’. The ability to operate under water received theleast positive response, but even here, 33% gave a ‘critical’ rating – the modal response.
Figure 18 displays the importance which Firefighters attach to their ability to operate listeditems of equipment; the frequency response to these items being used having beendisplayed in Figure 8. The overwhelming majority regarded their ability to operate in fire-protective PPE and use SCBA as being ‘critical’. ‘Critical’ was also the modal response tothe ability to use EDBA, vibrating equipment and a hand-held radio (the medianresponses being ‘very important’ for the fist two items and ‘critical’ for the third), with 40-50% of respondents selecting this category. Opinion was divided about the importanceof using a computer, though approximately 76% indicated it to be ‘important’ or higher.
Figure 18: Degree of importance attributed to being able to operate various
items of equipment
Figure 17: Degree of importance attributed to the ability to perform operational
tasks
0
10
20
30
40
50
60
70
freq
uen
cy (
%)
critical very important important not very important unimportant not applicable
>100
deg C
30-1
00 de
g C
<0 de
g C dust
overc
rowdin
g
open
spac
e
heigh
t
encl
spac
e
total
dark
parti
al da
rk
in wate
r
unde
r wate
r
HAZMAT
smok
e
humidi
ty
0SCBAPPE vibrating
equipmentEDBA PC phone radio
90
80
70
60
50
40
30
20
10
freq
uen
cy (
%)
critical very important important not very important unimportant not applicable

Job analysis of Fire and Rescue Service roles
2-19
Revisions to the clusters of rolesAs illustrated in Table 2 in the section entitled Statistical Analysis, six Activity Categorieswere formed (Movement, Strength, Environment, Addressing Groups, OperationalPressure, and wearing SCBA) and these were used as the basis for conducting a clusteranalysis to verify if the clusters proposed by IPDS were optimal4. The steps performed inthe cluster analysis (which are not displayed in this report) show that a range of clusters (5 to 3) are good candidates for the final partition. Closer investigation of the ActivityCategory Scores suggests that having four clusters makes intuitive sense, as indicated inTable 4.
Table 4: Revised clustering of roles
Management/ Station ManagerSafety roles Group Manager
Area ManagerBrigade ManagerControl Ops ManagerFire Safety OfficerFire Safety ManagerFire Safety Adv/EngFire InvestigatorTechnical SupportTraining Manager
Operational roles FirefighterCrew ManagerWatch Manager
Control roles Control OperatorControl Supervisor ControlWatch Manager
Training roles Trainer
Six bargraphs showing the Activity Category scores for each role are shown on thefollowing pages. The roles are shown in rank order on the x-axis and the vertical bars arecolour-coded indicating the cluster to which they belong. The y-axis shows the ActivityCategory score achieved, ranging from 0 (not at all important and/or never performed) to25 (critical and performed many times per day).
4 An exploratory factor analysis was also conducted to investigate the dimensionality of the six ActivityCategories. The analysis suggested a two-factor solution. Component 1, with the weighting shown inparentheses, included Environment (0.99), Strength (0.98), SCBA (0.98) and Movement (0.98).Component 2 included Addressing Groups (0.90) and Operational Pressure (-0.73). This resultsuggests that the 6 Activity Categories do not reflect independent themes (or principle components)but they would better be interpreted as having two separate dimensions or themes. The first factorwas primarily ‘Physical’ with all components positively related. The second factor was primarily‘Psycho-Social’, but these were inversely related to each other.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2-20
Figure 20: Activity Category Strength
Figure 19: Activity Category Movement
0
2
4
6
8
10
12
14
16
18
20
Operational
Managers
Controllers
Trainer
Task
Sco
re
Ff CMW
M Tr Fl SM GM TM AM TS FSA
FSO BM FS
M CSCW
MCOM CO
Fire Service Role
Movement
0
2
4
6
8
10
12
14
16
18
20
Operational
Managers
Controllers
Trainer
Task
Sco
re
Ff CMW
MTr FlSM GM TM AMTS FSA
FSOBM FS
M CSCW
MCOM CO
Fire Service Role
Strength

Annex A to Chapter 1
2-21
Figure 22: Activity Category Addressing Groups
Figure 21: Activity Category Environment
0
2
4
6
8
10
12
14
16
18
20
Operational
Managers
Controllers
Trainer
Task
Sco
re
Ff CMW
MTr Fl SM GM TM AM TSFSA
FSO BMFS
M CSCW
MCOM CO
Fire Service Role
Environment
0
2
4
6
8
10
12
14
16
18
20
Operational
Managers
Controllers
Trainer
Task
Sco
re
Ff CMW
M Tr Fl SM GM TM AM TS FSA
FSO BM FS
M CSCW
MCOM CO
Fire Service Role
Addressing Groups

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2-22
Figure 24: Activity Category SCBA
Figure 23: Activity Category Operational Pressure
0
2
4
6
8
10
12
14
16
18
20
Operational
Managers
Controllers
Trainer
Task
Sco
re
FfCMW
M TrFlSM GM TMAM TSFSA
FSOBM FS
MCSCW
MCOMCO
Fire Service Role
Operational Pressure
0
2
4
6
8
10
12
14
16
18
20
Operational
Managers
Controllers
Trainer
Task
Sco
re
Ff CMW
MTr FlSM GMTM AM TS FSA
FSOBM FS
M CSCW
MCOMCO
Fire Service Role
SCBA

Job analysis of Fire and Rescue Service roles
2-23
Overview of Requirements of revised Role Clusters
Introduction
The following four subsections provide a high-level overview of the job requirements ofeach of the four revised clusters – Operational, Management/Safety, Control and Trainerroles. Mean scores for the clusters are provided for each of the Activity Categories(Movement, Strength, Environment, Addressing Groups, Operational Pressure andSCBA), where theoretical scores range from 0 indicating either the activity is neverperformed or has no importance to the role requirement, to 25 indicating the activity isperformed many times per day and is critical to the role requirement. In reality, ActivityCategory scores range from 0 (e.g. SCBA worn by Control roles) to 18.8 (e.g. AddressGroups by Trainers). The mean Activity Category scores by cluster are shown in Table 5;these are further described in the text.
Operational RolesThere are three roles in this cluster – Firefighter, Crew Manager and Watch Manager.These Operational roles are characterised by scoring the highest of any cluster of roles on5 of the 6 Activity Categories, namely Movement (mean score 10), Strength (12),Environment (8), Operational Pressure (12) and SCBA (14). For Addressing Groups theyscore moderately (10), relative to the other clusters of roles. With one exception, the 3Operational roles clustered well on the Activity Categories; the exception being thatFirefighters scored considerably lower on Addressing Groups than Crew Managers andWatch Managers.
On average, the roles reported they performed each of the movements listed (e.g. running,climbing ladders) once per week and they considered these movements to be important forthe effective performance of their role. The strength tasks (lifting, carrying) were typicallyeach performed once per week and were considered to be very important for the effectiveperformance of their role. On average they encountered each of the Environments listed(e.g. extreme temperatures, darkness, water) once per month and regarded being able tooperate in these environments as very important. They Addressed Groups and encounteredeach aspect of Operational Pressure (e.g. dealing with traumatised victims) once per weekand regarded being able to cope with these aspects as being very important. SCBA wastypically worn once per week and was deemed critical to effective performance.
Table 5: Mean Activity Category scores by Role cluster
Clustered Movement Strength Environment Address Op. SCBARoles Gps Pressure
Operational 9.7 11.6 8.0 10.1 12.1 13.7
Managers/Safety 3.0 2.4 2.0 12.3 6.4 1.9
Control 0.7 0.1 0.0 5.6 10.1 0.0
Trainers 6.0 11.0 7.1 18.8 5.8 11.4

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2-24
In order to be effective, respondents in these Operational roles reported having tocomplete many of the Near Vision Tasks (e.g. reading the BA Control Board, pressuregauge numbers), Distance Vision Tasks (e.g. reading house numbers, road signs), HearingTasks (e.g. hearing the radio, warning whistle), and use their senses of touch, smelland taste.
Management & Safety RolesThere are eleven roles in this cluster – Station Manager, Group Manager, Area Manager,Brigade Manager, Control Operations Manager, Fire Safety Officer, Fire Safety Manager,Fire Safety Advisor / Engineer, Fire Investigator, Technical Support and Training Manager.These Management and Safety roles are characterised by scoring relatively high inAddressing Groups (mean score 12), moderate on Operational Pressure (6), andmoderately low relative to their counterparts in other role clusters on Movement (2),Strength (2), Environment (2), and SCBA (2). The 11 Management and Safety rolesclustered reasonably well on all Activity Categories.
On average, the Managers and Safety roles reported they performed each of themovements (e.g. running, climbing ladders) and strength tasks listed (lifting, carrying) andencountered the Environments listed (e.g. extreme temperatures, darkness, water) once peryear and they considered these movements to be not very important for the effectiveperformance of their role. They wore SCBA less than once per year but regarded thecapability to do so as important for their role. They Addressed Groups once per week,regarding this as a very important role requirement. They encountered aspects ofOperational Pressure (e.g. dealing with traumatised victims) once per month and regardedbeing able to cope with these aspects as important.
In order to be effective, respondents in these Management and Safety roles reportedhaving to complete a number of the Near Vision Tasks (e.g. reading the BA ControlBoard, pressure gauge numbers), and many of the Distance Vision Tasks (e.g. reading housenumbers, road signs), though this did not hold true for the Control Operations Managerwho had to achieve few of the Near and Distance Vision tasks. Hearing Tasks (e.g. hearingthe radio, warning whistle) and tasks involving use of touch, smell and taste were requiredto a moderate degree by the majority of roles within this cluster, though markedly less sofor the Control Operations Manager, whose sensory requirements were more akin to theControl cluster.
Control RolesThere are three roles in this cluster – Control Operator, Control Supervisor and ControlWatch Manager. These Control roles are characterised by scoring moderately high onOperational Pressure (mean score 10), moderately low on Addressing Groups (6) and verylow on the four Physical Activity Categories, namely Movement (1), Strength (0),Environment (0), and SCBA (0). The 3 Control roles clustered well on all ActivityCategories.
On average, the roles reported they performed each of the movements listed (e.g. running,climbing ladders) once per year and they considered these movements to be unimportant forthe effective performance of their role. The strength tasks (lifting, carrying), theEnvironments listed (e.g. extreme temperatures, darkness, water) and the wearing ofSCBA were typically not performed or encountered at all and were considered to be notapplicable to the effective performance of their role. They Addressed Groups on averageonce per month and considered this activity to be important for their role. Typically theyencountered each aspect of Operational Pressure (e.g. dealing with traumatised victims)once per week and regarded being able to cope with this aspect as important.

Job analysis of Fire and Rescue Service roles
2-25
In order to be effective, respondents in these Control roles reported having to completefew of the Near Vision Tasks, though a small majority reported the need to see a computermonitor and read general paperwork and maps. Similarly, a requirement to perform any ofthe Far Vision Tasks was reported infrequently. Of the Hearing Tasks the majority reportedthe need to hear the radio, telephone and verbal communication with and withoutbackground noise. The requirement to use their senses of touch, smell and taste was leastamong the clustered roles.
Training RoleThere is only one role in this cluster – Trainer. The Trainer role is characterised by scoringthe highest of any cluster of roles on Addressing Groups (19), having a high requirementfor Strength (11), SCBA (11) and Environments (7), and a moderate requirement forMovement (6) and Operational Pressure (6).
On average, the Trainers reported they performed each of the movements listed (e.g.running, climbing ladders) once per month and they considered these movements to beimportant for the effective performance of their role. The strength tasks (lifting, carrying)were typically each performed once per week and were considered to be very important foreffective role performance. On average they encountered each of the Environments listed(e.g. extreme temperatures, darkness, water) once per month and regarded being able tooperate in these environments as important. They Addressed Groups many times per day andsaw this requirement as very important. They encountered Operational Pressure (e.g.dealing with traumatised victims) once per month and regarded being able to cope withthese aspects as important. SCBA was typically worn once per week and was deemed veryimportant to effective performance.
In order to be effective, the Trainers reported having to complete many of the Near VisionTasks (e.g. reading the BA Control Board, pressure gauge numbers), Distance Vision Tasks(e.g. reading house numbers, road signs), Hearing Tasks (e.g. hearing the radio, warningwhistle), and use their senses of touch, smell and taste.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2-26
Summary and Concluding Remarks
This chapter contains the findings from a high-level Job Analysis conducted byquestionnaire in support of the ODPM project to revise Medical Guidelines for bothrecruitment and retention within the UK Fire and Rescue Service in light of removal of theService’s exemption of uniformed roles to the Disability Discrimination Act 1995, from 1October 2004. Its aim is to provide an evidence base for Medical Advisors and Managementwhich they may use as a source of information to judge an individual employee’s suitabilityfor role and to estimate the implications of making reasonable adjustment.
Eighteen discrete roles were identified by IPDS within the Service. Following developmentand piloting, 4000 questionnaires were distributed to all 58 Services in the UnitedKingdom. 1057 usable returns were received representing a response rate of 26.4%.
For each of the 18 roles, the frequency with which the listed activities and tasks arereportedly performed by the job incumbents in a typical year, and the importance attachedto being able to fulfil these possible requirements to be effective in their role are reported.One worked example of the Firefighter role is provided in detail. The corresponding datafor all of the roles are summarised in tables in the Appendices.
The four clusters of roles proposed by IPDS were revisited using statistical techniques toinvestigate for commonality across six Activity Categories. These six categories were foundto comprise one ‘Physical’ component and one ‘Psycho-Social’ component. The Physicalcomponent included Movements performed, Strength tasks, Environments Encountered,and the wearing of SCBA. The Psycho-Social component comprised Addressing Groupsand Operational Pressure.
Four revised clusters of roles were formed, referred to as Operational, Management/Safety,Control and Trainer roles. The clusters are listed below in Table 6.
Table 6: Revised clusters of UK Fire and Rescue Service roles
Management/ Station ManagerSafety roles Group Manager
Area ManagerBrigade ManagerControl Ops ManagerFire Safety OfficerFire Safety ManagerFire Safety Adv/EngFire InvestigatorTechnical SupportTraining Manager
Operational roles FirefighterCrew ManagerWatch Manager
Control roles Control OperatorControl Supervisor ControlWatch Manager
Trainer roles Trainer

Job analysis of Fire and Rescue Service roles
2-27
The requirement for each of the revised clustered roles to perform each of the ActivityCategories has been described in the text and is summarised in Table 7. The detailunderpinning these high level classifications are provided in the Appendices to this report.We anticipate that these detailed data will need to be accessed by both Medical Advisorsand Management to inform their decision making.
Table 7: Summary requirement of revised clustered roles
Clustered Movement Strength Environment Address Op. SCBARoles Gps Pressure
Operational high high high high very high very high
Managers/Safety low low low very high moderate low
Control none none none moderate high none
Trainers moderate low moderate very high moderate high

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2-28

CHAPTER 3
Cardiovascular problems


CHAPTER 3Cardiovascular Problems
CONTENTS
INTRODUCTION 3-3
CARDIAC RHYTHMS 3-3
Sinus rhythm 3-3Conduction disturbances 3-4Atrial arrhythmias 3-5Supraventricular tachycardia (SVT) 3-7Ventricular arrhythmias 3-7
ISCHAEMIC HEART DISEASE 3-8
General 3-8Angina 3-9Myocardial infarction 3-11
REVASCULARISATION 3-12
HEART FAILURE DUE TO ISCHAEMIC HEART DISEASE 3-14
General 3-14Valvular heart disease 3-14Congenital heart disease 3-15Heart muscle disorders 3-17Pericardial disease 3-17
INFECTIVE ENDOCARDITIS 3-17
HYPERTENSION 3-17
General 3-17Advising on employment 3-20
CARDIAC TUMOURS 3-21
PERIPHERAL VASCULAR DISEASE 3-21
Claudication 3-21Varicose veins 3-21
3-1

Fire and Rescue Service: Draft Medical Guidelines – June 2004
3-2
PULMONARY HYPERTENSION 3-21
PACEMAKERS 3-22
ANTICOAGULANTS 3-22
EXERCISE 3-23
General 3-23Fitness testing 3-24
REFERENCES 3-25
AUTHORS
Dr Tony Williams MFOM, Consultant Occupational Physician, Working Fit Ltd.
Dr Neil Ineson FRCP, Consultant Cardiologist Frimley Park Hospital and formerConsultant Adviser to Defence Medical Services.

Cardiovascular problems
3-3
Introduction
Cardiovascular problems are common and can be a major risk to firefighters andcolleagues. At best a condition can cause pain or discomfort that is a distraction, at worseit can lead to altered consciousness, reduced physical capability or sudden collapse.
If there is any doubt about fitness, an assessment by a cardiologist should be sought toenable the Medical Adviser to assess the risk and advise on short and long-termmanagement of the individual.
Cardiac rhythms
SINUS RHYTHM
GeneralThe rate and rhythm of the heart is normally controlled by an impulse originating in thesino-atrial node and spreading through the atria then the ventricles. Normal sinus rhythmimplies normal conduction through this pathway.
Sinus ArrhythmiasSinus arrhythmia is a variation of normal sinus rhythm where there are alternate periods ofslow and more rapid discharges from the sino-atrial node. It is usually related to respirationwith the faster heart rates towards the end of inspiration. It is most obvious in youngerpeople. If it is not related to respiration an underling cause should be considered1.
Sinus BradycardiaClassically defined as a pulse rate less than 60 bpm, sinus bradycardia is a normal findingin many individuals, particularly the athletically trained where rates as low as 35 – 40 andpauses of up to 2 seconds are not uncommon. These are often found on 24 hour ECGmonitoring. In these circumstances there should be no cause for concern in pre-employment or routine medical screening. The presence of these findings on a routineECG should however prompt the examiner to check that the individual is asymptomaticand is physically fit2 3.
Sinus bradycardia may also be related to sinus node dysfunction associated with drugtherapy, chronic degenerative changes of the sinus node, excessive enhancement of vagaltone, and acute ischaemic infarction of the sinus node. If underlying pathology is suspectedyou should seek a cardiologist opinion and only recommend employment if the individualis at low risk from employment as a firefighter and the long term prognosis is good.
Sinus TachycardiaDefined as a pulse rate greater than 100 originating from the sino-atrial node. Anaemiaand thyrotoxicosis should be excluded as the underlying cause. Caffeine and anxiety mayalso cause tachycardia. The presence of tachycardia may make step-test results difficult tointerpret, but in the absence of any related medical conditions it should not be consideredsignificant.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
3-4
CONDUCTION DISTURBANCES
Sick Sinus SyndromeSick sinus syndrome may present as palpitations, syncope or presyncope. Most cases areidiopathic and probably related to a degenerative disease of the sinus node, atria andpossibly other parts of the conducting system4 5. Many individuals will be asymptomaticinitially, but can develop significant signs such as pauses, bradycardia, and escapetachycardias, and there is a risk of presyncope or syncope. The risk of sudden collapse issignificant. A cardiology report should be sought although it is unlikely that employmentas a firefighter will be recommended.
Atrioventricular (AV) Block
First degree
Generally benign, first degree block is defined as a prolonged P-R interval greater than0.22-0.23 seconds. This implies slowing of atrio-ventricular conduction. If there aresymptoms of syncope or presyncope, investigation to exclude other conditions should beconsidered with a cardiology opinion. If the individual is asymptomatic, first degree heartblock can be accepted as a normal variant and employment as a firefighter can berecommended.
Second degree
Defined as occasional blocked ordinary P waves, Mobitz type I (Wenkebach) and Mobitztype II can both progress to complete heart block, with the risk of both presyncope andsyncope. In young people an intermittent type l (Wenkebach phenomenon) may be seenin fit individuals, often just nocturnally on a 24 hour ECG, that is due to high vagal tone.Over the age of 45 it is unlikely to be benign and even in asymptomatic individualspacemakers should be considered6. If high vagal tone is suspected, a cardiology opinionshould be sought before recommending employment as a firefighter. The finding of eithertype of second degree block on a standard ECG requires further assessment. Most cases ofsecond degree AV block, apart from type I in the young, will need pacing7.
Third degree
Often referred to as complete heart block, there is complete independence of atria andventricles. Even in its congenital form this is not benign8, and any development ofsymptoms will need pacing (see pacemakers below).
Interventricular Conduction Disturbances
Incomplete Bundle Branch Block
There is a delay in conduction through either right or left ventricle but overall QRSduration is <0.12 seconds.
Incomplete Right Bundle Branch Block pattern is seen in 2% of children and youngadults9. It may also be present in Congenital Heart Disease. In middle aged males there isno evidence of increased cardiovascular risk9.
Incomplete Left Bundle Branch Block is thought to be a step in development of thecomplete form and should be considered as such.

Cardiovascular problems
3-5
Right Bundle Branch Block (RBBB)
RBBB can occur as a congenital, normal, finding in 1% of young adults10, although it maybe associated with congenital heart disease. Its development in adults may be associatedwith conditions such as hypertension although about 30% still have no cause(Framingham Data11).
Left Bundle Branch Block (LBBB)
LBBB generally indicates underlying hypertension or coronary heart disease. It may alsooccur in other conditions such as cardiomyopathy and valvular disease (see below). Itsdevelopment in adults is often associated with cardiac disease with a high mortality(Framingham Data11). A cardiology opinion should be sought before advising onemployment in a physically active or high pressure role.
Complete Heart Block
Complete heart block at ventricular level is generally incompatible with long-termsurvival without pacing (see pacemakers below). Where this is a result of myocardialinfarction it is generally associated with extensive myocardial damage and poor long-termsurvival. Right or left bundle branch block is also associated with large infarct size andalthough it is not an indication for pacing it is associated with higher one-year mortality,although this is mostly early mortality in-hospital3-5. Mortality is greatly increased in thepresence of heart failure. A cardiology opinion should be sought before advising onemployment in a physically active or high pressure role.
ATRIAL ARRHYTHMIAS
Atrial ExtrasystolesAtrial extrasystoles are occasionally found on 12 lead ECGs, with an incidence of around0.5%. They will be seen on 24 hour tapes in the majority of adults. Rarely they may triggersymptomatic palpitations, and will need to be differentiated from other causes. They aregenerally of no prognostic significance.
Atrial FlutterAtrial flutter is almost always associated with underlying organic atrial disease and is veryrarely seen in normal subjects12. It can be paroxysmal or chronic, and the rate and anyother symptoms are related to the degree of atrioventricular block. The predominantsymptoms are palpitations although a degree of deterioration of exercise capacity can beseen. Palpitations can be precipitated by exercise. This would compromise an individual’sability to function. Individuals may be successfully treated with either drugs or ablationtherapy. Fitness for work should be determined by the individual’s symptoms taking intoaccount the nature of any underlying cardiac condition, with advice from a cardiologist.This is a complex area as some individuals tolerate this rhythm well whilst others do sobadly, even at similar rates.
Atrial Fibrillation (AF)Atrial fibrillation is the most common cardiac arrhythmia. It can be paroxysmal or chronicand has a very variable presentation from being asymptomatic through palpitationswithout haemodynamic effect to those that include haemodynamic collapse and heartfailure. Exercise intolerance is not uncommon, even in those who feel they areasymptomatic. Paroxysmal AF develops into chronic AF in about 30% of patients13.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
3-6
AF is most often associated with hypertension but is also due to underlying ischaemicheart disease in men only14, whilst high alcohol consumption, thyrotoxicosis, and valvularheart disease are amongst the many other causes. It is more common with increasing ageand can be present in normal hearts (lone AF). Prevalence in the 55-64 age group is6.2/1000 for men and 3.8/1000 for women15.
When AF occurs in young patients it may be due to a focal arrhythmia that can beeffectively treated by ablation in some patients.
AF may be vagally mediated; this occurs more commonly in younger men aged 30-50 andonly rarely progresses to permanent AF. Attacks tend to occur at night and are oftenaborted by exercise although they may be precipitated by rest and alcohol and the relaxedstate after exercise or eating. It is usually unrelated to structural heart disease15, and shouldnot be considered a contra-indication to employment as a firefighter.
AF may also be adrenergically mediated; this tends to occur during the day, and isassociated with stress, exercise, caffeine or alcohol. Although rarer than vagally mediatedAF, and usually only lasting a few minutes, it is more frequently associated with structuralheart disease16.
AF is of clinical significance both because of its immediate clinical effects, and because oflong-term complications. Immediate effects may be palpitations, chest pain, shortness ofbreath, and low exercise tolerance. Heart failure may follow. Syncope is rare but may beassociated with the start or termination of arrhythmia. Long-term effects includeventricular dysfunction and complications from thromboemboli. The relative risk of deathis twice that of individuals with normal sinus rhythm17 and the risk of stroke is increasedby a factor of five independent of age18.
Rheumatic mitral valvular atrial fibrillation has a 17 fold increased risk of TIA or CVAwhile non-rheumatic AF has over a five fold increased risk. Both have an annual rate ofstroke of around 4.5%19. A meta-analysis of trial outcomes with warfarin demonstrates anaverage of 45/1000 strokes per year in untreated patients, with a reduction to 14/1000 onwarfarin associated with an increase of 3/1000 with major bleeds20. These are generalstatistics, and the risk of stroke is significantly lower in individuals under 60 with no otherrisk factors. One such study had no strokes among 112 patients21.
A number of anti-arrhythmic treatments are available; however individuals on treatmentshould be viewed with caution. Paroxysmal AF is often diminished by treatment, notcured. It recurs in over 90% of patients in spite of treatment, and up to 50% of patientsdiscontinue drug therapy because of side effects of drugs or treatment failure22. One studyof sotalol versus propafenone showed 37% and 30% of patients attack-free during a one-year period23. Cardioversion may have good short-term results, however only around 10%can be expected to remain free of AF over four years, and this increases to only 27% whencombined with anti-arrhythmic treatment24. Anti-arrhythmic drugs are not without sideeffects; these include heart failure and other arrhythmias, including fatal ventriculardysrhythmias associated with co-existing heart disease.
Current DVLA guidelines for Group 2 drivers require the arrhythmia to be controlled forat least 3/12, and allow driving provided that the left ventricular ejection fraction is good(i.e. LVEF is >0.4), and there is no other disqualifying condition25.

Cardiovascular problems
3-7
In summary, AF is associated with serious physical symptoms that are incompatible witheffective operational firefighting, although symptoms vary significantly betweenindividuals. There is also a significant risk of sudden collapse, again varying betweenindividuals with varying risk factors. Young individuals with no other risk factors who arerelatively or absolutely asymptomatic may be considered fit for operational firefightingafter advice from a consultant cardiologist.
SUPRAVENTRICULAR TACHYCARDIA (SVT)
GeneralThere are three main types:
• Atrial tachycardia
• Atrio-ventricular nodal (junctional) re-entrant tachycardia
• Atrio-ventricular re-entrant tachycardia.
In atrial tachycardia (the rarest) there is usually underlying heart disease.
In the other two types there is usually no associated gross structural heart disease but theremay be demonstrable electrocardiographic or electrophysiological abnormalities. Treatmentof accessory pathways by ablation therapy can eliminate the problem but not allindividuals are suitable. They generally appear in youth with recurrent attacks throughoutlife. Attacks tend to present as palpitations that may be associated with syncope or reducedexercise tolerance and in some cases shortness of breath and chest pain. They areconsidered benign unless they are associated with a rapid heart rate greater than 250 bpmor if attacks are prolonged.
Wolfe Parkinson White SyndromeWolfe Parkinson White Syndrome is a condition associated with pre-excitation via anaccessory pathway and ranges in incidence from 0.1 to 3.7/100026. The risk of suddendeath is low at approximately 0.0015 per patient year27 but many deaths occur withoutwarning28. Frequency of tachycardia increases with age and can rarely be fatal, especiallywith paroxysmal AF which can degenerate into VF. The diversity of presentations meansthat specialist opinion will usually need to be sought for risk stratification, and restrictionsplaced on virtually all symptomatic individuals. Those who have successful ablationhowever are usually cured and returned to normal risk levels.
VENTRICULAR ARRHYTHMIAS
Ventricular ExtrasystoleVentricular extrasystoles (ectopic beats) are generally asymptomatic and although seen inless than 1% of 12 lead ECGs29 they are expected as an incidental finding in 24 hour tapesin the majority of adults. They are usually benign and can be caused by nicotine or coffee.In rare cases they may indicate underlying disease. If the individual is asymptomatic andthe finding is incidental with no clinical abnormality of the cardiovascular system theindividual should be considered fit.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
3-8
If symptoms such as discomfort, palpitations, syncope or breathlessness are present, theindividual should have 24 hour monitoring to quantify the extrasystoles and look for otherdysrhythmias. A specialist opinion should be sought before providing advice onemployment in these circumstances. The presence of ventricular ectopics with underlyingcardiac disease, especially if accompanied by left ventricular dysfunction, often indicates aworse prognosis. Ventricular ectopics provoked by exercise or occurring in the recoveryperiod of an exercise test also carry a worse outcome30.
Ventricular TachycardiaVentricular tachycardia is defined as five or more consecutive ventricular beats at a rate of>120 bpm. There are many forms and mechanisms but individuals should be considered atpotential risk of sudden cardiac death or major debilitating symptoms and should beinvestigated. A specialist opinion must be sought before providing advice on employmentas there is great variety between individual types.
Ventricular FibrillationIndividuals presenting with a history of ventricular fibrillation would be survivors of aserious cardiac event. It is essential to investigate the underlying pathology and steps takento prevent recurrence before advising on employment.
Ischaemic heart disease
GENERAL
The major manifestations of ischaemic heart disease are myocardial infarction (MI),sudden cardiac death, chronic stable angina and unstable angina. The underlyingmechanism is a variable degree of coronary artery narrowing/occlusion.
There is debate as to what constitutes significant narrowing. Significant flow limitationdoes not occur until there is a reduction in cross-sectional area by 70% in animal studies.This equates to a 50% reduction in diameter31. The latter is usually measured onangiograms. Flow limitation sufficient enough to produce effort angina does not usuallyoccur until it is greater than 70% luminal diameter32.
Ischaemic heart disease is very common throughout the population. It is responsible for aquarter of all deaths, and among 55-64 year olds, 6% of men and 3% of women haveangina33.
Modern interventions have significantly reduced event rates in survivors. The recentEUROPA study in low risk proven ischaemic heart disease patients demonstrated an event(MI, cardiovascular death or sudden death) rate of less than 2% per annum34.Unfortunately many will have symptoms that will limit lifestyle and employability.
In general, decisions on employment will need to consider the risk of work precipitatingill-health, the risk of sudden incapacity to the individual, colleagues and the public, andthe impact of symptoms on the ability to work. Any decisions should be made with inputfrom a cardiologist, and regular review should be a core part of individual riskmanagement.

Cardiovascular problems
3-9
ANGINA
GeneralAngina is chest pain related to myocardial ischaemia and it is therefore essential todifferentiate from other causes of pain in the chest, neck or arms that mimics the pain ofangina. A useful classification of angina based on history divides symptomatic individualsinto three groups. Typical angina is substernal pain precipitated by exertion and relievedby rest or nitroglycerin. Atypical angina has two of these features, while non-anginal chestpain has one or none of these three features35.
The most important aspect of a history of angina, besides the immediate limitations itmakes on individual capability, is the prediction of future risk, particularly of myocardialinfarction. Sudden collapse or inability to continue in a physical task when firefightingwill clearly present a very serious risk both to the individual and to others in the team andthe general public. Medical advisers must therefore be particularly careful before eitheraccepting individuals with such a history, or of allowing such individuals to continueoperational firefighting.
Atypical chest pain needs cardiological assessment to exclude angina, progressing, ifnecessary, to coronary angiography or myocardial perfusion imaging.
Subjects with typical angina are 13 times more likely to have significant coronary diseasethan those without36. The risk varies with symptoms and age, and the following table37
illustrates the predictive probability of an individual having significant coronary arterydisease:
Diamond GA, Forrester JS. Analysis of probability as an aid in the clinical diagnosis ofcoronary artery disease. N Engl J Med 1979;300:1350-8. Copyright ©1979 MassachusettsMedical Society. All rights reserved.
The risk is also affected by the co-existence of smoking, hyperlipidaemia, diabetes, ECGchanges and previous myocardial infarct. The above percentages are therefore an amalgamof a spectrum of risk depending on the presence or absence of these factors. A variety oftools are available to calculate an accurate risk depending on the presence or absence of allthese variables. Studies have demonstrated that analysis of these factors has highpredictive value. The addition of further tests may confirm the assessment but infrequentlychanges the assessment. Common diagnostic tests performed are exercise ECG assessment,myocardial perfusion imaging and angiography.
The main advantage of exercise ECG testing is that, although it may not predict long-termrisk, it helps predict short term risk and is therefore used by agencies such as the DVLA asa simple and effective method of assessing risk of a sudden incapacitating event.
Pre-test probability of coronary artery disease (%)
Age Asymptomatic Non-anginal Atypical Typical chest pain angina angina
(yr) F M F M F M F M
30-39 <1 2 1 5 4 22 26 70
40-49 1 6 3 14 13 46 55 87
50-59 4 9 8 22 32 59 79 92
60-69 8 11 19 28 54 67 91 94

Fire and Rescue Service: Draft Medical Guidelines – June 2004
3-10
On the other hand angiography is not as predictive but demonstrates the need fortreatment.
Individuals with new onset angina have a high risk of an acute ischaemic event. Withinfifteen months of the onset of symptoms, 7% develop non-fatal MI and 4% die. A further19% require revascularisation38. There does, however, appear to be a significant variationin plaque type that causes symptoms of angina. Acute ischaemic events are related tounstable plaques and significant intimal damage caused by the inflammatory process ofarteriosclerosis. Individuals with stable angina often appear to have more stable plaqueswithout associated intimal damage and these in turn appear less likely to lead to suddenrupture with either direct luminal occlusion or associated thrombus formation.
Angina after MI has a particularly poor prognosis. One trial showed that after 2.4 years offollow-up, MI had recurred in 10.5% of untreated patients and 5.6% of patients treatedwith angioplasty or CABG, with mortality of 4.4% and 3.6% respectively39.
Modern management reduces the risk through risk factor intervention but does notremove it.
Variant or Prinzmetal AnginaVariant angina presents as angina at rest, often with recurrent episodes, but with a well-preserved exercise capacity. There also tends to be diurnal periodicity to the symptoms,clustering of episodes and symptom-free periods. The underlying cause appears to becoronary artery vasospasm, and at other times the coronary arteries may appearangiographically normal in some individuals. It is essential to differentiate betweensymptoms of unstable angina, minor plaque rupture and embolisation which can also leadto a similar clinical picture40.
Where there is a confirmed diagnosis of variant angina, the risk pattern is different fromother forms of angina, and the individual may be considered fit for firefighting dutiesproviding this is supported by a cardiologist.
Unstable AnginaStable angina may progress to unstable angina where symptoms worsen, are harder tocontrol, there may be pain at rest, and ECG changes may persist at rest. It may beaccompanied by changes in the sensitive cardiac markers such as the troponins indicatingmyocardial damage (infarction) even in the absence of typical ECG changes. Risk scorepredictors such as the TIMI risk score can be used to predict the risk of cardiac events at14 days in these individuals. Death or MI occurs in around 20% and death, MI or urgentrevascularisation in up to 41%41. This has improved considerably with aggressive treatmentand current expectations are for a non-fatal MI in 6.5% and death in 1.2% aftersix weeks42.
In these circumstances great care should be taken in recommending a return to sedentarywork. Working in a role exposing individuals to significant pressure such as control roomwork, and particularly to any physical workload, should not be considered in such casesuntil they have either stabilised or had revascularisation. The medical adviser will not onlyhave to consider what has happened but take account of the disease modifying therapyprescribed to the individual and future diagnostic/interventional plans.

Cardiovascular problems
3-11
MYOCARDIAL INFARCTION
GeneralMyocardial infarction represents a serious event in any current or prospective employeethat merits further assessment or investigation.
There are two main issues: Firstly a previous, proven myocardial infarction indicates thepresence of significant underlying ischaemic heart disease with the associated risk of futureevents. Secondly there are specific complications that can arise as a result of MI that intheir own right can affect employability.
In most cases, risk assessment will rely heavily on the results of specialist investigationspost-MI, and a report from a cardiologist is essential to enable an appropriate occupationalrisk assessment. The risk to colleagues or members of the public, and the risk to theindividual from work exacerbating the condition must be differentiated from the risk of anevent happening regardless of work. The former are health and safety issues, while thelatter should be governed by individual choice and common sense.
Acute complications are not particularly relevant to occupational physicians as they arelikely to occur either in a hospital environment or during very early convalescence whenindividuals are not at work. Clinicians are most unlikely to recommend a return to anysort of work in these early stages unless there has been a diagnostic failure, andoccupational physicians are likely to advise further time off work until recovery is wellunder way.
Chronic complications include heart failure, ventricular aneurysm formation, mitralregurgitation secondary to papillary muscle dysfunction (see under mitral valve below) anda variety of electrical complications (see under arrhythmias above). The psychologicalimpact of an MI is of major importance, particularly if the individual previously consideredthemselves fit and healthy.
Depression is a common symptom post-MI, and is strongly associated with mortality withina few months of the initial event. The 18-month risk of mortality is increased by a factorof 3.5 to 8 in those with clinical depression43. Specific psychological support interventionsdo not appear to have had any significant effect on reducing this mortality44; howeverexercise therapy does appear to have a beneficial effect45.
The continued presence of symptoms following infarction places an individual in a highrisk group for further ischaemic events. These individuals are very unlikely to be suitable asfirefighters, and are rarely fit to continue with operational firefighting. Care should also betaken in employment in high pressure environments such as the control room, and in keymanagement roles.
In asymptomatic individuals already in service, full post-infarction assessment, includingstress testing is required. A negative stress test should include no symptoms, no significantST changes and the individual should have completed Stage III (at least 9 minutes) of theBruce Protocol with no anti-anginal therapy. Any doubt about the stress test should leadto angiography.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
3-12
Ventricular AneurysmVentricular aneurysms may be formed post-infarct in the ventricular wall from a full-thickness or near-full thickness infarct. They are therefore indicators of a severe MI withsignificant myocardial damage and reduced cardiac capabilities long-term. They do notthemselves cause symptoms but are associated with reduced efficiency because they ‘steal’stroke volume, and they are commonly associated with thromboembolic events anddysrhythmias. It is thought that up to half are associated with thrombus within theventricle and around 5% lead to embolic events46.
Treatment by aneurysmectomy may be possible, often accompanied by CABG. Untreatedventricular aneurysm carries a high risk of sudden collapse as well as a reduced exercisetolerance, and is generally incompatible with operational firefighting.
Revascularisation
In the 1970s and early 1980s several trials looked at the long term outcome of coronaryartery bypass graft surgery against standard medical treatment. A consensus of opinionemerged that individuals who had either significant triple vessel disease or left main stemdisease or reduced left ventricular function benefited in terms of prognosis from coronaryartery bypass graft surgery. It was also indicated for symptomatic relief of individuals withsignificant triple vessel disease.
Where symptoms were not severe or troublesome and investigation showed single ordouble vessel disease (excluding proximal anterior descending disease and left main stemdisease), particularly in the presence of good left ventricular function, medical therapy wasfound to offer comparable long term results47 48 49 50 51 52. These trials were summarised inguidelines and indication for coronary artery bypass graft surgery such as those by Kirklin53.
Around twenty years ago coronary angioplasty started to develop. The ACME trialcompared angioplasty with medical treatment and demonstrated that patients with singlevessel disease treated with angioplasty showed at six months a reduction in numbers ofattacks of angina and improved quality of life over those treated medically. Nevertheless46% of this angioplasty group still had angina54. Similarly the RITA 2 study comparingangioplasty to medical care for an initial treatment strategy showed that after a median of7 years, death or MI had occurred in 14.5% of angioplasty patients and 12.3% of themedical care patients. Symptom improvement was greater in the angioplasty group55. Thusdespite symptomatic improvement adverse events were similar in both groups.
Despite these successes of angioplasty against medical treatment, the longer term resultsversus surgery were less convincing. The RITA I trial compared outcome in patients withsingle or multi vessel disease that was considered suitable for either angioplasty or surgery.These results showed that mortality was similar but at six months those patientsrandomised for coronary angioplasty had a higher incidence of recurrent angina (32%compared to 11% in those randomised to surgery). There was also a greater need for bothrepeat angiography and procedures in the angioplasty group56. This supported previouspublished observational data on the early natural history of angioplasty which reportedrestenosis following angioplasty in up to 40% of patients57. It was also noted that restenosiswas most likely to happen in the first four to six months. The two year follow up data fromthe RITA trial supported this.

Cardiovascular problems
3-13
For the longer term however graft occlusion resulted in recurrent disease in the coronaryartery bypass graft patients. Meta-analyses support this with little difference in mortalitybut around one third of patients treated with angioplasty requiring a further procedurecompared to around 3.3% of surgical ones58 59.
These factors led to further developments. Unfortunately saphenous vein grafts occludewith time60 61. With around 50% of vein grafts being blocked by ten years arterial graftswere increasingly used as these have lower occlusion rates with around 90% of thesearterial grafts being patent at ten years62 63 64 65 66.
Angioplasty also developed with the use of stents to try and reduce early restenosis. Thiswas endorsed in 2000 by the National Institute of Clinical Excellence. The BENESTENTstudy clearly showed that stenting in native vessels reduced the incidence of restenosis67.
The arterial revascularisation therapy study (ARTS) is looking at these more efficacioustreatments68. It compares coronary artery bypass graft surgery to angioplasty in patientswith multi vessel disease in terms of major cardiac or cerebrovascular events. In thesurgical group 93% of patients received an arterial graft. The angioplasty group used stents.The one year results show the rates of death, acute MI or stroke were low, not differingbetween the two groups (9.5% for stented patients and 8.8% for surgical patients) howeverthe event free survival was higher in the surgical patients (87.3% versus 73.3% of patients)entirely because of the need for re-intervention in the stented patients.
From an occupational health point of view these studies offer clear messages. Despiteactive intervention there are still significant proven long term problems for patients whorequired intervention. New methods such as stenting and bypass graft surgery with arterialgrafts are reducing the event rate but it remains significant and all patients will need verycareful assessment which will have to take in to account the procedures, the length of timefrom the procedure and the underlying state of the coronary artery disease together withintervention.
Single vessel arterial grafting carries the best prognosis if all other vessels are normal, thereis no evidence of myocardial damage and full risk factor intervention is in place. In thesecircumstances, a single stent with the same preconditions will be expected to do well afterthe first 6 month high recurrence period is over.
In both of these groups employment will need careful consideration, with the results of arecent exercise test to confirm good exercise tolerance and lack of evidence of myocardialischaemia (symptoms and electrocardiographic evidence). More diffuse disease andmultiple stenting/grafting have more risk of recurrence and ongoing symptoms.
Many individuals will consider themselves effectively cured by these procedures but theevidence is not in favour of this. Palliation has occurred with a significant future eventrate and need for further intervention.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
3-14
Heart failure due to ischaemic heart disease
GENERAL
Heart failure generally represents the terminal stages of ischaemic heart disease with a highrisk of acute events and poor long-term prognosis. Mortality within 2 years for all grades ofheart failure in the Framingham study was 25%. This varies from 10-20% for mild heartfailure to 75% for severe heart failure. Of all deaths, up to 50% will die suddenly fromeither arrhythmic or embolic causes69. Such a high risk would generally be consideredincompatible with operational firefighting, and could have a significant impact on control-room operators.
VALVULAR HEART DISEASE
Mitral StenosisMitral stenosis is almost always due to rheumatic heart disease. As the incidence ofrheumatic fever has declined in Western Europe it is no longer frequent in the young. Bycontrast it remains prevalent in many parts of the world including Eastern Europe where itcauses significant morbidity even in young adults. Signs will often be present at pre-employment screening but any history of rheumatic fever should alert the examiner to acareful search. There are underlying risks with further damage to the valves and a need forongoing surveillance, and as the condition progresses, there is usually a requirement formedication and often intervention. If atrial fibrillation develops, anticoagulants will beneeded (see separate guidance).
Mitral RegurgitationMitral Regurgitation was also mainly due to rheumatic heart disease but now the majorityis non rheumatic in the Western World70. Mitral regurgitation should be investigated forthe underlying cardiac cause (including ischaemic heart disease, chordal rupture, mitralvalve prolapse and secondary to cardiac dilatation from other causes). There is asignificant risk of progression with cardiac chamber dilatation.
Serving firefighters should be fully assessed and only advised to continue if their conditionis mild, investigations (such as echocardiography) show no major haemodynamic upset andthe risk of sudden incapacity is very low. They must be kept under annual specialist review.
Mitral regurgitation is also a sequel to myocardial infarction. Severe regurgitation is usuallyrelated to papillary muscle rupture or severe dysfunction and is not generally compatiblewith long-term survival without valve replacement. Individuals with mitral regurgitationpost-MI have twice the relative risk of death compared to post-MI individuals with noregurgitation71.
Applicants with mild mitral regurgitation may be considered for firefighting followingcardiac assessment, which will take into account the underlying cause, and should be keptunder annual review.

Cardiovascular problems
3-15
Mitral Valve ProlapseThe commonest cause of malfunction of the mitral valve is prolapse of one or both of itscusps during systole. The extent of this is extremely variable as are the consequent signsand haemodynamic effects1. Mitral valve prolapse is more commonly found in adultwomen72 73. Mild degrees are so common as to be regarded as normal a variant. Rarelysignificant regurgitation may give rise to haemodynamic consequences. If found at pre-employment screening or during routine medical examination it needs cardiologicalassessment.
Aortic StenosisAortic stenosis is now most frequently related to degeneration of the aortic valve, oftenwith an underlying bicuspid valve. The natural history is very variable with some casesremaining static for years whilst others can progress quite quickly74 75 76 77 78. Chest pain,syncope and dyspnoea are the classic symptoms and sudden death is a risk79. Generallyaortic stenosis is considered critical when the gradient exceeds 50 mm Hg or the valve areais less than 0.4cm2 /m2 body surface area80. Symptoms including sudden death are oftenprovoked by exertion; therefore intensive follow-up is required in any symptomaticindividual exposed to exertion in their occupation.
Aortic RegurgitationIn aortic regurgitation there is a significant risk of progression with dilation of the cardiacchambers. This will eventually lead to cardiac failure. Exercise tolerance will be limited asthe condition progresses. At pre-employment screening, great care should be taken inassessing recruits to detect the early diastolic murmur of aortic regurgitation. Other signsand the development of symptoms occur relatively late in the disease process. Servingfirefighters should be assessed by a cardiologist and kept under annual review.
Prosthetic Heart ValvesIndividuals with mechanical prosthetic heart valves will need permanent anticoagulation.See separate guidance on this.
Individuals with tissue prosthetic heart valves are not routinely anticoagulated. Themajority of these individuals will develop problems later as the prosthetic valvedegenerates faster than the native valve, and they will require a mechanical valve later inlife. This is often 10 or more years down the line from surgery (and lengthening withbetter surgical techniques). Firefighters with tissue valves should be kept under annualcardiology review.
CONGENITAL HEART DISEASE
GeneralDefects are often associated with each other and in any individual it is necessary to get fullinformation from the centre that provided care for the patient.
Ventricular Septal DefectSmall, high membranous lesions are benign and occur in 1 in 500 live births. Most closespontaneously with most no longer patent by 10 years of age. Apart from the risk ofendocarditis small residual defects pose no problem.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
3-16
Individuals with large lesions can develop haemodynamic disturbances and pulmonaryhypertension. This usually occurs early in childhood. Where a successful repair has beencarried out, individuals should be able to serve as firefighters if they are symptom free.
Atrial Septal DefectSmall defects are benign, but should not be confused with patent foramen ovale which isnot a true defect and does not normally lead to symptoms or pathology later in life.
Larger defects with significant shunting of blood can lead to haemodynamic disturbancesand pulmonary hypertension. These complications usually start in mid-adult life. Since amurmur is often the only presenting feature this is one of the reasons why individuals withejection systolic murmurs should be investigated by a cardiologist. Significant signs such asfixed splitting of the second sound, and any symptoms such as reduced exercise toleranceshould be treated with particular caution. Specific advice should be sought for thosetreated with the new percutaneous closure devices as there is little evidence for the long-term prognosis with these techniques.
Patent Ductus ArteriosusPatent ductus arteriosus may be successfully treated pharmacologically in the newborn, andby ligation and device closure. Unless associated with other significant pathologyindividuals should be considered fit for all duties.
CoarctationAortic coarctation is strongly associated with bicuspid (potentially stenotic) aortic valves.Untreated coarctation has a high risk of morbidity and mortality. Even after ‘successful’surgery there are long term sequelae81. Systemic hypertension may persist after surgery.Individuals should be kept under regular cardiologist review to ensure they do not developfurther cardiovascular disease.
Pulmonary StenosisPulmonary stenosis does not always require treatment. If necessary, balloon valvuloplasty orvalve replacement is carried out in childhood following which the condition is rarelyprogressive. Potential recruits who are symptom free should therefore be considered fully fit.
Biscuspid Aortic ValveBicuspid aortic valve occurs in 1–2% of the population and is more common in males thanfemales. Problems usually only arise later in life when one third will calcify leading toaortic stenosis and another third will lead to aortic regurgitation82 83.
Asymptomatic bicuspid valves will not usually present at medical screening other than bya soft ejection systolic murmur. Any identified either through history or signs such as amurmur should be referred to a cardiologist. Further five-yearly assessments arerecommended to identify any significant degree of aortic stenosis or regurgitation. It isthese consequences which limit employability.
Complex Congenital Heart DiseaseMany individuals with complex lesions such as tetralogy of Fallot are surviving in to adultlife after surgery. In many cases the results are excellent but the surgery has to be viewed as‘repair’ rather than ‘correction’. There are still significant risks from decompensation andtherefore despite seemingly good results specialist advice is always necessary84 85.

Cardiovascular problems
3-17
HEART MUSCLE DISORDERS
CardiomyopathiesHypertrophic86 87 88 89 90, dilated91 and restrictive cardiomyopathy are all associated withsignificant morbidity and mortality. To this classic list, arrhythmogenic right ventricularcardiomyopathy (also referred to as ‘right ventricular dysplasia’) has been added and alsohas significant risk associated with it92. Individuals may develop permanent disease as aresult of chemotherapy.
Besides the physical limitations these conditions impose, there is also a considerable risk ofincreased morbidity and mortality to themselves and risk to others if individuals were tocontinue to work as active firefighters.
MyocarditisAcute viral myocarditis can be self limiting with full resolution of any associated cardiacfailure. It can also lead to chronic cardiac failure with permanent cardiac damage. Suchindividuals will need careful assessment.
PERICARDIAL DISEASE
PericarditisMost episodes of pericarditis are either viral or idiopathic in origin. They are usually selflimiting but may be recurrent. A cardiologist opinion should be sought if there is a recenthistory of the condition or the individual is subject to recurrent bouts, although most havea complete and uncomplicated recovery.
Constrictive PericarditisIndividuals with constrictive pericarditis generally have significant underlying pathology,morbidity and mortality.
Infective endocarditis
Episodes of infective endocarditis usually indicate underlying structural cardiac diseasesuch as valvular or septal abnormalities. Any history of endocarditis should require acardiology assessment and decisions on employment should depend on the nature of theunderlying pathology.
Hypertension
GENERAL
There is a continuous relationship between blood pressure and cardiovascular risk whichrenders a numerical definition arbitrary. In the 2003 European Guidelines93 they retainedthe 1999 World Health Organisation /International Society for Hypertension classificationas in the table below without retaining the term ‘borderline’ to reflect the fact that thethreshold for treatment is flexible and dependent upon total risk94.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
3-18
‘Hypertension’ is often referred to as a systolic pressure of 140mmHg or more and diastolicpressure of 90mmHg or more but the true management of an individual must take in toaccount the complete risk profile.
Blood pressure can be affected by several factors. The following table lists some of thesefactors and the degree they may affect blood pressure95. In the context of an employmentmedical the white coat effect is often the major problematical area and may lead to furtherassessment being required such as ambulatory recording. Choice of sphygmomanometerand calibration are also relevant.
Reeves RA. The rational clinical examination. Does this patient have hypertension? How to measure blood pressure. Journal of the American Medical Association 1995; 273:1211-18. Copyright ©1995 American Medical Association. All rights reserved.
Correct conditions for measuring blood pressure96 are to have the patient seated, relaxed,with tight clothing removed from the arm. The arm should be supported at heart level.Avoid talking during the procedure. Lower the pressure slowly at 2mmHg per second,reading to the nearest 2mmHg. Measure the diastolic as the disappearance of sounds(phase V).
Patient factor Systolic Diastolic Technical factor Systolic Diastolic
‘White coat’ to physician +11 to 28 +3 to 15 Cuff too narrow -8 to +10 +2 to 8
‘White coat’ tonon-physician +1 to 12 +2 to 7 Cuff not centred +4 +3
Acute smoking +6 +5 Low elbow +6 +6
Acute caffeine +11 +5 Back unsupported +6 to 10 +6 to 10
Acute ethanol +8 +8 Arm unsupported +1 to 7 + 5 to 11
Distended bladder +15 +10 Cold season +6 +3 to 10
Talking, sighing +7 +8
Category Systolic Diastolic
Optimal <120 <80
Normal 120-129 80-84
High Normal 130-139 85-89
Grade 1 Hypertension (mild) 140-159 90-99
Grade 2 Hypertension (mod) 160-179 100-109
Grade 3 Hypertension (severe) >180 >110
Isolated Systolic Hypertension >140 <90

Cardiovascular problems
3-19
Blood pressure effects are influenced significantly by the presence of additional risk factorsand target organ damage:
Risk factors Target organ damage
Heart disease
Left ventricular hypertrophy
Angina/MI
Coronary revascularisation
Heart failure
Stroke or TIA
Nephropathy
Peripheral arterial disease
Retinopathy
Smoking
Dyslipidaemia
Diabetes mellitus
Male or postmenopausal woman
Family history of cardiovascular disease
Men under 55
Women under 65
The previous graph shows the absolute risk associated with cardiovascular disease. TheFramingham study also showed that individuals in the highest risk group of systolic bloodpressure over 195 with no associated cardiovascular disease had a risk of a cardiovascularevent of under a third over a fifteen year period98.
Evidence suggests that treatment reduces the risk to individuals. As the risk of acardiovascular event is small in such individuals it would be reasonable to supportemployment in those with isolated hypertension that is effectively treated.
Figure 1: Absolute and relative risk for a cardiovascular disease event in a
high risk and low risk 55 year old man by systolic pressure
(Used with permission of the American College of Physicians97)
High risk = left ventricular hypertrophy, cigarette smoker, glucose intolerance, cholesterol > 8.02mmol/L.
Low risk = no cardiovascular risk factors other than systolic blood pressure level.
0
200
105 120 135 150Systolic Blood Pressure
8 Y
ear
Pro
bab
ility
of
Car
dio
vasc
ula
rD
isea
se E
ven
t p
er 1
000
Pati
ent
Yea
rs
165 180 200 mm Hg
400
600
800Low Risk
High Risk

Fire and Rescue Service: Draft Medical Guidelines – June 2004
3-20
Medical advisers assessing absolute risk of an adverse event related to blood pressure mustconsider the risk factors rather than basing their advice on employment solely on bloodpressure readings.
The MRC trial identified the following factors to enable grouping into high or low risk99.
The additional factors of lack of exercise, high salt intake, alcohol intake and other dietaryfactors are harder to quantify for absolute risk although they have been shown to havesignificant relative risk reduction.
ADVISING ON EMPLOYMENT
Where hypertension (systolic > 140, diastolic > 90) is identified at pre-employmentscreening, the individual should be referred to their GP and recruitment delayed until thecondition has been assessed and the outcome of any treatment required is known.
It would be prudent to remove firefighters from operational duties if their resting bloodpressure exceeds 180mmHg systolic and 120mmHg diastolic.
Factor High risk Low risk
Age >65 <45
Serum cholesterol in mmol/l >8 <5
Body mass index >30 <27
Ischaemic electrocardiogram +ve -ve
Smoking no of cigarettes/day 40 0
Figure 2: Relative risk for stroke and coronary heart disease by usual diastolic
blood pressure
(Used with permission of the American College of Physicians97)
High risk = left ventricular hypertrophy, cigarette smoker, glucose intolerance, cholesterol > 8.02mmol/L.
Low risk = no cardiovascular risk factors other than systolic blood pressure level.
76 84 91 98 105 mm Hg
1 2 3 4 5
0.25
0.50
1.00
2.00
4.00
0.25
0.50
1.00
2.00
4.00
Approximate Mean Usual DBP Approximate Mean Usual DBP
Rel
ativ
e R
isk
of
Stro
ke
Rel
ativ
e R
isk
of
Co
ron
ary
Hea
rt D
isea
se
76 84 91 98 105 mm Hg
1 2 3 4 5BaselineDBP category
BaselineDBP category

Cardiovascular problems
3-21
Individuals with controlled hypertension with no symptoms from medication are usually fitfor service as firefighters. The choice of drug should be tailored to the individual’s need tocope with physical exertion. A small dose of diuretic, an angiotensin converting enzymeinhibitor, angiotensin II receptor blocker, alpha blocker or calcium channel blocker isgenerally acceptable. Beta-blockers should be used with caution as the stress response maybe reduced, and fatigue can be a problem; this will need to be assessed on an individualbasis. Exercise test results (such as the step test) will also be affected. Approximately 70%of individuals will need two or more drugs to achieve control.
Hypertension combined with other disease or other factors such as obesity may increasethe risk of morbidity and careful judgement should be used before advising on fitness foremployment.
Cardiac tumours
If a cardiac tumour is found, or is declared, a specialist opinion should be sought.Malignant cardiac tumours are rarely successfully managed by surgical excision. Myxomaresponds well to complete excision, with a 1-5% recurrence rate.
Peripheral vascular disease
CLAUDICATION
The symptoms of claudication are likely to limit the effectiveness of firefighters. They areunlikely to reach the fitness standards required to serve operationally. Claudication is alsoassociated with other significant cardiovascular disease and a full assessment should beconducted with specialist opinion sought on any positive findings.
In some rare cases claudication will be due to a congenital lesion which can be successfullytreated. Specialist advice should be sought in each case and the nature of intervention(medical, angioplasty and surgical), together with the extent of the disease will need to beconsidered.
VARICOSE VEINS
Asymptomatic varicose veins do not usually result in significant morbidity. Providedindividuals are able to pass the relevant physical tests there should be little cause forconcern.
Very prominent veins could give rise to traumatic haemorrhage. If individuals havesymptoms that affect their physical ability, advice on employment should be deferred untilafter treatment.
Pulmonary hypertension
There are numerous underlying causes of pulmonary hypertension. The condition generallyindicates significant heart and/or lung pathology with serious risk of sudden incapacitatingevents and long term morbidity. Specialist reports are essential.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
3-22
Pacemakers
Pacemakers may be affected by either electromagnetic interference or direct trauma. Anexpert opinion should be sought from the manufacturer before advice is given onemployment.
Electromagnetic radiation is extremely unlikely to cause permanent damage to the unit,but it may inhibit output or in some cases cause a variable rate pacemaker to change tofixed rate. The effects are usually temporary while in close proximity to the source ofinterference. As a rule of thumb some manufacturers recommend that individuals shouldremain around 1m per 10kV distant from sources of high voltage.
The evidence for interference from radio transmitting equipment such as mobile phonesand personal radio communication equipment shows a very low risk, probably around1:100,000, of adverse events. The advice from most studies suggests the handset should bekept between 10 and 50 cm away from the pacemaker although the risk may be effectivelyzero for many modern pacemakers 100 101 102.
There is a risk of damage to the pacemaker or pacemaker site from direct trauma.Individuals should therefore avoid contact sports, and any firefighting duties should beassessed depending on the location of the pacemaker and the expected activity. Fracture ofa pacemaker lead as a result of wearing or carrying equipment may pose a threat.Individuals who are pacemaker-dependent face real risk from pacemaker malfunctionwhich could lead to disabling symptoms and this aspect must also be considered. An expertopinion should be sought from a cardiologist on both risk of pacemaker failure and risk oftrauma to the leads.
Anticoagulants
Warfarin may be prescribed either short or long term for a variety of conditions. Theobvious side effect of this is an increase in clotting time and therefore an increased risk ofboth internal and external bleeding.
There is a significant increase in the risk of deep and superficial bruising with associatedmorbidity although there does not appear to be an increase in risk of fatal bleedingfollowing trauma without head injury103. There is a small but devastating risk of brainhaemorrhage following head trauma. There does not appear to be a significant risk below aPTR of 2, however the risk rises to about 10 fold at a PTR of 3 with a continued increasein risk as PTR rises further104. Individuals should therefore avoid exposure to the risk ofsignificant trauma, particularly trauma to the head.

Cardiovascular problems
3-23
Exercise
GENERAL
There is some evidence that a single exercise session has an acute beneficial effect on lipidlevels by reducing triglycerides, increasing high-density lipoprotein and cholesterol andreducing blood pressure as well as improving insulin sensitivity and glucose homeostasis105.There is considerable evidence that long-term physical exercise reduces blood pressure106
although isolated exercise does not appear to have a prolonged beneficial effect. Exerciseshould be combined with other lifestyle changes107.
Physical exercise is known to produce an acute rise in blood pressure. An increase of theorder of 35-50mmHg systolic and 8-29mmHg diastolic can be expected108. It is also knownthat vigorous physical activity predisposes to an acute coronary or cerebral vascular event.
The risk associated with vigorous activity varies by a factor of 5-100 depending on age,cardiac risk factors including target organ damage and the physical and emotionalcircumstances of the individual. In fit individuals, sudden unexpected death related toexercise109 remains rare even though overall there is an increased risk of sudden death of 3-7 episodes per 100,000 per year during demanding physical work.
In the absence of a history of cardiovascular disease, in normotensive individuals, the riskfrom either physical assessment or from demanding physical work is considered very low.There are no medical grounds for supervision of occupational fitness assessments in theselow risk individuals110.
Individuals with a significant cardiovascular history or with hypertension that is moderateor high should be formally assessed by a cardiologist before undertaking fitness assessmentsor resuming operational firefighting duties.
Individuals with controlled hypertension with no symptoms from medication are usually fitfor service as firefighters. There is evidence that those taking treatment have a higher riskthan those normotensive individuals on no treatment111, but the risk is low. The choice ofdrug should be tailored to the individual’s need to cope with physical exertion. A smalldose of diuretic or ACE inhibitor is generally acceptable. Beta-blockers should be usedwith caution as the stress response is often reduced, and fatigue can be a problem. Step testresults will also be affected.
There are several guidelines available for assessing risk of exercise in those withcardiovascular risk factors. Firefighters who have remained operational and have notdeveloped any cardiovascular problems should not need any specific assessment.Individuals who have developed symptoms of angina, rhythm disturbance or a coronaryevent should be formally assessed by exercise ECG, and preferably by a cardiologist, beforereturning to active training for firefighting duties. They should be able to reach at least theend of stage 3 of the Bruce protocol without any significant ST segment depression.
Exercise is known to increase the blood pressure (see above), and this rise is directlyrelated to the increase in heart rate. There is a theoretical risk of exercise in individualswith severe hypertension, although no studies could be found that demonstrated a definiterisk. Exercise may be a part of treatment of those with cardiovascular disease, but in asteady state manner rather than in bursts as may be required in operational firefighting.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
3-24
FITNESS TESTING
GeneralWhere it is determined that an individual should have a medical assessment beforeundertaking fitness assessments, it is important to get this process in chronological order.There is no point undertaking medical assessments after the fitness testing has taken place.This may seem self-evident, however timetables are frequently re-organised and do notalways take medical assessments into account.
Medical Advisers should use their common sense in advising on medical fitness for tests.There is an onus on the individual to raise specific issues, and a simple questionnaireapproach to screen individuals for health problems is often sufficient unless testing isparticularly arduous.
Certain specific hazards should be avoided. The valsalva manoeuvre, straining against aclosed glottis particularly when lifting, is potentially dangerous as it increases intra-thoracic pressure and puts strain on the heart. It is completely unnecessary, and individualsshould be taught to exhale when lifting.
All significant lifting or other manual tasks should be conducted in accordance withManual Handling Regulations. This is an issue for safety staff and need not involvemedical staff. Provided these regulations are followed there should be no significant risk fornormal individuals. Obviously those with specific musculoskeletal problems should beassessed and advised where appropriate.
The Step TestThe step test has been used in the estimation of fitness for operational firefighting duties.It is inexpensive, and can be carried out anywhere. It allows the assessor to observe thesubject undertaking sustained exercise relevant to firefighting and at an exertion levelappropriate to the types of tasks required by the job. The medical observer may also beable to identify many orthopaedic or neurological disorders affecting the lower limbs, asthe subject is unlikely to be able to disguise these for the duration of the test.
Dear Chief Fire Officer Letter 2/96 endorsed the Chester Step Test as the recommendedtool for assessing aerobic capacity.
Leg back pull testThere is no requirement or benefit for serving firefighters to undertake this test, unlessused by medical staff to assess recovery after injury. The recruit is only required to register apull of 117kg, and this may be aided by a series of ‘warm-up’ lighter pulls until the target isreached.
Some dynamometers have misleading instructions. Applicants should bend the knees andkeep the back straight while pulling; a bent back is contrary to all good manual handlingtraining and can lead to serious injury.
Grip strength testIt is important to ensure the equipment is adjusted correctly as performance using the gripdynamometer is significantly reduced if the incorrect hand size adjustment is used. It is alsoimportant to ensure the individual keeps the equipment away from the body or otherobjects to prevent levering or pushing to increase the reading.

Cardiovascular problems
3-25
References
1 Julian D. Diseases of the Heart. Second Edition. London: WB Saunders. 1996
2 Viitasalo MT, Kala R, Eissalo A. Ambulatory electrocardiographic findings in youngathletes between 14 and 16 years of age. Eur Heart J 1984;5:2-6.
3 Talan DA, Bauernfeind RA, Ashley WW et al. Twenty-four hour continuous ECGrecordings in long distance runners. Chest 1982;82:19-24.
4 Benditt DG, Milstein S, Goldstein M, Reyes W, Gornick CC. Sinus node dysfunction:pathophysiology, clinical features, evaluation and treatment. In CardiacElectrophysiology (eds DP Zipes and J Jalife). Philadelphia, WB Saunders, 1990.
5 Thery C, Gosselin B, Lekieffre J, Warembourg H. Pathology of sinoatrial node.Correlations with electrocardiographic findings in 111 patients. Am Heart J 1977;6:735-40.
6 Shaw DB, Gowers JI, Keswick CA, New KH, Whistance AW. Is Mobitz type Iatrioventricular block benign in adults? Heart 2004 Feb;90(2):169-74.
7 Levander-Lindgren M, Lantz B. Bradyarrhythmia profile and associated diseases in 1,265patients with cardiac pacing. Pacing Clin Electrophysiol 1988;11:2207-15.
8 Esscher EB. Congenital complete heart block in adolescence and adult life. A follow-upstudy. Eu Heart J 1981;2:281-8.
9 Hiss RG, Lamb IE. Electrocardiographic findings in 122,043 individuals. Circulation1962;25:947-61.
10 Liao YL, Emidy LA, Dyer A. Characteristics and prognosis of incomplete right bundlebranch block. An epidemiologic study. J.Am Coll Cardiol 1986;7:492-9.
11 Schneider JF, Thomas ME, Kreges BE. Newly acquired left bundle branch block: TheFramingham study. Ann Intern Med. 1979;90:303-10.
12 Ricou F et al. Influence of right bundle branch block on short- and long-term survivalafter acute anterior myocardial infarction. J Am Coll Cardiol 1991;17:858-63.
13 Fosmoe RJ, Averill KH, Lamb LE. Electrocardiographic findings in 67,375 asymptomaticsubjects: II. Supraventricular Arrhythmias. Am J Cardiol 1960;6:84-95.
14 Godtfredsen J. Atrial fibrillation. Etiology, course and prognosis. A follow-up study of1212 cases. Thesis, University of Copenhagen, 1975.
15 Benjamin EJ et al. Independent risk factors for atrial fibrillation in a population-basedcohort. The Framingham study. JAMA 1994;271:840-4.
16 Coumel P. Neural aspects of paroxysmal atrial fibrillation. In Falk RH, Podrid PJ eds.Atrial fibrillation: mechanisms and management. New York: Raven Press, 1992, pp109-25.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
3-26
17 Kannel WB et al. Epidemiologic features of chronic atrial fibrillation. N Engl J Med1982;306:1018-22.
18 Wolf PA et al. Atrial fibrillation: a major contribution to stroke in the elderly. ArchIntern Med 1987;147:1561-4.
19 Wolf PA et al. Epidemiologic assessment of chronic atrial fibrillation and risk of stroke:the Framingham study. Neurology 1978;28:973-7.
20 Cairns JA. Atrial fibrillation: anthithrombotic therapy. In Yusuf S et al. Evidence BasedCardiology. London: BMJ Books, 1998. pp 544-52.
21 Atrial Fibrillation Investigators. Risk factors for stroke and efficiency of antithrombotictherapy in atrial fibrillation. Analysis of pooled data from five randomised controlledtrials. Arch Intern Med 1994;154:1449-57.
22 Crijns HJG et al. Atrial fibrillation: antiarrhythmic therapy. In Yusuf S et al. EvidenceBased Cardiology. London: BMJ Books, 1998. pp 527-43.
23 Reimold SC et al. Propafenone versus sotalol for suppression of recurrent symptomaticatrial fibrillation. AM J Cardiol. 1993;71:558-63.
24 Van Gelder IC et al. Chronic atrial fibrillation. Success of serial cardioversion therapyand safety of oral anticoagulation. Arch Intern Med 1996;156:2585-92.
25 Drivers Medical Group, DVLA. At a glance guide to the current medical standards offitness to drive. http://www.dvla.gov.uk/at_a_glance/ch2_cardiovascular.htm
26 Josephson M. Preexcitation syndromes. In Clinical Cardiac Electrophysiology. Lea &Febiger, 1993; 311-416.
27 Munger TM, Packer DL, Hammil SC et al. A population study of the natural history ofWolff-Parkinson-White syndrome in Olmsted county, Minessota, 1953-1989.Circulation 1993;87:866-73.
28 Montoya PT, on behalf of the European Registry on Sudden Death in the Wolff-Parkinson-White syndrome: Ventricular fibrillation in the Wolff-Parkinson-Whitesyndrome. Circulation 1988;78(suppl. II):II-22(abstr).
29 Averill KH, Lamb LE. Electrocardiographic findings in 67,375 asymptomatic subjects: I.Incidence of abnormalities. Am J Cardiol 1960;6:76-83.
30 Frolkis JP, Pothier CE, Blackstone EH Lauer MS. Frequent ventricular ectopy afterexercise as a predictor of death. N Engl J Med. 2003 Feb 27;348(9):781-90.
31 Robbins SL, Bentov I. The kinetics of viscous flow in a model 1 vessel: effect of stenosisof varying size, shape and length. Lab Invest 1967;16:864-74.
32 McMahon M, Brown B, Cukingnan R. et al. Quantitative coronary arteriography;measurement of the ‘critical’ stenosis in patients with unstable angina and single vesseldisease without collaterals. Circulation 1979;60:106-13.

Cardiovascular problems
3-27
33 Ness AR, Davey Smith G. Cardiovascular Medicine. In Warrell DA et al. OxfordTextbook of Medicine 4th Edn (electronic version). Oxford: Oxford University Press,2003.
34 Fox KM et al. Efficiency of Perindopril in reduction of cardiovascular events amongpatients with stable coronary artery disease: randomized, double-blind, placebo –controlled, multi-centre trial (the EUROPA Study). Lancet 2003; 362: 782-8.
35 Diamond GA. Letter: a clinical relevant classification of chest discomfort. J Am CollCardiol 1983;1:574-5.
36 Pryor DB et al. Value of the history and physical in identifying patients at increased riskfor coronary artery disease. Ann Intern Med 1993;118:81-90.
37 Diamond GA, Forrester JS. Analysis of probability as an aid in the clinical diagnosis ofcoronary artery disease. N Engl J Med 1979;300:1350-8.
38 Fox KAA. Management of acute coronary syndromes: unstable angina and myocardialinfarction. In Warrell DA et al. Oxford Textbook of Medicine 4th Edn (electronicversion). Oxford University Press 2003. Oxford.
39 Madsen JK et al. Danish multicenter randomized study of invasive vs conservativetreatment in patients with inducible ischaemia after thrombolysis in acute myocardialinfarction (DANAMI). Circulation 1997;96:748-55.
40 Fox KAA. Management of acute coronary syndromes: unstable angina and myocardialinfarction. In Warrell DA et al. Oxford Textbook of Medicine 4th Edn (electronicversion). Oxford University Press 2003. Oxford.
41 Antman EM, Cohen M, Bernink PJ et al The TIMI risk score for unstable angina/nonST elevation MI: A method for prognostication and therapeutic decision making.JAMA 2000 Aug 16;284(7):835-42.
42 The TIMI-3B Investigators. Effects of tissue plasminogen activator and a comparison ofearly invasive and conservative strategies in unstable angina and non-Q wavemyocardial infarction. Results of the TIMI-3B trial. Circulation 1994;89:1545-56.
43 Frasure-Smith N et al. Depression and 18-month prognosis after myocardial infarction.Circulation 1995;91:999-1005.
44 Cody RJ. Results from late breaking clinical trials sessions at ACC ’97. J Am CollCardiol 1997;30:1-7.
45 O’Connor GT et al. An overview of randomized trials of rehabilitation with exerciseafter myocardial infarction. Circulation 1989;80:234-44.
46 Lapeyre AC et al. Systemic embolism in chronic left ventricular aneurysm: incidenceand the role of anticoagulation. J Am Coll Cardiol 1985;6:534-8.
47 Long term results of prospective randomised study of coronary artery bypass surgery instable angina pectoris. European Coronary Surgery Study Group. Lancet 1982 Nov27;2(8309):1173-80.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
3-28
48 Takaro T, Hultgreen HN, Detre KM, Peduzzi P. The Veterans AdministrationCooperative Study of stable angina; current status; Circulation 1982 Jun;65(7 pt 2):60-7.
49 Weinstein GS, Levin B. The Coronary Artery Surgery Study (CASS). A criticalappraisal. J Thorac Cardiovasc Surg. 1985 Oct;90(4):541-8.
50 Bonow RO, Epstein SE. The indications for coronary artery bypass surgery in patientswith chronic angina pectoris; implications of the multi centre randomised trials.Circulation 1985: Dec; 76 6 (pt 2);V23-30.
51 Myers WO, Gersh BJ, Fisher LD et al Medical versus early surgical therapy in patientswith triple-vessel disease and mild angina pectoris; a CASS registry study of survival.Ann Thorac Surg 1987 Nov;44(5);471-86.
52 Loop FD, CASS continued. Circulation 1985; 72 (3 Pt 2): II1-6.
53 Kirklin JW, Akins CW, Blackstone EH et al. Guidelines and indications for coronaryartery bypass graft surgery. J Am Coll Cardiol 1991;17:543-89.
54 Parisi AF, Folland ED, Hartigen P. A comparison of angioplasty with medical therapy inthe treatment of single-vessel coronary artery disease. Veterans affairs ACMEInvestigators. N Eng J Med 1992 Jan 2; 326 (1): 10-16.
55 Henderson RA, Pocock SJ, Clayton TC et al Seven year outcome in the RITA-2 trial:Coronary angioplasty versus medical therapy. J Am Coll Cardiol 2003 Oct 1;42(7):1161-70.
56 RITA trial investigators. Coronary angioplasty versus coronary artery bypass surgery: therandomised intervention treatment of angina (RITA) trial. Lancet 1993; 341:573-80.
57 Gershlick AH, de Bono P. Restenosis after angioplasty. Br Heart J 1990;64:351-3.
58 Pocock SJ, Henderson RA, Rickards AF et al . Meta-analysis of randomised trialscomparing coronary angioplasty with bypass surgery. Lancet 1995;346:1184-9.
59 Rickards AF, Davies SV. Coronary angioplasty versus coronary surgery in themanagement of angina. Curr Opin Cardiol 1995;10:399-403.
60 Fitzgibbon GM, Leach AJ, Keon WJ,et al. Coronary bypass graft fate. Angiographicstudy of 1,179 vein grafts early, one year, and five years after operation. J. Thorac.Cardiovasc Surg. 1986;91: 773-8.
61 Lytle BW, Loop FD, Taylor PC et al. Vein graft disease: The clinical impact of stenosesin saphenous vein bypass grafts to coronary arteries. J. Thorac. Cardiovasc. Surg.1992;103:831-40.
62 Okies JE, Page US, Bigelow JC et al. The left internal mammary artery: the graft ofchoice. Circulation 1984;70(suppl. I)I-213-21.
63 Tector AJ. Fifteen years’ experience with the internal mammary artery graft. AnnThorac Thorac Surg 1986;42(suppl):S22-7.

Cardiovascular problems
3-29
64 Tector AJ, Schmahl TM, CaninoVR. Expanding the use of the internal mammary arteryto improve patency in coronary artery bypass grafting. J Thorac Cardiovasc Surg1986;91:9-16.
65 Loop FD, Lytle BW, Cosgrove DM et al. Free (aorta-coronary) internal mammary graft.Late results. Cardiovasc. Surg. 1986;92:827-31.
66 Green GE, Swistel DG, Cameron AA. Bilateral internal thoracic artery surgery: 17 yearexperience. Eur Heart J 1989;10 (suppl. H):57-60.
67 Serruys PW, de Jaegere P, Kiemeneij F et al. A comparison of balloon – expandable –stent implantation with balloon angioplasty in patients with coronary artery disease.Benestent Study Group. N Eng J Med 1994 Aug 25;331:489-95.
68 Serruys PW, Unger F, van Hout BA et al. The ARTS Study (Arterial RevascularisationTherapies Study). Seminars in Interventional Cardiology 1999;4:209-19.
69 Kannel WB et al. Cardiac failure and sudden death in the Framingham study. Am HeartJ 1988;115:869-75.
70 Selzer A, Katayama . Mitral regurgitation: Clinical patterns, pathophysiology andnatural history. Medicine 1972;51:337-66.
71 Lamas GA et al. Clinical significance of mitral regurgitation after acute myocardialinfarction. Circulation 1997;96:827-33.
72 Jeresaty RM. Mitral Valve Prolapse. New York: Raven Press, 1979: 139.
73 Savage DD, Garrison RJ, Devereux RB et al. Mitral valve prolapse in the generalpopulation. 1. Epidemiologic features. The Framingham Study. Am Heart J. 1983;106:571-6.
74 Selzer A.Changing aspect of the natural history of valvular aortic stenosis. N Engl JMed. 1987; 317: 91-8
75 Wagner S, Selzer A. Patterns of progression of aortic stenosis: a longitudinalhemodynamic study. Circulation 1982;65:709-12.
76 Bogart DB, Murphy BL, Wong BYS et al. Progression of aortic stenosis. Chest1979;76:391-6.
77 Cheitlin MD, Gertz EW, Brundage BH et al. Rate of progression of severity of aorticstenosis. Am Heart J. 1979;98(6):689-700.
78 Jonasson R, Jonasson B, Nordlander R et al. Rate of progression of severity of aorticstenosis. Acta Med Scand 1983;213:51-4.
79 Hohn AR, van Praagh S, Moore AAD et al. Aortic stenosis. Circulation 1965;32(suppl 3):III 4-12.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
3-30
80 Morrow AG, Roberts WC, Ross J Jr et al. Clinical staff conference. Obstruction to leftventricular outflow. Curent concepts of management and operative treatment. AnnIntern Med 1968;69:1255-86.
81 Celermajer DS, Greaves K. Survivors of Coarctation repair: fixed but not cured.Editorial. Heart 2002; 88:113-114.
82 Roberts WC. The congenitally bicuspid aortic valve. A study of 85 autopsy cases. Am JCardiol 1970; 26:72-83.
83 Fenoglio JJ, McAllister HA, DeCastro CM, Davis JE, Cheitlin MD. Congenital bicuspidaortic valve after age 20. Am J Cardiol 1977;39:164-9.
84 Hokanson JS, Moller JH. Adults with tetralogy of Fallot: Long term follow up. CardiolRev 1999 May;7:149-155.
85 Nollert G, Fischlein T, Bourtewek S, Bohmer C, Klinner W, Reichart B. Long termsurvival in patients with repair of Tetralogy of Fallot 36 year follow up of the first yearafter surgical repair. J Am Coll Cardiol 1997 Nov 1:30(5):1374-83.
86 Maron BJ, Roberts WC, Epstein SE. Sudden Death in Hypertrophic Cardiomyopathy:A Profile of 78 patients. Circulation 1982;65:1388-94.
87 Maron BJ Bonow RO, Cannon RO III, Leon MB, Epstein SE. HypertrophicCardiomyopathy: Interrelations of Clinical Manifestations, Pathophysiology andTherapy. Part 1. N engl J Med 1987;316:780-9.
88 Maron BJ, Roberts WC, Edwards JE, McAllister HA, Foley DD, Epstein SE. SuddenDeath in Hypertrophic Cardiomyopathy: Characterisation of 26 patients withoutFunctional Limitation. Am J Cardiol 1978;41:803-10.
89 Maron BJ, Bonow RO, Cannon RO, III, Leon MB, Epstein SE. HypertrophicCardiomyopathy: Interrelations of Clinical Manifestations, Pathophysiology andTherapy. Part 2. N Engl J Med 1987;316:844-52.
90 Lynch P, Ineson N, Jones KP, Scott AWM. Sudden Death in Sport before and afterintroduction of the basic fitness test. J R Army Med Corps 1985;131:42-46.
91 Redfield MM, Gersh BJ, Bailey KR et al. Natural history of idiopathic dilatedcardiomyopathy: effect of referral bias and secular trend. J Am Coll Card 1993;22:1921-6.
92 Thiene G,Nava, Corrado D et al. Right ventricular cardiomyopathy and sudden deathin young people. N Engl J Med 1988;318:129-33.
93 Guidelines Committee. 2003 European Society of Hypertension – European Society ofCardiology guidelines for the management of arterial hypertension. J Hypertens2003;21:1011-53.
94 Guidelines Sub-Committee. 1999. World Health Organisation / International Societyfor Hypertension guidelines for the management of hypertension. J Hypertens1999;17:151-183 GL.

Cardiovascular problems
3-31
95 Reeves RA. The rational clinical examination. Does this patient have hypertension?How to measure blood pressure. Journal of the American Medical Association 1995;273:1211-18.
96 British Hypertension Society. www.bhsoc.org
97 Alderman MH. Blood pressure management: individualised treatment based onabsolute risk and the potential for benefit. Ann Intern Med 1993;119:329-35.
98 Madhavan S, Alderman MH. The potential effect of blood pressure reduction oncardiovascular disease. A cautionary note. Arch Intern Med 1981;141:1583-6.
99 Medical Research Council Working Party. Stroke and coronary heart disease in mildhypertension: risk factors and the value of treatment. BMJ 1988;296:1565-70.
100 Myerson SG, Mitchell AR. Mobile phones in hospitals. BMJ 2003;326:460-1.
101 Kainz W et al. Electromagnetic compatibility of electronic implants – review of theliterature. Wien Klin Wochenschr. 2001 Dec 17:113(23-24):903-14.
102 Irnich et al. Electromagnetic interference of pacemakers by mobile phones. PacingClin Electrophysiol 1996 Oct;19(10):1431-46.
103 Mina AA et al. Complications of preinjury warfarin use in the trauma patient.J Trauma. 2003 May;54(5):842-7
104 Hylek EM, Singer DE. Risk factors for intracranial hemorrhage in outpatients takingwarfarin. Ann Intern Med 1994 Jun1;120(11):897-902.
105 Thompson PD et al. The acute versus the chronic response to exercise. Med Sci SportsExerc. 2001;33(6 Suppl):S438-45; discussion S452-3.
106 Faggard RH. Prescription and results of physical activity. J Cardiovasc Pharmacol1995;25(Suppl 1):S20-S27.
107 National High Blood Pressure Education Program. The fifth report of the JointNational Committee on Detection, Evaluation and Treatment of High Blood Pressure.NIH publication no. 93-1088. Bethesda MD: National Institutes of Health, NationalHeart, Lung & Blood Institute, 1993.
108 Wright RL et al. Blood pressure responses to acute static and dynamic exercise in threeracial groups. Med Sci Sports Exerc. 1999;31(12):1793-8.
109 Shephard RJ, Bonneau J. Supervision of occupational fitness assessments. Can J ApplPhysiol 2003;28(2):225-39.
110 Jensen G et al. Risk factors for acute myocardial infarction in Copenhagen, II:Smoking, alcohol intake, physical activity, obesity, oral contraception, diabetes, lipids,and blood pressure. Eur Heart J 1991;12(3):298-308.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
3-32

CHAPTER 4
Respiratory problems


CHAPTER 4Respiratory problems
CONTENTS
INTRODUCTION 4-3
ASTHMA 4-3
Adult Onset Asthma 4-5
OBSTRUCTIVE LUNG DISEASE 4-6
ACUTE EFFECTS OF SMOKE INHALATION 4-6
CHRONIC EFFECTS OF SMOKE INHALATION 4-6
RESTRICTIVE LUNG DISEASES 4-7
SPONTANEOUS PNEUMOTHORAX 4-7
PULMONARY EMBOLISM 4-7
GROWTHS IN THE LUNG 4-8
Benign Growths 4-8Malignant Growths 4-8References 4-9
4-1

Fire and Rescue Service: Draft Medical Guidelines – June 2004
4-2
Authors
Dr Ian Gemmell MB ChB MSc MA(Law) MFOM, Consultant Occupational Physician,Employment Medical Services Ltd.
Dr Paul Cullinan FRCP, Reader in Occupational and Environmental Medicine Imperial College(NHLI) and Consultant Physician Royal Brompton Hospital.

Respiratory problems
4-3
Introduction
The lungs are the main organs responsible for gaseous exchange. An adequate intake ofoxygen is essential when carrying out firefighting duties which can require considerableexertion over long hours of duty. The early use of breathing apparatus protects the lungsfrom many of the hazardous fumes found at fires but a disease-free respiratory system isessential for a healthy firefighter.
Asthma
Asthma is a disease characterised by variable constriction of the airways causing anincreased resistance to air flow leading to reductions in ventilation and hyperinflation ofthe lungs. Symptoms vary from a slight dry cough to an audible wheeze. Status Asthmaticusis the condition whereby air is trapped in the lower airways and cannot be exhaled,resulting in severe hypoxia which may be life threatening.
People who suffer from asthma often have airways which constrict in response to non-specific stimulants such as exercise, respiratory infections, cold dry air, and exposure toirritant dusts or vapours including smoke. This condition is known as bronchial hyper-reactivity. Because asthma is a variable disease the degree of hyper-reactivity may itselfvary over time and in response to treatment. Furthermore it must be recognised thatbronchial hyper-reactivity may occur in otherwise normal people generally as aconsequence of a chest infection, and this may not resolve for up to six weeks postinfection. In such people, exercise is the commonest precipitant1.
Frequent or prolonged admissions to hospital as a child, with treatment using steroids andtheophylline derivatives, signifies a degree of asthma which is likely to have resulted inpersisting abnormal lung function in adulthood.
About 25% of contemporary UK children will have a diagnosis of ‘asthma’ recorded intheir general practitioner notes and about 40% of all children will have been treatedwith salbutamol before the age of six years. In most cases this is not true ‘asthma’ but theresponse to viral respiratory infection. The prevalence of true childhood asthma is around15%. Thus reference to early medical records is likely to be unhelpful.
The following definitions are used:
Mild Childhood Asthma Onset >10 years, <5 attacks per year, few or no hospitalisations,remission by age 16
Moderate asthma 5 or 6 attacks per year, few hospitalisations, requires nebulisers butnot IV therapy, no residual spirometric changes
Severe Childhood Asthma Onset <10 years, >6 attacks per year, lost schooling, hospitalisationsrequiring IV Theophylline and steroids, spirometric changes
Adult Asthma Onset >16 years
RADS Onset >16 years following chemical incident

Fire and Rescue Service: Draft Medical Guidelines – June 2004
4-4
True childhood asthma, generally atopic, typically presents before the age of eight andmost children ‘grow out of it’ by the age of 20. Of the remainder, 27% have remissionslasting six months to three years and 21% have attacks more frequently than six monthly.2
Atopic asthma in childhood is therefore associated with a relatively good prognosis.Among 880 UK adults aged 23 who had reported asthma or wheezy bronchitis from birthto age seven, 81% reported no further asthma or wheezing after their 16th birthday. Eightpercent, free of these symptoms between 16 and 23, reported wheeze at the age of 23.Relapse at 33 was more common among current smokers and atopic subjects. The riskfactors for a recurrence in, or persistence through, to adulthood are severe or frequentchildhood asthma, early onset, disturbed lung function in childhood, co-existing eczemaand cigarette smoking3 4 5 6. Despite improvement in symptoms, it is widely held thatalthough bronchial hyper-responsiveness improves to the point that the asthma seems tohave disappeared, the airways remain vulnerable in adult life7 with a potential recurrenceof symptoms in middle age as a result of the ageing process, disease and smoking.
Occupations which routinely expose the person to irritant or volatile chemicals, strenuousexertion, heat and smoke should be avoided by people with a clear history of severe ormoderate childhood asthma – and certainly by those with current asthma. It should beremembered that although successful treatment may abolish almost all asthmaticsymptoms, such a situation does not mean that the individual no longer has asthma.Studies have shown that the wearing of respiratory masks and BA sets may precipitateasthma attacks because of the challenge of cold dry air8. Under these circumstancesimmediate treatment could be necessary and the removal of a BA set for treatment is notan option in a hostile environment. The wearing of BA sets or respiratory masks shouldtherefore be avoided in those known to be currently asthmatic or at risk ofrecurring asthma.
A history of childhood asthma which appears to have gone into remission should notautomatically bar an applicant from becoming a firefighter if the asthma was mild, wentinto remission before 16 years and there is no residual loss of function on spirometry.‘Remission’ should be defined as an absence of asthmatic symptoms for 4 years sincecessation of anti-asthma medication, in line with HM Forces requirements owing to theknown requirement to wear respirators and be exposed to an ever changing environment.Medical history in such cases is very important, and where a consultant respiratoryphysician is of the opinion that the individual has a significant risk of asthma theindividual should not be exposed to the risks associated with firefighting. Where there isless certainty, all such individuals will require spirometry and some form of bronchialchallenge (see below).
It should be remembered that due to the variable nature of the disease, spirometry isfrequently normal in asthma and is therefore an insensitive measure of either diagnosis orseverity. Bronchial reactivity testing, using non-specific agents such as histamine ormethacholine, is performed in most district hospitals but is unlikely to be done routinely.A small proportion of people have increased bronchial reactivity on such testing but areand have always been asymptomatic and would therefore not be regarded as havingasthma. The results of such tests should therefore be considered only in the light of anappropriate medical history. A number of fire services have local arrangements for this test.
Exercise testing relies on the fact that exercise is a common trigger for asthmaticsymptoms9 and has been used successfully by the British Army since 1997. The BritishArmy exercise test involves repeat spirometry after the individual has exercised to 80%

Respiratory problems
4-5
maximum heart rate (see box). This mechanism is useful as it identifies those who choosenot to declare a history of asthma. Of 80 army applicants who had not declared previousasthma but who had a low peak expiratory flow rate (PEFR) on routine testing, 50%subsequently failed the exercise challenge10. The test should be interpreted with the samecare as for the pharmacological methods described above.
Adult Onset Asthma
Adult onset asthma is bronchial hyper-reactivity developing after the age of 20 years in theabsence of a history of atopy. Many individuals subsequently develop eczema or show othersigns of atopy and so a significant proportion is believed to be previously undiagnosedatopy – or atopy in remission. The management is as for atopic asthma and theoccupational considerations are the same.
True adult onset with no features of atopy should raise the question of OccupationalAsthma, and a careful occupational history will need to be taken. Reactive AirwaysDysfunction Syndrome (RADS) is an asthma-like bronchoconstriction which occurs as aconsequence of exposure to irritant gases, fumes and vapours. Applicants with a history ofRADS should be treated as if they have asthma. Some studies consider many sufferers asbeing originally asthmatic, with the chemical stimulus providing the necessary trigger for arelapse11. Serving uniformed fire personnel with RADS should not be exposed to smoke orfumes, so the development of this condition in a firefighter warrants careful investigationand may necessitate redeployment12 13 14 15.
The control of asthma by the use of prophylactic medication is usually compatiblewith normal work in a range of occupations. Caution should still be exercised wherethe occupation will expose the individual to possible irritants and asthma precipitants,including the breathing of pressurised dry air. When the asthmatic tendency is known tothe employer, the employer’s duty of care is enhanced and it is both appropriate andlegitimate to refuse to employ the individual in such a capacity16.
Exercise testing for asthma
• Ask all applicants about asthmatic symptoms and check all applicants PEFR.
• If there is a history of asthma, or recorded PEFR is more than 75l/min belowpredicted PEFR refer for exercise testing
• Measure FEV1, FVC and PEFR at rest
• Exercise on treadmill until applicant reaches 80% maximum heart rate, then stop
• Repeat spirometry at 1, 5, 8, 10 and 12 minutes post exercise
• If FEV1 falls by >15% of pre-exercise level (typically at 8 minutes post exercise),there is a residual asthmatic tendency

Fire and Rescue Service: Draft Medical Guidelines – June 2004
4-6
Obstructive lung disease
Obstructive lung disease is characterised by airways obstruction which is mainlyirreversible. There is disease of the airways plus or minus a varying degree of emphysema.Cigarette smoking is a major cause. Symptoms are those of cough, shortness of breath onexertion and sputum production. Pulmonary function tests show the ratio of FEV1/FVCusually less than 60%, although initially the symptoms of chronic bronchitis may bepresent without such significant reduction in lung function. Cessation of smoking will helpto arrest deterioration and ‘No Smoking’ policies should be encouraged in the Fire stations.
Anyone who is developing obstructive lung disease is likely to have difficulty inmaintaining the fitness required as an active firefighter. They will be increasingly short ofbreath on exertion and serial lung function tests will show deterioration. FVC is usuallyunaffected however FEV1 is reduced and the total time of expiration is increased. Whereobstructive lung disease is suspected, FEF 25% -75% should be measured and a significantreduction from the predicted value would confirm an obstructive pattern and shouldwarrant referral. This is frequently seen in long-term smokers. Smokers should be warnedif this is noted on routine testing and given every help to stop smoking.
Obstructive lung disease is unlikely to be a problem in recruits. This will alert observersto early changes in airways resistance. If routine lung function tests show an FEV1/FVCpercentage less than 60%, such lung function is generally incompatible with firefightingduties. These individuals are likely to have difficulty meeting the physical requirements ofoperational firefighter training.
It is advisable to refer to a specialist respiratory physician for a full assessment, includingpermeability and reversibility before any permanent decision on employment is made.Acute infections can produce a marked transient deterioration in lung function. Airwaysobstruction may be partially reversed by bronchodilators but the possible acute effects ofexposure on compromised lungs must be considered.
Acute effects of smoke inhalation
Acute smoke inhalation will result in pneumonitis and may result in pulmonary oedemarequiring ventilation. Subsequent management should include assessment for RADS.
Chronic effects of smoke inhalation
It has been suggested for many years that the conditions under which firefighters workmight cause permanent lung damage. Most longitudinal studies in firefighters have failedto show any long term deterioration in lung functions when smoking was allowed forcompared with other groups of workers17 18 19 20. In a study of firefighters in 1991 deathsfrom all types of respiratory disease, including growths occurred less often than expected21.This is perhaps surprising given the potential exposure of the firefighter to organiccarcinogens and asbestos. One small French study does show some long-term deteriorationin small airways function and decrease in permeability22.

Respiratory problems
4-7
These abnormalities were worse in firefighters who smoked. The study suggests thatmonitoring lung function in all professional firefighters is necessary. The routine lungfunctions carried out now under recommendations in Fire & Rescue Service Circularsshould give valuable information and be a safeguard to their health.
Restrictive lung diseases
Conditions giving rise to a restrictive pattern of lung disease are much rarer than thoseproducing obstructive lesions but in general are likely to have more serious consequences.Restrictive lesions affect the lung tissue itself, interfere with gaseous exchange and makethe lungs stiffer. They can occur in acute or chronic forms and the main symptom isbreathlessness. Lung function tests show a reduced FVC with no evidence of airwaysobstruction and more sophisticated tests will show a reduced transfer factor withdecreasing compliance and decreased oxygen levels in the blood.
Although firefighters may be exposed to a variety of substances that can cause restrictivedisease as a result of secondary occupation or hobbies, the only exposure of significancein firefighting is to asbestos. Firefighters would normally use BA on the fireground whenexposed to smoke or fume and therefore significant asbestos exposure is very rare. Thereis a greater risk in fire investigation where significant dust is present. There is no statutoryrequirement for health surveillance following asbestos exposure in firefighters and noclinical justification for implementing any surveillance. As there is a known link betweensmoking, asbestos exposure and the development of restrictive lung disease and tumours,firefighters should be given advice and support to help stop smoking.
Although most causes of restrictive disease are chronic, sarcoidosis frequently resolvesspontaneously over a period of 12-18 months. Any redeployment may therefore betemporary unless the condition becomes chronic.
Any condition affecting gaseous exchange is likely to be incompatible with firefightingduties. All cases of firefighters suffering with restrictive lung disease will need regularmonitoring. It should be remembered that oxygen saturation may fall markedly on exertionwhen showing almost normal levels at rest.
Spontaneous pneumothorax
It is not generally possible to predict susceptibility to spontaneous pneumothorax. There isa need for careful rehabilitation after the initial episode. A return to full duties with liftingand carrying should be delayed for at least three months. Any recurrence should be fullyinvestigated in order to exclude bullae when pleurodesis may be required.
Pulmonary embolism
Any recommendation to employ an individual with a history of pulmonary embolismdepends on the underlying medical condition that led to thrombosis and embolism.Information on occupational issues of anticoagulation will be found in the section onthe cardiovascular system.
Once individuals have stopped taking anticoagulants, fitness for employment depends onthe lung function and any other underlying conditions.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
4-8
Growths in the lung
Benign Growths
Benign growths of the lung are rare and after resection it is likely that a firefighter will beable to continue normal duties.
Malignant Growths
Even if a satisfactory resection is possible and sufficient pulmonary function remains, greatcare should be taken before returning individuals to active duties. There is a high risk ofmetastasising to the brain giving rise to the possibility of sudden haemorrhage andunconsciousness or epilepsy.

Respiratory problems
4-9
References
1 Sheth KK. Activity-induced asthma. Pediatr Clin North Am. 2003 Jun;50(3):697-716.
2 Blair H. Natural history of childhood asthma. 20-year follow-up. Arch Dis Child. 1977Aug;52(8):613-9.
3 Dierkes-Globisch A, Merget R, Baur X. Prognosis of bronchial asthmaVersicherungsmedizin. 1998 Apr 1;50(2):50-4.
4 Kjellman B, Hesselmar B. Prognosis of asthma in children: a cohort study intoadulthood. Acta Paediatr 1994 Aug;83(8):854-61.
5 Kokkonen J, Linna O. The state of childhood asthma in young adulthood. Eur Respir J.1993 May;6(5):657-61.
6 Strachan DP, Butland BK, Anderson HR. Incidence and prognosis of asthma andwheezing illness from early childhood to age 33 in a national British cohort. BMJ. 1996May 11;312(7040):1195-9.
7 Morris-Owen R. The natural history of asthma. In Lane DJ (ed) Respiratory Disease.New York; Appleton Century Crofts. 1976
8 Eschenbacher WL, Sheppard D. Respiratory heat loss is not the sole stimulus forbronchoconstriction induced by isocapnic hyperpnea with dry air. Am Rev Respir Dis.1985 Jun;131(6):894-901.
9 Feinstein RA, LaRussa J, Wang-Dohlman A, Bartolucci AA. Screening adolescentathletes for exercise-induced asthma. Clin J Sport Med. 1996 Apr;6(2):119-23.
10 Gemmell IMM, Robertson F. Exercise Testing for Asthma in Army Selection. Submittedfor publication 2003.
11 Bardana EJ Jr. Reactive airways dysfunction syndrome (RADS): guidelines for diagnosisand treatment and insight into likely prognosis. Ann Allergy Asthma Immunol.1999Dec;83(6(2)):583-6.
12 Brooks S M. Reactive Airways Syndromes. Journal of Occupational Health & Safety.June 1992;8(3);215-220.
13 Brooks S M et al. Reactive Airways Dysfunction Syndrome. Chest 1985;Sep 88(3):376-84.
14 Cohen M A. Inhalation of products of combustion. Ann Emerg Med 1983Oct;12(10):628-32.
15 Fogarty P W et al. Long term effects of smoke inhalation in survivors of the King’s Crossunderground station fire. Thorax 1991 Dec;46(12):414-8.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
4-10
16 Coxall v Goodyear [2002] EWCA Civ 1010; [2002] TLR 335 CA.
17 Musk A.W Pulmonary functions in firefighters: a six year follow up in the BostonFire Department. American Journal Industrial Medicine 1982;3(1):3-9.
18 Shephard D et al. Acute effects of routine fire fighting on lung functions. AmericanJournal Industrial Medicine 1986:9(4):333-40.
19 Douglas D B et al. Pulmonary function of London firemen. British Journal IndustrialMedicine 1985 Jan;42(1):55.-8.
20 Horsfield K et al. Lung function in West Sussex firemen – a four year study. BritishJournal Industrial Medicine 1988 Feb;45(2):116-21.
21 Beaumont J J et al. An epidemiological study of cancer and other causes of mortality inSan Francisco firefighters. American Journal of Industrial Medicine 1991;19(3):357-72.
22 Barthelemy L et al. Abnormalities of respiratory function in civil defence firefighter-submarine divers. Rev Pneurnol Clin 1990;46(6):271-6.

CHAPTER 5
Problems with the nervoussystem and special senses


Problems with the nervous system and special senses
5-1
CHAPTER 5Problems with the nervous system andspecial senses
CONTENTS
INTRODUCTION 5-3
EPILEPSY 5-3
Febrile Convulsions 5-3Childhood Epilepsy Syndromes 5-4Major Generalised Epilepsy 5-5
BRAIN INJURY 5-6
Head Injury 5-6Cerebral Palsy 5-6Cerebrovascular Accident 5-6
DEGENERATIVE NEUROLOGICAL DISEASE 5-7
Multiple Sclerosis 5-7Motor Neurone Disease 5-7Parkinson’s Disease 5-7
PROBLEMS WITH VISION 5-7
Introduction 5-7Contrast Sensitivity, Snellen And LogMAR Charts 5-8Status Of These Guidelines For Vision 5-8
REFRACTIVE ERROR 5-9
Myopia 5-9Hypermetropia 5-11Astigmatism 5-11Keratoconus 5-11
REFRACTIVE SURGERY 5-12
Radial Keratotomy and Astigmatic Keratotomy 5-13Laser Refractive Surgery 5-14Presbyopia and refractive surgery 5-18Wavefront Guided Laser Refractive Surgery (customised ablation) 5-18Night Vision And Contrast Sensitivity Following Laser Surgery 5-18Assessment After Refractive Surgery 5-19

Fire and Rescue Service: Draft Medical Guidelines – June 2004
5-2
COLOUR DEFECTS 5-20
Types of colour defect 5-20Acquired colour defects 5-20Effect of Colour Deficiency 5-21Colour Defect Screening 5-21Standards for Colour Vision 5-22Visual Field Defects 5-23Age Related Disorders 5-23
HEARING STANDARDS FOR FIREFIGHTERS 5-23
Introduction 5-23Reduction in Hearing Ability During Employment 5-23Hearing Requirements in the Service 5-23Selection of Appropriate Standards 5-24Summary of standards 5-25Investigating Hearing Loss 5-26Tinnitus 5-26
REFERENCES 5-27
AUTHORS:
Dr Catherine Chisholm BSc (Hons) MCOptom, Research Fellow, Applied Vision Research Centre,City University.
Mr David Gartry MD FRCS FRCOpth, Consultant in Ophthalmology, Moorfields Eye Hospital.
Dr Ian Gemmell MB ChB MSc MA(Law) MFOM, Consultant Occupational Physician,Employment Medical Services Ltd.
Mr Ben Lawton MSc DiplAud MIOA, Institute of Sound and Vibration Research, University ofSouthampton.
Professor Simon Shorvon MA MD FRCP, Institute of Neurology, Queens Square, LONDON.WC1N 3BG.

Problems with the nervous system and special senses
5-3
Introduction
Neurological disease may have an adverse impact on an individual’s career in terms of:
• Mobility
• Risk of sudden incapacity
• Cognition – including the perception of danger
• Communication – expressive and receptive
• Special senses.
There may be an increased tendency towards sickness absence and a heightened risk that afull career term will not be completed.
The assessment of an individual requires each of these areas to be reviewed with regardto knowledge of the severity of the disorder and its likely rate of progression or resolution.There may be profound health and safety concerns in relation to firefighters but relativelyfew concerns in other areas of the Service. Whilst this may preclude working as a firefighter,it does allow for firefighters affected by neurological disease to be retrained into other roleswith or without reasonable adjustment.
Epilepsy
The term epilepsy covers conditions which may lead to a sudden disturbance inconsciousness. Three broad topics will be discussed here; febrile convulsions, childhoodsyndromes and major generalised epilepsy.
A risk assessment should be made in each individual case, based on a report from aspecialist. It is essential to consider the long-term history of the condition in relation toperiods of pressure or stress, and shift work as well as the response to medication. Wherethe risk is considered low it may be safe for these individuals to undertake operationalfirefighting. Individuals should have been fit-free for at least one year, with a low risk inrelation to the pressures of work. Any changes in medication should be accompanied by asuitable period away from operational firefighting to ensure the individual remains fit-free.
Febrile Convulsions
Generalised convulsions are more common in the first five years of life than at any othertime. Febrile convulsions occur in 3% of children and demonstrate an idiopathic susceptibilityto convulsions. There is a genetic component. They are rare below the age of six monthsor above the age of five years. About 90% of febrile convulsions occur within the first 24hrs of a febrile illness, typically when the rate of temperature rise is greatest.
When assessing the likelihood of brain damage and susceptibility to adult epilepsy, the ageof the child at the time of the febrile convulsion is important. Convulsions in the youngerchild tend to be more damaging. The chance of a severe seizure (longer than 15 minutes)falls after the age of two.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
5-4
The risk of epilepsy amongst children who have not suffered a febrile convulsion is 0.5%1.The incidence of epilepsy following febrile convulsion ranges from 5-10% and the epilepsygenerally appears by the age of seven years2.
Convulsions associated with a febrile illness after the age of five years have the samesignificance as a non-febrile convulsion and carry a 16% risk of late onset epilepsy3.
It is difficult to justify precluding an individual from a particular uniformed role for whatmight become a problem, based on an event many years previously. The vast majority ofearly febrile convulsions that result in epilepsy do so by the age of seven. An individualwith a history of febrile convulsions but clear of epilepsy by the age of 25 should be viewedas having the same risk as the general population. A history of multiple or severe febrileconvulsions may warrant delay in recruitment until after the age of 25.
A history of late onset febrile convulsion with or without residual brain damage should beviewed with extreme caution in relation to safety critical roles. Advice from a specialistshould be sought, and careful consideration given to the effectiveness of treatment and theoverall risk of an event at work.
Childhood Epilepsy Syndromes
Childhood absence epilepsy (petit mal)Childhood absence epilepsy, formerly known as ‘petit mal’ is an interruption ofconsciousness typically occurring between 5-12 years of age and frequently precipitated byhyperventilation. It is generally benign and resolves spontaneously although there is adistinction to be made between simple absences seizures and absences occurring as part of atemporal lobe epilepsy.
Some researchers have shown that up to 56% of children with absence seizures continue tohave attacks after the age of 21 years4 although most put the prevalence at a much lowerfigure. Livingston found that of 15,000 children with epilepsy, only 2.3% had ‘pure’ petitmal. Of those children with the ‘pure’ form, 92 of 117 patients followed up ceased to haveeither EEG abnormality or seizures by the time they were 20 years and only 17 childrencontinued to have absence seizures in adulthood. However, of those 100 children whorecovered from ‘pure petit mal’, 54 developed grand mal epilepsy in adolescence oradulthood, particularly if the onset of petit mal occurred after the age of ten years5. Rogeralso found an unfavourable prognosis if the onset was after the age of ten years or beforethe age of five, with an overall favourable result in 48% of patients studied6.
Benign Focal Epilepsy (Rolandic or Sylvian Epilepsy)Benign Focal Epilepsy, also referred to as Rolandic or Sylvian Epilepsy, is a partial epilepsywhich originates in the same well defined area of the brain. The manifestation may besimple or quite complex and it is the commonest partial epilepsy of childhood, accountingfor up to 16% of childhood epilepsy.
Simple focal epilepsy is usually motor, with conservation of consciousness, although somepatients suffer from somatosensory changes as well. These changes may be confused withan aura of a complex partial seizure (temporal lobe epilepsy).

Problems with the nervous system and special senses
5-5
Onset is typically between five and ten years and rarely after 12 years. The conditionpredominantly affects boys and there is no neurological or intellectual deficit. Attacksoccur only during sleep in 75-80% of cases and the condition resolves spontaneouslyduring adolescence7.
There is a strong genetic component and most children with benign focal epilepsy recoverby their mid-teens and do not go on to develop any other form of epilepsy8. The incidenceof further seizures in this group is estimated at 2%9.
Complex Partial EpilepsyThis is amongst the commonest and most intractable forms of epilepsies. Its onset istypically before 20 years of age. The lesion may be in the temporal lobe but in somechildren the lesion is extra-temporal.
About a third of cases have a cause such as birth trauma, head trauma or meningitis.Another third have an identifiable severe seizure – such as a severe febrile convulsionwhilst the final third have no identifiable cause. There appears to be no genetic linkother than amongst those whose temporal lobe epilepsy followed a febrile convulsion.
Most complex partial seizures are generally paroxysmal, beginning and ending abruptly.Déjà vu phenomena and auditory and olfactory hallucinations are common as are changesin affect.
Exact incidence is difficult to quantify given the range of possible manifestations, but it isthought to range between 10-25% of all epilepsies of childhood. Chronicity is commonand the appearance of disturbing automatisms and degeneration of cognitive-intellectualfunction gives such epilepsy a poor prognosis. Patients with complex partial seizures tendto suffer more frequent attacks, require more drugs and suffer more psychosocial stress thanpeople with generalised seizures10. A follow up study in 1966 showed that 62% of personswith childhood temporal lobe epilepsy were dependant on others for all or part of theircare. In a more recent study, only 10% of sufferers managed on drug treatment alone werefree of seizures after 6 years11.
Neurosurgery may be indicated in some and this is usually carried out in children prior toadolescence so as to maximise their chances of learning during their school age. Any suchindividual applying for the Service in any operational or control role should be reviewedon the basis of function and the absence of seizures for ten years.
Major Generalised Epilepsy
Major Generalised Epilepsy includes grand mal epilepsy and is characterised by loss ofconsciousness. There may be tonic-clonic convulsions, a non-convulsive absence ormassive bilateral myoclonic jerks followed by a post-ictal state. It is the commonestepilepsy of childhood affecting about 80% of children with epilepsy, either alone or intandem with another form of epilepsy.
Primary grand mal epilepsy may occur at any stage of life but usually after the age offive years and before adolescence. There is a strong genetic component when the diseasestarts in early childhood and remission rates of over 90% have been reported in such cases.However, when absence attacks or other forms of epilepsy are present, or when the onset isin adolescence or later (secondary grand mal), the prognosis is not so good12.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
5-6
In general, primary grand mal epilepsy is the generalised epilepsy most likely to remit andleast likely to relapse later, although it may relapse even after a long period of remission.Secondary grand mal epilepsy however is a much commoner manifestation of childhoodepilepsy than are primary grand mal attacks. A family history is usually absent in secondaryepilepsy and the individual frequently has a history of partial seizures or severe febrileconvulsion. MR scans may show signs of structural brain lesions. Secondary epilepsies aremore likely to be resistant to anticonvulsant medication and they therefore carry apoor prognosis.
Brain injury
Head Injury
Head Injury affects approximately 250/100 000 people and most typically results fromroad traffic crashes or assaults. The peak incidence is amongst men in the 15-24 age group.The most common sites of injury are the frontal and temporal lobes thereby affectinghigher cognitive functions such as planning & sequencing, speech, hearing and memorytasks including recognition of colleagues. There may also be behavioural changes and someloss of motor co-ordination.
In general, whilst the primary causes of brain injury may last seconds and the secondarycauses hours or days, the extent of permanent damage will not become clear for 12-18months afterwards as repair and restoration of function take place. The vast majority ofhead injuries are minor and the individual suffers no long term consequence. Such personsmay be accepted or return to duty after between one and three months convalescence,depending on residual fatigue and executive function.
In major head injury, employability decisions should be reserved until at least 12 monthspost-injury. The decision should be based on which higher and lower functions have beenaffected. Occupational Health staff should obtain clinical reports including an educationalpsychologist’s report of cognitive ability and a careful assessment of functional capabilityshould be made by line managers.
Cerebral Palsy
Cerebral palsy affects approximately two per 1000 adults and leads to a wide range ofdisabilities. Each case must be assessed on its merits and relative weaknesses. Intellect,mobility, communication, behavioural concerns and the requirement for medication tocontrol spasms or epilepsy needs to be taken into account. Should employment be offered,all appropriate reasonable adjustments must be considered.
Cerebrovascular Accident
Strokes are relatively common after the age of 50 and about 60% of stroke victims haveresidual neurological signs. Like cerebral palsy, the range of disability following CVA isenormous, however, as few as 20% of sufferers eventually return to work13. The likelihoodof a return to work is dependent on the degree of functional loss and the onset of anxietywhich accompanies a profound loss of confidence.

Problems with the nervous system and special senses
5-7
Each case should be considered on its merits and the level of residual function, whilsttaking into account aggravating factors such as age, smoking, hypertension andpredisposing conditions. Recurrent episodes suggest a high risk of sudden incapacity. Theonset of epilepsy is a possibility as is further incapacity through a repeat episode. Thoseemployed in safety critical posts may therefore require removal from post andredeployment if possible. Shift work should be avoided following a stroke.
Degenerative neurological disease
An assessment of current function and the job characteristics must be carefully balanced inrelation to the likely rate of progression. The employer’s decision must take into accountHealth & Safety issues and may also include the cost of redeployment after five to ten years.
Multiple Sclerosis
Multiple Sclerosis affects between 50-125 people per 100 000. Its progression is usuallygradual and in one study there was a more than even chance of the individual remainingemployed 15 years after diagnosis, although transfer to sedentary occupations is normal14.Placement is clearly dependant on level of function, the frequency of relapses and levelof sickness absence. Loss of manual dexterity and visual problems are likely to have aprofound effect on employability and redeployment should be considered early.
Motor Neurone Disease
Motor Neurone Disease affects five per 100 000 adults. It typically affects those over 50but there are progressive forms which occur in younger age groups. Progressive weaknesspredominates and the early consideration of redeployment will prolong the working life ofthe individual.
Parkinson’s Disease
Parkinson’s Disease affects about 160 people per 100 000, typically striking after the age of45 years. The rate of progression and level of functional loss is not readily apparent and somanagement of each case must be on an individual basis.
Problems with vision
Introduction
The ability to resolve complex visual information depends on the receipt of good qualityoptical information, its transfer by the retina and processing and modification by the brain.Clearly disease or damage to the eye or the neural pathways and visual cortex will affect anindividual’s ability to ‘see’ in the fullest range of environments. The perception of animage depends on extrinsic factors such as size (visual angle), colour, contrast and the levelof illumination, and intrinsic factors such as visual acuity, colour perception and contrastsensitivity. Visual acuity and colour perception are discussed in some detail below.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
5-8
Abnormal vision may impact on:
• Reaction time
• Mobility
• Target/casualty recognition
• Information exchange
• Spatial awareness.
The assessment of an individual with poor vision requires an holistic approach with eachof these areas being considered, particularly in relation to health and safety. This maypreclude employment as a fire fighter yet enable the individual to be employed in firesafety or investigation.
Contrast Sensitivity, Snellen and LogMAR Charts
Contrast sensitivity is reasonably stable in 20-40 year olds but deteriorates slightly withadvancing age, certain forms of ocular pathology or in a minority (8-10%) of individualsfollowing corneal refractive eye surgery. This deterioration is unlikely to be of significancein most occupational settings, however it becomes significant amongst safety criticalworkers expected to work in conditions of poor visibility such as at night or in smoke. Thetesting of contrast sensitivity is therefore only recommended for firefighters with a historyof eye surgery or who develop eye disease.
Acuity is usually measured using a standard chart with black letters on a whitebackground. The Snellen chart is universally used, although the logMAR chart is moreaccurate because it has:
• several charts with different shading of letters to produce different contrast values
• geometrical progression in size between lines
• the same number of letters on each line to ensure the ‘crowding effect’ is the same oneach line
• Scoring letter by letter, improving repeatability and reliability
The standard Snellen chart has a contrast of 94% when correctly illuminated. The mostuseful additional contrast level to test is 10%. In the normal eye, one would expect a dropof approximately 3 lines of acuity on a 10% contrast logMAR chart compared to the 100%contrast logMAR chart.

Problems with the nervous system and special senses
5-9
Status of These Guidelines for Vision
Medical Advisers must appreciate that the information below represents guidelines onmedical aspects of vision. Managers may take a flexible approach appropriate to theirrequirements, particularly with retained firefighters, and will expect medical staff to adviseappropriately when assessing the fitness of recruits.
Refractive error
Refractive errors are predominantly due to mismatch between the axial length of the globeof the eye and the curvature of the cornea. The cornea is responsible for two thirds of lightrefraction and the lens plays a smaller (but important) part in image focussing.
Standards for LGV (Group 2) driving require the driver to have a normal binocular fieldwith an unaided acuity of 6/36 or better corrected to at least 6/9, 6/12 although this may intime be revised to 6/7.5 and 6/10 respectively15. The Group 1 standard equates to 6/10with both eyes together although the official test is the ‘number plate test’ which has noexact equivalent.
Myopia
Visually significant myopia affects about 20% of the UK population although it is morecommon in the Jewish population and people of Far Eastern origin16 and is becoming moreprevalent. The condition is often inherited and in the majority of cases is due to axialenlargement of the globe, manifesting itself in childhood or adolescence with progressivedeterioration until mid to late 20s. Subsequent deterioration and late onset myopia isusually much more gradual. In some, early acceleration may be related to excessive use ofnear vision in childhood and adolescence; prolonged near-vision activity is a commonfeature of studying in further education and in some occupations. The percentage of thepopulation with varying degrees of myopia is shown in the table below.
Myopia above a correction of -4.00D carries an increased risk of retinal detachment (dueto the elongation of the globe), primary open angle glaucoma and cataract. The risksincrease as the myopic prescription increases and above a correction of -10D there is alsoan increased risk of pigment dispersion syndrome, keractasia and serious complications ofrefractive surgery17 18.
% Population (unaided) % Population (aided)
6/12 93%
6/10 90%
6/9 87%
6/6 65% 89%

Fire and Rescue Service: Draft Medical Guidelines – June 2004
5-10
Good visual function in safety critical occupations enables vision to remain functionallyadequate for as long as possible in adverse environments where vision has beencompromised. Such environments include low light levels or where smoke and glareinterfere with image perception. Adding significant degrees of myopia (unaided visualacuity 6/12 or worse), astigmatism and severe hyperopia to this environment willsignificantly degrade the operational effectiveness of the individual. Consideration shouldalso be given to the risk of loss or damage to aids to vision, and the impact this would haveon safety.
Ninety percent of 20 year olds achieve Group 1 driving standard unaided. With largenumbers achieving such a high standard, there is no need to reduce visual standards forrecruiting purposes alone. The problem with myopia is that it advances at different rates atdifferent ages. The general pattern is a myopic shift of about 0.75D between ages 20-50 yrsfollowed by a hyperopic shift (~0.25D) thereafter. A firefighter aged 20 who is borderlinefor unaided vision may therefore advance over the next 5-10 years whereas a 30 yr oldwith a borderline vision probably won’t.
An example of a key distance vision task in firefighting could include the ability toidentify a gas cylinder at a distance of 20 metres. Such standards would be required at thescene of a fire where the need to go closer to identify the object would endanger thefirefighter. The situation also equates to casualty identification. It is recognised that thosewith ‘perfect’ vision who achieve 6/6 or higher will perform slightly better in this scenario.If this is regarded as critical to the performance as a firefighter, Services may be justified insetting higher standards at point of entry selection.
Those responsible for making this decision should bear in mind that individuals who havedeveloped mild myopia in early adulthood (18-22) perhaps corresponding to excessive nearvision while studying for higher education will be discriminated against if higher unaidedvision standards are set. The result would be a significantly lower proportion of graduatesrecruited to the Service. It should, however, be noted that most of these late onset myopeswill end up with -0.75 to -1.50D of myopia giving them 6/12 or worse unaided vision.
An unaided distance vision of 6/9 will generally achieve an acceptable standard of casualtyrecognition in adverse conditions, and is a reasonable level to set as the minimumrequirement for safety critical work.
Individuals who fail to achieve 6/12 aided visual acuity will probably fail to achieve thestandard for Group 1 driving and may have other difficulties in the working environment.It is important to determine whether they are capable of undertaking the required tasks,with or without reasonable adjustments. Specialist advice may need to be sought,particularly if there is a requirement to use specialist software; there could be compatibilityissues and other issues of capability for example with control room staff where additionaltime to undertake tasks may not be reasonable in this role.
Standards for myopiaIn summary, individuals with uncorrected distance acuity of 6/9 aged 22 or younger aremore likely to need to be redeployed later in life, while those over 22 should remain fit forfirefighting duties. Individuals failing to achieve a standard of 6/12 unaided are unlikely tomeet the required visual standards for safety on the fireground.
Individuals must meet a corrected visual acuity standard of 6/12 or better to be safe onthe fireground.

Problems with the nervous system and special senses
5-11
Hypermetropia
Long sightedness or hypermetropia is more common than myopia and affects about 40% of20 year olds. The mode for refractive error in the population is about +0.25D. Most peoplewith low grade hypermetropia are able to focus to correct for this by accommodatingwithout the need for corrective lenses. Those with higher hypermetropia may also be ableto focus for distance but by using some of their accommodative reserve to overcome theirhypermetropia, they may run out of focussing power for near vision.
The measurement of near vision is a relatively new concept for the Service and derivesfrom the requirement to read a BA set contents gauge at a distance of 33 cm. This equatesto reading N12 letters at 33cm. Although it would be possible to alter the gauge to enablethose with worse near vision to read it, there are a number of other tasks firefighters haveto undertake, such as adjusting the frequency on their radio sets, reading a variety ofinstructions and checking equipment, where a higher standard of near vision acuityis required.
Measurement of a population of UK Firefighters demonstrated that 80% achieve a nearvision acuity of N5 and only 3% had a near vision acuity at 33 cm of N14 or worse. Theproblem is compounded with age with the onset of presbyopia (difficulty focussing on closework with age due to loss of accommodation). Although individuals with hypermetropiamay have sufficient accommodation to overcome their hypermetropia and focus forreading when young, they will require reading spectacles at an earlier age than average.Difficulty with small type rarely develops before the age of 40 in individuals with perfectsight, while a study showed that 60% of a population of fire fighters aged 38 wereaffected19.
The 2002 entry standard of requiring the individual to read N12 at 30 cm is the absoluteminimum standard for reading the BA set gauge yet no allowance for age relateddeterioration is made. The standards for hypermetropia are therefore more generous thanthe standards for myopia as there is a significant risk that a hyperopic 25 year old who canaccommodate and read N12 letters at 30 cm may be unable to use a BA set safely 12-15years later without correction.
A more appropriate standard for near vision acuity on entry for those under 25 would bebilateral N6 at 30 cm, to allow for some deterioration. N6 also equates to the standardrequired to read the dial on a radio set, enabling all firefighters to adjust their own radiofrequencies without assistance20.
StandardsIndividuals who have vision worse than N8 have a significant reduction in capability,particularly in an emergency situation and those who cannot achieve N8 corrected mayneed redeployment later in their careers. Individuals should meet an uncorrected near-vision standard of N12 and must meet a corrected standard of N12 to be safe onthe fireground.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
5-12
Astigmatism
Astigmatism affects 33% of the population and is corrected by the use of cylindricallenses. Simple astigmatism occurs where the image from one meridian falls correctly onthe retina while the image in the opposite meridian does not. Compound astigmatism iswhere neither foci falls on the retina and the refraction is either wholly myopic or whollyhypermetropic. Mixed astigmatism is where one image is in front and the other behind theretina so that correction is myopic in one axis and hypermetropic in the other. Eye strainmay occur with small uncorrected errors and blurred vision from larger errors. Those withcompound astigmatism should be carefully assessed for capability, and particularly for ahistory of headaches and eye strain that could affect safety.
Keratoconus
Keratoconus is a steeply curved and thinned cornea which adopts the shape of a cone dueto corneal thinning. It is a progressive condition which leads to high degrees of myopiaand astigmatism and is poorly corrected. During progression there is a requirement forregular alterations of lens prescription, and there are a number of serious potentialcomplications including corneal rupture; these may be resolved by corneal grafting, andspecialised contact lenses may help. Individuals with keratoconus are at high risk fromtrauma as well as from poor vision and should generally be considered unfit forfirefighting duties.
Refractive surgery
The cornea is responsible for two thirds of the refractive power of the eye, so minorchanges to its structure can significantly affect visual function. Various surgical techniqueshave been available for the past thirty years or so to correct vision and avoid or reduce therequirement to use glasses or contact lenses. There have been considerable advances intechnique including the now widespread use of lasers. The main risks involve aberrantvisual function caused by scarring or irregular structural defects within the cornea andrarely weakening of the corneal structure.
Refractive surgery does not alter the underlying structure of the eye. Individuals who are atgreater risk of eye pathology such as retinal detachment because of abnormal eye shape(high myopia) will remain at risk. In the past they would not have been selected forcertain employments where this risk would be important because of poor unaided vision. Itis important to determine whether there are other risk factors in these individuals whenadvising on their overall fitness for employment in the Service.
An individual who has undergone correction for refractive error remains at risk ofunderlying pathologies such as cataract, glaucoma and retinal detachment. The greater isthe pre-operative refractive error, the greater is the risk of these diseases.
A significant amount of information is covered below, both to allow Medical Advisers toassess the risk to individuals who have already had one of the procedures, and to allowadvice to be given to individuals and management on the predicted outcome. Individualsshould also expect detailed advice from the ophthalmic surgeon on prognosis; the use ofoverseas ‘cheap offers’ where preliminary advice may not be available and the outcomemay not be so predictable is not advisable.

Problems with the nervous system and special senses
5-13
The wide variety of treatments currently available reflects the early stages in developmentof this important surgical capability. It is likely that evidence will lead to fewer techniquesdominating, when guidance for employability will be much clearer and much moreconcise.
Personnel being considered following refractive surgery must have obtained a good resultfrom the procedure (better than 6/12 uncorrected) if they are to operate without anyrestrictions in safety critical work or where lighting conditions may be less than optimal.Entry should not be considered until 12 months post surgery to allow for stabilisation.
The following assessments should be performed on personnel who have undergonerefractive surgery and who may be involved in safety critical work21.
Radial Keratotomy and Astigmatic Keratotomy
These are invasive procedures which involve making incisions through 95% of the corneallayers leaving a central untreated area of 3-4mm in diameter (can be even smaller). Theincisions weaken the periphery, causing it to bulge, resulting in a relative flattening of thecentral cornea and a reduction in myopia. Astigmatism can be treated by placing incisionsalong just one of the principle meridians or arcuate incisions close to the limbus.
Permanent radial corneal scars are visible following this procedure and in a small numbermay overlap the pupil when dilated under low illumination. Side effects include mistingand halos, particularly in the periphery and at night. Image distortion may also be due toirregular astigmatism that has not been corrected by this procedure.
In addition, because the surgical procedure disrupts so many of the corneal layers, thecornea is significantly weakened against blunt trauma. A serious but rare complication ofradial keratotomy is a 2.2% risk of corneal rupture. One study reported three casesoccurring more than ten years after RK22. Another study considered 28 eyes that hadruptured after RK and attributed seven cases to assault, four to sport injuries, five to carcrashes and 12 to ‘daily living’23.
The PERK study ran in the United States from 1980-1985 and studied the effects of RKon 793 eyes. The study found that 53% of eyes achieved 6/6 or better unaided at 6 monthsand 85% achieved 6/12 or better after 10 years.24 The procedure is more accurate andreliable for lower degrees of myopia (62-84% of < -4.5D patients achieving emmetropia +/-1 D). Only 38% of higher myopes (-4.50 to -8.00D) achieved emmetropia. Long-termstability of the result has been questioned following the detection of a drift towardshyperopia in 43% of eyes after ten years.
Pre-OpCorrection Post Operative
Uncorrected Corrected Contrast Corneal Night Vision Stabilityvision visual acuity Sensitivity clarity
<-6.00D 6/12 or better 6/9 or better < 2 lines No central No glare, <0.5 D changeor in each eye difference at scarring or halos or in 2<+4.00D 10% contrast opacity seen scatter. assessments
from high on slit lamp six monthscontrast. exam. apart.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
5-14
A common complication is a diurnal fluctuation in refractive error and hence visualacuity25. Along with other forms of refractive surgery, RK can cause a reduction in thequality of vision due to an increase in forward light scatter and corneal aberrations leadingto reduced contrast sensitivity26. This is more marked in low lighting levels, leading tocomplaints of glare and problems with night vision. Radial keratotomy is hardly everperformed today because of the risk of rupture, the drift towards hypermetropia andadvances in excimer laser technology. Ongoing glare disability is cited as the main reasonfor exclusion from work as flight deck air crew27 28.
Laser Refractive Surgery
This involves the use of an ultraviolet argon fluoride gas discharge laser, the ‘excimerlaser’, to remove minute layers of superficial corneal tissue under computer control.
Photorefractive Keratectomy (PRK)This was the original excimer laser refractive surgical technique. PRK can be used to treatmyopia, astigmatism or hypermetropia. When treating myopia, more tissue must beremoved from the centre of the cornea than the periphery to produce a flatter profile. Theamount of tissue removed for low myopia is in the region of approximately 50?m – lessthan 10% of the overall corneal thickness. The treatment of astigmatism involves greaterablation of one principal meridian than the other. Hypermetropic treatments attempt tosteepen the optically significant central cornea by producing a smoothly transitionedannular ablation in the stroma at the periphery of the 5-6mm central optical zone.
Vision remains poor for 3-6 days until the epithelium has healed over the treated area29.Unlike radial keratotomy, PRK involves treating the centre of the cornea thereforechanges in corneal clarity are of concern. A sub-epithelial opacification referred to as‘haze’ develops over the first 2-3 months but this subsides by approximately 12 months30 31.This may not resolve completely in every case however, and traces of corneal haze can beseen many years after PRK.
As with radial keratotomy, PRK is more successful for lower degrees of myopia (<-6.00D),where 88-99% achieve uncorrected vision of 6/12 or better and 58-78% achieving 6/6 orbetter by 12 months32 33. For higher degrees of myopia (>-6.00D), 68-74% achieve 6/12 orbetter but only 26% obtain 6/6 at 12 months. Enhancement procedures can be performedbut predictability is not as good as for the initial procedure. Regression (a gradual partial orcomplete return to the myopic state) is a common complication of PRK with 10-20%requesting a repeat PRK procedure. A deliberate overcorrection by 50% reduces thechance of further regression; however individuals with a regression beyond -3.50 dioptresand who have significant anterior stromal haze show a poor response to furthertreatment34. PRK is now restricted to the treatment of myopia up to about -4.00D.
The results for astigmatism are slightly less accurate than those for myopic PRK since theaxis alignment is critical and there are variations in meridional wound healing with greaterregression occurring in the meridian of greater tissue loss35. Only a limited number ofpatients with high cylinder correction achieve 6/1236 and some patients are worsened bythe technique.37

Problems with the nervous system and special senses
5-15
Photo Astigmatic Refractive Keratectomy (PARK)PARK was developed after PRK and is used to treat astigmatism. The results are lessaccurate than those for myopic PRK since the axis alignment is critical and there arevariations in meridional wound healing with greater regression occurring in the meridianof greater tissue loss38. Only a limited number of patients with high cylinder correctionachieve 6/1239 and some patients are worsened by the technique.40
Hypermetropic PRKHypermetropic PRK is more predictable for lower refractive errors (<+3.50D) 41 however,stabilisation of the refractive error can take up to 12 months42 and the risk of losing two ormore lines of best-corrected visual acuity is greater than for myopic treatments43.
Post operatively, forward light scatter increases and peaks at around three months beforereturning to normal levels comparable to spectacle wearers by 12 months44. There isevidence to suggest that the distribution of light scatter around the retinal image ispermanently modified by PRK, with an increase in the spread of stray light leading to areduction in retinal image contrast45. Studies indicate that visual performance under lowillumination when the pupil is dilated (and aberrations are greatest), may be compromisedfor a year or more, particularly for low contrast tasks and amongst high myopes46.
Unlike RK, diurnal variations in refractive error post-PRK are not clinically significant47
and neither hyperbaric nor hypobaric conditions cause corneal deformation or a refractiveshift48. Studies have indicated that ocular integrity is not significantly compromisedfollowing PRK49.
Laser Assisted In-Situ Keratomileusis (LASIK)LASIK was developed in the early 1990s. It involves the use of a microkeratome to cut athin flap of superficial corneal tissue followed by ablation of the underlying stroma. Theflap is then repositioned and is held in place by surface tension and strong osmotic forcesuntil the epithelium heals over the peripheral annular wound margins. The aggressivewound healing that occurs following PRK is not seen post-LASIK because of limiteddisruption of the corneal epithelium and so haze production is minimized, allowing higherrefractive errors to be corrected. Post-operatively, a C-shaped ring is visible although thisfades with time.
Retreatment following LASIK is possible and involves lifting the initial flap and re-ablating the stromal bed. The time course of corneal healing post-surgery means that theflap is more easily lifted in the first 12 months after the initial procedure. LASIK is nowthe most popular refractive surgery technique in both Europe and USA, accounting for inexcess of 95% of all laser refractive techniques and in excess of 90% of refractive surgeryin general.
The percentage of eyes achieving 6/12 vision or better has been quoted as 86-100% at 6months post-LASIK for corrections of -8.00D or less50. The refraction tends to stabilisewithin 1-3 months and less than 2% of eyes treated for myopia <-6.00D lose two or morelines of best corrected visual acuity. Recovery is rapid, with most patients seeing well thefollowing day and the majority returning to work within a few days. Most experiencedLASIK surgeons will therefore treat both eyes at the same time.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
5-16
Hypermetropic LASIKHypermetropic LASIK has proved slightly more successful than hypermetropic PRK forthe correction of low hypermetropia with 80% of eyes achieving 6/12 or better51. Anunacceptably high percentage of patients treated for hypermetropia of greater than +4.00Dlose two or more lines of best corrected acuity (7.3%)52.
The majority of surgeons restrict LASIK treatment to refractive errors between +4.00 and -10.00D due to the reduction in accuracy and increased risk of complications53. The vastmajority of complications manifest within the first 6-8 weeks. Surgeon experience is a keyfactor in the initial outcome.
Ocular integrityThere have been questions raised about the integrity of the globe post-LASIK, however, astudy examining the integrity of the globe following a range of different refractive surgeryprocedures concluded that although LASIK eyes required slightly less energy to rupturethan control eyes, the difference was not statistically significant54 55. Because the ablationtakes place within the cornea, LASIK requires sufficient corneal thickness to prevent theablation encroaching within 250µm of the endothelium. If this does occur there is a risk ofkeratectasia – a rare but serious condition that may not present for a year or so post-surgery(mean of 1 year +/- 0.3)56. The induced corneal thinning leads to protrusion of the cornealtissue, severe irregularity and a reduction in visual performance. It is almost alwaysassociated with treatment for high myopia57.
The risk of the flap being dislodged is very low although there have been reports of flapdamage as a result of focal trauma at 6 months. A good visual outcome was achieved onflap repositioning.58
Laser epithelial keratomileusis (LASEK) and EpiLASIKLASEK is a relatively new technique used for low myopia and hypermetropia, falling partway between PRK and LASIK. It involves the production of an epithelial flap using asolution of 20% alcohol which softens the attachment of the epithelium to the underlyingcorneal stroma allowing the epithelium to be moved in a continuous sheet to one side.The underlying anterior stroma is ablated, as in PRK, but the epithelial flap is thenreplaced, acting as a bandage lens to minimise post-surgical inflammation.
It is currently being used to treat low myopia, where it produces less haze than PRKand therefore better best-corrected visual acuity whilst it avoids the potential flapcomplications of LASIK. There is a rapid recovery of vision following LASEK; in onestudy of 222 eyes ranging from -1D to -11D, 98% achieved 6/12 unaided vision within twoweeks of LASEK and 63% achieved 6/6 unaided vision at one year59. EpiLASIK is verysimilar and about to become popular – the epithelium is removed using a keratome whichcauses less damage than alcohol.
The procedure appears to be safe since no eyes showed a reduction in best-corrected visualacuity despite the wide range of pre-operative myopia. Another study comparing LASEKwith conventional PRK for the treatment of -3D to -6.5D reported significantly lesscorneal haze following LASEK although there was no significant difference at 3 monthspost-surgery60. Some surgeons believe that LASEK will replace PRK in the near futurealthough others regard the corneal haze generated as unacceptable and the post-operativepain (which can last around one week) can be difficult for patients to tolerate. Oneindividual required a corneal graft in one eye after an otherwise routine bilateral LASEKprocedure (personal communication – DG).

Problems with the nervous system and special senses
5-17
Since photoablation is a relatively new technique (1990), the long-term side effects are asyet unknown. There appear to be no adverse effects on the corneal endothelium, whichcontrols the hydration of the cornea but one study detected prolonged biochemicalchanges in the crystalline lens of rabbit eyes amongst LASIK but not PRK treated eyeswhich may be the precursor to cataractogenic changes61. No increase in the incidence ofcataract has yet occurred.
Intrastromal rings (or intracorneal stromal rings)The curvature of the cornea can be modified to correct low levels of myopia (up to -5D)by inserting semicircular perspex rings in to the corneal stroma. This technique was neververy popular and is virtually obsolete.
Laser Thermokeratoplasty (LTK)A diode laser (DLK) or heated probe is used to cause localized scarring and thereforecontraction of stromal tissue in the midperipheral cornea. A ring of such ‘burns’ causessteepening of the central cornea and hence a reduction in low hyperopia (<+4D). Thisprocedure has recently received FDA approval as a temporary procedure; the effects tendto wear off after 2-3 years.
Intraocular refractive surgeryAlthough not commonly performed in commercial UK clinics, non-corneal refractivesurgery is also available. Such intraocular surgery is generally reserved for higher refractiveerrors that cannot be treated safely with corneal surgery, as too much corneal tissue wouldhave to be removed. Procedures include the insertion of an additional lens in to the eye(Phakic IOL) or lens extraction with lens implantation. Intraocular surgery carries aslightly higher risk of infection than corneal procedures and other possible complicationsinclude secondary glaucoma, cataract and uveitis.
A key factor of importance to recruitment is that corrected high myopes will still be at aslightly increased risk of conditions such as retinal detachment and glaucoma.
Phakic Intraocular lenses (PIOL) or implantable contact lensesAn additional lens is placed inside the eye to modify the refractive power of the eye.Lenses are available for placement in the anterior chamber, attached to the iris (iris-cliplenses) or in the posterior chamber. Although the results are relatively predictable and thecorneal shape is not modified (so aberrations do not increase), some individuals(particularly younger patients with large pupils) suffer from glare and halos at night due tothe small optic zone. PIOL are reserved almost exclusively for the correction of highprescriptions (>-10D, or >+4D).
Cataract extraction and clear lens extractionIndividuals with cataract and very high myopes and hypermetropes can achieve a goodrefractive outcome by simply having their crystalline lens removed and replaced with anartificial lens. Removal of the crystalline lens obviously removes the patient’s ability toaccommodate and therefore focus for near without spectacles. However, multifocalimplants are now available, although the quality of vision tends to be slightly reduced withsuch implants (reduced contrast sensitivity) due to the division of light between thedistance and near foci.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
5-18
Presbyopia and refractive surgery
In treating presbyopia, a number of refractive surgeons advocate monovision. Thedominant eye is corrected to achieve a refractive error close to emmetropia and the non-dominant eye is left with a small myopic undercorrection, usually in the region of about -1.25D. In a study of patients treated by PRK, all patients maintained binocular fusion andsome degree of stereopsis but those who are most satisfied appear to be people with lowervisual expectations. The implications of monovision for tasks such as rapid responsedriving have not been considered62. Some clinics are now offering scleral expansionsurgery for presbyopia. This is a dangerous and flawed procedure. Any effects aretemporary and complications are common and serious.
Wavefront Guided Laser Refractive Surgery (customised ablation)
This is the latest advance in the field of laser refractive surgery. Refractive errors as definedabove (myopia, hypermetropia and astigmatism) account for approximately 95% of theblur we experience when not wearing our spectacles or contact lenses. The remaining 5%of the ‘blur’ or defocus is made up of a variety of additional optical defects or aberrations.A Wavefront scanner measures these aberrations and the additional information obtainedcan then be used to program the excimer laser with the exact treatment required (a customablation treatment). The aim is to re-profile the cornea to exactly the correct contour tocancel all optical defects.
In theory at least, if all refractive error and all aberrations are eliminated the individualcould expect to see better than ever before. This has led to the term ‘Super Vision’ inrelation to this technology and is being sought by those with particularly demanding visualrequirements. There are, however, many problems that can prevent this ideal outcome.Individual healing characteristics, pupil size, accuracy of alignment of the treatment area,and accuracy of the original measurements are just some problems. This is an expandingarea of laser treatment and it is quite likely that all treatments in the future will becustomised using Wavefront technology or a refinement of it.
Since a Wavefront treatment aims to reduce aberrations, in theory it should produce betteroutcomes for night vision and vision in difficult low lighting levels or reduced contrast asmight be encountered in a smoke-filled room. This technology could therefore have greatrelevance for firefighters. Research is still underway to aid our understanding of thisrelatively new technology.
Night Vision and Contrast Sensitivity Following Laser Surgery
Any reduction in the clarity of the cornea or lens will result in a higher proportion ofincident light being scattered within the eye. This stray light is superimposed over theretinal image thereby reducing its contrast because of forward scatter. A reduction in thecontrast of a high contrast object such as a letter on a Snellen chart will have limitedimpact, but reducing the image contrast of a low contrast scene such as in the ‘real-world’is likely to result in the image falling below the threshold for discrimination, i.e. the objectwill no longer be visible.

Problems with the nervous system and special senses
5-19
Night vision in the normal population is poor compared to vision under good illuminationfor a number of reasons. Firstly the dark-adapted retina relies on the rod receptors, whichhave poor resolution; secondly, as the pupil dilates, aberrations from the more peripheralparts of the cornea increase by up to 30 times; thirdly the contrast of an object against thebackground tends to be much lower at night. In addition, the highly myopic retina is lesssensitive at low light levels and this problem might be compounded by laserrefractive surgery.
Many studies in the literature in the past reported a high incidence of night visionproblems such as halos, starbursts and poor quality vision following laser surgery63. Theseproblems were associated with high levels of haze causing scattered light, but nowadayshaze is much less severe and generally only present for the first 2-3 months post-PRKbecause high myopes are not treated with PRK. LASIK causes little or no haze in themajority of cases and ablation zone diameters for both PRK and LASIK have increasedfrom around 4 or 5mm up to 6 or 6.5mm, often in combination with 8mm ‘blend zones’ tominimize these halo or scatter effects, making them larger or the same size as the averagepupil under low illumination.
Tests of contrast sensitivity that are quick and simple to use are the Pelli-Robson chart andthe 10% contrast logMAR chart, but both test under brightly lit conditions. If night visionis critical to the job, specialist ophthalmic assessment is advised, which should includeassessment under low illumination.
Assessment after Refractive Surgery
An examination to consider the suitability of a refractive surgery patient for operationalfirefighting should include:
• A slit lamp examination to confirm that the eye has returned to normal and thatthere is no significant loss of corneal transparency over the pupil area.
• Refraction, topographic examination and pachymetry to screen for keratectasia (abulging forward of the cornea as is seen in keratoconus). The candidate shouldprovide details of their pre-operative refractive error and if possible details such astheir post-operative corneal thickness and the nature of any complications that mayhave occurred during or following the procedure.
• Candidates should have their visual performance assessed using a technique sensitiveto the presence of scattered light and aberrations. The Snellen letter chart isinadequate alone but a low contrast logMAR chart or Pelli Robson chart providesome information.
• Candidates should not be considered until at least 12 months post surgery and whenall medication has ceased.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
5-20
Colour defects
The processing of colour information begins at the level of the retina in the cones(concentrated at the macula), with further processing at higher levels of the retina andvisual cortex. Good colour vision improves visual search times by a factor of two64 and is auseful aid to identification in a visually degraded environment65. Defective colour visionmay be inherited (affecting 8% of men and 0.5% of women), or acquired (as a result ofageing, systemic disease or drug toxicity), therefore periodic reviews are justified. Thecondition is rare in people of Japanese, Chinese or African origin and complete loss ofcolour sense, achromatopsia (true colour blindness), is extremely rare.
Most occupations do not require perfect colour vision, however there are many with asafety critical component where colour is used to differentiate safe from unsafe (e.g.electrical cabling, warning lights) and such occupations generally exclude all but themildest colour defectives. The Health and Safety at Work Act 1974 demands that anindividual must be safe at work for his own protection and that of others. Therefore in asafety critical occupation such as firefighting, colour vision is essential.
Types of colour defect
The types of colour defect derive their names from the Greek roots of the 3 primarycolours:
Dichromats are missing one of the three colour pigments whereas Trichromats have allthree pigments but one pigment has an abnormal spectral sensitivity. Protan and Deutandefects are referred to collectively as red/green colour deficiency because they lead torelatively similar colour confusions. As displayed in the above table, DeuteranomalousTrichromatism accounts for more than half of colour deficiencies in the population. Withall congenital colour defects, there is a range of severity so that some anomaloustrichromats have a severe colour deficiency so that their vision approaches that of adichromat, whereas others have only a mild deficiency that leads to only occasional colourconfusions (e.g. pastels but not saturated hues).
Acquired colour defects
Acquired defects occur in many retinal and optic nerve conditions or as a result ofsystemic disease or drug toxicity:
Deficiency Condition Males Females
Red (severe) Protanopic Dichromatism (known as protanopia) 1% 0.01%
Red (mild to severe) Protanomalous Trichromatism 1% 0.01%
Green (severe) Deuteranopic Dichromatism (known as deuteranopia) 1% 0.01%
Green (mild to severe) Deuteranomalous Trichromatism 5% 0.35%
Blue Tritanopia and Tritanomalous trichromatism Rare – usually acquired
Colour blind Monochromatism Exceedingly rare

Problems with the nervous system and special senses
5-21
• Macular degeneration
• Toxic Amblyopia (excessive use of alcohol or tobacco)
• Chronic Glaucoma
• Senile cataracts (reversible)
• Diabetic retinopathy
• Multiple Sclerosis
Effect of Colour Deficiency
A colour defective individual cannot distinguish between as many colours as a colournormal individual; some colours will be confused. The range of colours they candistinguish depends on the severity of the defect; however colours will only be confusedif they have exactly the same luminance or brightness.
Red light is used as a warning light because it retains its colour at a distance when othercolours appear colourless. Green is the next colour to be determined at distance and so isused as the opposite colour in the traffic light system (although it also contains some bluelight as a concession to deuteranomalous trichromats).
Protanopic individuals lack red pigment and therefore colours around the red wavelengthappear less bright than surrounding colours. This has implications for protanopes andsevere protanomalous individuals in the workplace; a red warning sign may be overlookedor a red warning light missed or reactions times to red may be greatly increased.
Protanopic individuals have recognition distances for red traffic lights that are 50-70% ofthe normal range which has the effect of doubling the safe stopping distance of a vehicleat a red traffic light66. Verriest was able to show that protanopes are twice as likely to beinvolved in rear end traffic collisions. Difficulty interpreting traffic lights was reported by53% of protanopes, 44% of deuteranopes, 24% of protanomalous trichromats and 17% ofdeuteranomalous trichromats67.
In other situations such as the identification of gas cylinder contents or the correctidentification of coloured hoses, non colour clues may be used to aid identification butthese clues will be degraded in less than perfect visibility or where speed of action isrequired.
Colour Defect Screening
Screening for colour defects is required to exclude applicants with very poor colourdiscrimination (dichromats and severe anomalous trichromats) from safety critical workwhilst identifying those with potentially safe, milder degrees of anomalous trichromatism.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
5-22
Vocational testing has little place in the pre-employment screen due to examiner error,poor standardisation of test conditions and the use of colour naming. In addition, for safetyon the fireground, the range of colours, levels of illumination and range of backgroundcontrast make true vocational testing highly complex with poor levels of repetition.
Colour charts provide a quick and repeatable method of screening for defective colourvision. Ishihara, City University Colour Vision Test and the Hardy, Rand and Rittler(HRR) test are all popular types. The Ishihara appears to be the industry standard forinitial screening as it is the strictest screening test available; it will only pass those withnormal colour vision or with a very mild defect but it does not test for tritan (blue)defects. The Ishihara and HRR exploit common colour confusions, where as the CityUniversity test exploits colour matching.
All tests should be viewed under Standard Illuminant C (overcast daylight is a reasonablecompromise but not tungsten or fluorescent lighting). Should an individual fail to correctlyidentify 2 or more plates (pass/fail criteria vary between occupations and misreading ofcertain plates by normals is not uncommon), a second test is required to identify severefrom medium levels of colour deficiency.
The industry standard definitive test is the Farnsworth D15 test. This will be failed bydichromats and severe anomalous trichromats (whether protan, deutan or tritan) andtherefore allows those with less severe colour defects to be selected.
Standards for Colour Vision
Monochromatic persons will fail all colour tests but are generally easily identified as theyusually have significant co-existing visual disability.
Individuals who fail the Ishihara test and fail the Farnsworth D15 test by making one ormore colour confusions which cross the hue circle are likely to be dichromatic or havesevere anomalous trichromatism and they are unsafe for safety critical work.
If an applicant fails Ishihara but makes no errors which cross the hue circle of theFarnsworth D15 test, they have either mild deuteranomalous trichromatism orprotanomalous trichromatism. At this point they can be accepted for non operational rolesbut an occupational test is required for entry as a fire fighter because protanomaloustrichromats may confuse blue-green hoses with black hoses and black oxygen cylinderswith maroon acetylene ones as well as remaining insensitive to red warning lights68.Red/Green ‘safe’ deuteranomaly is five times more common than protanomaly and sooccupational testing is preferable to costly external specialist investigation with ananomaloscope.
Summary of standardsIndividuals with protanopia, deuteranopia, monochromatism and tritanopia/tritanomalyare unfit for service as a firefighter. Individuals with protanomaly rarely meet the requiredstandards while deuteronamalous individuals should be safe for firefighting.
Whilst diagnosis of the defect is an important part of the assessment, subsequentconfirmation of severity is essential to determine whether they are colour safe.

Problems with the nervous system and special senses
5-23
Visual Field Defects
A group I and II driving licence requires a normal binocular field. This should be 120degrees along the horizontal with no significant defect within the central 20 degreesassessed on the Goldmann test. Up to three consecutive points can be missed on theEsterman test before it is counted as significant.
[Subject to be considered in future amendments]
Age Related Disorders
Presbyopia, Cataract, Glaucoma
[Subjects to be considered in future amendments]
Hearing standards for firefighters
Introduction
Any auditory standard must be developed on a capability basis. Those involved inactivities in which environmental safety may change at a moments notice will requiregood standards of vision, hearing, speech and mobility. The ability to perceive risk andcommunicate that to others is of paramount importance.
Reduction in Hearing Ability during Employment
Hearing capability decreases with age. Individuals may therefore meet employmentstandards when young, but fall below them after a number of years in employment. Thisdecrease is unpredictable between individuals, and the noise exposure of firefighters is bothvariable and unpredictable. Although Management will do their best to ensure firefightersare protected from noise, the emergency nature of the task will at times expose individualsto events such as explosions that could not have been foreseen and cannot be protectedagainst.
It is not therefore possible to apply a fair or reasonable standard that allows for a degree ofage-related hearing loss.
Hearing Requirements in the Service
Active firefighters must not only communicate over the radio but they must respond toshouted warnings, audible alarms and cries for help – all above the environmental noise atthe incident. In addition, they may be exposed to noise in the form of explosions, cuttingor vibrating equipment and sirens reaching 109 dB(A) for periods of a minute or so69.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
5-24
Control room staff must also be able to communicate clearly and effectively in difficultcircumstances. While it may be possible to provide aids to hearing that are compatiblewith communications equipment, the safety and effectiveness of control room staff mustnot allow disability issues to lower standards. Any reasonable adjustment must enablecontrol room staff to be fully functional.
Selection of Appropriate Standards
To aid medical staff and managers, the point at which an individual’s hearing may interferewith their function in a safety critical area is taken as the point at which loss of perceptionof the speech frequencies becomes symptomatic and interferes with normal life. This isknown as the Low Fence Value and is an average of the hearing thresholds over the speechfrequencies 1, 2 and 3 kHz. A 30 dB HL LFV is widely accepted as the onset ofdisability70. In the medico-legal context, such a three-frequency average hearing loss ineach ear would be expected to produce 18% speech-hearing disability71.
Standards that sum the low frequencies (LF: 500 Hz, 1 kHz, 2 kHz) and the highfrequencies (HF: 3 kHz, 4 kHz, 6 kHz) are used in the military PULHHEEMS standards.The military standards are generous enough to enable recruitment despite quite markedhearing loss or alternatively they allow for quite marked deterioration of hearing beforeany change in medical grade is made. This may be appropriate for the military where rolesvary widely but is less appropriate for the Service where it is important to both maximiserecruitment opportunity and minimise noise damage to hearing.
The approach that has been taken is to split the military “H2” grade (45-83 dB HL [LF]and 45-123 dB HL [HF]) so that a middle grade exists which corresponds withasymptomatic non disabling hearing loss. Recruitment and placement in safety criticalareas is possible at this level without significantly affecting safety on the fireground.
In addition, greater emphasis should be placed on auditory function at 1, 2 and 3 kHz asthis reflects the bulk of frequencies found in normal speech and therefore radiocommunications. They can also be accurately measured using bone conduction shouldspecialist referral become necessary.
It is said that individuals who have been employed as aircrew regularly usingcommunications equipment learn to adapt and maintain their capability in the presence ofsignificant hearing loss. Therefore while new Service applicants may fail to meet thecapability standard because of a degree of hearing loss, serving firefighters and controlroom staff may maintain their capability in the presence of a greater degree of hearing loss.It may therefore appropriate to deny recruitment at a standard where serving personnel arepermitted to continue in employment.
Three separate measures should be recorded from the basic data:
• The sum of LF thresholds (0.5, 1 and 2 kHz)
• The sum of HF thresholds (3, 4 and 6 kHz)
• The sum of the Speech Frequency thresholds (1, 2, 3 kHz).

Problems with the nervous system and special senses
5-25
Using this table, each individual can be assigned a hearing risk score – both at the time ofrecruitment and on subsequent reviews.
The following summative measures are used to assign an overall score for each ear. Theworse ear is used to grade the individual in their placement within the Service:
Using the H1 criteria for recruitment purposes will allow 70% of the male population aged18-30 years to be considered for safety critical roles. Relaxing these standards slightly tothe H2 level would mean a larger population base can be considered for full-time orretained firefighter training without affecting fireground safety.
Summary of standards
Applicants for firefighting or control room work who meet the H2 standard should beconsidered fit for role. Applicants who are between H2 and H3 should have a capabilityassessment before employment. Applicants who fail to meet H3 should not be recruitedas firefighters.
Serving personnel who drop below H3 should have a capability assessment before anydecisions are made on redeployment or retirement.
Control room staff who drop below H3 should be reviewed by a specialist, and possibleadjustments to headsets considered to maintain capability. Where it is not possible toimprove hearing sufficiently with reasonable adjustments, redeployment or retirement willbe necessary.
Whilst referral through the individual’s GP maintains normal medical protocols, it isunusual for such referrals to take precedence over other NHS activities. Brigade funds mayhave to be released in order to fund specialist referral in a timely fashion, especially ifrestricted duties or a medical suspension is involved.
LF sum HF sum Speech sum
H1 ≤ 45 dB HL ≤ 45 dB HL ≤ 35 dB HL
H2 ≤ 60 dB HL ≤ 80 dB HL ≤ 60 dB HL (no value > 25 dB HL)
H3 ≤ 80 dB HL ≤ 120 dB HL ≤ 90 dB HL (no value > 40 dB HL)
H4 < 120 dB HL ≤ 150 dB HL ≤ 120 dB HL
H5 > 120 dB HL > 150 dB HL > 120 dB HL
Right
Right Speech
500 Hz 1 kHz 2 kHz SUM 3 kHz 4 kHz 6 kHz SUM 8 kHz
Left
Left Speech

Fire and Rescue Service: Draft Medical Guidelines – June 2004
5-26
Investigating Hearing Loss
Consideration of Noise-Induced Hearing Loss (NIHL) centres on a threshold ‘notch’ at 4kHz with a positive history of excessive noise exposure. However, this is not a prescriptivedefinition. If the criteria72 below are met, the hearing loss should merit specialist referral.
Criteria For Noise – Induced Hearing LossIt is always sensorineural, affecting the hair cells in the inner ear.
• It is almost always bilateral and is usually symmetrical.
• The earliest damage to the inner ear occurs at 4 kHz and is seen as a characteristic‘notch’ on the audiogram. Over time, this may deepen and ‘widen’ as 3 kHz and 6kHz become affected.
• High-frequency losses may reach 75 dB and are always greater than low frequencylosses (500 Hz, 1 kHz and 2 kHz) which may reach 40 dB. It rarely produces aprofound hearing loss.
• Once the exposure to noise is discontinued, there is no significant further progressionof the hearing loss.
• Previous NIHL does not make the ear more sensitive to future noise exposure. Givenstable exposure conditions, high-frequency losses usually reach their maximum level inabout 10 to 15 years. Further loss is minimal and slow.
• Diagnosis is based on consistently raised auditory thresholds of the characteristicpattern, in association with a positive history for noise exposure.
Tympanometric impedance testing should be performed by competent occupational healthstaff, in response to an unexpected low-frequency hearing loss. If the history suggests anupper respiratory tract infection and the tympanometry supports this, re-testing should beconducted once the symptoms have resolved.
Tinnitus
Tinnitus is a ‘sound’ which is audible to the individual but has no external origin; this maybe termed subjective tinnitus. Tinnitus is, in the majority of cases, a transient non-intrusive perception. 8% of the population experience tinnitus causing moderate to severeannoyance but only 0.5% experience tinnitus which is of such severity as to effect theirability to lead a normal life.
The vast majority of people who experience tinnitus do not complain about it. However,any persistent tinnitus associated with noise exposure may require a firefighter to beprotected from further exposure, to minimise the possibility of the sensation becomingworse. A number of reports have confirmed that the intrusiveness is correlated withpsychological factors. Severe intrusive tinnitus warrants detailed otological investigation.Before any decisions are made on redeployment or retirement, an opinion should be soughtfrom a psychologist with particular expertise in this field.

Problems with the nervous system and special senses
5-27
References
1 Nelson KB, Ellenberg JH. Predictors of epilepsy in children who have experiencedfebrile convulsions. New England Journal of Medicine 1976; 295:1029-33.
2 Hauser WA, Annegers JF, Kurland JT. Febrile Convulsions: prognosis for subsequentseizures. Neurology 1977;27:341.
3 Pavone L, Cavazzuti GB, Incorpora G et al. Late febrile convulsions: a clinicalfollow-up. Brain and Development. 1989; 11: 183-5.
4 Currier RD, Kooi KA, Saidman LJ. Prognosis of pure petit mal. A follow up study.Neurology 1963;13:959-67.
5 Livingston S, Torres I, Pauli LL, Rider RV. Petit mal epilepsy: results of a prolongedfollow-up of 117 patients. JAMA 1965;194:227-32.
6 Roger J. Prognostic features of petit mal absence. Epilepsia 1974;15:433.
7 Lerman P, Kivity S. Benign focal epilepsies of childhood. Recent advances in epilepsy.Churchill Livingstone, Edinburgh 1986. pp 137.
8 Beaussart M, Faou R. Evolution of epilepsy with Rolandic paroxysmal foci: a study of324 cases. Epilepsia 1978; 19: 337-42.
9 Loiseau P, Duche B. Benign childhood epilepsy with centrotemporal spikes. Clevelandclinic Journal of Medicine. 1989; 56 (supp 1): S17-22.
10 Reynolds EH. Interictal behaviour in temporal lobe epilepsy. BMJ 1983;21:22
11 Harbord MG, Manson JL. Temporal Lobe Epilepsy in childhood. A reappraisal ofetiology and outcome. Pediatric Neurology 1987; 3: 263-8.
12 Oller-Daurella L, Oller FV. Epilepsy with generalised tonic clonic seizures in childhood.Does a childhood ‘grand-mal’ syndrome exist? Epileptic Syndromes in Infancy,Childhood and Adolescence. (Eds J Roger, M Bureau, C Dravet et al) John Libbey,London 1992. pp. 161.
13 Holbrook M. Stroke: Social and emotional outcome. JR Coll Physicians Lond1982;16:100-4.
14 Mitchell JN. Multiple Sclerosis and the prospects for employment. J Soc Occ Med.1981;31:134-8.
15 Minutes of the Secretary of State for Transport’s Honorary Medical Advisory Panel onDriving and Visual Disorders meeting. 30th April 2002.
16 Fireground Vision Research Unit. Aids to Vision on the Fireground p 133 CityUniversity, London 1996.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
5-28
17 Mitchell P, Hourihan F, Sandbach J, Wang JJ. The relationship between glaucoma andmyopia – The blue mountains eye study. Ophthalmology 1999;106:2010-5.
18 Ivanisevic M, Bojic L, Eterovic D. Epidemiological study of nontraumatic phakicrhegmatogenous retinal detachment. Ophthalmic Research 2000;32:237-239.
19 Fireground Vision Research Unit. Aids to Vision on the Fireground p144. CityUniversity, London 1996.
20 Fireground Vision Research Unit. Aids to Vision on on the Fireground p143. CityUniversity, London 1996.
21 Chisholm C in British Society for Refractive Surgery:www.bsrs2000.fsnet.co.uk/new_page_13.htm
22 Panda A, Sharma N, Kumar A. Ruptured globe 10 years after radial keratotomy. Journalof Refractive Surgery 1999;15:64-5.
23 Vinger PF, Mieler WF, Oestreicher JH, Easterbrook M. Ruptured globes following radialand hexagonal keratotomy surgery. Archives Of Ophthalmology 1996;114:129-34.
24 Waring GO, Lynn MJ, McDonnell PJ. Results of the Prospective Evaluation of RadialKeratotomy (PERK) study at ten years after surgery. Archives Of Ophthalmology1994;112:1298-308.
25 Bores LD, Myers W, Cowden J. Radial keratotomy: an analysis of the Americanexperience. Annuals of Ophthalmology 1981;13:941-8.
26 Applegate RA et al. Corneal aberrations and visual performance after radial keratotomy.Journal of Refractive Surgery 1998;14:397-407.
27 Corbe C et al. Aircrew fitness decisions and advances in refractive surgery techniques.German Journal of Ophthalmology 1993;2:146-9.
28 Enzenauer RW et al. Radial keratotomy in the soldier-aviator. Military Medicine1993;158:521-8.
29 McDonald MB et al. Central photorefractive keratectomy for myopia – partially sightedand normally sighted eyes. Ophthalmology 1991;98:1327-37.
30 Gartry DS, Kerr Muir MG, Marshall J. (1992) Excimer laser photorefractivekeratectomy: 18 month follow-up. Ophthalmology 1992;99:1209-19.
31 Gartry DS, Kerr Muir MG, Marshall J. The effect of topical corticosteroids on refractionand corneal haze following excimer laser treatment of myopia: An update.A prospective, randomised, double-masked study. Eye 1993;7:584-90.
32 Tuunanen TH, Tervo TT. Results of photorefractive keratectomy for low, moderate andhigh myopia. Journal of Refractive Surgery 1998;14:437-46.

Problems with the nervous system and special senses
5-29
33 McDonald MB et al. Photorefractive keratectomy for low-to-moderate myopia andastigmatism with a small-beam, tracker-directed excimer laser. Ophthalmology1999;106:1481-8.
34 Gartry DS et al. Retreatment for significant regression after excimer laserphotorefractive keratectomy. A prospective, randomized, masked trial. Ophthalmology1998;105(1):131-41.
35 Shieh E et al. Quantitative analysis of wound healing after cylindrical and sphericalexcimer laser ablations. Ophthalmology 1992;99:1050-5.
36 Shah S et al. Astigmatism induced by spherical photorefractive keratectomy corrections.Ophthalmology 1997;104:1317-20.
37 Higa H et al. Predictability of excimer laser treatment of myopia and astigmatism by theVISX Twenty-Twenty. Melbourne Excimer Laser Group. J Cataract Refract Surg 1997Dec;23(10):1457-64.
38 Shieh, E., Moreira, H., D’Arcy, J., Clapham, T.N., and McDonnell, P.J. (1992)Quantitative analysis of wound healing after cylindrical and spherical excimer laserablations. Ophthalmology 99, 1050-1055.
39 Shah, S., Chatterjee, A., Doyle, S.J., and Bessant, D.A. (1997) Astigmatism induced byspherical photorefractive keratectomy corrections. Ophthalmology 104, 1317-1320.
40 Higa et al. (1997) PRK for the treatment of astigmatism and myopia between -1.00 and-19.00D. Journal of Cataract and Refractive Surgery 23,
41 Daya SM, Tappouni FR, Habib NE. Photorefractive keratectomy for hyperopia – sixmonths results in 45 eyes. Ophthalmology 1997;104:1952-8.
42 Corones F et al. Photorefractive keratectomy for hyperopia: long-term nonlinear andvector analysis of refractive outcome. Ophthalmology 1999;106:1976-82.
43 Nagy ZZ et al. Photorefractive keratectomy for hyperopia in 800 eyes with the MeditecMEL 60 laser. Journal of Refractive Surgery 2001;17:525-33.
44 Miller WL, Schoessler JP. Comparison of forward and backward scattered light in preand post-surgical photorefractive keratectomy. Investigative Ophthalmology and VisualScience 1995;36:S709 (Abstract)
45 Chisholm CM. Assessment of visual performance: comparison of normal subjects andpost-refractive surgery patients. 2002. City University. Thesis/Dissertation.
46 Montes-Mico R, Charman WN. Mesopic contrast sensitivity function after excimerlaser photorefractive keratectomy. Journal of Refractive Surgery 2002;18:9-13.
47 Goldberg MA, Dorr DA, Pepose JS. Lack of diurnal variation in vision, refraction, orkeratometry after excimer laser photorefractive keratectomy. American Journal OfOphthalmology 1997;123:407-8.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
5-30
48 Hjortdal JO et al. Mechanical stability of the cornea after radial keratotomy andphotorefractive keratectomy. Journal of Refractive Surgery 1996;12:459-66.
49 Galler EL et al. Ocular integrity after quantitated trauma following photorefractivekeratectomy and automated lamellar keratectomy. Investigative Ophthalmology &Visual Science 1995;36:580 (Abstract)
50 Montes M et al. Laser in situ keratomileusis for myopia of -1.50 to -6.00 diopters.Journal of Refractive Surgery 1999;15:106-110.
51 Condon P. LASIK for hypermetropia. Session 4. 1997. BEKLS conference proceeding.
52 Goker S, Er H, Kahvecioglu C. Laser in situ keratomileusis to correct hyperopia from+4.25 to +8.00 diopters. Journal of Refractive Surgery 1998;14:26-30
53 Puk DE, Probst LE, Holland EJ. Recurrent erosion after photorefractive keratectomy.Cornea 1996;15:277
54 Peacock LW et al. Ocular integrity after refractive procedures. Ophthalmology1997;104:1079-83.
55 Galler EL et al. Ocular integrity after quantitated trauma following photorefractivekeratectomy and automated lamellar keratectomy. Investigative Ophthalmology &Visual Science 1995;36:580 (Abstract)
56 Argento C et al. Corneal ectasia after laser in situ keratomileusis. Journal of Cataractand Refractive Surgery 2001;27:1440-8.
57 Joo CK, Kim TG. Corneal ectasia detected after laser in situ keratomileusis forcorrection of less than -12 diopters of myopia. Journal of Cataract and RefractiveSurgery 2000;26:292-5.
58 Geggel HS, Coday MP. Late-onset traumatic laser in situ keratomileusis (LASIK) flapdehiscence. American Journal Of Ophthalmology 2001;13:505-6.
59 Claringbold TV. Laser-assisted subepithelial keratectomy for the correction of myopia.Journal of Cataract and Refractive Surgery 2002;28:18-22.
60 Lee JB et al. Comparison of laser epithelial keratomileusis and photorefractivekeratectomy for low to moderate myopia. Journal of Cataract and Refractive Surgery2002;27:565-570.
61 Costagliola C et al. ArF 193nm excimer laser corneal surgery and photo-oxidation stressin aqueous humor and lens of rabbit: one-month follow-up. Current Eye Research1996;15:355-61.
62 Goldberg DB. Laser in situ keratomileusis monovision. Journal of Cataract andRefractive Surgery 2001;27:1449-55.
63 O’Brart DPS et al. Night vision after excimer laser photorefractive keratectomy: hazeand halos. European Journal of Ophthalmology 1994;4:43-51.

Problems with the nervous system and special senses
5-31
64 Christ RE. Review and analysis of colour coding research for visual displays. HumanFactors 1975;17:542-70.
65 Markoff JI. Target recognition performance with chromatic and achromatic displays.SRM 1972;148:72.
66 Verriest G, Naubauer O, Marre M, Uviljis A. New investigations concerning therelationships between congenital colour vision defects and road traffic security.In Verriest G ed. Colour Vision Deficiencies. Bristol: Hilger 1980:331-42.
67 Steward KM, Cole BL. What do colour vision defectives say about everyday tasks?Optom & Vision Sci. 1989;5:288-95.
68 Margrain TH, Birch J, Owen CG. Colour Vision requirements for firefighters.Occup Med (Lond). 1996;46(2):114-24.
69 Tubbs RL. Occupational Noise Exposure and Hearing Loss in Fire Fighters assigned toairport Fire Stations. Am Ind Hyg Assoc J. 1991; 52(9): 372-8.
70 Robinson DW, Wilkins PA, Thyer NJ, Lawes JF. Auditory impairment and the onset ofdisability and handicap in noise induced hearing loss. ISVR Technical Report no. 126Southampton, University of Southampton, 1984.
71 King PF, Coles RRA, Lutman ME, Robinson DW. Assessment of hearing disability:Guidelines for medicolegal practice. London: Whurr Publishers. See Table A2.
72 American College of Occupational Medicine, Noise and Hearing ConservationCommittee. Occupational hearing loss. J Occup Med, 1989; 31(1): 996.Updated 1997 and 2002 and posted on the Internet, accessed February 2004:http://www.acoem.org/guidelines/pdf/Noise-induced-Hearing-Loss-10-02.pdf

Fire and Rescue Service: Draft Medical Guidelines – June 2004
5-32

CHAPTER 6
Mental health problems


CHAPTER 6Mental Health Problems
CONTENTS
INTRODUCTION 6-3
Assessment of Fitness 6-3
PERSONALITY DISORDERS 6-4
NEUROSES 6-5
Anxiety Disorders 6-5Generalised anxiety disorders 6-5Simple phobia 6-6Social phobia 6-3Agoraphobia 6-7Panic disorder 6-7Obsessive compulsive disorder 6-7Conversion and dissociative disorders 6-8
DISORDERS OF MOOD 6-8
Bipolar affective disorder 6-9Unipolar depressive disorders 6-9
REACTIONS TO STRESSFUL EXPERIENCES 6-11
Acute Stress Disorder 6-11Adjustment Disorders 6-11Post Traumatic Stress Reactions (PTSR) 6-11Post Traumatic Stress Disorder (PTSD) 6-12Critical Incident Support 6-13
SCHIZOPHRENIA 6-14
DELIBERATE SELF HARM 6-15
COGNITIVE DISORDERS AND ORGANIC MENTAL ILL HEALTH 6-15
EATING DISORDERS 6-16
6-1

Fire and Rescue Service: Draft Medical Guidelines – June 2004
6-2
THE ABUSE OF ALCOHOL AND OTHER DRUGS 6-16
Alcohol 6-16Other substances 6-17
TREATMENT WITH PSYCHOACTIVE MEDICATIONS 6-17
Psychoactive drugs usually incompatible with safe firefighting 6-18
REFERENCES 6-19
Authors
Original Author 1999:
Dr Charles Baron FRCP FFOM, Consultant Occupational Physician, BrigadeMedical Adviser North Wales Fire Service.
Updated 2004 by:
Dr Martin Baggaley MRCPsych, Consultant Psychiatrist & Senior Lecturer, Guy’s,Kings & St Thomas’s Medical School.
Dr Tony Williams MFOM, Consultant Occupational Physician, Working Fit Ltd.

Mental health problems
6-3
Introduction
Mental ill health in one form or another is extremely common in the UK adultpopulation. In many cases its effects are transient and effectively treated by drug orpsychological therapies. In other cases, features are longer lasting or recurring and are morelikely to present a permanent barrier to safe service as an operational firefighter. Featureswhich are likely to be most problematical and of greatest concern to medical advisers arealtered behaviours which may be unsafe and unpredictable, and altered concentration,cognition and reaction time which may give rise to increased errors and risk to safety.These latter features may result from the condition itself and from its treatment.
Disease classification is particularly important in psychiatry, as a tool for diagnosis, andan aid to treatment and research. The WHO has sponsored an international diseaseclassification process, the International Classification of Diseases, now in its tenth version(ICD10)1. In parallel the United States developed its own Diagnostic and StatisticalManual of Mental Disorders, now in its fourth version (DSMIV)2. Initially developed fordifferent reasons, these classifications are now much more similar in their latest versions.Although in UK the ICD10 classifications are generally used, they are not ideal in someareas where the DSMIV classification is preferred.
In this chapter, where possible, each condition or group of conditions has been givensystematic consideration with ICD10 definitions and categorisations (where relevant),features causing problems for firefighting, prevalence rates (where available), treatmentand prognosis. DSMIV is used occasionally where this is more relevant.
This guide is not intended as a substitute for a good general psychiatric reference and theOxford Textbook of Psychiatry by Michael Gelder et al3 is recommended as a readabletext. This text also includes a full explanation of the differences in classifications andreasons behind them.
Assessment of Fitness
Psychiatric disorders can lead to sudden onset risks to safety of both the individual andothers. This is unusual and in most cases the problem is one of capability while theindividual is symptomatic. While the risk to health and safety should lead to a carefulconsideration of fitness for initial employment, the longer-term capability issue should becarefully balanced against the requirements of the Disability Discrimination Act 1995.
Where the issue is a question of ‘reasonable adjustment’ the decision on employment mustbe a managerial one, particularly when long periods of sickness absence would have to betolerated and/or issues of behaviour or capability would have to be considered. It is mucheasier to make decisions when the individual is already in employment, is known tomanagement, and at least some of their past psychiatric history is familiar. It is much moredifficult to assess recruits, and in general a decision to employ an individual with asignificant psychiatric history should only be made with the benefit of a detailedpsychiatric report from a specialist, and where appropriate a detailed psychologicalassessment.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
6-4
The assessment of early retirement of serving firefighters depends on a judgement ofpermanent incapacity. Redeployment may become an alternative, however it is importantto distinguish between the different physical demands of different roles as opposed to themental pressures that may remain while employed by with the Fire Service.
Personality disorders
The definition in ICD9 is widely accepted. It refers to: deeply ingrained maladaptivepatterns of behaviour recognisable by the time of adolescence or earlier and continuingthrough most of adult life although often becoming less obvious in middle or old age. Thepersonality is abnormal either in the balance of its components, their quality andexpression or in its total aspect. Because of this the patient suffers or others have to sufferand there is an adverse effect on the individual or on society. The wording in ICD10 is lessconcise but conveys the same meaning.
A clear distinction should be drawn between personality traits or types and personalitydisorders. Some individuals with the less intense manifestations of a given personality traitmay be seen very positively by others. However, those with personality disorders will havedisplayed behaviours that are maladaptive, disruptive or destructive. Diagnosis is best madeby a careful clinical assessment in addition to objective accounts by others of pastbehaviour over a number of years.
A diagnosis of personality disorder should not be made without a good collateral history.Indicators of possible personality disorder would include behaviour such as frequentepisodes of deliberate self harm and a pattern of very unstable relationships. Psychologicaltests of personality may be useful but are less reliable than a good clinical assessment.
ICD10 classifies personality disorders into the following: Paranoid, schizoid, dissocial(antisocial), emotionally unstable (impulsive or borderline), histrionic, anakastic(obsessive, compulsive), anxious (avoidant), dependent and passive aggressive. Althoughthis categorical classification can be helpful, in practice many individuals will display thefeatures of a number of specific disorders. The terms psychopathic, inadequate andimmature are not used in ICD10 to describe personality disorders. They are generally feltto be clinically unhelpful and are best avoided. Personality disorder can and frequentlydoes occur with a mental illness such as depression.
Estimates of the prevalence of personality disorders in the UK adult population varybetween 10% and 13%. The most common types seem to be emotionally unstable,dependent and compulsive. Because, by definition, people with personality disorders willhave displayed behaviours that are deemed undesirable, they are much less likely to belongto populations who seek employment as firefighters. In general, those who do apply to jointhe service are less likely to succeed in aptitude tests and interviews.
Psychological therapies have been used for treatment of various personality disorders butwith variable success. Generally speaking, drug treatments are not seen as effective inmanaging personality disorders though in the acute phase there may be some benefits. Theprognosis of personality disorders is poor. Their effects on behaviour are likely to lastthroughout adult life although they may improve somewhat in middle and older age.

Mental health problems
6-5
Because behaviours associated with personality disorder (of whichever type) are disruptive,destructive or maladaptive, they are likely to be undesirable on the grounds of safety in anoperational firefighter. When a clear diagnosis can be made and confirmed by anappropriate psychiatric specialist, it is likely that recruits for firefighting or the controlroom would be not be considered fit and serving firefighters (whose diagnosis hadpreviously been unrecognised) would have to redeploy or retire on the grounds of ill-health. However, because of the potential for confusion between personality traits andpersonality disorders, it is possible that certain individuals might be considered safefollowing an appropriate risk assessment.
In addition, in serving firefighters who undergo an apparent change in their personality,consideration must be given to the cause of this which is most likely to be injury ororganic disease of the brain, severe mental disorder (especially schizophrenia), orexceptional severe stressful experiences. Consideration should also be given to thepossibility of drug induced personality changes. In any of these circumstances, theunderlying cause, its potential treatments and prognosis must be assessed in eachindividual case before arriving at a judgement about the longer term risks for operationalfirefighting.
Neuroses
Anxiety Disorders
These are abnormal states in which the most striking features are mental and physicalsymptoms of anxiety. These include symptoms such as fearful anticipation, irritability andpoor concentration in addition to physical symptoms of the gastrointestinal, respiratory,cardiovascular, genitourinary and neuromuscular systems (which may be distracting anddisabling) and sleep disturbance. When present in any degree of severity, these features areclearly incompatible with safe firefighting and are often incompatible with safety in thecontrol room. Although anxiety commonly occurs in association with depression, thesedisorders have been addressed separately.
Generalised anxiety disorders
ICD 10 requires that symptoms should have been present for ‘most days for at least severalweeks at a time, and usually several months’. One-year prevalence rates in studies in theUSA vary from 2.5% to 6.4%4. Many anxious patients do not meet the diagnostic criteriaand it is important to ensure that an individual has been properly diagnosed, preferably bya psychiatric specialist, before decisions on employment are made.
Treatment with cognitive behavioural therapy can be helpful in many cases. Drugtreatment with anxiolytics such as benzodiazepines many be helpful in the short termstabilisation of anxiety symptoms. They should however seldom be prescribed for longerthan three weeks because of the risk of dependence. It is now recognised that anti-depressants (SSRIs & SNRIs) are effective in the management of anxiety disorders. Theymay need to be prescribed in higher doses than usual for depression. The treatment needsto be long term as the anxiety disorder usually relapses on stopping the medication.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
6-6
Most anxiety disorders improve within six months but of those lasting longer, about 80%persist for more than three years5. In one major study, even with 80% receiving treatment,remission was only 15 per cent at one year and 27 per cent by three years. Where patientshad co-morbid psychiatric disorders, the proportions achieving remission from anxietydisorders were only 8% and 17% at one and three years respectively6 7.
Poorer prognosis is associated with severe symptoms and with syncopal episodes, agitation,derealisation, hysterical features and suicidal ideas. Somatisation is also a poor prognosticsign. A single episode of anxiety disorder, particularly related to some stressful event,which resolves within six months, should not be a contraindication to employment as anoperational firefighter. Recurrent or longer lasting episodes however are more likely to givecause for concern.
There is evidence that anxiety disorder predisposes to development of PTSD (see below).
Simple phobia
In this disorder a person is inappropriately anxious in the presence of one or moreparticular objects or situations. Most simple phobias of adult life are a continuation ofchildhood phobias. A minority begin in adult life as a result of a particularly stressfulexperience. In one study, lifetime prevalence in adults has been estimated as 4% in menand 13% in women8.
The relevance of simple phobias to firefighting depends on the nature of the phobia.A phobia of something commonly encountered during firefighting (for exampleclaustrophobia) will clearly cause the occurrence of anxiety symptoms with consequentunacceptable risks to safety. A fear of flying or of snakes for example may be less of aproblem to the operational firefighter. Though no systematic study of prognosis has beenavailable, clinical experience indicates that simple phobias originating in childhood lastfor many years but those occurring as a result of stressful events in adulthood have abetter prognosis3.
Social phobia
In this disorder, inappropriate anxiety is experienced in situations in which the person isobserved and could be criticised. The condition usually begins between the ages of 17 and30. As socially phobic people tend to avoid situations where they might be criticised, theywill avoid making conversation or will sit in a place where they are least conspicuous.
If the condition arises prior to application for employment as a firefighter, then it is likelythat such an individual would not be successful in application because of these disablingfeatures. If it arises after employment as a firefighter, then it could give rise to the featuresof anxiety mentioned above which may increase risks to safety. Treatment by cognitivebehaviour therapy is effective in many cases9. Drug treatment is probably inappropriateexcept for short-term control of symptoms. In the untreated patient, the condition manylast for many years.

Mental health problems
6-7
Agoraphobia
Agoraphobic patients are anxious when they are away from home, in crowds, or insituations that they cannot leave easily. Symptoms are similar to those of other anxietydisorders but panic attacks and anxious cognitions about fainting and loss of control aremore frequent among agoraphobic patients. The features are likely to be a significant riskand cause of disability to serving firefighters. One study estimated the one-year prevalenceof agoraphobia to be 1.7% in men and 3.8% in women8.
Treatment with behaviour therapy will often give some improvement in symptoms butpersistence of anxiety responses is common. Agoraphobia lasting for one year or morechanges little in the next five years10.
Panic disorder
The essential feature of this condition is the occurrence of panic attacks; these are suddenattacks of anxiety in which physical symptoms predominate and are accompanied by fearof a serious consequence such as a heart attack. Symptoms resulting from hyperventilationare common. Such features would clearly present serious risks to safety in the context ofoperational firefighting and the control room.
Treatment with cognitive behaviour therapy has been found to be successful to someextent in many cases11. Drug treatment with benzodiazepines control panic attacks whengiven in high doses but cannot be used in the longer term. The antidepressant drugs suchas imipramine (a tricyclic antidepressant) as well as other antidepressants (includingSSRIs) also control panic attacks but side effects from some drugs may be incompatiblewith operational firefighting (see below). Studies of patients with panic disorder (with orwithout agoraphobia) have indicated that the course is characterised by fluctuating anxietyand depression12.
Obsessive compulsive disorder
This condition is characterised by obsessional thinking and compulsive behaviour withvarious degrees of anxiety, depression and personal isolation. This would be seriouslyincapacitating and of high risk in the context of operational firefighting. The condition isless common than anxiety neuroses. Estimates of one-year prevalence rates vary from 1.1%to 1.8% with lifetime prevalence varying from 1.9% to 2.5%. About two-thirds of casesimprove by the end of one year. If symptoms last for more than one year, the condition willnormally run a remitting and relapsing course sometimes for many years. Prognosis is worsewhen the symptoms have been severe or where there are continuing stressful events in thepersons life3.
Treatment with counselling, anxiolytic drugs, clomipramine, SSRI’s, behaviour therapy,psychotherapy and psychosurgery have varying degrees of success. However, none of thesehas been proved to affect long term prognosis. Because of the uncertain prognosis, recruitsfor firefighting or the control room with a history of obsessive compulsive disorder areunlikely to be considered fit and serving firefighters and control room staff must be verycarefully assessed according to their clinical state and medical history.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
6-8
Conversion and dissociative disorders
These terms refer to disorders that until recently were known as hysteria. The mainfeatures of these disorders are physical symptoms, and certain mental symptoms, whichoccur without the expected physical pathology but with psychological causes. Thesymptoms usually confer some advantage on the patient, which is commonly referred to asa secondary gain. Dissociative disorders take a number of forms including amnesia,pseudodementia, fugue (amnesia with wandering), stupor, identity disorder and trance.The related conversion disorders include dissociated motor disorder, convulsions andsensory disorder.
The differential diagnosis from organic disease may be difficult and conditions such asMultiple Sclerosis have presented and been misdiagnosed as hysteria in the past. In thecontext of firefighting, the most likely presentation of such a condition is wherecompensation or injury-award is the secondary gain leading to psychological reinforcementof physical or mental symptoms. In these cases, a distinction must be drawn betweendissociative disorders and malingering or fraud.
This diagnosis should not be made without specialist confirmation regarding the absenceof organic disease and psychiatric confirmation of the congruity of the diagnosis. In caseswhere the diagnosis is certain, these disorders are likely to be incompatible with future safefirefighting and must be very carefully considered.
Disorders of mood
There are a number of different classifications of depressive disorders. These conditionshave in common various features that are to a greater or lesser extent disabling. Inaddition to low mood, these may include lack of interest and enjoyment, reduced energy,psychomotor retardation, anxiety, irritability, loss of concentration, poor memory, andsleep disturbance with consequent fatigue.
In severe depressive disorder, these features occur with greater intensity and may beaccompanied by psychotic symptoms including delusions and hallucinations3. The natureand severity of symptoms will determine how disabling the condition will be in thecontext of operational firefighting or working in the control room. Firefighters may notreport mild degrees of depression, but if cognition, concentration or memory is affected,risks to safety on the fireground may become significant.
Certain treatments may also affect cognition, concentration and reaction time andconsequently increase risks to safety. These effects are discussed in a later section of thischapter. For the purposes of considering prevalence and prognosis in the context of fitnessfor firefighting, depressive disorders may best be classified as bipolar (manic depressivepsychosis) and unipolar.

Mental health problems
6-9
Bipolar affective disorder
Episodes of manic disorders can last for considerable periods, sometimes up to two or threeyears. 20% to 30% of patients have three or four episodes of mania or hypomania per year.Psychotic features with manic episodes are not uncommon. Manic disorders often recurand subsequent depressive disorders are frequent. Relapse is less common in those onlithium therapy3 or other mood stabilisers such as carbamazepine. Some individuals maydevelop a progressive pattern with more frequent, more intense episodes.
Where recurrence is more often than four times per year the term ‘rapid cycling’ may beused, and the terms ‘ultra-rapid’ and ‘ultra-ultra-rapid’ may be used where the episode ofhypomania can run its course within 24 hours. It should be possible to identify theseindividuals from the history of disease progression, and where there is a very rapidfluctuation there may be a risk to the individual and others on the fireground or in thecontrol room before treatment has commenced13.
Because of the risk of the recurrence of symptoms on withdrawal of treatment andconsequent risks to safety, it is likely that a firefighter or controller with a history ofbipolar affective disorder will be considered permanently unfit for operational firefightingor control room work. There may be exceptions to this rule but every case must beconsidered very carefully before allowing the individual to return to operational duties.
Unipolar depressive disorders
Depressive disorders are common. Prevalence is mainly given as a point prevalence orperiod prevalence rate. The point prevalence rate of major depressive disorder is around4%. The six-month and one year prevalence is between 3-6% and the lifetime prevalenceis probably of the order of 18% although some studies indicate a much lower prevalence14.Brief depressive episodes that do not meet the criteria for major depression are alsocommon (one-year prevalence of 4-6% in the age group 20-30 years), they last less thantwo weeks (generally one to three days) and are highly recurrent, with 10-12 episodesper year15.
The severity and duration of depressive episodes varies widely. Most people withdepression recover within a period of two years from the onset of clinical illness. Anti-depressant medication and cognitive behavioural psychotherapy have been shown to beeffective treatments for depression. Simple counselling alone has not been shown to beeffective. Around 25% of people with unipolar disorders will have a recurrence within oneyear. 75% will have a recurrence in the following ten years16.
It is essential to distinguish between those with low mood who may continue at work andmay or may not require any drug treatment and those with depression as defined by DSMIV. In the former case they may state that they have a diagnosis of depression, howeverthis diagnosis may be unhelpful in assessing their fitness for work now or in the future. Keyaspects of the history include hospitalisation, sectioning under the Mental Health Act,treatment and review by a psychiatrist and/or the community mental health team. Theselatter aspects of history indicate a more severe disorder, with the advantage of thepossibility of requesting a report from a specialist.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
6-10
Where an individual has a diagnosis of depression, possibly including medication, but haveremained at work their assessment should be based on their capability while at work ratherthan their medical diagnosis. Recurrent episodes and recent episodes should be verycarefully assessed and these individuals are unlikely to be considered fit as firefighters orcontrol room staff.
The past history of the illness is essential in assessing future capability. Where thecondition is related to home or work circumstances that were relatively abnormal orextreme and which have now changed there will be a lower risk of recurrence than forthose where there was little obvious external cause and little change in personalcircumstances since. Recurrence is generally very difficult to predict, however it isassociated with bipolarity, early age of onset, number of previous episodes, and no obviousexternal cause. There is evidence that presence of a sick spouse may increase the relapserate16.
A history of mild depression over a year or two ago may be acceptable in an applicant.Mild depression that is not related to work is unlikely to be a cause for retirement orredeployment of serving firefighters. Recurrent or severe episodes and those which arecausally related to work may be disabling in the long-term and therefore require verycareful consideration. Prognosis of outcome is particularly difficult as there are fewvariables that appear to be related to outcome. A poor outcome is associated with socialisolation, uncertain situations and physical poor health. The presence of a confidingrelationship appears to improve outcome and some studies suggest that good social supportand older age are predictive of better recovery at 6-30 months. One major study suggestswomen over 30, women with unstable marital history and both sexes with a pooreducation are significantly associated with persistence of depression. History of previousdepression, severity and greater co-morbidity are also associated with persistence ofdepression, and all these factors have more impact than sociological factors16.
When suffering from depression, people commonly selectively recall negative experiencesand suffer from troubling dreams. This is important in a population such as firefighters whoare likely during their career to encounter a number of events which would be sufficientlyhorrific to be a potential cause for PTSD. If a firefighter develops a depressive disorder, onewould commonly expect them to have bad dreams and perhaps ruminate over pasttraumatic events. This may be incorrectly diagnosed as PTSD, especially if the are otherincentives or encouragement from spouse or colleagues for the firefighter to label it so.
Overall, the premorbid personality features are of best prognostic value. Low intelligence,hysterical and obsessional personality traits, social deviation and high neuroticism scoresare poor predictors while high extraversion scores predict a more favourable outcome16.
It is usual for maintenance treatment to continue for around six months after remission ofsymptoms in order to help avoid relapse at this early stage. There are no reasons whyindividuals should not return to normal duties during this period provided theirmedication does not affect their performance. Where recurrence does occur the process israrely immediate and acute (unlike bipolar disorder where some individuals may cyclethrough mania within 24 hours). It is therefore very unlikely that the individual who has arisk of relapse represents a risk to colleagues on the fireground. The risk is for long-termsickness absence and the associated disruption to human resources management.

Mental health problems
6-11
Reactions to stressful experiences
Acute Stress Disorder
Acute stress disorder is a prolonged response to a stressful event, lasting from a few days tofour weeks. The core symptoms are anxiety and depression3. A history of such an episodein an applicant for the Fire and Rescue Service should not be a bar to entry. However, theoccurrence of an acute stress disorder is a significant risk factor for the development of posttraumatic stress disorder, so such cases should be carefully considered. By definition(ICD10), acute stress disorder will resolve and is therefore not grounds for retirement forserving firefighters.
Adjustment Disorders
These are psychological reactions resulting form the adaptation to new circumstancesincluding for example bereavement, divorce, major job change, birth of a handicappedchild etc. The features include those of anxiety and depression. Although the stressfulevent is the necessary cause of this disorder, individual vulnerability is thought to be animportant factor3. The term adjustment disorder can be used to classify individuals whosuffer from a post traumatic stress response of insufficient severity to satisfy the full criteriafor PTSD.
Problem solving counselling has been found to be helpful and drug treatment fordepressive symptoms may be necessary. There is no systematic evidence relating toprognosis but most cases last for several months and some may last for years. In the lattercase, such episodes would eventually be reclassified as an anxiety or depressive disorder.
Symptoms may well interfere with operational firefighting in the same way as those ofanxiety and depression (see above). Because of the vulnerability that may underlie a pasthistory of this disorder, recruits will need to be considered very carefully as recurrence ofthis or related disorders might require redeployment or early retirement on health grounds.
Sudden onset, with associated risks to safety, is less likely so judgements about servingfirefighters must be made according to the history and course of the condition.
Post Traumatic Stress Reactions (PTSR)
Most individuals will react to traumatic events, and do so in a wide variety of ways,developing a range of symptoms. Post-traumatic stress disorder is only one of these and istightly defined. In most cases individuals will demonstrate symptoms of PTSR but not ofPTSD. PTSD is a much over-diagnosed condition and an overused term, particularly bygeneral practitioners. This is unhelpful in managing individuals who then haveunreasonable and incorrect expectations in terms of treatment and employment that needto be addressed along with their symptoms.
It is more helpful to discuss the concept of PTSR with individuals, and leave a diagnosis ofPTSD for a specialist to make.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
6-12
Post Traumatic Stress Disorder (PTSD)
Post traumatic stress disorder is a relatively new term (coined in the early 1980s) todescribe a condition that has been know throughout history, but has sadly beenmisdiagnosed and individual responses have been misinterpreted17 (see ‘depression’ above).The natural history of the condition in relation to current social expectations remains thesubject of debate, and it is likely that the response to trauma and development of PTSD isin part conditioned by our social surroundings18. Recent research suggests that there is adistinct neuro-biochemical basis to the condition which represents an incompleteemotional processing of the event19.
PTSD is a diagnosis rather than a disease, and therefore individuals have to meet strictdiagnostic criteria as laid down in DSM IV. It is best considered as a part of a spectrum ofthe normal reaction to exposure to traumatic events rather than an abnormal process.Everyone exposed to a traumatic event can have some features of PTSD; however in mostindividuals they will be mild and transient, and full recovery should be expected. Evenwhen the condition is severe it usually responds well to treatment.
Post traumatic stress disorder requires, by definition, a precipitating traumatic event. Thishas been defined by DSM IIIR as ‘outside the range of usual human experience’ and that it‘would be markedly distressing to almost anyone’. Some feel this is too narrow a definition;is a road traffic crash part of the usual human experience now, or outside it? ICD10 definesthe event as ‘a stressful event or situation...of an exceptionally threatening or catastrophicnature, which is likely to cause pervasive distress in almost anyone’. DSM-IV requires thatthe person ‘experienced, witnessed, or was confronted with an event or events thatinvolved actual or threatened death or serious injury, or a threat to the physical integrityof self or others’ and importantly that the ‘person’s response involved intense fear,helplessness, or horror’.
The symptoms of PTSD are the triad of intrusive re-experiencing, avoidance of associatedactivity or location, and hyperarousal. Continuing impairment is best identified by peerswho may note cognitive impairment and disturbed interpersonal relationships. Increasedarousal, irritability and loss of interest or withdrawal are also key features20.
Symptoms may begin very soon after the stressful event, although classically there is adelay which is rarely more than six months. Most cases resolve within a few months butsome may persist for years3. The prevalence of the condition varies with an overall pointprevalence of 1%21 while subgroups may have a much higher level. Levels of 30% havebeen described in firefighters exposed to a major bush fire22. There is a lifetime prevalenceof 5-6% in men and 10-12% for women23 24.
Predicting PTSDIt is very difficult to predict those at higher risk of developing PTSD; however neuroticismand past psychiatric disorder may be contributory factors25. There is a high incidence ofco-morbidity with other psychiatric disorders. While depression and substance abuseappear to follow from PTSD in most cases, where there is associated anxiety this precededPTSD in around half the cases26.
However, other studies have suggested that alcohol abuse may increase the likelihood oftraumatization because of its association with violence and accidents27.

Mental health problems
6-13
After an event that meets the DSM IV definition of ‘traumatic’ there may be some factorsthat could predict individuals at risk. Emotional numbing at the time of the traumaticevent has been shown to predispose to PTSD28 and individuals who feel guilt may also bemore at risk. Guilt may be because the individual feels they either made a mistake on thefireground, or that they could have done more. This is of relevance in considering that theICD10 classification considers PTSD alongside adjustment reaction; adjustment reaction isan important differential diagnosis.
If the person experiences a new traumatic event, symptoms may return even if the secondevent is less severe than the original. Since firefighting is a potential source ofexceptionally stressful experiences, those with a definite history of PTSD, fulfilling theICD10 criteria, may be more vulnerable to a recurrence of their problem although there iscurrently little good evidence available. While such individuals may be unsuitable forrecruitment as operational firefighters because of the potential risk, it may be possible toretain firefighters where specialist opinion supports this. Decisions on fitness forrecruitment should be based on a report from a psychiatric specialist and carefulconsideration.
Outcome of PTSDIf the stressful event occurs in a serving firefighter or control room staff during the courseof their work, the outcome will be very dependent upon response to treatment. Cognitivebehaviour techniques and desensitisation therapies have been shown to be effective. Eyemovement desensitisation and reprocessing (EMDR) has become very commonly used andalthough controversial there is some evidence of efficacy. Anti-depressant medication hasalso been shown to be effective and SSRIs (such as paroxetine) and SNRIs (such asvenlafaxine) have licences for PTSD.
Most individuals recover over a period of six months to a year with little intervention, andwill continue at work. A few will be unable to work, and many of these will recover withtreatment. Some firefighters may recover if removed from the job but may find theirsymptoms relapse on returning to work. As there is little evidence on the question as towhether a previous episode of PTSD makes individuals significantly more vulnerable if re-exposed to similar circumstances, one episode of PTSD related to firefighting should notautomatically bar an individual from further service as a firefighter.
Any decision to retire a firefighter with this diagnosis should be considered very carefullyfollowing appropriate advice from a psychiatric specialist and only after sensible treatmentoptions have been tried and failed.
Critical Incident Support
A small number of individuals who develop PTSR may go on to develop significant longterm problems including PTSD. Medical practitioners became aware that the problem wassignificant and that ‘something needed to be done’ both to treat individuals sufferingPTSR and to try to prevent the problems arising.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
6-14
A significant step in prevention was the development of ‘Critical Incident StressDebriefing’ (CISD), a concept first suggested by Mitchell29 following his work with NewYork firefighters, and subsequently studied by Dyregrov30. However this process has sincebeen rigorously assessed31 and two key issues identified; some individuals benefit from thespecific CISD process while others can be harmed by the process. It should therefore onlybe used by specialists who are in a position to identify those specific individuals whowill benefit.
This does not mean that nothing should be done. It is only the specific CISD processfollowing the Mitchell seven-point plan that should be used with care. There are other lessspecific support mechanisms that are of benefit and should be provided32 33.
General support from colleagues and managers is one of the most important aspects ofgood post-incident management. The other important aspect is identification of thosewho have specific problems and require referral to specialist medical and psychologicalpractitioners. This can be achieved through a risk assessment process. Events that meetthe DSM IV criterion for ‘traumatic’ can be identified, and represent the hazard.Those exposed to the hazard may therefore be at risk of developing post-traumaticstress reactions.
It is accepted that many individuals develop minor, short-term, self-limited PTSR and onlya few will develop clinically significant PTSR. There are no clearly defined strategies foridentifying those firefighters who are at risk of developing clinically significant PTSR, andno evidence that early intervention makes a significant difference. What is important isthat steps are taken to identify firefighters who are developing PTSR and to provideappropriate support.
The task of risk assessment can be carried out by management following appropriatetraining without direct occupational health involvement. Any advice then required orfollow-up of individuals considered to be vulnerable or showing signs or symptoms ofPTSD would then involve occupational health and clinical specialists as appropriate.
A number of organisations are now replacing ‘stress debriefing’ models with ‘stress supportand risk management’ models including the Royal Marines and some police, ambulanceand fire services34. Currently there is the need for more evidence before firmrecommendations can be made, however it is clear that formal Critical Incident StressDebriefing should be used with extreme caution. It is likely that a more general defusing-risk assessment model is most appropriate for the Fire Service.
Schizophrenia
Schizophrenia is a rare condition. The incidence and prevalence of the disorder depend onthe criteria for diagnosis and the populations surveyed but the prevalence in the UK isestimated to be almost 1%. The annual inception rate in various studies has been found tobe around 0.1 per 100035. Some of the features of schizophrenia including thoughtdisorders, delusions and hallucinations could have serious and dangerous effects in thecontext of operational firefighting or the control room.

Mental health problems
6-15
A small proportion of patients with schizophrenia in this country (less than 20%) have acomplete and permanent remission following a single episode36. In others, the conditionwill be only partially controlled or regularly relapsing.
Good prognostic signs include sudden onset, short episode, no previous psychiatric history,prominent affective symptoms, paranoid type of illness, older age at onset, married, goodprevious personality, good work record, good social relationships and good compliance.
It is conceivable that an applicant for the Fire and Rescue Service who has a history of asingle episode of schizophrenia and who has been in complete remission for more than twoyears could be deemed at low risk of recurrence and be considered fit for employment as afirefighter or controller. It seems much more likely that people with a past history ofschizophrenia would either not apply for employment as a firefighter or would be foundunsuitable.
If a single episode occurs in a serving firefighter, it may be inappropriate to retire theemployee until very careful consideration has been given to their prognosis. However, it isunlikely, though possible, that such an individual would be deemed fit to return tooperational firefighting or control room duties.
Deliberate self harm
People harm themselves for a variety of reasons including an intention to end their lifeand a wish to express their desperation but without an intention to die. In either casethere is often a history of long-term relationship or social problems includingunemployment and financial difficulties. In addition there is often an underlyingpsychiatric disorder such as depressive disorder, personality disorder or dependence onalcohol or other substances. There is usually a history of excessive life stresses in thepreceding six months3.
Prognosis for these people is dependent on any underlying condition and its response totreatment in addition to the ongoing life circumstances of the person concerned. Anapplicant for the Fire Service with a past history of deliberate self-harm is at greater risk ofsubsequent psychiatric illness and potential ill health retirement. Where the problemhappened many years previously in response to a particular set of circumstances which areunlikely to recur and the applicant is considered free from any psychiatric disorder, he orshe might be accepted after very careful consideration. Recruits and serving firefighters andcontrollers must be carefully assessed for the likelihood of sudden onset, uncontrolled risksto safety.
Cognitive disorders and organic mental ill health
Any significant current cognitive impairment secondary to organic disease or injury islikely to preclude application for operational roles with the Fire Service. Applicationfollowing full or partial recovery from such a disorder must be judged on its meritsincluding the level of functional ability and the prognosis of the causative condition. Inserving individuals, the prognosis will relate to the underlying condition and judgementsabout ill health retirement cannot be made until this is fully understood.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
6-16
Eating disorders
Eating disorders are most prevalent in young women but can occur in men. Such disordersinclude anorexia nervosa, in which there is significant weight loss together with distortedviews of body image and fatness. The other major category is bulimia nervosa, in whichsubjects binge and vomit and this too is associated with a distorted view of body image.There is also a milder problem of excessive preoccupation with weight and dieting whichis very common and is difficult to distinguish from normal behaviour.
Anorexia is associated with behaviours such as laxative abuse, and the illicit use ofdiuretics, thyroid hormone, appetite suppressants and excessive exercising. This, togetherwith loss of body weight may have serious implications for operational fire fighting.Anorexia nervosa has a poor prognosis and often runs a chronic course. The diagnosis ofcontinuing anorexia nervosa would normally lead to advice not to employ candidates asfirefighters and the consideration of redeployment or medical retirement in those alreadyserving.
Bulimia nervosa is not associated with such a poor prognosis, and in general there is lesslikelihood of physical incapacity. However it can be associated with other mental disorderssuch as depression, personality difficulties and substance abuse, such that the discovery ofsuch a diagnosis should lead to the careful examination for other problems.
The abuse of alcohol and other drugs
Intoxication with alcohol or other substances while on duty is a matter for discipline,which is quite likely to result in dismissal. The medical issues relate to the medicalconditions consequent on longer-term misuse. These will be addressed separately foralcohol and other substances.
Alcohol
Epidemiological evidence from the USA suggests a 1 year prevalence of alcoholdependence between 7% and 10%8. The predominantly male (and some might say macho)culture of the Fire Service might lead to the view that prevalence in this occupationalgroup is at least as high.
In addition to the social effects of excessive drinking, medical effects fall into two generalcategories, physical (including hepatic and neurological conditions) and psychiatric(including psychosis, personality and mood disorders and suicide behaviour). Thephenomenon of dependency is defined in ICD10 by (three out of) six criteria.
Prognosis for psychiatric or physical effects depends on the effect concerned, its severity,and the long-term success or otherwise of withdrawal. In a prospective study in the USA,only 25% of subjects remained abstinent after 6 months and only 10% after 18 monthsalthough 70% had reduced their alcohol intake37.

Mental health problems
6-17
An actuarial assessment of fitness for applicants to whole time service is concerned withthe risk of subsequent medical problems and consequent premature retirement. This islikely to be considered unacceptably high in those with a previous history of alcoholdependency and associated physical or psychiatric disorders even in those who haveapparently made a full recovery.
In serving firefighters and controllers, the assessment is one of the likelihood of suddenonset, uncontrolled risks to safety. Careful consideration will need to be given beforejudging the recovering alcoholic as fit for operational duties.
Other substances
In practice, neither serving staff nor recruits are likely to admit to illicit use of drugs suchas amphetamines, opiates, cocaine, ecstasy, cannabis or hallucinogens. Proven use of suchsubstances which becomes known to management is likely to result in discipline andpossibly dismissal.
The use of performance or muscle enhancing drugs such as anabolic steroids by bodybuilders etc. presents a similar quandary for the medical adviser, particularly where thereare known harmful physical effects. It is not appropriate to discuss ethical issues about thedisclosure of such information in this guidance and other references do cover these issuesin more depth38. There should be a Service policy on drug abuse.
With regards to assessment of fitness for firefighting and the control room, the medicalissues are very similar to those discussed above under alcohol. Physical or psychiatricdisorders apparently resulting from use of and dependency on illicit substances must beassessed separately for their prognosis. Medical Advisers should base advice onemployment on medical issues, relying on the Service policy on drug abuse to deal withany future disciplinary issues.
Treatment with psychoactive medications
In the context of assessing long-term fitness for firefighting, the issues that needconsideration with psychoactive medications are as follows:
Does the drug (or interaction between drugs) cause unwanted effects which might beassociated with an unacceptable risk to safety in operational firefighting?
Does the condition being treated have residual uncontrolled features that might beassociated with an unacceptable risk to safety in operational firefighting?
Will treatment be required in the longer-term? (How long?)
Will withdrawal of treatment carry a risk of relapse of the disorder being treated?

Fire and Rescue Service: Draft Medical Guidelines – June 2004
6-18
Psychoactive drugs usually incompatible with safe firefighting
Drugs that can produce drowsiness, ataxia, impaired vision, impaired co-ordination,impaired judgement/cognition or impaired reaction times are clearly incompatible withsafe firefighting and can be dangerous in the control room. Many drugs cause these effectswithout the patient being aware of them. Those on treatment with the following shouldnormally be excluded from operational firefighting duties:
Benzodiazepines (used as anxiolytics or hypnotics), azapirones, barbiturates,antipsychotic drugs, MAOIs, tricyclic antidepressants, lithium, carbamazepine andsodium valproate.
Low dose treatment with beta-adrenoceptor antagonists for control of symptoms ofanxiety is not in itself a contraindication to operational duties though side effects caninclude undue fatigue on exertion and step test results will be affected. However, carefulconsideration should be given to the effects on safety of the various features of thecondition being treated.
Selective serotonin reuptake inhibitors (SSRIs) lack the anticholinergic and sedativeeffects of tricyclic antidepressants. There is a range of reported gastrointestinal,neuropsychiatric and extrapyramidal side effects but many of these occur early on intreatment and are more obvious to the patient. Ongoing treatment and prophylaxis ofdepression symptoms using SSRIs is not in itself a contraindication to operational duties.However, careful consideration should be given to any possible unwanted effects of the drugin addition to the effects on safety of the various features of the condition being treated.

Mental health problems
6-19
References
1 World Health Organization. The ICD-10 classification of mental and behaviouraldisorders-clinical descriptions and diagnostic guidelines. World Health Organization,Geneva 1992.
2 American Psychiatric Association. Diagnostic and statistical manual of mental disorders(4th edn). American Psychiatric Association, Washington, DC. 1994.
3 Gelder M, Gath D, Mayou R, Cowen P. Oxford Textbook of Psychiatry 3rd Edition,Oxford: Oxford University Press, 1996.
4 Weissman M, Merikangas K. The epidemiology of anxiety and panic disorders. Journalof Clinical Psychiatry 1986;47(Suppl): 11-17.
5 Kedward H, Cooper B. Neurotic disorders in urban practice: A 3-year follow-up. Journalof the Royal College of General Practitioners 1966; 12(2):148-63.
6 Massion A et al. Quality of life and psychiatric morbidity in panic disorder andgeneralized anxiety disorder. American Journal of Psychiatry, 1993; 150(4):600-7.
7 Yonkers KA et al. Phenomenology and course of generalised anxiety disorder. BritishJournal of Psychiatry, 1996j68:308-13.
8 Kessler R, McGonagle K, Zhao S, et al. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States: Results from the national co-morbiditysurvey. Archives of General Psychiatry 1994;51:8A9.
9 Butler G, Cullington A, Munby M, et al. Exposure and anxiety management in thetreatment of social phobia. Journal of Consulting and Clinical Psychology 1984;52:642-50.
10 Marks 1. Fears and Phobias. Heinemann. London 1969.
11 Clark D, Salkovskis P, Hackmann A, et al. A comparison of cognitive therapy, appliedrelaxation and imipramine in the treatment of panic disorder. British Journal ofPsychiatry 1994; 164(16):759-69.
12 Noyes R, et al. Outcome of panic disorder. Relationship between diagnostic subtypesand comorbidity. Archives of General Psychiatry. 1990;47:809-18.
13 Post R M. Rapid cycling and depression in Perspectives. in Psychiatry vol 3 Long-termtreatment of depression. S Montgomery & F Rouillon (eds). John Wiley & Sons.Chichester. 1992.
14 Angst J. How recurrent and predictable is depressive illness? In Perspectives inPsychiatry vol 3 Long-term treatment of depression. S Montgomery & F Rouillon eds.John Wiley & Sons. Chichester. 1992

Fire and Rescue Service: Draft Medical Guidelines – June 2004
6-20
15 Angst J et al. New aspects on epidemiology of depression. In: Angst J, Woggon B (eds)Lofepramine in the treatment of depressive disorders: review of the past 10 years andfuture prospects, pp 1-14. International symposium organised by the PsychiatricUniversity Hospital Zurich, Lugano, 1987. Braunschweig: Vieweg-Veriag. 1988.
16 Piceinelli N, Wilkinson G. Outcome of depression in psychiatric settings. BritishJournal of Psychiatry 1994j64:297-304.
17 Raphael B and Middleton W. After the horror. British Medical Journal 1988;296:1142-3.
18 Summerfield D. The invention of post-traumatic stress disorder and the social usefulnessof a psychiatric category. British Medical Journal 2001;322:95-98.
19 Mezey G, Robbins 1. Usefulness and validity of post-traurnatie stress disorder as apsychiatric category. British Medical Journal 2001;323:561-3.
20 Raphael B et al. Rescuers’ psychological responses to disasters. British Medical Journal1991;303:1346-7.
21 Jackson G. The rise of post-traumatic stress disorders. British Medical Journal1991;303:533-4.
22 McFarlane AC. Life events and psychiatric disorder: the role of a natural disaster. BritishJournal of Psychiatry. 1987;151:362-7.
23 Resnick HS et al. Prevalence of civilian trauma and post-traumatic stress disorder in arepresentative national sample of wornen. Journal of Consulting and ClinicalPsychology 1993;61:984-9 1.
24 Breslau N et a]. Sex differences in post-traumatic stress disorder. Archives of GeneralPsychiatry 1997;54:1044-8.
25 McFarlane AC. The aetiology of post-traumatic morbidity: predisposing, precipitatingand perpetuating factors. British Journal of Psychiatry. 1989; 154:221-8.
26 Kessler RC et al. Post-traumatic stress disorder in the National Comorbidity Survey.Archives of General Psychiatry 1995;52:1048-60.
27 McFarlane AC. Epidemiological evidence about the relationship between PTSD andalcohol abuse: the nature of the association. Addictive Behaviors 1998;23:813-25.
28 Roemer L et al. Emotional response at the time of a potentially traumatizing event andPTSD symptomatology: a preliminary retrospective analysis of the DSMAV criterion A-2. Journal of Behavioural Therapy and Experimental Psychiatry 1998;29:123-30.
29 Mitchell J. When disaster strikes... the critical incident stress debriefing procedure.Journal of Emergency Medical Services 1983;8:36-9.
30 Dyregrov A. The process in Psychological Debriefings. Journal of Traumatic Stress1997;10(4):589-605.

Mental health problems
6-21
31 Wessely S, Rose S, Bisson J, Brief psychological interventions (‘debriefing’) for trauma-related symptoms and the prevention of post-traumatic stress disorder. (CochraneReview) In: The Cochrane Library, Issue 1, 2004. Oxford: Update Software.
32 Kenardy J. (2000). The current status of psychological debriefing. British MedicalJournal 2000;321:1032-3.
33 Palmer 1 and Baron C. Critical incidents and violence at work. In Work and MentalHealth – an employers' guide. Gaskell and Faculty of Occupational Medicine. London2002.
34 N Jones et al. Peer-group risk assessment: a post-traurnatie management strategy forhierarchical organisations. Journal of the Society of Occupational Medicine2003;53(7):469-75.
35 Jablenski A, Sartorius N, Ernber- G, et al. Schizophrenia: Manifestations, incidence andcourse in different cultures. A World Health Organisation 10 country study.Psychological Medicine Monograph (Suppi 20). 1992
36 Bleuler M. The long term course of schizophrenic psychoses. Psychological Medicine1974;4:244-54.
37 Armor D, Polich J, Stambul H. Alcoholism and Treatment. Rand Corporation andInterscience, Santa Monica, CA. 1976
38 Faculty of Occupational Medicine. Guidance on Ethics for Occupational Physicians 4thEdition. F.O.M. Royal College of Physicians. London 1999

CHAPTER 7
Musculoskeletal problems


CHAPTER 7Muscoskeletal Problems
CONTENTS
INTRODUCTION 7-5
UPPER LIMB 7-5
SHOULDER CONDITIONS 7-5
Dislocation 7-5Frozen Shoulder 7-6Rotator Cuff Degeneration and Impingement Syndrome 7-6Acromio Clavicular Joint Subluxation and Dislocation 7-6
ELBOW WRIST AND HAND CONDITIONS 7-7
Epicondylitis – Tennis Elbow/Golfer’s Elbow 7-7The Wrist and Hand 7-7
LOWER LIMB 7-7
THE HIPS 7-7
Osteoarthritis of the Hip 7-8Hip Replacement 7-8
THE KNEE 7-8
Osteoarthritis of the Knee 7-8Knee instability 7-8Meniscal Injuries 7-9Anterior Knee Pain, Chondromalacia Patellae 7-10Patellar Instability 7-11History of Osgood-Schlatter’s Disease 7-12Osteochondritis Dessicans 7-12
THE ANKLE 7-12
Ruptured Tendon Achilles 7-12Ankle Instability 7-12
7-1

Fire and Rescue Service: Draft Medical Guidelines – June 2004
7-2
INTRA-ARTICULAR FRACTURES 7-13
POST TRAUMATIC OSTEOARTHRITIS 7-13
Factors Leading To Post Traumatic Osteoarthritis After Trauma 7-13
SPECIFIC SITES OF INJURY 7-14
Shoulder 7-14Elbow 7-14Wrist Fractures 7-14Hip Fractures 7-15Knee Fractures 7-15The Ankle 7-16The Foot 7-16
METAL IMPLANTS AND SHOULD THEY BE REMOVED? 7-17
Plates and Screws 7-17Intramedullary Nails 7-18Complications of Implant Removal 7-18Summary 7-19
SPINE 7-19
CERVICAL SPINE 7-19
Cervical Rib 7-19Whiplash 7-19Cervical Spondylosis 7-20
LUMBAR SPINE 7-21
History and Diagnosis 7-22Applicants With a History of Back Pain 7-22Does Firefighting Cause Degenerative Disease in the Spine? 7-23Recovery and Rehabilitation 7-23What Treatments Should Be Tried Before Making a Final Decision? 7-24Fairbank-Hall Classification of Low Back Pain 7-24Causation 7-27Lumbar Disc Herniation 7-27Laminectomy, Discectomy and Microdiscectomy 7-28Spondylolisthesis 7-29Spina Bifida 7-29
INFLAMMATORY ARTHRITIS 7-29

Musculoskeletal problems
7-3
Original Authors 1999:
Mr David Campbell FCS, Consultant Orthopaedic Surgeon.
Dr Susan Robson FFOM FRCP, Consultant Occupational Physician and BrigadeMedical Adviser.
Updated 2004 by:
Dr John Etherington MBChB MSc FRCP Consultant in Rheumatology and Rehabilitation.
Mr Ian Nugent FRCS Orth, Consultant Orthopaedic Surgeon, Royal Berkshire Hospital,Reading.
Mr John O’Dowd FRCS Orth, Consultant Spinal Surgeon,Guys and St Thomas’s Hospitals.
Mr Shawn Tavares FRCS Orth, Consultant Orthopaedic Surgeon, Royal BerkshireHospital, Reading.
Dr Tony Williams MFOM, Consultant Occupational Physician, Working Fit Ltd.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
7-4

Musculoskeletal problems
7-5
Introduction
Musculoskeletal problems make up one of the largest groups of disabilities. Unlike manyother medical conditions, they are also common in younger people often resulting fromsporting activities, road traffic accidents and congenital abnormalities.
Firefighting is a physically demanding job and some of the typical tasks required offirefighters produced a high load on the musculoskeletal system. Ill-health retirementstatistics1 for all fire brigade employees for 1999/2000 show:
Medical Advisers will regularly be faced with these problems and as a result will have tomake difficult decisions on fitness for appointment or to continue in service.
There are a number of considerations for assessment:
• Is the individual currently fit to undertake their role?
• Is the individual at risk of sudden incapacity that might affect safety?
• Is the individual at increased risk of developing long-term damage and/or disability asa result of his employment?
• Is the individual at risk of developing long-term problems that will affect fitness andmay require early payment of pension?
This chapter does not intend to be comprehensive, but provides guidance on fitness forthose suffering from the more commonly presenting musculoskeletal problems.
Upper limb
Shoulder conditions
Dislocation
Anterior dislocation of the shoulder is an extremely common injury, usually caused by afall or a wrenching external rotation force. Posterior dislocation is much less common.
After dislocation, there is a risk in the long-term of a painful shoulder with limitedmovement or recurrent dislocation. Fitness for work following dislocation depends to agreat extent on the method of treatment. Even a single dislocation treated with strictimmobilisation for at least three weeks can recur in up to 30% of cases in young men.
Back Upper limb/neck Lower Limb Total
Injury/illness due to service 73 25 39 230
Injury/illness not due to service 78 47 55 545

Fire and Rescue Service: Draft Medical Guidelines – June 2004
7-6
There are grounds for optimism if there has been no recurrence during the preceding twoyears and there is a negative apprehension test. (Backward pressure with arm in ballthrowing position.)
In recurrent dislocation treated with surgery there is a potential risk of further dislocation(5-10%), although the figure may be greater in physically demanding jobs. There is alsothe risk of a painful shoulder or limited mobility as a result of pre-operative damage to thejoint surfaces.
If a dislocation has recurred prior to application, a careful history and examination shouldbe made to determine future risk, with specialist advice sought if the recurrence has beenwithin two years or apprehension test is positive. If a surgical repair has been undertaken, aspecialist opinion should be sought to determine increased risk to the prospectivefirefighter.
Serving firefighters who have had a surgical repair should be reassessed after twelve weeksto determine whether they should be redeployed or are fit to continue.
Frozen Shoulder
Frozen shoulder due to adhesive capsulitis or periarthritis is more commonly found inpatients aged 45-60 years and is usually associated with a history of some kind of trauma.The symptoms (pain, stiffness and limitation of movement) are likely to continue for upto a year or even longer. Steroid injections and/or manipulation under anaesthetic mayhasten recovery. Once the problem has resolved it is unlikely to recur at the same site.
The firefighter may be unfit for operational duties for a period which may exceed a year,and depending on age and experience it may be better to consider temporary or permanentredeployment. Individuals should not return to operational firefighting duties until theyhave a full pain-free range of movement.
Rotator Cuff Degeneration and Impingement Syndrome
In these cases there is a high risk of continuing problems or recurrence, especially in thoseinvolved in physically demanding jobs. Mild cases may respond to steroid injections, butsevere cases may be offered an operation with only 60-80% success rate depending on thedamage.
Acromio Clavicular Joint Subluxation and Dislocation
Injuries to the acromio clavicular joint often follow a fall on the shoulder and therefore arecommonly seen in rugby players and wrestlers. They usually result in no disability or loss offunction, but may take several months to settle. The straps of breathing apparatus mayprove a problem, in which case surgery is a possibility. A functional assessment should becarried out. Individuals with significant problems are likely to have difficulty with thestandard service drills.

Musculoskeletal problems
7-7
Elbow wrist and hand conditions
Epicondylitis – Tennis Elbow/Golfer’s Elbow
This is one of the commonest forms of elbow disorder and is only occasionally due totennis or golf. Most cases follow minor and often unrecognised trauma. Individuals whohave been symptom free for over two years are at low risk of recurrence.
Individuals with a history of pain and tenderness within the last two years are more likelyto develop a recurrence, particularly during recruit training, and they should be advised todefer training until they have been pain free for two years.
Conservative treatment is usually offered initially, but surgery may be an alternative inresistant cases although not always successful. If surgery is successful, the outcome is usuallymaintained long-term.
The Wrist and Hand
Firefighting requires considerable forearm and wrist strength and any defect is likely tolead to long-term problems. Any history of trauma, deformity or medical problems withthe wrist should be fully investigated.
Fractured ScaphoidThis usually results from a fall on the dorsiflexed hand and if ununited often gives rise toosteoarthritis in the long-term. Those with radiological evidence of a well united fracturewith no complications are at low risk of further problems.
Firefighters with a screw in situ or non-union should be assessed by a specialist beforeadvising on employment.
Carpal Tunnel SyndromeThe condition is more commonly found in women and in many cases the cause remains amystery. If treated surgically, symptoms are unlikely to recur. Recruits should not beaccepted until they have been clear of symptoms for at least six months.
Lower limb
The hips
Pain, limp and deformity in the hip most often results from congenital dislocation,childhood hip disorders, Perthes disease, slipped epiphysis, and osteoarthritis.
Where individuals develop and have treatment for hip problems at an early age (less thaneight years) the prognosis is usually excellent. Individuals should be assessed to ensure theyhave a spherical femoral head within an undeformed acetabulum. The majority (70-90%)of patients are pain free at 20-40 year follow up.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
7-8
Where there has been significant trauma to the hip, it is important to seek a specialistopinion to determine the current state of the hip joint. Any signs of deterioration willimply a significant risk of further damage through work as an operational firefighter.The presence of metalwork is covered elsewhere.
Osteoarthritis of the Hip
If there is any significant osteoarthritis of the hip, there will be a risk of further damagethrough work as a firefighter. High levels of physical activity are known to be related toexacerbation of osteoarthritis; retired footballers had more OA of the hip than age andweight matched controls2. Those already employed should be carefully assessed and anydecision on employment should be based on the progress of the disease following specialistadvice. Redeployment would normally be the best option.
Hip Replacement
The risk of complications with hip prostheses, including the newer metal-on-metalresurfacing techniques, is significant in any heavy manual employment. The forces on aresurfaced hip are significantly lower than the torque induced in the femoral shaft from areplacement prosthesis, and a better long-term prognosis should be expected. In general, asuccessful return to full long-term firefighting duties after replacement is unlikely.
Firefighters have been able to return to operational duties after these procedures. Aninternet response among Medical Advisers identified ten firefighters who had recentlyundergone total hip replacement; 7 had reached retirement age and left, or left early on ill-health retirement while the 3 remaining had yet to serve five years post-surgery. Of fivehip resurfacing operations (Birmingham) four were still serving within five years ofsurgery3. There is a significant difference between the physical requirements of a youngfirefighter as against an older more senior fire officer4.
The knee
Five common symptoms in the knee are pain, swelling, stiffness, mechanical disorders(locking, giving way, clicking) and limp. Anyone with a significant history of knee painshould be carefully assessed to exclude underlying pathology.
Osteoarthritis of the Knee
Mechanical factors are likely to contribute to knee osteoarthritis where there is a pre-existing condition. Osteoarthritis is more common in individuals undertaking heavymanual work5. Normal physical activity does not cause osteoarthritis; runners do notdevelop higher levels of osteoarthritis6 7.
Any degeneration will be accelerated by significant physical activity, and therefore putsfirefighters at high risk. Those already in service may continue if symptoms are mild,however specialist opinion should be sought early to ensure they are not at increased risk.Early redeployment is the best option.

Musculoskeletal problems
7-9
Unicompartmental arthritis (usually the medial compartment) may be managed by a hightibial osteotomy in younger patients. This does allow return to manual labour but haslimited efficacy.
Advanced arthritis is managed surgically with either uni-compartmental or total kneereplacement as appropriate. These procedures may preclude kneeling and heavy impactactivities may accelerate wear and produce early failure8 9. Joint replacements are thereforeincompatible with active firefighting. A managerial role is suitable for this group.
Knee instability
This most commonly results from anterior cruciate ligament rupture. Combined cruciateand collateral ligament injuries are often due to high energy injuries. These complexligament injuries are incompatible with active service as a firefighter.
Anterior Cruciate Ligament (ACL) InjuriesThe incidence of ACL rupture is 20 per 100,000 per annum in UK. One third of thesewill have symptoms of disabling instability sufficient to warrant reconstruction, one thirdwill have other symptoms that would justify reconstruction although this is not alwayscarried out and it is thought that one third have no symptoms. A ruptured ACL maypredispose to osteoarthritis and an unstable knee predisposes to damage to the menisci.Following ACL rupture, only 17% are able to return to competitive sports other thancycling and cross-country skiing, while 50% can return to active work (including forestryand construction) and recreational sports such as tennis, basketball and downhill skiing10.
This natural history is incompatible with the functional requirements of the modernfirefighter. Individuals who have recurrent ‘giving way’ of the injured knee should beconsidered unfit for operational firefighting because of the immediate risk to themselvesand others.
Surgical reconstruction of the ACL is recommended for young firemen. No reconstructionis perfect and the biomechanics will always be altered, however this operation does allowelite sportsmen to return to top level sport, and should allow a firefighter to return to fulloperational fitness. Older firefighters may have to consider transfer to non-operationalduties. ACL reconstruction with appropriate rehabilitation has a success rate of 75-90%.Firefighters will not be able to return to operational duty until completion of anaccelerated rehabilitation programme. These programmes usually last 4-6 months.
Potential recruits should only be accepted if they have reconstruction of ACL deficientknees, and only then on the advice of their orthopaedic surgeon; they must understandthat there are risks associated with the operation and subsequent employment by the FireService is not guaranteed.
Revision of torn ACL grafts is possible but currently has a poor success rate. It is possibleto remain in service with lower functional demands.
Specialist opinion should be sought in all cases on the prognosis and return to the highfunctional requirements of active firefighting. This will be dependent on the specificfindings at arthroscopy including the state of the chondral surfaces and menisci.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
7-10
The orthopaedic literature indicates that there may a significant risk of long-termdegeneration of the knee in those who have had ACL reconstructions. There isevidence that degeneration is more likely in the reconstructed knee than in theunreconstructed knee following ACL rupture11 12. It is likely that this process isinevitable regardless of occupation, and the short-term success of top sportsmen,particularly professional footballers who experience far greater and more frequent forceand wear to their knees than firefighters, indicates that firefighting alone should notbe responsible for long-term osteoarthritis.
Posterior Cruciate Ligament (PCL) InjuriesPosterior cruciate ligament rupture in isolation is rare, occurring in around 3.5% of kneeligament injuries. In most cases it is seen as part of a major disruption to the knee, eitheras a result of sporting injury or a motor vehicle crash. Most patients do not havesymptomatic instability and may be able to return to the pre-injury functional level afterrehabilitation. Specialist advice should be obtained before returning to active firefightingduties. The PCL deficient knee may be at risk for medial and patello-femoral compartmentarthritis13 14.
Combined ligament injuries especially the postero-lateral corner has recently beenrecognized as a potent source of on-going instability13 14. Acute repair or reconstruction ofthe postero-lateral structures may be required. Long term results of these procedures arenot available and the prognosis with respect to return to full operational duty should beguarded at best.15.
Collateral Ligament InjuriesIsolated partial tears of the collateral ligaments recover completely with conservativemanagement. They should be treated initially with bracing, partial weight-bearing oncrutches and physiotherapy. If clinically indicated, co-existing cruciate ligament andmeniscal injuries should be ruled out by MRI scanning or arthroscopy. Once an individualhas a full range of movement, no effusion and 80% of normal strength they can safelyreturn to operational firefighting.
A non-operative approach is also adopted for complete rupture of the medial collateralligament with a good prognosis. A longer period of bracing and physiotherapy is required.
Isolated lateral collateral ligament injuries are treated in a similar fashion.
Meniscal Injuries
Meniscal tears can either be traumatic or degenerative in nature.
Degeneration of the menisci is a normal consequence of ageing and is frequently seen onmagnetic resonance imaging (MRI). Degenerative tears have been found in up to 60% ofpeople over the age of 65. The majority of meniscal tears involve the posterior horn of themedial meniscus. Joint line tenderness is the most accurate clinical sign. MRI is the goldstandard for assessment of meniscal disorders. It is a highly sensitive test which can oftenidentify asymptomatic lesions and normal variants.
Symptomatic meniscal tears are usually treated by arthroscopic partial resection. Opencomplete meniscectomy is now confined to the history pages, but there may be servingolder firefighters who have had this procedure. The outcome of this procedure is quite

Musculoskeletal problems
7-11
poor. Following open full meniscectomy up to 23% of patients will show radiologicalchanges within 19 years and 27% will have symptoms. Within 20-29 years, 53% will showradiological changes. Even removing only 25% of the meniscus (by open surgery orarthroscopy) will result in a 350% increase in the pressures on the articular surfaces16.
Isolated meniscal tears are very common, and have good outcomes. Firefighters should beable to return to full duties in 4-6 weeks. They can return to light duties in 1-2 weeks.Arthroscopic partial medial meniscectomies do better than partial lateral meniscectomies.One study reported 88% good to excellent results of arthroscopic meniscal resection in 146patients with an isolated meniscal tear (75% underwent partial medial meniscectomy) atan average follow-up of 15 years. There were some progressive radiographic degenerativechanges but these were only marginally worse than the unaffected leg. Two further studiesreported similar or better outcomes17 18 19.
The prognosis is not as good in patients with associated chronic ACL tears andosteoarthritic changes.
Meniscal repair as opposed to resection is a relatively new technique, and as such there arelimited long-term follow-up data. The overall success rate is 60-85%. One study notednormal knee function in 90% of subjects at an average of 7.5 years follow-up20 whileanother reported average subjective scores of 90/100 on the modified Lysholm scale at anaverage of 5 years follow-up21. Patients are often braced with limitations of knee flexionand squatting for several weeks to protect the repair.
Patients should also be advised that further surgery may be required if the repair fails.Meniscal repair in the ACL deficient knee is doomed to failure without concomitantstabilization. Where there is a combined peripheral meniscal tear and ACL rupture, a goodoutcome has been reported when both are repaired together, however a poor outcome isreported when the meniscus is repaired but the ACL is left deficient22 23 24.
Effects of Degenerative ChangeStudies suggest that the outcome from meniscectomy when degenerative change is presentis significantly worse25 26. Recovery and return to sports is quicker in those with isolatedmeniscal tears as opposed to those with associated degenerative articular changes27.Greater long-term arthritic changes are also noted in those who demonstrate varusmalalignment after medial meniscectomy28 and valgus malalignment after lateralmeniscectomy29.
Advice should be taken from a specialist on both short term risk of collapse and long termrisk of degeneration before advising on future employment. There is no evidence that workas a firefighter will increase the process of degeneration in the knee, however the presenceof early signs of degeneration or damage should be taken into account in advising onemployment as a firefighter.
Anterior Knee Pain, Chondromalacia Patellae
CP presents with patello femoral pain from damage to the patellar articular cartilage.There may be a history of injury or no relevant history. There is likely to be long-term riskof continuing pain and sometimes osteoarthritis.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
7-12
The presence of crepitus and pain on examination is indicative of continued underlyingpathology which is likely to prevent the individual from training effectively. Recruits aretherefore very unlikely to complete the training course. Serving firefighters should beassessed by a specialist, however if the symptoms continue for more than six months,redeployment would be the best option. Surgery does help in some individuals.
Patellar Instability
Patellar instability commonly (but not inevitably) follows direct violence to a flexed knee.The dislocation is more likely to recur if the quadriceps muscle has not been redevelopedor the torn medial capsule has not healed satisfactorily.
There is a significant risk of sudden dislocation while operational; therefore a history ofrecurrent dislocation would generally be incompatible with operational firefighting.Patellar stabilization procedures have an 85% success rate and should be considered inpotential recruits/active firefighters with recurrent instability. A history of singledislocation or a good result from surgery and/or physiotherapy may be compatible withfirefighting.
History of Osgood-Schlatter’s Disease
This is a common condition in young adolescents that usually results from a traction injuryof the patellar tendon on the tibial tubercle. Spontaneous recovery usually occurs. Theresidual bump may cause problems with kneeling. This condition rarely presents after age19/20 years. A history of Osgood-Schlatter’s disease without any other knee problems shouldgenerally be regarded as of minimal significance when assessing fitness for firefighting.
Osteochondritis Dessicans
This condition most commonly occurs in adolescents aged 14-15 years and more usuallyaffects the knee, although can involve the elbow or ankle. It is associated with a risk offuture arthritis, and firefighting duties may contribute significantly to early degeneration.
The ankle
Ruptured Tendon Achilles
Rupture usually occurs only if the tendon is degenerate (avascular); therefore most patientsare aged over 40. Incomplete tears are uncommon. Recurrence is unlikely after satisfactoryrecovery after repair or conservative treatment. Recovery normally takes at least six months.
Ankle Instability
This may be diagnosed on history confirmed by stress x-rays. Mildly unstable ankles mayoccur as a result of ligament strain and may be treated with strapping. More seriousligament tears are treated with physiotherapy and proprioceptive exercises. Surgery forruptured external collateral ligaments has a good success rate.

Musculoskeletal problems
7-13
Firefighters are not generally at increased risk of ankle injuries while wearing boots;however injuries during training are not uncommon. Once recovered, individuals shouldavoid contact sports and take care on uneven ground. Successful operational returndepends on confidence in proprioception. Individuals with persistent severe instability areunlikely to develop sufficient confidence to return to operational firefighting.
Intra-articular fractures
Intra-articular fractures are of particular importance because of involvement of thearticular cartilage and the supporting ligaments around the joints. Fractures throughjoints can affect the stability, range of motion and possible development of post traumaticosteoarthritis. The incidence of post traumatic osteoarthritis depends on the joint involvedand the nature of the fracture30.
The outcome for any particular intra-articular fracture depends upon the original injuryand the nature of the treatment. Early stable fixation allowing prompt mobilisation willreduce stiffness. Early mobilisation with insufficient fixation may lead to osteoarthritis.
There needs to be a distinction made between subsequent function of a joint and adiagnosis of radiological arthritis. A firefighter with X ray evidence of arthritis, e.g. in awrist, may have stiffness, no pain and a functionally normal joint.
It is not always possible to predict the eventual progression of arthritis or whetherparticular physical activities will exacerbate the condition. Post-fracture arthritis dependsupon joint congruity, joint stability and maintenance of normal movement, and survivalof articular cartilage following a blunt injury. Direct trauma to cartilage may producechondrocyte death (chondrolysis) even in the absence of fracture and instability.
Comparison of outcomes of articular fractures between different joints is meaningless andeach must be considered individually. Most research into long-term outcome of fracturesrelies on scoring systems which are different for different parts of the body, and are basedon measurements of range of movement, strength, mal-alignment or x-ray appearances.
Each individual should be assessed on their own merits, with the benefit of a specialistreport. The emphasis on assessment should be on functional capability, and the likelihoodof future employment contributing to any degenerative process.
Post traumatic osteoarthritis
Post traumatic osteoarthritis seen radiographically is usually functionally detrimental.Impairment of function is often a combination of an objective deficit (i.e. loss of movement)and a collection of symptoms which are subjective (i.e. pain). The combination of theseproduces a functional limitation or handicap, which varies from individual to individual.
Factors Leading to Post Traumatic Osteoarthritis after Trauma
Features predisposing to post traumatic arthritis include a residual gap or step in the jointsurface, abnormal soft tissue stability, malalignment or any combination of these features.The progression of arthritis and the significance of it depend on the site of injury. Not all

Fire and Rescue Service: Draft Medical Guidelines – June 2004
7-14
osteoarthritis is significantly symptomatic. A combination of radiological and clinicalexamination is required in most cases when assessing fitness for work. Factors associatedwith poor outcome from articular damage include older age and conservative as opposed tosurgical management.
Specific sites of injury
Shoulder
The majority of shoulder fractures are extra-articular and function is determined by theconcomitant soft tissue injury31. Articular fractures have a high incidence of avascularnecrosis particularly when displaced. Avascular necrosis occurs in less than 10% of extra-articular fractures but in more than 60% of displaced articular fractures32 .
Elbow
Fractures of the distal humerus in the working population are often high energy injuries.However, 75% of patients have satisfactory results after internal fixation33. Significant posttraumatic osteoarthritis occurs in approximately 12% of patients at 6 year follow-up.Fractures of the radial head and ulnar are extremely common and are usually caused bylower energy injuries. Ulnar olecranon injuries are invariably treated with internal fixationand early movement with the majority returning to full activities. Radial head fractures arecommon and caused by a fall onto the outstretched hand. These are classified by Masoninto three types34:
Type 1 – an undisplaced segmental fracture of radial head.
Type II – the fracture segment is displaced with a step of greater than 1mm
Type III – Gross comminution of the radial head
Radial head fractures are often treated non-surgically except for Type II fractures which arefrequently internally fixed. Almost all Type I fractures will heal with minimal functionalimpairment. 80% of patients with Type II fractures whether treated surgically orconservatively will return to their previous employment but with some restriction in rangeof motion. Despite good clinical recovery from this injury degenerative changes are seen inover half of patients on x-ray. The outcome from Type III fractures is generally poor.
Wrist Fractures
Extra-articular fractures whether of the Colles type (dorsal displacement) or the Smith’stype (volar displacement) make a good functional recovery. 75% of patients experiencesubjective discomfort following such injuries for up to a year and up to 10% describefatigability. Fractures that include an intra-articular extension however have a significantlyworse outcome35 36. Comminuted fractures have only 50% satisfactory outcome and this isreduced if the radio-ulnar distal joint is involved. Factors associated with a poor outcomeinclude a dorsal radial tilt of over 10°, radial deviation of greater than 10° and older age.Up to 18% of fractures of the distal radius result in post traumatic arthritis. In youngeradults with higher energy injuries arthritis is reported on x-ray in up to 65% although only30% of patients with radiological evidence are symptomatic.

Musculoskeletal problems
7-15
Hip Fractures
Fractures of the hip comprise two main groups.
acetabular fractures
femoral head fractures.
Acetabular FracturesSignificant fractures of the acetabulum are those which include the weight-bearing dome.Comminution of this area is a significant prognostic sign and presence of a joint articularstep exceeding 2-3mm is significant37. A combined acetabular and femoral head fracturehas a poor prognosis. Patients over the age of 40 have worse results. Following acetabularfractures an accurate prognosis may be given approximately one year following injury. Thefunctional recovery at 12 months reflects the final outcome.
Femoral Head FracturesThe majority of fractures of the femur in the population of working age are extra-capsular(and therefore extra-articular). Intracapsular fractures which are also mainly extra-articularare rare but are often of high impact origin. Minimally displaced fractures (Garden stages Iand II) are internally fixed in situ whereas displaced fractures (Garden III and IV) needreduction and then internal fixation and have a high risk of avascular necrosis. Fractures ofthe femoral neck under 50 years of age are rare because of strong sub-cortical bone and ifthey occur are a sign of high energy impact.
The incidence of avascular necrosis is 14% in Garden I and II fractures and 30% inGarden III and IV fractures. Confirmation of bony union cannot be confirmed until 6months post-injury and any subsequent arthritis should be evident within one year. Latesegmental collapse of the femoral head can occur beyond one year in up to 18%. Somereports in younger patients suggest avascular necrosis as high as 40% in the overall group38.
Knee Fractures
Laubenthal39 advised that average knee movement necessary for sitting is approximately90°, for climbing stairs 100°, crouching 120° but for unrestricted movement for themajority of activities 125° is ideal. Intra-articular distal femoral fractures transgressing theknee inevitably produce a degree of loss of movement. Recovery producing less than 90° offlexion or with a varus/valgus deformity greater than 15° result in significant disability.
Open reduction and rigid internal fixation produce the most satisfactory results40.Anatomical realignment and early movement should obtain good function in more than90% of individuals. The most significant predictor for the development of post traumaticosteoarthritis is an articular surface step of greater than 3mm. Often arthritis affects thepatello-femoral joint rather than the tibio-femoral joint.
Tibial Plateau FracturesTibial plateau fractures are caused mainly as a result of a fall from a height involving acombination of axial loading and a valgus stress. Most of the remaining injuries are causedby lateral impact to the knee such as a strike by the bumper of a car. The most widely usedclassification41 has six types of fracture depending on location of joint surface depressionand cleavage of the plateau. Those of a splint compression type with displacement less

Fire and Rescue Service: Draft Medical Guidelines – June 2004
7-16
than 5mm had 66% excellent results after internal fixation. Medial plateau fractures areoften of high energy impact and have the worst results and are often in poor bone in theolder population. Long term prognosis is significantly worse if there is co-incidentalligament and meniscal injury.
The Ankle
Ankle fracture accounts for approximately 10% of all fractures. It is the most commonlyinjured weight bearing joint and fracture is frequent in the working age population. Anklefractures are of two main types, malleolar fractures and tibial plafond or pilon fractures.
Malleolar FracturesMalleolar fractures may involve the lateral malleolus, the medial malleolus and theposterior malleolus either individually or in combination. The mechanism and severity ofthe injuring force gives a direct indication of the likely outcome. Precise reduction ofmalleolar fractures is essential in obtaining a good result.
Following the treatment of an ankle injury Lindsjo42 concluded that arthritic change willhave occurred by 18 months post-injury and is entirely dependent on the congruity andstability of the joint. Following accepted principals of internal fixation 90% of individualsreturn to the same occupation, 80% continue with sport at the pre-injury level andrecovery in male and female patients is similar. It is evident that an associated fracture tothe posterior malleolus is a poor prognostic factor. Arthritis is evident in 30-40% of suchpatients in the long term.
Tibial Plafond/Pilon FracturesThese injuries are usually more severe than malleolar fractures, particularly whencombined with the above. Recovery is slower and permanent articular surface damagemore likely. Good clinical results may still be achieved in 75% of patients following rigidinternal fixation although non-weight bearing is often required for 3 months post-surgeryand return to active service could be delayed by up to one year. Long term sequelae of thisinjury may not be evident or full recovery achieved for 18 months to 2 years.
The Foot
The most significant fracture of the foot for a firefighter is a calcaneal fracture. It is anoccupational hazard for individuals who work at heights. Of all calcaneal fractures 75% areintra-articular. Displaced fractures are best treated by a specialist familiar with thisparticular injury and require internal fixation43 44. Treated appropriately, 60% will have agood outcome. The rest result in post traumatic osteoarthritis or shortening and wideningof the heel, making boot fitting uncomfortable and walking on uneven surfaces hazardous.Residual symptoms of injury and recovery from the surgery can take 18-36 months to settleand final assessment for return to full active duties may take 2 years.

Musculoskeletal problems
7-17
Metal implants and should they be removed?
The majority of metalwork is implanted for either fracture fixation or as a component ofa joint replacement for the treatment of arthritis or tumour. A member of the Fire Serviceinvolved in full active service is unlikely to be able to continue full duties followingreplacement of a major joint. Each specific joint replacement will be discussed in thesection related to arthritis.
The significant issue related to the active population employed by the fire service ismetalwork implanted in the treatment of trauma. This population is a high risk groupfor fractures both in the service and during recreational sport. The commonest fracturesrequiring fixation are ankle, wrist and forearm fractures usually requiring fixation withplates and screws. Less common but more significant injuries are related to long bone shaftfractures requiring intramedullary nail fixation. These different types of fracture fixationhave their own features and will be discussed separately.
There is no absolute indication for removal of metalwork in an asymptomatic patient. Ifremoval of percutaneous wires or stabilising screws (such as diastasis screws in unstableankle fractures or interlocking bolts in intramedullary nails) is an essential part of fracturemanagement in the early stages, this will have occurred before fracture union. Some fire-fighters could return to light duties in a non active role at this stage but may still needcrutches or be unable to drive or manage stairs safely.
Issues about removing periarticular metalwork usually relate to soft tissue irritationor restriction of movement. There is an argument that screws inserted in subchondralpositions to support articular surfaces in weight bearing joints (such as tibial plateau orankle pilon fracture) do alter the biomechanics of cartilage wear and tear and should beremoved before full active service is resumed.
Following fracture union some prominent metalwork may need removing to allow fullrehabilitation of joint mobility and muscle strength. Once rehabilitated there are very fewindications to remove residual metalwork that is asymptomatic. There is more publishedliterature on the complications associated with removing metalwork than of leaving itin situ.
Plates and Screws
Plates and screws are used in two contrasting techniques to fix fractures. Firstly absolutestability can be achieved by using techniques to compress bone fragments together. This isused to fix articular, periarticular and simple shaft fractures. This promotes healing withminimal callus formation, a situation appropriate around mobile joints.
Secondly plates and screws are used to stabilise highly comminuted long bone shaft fracturesto restore alignment and rotation in a biological way. This controls stability allowing earlyjoint mobilisation but not load bearing and tends to generate callus in abundance.
There are two main reasons for removing plates and/or screws after satisfactory union ofthe fracture. The first is for mechanical reasons, with prominence of the metalworkcausing either pain or pressure on the skin. The second is interference with muscle,ligament or tendon movement. Each case must be assessed on an individual basis.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
7-18
Very occasionally individuals demonstrate an allergic sensitivity to the metalwork anda soft tissue swelling or dermatitis results45 46. Removal of the metal usually resolvesthe problem. Theoretical arguments exist for removing screws and plates related to thebiomechanics of bone and metal. The presence of metal near joints has been discussed.Also it is sometimes suggested that the ends of plates or the sites of screw holes can act as‘stress risers’ and increase the likelihood of fracture at these places. However there is noclinical evidence to support this and it is generally accepted that if further fractures occurat these sites the force that caused the fracture would have broken the bone anyway.
Intramedullary Nails
Nails are generally used to treat diaphyseal (shaft) fractures although the versatility of theiruse for periarticular fractures is increasing. Rotational and axial stability of the fixation isensured by locking bolts or screws drilled through holes in the ends of the nails and thebone. Dynamisation of the fracture can be introduced during treatment by removing thebolts from one end of the nail. This can stimulate consolidation of early callus.
Once a fracture has united and consolidated an intramedullary nail can be left in placewithout detriment. Nails are designed to compliment the biomechanics of the bone theyare implanted in and neither strengthen or weaken the construction in the long term.
Pain at the site of nail insertion is not uncommon. This is usually at the hip for afemoral nail, the knee for a tibial nail and the shoulder for a humeral nail. Often becauseof technical reasons at initial surgery a nail is left slightly proud at the point of insertion.If pain is experienced, removal of the nail can be helpful47. Conversely routine removalof nails previously asymptomatic can cause post surgical pain48.
Complications of Implant Removal
Plates and ScrewsRemoving plates and screws is not an operation without risk of complications.The mechanical weakness of removing a plate and leaving empty screw holes must beappreciated49 50. There is significant risk of damage to blood vessels, nerves and tendonsduring the surgical approach to remove plates, especially in the forearm and upper arm.Risk of refracture is significant51 unless necessary post operative precautions are taken,and far outweighs the risk of complication if the plate is left in place.
The Armed Services have in the past required the removal of lower limb plates and screwsbecause of specific physiological and physical demands of military training. There is noobjective evidence to support this for the Fire Service and firefighters should be assessedon an individual basis.
Firefighters may have specific problems with plates and screws for fixation of claviclefractures. Prominent plates may be painful while wearing a shoulder harness or breathingapparatus. Clavicle fractures are common but internal fixation for clavicle fractures is rare.Often plates are asymptomatic and removal should be assessed on an individual basis.Complications associated with the removal of clavicular plates are minimal.

Musculoskeletal problems
7-19
Intramedullary Nails
If symptoms dictate, intramedullary nails may need to be removed but the surgery is notinsignificant or without complication. Changes in bone architecture and density occurwhile an intramedullary nail is in place52. After removal of an intramedullary nail thispotential weakness must be considered until remodelling occurs over 2-3 months.
Summary
Once metalwork is redundant after completion of bone healing there are no absoluteindications to remove it. All indications are relative and should be discussed with theindividual and the orthopaedic surgeon responsible for his/her care.
Spine
Cervical spine
Cervical Rib
A cervical rib may go unrecognised. However, if known it is necessary to assess carefully asproblems may present in a physically demanding job. Downward and backward traction onthe shoulder wearing breathing apparatus sometimes results in pain and tingling in thearm. Therefore, a functional assessment is recommended.
Whiplash
Whiplash is a term used to describe a group of symptoms associated with an acuteacceleration or deceleration injury to the neck. It may be used to describe the acutesymptoms associated with soft tissue injury as well as the long-term symptoms where thereis no demonstrable physiological or physical underlying cause. Some individuals may havelonger term damage to structures such as the brachial plexus nerve roots, cervical discs oreven the spinal cord itself; these injuries are best considered as separate entitities as theprognosis and management is more specific and defined.
Following acute whiplash injury, a study of 201 patients demonstrated that there is betterpain reduction at six months for those who resume normal activities immediately than forthose who remain off work and immobilized with a cervical collar for the first two weeks53.
There is no evidence that whiplash accelerates the progression of degenerative changes inthe cervical spine54.
There is significant evidence that the pursuit of compensation has an adverse effect on theoutcome following whiplash. The change in the system of compensation in Saskatchewan,Canada to a no-fault compensation approach on 1 Jan 1995 resulted in a considerablereduction in morbidity from whiplash. The reduction in time to settlement from anaverage 433 days to 194 days was associated with an identical reduction in durationof symptoms55.
Fire and Rescue Service: Draft Medical Guidelines – June 2004
7-20
Cervical Spondylosis
Cervical spondylosis is a non-specific term describing any degenerative condition of thecervical spine, including the vertebrae, intervertebral discs and surrounding soft tissue. Neckpain is a common symptom. Besides the mechanical pain associated with degeneration, painand disability can be caused by compression of the spinal cord or nerve roots. Surgery may bea treatment option in some of these cases.
There are two main symptomatic groups of concern with patients. Those with radiculopathyhave pain associated with the distribution of one or more cervical nerve roots, withassociated weakness and reduced reflexes. Those with myelopathy have damage to thespinal cord with associated spasticity and/or weakness in the lower limbs and may have‘numb and clumsy hands’.
As many as 12 percent of women and 9% of men experience pain in the neck at any onetime, and 35% of the overall population can recall an episode of neck pain56. 80% of apopulation of industrial and forestry workers had a history of neck stiffness with arm pain.In a group of male workers in a broad spectrum of jobs 51% had a history of neck painwhile 5.4% had spent some time of work as a result57.
Imaging is not always indicative of significant lesions. 16-26% of asymptomatic patientswere found to have significant cervical spinal cord impingement on MR scans and 15%have root or cord compression58. Over half the population in middle age have radiologicalor pathological evidence of cervical spondylosis59 60. Similarly, 20% of clinically significantlumbar disc herniations may appear normal or with only spondylotic changes on MRscan61 (see below).
The majority of symptomatic cases will not progress to significant disability and someindividuals who are significantly disabled will remain static or improve without treatment62
63. The mean duration of pain in one study was 28-40 months with a range of 5-120months64. There is evidence that surgery may contribute to long-term accelerateddegeneration of the adjacent structures as well as the site of surgery65.
In a community based 15- year study, the annual age-adjusted incidence of cervicalradiculopathy per 100,000 was 107.3 for males and 63.5 for females, reaching a peak of202.9 in the age group 50-54 years. Of 561 patients with cervical radiculopathy, physicalexertion or trauma preceded symptoms in only 14.8% of cases, and confirmed discprotrusion was responsible for symptoms in only 21.9% of cases. The condition recurred in31.7% of patients over a 4.9 year period. Spontaneous improvement within 4.9 years wasreported in 74% of patients66. At the end of the study, 90% of patients were eitherasymptomatic or only mildly incapacitated by their symptoms.
In most cases with pain, activity modification, neck immobilization, isometric exercisesand medication will result in significant improvement. Where pain is the main feature,manual therapy (low velocity passive movements within the normal range rather thanhigh velocity low amplitude manipulation) is considered better than physiotherapy or painrelief67. Mobilisation and or manipulation when combined with exercise have short andlong-term maintained benefits for subacute or chronic mechanical neck disorders68. Theevidence did not favour manipulation and/or mobilisation done alone and neither wassuperior to the other. There was insufficient evidence available to draw conclusions forneck disorder with radicular findings. There appears to be little scientific evidence for theeffectiveness of multidisciplinary biopsychosocial rehabilitation compared with otherrehabilitation facilities for neck and shoulder pain69.

Musculoskeletal problems
7-21
A systematic review revealed relatively strong evidence supporting the effectiveness ofproprioceptive exercises and dynamic resisted strengthening exercises of the neck-shouldermusculature for chronic neck disorders. There was no evidence identified to support theeffectiveness of group exercise, neck schools or single sessions of extension-retractionexercise70. In those with minor non-progressive neurological symptoms simple neckimmobilisation will result in improvement in 30-50% of cases71.
A number of factors affect prognosis. Deterioration is more likely in females and thosewith significantly more cervical mobility72. Worse prognosis is also associated with olderpatients, significant disability at presentation, cord diameter, cord area, altered cord signalon MRI73 and a congenitally narrowed spinal canal.
The outcomes for surgery in mild cases show little or no advantage to surgery overphysiotherapy or soft collar treatment. Although there may be significant improvement inpain, limb paraesthesia, sensory loss and disability at 3-4 months, no difference was foundat one or two years, while some studies show gait scores and the score of daily activitieswere better in conservatively treated patients74 75. The studies available do not showreliable evidence on the effects of surgery and it remains unclear whether the short-termrisks of surgery are offset by any long-term benefit76.
Firefighters are expected to wear helmets and undergo significant physical stress.Although there is no evidence that this will cause early degeneration in the cervical spine,it is likely to exacerbate symptoms associated with degeneration with associated risks tohealth and safety.
Applicants for firefighting service with signs or symptoms considered advanced for theirage should only be accepted if supported by both a specialist report and a consultantoccupational physician. Any history of radiculopathy or myelopathy will be associated witha significant risk of recurrence or degeneration; applicants should not therefore beaccepted with this history.
Because of the widespread nature of the disease, asymptomatic individuals and individualswith minor symptoms associated with general degenerative disease who are already servingshould be considered fit for active firefighting duties. It is important to differentiatebetween those with findings considered normal for their age and those with advanceddisease or clear signs of neurological sequelae.
A judgement will be required where individuals have significant symptoms ofdegeneration particularly with associated ankylosis. Individuals with specific signs orsymptoms of radiculopathy or myelopathy should however be assessed very carefullywith advice from a specialist, although the widespread belief that patients with radicularsymptoms will eventually develop overt myelopathy is not based on good evidence76.Where early improvement of symptoms is noted, a return to active duty should beanticipated. Where symptoms fail to resolve after a year or so, the likelihood of areturn to active firefighting is lower.
Lumbar spine
Low back pain is one of the commonest presenting symptoms in occupational medicine.Six percent of the population report constant disabling back pain over the past 12 monthsand 49-80% will have back pain at some time in their life77. The lifetime prevalence of

Fire and Rescue Service: Draft Medical Guidelines – June 2004
7-22
‘sciatica’ is 4-5%. There are major psychosocial factors affecting the presentation, courseand prognosis of back pain and these frequently complicate rehabilitation and make ill-health retirement decisions difficult.
History and Diagnosis
Medical Advisers will have to rely heavily on the history. It is common for the history todiffer significantly on separate occasions, particularly if clinicians do not have a standardprocess or proforma to follow. It is essential to exclude ‘red flag’ symptoms in every case,and it is useful to identify ‘yellow flags’ early so these can be addressed before they interferesignificantly with rehabilitation78.
Although identifying the cause may be difficult it is important to be proactive in healthand safety, to avoid further injury to this individual or others, and for medico-legal reasons.It is also important to ensure that the cause suggested is reasonable. There must be alegitimate mechanism likely to lead to back pain. For example, a direct blow to the back(such as falling backwards in the supine position) is very unlikely to lead to disc lesionsunless there is major trauma to other vertebral structures.
Most individuals with back pain are capable of working normally and most back painsymptoms recover quickly. In most cases specific treatment is not just unnecessary but canbe harmful because it may cause worry and it may lead individuals to expect medicalpersonnel to effect a cure rather than waiting for the natural healing process to take place.Medical advisers must therefore be confident in assessing low back pain so they canreassure, and identify those few individuals who may benefit from a workplacerehabilitation programme, specific workplace treatment such as physiotherapy, or referralto a specialist clinician for advice or treatment.
A number of guidelines have been developed to assist clinicians in this process, and theFaculty of Occupational Medicine guidelines78 should be the mainstay of assessment andmanagement of low back pain in the workplace.
Patients present with symptoms, but with few signs, most of which are subjective. Theyrarely present with diagnoses, although when they do, these diagnoses are often incorrect.Although specific conditions are discussed below, in many cases a diagnosis will not bemade, and Medical Advisers will have to base decisions largely on presenting history,symptoms and signs.
Applicants with a History of Back Pain
Back pain is very common, and most applicants for the fire service will have had someback pain in the past. Provided the episode of back pain was short lived, and led to littleor no time off work or the individual remained able to participate in normal activitiesthere should be no cause for concern.
Where the individual had more than six weeks off work, or was unable to participate innormal sport or recreational activities, a very careful history should be taken, with asupporting assessment by a specialist if there is any concern that there is an underlyingproblem that may be physical or psychological.

Musculoskeletal problems
7-23
In applicants with a history of lumbar disc herniation it is the impact of symptoms thatis important; this reflects the psychosocial as well as physical liability to future backproblems. A history of absence from work for more than six weeks is a critical factor indetermining future sickness patterns. In general, if the episode was five or more years agoand the individual has been undertaking normal physical activities since, they should beconsidered fit for firefighting.
Does Firefighting Cause Degenerative Disease in the Spine?
It has long been thought that physical activity leads to degenerative disease in the spine.Individuals may therefore claim that the degenerative disease in their backs has beencaused by service as a firefighter.
There is evidence that significant acute injury to the spine may be caused by a specificincident at work, particularly when there is clear evidence of acute trauma at the time.A firefighter in these circumstances would be expected to have attended for acute medicalcare either as a result of back pain or as a result of other trauma, with demonstrable signsand symptoms of an acute injury.
There is, however, evidence that moderate or mixed physical loading results in the leastpathology to the spine; symmetric disc degeneration is associated with sedentary ratherthan active work, while vertebral osteophytes are related to heavy work. Back pain, ratherthan back pathology, is however related to more active work79. There are many studiesthat demonstrate a clear link between physical workload, including frequent bending andtwisting, and low back pain but there is no evidence in most studies linking this work todegenerative conditions in the spine. One study in Dockers who are undergoing constantheavy manual work shows a link to degenerative conditions, although there is no evidencethat a transfer to light duties slows the process of degenerative disease80.
Firefighting does involve heavy manual work at times, but would be best described as‘mixed physical loading’ and therefore represents the optimal activity for the spine.
Recovery and Rehabilitation
A number of factors affect the rate of recovery and rehabilitation besides the underlyingphysical cause. Individuals intending to litigate or in the process of litigation experience amuch slower recovery81. For this reason a number of rehabilitation clinics are reluctant totake litigants because they do not respond to treatment. Smoking is also related to a slowerrecovery, as are a number of other psychosocial factors.
The main factor against successful rehabilitation is the development of illness behaviourand external factors reinforcing this behaviour, where secondary gain may be a keyaspect82 83. The effect of a spouse can be very significant when illness behaviour issupported, and others such as workplace colleagues can also have a major impact inencouraging illness behaviour and reinforcing potential secondary gain. Although well-meaning, this may lead to a situation where the cause of an individual’s pain is thereinforcing behaviour from spouse or colleagues rather than any initial injury.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
7-24
Where the individual is caught in a ‘downward spiral’ of inappropriate coping mechanismsand illness behaviour, it can be extremely difficult to introduce a successful rehabilitationprogramme without a significant change to disrupt the spiral. One factor that may achievethis change is the clear statement that the individual is either not eligible for ill-healthretirement because the condition is not permanent, or that there is insufficient evidence tosupport an injury on duty award. Great care must be taken in analyzing the history,mechanism of potential injury and evidence to support your assessment, in order to avoidfurther reinforcing illness behaviour.
What Treatments should be tried before making a Final Decision?
Lumbar supports may be advocated and are often used for low back pain. There is evidencethat shows they are no better than other forms of treatment for primary prevention, andno evidence that they are effective in secondary prevention. The results may be affected bypoor compliance overall in the various studies and more, better, studies are needed84.
Spinal manipulative therapy is often advocated, either through a physiotherapist,chiropractor or osteopath. Studies of its use in acute or chronic low back pain have shownthat it is no more effective than analgesia, other physical therapies, exercises or backschool, and the profession of the manipulator did not affect outcomes85. It is not superiorto other forms of treatment but may have a part to play in managing some individuals,particularly if they are known to respond well to this treatment.
The use of ‘work conditioning’ programs has been shown to be effective in treatingchronic back pain but not acute back pain86. These programs combine intensive physicaltraining that includes aerobic capacity, muscle strength and endurance and coordination,in a process that is work related, with cognitive behavioural therapy.
Other treatments are covered below under the specific condition. The first line treatmentfrom GPs should be analgesia with physiotherapy following the FOM guidelines or theguidelines from the Royal College of General Practitioners87. Although treatment itself isnot within the remit of the occupational physician, the evidence base behind varioustreatments is covered to enable the Medical Adviser to decide whether all options havebeen explored before definitive decisions on future employability are made.
Fairbank-Hall Classification of Low Back Pain
One useful system of classification that has been validated was first proposed by Fairbankand Hall88. It is outlined below:
Simple or non-specific low back painAttacks occur acutely, with or without obvious precipitating events. Precipitating eventsmay be relatively minor and it is not always helpful to dwell too much on this aspect of thehistory. The patient’s view of what led to the pain may be subjective and is often related tooccupational factors although in practice sport, DIY or other home factors are frequentcauses of acute low back pain.

Musculoskeletal problems
7-25
The pain is generally limited to the lumbar spine and adjacent muscles. There may besome pain referral to buttocks and the back of the thighs, but pain is not felt below theknee. Many patients will describe their symptoms as ‘sciatica’ but this is not a usefuldescriptive term for referred pain that is classically confined largely to the lower back withradiation limited to above the knee. Pain tends to be worse when sitting and improveswith activity.
Ninety percent of acute low back pain attacks settle within six weeks, regardless oftreatment89. Individuals may spend considerable amounts of money on private treatmentthat is not always necessary. Bed rest should not be prescribed, although individuals mayfeel so acutely disabled they require bed rest; in these circumstances it should be limited to3 days89. Analgesia and physical treatments are both useful and because of the shortduration of symptoms, any intervention will, or will be perceived as having, a good effect.
There is moderate evidence that multidisciplinary rehabilitation is effective in treatingsub-acute low back pain and a workplace visit and close liaison with occupational healthproviders increases effectiveness. These interventions may not prove cost-effective andmore research is needed90.
Although these attacks are self-limiting they may be recurrent. This does not imply anunderlying defect or problem even though individuals may state they have a ‘weak back’ ora ‘bad back’.
Chronic Back Pain or Mechanical Back PainThere is no clear distinction between acute, simple back pain, and chronic back pain.Those with chronic pain tend to have persistent underlying pain or discomfort withoccasional acute exacerbations. Some of these individuals have definitive signs fromimaging tests that demonstrate degenerative disease within the lumbar spine, althoughmost individuals with signs of degeneration of the spine in imaging tests are asymptomatic.
The distribution of pain is similar to that of simple back pain, predominantly in the lowerback with some buttock and thigh radiation. Referred pain classically varies in distributionwith intensity, being felt further down the leg the more severe the pain (‘thermometerpain’). This history helps distinguish referred pain from root pain.
It is not helpful to regard chronic back pain as a purely physical ailment. It is bestconsidered in terms of a biopsychosocial model as described by Waddell, with complexinteractions between physical symptoms, mood, and illness behaviour91. The relevanceof all three is very important in determining long-term prognosis.
The older firefighter will inevitably develop a number of psychological issues with shiftwork, family commitments, having to accept that they are less physically able as theybecome older, and having to cope with the normal musculoskeletal aging process. Theseissues may well reinforce the symptoms of low back pain and need to be considered as anintegral part of the management of chronic back pain in the older firefighter.
Physical treatment is in many cases unsuccessful because of the multimodal nature of theillness. Acupuncture has not been shown to be effective92, nor has TENS although thelack of standardization in its use may have hampered researchers93. Advice to stay activehas small beneficial effects when used without other forms of treatment94.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
7-26
Psychological rehabilitation particularly using treatment programmes such as cognitivebehavioural therapy is effective95 96. Multi-disciplinary rehabilitation such as functionalrehabilitation and pain management is also effective97 98, and the use of back schools inthe occupational setting (such as the Penrith rehabilitation facility for firefighters) isthought to be effective99.
Permanent disability in individuals with chronic back pain is not therefore automatic, andmany will make a good functional recovery. Some individuals may have a psychologicalbarrier to returning to active firefighting, but most of these should be capable ofredeployment to more predictable employment that can include significant physical work.
Nerve Root PainIn these patients, the predominant symptom tends to be pain in the leg or legs with adermatomal distribution. This is classic ‘sciatica’.
There may initially be more back pain than leg pain, however in most cases after a fewweeks or months the leg pain takes over as the most important symptom for the patient. Itis not generally possible to distinguish between pain from lateral recess stenosis and painfrom disc herniation on clinical assessment although a careful history may differentiatebetween them.
Pain must be distinguished from numbness which is a ‘red flag’ symptom. Always ask aboutsaddle numbness and incontinence to exclude cauda equine syndrome which is a surgicalemergency. Root pain may co-exist with referred pain, while in many cases root pain is feltin isolation with no back pain. Many of the psychosocial issues described above underchronic low back pain are just as relevant to nerve root pain.
The majority of individuals with nerve root pain, including those where disc prolapse isidentified as the most likely cause, will recover in time and a complete resolution ofsymptoms is the expected outcome.
Non-surgical treatment is not particularly successful. There is no evidence that bed rest100,advice to stay active without other forms of treatment94, traction101, TENS, wearing abrace or corset, or manipulation102 is more successful than placebo in treating nerve rootpain. Epidural steroids may produce short-term relief but no long term functionalbenefit103.
Treatment should therefore be holistic and multi-disciplinary with the expectation ofgradual recovery with time. Exercises do not appear to be specifically beneficial intreatment but may be helpful to increase the return to normal daily activities and work104.
Few individuals should be permanently unfit for firefighting, so any decision on permanentdisability should only be made after all appropriate treatment options have been pursued, andyou have specific advice to this effect from a specialist with expertise in spinal problems.
Nerve root Location of symptoms
S1 Posterior calf and lateral side and sole of foot
L5 Lateral calf and dorsum of foot
L4 Medial calf
L3 Anterior thigh just above knee

Musculoskeletal problems
7-27
Neurogenic ClaudicationIn these patients, the leg pain is provoked by standing or walking, and resolves when theysit or lie down. The underlying condition of spinal stenosis may require nerve root blocksor surgery to relieve symptoms, but a third of patients will improve spontaneously.
UnclassifiableWhere symptoms are unusual, are not relieved by postural change or include rest painor pain at night, these individuals may have a tumour or infection, an isolated fracturesecondary to osteoporosis or steroid use, or psychogenic pain. This group includes anumber of ‘red flag’ signs and symptoms as well as most ‘yellow flag’ symptoms.
Causation
Acute low back pain tends to follow fairly soon after an event or after trauma. There isoften a delay of one to three days before pain ensues, but rarely longer. Annular tears arenot always painful, but when pain does arise it is usually within two weeks of injury.Longer delays would need a convincing explanation such as distracting fractures elsewhere.Root pain, or pain related to disc degeneration may be delayed for much longer.
Lumbar Disc Herniation
Lumbar disc herniation is common. At least 20% of individuals under the age of 60 haveasymptomatic lumbar disc herniation seen on MRI and this number increases above thisage105. After one year, 60% of symptomatic patients were pain free, and remained pain freeat 10 years, while of the small group treated with surgery, 92% were pain free at one yearbut this reduced to the same level of 60% at four and ten years. Of those with some pain,a return to work can be expected and 90% of both groups had returned to work after fouryears106. It is important to appreciate that most studies include a subjective element and‘work’ is not usually well defined. It is likely that fewer would have returned to heavymanual work.
Classic disc herniation occurs when the nucleus pulposus extrudes through and outside theannulus. This process is unlikely to occur in one single event, as there are twenty rings offibres in the annulus running obliquely, with the fibres in each layer running in thecrosswise direction of the adjacent layer. It is thought that the process of herniation isgradual, with the nucleus pulposus penetrating progressively further probably as a result ofsequential insults over time. It is then possible for a relatively small insult such as a sneezeto produce the final rupture of the outermost fibrous ring and produce acute symptoms forthe first time.
There is a nerve supply to the outer layer of the annulus, so incomplete annular tears maybe painful, without any herniation. This may lead to acute or chronic back pain withoutany root symptoms. Although acute pain can be related to the tear in the annulus thatprecedes herniation, remaining symptoms are related predominantly to pressure on nerveroots. Chronic pain may come directly from damaged or degenerative discs. Sciatica causedby disc herniation is diagnosed by the classical signs of root pain (see above) combinedwith a similar radicular distribution of paraesthesia or numbness, a significantly reducedstraight leg raise and a radicular distribution of any other neurological signs (power,reflexes, wasting)107.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
7-28
Lumbar disc herniation is not in itself a problem that should limit firefighting capability.Those who are symptomatic but able to continue with active firefighting should beallowed to do so. Where pain is the predominant symptom, it is reasonable to consider thisaspect in isolation. Both low back pain and sciatic pain reflect cortical stimulation ratherthan a disease process in the lower back108 and are not necessarily proportional to thephysical and inflammatory process in the lower back itself. Pain may be a very realproblem for the individual but does not necessarily imply risk or harm from continuedactivity.
As above, most individuals can expect a recovery within a year sufficient to allow a return tonormal duties. A small number will go on to have recurrences. Of those who have a secondepisode of sciatica, 90% will recover but 50% will have a recurrence of symptoms, while aftera third episode, 90% will recover but almost all will have recurrent episodes106. Individualswho fail to make a good recovery, or in whom symptoms return, may have problems withcalcified disc remnants which may also become dislodged within the spinal canal, and shouldtherefore be investigated with MRI. Individuals with more than one episode of sciaticsymptoms are at significant risk of further symptoms through active firefighting. Applicantsshould not be recruited and firefighters should be carefully assessed after a second episodeand redeployed after three separate episodes of sciatica unless clear supporting advice froma spine specialist is acceptable to the Medical Adviser and the Service.
Laminectomy, Discectomy and Microdiscectomy
Surgical treatment for disc herniation associated with sciatica has seen a significantimprovement in technique over the past twenty years. The operating microscope isreplacing other procedures as the treatment of choice, and the change in terminologymerely reflects a change in tools rather than a different procedure. The reduction in sizeof incision and the more accurate approach possible with the operating microscope hasreduced morbidity, shortened recovery times but not had a major impact on outcomes.
A 70-95% success rate can be expected from discectomy109. Success is a combination ofpain relief and functional improvement, and is largely subjective. It also depends on theparameters measured and the occupation of the individual; successful return to a desk jobdoes not equate to successful return to active firefighting. Firefighters have successfullyreturned to operational firefighting duties; however a number have been unable to sustainthis level of work for more than a few years.
There is no evidence that rehabilitation treatment starting immediately after surgery iseffective, however there is strong evidence that treatments starting four to six weeks aftersurgery are effective. Intensive exercise programs are more effective than mild exerciseprograms in speeding a return to work but there is no difference in long-term outcomes.There is no evidence that patients need to have their activities restricted after first-timelumbar disc surgery, after an appropriate delay and rehabilitation110.
Applicants for the fire service with a history of microdiscectomy are at slightly increasedrisk of developing long-term problems as a part of the normal degenerative process, notspecifically because of the physical nature of the job, and should therefore be very carefullyassessed before advising on employment. Serving firefighters may, after a good recovery andon the advice of a spinal surgeon, return to active duties. They may develop symptoms ofmechanical back pain over time that requires redeployment.

Musculoskeletal problems
7-29
A history of more significant surgery such as cage fusion represents a high risk in activefirefighting. There is as yet little evidence on the long-term outcomes for newer proceduressuch as disc replacement surgery; individual assessment should in these cases be combinedwith expert advice from a spinal surgeon.
Spondylolisthesis
Spondylolysis, a fracture of the vertebral arch (usually a stress fracture in those under 40rather than following a single traumatic event), is present in 9% of the population. Insome individual’s spondylolisthesis, a displacement of the vertebral body may occur. Inolder people, it usually occurs at L4/5 in association with disc degeneration andspondylolysis. Individuals are not at increased risk of trauma to the spine. The backgroundincidence of pain in spondylolysis and spondylolisthesis is no different to that of thenormal population.
Any decision on spondylolisthesis depends on symptoms and the degree of displacement.An expert opinion should be sought before advising on employability.
Spina Bifida
The incidence of spina bifida in Great Britain is approximately 3 per 100,000 live births.There is a wide variation in the severity of the condition. Spina bifida occulta may befound incidentally and the condition may be completely asymptomatic. Any decision torecruit depends entirely on symptoms and functional capability.
Inflammatory arthritis
Many of these conditions including rheumatoid arthritis, psoriatic arthritis, polyarthritisand ankylosing spondylitis are seen in young people and generally lead to chronic pain andmobility problems. Heavy physical work is likely to exacerbate the condition. Individualswith these conditions are therefore very unlikely to be suitable as recruits. Firefighters whodevelop these conditions should be individually assessed, and any decision onredeployment should by guided by expert opinion.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
7-30
References
1 Office of the Deputy Prime Minister Annual Statistics 1999/2000.
2 Klunder KB et al. Osteoarthritis of the hip and knee in retired football players.Acta Orthop Scand 1980; 51:925-7.
3 ALAMA website members forum Dec 2003. http://www.alama.org.uk/
4 Torchia ME et al. Total hip arthroplasty with cement in patients less than twenty yearsold. Journal of Bone and Joint Surgery, American Volume 1996; 78:995-1003.
5 Lindberg H and Montgomery F. Heavy labor and the occurrence of gonarthrosis.Clin Orthop 1987;214:235-6.
6 Lane NE et al. Running, osteoarthritis and bone density: Initial 2-year longitudinalstudy. Am J Med 1990;88(5): 452-9.
7 Konradsen L et al. Long distance running and osteoarthrosis. Am J Sports Med1990;18(4): 379-81.
8 Walsh M et al. Physical impairments and functional limitations: a comparison ofindividuals 1 year after total knee arthroplasty with control subjects. Phys Ther 1998Mar;78(3):248-58.
9 Diduch DR et al. Total knee replacement in young active patients: long term follow-upand functional outcome. Journal of Bone and Joint Surgery, American Volume1997;79(4):575-82.
10 Gillquist J. Outcome measurement after anterior cruciate ligament reconstruction.pp 1187-94 In: Bulstrode C, Bowden G, Buckwalter J, Carr A, Fairbank J, Marsh L,Wilson-MacDonald J (Eds) The Oxford Textbook of Orthopaedics and Trauma. Oxford;Oxford University Press 2002.
11 Daniel DM et al. Fate of the ACL injured patient. A prospective outcome study.American Journal of Sports Medicine. 1994;22:632-44.
12 Allum R. The stiff knee following anterior cruciate ligament reconstruction. In: AllumRL, Fergusson CM, Thomas NP (Eds). Clinical Challenges in Orthopaedics: The Knee.London; Taylor & Francis 2000.
13 Bisson LJ, Clancy WG. Posterior cruciate ligament injuries. pp 879-91. In: Insall JN(Ed) Insall & Scott. Surgery of the Knee. Vol 1 3rd Edn. New York; ChurchillLivingstone 2001.
14 Dowd GSE. The patient with a torn posterior cruciate ligament. In: Allum RL,Fergusson CM, Thomas NP (Eds). Clinical Challenges in Orthopaedics: The Knee.London; Taylor & Francis 2000.
15 Shino K et al. Conservative treatment of isolated injuries to the posterior cruciateligament in athletes. Journal of Bone and Joint Surgery, British Volume 1995;77(6):895-900.

Musculoskeletal problems
7-31
16 Seedholm BB, Hargreaves DJ. Transmission of the load in the knee joint with specialreference to the role of the menisci: part II. Eng Med 1979;8:220.
17 Burks RT et al. Fifteen-year follow up of arthroscopic partial meniscectomy.Arthroscopy 1997;13: 673-9.
18 Rockborn P and Gillquist J. Outcome of arthroscopic meniscectomy, a 13-year physicaland radiographic follow-up of 43 patients under 23 years of age. Acta Orthop Scand1995;66(2):113-7.
19 Schimmer RC et al. Arthroscopic partial meniscectomy: a 12-year follow-up and two-step evaluation of the long-term course. Arthroscopy 1998;14(2):136-42.
20 Eggli S et al. Long term results of arthroscopic meniscal repair. American Journal ofSports Medicine 1995;23(6):715-20.
21 Mintzer CM et al. Meniscal repair in the young athlete. American Journal of SportsMedicine 1998;26(5):630-3.
22 Tenuta JJ and Arciero RA. Arthroscopic evaluation of meniscal repairs – factors thataffect healing. American Journal of Sports Medicine 1994;22:797-802.
23 Horibe S et al. Second look at arthroscopy after meniscal repair. Journal of Bone andJoint Surgery, British Volume 1995;77(2):245-9.
24 Cannon WD. Arthroscopic meniscal repair. pp 521-37. In: Insall JN (Ed) Insall &Scott. Surgery of the Knee. Vol 1 3rd Edn. New York; Churchill Livingstone. 2001
25 Northmore-Ball et al. Arthroscopic, open partial and total meniscectomy: Acomparative study. Journal of Bone and Joint Surgery of Britain 1983;65(4):400-4.
26 Hamberg P et al. Comparison between arthroscopic meniscectomy and openmeniscectomy. Journal of Bone and Joint Surgery of Britain 1984;66(2):189-92.
27 Osti L et al. Partial lateral meniscectomy in athletes. Arthroscopy 1994;10(4):424-30.
28 Maletius W, Messner K. The effect of partial meniscectomy on the long-term prognosisof knees with localised, severe, chondral damage. American Journal of Sports Medicine1996;24(3):258-62.
29 Barrett GR et al. The effect of partial lateral meniscectomy in patients greater than 60years. Orthopaedics 1998;21(3):251-7.
30 Wright V. Post traumatic osteoarthritis - a medico-legal minefield. British Journal ofRheumatology 1990;29(6):474–8.
31 Neer CS. Displaced proximal humeral fractures. Part 1. Classification and evaluation.J Bone Joint Surg Am 1970;52(6):1077-89.
32 Sturzenegger M, Fornaro E, Jakob RP. Results of surgical treatment of multifragmentedfractures of the humeral head. Archives of Orthopaedics and Traumatic Surgery1982;100(4):249-59.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
7-32
33 Wildburger R, Mohring M, Hofer HP. Supraintercondylar fractures of the distalhumerus: results of internal fixation. Journal of Orthopaedic Trauma 1991;5(3):301-7.
34 Mason ML. Some observations on fractures of the head of the radius with a review ofone hundred cases. British Journal of Surgery 1954;42(172):123-32.
35 Lidstrom A. Fractures of the distal end of the radius. A clinical and statistical study ofend results. Acta Orthopaedica Scandinavica 1959;Suppl 41:1-118.
36 Knirk JL, Jupiter JB. Intra-articular fractures of the distal end of the radius in youngadults. J Bone Joint Surg Am 1986;68(5):647-59.
37 Letournal E, Judet R Fractures of the acetabulum. Translated and edited by R A Elson.Springer-Verlag, Berlin 1981.
38 Barnes R, Brown JT, Garden RS, Nicoll EA. Subcapital fractures of the femur. Aprospective review. J Bone Joint Surg Br 1976;58(1):2-24.
39 Laubenthal RN, Smidt GL, Kettelkamp DB. A quantitative analysis of knee motionduring activities of daily living. Physical Therapy 1972;52(1):34-43.
40 Schatzker J, Lambert DC Supracondylar fractures of the femur. Clinical Orthopaedics1979;138:77-83.
41 Schatzker J, McBroom R, Bruce D. The tibial plateau fracture. The Toronto experience1968-1975. Clinical Orthopaedics 1979;138:94-104.
42 Lindsjo U. Operative treatment of ankle fractures. Acta Orthop ScandSuppl.1981;189:1-131.
43 Eastwood DM, Gregg PJ, Atkins RM. Intra articular fractures of the calcaneum. Part I:Pathological anatomy and classification. J Bone Joint Surg Br 1993;75(2):183-8.
44 Eastwood DM, Langmaher VG, Atkins RM. Intra-articular fractures of the calcaneum.Part II: Open reduction and internal fixation by the extended lateral transcalcanealapproach. J Bone Joint Surg Br 1993;75(2):189-95.
45 Hallab N, Merritt K, Jacobs JJ. Metal sensitivity in patients with orthopaedic implants.J Bone Joint Surg Am. 2001 Mar;83-A(3):428-36.
46 Rostoker G, Robin J, Binet O, Blamoutier J, Paupe J, Lessana-Leibo M, Bedoulle J,Sonneck JM, Garrel JB, Millet P. Dermatitis due to orthopaedic implants. A review ofthe literature and report of three cases. J Bone Joint Surg Am. 1987 Dec;69(9):1408-12.
47 Howell GE, Hand CJ, Dodenhoff R. Orthopaedic implant removal at Royal NavalHospital Stonehouse, a three year review. J R Nav Med Serv. 1995 Spring;81(1):39-41.
48 Boerger TO, Patel G, Murphy JP. Is routine removal of intramedullary nails justified.Injury. 1999 Mar;30(2):79-81.
49 Rumball K, Finnegan M. Refractures after forearm plate removal. J Orthop Trauma.1990;4(2):124-9.

Musculoskeletal problems
7-33
50 Bednar DA, Grandwilewski W. Complications of forearm-plate removal. Can J Surg.1992 Aug;35(4):428-31.
51 Sanderson PL, Ryan W, Turner PG. Complications of metalwork removal. Injury.1992;23(1):29-30.
52 Kroger H, Kettunen J, Bowditch M, Joukainen J, Suomalainen O, Alhava E. Bonemineral density after the removal of intramedullary nails, a cross sectional andlongitudinal study. J Orthop Sci. 2002;7(3):325-330.
53 Borchgrevink GE et al. Acute treatment of whiplash neck sprain injuries. A randomisedtrial of treatment during the first 14 days after a car accident. Spine 1998;23:25-31.
54 Hamer AJ et al. Whiplash injury and surgically treated cervical disc disease. Injury1993;24:549-50.
55 Cassidy JD et al. Effect of eliminating compensation for pain and suffering on theoutcome of insurance claims for whiplash injury. N Engl J Med 2000; 16:1179-86.
56 Hult L. Cervical, dorsal and lumbar spinal syndromes. Acta Orthop Scand 1954;17(Suppl):1-102.
57 Hult L. The Munkfors investigation: a study of the frequency and causes of stiff neck-brachialgia and lumbago-sciatic syndromes, as well as obsergations on certain signs andsymptoms from the dorsal spine and the joints of the extremities in industrial and forestworkers. Acta Orthop Scand 1954;16 (Suppl):1.
58 Teresi LM et al. Asymptomatic degenerative disc disease and spondylosis of the cervicalspine: MR imaging. Radiology 1987; 64:83-8.
59 Irvine DH et al. Prevalence of cervical spondylosis in a general practice. Lancet1965;14:1089-92.
60 Hughes JT, Brownell B. Necropsy observations on the spinal cord in cervicalspondylosis. Riv Patol Nerv Ment 1965;86:196-204.
61 Miller GM. Controversies, communication and diagnosis in lumbar disc disease.Presented at the Radiological Society of North America, Chicago, IL, Dec 1-6, 1991.
62 Lees F, Aldren Turner JW. Natural history and prognosis of cervical spondylosis. BMJ1963; 5373:1607-1610.
63 Nurick S. Natural history and results of surgical treatment of the spinal cord disorderassociated with cervical spondylosis. Brain 1972; 95:101-108.
64 Persson LC et al. Cervical radiculopathy: pain, muscle weakness and sensory loss inpatients with cervical radiculopathy treated with surgery, physiotherapy or cervicalcollar. A prospective randomized controlled study. European Spine Journal 1997;6:256-66.
65 Ebershold MJ et al. Surgical treatment for cervical spondylitic myelopathy. Journal ofNeurosurgery 1995; 82:745-751.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
7-34
66 Radhakrishnan K et al. Epidemiology of cervical radiculopathy. A population-basedstudy from Rochester, Minnesota, 1976 through 1990. Brain 1994; 117:325-335.
67 Korthals-de Bos BC et al. Cost effectiveness of physiotherapy, manual therapy andgeneral practitioner care for neck pain: economic evaluation alongside a randomisedcontrolled trial. BMJ 2003; 326:911-6.
68 Gross AR, Hoving JL, Haines TA, Goldsmith CH, Kay T, Aker P, Bronfort G, Cervicaloverview group Manipulation and Mobilisation for Mechanical Neck Disorders(Cochrane Review). In: The Cochrane Library, Issue 1, 2004. Chichester, UK: JohnWiley & Sons, Ltd.
69 Karjalainen K, Malmivaara A, van Tulder M, Roine R, Jauhiainen M, Hurri H, Koes BMultidisciplinary biopsychosocial rehabilitation for neck and shoulder pain amongworking age adults (Cochrane Review). In: The Cochrane Library, Issue 1, 2004.Chichester, UK: John Wiley & Sons, Ltd.
70 Sarig-Bahat H Evidence for exercise therapy in mechanical neck disorders. ManualTherapy 2003;8(1):10-20.
71 McCormack BM, Weinstein PR. Cervical spondylosis. An update. West J Med1996;165(1):43-51.
72 Barnes MP, Saunders M. The effect of cervical mobility on the natural history ofcervical spondylotic myelopathy. J Neurol Neurosurg Psychiatry. 1984 47(1):17-20.
73 Mehalic TF et al. Magnetic resonance imaging and cervical spondylotic myelopathy.Neurosurgery 1990; 26(2):217-27.
74 Persson LC et al. Long-lasting cervical radicular pain managed with surgery,physiotherapy, or a cervical collar. Spine 1997 ;22:751-758.
75 Kadanka Z et al. Conservative treatment versus surgery in spondylotic cervicalmyelopathy: a prospective randomised study. Eur Spine J 2000;9(6):538-46.
76 Fouyas IP et al. Surgery for cervical radiculomyelopathy (Cochrane Review) In:The Cochrane Library, Issue 1, 2003. Oxford: Update Software.
77 Klaber Moffett J et al. Back pain: its management and cost to society. York; Centre forHealth Economics 1995.
78 Carter JT, Birrell LN (Eds) Occupational health guidelines for the management of lowback pain at work – principal recommendations. London; Faculty of OccupationalMedicine 2000.
79 Videman T et al. Lubar spinal pathology in cadaveric material in relation to history ofback pain, occupation, and physical loading. Spine 1990; 15:728-40.
80 Waskiewicz J. The effect of heavy work on the musculoskeletal system of dockers.Bull Inst Marit Trop Med Gdynia 1996; 47:25-32.

Musculoskeletal problems
7-35
81 Anderson JAD. Back pain and occupation. pp 16-37. In: Jayson MIV (ed) The lumbarspine and back pain. Edinburgh; Churchill Livingstone 1987.
82 Fordyce WE et al. Operant conditioning in the treatment of chronic pain. Arch PhysMed Rehabil 1973; 54:399-408.
83 Tollison CD et al. Psychological concepts of pain. In Mayer TG et al (Eds)Conservative Care for Painful Spinal Disorders. Lea & Febiger, Philadelphia 1991.
84 Van Tulder et al. Lumbar supports for prevention and treatment of low back pain(Cochrane Review) In: The Cochrane Library, Issue 1, 2004. Oxford: Update Software.
85 Assendelft WJJ et al. Spinal manipulative therapy for low back pain (Cochrane Review)In: The Cochrane Library, Issue 1, 2004. Oxford: Update Software.
86 Schonstein E et al. Work conditioning, work hardening and functional restoration forworkers with back and neck pain (Cochrane Review) In: The Cochrane Library, Issue 1,2004. Oxford: Update Software.
87 Waddell G, McIntosh A, Hutchinson A, Feder G, Lewis M, (1999) Low Back PainEvidence Review London: Royal College of General Practitioners.
88 Fairbank J. Clinical presentations of the Lumbar Spine pp 505-12. In: Bulstrode C,Bowden G, Buckwalter J, Carr A, Fairbank J, Marsh L, Wilson-MacDonald J (Eds) TheOxford Textbook of Orthopaedics and Trauma. Oxford; Oxford University Press 2002.
89 Waddell G. The back pain revolution. Edinburgh; Churchill Livingstone 1998.
90 Karjalainen K et al. Multidisciplinary biopsychosocial rehabilitation for subacute lowback pain among working age adults (Cochrane Review) In: The Cochrane Library,Issue 1, 2004. Oxford: Update Software.
91 Waddell G. Biopsychosocial analysis of low back pain. Baillieres Clin Rheumatol1992;6:523-77.
92 Van-Tulder MW et al. Acupuncture for low back pain. (Cochrane Review) In: TheCochrane Library, Issue 1, 2004. Oxford: Update Software.
93 Milne S et al. Transcutaneous electrical nerve stimulation (TENS) for chronic loc backpain (Cochrane Review) In: The Cochrane Library, Issue 1, 2004. Oxford: UpdateSoftware.
94 Hilde G et al. Advice to stay active as a single treatment for low back pain and sciatica.(Cochrane Review) In: The Cochrane Library, Issue 1, 2004. Oxford: Update Software.
95 Flor H et al. Efficacy of multidisciplinary pain treatment centers: a meta-analytic review.Pain 1992; 49:221-30.
96 Van-Tulder MW et al. Behavioural treatment for chronic low back pain (CochraneReview) In: The Cochrane Library, Issue 1, 2004. Oxford: Update Software.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
7-36
97 Clinical Standards Advisory Group. Report on back pain. London; HMSO 1994.
98 Guzman J et al. Multidisciplinary bio-psycho-social rehabilitation for chronic lowback pain (Cochrane Review) In: The Cochrane Library, Issue 1, 2004. Oxford:Update Software.
99 Van-Tulder MW et al. Back schools for non-specific low back pain (Cochrane Review)In: The Cochrane Library, Issue 1, 2004. Oxford: Update Software.
100Vroomen P et al. Lack of effectiveness of bed rest for sciatica. N Engl J Med 1999;340:418-23.
101Werners R et al. Randomised trial comparing interferential therapy with motorisedlumbar traction and massage in the management of low back pain in primary care.Spine 1999; 24:1579-84.
102Koes B et al. Spinal manipulation and mobilisation of back and neck pain: a blindedreview. BMJ 1991; 303:1298-1303.
103Watts R, Silagy C. A meta-analysis of the efficacy of epidural corticosteroids in thetreatment of sciatica. Anaesthesia and Intensive Care 1995; 23:564-9.
104Van-Tulder MW et al. Exercise therapy for low back pain (Cochrane Review) In:The Cochrane Library, Issue 1, 2004. Oxford: Update Software.
105Boden SD et al. Abnormal magnetic resonance scans of the lumbar spine inasymptomatic subjects. A prospective investigation. J Bone Joint Surg Am 1990;72:403-8.
106Weber H. Lumbar disc herniation: a controlled prospective study with 10 years ofobservation. Spine 183 8:131-40.
107Waddell G. Evaluation of results in lumbar spine surgery. Clinical outcome measures –assessment of severity. Acta Ortho Scand. 1993 Suppl; 251:134-7.
108Barr JS. Low back pain and sciatica. J Bone Joint Surg Br 1951; 33B:469.
109Papavero L, Caspar W. The lumbar microdiscectomy. Acta Ortho Scand 1993;Suppl 251:34-7.
110Ostelo RWJG et al. Rehabilitation after lumbar disc surgery (Cochrane Review) In:The Cochrane Library, Issue 1, 2004.

CHAPTER 8
Endocrine disorders


CHAPTER 8Endocrine disorders
CONTENTS
INTRODUCTION 8-3
DIABETES MELLITUS 8-3
Classification 8-3Diabetic complications 8-4Glycaemic control and complications 8-5Modern diabetic treatment 8-6Hypoglycaemia 8-7Diabetes and hazardous occupations 8-8Guidelines for individual considerations 8-9Coping strategies for diabetic firefighters 8-10
REFERENCES 8-12
Authors:
Dr Tony Williams MFOM, Consultant Occupational Physician, Working Fit Ltd.
Dr Geoff Gill MD FRCP, Reader and Consultant Physician, Department of Diabetesand Endocrinology, University Hospital Aintree, Liverpool.
8-1

Fire and Rescue Service: Draft Medical Guidelines – June 2004
8-2

Endocrine disorders
8-3
Introduction
Diabetes is a common disorder and is covered below. The clinical presentation, treatmentand outcome are covered in detail to enable Medical Advisers to make an informed riskassessment of both acute and chronic issues in individual cases.
Thyroid disease is also relatively common, particularly among women. Hyperthyroidismcan pose significant problems, while hypothyroidism is generally well controlled byreplacement treatment. Other endocrine disorders are much rarer. An individual riskassessment should be conducted in every case, with supporting evidence from specialists.Medical Advisers should consider in particular the risks of sudden incapacity eitherbecause of the condition or because of treatment.
Diabetes mellitus
Diabetes has an overall prevalence of about 3% in the United Kingdom, though the ratesare much higher in certain sub-groups – notably Asian immigrant populations, the elderly,and those from socio-economically deprived areas. The disease has a serious impact onmortality and morbidity because of its association with long-term small and large bloodvessel disease. It is the most expensive single disease in health care costs, consuming about10% of the UK National Health Service (NHS) budget1.
Classification
The terms ‘type 1’ and ‘type 2’ have now replaced those of ‘insulin-dependent diabetesmellitus’ (IDDM) and ‘non-insulin-dependent diabetes mellitus’ (NIDDM) respectively.Type 1 diabetes predominantly affects the young and is characterised by auto-immunebeta-cell destruction. These patients have effectively no endogenous insulin secretion, andare dependent on externally-delivered insulin for survival. Type 2 diabetes occurs in olderindividuals and is due to a combination of reduced insulin secretion and peripheral insulinresistance. Such patients are usually controllable initially on dietary adjustment alone,though later oral hypoglycaemic agents (OHAs) may be needed, and often eventuallyinsulin.
In Europe, about 15% of the total diabetic population have type 1 disease, and the resthave type 2 diabetes. The incidence of type 1 diabetes in the UK is about 20/100,000 peryear2.
Nowadays, a large number of type 2 diabetic patients are on insulin treatment, and from anoccupational point of view it is often more useful to classify patients as ‘insulin-treated’(i.e. type 1 plus type 2 on insulin) and ‘non-insulin treated’. The most important diabeticcomplication from a work point of view is hypoglycaemia, and this is almost always(though not exclusively) associated with insulin treatment.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
8-4
Diabetic complications
These can be divided into acute and chronic. Acute complications are those of metabolicdecompensation – hypoglycaemia, ketoacidosis (DKA), and hyperglycaemic non-ketoticcoma or pre-coma (HNK). DKA occurs almost always in type 1 diabetes, and HNK in type2. Hypoglycaemia will be dealt with separately later, because of its important relation tohazardous occupations.
Chronic diabetic complications are due to either large or small vessel damage. Large vesseldisease (macroangiopathy) comprises coronary artery disease, cerebrovascular disease, andperipheral vascular disease. The major cause of death in diabetes is coronary artery disease,which carries 2 to 4 times the mortality risk than in non-diabetic individuals3. Small vesseldisease (microangiopathy) affects predominantly the eyes (diabetic retinopathy), thekidneys (diabetic nephropathy), and the peripheral nerves (diabetic neuropathy).
RetinopathyRetinal changes include microaneurysms, haemorrhages, exudates, macular oedema, andnew vessel proliferation (with a risk of bleeding). Retinopathy occurs in both type 1 and 2diabetes. In the early stages this will be an incidental finding on fundoscopy. Howeversome effect on visual acuity may occur during the pre-proliferative stages as haemorrhagesand cotton-wool spots appear, and proliferative retinopathy often results in significantvisual impairment. Visual acuity standards for firefighting will restrict most individualswith proliferative retinopathy to non-operational duties.
In older onset individuals with type 2 diabetes there is a higher initial prevalence ofretinopathy, with 39% of men and 35% of women having some retinopathy in at least oneeye on diagnosis4. In type 1 disease, retinopathy is rare before 5 year’s duration of disease,but rates rise thereafter (dependent on glycaemic control). Some degree of backgroundretinopathy may be present in most diabetic subjects by 20 years duration. Proliferativeretinopathy and maculopathy are the most important forms of retinopathy as they canreduce visual acuity and threaten sight. Some degree of these complications can be presentin up to one-third of diabetic patients by 14 years disease duration5 6.
Treatment of proliferative retinopathy with laser photocoagulation is very successful atslowing the disease progression, but cannot reverse the visual loss. There is a 50%reduction of severe visual loss at two and five years in those with high risk factors and a70% reduction in those with moderate risk. Severe visual loss is defined as an acuity of1/60 or worse. High risk factors are new vessels at the disc covering at least a quarter of thedisc area, new vessels at the disc with vitreous or pre-retinal haemorrhage, or new vesselselsewhere greater or equal to half the disc area with vitreous or pre-retinal haemorrhage7.Full pan-retinal photocoagulation can reduce visual fields by 40-50% bringing individualsbelow DVLA standards for Group 1 driving8.
NephropathyDiabetes-related renal disease affects about one-third of patients, though the severity isvery variable9. Although in many cases there is little direct occupational relevance ofdiabetic nephropathy its presence is an indicator of overall disease severity. Nephropathyrisk rises up to about 15-20 years of disease duration, after which rates remain stable. Aswell as disease duration, glycaemic control affects the risk of nephropathy developing, butthere is also familial clustering suggesting genetic susceptibility10.

Endocrine disorders
8-5
Nephropathy is characterised by initially intermittent followed by persistent proteinuria inthe absence of other non-diabetic causes. Retinopathy is almost invariably present. Later,renal function declines, leading eventually to end stage renal failure. The natural historycan, however, be very long, and many patients die of cardiovascular disease before dialysisor transplantation is necessary.
Treatment of nephropathy includes optimising glycaemic control, strict blood pressurecontrol, and the use of angiotensin converting enzyme (ACE) inhibitors, or angiotensinreceptor blockers. These drugs have a reno-protective effect separate from their action onlowering blood pressure. These therapeutic strategies delay progression to end stage renalfailure, and are also effective in patients with microalbuminuria. Microalbuminuria is apre-clinical phase of diabetic renal disease, when urine protein excretion is abnormal, butnot sufficient to cause dipstick-positive proteinuria (levels are about 30-300 mg/l).
NeuropathyAbout 30-50% of diabetic patients have some degree of peripheral nerve damage. This isusually a symmetrical distal sensory loss, but many other patterns can occur. These includesensori-motor, motor (e.g. amyotrophy), mononeuritis simplex and multiplex, spinalradiculopathies and autonomic loss. The latter can cause a variety of syndromes includingnocturnal diarrhoea (‘diabetic diarrhoea’), profuse vomiting (gastropathy), sweating,bladder dysfunction and erectile impotence. Sensory neuropathy can sometimes be painful,which can be difficult to treat. Drugs such as tricyclic antidepressants, carbamazepine andgabapentin can help as well as good glycaemic control. Some of these patients however areresistant to treatment, and may continue with long-term debilitating symptoms11.
Besides being an indicator of other disease processes, neuropathy can have a significantoccupational impact. This may include a reduction in fine motor skills and reducedpositional awareness leading to balance problems when visual mechanisms are impaired(such as in dense smoke). Sensory loss may also facilitate secondary damage to peripheraltissues and is a common complication in individuals with long-term diabetes; avoidance ofoccupationally-related trauma is important in these circumstances.
Glycaemic control and complications
In the last decade, 2 major studies (one in type 1 and the other in type 2 diabetes) haveconfirmed the long-held belief that good blood glucose control reduces complication risk.The Diabetes Control and Complications Trial (DCCT) was a US study in type 1 diabetes,published in 199312. The United Kingdom Prospective Diabetes Study (UKPDS) was asimilar trial in type 2 diabetes, reported in 199813. Both studies utilised measurement ofwhole blood glycosylated haemoglobin (HbA1c) as the ‘gold standard’ parameter ofglycaemic control (HbA1c reflects mean glycaemia over the proceeding 2 months).
Coincidentally, the intensively controlled group in both the UKPDS and DCCT studieshad a mean HbA1c of about 7.0%. The non-intensively controlled groups had mean HbA1clevels of 8.0% in the UKPDS (type 2), and 9.0% in the DCCT (type 1). Long-termsurveillance in both studies showed significant separations in complication development,strongly in favour of the ‘tightly’ controlled cohort.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
8-6
In the UKPDS study, the intensively controlled group had a 10% reduction in diabetes-related deaths, a 6% reduction in all-cause mortality, and 15% reduction in microvascularcomplications. There was an insignificant reduction in large vessel disease. This study alsoshowed the benefit of tight (<140/85) BP control; a 32% reduction in mortality, 44%reduction in stroke, and 37% reduction in micro-vascular disease13.
The DCCT study demonstrated in their intensively controlled group a 34% reduction inretinopathy, and 60% reduction in nephropathy12. Again large vessel disease prevalencewas not affected. Both studies achieved these results over an approximate 10 years offollow-up.
Modern diabetic treatment
Oral agentsRelatively few patients are nowadays on dietary treatment alone. The range of availabledrugs has greatly increased in recent years:
• Sulphonylureas (e.g. gliclazide, glibenclamide, etc)
• Biguanides (metformin)
• Glucosidase inhibitors (acarbose)
• Insulin secretagogues (repaglinide, netaglinide)
• Thiazolidinediones (pioglitazone, rosiglitazone)
Sulphonylureas and metformin remain the commonest oral agents, but the recentlyintroduced ‘glitazone’ drugs (pioglitazone and rosiglitazone) are in increasing use. Theywork by increasing insulin receptor sensitivity, and can be very effective14. The insulinsecretagogues are also relatively new, and act similarly to sulphonylureas (increasingpancreatic insulin secretion), but are relatively little used15. Acarbose has been availablefor some time, but its use is limited by significant gastro-intestinal side-effects.
From an occupational point of view the important oral hypoglycaemic agents (OHA) arethose which may directly cause hypoglycaemia. These are the sulphonylurea group, andthe insulin secretagogues.
InsulinsTwice-daily mixtures of short and intermediate-acting insulins remain popular – usuallygiven as a 30/70 mixture (e.g. Mixtard 30, Humulin M3). However, there is more flexibilitywith a multiple (usually 4) daily injection system and this is appropriate for shift workersand/or those with unpredictable and potentially hazardous occupations, such as firefighters.
Important recent additions to the insulin formulary are the insulin analogues, or ‘designerinsulins’, where the amino acid chain of the insulin molecule has been altered to affectabsorption characteristics. The short-acting insulin analogues (Lispro and Aspart) mimicmore closely physiological insulin secretion post-prandially16. The long-acting analogueGlargine has a smooth 24 hour absorption profile17.

Endocrine disorders
8-7
The insulin analogues do not usually improve overall glycaemic control as measured byHbA1c levels, but they have been shown to reduce hypoglycaemic episodes – particularlypost-prandially (Lispro and Aspart)16, and nocturnally (Glargine)17. They are thereforepotentially important advances from an occupational viewpoint.
Achieving good control on insulin
Good glycaemic control on insulin treatment requires the following -
• Motivation and education
• Structured care18 19
• Regular blood glucose self-monitoring
• 2-4 daily injection regimens
Achieving good control is however a double-edged sword. Though there are definite long-term benefits of protection from complications, there is also an increased hypoglycaemicrisk (2-3 times the ‘non-intensive’ group in the DCCT study12). However, suchhypoglycaemic excess in reported studies are mean effects, and inside these groups (andindeed in clinical practice) are a number of individuals who do succeed in achievingexcellent glycaemic control with no hypoglycaemia.
Hypoglycaemia
Hypoglycaemic usually results in symptoms when the blood glucose is below 4.0mmol/l.Symptoms are generated both by catecholamine release and reduction in glucose to thebrain. Adrenergic signs and symptoms are pallor, anxiety, sweating, tachycardia, nauseaand hunger. Low brain glucose levels results in headache, blurred vision, cognitiveimpairment, and eventually collapse, fits and coma. Significant changes in brain functionhave been found to occur at plasma glucose concentrations of less than 3.0mmol/l.
Hypoglycaemia in diabetes occurs in patients on insulin or sulphonylurea (including thenew secretagogues) treatment. Other medications do not cause hypoglycaemia, thoughwhen added to insulin or sulphonylureas, they may increase the risk. Attacks ofhypoglycaemia are considered ‘mild’ if they can be self-corrected and ‘severe if they needthird party assistance.
Risk factors for hypoglycaemia include poor education and compliance, erratic dietaryhabits, exercise (especially when brisk and unpredictable), alcohol, renal failure, andintensification of treatment. In both the DCCT12 20 and UKPDS13 studies there was a twoto three times increase in severe hypoglycaemic episodes in the intensively treated groups,compared to those on ‘routine’ therapy. This effect has been found in other studies21. Itremains to be seen whether intensification of control using the recently-introducedanalogue insulins can reduce the attendant hypoglycaemic risks.
A major problem increasing the hazard of hypoglycaemia in insulin-treated diabetes (andspecifically type 1 diabetes) is ‘hypoglycaemia unawareness’ or ‘reduced hypoglycaemiaawareness’. This is usually due to a reduction in the usual counter-regulatory hormoneresponse to early hypoglycaemia, such that patients do not experience their usual

Fire and Rescue Service: Draft Medical Guidelines – June 2004
8-8
premonitory warning signs (e.g. hunger, sweating, dizziness etc). This problem can occur inpatients with long-duration type 1 diabetes, and also when glycaemic control is rapidly andsignificantly improved (though the degree of effect is variable)22 23 24.
Frequent hypoglycaemia itself can lead to reduced awareness25, and can be reversed byinsulin-dose reduction to raise blood glucose levels and prevent hypoglycaemia26.Whatever the mechanism, absent or reduced hypoglycaemic awareness is a significantproblem, increasing the frequency of hypoglycaemic attacks and making them potentiallymore serious27.
Hypoglycaemia in type 2 diabetes may be due to sulphonylurea or secretagogue drugs orinsulin, depending on the therapy used by an individual patient. Attacks are much lessfrequent than in type 1 diabetes, even when insulin is used. In one study severehypoglycaemia was 10 times less frequent in insulin-treated type 2 patients (even whenundergoing intensification of treatment), compared with type 1 patients13 28. This is animportant point occupationally, since a number of diabetic firefighters have insulin-treatedtype 2 (rather than type 1) diabetes.
For patients on sulphonylurea treatment, risks vary with the type of drug used.Chlorpropamide and glibenclamide appear to carry higher risks than the newer shorter-acting drugs (such as gliclazide and glipizide).
Diabetes and hazardous occupations
Hypoglycaemia is the major problem affecting the safety of persons with diabetes inpotentially hazardous occupations. Obviously, many other complications of diabetes willaffect the capacity to work safely and effectively (e.g. reduced visual acuity due toretinopathy, stroke, myocardial infarction, amputation, etc), but these are generally easy todetect or screen for medically. The difficulty with hypoglycaemia is that its detectionusually rests on self-reporting, unless witnessed significant attacks occur in the workplace.This also means that there is the possibility of deception on the part of the diabetic workerresponding to medical enquiries.
Hypoglycaemia in hazardous occupations has obvious dangers, both to the individual andhis or her colleagues. In firefighting, the potential dangers are obvious, particularly duringrescue operations at heights, and using breathing apparatus (BA). As previouslymentioned, diabetic workers at risk are those on sulphonylureas, secretagogues or insulin.There is no risk for those on diet alone, or on treatment with non-sulphonylurea orsecretagogue drugs (e.g. metformin, acarbose and glitazones). Hypoglycaemic risks aremuch greater for those on insulin compared with sulphonylureas, and amongst insulin-treated diabetic persons the risk is greater with those with type 1 disease, than those withinsulin-treated type 2 diabetes.
Formulating guidelines for the safe employment of diabetic persons in the firefightingprofession is difficult, as there is essentially no directly relevant evidence-base. There are,however, some studies involving other occupations, and particularly driving, which areworth reviewing.

Endocrine disorders
8-9
Studies of employment suggest that people with diabetes are no more likely than others tobe unemployed29. For those in work, there is an excess of time off due to sickness, but theexcess is small or non-existent in those whose diabetes is well-controlled30 31 32 33. A smallexcess of problems during shift work has been reported30, but this study is now rather datedand has not been repeated. With modern multiple insulin injection treatment and sensibleself-blood glucose monitoring, few insulin-treated diabetic persons experience significantproblems with shift work34.
Motor vehicle driving has been studied in relation to diabetes-related hypoglycaemia.A study in Scotland of type 1 diabetic drivers35 revealed a crash rate of 5.4 per 100,000miles driven, compared with 9.5 in a comparative non-diabetic group. A similar study oninsulin-treated diabetic drivers in Belfast36 gave figures of 4.9 and 4.8 for the diabetic andnon-diabetic groups respectively. Both studies showed no statistical difference betweendiabetic and non-diabetic crash rates. Similar negative results have been reported in 3separate studies in the USA37 38 39. Only one report has shown a slight excess of accidentsin the diabetic group40. Many of these studies are now rather dated, and have a number ofdesign faults. However, the available evidence is that there is no convincing excess ofaccidents amongst diabetic drivers on insulin treatment. Accidents due to hypoglycaemiacertainly do occur, but they are relatively infrequent, and are presumably offset by themajority of drivers acting in a particularly careful and responsible manner41 42.
The evidence-base concerning diabetes, employment and driving is thus limited andincomplete, but does not give definite evidence of a significant excess risk due to diabetes.Legislation in relation to diabetes varies widely43. In the UK, diabetic persons on insulincannot drive ‘Group 2’ vehicles (large goods vehicles and trucks, and large passenger-carrying vehicles). This excludes firefighters with insulin-treated diabetes from driving fireappliances, for example. In a number of countries however (notably many states in theUSA), insulin treated drivers can drive trucks, provided there is supportive medicalevidence. Even flying planes in the USA and Canada has recently been allowed for pilotson insulin, though a total ban remains in the UK and the rest of Europe.
Guidelines for individual considerations
In the light of the evidence and experience discussed above, Diabetes UK (formerly theBritish Diabetic Association (BDA)) and the American Diabetic Association bothpromote a policy of individual considerations for insulin treated diabetic drivers beingconsidered for potentially hazardous employment (including firefighting). In 1996 theBDA produced the following guidelines for the acceptance of insulin-treated diabeticpersons into potentially hazardous occupations44. These were produced by the BDADriving and Employment Working Party after considerable scrutiny of the literature, andin close consultation between diabetologists, occupational physicians and persons withdiabetes.
Diabetes UK Guidelines for Employment of Insulin-Treated Diabetic Personsin Potentially Hazardous Occupations• People should be physically and mentally fit in accordance with non-diabetic
standards
• Diabetes should be under regular (at least annual) specialist review
• Diabetes should be under stable control

Fire and Rescue Service: Draft Medical Guidelines – June 2004
8-10
• Diabetic persons should monitor their blood glucose and be well educated andmotivated in diabetes self-care
• There should be no disabling hypoglycaemia and normal awareness of individualhypoglycaemic symptoms
• There should be no advanced retinopathy or nephropathy, nor severe peripheral orautonomic neuropathy
• There should be no significant coronary heart disease, peripheral vascular disease orcerebrovascular disease
• Suitability for employment should be re-assessed annually by both an occupationaland diabetes specialist physician, and should be based on the above criteria.
It can be seen that these criteria are strict and stringent, emphasise motivation and self-care, and support the involvement of both occupational physicians and diabetologists. Theguidelines have been widely accepted, and have been used for the individual considerationof insulin-treated diabetic firefighters for operational duties. At present there are 63firefighters in the UK with diabetes on insulin who are fully operational (including BAuse). To date there have been no hypoglycaemia-related incidents in over 600 man-yearsof operational duties by insulin-treated diabetic firefighters45.
The Diabetes UK 1996 guidelines were also adapted for use by the UK Driver VehicleLicensing Agency (DVLA) in 1999, when the licensing of C1 vehicles (small lorries andvans) for diabetic drivers on insulin was allowed by law. This system also has so far workedwell.
The guidelines are specifically for those on insulin, but can be adapted for non-insulintreated individuals with diabetes. Those on sulphonylureas or insulin secretagogues have asmall risk of hypoglycaemia, and the guidelines should be broadly adopted. For those ondiet only, or drugs not associated with hypoglycaemia (metformin, acarbose andglitazones), the 4th and 5th requirements can be omitted (relating to hypoglycaemic attacksand hypoglycaemia awareness, and the requirement for self-monitoring of blood glucose).The 8th requirement (joint annual assessment by occupational physician and diabetologist)can also be discretionary for those not on insulin.
Coping strategies for diabetic firefighters
The experience of the last decade, in which several diabetic firefighters on insulintreatment have been allowed to be fully operational (subject to assessment based on theabove guidelines), has given useful insights into the specific coping strategies adopted bythese individuals to safely maintain a normal work pattern. Different firefighters may usedifferent systems, but there are some common methods used by most, which are listedbelow:
• In depth knowledge of diabetes and self-care strategies
• Commitment and motivation

Endocrine disorders
8-11
• Frequent and sensible self-blood glucose monitoring
• The ability to react appropriately to particular blood glucose levels
• Multiple insulin injection treatment – usually short-acting insulin 3 times daily and amedium or long-acting insulin at bed time
• Use of analogue insulins (eg. Lispro, Aspart, Glargine) which reduce hypoglycaemicrisks
• Available supply of short-acting and long-acting carbohydrate food on person
• ‘Running high’ (in terms of blood glucose) on duty eg perhaps 4-10 mmol/l off duty,but 6-12 mmol/l on duty
• Injecting short-acting insulin after a meal when on duty (in case of a ‘shout’immediately after injecting)
• Taking carbohydrate food in the appliance on the way to an incident.
These techniques and systems of self-care can be usefully suggested or advised tofirefighters recently treated with insulin who, after individual assessment as suggestedabove, are considered fit for operational duties.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
8-12
References
1 Williams R. Prevalence and costs of diabetes in the UK. Modern Diabetes Management2001; 2: 2-4.
2 Lorenzen T et al. Long term risk of IDDM in first degree relatives of patients withIDDM. Diabetologia 1994;37:321-7.
3 Haffner SM, Lehto S, Ronnemaa T, Pylora K, Laakso M. Mortality from coronary heartdisease in subjects with type 2 diabetes and in non-diabetic subjects with and withoutprior myocardial infarction. New Eng J Med 1998; 339: 229-34.
4 United Kingdom Prospective Diabetes Study (UKPDS). Diabetic retinopathy atdiagnosis of non-insulin dependent diabetes mellitus and associated risk factors. ArchOphthal 1998;116:297-303.
5 Klein R et al. The Wisconsin Epidemiologic Study of diabetic retinopathy: XVII. The14-year incidence and progression of diabetic retinopathy and associated risk factors intype 1 diabetes. Ophthalmology 1998;105:1801-15.
6 Klein R et al. The Wisconsin Epidemiologic Study of diabetic retinopathy: XV. Thelong-term incidence of macular oedema. Ophthalmology 1995;102:7-16.
7 Diabetic Retinopathy Research Group. Photocoagulation treatment of proliferativediabetic retinopathy; the second report of Diabetic Retinopathy Study findings.Ophthalmology 1978;85:82-106.
8 Williamson TH et al. Driving standard visual fields in diabetic patients after panretinallaser photocoagulation. Vision in Vehicles, Amsterdam: North Holland 1991;111:265-72.
9 Joss N, Paterson KR, Deighan CJ, Simpson K, Boulton-Jones JM. Diabetic nephropathy:how effective is treatment in clinical practice? Quart J Med 2002; 95: 41-9.
10 Quinn M et al. Familial factors determine the development of diabetic nephropathy inpatients with IDDM. Diabetologia 1996;39:940-5.
11 Benbow SJ, Wallmahmed ME, MacFarlane IA. Diabetic peripheral neuropathy andquality of life. QJM 1998; 91: 733-7.
12 Diabetes Control and Complications Trial Research Group (DCCT). The effect ofintensive treatment of diabetes on the development and progression of long-termcomplications in insulin-dependent diabetes mellitus. New England Journal of Medicine1993;329:977-86.
13 UK Prospective Diabetes Study Group (UKPDS). Intensive blood glucose control withsulphonylureas or insulin compared with conventional treatment and risk ofcomplications in patients with type 2 diabetes (UKPDS 33). Lancet 1998;352:837-53.
14 Aljabri K, Kozak SE, Thompson DM. Addition of pioglitazone or bedtime insulin tomaximal doses of sulphonylurea and metformin in type 2 diabetes patients with poorglucose control: a prospective, randomised trial. Am J Med 2004; 116: 230-5.

Endocrine disorders
8-13
15 Dornhorst A. Insulinotropic meglitinide analogues. Lancet 2001; 358: 1709-16.
16 Bolli GB, Marchi RDD, Park GD, Pramming S, Koivisto VA. Insulin analogues andtheir potential in the management of diabetes. Diabetologia 1999; 42: 1151-67.
17 Younis N, Soran H, Bowen-Jones D. Insulin Glargine: a new basal insulin analogue.QJM 2002; 95: 757-61.
18 Griffin S, Kinmonth AL. Systems for routine surveillance for people with diabetesmellitus (Cochrane Review) In: The Cochrane Library, Issue 1, 2004. Oxford: UpdateSoftware.
19 Renders CM et al. Interventions to improve the management of diabetes mellitus inprimary care, outpatient and community settings (Cochrane Review) In: The CochraneLibrary, Issue 1, 2004. Oxford: Update Software.
20 DCCT Research Group. Epidemiology of severe hypoglycaemia in the Diabetes Controland Complications Trial. Am J Med 1991;90:450-9.
21 Bott S et al. Intensified insulin therapy and the risk of severe hypoglycaemia.Diabetologia 1997;40:926-32.
22 Amiel SA et al. Defective glucose counterregulation after strict control of insulin-dependent diabetes mellitus. N Eng J Med 1987;316:1376-83.
23 Amiel SA et al. Effect of intensive insulin therapy on glycaemic thresholds for counter-regulatory hormone release. Diabetes 1988;37:901-7.
24 Berger M, Muhlhauser I. Implementation of intensified insulin therapy: a Europeanperspective. Diabetic Medicine 1995:12:201-8.
25 Fanelli CG et al. Meticulous prevention of hypoglycaemia normalises glycaemicthresholds and magnitude of most of the neuroendocrine responses to, and symptoms of,and cognitive function during hypoglycaemia in intensively-treated patients with short-term IDDM. Diabetes 1993;42:1683-89.
26 Cranston I et al. Restoration of hypoglycaemia awareness in patients with long-standinginsulin dependent diabetes. Lancet 1994;344:283-7.
27 Gold AE, MacLeod KM, Frier BM. Frequency of severe hypoglycaemia in patients withtype 1 diabetes with impaired awareness of hypoglycaemia. Diabetes Care 1994;17:697-703.
28 Miller CD, Phillips LS, Ziemer DC et al. Hypoglycaemia in patients with type 2diabetes mellitus. Arch Int Med 2001; 161:1653-9.
29 Ardron M, MacFarlane I, Robinson C. Educational achievements, employment andsocial class of insulin-dependent diabetics: a survey of a young adult clinic in Liverpool.Diabetic Medicine 1987; 4: 546-8.
30 Robinson N, Yateman NA, Protapapa LE, Bush L. Employment problems and diabetes.Diabetic Medicine 1990; 7: 16-22

Fire and Rescue Service: Draft Medical Guidelines – June 2004
8-14
31 Griffiths RD, Moses RG. Diabetes in the workplace. Employment experience of youngpeople with diabetes mellitus. Med J Aust 1993; 158: 169-71.
32 Poole CJ, Gibbons D, Calvert IA. Sickness absence in diabetic employees at a largeengineering factory. Occup Envir Med 1994; 51: 299-301.
33 Waclawski ER. Sickness absence among insulin-treated diabetic employees. DiabeticMedicine 1990; 7: 41-4.
34 Waclawski ER, Gill GV. Diabetes mellitus and other endocrine disorders. In: ‘Fitness forWork – the medical aspects’, Eds Cox RAF, Edwards FC, Palmer K. Publs OxfordUniversity Press 2000, pp 322-34.
35 Eadington DW, Frier BM. Type 1 diabetes and driving experience: an eight year cohortstudy. Diabetic Medicine 1989; 6: 137-41.
36 Stevens AB, Roberts M, McKane R, Atkinson AB, Bell PM, Hayes JR. Motor vehicledriving among diabetics taking insulin and non-diabetics. BMJ 1989; 299: 591-5.
37 Songer TJ, LaPorte RE, Dorman JS et al. Motor vehicle accidents and IDDM. DiabetesCare 1988; 11: 701-7.
38 Davis TG, Wehling EH. Oklahoma’s medically restricted drivers. A study of selectedmedical conditions. J Okla State Med Assoc 1973; 66: 322-7.
39 Waller JA. Chronic medical conditions and traffic safety. Review of the Californiaexperience. N Engl J Med 1965; 273: 1413-20.
40 Hansotia P, Broste SK. The effect of epilepsy or diabetes mellitus on the risk ofautomobile accidents. New Eng J Med 1991; 324: 22-6.
41 Macleod KM. Diabetes and driving: towards equitable, evidence-based decision-making.Diabetic Medicine 1999; 16: 282-90.
42 Macleod KM, Johnston RV. Should there be driving and employment restrictions forpeople with diabetes? In: ‘Difficult Diabetes’. Eds Gill GV, Pickup JC, Williams G. PublBlackwell Science 2001, pp 237-57.
43 Mawby M. Time for the law to catch up with life. Diabetes Care 1997; 20: 1640-1.
44 British Diabetic Association. Diabetes and Potentially Hazardous Occupations. London.BDA; 1996.
45 International Register of Firefighters with Diabetes (IRFD), 2004.http://welcome.to/irfduk

CHAPTER 9
Gastro-intestinal disorders


CHAPTER 9Gastro-intestinal disorders
CONTENTS
INTRODUCTION 9-3
Irritable Bowel Syndrome 9-3
INFLAMMATORY BOWEL DISEASE 9-5
Crohn’s Disease 9-5Ulcerative Colitis 9-6
REFERENCES 9-8
Authors:
Dr Ian Gemmell, MB ChB MSc MA(Law) MFOM, Consultant OccupationalPhysician, Employment Medical Services Ltd.
Professor Derek Jewell, Professor of Gastroenterology, University of Oxford.
9-1

Fire and Rescue Service: Draft Medical Guidelines – June 2004
9-2

Gastro-intestinal disorders
9-3
Introduction
Gastro-intestinal disease may have an adverse impact on an individual’s career in theService in terms of:
• Nutritional status
• Persistent or recurrent abdominal pain
• Risk of incapacity
• Risk of soiling
• Risk of haemorrhage.
Many abdominal conditions are associated with an increased tendency to sickness absenceand a heightened risk that a full career term will not be completed.
The assessment of every individual requires each of these areas to be reviewed with regardto knowledge of the severity of the disorder, its likely rate of progression and thecharacteristics of the proposed job. There may be profound health and safety concerns inrelation to firefighters but relatively few concerns in other areas of the service.
Much of the text regarding incidence rates and prognosis has been taken from Section 14of: Warrell, David, Cox, Timothy M, Firth, John D, Benz, Edward J. The Oxford Textbookof Medicine. 4th Ed. OUP, Oxford, Feb 2004.
Irritable Bowel Syndrome
Irritable Bowel Syndrome (IBS) is a syndrome of:
• abdominal pain that is relieved by defaecation and an associated change in frequencyand/or stool consistency
together with one or more of the following symptoms:
• altered ease of defaecation
• passage of mucus
• sensation of bloating.
The condition is generally diagnosed by gastroenterologists according to the ‘Rome IIcriteria’ which require 12 weeks of symptoms in a 12 month period. They are a stricterversion of previous criteria and some patients previously given the diagnosis may now bereclassified 1 2. Milk products may exacerbate the condition but lactose intolerance is nocommoner amongst IBS sufferers than in the general population (5%)3. On the otherhand, a British study found that 22% of IBS sufferers had co-existing coeliac disease(coeliac disease affects less than 1% of the general population)4.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
9-4
Diagnosis tends to be made on the history and a few simple investigations to excludealternative pathologies. Individuals would be expected to have rectal examination, faecaloccult bloods, full blood count, erythrocyte sedimentation rate and C-reactive protein.There are a number of ‘alarm features’ that indicate alternative pathologies including5:
Significant weight loss Persistent diarrhoea Family history of inflammatory bowel disease
Onset after 50 years Tropical travel Family history of bowel cancer
Intestinal obstruction Malabsorption Abdominal mass
Faecal occult blood Overt rectal bleeding Arthritis
Individuals with mild symptoms, no alarm features and who don’t meet the Rome IICriteria are considered to have some other functional enteric disorder. For those who meetthe Rome II criteria but have alarm features, other pathologies including Crohn’s disease,ulcerative colitis and adenocarcinoma may need to be excluded.
One of the major features of IBS is the link between anxiety and exacerbation of thesyndrome. There is convincing evidence that psychiatric disease and abnormal illnessbehaviour are more prevalent in patients with irritable bowel syndrome. Sufferers tend tohave more than twice the average rate of sickness absence and GP attendance6 7 8. Therelationship between the psychological problem and any neuromuscular abnormalityremains uncertain, although it is recognized that a heightened awareness of visceralsensation is a feature of affective disorders, particularly depression. To this end, tricyclicantidepressants can play a role in the management of IBS9.
IBS affects about 15-25% of the population. Because it increases sickness absence andalters the perception of illness, and consequently changes illness related behaviour, there isa significant impact on the economy.10 Occupations most suited to someone with moderateto severe IBS possess characteristics which will promote the individual’s autonomy whilstprotecting them from conflict or other stressful situations and allow for adequate rest.Work characteristics may therefore include routine work patterns, regular hours,uninterrupted sleep, protection from conflict or confrontation and roles where short termabsences of little or no notice will have minimal effect on the workplace.
The shift patterns, work characteristics of fire fighters and control staff therefore may notbe suited to someone diagnosed as suffering from IBS. Decisions on employment should bebased on previous history of the illness in relation to employment and the severity ofsymptoms.

Gastro-intestinal disorders
9-5
Inflammatory bowel disease
Twelve to eighteen percent of people with IBD may have one or more family membersaffected. The link is strongest for Crohn’s Disease where specific gene mutations have beenidentified. Therefore a family history of inflammatory bowel disease may indicate apredisposition to developing IBD11.
Crohn’s Disease
Crohn’s disease is a chronic inflammatory process of the small and large bowel consistingof ulceration, submucosal oedema, fibrosis, and mesenteric lymphadenopathy. It may affectany part of the alimentary tract, is usually interspersed with lengths of normal bowel (skiplesions) and in the majority of cases is confined to the terminal ileum.
The typical patient with Crohn’s disease has recurrent episodes of abdominal colicpreceding diarrhoea. Bleeding is unusual outside periods of active disease, howevermacrocytic or a mixed anaemia is common because the absorption of bile salts andVitamin B12 is adversely affected. As the absorption of bile salts is affected, the absorptionof fats and the fat soluble vitamins (A, D E and K) is also affected leading to significantmalnutrition.
Age of initial presentation is usually between 20 and 40. Cause appears to be an interplaybetween genetic predisposition and environmental factors such as smoking (relative risk6). The disease may be managed using salicylate derivatives but this is only beneficialwhen the colon is affected. It is of marginal benefit in small bowel disease. Active diseaseis generally managed using systemic steroids or elemental diets. Long term steroiddependency may warrant immunosuppressive agents such as Methotrexate or Azathioprine.
Crohn’s disease is unpredictable. In a small minority, the disease appears to be short livedand resolves after a handful of attacks. In most, however, the disease is progressive overtheir lifetime but with periods of remission. Because the granulomatous inflammationaffects the entire thickness of the intestinal mucosa, ulceration and fistulae often develop.At best these affect nutrition and at worst lead to severe disability. Even in relatively mildcases, the abdominal pain of an acute attack can last from several hours to several days andconfine the person to bed. During an exacerbation, a rapid build up of stool may lead to asudden and irresistible urge to defaecate, leading to soiling.
The most common complications of Crohn’s disease are stenoses, dilatation, perforation,fistulae, intestinal obstruction, perianal fistulae and abscesses12. Colonic Crohn’s disease isassociated with colonic adenocarcinoma in a similar way to ulcerative colitis although theincidence is 8-10% after 20 years. Ileal malignancy and amyloidosis are also seen but areless common. External fistulae are less common and usually only follow abdominal surgery.
About 75% of patients will receive surgical treatment during the course of their illness.After a resection, the symptoms recur in about 30 per cent of patients in the subsequent5 years and in 50 per cent of patients by 10 years. Half will require further surgery. Ingeneral, mortality from Crohn’s disease is twice that expected in the general population.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
9-6
Considerable morbidity can be expected and this may translate into regular sicknessabsence. About 10% are forced to change careers, 23% of sufferers cannot undertake fulltime work and 10% are on long-term pensions.13 In general, Crohn’s disease has a greatereffect on employment than ulcerative colitis.14 Additionally, Crohn’s disease has a similarassociation with psychological disturbance as irritable bowel syndrome and many sufferersdisplay a predisposition to anxiety which then triggers an attack7 8 9. Whilst this may be along-term reaction to chronic pain, low dose anti-depressants with anxiolytic activity havebeen shown to improve the quality of life and reduce the frequency of severe relapses10.
Ideal working conditions for someone with Crohn’s disease therefore reflect those for IBS:regular hours, autonomy, low stress and roles where ‘cover’ for sudden absence exists.
Individuals with Crohn’s disease are therefore unlikely to be considered fit for firefighting,and should be considered carefully, with expert opinion being sought, beforerecommending employment in the control room. Any decision on employment should bedelayed eighteen months to identify the outcome of treatment, or twelve months followingsurgery.
Ulcerative Colitis
Unlike Crohn’s disease, ulcerative colitis is confined to the large intestine. It alwaysinvolves the rectum, extending proximally in a continuous band of inflammation andulceration. ‘Skip lesions’ where normal mucosa interrupts patches of inflammation are notseen. About 40% of patients have disease confined to the rectum and sigmoid colon and20% have disease affecting the entire colon. The typical presentation is of mucus riddenblood stained diarrhoea and in severe cases the stool resembles anchovy sauce. Abdominalpain is much less of a feature than with Crohn’s disease or IBS, however urgency todefaecate is a greater problem because of the loss of elasticity of the inflamed rectum andits proximity to the anus.
Because involvement of the terminal ileum is unlikely, fat absorption is generally normaland so malnutrition and extreme weight loss are unusual except in severe disease. In longstanding severe disease the colon becomes shortened and featureless. Strictures areuncommon – unlike Crohn’s disease. Disease classification is as follows:
There are several concerns regarding ulcerative colitis. The onset of an attack ischaracterised by a disabling bloody diarrhoea which often carries little warning. As a resultit interferes with mobility and leads to sickness absence. The risk of haemorrhage is greaterin ulcerative colitis than in Crohn’s and a severe attack may cause collapse and warranthospitalisation, although this is unusual after the first year. Long term ulcerative colitiscarries with it a risk of adenocarcinoma in 7-15% of cases at 20 years with very little riskup to the 15 year point.
Mild < 4 stools daily, +/- blood, no systemic disturbance and a normal ESR
Severe > 6 stools daily, + bleeding, systemic illness with fever, tachycardia and anaemia.Raised ESR and C-reactive protein.

Gastro-intestinal disorders
9-7
Extra-intestinal effects of ulcerative colitis include:
• Erythema nodosum in 2% of patients
• Pyoderma gangrenosum in 2%
• Anterior uveitis in 8% of patients
• An asymmetric large joint arthropathy in 10-15% of ulcerative colitis sufferers andsacro-ileitis in 12-15%. It has only a weak association with HLA B27 and rarelyprogresses to ankylosing spondylitis.
Treatment of mild disease is dependant on salicylate derivatives which reduce theincidence of relapses fourfold. Steroid enemas have more use in ulcerative colitis thanCrohn’s and many people with ulcerative colitis can remain well controlled on relativelylow doses of topically applied steroid. Most patients with ulcerative colitis haveintermittent attacks of the disease, but the duration of remission between attacks variesfrom a few weeks to many years and 10-15% of patients will have a chronic continuouscourse and rarely achieve a full remission. Few, if any, have one attack and no relapse.
Between 5 and 10% will have a severe first attack due to extensive or total disease andthey are much more likely to proceed to colectomy. The severity of attacks in the first yearof the disease is a good prognostic indicator and about 25% of people with severe diseaserequire urgent colectomy at some time. Most will have an ileal pouch fashioned and thiswill require emptying 6-12 times a day. The incidence of pouchitis is 40%.
However, a year after diagnosis, the risk of subsequent colectomy falls to a cumulative rateof about 1% per year in all groups of the disease. Patients with disease limited to therectum (proctitis) are a special group, in so far as most of them continue to have limitedinvolvement, and only about 30% develop more extensive disease over 20 years. Despitehaving a chronic relapsing disease, 90% of ulcerative colitis sufferers are able to work withsurprisingly little sickness absence. Nevertheless, quality of life can be impaired in manypatients and rapid access to toilet facilities may prove to limit employability.
While individuals with mild disease may be fit to serve as firefighters, individuals withmoderate to severe disease are unlikely to be able to cope. As with Crohn’s disease, aperiod of eighteen months should be allowed before making a firm decision onemployment to allow for the disease process to stabilize. Those who have had a goodoutcome from surgery may be considered fit after allowing twelve months to stabilize.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
9-8
References
1 Mearin F, Roset M, Badia X, Balboa A, Baro E, Ponce J, Diaz-Rubio M, Caldwell E,Cucala M, Fueyo A, Talley NJ. Splitting Irritable Bowel Syndrome: From Original Rometo Rome II Criteria. Am J Gastroenterol. 2004 Jan;99(1):122-130.
2 Mearin F, Badia X, Balboa A, Baro E, Caldwell E, Cucala M, Diaz-Rubio M, Fueyo A,Ponce J, Roset M, Talley NJ. Irritable bowel syndrome prevalence varies enormouslydepending on the employed diagnostic criteria: comparison of Rome II versus previouscriteria in a general population. Scand J Gastroenterol. 2001 Nov; 36(11):1155-61.
3 Tolliver BA, Jackson MS, Jackson KI et al. Does lactose maldigestion really play a rolein the irritable bowel? J Clin Gastroenterol. 1996;23:15-17.
4 Sanders DS, Carter MJ, Hurlstone DP et al. Association of adult celiac disease withirritable bowel syndrome: a case control study in patients fulfilling ROME II criteriareferred to secondary care. Lancet. 2001;358:1504-8.
5 Talley NJ. When to conduct testing in patients with suspected Irritable BowelSyndrome. Rev Gastroenterol Disord. 2003;3(Suppl.3):S18-24.
6 Solmaz M, Sayar K, Kavuk I. Psychological factors in the irritable bowel syndrome. Eur JMed Res. 2003;8(12):549-56.
7 Hazlett-Stevens H, Craske MG, Mayer EA, Chang L, Naliboff BD. Prevalence ofirritable bowel syndrome among university students. The roles of worry, neuroticism,anxiety sensitivity and visceral anxiety. J Psychosom Res. 2003 Dec;55(6):501-5.
8 Inadomi JM, Fennerty MB, Bjorkman D. Systematic review: the economic impact ofirritable bowel syndrome. Aliment Pharmacol Ther. 2003 Oct 1;18(7):671-82.
9 Spiller RC. Treatment of Irritable Bowel Syndrome. Curr Treat Options Gastroenterol.2003 Aug;6(4):329-337.
10 Leong SA, Barghout V, Birnbaum HG, Thibeault CE, Ben-Hamadi R, Frech F, OfmanJJ. The economic consequences of irritable bowel syndrome: a US employer perspective.Arch Intern Med. 2003; 163(8): 929-35.
11 Newman B, Siminovitch K. Inflammatory bowel disease: Crohn’s disease and the success ofNODern genetics. Clin Invest Med. 2003 Dec;26(6):303-14.
12 Cheung O, Regueiro MD. Inflammatory bowel disease emergencies. Gastroenterol ClinNorth Am. 2003 Dec;32(4):1269-88.
13 Feurle GE, Keller O, Hassels K, Jesdinsky HJ. Social consequences of Crohn’s disease.Dtsch Med Wochenschr. 1983 Jun 24;108(25):971-5.
14 Bernstein CN, Kraut A, Blanchard JF, Rawsthorne P, Yu N, Walld R. The relationshipbetween inflammatory bowel disease and socioeconomic variables. Am J Gastroenterol.2001 Jul;96(7):2117-25.

CHAPTER 10
Skin problems


CHAPTER 10Skin problems
CONTENTS
INTRODUCTION 10-3
ECZEMAS 10-3
Seborrhoeic eczema 10-3Varicose eczema 10-3Atopic eczema 10-3Discoid (nummular) eczema 10-4Pompholyx 10-4
OCCUPATIONAL DERMATITIS 10-4
Contact Irritant Dermatitis 10-4Allergic Contact Dermatitis 10-5
PSORIASIS 10-5
Guttate Psoriasis 10-5Classical Psoriasis 10-6Psoriatic Arthropathy 10-6
OTHER CONDITIONS 10-6
Severe acne 10-6Acne Rosacea 10-7Dermatomycoses 10-7
REFERENCES 10-8
AUTHORS:
Dr Ian Gemmell MB ChB MSc MA(Law) MFOM, Consultant OccupationalPhysician, Employment Medical Services Ltd.
Dr John English FRCP, Consultant Dermatologist Queens Medical CentreNottingham.
10-1

Fire and Rescue Service: Draft Medical Guidelines – June 2004
10-2

Skin problems
10-3
Introduction
Overall, skin problems are a common cause of occupational morbidity. Around 10% ofreported cases of occupationally related disease or injury compiled by OPRA1 are skinconditions, however sickness absence related to skin conditions is considerably lower.
Firefighting involves the exposure to a variety of chemicals which have varying rates ofpenetration of the skin. In addition, this occupational group are routinely exposed tohot and humid conditions and water itself can lead to a form of contact dermatitis.Fire Investigators are also exposed to a variety of chemicals with varying degrees of skinpenetration and different toxic characteristics. Chronically broken skin may reduce theeffectiveness of this physical barrier and lead to greater absorption than otherwiseanticipated.
Although unusual, firefighters will occasionally have to attend chemical spills and may beexposed before the hazard is identified and full chemical protective clothing andequipment can be used. There is therefore a significant risk for firefighters who havechronic damage to the skin structure and careful assessment is needed for all applicants,and for serving firefighters who develop skin conditions.
Eczemas
Seborrhoeic eczema
Typically seborrhoeic eczema affects the head and neck, the axillae and groin. Sufferers arenot as susceptible to contact irritants as atopic individuals but dusty environments canexacerbate the condition. Hot and humid environments may cause extension from theusual sites.
Varicose eczema
Varicose eczema occurs as a result of stasis in dependant engorged leg veins. This reducesblood flow to the skin, typically around the ankle, and is aggravated by occupationsrequiring standing for long periods. Varicose ulcers may develop and these may requiretime away from work in order to maintain hygiene and for surgical dressing. Individualswith prominent varicose veins may develop a tendency towards varicose eczema andtherefore may require support stockings or compression bandaging which may beuncomfortable in hot and humid conditions.
Atopic eczema
Atopic skin disease renders an individual more susceptible to irritant chemicals becauseof the thin, relatively permeable stratum corneum and the cracking and fissuring whichaccompany the disease. This means that people with atopic eczema should be carefullyassessed prior to any employment which may expose them to irritant chemicals as there is anincreased susceptibility to contact irritant dermatitis. About 75% of people with moderatechildhood eczema develop an irritant occupational dermatitis2. A history of atopy shouldalso raise questions regarding the individual’s lung function (underlying atopic asthma).

Fire and Rescue Service: Draft Medical Guidelines – June 2004
10-4
On the other hand, there is no evidence that atopic individuals with unbroken skin are atany greater risk of developing contact allergic dermatitis3. However, about 8% of atopicshave to change their jobs because of troublesome eczema and this is clearly more likely injobs where exposure to irritants is common4. Problems with eczema at work usually arise inpeople who suffered from childhood hand eczema.
Individuals with a significant history of atopic eczema, including those who only had asignificant problem during childhood, are at risk of developing further problems if theybecome operational firefighters. Specialist opinion should therefore be sought, and onlythose who are at low risk should be considered fit for firefighting duties.
Discoid (nummular) eczema
This condition affects any part of the body but classically the hands, arms and legs. Itconsists of coin shaped plaques, usually on the extensor surfaces and may form serouscrusting. It is commonest in middle age but can occur at any age. It is unrelated to atopiceczema and can sometimes be difficult to distinguish from contact irritant dermatitis whenit affects the hands, however the distinction is important with regard to cause, treatmentand prognosis. There are few implications for employment.
Pompholyx
Pompholyx consists of a pruritic vesicular reaction affecting the palms and soles. Typically,the vesicles are deep and over a few days they discolour to a dark red/purple colour.Widespread superficial peeling may occur as the lesions heal. It is related to dishydrosis andtherefore occurs more commonly in summer months. It may also be associated withbacterial and fungus skin infections5 or as a result of exposure to nickel, chromium andcobalt salts6. In the latter scenario, patch testing is often negative and ingestion of verysmall quantities of metal salt solution may be tried7.
The cause of pompholyx is believed to be multifactorial. Following treatment of theunderlying cause it heals. If metal allergy is demonstrated then protection from exposure isthe treatment of choice.
Occupational dermatitis
Collated reports from dermatologists and occupational physicians in the 3 month periodJuly-Sep 2003 showed that of 2130 case reports, over 13% of all reported occupationaldisease involved the skin. 57% of dermatological cases were contact dermatitis8.
Contact Irritant Dermatitis
Three quarters of all occupational dermatoses are of this type. Irritants produce a directeffect on skin and include compounds which increase the permeability of the skin such asdetergents, surfactants and alkalis. Apart from chemical irritants, water itself is an irritantafter prolonged contact, even in non-atopic individuals.

Skin problems
10-5
Contact irritant dermatitis classically consists of erythema, fissures and scaling. It typicallyfollows a glove distribution on the hands and forearms. Irritant dermatitis is unusualelsewhere on the body. Barrier creams may help once the skin of the hands has recoveredbut frequently, once the dermatitis has become established, removal from the workinvolved is necessary.
Allergic Contact Dermatitis
This accounts for 15-20% of occupational skin disorders. It is usually a response to onespecific agent and is usually a Type IV delayed hypersensitivity reaction involving antigenscombining with epidermal proteins. The initial sensitizing contact may be for severalhours, although subsequent contacts may only be transient and yet produce a skinreaction.
Latex allergy is a well known problem in the health service and is a Type I allergicresponse to natural rubber latex proteins, producing an immediate response which causescontact urticaria that may lead to anaphylaxis.
Allergic contact dermatitis produces a reddened weal at the site of contact with blisteringand later fissuring. Long term dermatitis produces a thickening of the skin with a mixedpicture often difficult to distinguish from contact irritant dermatitis. Whilst allergiccontact dermatitis may develop on any part of the body, it is usually found on the hands,head and neck.
There are few specific known allergens in frequent usage by Fire and Rescue Services.Hazard data sheets may need to be reviewed to determine the presence of allergens orsensitizers. Individuals who are clearly at significant risk from a known sensitiser shouldavoid exposure, and applicants should be assessed for risk. Individuals who developproblems in service may require referral for patch testing.
Occasional contact may be acceptable to the individual and to the Service but repeatedcontact should be avoided and this may necessitate redeployment. Because of theoccasional and usually unquantified nature of exposure, it is rarely possible to correlatesensitisation to specific occupational exposures. In most cases where sensitisation isidentified, the substance, such as nickel or chromium, is so commonly encountered thatgreat care should be taken before attributing the sensitisation to an occupational cause.
Psoriasis
Guttate Psoriasis
This affects children and young adults and may follow a streptococcal sore throat. Ittypically affects the trunk and resolves spontaneously although classical psoriasis maydevelop subsequently. In the absence of predictive factors for late onset disease, guttatepsoriasis can be ignored.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
10-6
Classical Psoriasis
Psoriasis affects 2% of adults in NW Europe and about 30% of sufferers have a familyhistory of the disease. The condition may be aggravated by physical or chemical traumaand some individuals find their disease exacerbated by bacterial sore throats9. Clearly, ifexacerbation occurs with certain physical or chemical stimuli, there will be manualoccupations which are not suited to a person with established psoriasis.
Unlike atopic eczema, psoriasis leads to a thickening of the stratum corneum and so anypredisposition to irritant dermatitis is less marked and most psoriasis sufferers havereasonably stable disease. Men in lower paid, predominantly manual jobs, have the greatestdifficulty with their psoriasis10 11. A British study of 150 patients with severe psoriasis andcurrently working found almost 60% had lost a mean of 26 days from work during thepreceding year because of their psoriasis12.
A number of studies have looked at the relationship of stress with both the onset andexacerbation of psoriasis. Unlike other skin diseases, there seems to be clear correlationbetween stressful events and the onset and aggravation of the condition13.
In summary therefore, whilst mild psoriasis is unlikely to result in excessive sicknessabsence or predispose the individual to irritant dermatitis, severe forms of the disease may.In addition there does appear to be evidence of a link with stressful events and manualwork, which in the case of severe psoriasis may result in excessive absenteeism and workrelated skin disease.
Therefore, only severe forms of the disease need be reviewed with care, with specialistadvice where appropriate.
Psoriatic Arthropathy
Psoriatic arthropathy resembles rheumatoid arthritis in that it usually affects the distalfinger joints and the large joints of the limbs. It occurs in 5-10% of psoriasis sufferers andits effects can be severe, affecting both peripheral joints and causing spondylitis of thespine. There is a direct link with HLA B27. Management is based on the degree andseverity of symptoms. Those in physical roles should be protected from excessive forceswhich will aggravate the condition.
Other conditions
Severe acne
Acne Vulgaris affects most adolescents and many adults. In general, mild casespredominantly affecting the face and resulting in occasional pustules can be discounted.Severe acne however, with multiple pustules and cysts, results in severe disfigurement andmay involve the face, neck and trunk. It is made worse by hot or humid conditions andclose fitting clothing. For this reason, an applicant with severe acne may quite reasonablyhave entry deferred until a course of a retinoid compound has been completed.

Skin problems
10-7
Certain occupational exposures such as mineral oils, PCBs and chemical spillages maycause halogen acne but prolonged exposures are unlikely in the Fire Service.
Acne Rosacea
This is an inflammatory dermatosis of unknown aetiology. The condition tends to beworsened by heat. Individuals with a history of severe acne rosacea may find operationalfirefighting causes an unacceptable exacerbation of their symptoms and care should betaken in accepting them for firefighter training. Serving firefighters should be assessed onan individual basis.
Dermatomycoses
These fungal conditions may be endemic where shared showering facilities are available.The condition may also be aggravated by wearing heavy footwear for long periods inhumid conditions. Both these scenarios apply to firefighters and although this conditionwould not normally bar new recruits or existing firefighters from work, the conditionshould at least be recognised. It is associated with pompholyx of the palms and soles.
Tinea unguum may lead to onychogryphosis and be very difficult to eradicate. Other thanits association with pompholyx, there is little occupational caution in relation to fireservice work.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
10-8
References
1 Occupational Physicians Reporting Activity. Various quarterly reports. Universityof Manchester.
2 Rystedt I. Work related hand eczema in atopics. Contact Dermatitis 1985;12:164-71.
3 Rudzki E, Grzywa Z. Contact Sensitivity in atopic dermatitis. Contact Dermatitis1975;1:285-7.
4 Rystedt I. Factors influencing the occurrence of hand eczema in adults with a history ofatopic dermatitis in childhood. Contact Dermatitis. 1985;12:185-91.
5 Nowicki R. [Allergic phenomena in the course of the dermatomycoses] Pol MerkuriuszLek. 2003 Jun;14(84):532-4.
6 Bryld LE, Agner T, Menne T. Relation between vesicular eruptions on the hands andtinea pedis, atopic dermatitis and nickel allergy. Acta Derm Venerol. 2003;83(3):186-8.
7 Veien NK, Hattel T, Justesen O, Norholm A. Oral challenge with metal salts. (I).Vesicular patch-test-negative hand eczema. Contact Dermatitis. 1983 Sep;9(5):402-6.
8 OPRA Quarterly Report Dec 2003. University of Manchester.
9 Wardrop P, Weller R, Marais J, Kavanagh G. Tonsillitis and chronic psoriasis. ClinOtolaryngol. 1998 Feb;23(1):67-8.
10 Feldman SR, Fleischer AB Jr, Reboussin DM, Rapp SR, Bradham DD, Exum ML,Clark AR. The economic impact of psoriasis increases with psoriasis severity. J Am AcadDermatol. 1997; 37: 564-9.
11 Holness DL, Nethercott JR. Work outcome in workers with occupational skin disease.Am J Ind Med. 1995; 27: 807-15.
12 Finlay AY, Coles EC. The effect of severe psoriasis on the quality of life of 369 patients.Br J Dermatol. 1995; 132: 236-44.
13 Al’Abadie MS, Kent GG, Gawkrodger DJ. The relationship between stress and theonset and exacerbation of psoriasis and other skin conditions. Br J Dermatol.1994;130:199-203.

CHAPTER 11
The pregnant firefighter


CHAPTER 11The pregnant firefighter
CONTENTS
INTRODUCTION 11-3
LEGISLATION 11-3
Equal Pay Act 1970 (amended 1984) 11-3Sex Discrimination Act 1975 11-3Employment Act 1989 11-3Employment Rights Act 1996 11-3Management of Health and Safety at Work Regulations 1999 11-4Maternity and Parental Leave etc Regulations 1999 11-4HSG 122 New and Expectant Mothers at Work 11-4Summary of Application of Legislation by Medical Advisers 11-4In-Vitro Fertilisation 11-5
HAZARDS AND EFFECTS 11-5
PHYSICAL (NON-CHEMICAL HAZARDS) 11-5
Physical Exertion 11-5Psychological Stress 11-6Hvperthermia 11-6Noise 11-7Radiation 11-7Biological Agents 11-7
CHEMICAL HAZARDS 11-7
Irritant Gases 11-8Asphyxiant Gases 11-8Other Toxins 11-9
PRESENT PRACTICE AND POLICY 11-9
Recommendations for Pregnant Applicants and Employees of the Fire andRescue Service: 11-9
11-1

Fire and Rescue Service: Draft Medical Guidelines – June 2004
11-2
REFERENCES 11-11
ORIGINAL AUTHOR 1999:
Dr Susan Robson FFOM FRCP, Consultant Occupational Physician and Brigade Medical Adviser.
UPDATED 2004 BY:
Dr Tony Williams MFOM, Consultant Occupational Physician, Working Fit Ltd.
The pregnant firefighter
11-3
Introduction
As the result of legislative changes throughout the 1970s, more and more women are nowentering what was previously considered male-dominated areas of employment. This hasgiven rise to a number of difficult questions on the issue of pregnancy and work especiallywhere there is a potential for foetal damage occurring as a result of workplace exposure tochemicals and physical agents. There is some considerable difficulty in reconciling thedesire for equal opportunities for women and the concerns for adverse pregnancy outcomesin what is an increasingly litigious society. Compounding this problem (when it comes tomaking policy decisions) is the limited scientific evidence concerning the adversereproductive effects of exposure to an increasing number of chemical and physical agents.
Legislation
Equal Pay Act 1970 (amended 1984)
Women must be paid the same as men when they are doing the same (or broadly similar)work, or work which is of equal value.
Sex Discrimination Act 1975
This makes it unlawful for employers to discriminate on grounds of gender, marital statusor because someone intends to undergo, is undergoing or has undergone genderreassignment.
Employment Act 1989
This includes an exemption from the operation of the Sex Discrimination Act for actsdone in connection with employment or vocational training to comply with certainspecified statutory provisions relating to the protection of women at work. Examples arethe Code of Practice on Lead at Work and the Ionising Radiation Regulations.
Employment Rights Act 1996
This includes the following rights:
• The right not to be unfairly dismissed. A dismissal is automatically unfair if it is for areason related to pregnancy, childbirth, maternity leave, parental leave, or time off fordependants.
• The right to maternity leave.
• The right to paid time off for ante-natal care.
• The right to unpaid time off to care for or to arrange care for dependants where thedependant is ill, injured, assaulted, gives birth or dies; if arrangements for the care ofa dependant break down; or if there is an unexpected incident involving a childat school.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
11-4
• The right to be offered suitable alternative work on not substantially less favourableterms and conditions if a legislative requirement or a health and safetyrecommendation prohibits a woman from doing her usual job because she is pregnant,has recently given birth or is breastfeeding.
• The right to be suspended on full pay if a woman is unable to do her usual job onmaternity grounds as described above and no suitable alternative work is available.
Management of Health and Safety at Work Regulations 1999
These require employers to carry out risk assessments. There are specific obligations onemployers to assess risk where there are women of childbearing age at work. Employersmay have to alter working conditions or hours of work, offer suitable alternative work orsuspend an expectant or new mother on full pay if necessary to avoid risk to her orher baby.
These regulations implement the European Directive on Pregnant Workers (SI No. 2865),Council Directive 92/85/EEC, putting a duty of care on employers for a safe system of workto all women of reproductive age, their unborn children, and all working mothers who arebreast feeding.
Maternity and Parental Leave etc Regulations 1999
These contain the detail of the rights to maternity and parental leave contained in theEmployment Rights Act 1996 (ERA). They also prescribe the circumstances in which adismissal will be automatically unfair for the purposes of the ERA if the dismissal is for areason related to pregnancy, childbirth, maternity leave, parental leave, or time off fordependants.
Most employees have the right to take up to four weeks unpaid parental leave per child(usually under 5 years of age) in any one calendar year (to a total of 13 weeks per child)provided they have given their employer 21 days notice and the employer has agreed.They are also entitled to take reasonable periods of time off work at short notice to dealwith an emergency involving a dependant. The determination of what is and what is notreasonable is for management to determine and advise the employee accordingly.
HSG 122 New and Expectant Mothers at Work
The Health and Safety Executive have produced clear guidance to employers, HSG 122,which outlines the relevant legislation and explains the risk assessment process needed.
Summary of Application of Legislation by Medical Advisers
Much of the legislation is directed at the employer, however you will be expected tounderstand it in order to manage individuals who either have psychological problems inrelation to potential sex discrimination or pressure placed on them contrary to the legalrequirements outlined above.

The pregnant firefighter
11-5
You will also be expected to advise in relation to specific requirements. The risk assessmentrequired by the Management of Health and Safety at Work Regulations is a managementresponsibility, but you may advise on working hours or activities. In many cases the issue issubjective, for example working hours where some pregnant women are quite happy tocontinue to work shifts or do night work, while others are having difficulty and need tochange working hours.
In some cases where there are complications with pregnancy you will be expected to advisewhether maternity leave should start early, rather than recommending sick leave.
In-Vitro Fertilisation
Some individuals working for the Fire Service may undergo in-vitro fertilization. This is asensitive issue and requires some flexibility to allow them to attend hospital for preparationand for the procedure itself. This should not represent a significant period of absence, andMedical Advisers may wish to discuss the requirements with the specialist in order to beable to advise management appropriately.
Hazards and effects
Firefighting is a potentially hazardous occupation and some of these hazards are ofparticular concern to the pregnant firefighter. There is the potential to be exposed to aspectrum of potential reproductive hazards including physical hazards such as extremes oftemperature and ionising radiation, ergonomic and psychological stress, biological agentsand chemical agents including irritant gases, asphyxiant gases and other toxins such asmutagens and teratogens.
In many of the situations in which firefighters are called to work, it is impossible to analyseor quantify the possible exposures. However, they can be considered under two majorheadings, physical (non-chemical) hazards and chemical hazards.
Physical (non-chemical hazards)
Physical Exertion
The physiological changes that occur during a normal pregnancy make many types ofphysical activity difficult. During pregnancy, increased physical demands affect mainly thecardiovascular and musculo-skeletal systems. Pregnancy is marked by a number of changesto the cardiovascular system including increased cardiac output and blood volume anddecreased venous return to the heart and peripheral pooling. Pregnant women are moresusceptible to dizziness and syncope especially after prolonged standing or working in hotenvironments. This is of obvious concern to pregnant firefighters since severe injury couldoccur from loss of consciousness or equilibrium.
There is also a degree of debate as to whether in theory the foetus could be subject tohypoxia as a result of vigorous exercise by the mother shunting blood away from theplacenta. The degree to which this is significant in humans is unknown. During sustainedfirefighting, heart rates in the 85%-100% maximum range have been described. This isalso aggravated by the use of breathing apparatus whilst working in an oxygen-deficient or

Fire and Rescue Service: Draft Medical Guidelines – June 2004
11-6
toxic environment. Such high levels of exertion could have an adverse effect on thefoetus, especially in later pregnancy.
The strenuous nature of firefighting also adversely affects the musculo-skeletal system.With the weight gain and the increasing abdominal girth associated with pregnancy, pelviclordosis and thoracic kyphosis occur. The sacroiliac joints become more mobile and duringthe second trimester low back pain occurs. This can adversely affect manoeuvrability inperforming duties such as climbing ladders. During the third trimester, strenuous activitywould be severely limited.
One study1 analysed spontaneous abortions occurring at less than 10 weeks, mid-term(10-16 weeks) and late (16-28 weeks) and stillbirths (more than 28 weeks) and showed astatistically increased ratio of observed to expected outcomes in occupations involvingheavy weights (more than 15 times daily) and/or other physical effort.
Psychological Stress
Fire and Rescue Service staff may experience stress related to the characteristics ordemands of the job, including the unpredictable and emergency nature of the work, erraticwork schedules and prevalent hazards. Various indicators of psychological distress havebeen documented for firefighters involved in major disasters and potentially toxicexposures. Psychological distress has been examined in a limited number of studies withpotential reproductive effects affecting both males and females. The literature regardingwork-related stress in pregnancy outcome is sparse.
Shift work, one factor that could contribute to the level of job stress of the firefighter, wasfound in one study of Swedish laboratory workers to be associated with increased rates ofmiscarriage. However, other studies have failed to support this conclusion. Other studieshave however shown that babies born to non-smoking women, who worked irregular workschedules, evenings or rotating shifts during the second and third trimesters had asignificantly lower birth weight than infants of non-smoking mothers who worked duringthe day only.
It is reasonable to assume that excessive pressure leading to stress is an important aspect ofrisk. A subjective assessment of stress levels should therefore be made if the individualwishes to continue working shifts. In general if a pregnant woman does not wish to worklong or late/night shifts you should recommend alternative arrangements to Management.
Hvperthermia
Heat exposure is known to cause adverse reproductive effects in humans and based onavailable evidence a limit of 38.9oC has been considered the minimum core temperaturelikely to pose a teratogenic hazard to the human embryo or foetus. The routine heatexposures encountered by firefighters are probably safe for the developing foetus. However,firefighters are not always able to regulate their exposure to heat and some studies haveshown that 2.1% of fire injuries are due to heat exhaustion. Pregnancy also decreases heattolerance.

The pregnant firefighter
11-7
Noise
Sources of noise in a firefighters work environment include sirens, air horns, vehiclesand auxiliary power equipment. There have been a number of studies which haveconcentrated on the potential adverse effects of noise on pregnancy outcomes. Severallaboratory investigations have been carried out on pregnant rodents exposed in most casesto very loud noise levels (usually at more than 100 dBA of continuous or intermittentnoise). Findings have supported an exposure effect manifested most often by increasedlitter absorption, increased foetal mortality and decreased foetal weight.
Foetal malformations have been demonstrated less consistently. It is unknown whetherthis effect is due to a direct effect on the developing embryo or if they are caused by thematernal psychological response to the stress of noise exposure. The appropriateness ofthese species as models for the prediction of human reproductive response to noise issimilarly unknown.
The association between occupational noise exposure and reproductive outcome has notbeen thoroughly investigated, although one group has reported an increased risk of highfrequency hearing loss (more than 10 dBA at 4,000 Hz) in children whose mothers wereexposed during their pregnancy to an 8 hour time weighted average of 85-95 dBA. Studiesto date have concentrated on industrial job exposures and have not consistently addressedpossible social or economic influences. However, if their results are confirmed they couldbe relevant to the pregnant firefighters whose level of noise exposures may be comparable.
Radiation
The well documented human reproductive effects of ionising radiation justify protection ofany potentially exposed worker and pregnant workers in particular. It must be stressed,however, that exposure opportunities in firefighting are very uncommon, thus constitutingonly an infrequent and relatively unusual hazard for the firefighter.
Biological Agents
Although not predominantly a hazard of firefighting, exposure to biological agents mayarise out of emergency medical response duties. Obviously there would be a range of effectsboth to the pregnant woman and to the foetus if infection resulted. However exposureopportunities for pregnant firefighters are limited and are minimised through adequateprocedural policies.
Chemical hazards
Research shows that the toxicity is dominated by effects arising from carbon monoxideand/or hydrogen cyanide or products with high irritancy such as hydrogen chloride, oxidesof nitrogen and substances such as formaldehyde and acrolein in oxidised hydrocarbonatmospheres2.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
11-8
However, the pyrolysis and combustion products of fires contain hundreds of compounds,some of which are common to all fires and others of which are formed to a varying degreedepending on such factors as the composition of the materials burned and the temperatureand the amount of oxygen present. The toxic gases found in the fire environment can becategorised as irritants, asphyxiants or other gases with a wide array of effects that mayinclude carcinogenosis, mutagenesis and teratogenesis.
Irritant Gases
A large number of irritant gases are found in the fire environment including hydrogenchloride, ammonia, acrolein, sulphur dioxide, isocyanates, halogen acids and nitrogenoxides. These compounds act primarily by damaging the epithelial surfaces of therespiratory tract and are absorbed peripherally to varying degrees. Though acrolein hasteratogenic potential when ingested or injected into experimental animals, the chiefknown danger to the foetus posed by this group of compounds is the potentially life-threatening maternal chemical pneumonitis that may follow acute exposure.
Asphyxiant Gases
The most common toxic hazard faced by firefighters is carbon monoxide. Measures ofcarboxyhaemoglobin levels have been shown to be consistently higher in firefightersthan in non-exposed control subjects matched for smoking status. The levels ofcarboxyhaemoglobin demonstrated pose a health hazard to any unprotected womanfirefighter and the foetus. Acute exposure to carbon monoxide has been associated withfoetal loss. A more difficult problem is the assessment of risk to the foetus of a motherchronically exposed to low levels of carboxyhaemoglobin.
There have been a number of conflicting studies on these effects, most of which haveconcentrated on mothers who smoked. Smoking has been shown to increase the level ofcarboxyhaemoglobin in both the foetus and the mother. Smoking during pregnancy isassociated with the increased incidence of pre-term births, low births weights, increase in neo-natal mortality, retarded intrauterine growth, spontaneous abortions and bleeding disorders.
In summary, firefighters are sometimes exposed to levels of carbon monoxide that couldlead to acute anoxic damage to the foetus of an unprotected mother. The foetus of anactive firefighter is also at increased risk of chronic anoxia because of the elevatedcarboxyhaemoglobin levels. The foetus of an active firefighter who smokes is at special risksince the effects of smoking and carbon monoxide exposure is additive. The risk of chronicanoxia in the foetus of a firefighter is certainly greater than the risk to the foetus of a non-smoking mother who is not routinely exposed to carbon monoxide.
The risk to the foetus of a non-smoking firefighter who consistently uses breathingapparatus is probably less than the risk to the foetus of a smoker that is not otherwiseexposed to carbon monoxide. Although a firefighter can significantly reduce the risk ofcarbon monoxide exposure to the foetus by wearing breathing apparatus, the problem isthat this may in some cases increase the risk of heat exertion.

The pregnant firefighter
11-9
The other asphyxiant gas of concern is hydrogen cyanide which is present at low levels infire atmospheres. Firefighters have been shown to have significantly higher levels ofmetabolites of hydrogen cyanide in their blood than in controlled subjects not exposed tofire atmospheres. Exposure to hydrogen cyanide occurs much less frequently than carbonmonoxide exposure and although still controversial, hydrogen cyanide exposures aregenerally thought not to pose an acute health hazard to firefighters. The risks of hydrogencyanide to a foetus are not quantified, but hydrogen cyanide exposure would be expectedto exacerbate the asphyxiant effects of carbon monoxide exposure.
Other Toxins
The growing use of plastics and other synthetic substances in buildings and homes hasincreased the uncertainties of assessing the risks posed by toxic exposures to firefighters.A number of pyrolysis and combustion products are known or are suspected carcinogens,mutagens or teratogens. Little data is available to document the level of these exposures.
Present practice and policy
There are a number of conflicts in attempting to ensure reproductive health whilstproviding equal opportunities for women. The ideal solution to the conflict is to make theworksite safe for both sexes since many, if not all, reproductive hazards affect both menand women.
Evanoff and Rosenstock, having reviewed reproductive hazards in the workplacerecommended that pregnant firefighters should cease active firefighting during the secondtrimester of pregnancy. They additionally recommended that special attention should bepaid to adequate respiratory protection in toxic atmospheres.
This policy may well be adequate, however, there are a number of other issues that shouldbe given active consideration:
• The foetus is at its most vulnerable during the first trimester and especially during thefirst six weeks of gestation when the woman herself may be unaware or only suspectthat she is pregnant. Modern pregnancy testing is however now accurate at a veryearly stage.
• There is already a high risk of spontaneous abortion (1 in 5) within the generalpopulation and we are now living in an increasing litigious society where anyabortion, pre-term birth or congenital disability could be the subject of litigation.
Recommendations for Pregnant Applicants and Employees of the Fire andRescue Service:
• Pregnant applicants to be firefighters should undertake all the normal pre-employmentselection tests excluding those for fitness and aptitude. If the applicant is successfulthese tests should be deferred until pregnancy or breast feeding has come to an end.

Fire and Rescue Service: Draft Medical Guidelines – June 2004
11-10
• Pregnant officers should be required to notify their Officer in Charge or the MedicalAdviser as soon as pregnancy is suspected.
• The pregnant officer should then be accommodated on non operational day duties.
• If for any reason the pregnancy does not proceed to term (miscarriage, terminationetc) the woman should be assessed by the Medical Adviser prior to returning to fulloperational duties on shifts.
• Following the usual maternity leave whether breast feeding or not the woman mayreturn to non operational day duties. In the case of breast feeding these duties shouldcontinue until breast feeding ceases, and in all cases women must be assessed by theMedical Adviser prior to returning to full operational duties on shifts.

The pregnant firefighter
11-11
References
1 Eskenazi B et al. Physical exertion as a risk factor for spontaneous abortion.Epidemiology 1994 Jan;5(1):4-5
2 Work undertaken by D A Purser at the Department of Inhalation ToxicologyHuntington Research Centre and W D Woolley at the Fire Research Station,Borehamwood and presented in 1982 at the conference – “Smoke and Toxic Productsfrom Burning Polymers”

Fire and Rescue Service: Draft Medical Guidelines – June 2004
11-12

APPENDICES TO CHAPTER 2
CONTENTS
APPENDIX 1
Firefighter Role Requirements 2-A1
APPENDIX 2
Crew Manager Role Requirements 2-A7
APPENDIX 3
Watch Manager Role Requirements 2-A13
APPENDIX 4
Station Manager Role Requirements 2-A19
APPENDIX 5
Group Manager Role Requirements 2-A25
APPENDIX 6
Area Manager Role Requirements 2-A31
APPENDIX 7
Brigade Manager Role Requirements 2-A37
APPENDIX 8
Control Operator Role Requirements 2-A43
APPENDIX 9
Control Supervisor Role Requirements 2-A49
APPENDIX 10
Control Watch Manager Role Requirements 2-A55

Fire and Rescue Service: Draft Medical Guidelines – June 2004
APPENDIX 11
Control Operations Manager Role Requirements 2-A61
APPENDIX 12
Fire Safety Officer Role Requirements 2-A67
APPENDIX 13
Fire Safety Manager Role Requirements 2-A73
APPENDIX 14
Fire Safety Advisor / Engineer Role Requirements 2-A79
APPENDIX 15
Fire Investigator Role Requirements 2-A85
APPENDIX 16
Technical Support Role Requirements 2-A91
APPENDIX 17
Trainer Role Requirements 2-A97
APPENDIX 18
Training Manager Role Requirements 2-A103

2A-1
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Sprinting 23 6 21 26 13 11 4 4 119
Running 10 4 14 26 23 23 4 4 121
Jogging 5 1 14 29 25 26 4 5 121
Walking 0 0 1 3 6 90 6 6 125
Climbing stairs 0 0 1 5 7 87 6 6 126
Climbing ladders 0 1 18 40 23 18 4 4 125
Crawling 4 10 39 32 7 8 3 3 123
Jumping 14 6 30 21 20 9 3 4 124
Hammering 5 8 44 30 8 4 3 3 122
Digging 7 23 45 19 3 3 3 3 123
Strength tasksLifting more than 5 kg or 11 pounds 1 2 1 15 22 59 6 6 123
Lifting more than 10 kg or 22 pounds 1 1 2 25 30 41 6 5 122
Lifting more than 20 kg or 44 pounds 0 2 13 29 37 19 5 5 121
Lifting more than 40 kg or 88 pounds 6 13 14 34 20 13 4 4 119
Carrying more than 5 kg or 11 pounds 1 1 5 16 24 53 6 6 117
Carrying more than 10 kg or 22 pounds 0 1 8 24 29 39 6 5 119
Carrying more than 20 kg or 44 pounds 1 4 13 30 37 15 5 5 117
Carrying more than 40 kg or 88 pounds 8 11 14 37 23 7 4 4 115
Pushing/pulling more than 5 kg or 11 pounds 3 3 13 21 18 43 6 5 120
Pushing/pulling more than 10 kg or 22 pounds 1 1 14 24 28 33 6 5 119
Pushing/pulling more than 20 kg or 44 pounds 3 6 17 29 25 21 4 4 119
Pushing/pulling more than 40 kg or 88 pounds 7 11 20 28 19 14 4 4 118
Static posturesStanding 1 0 0 1 6 93 6 6 127
Sitting 1 1 0 2 9 87 6 6 126
Squatting 2 2 5 10 35 45 6 5 124
Kneeling 2 2 5 21 40 31 5 5 123
Lying down 11 2 11 24 33 19 5 5 123
Table 1: Respondents’ Details
Age Bracket 18-19(1) 20-29(2) 30-39(3) 40-49(4) 50+(5) Mode Median N0 33 40 22 5 3 3 129
Years of Service 0-4 (1) 5-9 (2) 10-14(3) 15-19(4) 20-24(5) 25+(6) Mode Median N39 22 12 8 7 12 1 2 129
Gender Male Female Mode Median N95 5 1 1 129
Employment Status Fulltime(1) Retained(2) Mode Median N96 4 1 1 128
Appendix 1. Summary of Results for Firefighters fromOccupational Guidelines QuestionnaireNote: Results are displayed as a percentage of the total responses for each role, and as the mode, median and total number (N) ofrespondents for the role

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-2
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time) (continued)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Dynamic flexibility requirementsBending at waist 1 0 2 3 18 76 6 6 125
Reaching 0 0 1 2 17 80 6 6 124
Stooping 2 0 3 10 19 66 6 6 125
Turning/twisting 1 0 0 5 14 81 6 6 124
Object activitiesCatching 8 7 19 25 27 14 5 4 122
Throwing 7 7 17 31 25 13 4 4 123
Fine dexterity (eg writing, assembling equipment) 1 0 3 6 23 67 6 6 126
Foot control (eg driving) 6 1 2 9 17 66 6 6 127
Table 3: Importance respondents considered these activities to be to the effective performanceof their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Sprinting 18 13 29 21 12 8 3 3 125
Running 21 28 34 12 2 3 3 3 126
Jogging 22 31 35 10 1 2 3 2 127
Walking 55 18 23 2 1 1 1 1 127
Climbing stairs 56 23 17 3 1 0 1 1 127
Climbing ladders 61 18 17 3 1 0 1 1 127
Crawling 42 22 24 10 2 1 1 2 125
Jumping 22 17 25 27 6 2 4 3 126
Hammering 20 17 27 26 6 3 3 3 125
Digging 20 15 31 25 5 4 3 3 124
Strength tasksLifting more than 5 kg or 11 pounds 52 22 21 4 0 1 1 1 126
Lifting more than 10 kg or 22 pounds 50 25 21 4 0 0 1 1 125
Lifting more than 20 kg or 44 pounds 43 26 26 4 1 0 1 2 125
Lifting more than 40 kg or 88 pounds 33 28 24 13 1 1 1 2 123
Carrying more than 5 kg or 11 pounds 51 20 23 6 0 1 1 1 124
Carrying more than 10 kg or 22 pounds 48 26 22 4 0 1 1 2 125
Carrying more than 20 kg or 44 pounds 43 26 25 5 2 0 1 2 124
Carrying more than 40 kg or 88 pounds 34 23 28 12 1 2 1 2 122
Pushing/pulling more than 5 kg or 11 pounds 52 18 23 6 1 2 1 1 124
Pushing/pulling more than 10 kg or 22 pounds 49 20 23 4 2 1 1 2 124
Pushing/pulling more than 20 kg or 44 pounds 41 23 31 3 1 1 1 2 124
Pushing/pulling more than 40 kg or 88 pounds 36 27 26 9 1 2 1 2 123
Static posturesStanding 55 17 22 4 0 2 1 1 128
Sitting 44 17 24 13 0 1 1 2 127
Squatting 41 20 22 13 2 1 1 2 126
Kneeling 42 18 26 12 2 1 1 2 125
Lying down 33 14 22 21 6 6 1 3 125
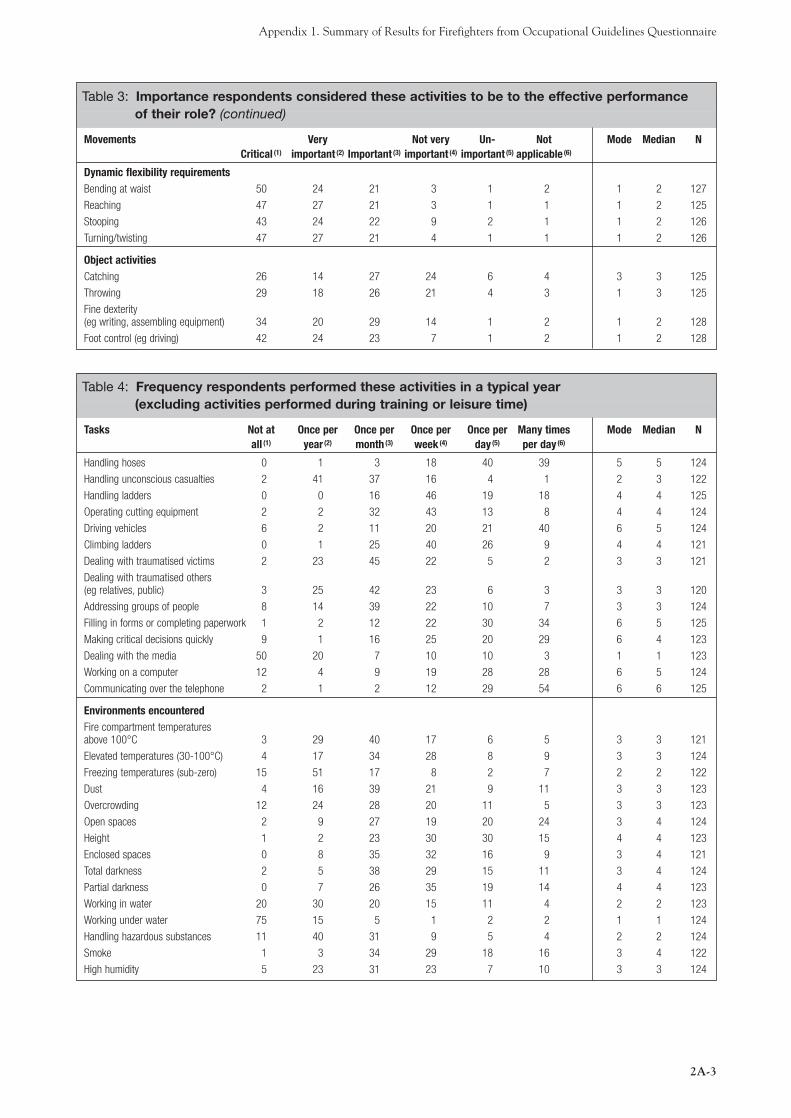
Appendix 1. Summary of Results for Firefighters from Occupational Guidelines Questionnaire
2A-3
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Handling hoses 0 1 3 18 40 39 5 5 124
Handling unconscious casualties 2 41 37 16 4 1 2 3 122
Handling ladders 0 0 16 46 19 18 4 4 125
Operating cutting equipment 2 2 32 43 13 8 4 4 124
Driving vehicles 6 2 11 20 21 40 6 5 124
Climbing ladders 0 1 25 40 26 9 4 4 121
Dealing with traumatised victims 2 23 45 22 5 2 3 3 121
Dealing with traumatised others (eg relatives, public) 3 25 42 23 6 3 3 3 120
Addressing groups of people 8 14 39 22 10 7 3 3 124
Filling in forms or completing paperwork 1 2 12 22 30 34 6 5 125
Making critical decisions quickly 9 1 16 25 20 29 6 4 123
Dealing with the media 50 20 7 10 10 3 1 1 123
Working on a computer 12 4 9 19 28 28 6 5 124
Communicating over the telephone 2 1 2 12 29 54 6 6 125
Environments encounteredFire compartment temperatures above 100°C 3 29 40 17 6 5 3 3 121
Elevated temperatures (30-100°C) 4 17 34 28 8 9 3 3 124
Freezing temperatures (sub-zero) 15 51 17 8 2 7 2 2 122
Dust 4 16 39 21 9 11 3 3 123
Overcrowding 12 24 28 20 11 5 3 3 123
Open spaces 2 9 27 19 20 24 3 4 124
Height 1 2 23 30 30 15 4 4 123
Enclosed spaces 0 8 35 32 16 9 3 4 121
Total darkness 2 5 38 29 15 11 3 4 124
Partial darkness 0 7 26 35 19 14 4 4 123
Working in water 20 30 20 15 11 4 2 2 123
Working under water 75 15 5 1 2 2 1 1 124
Handling hazardous substances 11 40 31 9 5 4 2 2 124
Smoke 1 3 34 29 18 16 3 4 122
High humidity 5 23 31 23 7 10 3 3 124
Table 3: Importance respondents considered these activities to be to the effective performanceof their role? (continued)
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Dynamic flexibility requirementsBending at waist 50 24 21 3 1 2 1 2 127
Reaching 47 27 21 3 1 1 1 2 125
Stooping 43 24 22 9 2 1 1 2 126
Turning/twisting 47 27 21 4 1 1 1 2 126
Object activitiesCatching 26 14 27 24 6 4 3 3 125
Throwing 29 18 26 21 4 3 1 3 125
Fine dexterity(eg writing, assembling equipment) 34 20 29 14 1 2 1 2 128
Foot control (eg driving) 42 24 23 7 1 2 1 2 128

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-4
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time) (continued)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Equipment usedFire-protective Personnel Protective Equipment 0 1 2 8 20 69 6 6 121
Self-Contained Breathing Apparatus 0 1 17 33 28 22 4 5 120
Extended Duration Breathing Apparatus 56 12 19 10 3 0 1 1 118
Vibrating equipment 22 13 31 15 12 8 3 3 120
Computer 11 2 7 18 30 32 6 5 122
Telephone 2 0 4 11 25 58 6 6 122
Hand-held radio 0 0 5 9 32 54 6 6 121
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Handling hoses 67 20 12 0 1 0 1 1 123
Handling unconscious casualties 66 19 14 0 1 0 1 1 125
Handling ladders 66 23 11 0 0 0 1 1 125
Operating cutting equipment 67 20 12 1 0 0 1 1 125
Driving vehicles 52 29 17 1 1 2 1 1 126
Climbing ladders 65 21 14 0 0 0 1 1 125
Dealing with traumatised victims 63 22 14 0 0 0 1 1 125
Dealing with traumatised others (eg relatives, public) 57 21 22 1 0 0 1 1 125
Addressing groups of people 25 18 40 13 4 0 3 3 126
Filling in forms or completing paperwork 25 16 40 13 6 0 3 3 126
Making critical decisions quickly 62 17 16 3 2 0 1 1 125
Dealing with the media 18 7 39 22 10 5 3 3 125
Working on a computer 18 12 42 19 10 0 3 3 125
Communicating over the telephone 24 18 51 5 2 1 3 3 126
Environments encounteredFire compartment temperatures above 100°C 62 19 16 3 0 0 1 1 121
Elevated temperatures (30-100oC) 61 21 15 2 0 0 1 1 123
Freezing temperatures (sub-zero) 47 22 22 7 1 1 1 2 123
Dust 43 24 27 6 0 0 1 2 123
Overcrowding 37 19 34 10 1 0 1 2 123
Open spaces 46 17 27 9 1 0 1 2 124
Height 58 23 17 2 1 0 1 1 123
Enclosed spaces 58 26 14 2 1 0 1 1 123
Total darkness 63 22 13 2 0 0 1 1 123
Partial darkness 59 24 14 3 1 0 1 1 123
Working in water 43 18 28 7 2 2 1 2 123
Working under water 33 11 19 18 5 15 1 3 123
Handling hazardous substances 52 26 19 2 0 0 1 1 122
Smoke 64 24 11 2 0 0 1 1 123
High humidity 59 26 13 2 0 0 1 1 123

Appendix 1. Summary of Results for Firefighters from Occupational Guidelines Questionnaire
2A-5
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Equipment usedFire-protective Personnel Protective Equipment 83 10 7 0 0 0 1 1 123
Self-Contained Breathing Apparatus 84 7 7 1 0 1 1 1 123
Extended Duration Breathing Apparatus 46 11 18 5 3 18 1 2 120
Vibrating equipment 44 16 22 11 4 3 1 2 122
Computer 25 15 35 19 3 2 3 3 124
Telephone 31 19 38 8 2 2 3 3 124
Hand-held radio 50 27 19 2 2 0 1 1 123
Table 6: Near Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
BA control board-Old style MK 1 Read clock 78 22 1 1 129
BA control board-Old style MK 1 Graduations & cylinder pressure 76 24 1 1 129
BA tag Read tag 88 12 1 1 129
BA control board-New style MK 2 Read clock 84 16 1 1 129
BA control board-New style MK 2 Dial calculator 81 19 1 1 129
BA tag MK 2 Read tag 83 17 1 1 129
BA main control board Read clock 81 19 1 1 129
BA main control board Read 77 23 1 1 129
Sabre centurion Read BA graduations 53 47 1 1 129
Sabre centurion Read needle position 53 47 1 1 129
Siebe Gorman Read BA graduations 33 67 2 2 129
Siebe Gorman Read needle position 33 67 2 2 129
Drager Read BA graduations 58 42 1 1 129
Drager Read needle position 57 43 1 1 129
Philips PFX Handheld radio Read channel selector 70 30 1 1 129
Philips PFX Handheld radio Read numbered channel selector 72 28 1 1 129
BA log book Handwritten 85 15 1 1 129
Universal airline pack (Drager) BA supply BA cylinder gauge 59 41 1 1 129
Low pressure air bags Air pressure gauge 77 23 1 1 129
High pressure air bag Read graduations on console 79 21 1 1 129
High pressure air bag Needle position 78 22 1 1 129
Hurst high pressure lift bags Needle position 59 41 1 1 129
Microvent resuscitation equipment Read scale 52 48 1 1 129
Carmichael Godiva appliance Pressure gauge numbers 55 45 1 1 129
Saxon Volvo appliance pump Pressure gauge numbers 51 49 1 1 129
Dennis appliance pump Pressure gauge numbers 71 29 1 1 129
Read turnout sheet 91 9 1 1 129
Read dosimeter 87 13 1 1 129
Read survey meter 79 21 1 1 129
Read computer VDU 85 15 1 1 129
Read general paperwork 84 16 1 1 129
Read pager 53 47 1 1 129
Read mobile phone text 63 37 1 1 129
Read fire control panels 80 20 1 1 129
Read maps 91 9 1 1 129
Read fire extinguishers 84 16 1 1 129
Read plan inspections 80 20 1 1 129
Inspect premises 81 19 1 1 129
Read scale ruler 56 44 1 1 129
Read sound meter 47 53 2 2 129
Read light meter 43 57 2 2 129

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-6
Table 7: Distance Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
Street names White letters on a blue background 88 12 1 1 129
House numbers Copper figures on a blue background 86 14 1 1 129
House numbers White figures on a red background 85 15 1 1 129
Retail shop numbers Gold figures on a dark green background 83 17 1 1 129
House numbers Grey figures on a white background 85 15 1 1 129
Corporate building numbers Black figure on a silver background 83 17 1 1 129
Street names Black letters on a white background 92 8 1 1 129
House numbers Gold figures on a black background 84 16 1 1 129
House numbers Handpainåted black figures on a white background 86 14 1 1 129
House numbers Gold figures on a black background 84 16 1 1 129
House numbers Black figures on a white background 88 12 1 1 129
Carmichael Godiva appliance pump Pressure gauge needle at rear of appliance 62 38 1 1 129
Carmichael Godiva appliance Measuring water in tank 60 40 1 1 129
Saxon Volvo appliance pump Pressure gauge needle at rear of appliance 54 46 1 1 129
Dennis appliance pump Pressure gauge needle at rear of appliance 71 29 1 1 129
Stop sign Road traffic signs 93 7 1 1 129
Give way sign Road traffic signs 93 7 1 1 129
One way street sign Road traffic signs 92 8 1 1 129
Chemical warning sign As EC Directive 92/58/EEC Hazardous substances 91 9 1 1 129
Vehicle signs Break lights/indicators on vehicles 91 9 1 1 129
Fire safety signs 91 9 1 1 129
Exit signs 91 9 1 1 129
Table 8: Hearing Tasks that are a requirement for role
Description Yes(1) No (2) Mode Median N
Distress signal unit 93 7 1 1 129
Warning whistle 95 5 1 1 129
Radio 95 5 1 1 129
Fireground orders 95 5 1 1 129
Evacuation signals/alarms 95 5 1 1 129
Telephone 90 10 1 1 129
Traffic 91 9 1 1 129
Vibraphone 57 43 1 1 129
Pager 56 44 1 1 129
Normal verbal communication with little background noise 92 8 1 1 129
Normal verbal communication with background noise 92 8 1 1 129
Hand clapping 86 14 1 1 129
Cries of help 93 7 1 1 129
Table 9: Other senses that are a requirement for role
Description Yes(1) No (2) Mode Median N
Touch 96 4 1 1 129
Smell 95 5 1 1 129
Taste 53 47 1 1 129

2A-7
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Sprinting 32 18 15 22 9 4 1 3 68
Running 8 7 27 27 23 8 4 4 71
Jogging 6 4 19 31 30 10 4 4 70
Walking 1 0 0 4 15 79 6 6 73
Climbing stairs 0 0 1 7 8 83 6 6 72
Climbing ladders 0 3 28 57 10 3 4 4 72
Crawling 6 17 51 21 4 0 3 3 70
Jumping 14 13 37 24 11 1 3 3 71
Hammering 14 25 43 13 4 1 3 3 72
Digging 15 35 38 10 1 0 3 2 71
Strength tasksLifting more than 5 kg or 11 pounds 0 0 6 22 29 43 6 5 72
Lifting more than 10 kg or 22 pounds 0 1 11 38 31 19 4 5 72
Lifting more than 20 kg or 44 pounds 3 7 22 42 19 7 4 4 72
Lifting more than 40 kg or 88 pounds 23 14 21 28 10 4 4 3 71
Carrying more than 5 kg or 11 pounds 0 3 10 20 28 39 6 5 71
Carrying more than 10 kg or 22 pounds 1 4 13 35 29 18 4 4 72
Carrying more than 20 kg or 44 pounds 7 11 21 39 15 6 4 4 71
Carrying more than 40 kg or 88 pounds 21 15 27 25 8 3 3 3 71
Pushing/pulling more than5 kg or 11 pounds 6 3 18 35 20 18 4 4 71
Pushing/pulling more than10 kg or 22 pounds 7 7 21 37 18 10 4 4 71
Pushing/pulling more than20 kg or 44 pounds 10 15 27 30 14 4 4 3 71
Pushing/pulling more than40 kg or 88 pounds 20 21 30 20 7 3 3 3 71
Static posturesStanding 0 0 0 1 5 93 6 6 73
Sitting 0 0 1 1 10 88 6 6 73
Squatting 1 1 8 28 31 30 5 5 71
Kneeling 4 0 10 30 30 27 4 5 71
Lying down 7 7 17 18 41 10 5 5 71
Table 1: Respondents’ Details
Age Bracket 18-19(1) 20-29(2) 30-39(3) 40-49(4) 50+(5) Mode Median N0 15 48 29 8 3 3 73
Years of Service 0-4 (1) 5-9 (2) 10-14(3) 15-19(4) 20-24(5) 25+(6) Mode Median N11 29 30 12 4 14 3 3 73
Gender Male Female Mode Median N96 4 1 1 73
Employment Status Fulltime(1) Retained(2) Mode Median N89 11 1 1 72
Appendix 2. Summary of Results for Crew Managerfrom Occupational Guidelines QuestionnaireNote: Results are displayed as a percentage of the total responses for each role, and as the mode, median and total number (N) ofrespondents for the role

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-8
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time) (continued)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Dynamic flexibility requirementsBending at waist 0 3 1 7 21 68 6 6 72
Reaching 0 0 3 6 28 64 6 6 72
Stooping 1 1 3 13 21 61 6 6 71
Turning/twisting 0 3 4 6 17 70 6 6 71
Object activitiesCatching 11 16 19 31 13 10 4 4 70
Throwing 8 8 30 31 13 10 4 4 71
Fine dexterity(eg writing, assembling equipment) 1 0 1 4 11 82 6 6 72
Foot control (eg driving) 4 1 10 11 18 56 6 6 72
Table 3: Importance respondents considered these activities to be to the effective performanceof their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Sprinting 10 7 18 43 18 4 4 4 72
Running 15 19 41 22 1 1 3 3 73
Jogging 16 27 41 11 3 1 3 3 73
Walking 48 29 23 0 0 0 1 2 73
Climbing stairs 51 26 19 4 0 0 1 1 73
Climbing ladders 55 25 18 1 1 0 1 1 73
Crawling 37 23 21 15 4 0 1 2 73
Jumping 18 12 26 30 10 4 4 3 73
Hammering 14 12 30 30 10 4 3 3 73
Digging 12 14 36 21 12 5 3 3 73
Strength tasksLifting more than 5 kg or 11 pounds 48 16 29 5 1 0 1 2 73
Lifting more than 10 kg or 22 pounds 45 19 29 7 0 0 1 2 73
Lifting more than 20 kg or 44 pounds 36 23 32 10 0 0 1 2 73
Lifting more than 40 kg or 88 pounds 26 7 45 16 4 1 3 3 73
Carrying more than 5 kg or 11 pounds 44 21 26 10 0 0 1 2 73
Carrying more than 10 kg or 22 pounds 41 21 27 11 0 0 1 2 73
Carrying more than 20 kg or 44 pounds 34 22 32 11 1 0 1 2 73
Carrying more than 40 kg or 88 pounds 25 7 44 16 5 3 3 3 73
Pushing/pulling more than5 kg or 11 pounds 41 11 30 15 1 1 1 2 73
Pushing/pulling more than10 kg or 22 pounds 40 13 29 17 0 1 1 2 72
Pushing/pulling more than20 kg or 44 pounds 33 15 33 17 0 1 1 3 72
Pushing/pulling more than40 kg or 88 pounds 25 5 47 18 1 4 3 3 73
Static posturesStanding 45 22 30 3 0 0 1 2 73
Sitting 30 30 27 11 1 0 1 2 73
Squatting 26 30 25 15 3 1 2 2 73
Kneeling 27 30 23 15 3 1 2 2 73
Lying down 25 18 21 18 17 1 1 3 72

Appendix 2. Summary of Results for Crew Manager from Occupational Guidelines Questionnaire
2A-9
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Handling hoses 1 4 12 44 25 14 4 4 73
Handling unconscious casualties 3 44 41 8 1 3 2 3 73
Handling ladders 3 3 40 44 7 4 4 4 73
Operating cutting equipment 3 5 49 33 7 3 3 3 73
Driving vehicles 6 1 28 28 22 15 3 4 72
Climbing ladders 1 7 41 38 7 5 3 4 73
Dealing with traumatised victims 1 13 60 21 1 4 3 3 72
Dealing with traumatised others(eg relatives, public) 1 18 53 22 1 4 3 3 72
Addressing groups of people 0 4 34 33 14 15 3 4 73
Filling in forms or completing paperwork 0 0 1 11 8 79 6 6 73
Making critical decisions quickly 0 0 10 15 29 47 6 5 73
Dealing with the media 10 23 21 14 23 10 2 3 73
Working on a computer 0 0 3 6 14 78 6 6 72
Communicating over the telephone 0 1 1 5 4 88 6 6 73
Environments encounteredFire compartment temperaturesabove 100˚C 6 39 41 8 3 3 3 3 71
Elevated temperatures (30-100˚C) 1 28 43 22 4 1 3 3 72
Freezing temperatures (sub-zero) 11 52 31 4 1 0 2 2 71
Dust 3 18 47 25 6 1 3 3 72
Overcrowding 13 39 22 19 4 3 2 2 72
Open spaces 0 3 25 38 11 23 4 4 73
Height 1 6 32 44 8 8 4 4 72
Enclosed spaces 1 17 39 35 6 3 3 3 72
Total darkness 3 11 42 32 8 4 3 3 73
Partial darkness 0 5 30 49 8 7 4 4 73
Working in water 19 42 22 15 0 1 2 2 72
Working under water 85 8 3 4 0 0 1 1 73
Handling hazardous substances 5 58 32 4 0 1 2 2 73
Smoke 1 7 36 32 21 4 3 4 73
High humidity 4 26 44 22 1 3 3 3 73
Table 3: Importance respondents considered these activities to be to the effective performanceof their role? (continued)
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Dynamic flexibility requirementsBending at waist 44 19 36 1 0 0 1 2 73
Reaching 42 21 32 5 0 0 1 2 73
Stooping 36 25 25 14 0 1 1 2 73
Turning/twisting 40 22 32 4 0 1 1 2 72
Object activitiesCatching 8 16 29 38 8 0 4 3 73
Throwing 12 18 38 27 4 0 3 3 73
Fine dexterity(eg writing, assembling equipment) 33 22 33 11 1 0 1 2 73
Foot control (eg driving) 36 22 32 7 1 3 1 2 73

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-10
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time) (continued)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Equipment usedFire-protective PersonnelProtective Equipment 1 1 3 12 19 63 6 6 73
Self-Contained Breathing Apparatus 4 4 27 27 25 12 3 4 73
Extended Duration Breathing Apparatus 68 14 10 6 0 3 1 1 73
Vibrating equipment 38 16 26 12 1 5 1 2 73
Computer 0 0 1 8 11 79 6 6 73
Telephone 0 0 1 3 7 89 6 6 73
Hand-held radio 1 0 3 4 19 73 6 6 73
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Handling hoses 47 30 19 3 1 0 1 2 73
Handling unconscious casualties 53 37 7 1 1 0 1 1 73
Handling ladders 51 30 14 4 1 0 1 1 73
Operating cutting equipment 56 33 5 3 1 1 1 1 73
Driving vehicles 38 34 19 5 0 3 1 2 73
Climbing ladders 49 32 17 3 0 0 1 2 72
Dealing with traumatised victims 54 41 3 1 1 0 1 1 71
Dealing with traumatised others(eg relatives, public) 47 48 1 3 1 0 2 2 73
Addressing groups of people 22 34 40 1 3 0 3 2 73
Filling in forms or completing paperwork 26 18 48 4 4 0 3 3 73
Making critical decisions quickly 62 29 8 1 0 0 1 1 73
Dealing with the media 12 16 48 21 3 0 3 3 73
Working on a computer 22 18 42 14 4 0 3 3 73
Communicating over the telephone 26 19 48 5 1 0 3 3 73
Environments encounteredFire compartment temperaturesabove 100˚C 41 30 25 3 1 0 1 2 73
Elevated temperatures (30-100˚C) 34 40 23 1 1 0 2 2 73
Freezing temperatures (sub-zero) 22 28 29 17 4 0 3 3 72
Dust 17 29 36 15 3 0 3 3 72
Overcrowding 10 22 34 27 4 3 3 3 73
Open spaces 19 18 29 23 10 1 3 3 73
Height 38 27 26 4 4 0 1 2 73
Enclosed spaces 36 31 22 8 3 0 1 2 72
Total darkness 37 30 23 7 3 0 1 2 73
Partial darkness 34 33 25 5 3 0 1 2 73
Working in water 22 30 36 7 3 3 3 2 73
Working under water 10 11 18 14 14 34 6 4 73
Handling hazardous substances 33 25 30 5 4 3 1 2 73
Smoke 41 34 21 1 3 0 1 2 73
High humidity 34 37 22 3 3 1 2 2 73

Appendix 2. Summary of Results for Crew Manager from Occupational Guidelines Questionnaire
2A-11
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Equipment usedFire-protective PersonnelProtective Equipment 77 18 4 0 1 0 1 1 73
Self-Contained Breathing Apparatus 84 14 1 0 1 0 1 1 73
Extended Duration Breathing Apparatus 18 17 18 7 7 33 6 3 72
Vibrating equipment 21 18 21 18 4 18 1 3 72
Computer 27 26 32 11 3 1 3 2 73
Telephone 29 36 26 8 0 1 2 2 73
Hand-held radio 39 31 24 4 1 1 1 2 72
Table 6: Near Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
BA control board-Old style MK 1 Read clock 78 22 1 1 73
BA control board-Old style MK 1 Graduations & cylinder pressure 75 25 1 1 73
BA tag Read tag 82 18 1 1 73
BA control board-New style MK 2 Read clock 79 21 1 1 73
BA control board-New style MK 2 Dial calculator 75 25 1 1 73
BA tag MK 2 Read tag 79 21 1 1 73
BA main control board Read clock 77 23 1 1 73
BA main control board Read 78 22 1 1 73
Sabre centurion Read BA graduations 42 58 2 2 73
Sabre centurion Read needle position 34 66 2 2 73
Siebe Gorman Read BA graduations 8 92 2 2 73
Siebe Gorman Read needle position 12 88 2 2 73
Drager Read BA graduations 53 47 1 1 73
Drager Read needle position 44 56 2 2 73
Philips PFX Handheld radio Read channel selector 59 41 1 1 73
Philips PFX Handheld radio Read numbered channel selector 62 38 1 1 73
BA log book Handwritten 81 19 1 1 73
Universal airline pack (Drager) BA supply BA cylinder gauge 34 66 2 2 73
Low pressure air bags Air pressure gauge 71 29 1 1 73
High pressure air bag Read graduations on console 70 30 1 1 73
High pressure air bag Needle position 68 32 1 1 73
Hurst high pressure lift bags Needle position 40 60 2 2 73
Microvent resuscitation equipment Read scale 34 66 2 2 73
Carmichael Godiva appliance Pressure gauge numbers 37 63 2 2 73
Saxon Volvo appliance pump Pressure gauge numbers 41 59 2 2 73
Dennis appliance pump Pressure gauge numbers 66 34 1 1 73
Read turnout sheet 92 8 1 1 73
Read dosimeter 92 8 1 1 73
Read survey meter 79 21 1 1 73
Read computer VDU 92 8 1 1 73
Read general paperwork 86 14 1 1 73
Read pager 42 58 2 2 73
Read mobile phone text 60 40 1 1 73
Read fire control panels 86 14 1 1 73
Read maps 92 8 1 1 73
Read fire extinguishers 82 18 1 1 73
Read plan inspections 81 19 1 1 73
Inspect premises 71 29 1 1 73
Read scale ruler 40 60 2 2 73
Read sound meter 32 68 2 2 73
Read light meter 30 70 2 2 73

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-12
Table 7: Distance Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
Street names White letters on a blue background 90 10 1 1 73
House numbers Copper figures on a blue background 82 18 1 1 73
House numbers White figures on a red background 86 14 1 1 73
Retail shop numbers Gold figures on a dark green background 81 19 1 1 73
House numbers Grey figures on a white background 89 11 1 1 73
Corporate building numbers Black figure on a silver background 78 22 1 1 73
Street names Black letters on a white background 89 11 1 1 73
House numbers Gold figures on a black background 84 16 1 1 73
House numbers Handpainted black figures on a white background 89 11 1 1 73
House numbers Gold figures on a black background 84 16 1 1 73
House numbers Black figures on a white background 84 16 1 1 73
Carmichael Godiva appliance pump Pressure gauge needle at rear of appliance 40 60 2 2 73
Carmichael Godiva appliance Measuring water in tank 29 71 2 2 73
Saxon Volvo appliance pump Pressure gauge needle at rear of appliance 36 64 2 2 73
Dennis appliance pump Pressure gauge needle at rear of appliance 53 47 1 1 73
Stop sign Road traffic signs 93 7 1 1 73
Give way sign Road traffic signs 96 4 1 1 73
One way street sign Road traffic signs 95 5 1 1 73
Chemical warning sign As EC Directive 92/58/EEC Hazardous substances 90 10 1 1 73
Vehicle signs Break lights/indicators on vehicles 95 5 1 1 73
Fire safety signs 89 11 1 1 73
Exit signs 90 10 1 1 73
Table 8: Hearing Tasks that are a requirement for role
Description Yes(1) No (2) Mode Median N
Distress signal unit 96 4 1 1 73
Warning whistle 95 5 1 1 73
Radio 97 3 1 1 73
Fireground orders 96 4 1 1 73
Evacuation signals/alarms 99 1 1 1 73
Telephone 96 4 1 1 73
Traffic 90 10 1 1 73
Vibraphone 32 68 2 2 73
Pager 34 66 2 2 73
Normal verbal communication with little background noise 96 4 1 1 73
Normal verbal communication with background noise 92 8 1 1 73
Hand clapping 71 29 1 1 73
Cries of help 97 3 1 1 73
Table 9: Other senses that are a requirement for role
Description Yes(1) No (2) Mode Median N
Touch 95 5 1 1 73
Smell 89 11 1 1 73
Taste 40 60 2 2 73

2A-13
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Sprinting 32 11 23 21 9 4 1 3 75
Running 7 4 22 37 20 11 4 4 76
Jogging 13 1 13 39 21 12 4 4 76
Walking 0 0 1 4 5 90 6 6 79
Climbing stairs 0 0 5 6 16 73 6 6 80
Climbing ladders 1 4 47 32 8 8 3 3 77
Crawling 7 25 41 22 3 3 3 3 76
Jumping 16 21 30 17 8 9 3 3 77
Hammering 16 30 32 18 3 1 3 3 76
Digging 18 45 26 9 0 1 2 2 77
Strength tasksLifting more than 5 kg or 11 pounds 4 0 8 31 20 37 6 5 75
Lifting more than 10 kg or 22 pounds 4 0 17 43 23 13 4 4 75
Lifting more than 20 kg or 44 pounds 8 7 33 35 15 3 4 4 75
Lifting more than 40 kg or 88 pounds 16 19 32 28 4 1 3 3 75
Carrying more than 5 kg or 11 pounds 4 3 14 27 24 28 6 5 74
Carrying more than 10 kg or 22 pounds 4 4 27 33 16 16 4 4 75
Carrying more than 20 kg or 44 pounds 9 13 36 28 11 4 3 3 76
Carrying more than 40 kg or 88 pounds 19 23 23 25 6 3 4 3 77
Pushing/pulling more than5 kg or 11 pounds 9 7 18 30 20 16 4 4 76
Pushing/pulling more than10 kg or 22 pounds 8 9 30 33 11 9 4 4 76
Pushing/pulling more than20 kg or 44 pounds 12 24 32 20 9 4 3 3 76
Pushing/pulling more than40 kg or 88 pounds 18 25 29 17 8 3 3 3 76
Static posturesStanding 0 0 1 4 1 94 6 6 80
Sitting 0 0 1 4 5 90 6 6 80
Squatting 8 0 11 17 29 36 6 5 76
Kneeling 5 1 11 22 42 19 5 5 79
Lying down 10 4 10 27 36 12 5 4 77
Table 1: Respondents’ Details
Age Bracket 18-19(1) 20-29(2) 30-39(3) 40-49(4) 50+(5) Mode Median N0 1 46 46 6 3 4 80
Years of Service 0-4 (1) 5-9 (2) 10-14(3) 15-19(4) 20-24(5) 25+(6) Mode Median N0 11 25 26 21 16 4 4 80
Gender Male Female Mode Median N99 1 1 1 80
Employment Status Fulltime(1) Retained(2) Mode Median N92 8 1 1 79
Appendix 3. Summary of Results for Watch Managerfrom Occupational Guidelines QuestionnaireNote: Results are displayed as a percentage of the total responses for each role, and as the mode, median and total number (N) ofrespondents for the role

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-14
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time) (continued)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Dynamic flexibility requirementsBending at waist 1 0 3 9 14 74 6 6 80
Reaching 1 0 1 9 14 75 6 6 80
Stooping 4 0 9 11 25 51 6 6 79
Turning/twisting 3 0 4 6 13 75 6 6 80
Object activitiesCatching 13 6 21 29 21 10 4 4 78
Throwing 8 13 18 35 16 10 4 4 77
Fine dexterity(eg writing, assembling equipment) 0 0 1 5 6 88 6 6 80
Foot control (eg driving) 8 3 10 8 15 57 6 6 79
Table 3: Importance respondents considered these activities to be to the effective performanceof their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Sprinting 4 11 34 23 13 15 3 4 79
Running 9 23 37 16 5 10 3 3 79
Jogging 10 24 46 9 4 8 3 3 79
Walking 50 25 25 0 0 0 1 2 80
Climbing stairs 45 24 29 3 0 0 1 2 80
Climbing ladders 56 20 22 1 0 1 1 1 79
Crawling 33 23 27 14 0 4 1 2 79
Jumping 14 18 28 34 3 4 4 3 79
Hammering 8 21 26 31 12 4 4 3 78
Digging 8 18 29 33 8 5 4 3 79
Strength tasksLifting more than 5 kg or 11 pounds 48 19 26 4 0 3 1 2 77
Lifting more than 10 kg or 22 pounds 47 19 29 3 0 3 1 2 77
Lifting more than 20 kg or 44 pounds 38 21 29 9 0 4 1 2 77
Lifting more than 40 kg or 88 pounds 24 22 31 18 0 5 3 3 78
Carrying more than 5 kg or 11 pounds 43 22 25 5 0 4 1 2 76
Carrying more than 10 kg or 22 pounds 42 27 25 4 0 3 1 2 77
Carrying more than 20 kg or 44 pounds 34 25 29 10 0 3 1 2 77
Carrying more than 40 kg or 88 pounds 25 23 30 17 0 5 3 3 77
Pushing/pulling more than5 kg or 11 pounds 36 23 29 8 0 4 1 2 78
Pushing/pulling more than10 kg or 22 pounds 36 25 27 8 0 4 1 2 77
Pushing/pulling more than20 kg or 44 pounds 29 26 30 10 0 5 3 2 77
Pushing/pulling more than40 kg or 88 pounds 24 22 29 19 0 5 3 3 78
Static posturesStanding 63 18 14 5 1 0 1 1 80
Sitting 50 21 20 8 1 0 1 2 80
Squatting 32 22 28 15 1 3 1 2 79
Kneeling 30 24 29 13 1 3 1 2 79
Lying down 19 18 25 23 9 6 3 3 79

Appendix 3. Summary of Results for Watch Manager from Occupational Guidelines Questionnaire
2A-15
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Handling hoses 4 1 19 52 18 6 4 4 79
Handling unconscious casualties 4 43 38 11 3 1 2 3 79
Handling ladders 3 5 46 34 8 5 3 3 79
Operating cutting equipment 5 14 47 29 1 4 3 3 79
Driving vehicles 9 14 27 24 13 14 3 4 79
Climbing ladders 1 9 48 32 3 6 3 3 77
Dealing with traumatised victims 1 15 49 30 1 3 3 3 79
Dealing with traumatised others(eg relatives, public) 0 13 48 30 4 5 3 3 77
Addressing groups of people 0 6 29 37 15 13 4 4 79
Filling in forms or completing paperwork 0 0 3 5 14 79 6 6 80
Making critical decisions quickly 0 4 9 14 16 58 6 6 80
Dealing with the media 8 20 20 18 26 9 5 4 80
Working on a computer 0 0 1 4 10 85 6 6 80
Communicating over the telephone 0 0 0 5 3 93 6 6 80
Environments encounteredFire compartment temperaturesabove 100˚C 19 48 18 10 3 3 2 2 79
Elevated temperatures (30-100˚C) 11 32 34 18 3 3 3 3 79
Freezing temperatures (sub-zero) 15 57 20 5 1 1 2 2 79
Dust 5 27 40 17 6 5 3 3 78
Overcrowding 18 32 26 17 5 3 2 3 78
Open spaces 3 8 22 31 17 21 4 4 78
Height 1 6 29 46 13 4 4 4 78
Enclosed spaces 3 13 35 38 5 6 4 4 78
Total darkness 5 19 35 32 4 5 3 3 78
Partial darkness 1 13 31 38 12 5 4 4 78
Working in water 17 48 30 4 0 1 2 2 77
Working under water 79 13 5 1 0 1 1 1 78
Handling hazardous substances 14 56 19 3 3 5 2 2 78
Smoke 6 9 28 35 17 5 4 4 78
High humidity 5 40 35 15 0 5 2 3 78
Table 3: Importance respondents considered these activities to be to the effective performanceof their role? (continued)
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Dynamic flexibility requirementsBending at waist 49 24 21 4 1 1 1 2 80
Reaching 46 25 21 5 1 1 1 2 80
Stooping 41 23 24 9 1 3 1 2 79
Turning/twisting 49 23 20 5 1 3 1 2 80
Object activitiesCatching 19 14 33 24 5 5 3 3 79
Throwing 22 14 39 18 3 5 3 3 79
Fine dexterity(eg writing, assembling equipment) 41 28 28 4 0 0 1 2 80
Foot control (eg driving) 42 24 25 8 1 0 1 2 79

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-16
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time) (continued)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Equipment usedFire-protective PersonnelProtective Equipment 3 3 5 5 19 65 6 6 77
Self-Contained Breathing Apparatus 5 21 45 14 9 5 3 3 77
Extended Duration Breathing Apparatus 83 7 7 1 1 1 1 1 76
Vibrating equipment 45 25 22 5 0 3 1 2 76
Computer 0 0 1 3 8 88 6 6 76
Telephone 0 0 1 1 5 92 6 6 77
Hand-held radio 3 0 3 8 16 71 6 6 77
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Handling hoses 49 27 10 11 0 3 1 2 79
Handling unconscious casualties 51 27 19 3 0 1 1 1 79
Handling ladders 53 23 15 6 0 3 1 1 79
Operating cutting equipment 54 23 19 3 0 1 1 1 79
Driving vehicles 42 24 25 6 0 3 1 2 79
Climbing ladders 52 19 19 8 0 3 1 1 79
Dealing with traumatised victims 48 34 15 1 0 1 1 2 79
Dealing with traumatised others(eg relatives, public) 39 41 19 1 0 0 2 2 79
Addressing groups of people 15 44 35 5 0 0 2 2 79
Filling in forms or completing paperwork 21 35 43 1 0 0 3 2 80
Making critical decisions quickly 74 15 9 1 0 1 1 1 80
Dealing with the media 10 24 49 15 3 0 3 3 80
Working on a computer 14 30 50 5 1 0 3 3 80
Communicating over the telephone 20 38 40 1 1 0 3 2 80
Environments encounteredFire compartment temperatures above 100˚C 41 24 22 6 4 3 1 2 78
Elevated temperatures (30-100˚C) 38 26 24 5 4 3 1 2 78
Freezing temperatures (sub-zero) 24 22 32 9 8 6 3 3 79
Dust 24 23 27 15 8 3 3 3 78
Overcrowding 15 23 27 19 10 5 3 3 78
Open spaces 18 24 24 23 5 5 3 3 78
Height 44 27 25 1 1 1 1 2 77
Enclosed spaces 44 27 24 3 1 1 1 2 79
Total darkness 46 20 24 6 3 1 1 2 79
Partial darkness 44 22 27 4 3 1 1 2 79
Working in water 24 25 41 6 1 3 3 3 79
Working under water 13 10 23 20 16 18 3 4 79
Handling hazardous substances 28 32 28 5 5 1 2 2 78
Smoke 43 29 20 1 5 1 1 2 79
High humidity 38 28 25 1 4 4 1 2 79

Appendix 3. Summary of Results for Watch Manager from Occupational Guidelines Questionnaire
2A-17
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Equipment usedFire-protective PersonnelProtective Equipment 79 12 8 0 0 1 1 1 78
Self-Contained Breathing Apparatus 76 13 9 0 0 3 1 1 78
Extended Duration Breathing Apparatus 15 12 22 10 8 33 6 4 78
Vibrating equipment 21 14 33 10 6 15 3 3 78
Computer 21 28 46 4 1 0 3 3 78
Telephone 26 32 40 1 1 0 3 2 78
Hand-held radio 32 35 29 3 0 1 2 2 78
Table 6: Near Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
BA control board-Old style MK 1 Read clock 71 29 1 1 80
BA control board-Old style MK 1 Graduations & cylinder pressure 71 29 1 1 80
BA tag Read tag 78 23 1 1 80
BA control board-New style MK 2 Read clock 68 33 1 1 80
BA control board-New style MK 2 Dial calculator 63 38 1 1 80
BA tag MK 2 Read tag 63 38 1 1 80
BA main control board Read clock 84 16 1 1 80
BA main control board Read 81 19 1 1 80
Sabre centurion Read BA graduations 46 54 2 2 80
Sabre centurion Read needle position 45 55 2 2 80
Siebe Gorman Read BA graduations 24 76 2 2 80
Siebe Gorman Read needle position 24 76 2 2 80
Drager Read BA graduations 45 55 2 2 80
Drager Read needle position 41 59 2 2 80
Philips PFX Handheld radio Read channel selector 71 29 1 1 80
Philips PFX Handheld radio Read numbered channel selector 74 26 1 1 80
BA log book Handwritten 80 20 1 1 80
Universal airline pack (Drager) BA supply BA cylinder gauge 34 66 2 2 80
Low pressure air bags Air pressure gauge 61 39 1 1 80
High pressure air bag Read graduations on console 58 43 1 1 80
High pressure air bag Needle position 50 50 2 2 80
Hurst high pressure lift bags Needle position 33 68 2 2 80
Microvent resuscitation equipment Read scale 24 76 2 2 80
Carmichael Godiva appliance Pressure gauge numbers 28 73 2 2 80
Saxon Volvo appliance pump Pressure gauge numbers 23 78 2 2 80
Dennis appliance pump Pressure gauge numbers 41 59 2 2 80
Read turnout sheet 79 21 1 1 80
Read dosimeter 76 24 1 1 80
Read survey meter 73 28 1 1 80
Read computer VDU 88 13 1 1 80
Read general paperwork 85 15 1 1 80
Read pager 49 51 2 2 80
Read mobile phone text 56 44 1 1 80
Read fire control panels 81 19 1 1 80
Read maps 86 14 1 1 80
Read fire extinguishers 69 31 1 1 80
Read plan inspections 69 31 1 1 80
Inspect premises 70 30 1 1 80
Read scale ruler 43 58 2 2 80
Read sound meter 25 75 2 2 80
Read light meter 24 76 2 2 80

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-18
Table 7: Distance Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
Street names White letters on a blue background 84 16 1 1 80
House numbers Copper figures on a blue background 80 20 1 1 80
House numbers White figures on a red background 80 20 1 1 80
Retail shop numbers Gold figures on a dark green background 74 26 1 1 80
House numbers Grey figures on a white background 79 21 1 1 80
Corporate building numbers Black figure on a silver background 78 23 1 1 80
Street names Black letters on a white background 88 13 1 1 80
House numbers Gold figures on a black background 81 19 1 1 80
House numbers Handpainted black figures on a white background 83 18 1 1 80
House numbers Gold figures on a black background 81 19 1 1 80
House numbers Black figures on a white background 85 15 1 1 80
Carmichael Godiva appliance pump Pressure gauge needle at rear of appliance 36 64 2 2 80
Carmichael Godiva appliance Measuring water in tank 34 66 2 2 80
Saxon Volvo appliance pump Pressure gauge needle at rear of appliance 26 74 2 2 80
Dennis appliance pump Pressure gauge needle at rear of appliance 53 48 1 1 80
Stop sign Road traffic signs 84 16 1 1 80
Give way sign Road traffic signs 83 18 1 1 80
One way street sign Road traffic signs 83 18 1 1 80
Chemical warning sign As EC Directive 92/58/EEC Hazardous substances 90 10 1 1 80
Vehicle signs Break lights/indicators on vehicles 83 18 1 1 80
Fire safety signs 84 16 1 1 80
Exit signs 84 16 1 1 80
Table 8: Hearing Tasks that are a requirement for role
Description Yes(1) No (2) Mode Median N
Distress signal unit 95 5 1 1 80
Warning whistle 96 4 1 1 80
Radio 99 1 1 1 80
Fireground orders 95 5 1 1 80
Evacuation signals/alarms 95 5 1 1 80
Telephone 98 3 1 1 80
Traffic 88 13 1 1 80
Vibraphone 36 64 2 2 80
Pager 43 58 2 2 80
Normal verbal communication with little background noise 96 4 1 1 80
Normal verbal communication with background noise 95 5 1 1 80
Hand clapping 86 14 1 1 80
Cries of help 93 8 1 1 80
Table 9: Other senses that are a requirement for role
Description Yes(1) No (2) Mode Median N
Touch 90 10 1 1 80
Smell 85 15 1 1 80
Taste 41 59 2 2 80

2A-19
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Sprinting 66 17 6 8 3 0 1 1 88
Running 32 24 24 14 7 0 1 2 88
Jogging 16 19 32 19 13 1 3 3 90
Walking 0 0 1 10 9 80 6 6 92
Climbing stairs 0 0 3 6 12 79 6 6 90
Climbing ladders 11 44 34 10 0 0 2 2 88
Crawling 36 39 20 4 1 0 2 2 90
Jumping 51 30 12 6 0 1 1 1 89
Hammering 68 10 18 3 1 0 1 1 90
Digging 67 12 17 3 1 0 1 1 90
Strength tasksLifting more than 5 kg or 11 pounds 9 7 20 29 16 19 4 4 89
Lifting more than 10 kg or 22 pounds 16 14 31 22 15 3 3 3 88
Lifting more than 20 kg or 44 pounds 27 24 25 20 4 0 1 2 89
Lifting more than 40 kg or 88 pounds 50 29 14 7 0 0 1 2 86
Carrying more than 5 kg or 11 pounds 18 6 17 28 15 16 4 4 87
Carrying more than 10 kg or 22 pounds 22 15 28 20 11 3 3 3 88
Carrying more than 20 kg or 44 pounds 36 22 21 20 2 0 1 2 87
Carrying more than 40 kg or 88 pounds 51 28 16 3 1 0 1 1 86
Pushing/pulling more than5 kg or 11 pounds 25 17 20 21 8 9 1 3 89
Pushing/pulling more than10 kg or 22 pounds 30 17 28 15 9 1 1 3 88
Pushing/pulling more than20 kg or 44 pounds 39 28 22 9 2 0 1 2 88
Pushing/pulling more than40 kg or 88 pounds 50 30 15 6 0 0 1 2 88
Static posturesStanding 0 0 2 5 5 87 6 6 91
Sitting 1 2 2 2 4 88 6 6 90
Squatting 14 7 19 22 26 13 5 4 88
Kneeling 13 13 23 21 21 9 3 4 86
Lying down 58 13 6 7 9 7 1 1 89
Table 1: Respondents’ Details
Age Bracket 18-19(1) 20-29(2) 30-39(3) 40-49(4) 50+(5) Mode Median N0 1 29 63 7 4 4 92
Years of Service 0-4 (1) 5-9 (2) 10-14(3) 15-19(4) 20-24(5) 25+(6) Mode Median N0 1 15 26 30 27 5 5 91
Gender Male Female Mode Median N98 2 1 1 92
Employment Status Fulltime(1) Retained(2) Mode Median N98 2 1 1 91
Appendix 4. Summary of Results for Station Managerfrom Occupational Guidelines QuestionnaireNote: Results are displayed as a percentage of the total responses for each role, and as the mode, median and total number (N) ofrespondents for the role

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-20
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time) (continued)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Dynamic flexibility requirementsBending at waist 1 1 12 9 11 66 6 6 90
Reaching 1 1 11 9 20 58 6 6 91
Stooping 2 2 13 16 18 49 6 5 90
Turning/twisting 1 1 11 10 16 60 6 6 91
Object activitiesCatching 42 20 17 11 7 3 1 2 90
Throwing 43 20 16 10 7 4 1 2 89
Fine dexterity(eg writing, assembling equipment) 2 0 0 1 3 93 6 6 89
Foot control (eg driving) 0 0 0 0 6 94 6 6 90
Table 3: Importance respondents considered these activities to be to the effective performanceof their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Sprinting 2 1 12 33 30 22 4 5 91
Running 2 3 36 31 14 13 3 4 91
Jogging 3 10 43 23 12 9 3 3 91
Walking 50 17 30 1 0 1 1 2 92
Climbing stairs 45 17 34 1 1 2 1 2 92
Climbing ladders 22 17 36 16 4 6 3 3 90
Crawling 12 9 22 36 15 5 4 4 91
Jumping 8 3 15 41 25 8 4 4 91
Hammering 3 1 13 31 30 22 4 5 91
Digging 2 2 19 30 25 22 4 4 91
Strength tasksLifting more than 5 kg or 11 pounds 22 16 46 6 4 7 3 3 90
Lifting more than 10 kg or 22 pounds 17 14 51 7 4 7 3 3 90
Lifting more than 20 kg or 44 pounds 9 12 38 21 10 9 3 3 89
Lifting more than 40 kg or 88 pounds 6 7 30 32 12 13 4 4 90
Carrying more than 5 kg or 11 pounds 22 14 41 11 3 8 3 3 90
Carrying more than 10 kg or 22 pounds 18 13 43 13 4 8 3 3 90
Carrying more than 20 kg or 44 pounds 11 11 37 23 10 8 3 3 90
Carrying more than 40 kg or 88 pounds 7 8 30 32 11 12 4 4 90
Pushing/pulling more than5 kg or 11 pounds 18 12 38 19 3 9 3 3 89
Pushing/pulling more than10 kg or 22 pounds 16 12 37 19 7 10 3 3 90
Pushing/pulling more than20 kg or 44 pounds 10 9 30 31 10 10 4 4 90
Pushing/pulling more than40 kg or 88 pounds 7 8 26 32 14 13 4 4 90
Static posturesStanding 51 13 31 3 1 1 1 1 91
Sitting 49 14 31 4 1 0 1 2 91
Squatting 18 14 29 22 9 8 3 3 90
Kneeling 18 13 32 20 11 6 3 3 90
Lying down 10 4 20 20 27 18 5 4 89

Appendix 4. Summary of Results for Station Manager from Occupational Guidelines Questionnaire
2A-21
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Handling hoses 22 40 35 3 0 0 2 2 92
Handling unconscious casualties 33 58 9 1 0 0 2 2 92
Handling ladders 29 50 21 0 0 0 2 2 92
Operating cutting equipment 45 41 13 0 0 1 1 2 92
Driving vehicles 1 3 4 0 2 89 6 6 92
Climbing ladders 13 45 37 3 0 1 2 2 89
Dealing with traumatised victims 11 26 47 15 0 0 3 3 91
Dealing with traumatised others(eg relatives, public) 9 20 50 13 2 6 3 3 90
Addressing groups of people 0 2 32 28 25 13 3 4 92
Filling in forms or completing paperwork 0 0 0 2 11 87 6 6 92
Making critical decisions quickly 0 1 12 23 27 37 6 5 92
Dealing with the media 0 16 46 22 7 10 3 3 92
Working on a computer 0 0 1 1 1 97 6 6 92
Communicating over the telephone 1 1 0 0 1 97 6 6 92
Environments encounteredFire compartment temperaturesabove 100˚C 37 44 16 1 0 2 2 2 90
Elevated temperatures (30-100˚C) 22 57 16 4 0 1 2 2 92
Freezing temperatures (sub-zero) 24 51 22 2 0 1 2 2 92
Dust 21 33 36 11 0 0 3 2 92
Overcrowding 32 39 17 9 2 1 2 2 92
Open spaces 10 16 32 21 10 11 3 3 90
Height 10 26 48 14 1 1 3 3 92
Enclosed spaces 16 43 24 13 2 1 2 2 91
Total darkness 23 51 16 5 4 0 2 2 91
Partial darkness 11 23 41 14 11 0 3 3 92
Working in water 51 41 6 1 1 0 1 1 90
Working under water 95 5 0 0 0 0 1 1 91
Handling hazardous substances 47 33 18 1 0 1 1 2 92
Smoke 11 25 53 10 1 0 3 3 92
High humidity 21 52 22 3 2 0 2 2 92
Table 3: Importance respondents considered these activities to be to the effective performanceof their role? (continued)
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Dynamic flexibility requirementsBending at waist 35 15 44 4 1 0 3 2 91
Reaching 32 14 43 7 3 1 3 3 91
Stooping 29 14 36 15 3 2 3 3 91
Turning/twisting 32 13 46 7 2 0 3 3 91
Object activitiesCatching 7 7 21 29 22 15 4 4 91
Throwing 8 9 23 24 21 14 4 4 90
Fine dexterity(eg writing, assembling equipment) 48 28 20 3 0 1 1 2 90
Foot control (eg driving) 53 26 21 0 0 0 1 1 91

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-22
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time) (continued)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Equipment usedFire-protective PersonnelProtective Equipment 1 7 15 52 22 3 4 4 92
Self-Contained Breathing Apparatus 22 57 18 2 0 1 2 2 92
Extended Duration Breathing Apparatus 99 1 0 0 0 0 1 1 92
Vibrating equipment 79 7 4 0 3 7 1 1 92
Computer 1 0 0 0 3 96 6 6 92
Telephone 0 0 0 1 3 96 6 6 92
Hand-held radio 1 1 22 32 17 27 4 4 92
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Handling hoses 18 14 13 33 13 9 4 4 91
Handling unconscious casualties 25 20 32 11 7 5 3 3 91
Handling ladders 16 11 22 35 10 5 4 4 91
Operating cutting equipment 17 13 13 37 12 7 4 4 89
Driving vehicles 62 24 12 2 0 0 1 1 91
Climbing ladders 20 20 30 20 4 4 3 3 89
Dealing with traumatised victims 27 31 35 4 1 1 3 2 91
Dealing with traumatised others(eg relatives, public) 29 34 31 3 1 1 2 2 90
Addressing groups of people 27 42 31 0 0 0 2 2 91
Filling in forms or completing paperwork 29 38 32 1 0 0 2 2 91
Making critical decisions quickly 57 34 9 0 0 0 1 1 90
Dealing with the media 15 44 38 1 1 0 2 2 91
Working on a computer 38 35 23 4 0 0 1 2 92
Communicating over the telephone 41 36 22 1 0 0 1 2 91
Environments encounteredFire compartment temperaturesabove 100˚C 14 20 33 18 8 8 3 3 92
Elevated temperatures (30-100˚C) 10 22 42 14 7 5 3 3 91
Freezing temperatures (sub-zero) 4 20 42 23 7 4 3 3 91
Dust 7 12 42 25 8 7 3 3 91
Overcrowding 4 14 36 29 10 7 3 3 91
Open spaces 8 16 35 27 10 3 3 3 91
Height 18 29 37 11 2 3 3 3 91
Enclosed spaces 14 31 33 14 3 4 3 3 91
Total darkness 16 27 32 18 2 4 3 3 91
Partial darkness 15 24 36 20 1 3 3 3 91
Working in water 7 24 32 23 5 9 3 3 91
Working under water 3 9 12 30 13 32 6 4 90
Handling hazardous substances 13 27 29 16 7 9 3 3 90
Smoke 20 28 33 13 2 4 3 3 92
High humidity 13 22 36 19 4 5 3 3 91

Appendix 4. Summary of Results for Station Manager from Occupational Guidelines Questionnaire
2A-23
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Equipment usedFire-protective PersonnelProtective Equipment 66 23 10 1 0 0 1 1 92
Self-Contained Breathing Apparatus 52 17 18 8 2 2 1 1 92
Extended Duration Breathing Apparatus 7 5 16 22 8 42 6 5 92
Vibrating equipment 7 5 18 27 14 29 6 4 91
Computer 38 41 18 2 0 0 2 2 92
Telephone 43 40 16 0 0 0 1 2 92
Hand-held radio 39 45 16 0 0 0 2 2 92
Table 6: Near Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
BA control board-Old style MK 1 Read clock 46 54 2 2 92
BA control board-Old style MK 1 Graduations & cylinder pressure 43 57 2 2 92
BA tag Read tag 55 45 1 1 92
BA control board-New style MK 2 Read clock 52 48 1 1 92
BA control board-New style MK 2 Dial calculator 46 54 2 2 92
BA tag MK 2 Read tag 48 52 2 2 92
BA main control board Read clock 66 34 1 1 92
BA main control board Read 66 34 1 1 92
Sabre centurion Read BA graduations 35 65 2 2 92
Sabre centurion Read needle position 36 64 2 2 92
Siebe Gorman Read BA graduations 8 92 2 2 92
Siebe Gorman Read needle position 10 90 2 2 92
Drager Read BA graduations 32 68 2 2 92
Drager Read needle position 28 72 2 2 92
Philips PFX Handheld radio Read channel selector 65 35 1 1 92
Philips PFX Handheld radio Read numbered channel selector 64 36 1 1 92
BA log book Handwritten 65 35 1 1 92
Universal airline pack (Drager) BA supply BA cylinder gauge 16 84 2 2 92
Low pressure air bags Air pressure gauge 28 72 2 2 92
High pressure air bag Read graduations on console 28 72 2 2 92
High pressure air bag Needle position 29 71 2 2 92
Hurst high pressure lift bags Needle position 21 79 2 2 92
Microvent resuscitation equipment Read scale 11 89 2 2 92
Carmichael Godiva appliance Pressure gauge numbers 18 82 2 2 92
Saxon Volvo appliance pump Pressure gauge numbers 21 79 2 2 92
Dennis appliance pump Pressure gauge numbers 32 68 2 2 92
Read turnout sheet 53 47 1 1 92
Read dosimeter 58 42 1 1 92
Read survey meter 54 46 1 1 92
Read computer VDU 77 23 1 1 92
Read general paperwork 82 18 1 1 92
Read pager 73 27 1 1 92
Read mobile phone text 73 27 1 1 92
Read fire control panels 62 38 1 1 92
Read maps 76 24 1 1 92
Read fire extinguishers 42 58 2 2 92
Read plan inspections 61 39 1 1 92
Inspect premises 57 43 1 1 92
Read scale ruler 47 53 2 2 92
Read sound meter 28 72 2 2 92
Read light meter 29 71 2 2 92

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-24
Table 7: Distance Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
Street names White letters on a blue background 88 12 1 1 92
House numbers Copper figures on a blue background 83 17 1 1 92
House numbers White figures on a red background 80 20 1 1 92
Retail shop numbers Gold figures on a dark green background 80 20 1 1 92
House numbers Grey figures on a white background 82 18 1 1 92
Corporate building numbers Black figure on a silver background 76 24 1 1 92
Street names Black letters on a white background 93 7 1 1 92
House numbers Gold figures on a black background 78 22 1 1 92
House numbers Handpainted black figures on a white background 82 18 1 1 92
House numbers Gold figures on a black background 79 21 1 1 92
House numbers Black figures on a white background 83 17 1 1 92
Carmichael Godiva appliance pump Pressure gauge needle at rear of appliance 28 72 2 2 92
Carmichael Godiva appliance Measuring water in tank 24 76 2 2 92
Saxon Volvo appliance pump Pressure gauge needle at rear of appliance 21 79 2 2 92
Dennis appliance pump Pressure gauge needle at rear of appliance 36 64 2 2 92
Stop sign Road traffic signs 97 3 1 1 92
Give way sign Road traffic signs 99 1 1 1 92
One way street sign Road traffic signs 99 1 1 1 92
Chemical warning sign As EC Directive 92/58/EEC Hazardous substances 96 4 1 1 92
Vehicle signs Break lights/indicators on vehicles 99 1 1 1 92
Fire safety signs 91 9 1 1 92
Exit signs 90 10 1 1 92
Table 8: Hearing Tasks that are a requirement for role
Description Yes(1) No (2) Mode Median N
Distress signal unit 89 11 1 1 92
Warning whistle 92 8 1 1 92
Radio 99 1 1 1 92
Fireground orders 99 1 1 1 92
Evacuation signals/alarms 99 1 1 1 92
Telephone 100 0 1 1 92
Traffic 92 8 1 1 92
Vibraphone 36 64 2 2 92
Pager 88 12 1 1 92
Normal verbal communication with little background noise 99 1 1 1 92
Normal verbal communication with background noise 98 2 1 1 92
Hand clapping 72 28 1 1 92
Cries of help 90 10 1 1 92
Table 9: Other senses that are a requirement for role
Description Yes(1) No (2) Mode Median N
Touch 87 13 1 1 92
Smell 92 8 1 1 92
Taste 32 68 2 2 92

2A-25
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Sprinting 67 14 12 7 0 0 1 1 94
Running 41 25 20 11 3 0 1 2 96
Jogging 28 21 30 14 6 2 3 3 101
Walking 0 0 2 7 9 83 6 6 103
Climbing stairs 1 0 4 1 6 88 6 6 102
Climbing ladders 19 50 28 2 0 0 2 2 103
Crawling 43 46 11 0 0 0 2 2 102
Jumping 52 26 20 2 0 0 1 1 101
Hammering 70 17 12 2 0 0 1 1 103
Digging 75 14 9 3 0 0 1 1 103
Strength tasksLifting more than 5 kg or 11 pounds 11 6 27 21 16 20 3 4 101
Lifting more than 10 kg or 22 pounds 20 13 23 26 14 3 4 3 99
Lifting more than 20 kg or 44 pounds 32 28 14 24 1 0 1 2 99
Lifting more than 40 kg or 88 pounds 59 22 14 2 3 0 1 1 97
Carrying more than 5 kg or 11 pounds 13 6 30 20 10 21 3 4 100
Carrying more than 10 kg or 22 pounds 25 19 24 16 12 3 1 3 99
Carrying more than 20 kg or 44 pounds 37 30 15 17 0 0 1 2 99
Carrying more than 40 kg or 88 pounds 64 23 7 3 2 0 1 1 98
Pushing/pulling more than5 kg or 11 pounds 38 16 22 12 3 8 1 2 99
Pushing/pulling more than10 kg or 22 pounds 44 19 18 13 6 0 1 2 97
Pushing/pulling more than20 kg or 44 pounds 53 25 13 8 1 0 1 1 97
Pushing/pulling more than40 kg or 88 pounds 66 25 6 1 1 1 1 1 97
Static posturesStanding 0 0 1 3 5 91 6 6 104
Sitting 0 0 0 3 5 92 6 6 102
Squatting 13 11 21 24 24 5 4 4 98
Kneeling 16 7 31 27 16 2 3 3 99
Lying down 57 17 10 2 8 5 1 1 98
Table 1: Respondents’ Details
Age Bracket 18-19(1) 20-29(2) 30-39(3) 40-49(4) 50+(5) Mode Median N0 0 12 63 25 4 4 105
Years of Service 0-4 (1) 5-9 (2) 10-14(3) 15-19(4) 20-24(5) 25+(6) Mode Median N0 0 5 16 23 56 6 6 105
Gender Male Female Mode Median N100 0 1 1 105
Employment Status Fulltime(1) Retained(2) Mode Median N100 0 1 1 101
Appendix 5. Summary of Results for Group Managerfrom Occupational Guidelines QuestionnaireNote: Results are displayed as a percentage of the total responses for each role, and as the mode, median and total number (N) ofrespondents for the role

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-26
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time) (continued)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Dynamic flexibility requirementsBending at waist 3 1 5 8 31 52 6 6 103
Reaching 3 2 9 7 24 56 6 6 104
Stooping 6 1 12 10 31 41 6 5 104
Turning/twisting 3 1 6 9 23 58 6 6 101
Object activitiesCatching 48 23 18 10 2 0 1 2 102
Throwing 51 19 20 7 2 2 1 1 102
Fine dexterity(eg writing, assembling equipment) 1 0 1 0 0 98 6 6 104
Foot control (eg driving) 0 0 1 0 3 96 6 6 104
Table 3: Importance respondents considered these activities to be to the effective performanceof their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Sprinting 1 3 11 26 31 28 5 5 103
Running 1 12 20 29 22 16 4 4 104
Jogging 3 12 32 22 18 13 3 4 103
Walking 48 29 16 5 2 0 1 2 104
Climbing stairs 38 31 19 8 4 0 1 2 104
Climbing ladders 18 20 22 23 12 4 4 3 103
Crawling 6 11 22 31 22 9 4 4 104
Jumping 1 9 14 35 30 12 4 4 103
Hammering 1 3 6 31 35 25 5 5 104
Digging 1 1 7 28 35 29 5 5 104
Strength tasksLifting more than 5 kg or 11 pounds 19 18 30 21 8 5 3 3 102
Lifting more than 10 kg or 22 pounds 9 20 34 22 10 6 3 3 102
Lifting more than 20 kg or 44 pounds 4 12 32 25 15 12 3 4 102
Lifting more than 40 kg or 88 pounds 1 7 16 46 19 12 4 4 102
Carrying more than 5 kg or 11 pounds 17 17 31 19 9 8 3 3 102
Carrying more than 10 kg or 22 pounds 10 18 34 22 10 7 3 3 101
Carrying more than 20 kg or 44 pounds 4 14 27 30 16 10 4 4 101
Carrying more than 40 kg or 88 pounds 1 6 17 43 22 12 4 4 101
Pushing/pulling more than5 kg or 11 pounds 10 15 26 26 11 12 3 3 102
Pushing/pulling more than 10 kg or 22 pounds 6 16 25 30 12 11 4 4 102
Pushing/pulling more than20 kg or 44 pounds 4 10 23 35 17 12 4 4 102
Pushing/pulling more than40 kg or 88 pounds 2 4 15 48 20 12 4 4 102
Static posturesStanding 47 26 16 9 2 1 1 2 103
Sitting 48 20 24 6 1 1 1 2 103
Squatting 12 16 24 28 14 6 4 3 104
Kneeling 10 14 24 32 13 7 4 4 104
Lying down 8 4 14 24 17 33 6 5 104

Appendix 5. Summary of Results for Group Manager from Occupational Guidelines Questionnaire
2A-27
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Handling hoses 33 47 19 1 0 0 2 2 104
Handling unconscious casualties 46 46 9 0 0 0 2 2 105
Handling ladders 44 48 9 0 0 0 2 2 103
Operating cutting equipment 63 30 6 0 0 2 1 1 104
Driving vehicles 1 3 0 0 5 91 6 6 104
Climbing ladders 25 52 22 1 0 0 2 2 105
Dealing with traumatised victims 17 37 40 4 2 0 3 2 103
Dealing with traumatised others(eg relatives, public) 11 34 43 7 3 3 3 3 104
Addressing groups of people 0 3 16 43 22 15 4 4 104
Filling in forms or completing paperwork 0 0 0 1 13 86 6 6 104
Making critical decisions quickly 0 0 16 19 29 36 6 5 104
Dealing with the media 2 19 47 23 3 7 3 3 105
Working on a computer 0 0 0 1 1 98 6 6 104
Communicating over the telephone 1 0 0 0 0 99 6 6 103
Environments encounteredFire compartment temperatures above 100˚C 41 48 8 1 0 1 2 2 99
Elevated temperatures (30-100˚C) 19 55 23 3 0 0 2 2 104
Freezing temperatures (sub-zero) 27 50 23 0 0 1 2 2 105
Dust 24 43 27 6 0 1 2 2 101
Overcrowding 33 35 23 5 3 1 2 2 102
Open spaces 12 15 33 15 20 6 3 3 103
Height 10 41 37 6 4 2 2 2 102
Enclosed spaces 17 50 25 4 2 2 2 2 103
Total darkness 25 44 20 6 4 1 2 2 103
Partial darkness 18 24 35 10 13 1 3 3 104
Working in water 59 37 3 0 1 0 1 1 102
Working under water 95 5 0 0 0 0 1 1 102
Handling hazardous substances 50 35 12 1 1 0 1 1 105
Smoke 14 39 42 4 1 0 3 2 105
High humidity 26 57 15 2 0 0 2 2 103
Table 3: Importance respondents considered these activities to be to the effective performanceof their role? (continued)
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Dynamic flexibility requirementsBending at waist 25 27 31 13 3 2 3 2 104
Reaching 26 23 31 14 5 1 3 3 104
Stooping 24 21 30 17 6 1 3 3 103
Turning/twisting 28 22 33 11 5 2 3 3 104
Object activitiesCatching 7 4 17 34 21 17 4 4 103
Throwing 6 7 15 37 19 17 4 4 103
Fine dexterity(eg writing, assembling equipment) 49 33 9 9 0 1 1 2 104
Foot control (eg driving) 60 29 6 4 0 1 1 1 103

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-28
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time) (continued)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Equipment usedFire-protective PersonnelProtective Equipment 6 3 41 39 5 7 3 4 105
Self-Contained Breathing Apparatus 23 70 6 1 0 0 2 2 104
Extended Duration Breathing Apparatus 95 4 0 0 0 1 1 1 104
Vibrating equipment 83 10 1 1 3 3 1 1 103
Computer 0 0 0 0 1 99 6 6 105
Telephone 0 0 0 0 1 99 6 6 105
Hand-held radio 3 3 34 26 13 22 3 4 104
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Handling hoses 9 8 16 21 27 19 5 4 103
Handling unconscious casualties 9 12 24 21 18 16 3 4 104
Handling ladders 9 7 19 26 22 17 4 4 104
Operating cutting equipment 11 5 15 30 20 19 4 4 103
Driving vehicles 77 11 10 0 0 3 1 1 104
Climbing ladders 13 11 28 24 12 13 3 3 101
Dealing with traumatised victims 10 30 38 12 3 9 3 3 104
Dealing with traumatised others (eg relatives, public) 13 32 38 8 2 9 3 3104
Addressing groups of people 33 45 20 0 1 1 2 2 104
Filling in forms or completing paperwork 42 28 27 3 0 0 1 2 104
Making critical decisions quickly 64 19 16 0 0 0 1 1 104
Dealing with the media 19 48 31 2 0 0 2 2 103
Working on a computer 50 28 19 2 0 0 1 1 103
Communicating over the telephone 52 32 16 0 0 0 1 1 104
Environments encounteredFire compartment temperaturesabove 100˚C 9 15 19 30 14 14 4 4 103
Elevated temperatures (30-100˚C) 10 17 28 25 12 9 3 3 103
Freezing temperatures (sub-zero) 7 16 25 30 12 11 4 4 104
Dust 4 15 27 31 13 11 4 4 103
Overcrowding 4 13 28 34 13 8 4 4 104
Open spaces 5 15 32 26 14 8 3 3 104
Height 13 24 31 15 9 8 3 3 104
Enclosed spaces 13 19 30 20 10 8 3 3 104
Total darkness 12 19 32 18 10 10 3 3 104
Partial darkness 13 19 38 13 8 9 3 3 104
Working in water 8 12 23 30 17 11 4 4 104
Working under water 4 6 3 30 25 32 6 5 103
Handling hazardous substances 10 15 21 22 13 19 4 4 104
Smoke 14 21 26 20 10 9 3 3 104
High humidity 10 15 34 19 13 10 3 3 104

Appendix 5. Summary of Results for Group Manager from Occupational Guidelines Questionnaire
2A-29
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Equipment usedFire-protective PersonnelProtective Equipment 64 15 13 1 3 3 1 1 104
Self-Contained Breathing Apparatus 35 22 22 12 7 3 1 2 104
Extended Duration Breathing Apparatus 7 0 13 27 18 36 6 5 101
Vibrating equipment 8 1 14 30 24 23 4 4 104
Computer 51 24 15 4 1 5 1 1 104
Telephone 54 25 16 0 0 5 1 1 104
Hand-held radio 37 26 26 6 4 2 1 2 104
Table 6: Near Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
BA control board-Old style MK 1 Read clock 34 66 2 2 105
BA control board-Old style MK 1 Graduations & cylinder pressure 36 64 2 2 105
BA tag Read tag 46 54 2 2 105
BA control board-New style MK 2 Read clock 43 57 2 2 105
BA control board-New style MK 2 Dial calculator 41 59 2 2 105
BA tag MK 2 Read tag 38 62 2 2 105
BA main control board Read clock 65 35 1 1 105
BA main control board Read 68 32 1 1 105
Sabre centurion Read BA graduations 23 77 2 2 105
Sabre centurion Read needle position 22 78 2 2 105
Siebe Gorman Read BA graduations 9 91 2 2 105
Siebe Gorman Read needle position 11 89 2 2 105
Drager Read BA graduations 29 71 2 2 105
Drager Read needle position 31 69 2 2 105
Philips PFX Handheld radio Read channel selector 75 25 1 1 105
Philips PFX Handheld radio Read numbered channel selector 74 26 1 1 105
BA log book Handwritten 48 52 2 2 105
Universal airline pack (Drager) BA supply BA cylinder gauge 12 88 2 2 105
Low pressure air bags Air pressure gauge 13 87 2 2 105
High pressure air bag Read graduations on console 16 84 2 2 105
High pressure air bag Needle position 14 86 2 2 105
Hurst high pressure lift bags Needle position 13 87 2 2 105
Microvent resuscitation equipment Read scale 11 89 2 2 105
Carmichael Godiva appliance Pressure gauge numbers 12 88 2 2 105
Saxon Volvo appliance pump Pressure gauge numbers 13 87 2 2 105
Dennis appliance pump Pressure gauge numbers 22 78 2 2 105
Read turnout sheet 39 61 2 2 105
Read dosimeter 54 46 1 1 105
Read survey meter 47 53 2 2 105
Read computer VDU 90 10 1 1 105
Read general paperwork 88 12 1 1 105
Read pager 80 20 1 1 105
Read mobile phone text 84 16 1 1 105
Read fire control panels 58 42 1 1 105
Read maps 90 10 1 1 105
Read fire extinguishers 37 63 2 2 105
Read plan inspections 59 41 1 1 105
Inspect premises 50 50 1 1 105
Read scale ruler 35 65 2 2 105
Read sound meter 27 73 2 2 105
Read light meter 24 76 2 2 105

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-30
Table 7: Distance Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
Street names White letters on a blue background 90 10 1 1 105
House numbers Copper figures on a blue background 77 23 1 1 105
House numbers White figures on a red background 78 22 1 1 105
Retail shop numbers Gold figures on a dark green background 75 25 1 1 105
House numbers Grey figures on a white background 77 23 1 1 105
Corporate building numbers Black figure on a silver background 79 21 1 1 105
Street names Black letters on a white background 90 10 1 1 105
House numbers Gold figures on a black background 78 22 1 1 105
House numbers Handpainted black figures on a white background 80 20 1 1 105
House numbers Gold figures on a black background 77 23 1 1 105
House numbers Black figures on a white background 81 19 1 1 105
Carmichael Godiva appliance pump Pressure gauge needle at rear of appliance 12 88 2 2 105
Carmichael Godiva appliance Measuring water in tank 10 90 2 2 105
Saxon Volvo appliance pump Pressure gauge needle at rear of appliance 11 89 2 2 105
Dennis appliance pump Pressure gauge needle at rear of appliance 17 83 2 2 105
Stop sign Road traffic signs 95 5 1 1 105
Give way sign Road traffic signs 96 4 1 1 105
One way street sign Road traffic signs 96 4 1 1 105
Chemical warning sign As EC Directive 92/58/EEC Hazardous substances 87 13 1 1 105
Vehicle signs Break lights/indicators on vehicles 93 7 1 1 105
Fire safety signs 84 16 1 1 105
Exit signs 85 15 1 1 105
Table 8: Hearing Tasks that are a requirement for role
Description Yes(1) No (2) Mode Median N
Distress signal unit 85 15 1 1 105
Warning whistle 85 15 1 1 105
Radio 95 5 1 1 105
Fireground orders 93 7 1 1 105
Evacuation signals/alarms 94 6 1 1 105
Telephone 96 4 1 1 105
Traffic 87 13 1 1 105
Vibraphone 30 70 2 2 105
Pager 86 14 1 1 105
Normal verbal communication with little background noise 97 3 1 1 105
Normal verbal communication with background noise 96 4 1 1 105
Hand clapping 62 38 1 1 105
Cries of help 79 21 1 1 105
Table 9: Other senses that are a requirement for role
Description Yes(1) No (2) Mode Median N
Touch 78 22 1 1 105
Smell 85 15 1 1 105
Taste 29 71 2 2 105

2A-31
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Sprinting 78 10 6 6 0 0 1 1 69
Running 57 10 20 7 4 1 1 1 69
Jogging 45 13 27 8 4 3 1 2 71
Walking 1 1 1 5 10 81 6 6 77
Climbing stairs 0 0 3 3 4 91 6 6 77
Climbing ladders 22 60 16 0 0 1 2 2 73
Crawling 51 41 5 1 1 0 1 1 74
Jumping 60 30 7 3 0 0 1 1 73
Hammering 78 8 11 3 0 0 1 1 73
Digging 79 12 8 0 0 0 1 1 73
Strength tasksLifting more than 5 kg or 11 pounds 18 12 25 13 16 16 3 3 68
Lifting more than 10 kg or 22 pounds 27 14 31 16 9 3 3 3 70
Lifting more than 20 kg or 44 pounds 37 34 16 9 3 0 1 2 67
Lifting more than 40 kg or 88 pounds 62 21 11 3 2 2 1 1 66
Carrying more than 5 kg or 11 pounds 29 16 16 13 17 10 1 3 70
Carrying more than 10 kg or 22 pounds 33 22 28 16 1 0 1 2 69
Carrying more than 20 kg or 44 pounds 41 33 23 1 1 0 1 2 69
Carrying more than 40 kg or 88 pounds 66 22 7 3 1 0 1 1 67
Pushing/pulling more than 5 kg or 11 pounds 40 26 13 10 6 4 1 2 68
Pushing/pulling more than 10 kg or 22 pounds 42 29 16 6 6 1 1 2 69
Pushing/pulling more than 20 kg or 44 pounds 51 35 7 4 1 0 1 1 68
Pushing/pulling more than 40 kg or 88 pounds 68 25 4 1 1 0 1 1 69
Static posturesStanding 0 0 0 0 12 88 6 6 77
Sitting 1 0 1 4 1 92 6 6 77
Squatting 25 11 22 21 13 8 1 3 72
Kneeling 28 16 23 18 11 4 1 3 74
Lying down 66 15 4 1 7 6 1 1 71
Table 1: Respondents’ Details
Age Bracket 18-19(1) 20-29(2) 30-39(3) 40-49(4) 50+(5) Mode Median N0 0 4 71 25 4 4 77
Years of Service 0-4 (1) 5-9 (2) 10-14(3) 15-19(4) 20-24(5) 25+(6) Mode Median N0 0 1 16 24 59 6 6 76
Gender Male Female Mode Median N100 0 1 1 77
Employment Status Fulltime(1) Retained(2) Mode Median N100 0 1 1 77
Appendix 6. Summary of Results for Area Managerfrom Occupational Guidelines QuestionnaireNote: Results are displayed as a percentage of the total responses for each role, and as the mode, median and total number (N) ofrespondents for the role

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-32
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time) (continued)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Dynamic flexibility requirementsBending at waist 4 0 4 15 26 51 6 6 74
Reaching 4 1 3 15 32 45 6 5 73
Stooping 7 4 4 21 28 36 6 5 72
Turning/twisting 5 0 4 11 32 48 6 5 73
Object activitiesCatching 63 11 11 12 3 0 1 1 73
Throwing 60 15 10 13 3 0 1 1 72
Fine dexterity(eg writing, assembling equipment) 3 1 0 0 1 95 6 6 77
Foot control (eg driving) 1 1 0 0 4 94 6 6 77
Table 3: Importance respondents considered these activities to be to the effective performanceof their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Sprinting 0 3 7 20 27 43 6 5 74
Running 0 4 21 26 25 24 4 4 76
Jogging 3 5 16 38 21 16 4 4 73
Walking 45 21 27 3 1 3 1 2 77
Climbing stairs 35 22 26 9 4 4 1 2 77
Climbing ladders 9 13 24 28 17 9 4 4 76
Crawling 4 5 19 33 23 16 4 4 75
Jumping 1 3 15 31 33 17 5 5 75
Hammering 0 1 5 24 43 26 5 5 74
Digging 0 1 7 25 40 27 5 5 75
Strength tasksLifting more than 5 kg or 11 pounds 8 5 33 25 19 9 3 4 75
Lifting more than 10 kg or 22 pounds 4 5 32 30 16 13 3 4 76
Lifting more than 20 kg or 44 pounds 4 1 27 33 19 16 4 4 75
Lifting more than 40 kg or 88 pounds 1 0 16 34 30 19 4 4 74
Carrying more than 5 kg or 11 pounds 9 5 28 26 16 15 3 4 74
Carrying more than 10 kg or 22 pounds 5 4 29 32 15 15 4 4 75
Carrying more than 20 kg or 44 pounds 3 3 21 35 23 16 4 4 75
Carrying more than 40 kg or 88 pounds 0 1 17 29 33 19 5 5 75
Pushing/pulling more than5 kg or 11 pounds 5 4 28 27 16 20 3 4 75
Pushing/pulling more than10 kg or 22 pounds 4 1 24 35 17 19 4 4 75
Pushing/pulling more than20 kg or 44 pounds 1 4 16 35 25 19 4 4 75
Pushing/pulling more than40 kg or 88 pounds 0 3 15 28 33 21 5 5 75
Static posturesStanding 39 26 23 8 3 1 1 2 77
Sitting 40 29 19 8 3 1 1 2 77
Squatting 5 4 35 33 12 11 3 4 75
Kneeling 7 3 29 33 16 12 4 4 75
Lying down 4 3 13 27 25 28 6 5 75

Appendix 6. Summary of Results for Area Manager from Occupational Guidelines Questionnaire
2A-33
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Handling hoses 48 48 4 0 0 0 1 2 77
Handling unconscious casualties 62 34 4 0 0 0 1 1 77
Handling ladders 60 36 4 0 0 0 1 1 77
Operating cutting equipment 73 25 3 0 0 0 1 1 77
Driving vehicles 3 1 0 1 8 87 6 6 77
Climbing ladders 32 53 15 0 0 0 2 2 75
Dealing with traumatised victims 30 43 25 1 0 0 2 2 76
Dealing with traumatised others (eg relatives, public) 15 54 28 3 0 0 2 2 74
Addressing groups of people 0 1 14 45 24 16 4 4 76
Filling in forms or completing paperwork 0 3 1 0 5 91 6 6 77
Making critical decisions quickly 0 1 16 14 22 46 6 5 76
Dealing with the media 0 8 49 30 8 5 3 3 76
Working on a computer 0 1 0 0 0 99 6 6 77
Communicating over the telephone 0 1 0 0 1 97 6 6 77
Environments encounteredFire compartment temperatures above 100˚C 59 39 1 0 0 0 1 1 76
Elevated temperatures (30-100˚C) 37 50 13 0 0 0 2 2 76
Freezing temperatures (sub-zero) 33 57 11 0 0 0 2 2 76
Dust 34 44 18 4 0 0 2 2 77
Overcrowding 40 38 19 3 0 0 1 2 77
Open spaces 20 35 19 12 7 8 2 2 75
Height 19 55 24 3 0 0 2 2 75
Enclosed spaces 27 56 14 3 0 0 2 2 77
Total darkness 31 58 9 0 1 0 2 2 77
Partial darkness 17 49 26 5 3 0 2 2 77
Working in water 70 27 3 0 0 0 1 1 77
Working under water 95 5 0 0 0 0 1 1 76
Handling hazardous substances 58 34 8 0 0 0 1 1 77
Smoke 23 51 21 5 0 0 2 2 77
High humidity 34 53 12 1 0 0 2 2 76
Table 3: Importance respondents considered these activities to be to the effective performanceof their role? (continued)
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Dynamic flexibility requirementsBending at waist 25 25 29 14 4 4 3 3 77
Reaching 22 22 34 13 4 5 3 3 77
Stooping 18 20 36 14 7 5 3 3 76
Turning/twisting 25 21 32 14 4 4 3 3 77
Object activitiesCatching 4 1 11 36 19 28 4 4 74
Throwing 5 3 12 30 20 30 6 5 74
Fine dexterity(eg writing, assembling equipment) 53 24 14 4 1 4 1 1 76
Foot control (eg driving) 62 16 16 1 1 4 1 1 76

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-34
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time) (continued)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Equipment usedFire-protective PersonnelProtective Equipment 4 14 57 25 0 0 3 3 76
Self-Contained Breathing Apparatus 31 68 1 0 0 0 2 2 77
Extended Duration Breathing Apparatus 94 6 0 0 0 0 1 1 77
Vibrating equipment 84 16 0 0 0 0 1 1 77
Computer 0 0 0 0 1 99 6 6 77
Telephone 0 0 0 0 0 100 6 6 77
Hand-held radio 3 8 45 19 9 16 3 3 77
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Handling hoses 3 6 6 30 27 27 4 5 77
Handling unconscious casualties 4 9 23 18 23 22 5 4 77
Handling ladders 3 9 14 26 23 25 4 4 77
Operating cutting equipment 8 5 12 24 28 24 5 5 76
Driving vehicles 57 26 4 4 4 5 1 1 77
Climbing ladders 4 16 19 30 14 17 4 4 77
Dealing with traumatised victims 8 23 39 18 6 5 3 3 77
Dealing with traumatised others (eg relatives, public) 12 29 43 8 5 4 3 3 77
Addressing groups of people 32 53 13 0 0 1 2 2 77
Filling in forms or completing paperwork 27 48 19 4 0 1 2 2 77
Making critical decisions quickly 52 38 9 1 0 0 1 1 77
Dealing with the media 20 49 24 7 0 1 2 2 76
Working on a computer 44 38 16 1 0 1 1 2 77
Communicating over the telephone 44 39 14 1 0 1 1 2 77
Environments encounteredFire compartment temperatures above 100˚C 5 14 21 18 18 22 6 4 76
Elevated temperatures (30-100˚C) 5 13 25 21 21 14 3 4 76
Freezing temperatures (sub-zero) 4 12 25 25 22 12 3 4 76
Dust 4 10 25 26 22 13 4 4 77
Overcrowding 3 12 23 30 21 12 4 4 77
Open spaces 4 11 29 25 18 13 3 4 76
Height 5 18 29 20 14 13 3 3 76
Enclosed spaces 5 17 27 23 14 13 3 4 77
Total darkness 6 12 30 25 13 14 3 4 77
Partial darkness 9 10 34 21 13 13 3 3 77
Working in water 4 9 26 22 19 19 3 4 77
Working under water 3 4 13 16 25 39 6 5 76
Handling hazardous substances 5 10 27 17 17 23 3 4 77
Smoke 8 14 30 19 14 14 3 3 77
High humidity 4 16 27 23 16 14 3 4 77

Appendix 6. Summary of Results for Area Manager from Occupational Guidelines Questionnaire
2A-35
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Equipment usedFire-protective PersonnelProtective Equipment 53 22 18 0 0 6 1 1 77
Self-Contained Breathing Apparatus 22 31 17 14 4 12 2 2 77
Extended Duration Breathing Apparatus 1 6 9 14 22 47 6 5 77
Vibrating equipment 3 8 11 20 24 36 6 5 76
Computer 51 30 14 4 0 1 1 1 77
Telephone 49 34 16 0 0 1 1 2 77
Hand-held radio 35 34 22 5 0 4 1 2 77
Table 6: Near Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
BA control board-Old style MK 1 Read clock 19 81 2 2 77
BA control board-Old style MK 1 Graduations & cylinder pressure 17 83 2 2 77
BA tag Read tag 29 71 2 2 77
BA control board-New style MK 2 Read clock 31 69 2 2 77
BA control board-New style MK 2 Dial calculator 30 70 2 2 77
BA tag MK 2 Read tag 27 73 2 2 77
BA main control board Read clock 43 57 2 2 77
BA main control board Read 44 56 2 2 77
Sabre centurion Read BA graduations 17 83 2 2 77
Sabre centurion Read needle position 17 83 2 2 77
Siebe Gorman Read BA graduations 6 94 2 2 77
Siebe Gorman Read needle position 8 92 2 2 77
Drager Read BA graduations 26 74 2 2 77
Drager Read needle position 23 77 2 2 77
Philips PFX Handheld radio Read channel selector 53 47 1 1 77
Philips PFX Handheld radio Read numbered channel selector 53 47 1 1 77
BA log book Handwritten 35 65 2 2 77
Universal airline pack (Drager) BA supply BA cylinder gauge 10 90 2 2 77
Low pressure air bags Air pressure gauge 12 88 2 2 77
High pressure air bag Read graduations on console 13 87 2 2 77
High pressure air bag Needle position 13 87 2 2 77
Hurst high pressure lift bags Needle position 13 87 2 2 77
Microvent resuscitation equipment Read scale 6 94 2 2 77
Carmichael Godiva appliance Pressure gauge numbers 8 92 2 2 77
Saxon Volvo appliance pump Pressure gauge numbers 10 90 2 2 77
Dennis appliance pump Pressure gauge numbers 14 86 2 2 77
Read turnout sheet 25 75 2 2 77
Read dosimeter 32 68 2 2 77
Read survey meter 30 70 2 2 77
Read computer VDU 70 30 1 1 77
Read general paperwork 69 31 1 1 77
Read pager 68 32 1 1 77
Read mobile phone text 73 27 1 1 77
Read fire control panels 35 65 2 2 77
Read maps 77 23 1 1 77
Read fire extinguishers 25 75 2 2 77
Read plan inspections 45 55 2 2 77
Inspect premises 32 68 2 2 77
Read scale ruler 23 77 2 2 77
Read sound meter 14 86 2 2 77
Read light meter 13 87 2 2 77

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-36
Table 7: Distance Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
Street names White letters on a blue background 75 25 1 1 77
House numbers Copper figures on a blue background 61 39 1 1 77
House numbers White figures on a red background 61 39 1 1 77
Retail shop numbers Gold figures on a dark green background 57 43 1 1 77
House numbers Grey figures on a white background 58 42 1 1 77
Corporate building numbers Black figure on a silver background 60 40 1 1 77
Street names Black letters on a white background 69 31 1 1 77
House numbers Gold figures on a black background 61 39 1 1 77
House numbers Handpainted black figures on a white background 62 38 1 1 77
House numbers Gold figures on a black background 60 40 1 1 77
House numbers Black figures on a white background 65 35 1 1 77
Carmichael Godiva appliance pump Pressure gauge needle at rear of appliance 14 86 2 2 77
Carmichael Godiva appliance Measuring water in tank 12 88 2 2 77
Saxon Volvo appliance pump Pressure gauge needle at rear of appliance 8 92 2 2 77
Dennis appliance pump Pressure gauge needle at rear of appliance 18 82 2 2 77
Stop sign Road traffic signs 91 9 1 1 77
Give way sign Road traffic signs 92 8 1 1 77
One way street sign Road traffic signs 90 10 1 1 77
Chemical warning sign As EC Directive 92/58/EEC Hazardous substances 84 16 1 1 77
Vehicle signs Break lights/indicators on vehicles 91 9 1 1 77
Fire safety signs 75 25 1 1 77
Exit signs 74 26 1 1 77
Table 8: Hearing Tasks that are a requirement for role
Description Yes(1) No (2) Mode Median N
Distress signal unit 76 24 1 1 77
Warning whistle 75 25 1 1 77
Radio 95 5 1 1 77
Fireground orders 88 12 1 1 77
Evacuation signals/alarms 88 12 1 1 77
Telephone 97 3 1 1 77
Traffic 87 13 1 1 77
Vibraphone 25 75 2 2 77
Pager 86 14 1 1 77
Normal verbal communication with little background noise 95 5 1 1 77
Normal verbal communication with background noise 94 6 1 1 77
Hand clapping 55 45 1 1 77
Cries of help 64 36 1 1 77
Table 9: Other senses that are a requirement for role
Description Yes(1) No (2) Mode Median N
Touch 77 23 1 1 77
Smell 73 27 1 1 77
Taste 31 69 2 2 77

2A-37
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Sprinting 75 16 4 2 4 0 1 1 55
Running 57 20 9 11 4 0 1 1 56
Jogging 52 20 7 13 7 0 1 1 54
Walking 2 2 0 9 11 77 6 6 57
Climbing stairs 2 2 4 0 11 82 6 6 57
Climbing ladders 44 41 9 4 0 2 1 2 54
Crawling 65 31 4 0 0 0 1 1 55
Jumping 73 16 9 0 0 2 1 1 56
Hammering 79 9 13 0 0 0 1 1 56
Digging 78 4 11 7 0 0 1 1 55
Strength tasksLifting more than 5 kg or 11 pounds 20 7 25 24 15 9 3 3 55
Lifting more than 10 kg or 22 pounds 39 15 19 20 7 0 1 2 54
Lifting more than 20 kg or 44 pounds 43 20 16 18 4 0 1 2 56
Lifting more than 40 kg or 88 pounds 64 15 9 11 2 0 1 1 55
Carrying more than 5 kg or 11 pounds 24 11 22 24 11 9 1 3 55
Carrying more than 10 kg or 22 pounds 38 15 20 20 5 2 1 2 55
Carrying more than 20 kg or 44 pounds 52 15 17 15 0 2 1 1 54
Carrying more than 40 kg or 88 pounds 73 13 5 7 0 2 1 1 55
Pushing/pulling more than 5 kg or 11 pounds 53 7 16 16 4 4 1 1 55
Pushing/pulling more than 10 kg or 22 pounds 53 11 20 15 2 0 1 1 55
Pushing/pulling more than 20 kg or 44 pounds 58 20 13 9 0 0 1 1 55
Pushing/pulling more than 40 kg or 88 pounds 73 15 5 7 0 0 1 1 55
Static posturesStanding 2 0 0 0 4 95 6 6 57
Sitting 5 4 0 2 0 89 6 6 57
Squatting 29 11 16 18 15 11 1 3 55
Kneeling 30 14 18 20 13 5 1 3 56
Lying down 67 4 5 0 18 5 1 1 55
Table 1: Respondents’ Details
Age Bracket 18-19(1) 20-29(2) 30-39(3) 40-49(4) 50+(5) Mode Median N0 0 3 55 41 4 4 58
Years of Service 0-4 (1) 5-9 (2) 10-14(3) 15-19(4) 20-24(5) 25+(6) Mode Median N0 0 0 4 19 77 6 6 57
Gender Male Female Mode Median N100 0 1 1 58
Employment Status Fulltime(1) Retained(2) Mode Median N100 0 1 1 57
Appendix 7. Summary of Results for Brigade Managerfrom Occupational Guidelines QuestionnaireNote: Results are displayed as a percentage of the total responses for each role, and as the mode, median and total number (N) ofrespondents for the role

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-38
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time) (continued)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Dynamic flexibility requirementsBending at waist 5 0 11 11 14 59 6 6 56
Reaching 9 0 7 20 11 54 6 6 56
Stooping 11 4 7 9 24 44 6 5 54
Turning/twisting 7 0 6 11 15 61 6 6 54
Object activitiesCatching 56 16 11 13 2 2 1 1 55
Throwing 56 15 11 16 0 2 1 1 55
Fine dexterity(eg writing, assembling equipment) 4 0 0 0 0 96 6 6 56
Foot control (eg driving) 0 0 0 0 5 95 6 6 56
Table 3: Importance respondents considered these activities to be to the effective performanceof their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Sprinting 0 0 9 18 32 42 6 5 57
Running 0 0 11 23 35 32 5 5 57
Jogging 0 0 26 19 26 28 6 5 57
Walking 40 21 19 5 5 9 1 2 57
Climbing stairs 33 23 19 9 9 7 1 2 57
Climbing ladders 2 2 14 34 23 25 4 4 56
Crawling 2 0 4 29 32 34 6 5 56
Jumping 2 0 7 25 27 39 6 5 56
Hammering 2 0 0 21 27 50 6 6 56
Digging 0 0 2 23 23 52 6 6 56
Strength tasksLifting more than 5 kg or 11 pounds 7 9 26 16 18 25 3 4 57
Lifting more than 10 kg or 22 pounds 4 11 14 23 21 28 6 4 57
Lifting more than 20 kg or 44 pounds 2 4 14 28 23 30 6 5 57
Lifting more than 40 kg or 88 pounds 0 0 9 30 32 30 5 5 57
Carrying more than 5 kg or 11 pounds 9 7 16 19 21 28 6 4 57
Carrying more than 10 kg or 22 pounds 7 7 11 23 23 30 6 5 57
Carrying more than 20 kg or 44 pounds 2 4 12 26 26 30 6 5 57
Carrying more than 40 kg or 88 pounds 0 0 9 26 33 32 5 5 57
Pushing/pulling more than 5 kg or 11 pounds 7 5 9 30 18 32 6 4 57
Pushing/pulling more than 10 kg or 22 pounds 5 7 5 26 25 32 6 5 57
Pushing/pulling more than 20 kg or 44 pounds 2 5 7 26 28 32 6 5 57
Pushing/pulling more than 40 kg or 88 pounds 0 0 5 25 38 32 5 5 56
Static posturesStanding 45 21 20 4 7 4 1 2 56
Sitting 46 19 18 5 9 4 1 2 57
Squatting 4 4 14 37 19 23 4 4 57
Kneeling 4 2 16 34 21 23 4 4 56
Lying down 2 0 5 21 26 46 6 5 57

Appendix 7. Summary of Results for Brigade Manager from Occupational Guidelines Questionnaire
2A-39
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Handling hoses 73 25 2 0 0 0 1 1 56
Handling unconscious casualties 79 21 0 0 0 0 1 1 56
Handling ladders 77 20 4 0 0 0 1 1 56
Operating cutting equipment 82 15 4 0 0 0 1 1 56
Driving vehicles 4 2 2 2 7 84 6 6 57
Climbing ladders 61 28 9 0 0 2 1 1 54
Dealing with traumatised victims 68 30 2 0 0 0 1 1 56
Dealing with traumatised others (eg relatives, public) 36 45 9 2 5 4 2 2 56
Addressing groups of people 0 0 9 30 40 21 5 5 57
Filling in forms or completing paperwork 0 0 2 2 9 88 6 6 58
Making critical decisions quickly 0 3 2 16 17 62 6 6 58
Dealing with the media 2 5 28 40 16 9 4 4 57
Working on a computer 0 0 0 0 2 98 6 6 58
Communicating over the telephone 0 0 0 0 0 100 6 6 58
Environments encounteredFire compartment temperatures above 100˚C 61 37 2 0 0 0 1 1 57
Elevated temperatures (30-100˚C) 45 47 9 0 0 0 2 2 58
Freezing temperatures (sub-zero) 43 48 9 0 0 0 2 2 58
Dust 49 39 11 0 0 2 1 2 57
Overcrowding 50 24 16 10 0 0 1 2 58
Open spaces 26 34 19 2 10 9 2 2 58
Height 29 50 14 7 0 0 2 2 58
Enclosed spaces 29 53 10 3 2 2 2 2 58
Total darkness 41 47 9 2 2 0 2 2 58
Partial darkness 33 48 9 10 0 0 2 2 58
Working in water 88 12 0 0 0 0 1 1 58
Working under water 97 3 0 0 0 0 1 1 58
Handling hazardous substances 81 12 7 0 0 0 1 1 58
Smoke 43 40 17 0 0 0 1 2 58
High humidity 60 29 10 0 0 0 1 1 58
Table 3: Importance respondents considered these activities to be to the effective performanceof their role? (continued)
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Dynamic flexibility requirementsBending at waist 18 16 20 21 16 9 4 3 56
Reaching 18 14 25 18 18 9 3 3 57
Stooping 16 9 25 19 23 9 3 4 57
Turning/twisting 18 14 18 26 16 9 4 4 57
Object activitiesCatching 0 2 9 20 32 38 6 5 56
Throwing 0 4 13 14 32 38 6 5 56
Fine dexterity (eg writing, assembling equipment) 47 30 9 5 4 5 1 2 57
Foot control (eg driving) 61 18 9 4 5 4 1 1 57

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-40
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time) (continued)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Equipment usedFire-protective PersonnelProtective Equipment 13 40 45 2 0 0 3 2 55
Self-Contained Breathing Apparatus 49 47 2 2 0 0 1 2 57
Extended Duration Breathing Apparatus 95 2 2 2 0 0 1 1 57
Vibrating equipment 86 9 0 0 2 3 1 1 58
Computer 0 0 3 0 0 97 6 6 58
Telephone 0 0 2 0 2 96 6 6 57
Hand-held radio 12 28 49 4 4 4 3 3 57
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Handling hoses 3 3 10 5 33 45 6 5 58
Handling unconscious casualties 9 2 9 10 26 45 6 5 58
Handling ladders 3 3 10 10 28 45 6 5 58
Operating cutting equipment 3 5 12 5 29 45 6 5 58
Driving vehicles 50 16 19 3 7 5 1 2 58
Climbing ladders 7 4 16 12 25 37 6 5 57
Dealing with traumatised victims 7 7 19 9 26 33 6 5 58
Dealing with traumatised others (eg relatives, public) 7 21 25 11 16 21 3 3 57
Addressing groups of people 45 38 14 2 0 2 1 2 58
Filling in forms or completing paperwork 40 43 14 3 0 0 2 2 58
Making critical decisions quickly 67 26 7 0 0 0 1 1 57
Dealing with the media 38 47 12 3 0 0 2 2 58
Working on a computer 47 32 19 2 0 0 1 2 57
Communicating over the telephone 55 34 10 0 0 0 1 1 58
Environments encounteredFire compartment temperatures above 100˚C 11 2 7 18 23 39 6 5 56
Elevated temperatures (30-100˚C) 5 5 9 20 20 41 6 5 56
Freezing temperatures (sub-zero) 4 4 9 23 23 38 6 5 56
Dust 2 5 7 23 21 41 6 5 56
Overcrowding 0 7 13 20 23 38 6 5 56
Open spaces 2 7 11 20 30 30 5 5 56
Height 7 11 9 16 25 32 6 5 56
Enclosed spaces 9 2 16 20 23 30 6 5 56
Total darkness 7 7 13 14 23 36 6 5 56
Partial darkness 7 5 16 14 23 34 6 5 56
Working in water 4 7 7 15 24 44 6 5 55
Working under water 5 0 2 18 25 50 6 6 56
Handling hazardous substances 5 2 7 18 25 43 6 5 56
Smoke 5 4 14 18 25 34 6 5 56
High humidity 4 9 7 16 27 38 6 5 56

Appendix 7. Summary of Results for Brigade Manager from Occupational Guidelines Questionnaire
2A-41
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Equipment usedFire-protective PersonnelProtective Equipment 38 18 18 16 4 5 1 2 55
Self-Contained Breathing Apparatus 15 13 11 24 11 27 6 4 55
Extended Duration Breathing Apparatus 4 2 15 20 13 47 6 5 55
Vibrating equipment 4 4 9 18 13 53 6 6 55
Computer 54 27 9 4 2 5 1 1 56
Telephone 57 23 13 0 2 5 1 1 56
Hand-held radio 18 21 30 14 9 7 3 3 56
Table 6: Near Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
BA control board-Old style MK 1 Read clock 16 84 2 2 58
BA control board-Old style MK 1 Graduations & cylinder pressure 16 84 2 2 58
BA tag Read tag 19 81 2 2 58
BA control board-New style MK 2 Read clock 14 86 2 2 58
BA control board-New style MK 2 Dial calculator 14 86 2 2 58
BA tag MK 2 Read tag 14 86 2 2 58
BA main control board Read clock 14 86 2 2 58
BA main control board Read 21 79 2 2 58
Sabre centurion Read BA graduations 9 91 2 2 58
Sabre centurion Read needle position 10 90 2 2 58
Siebe Gorman Read BA graduations 5 95 2 2 58
Siebe Gorman Read needle position 7 93 2 2 58
Drager Read BA graduations 17 83 2 2 58
Drager Read needle position 17 83 2 2 58
Philips PFX Handheld radio Read channel selector 48 52 2 2 58
Philips PFX Handheld radio Read numbered channel selector 43 57 2 2 58
BA log book Handwritten 22 78 2 2 58
Universal airline pack (Drager) BA supply BA cylinder gauge 9 91 2 2 58
Low pressure air bags Air pressure gauge 7 93 2 2 58
High pressure air bag Read graduations on console 7 93 2 2 58
High pressure air bag Needle position 7 93 2 2 58
Hurst high pressure lift bags Needle position 7 93 2 2 58
Microvent resuscitation equipment Read scale 3 97 2 2 58
Carmichael Godiva appliance Pressure gauge numbers 5 95 2 2 58
Saxon Volvo appliance pump Pressure gauge numbers 3 97 2 2 58
Dennis appliance pump Pressure gauge numbers 5 95 2 2 58
Read turnout sheet 21 79 2 2 58
Read dosimeter 24 76 2 2 58
Read survey meter 16 84 2 2 58
Read computer VDU 74 26 1 1 58
Read general paperwork 76 24 1 1 58
Read pager 69 31 1 1 58
Read mobile phone text 78 22 1 1 58
Read fire control panels 22 78 2 2 58
Read maps 72 28 1 1 58
Read fire extinguishers 10 90 2 2 58
Read plan inspections 36 64 2 2 58
Inspect premises 17 83 2 2 58
Read scale ruler 12 88 2 2 58
Read sound meter 5 95 2 2 58
Read light meter 5 95 2 2 58

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-42
Table 7: Distance Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
Street names White letters on a blue background 57 43 1 1 58
House numbers Copper figures on a blue background 43 57 2 2 58
House numbers White figures on a red background 43 57 2 2 58
Retail shop numbers Gold figures on a dark green background 36 64 2 2 58
House numbers Grey figures on a white background 43 57 2 2 58
Corporate building numbers Black figure on a silver background 45 55 2 2 58
Street names Black letters on a white background 55 45 1 1 58
House numbers Gold figures on a black background 38 62 2 2 58
House numbers Handpainted black figures on a white background 38 62 2 2 58
House numbers Gold figures on a black background 36 64 2 2 58
House numbers Black figures on a white background 40 60 2 2 58
Carmichael Godiva appliance pump Pressure gauge needle at rear of appliance 3 97 2 2 58
Carmichael Godiva appliance Measuring water in tank 5 95 2 2 58
Saxon Volvo appliance pump Pressure gauge needle at rear of appliance 3 97 2 2 58
Dennis appliance pump Pressure gauge needle at rear of appliance 10 90 2 2 58
Stop sign Road traffic signs 88 12 1 1 58
Give way sign Road traffic signs 90 10 1 1 58
One way street sign Road traffic signs 90 10 1 1 58
Chemical warning sign As EC Directive 92/58/EEC Hazardous substances 53 47 1 1 58
Vehicle signs Break lights/indicators on vehicles 86 14 1 1 58
Fire safety signs 60 40 1 1 58
Exit signs 62 38 1 1 58
Table 8: Hearing Tasks that are a requirement for role
Description Yes(1) No (2) Mode Median N
Distress signal unit 62 38 1 1 58
Warning whistle 59 41 1 1 58
Radio 81 19 1 1 58
Fireground orders 74 26 1 1 58
Evacuation signals/alarms 79 21 1 1 58
Telephone 100 0 1 1 58
Traffic 83 17 1 1 58
Vibraphone 17 83 2 2 58
Pager 86 14 1 1 58
Normal verbal communication with little background noise 88 12 1 1 58
Normal verbal communication with background noise 83 17 1 1 58
Hand clapping 43 57 2 2 58
Cries of help 59 41 1 1 58
Table 9: Other senses that are a requirement for role
Description Yes(1) No (2) Mode Median N
Touch 59 41 1 1 58
Smell 52 48 1 1 58
Taste 24 76 2 2 58

2A-43
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Sprinting 95 0 0 3 1 1 1 1 79
Running 83 3 4 9 0 1 1 1 78
Jogging 85 3 6 3 0 4 1 1 79
Walking 22 0 0 1 6 70 6 6 81
Climbing stairs 24 0 4 3 23 47 6 5 79
Climbing ladders 95 3 1 0 0 1 1 1 78
Crawling 95 3 1 1 0 0 1 1 79
Jumping 97 0 1 1 0 0 1 1 78
Hammering 99 0 1 0 0 0 1 1 78
Digging 97 1 1 0 0 0 1 1 76
Strength tasksLifting more than 5 kg or 11 pounds 76 3 8 9 5 0 1 1 80
Lifting more than 10 kg or 22 pounds 87 3 4 3 3 1 1 1 79
Lifting more than 20 kg or 44 pounds 95 1 3 1 0 0 1 1 78
Lifting more than 40 kg or 88 pounds 96 4 0 0 0 0 1 1 78
Carrying more than 5 kg or 11 pounds 81 4 8 5 3 0 1 1 79
Carrying more than 10 kg or 22 pounds 91 3 3 3 1 0 1 1 78
Carrying more than 20 kg or 44 pounds 96 1 3 0 0 0 1 1 78
Carrying more than 40 kg or 88 pounds 97 3 0 0 0 0 1 1 78
Pushing/pulling more than 5 kg or 11 pounds 90 1 3 5 1 0 1 1 79
Pushing/pulling more than 10 kg or 22 pounds 95 0 0 1 3 1 1 1 78
Pushing/pulling more than 20 kg or 44 pounds 99 1 0 0 0 0 1 1 78
Pushing/pulling more than 40 kg or 88 pounds 99 1 0 0 0 0 1 1 78
Static posturesStanding 18 0 0 0 5 77 6 6 82
Sitting 0 0 0 0 0 100 6 6 82
Squatting 70 1 3 4 12 11 1 1 76
Kneeling 74 1 4 8 8 5 1 1 77
Lying down 85 0 0 5 8 3 1 1 79
Table 1: Respondents’ Details
Age Bracket 18-19(1) 20-29(2) 30-39(3) 40-49(4) 50+(5) Mode Median N0 21 48 24 7 3 3 84
Years of Service 0-4 (1) 5-9 (2) 10-14(3) 15-19(4) 20-24(5) 25+(6) Mode Median N35 24 15 18 5 4 1 2 84
Gender Male Female Mode Median N10 90 2 2 84
Employment Status Fulltime(1) Retained(2) Mode Median N99 0 1 1 80
Appendix 8. Summary of Results for Control Operatorfrom Occupational Guidelines QuestionnaireNote: Results are displayed as a percentage of the total responses for each role, and as the mode, median and total number (N) ofrespondents for the role

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-44
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time) (continued)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Dynamic flexibility requirementsBending at waist 28 0 3 4 21 45 6 5 80
Reaching 23 0 1 5 16 55 6 6 80
Stooping 48 0 3 3 14 33 1 3 79
Turning/twisting 23 0 1 0 4 72 6 6 82
Object activitiesCatching 84 4 4 4 1 3 1 1 77
Throwing 85 4 4 4 1 3 1 1 78
Fine dexterity (eg writing, assembling equipment) 5 0 0 0 0 95 6 6 80
Foot control (eg driving) 19 6 6 4 3 63 6 6 80
Table 3: Importance respondents considered these activities to be to the effective performanceof their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Sprinting 4 3 1 0 8 85 6 6 79
Running 4 4 4 4 10 75 6 6 80
Jogging 4 3 3 4 8 80 6 6 79
Walking 11 11 22 12 11 33 6 4 82
Climbing stairs 9 9 14 15 15 38 6 5 79
Climbing ladders 1 0 0 0 3 96 6 6 79
Crawling 3 0 0 0 6 91 6 6 79
Jumping 3 0 0 1 6 90 6 6 79
Hammering 3 0 0 0 3 95 6 6 79
Digging 3 0 0 0 3 95 6 6 79
Strength tasksLifting more than 5 kg or 11 pounds 3 0 6 8 8 76 6 6 78
Lifting more than 10 kg or 22 pounds 3 0 3 1 10 83 6 6 78
Lifting more than 20 kg or 44 pounds 3 0 1 1 6 88 6 6 77
Lifting more than 40 kg or 88 pounds 3 0 0 1 6 90 6 6 77
Carrying more than 5 kg or 11 pounds 3 0 4 8 6 79 6 6 77
Carrying more than 10 kg or 22 pounds 3 0 1 1 9 86 6 6 77
Carrying more than 20 kg or 44 pounds 3 0 1 1 6 88 6 6 77
Carrying more than 40 kg or 88 pounds 3 0 0 1 6 90 6 6 77
Pushing/pulling more than 5 kg or 11 pounds 1 0 4 4 6 84 6 6 77
Pushing/pulling more than 10 kg or 22 pounds 4 0 0 1 6 88 6 6 77
Pushing/pulling more than 20 kg or 44 pounds 3 0 0 1 6 90 6 6 77
Pushing/pulling more than 40 kg or 88 pounds 3 0 0 1 7 89 6 6 76
Static posturesStanding 17 11 26 16 12 17 3 3 81
Sitting 62 16 14 1 1 6 1 1 81
Squatting 3 0 6 19 14 58 6 6 79
Kneeling 3 0 6 15 15 61 6 6 79
Lying down 3 1 1 10 10 75 6 6 79

Appendix 8. Summary of Results for Control Operator from Occupational Guidelines Questionnaire
2A-45
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Handling hoses 100 0 0 0 0 0 1 1 79
Handling unconscious casualties 100 0 0 0 0 0 1 1 79
Handling ladders 100 0 0 0 0 0 1 1 79
Operating cutting equipment 99 0 0 0 0 1 1 1 79
Driving vehicles 53 23 11 5 4 5 1 1 80
Climbing ladders 97 0 0 0 0 3 1 1 77
Dealing with traumatised victims 41 5 13 13 5 24 1 3 79
Dealing with traumatised others (eg relatives, public) 30 5 18 14 9 24 1 3 79
Addressing groups of people 41 27 19 5 1 8 1 2 79
Filling in forms or completing paperwork 0 0 2 5 11 82 6 6 83
Making critical decisions quickly 1 0 1 2 4 92 6 6 83
Dealing with the media 0 0 1 10 13 76 6 6 83
Working on a computer 0 0 0 0 0 100 6 6 83
Communicating over the telephone 0 0 0 0 0 100 6 6 83
Environments encounteredFire compartment temperatures above 100˚C 100 0 0 0 0 0 1 1 80
Elevated temperatures (30-100˚C) 100 0 0 0 0 0 1 1 80
Freezing temperatures (sub-zero) 100 0 0 0 0 0 1 1 80
Dust 89 0 0 1 0 10 1 1 81
Overcrowding 99 0 0 0 1 0 1 1 80
Open spaces 98 0 0 0 0 3 1 1 80
Height 100 0 0 0 0 0 1 1 80
Enclosed spaces 98 0 0 0 0 3 1 1 80
Total darkness 100 0 0 0 0 0 1 1 80
Partial darkness 99 0 0 1 0 0 1 1 80
Working in water 100 0 0 0 0 0 1 1 80
Working under water 100 0 0 0 0 0 1 1 80
Handling hazardous substances 99 0 1 0 0 0 1 1 80
Smoke 98 0 0 0 0 3 1 1 80
High humidity 99 0 0 0 0 1 1 1 80
Table 3: Importance respondents considered these activities to be to the effective performanceof their role? (continued)
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Dynamic flexibility requirementsBending at waist 11 14 17 20 14 25 6 4 81
Reaching 15 15 16 18 11 25 6 4 80
Stooping 8 3 13 26 15 36 6 5 78
Turning/twisting 14 20 23 14 4 26 6 3 81
Object activitiesCatching 1 0 0 9 10 80 6 6 79
Throwing 1 0 0 9 10 80 6 6 79
Fine dexterity (eg writing, assembling equipment) 66 17 6 0 0 11 1 1 82
Foot control (eg driving) 23 21 18 9 5 24 6 3 82

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-46
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time) (continued)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Equipment usedFire-protective Personnel Protective Equipment 100 0 0 0 0 0 1 1 79
Self-Contained Breathing Apparatus 100 0 0 0 0 0 1 1 80
Extended Duration Breathing Apparatus 100 0 0 0 0 0 1 1 80
Vibrating equipment 100 0 0 0 0 0 1 1 80
Computer 1 0 0 0 0 99 6 6 83
Telephone 0 0 0 0 0 100 6 6 83
Hand-held radio 48 6 17 11 1 16 1 2 81
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Handling hoses 1 0 0 0 0 99 6 6 81
Handling unconscious casualties 1 0 0 0 0 99 6 6 81
Handling ladders 1 0 0 0 0 99 6 6 81
Operating cutting equipment 1 0 0 1 0 98 6 6 81
Driving vehicles 5 2 12 13 4 63 6 6 82
Climbing ladders 4 1 0 0 0 95 6 6 81
Dealing with traumatised victims 31 18 9 0 0 43 6 3 80
Dealing with traumatised others (eg relatives, public) 37 18 13 1 0 30 1 2 82
Addressing groups of people 4 13 26 18 1 38 6 4 82
Filling in forms or completing paperwork 37 35 21 4 0 4 1 2 84
Making critical decisions quickly 70 18 8 0 0 4 1 1 84
Dealing with the media 21 25 42 6 4 2 3 3 84
Working on a computer 82 13 2 0 0 2 1 1 84
Communicating over the telephone 81 14 0 0 0 5 1 1 84
Environments encounteredFire compartment temperatures above 100˚C 3 0 0 0 0 97 6 6 78
Elevated temperatures (30-100˚C) 1 0 0 0 0 99 6 6 79
Freezing temperatures (sub-zero) 1 0 0 0 0 99 6 6 79
Dust 3 0 3 1 0 94 6 6 79
Overcrowding 3 0 1 0 0 96 6 6 79
Open spaces 1 0 0 1 1 96 6 6 79
Height 1 0 0 0 0 99 6 6 79
Enclosed spaces 1 0 0 0 0 99 6 6 79
Total darkness 1 0 0 0 0 99 6 6 79
Partial darkness 1 0 0 0 0 99 6 6 79
Working in water 1 0 0 0 0 99 6 6 79
Working under water 1 0 0 0 0 99 6 6 79
Handling hazardous substances 1 0 0 0 0 99 6 6 79
Smoke 1 0 1 0 0 97 6 6 79
High humidity 3 0 0 0 0 97 6 6 78

Appendix 8. Summary of Results for Control Operator from Occupational Guidelines Questionnaire
2A-47
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Equipment usedFire-protective PersonnelProtective Equipment 1 0 0 0 0 99 6 6 78
Self-Contained Breathing Apparatus 1 0 0 0 0 99 6 6 78
Extended Duration Breathing Apparatus 1 0 0 0 0 99 6 6 78
Vibrating equipment 3 0 0 1 0 96 6 6 77
Computer 84 12 1 0 0 2 1 1 83
Telephone 90 7 1 0 0 1 1 1 83
Hand-held radio 22 10 18 11 0 39 6 4 79
Table 6: Near Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
BA control board-Old style MK 1 Read clock 0 100 2 2 84
BA control board-Old style MK 1 Graduations & cylinder pressure 0 100 2 2 84
BA tag Read tag 0 100 2 2 84
BA control board-New style MK 2 Read clock 0 100 2 2 84
BA control board-New style MK 2 Dial calculator 0 100 2 2 84
BA tag MK 2 Read tag 0 100 2 2 84
BA main control board Read clock 0 100 2 2 84
BA main control board Read 0 100 2 2 84
Sabre centurion Read BA graduations 0 100 2 2 84
Sabre centurion Read needle position 0 100 2 2 84
Siebe Gorman Read BA graduations 0 100 2 2 84
Siebe Gorman Read needle position 0 100 2 2 84
Drager Read BA graduations 0 100 2 2 84
Drager Read needle position 1 99 2 2 84
Philips PFX Handheld radio Read channel selector 10 90 2 2 84
Philips PFX Handheld radio Read numbered channel selector 8 92 2 2 84
BA log book Handwritten 0 100 2 2 84
Universal airline pack (Drager) BA supply BA cylinder gauge 0 100 2 2 84
Low pressure air bags Air pressure gauge 0 100 2 2 84
High pressure air bag Read graduations on console 0 100 2 2 84
High pressure air bag Needle position 0 100 2 2 84
Hurst high pressure lift bags Needle position 0 100 2 2 84
Microvent resuscitation equipment Read scale 0 100 2 2 84
Carmichael Godiva appliance Pressure gauge numbers 0 100 2 2 84
Saxon Volvo appliance pump Pressure gauge numbers 0 100 2 2 84
Dennis appliance pump Pressure gauge numbers 0 100 2 2 84
Read turnout sheet 5 95 2 2 84
Read dosimeter 0 100 2 2 84
Read survey meter 1 99 2 2 84
Read computer VDU 54 46 1 1 84
Read general paperwork 54 46 1 1 84
Read pager 21 79 2 2 84
Read mobile phone text 29 71 2 2 84
Read fire control panels 30 70 2 2 84
Read maps 55 45 1 1 84
Read fire extinguishers 8 92 2 2 84
Read plan inspections 8 92 2 2 84
Inspect premises 0 100 2 2 84
Read scale ruler 4 96 2 2 84
Read sound meter 0 100 2 2 84
Read light meter 0 100 2 2 84

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-48
Table 7: Distance Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
Street names White letters on a blue background 6 94 2 2 84
House numbers Copper figures on a blue background 4 96 2 2 84
House numbers White figures on a red background 5 95 2 2 84
Retail shop numbers Gold figures on a dark green background 1 99 2 2 84
House numbers Grey figures on a white background 2 98 2 2 84
Corporate building numbers Black figure on a silver background 1 99 2 2 84
Street names Black letters on a white background 2 98 2 2 84
House numbers Gold figures on a black background 1 99 2 2 84
House numbers Handpainted black figures on a white background 1 99 2 2 84
House numbers Gold figures on a black background 1 99 2 2 84
House numbers Black figures on a white background 4 96 2 2 84
Carmichael Godiva appliance pump Pressure gauge needle at rear of appliance 0 100 2 2 84
Carmichael Godiva appliance Measuring water in tank 0 100 2 2 84
Saxon Volvo appliance pump Pressure gauge needle at rear of appliance 0 100 2 2 84
Dennis appliance pump Pressure gauge needle at rear of appliance 0 100 2 2 84
Stop sign Road traffic signs 8 92 2 2 84
Give way sign Road traffic signs 8 92 2 2 84
One way street sign Road traffic signs 8 92 2 2 84
Chemical warning sign As EC Directive 92/58/EEC Hazardous substances 0 100 2 2 84
Vehicle signs Break lights/indicators on vehicles 7 93 2 2 84
Fire safety signs 4 96 2 2 84
Exit signs 8 92 2 2 84
Table 8: Hearing Tasks that are a requirement for role
Description Yes(1) No (2) Mode Median N
Distress signal unit 0 100 2 2 84
Warning whistle 0 100 2 2 84
Radio 87 13 1 1 84
Fireground orders 7 93 2 2 84
Evacuation signals/alarms 27 73 2 2 84
Telephone 89 11 1 1 84
Traffic 7 93 2 2 84
Vibraphone 4 96 2 2 84
Pager 23 77 2 2 84
Normal verbal communication with little background noise 74 26 1 1 84
Normal verbal communication with background noise 79 21 1 1 84
Hand clapping 10 90 2 2 84
Cries of help 35 65 2 2 84
Table 9: Other senses that are a requirement for role
Description Yes(1) No (2) Mode Median N
Touch 43 57 2 2 84
Smell 1 99 2 2 84
Taste 0 100 2 2 84

2A-49
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Sprinting 93 2 2 4 0 0 1 1 57
Running 76 5 8 5 5 0 1 1 59
Jogging 90 0 5 0 3 2 1 1 58
Walking 8 0 2 0 8 82 6 6 61
Climbing stairs 5 0 3 3 34 55 6 6 62
Climbing ladders 95 4 0 0 2 0 1 1 57
Crawling 100 0 0 0 0 0 1 1 58
Jumping 98 0 2 0 0 0 1 1 58
Hammering 93 2 3 0 2 0 1 1 58
Digging 95 3 0 2 0 0 1 1 58
Strength tasksLifting more than 5 kg or 11 pounds 63 4 4 16 9 5 1 1 57
Lifting more than 10 kg or 22 pounds 84 5 2 7 0 2 1 1 56
Lifting more than 20 kg or 44 pounds 96 0 2 0 2 0 1 1 57
Lifting more than 40 kg or 88 pounds 98 0 0 2 0 0 1 1 56
Carrying more than 5 kg or 11 pounds 73 2 4 11 7 4 1 1 56
Carrying more than 10 kg or 22 pounds 89 4 2 4 0 2 1 1 54
Carrying more than 20 kg or 44 pounds 95 2 2 0 2 0 1 1 56
Carrying more than 40 kg or 88 pounds 98 0 0 2 0 0 1 1 54
Pushing/pulling more than 5 kg or 11 pounds 84 2 2 4 4 5 1 1 56
Pushing/pulling more than 10 kg or 22 pounds 91 4 0 2 2 2 1 1 56
Pushing/pulling more than 20 kg or 44 pounds 98 0 0 0 2 0 1 1 56
Pushing/pulling more than 40 kg or 88 pounds 98 0 0 2 0 0 1 1 56
Static posturesStanding 10 0 0 3 8 78 6 6 59
Sitting 6 0 2 0 0 92 6 6 63
Squatting 66 0 4 4 20 7 1 1 56
Kneeling 56 0 9 20 11 4 1 1 54
Lying down 79 0 2 5 7 7 1 1 57
Table 1: Respondents’ Details
Age Bracket 18-19(1) 20-29(2) 30-39(3) 40-49(4) 50+(5) Mode Median N0 6 38 44 13 4 4 64
Years of Service 0-4 (1) 5-9 (2) 10-14(3) 15-19(4) 20-24(5) 25+(6) Mode Median N5 25 16 32 11 11 4 4 63
Gender Male Female Mode Median N17 83 2 2 64
Employment Status Fulltime(1) Retained(2) Mode Median N100 0 1 1 63
Appendix 9. Summary of Results for Control Supervisorfrom Occupational Guidelines QuestionnaireNote: Results are displayed as a percentage of the total responses for each role, and as the mode, median and total number (N) ofrespondents for the role

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-50
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time) (continued)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Dynamic flexibility requirementsBending at waist 22 0 2 5 14 58 6 6 59
Reaching 15 0 0 7 10 69 6 6 61
Stooping 34 2 0 9 11 45 6 5 56
Turning/twisting 20 0 3 2 0 75 6 6 60
Object activitiesCatching 82 7 4 0 7 0 1 1 56
Throwing 84 5 2 0 9 0 1 1 56
Fine dexterity (eg writing, assembling equipment) 2 0 0 0 0 98 6 6 63
Foot control (eg driving) 15 3 5 2 8 67 6 6 60
Table 3: Importance respondents considered these activities to be to the effective performanceof their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Sprinting 2 3 2 2 8 83 6 6 59
Running 2 2 2 10 10 75 6 6 60
Jogging 3 2 3 9 9 74 6 6 58
Walking 28 16 28 11 5 11 1 3 61
Climbing stairs 24 10 23 15 10 19 1 3 62
Climbing ladders 2 0 0 3 5 90 6 6 58
Crawling 2 0 0 3 5 90 6 6 58
Jumping 2 0 0 3 5 90 6 6 59
Hammering 2 0 0 3 3 92 6 6 59
Digging 2 0 0 2 3 93 6 6 59
Strength tasksLifting more than 5 kg or 11 pounds 3 3 14 12 7 61 6 6 59
Lifting more than 10 kg or 22 pounds 2 2 2 5 10 79 6 6 58
Lifting more than 20 kg or 44 pounds 3 0 0 0 7 90 6 6 59
Lifting more than 40 kg or 88 pounds 2 0 0 0 7 91 6 6 58
Carrying more than 5 kg or 11 pounds 3 3 9 9 5 71 6 6 58
Carrying more than 10 kg or 22 pounds 2 2 2 5 9 81 6 6 58
Carrying more than 20 kg or 44 pounds 3 0 0 0 7 90 6 6 59
Carrying more than 40 kg or 88 pounds 2 0 0 0 7 91 6 6 58
Pushing/pulling more than 5 kg or 11 pounds 2 3 7 3 3 81 6 6 58
Pushing/pulling more than 10 kg or 22 pounds 2 5 2 0 7 84 6 6 58
Pushing/pulling more than 20 kg or 44 pounds 2 0 0 0 7 91 6 6 58
Pushing/pulling more than 40 kg or 88 pounds 2 0 0 0 7 91 6 6 58
Static posturesStanding 23 11 26 25 8 7 3 3 62
Sitting 68 19 6 0 2 5 1 1 63
Squatting 5 3 5 21 19 47 6 5 58
Kneeling 5 3 8 15 18 50 6 6 60
Lying down 3 3 2 7 19 66 6 6 59

Appendix 9. Summary of Results for Control Supervisor from Occupational Guidelines Questionnaire
2A-51
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Handling hoses 100 0 0 0 0 0 1 1 59
Handling unconscious casualties 100 0 0 0 0 0 1 1 59
Handling ladders 100 0 0 0 0 0 1 1 59
Operating cutting equipment 98 2 0 0 0 0 1 1 59
Driving vehicles 27 38 20 2 5 8 2 2 60
Climbing ladders 98 0 0 0 2 0 1 1 59
Dealing with traumatised victims 49 0 19 11 2 19 1 3 57
Dealing with traumatised others (eg relatives, public) 40 2 12 10 10 26 1 3 58
Addressing groups of people 13 30 28 13 7 8 2 3 60
Filling in forms or completing paperwork 0 0 5 6 6 83 6 6 63
Making critical decisions quickly 0 0 0 0 2 98 6 6 63
Dealing with the media 0 0 0 6 11 83 6 6 63
Working on a computer 0 0 0 0 2 98 6 6 63
Communicating over the telephone 0 0 0 0 0 100 6 6 62
Environments encounteredFire compartment temperatures above 100˚C 100 0 0 0 0 0 1 1 59
Elevated temperatures (30-100˚C) 97 0 0 0 2 2 1 1 60
Freezing temperatures (sub-zero) 100 0 0 0 0 0 1 1 59
Dust 92 5 0 0 2 2 1 1 59
Overcrowding 97 2 2 0 0 0 1 1 59
Open spaces 98 2 0 0 0 0 1 1 59
Height 100 0 0 0 0 0 1 1 59
Enclosed spaces 98 0 0 0 0 2 1 1 59
Total darkness 100 0 0 0 0 0 1 1 59
Partial darkness 98 0 0 0 2 0 1 1 59
Working in water 100 0 0 0 0 0 1 1 59
Working under water 100 0 0 0 0 0 1 1 59
Handling hazardous substances 100 0 0 0 0 0 1 1 59
Smoke 98 0 0 0 0 2 1 1 59
High humidity 100 0 0 0 0 0 1 1 59
Table 3: Importance respondents considered these activities to be to the effective performanceof their role? (continued)
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Dynamic flexibility requirementsBending at waist 15 13 23 17 12 20 3 3 60
Reaching 18 16 31 13 8 15 3 3 62
Stooping 13 5 8 21 16 36 6 5 61
Turning/twisting 26 23 16 5 6 24 1 3 62
Object activitiesCatching 2 0 0 10 3 85 6 6 59
Throwing 3 0 0 8 3 85 6 6 60
Fine dexterity (eg writing, assembling equipment) 74 16 5 0 0 5 1 1 62
Foot control (eg driving) 26 23 26 10 2 15 3 3 62

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-52
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time) (continued)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Equipment usedFire-protective Personnel Protective Equipment 100 0 0 0 0 0 1 1 58
Self-Contained Breathing Apparatus 100 0 0 0 0 0 1 1 58
Extended Duration Breathing Apparatus 100 0 0 0 0 0 1 1 58
Vibrating equipment 98 0 0 0 0 2 1 1 58
Computer 2 0 0 0 0 98 6 6 63
Telephone 2 0 0 0 0 98 6 6 63
Hand-held radio 39 16 16 8 8 11 1 2 61
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Handling hoses 0 0 0 0 0 100 6 6 58
Handling unconscious casualties 0 0 0 0 0 100 6 6 58
Handling ladders 0 0 0 0 0 100 6 6 58
Operating cutting equipment 0 0 0 0 0 100 6 6 57
Driving vehicles 2 8 15 17 14 44 6 5 59
Climbing ladders 3 0 0 0 3 93 6 6 58
Dealing with traumatised victims 27 24 3 2 0 44 6 2 59
Dealing with traumatised others (eg relatives, public) 37 25 5 2 0 32 1 2 60
Addressing groups of people 15 15 51 10 2 8 3 3 61
Filling in forms or completing paperwork 43 30 25 0 0 2 1 2 63
Making critical decisions quickly 86 13 2 0 0 0 1 1 63
Dealing with the media 29 27 38 5 2 0 3 2 63
Working on a computer 81 16 3 0 0 0 1 1 63
Communicating over the telephone 84 13 3 0 0 0 1 1 63
Environments encounteredFire compartment temperatures above 100˚C 0 0 0 0 0 100 6 6 59
Elevated temperatures (30-100˚C) 0 2 2 0 0 97 6 6 60
Freezing temperatures (sub-zero) 0 0 0 0 0 100 6 6 59
Dust 2 0 0 0 5 93 6 6 60
Overcrowding 2 0 0 0 2 97 6 6 60
Open spaces 0 0 0 0 0 100 6 6 59
Height 0 0 0 0 0 100 6 6 59
Enclosed spaces 0 0 0 0 0 100 6 6 59
Total darkness 0 0 0 0 0 100 6 6 59
Partial darkness 0 2 0 0 0 98 6 6 59
Working in water 0 0 0 0 0 100 6 6 59
Working under water 0 0 0 0 0 100 6 6 59
Handling hazardous substances 0 0 0 2 0 98 6 6 59
Smoke 0 0 0 0 0 100 6 6 59
High humidity 0 0 0 0 0 100 6 6 59

Appendix 9. Summary of Results for Control Supervisor from Occupational Guidelines Questionnaire
2A-53
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Equipment usedFire-protective Personnel Protective Equipment 0 0 0 0 0 100 6 6 58
Self-Contained Breathing Apparatus 0 0 0 0 0 100 6 6 58
Extended Duration Breathing Apparatus 0 0 0 0 0 100 6 6 58
Vibrating equipment 0 0 2 0 0 98 6 6 58
Computer 84 14 2 0 0 0 1 1 63
Telephone 86 13 2 0 0 0 1 1 63
Hand-held radio 23 11 30 2 2 33 6 3 61
Table 6: Near Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
BA control board-Old style MK 1 Read clock 2 98 2 2 64
BA control board-Old style MK 1 Graduations & cylinder pressure 2 98 2 2 64
BA tag Read tag 2 98 2 2 64
BA control board-New style MK 2 Read clock 2 98 2 2 64
BA control board-New style MK 2 Dial calculator 2 98 2 2 64
BA tag MK 2 Read tag 2 98 2 2 64
BA main control board Read clock 2 98 2 2 64
BA main control board Read 2 98 2 2 64
Sabre centurion Read BA graduations 2 98 2 2 64
Sabre centurion Read needle position 2 98 2 2 64
Siebe Gorman Read BA graduations 2 98 2 2 64
Siebe Gorman Read needle position 2 98 2 2 64
Drager Read BA graduations 2 98 2 2 64
Drager Read needle position 3 97 2 2 64
Philips PFX Handheld radio Read channel selector 9 91 2 2 64
Philips PFX Handheld radio Read numbered channel selector 6 94 2 2 64
BA log book Handwritten 2 98 2 2 64
Universal airline pack (Drager) BA supply BA cylinder gauge 2 98 2 2 64
Low pressure air bags Air pressure gauge 2 98 2 2 64
High pressure air bag Read graduations on console 2 98 2 2 64
High pressure air bag Needle position 2 98 2 2 64
Hurst high pressure lift bags Needle position 2 98 2 2 64
Microvent resuscitation equipment Read scale 2 98 2 2 64
Carmichael Godiva appliance Pressure gauge numbers 2 98 2 2 64
Saxon Volvo appliance pump Pressure gauge numbers 2 98 2 2 64
Dennis appliance pump Pressure gauge numbers 2 98 2 2 64
Read turnout sheet 6 94 2 2 64
Read dosimeter 2 98 2 2 64
Read survey meter 6 94 2 2 64
Read computer VDU 64 36 1 1 64
Read general paperwork 61 39 1 1 64
Read pager 23 77 2 2 64
Read mobile phone text 33 67 2 2 64
Read fire control panels 23 77 2 2 64
Read maps 59 41 1 1 64
Read fire extinguishers 9 91 2 2 64
Read plan inspections 11 89 2 2 64
Inspect premises 2 98 2 2 64
Read scale ruler 2 98 2 2 64
Read sound meter 0 100 2 2 64
Read light meter 0 100 2 2 64

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-54
Table 7: Distance Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
Street names White letters on a blue background 2 98 2 2 64
House numbers Copper figures on a blue background 2 98 2 2 64
House numbers White figures on a red background 2 98 2 2 64
Retail shop numbers Gold figures on a dark green background 2 98 2 2 64
House numbers Grey figures on a white background 2 98 2 2 64
Corporate building numbers Black figure on a silver background 2 98 2 2 64
Street names Black letters on a white background 2 98 2 2 64
House numbers Gold figures on a black background 2 98 2 2 64
House numbers Handpainted black figures on a white background 2 98 2 2 64
House numbers Gold figures on a black background 2 98 2 2 64
House numbers Black figures on a white background 3 97 2 2 64
Carmichael Godiva appliance pump Pressure gauge needle at rear of appliance 0 100 2 2 64
Carmichael Godiva appliance Measuring water in tank 0 100 2 2 64
Saxon Volvo appliance pump Pressure gauge needle at rear of appliance 0 100 2 2 64
Dennis appliance pump Pressure gauge needle at rear of appliance 0 100 2 2 64
Stop sign Road traffic signs 9 91 2 2 64
Give way sign Road traffic signs 9 91 2 2 64
One way street sign Road traffic signs 8 92 2 2 64
Chemical warning sign As EC Directive 92/58/EEC Hazardous substances 2 98 2 2 64
Vehicle signs Break lights/indicators on vehicles 6 94 2 2 64
Fire safety signs 8 92 2 2 64
Exit signs 13 88 2 2 64
Table 8: Hearing Tasks that are a requirement for role
Description Yes(1) No (2) Mode Median N
Distress signal unit 2 98 2 2 64
Warning whistle 0 100 2 2 64
Radio 81 19 1 1 64
Fireground orders 8 92 2 2 64
Evacuation signals/alarms 39 61 2 2 64
Telephone 91 9 1 1 64
Traffic 3 97 2 2 64
Vibraphone 2 98 2 2 64
Pager 28 72 2 2 64
Normal verbal communication with little background noise 80 20 1 1 64
Normal verbal communication with background noise 80 20 1 1 64
Hand clapping 2 98 2 2 64
Cries of help 30 70 2 2 64
Table 9: Other senses that are a requirement for role
Description Yes(1) No (2) Mode Median N
Touch 48 52 2 2 64
Smell 5 95 2 2 64
Taste 0 100 2 2 64

2A-55
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Sprinting 86 0 7 5 1 0 1 1 74
Running 83 1 7 4 5 0 1 1 76
Jogging 91 1 4 3 1 0 1 1 74
Walking 14 0 0 3 8 76 6 6 78
Climbing stairs 16 0 5 1 28 50 6 6 76
Climbing ladders 89 3 5 1 0 1 1 1 75
Crawling 89 3 4 3 0 1 1 1 75
Jumping 96 3 1 0 0 0 1 1 75
Hammering 95 1 3 1 0 0 1 1 75
Digging 96 1 3 0 0 0 1 1 75
Strength tasksLifting more than 5 kg or 11 pounds 61 3 7 17 9 3 1 1 75
Lifting more than 10 kg or 22 pounds 79 3 7 12 0 0 1 1 76
Lifting more than 20 kg or 44 pounds 88 4 1 7 0 0 1 1 76
Lifting more than 40 kg or 88 pounds 97 3 0 0 0 0 1 1 76
Carrying more than 5 kg or 11 pounds 69 1 8 10 9 3 1 1 77
Carrying more than 10 kg or 22 pounds 79 5 4 12 0 0 1 1 76
Carrying more than 20 kg or 44 pounds 91 3 1 5 0 0 1 1 76
Carrying more than 40 kg or 88 pounds 99 0 1 0 0 0 1 1 75
Pushing/pulling more than5 kg or 11 pounds 79 1 7 7 4 3 1 1 75
Pushing/pulling more than10 kg or 22 pounds 85 3 8 3 0 1 1 1 75
Pushing/pulling more than20 kg or 44 pounds 88 3 4 3 0 3 1 1 74
Pushing/pulling more than40 kg or 88 pounds 93 3 3 0 0 1 1 1 75
Static posturesStanding 10 1 1 1 8 79 6 6 80
Sitting 1 0 0 0 1 98 6 6 82
Squatting 59 0 3 3 21 15 1 1 75
Kneeling 55 0 6 16 17 6 1 1 77
Lying down 79 1 1 9 5 4 1 1 75
Table 1: Respondents’ Details
Age Bracket 18-19(1) 20-29(2) 30-39(3) 40-49(4) 50+(5) Mode Median N0 0 33 44 23 4 4 82
Years of Service 0-4 (1) 5-9 (2) 10-14(3) 15-19(4) 20-24(5) 25+(6) Mode Median N0 9 11 26 21 33 6 5 81
Gender Male Female Mode Median N27 73 2 2 81
Employment Status Fulltime(1) Retained(2) Mode Median N100 0 1 1 82
Appendix 10. Summary of Results for Control WatchManager from Occupational Guidelines QuestionnaireNote: Results are displayed as a percentage of the total responses for each role, and as the mode, median and total number (N) ofrespondents for the role

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-56
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time) (continued)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Dynamic flexibility requirementsBending at waist 26 0 4 6 10 54 6 6 78
Reaching 21 0 3 5 11 60 6 6 80
Stooping 40 1 6 3 18 32 1 5 78
Turning/twisting 20 1 3 1 9 66 6 6 80
Object activitiesCatching 88 3 3 3 4 0 1 1 74
Throwing 85 1 3 4 4 3 1 1 73
Fine dexterity(eg writing, assembling equipment) 0 0 0 0 0 100 6 6 79
Foot control (eg driving) 27 3 12 5 5 49 6 5 78
Table 3: Importance respondents considered these activities to be to the effective performanceof their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Sprinting 0 4 1 9 5 80 6 6 75
Running 1 1 3 12 8 75 6 6 76
Jogging 1 0 3 8 10 78 6 6 73
Walking 21 13 26 25 3 13 3 3 77
Climbing stairs 12 16 22 27 4 19 4 4 77
Climbing ladders 0 0 3 4 3 91 6 6 75
Crawling 0 1 0 7 12 80 6 6 76
Jumping 0 0 0 4 7 89 6 6 76
Hammering 0 0 0 3 7 91 6 6 76
Digging 0 0 0 3 5 92 6 6 76
Strength tasksLifting more than 5 kg or 11 pounds 1 5 3 20 7 64 6 6 75
Lifting more than 10 kg or 22 pounds 0 4 0 12 9 74 6 6 74
Lifting more than 20 kg or 44 pounds 0 1 0 7 14 78 6 6 74
Lifting more than 40 kg or 88 pounds 0 0 0 7 14 80 6 6 74
Carrying more than 5 kg or 11 pounds 1 4 1 15 7 72 6 6 74
Carrying more than 10 kg or 22 pounds 0 4 1 9 11 74 6 6 74
Carrying more than 20 kg or 44 pounds 0 1 0 7 14 78 6 6 74
Carrying more than 40 kg or 88 pounds 0 0 0 7 14 80 6 6 74
Pushing/pulling more than5 kg or 11 pounds 1 1 0 12 8 77 6 6 74
Pushing/pulling more than10 kg or 22 pounds 1 1 0 11 9 77 6 6 74
Pushing/pulling more than20 kg or 44 pounds 1 1 0 8 9 80 6 6 74
Pushing/pulling more than40 kg or 88 pounds 3 0 0 8 9 80 6 6 75
Static posturesStanding 23 14 27 20 9 8 3 3 79
Sitting 64 19 13 3 0 3 1 1 80
Squatting 4 5 14 18 11 48 6 5 73
Kneeling 1 5 13 20 14 46 6 5 76
Lying down 0 1 5 12 16 66 6 6 76

Appendix 10. Summary of Results for Control Watch Manager from Occupational Guidelines Questionnaire
2A-57
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Handling hoses 100 0 0 0 0 0 1 1 75
Handling unconscious casualties 100 0 0 0 0 0 1 1 76
Handling ladders 100 0 0 0 0 0 1 1 76
Operating cutting equipment 100 0 0 0 0 0 1 1 76
Driving vehicles 42 20 25 4 5 4 1 2 79
Climbing ladders 93 3 3 1 0 0 1 1 75
Dealing with traumatised victims 51 9 11 8 7 15 1 1 75
Dealing with traumatised others(eg relatives, public) 34 9 17 12 11 17 1 3 76
Addressing groups of people 9 17 31 14 6 23 3 3 78
Filling in forms or completing paperwork 0 0 1 4 2 93 6 6 82
Making critical decisions quickly 0 0 0 1 2 96 6 6 81
Dealing with the media 1 2 4 7 16 70 6 6 82
Working on a computer 0 0 0 0 0 100 6 6 83
Communicating over the telephone 0 0 0 0 0 100 6 6 83
Environments encounteredFire compartment temperaturesabove 100˚C 100 0 0 0 0 0 1 1 75
Elevated temperatures (30-100˚C) 97 1 0 1 0 0 1 1 77
Freezing temperatures (sub-zero) 99 1 0 0 0 0 1 1 77
Dust 91 1 1 3 1 3 1 1 77
Overcrowding 97 3 0 0 0 0 1 1 77
Open spaces 96 0 1 0 1 1 1 1 77
Height 97 1 0 0 1 0 1 1 77
Enclosed spaces 97 1 0 0 0 1 1 1 77
Total darkness 99 1 0 0 0 0 1 1 77
Partial darkness 96 0 1 1 1 0 1 1 77
Working in water 100 0 0 0 0 0 1 1 77
Working under water 100 0 0 0 0 0 1 1 77
Handling hazardous substances 96 0 1 1 1 0 1 1 77
Smoke 99 0 1 0 0 0 1 1 77
High humidity 96 1 0 1 0 1 1 1 77
Table 3: Importance respondents considered these activities to be to the effective performanceof their role? (continued)
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Dynamic flexibility requirementsBending at waist 19 15 21 20 4 21 6 3 75
Reaching 22 12 32 17 1 16 3 3 76
Stooping 13 7 13 32 1 33 6 4 75
Turning/twisting 21 20 21 20 1 17 3 3 76
Object activitiesCatching 0 0 0 5 16 78 6 6 74
Throwing 0 0 0 5 15 80 6 6 74
Fine dexterity(eg writing, assembling equipment) 80 11 5 0 0 4 1 1 79
Foot control (eg driving) 27 6 18 24 1 23 1 3 78

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-58
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time) (continued)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Equipment usedFire-protective PersonnelProtective Equipment 99 0 0 1 0 0 1 1 76
Self-Contained Breathing Apparatus 100 0 0 0 0 0 1 1 76
Extended Duration Breathing Apparatus 100 0 0 0 0 0 1 1 76
Vibrating equipment 99 0 1 0 0 0 1 1 76
Computer 4 0 0 0 0 96 6 6 82
Telephone 2 0 0 0 0 98 6 6 82
Hand-held radio 32 11 19 13 11 14 1 3 79
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Handling hoses 1 0 0 1 3 95 6 6 76
Handling unconscious casualties 1 0 0 1 3 95 6 6 76
Handling ladders 1 0 0 1 3 95 6 6 76
Operating cutting equipment 3 0 0 1 1 95 6 6 75
Driving vehicles 5 4 19 16 5 51 6 6 77
Climbing ladders 1 0 3 1 3 92 6 6 74
Dealing with traumatised victims 36 8 7 0 0 49 6 3 72
Dealing with traumatised others(eg relatives, public) 38 22 12 0 0 28 1 2 78
Addressing groups of people 19 21 45 3 3 10 3 3 80
Filling in forms or completing paperwork 51 28 16 2 0 2 1 1 82
Making critical decisions quickly 84 10 4 1 0 1 1 1 83
Dealing with the media 27 26 41 5 0 1 3 2 82
Working on a computer 84 7 7 0 0 1 1 1 83
Communicating over the telephone 86 11 2 0 0 1 1 1 83
Environments encounteredFire compartment temperaturesabove 100˚C 4 0 1 0 0 95 6 6 77
Elevated temperatures (30-100˚C) 3 0 1 0 3 94 6 6 77
Freezing temperatures (sub-zero) 4 0 1 0 0 95 6 6 77
Dust 4 0 3 3 0 91 6 6 77
Overcrowding 3 0 0 1 1 95 6 6 77
Open spaces 4 0 1 1 0 94 6 6 77
Height 4 0 1 1 1 92 6 6 77
Enclosed spaces 5 0 1 1 0 92 6 6 77
Total darkness 4 0 3 0 0 94 6 6 77
Partial darkness 4 0 3 1 0 92 6 6 77
Working in water 4 0 0 1 0 95 6 6 77
Working under water 4 0 0 0 0 96 6 6 77
Handling hazardous substances 4 1 0 3 1 91 6 6 77
Smoke 4 0 1 0 1 94 6 6 77
High humidity 4 0 0 1 1 94 6 6 77

Appendix 10. Summary of Results for Control Watch Manager from Occupational Guidelines Questionnaire
2A-59
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Equipment usedFire-protective PersonnelProtective Equipment 4 0 0 1 0 95 6 6 77
Self-Contained Breathing Apparatus 3 0 1 1 0 95 6 6 77
Extended Duration Breathing Apparatus 3 0 0 3 0 95 6 6 77
Vibrating equipment 3 0 1 3 0 93 6 6 76
Computer 86 7 4 0 0 4 1 1 83
Telephone 87 8 1 0 0 4 1 1 83
Hand-held radio 20 8 21 16 1 34 6 4 80
Table 6: Near Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
BA control board-Old style MK 1 Read clock 1 99 2 2 83
BA control board-Old style MK 1 Graduations & cylinder pressure 1 99 2 2 83
BA tag Read tag 1 99 2 2 83
BA control board-New style MK 2 Read clock 1 99 2 2 83
BA control board-New style MK 2 Dial calculator 1 99 2 2 83
BA tag MK 2 Read tag 1 99 2 2 83
BA main control board Read clock 1 99 2 2 83
BA main control board Read 1 99 2 2 83
Sabre centurion Read BA graduations 1 99 2 2 83
Sabre centurion Read needle position 1 99 2 2 83
Siebe Gorman Read BA graduations 1 99 2 2 83
Siebe Gorman Read needle position 1 99 2 2 83
Drager Read BA graduations 1 99 2 2 83
Drager Read needle position 2 98 2 2 83
Philips PFX Handheld radio Read channel selector 8 92 2 2 83
Philips PFX Handheld radio Read numbered channel selector 6 94 2 2 83
BA log book Handwritten 1 99 2 2 83
Universal airline pack (Drager) BA supply BA cylinder gauge 1 99 2 2 83
Low pressure air bags Air pressure gauge 1 99 2 2 83
High pressure air bag Read graduations on console 1 99 2 2 83
High pressure air bag Needle position 1 99 2 2 83
Hurst high pressure lift bags Needle position 1 99 2 2 83
Microvent resuscitation equipment Read scale 1 99 2 2 83
Carmichael Godiva appliance Pressure gauge numbers 1 99 2 2 83
Saxon Volvo appliance pump Pressure gauge numbers 1 99 2 2 83
Dennis appliance pump Pressure gauge numbers 2 98 2 2 83
Read turnout sheet 5 95 2 2 83
Read dosimeter 1 99 2 2 83
Read survey meter 1 99 2 2 83
Read computer VDU 52 48 1 1 83
Read general paperwork 55 45 1 1 83
Read pager 17 83 2 2 83
Read mobile phone text 33 67 2 2 83
Read fire control panels 23 77 2 2 83
Read maps 55 45 1 1 83
Read fire extinguishers 7 93 2 2 83
Read plan inspections 10 90 2 2 83
Inspect premises 1 99 2 2 83
Read scale ruler 5 95 2 2 83
Read sound meter 1 99 2 2 83
Read light meter 1 99 2 2 83

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-60
Table 7: Distance Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
Street names White letters on a blue background 5 95 2 2 83
House numbers Copper figures on a blue background 5 95 2 2 83
House numbers White figures on a red background 5 95 2 2 83
Retail shop numbers Gold figures on a dark green background 5 95 2 2 83
House numbers Grey figures on a white background 5 95 2 2 83
Corporate building numbers Black figure on a silver background 5 95 2 2 83
Street names Black letters on a white background 8 92 2 2 83
House numbers Gold figures on a black background 5 95 2 2 83
House numbers Handpainted black figures on a white background 5 95 2 2 83
House numbers Gold figures on a black background 5 95 2 2 83
House numbers Black figures on a white background 6 94 2 2 83
Carmichael Godiva appliance pump Pressure gauge needle at rear of appliance 2 98 2 2 83
Carmichael Godiva appliance Measuring water in tank 1 99 2 2 83
Saxon Volvo appliance pump Pressure gauge needle at rear of appliance 2 98 2 2 83
Dennis appliance pump Pressure gauge needle at rear of appliance 2 98 2 2 83
Stop sign Road traffic signs 13 87 2 2 83
Give way sign Road traffic signs 14 86 2 2 83
One way street sign Road traffic signs 14 86 2 2 83
Chemical warning sign As EC Directive 92/58/EEC Hazardous substances 10 90 2 2 83
Vehicle signs Break lights/indicators on vehicles 13 87 2 2 83
Fire safety signs 10 90 2 2 83
Exit signs 11 89 2 2 83
Table 8: Hearing Tasks that are a requirement for role
Description Yes(1) No (2) Mode Median N
Distress signal unit 2 98 2 2 83
Warning whistle 5 95 2 2 83
Radio 82 18 1 1 83
Fireground orders 6 94 2 2 83
Evacuation signals/alarms 33 67 2 2 83
Telephone 90 10 1 1 83
Traffic 6 94 2 2 83
Vibraphone 4 96 2 2 83
Pager 27 73 2 2 83
Normal verbal communication with little background noise 78 22 1 1 83
Normal verbal communication with background noise 87 13 1 1 83
Hand clapping 8 92 2 2 83
Cries of help 25 75 2 2 83
Table 9: Other senses that are a requirement for role
Description Yes(1) No (2) Mode Median N
Touch 53 47 1 1 83
Smell 2 98 2 2 83
Taste 1 99 2 2 83

2A-61
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Sprinting 100 0 0 0 0 0 1 1 28
Running 96 0 4 0 0 0 1 1 28
Jogging 93 0 7 0 0 0 1 1 27
Walking 11 0 4 0 0 86 6 6 28
Climbing stairs 7 0 0 0 11 82 6 6 28
Climbing ladders 93 0 7 0 0 0 1 1 28
Crawling 96 0 4 0 0 0 1 1 28
Jumping 100 0 0 0 0 0 1 1 28
Hammering 96 0 4 0 0 0 1 1 28
Digging 96 4 0 0 0 0 1 1 27
Strength tasksLifting more than 5 kg or 11 pounds 67 0 15 11 4 4 1 1 27
Lifting more than 10 kg or 22 pounds 74 4 15 4 4 0 1 1 27
Lifting more than 20 kg or 44 pounds 86 4 4 4 4 0 1 1 28
Lifting more than 40 kg or 88 pounds 89 7 0 0 4 0 1 1 28
Carrying more than 5 kg or 11 pounds 68 0 18 4 4 7 1 1 28
Carrying more than 10 kg or 22 pounds 79 4 14 4 0 0 1 1 28
Carrying more than 20 kg or 44 pounds 89 7 4 0 0 0 1 1 28
Carrying more than 40 kg or 88 pounds 96 4 0 0 0 0 1 1 28
Pushing/pulling more than 5 kg or 11 pounds 89 0 4 0 4 4 1 1 28
Pushing/pulling more than10 kg or 22 pounds 93 4 0 4 0 0 1 1 28
Pushing/pulling more than 20 kg or 44 pounds 93 4 4 0 0 0 1 1 28
Pushing/pulling more than 40 kg or 88 pounds 93 4 4 0 0 0 1 1 28
Static posturesStanding 7 0 4 0 4 86 6 6 28
Sitting 4 0 0 4 0 93 6 6 28
Squatting 61 0 7 11 21 0 1 1 28
Kneeling 63 0 11 15 7 4 1 1 27
Lying down 89 0 7 0 4 0 1 1 28
Table 1: Respondents’ Details
Age Bracket 18-19(1) 20-29(2) 30-39(3) 40-49(4) 50+(5) Mode Median N0 0 4 61 36 4 4 28
Years of Service 0-4 (1) 5-9 (2) 10-14(3) 15-19(4) 20-24(5) 25+(6) Mode Median N0 0 4 11 21 64 6 6 28
Gender Male Female Mode Median N39 61 2 2 28
Employment Status Fulltime(1) Retained(2) Mode Median N96 4 1 1 28
Appendix 11. Summary of Results for Control OperationsManager from Occupational Guidelines QuestionnaireNote: Results are displayed as a percentage of the total responses for each role, and as the mode, median and total number (N) ofrespondents for the role

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-62
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time) (continued)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Dynamic flexibility requirementsBending at waist 19 0 0 7 11 63 6 6 27
Reaching 11 0 0 0 19 70 6 6 27
Stooping 22 0 0 4 19 56 6 6 27
Turning/twisting 26 0 0 0 7 67 6 6 27
Object activitiesCatching 89 0 4 4 4 0 1 1 28
Throwing 86 0 4 4 7 0 1 1 28
Fine dexterity(eg writing, assembling equipment) 0 0 0 0 0 100 6 6 28
Foot control (eg driving) 11 0 4 4 25 57 6 6 28
Table 3: Importance respondents considered these activities to be to the effective performanceof their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Sprinting 0 0 0 7 4 89 6 6 28
Running 0 0 0 7 7 86 6 6 28
Jogging 0 4 0 7 11 79 6 6 28
Walking 21 18 18 14 7 21 1 3 28
Climbing stairs 25 14 21 18 4 18 1 3 28
Climbing ladders 0 0 7 4 4 86 6 6 28
Crawling 0 0 0 7 4 89 6 6 28
Jumping 0 0 0 4 4 93 6 6 28
Hammering 0 0 0 4 4 93 6 6 28
Digging 0 0 0 4 4 93 6 6 28
Strength tasksLifting more than 5 kg or 11 pounds 7 0 11 18 7 57 6 6 28
Lifting more than 10 kg or 22 pounds 4 0 4 18 14 61 6 6 28
Lifting more than 20 kg or 44 pounds 4 0 0 7 11 79 6 6 28
Lifting more than 40 kg or 88 pounds 0 0 4 4 11 82 6 6 28
Carrying more than 5 kg or 11 pounds 4 0 7 11 11 68 6 6 28
Carrying more than 10 kg or 22 pounds 4 0 0 14 11 71 6 6 28
Carrying more than 20 kg or 44 pounds 4 0 0 7 11 79 6 6 28
Carrying more than 40 kg or 88 pounds 0 0 0 4 11 85 6 6 27
Pushing/pulling more than 5 kg or 11 pounds 4 0 4 7 11 75 6 6 28
Pushing/pulling more than10 kg or 22 pounds 4 0 0 7 11 79 6 6 28
Pushing/pulling more than20 kg or 44 pounds 4 0 0 7 11 79 6 6 28
Pushing/pulling more than40 kg or 88 pounds 0 0 4 4 11 82 6 6 28
Static posturesStanding 11 14 21 46 4 4 4 4 28
Sitting 57 29 7 4 0 4 1 1 28
Squatting 4 4 11 29 21 32 6 5 28
Kneeling 0 7 7 32 11 43 6 5 28
Lying down 0 0 4 15 4 78 6 6 27

Appendix 11. Summary of Results for Control Operations Manager from Occupational Guidelines Questionnaire
2A-63
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Handling hoses 100 0 0 0 0 0 1 1 26
Handling unconscious casualties 100 0 0 0 0 0 1 1 27
Handling ladders 96 0 0 4 0 0 1 1 27
Operating cutting equipment 100 0 0 0 0 0 1 1 27
Driving vehicles 30 0 0 19 22 30 6 5 27
Climbing ladders 81 0 7 7 4 0 1 1 27
Dealing with traumatised victims 70 4 15 4 0 7 1 1 27
Dealing with traumatised others(eg relatives, public) 69 12 8 0 0 12 1 1 26
Addressing groups of people 7 0 29 25 4 36 6 4 28
Filling in forms or completing paperwork 0 0 4 0 7 89 6 6 28
Making critical decisions quickly 4 0 0 7 21 68 6 6 28
Dealing with the media 14 11 25 21 7 21 3 4 28
Working on a computer 0 0 0 0 0 100 6 6 28
Communicating over the telephone 4 0 0 0 0 96 6 6 28
Environments encounteredFire compartment temperaturesabove 100˚C 100 0 0 0 0 0 1 1 26
Elevated temperatures (30-100˚C) 100 0 0 0 0 0 1 1 28
Freezing temperatures (sub-zero) 100 0 0 0 0 0 1 1 28
Dust 93 0 4 0 4 0 1 1 28
Overcrowding 96 0 0 0 4 0 1 1 28
Open spaces 89 0 0 0 7 4 1 1 28
Height 96 0 0 4 0 0 1 1 28
Enclosed spaces 89 0 4 4 0 4 1 1 28
Total darkness 96 4 0 0 0 0 1 1 28
Partial darkness 93 4 4 0 0 0 1 1 28
Working in water 100 0 0 0 0 0 1 1 28
Working under water 100 0 0 0 0 0 1 1 28
Handling hazardous substances 96 0 0 4 0 0 1 1 28
Smoke 96 0 0 4 0 0 1 1 28
High humidity 96 0 0 4 0 0 1 1 28
Table 3: Importance respondents considered these activities to be to the effective performanceof their role? (continued)
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Dynamic flexibility requirementsBending at waist 11 11 25 29 11 14 4 4 28
Reaching 14 25 18 29 11 4 4 3 28
Stooping 4 14 11 43 11 18 4 4 28
Turning/twisting 14 18 14 25 11 18 4 4 28
Object activitiesCatching 0 0 0 19 7 74 6 6 27
Throwing 0 0 0 19 7 74 6 6 27
Fine dexterity(eg writing, assembling equipment) 70 26 0 4 0 0 1 1 27
Foot control (eg driving) 26 15 22 19 4 15 1 3 27

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-64
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time) (continued)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Equipment usedFire-protective PersonnelProtective Equipment 100 0 0 0 0 0 1 1 26
Self-Contained Breathing Apparatus 100 0 0 0 0 0 1 1 27
Extended Duration Breathing Apparatus 100 0 0 0 0 0 1 1 27
Vibrating equipment 93 0 0 0 4 4 1 1 27
Computer 0 0 0 0 0 100 6 6 28
Telephone 0 0 0 0 0 100 6 6 28
Hand-held radio 48 4 19 15 7 7 1 2 27
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Handling hoses 7 0 0 0 0 93 6 6 28
Handling unconscious casualties 7 0 0 0 0 93 6 6 28
Handling ladders 7 0 0 0 0 93 6 6 28
Operating cutting equipment 7 0 4 0 0 89 6 6 28
Driving vehicles 14 21 25 7 0 32 6 3 28
Climbing ladders 8 0 4 0 0 88 6 6 26
Dealing with traumatised victims 18 11 7 4 0 61 6 6 28
Dealing with traumatised others(eg relatives, public) 25 7 7 0 0 61 6 6 28
Addressing groups of people 21 43 32 4 0 0 2 2 28
Filling in forms or completing paperwork 39 50 11 0 0 0 2 2 28
Making critical decisions quickly 71 14 14 0 0 0 1 1 28
Dealing with the media 26 26 37 7 0 4 3 2 27
Working on a computer 75 25 0 0 0 0 1 1 28
Communicating over the telephone 75 25 0 0 0 0 1 1 28
Environments encounteredFire compartment temperaturesabove 100˚C 0 0 0 0 0 100 6 6 25
Elevated temperatures (30-100oC) 0 0 0 0 0 100 6 6 26
Freezing temperatures (sub-zero) 0 0 0 0 0 100 6 6 26
Dust 0 0 0 8 0 92 6 6 26
Overcrowding 0 0 0 4 0 96 6 6 26
Open spaces 0 0 4 4 0 92 6 6 26
Height 0 0 0 4 0 96 6 6 26
Enclosed spaces 4 0 0 4 0 92 6 6 26
Total darkness 0 0 4 0 0 96 6 6 26
Partial darkness 0 4 0 0 0 96 6 6 26
Working in water 0 0 0 0 0 100 6 6 26
Working under water 0 0 0 0 0 100 6 6 26
Handling hazardous substances 0 0 0 0 0 100 6 6 26
Smoke 0 0 4 0 0 96 6 6 26
High humidity 0 0 4 0 0 96 6 6 26

Appendix 11. Summary of Results for Control Operations Manager from Occupational Guidelines Questionnaire
2A-65
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Equipment usedFire-protective PersonnelProtective Equipment 0 0 0 0 0 100 6 6 26
Self-Contained Breathing Apparatus 0 0 0 0 0 100 6 6 27
Extended Duration Breathing Apparatus 0 0 0 0 0 100 6 6 27
Vibrating equipment 0 0 0 4 0 96 6 6 27
Computer 79 18 4 0 0 0 1 1 28
Telephone 79 18 4 0 0 0 1 1 28
Hand-held radio 14 4 32 7 0 43 6 4 28
Table 6: Near Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
BA control board-Old style MK 1 Read clock 0 100 2 2 28
BA control board-Old style MK 1 Graduations & cylinder pressure 0 100 2 2 28
BA tag Read tag 0 100 2 2 28
BA control board-New style MK 2 Read clock 0 100 2 2 28
BA control board-New style MK 2 Dial calculator 0 100 2 2 28
BA tag MK 2 Read tag 0 100 2 2 28
BA main control board Read clock 0 100 2 2 28
BA main control board Read 0 100 2 2 28
Sabre centurion Read BA graduations 0 100 2 2 28
Sabre centurion Read needle position 0 100 2 2 28
Siebe Gorman Read BA graduations 0 100 2 2 28
Siebe Gorman Read needle position 0 100 2 2 28
Drager Read BA graduations 0 100 2 2 28
Drager Read needle position 0 100 2 2 28
Philips PFX Handheld radio Read channel selector 7 93 2 2 28
Philips PFX Handheld radio Read numbered channel selector 7 93 2 2 28
BA log book Handwritten 0 100 2 2 28
Universal airline pack (Drager) BA supply BA cylinder gauge 0 100 2 2 28
Low pressure air bags Air pressure gauge 0 100 2 2 28
High pressure air bag Read graduations on console 0 100 2 2 28
High pressure air bag Needle position 0 100 2 2 28
Hurst high pressure lift bags Needle position 0 100 2 2 28
Microvent resuscitation equipment Read scale 0 100 2 2 28
Carmichael Godiva appliance Pressure gauge numbers 0 100 2 2 28
Saxon Volvo appliance pump Pressure gauge numbers 0 100 2 2 28
Dennis appliance pump Pressure gauge numbers 0 100 2 2 28
Read turnout sheet 0 100 2 2 28
Read dosimeter 0 100 2 2 28
Read survey meter 0 100 2 2 28
Read computer VDU 57 43 1 1 28
Read general paperwork 54 46 1 1 28
Read pager 46 54 2 2 28
Read mobile phone text 43 57 2 2 28
Read fire control panels 25 75 2 2 28
Read maps 61 39 1 1 28
Read fire extinguishers 4 96 2 2 28
Read plan inspections 7 93 2 2 28
Inspect premises 0 100 2 2 28
Read scale ruler 0 100 2 2 28
Read sound meter 0 100 2 2 28
Read light meter 0 100 2 2 28

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-66
Table 7: Distance Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
Street names White letters on a blue background 7 93 2 2 28
House numbers Copper figures on a blue background 4 96 2 2 28
House numbers White figures on a red background 4 96 2 2 28
Retail shop numbers Gold figures on a dark green background 4 96 2 2 28
House numbers Grey figures on a white background 4 96 2 2 28
Corporate building numbers Black figure on a silver background 4 96 2 2 28
Street names Black letters on a white background 7 93 2 2 28
House numbers Gold figures on a black background 4 96 2 2 28
House numbers Handpainted black figures on a white background 4 96 2 2 28
House numbers Gold figures on a black background 4 96 2 2 28
House numbers Black figures on a white background 4 96 2 2 28
Carmichael Godiva appliance pump Pressure gauge needle at rear of appliance 0 100 2 2 28
Carmichael Godiva appliance Measuring water in tank 0 100 2 2 28
Saxon Volvo appliance pump Pressure gauge needle at rear of appliance 0 100 2 2 28
Dennis appliance pump Pressure gauge needle at rear of appliance 0 100 2 2 28
Stop sign Road traffic signs 25 75 2 2 28
Give way sign Road traffic signs 29 71 2 2 28
One way street sign Road traffic signs 29 71 2 2 28
Chemical warning sign As EC Directive 92/58/EEC Hazardous substances 7 93 2 2 28
Vehicle signs Break lights/indicators on vehicles 21 79 2 2 28
Fire safety signs 11 89 2 2 28
Exit signs 14 86 2 2 28
Table 8: Hearing Tasks that are a requirement for role
Description Yes(1) No (2) Mode Median N
Distress signal unit 0 100 2 2 28
Warning whistle 0 100 2 2 28
Radio 86 14 1 1 28
ireground orders 14 86 2 2 28
Evacuation signals/alarms 25 75 2 2 28
Telephone 93 7 1 1 28
Traffic 11 89 2 2 28
Vibraphone 4 96 2 2 28
Pager 79 21 1 1 28
Normal verbal communication with little background noise 89 11 1 1 28
Normal verbal communication with background noise 86 14 1 1 28
Hand clapping 7 93 2 2 28
Cries of help 14 86 2 2 28
Table 9: Other senses that are a requirement for role
Description Yes(1) No (2) Mode Median N
Touch 54 46 1 1 28
Smell 4 96 2 2 28
Taste 0 100 2 2 28

2A-67
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
printing 89 2 2 5 2 0 1 1 55
Running 69 10 2 16 3 0 1 1 58
Jogging 56 12 9 12 9 2 1 1 57
Walking 3 0 0 5 11 81 6 6 62
Climbing stairs 3 0 0 0 8 89 6 6 62
Climbing ladders 44 16 26 7 4 4 1 2 57
Crawling 61 26 11 2 0 0 1 1 57
Jumping 70 12 11 4 4 0 1 1 57
Hammering 88 4 9 0 0 0 1 1 57
Digging 82 4 14 0 0 0 1 1 57
Strength tasksLifting more than 5 kg or 11 pounds 22 9 21 24 9 16 4 3 58
Lifting more than 10 kg or 22 pounds 36 14 24 14 10 2 1 3 58
Lifting more than 20 kg or 44 pounds 60 18 14 5 4 0 1 1 57
Lifting more than 40 kg or 88 pounds 79 9 4 5 4 0 1 1 57
Carrying more than 5 kg or 11 pounds 35 7 19 16 12 11 1 3 57
Carrying more than 10 kg or 22 pounds 43 17 19 14 5 2 1 2 58
Carrying more than 20 kg or 44 pounds 68 14 13 2 4 0 1 1 56
Carrying more than 40 kg or 88 pounds 82 7 7 2 2 0 1 1 55
Pushing/pulling more than5 kg or 11 pounds 60 7 19 5 9 0 1 1 57
Pushing/pulling more than10 kg or 22 pounds 58 12 19 7 4 0 1 1 57
Pushing/pulling more than20 kg or 44 pounds 70 16 11 2 2 0 1 1 56
Pushing/pulling more than40 kg or 88 pounds 82 13 2 2 2 0 1 1 56
Static posturesStanding 3 0 2 0 5 90 6 6 63
Sitting 3 0 2 2 3 90 6 6 63
Squatting 28 4 9 18 21 21 1 4 57
Kneeling 22 2 16 26 24 10 4 4 58
Lying down 76 7 3 2 7 5 1 1 58
Table 1: Respondents’ Details
Age Bracket 18-19(1) 20-29(2) 30-39(3) 40-49(4) 50+(5) Mode Median N0 3 24 57 16 4 4 63
Years of Service 0-4 (1) 5-9 (2) 10-14(3) 15-19(4) 20-24(5) 25+(6) Mode Median N2 6 13 22 21 37 6 5 63
Gender Male Female Mode Median N98 2 1 1 62
Employment Status Fulltime(1) Retained(2) Mode Median N100 0 1 1 61
Appendix 12. Summary of Results for Fire SafetyOfficer from Occupational Guidelines QuestionnaireNote: Results are displayed as a percentage of the total responses for each role, and as the mode, median and total number (N) ofrespondents for the role

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-68
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time) (continued)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Dynamic flexibility requirementsBending at waist 8 0 5 7 18 62 6 6 61
Reaching 10 0 3 13 13 61 6 6 61
Stooping 16 0 10 8 13 52 6 6 61
Turning/twisting 13 0 2 8 10 67 6 6 60
Object activitiesCatching 69 5 12 3 5 5 1 1 58
Throwing 66 5 13 2 5 9 1 1 56
Fine dexterity(eg writing, assembling equipment) 3 0 0 0 7 90 6 6 61
Foot control (eg driving) 2 0 0 2 13 84 6 6 62
Table 3: Importance respondents considered these activities to be to the effective performanceof their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Sprinting 0 0 3 15 22 59 6 6 59
Running 0 0 11 15 23 51 6 6 61
Jogging 0 2 21 10 19 48 6 5 62
Walking 52 19 19 3 5 2 1 1 62
Climbing stairs 50 19 21 3 5 2 1 2 62
Climbing ladders 3 10 25 23 10 30 6 4 61
Crawling 0 0 10 32 15 42 6 5 59
Jumping 0 0 3 25 18 53 6 6 60
Hammering 0 0 2 13 17 68 6 6 60
Digging 0 0 7 12 12 70 6 6 60
Strength tasksLifting more than 5 kg or 11 pounds 3 13 30 23 8 23 3 4 61
Lifting more than 10 kg or 22 pounds 0 7 26 23 15 30 6 4 61
Lifting more than 20 kg or 44 pounds 0 2 15 23 22 38 6 5 60
Lifting more than 40 kg or 88 pounds 0 0 8 25 22 44 6 5 59
Carrying more than 5 kg or 11 pounds 2 13 23 20 15 28 6 4 61
Carrying more than 10 kg or 22 pounds 0 5 25 21 18 31 6 4 61
Carrying more than 20 kg or 44 pounds 0 0 13 30 18 38 6 5 60
Carrying more than 40 kg or 88 pounds 0 2 8 25 22 43 6 5 60
Pushing/pulling more than5 kg or 11 pounds 0 7 20 19 19 36 6 5 59
Pushing/pulling more than10 kg or 22 pounds 0 3 17 18 23 38 6 5 60
Pushing/pulling more than20 kg or 44 pounds 0 0 10 23 27 40 6 5 60
Pushing/pulling more than40 kg or 88 pounds 0 2 7 20 28 43 6 5 60
Static posturesStanding 46 27 16 5 6 0 1 2 63
Sitting 49 21 17 10 3 0 1 2 63
Squatting 5 7 23 31 16 18 4 4 61
Kneeling 3 5 25 31 19 17 4 4 59
Lying down 3 3 0 13 18 62 6 6 60

Appendix 12. Summary of Results for Fire Safety Officer from Occupational Guidelines Questionnaire
2A-69
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Handling hoses 67 23 5 3 2 0 1 1 60
Handling unconscious casualties 76 17 5 2 0 0 1 1 59
Handling ladders 68 23 2 5 2 0 1 1 60
Operating cutting equipment 77 17 2 5 0 0 1 1 60
Driving vehicles 5 2 2 2 17 73 6 6 60
Climbing ladders 47 20 25 3 2 2 1 2 59
Dealing with traumatised victims 68 17 13 2 0 0 1 1 60
Dealing with traumatised others(eg relatives, public) 61 20 15 3 0 0 1 1 59
Addressing groups of people 3 10 35 29 17 6 3 4 63
Filling in forms or completing paperwork 0 0 0 5 5 90 6 6 62
Making critical decisions quickly 16 8 10 19 19 27 6 4 62
Dealing with the media 27 31 18 8 3 13 2 2 62
Working on a computer 2 0 2 2 6 89 6 6 63
Communicating over the telephone 0 0 0 2 2 97 6 6 63
Environments encounteredFire compartment temperaturesabove 100˚C 69 26 3 0 0 2 1 1 61
Elevated temperatures (30-100˚C) 65 21 13 0 0 2 1 1 62
Freezing temperatures (sub-zero) 50 42 6 2 0 0 1 2 62
Dust 35 21 37 3 3 0 3 2 62
Overcrowding 38 25 26 7 3 2 1 2 61
Open spaces 19 8 26 18 15 15 3 3 62
Height 21 21 23 26 3 5 4 3 61
Enclosed spaces 26 30 18 18 5 3 2 2 61
Total darkness 49 30 16 3 0 2 1 2 61
Partial darkness 26 30 23 15 2 5 2 2 61
Working in water 85 8 5 2 0 0 1 1 59
Working under water 95 3 0 2 0 0 1 1 61
Handling hazardous substances 79 13 5 3 0 0 1 1 61
Smoke 62 20 11 5 2 0 1 1 61
High humidity 67 28 3 2 0 0 1 1 61
Table 3: Importance respondents considered these activities to be to the effective performanceof their role? (continued)
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Dynamic flexibility requirementsBending at waist 10 30 38 13 5 5 3 3 61
Reaching 10 29 31 19 6 5 3 3 62
Stooping 5 21 32 21 13 8 3 3 62
Turning/twisting 8 30 31 16 8 7 3 3 61
Object activitiesCatching 0 0 3 15 27 55 6 6 60
Throwing 0 0 5 13 28 53 6 6 60
Fine dexterity(eg writing, assembling equipment) 56 23 10 3 6 2 1 1 62
Foot control (eg driving) 61 18 10 3 5 3 1 1 62

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-70
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time) (continued)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Equipment usedFire-protective PersonnelProtective Equipment 46 22 12 17 0 3 1 2 59
Self-Contained Breathing Apparatus 68 25 2 2 3 0 1 1 59
Extended Duration Breathing Apparatus 90 5 5 0 0 0 1 1 59
Vibrating equipment 90 5 2 2 2 0 1 1 59
Computer 3 2 0 3 3 89 6 6 61
Telephone 3 2 0 0 0 95 6 6 60
Hand-held radio 59 14 10 5 2 10 1 1 59
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Handling hoses 0 3 8 10 21 57 6 6 61
Handling unconscious casualties 2 3 23 7 11 54 6 6 61
Handling ladders 2 3 18 8 16 52 6 6 61
Operating cutting equipment 2 5 10 12 20 51 6 6 59
Driving vehicles 60 18 8 3 2 8 1 1 60
Climbing ladders 3 10 26 13 11 36 6 4 61
Dealing with traumatised victims 2 8 20 15 5 50 6 6 60
Dealing with traumatised others(eg relatives, public) 2 12 22 15 7 42 6 4 59
Addressing groups of people 16 49 32 0 0 3 2 2 63
Filling in forms or completing paperwork 52 24 24 0 0 0 1 1 63
Making critical decisions quickly 27 26 29 8 5 5 3 2 62
Dealing with the media 5 28 40 13 8 5 3 3 60
Working on a computer 49 27 22 2 0 0 1 2 63
Communicating over the telephone 57 27 16 0 0 0 1 1 63
Environments encounteredFire compartment temperaturesabove 100˚C 3 7 13 10 12 55 6 6 60
Elevated temperatures (30-100˚C) 3 5 16 11 11 52 6 6 61
Freezing temperatures (sub-zero) 3 3 16 16 18 43 6 5 61
Dust 3 3 13 25 18 37 6 5 60
Overcrowding 5 7 20 22 20 27 6 4 60
Open spaces 8 5 18 22 25 22 5 4 60
Height 8 15 20 15 18 23 6 4 60
Enclosed spaces 8 10 20 18 17 27 6 4 60
Total darkness 7 12 13 20 18 30 6 4 60
Partial darkness 10 8 22 17 15 28 6 4 60
Working in water 3 3 10 12 13 58 6 6 60
Working under water 5 2 5 8 17 63 6 6 60
Handling hazardous substances 5 5 8 8 17 57 6 6 60
Smoke 8 5 10 8 17 52 6 6 60
High humidity 7 7 5 13 15 53 6 6 60

Appendix 12. Summary of Results for Fire Safety Officer from Occupational Guidelines Questionnaire
2A-71
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Equipment usedFire-protective PersonnelProtective Equipment 15 18 16 7 2 43 6 4 61
Self-Contained Breathing Apparatus 11 11 8 8 7 54 6 6 61
Extended Duration Breathing Apparatus 3 5 3 10 16 62 6 6 61
Vibrating equipment 5 5 3 13 16 57 6 6 61
Computer 51 30 16 3 0 0 1 1 63
Telephone 54 30 13 2 0 2 1 1 63
Hand-held radio 10 16 11 8 5 49 6 5 61
Table 6: Near Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
BA control board-Old style MK 1 Read clock 10 90 2 2 63
BA control board-Old style MK 1 Graduations & cylinder pressure 10 90 2 2 63
BA tag Read tag 10 90 2 2 63
BA control board-New style MK 2 Read clock 11 89 2 2 63
BA control board-New style MK 2 Dial calculator 13 87 2 2 63
BA tag MK 2 Read tag 13 87 2 2 63
BA main control board Read clock 14 86 2 2 63
BA main control board Read 13 87 2 2 63
Sabre centurion Read BA graduations 6 94 2 2 63
Sabre centurion Read needle position 5 95 2 2 63
Siebe Gorman Read BA graduations 2 98 2 2 63
Siebe Gorman Read needle position 2 98 2 2 63
Drager Read BA graduations 6 94 2 2 63
Drager Read needle position 6 94 2 2 63
Philips PFX Handheld radio Read channel selector 13 87 2 2 63
Philips PFX Handheld radio Read numbered channel selector 14 86 2 2 63
BA log book Handwritten 14 86 2 2 63
Universal airline pack (Drager) BA supply BA cylinder gauge 5 95 2 2 63
Low pressure air bags Air pressure gauge 5 95 2 2 63
High pressure air bag Read graduations on console 3 97 2 2 63
High pressure air bag Needle position 3 97 2 2 63
Hurst high pressure lift bags Needle position 5 95 2 2 63
Microvent resuscitation equipment Read scale 3 97 2 2 63
Carmichael Godiva appliance Pressure gauge numbers 3 97 2 2 63
Saxon Volvo appliance pump Pressure gauge numbers 2 98 2 2 63
Dennis appliance pump Pressure gauge numbers 8 92 2 2 63
Read turnout sheet 10 90 2 2 63
Read dosimeter 13 87 2 2 63
Read survey meter 14 86 2 2 63
Read computer VDU 67 33 1 1 63
Read general paperwork 75 25 1 1 63
Read pager 24 76 2 2 63
Read mobile phone text 49 51 2 2 63
Read fire control panels 40 60 2 2 63
Read maps 70 30 1 1 63
Read fire extinguishers 62 38 1 1 63
Read plan inspections 71 29 1 1 63
Inspect premises 70 30 1 1 63
Read scale ruler 65 35 1 1 63
Read sound meter 43 57 2 2 63
Read light meter 30 70 2 2 63

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-72
Table 7: Distance Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
Street names White letters on a blue background 86 14 1 1 63
House numbers Copper figures on a blue background 75 25 1 1 63
House numbers White figures on a red background 71 29 1 1 63
Retail shop numbers Gold figures on a dark green background 81 19 1 1 63
House numbers Grey figures on a white background 75 25 1 1 63
Corporate building numbers Black figure on a silver background 76 24 1 1 63
Street names Black letters on a white background 89 11 1 1 63
House numbers Gold figures on a black background 68 32 1 1 63
House numbers Handpainted black figures on a white background 68 32 1 1 63
House numbers Gold figures on a black background 70 30 1 1 63
House numbers Black figures on a white background 68 32 1 1 63
Carmichael Godiva appliance pump Pressure gauge needle at rear of appliance 5 95 2 2 63
Carmichael Godiva appliance Measuring water in tank 5 95 2 2 63
Saxon Volvo appliance pump Pressure gauge needle at rear of appliance 3 97 2 2 63
Dennis appliance pump Pressure gauge needle at rear of appliance 11 89 2 2 63
Stop sign Road traffic signs 89 11 1 1 63
Give way sign Road traffic signs 92 8 1 1 63
One way street sign Road traffic signs 90 10 1 1 63
Chemical warning sign As EC Directive 92/58/EEC Hazardous substances 54 46 1 1 63
Vehicle signs Break lights/indicators on vehicles 92 8 1 1 63
Fire safety signs 92 8 1 1 63
Exit signs 92 8 1 1 63
Table 8: Hearing Tasks that are a requirement for role
Description Yes(1) No (2) Mode Median N
Distress signal unit 25 75 2 2 63
Warning whistle 25 75 2 2 63
Radio 29 71 2 2 63
Fireground orders 24 76 2 2 63
Evacuation signals/alarms 48 52 2 2 63
Telephone 98 2 1 1 63
Traffic 89 11 1 1 63
Vibraphone 13 87 2 2 63
Pager 25 75 2 2 63
Normal verbal communication with little background noise 84 16 1 1 63
Normal verbal communication with background noise 76 24 1 1 63
Hand clapping 21 79 2 2 63
Cries of help 27 73 2 2 63
Table 9: Other senses that are a requirement for role
Description Yes(1) No (2) Mode Median N
Touch 59 41 1 1 63
Smell 41 59 2 2 63
Taste 16 84 2 2 63

2A-73
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Sprinting 96 4 0 0 0 0 1 1 25
Running 81 4 4 4 8 0 1 1 26
Jogging 70 0 15 7 4 4 1 1 27
Walking 0 0 7 4 11 78 6 6 27
Climbing stairs 4 4 4 7 14 68 6 6 28
Climbing ladders 52 19 22 4 0 4 1 1 27
Crawling 69 19 4 8 0 0 1 1 26
Jumping 76 12 12 0 0 0 1 1 25
Hammering 85 4 0 12 0 0 1 1 26
Digging 76 4 12 8 0 0 1 1 25
Strength tasksLifting more than 5 kg or 11 pounds 32 8 16 28 16 0 1 3 25
Lifting more than 10 kg or 22 pounds 40 4 28 20 8 0 1 3 25
Lifting more than 20 kg or 44 pounds 60 12 16 4 8 0 1 1 25
Lifting more than 40 kg or 88 pounds 76 12 8 4 0 0 1 1 25
Carrying more than 5 kg or 11 pounds 31 8 15 31 12 4 4 3 26
Carrying more than 10 kg or 22 pounds 48 0 28 20 0 4 1 3 25
Carrying more than 20 kg or 44 pounds 62 15 12 8 4 0 1 1 26
Carrying more than 40 kg or 88 pounds 76 20 4 0 0 0 1 1 25
Pushing/pulling more than5 kg or 11 pounds 52 28 4 8 0 8 1 1 25
Pushing/pulling more than10 kg or 22 pounds 64 12 16 0 4 4 1 1 25
Pushing/pulling more than20 kg or 44 pounds 72 12 12 4 0 0 1 1 25
Pushing/pulling more than40 kg or 88 pounds 69 15 8 8 0 0 1 1 26
Static posturesStanding 0 0 0 3 3 93 6 6 29
Sitting 0 0 0 0 0 100 6 6 29
Squatting 38 8 19 15 15 4 1 3 26
Kneeling 29 11 25 18 7 11 1 3 28
Lying down 74 7 7 0 7 4 1 1 27
Table 1: Respondents’ Details
Age Bracket 18-19(1) 20-29(2) 30-39(3) 40-49(4) 50+(5) Mode Median N0 0 14 59 28 4 4 29
Years of Service 0-4 (1) 5-9 (2) 10-14(3) 15-19(4) 20-24(5) 25+(6) Mode Median N3 0 3 17 28 48 6 5 29
Gender Male Female Mode Median N97 3 1 1 29
Employment Status Fulltime(1) Retained(2) Mode Median N100 0 1 1 29
Appendix 13. Summary of Results for Fire SafetyManager from Occupational Guidelines QuestionnaireNote: Results are displayed as a percentage of the total responses for each role, and as the mode, median and total number (N) ofrespondents for the role

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-74
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time) (continued)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Dynamic flexibility requirementsBending at waist 14 3 7 7 14 55 6 6 29
Reaching 14 3 0 17 14 52 6 6 29
Stooping 17 7 7 14 14 41 6 5 29
Turning/twisting 17 3 0 14 17 48 6 5 29
Object activitiesCatching 81 4 0 11 4 0 1 1 27
Throwing 78 4 0 11 4 4 1 1 27
Fine dexterityeg writing, assembling equipment) 4 0 0 0 0 96 6 6 28
Foot control (eg driving) 4 0 0 11 7 79 6 6 28
Table 3: Importance respondents considered these activities to be to the effective performanceof their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Sprinting 0 0 7 22 22 48 6 5 27
Running 0 7 19 15 11 48 6 5 27
Jogging 0 4 21 18 11 46 6 5 28
Walking 38 21 38 0 0 3 1 2 29
Climbing stairs 39 18 32 7 0 4 1 2 28
Climbing ladders 11 11 21 14 14 29 6 4 28
Crawling 0 7 11 19 19 44 6 5 27
Jumping 0 0 19 15 15 52 6 6 27
Hammering 0 4 11 11 11 63 6 6 27
Digging 0 4 11 7 11 67 6 6 27
Strength tasksLifting more than 5 kg or 11 pounds 16 16 16 12 20 20 6 4 25
Lifting more than 10 kg or 22 pounds 8 19 8 19 23 23 6 4 26
Lifting more than 20 kg or 44 pounds 4 8 12 19 31 27 5 5 26
Lifting more than 40 kg or 88 pounds 4 4 15 19 33 26 5 5 27
Carrying more than 5 kg or 11 pounds 15 19 11 19 19 19 2 4 27
Carrying more than 10 kg or 22 pounds 8 15 8 23 23 23 6 4 26
Carrying more than 20 kg or 44 pounds 4 8 15 19 27 27 6 5 26
Carrying more than 40 kg or 88 pounds 4 4 8 24 32 28 5 5 25
Pushing/pulling more than5 kg or 11 pounds 8 16 0 20 32 24 5 5 25
Pushing/pulling more than10 kg or 22 pounds 4 16 0 20 32 28 5 5 25
Pushing/pulling more than20 kg or 44 pounds 8 8 8 15 35 27 5 5 26
Pushing/pulling more than40 kg or 88 pounds 7 7 7 19 33 26 5 5 27
Static posturesStanding 45 7 38 7 3 0 1 2 29
Sitting 45 17 31 3 3 0 1 2 29
Squatting 7 14 21 21 21 14 5 4 28
Kneeling 7 11 14 18 25 25 5 5 28
Lying down 7 4 7 7 22 52 6 6 27

Appendix 13. Summary of Results for Fire Safety Manager from Occupational Guidelines Questionnaire
2A-75
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Handling hoses 50 36 14 0 0 0 1 2 28
Handling unconscious casualties 54 43 4 0 0 0 1 1 28
Handling ladders 59 33 7 0 0 0 1 1 27
Operating cutting equipment 75 18 4 0 0 4 1 1 28
Driving vehicles 17 0 3 7 10 62 6 6 29
Climbing ladders 46 25 21 7 0 0 1 2 28
Dealing with traumatised victims 54 25 21 0 0 0 1 1 28
Dealing with traumatised others(eg relatives, public) 46 25 25 4 0 0 1 2 28
Addressing groups of people 3 14 34 24 21 3 3 3 29
Filling in forms or completing paperwork 0 0 0 3 17 79 6 6 29
Making critical decisions quickly 0 3 34 10 28 24 3 5 29
Dealing with the media 0 31 34 17 7 10 3 3 29
Working on a computer 0 0 0 0 7 93 6 6 29
Communicating over the telephone 0 0 0 0 3 97 6 6 29
Environments encounteredFire compartment temperaturesabove 100˚C 57 39 4 0 0 0 1 1 28
Elevated temperatures (30-100˚C) 54 29 18 0 0 0 1 1 28
Freezing temperatures (sub-zero) 43 39 18 0 0 0 1 2 28
Dust 37 37 22 4 0 0 2 2 27
Overcrowding 48 41 11 0 0 0 1 2 27
Open spaces 33 22 22 15 7 0 1 2 27
Height 28 28 41 3 0 0 3 2 29
Enclosed spaces 34 34 28 3 0 0 1 2 29
Total darkness 54 39 7 0 0 0 1 1 28
Partial darkness 34 34 28 0 3 0 1 2 29
Working in water 71 21 7 0 0 0 1 1 28
Working under water 96 4 0 0 0 0 1 1 28
Handling hazardous substances 79 14 7 0 0 0 1 1 28
Smoke 38 34 28 0 0 0 1 2 29
High humidity 52 45 3 0 0 0 1 1 29
Table 3: Importance respondents considered these activities to be to the effective performanceof their role? (continued)
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Dynamic flexibility requirementsBending at waist 28 14 28 14 10 7 1 3 29
Reaching 24 14 31 14 10 7 3 3 29
Stooping 24 7 28 17 14 10 3 3 29
Turning/twisting 24 14 28 14 14 7 3 3 29
Object activitiesCatching 4 0 11 7 30 48 6 5 27
Throwing 4 0 7 11 30 48 6 5 27
Fine dexterity(eg writing, assembling equipment) 50 18 14 4 7 7 1 2 28
Foot control (eg driving) 43 18 25 0 7 7 1 2 28

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-76
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time) (continued)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Equipment usedFire-protective Personnel Protective Equipment 21 4 36 36 4 0 4 3 28
Self-Contained Breathing Apparatus 45 55 0 0 0 0 2 2 29
Extended Duration Breathing Apparatus 89 11 0 0 0 0 1 1 28
Vibrating equipment 93 0 4 0 0 4 1 1 28
Computer 0 0 0 0 0 100 6 6 29
Telephone 3 0 0 0 0 97 6 6 29
Hand-held radio 34 14 21 14 7 10 1 3 29
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Handling hoses 4 0 4 21 32 39 6 5 28
Handling unconscious casualties 7 4 21 21 11 36 6 4 28
Handling ladders 4 0 7 32 21 36 6 5 28
Operating cutting equipment 0 4 4 37 19 37 4 5 27
Driving vehicles 52 31 7 0 0 10 1 1 29
Climbing ladders 4 11 22 19 15 30 6 4 27
Dealing with traumatised victims 11 14 21 14 4 36 6 4 28
Dealing with traumatised others(eg relatives, public) 14 14 29 7 4 32 6 3 28
Addressing groups of people 28 34 31 3 0 3 2 2 29
Filling in forms or completing paperwork 45 24 28 3 0 0 1 2 29
Making critical decisions quickly 31 34 34 0 0 0 2 2 29
Dealing with the media 10 34 52 3 0 0 3 3 29
Working on a computer 52 31 14 3 0 0 1 1 29
Communicating over the telephone 55 31 14 0 0 0 1 1 29
Environments encounteredFire compartment temperaturesabove 100˚C 4 4 21 14 18 39 6 5 28
Elevated temperatures (30-100˚C) 4 4 21 21 11 39 6 5 28
Freezing temperatures (sub-zero) 4 4 18 25 11 39 6 5 28
Dust 7 4 14 32 14 29 4 4 28
Overcrowding 4 4 15 41 15 22 4 4 27
Open spaces 4 4 19 33 22 19 4 4 27
Height 7 14 25 11 18 25 3 4 28
Enclosed spaces 4 7 29 14 18 29 3 4 28
Total darkness 7 7 21 14 14 36 6 5 28
Partial darkness 7 10 24 17 17 24 3 4 29
Working in water 4 7 11 14 21 43 6 5 28
Working under water 0 0 4 25 18 54 6 6 28
Handling hazardous substances 7 7 14 11 21 39 6 5 28
Smoke 10 3 17 21 14 34 6 4 29
High humidity 3 14 14 21 10 38 6 4 29

Appendix 13. Summary of Results for Fire Safety Manager from Occupational Guidelines Questionnaire
2A-77
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Equipment usedFire-protective PersonnelProtective Equipment 36 18 14 4 0 29 1 2 28
Self-Contained Breathing Apparatus 14 14 10 14 14 34 6 4 29
Extended Duration Breathing Apparatus 4 4 14 14 14 50 6 6 28
Vibrating equipment 0 0 11 11 29 50 6 6 28
Computer 59 21 17 0 0 3 1 1 29
Telephone 62 21 14 3 0 0 1 1 29
Hand-held radio 21 17 21 7 7 28 6 3 29
Table 6: Near Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
BA control board-Old style MK 1 Read clock 10 90 2 2 29
BA control board-Old style MK 1 Graduations & cylinder pressure 7 93 2 2 29
BA tag Read tag 24 76 2 2 29
BA control board-New style MK 2 Read clock 14 86 2 2 29
BA control board-New style MK 2 Dial calculator 14 86 2 2 29
BA tag MK 2 Read tag 21 79 2 2 29
BA main control board Read clock 28 72 2 2 29
BA main control board Read 28 72 2 2 29
Sabre centurion Read BA graduations 14 86 2 2 29
Sabre centurion Read needle position 14 86 2 2 29
Siebe Gorman Read BA graduations 10 90 2 2 29
Siebe Gorman Read needle position 10 90 2 2 29
Drager Read BA graduations 21 79 2 2 29
Drager Read needle position 21 79 2 2 29
Philips PFX Handheld radio Read channel selector 31 69 2 2 29
Philips PFX Handheld radio Read numbered channel selector 31 69 2 2 29
BA log book Handwritten 24 76 2 2 29
Universal airline pack (Drager) BA supply BA cylinder gauge 3 97 2 2 29
Low pressure air bags Air pressure gauge 3 97 2 2 29
High pressure air bag Read graduations on console 3 97 2 2 29
High pressure air bag Needle position 3 97 2 2 29
Hurst high pressure lift bags Needle position 3 97 2 2 29
Microvent resuscitation equipment Read scale 3 97 2 2 29
Carmichael Godiva appliance Pressure gauge numbers 3 97 2 2 29
Saxon Volvo appliance pump Pressure gauge numbers 7 93 2 2 29
Dennis appliance pump Pressure gauge numbers 7 93 2 2 29
Read turnout sheet 10 90 2 2 29
Read dosimeter 14 86 2 2 29
Read survey meter 17 83 2 2 29
Read computer VDU 62 38 1 1 29
Read general paperwork 66 34 1 1 29
Read pager 41 59 2 2 29
Read mobile phone text 55 45 1 1 29
Read fire control panels 38 62 2 2 29
Read maps 62 38 1 1 29
Read fire extinguishers 38 62 2 2 29
Read plan inspections 45 55 2 2 29
Inspect premises 45 55 2 2 29
Read scale ruler 41 59 2 2 29
Read sound meter 17 83 2 2 29
Read light meter 17 83 2 2 29

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-78
Table 7: Distance Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
Street names White letters on a blue background 69 31 1 1 29
House numbers Copper figures on a blue background 55 45 1 1 29
House numbers White figures on a red background 55 45 1 1 29
Retail shop numbers Gold figures on a dark green background 66 34 1 1 29
House numbers Grey figures on a white background 55 45 1 1 29
Corporate building numbers Black figure on a silver background 62 38 1 1 29
Street names Black letters on a white background 72 28 1 1 29
House numbers Gold figures on a black background 55 45 1 1 29
House numbers Handpainted black figures on a white background 59 41 1 1 29
House numbers Gold figures on a black background 55 45 1 1 29
House numbers Black figures on a white background 55 45 1 1 29
Carmichael Godiva appliance pump Pressure gauge needle at rear of appliance 10 90 2 2 29
Carmichael Godiva appliance Measuring water in tank 7 93 2 2 29
Saxon Volvo appliance pump Pressure gauge needle at rear of appliance 7 93 2 2 29
Dennis appliance pump Pressure gauge needle at rear of appliance 10 90 2 2 29
Stop sign Road traffic signs 86 14 1 1 29
Give way sign Road traffic signs 86 14 1 1 29
One way street sign Road traffic signs 83 17 1 1 29
Chemical warning sign As EC Directive 92/58/EEC Hazardous substances 59 41 1 1 29
Vehicle signs Break lights/indicators on vehicles 86 14 1 1 29
Fire safety signs 86 14 1 1 29
Exit signs 86 14 1 1 29
Table 8: Hearing Tasks that are a requirement for role
Description Yes(1) No (2) Mode Median N
Distress signal unit 52 48 1 1 29
Warning whistle 55 45 1 1 29
Radio 66 34 1 1 29
Fireground orders 59 41 1 1 29
Evacuation signals/alarms 66 34 1 1 29
Telephone 97 3 1 1 29
Traffic 69 31 1 1 29
Vibraphone 10 90 2 2 29
Pager 52 48 1 1 29
Normal verbal communication with little background noise 90 10 1 1 29
Normal verbal communication with background noise 83 17 1 1 29
Hand clapping 41 59 2 2 29
Cries of help 59 41 1 1 29
Table 9: Other senses that are a requirement for role
Description Yes(1) No (2) Mode Median N
Touch 59 41 1 1 29
Smell 62 38 1 1 29
Taste 10 90 2 2 29

2A-79
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Sprinting 100 0 0 0 0 0 1 1 6
Running 100 0 0 0 0 0 1 1 6
Jogging 83 0 0 17 0 0 1 1 6
Walking 0 0 0 0 0 100 6 6 6
Climbing stairs 0 0 0 17 17 67 6 6 6
Climbing ladders 17 50 33 0 0 0 2 2 6
Crawling 50 33 17 0 0 0 1 2 6
Jumping 100 0 0 0 0 0 1 1 6
Hammering 100 0 0 0 0 0 1 1 6
Digging 83 0 17 0 0 0 1 1 6
Strength tasksLifting more than 5 kg or 11 pounds 17 0 33 33 0 17 3 4 6
Lifting more than 10 kg or 22 pounds 40 0 40 0 20 0 3 3 5
Lifting more than 20 kg or 44 pounds 60 20 0 20 0 0 1 1 5
Lifting more than 40 kg or 88 pounds 80 20 0 0 0 0 1 1 5
Carrying more than 5 kg or 11 pounds 40 20 0 20 0 20 1 2 5
Carrying more than 10 kg or 22 pounds 60 20 0 0 20 0 1 1 5
Carrying more than 20 kg or 44 pounds 60 40 0 0 0 0 1 1 5
Carrying more than 40 kg or 88 pounds 80 20 0 0 0 0 1 1 5
Pushing/pulling more than5 kg or 11 pounds 60 0 40 0 0 0 1 1 5
Pushing/pulling more than10 kg or 22 pounds 80 0 20 0 0 0 1 1 5
Pushing/pulling more than20 kg or 44 pounds 80 20 0 0 0 0 1 1 5
Pushing/pulling more than40 kg or 88 pounds 100 0 0 0 0 0 1 1 5
Static posturesStanding 0 0 0 0 0 100 6 6 6
Sitting 0 0 0 0 0 100 6 6 6
Squatting 20 0 0 20 60 0 5 5 5
Kneeling 20 20 20 20 20 0 #N/A 3 5
Lying down 80 20 0 0 0 0 1 1 5
Table 1: Respondents’ Details
Age Bracket 18-19(1) 20-29(2) 30-39(3) 40-49(4) 50+(5) Mode Median N0 0 0 100 0 4 4 6
Years of Service 0-4 (1) 5-9 (2) 10-14(3) 15-19(4) 20-24(5) 25+(6) Mode Median N0 0 0 17 33 50 6 6 6
Gender Male Female Mode Median N100 0 1 1 6
Employment Status Fulltime(1) Retained(2) Mode Median N100 0 1 1 6
Appendix 14. Summary of Results for Fire Safety Advisor/Engineer from Occupational Guidelines QuestionnaireNote: Results are displayed as a percentage of the total responses for each role, and as the mode, median and total number (N) ofrespondents for the role

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-80
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time) (continued)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Dynamic flexibility requirementsBending at waist 0 0 0 17 33 50 6 6 6
Reaching 0 0 17 0 17 67 6 6 6
Stooping 0 0 17 17 17 50 6 6 6
Turning/twisting 0 0 17 0 33 50 6 6 6
Object activitiesCatching 83 17 0 0 0 0 1 1 6
Throwing 83 0 17 0 0 0 1 1 6
Fine dexterity(eg writing, assembling equipment) 0 0 0 0 0 100 6 6 6
Foot control (eg driving) 0 0 0 0 17 83 6 6 6
Table 3: Importance respondents considered these activities to be to the effective performanceof their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Sprinting 0 0 17 0 17 67 6 6 6
Running 0 0 17 0 17 67 6 6 6
Jogging 0 0 17 0 17 67 6 6 6
Walking 83 17 0 0 0 0 1 1 6
Climbing stairs 100 0 0 0 0 0 1 1 6
Climbing ladders 33 17 33 17 0 0 1 3 6
Crawling 0 33 17 17 0 33 2 4 6
Jumping 0 17 0 17 17 50 6 6 6
Hammering 0 0 0 17 33 50 6 6 6
Digging 0 0 0 17 33 50 6 6 6
Strength tasksLifting more than 5 kg or 11 pounds 33 17 33 0 0 17 1 3 6
Lifting more than 10 kg or 22 pounds 17 17 17 17 0 33 6 4 6
Lifting more than 20 kg or 44 pounds 0 17 17 17 0 50 6 5 6
Lifting more than 40 kg or 88 pounds 0 0 17 17 17 50 6 6 6
Carrying more than 5 kg or 11 pounds 50 17 17 0 0 17 1 2 6
Carrying more than 10 kg or 22 pounds 17 33 17 17 0 17 2 3 6
Carrying more than 20 kg or 44 pounds 17 0 17 17 0 50 6 5 6
Carrying more than 40 kg or 88 pounds 0 0 17 17 17 50 6 6 6
Pushing/pulling more than5 kg or 11 pounds 17 17 0 0 33 33 6 5 6
Pushing/pulling more than10 kg or 22 pounds 17 17 17 0 33 17 5 4 6
Pushing/pulling more than20 kg or 44 pounds 17 0 0 0 33 50 6 6 6
Pushing/pulling more than40 kg or 88 pounds 0 0 17 0 33 50 6 6 6
Static posturesStanding 67 0 33 0 0 0 1 1 6
Sitting 83 0 17 0 0 0 1 1 6
Squatting 20 0 20 40 0 20 4 4 5
Kneeling 17 0 17 50 0 17 4 4 6
Lying down 17 0 0 17 33 33 5 5 6

Appendix 14. Summary of Results for Fire Safety Advisor/ Engineer from Occupational Guidelines Questionnaire
2A-81
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Handling hoses 83 17 0 0 0 0 1 1 6
Handling unconscious casualties 67 33 0 0 0 0 1 1 6
Handling ladders 67 33 0 0 0 0 1 1 6
Operating cutting equipment 83 17 0 0 0 0 1 1 6
Driving vehicles 0 0 0 0 0 100 6 6 6
Climbing ladders 17 33 50 0 0 0 3 3 6
Dealing with traumatised victims 50 33 17 0 0 0 1 2 6
Dealing with traumatised others(eg relatives, public) 40 20 20 20 0 0 1 2 5
Addressing groups of people 0 0 17 67 0 17 4 4 6
Filling in forms or completing paperwork 0 0 0 0 0 100 6 6 6
Making critical decisions quickly 20 0 0 20 0 60 6 6 5
Dealing with the media 0 33 33 33 0 0 4 3 6
Working on a computer 0 0 0 0 0 100 6 6 6
Communicating over the telephone 0 0 0 0 0 100 6 6 6
Environments encounteredFire compartment temperaturesabove 100˚C 83 0 17 0 0 0 1 1 6
Elevated temperatures (30-100˚C) 50 17 17 17 0 0 1 2 6
Freezing temperatures (sub-zero) 33 33 33 0 0 0 3 2 6
Dust 0 67 17 17 0 0 2 2 6
Overcrowding 17 33 33 17 0 0 3 3 6
Open spaces 17 0 17 67 0 0 4 4 6
Height 0 17 0 83 0 0 4 4 6
Enclosed spaces 17 17 17 50 0 0 4 4 6
Total darkness 33 33 17 17 0 0 1 2 6
Partial darkness 0 17 33 50 0 0 4 4 6
Working in water 83 0 17 0 0 0 1 1 6
Working under water 100 0 0 0 0 0 1 1 6
Handling hazardous substances 60 40 0 0 0 0 1 1 5
Smoke 67 17 17 0 0 0 1 1 6
High humidity 67 17 0 17 0 0 1 1 6
Table 3: Importance respondents considered these activities to be to the effective performanceof their role? (continued)
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Dynamic flexibility requirementsBending at waist 50 17 17 17 0 0 1 2 6
Reaching 33 17 33 17 0 0 1 3 6
Stooping 17 17 33 33 0 0 4 3 6
Turning/twisting 33 0 0 67 0 0 4 4 6
Object activitiesCatching 0 20 0 20 20 40 6 5 5
Throwing 0 20 0 20 20 40 6 5 5
Fine dexterity(eg writing, assembling equipment) 80 20 0 0 0 0 1 1 5
Foot control (eg driving) 100 0 0 0 0 0 1 1 5

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-82
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time) (continued)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Equipment usedFire-protective PersonnelProtective Equipment 17 33 33 17 0 0 2 3 6
Self-Contained Breathing Apparatus 83 17 0 0 0 0 1 1 6
Extended Duration Breathing Apparatus 100 0 0 0 0 0 1 1 6
Vibrating equipment 100 0 0 0 0 0 1 1 6
Computer 0 0 0 0 0 100 6 6 6
Telephone 0 0 0 0 0 100 6 6 6
Hand-held radio 17 33 33 0 17 0 3 3 6
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Handling hoses 17 0 17 0 17 50 6 6 6
Handling unconscious casualties 17 17 17 0 17 33 6 4 6
Handling ladders 17 0 17 17 17 33 6 5 6
Operating cutting equipment 17 0 17 0 17 50 6 6 6
Driving vehicles 100 0 0 0 0 0 1 1 6
Climbing ladders 17 50 17 17 0 0 2 2 6
Dealing with traumatised victims 33 0 33 17 0 17 1 3 6
Dealing with traumatised others(eg relatives, public) 33 0 33 17 0 17 1 3 6
Addressing groups of people 33 50 17 0 0 0 2 2 6
Filling in forms or completing paperwork 83 0 17 0 0 0 1 1 6
Making critical decisions quickly 67 0 17 17 0 0 1 1 6
Dealing with the media 17 17 67 0 0 0 3 3 6
Working on a computer 83 0 17 0 0 0 1 1 6
Communicating over the telephone 83 0 17 0 0 0 1 1 6
Environments encounteredFire compartment temperaturesabove 100˚C 17 17 0 0 17 50 6 6 6
Elevated temperatures (30-100˚C) 0 17 17 17 0 50 6 5 6
Freezing temperatures (sub-zero) 17 17 17 17 0 33 6 4 6
Dust 0 33 0 50 17 0 4 4 6
Overcrowding 50 17 17 0 17 0 1 2 6
Open spaces 17 17 50 0 0 17 3 3 6
Height 33 33 33 0 0 0 1 2 6
Enclosed spaces 50 0 33 17 0 0 1 2 6
Total darkness 50 0 17 17 0 17 1 2 6
Partial darkness 33 17 17 33 0 0 1 3 6
Working in water 33 0 0 0 17 50 6 6 6
Working under water 17 0 17 0 17 50 6 6 6
Handling hazardous substances 17 17 17 17 0 33 6 4 6
Smoke 17 17 0 17 0 50 6 5 6
High humidity 17 17 0 0 17 50 6 6 6

Appendix 14. Summary of Results for Fire Safety Advisor/ Engineer from Occupational Guidelines Questionnaire
2A-83
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Equipment usedFire-protective PersonnelProtective Equipment 40 40 20 0 0 0 1 2 5
Self-Contained Breathing Apparatus 40 20 0 20 0 20 1 2 5
Extended Duration Breathing Apparatus 40 0 0 40 0 20 1 4 5
Vibrating equipment 20 20 0 20 20 20 #N/A 4 5
Computer 80 0 0 20 0 0 1 1 5
Telephone 80 0 0 20 0 0 1 1 5
Hand-held radio 20 0 40 20 20 0 3 3 5
Table 6: Near Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
BA control board-Old style MK 1 Read clock 17 83 2 2 6
BA control board-Old style MK 1 Graduations & cylinder pressure 17 83 2 2 6
BA tag Read tag 17 83 2 2 6
BA control board-New style MK 2 Read clock 17 83 2 2 6
BA control board-New style MK 2 Dial calculator 17 83 2 2 6
BA tag MK 2 Read tag 17 83 2 2 6
BA main control board Read clock 17 83 2 2 6
BA main control board Read 17 83 2 2 6
Sabre centurion Read BA graduations 0 100 2 2 6
Sabre centurion Read needle position 0 100 2 2 6
Siebe Gorman Read BA graduations 17 83 2 2 6
Siebe Gorman Read needle position 17 83 2 2 6
Drager Read BA graduations 0 100 2 2 6
Drager Read needle position 17 83 2 2 6
Philips PFX Handheld radio Read channel selector 33 67 2 2 6
Philips PFX Handheld radio Read numbered channel selector 33 67 2 2 6
BA log book Handwritten 0 100 2 2 6
Universal airline pack (Drager) BA supply BA cylinder gauge 17 83 2 2 6
Low pressure air bags Air pressure gauge 17 83 2 2 6
High pressure air bag Read graduations on console 17 83 2 2 6
High pressure air bag Needle position 17 83 2 2 6
Hurst high pressure lift bags Needle position 0 100 2 2 6
Microvent resuscitation equipment Read scale 0 100 2 2 6
Carmichael Godiva appliance Pressure gauge numbers 0 100 2 2 6
Saxon Volvo appliance pump Pressure gauge numbers 17 83 2 2 6
Dennis appliance pump Pressure gauge numbers 17 83 2 2 6
Read turnout sheet 33 67 2 2 6
Read dosimeter 33 67 2 2 6
Read survey meter 33 67 2 2 6
Read computer VDU 83 17 1 1 6
Read general paperwork 83 17 1 1 6
Read pager 33 67 2 2 6
Read mobile phone text 50 50 1 2 6
Read fire control panels 33 67 2 2 6
Read maps 83 17 1 1 6
Read fire extinguishers 50 50 1 2 6
Read plan inspections 83 17 1 1 6
Inspect premises 67 33 1 1 6
Read scale ruler 83 17 1 1 6
Read sound meter 83 17 1 1 6
Read light meter 83 17 1 1 6

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-84
Table 7: Distance Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
Street names White letters on a blue background 100 0 1 1 6
House numbers Copper figures on a blue background 100 0 1 1 6
House numbers White figures on a red background 100 0 1 1 6
Retail shop numbers Gold figures on a dark green background 100 0 1 1 6
House numbers Grey figures on a white background 100 0 1 1 6
Corporate building numbers Black figure on a silver background 100 0 1 1 6
Street names Black letters on a white background 100 0 1 1 6
House numbers Gold figures on a black background 100 0 1 1 6
House numbers Handpainted black figures on a white background 100 0 1 1 6
House numbers Gold figures on a black background 100 0 1 1 6
House numbers Black figures on a white background 100 0 1 1 6
Carmichael Godiva appliance pump Pressure gauge needle at rear of appliance 0 100 2 2 6
Carmichael Godiva appliance Measuring water in tank 0 100 2 2 6
Saxon Volvo appliance pump Pressure gauge needle at rear of appliance 0 100 2 2 6
Dennis appliance pump Pressure gauge needle at rear of appliance 17 83 2 2 6
Stop sign Road traffic signs 100 0 1 1 6
Give way sign Road traffic signs 100 0 1 1 6
One way street sign Road traffic signs 100 0 1 1 6
Chemical warning sign As EC Directive 92/58/EEC Hazardous substances 50 50 1 2 6
Vehicle signs Break lights/indicators on vehicles 100 0 1 1 6
Fire safety signs 100 0 1 1 6
Exit signs 100 0 1 1 6
Table 8: Hearing Tasks that are a requirement for role
Description Yes(1) No (2) Mode Median N
Distress signal unit 33 67 2 2 6
Warning whistle 33 67 2 2 6
Radio 67 33 1 1 6
Fireground orders 33 67 2 2 6
Evacuation signals/alarms 100 0 1 1 6
Telephone 100 0 1 1 6
Traffic 100 0 1 1 6
Vibraphone 17 83 2 2 6
Pager 50 50 1 2 6
Normal verbal communication with little background noise 100 0 1 1 6
Normal verbal communication with background noise 100 0 1 1 6
Hand clapping 33 67 2 2 6
Cries of help 67 33 1 1 6
Table 9: Other senses that are a requirement for role
Description Yes(1) No (2) Mode Median N
Touch 83 17 1 1 6
Smell 33 67 2 2 6
Taste 17 83 2 2 6

2A-85
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Sprinting 89 0 0 11 0 0 1 1 9
Running 44 33 11 11 0 0 1 2 9
Jogging 33 0 33 22 11 0 1 3 9
Walking 0 0 10 10 10 70 6 6 10
Climbing stairs 0 0 0 10 10 80 6 6 10
Climbing ladders 11 22 44 11 11 0 3 3 9
Crawling 11 33 44 0 0 11 3 3 9
Jumping 67 11 0 11 11 0 1 1 9
Hammering 11 33 22 22 11 0 2 3 9
Digging 13 13 25 13 25 13 3 4 8
Strength tasksLifting more than 5 kg or 11 pounds 0 22 33 22 11 11 3 3 9
Lifting more than 10 kg or 22 pounds 13 38 13 25 13 0 2 3 8
Lifting more than 20 kg or 44 pounds 50 38 0 13 0 0 1 2 8
Lifting more than 40 kg or 88 pounds 57 29 14 0 0 0 1 1 7
Carrying more than 5 kg or 11 pounds 11 33 22 11 0 22 2 3 9
Carrying more than 10 kg or 22 pounds 13 38 13 25 13 0 2 3 8
Carrying more than 20 kg or 44 pounds 50 13 38 0 0 0 1 2 8
Carrying more than 40 kg or 88 pounds 75 13 13 0 0 0 1 1 8
Pushing/pulling more than5 kg or 11 pounds 33 22 33 0 0 11 1 2 9
Pushing/pulling more than10 kg or 22 pounds 38 25 25 13 0 0 1 2 8
Pushing/pulling more than20 kg or 44 pounds 50 13 25 13 0 0 1 2 8
Pushing/pulling more than40 kg or 88 pounds 75 13 13 0 0 0 1 1 8
Static posturesStanding 0 0 10 0 0 90 6 6 10
Sitting 0 0 10 0 0 90 6 6 10
Squatting 0 0 30 20 30 20 5 5 10
Kneeling 0 0 30 30 0 40 6 4 10
Lying down 40 10 0 20 10 20 1 3 10
Table 1: Respondents’ Details
Age Bracket 18-19(1) 20-29(2) 30-39(3) 40-49(4) 50+(5) Mode Median N0 0 30 70 0 4 4 10
Years of Service 0-4 (1) 5-9 (2) 10-14(3) 15-19(4) 20-24(5) 25+(6) Mode Median N0 0 20 20 30 30 6 5 10
Gender Male Female Mode Median N100 0 1 1 10
Employment Status Fulltime(1) Retained(2) Mode Median N100 0 1 1 10
Appendix 15. Summary of Results for Fire Investigatorfrom Occupational Guidelines QuestionnaireNote: Results are displayed as a percentage of the total responses for each role, and as the mode, median and total number (N) ofrespondents for the role

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-86
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time) (continued)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Dynamic flexibility requirementsBending at waist 0 0 22 0 44 33 5 5 9
Reaching 0 0 22 0 22 56 6 6 9
Stooping 0 0 22 0 33 44 6 5 9
Turning/twisting 0 0 22 0 44 33 5 5 9
Object activitiesCatching 60 10 20 0 10 0 1 1 10
Throwing 60 10 20 0 10 0 1 1 10
Fine dexterity(eg writing, assembling equipment) 0 0 10 0 0 90 6 6 10
Foot control (eg driving) 0 0 10 0 0 90 6 6 10
Table 3: Importance respondents considered these activities to be to the effective performanceof their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Sprinting 0 0 0 33 44 22 5 5 9
Running 0 11 0 44 44 0 4 4 9
Jogging 0 10 20 50 20 0 4 4 10
Walking 50 40 10 0 0 0 1 2 10
Climbing stairs 50 40 10 0 0 0 1 2 10
Climbing ladders 0 30 60 10 0 0 3 3 10
Crawling 0 10 60 20 10 0 3 3 10
Jumping 0 20 0 30 40 10 5 5 10
Hammering 0 20 20 30 30 0 5 4 10
Digging 10 20 30 20 20 0 3 3 10
Strength tasksLifting more than 5 kg or 11 pounds 30 10 40 10 10 0 3 3 10
Lifting more than 10 kg or 22 pounds 20 10 40 20 10 0 3 3 10
Lifting more than 20 kg or 44 pounds 0 11 22 44 22 0 4 4 9
Lifting more than 40 kg or 88 pounds 0 10 10 30 40 10 5 5 10
Carrying more than 5 kg or 11 pounds 20 10 40 20 10 0 3 3 10
Carrying more than 10 kg or 22 pounds 20 10 20 30 20 0 4 4 10
Carrying more than 20 kg or 44 pounds 0 10 30 40 10 10 4 4 10
Carrying more than 40 kg or 88 pounds 0 10 10 30 40 10 5 5 10
Pushing/pulling more than5 kg or 11 pounds 10 10 30 20 20 10 3 4 10
Pushing/pulling more than10 kg or 22 pounds 0 10 30 30 20 10 4 4 10
Pushing/pulling more than20 kg or 44 pounds 0 10 10 50 20 10 4 4 10
Pushing/pulling more than40 kg or 88 pounds 0 10 10 40 30 10 4 4 10
Static posturesStanding 40 40 20 0 0 0 1 2 10
Sitting 20 40 40 0 0 0 3 2 10
Squatting 10 40 30 20 0 0 2 3 10
Kneeling 20 40 20 10 10 0 2 2 10
Lying down 0 10 40 20 0 30 3 4 10

Appendix 15. Summary of Results for Fire Investigator from Occupational Guidelines Questionnaire
2A-87
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Handling hoses 40 40 10 10 0 0 1 2 10
Handling unconscious casualties 40 50 10 0 0 0 2 2 10
Handling ladders 30 50 10 10 0 0 2 2 10
Operating cutting equipment 50 30 10 0 0 10 1 2 10
Driving vehicles 0 10 10 0 10 70 6 6 10
Climbing ladders 30 10 50 0 10 0 3 3 10
Dealing with traumatised victims 0 40 20 10 20 10 2 3 10
Dealing with traumatised others(eg relatives, public) 11 22 33 11 11 11 3 3 9
Addressing groups of people 0 10 40 20 10 20 3 4 10
Filling in forms or completing paperwork 0 0 10 10 10 70 6 6 10
Making critical decisions quickly 10 0 20 20 20 30 6 5 10
Dealing with the media 20 20 30 0 20 10 3 3 10
Working on a computer 0 0 10 0 10 80 6 6 10
Communicating over the telephone 0 0 10 0 0 90 6 6 10
Environments encounteredFire compartment temperaturesabove 100˚C 50 30 0 10 10 0 1 2 10
Elevated temperatures (30-100˚C) 10 30 30 0 20 10 3 3 10
Freezing temperatures (sub-zero) 11 56 33 0 0 0 2 2 9
Dust 10 20 20 10 20 20 3 4 10
Overcrowding 44 22 11 11 11 0 1 2 9
Open spaces 0 33 44 0 11 11 3 3 9
Height 0 40 20 30 10 0 2 3 10
Enclosed spaces 11 44 11 22 11 0 2 2 9
Total darkness 40 40 10 0 10 0 1 2 10
Partial darkness 0 20 40 20 20 0 3 3 10
Working in water 60 30 0 10 0 0 1 1 10
Working under water 90 10 0 0 0 0 1 1 10
Handling hazardous substances 50 20 10 0 20 0 1 2 10
Smoke 0 33 22 33 0 11 2 3 9
High humidity 22 22 33 11 0 11 3 3 9
Table 3: Importance respondents considered these activities to be to the effective performanceof their role? (continued)
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Dynamic flexibility requirementsBending at waist 40 10 30 20 0 0 1 3 10
Reaching 40 10 30 20 0 0 1 3 10
Stooping 40 10 20 10 20 0 1 3 10
Turning/twisting 40 10 10 20 20 0 1 3 10
Object activitiesCatching 0 20 0 40 30 10 4 4 10
Throwing 0 20 0 40 30 10 4 4 10
Fine dexterity(eg writing, assembling equipment) 50 30 20 0 0 0 1 2 10
Foot control (eg driving) 50 30 20 0 0 0 1 2 10

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-88
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time) (continued)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Equipment usedFire-protective PersonnelProtective Equipment 0 0 30 20 30 20 3 5 10
Self-Contained Breathing Apparatus 30 70 0 0 0 0 2 2 10
Extended Duration Breathing Apparatus 100 0 0 0 0 0 1 1 10
Vibrating equipment 90 0 10 0 0 0 1 1 10
Computer 0 0 10 0 0 90 6 6 10
Telephone 0 0 10 0 0 90 6 6 10
Hand-held radio 10 0 40 10 10 30 3 4 10
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Handling hoses 0 0 11 67 11 11 4 4 9
Handling unconscious casualties 10 10 40 20 10 10 3 3 10
Handling ladders 0 0 60 20 10 10 3 3 10
Operating cutting equipment 0 0 20 60 10 10 4 4 10
Driving vehicles 80 0 20 0 0 0 1 1 10
Climbing ladders 10 40 30 10 10 0 2 3 10
Dealing with traumatised victims 20 30 20 20 0 10 2 3 10
Dealing with traumatised others(eg relatives, public) 20 40 20 20 0 0 2 2 10
Addressing groups of people 10 60 30 0 0 0 2 2 10
Filling in forms or completing paperwork 30 60 10 0 0 0 2 2 10
Making critical decisions quickly 50 20 20 10 0 0 1 2 10
Dealing with the media 0 30 50 0 10 10 3 3 10
Working on a computer 20 60 20 0 0 0 2 2 10
Communicating over the telephone 30 60 10 0 0 0 2 2 10
Environments encounteredFire compartment temperaturesabove 100˚C 0 20 20 40 20 0 4 4 10
Elevated temperatures (30-100˚C) 0 20 40 40 0 0 3 3 10
Freezing temperatures (sub-zero) 0 20 30 40 10 0 4 4 10
Dust 0 20 40 40 0 0 3 3 10
Overcrowding 0 10 0 70 10 10 4 4 10
Open spaces 0 20 40 30 10 0 3 3 10
Height 0 30 50 20 0 0 3 3 10
Enclosed spaces 0 20 50 20 10 0 3 3 10
Total darkness 0 20 30 50 0 0 4 4 10
Partial darkness 0 20 70 10 0 0 3 3 10
Working in water 0 10 10 50 10 20 4 4 10
Working under water 0 10 0 30 10 50 6 6 10
Handling hazardous substances 0 20 30 20 20 10 3 4 10
Smoke 0 30 30 30 10 0 3 3 10
High humidity 0 30 30 30 10 0 3 3 10

Appendix 15. Summary of Results for Fire Investigator from Occupational Guidelines Questionnaire
2A-89
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Equipment usedFire-protective PersonnelProtective Equipment 70 20 10 0 0 0 1 1 10
Self-Contained Breathing Apparatus 10 20 30 30 0 10 3 3 10
Extended Duration Breathing Apparatus 0 0 0 40 30 30 4 5 10
Vibrating equipment 0 10 10 30 20 30 4 5 10
Computer 30 60 10 0 0 0 2 2 10
Telephone 40 50 10 0 0 0 2 2 10
Hand-held radio 0 70 10 20 0 0 2 2 10
Table 6: Near Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
BA control board-Old style MK 1 Read clock 0 100 2 2 10
BA control board-Old style MK 1 Graduations & cylinder pressure 10 90 2 2 10
BA tag Read tag 0 100 2 2 10
BA control board-New style MK 2 Read clock 10 90 2 2 10
BA control board-New style MK 2 Dial calculator 10 90 2 2 10
BA tag MK 2 Read tag 0 100 2 2 10
BA main control board Read clock 10 90 2 2 10
BA main control board Read 10 90 2 2 10
Sabre centurion Read BA graduations 20 80 2 2 10
Sabre centurion Read needle position 20 80 2 2 10
Siebe Gorman Read BA graduations 10 90 2 2 10
Siebe Gorman Read needle position 10 90 2 2 10
Drager Read BA graduations 10 90 2 2 10
Drager Read needle position 20 80 2 2 10
Philips PFX Handheld radio Read channel selector 70 30 1 1 10
Philips PFX Handheld radio Read numbered channel selector 60 40 1 1 10
BA log book Handwritten 40 60 2 2 10
Universal airline pack (Drager) BA supply BA cylinder gauge 0 100 2 2 10
Low pressure air bags Air pressure gauge 0 100 2 2 10
High pressure air bag Read graduations on console 0 100 2 2 10
High pressure air bag Needle position 0 100 2 2 10
Hurst high pressure lift bags Needle position 0 100 2 2 10
Microvent resuscitation equipment Read scale 10 90 2 2 10
Carmichael Godiva appliance Pressure gauge numbers 0 100 2 2 10
Saxon Volvo appliance pump Pressure gauge numbers 0 100 2 2 10
Dennis appliance pump Pressure gauge numbers 0 100 2 2 10
Read turnout sheet 40 60 2 2 10
Read dosimeter 20 80 2 2 10
Read survey meter 10 90 2 2 10
Read computer VDU 50 50 1 2 10
Read general paperwork 60 40 1 1 10
Read pager 50 50 1 2 10
Read mobile phone text 50 50 1 2 10
Read fire control panels 40 60 2 2 10
Read maps 60 40 1 1 10
Read fire extinguishers 20 80 2 2 10
Read plan inspections 40 60 2 2 10
Inspect premises 50 50 1 2 10
Read scale ruler 40 60 2 2 10
Read sound meter 20 80 2 2 10
Read light meter 0 100 2 2 10

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-90
Table 7: Distance Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
Street names White letters on a blue background 90 10 1 1 10
House numbers Copper figures on a blue background 90 10 1 1 10
House numbers White figures on a red background 90 10 1 1 10
Retail shop numbers Gold figures on a dark green background 80 20 1 1 10
House numbers Grey figures on a white background 80 20 1 1 10
Corporate building numbers Black figure on a silver background 80 20 1 1 10
Street names Black letters on a white background 80 20 1 1 10
House numbers Gold figures on a black background 80 20 1 1 10
House numbers Handpainted black figures on a white background 90 10 1 1 10
House numbers Gold figures on a black background 90 10 1 1 10
House numbers Black figures on a white background 80 20 1 1 10
Carmichael Godiva appliance pump Pressure gauge needle at rear of appliance 0 100 2 2 10
Carmichael Godiva appliance Measuring water in tank 0 100 2 2 10
Saxon Volvo appliance pump Pressure gauge needle at rear of appliance 0 100 2 2 10
Dennis appliance pump Pressure gauge needle at rear of appliance 10 90 2 2 10
Stop sign Road traffic signs 90 10 1 1 10
Give way sign Road traffic signs 90 10 1 1 10
One way street sign Road traffic signs 80 20 1 1 10
Chemical warning sign As EC Directive 92/58/EEC Hazardous substances 80 20 1 1 10
Vehicle signs Break lights/indicators on vehicles 80 20 1 1 10
Fire safety signs 80 20 1 1 10
Exit signs 80 20 1 1 10
Table 8: Hearing Tasks that are a requirement for role
Description Yes(1) No (2) Mode Median N
Distress signal unit 60 40 1 1 10
Warning whistle 70 30 1 1 10
Radio 90 10 1 1 10
Fireground orders 90 10 1 1 10
Evacuation signals/alarms 90 10 1 1 10
Telephone 100 0 1 1 10
Traffic 90 10 1 1 10
Vibraphone 10 90 2 2 10
Pager 90 10 1 1 10
Normal verbal communication with little background noise 90 10 1 1 10
Normal verbal communication with background noise 100 0 1 1 10
Hand clapping 30 70 2 2 10
Cries of help 60 40 1 1 10
Table 9: Other senses that are a requirement for role
Description Yes(1) No (2) Mode Median N
Touch 90 10 1 1 10
Smell 80 20 1 1 10
Taste 40 60 2 2 10

2A-91
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Sprinting 88 6 6 0 0 0 1 1 16
Running 56 6 25 6 6 0 1 1 16
Jogging 63 0 13 19 6 0 1 1 16
Walking 0 0 0 0 0 100 6 6 17
Climbing stairs 0 0 0 5 5 89 6 6 19
Climbing ladders 35 35 24 6 0 0 1 2 17
Crawling 47 41 6 6 0 0 1 2 17
Jumping 56 31 6 0 6 0 1 1 16
Hammering 69 6 19 0 0 6 1 1 16
Digging 81 13 0 0 0 6 1 1 16
Strength tasksLifting more than 5 kg or 11 pounds 25 0 0 31 25 19 4 4 16
Lifting more than 10 kg or 22 pounds 25 0 25 31 19 0 4 4 16
Lifting more than 20 kg or 44 pounds 38 13 38 13 0 0 3 3 16
Lifting more than 40 kg or 88 pounds 56 38 6 0 0 0 1 1 16
Carrying more than 5 kg or 11 pounds 25 0 0 31 25 19 4 4 16
Carrying more than 10 kg or 22 pounds 24 6 18 35 18 0 4 4 17
Carrying more than 20 kg or 44 pounds 44 19 25 13 0 0 1 2 16
Carrying more than 40 kg or 88 pounds 63 31 6 0 0 0 1 1 16
Pushing/pulling more than5 kg or 11 pounds 31 13 19 25 6 6 1 3 16
Pushing/pulling more than10 kg or 22 pounds 38 13 25 19 6 0 1 3 16
Pushing/pulling more than20 kg or 44 pounds 44 38 19 0 0 0 1 2 16
Pushing/pulling more than40 kg or 88 pounds 63 25 13 0 0 0 1 1 16
Static posturesStanding 0 0 0 0 6 94 6 6 18
Sitting 0 0 0 0 0 100 6 6 19
Squatting 25 6 13 19 19 19 1 4 16
Kneeling 41 0 12 18 24 6 1 3 17
Lying down 81 13 0 0 6 0 1 1 16
Table 1: Respondents’ Details
Age Bracket 18-19(1) 20-29(2) 30-39(3) 40-49(4) 50+(5) Mode Median N0 0 22 56 22 4 4 18
Years of Service 0-4 (1) 5-9 (2) 10-14(3) 15-19(4) 20-24(5) 25+(6) Mode Median N0 5 16 16 26 37 6 5 19
Gender Male Female Mode Median N89 11 1 1 19
Employment Status Fulltime(1) Retained(2) Mode Median N100 0 1 1 18
Appendix 16. Summary of Results for TechnicalSupport from Occupational Guidelines QuestionnaireNote: Results are displayed as a percentage of the total responses for each role, and as the mode, median and total number (N) ofrespondents for the role

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-92
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time) (continued)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Dynamic flexibility requirementsBending at waist 6 0 0 6 18 71 6 6 17
Reaching 6 0 0 6 25 63 6 6 16
Stooping 6 0 0 6 19 69 6 6 16
Turning/twisting 7 0 0 0 7 87 6 6 15
Object activitiesCatching 69 0 13 6 13 0 1 1 16
Throwing 75 0 13 6 6 0 1 1 16
Fine dexterity(eg writing, assembling equipment) 0 0 0 0 0 100 6 6 19
Foot control (eg driving) 6 0 0 11 11 72 6 6 18
Table 3: Importance respondents considered these activities to be to the effective performanceof their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Sprinting 0 0 11 17 17 56 6 6 18
Running 0 0 22 11 17 50 6 6 18
Jogging 0 6 11 28 11 44 6 5 18
Walking 32 21 21 16 5 5 1 2 19
Climbing stairs 28 22 17 22 11 0 1 3 18
Climbing ladders 18 18 6 18 24 18 5 4 17
Crawling 0 6 18 12 35 29 5 5 17
Jumping 6 6 12 6 41 29 5 5 17
Hammering 0 0 6 24 29 41 6 5 17
Digging 0 0 6 18 35 41 6 5 17
Strength tasksLifting more than 5 kg or 11 pounds 13 13 47 13 7 7 3 3 15
Lifting more than 10 kg or 22 pounds 12 18 35 18 6 12 3 3 17
Lifting more than 20 kg or 44 pounds 0 19 13 50 6 13 4 4 16
Lifting more than 40 kg or 88 pounds 0 0 19 44 19 19 4 4 16
Carrying more than 5 kg or 11 pounds 13 13 38 13 6 19 3 3 16
Carrying more than 10 kg or 22 pounds 13 19 25 25 6 13 3 3 16
Carrying more than 20 kg or 44 pounds 0 25 6 50 6 13 4 4 16
Carrying more than 40 kg or 88 pounds 0 6 13 44 19 19 4 4 16
Pushing/pulling more than5 kg or 11 pounds 6 6 31 25 13 19 3 4 16
Pushing/pulling more than10 kg or 22 pounds 13 6 25 31 13 13 4 4 16
Pushing/pulling more than20 kg or 44 pounds 0 19 6 50 13 13 4 4 16
Pushing/pulling more than40 kg or 88 pounds 0 6 13 44 13 25 4 4 16
Static posturesStanding 28 22 28 17 0 6 1 3 18
Sitting 37 26 32 5 0 0 1 2 19
Squatting 12 12 18 18 29 12 5 4 17
Kneeling 6 18 12 29 24 12 4 4 17
Lying down 0 12 6 12 18 53 6 6 17

Appendix 16. Summary of Results for Technical Support from Occupational Guidelines Questionnaire
2A-93
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Handling hoses 44 17 33 6 0 0 1 2 18
Handling unconscious casualties 56 44 0 0 0 0 1 1 18
Handling ladders 56 33 11 0 0 0 1 1 18
Operating cutting equipment 72 11 17 0 0 0 1 1 18
Driving vehicles 5 0 0 26 5 63 6 6 19
Climbing ladders 44 28 28 0 0 0 1 2 18
Dealing with traumatised victims 56 33 11 0 0 0 1 1 18
Dealing with traumatised others(eg relatives, public) 50 22 28 0 0 0 1 2 18
Addressing groups of people 0 5 47 32 11 5 3 3 19
Filling in forms or completing paperwork 0 0 0 5 5 89 6 6 19
Making critical decisions quickly 5 0 26 5 37 26 5 5 19
Dealing with the media 26 32 26 5 11 0 2 2 19
Working on a computer 0 0 0 0 5 95 6 6 19
Communicating over the telephone 0 0 0 0 5 95 6 6 19
Environments encounteredFire compartment temperaturesabove 100˚C 56 39 6 0 0 0 1 1 18
Elevated temperatures (30-100˚C) 33 44 22 0 0 0 2 2 18
Freezing temperatures (sub-zero) 39 33 28 0 0 0 1 2 18
Dust 50 11 39 0 0 0 1 2 18
Overcrowding 67 22 11 0 0 0 1 1 18
Open spaces 33 0 56 6 0 6 3 3 18
Height 39 33 17 6 6 0 1 2 18
Enclosed spaces 39 33 17 0 11 0 1 2 18
Total darkness 44 39 17 0 0 0 1 2 18
Partial darkness 44 22 28 6 0 0 1 2 18
Working in water 83 11 6 0 0 0 1 1 18
Working under water 94 6 0 0 0 0 1 1 18
Handling hazardous substances 67 17 17 0 0 0 1 1 18
Smoke 28 39 28 6 0 0 2 2 18
High humidity 50 39 6 6 0 0 1 2 18
Table 3: Importance respondents considered these activities to be to the effective performanceof their role? (continued)
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Dynamic flexibility requirementsBending at waist 17 28 28 17 11 0 2 3 18
Reaching 22 28 22 17 11 0 2 3 18
Stooping 18 24 24 24 12 0 3 3 17
Turning/twisting 18 29 24 18 12 0 2 3 17
Object activitiesCatching 6 0 24 24 35 12 5 4 17
Throwing 0 6 18 29 29 18 5 4 17
Fine dexterity(eg writing, assembling equipment) 47 47 0 0 5 0 1 2 19
Foot control (eg driving) 44 33 11 0 6 6 1 2 18

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-94
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time) (continued)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Equipment usedFire-protective PersonnelProtective Equipment 28 22 28 22 0 0 3 3 18
Self-Contained Breathing Apparatus 50 39 6 6 0 0 1 2 18
Extended Duration Breathing Apparatus 94 6 0 0 0 0 1 1 18
Vibrating equipment 94 6 0 0 0 0 1 1 18
Computer 0 5 0 0 0 95 6 6 19
Telephone 0 0 0 0 0 100 6 6 19
Hand-held radio 26 11 16 37 0 11 4 3 19
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Handling hoses 0 6 11 22 33 28 5 5 18
Handling unconscious casualties 0 6 17 28 17 33 6 5 18
Handling ladders 0 6 11 28 22 33 6 5 18
Operating cutting equipment 0 6 6 22 33 33 5 5 18
Driving vehicles 37 16 32 5 0 11 1 2 19
Climbing ladders 6 11 22 17 17 28 6 4 18
Dealing with traumatised victims 0 11 39 11 17 22 3 4 18
Dealing with traumatised others(eg relatives, public) 0 22 28 11 17 22 3 4 18
Addressing groups of people 16 26 42 16 0 0 3 3 19
Filling in forms or completing paperwork 42 37 21 0 0 0 1 2 19
Making critical decisions quickly 26 47 16 5 5 0 2 2 19
Dealing with the media 0 32 37 11 11 11 3 3 19
Working on a computer 53 21 21 0 0 5 1 1 19
Communicating over the telephone 53 32 16 0 0 0 1 1 19
Environments encounteredFire compartment temperaturesabove 100˚C 0 11 11 11 17 50 6 6 18
Elevated temperatures (30-100˚C) 0 17 17 6 17 44 6 5 18
Freezing temperatures (sub-zero) 0 11 11 11 22 44 6 5 18
Dust 0 11 6 22 22 39 6 5 18
Overcrowding 0 6 6 22 28 39 6 5 18
Open spaces 0 11 11 17 22 39 6 5 18
Height 6 11 28 0 22 33 6 5 18
Enclosed spaces 6 11 22 6 22 33 6 5 18
Total darkness 6 6 22 11 22 33 6 5 18
Partial darkness 6 6 28 11 22 28 3 5 18
Working in water 0 6 12 12 24 47 6 5 17
Working under water 0 0 0 6 39 56 6 6 18
Handling hazardous substances 0 11 22 0 22 44 6 5 18
Smoke 6 11 22 6 22 33 6 5 18
High humidity 0 17 11 17 17 39 6 5 18

Appendix 16. Summary of Results for Technical Support from Occupational Guidelines Questionnaire
2A-95
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Equipment usedFire-protective PersonnelProtective Equipment 33 17 6 0 11 33 1 3 18
Self-Contained Breathing Apparatus 22 6 0 22 17 33 6 5 18
Extended Duration Breathing Apparatus 0 0 6 17 11 67 6 6 18
Vibrating equipment 0 0 11 17 11 61 6 6 18
Computer 53 32 16 0 0 0 1 1 19
Telephone 53 32 16 0 0 0 1 1 19
Hand-held radio 21 5 26 16 11 21 3 3 19
Table 6: Near Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
BA control board-Old style MK 1 Read clock 21 79 2 2 19
BA control board-Old style MK 1 Graduations & cylinder pressure 21 79 2 2 19
BA tag Read tag 21 79 2 2 19
BA control board-New style MK 2 Read clock 21 79 2 2 19
BA control board-New style MK 2 Dial calculator 21 79 2 2 19
BA tag MK 2 Read tag 21 79 2 2 19
BA main control board Read clock 26 74 2 2 19
BA main control board Read 26 74 2 2 19
Sabre centurion Read BA graduations 11 89 2 2 19
Sabre centurion Read needle position 11 89 2 2 19
Siebe Gorman Read BA graduations 5 95 2 2 19
Siebe Gorman Read needle position 5 95 2 2 19
Drager Read BA graduations 26 74 2 2 19
Drager Read needle position 26 74 2 2 19
Philips PFX Handheld radio Read channel selector 16 84 2 2 19
Philips PFX Handheld radio Read numbered channel selector 32 68 2 2 19
BA log book Handwritten 32 68 2 2 19
Universal airline pack (Drager) BA supply BA cylinder gauge 11 89 2 2 19
Low pressure air bags Air pressure gauge 16 84 2 2 19
High pressure air bag Read graduations on console 11 89 2 2 19
High pressure air bag Needle position 11 89 2 2 19
Hurst high pressure lift bags Needle position 11 89 2 2 19
Microvent resuscitation equipment Read scale 5 95 2 2 19
Carmichael Godiva appliance Pressure gauge numbers 5 95 2 2 19
Saxon Volvo appliance pump Pressure gauge numbers 5 95 2 2 19
Dennis appliance pump Pressure gauge numbers 5 95 2 2 19
Read turnout sheet 21 79 2 2 19
Read dosimeter 32 68 2 2 19
Read survey meter 37 63 2 2 19
Read computer VDU 74 26 1 1 19
Read general paperwork 79 21 1 1 19
Read pager 47 53 2 2 19
Read mobile phone text 47 53 2 2 19
Read fire control panels 26 74 2 2 19
Read maps 58 42 1 1 19
Read fire extinguishers 26 74 2 2 19
Read plan inspections 37 63 2 2 19
Inspect premises 37 63 2 2 19
Read scale ruler 26 74 2 2 19
Read sound meter 42 58 2 2 19
Read light meter 37 63 2 2 19

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-96
Table 7: Distance Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
Street names White letters on a blue background 47 53 2 2 19
House numbers Copper figures on a blue background 47 53 2 2 19
House numbers White figures on a red background 42 58 2 2 19
Retail shop numbers Gold figures on a dark green background 42 58 2 2 19
House numbers Grey figures on a white background 47 53 2 2 19
Corporate building numbers Black figure on a silver background 42 58 2 2 19
Street names Black letters on a white background 53 47 1 1 19
House numbers Gold figures on a black background 42 58 2 2 19
House numbers Handpainted black figures on a white background 47 53 2 2 19
House numbers Gold figures on a black background 42 58 2 2 19
House numbers Black figures on a white background 47 53 2 2 19
Carmichael Godiva appliance pump Pressure gauge needle at rear of appliance 11 89 2 2 19
Carmichael Godiva appliance Measuring water in tank 5 95 2 2 19
Saxon Volvo appliance pump Pressure gauge needle at rear of appliance 5 95 2 2 19
Dennis appliance pump Pressure gauge needle at rear of appliance 5 95 2 2 19
Stop sign Road traffic signs 84 16 1 1 19
Give way sign Road traffic signs 84 16 1 1 19
One way street sign Road traffic signs 84 16 1 1 19
Chemical warning sign As EC Directive 92/58/EEC Hazardous substances 47 53 2 2 19
Vehicle signs Break lights/indicators on vehicles 84 16 1 1 19
Fire safety signs 84 16 1 1 19
Exit signs 84 16 1 1 19
Table 8: Hearing Tasks that are a requirement for role
Description Yes(1) No (2) Mode Median N
Distress signal unit 47 53 2 2 19
Warning whistle 47 53 2 2 19
Radio 63 37 1 1 19
Fireground orders 47 53 2 2 19
Evacuation signals/alarms 58 42 1 1 19
Telephone 100 0 1 1 19
Traffic 89 11 1 1 19
Vibraphone 16 84 2 2 19
Pager 63 37 1 1 19
Normal verbal communication with little background noise 100 0 1 1 19
Normal verbal communication with background noise 84 16 1 1 19
Hand clapping 32 68 2 2 19
Cries of help 47 53 2 2 19
Table 9: Other senses that are a requirement for role
Description Yes(1) No (2) Mode Median N
Touch 58 42 1 1 19
Smell 53 47 1 1 19
Taste 32 68 2 2 19

2A-97
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Sprinting 66 11 9 9 3 3 1 1 35
Running 34 11 26 11 11 6 1 3 35
Jogging 32 9 18 21 12 9 1 3 34
Walking 3 0 0 0 11 86 6 6 35
Climbing stairs 8 0 0 0 6 86 6 6 36
Climbing ladders 14 6 39 28 8 6 3 3 36
Crawling 22 6 36 28 6 3 3 3 36
Jumping 46 14 26 11 3 0 1 2 35
Hammering 44 28 19 8 0 0 1 2 36
Digging 64 14 17 6 0 0 1 1 36
Strength tasksLifting more than 5 kg or 11 pounds 0 3 12 26 21 38 6 5 34
Lifting more than 10 kg or 22 pounds 0 3 12 35 21 29 4 5 34
Lifting more than 20 kg or 44 pounds 0 6 26 26 29 12 5 4 34
Lifting more than 40 kg or 88 pounds 11 17 23 31 11 6 4 3 35
Carrying more than 5 kg or 11 pounds 0 3 15 21 29 32 6 5 34
Carrying more than 10 kg or 22 pounds 3 0 18 26 26 26 5 5 34
Carrying more than 20 kg or 44 pounds 9 9 26 26 26 3 4 4 34
Carrying more than 40 kg or 88 pounds 18 18 24 24 15 3 3 3 34
Pushing/pulling more than 5 kg or 11 pounds 9 9 12 24 26 21 5 4 34
Pushing/pulling more than10 kg or 22 pounds 9 6 24 21 24 15 5 4 33
Pushing/pulling more than20 kg or 44 pounds 15 12 24 24 21 6 4 4 34
Pushing/pulling more than40 kg or 88 pounds 23 14 20 26 14 3 4 3 35
Static posturesStanding 0 0 0 0 6 94 6 6 36
Sitting 0 0 0 3 8 89 6 6 36
Squatting 8 0 11 25 31 25 5 5 36
Kneeling 6 0 11 31 31 22 4 5 36
Lying down 43 11 34 6 6 0 1 2 35
Table 1: Respondents’ Details
Age Bracket 18-19(1) 20-29(2) 30-39(3) 40-49(4) 50+(5) Mode Median N0 3 44 36 17 3 4 36
Years of Service 0-4 (1) 5-9 (2) 10-14(3) 15-19(4) 20-24(5) 25+(6) Mode Median N0 11 33 14 14 28 3 4 36
Gender Male Female Mode Median N97 3 1 1 36
Employment Status Fulltime(1) Retained(2) Mode Median N100 0 1 1 36
Appendix 17. Summary of Results for Trainer fromOccupational Guidelines QuestionnaireNote: Results are displayed as a percentage of the total responses for each role, and as the mode, median and total number (N) ofrespondents for the role

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-98
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time) (continued)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Dynamic flexibility requirementsBending at waist 6 3 0 6 9 77 6 6 35
Reaching 0 3 3 3 14 77 6 6 35
Stooping 0 3 6 12 18 62 6 6 34
Turning/twisting 0 0 3 3 12 82 6 6 34
Object activitiesCatching 38 15 24 18 6 0 1 2 34
Throwing 29 17 17 23 6 9 1 3 35
Fine dexterity(eg writing, assembling equipment) 0 0 0 3 9 89 6 6 35
Foot control (eg driving) 0 0 0 11 20 69 6 6 35
Table 3: Importance respondents considered these activities to be to the effective performanceof their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Sprinting 3 6 17 23 20 31 6 5 35
Running 3 17 37 17 6 20 3 3 35
Jogging 9 26 32 6 12 15 3 3 34
Walking 60 23 14 3 0 0 1 1 35
Climbing stairs 63 20 6 6 6 0 1 1 35
Climbing ladders 62 9 18 9 0 3 1 1 34
Crawling 44 12 18 3 12 12 1 2 34
Jumping 20 0 29 20 14 17 3 4 35
Hammering 3 9 31 17 9 31 6 4 35
Digging 3 14 20 17 9 37 6 4 35
Strength tasksLifting more than 5 kg or 11 pounds 57 17 14 6 6 0 1 1 35
Lifting more than 10 kg or 22 pounds 57 14 17 6 6 0 1 1 35
Lifting more than 20 kg or 44 pounds 40 31 14 9 6 0 1 2 35
Lifting more than 40 kg or 88 pounds 23 11 40 11 9 6 3 3 35
Carrying more than 5 kg or 11 pounds 54 20 14 3 9 0 1 1 35
Carrying more than 10 kg or 22 pounds 54 17 17 3 9 0 1 1 35
Carrying more than 20 kg or 44 pounds 37 34 14 6 9 0 1 2 35
Carrying more than 40 kg or 88 pounds 24 15 35 15 12 0 3 3 34
Pushing/pulling more than5 kg or 11 pounds 46 17 20 6 11 0 1 2 35
Pushing/pulling more than10 kg or 22 pounds 43 17 23 6 11 0 1 2 35
Pushing/pulling more than20 kg or 44 pounds 37 17 23 11 9 3 1 2 35
Pushing/pulling more than40 kg or 88 pounds 23 17 26 20 9 6 3 3 35
Static posturesStanding 56 32 9 3 0 0 1 1 34
Sitting 47 32 15 6 0 0 1 2 34
Squatting 36 15 27 9 6 6 1 2 33
Kneeling 34 17 29 9 6 6 1 2 35
Lying down 9 12 29 12 9 29 6 4 34

Appendix 17. Summary of Results for Trainer from Occupational Guidelines Questionnaire
2A-99
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Handling hoses 9 9 18 26 24 15 4 4 34
Handling unconscious casualties 42 25 17 8 6 3 1 2 36
Handling ladders 11 11 28 33 8 8 4 4 36
Operating cutting equipment 14 19 25 25 11 6 3 3 36
Driving vehicles 3 3 3 19 25 47 6 5 36
Climbing ladders 11 11 31 31 8 8 3 3 36
Dealing with traumatised victims 56 28 14 0 3 0 1 1 36
Dealing with traumatised others(eg relatives, public) 54 34 6 0 6 0 1 1 35
Addressing groups of people 0 0 3 11 19 67 6 6 36
Filling in forms or completing paperwork 0 0 0 0 11 89 6 6 35
Making critical decisions quickly 6 6 8 11 31 39 6 5 36
Dealing with the media 61 22 8 8 0 0 1 1 36
Working on a computer 0 0 0 0 11 89 6 6 36
Communicating over the telephone 0 0 0 0 8 92 6 6 36
Environments encounteredFire compartment temperaturesabove 100˚C 25 0 28 22 11 14 3 3 36
Elevated temperatures (30-100˚C) 14 3 22 33 14 14 4 4 36
Freezing temperatures (sub-zero) 33 53 6 6 3 0 2 2 36
Dust 28 8 22 19 11 11 1 3 36
Overcrowding 44 19 6 3 14 14 1 2 36
Open spaces 11 6 9 20 26 29 6 5 35
Height 11 6 20 34 17 11 4 4 35
Enclosed spaces 11 11 14 39 11 14 4 4 36
Total darkness 14 8 11 36 19 11 4 4 36
Partial darkness 19 3 11 33 17 17 4 4 36
Working in water 53 28 11 6 0 3 1 1 36
Working under water 94 6 0 0 0 0 1 1 36
Handling hazardous substances 39 25 19 11 6 0 1 2 36
Smoke 11 9 14 31 17 17 4 4 35
High humidity 19 14 17 28 14 8 4 4 36
Table 3: Importance respondents considered these activities to be to the effective performanceof their role? (continued)
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Dynamic flexibility requirementsBending at waist 43 29 23 3 0 3 1 2 35
Reaching 43 26 29 3 0 0 1 2 35
Stooping 40 26 26 3 6 0 1 2 35
Turning/twisting 43 26 29 3 0 0 1 2 35
Object activitiesCatching 17 9 23 20 9 23 6 4 35
Throwing 17 9 29 20 6 20 3 3 35
Fine dexterity(eg writing, assembling equipment) 46 23 26 3 3 0 1 2 35
Foot control (eg driving) 51 23 23 0 3 0 1 1 35

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-100
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time) (continued)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Equipment usedFire-protective PersonnelProtective Equipment 6 3 9 14 29 40 6 5 35
Self-Contained Breathing Apparatus 17 6 11 31 19 17 4 4 36
Extended Duration Breathing Apparatus 97 3 0 0 0 0 1 1 35
Vibrating equipment 53 11 19 6 8 3 1 1 36
Computer 0 0 0 0 17 83 6 6 36
Telephone 0 0 0 0 8 92 6 6 36
Hand-held radio 11 3 11 28 17 31 6 4 36
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Handling hoses 53 14 14 11 0 8 1 1 36
Handling unconscious casualties 42 14 17 3 0 25 1 2 36
Handling ladders 56 11 14 11 0 8 1 1 36
Operating cutting equipment 53 17 11 8 3 8 1 1 36
Driving vehicles 53 17 22 6 3 0 1 1 36
Climbing ladders 56 17 11 8 0 8 1 1 36
Dealing with traumatised victims 36 17 19 3 0 25 1 2 36
Dealing with traumatised others(eg relatives, public) 33 14 25 3 0 25 1 3 36
Addressing groups of people 47 22 31 0 0 0 1 2 36
Filling in forms or completing paperwork 29 26 40 6 0 0 3 2 35
Making critical decisions quickly 46 29 20 3 0 3 1 2 35
Dealing with the media 14 11 23 26 3 23 4 4 35
Working on a computer 33 19 44 3 0 0 3 2 36
Communicating over the telephone 39 22 36 3 0 0 1 2 36
Environments encounteredFire compartment temperaturesabove 100˚C 53 17 14 6 6 6 1 1 36
Elevated temperatures (30-100˚C) 50 14 22 3 6 6 1 2 36
Freezing temperatures (sub-zero) 28 6 11 19 22 14 1 4 36
Dust 28 11 28 22 3 8 3 3 36
Overcrowding 25 8 31 19 6 11 3 3 36
Open spaces 28 8 28 17 11 8 3 3 36
Height 53 17 19 3 6 3 1 1 36
Enclosed spaces 58 11 19 3 3 6 1 1 36
Total darkness 53 17 14 8 6 3 1 1 36
Partial darkness 53 14 17 8 6 3 1 1 36
Working in water 28 17 25 6 6 19 1 3 36
Working under water 8 6 14 19 19 33 6 5 36
Handling hazardous substances 31 25 17 11 6 11 1 2 36
Smoke 58 17 17 3 3 3 1 1 36
High humidity 53 14 14 6 8 6 1 1 36

Appendix 17. Summary of Results for Trainer from Occupational Guidelines Questionnaire
2A-101
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Equipment usedFire-protective PersonnelProtective Equipment 72 14 8 0 0 6 1 1 36
Self-Contained Breathing Apparatus 67 11 8 0 3 11 1 1 36
Extended Duration Breathing Apparatus 6 8 8 17 6 56 6 6 36
Vibrating equipment 25 14 25 14 3 19 3 3 36
Computer 36 22 33 8 0 0 1 2 36
Telephone 33 25 36 6 0 0 3 2 36
Hand-held radio 33 33 19 6 0 8 1 2 36
Table 6: Near Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
BA control board-Old style MK 1 Read clock 75 25 1 1 36
BA control board-Old style MK 1 Graduations & cylinder pressure 75 25 1 1 36
BA tag Read tag 78 22 1 1 36
BA control board-New style MK 2 Read clock 64 36 1 1 36
BA control board-New style MK 2 Dial calculator 58 42 1 1 36
BA tag MK 2 Read tag 58 42 1 1 36
BA main control board Read clock 69 31 1 1 36
BA main control board Read 72 28 1 1 36
Sabre centurion Read BA graduations 25 75 2 2 36
Sabre centurion Read needle position 25 75 2 2 36
Siebe Gorman Read BA graduations 14 86 2 2 36
Siebe Gorman Read needle position 11 89 2 2 36
Drager Read BA graduations 47 53 2 2 36
Drager Read needle position 44 56 2 2 36
Philips PFX Handheld radio Read channel selector 50 50 2 2 36
Philips PFX Handheld radio Read numbered channel selector 56 44 1 1 36
BA log book Handwritten 72 28 1 1 36
Universal airline pack (Drager) BA supply BA cylinder gauge 33 67 2 2 36
Low pressure air bags Air pressure gauge 47 53 2 2 36
High pressure air bag Read graduations on console 47 53 2 2 36
High pressure air bag Needle position 44 56 2 2 36
Hurst high pressure lift bags Needle position 22 78 2 2 36
Microvent resuscitation equipment Read scale 22 78 2 2 36
Carmichael Godiva appliance Pressure gauge numbers 42 58 2 2 36
Saxon Volvo appliance pump Pressure gauge numbers 44 56 2 2 36
Dennis appliance pump Pressure gauge numbers 50 50 1 2 36
Read turnout sheet 36 64 2 2 36
Read dosimeter 39 61 2 2 36
Read survey meter 39 61 2 2 36
Read computer VDU 89 11 1 1 36
Read general paperwork 86 14 1 1 36
Read pager 33 67 2 2 36
Read mobile phone text 50 50 2 2 36
Read fire control panels 39 61 2 2 36
Read maps 56 44 1 1 36
Read fire extinguishers 50 50 2 2 36
Read plan inspections 31 69 2 2 36
Inspect premises 25 75 2 2 36
Read scale ruler 11 89 2 2 36
Read sound meter 11 89 2 2 36
Read light meter 8 92 2 2 36

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-102
Table 7: Distance Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
Street names White letters on a blue background 33 67 2 2 36
House numbers Copper figures on a blue background 28 72 2 2 36
House numbers White figures on a red background 28 72 2 2 36
Retail shop numbers Gold figures on a dark green background 31 69 2 2 36
House numbers Grey figures on a white background 31 69 2 2 36
Corporate building numbers Black figure on a silver background 42 58 2 2 36
Street names Black letters on a white background 44 56 2 2 36
House numbers Gold figures on a black background 33 67 2 2 36
House numbers Handpainted black figures on a white background 31 69 2 2 36
House numbers Gold figures on a black background 33 67 2 2 36
House numbers Black figures on a white background 33 67 2 2 36
Carmichael Godiva appliance pump Pressure gauge needle at rear of appliance 47 53 2 2 36
Carmichael Godiva appliance Measuring water in tank 42 58 2 2 36
Saxon Volvo appliance pump Pressure gauge needle at rear of appliance 44 56 2 2 36
Dennis appliance pump Pressure gauge needle at rear of appliance 50 50 2 2 36
Stop sign Road traffic signs 75 25 1 1 36
Give way sign Road traffic signs 78 22 1 1 36
One way street sign Road traffic signs 81 19 1 1 36
Chemical warning sign As EC Directive 92/58/EEC Hazardous substances 53 47 1 1 36
Vehicle signs Break lights/indicators on vehicles 83 17 1 1 36
Fire safety signs 75 25 1 1 36
Exit signs 69 31 1 1 36
Table 8: Hearing Tasks that are a requirement for role
Description Yes(1) No (2) Mode Median N
Distress signal unit 83 17 1 1 36
Warning whistle 86 14 1 1 36
Radio 83 17 1 1 36
Fireground orders 78 22 1 1 36
Evacuation signals/alarms 89 11 1 1 36
Telephone 97 3 1 1 36
Traffic 81 19 1 1 36
Vibraphone 17 83 2 2 36
Pager 36 64 2 2 36
Normal verbal communication with little background noise 94 6 1 1 36
Normal verbal communication with background noise 94 6 1 1 36
Hand clapping 83 17 1 1 36
Cries of help 89 11 1 1 36
Table 9: Other senses that are a requirement for role
Description Yes(1) No (2) Mode Median N
Touch 92 8 1 1 36
Smell 72 28 1 1 36
Taste 25 75 2 2 36

2A-103
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Sprinting 89 0 11 0 0 0 1 1 19
Running 53 16 16 5 11 0 1 1 19
Jogging 40 10 20 20 5 5 1 3 20
Walking 5 0 0 5 10 81 6 6 21
Climbing stairs 5 0 0 0 10 86 6 6 21
Climbing ladders 20 40 30 10 0 0 2 2 20
Crawling 45 25 25 5 0 0 1 2 20
Jumping 75 10 5 10 0 0 1 1 20
Hammering 70 10 15 5 0 0 1 1 20
Digging 70 15 10 5 0 0 1 1 20
Strength tasksLifting more than 5 kg or 11 pounds 24 10 5 29 19 14 4 4 21
Lifting more than 10 kg or 22 pounds 30 10 5 30 25 0 4 4 20
Lifting more than 20 kg or 44 pounds 50 10 10 25 5 0 1 2 20
Lifting more than 40 kg or 88 pounds 60 20 15 5 0 0 1 1 20
Carrying more than 5 kg or 11 pounds 30 5 10 30 5 20 1 4 20
Carrying more than 10 kg or 22 pounds 35 10 10 30 10 5 1 3 20
Carrying more than 20 kg or 44 pounds 45 15 20 20 0 0 1 2 20
Carrying more than 40 kg or 88 pounds 45 25 15 15 0 0 1 2 20
Pushing/pulling more than5 kg or 11 pounds 35 15 5 20 15 10 1 3 20
Pushing/pulling more than10 kg or 22 pounds 50 15 10 10 10 5 1 2 20
Pushing/pulling more than20 kg or 44 pounds 60 15 5 15 5 0 1 1 20
Pushing/pulling more than40 kg or 88 pounds 60 20 10 10 0 0 1 1 20
Static posturesStanding 0 0 0 10 0 90 6 6 20
Sitting 0 0 0 5 0 95 6 6 20
Squatting 35 0 5 20 35 5 1 4 20
Kneeling 25 5 20 15 25 10 5 4 20
Lying down 65 0 5 10 15 5 1 1 20
Table 1: Respondents’ Details
Age Bracket 18-19(1) 20-29(2) 30-39(3) 40-49(4) 50+(5) Mode Median N0 0 18 64 18 4 4 22
Years of Service 0-4 (1) 5-9 (2) 10-14(3) 15-19(4) 20-24(5) 25+(6) Mode Median N0 0 5 50 14 32 4 4 22
Gender Male Female Mode Median N100 0 1 1 22
Employment Status Fulltime(1) Retained(2) Mode Median N100 0 1 1 20
Appendix 18. Summary of Results for Training Managerfrom Occupational Guidelines QuestionnaireNote: Results are displayed as a percentage of the total responses for each role, and as the mode, median and total number (N) ofrespondents for the role

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-104
Table 2: Frequency respondents perform the following activities in a typical year (excluding activities performed during training or leisure time) (continued)
Movements Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Dynamic flexibility requirementsBending at waist 5 0 5 10 20 60 6 6 20
Reaching 15 0 5 10 15 55 6 6 20
Stooping 20 0 0 15 30 35 6 5 20
Turning/twisting 10 0 0 15 0 75 6 6 20
Object activitiesCatching 63 0 11 21 0 5 1 1 19
Throwing 65 0 10 20 0 5 1 1 20
Fine dexterity(eg writing, assembling equipment) 0 0 0 0 0 100 6 6 20
Foot control (eg driving) 5 0 0 5 10 80 6 6 20
Table 3: Importance respondents considered these activities to be to the effective performanceof their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Sprinting 0 5 0 20 30 45 6 5 20
Running 5 5 29 14 19 29 6 4 21
Jogging 0 17 28 17 11 28 6 4 18
Walking 62 14 19 5 0 0 1 1 21
Climbing stairs 48 14 24 10 5 0 1 2 21
Climbing ladders 24 10 10 38 5 14 4 4 21
Crawling 19 5 19 24 10 24 4 4 21
Jumping 5 10 5 29 19 33 6 5 21
Hammering 5 0 10 19 29 38 6 5 21
Digging 5 0 10 19 29 38 6 5 21
Strength tasksLifting more than 5 kg or 11 pounds 19 14 24 19 10 14 3 3 21
Lifting more than 10 kg or 22 pounds 14 14 29 24 5 14 3 3 21
Lifting more than 20 kg or 44 pounds 10 14 24 19 10 24 6 4 21
Lifting more than 40 kg or 88 pounds 0 14 19 29 14 24 4 4 21
Carrying more than 5 kg or 11 pounds 10 20 25 20 10 15 3 3 20
Carrying more than 10 kg or 22 pounds 19 14 24 19 10 14 3 3 21
Carrying more than 20 kg or 44 pounds 5 19 19 14 19 24 6 4 21
Carrying more than 40 kg or 88 pounds 0 14 19 24 19 24 6 4 21
Pushing/pulling more than5 kg or 11 pounds 10 19 19 19 19 14 3 4 21
Pushing/pulling more than10 kg or 22 pounds 5 19 24 19 14 19 3 4 21
Pushing/pulling more than20 kg or 44 pounds 5 14 24 14 19 24 6 4 21
Pushing/pulling more than40 kg or 88 pounds 5 14 14 24 19 24 6 4 21
Static posturesStanding 33 29 29 0 0 10 1 2 21
Sitting 43 19 24 5 0 10 1 2 21
Squatting 5 24 29 14 14 14 3 3 21
Kneeling 0 29 24 14 14 19 2 3 21
Lying down 5 14 14 10 14 43 6 5 21

Appendix 18. Summary of Results for Training Manager from Occupational Guidelines Questionnaire
2A-105
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Handling hoses 43 29 24 5 0 0 1 2 21
Handling unconscious casualties 76 19 5 0 0 0 1 1 21
Handling ladders 43 24 29 5 0 0 1 2 21
Operating cutting equipment 43 19 19 14 0 5 1 2 21
Driving vehicles 5 10 10 5 5 67 6 6 21
Climbing ladders 29 38 29 5 0 0 2 2 21
Dealing with traumatised victims 38 43 14 5 0 0 2 2 21
Dealing with traumatised others(eg relatives, public) 48 33 14 0 5 0 1 2 21
Addressing groups of people 0 0 19 33 5 43 6 4 21
Filling in forms or completing paperwork 0 0 0 0 10 90 6 6 21
Making critical decisions quickly 0 5 10 19 19 48 6 5 21
Dealing with the media 5 43 43 5 0 5 3 3 21
Working on a computer 0 0 0 0 0 100 6 6 20
Communicating over the telephone 0 0 0 0 0 100 6 6 21
Environments encounteredFire compartment temperaturesabove 100˚C 40 35 10 15 0 0 1 2 20
Elevated temperatures (30-100˚C) 30 40 15 15 0 0 2 2 20
Freezing temperatures (sub-zero) 38 62 0 0 0 0 2 2 21
Dust 32 37 16 11 5 0 2 2 19
Overcrowding 55 35 0 5 5 0 1 1 20
Open spaces 19 33 14 10 5 19 2 2 21
Height 24 24 33 19 0 0 3 3 21
Enclosed spaces 19 43 19 14 0 5 2 2 21
Total darkness 38 33 19 10 0 0 1 2 21
Partial darkness 14 33 29 19 5 0 2 3 21
Working in water 76 14 5 5 0 0 1 1 21
Working under water 95 5 0 0 0 0 1 1 21
Handling hazardous substances 67 29 5 0 0 0 1 1 21
Smoke 24 43 19 10 5 0 2 2 21
High humidity 43 33 10 14 0 0 1 2 21
Table 3: Importance respondents considered these activities to be to the effective performanceof their role? (continued)
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Dynamic flexibility requirementsBending at waist 24 14 38 10 5 10 3 3 21
Reaching 24 19 29 5 10 14 3 3 21
Stooping 19 14 19 19 19 10 5 3 21
Turning/twisting 29 24 24 5 5 14 1 2 21
Object activitiesCatching 10 14 14 5 14 43 6 5 21
Throwing 10 14 19 0 14 43 6 5 21
Fine dexterityeg writing, assembling equipment) 43 38 14 0 0 5 1 2 21
Foot control (eg driving) 43 19 29 0 0 10 1 2 21

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-106
Table 4: Frequency respondents performed these activities in a typical year(excluding activities performed during training or leisure time) (continued)
Tasks Not at Once per Once per Once per Once per Many times Mode Median Nall (1) year (2) month (3) week(4) day (5) per day (6)
Equipment usedFire-protective PersonnelProtective Equipment 0 0 43 48 10 0 4 4 21
Self-Contained Breathing Apparatus 29 48 10 10 5 0 2 2 21
Extended Duration Breathing Apparatus 95 0 0 5 0 0 1 1 21
Vibrating equipment 90 10 0 0 0 0 1 1 21
Computer 0 0 0 0 0 100 6 6 21
Telephone 0 0 0 0 0 100 6 6 21
Hand-held radio 0 10 24 43 10 14 4 4 21
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Handling hoses 19 10 10 24 19 19 4 4 21
Handling unconscious casualties 19 5 19 24 14 19 4 4 21
Handling ladders 19 10 14 19 19 19 6 4 21
Operating cutting equipment 14 14 14 19 19 19 6 4 21
Driving vehicles 52 19 14 5 0 10 1 1 21
Climbing ladders 14 14 33 10 10 19 3 3 21
Dealing with traumatised victims 10 29 33 10 0 19 3 3 21
Dealing with traumatised others(eg relatives, public) 5 29 33 10 0 24 3 3 21
Addressing groups of people 33 43 19 0 0 5 2 2 21
Filling in forms or completing paperwork 38 38 14 5 5 0 2 2 21
Making critical decisions quickly 71 14 14 0 0 0 1 1 21
Dealing with the media 10 48 33 5 5 0 2 2 21
Working on a computer 40 50 10 0 0 0 2 2 20
Communicating over the telephone 43 52 5 0 0 0 2 2 21
Environments encounteredFire compartment temperaturesabove 100˚C 17 6 22 11 17 28 6 4 18
Elevated temperatures (30-100˚C) 10 24 24 10 14 19 3 3 21
Freezing temperatures (sub-zero) 5 10 19 14 24 29 6 5 21
Dust 5 19 19 24 19 14 4 4 21
Overcrowding 5 19 10 24 24 19 5 4 21
Open spaces 5 24 10 29 14 19 4 4 21
Height 19 38 19 5 5 14 2 2 21
Enclosed spaces 14 38 19 10 5 14 2 2 21
Total darkness 19 38 14 10 5 14 2 2 21
Partial darkness 14 43 19 5 5 14 2 2 21
Working in water 10 19 19 10 24 19 5 4 21
Working under water 5 5 10 14 24 43 6 5 21
Handling hazardous substances 10 25 15 15 20 15 2 4 20
Smoke 14 38 29 0 5 14 2 2 21
High humidity 19 33 19 5 10 14 2 2 21

Appendix 18. Summary of Results for Training Manager from Occupational Guidelines Questionnaire
2A-107
Table 5: Criticality/importance respondents considered these activities to be to the effective performance of their role?
Movements Very Not very Un- Not Mode Median NCritical (1) important (2) Important (3) important (4) important (5) applicable (6)
Equipment usedFire-protective PersonnelProtective Equipment 62 19 19 0 0 0 1 1 21
Self-Contained Breathing Apparatus 48 5 33 0 5 10 1 2 21
Extended Duration Breathing Apparatus 5 10 5 15 5 60 6 6 20
Vibrating equipment 10 0 10 10 24 48 6 5 21
Computer 33 43 19 5 0 0 2 2 21
Telephone 38 38 24 0 0 0 2 2 21
Hand-held radio 19 43 33 0 5 0 2 2 21
Table 6: Near Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
BA control board-Old style MK 1 Read clock 41 59 2 2 22
BA control board-Old style MK 1 Graduations & cylinder pressure 36 64 2 2 22
BA tag Read tag 45 55 2 2 22
BA control board-New style MK 2 Read clock 36 64 2 2 22
BA control board-New style MK 2 Dial calculator 32 68 2 2 22
BA tag MK 2 Read tag 32 68 2 2 22
BA main control board Read clock 41 59 2 2 22
BA main control board Read 45 55 2 2 22
Sabre centurion Read BA graduations 27 73 2 2 22
Sabre centurion Read needle position 32 68 2 2 22
Siebe Gorman Read BA graduations 0 100 2 2 22
Siebe Gorman Read needle position 0 100 2 2 22
Drager Read BA graduations 27 73 2 2 22
Drager Read needle position 14 86 2 2 22
Philips PFX Handheld radio Read channel selector 59 41 1 1 22
Philips PFX Handheld radio Read numbered channel selector 64 36 1 1 22
BA log book Handwritten 45 55 2 2 22
Universal airline pack (Drager) BA supply BA cylinder gauge 5 95 2 2 22
Low pressure air bags Air pressure gauge 9 91 2 2 22
High pressure air bag Read graduations on console 14 86 2 2 22
High pressure air bag Needle position 14 86 2 2 22
Hurst high pressure lift bags Needle position 9 91 2 2 22
Microvent resuscitation equipment Read scale 5 95 2 2 22
Carmichael Godiva appliance Pressure gauge numbers 14 86 2 2 22
Saxon Volvo appliance pump Pressure gauge numbers 0 100 2 2 22
Dennis appliance pump Pressure gauge numbers 18 82 2 2 22
Read turnout sheet 14 86 2 2 22
Read dosimeter 32 68 2 2 22
Read survey meter 41 59 2 2 22
Read computer VDU 73 27 1 1 22
Read general paperwork 77 23 1 1 22
Read pager 59 41 1 1 22
Read mobile phone text 68 32 1 1 22
Read fire control panels 50 50 1 2 22
Read maps 77 23 1 1 22
Read fire extinguishers 14 86 2 2 22
Read plan inspections 50 50 1 2 22
Inspect premises 14 86 2 2 22
Read scale ruler 18 82 2 2 22
Read sound meter 9 91 2 2 22
Read light meter 5 95 2 2 22

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2A-108
Table 7: Distance Vision Tasks that are a requirement for role
Description Task Yes(1) No(2) Mode Median N
Street names White letters on a blue background 59 41 1 1 22
House numbers Copper figures on a blue background 55 45 1 1 22
House numbers White figures on a red background 55 45 1 1 22
Retail shop numbers Gold figures on a dark green background 55 45 1 1 22
House numbers Grey figures on a white background 55 45 1 1 22
Corporate building numbers Black figure on a silver background 55 45 1 1 22
Street names Black letters on a white background 64 36 1 1 22
House numbers Gold figures on a black background 55 45 1 1 22
House numbers Handpainted black figures on a white background 55 45 1 1 22
House numbers Gold figures on a black background 55 45 1 1 22
House numbers Black figures on a white background 55 45 1 1 22
Carmichael Godiva appliance pump Pressure gauge needle at rear of appliance 9 91 2 2 22
Carmichael Godiva appliance Measuring water in tank 9 91 2 2 22
Saxon Volvo appliance pump Pressure gauge needle at rear of appliance 14 86 2 2 22
Dennis appliance pump Pressure gauge needle at rear of appliance 27 73 2 2 22
Stop sign Road traffic signs 77 23 1 1 22
Give way sign Road traffic signs 77 23 1 1 22
One way street sign Road traffic signs 77 23 1 1 22
Chemical warning sign As EC Directive 92/58/EEC Hazardous substances 59 41 1 1 22
Vehicle signs Break lights/indicators on vehicles 77 23 1 1 22
Fire safety signs 64 36 1 1 22
Exit signs 64 36 1 1 22
Table 8: Hearing Tasks that are a requirement for role
Description Yes(1) No (2) Mode Median N
Distress signal unit 77 23 1 1 22
Warning whistle 82 18 1 1 22
Radio 86 14 1 1 22
Fireground orders 82 18 1 1 22
Evacuation signals/alarms 82 18 1 1 22
Telephone 91 9 1 1 22
Traffic 77 23 1 1 22
Vibraphone 32 68 2 2 22
Pager 68 32 1 1 22
Normal verbal communication with little background noise 82 18 1 1 22
Normal verbal communication with background noise 86 14 1 1 22
Hand clapping 55 45 1 1 22
Cries of help 64 36 1 1 22
Table 9: Other senses that are a requirement for role
Description Yes(1) No (2) Mode Median N
Touch 82 18 1 1 22
Smell 73 27 1 1 22
Taste 36 64 2 2 22

1
OCCUPATIONAL GUIDELINES QUESTIONNAIRE
In October 2004 changes to the Disability Discrimination will come into effect which will havea direct bearing on the Fire and Rescue Service. This survey is being conducted as part of aresearch project to update the Medical Guidelines for the Fire & Rescue Service in preparationfor these changes. The responses will inform the development of future medical guidelines forrecruitment and retention. Please answer the following questions by putting your answer, or across in the relevant box, using a back pen.
Completed questionnaires should be returned to your HR Manager in a sealed envelope withthe letters “OPL” clearly visible on the front.
All responses are anonymous, and none will be attributed to individual respondents or tospecific Fire & Rescue Services. Thank you for taking part in this survey.
1 Which of the following best describes your Fire & Rescue Service Role?Indicate one role – your main role only – and answer the questionnaire with respectto that role.
Firefighting Roles:
Firefighter 1
Crew Manager 2
Watch Manager 3
Station Manager 4
Group Manager 5
Area Manager 6
Brigade Manager 7
1

Fire and Rescue Service: Draft Medical Guidelines – June 2004
2
Fire Control Roles:
Control Operator 8
Control Supervisor 9
Control Watch Manager 10
Control Operations Manager 11
Fire Safety Roles:
Fire Safety Officer 12
Fire Safety Manager 13
Fire Safety Advisor/Engineer 14
Specialist Roles:
Fire Investigator 15
Technical Support 16
Trainer 17
Training Manager 18
2 Please tick the age bracket to which you belong 18-19 30-39 50+
20-29 40-49
3 How many years of service do you have? 0–4 10–14 20–24
5–9 15–19 25+
4 Which gender are you? 1 male 2 female
5 Are you fulltime or retained? 1 fulltime 2 retained

Occupational Guidelines Questionnaire
3
6 How frequently do you perform these activities in a typical year?Do not include activities performed during training or during leisure time – focus onyour F & RS duties
not at all once once once once manyper per per per times
Movements year month week day per day
sprinting 1 2 3 4 5 6
running 1 2 3 4 5 6
jogging 1 2 3 4 5 6
walking 1 2 3 4 5 6
climbing stairs 1 2 3 4 5 6
climbing ladders 1 2 3 4 5 6
crawling 1 2 3 4 5 6
jumping 1 2 3 4 5 6
hammering 1 2 3 4 5 6
digging 1 2 3 4 5 6
Strength Tasks
lifting more than 5 kg or 11 pounds 1 2 3 4 5 6
lifting more than 10 kg or 22 pounds 1 2 3 4 5 6
lifting more than 20 kg or 44 pounds 1 2 3 4 5 6
lifting more than 40 kg or 88 pounds 1 2 3 4 5 6
carrying more than 5 kg or 11 pounds 1 2 3 4 5 6
carrying more than 10 kg or 22 pounds 1 2 3 4 5 6
carrying more than 20 kg or 44 pounds 1 2 3 4 5 6
carrying more than 40 kg or 88 pounds 1 2 3 4 5 6
pushing/pulling more than 5 kg or 11 pounds 1 2 3 4 5 6
pushing/pulling more than 10 kg or 22 pounds 1 2 3 4 5 6
pushing/pulling more than 20 kg or 44 pounds 1 2 3 4 5 6
pushing/pulling more than 40 kg or 88 pounds 1 2 3 4 5 6

Fire and Rescue Service: Draft Medical Guidelines – June 2004
4
not at all once once once once manyper per per per times
Movements year month week day per day
Static postures
Standing 1 2 3 4 5 6
Sitting 1 2 3 4 5 6
Squatting 1 2 3 4 5 6
Kneeling 1 2 3 4 5 6
Lying down 1 2 3 4 5 6
Dynamic flexibility requirements
Bending at waist 1 2 3 4 5 6
Reaching 1 2 3 4 5 6
Stooping 1 2 3 4 5 6
Turning/twisting 1 2 3 4 5 6
Object activities
Catching 1 2 3 4 5 6
Throwing 1 2 3 4 5 6
Fine dexterity (eg writing, mouse control,
assembling equipment) 1 2 3 4 5 6
Foot control (eg driving) 1 2 3 4 5 6
7 How important do you consider these activities to be to the effective performanceof your role? Do not include activities performed during training or during leisuretime – focus on your F & RS duties
critical very important not very unimportant not
Movements important important applicable
sprinting 1 2 3 4 5 6
running 1 2 3 4 5 6
jogging 1 2 3 4 5 6
walking 1 2 3 4 5 6
climbing stairs 1 2 3 4 5 6

Occupational Guidelines Questionnaire
5
critical very important not very unimportant not
Movements important important applicable
climbing ladders 1 2 3 4 5 6
crawling 1 2 3 4 5 6
jumping 1 2 3 4 5 6
hammering 1 2 3 4 5 6
digging 1 2 3 4 5 6
Strength Tasks
lifting more than 5 kg or 11 pounds 1 2 3 4 5 6
lifting more than 10 kg or 22 pounds 1 2 3 4 5 6
lifting more than 20 kg or 44 pounds 1 2 3 4 5 6
lifting more than 40 kg or 88 pounds 1 2 3 4 5 6
carrying more than 5 kg or 11 pounds 1 2 3 4 5 6
carrying more than 10 kg or 22 pounds 1 2 3 4 5 6
carrying more than 20 kg or 44 pounds 1 2 3 4 5 6
carrying more than 40 kg or 88 pounds 1 2 3 4 5 6
pushing/pulling more than 5 kg or 11 pounds 1 2 3 4 5 6
pushing/pulling more than 10 kg or 22 pounds 1 2 3 4 5 6
pushing/pulling more than 20 kg or 44 pounds 1 2 3 4 5 6
pushing/pulling more than 40 kg or 88 pounds 1 2 3 4 5 6
Static postures
Standing 1 2 3 4 5 6
Sitting 1 2 3 4 5 6
Squatting 1 2 3 4 5 6
Kneeling 1 2 3 4 5 6
Lying down 1 2 3 4 5 6
55

Fire and Rescue Service: Draft Medical Guidelines – June 2004
6
critical very important not very unimportant not
Movements important important applicable
Dynamic flexibility requirements
Bending at waist 1 2 3 4 5 6
Reaching 1 2 3 4 5 6
Stooping 1 2 3 4 5 6
Turning/twisting 1 2 3 4 5 6
Object activities
Catching 1 2 3 4 5 6
Throwing 1 2 3 4 5 6
Fine dexterity (eg writing, mouse control,
assembling equipment) 1 2 3 4 5 6
Foot control (eg driving) 1 2 3 4 5 6
8 How frequently do you perform these activities in a typical year? Do not includeactivities performed during training or during your leisure time – focus on your F &RS duties
not at all once once once once manyper per per per times
Tasks year month week day per day
Handling hoses 1 2 3 4 5 6
Handling unconscious casualties 1 2 3 4 5 6
Handling ladders 1 2 3 4 5 6
Operating cutting equipment 1 2 3 4 5 6
Driving vehicles 1 2 3 4 5 6
Climbing ladders 1 2 3 4 5 6
Dealing with traumatised victims 1 2 3 4 5 6
Dealing with traumatised others
(eg relatives, public) 1 2 3 4 5 6
Addressing groups of people 1 2 3 4 5 6
Filling in forms or completing paperwork 1 2 3 4 5 6

Occupational Guidelines Questionnaire
7
not at all once once once once manyper per per per times
Tasks year month week day per day
Making critical decisions quickly 1 2 3 4 5 6
Dealing with the media 1 2 3 4 5 6
Working on a Computer 1 2 3 4 5 6
Communicating over the telephone 1 2 3 4 5 6
Environments Encountered
Fire compartment temperatures above 100oC 1 2 3 4 5 6
Elevated temperatures (30-100oC) 1 2 3 4 5 6
Freezing temperatures (sub-zero) 1 2 3 4 5 6
Dust 1 2 3 4 5 6
Overcrowding 1 2 3 4 5 6
Open spaces 1 2 3 4 5 6
Height 1 2 3 4 5 6
Enclosed spaces 1 2 3 4 5 6
Total darkness 1 2 3 4 5 6
Partial darkness 1 2 3 4 5 6
Working in water 1 2 3 4 5 6
Working under water 1 2 3 4 5 6
Handling hazardous substances 1 2 3 4 5 6
Smoke 1 2 3 4 5 6
High Humidity 1 2 3 4 5 6
Equipment used
Fire-protective Personnel Protective Equipment 1 2 3 4 5 6
Self-Contained Breathing Apparatus 1 2 3 4 5 6
Extended Duration Breathing Apparatus 1 2 3 4 5 6

Fire and Rescue Service: Draft Medical Guidelines – June 2004
8
not at all once once once once manyper per per per times
Tasks year month week day per day
Vibrating equipment 1 2 3 4 5 6
Computer 1 2 3 4 5 6
Telephone 1 2 3 4 5 6
Hand-held radio 1 2 3 4 5 6
9 How critical or important do you consider these activities to be? Do notinclude activities performed during training or during leisure time – focus on yourF & RS duties
critical very important not very unimportant not
Tasks important important applicable
Handling hoses 1 2 3 4 5 6
Handling unconscious casualties 1 2 3 4 5 6
Handling ladders 1 2 3 4 5 6
Operating cutting equipment 1 2 3 4 5 6
Driving vehicles 1 2 3 4 5 6
Climbing ladders 1 2 3 4 5 6
Dealing with traumatised victims 1 2 3 4 5 6
Dealing with traumatised others
(eg relatives, public) 1 2 3 4 5 6
Addressing groups of people 1 2 3 4 5 6
Filling in forms or completing paperwork 1 2 3 4 5 6
Making critical decisions quickly 1 2 3 4 5 6
Dealing with the media 1 2 3 4 5 6
Working on a Computer 1 2 3 4 5 6
Communicating over the telephone 1 2 3 4 5 6

Occupational Guidelines Questionnaire
9
critical very important not very unimportant not
Tasks important important applicable
Environments Encountered
Fire compartment temperatures above 100oC 1 2 3 4 5 6
Elevated temperatures (30-100oC) 1 2 3 4 5 6
Freezing temperatures (sub-zero) 1 2 3 4 5 6
Dust 1 2 3 4 5 6
Overcrowding 1 2 3 4 5 6
Open spaces 1 2 3 4 5 6
Height 1 2 3 4 5 6
Enclosed spaces 1 2 3 4 5 6
Total darkness 1 2 3 4 5 6
Partial darkness 1 2 3 4 5 6
Working in water 1 2 3 4 5 6
Working under water 1 2 3 4 5 6
Handling hazardous substances 1 2 3 4 5 6
Smoke 1 2 3 4 5 6
High Humidity 1 2 3 4 5 6
Equipment used
Fire-protective Personnel Protective Equipment 1 2 3 4 5 6
Self-Contained Breathing Apparatus 1 2 3 4 5 6
Extended Duration Breathing Apparatus 1 2 3 4 5 6
Vibrating equipment 1 2 3 4 5 6
Computer 1 2 3 4 5 6
Telephone 1 2 3 4 5 6
Hand-held radio 1 2 3 4 5 6

Fire and Rescue Service: Draft Medical Guidelines – June 2004
10
10 Indicate which of the following Near Vision Tasks are a requirement for your role bycrossing the relevant boxes
Description Task Requirement for role?
BA control board-Old style MK 1 1. Read clock 1
BA control board-Old style MK 1 2. Graduations & cylinder pressure 1
BA tag 3. Read tag 1
BA control board-New style MK 2 4. Read clock 1
BA control board-New style MK 2 5. Dial calculator 1
BA tag MK 2 6. Read tag 1
BA main control board 7. Read clock 1
BA main control board 8. Read 1
Sabre centurion 9. Read BA graduations 1
Sabre centurion 10. Read needle position 1
Siebe Gorman 11. Read BA graduations 1
Siebe Gorman 12. Read needle position 1
Drager 13. Read BA graduations 1
Drager 14. Read needle position 1
Philips PFX Handheld radio 15. Read channel selector 1
Philips PFX Handheld radio 16. Read numbered channel selector 1
BA log book 17. Handwritten 1
Universal airline pack (Drager) 18. BA supply BA cylinder gauge 1
Low pressure air bags 19. Air pressure gauge 1
High pressure air bag 20. Read graduations on console 1
High pressure air bag 21. Needle position 1
Hurst high pressure lift bags 22. Needle position 1
Microvent resuscitation equipment 23. Read scale 1

Occupational Guidelines Questionnaire
11
Description Task Requirement for role?
Carmichael Godiva appliance 24. Pressure gauge numbers 1
Saxon Volvo appliance pump 25. Pressure gauge numbers 1
Dennis appliance pump 26. Pressure gauge numbers 1
27. Read turnout sheet 1
28. Read Dosimeter 1
29. Read Survey meter 1
30. Read Computer VDU 1
31. Read general paperwork 1
32. Read Pager 1
33. Read Mobile phone text 1
34. Read fire control panels 1
35. Read maps 1
36. Read fire extinguishers 1
37. Read plan inspections 1
38. Inspect premises 1
39. Read scale ruler 1
40. Read sound meter 1
41. Read light meter 1
11 Indicate which of the following Distance Vision Tasks are a requirement for yourrole by crossing the relevant boxes
Description Task Requirement for role?
Street names 1. White letters on a blue background 1
House numbers 2. Copper figures on a blue background 1
House numbers 3. White figures on a red background 1
Retail shop numbers 4. Gold figures on a dark green background 1

Fire and Rescue Service: Draft Medical Guidelines – June 2004
12
Description Task Requirement for role?
House numbers 5. Grey figures on a white background 1
Corporate building numbers 6. Black figure on a silver background 1
Street names 7. Black letters on a white background 1
House numbers 8. Gold figures on a black background 1
House numbers 9. Handpainted black figures on a white background 1
House numbers 10. Gold figures on a black background 1
House numbers 11. Black figures on a white background 1
Carmichael Godiva appliance pump 12. Pressure gauge needle at rear of appliance 1
Carmichael Godiva appliance 13. Measuring water in tank 1
Saxon Volvo appliance pump 14. Pressure gauge needle at rear of appliance 1
Dennis appliance pump 15. Pressure gauge needle at rear of appliance 1
Stop sign 16. Road traffic signs 1
Give Way sign 17. Road traffic signs 1
One way street sign 18. Road traffic signs 1
Chemical warning sign 19. As EC Directive 92/58/EEC Hazardous substances 1
Vehicle signs 20. Break lights/indicators on vehicles 1
21. Fire safety signs 1
22. Exit signs 1

Occupational Guidelines Questionnaire
13
12 Indicate which of the following Hearing Tasks are a requirement for your role bycrossing the relevant boxes
Distress signal unit 1
Warning whistle 1
Radio 1
Fireground orders 1
Evacuation signals/alarms 1
Telephone 1
Traffic 1
Vibraphone 1
Pager 1
Normal verbal communication with little background noise 1
Normal verbal communication with background noise 1
Hand clapping 1
Cries of help 1
13 Indicate which of the other senses are a requirement for your role by crossing therelevant boxes
touch 1
smell 1
taste 1