foi ref: 19/252 freedom of information act...clinical guideline for the prevention, identification...
TRANSCRIPT

FOI REF: 19/252 13 May 2019
FREEDOM OF INFORMATION ACT I am responding to your request for information under the Freedom of Information Act. The answers to your specific questions are as follows: I anticipate that the trust has its own policy in relation to IUGR and introduction of a feeding regime and would like a copy of the policy. Please see the attached copy of East Sussex Healthcare NHS Trust’s ‘Clinical Guideline for the Prevention, Identification and Management of Hypoglycaemia of the Newborn’ and note the following: The baby would commence on our "red bobble hat" pathway. A care bundle designed to give additional monitoring until discharged home. This involves liaison between the paediatric team midwives and Nursery nurses and Special Care Baby Unit (SCBU) staff. Intrauterine Growth Restriction (IUGR) is listed on the hypoglycaemia pathway and feeding is part of the subsequent plan. We recommend the use of expressed breast milk (EBM) if a 'top up' is required or if breastfeeding is not yet initiated. The feeding will be individual to each mother baby dyad and the choice of feeding, but the observations and results obviously impact on subsequent decision making which should be discussed with the mother. Our feeding plan for all babies follows the Baby Friendly Initiative (BFI) guidelines which are included on the BFI Website: http://www.unicef.org.uk/babyfriendly/. If a baby is taken directly to SCBU the staff support women to express as soon as possible even if the woman does not intend to breastfeed. If I can be of any further assistance, please do not hesitate to contact me.

Should you be dissatisfied with the Trust’s response to your request, please write to Lynette Wells, Director of Corporate Affairs, East Sussex Healthcare NHS Trust ([email protected]) quoting the above reference. Yours sincerely Linda Thornhill (Mrs) Corporate Governance Manager [email protected]

Page 1 of 24 V2.0
Clinical Guideline for the Prevention, Identification and Management of Hypoglycaemia of the Newborn
Did you print this yourself? Please be advised the Trust discourages retention of hard copies of the procedural
document and can only guarantee that the procedural document on the Trust website is the most up to date version
Version: V 2.0
Ratified by: Women and Children’s Division
Medicine Optimisation Group
Date ratified: November 2017
Name of author and title: Neonatal Sister/Practice Educator,
Graham Whincup Paediatric consultant and neonatology lead, specialist midwife practice development
Mani Kandasamy – Paediatric Consultant
Date Written: August 2017
Name of responsible committee/individual: Chair of the Guideline Implementation Group for Maternity Services and Dr Whincup Neonatal lead consultant
Date issued: January 2018
Issue number: 2018020
Review date: November 2020
Target audience: All staff
Compliance with CQC Fundamental Standard 9,10,11,12
Compliance with any other external requirements (e.g. Information Governance)
NICE

Clinical Guideline for the Prevention, Identification and Management of Hypoglycaemia of the Newborn
Page 2 of 24 V2.0
Version Control Table
Version number and
issue number
Date Author Reason for Change
Description of Changes Made
January 2016 Graham Whincup –
New Guideline
V2 - 2018020 January 2018 Clinical update national change to blood sugar values addition of flow charts from BAPM
Consultation Table
This document has been developed in consultation with the groups and/or individuals in this table:
Name of Individual or group Title Date
Paediatric Guideline team Dec 2015
Women and Children’s Guideline implementation
group
Jan 2015
Women and Children’s Clinical Unit
Jan 2015
Paediatric Guideline team September 2017
Women and Children’s Guideline implementation
group
October 2017
Women and Children’s Clinical Unit
November 2017
Medicine Optimisation Group November 2017
This information may be made available in alternative languages and formats, such as large print, upon request. Please contact the document author to discuss.

Clinical Guideline for the Prevention, Identification and Management of Hypoglycaemia of the Newborn
Page 3 of 24 V2.0
Table of Contents
1. Introduction .................................................................................................................. 4 2. Rationale ............................................................................................................ ………4 3. Scope…………………………………………………………………………………………… 54. Definitions……………………………………………………………………………………… 55. Accountability………………………………………………………………………………………56. Process……………………………………………………………………………………………..56.1 Blood sugar levels in the neonate……………………………………………………………...5 6.1.1 Symptoms of Hypoglycaemia…………………………………………………………………6 6.2 Measures for preventing and management of Hypoglycaemia ……………………………6 6.3 Low risk infants…………………………………………………………………………………...6 6.4 High risk infants…………………………………………………………………………………..7 6.5 Hypoglycaemia – care plan for the prevention and management of hypoglycaemia on the labour ward and postnatal ward…………………………………………………………………….8 6.5.1 For women who choose to artificial feeding …………………………………………….….8 6.5.2 Management of the reluctant feeder with no risk factors for impaired adaptation …..…8 6.5.3 Arrival to postnatal ward ………………………………………………………………….…..9 6.6 Management for term infants (≥ 37 weeks) at risk of hypoglycaemia……………………...9 6.7 Addition information and guideline when following chart A + B…………………………….9 6.8 Clinical Concern Pathway………………………………………………………………..…….10 6.9 Persistent Hypoglycaemia……………………………………………………………………..11 6.10 Management of persistent hypoglycaemia requiring IV dextrose………………………..11 6.11 "5 & 50" glucose - link to 5&50 online calculator…………………………………………..13 6.12 Further management of persistent hypoglycaemia………………………………………..13 6.13 Emergency treatment of hypoglycaemia……………………………………………………14 6.14 Follow up ………………………………………………………………………………………14
7. Special Considerations…………………………………………………………………………..15 8. Evidence Base / References……………………………………………………………………15 9. Competencies and Training Requirements……………………………………………………16 10. Monitoring Arrangements………………………………………………………………………16 11. Equality and Human Rights Statement……………………………………………………….19
Appendix A Flowchart A. Management of term infants (≥37 weeks) at risk of hypoglycaemia (Box 1)……………………………………………………………………………..20 Appendix B Flowchart B. Pre-feed BG 1.0 – 1.9mmol/l and no abnormal clinical signs…..21 Appendix C Flowchart C. Blood glucose < 1.0mmol/l and / or clinical signs consistent with hypoglycaemia………………………………………………………………………………………22 Appendix D Flowchart D. Management of reluctant feeding in healthy tem infants…….. ..37 weeks…………………………………………………………………………………………………23 Appendix E EHRA………………………………………………………………………………… 24

Clinical Guideline for the Prevention, Identification and Management of Hypoglycaemia of the Newborn
Page 4 of 24 V2.0
1. Introduction
In line with the UK baby friendly initiative – we aim to promote and support breastfeeding mothers, whilst ensuring the safety of all infants at risk of hypoglycaemia. Moderate hypoglycaemia (ie Bsl 1.5-1.9 mmols in an otherwise well infant is not a contraindication to breastfeeding, and establishment of breastfeeding should be supported at all stages of the care pathway, even when supplemental formula is required. Expressed breast milk should be used first as a supplement (if available) and parents should be informed as to why formula is being used if this becomes necessary.
These guidelines are intended for the management of otherwise well babies on the postnatal ward and labour ward. They are not intended to replace clinical judgement, and if there are concerns at any point the on call SHO or Middle grade should be contacted and their management plan followed. Supplements (EBM or Formula) may be required at “day ahead” volumes: 90mls/kg/day on the first day, 120mls/kg/day on second day, 150mls/kg/day on the third day onwards.
If a baby is vomiting consider other causes (structural obstruction, sepsis) or consider a change to more frequent smaller volume feeds.
2. Rationale
2.1 Early anticipation and prevention of hypoglycaemia in high risk infants.
2.2 Early detection and management of hypoglycaemia in infants who are clinically symptomatic.
2.3 Early initiation of feeds and three hourly feeds thereafter for high risk babies
Support for breastfeeding mothers
Formula feeds to be initiates at 60mls/kg/day
2.4 To manage hypoglycaemia in high risk infants safely whilst avoiding separation ofmothers and infants if possible
2.5 Measures to support establishing breast feeding
Use of dextrose gel as first line treatment before supplements started
To encourage expressing of breast milk so as to use expressed breast milk `(EBM)as first line supplement, formula supplements if no EBM available
Passing of nasogastric tube and admission to SCBU if more frequent feeds/largerfeed volumes required
2.6 If enteral feeding not sufficient to maintain blood sugar levels, to commence IVdextrose
Avoid IV bolus if possible
Start IV glucose load at 4-6mg/kg/min and increase in steps of 2mg/Kg/minUse of “5 and 50” glucose regime for independent management of glucose load andflow rate

Clinical Guideline for the Prevention, Identification and Management of Hypoglycaemia of the Newborn
Page 5 of 24 V2.0
3. Scope: This guideline is for use on the delivery suite and postnatal ward initially however theguideline does go on to provide SCBU and paediatric staff recommendations for if a baby isthen admitted to SCBU and requiring treatment for persistent hypoglycaemia.
4. Definitions
Hypoglycaemia – is a blood sugar level (BSL) of < 2.0 mmols
Severe hypoglycaemia - is a BSL of <1.0mmol/L and is potentially serious, requiring immediate treatment. There is good evidence that prolonged and persistent hypoglycaemia can have a profound effect on the infant brain potentially causing a wide variety of neurodevelopmental sequelae
Persistent Hypoglycaemia - more than 2 measurements <2.0mmol/l within the first 48hours after birth) or severe hypoglycaemia (<1.0mmol/l at any time) and infants with signs of acute neurological dysfunction and blood glucose <2.5mmol/l.
5. Accountabilities
5.1.1 Midwives, Maternity Nurses, Maternity support workers, SCBU Staff and Paediatricians
To access, read, understand and follow this guidance
To use their professional judgement in application of this guideline
5.2 Management
To ensure the guideline is reviewed as required in line with the Trust and Nationalguidelines
To ensure the guideline is accessible to all relevant staff
To monitor the audit process
6. Process
6.1 Blood glucose levels in the neonate
As part of the normal adaptation to the extra-uterine life, newborn infants’ bloods glucose levels fall immediately following delivery, with subsequent spontaneous recovery in healthy, normally grown term babies. The neonatal brain uses first relatively high lactate and then ketone concentrations as an alternative metabolic fuel whilst feeding is being established in the first 24-48 hours of life so as to minimise glucose requirement.
However, there are several groups of newborns who are at greater risk of symptomatic hypoglycaemia causing neuronal damage. Preterm infants and babies
born with intra-‐uterine growth restriction may not only have reduced glycogen stores due to their size in combination with impaired gluconeogenesis due to an immature liver, but also an inability to produce ketones as an alternative substrate for neuronal metabolism. Large babies (>4.5kg) or those whose mothers are diabetic are at risk of hyperinsulinism causing profound hypoglycaemia

Clinical Guideline for the Prevention, Identification and Management of Hypoglycaemia of the Newborn
Page 6 of 24 V2.0
6.1.1 Symptoms of hypoglycaemia
Glucose is vital for neuronal metabolism. Therefore if the blood glucose level drops profoundly this can manifest itself as neurological symptoms.
Signs that may indicate Hypoglycaemia:
Lethargy
Abnormal feeding behaviour
especially after a period of feeding well
High pitched cry
Altered level of consciousness
Hypotonia
Seizures
Hypothermia (<36.5°C)
Cyanosis
Apnoea
Measurement of blood sugar levels (BSL)
The quickest and most convenient way to measure BSL is with a potable glucose meter.
A low/borderline reading on a portable glucose meter should be checked with a capillary blood
sugar using the blood gas analyser.
6.2 Measures for prevention and management of hypoglycaemia
Babies should be managed according to their predicted risk of hypoglycaemia:- Low or High
For all babies, hypoglycaemia needs to be anticipated and prevented:
General measures:
At birth keep the baby Dry and Warm
Offer a feed at birth – UNICEF suggests all babies should feed within 1 hour of birth
The risk of hypoglycaemia should be assessed on labour ward by the midwife caring for the
infant and appropriate action taken.
6.3 Low Risk Infants
Normally grown term infants who are well, warm and feeding well are at low risk of hypoglycaemia and do not require routine BSL testing. Infrequent feeding in a well infant is NOT an indication for BSL testing – it is usual for a baby to feed as little as 4 times in the first 24 hours of life. If the baby is slow to feed this will be managed by the midwifery team and they can refer to the Clinical Guideline - Infant Feeding of the Healthy Newborn or the Clinical Guideline for the management of breastfed babies that are reluctant to feed on the extranet for guidance or contact the Infant feeding specialist midwife for support. If there are clinical concerns – if the baby becomes systematically unwell or there are signs of
hypoglycaemia such as poor tone, irritability, apnoea, jitteriness or seizure activity, then the
infant should be managed according to the “clinical concern pathway” (see hypoglycaemia care
plan and Flow chart A for >37 weeks gestation). A blood sugar level should be tested and the
on call SHO informed (see next section for full management).

Clinical Guideline for the Prevention, Identification and Management of Hypoglycaemia of the Newborn
Page 7 of 24 V2.0
6.4 High Risk Infants
High risk babies should be identified by the midwife on labour ward and the “hypoglycaemic
Care plan” should be commenced and placed in the neonatal notes. They will follow the
“Infant at risk pathway” on the “hypoglycaemic Care Plan”.
If an infant fulfils any of the following criteria, they are at high risk for neonatal
hypoglycaemia.
Table 1: High risk infants trigger list
1 Prematurity (<37 weeks gestation – this includes all babies up to and including
36+6 weeks
2 Low birth weight ≤2.5Kg
3 Large for dates ≥4.5Kg
4 Diabetic Mother
5 Mothers receiving any medication that can cause hypoglycaemia in the newborn e.g Betablockers, Sodium Valproate. in the third trimester or at the time ofdelivery.
6 Any baby with any cord PH that has measured under 7.1
7 Any Baby with an apgar of <7 at 5 minutes – this is a trigger for admission to SCBU
8 Hypothermia <36.5oc
All of the above babies and any that the HCP deems appropriate should have a red bobble hat in place and follow correct pathway Standard Operating procedure for the Bobble hat care pathway
Infants of women with diabetes are also at higher risk of persistent respiratory distress, congenital heart disease and polycythaemia, and severe jaundice. If there are any clinical concerns in these infants the on call SHO should be called to review the baby. There are other factors which may lead infants to become hypoglycaemic in the neonatal period:
Sepsis
Polycythaemia
Hypoxic-ischaemic encephalopathy
Respiratory distress
Inborn errors of metabolism
Beckwith-wiedemann syndrome
Rebound hypoglycaemia following IV dextrose bolus.
Some of these are not immediately apparent and it is important that general principles of keeping infants warm and dry at birth and offering early feeds are followed when managing all infants, and that the blood sugar level is taken early when there is clinical concern. In sick neonates good blood sugar management should be an integral part of good clinical care.

Clinical Guideline for the Prevention, Identification and Management of Hypoglycaemia of the Newborn
Page 8 of 24 V2.0
6.5 Hypoglycaemia – care plan for the prevention and management of hypoglycaemia on the labour ward and postnatal ward
For infants entering onto the at risk pathway: these infants are who have one or more of the risk factors mentioned in Table 1: in point 6.4 above.
Any baby identified as at risk will also needs to have a red bobble hat applied, please refer to Standard Operating procedure for the Bobble hat care pathway with regards to these babies however; the hypoglycaemia care pathway takes priority and the bobble hat should alert staff to the neonates additional monitoring requirements.
If the first feed is taken within 1 hour of birth, check the pre feed blood sugar prior to the second feed, 2-4 hours after birth.
“If not fed or received any EBM within the 1st hour of life then the Midwife will use Proactive management including:
On-going observations to include:
Continuing skin to skin contact (All steps should be taken to ensure the infant is warmSkin to skin can help to regulate temperature control in the newborn and this can bedone by either mum or dad. This may also aid feeding to be established with mum)
Temperature maintenance Please record the temperature hourly for the next twohours to ensure that the at risk baby is not put at further risk by developinghypothermia.
Hand expressing – If EBM not available continue to provided active support withhand expressing for the woman
Then Within 3 hours of age (but not before 2 hours of age unless clinically indicated):
Perform pre-feed BSL and follow the care plan guidance.
Feed according to the mothers wishes i.e breastfeed, give EBM if available ordiscuss an alternative if required with the parents.
Feeds should be offered 3 hourly (Maximising mums milk supply by hand expressing 8-10 times in a 24 hour period with at least one being at night.)
If a feeding record is required and the use of an EBM / expressing log is required, both can be found on the extranet – A-Z, Maternity, under the tab ‘Infant feeding specialist midwife’. These tools can be printed when required used by the Mother while admitted and added to the Infants notes upon discharge.
6.5.1 For women who choose to formula feed offer within the first hour and plan to feed 3 hourly. Feed responsively when blood glucose measurements have been above 2.0mmol/l on two consecutive occasions. If the baby does not show feeding cues, i.e. is a reluctant feeder and has no signs of illness, refer to the following point and Appendix D P23
6.5.2 Management of the reluctant feeder with no risk factors for impaired adaptation A thorough clinical assessment should be made and documented within 6 hours after birth, at which time practitioners should differentiate between a well baby who is reluctant to feed versus a baby whose feeding pattern suggests an abnormal clinical state due to illness. Signs of reluctant feeding include not waking for feeds, not latching at the breast, not sucking effectively, and appearing unsettled. Skin-to-skin contact and laid-back nursing will stimulate the baby to use

Clinical Guideline for the Prevention, Identification and Management of Hypoglycaemia of the Newborn
Page 9 of 24 V2.0
innate abilities and help his / her mother recognize feeding cues. Feeding support should be provided to reluctant feeders using Flowchart D in Appendix D P23 and medical review should be prompt if there are concerns that feeding behaviours may reflect an abnormal clinical state.
Blood glucose should be measured if reluctant / non-effective feeding follows a period of effective feeding or if there are any abnormal clinical signs in addition to reluctant feeding. The ESHT Clinical Guideline for the management of breastfed babies that are reluctant to feed may also be able to provide you with some guidance on feeding cues, and advice re-expressing that you can discuss with the mother
6.5.3 On arrival to the postnatal ward
A Temperature must be taken on all at risk babies that are entered onto the hypoglycaemia pathway when they arrive on the postnatal ward. The findings are to be recorded onto the observation chart on the back page of the Hypoglycaemia care plan. If any triggers i.e one YELLOW: Contact neonatal team / senior midwife or Nurse in charge on SCBU for advice. Two observations in YELLOW / one RED contact the neonatal team immediately and advise Nurse in charge on SCBU at the same time.
6.6 Management for term infants (≥37 weeks) at risk of hypoglycaemia
6.6.1 The first (pre-feed) BSL should be checked on the portable blood glucose meter.
6.6.2 The baby’s temperature at the time of the BSL should be taken and recorded on the care plan.
6.6.3 Measure the blood glucose level before the second feed (2-4 hours after birth). Measure blood glucose immediately if there are clinical signs suggestive of hypoglycaemia (See point 6.1.1)
6.6.4 Based on the result of the first blood glucose (BG) measurement, place the baby on one of the following care pathways:
Flowchart B: First pre-feed BG 1.0-1.9mmol/l, and no abnormal signs See Appendix B P21
Flowchart C: First pre-feed BG <1.0mmol/l, and / or clinical signs consistent with hypoglycaemia at higher BG concentration See Appendix C P22
Do not transfer babies with risk factors for impaired metabolic adaptation and hypoglycaemia to community care until you are satisfied that the baby is maintaining blood glucose levels ≥ 2.0mmol/l on at least two consecutive occasions and is feeding well. Infants at risk of hypoglycaemia should not be transferred to the community until they are at least 24 hours old.
Clinical Guideline for the Prevention, Identification and Management of Hypoglycaemia of the Newborn
Page 10 of 24 V2.0
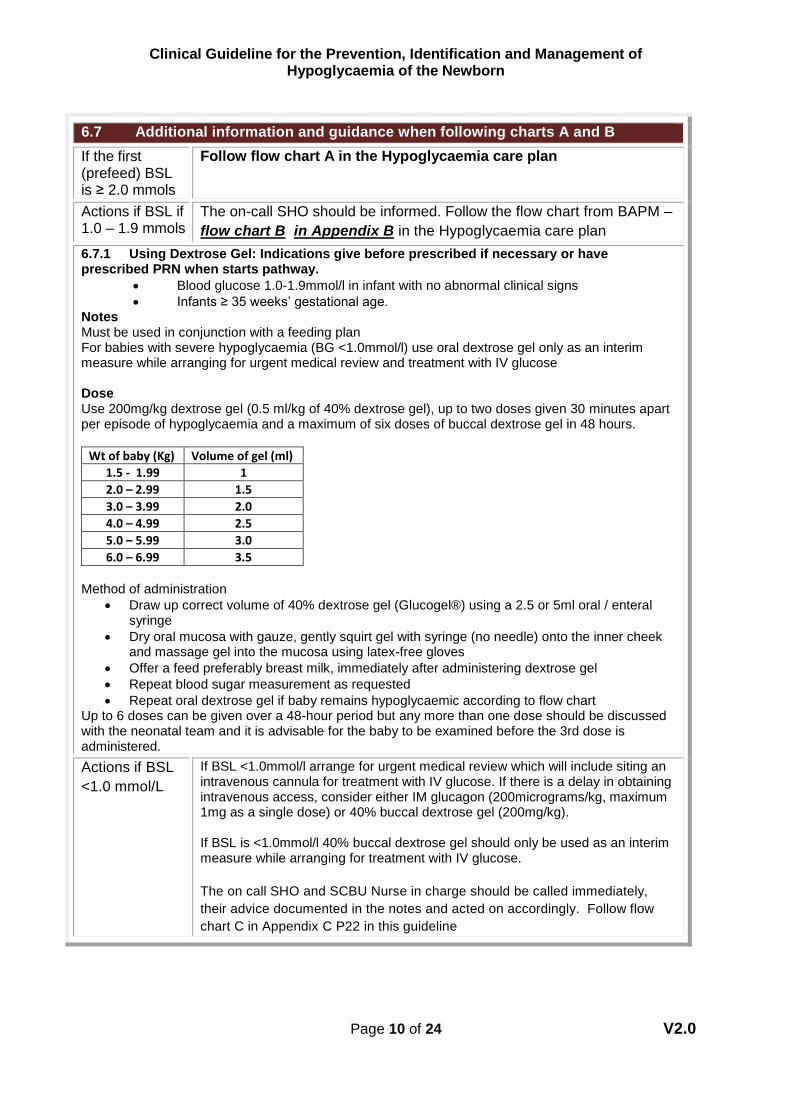
6.7 Additional information and guidance when following charts A and B
If the first (prefeed) BSL is ≥ 2.0 mmols
Follow flow chart A in the Hypoglycaemia care plan
Actions if BSL if 1.0 – 1.9 mmols
The on-call SHO should be informed. Follow the flow chart from BAPM –
flow chart B in Appendix B in the Hypoglycaemia care plan
6.7.1 Using Dextrose Gel: Indications give before prescribed if necessary or have prescribed PRN when starts pathway.
Blood glucose 1.0-1.9mmol/l in infant with no abnormal clinical signs
Infants ≥ 35 weeks’ gestational age.Notes Must be used in conjunction with a feeding plan For babies with severe hypoglycaemia (BG <1.0mmol/l) use oral dextrose gel only as an interim measure while arranging for urgent medical review and treatment with IV glucose
Dose Use 200mg/kg dextrose gel (0.5 ml/kg of 40% dextrose gel), up to two doses given 30 minutes apart per episode of hypoglycaemia and a maximum of six doses of buccal dextrose gel in 48 hours. Weight of baby(k
Wt of baby (Kg) Volume of gel (ml)
1.5 - 1.99 1
2.0 – 2.99 1.5
3.0 – 3.99 2.0
4.0 – 4.99 2.5
5.0 – 5.99 3.0
6.0 – 6.99 3.5
g)Volume of gel (ml)Method of administration
Draw up correct volume of 40% dextrose gel (Glucogel®) using a 2.5 or 5ml oral / enteralsyringe
Dry oral mucosa with gauze, gently squirt gel with syringe (no needle) onto the inner cheekand massage gel into the mucosa using latex-free gloves
Offer a feed preferably breast milk, immediately after administering dextrose gel
Repeat blood sugar measurement as requested
Repeat oral dextrose gel if baby remains hypoglycaemic according to flow chartUp to 6 doses can be given over a 48-hour period but any more than one dose should be discussed with the neonatal team and it is advisable for the baby to be examined before the 3rd dose is administered.
Actions if BSL
<1.0 mmol/L
If BSL <1.0mmol/l arrange for urgent medical review which will include siting an intravenous cannula for treatment with IV glucose. If there is a delay in obtaining intravenous access, consider either IM glucagon (200micrograms/kg, maximum 1mg as a single dose) or 40% buccal dextrose gel (200mg/kg).
If BSL is <1.0mmol/l 40% buccal dextrose gel should only be used as an interim measure while arranging for treatment with IV glucose.
The on call SHO and SCBU Nurse in charge should be called immediately,
their advice documented in the notes and acted on accordingly. Follow flow
chart C in Appendix C P22 in this guideline

Clinical Guideline for the Prevention, Identification and Management of Hypoglycaemia of the Newborn
Page 11 of 24 V2.0
6.8 Clinical concern pathway
Normally grown term infants may be started on the hypoglycaemia care plan if there is clinical concern: if the baby becomes systematically unwell or there are signs of hypoglycaemia such as poor tone, irritability, apnoea, jitteriness or seizure activity. In these cases the baby should have a first blood level as per the above pathway (ie if the first BSL is <2.0 mmol/L on portable glucose monitor a capillary sample should be taken and the same pathway as outlined above followed. Once the baby has had two consecutive blood sugar levels ≥2.0 mmol/L monitoring can be stopped.
With these infants there is no need to complete a further 24 hours observation as per high risk infants
For babies that are 35-36+6 gestation an individual plan must be put in place by the Paediatrician and must be discussed with the mother and the midwifery/Nursing team to ensure that that plan is understood and followed and that if any concerns or changes arise then an updated plan is documented and communicated again to the parents and the midwifery/Nursing team.
6.9 Persistent Hypoglycaemia If despite the above measures all infants high or low risk remain persistently hypoglycaemic or profoundly hypoglycaemic at any stage, further measures will need to be taken in discussion with the paediatric registrar.
6.10 Management of persistent hypoglycaemia requiring IV dextrose.
Investigations for hypoglycaemia
A newborn with persistent (more than 2 measurements <2.0mmol/l within the first 48 hours after birth) or severe hypoglycaemia (<1.0mmol/l at any time), and infants with signs of acute neurological dysfunction and blood glucose <2.5mmol/l should be referred urgently to a paediatrician for the following investigations during the period of hypoglycaemia:
Blood glucose, insulin, cortisol, growth hormone, fatty acids, ketone bodies, carnitine,acylcarnitine profile, amino acids, ammonia, lactate.
Urine ketones and organic acids
Consider evaluation for early onset sepsis
Further investigations should be based on the results of the initial screen and taken following specialist advice.
Infants with abnormal neurological signs should be admitted to the Neonatal Intensive Care Unit for neurocritical care investigations and monitoring.
Transient hypoglycaemia defined as one measurement of 1.0-1.9mmol/l within the first 48 hours after birth in an infant with no abnormal signs who is feeding effectively does not require the investigations listed above
Persistent low blood glucose measurement
Persistent hypoglycaemia (more than 2 measurements <2.0mmol/l within the first 48 hours after birth) can be the first sign of hyperinsulinism or another metabolic disorder characterized by

Clinical Guideline for the Prevention, Identification and Management of Hypoglycaemia of the Newborn
Page 12 of 24 V2.0
neonatal hypoglycaemia. It is important to refer to a paediatrician and screen such infants (see above for list) to identify hyperinsulinism or another disorder that requires specific therapy.
Hyperinsulinism should be considered if blood glucose concentration remains low (<2.0mmol/l on three or more occasions in first 48 hours despite adequate energy provision and a feeding plan), or if a glucose dose greater than 8mg/kg/min is required.
In cases of suspected or confirmed hyperinsulinism, aim to maintain blood glucose concentration ≥ 3.0mmol/l.
Any infant who has persistent symptoms, is not tolerating enteral feeds, or is unable to maintain
normoglycaemia with appropriate enteral feeds alone should be commenced on an intravenous
infusion of 10% dextrose. This will involve admission to SCBU.
Blood tests required will depend on the clinical scenario
Infants receiving IV dextrose should also receive enteral feeds IF there are no
contraindications
Normal neonatal hepatic production rate of glucose is 4-6 mg/kg/min – aim to start
IV 10% dextrose at this rate.
For an infant admitted to SCBU for IV dextrose for low BSL despite attempts at
enteral management with BSL 1.0-1.9mmol/L starting 10% dextrose at
60mls/kg/day with enteral feeds as extra. A dextrose bolus is not required unless
the baby is symptomatic, as boluses can provoke rebound hyperinsulinism.
If BSL is persistently <2.0 mmol/L (on capillary sample) despite treatment and/or
exhibiting severe symptoms such as seizures, increase the glucose load t0
90ml/kg/day consider changing the concentration if needed. The aim is to rapidly
increase BSL to ≥ 2.0 mmol/L.
Give 10% Dextrose bolus 2.5ml/kg only if BS< 1.0mmol or if <2.5mmols in
symptomatic baby.
Glucose load should be increased in steps of 2mg/kg/min. Use the [glucose
infusion calculator]
Check BSL 30 minutes after initiation of treatment and then at 2 hours. Frequency
of testing can be reduced if there has been an adequate response.
If BSL is still low, the glucose load needs to be increased. This can be done by
increasing wither the volume of 10% dextrose given or increasing the concentration
of the dextrose. It is important not to increase the volume of the fluid given beyond
120mls/kg/day on the first day of life as there is a risk of hyponatraemia.
To increase the concentration of dextrose use the “5 and 50” regime (5 & 50 online
calculator)
If the concentration of dextrose required >12.5% this must be given through a
central line (UVC/long line)
At all stages document the amount of glucose being given in mg/kg/min
Further boluses can be given if there are further episode of severe or symptomatic
hypoglycaemia but this should not be done in isolation: glucose load should also be
increased AND cause for the drop should be searched for (tissued line, possible
metabolic condition etc)

Clinical Guideline for the Prevention, Identification and Management of Hypoglycaemia of the Newborn
Page 13 of 24 V2.0
The attending / on call consultant should be informed of all infants with persistently
severely hypoglycaemia and infant requiring >12mg/kg/minutes IV glucose.
Once BSL >2.5 mmol/L for 24 hours, reduce IV fluids and increase enteral fluids as
appropriate every 6 hours, checking blood sugars 4 hourly. On full enteral feeds
check BSL every 6 hours for 24 hours, then 12 hourly for 24 hours, then cease
testing if BSL consistently >2.0 mmol/L.
6.11 “5 & 50” glucose regime – link to 5&50 online calculator
By running 5% and 50% dextrose as simultaneous infusion, glucose load
(mg/kg/min) and flow rate (mls/hr) can be independently adjusted.
If final glucose concentration is >12.5%, the infusion should be run through a central
line (UVC or long line).
Electrolytes can be added to these infusions – the total desired amount (in
mmol/kg/day) added to both infusions, calculated for both as if run at the full total
daily volume (mls/kg/day). For example, 4mmol/kg/day NaCl desired at
120mls/kg/day would need 16.6mmol NaCl to be added to one 500ml bag of fluid.
Therefore add 16.6mmol NaCl to BOTH the 5% dextrose and 50% dextrose bag (as
if each would run at 120mls/kg/day). 120mls/kg/day will be delivered by a
combination of the 5% and 50% dextrose depending on the glucose load required
but regardless of the final glucose concentration 4mmol/kg/day of NaCl will be
delivered)
6.12 Further management of persistent hypoglycaemia -
Central line access (UVC or long line) is required for glucose concentrations
>12.5%
If infant remains hypoglycaemic despite glucose load of 12mg/kg/min or profound
hypoglycaemia (<1.1mmols in a term neonate) contact Trevor Mann Baby Unit in
Brighton for guidance with management plan and take bloods (preferably when
baby is hypoglycaemic but do not delay treatment) for:
Tests Tube Blood Volume (ml) Comments
Glucose
Lactate
Grey Top 0.6 Please send all samples to the lab immediately on ice and phone the lab to inform them they are on the way.
Ammonia (needs to go to lab
Purple Top 0.6

Clinical Guideline for the Prevention, Identification and Management of Hypoglycaemia of the Newborn
Page 14 of 24 V2.0
immediately on ice)
Fatty acids Green Top 0.6
Insulin level Brown Top 0.6
Cortisol & Growth hormone
LFTs & TFTs
Brown Top
If LFT’s and TFT’s
are requested this
can be taken with
the Cortisol sample
and upped to 1ml
0.6
Or 1ml if LFT/TFT added
FBC Purple Top 0.6
Blood gas Glass tube Micro Sample
Carnitine and acetylcarnitine
(on NNST form)
Dip urine for ketones and send for urinary sample for organic acids
Sterile Container 2mls of Urine
Further testing such as Lumbar puncture for CSF glucose will depend on the clinical
scenario and history.
High insulin levels with hypoglycaemia and no urinary ketone indicated
hyperinsulinism. In hyperinsulinism it is not unusual to have a glucose requirement
of 15 -20mg/kg.min.
Treatment with diazoxide/chlorthiazide should be considered (by the attending
consultant). Total fluids should be reduced to 120mls/kg/day as diazoxide may
cause fluid retention.
6.13 Emergency treatment of hypoglycaemia
10% dextrose bolus
If baby is symptomatic (seizures/unrousable) or BSL <1.0mmol/L give IV bolus of
2.5 mls /kg 10% dextrose AND start dextrose infusion. Do NOT give boluses
without subsequent infusion of 10% dextrose, the decision of the bolus must be
made by the middle grade or consultant.
Glucagon (100mcg/kg IM) may be required in the following situations:
Unable to gain IV access in newly admitted infant with symptomatic hypoglycaemia
Loss of IV access in presence of significant / symptomatic hypoglycaemia
Persistence for hypoglycaemia despite increasing glucose infusion rate
Presence of seizures and hypoglycaemia

Clinical Guideline for the Prevention, Identification and Management of Hypoglycaemia of the Newborn
Page 15 of 24 V2.0
Rarely an IV bolus or infusion of glucagon might be needed. Rate of 15-30mcg/kg/hr can be given IV or subcutaneously
6.14 Follow up
All significantly symptomatic babies and those who have required more than 12mg/kg/min of glucose infusion should be followed up. If uncertain discuss with the attending consultant.
7. Special Considerations
None required.
8. Evidence Base/References
Alkalay AL, Sarnat HB, Flores-Sarant L, et al. Population meta-analaysis of low plasma glucose thresholds in full-term normal newborns. Am J Perinatol 2006: 23: 115 – 119.
Aynsley Green A et al. Practical management of hyperinsulinism in infancy. Arch Dis Child Fetal Neonatal Ed 2000; 82: F98 – F107.
British Association for Perinatal of Perinatal Medicine. Identification and Management of
Neonatal Hypoglycaemia in the Full Term Infant – A Framework for Practice April 2017.
Burns et al. Patterns of cerebral injury and neurodevelopmental outcomes after symptomatic neonatal hypoglycaemia. Pediatrics 2008; 122(1): 65 – 74.
Chantry CJ, Howard CR. Clinical Protocols for Management of Breastfeeding. Pediatr Clin N Am 2013; 60:1, 75 – 113.
Cornblath M et al. Controversies regarding definition of neonatal hypoglycaemia suggests operational thresholds. Pediatrics 2000 May; 105(5): 1141 – 5.
Cornblath M, Ichord R. Hypoglycaemia in the neonate. Semin Perinatol 2000; 24(2): 136 – 49.
Diwaker et al. Plasma glucose levels in term infants who are appropriate size for gestation and exclusively breast fed. Arch Dis Child Fetal Ed 2002; 87: F46 – 48.
Harris DL et al. Incidence of neonatal hypoglycaemia in babies def ined as at risk. J Pediatr 2012; 161: 787 – 91.
Harris DL et al. Dextrose gel for neonatal hypoglycaemia (the Sugar Babies Study): a randomised, double-blind, placebo-controlled trial. The Lancet 2013; 302: 2077 – 2083.
Hawdon JM. Investigation, prevention and management of neonatal hypoglycaemia (impaired postnatal metabolic adaptation). Paediatrics and Child Health 2012; 22:4, 131 – 135.
Hawdon JM. Definition of neonatal hypoglycaemia: time for a re-think? Arch Dis Child Fetal Neonatal Ed 2013; 98(5): F382 – 3.

Clinical Guideline for the Prevention, Identification and Management of Hypoglycaemia of the Newborn
Page 16 of 24 V2.0
Holmes AV. Establishing Successful Breastfeeding in the newborn. Pediatr Clin N Am 2013; 60:1, 147 – 168.
Hussain K. Investigations for neonatal hypoglycaemia. Clin Biochem 2011; 44(7): 465 – 6.
Lucas A et al. Adverse neurodevelopmental outcome of moderate neonatal hypoglycaemia. Arch Dis Child 1988; 1352 – 58.
National Institute for Health and Care Excellence. Diabetes in pregnancy: management of diabetes and its complications from pre-conception to the postnatal period. CG63. London: National Institute for Health and Care Excellence; 2008.
Sundercombe SL et al. Audit of a clinical guideline for neonatal hypoglycaemia screening. J Paediatr Child Health 2013.
Sweet CB, Grayson S, Polak M. Management Strategies for Neonatal Hypoglycaemia. J Pediatr Pharmacol Ther 2013; 18(3): 199 – 208. UNICEF. UK Baby Friendly Initiative. http:??www.unicef.org.uk/BabyFriendly/Healthy-Professionals/going-baby-friendly/ http://www.unicef.org.uk/Documetns/Baby_Friendly/Guidance/Baby_Friendly_guidance_2012.pdf
Vannucci RC. Hypoglycaemic brain injury. Semin Neonatal 2001 Apr; 6(2): 147 – 55.
9. Competencies and Training Requirements
Training will be carried out as a joint effort between the practice educators from Maternity and SCBU.
10. Monitoring Arrangements
Please see table below.

Document Title
Page 17 of 24 V2.0 V2.0
Document Monitoring Table
Element to be Monitored
Lead Tool for Monitoring
Frequency Responsible Individual/Group/ Committee for review of results/report
Responsible individual/ group/ committee for acting on recommendations/action plan
Responsible individual/group/ committee for ensuring action plan/lessons learnt are Implemented
Compliance with the guideline and care pathway
SCBU/Maternity Audit 6 months after launch
Clinical unit lead and lead neonatologist
Paediatric and Obstetric Audit meetings
Clinical unit lead and lead neonatologist
Paediatric and Obstetric Audit meetings
Practice development leads for Neonatology and Maternity.
Number of babies that are entered onto the pathway correctly
SCBU/Maternity Audit 6 months after launch
Clinical unit lead and lead neonatologist
Paediatric and Obstetric Audit meetings
Clinical unit lead and lead neonatologist
Paediatric and Obstetric Audit meetings
Practice development leads for Neonatology and Maternity.
Management and completion of the care pathway
SCBU/Maternity Audit 6 months after launch
Clinical unit lead and lead neonatologist
Paediatric and Obstetric Audit meetings
Clinical unit lead and lead neonatologist
Paediatric and Obstetric Audit meetings
Practice development leads for Neonatology and Maternity.

Document Title
Page 18 of 24 V2.0
V2.0
11. Equality and Human Rights Statement
A full Equality and Human rights analysis has been completed. Please see Appendix E.

Clinical Guideline for the Prevention, Identification and Management of Hypoglycaemia of the Newborn
Page 19 of 24 V2.0
Appendix A
Flowchart A. Management of term infants (≥37 weeks) at risk of hypoglycaemia (Box 1)
Dry and place baby skin-to-skin care in a warm,draught free room.
Put hat on baby, and cover with a warmblanket.
Encourage and support early breastfeedingwithin the first hour after birth.
For women who chose to formula feed60ml/kg within the first hour after birth.
Provide verbal and written information toparents that explains how to preventhypoglycaemia, why their baby needs bloodglucose monitoring, lists signs that mayindicate hypoglycaemia (see Box 2), andadvises parents to inform a member of thehealthcare team if they are concerned abouttheir baby’s well-being.
Check pre-feed blood glucose level prior to second feed (2-4 hours after birth):
Is the blood glucose level ≥ 2.0mmol/l?
Encourage frequent feeding and ensure nolonger than 3 hours between feeds.
Assess the need for helping the mother with:ongoing help with feeding; hand expression;recognition of early feeding cues; and signs ofeffective attachment and feeding.
For women who chose to formula feed, give60ml/kg per feed 3 hourly over the first 24 hoursafter birth.
Check blood glucose level prior to third feed(no longer than 8 hours after birth): Is theblood glucose level ≥ 2.0mmol/l?
Continue to support responsive breast feedingand ensure that mother understands how toassess effective feeding and knows how toescalate concerns.
If formula fed give 60ml/kg per feed 3 hourlyover the first 24 hours after birth.
No further blood glucose monitoring requiredunless there are clinical signs of hypoglycaemia(Box 2).
Baby must remain in hospital until 24 hours old.
Complete at least one recorded breastfeedingassessment using local / BFI tool prior totransfer home.
Box 1. Infants who require routine blood glucose monitoring
Premature <37 weeks
Low birth weight
Large for dates ≥4.5kg at
Baby of a Diabetic mother
Mother receiving betablockers – inthe third trimester or at the time ofdelivery.
Low PH <7.1
Low Apgar <7 @ 5 Mins
Hypothermia (<36.5oc)
Box 2. Signs that may indicate Hypoglycaemia:
Lethargy
Abnormal feeding behaviour
especially after a period of
feeding well
High pitched cry
Altered level of consciousness
Hypotonia
Seizures
Hypothermia (<36.5°C)
Cyanosis
Apnoea
Yes No
Yes
No
See flow chart B

Clinical Guideline for the Prevention, Identification and Management of Hypoglycaemia of the Newborn
Page 20 of 24 V2.0
Appendix B
Flowchart B. Pre-feed BG 1.0 – 1.9mmol/l and no abnormal clinical signs
Does the baby have clinical signs
consistent with hypoglycaemia (Box 1)?
Consider administration of 40% buccal dextrosegel 200mg/kg as part of feeding plan (see below)
Support breast feeding (see Box 2).
If mother is choosing to formula feed, aim todeliver 60ml/kg in 3 hourly feed volumes.
Recheck blood glucose before third feed, nolater than 8 hours after birth.
Is the blood glucose level ≥ 2.0mmol/l?
Give feed: breast feed and/or offer expressedbreast milk.
For formula fed infants give 60ml/kg in 3hourly feed volumes.
Recheck blood glucose before next feed.
Is the blood glucose level ≥ 2.0mmol/l?
Box 2: Supporting Breast Feeding
Encourage skin-to-skin contact.
Offer breast feed and if not feedingeffectively teach mother to handexpress.
Give colostrum obtained to baby bythe method suitable to parents.Continue to encourage handexpression at least 8-10 times in 24hours and support feeding on thebreast until infant is feedingeffectively.
Box 1. Signs that may indicate Hypoglycaemia:
Lethargy
Abnormal feeding behaviour
especially after a period of
feeding well
High pitched cry
Altered level of consciousness
Hypotonia
Seizures
Hypothermia (<36.5°C)
Cyanosis
Apnoea
Yes No
Yes
See flow chart C
Box 3: If more than 2 measurements 1.0 – 1.9 mmols/l, Inform neonatal team
Investigate for causes ofhyopglycaemia, consider sepsis.
Consider increased feed frequency,nasogastric tube insertion or IVinfusion of 10% glucose.
Continue to support responsive breastfeeding.
After 2 consecutive pre-feed BG measurements>2.0mmol/l discontinue BG monitoring unlessthere are abnormal clinical signs (Box 1), in whichcase use Flowchart C (in the Hypoglycaemia folder)
Baby must remain in hospital until 24 hours old.
Complete at least one recorded breastfeedingassessment using local / BFI tool prior to transferhome.
Yes
No See
Box 3
No Repeat
one loop,
then see Box 3
Use of Dextrose Gel: Indications:
Blood glucose 1.0-1.9mmol/l in infant with noabnormal clinical signs
Infants ≥ 35 weeks’ gestational ageNotes
Must be used in conjunction with a feedingplan
For babies with severe hypoglycaemia (BG<1.0mmol/l) use oral dextrose gel only as aninterim measure while arranging for urgentmedical review and treatment with IV glucose
Dose Use 200mg/kg dextrose gel (0.5 ml/kg of 40%
dextrose gel), up to two doses given 30minutes apart per episode of hypoglycaemiaand a maximum of six doses of buccaldextrose gel in 48 hours.
Wt of baby (Kg)
Volume of gel (ml)
1.5 - 1.99 1
2.0 – 2.99 1.5
3.0 – 3.99 2.0
4.0 – 4.99 2.5
5.0 – 5.99 3.0
6.0 – 6.99 3.5
For Method see Guideline.

Clinical Guideline for the Prevention, Identification and Management of Hypoglycaemia of the Newborn
Page 21 of 24 V2.0
Appendix C Flowchart C. Blood glucose < 1.0mmol/l and / or clinical signs consistent with hypoglycaemia
Obtain intravenous (i.v.) access.
Collect blood sample for: laboratory confirmation of blood glucose, hypoglycaemiascreening tests and site a urine bag.
Consider screening and treatment for sepsis.
Admit to Neonatal Unit.
Give i.v. 10% glucose 2.5ml/kg.
Start IV infusion of 10% glucose at60ml/kg/d.
40% dextrose gel 200mg/kg massaged intothe buccal mucosa can be given while i.v.access is obtained OR intramuscularglucagon (200micrograms/kg)
Do not stop the establishment of breast feeding unless the baby is too sick to feed or there is a clinicalcontraindication to enteral feeding. Support expression of breast milk.
In formula fed infants, continue feeds if no contraindication to enteral feeding.
Recheck blood glucose after 30 minutes.
Is the blood glucose 1.0-2.5mmol/l and no abnormal clinical signs?
Increase glucose deliveryrate by 2mg/kg/minute byincreasing volume and/orconcentration of glucoseinfusion*.
Continue to feed if nocontraindication. Recheckblood glucose after 30min.
Blood glucose <1.0mmol/l or abnormal clinical signs.
Give IV 10% glucose2.5ml/kg.
Increase glucose deliveryrate by 2mg/kg/minuteby increasing volumeand/or concentration ofglucose infusion*.
Recheck BG after 30minutes.
Repeat cycle if BG<1.0mmol/l or there areabnormal clinical signs
Blood glucose >2.5mmol/l.
Slow wean of i.v. infusion.
Continue enteral feeds.
Continue to monitor bloodglucose until infant is on fullenteral feeds and bloodglucose values are>2.5mmol/l or 3.0mmol/l incases of hyperinsulinismover several fast-feed cyclesfor at least 24 hours
Unable to obtain immediate IV access
*If glucose infusion rate >8mg/kg/min, test forhyperinsulinism.

Clinical Guideline for the Prevention, Identification and Management of Hypoglycaemia of the Newborn
Page 22 of 24 V2.0
Appendix D Flowchart D. Management of reluctant feeding in healthy tem infants ≥ 37 weeks
Complete initial Breastfeeding assessment. Within 6 hours of birth or once feeding initiated. Assess:
Signs of effective feeding.
Pain Free
Maternal concerns.
Breast / Nipple damage.
Baby readiness to feed.
Monitor well-being*
Active feeding plan**
Maintain skin contact.
Review every 2 - 4 hours.
Actively encourage breastfeeding.
Offer feeds according tofeeding cues at least 8-10times in 24 hours whenfeeding is established.
If breast feeding: handexpress at least 8-10times in 24 hours(commence pumpingwhen milk comes in ifmother chooses to do so)
Continue to giveexpressed breast milk andactively support untilsuccessfullybreastfeeding.
Avoid teats, dummies andnipple shields.
Support mother andlisten/ action anyconcerns voiced regardingill- health.
Refer to neonatal team ifany concerns.
Monitor well-being ofbaby at least 4 hourly*.
Continue until feedingissue resolves
Monitor well-being of baby at least 4 hourly* Check:
Any maternal concerns.
Colour
Tone
Respiratory well-being.
Temperature
Alertness / level ofconsciousness.
Number and consistencyof wet and dirty nappies.
Risk for sepsis
If any signs of illness refer to neonatal team.
Any concerns about possible hypoglycaemia or ill-health refer to relevant guideline.
Birth
Dry baby / keep warm
Initiate and maintain skin toskin contact for at least 1 hr oruntil after 1
st feed
Encourage responsivenesswith mother
Discuss signs of readiness tofeed
First feed in skin to skincontact preferably within 1 hr
For babies being fed formulafollow the chart but giveformula milk instead ofcolostrum
Fed Effectively?
1-2 Hours following birth
Maintain skin to skincontact
Review in 1-2
Assess well-being of thebaby and recordobservations on the backpage of the Care pathway
If breastfeeding,encourage mother tohand express and givesmall amounts ofcolostrum to the baby
Fed Effectively?
6-8 hours followingbirth
Second feedcompleted
Fed effectively?
Once the baby is feeding successfully. Breastfeeding assessments as per local guidelines
NO
NO
NO
YES
YES
Initiate active feeding plan**

Clinical Guideline for the Prevention, Identification and Management of Hypoglycaemia of the Newborn
Page 23 of 24 V2.0
Appendix E – EHRA Form
A Due Regard, Equality & Human Rights Analysis form must be completed for all procedural documents used by East Sussex Healthcare NHS Trust. Guidance for the form can be found here on the Equality and Diversity Extranet page.
Due Regard, Equality & Human Rights Analysis
Title of document: Clinical Guideline for the Prevention, Identification and Management of Hypoglycaemia of the Newborn
Who will be affected by this work? SCBU and Maternity staff
Please include a brief summary of intended outcome: This guideline gives advice on the Prevention, Identification and Management of Hypoglycaemia of the Newborn. Hypoglycaemia if undiscovered can be severely damaging to the baby and can even cause death – therefore this new guideline for staff to follow gives clear guidance to identifying those babies at risk and managing them within the multidisciplinary team.
Yes/No Comments, Evidence & Link to main content
1. Does the work affect one group less or more favourably than another on the basis of: (Ensure you comment on any affected characteristic and link to main policy with page/paragraph number)
Age yes This guideline pertains to only newborns on the delivery suite and postnatal ward and SCBU.
Disability (including carers) No
Race No
Religion & Belief No
Gender No
Sexual Orientation (LGBT) No
Pregnancy & Maternity No
Marriage & Civil Partnership No
Gender Reassignment No
Other Identified Groups No
2. Is there any evidence that some groups are affected differently and what is/are the evidence source(s)?
No
3. What are the impacts and alternatives of implementing / not implementing the work / policy?
N/A
4. Please evidence how this work / policy seeks to “eliminate unlawful discrimination, harassment and victimisation” as per the Equality Act 2010?
N/A
5. Please evidence how this work / policy seeks to “advance equality of opportunity between people sharing a
N/A

Clinical Guideline for the Prevention, Identification and Management of Hypoglycaemia of the Newborn
Page 24 of 24 V2.0
protected characteristic and those who do not” as per the Equality Act 2010?
6. Please evidence how this work / policy will “Foster good relations between people sharing a protected characteristic and those who do not” as per the Equality Act 2010?
N/A
7. Has the policy/guidance been assessed in terms of Human Rights to ensure service users, carers and staff are treated in line with the FREDA principles (fairness, respect, equality, dignity and autonomy)
N/A
8. Please evidence how have you engaged stakeholders with an interest in protected characteristics in gathering evidence or testing the evidence available?
N/A
9. Have you have identified any negative impacts or inequalities on any protected characteristic and others? (Please attach evidence and plan of action ensure this negative impact / inequality is being monitored and addressed).
N/A