foodborne chemical toxins; (1) a report based on who-ferg
TRANSCRIPT

Foodborne Chemical Toxins; (1) A report based on WHO-FERG
Reza Afshari, MD, MPH, PhD BCCDC, Environmental Health Services
Thursday, December 17, 2015

Conflict of interest None declared. Findings of an expert group (Foodborne Epidemiology Reference Group).
WHO ESTIMATES OF THE GLOBAL BURDEN
OF FOODBORNE DISEASES could be obtained from: http://www.who.int/foodsafety/publications/foodborne_disease/fergreport/en/

Objectives • To present the 2015 WHO-FERG Foodborne
Chemical Toxin Report
• Potential implications for Canada and BC
• Contextualizing toxicological data for new
Canadians
WHO ESTIMATES OF THE GLOBAL BURDEN OF FOODBORNE
DISEASES WHO - FOODBORNE DISEASE BURDEN EPIDEMIOLOGY REFERENCE GROUP
2006 2009 2012 2015
Budget for 2009 583 000 $

What is the definition of “Food”?
Codex Alimentarius Commission-2: - Any substance, whether processed, semi-processed or raw, which is intended for human consumption, and includes drinks, chewing gum and any substance which has been used in the manufacture, preparation or treatment of food, but does not include cosmetics or tobacco or substances used only as drugs. - The definition also includes bottled drinks.

Animal Head Cooking!
.

What are “Foodborne diseases (FBD)” - Those diseases associated with the ingestion of contaminated food including microbial, viral, chemicals and …. What is “The burden of disease (BOD)” - The incidence, prevalence of morbidity, disability,
and mortality associated with acute and chronic manifestations of foodborne diseases. [Impact of a health problems as measured by mortality, morbidity, financial cost, or other indicators]
They look fresh, but are they safe?

Food is essential to human health. As such it should not be a matter of concern.
2. Food aid
1. Underweight Children (2000)

.
FERG-WHO reports (2007 to 2015)

Methodological approaches 1. Syndromic approach
Generation of a list organized by disease/syndrome to measure
GBD caused by toxins (via food)
2. Etiologic agent and risk factor approach
Using data on pathogens causing laboratory-confirmed diseases

For the global estimates, 31 foodborne hazards causing 32 diseases are included:
- 11 diarrhoeal disease agents (1 virus, 7 bacteria, 3 protozoa),
- 7 invasive infectious disease agents (1 virus, 5 bacteria, 1 protozoon),
- 10 helminths
- 3 chemicals + peanut allergies.

What chemicals in food have been studied?
1.Aflatoxin
2.Dioxin
3.Cyanide (in Cassava)
4.Peanut allergies

that consume cassava, and about 200 million people derive a substantial proportion of their daily calorie intake from cassava. Cassava roots contain cyanogeic compounds Endemic ataxic polyneuropathy (in southwest Nigeria and Kerala-in India) and Konzo, a paralytic disease (Mozambique, D.R. Congo, the United Republic Tanzania, and the Central African Republic). Plus Sporadic cases. Dark stem is also contaminated with aflatoxin.
Cassava cyanide
Cassava, a root crop, contains cyanogenic compounds in its edible parts. Over two thirds of the world population live in countries

Food allergies are the leading cause of emergency room visits for anaphylaxis, and most fatal or near fatal anaphylactic reactions are associated with peanut allergy. Peanut allergy prevalence is reported to be increasing in Western countries and some reports indicate that it has doubled from 1997 through 2002.
Peanut allergens
The prevalence of peanut allergy in the USA is estimated at about 0.6-1.0 %.

“Dioxins (including dioxin like PCBs) Industrial & natural (volcanic eruptions and forest fires.) 90% of human exposure is through food (meat, dairy products, fish and shellfish)
Accumulation in body fat to a steady state.
Total thyroxine (TT; decrease of TT4 in adult blood), pre-natal thyroid stimulating hormone (TSH; increase in TSH in neonatal blood),
Decrease in sperm cell count (impaired fertility) Increase in TSH across a physiological threshold indicating a disease status (incidence of hypothyroidism).

Aflatoxins
Are naturally occurring in foods include • B1 and B2 • G1 and G2 • Aflatoxins M1 and M2 are the hydroxylation products
of B1 and B2 found in milk and milk products
Potential health effects • Aflatoxin B1 is the most potent liver carcinogen • Growth impairment in children
• Immunosuppression • Acute poisoning (aflatoxicosis)
4125 abstracts were checked as relevant and 348 papers for final review were included.

Global chemical foodborne “illnesses” in 2010, a comparison of Four foodborne Chemicals
(n) Number of Global chemical foodborne “illnesses” in 2010. ---
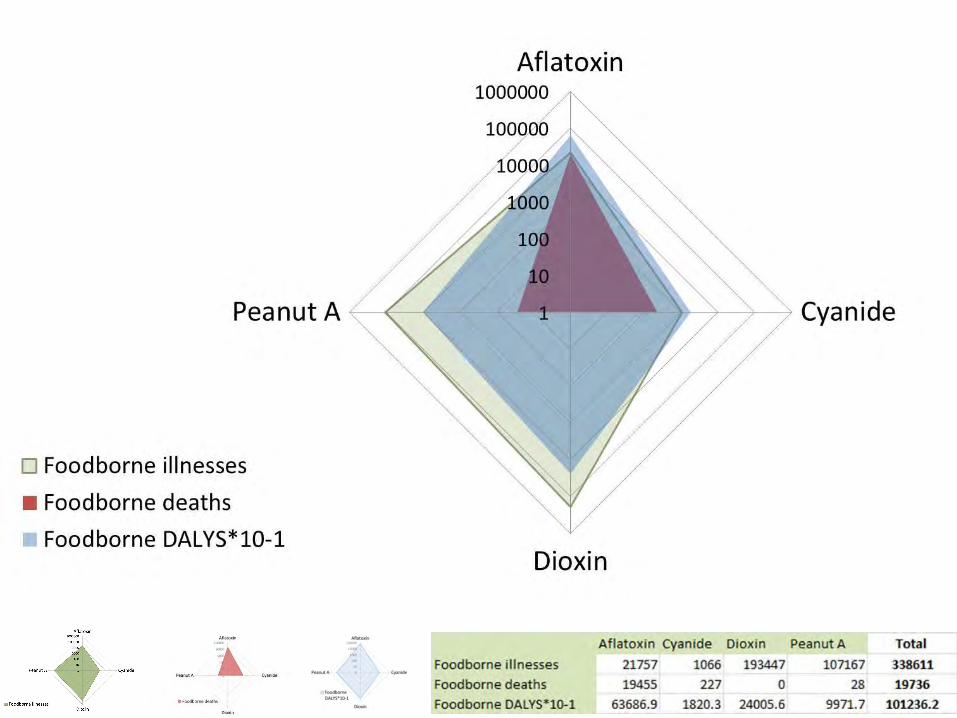
Logarithmic Scale

Comparison of WHO Regions

.
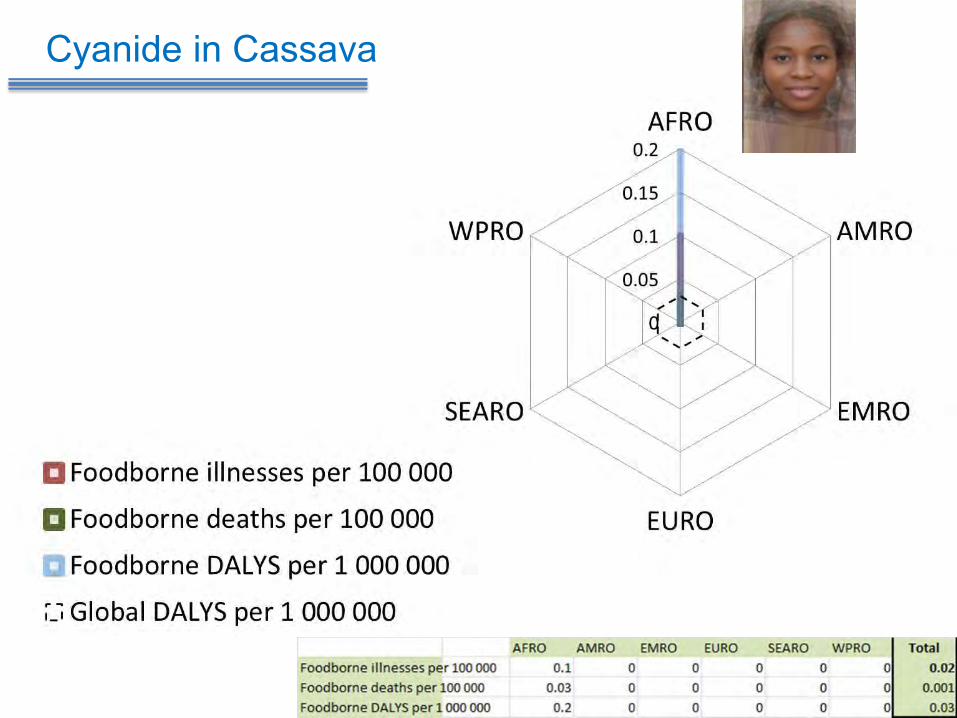
Cyanide in Cassava

Dioxin

Aflatoxin (Median rate)

. The relative contribution to the DALY incidence by each of
four chemicals for each of the WHO regions.
Peanut allergens
AMR WPR 1 EUR Australia ?


Foodborne Chemical Toxins; (2) Implications of this project for BC
Whose picture should we put at BC for health estimates?
27.5% of BC populations are new Canadians

Facts:
- BC receives a large numbers newcomers from various
WHO regions.
- Health data based on country of origin of immigrants are not available in Canada.
- Including minority immigrants as separate groups in future BC studies would substantially increase the sample size and cause studies to be more expensive.
- - - -

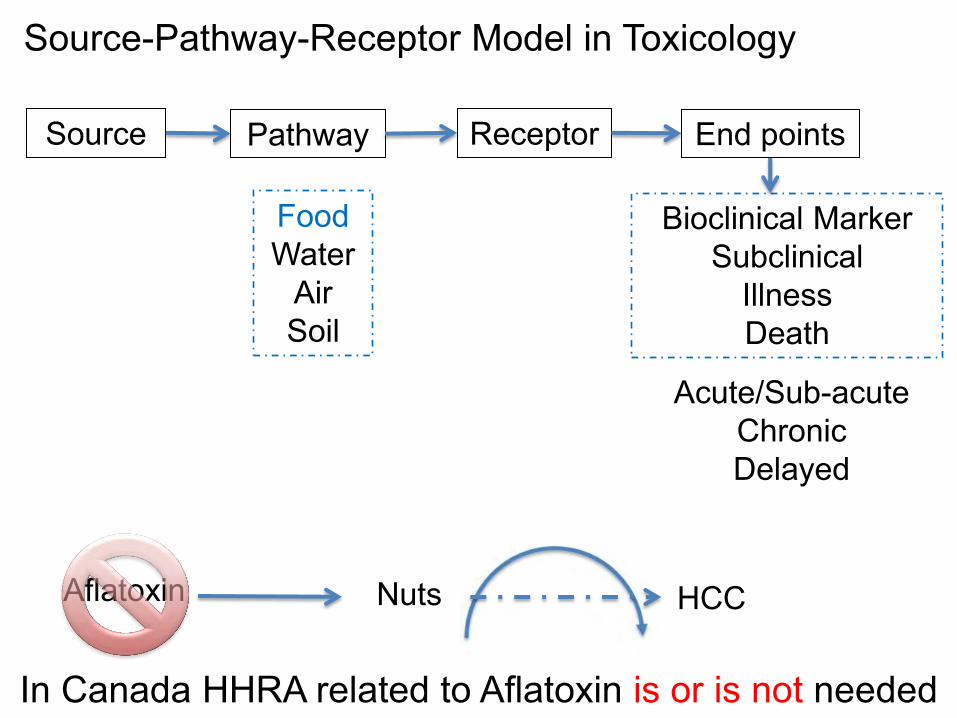
Source-Pathway-Receptor Model in Toxicology Source Pathway Receptor
Bioclinical Marker Subclinical
Illness Death
Food Water
Air Soil
Acute/Sub-acute Chronic Delayed
End points
HHRA is needed
Aflatoxin Nuts HCC
Source-Pathway-Receptor Model in Toxicology Source Pathway Receptor
Bioclinical Marker Subclinical
Illness Death
Food Water
Air Soil
Aflatoxin Nuts HCC
Acute/Sub-acute Chronic Delayed
In Canada HHRA related to Aflatoxin is or is not needed
End points

Global Geographic distributing of Chemical foodborne exposures

Diseases that could be attributed to chemical foodborne exposures in populations from different parts of the world

Toxic Exposures may have delayed complications

Great Grand Daughter in her
middle age
High risk of osteoporosis
2015 Toxic Exposures may have delayed
complications

Toxic Exposures may have delayed complications

Aflatoxin Exposure Estimated annual HCC 10-5 ng/kg b.w./day HBs Ag (-) HBs Ag (+) Canada 0.2-0.4 0.002-0.004 0.06-0.12 USA 0.26-1 0.003- 0.01 0.08-0.3 China 17-37 0.17-0.37 5.1-11.1
.
Estimated HCC incidence attributable to aflatoxin, by WHO region
Environmental Health Perspectives • volume 118 | number 6 | June 2010

Dose (mg) Overdose
Bio
logi
cal e
ffect
s (%
)
.001 .01 .1 1 10 100
Normal homeostasi
s
100
50
0
Cumulative risk of toxicity
Bio
logi
cal m
arke
r alo
ne
Duration of exposure (y) .01 .01 1 10 30 70
/ /
Maximum Allowable daily dose (mg)
Toxic exposure induced health end points are “dose” & “time” dependent

Dose (mg) Overdose
Bio
logi
cal e
ffect
s (%
)
.001 .01 .1 1 10 100
Normal homeostasi
s
100
50
0
Cumulative risk of toxicity
Bio
logi
cal m
arke
r alo
ne
Duration of exposure (y) .01 .01 1 10 30 70
/ /
Maximum Allowable daily dose (mg)
Sub
clin
ical
effe
cts
Toxic exposure induced health end points are “dose” & “time” dependent

Dose (mg) Overdose
Bio
logi
cal e
ffect
s (%
)
.001 .01 .1 1 10 100
Normal homeostasi
s
100
50
0
Cumulative risk of toxicity
Bio
logi
cal m
arke
r alo
ne
Duration of exposure (y) .01 .01 1 10 30 70
/ /
Maximum Allowable daily dose (mg)
Sub
clin
ical
effe
cts
Clin
ical
effe
cts
Toxic exposure induced health end points are “dose” & “time” dependent

Dose (mg) Overdose
Bio
logi
cal e
ffect
s (%
)
.001 .01 .1 1 10 100
Normal homeostasi
s
100
50
0
Cumulative risk of toxicity
Bio
logi
cal m
arke
r alo
ne
Duration of exposure (y) .01 .01 1 10 30 70
/ /
Maximum Allowable daily dose (mg)
Sub
clin
ical
effe
cts
Clin
ical
effe
cts
Dea
th
Toxic exposure induced health end points are “dose” & “time” dependent

40
1
0.1 1 10 20 30 40 50 60 70 Period of life (y)
/ /
Afla
toxi
n ex
posu
re
(ng/
kg b
.w./d
ay)
Living in BC
10000 1000 100 10 1 0.1
Living in BC
Afla
toxi
n at
tribu
ted
annu
al
burd
en o
f HC
C c
ases
Aflatoxin exposure (ng/kg b.w./day)
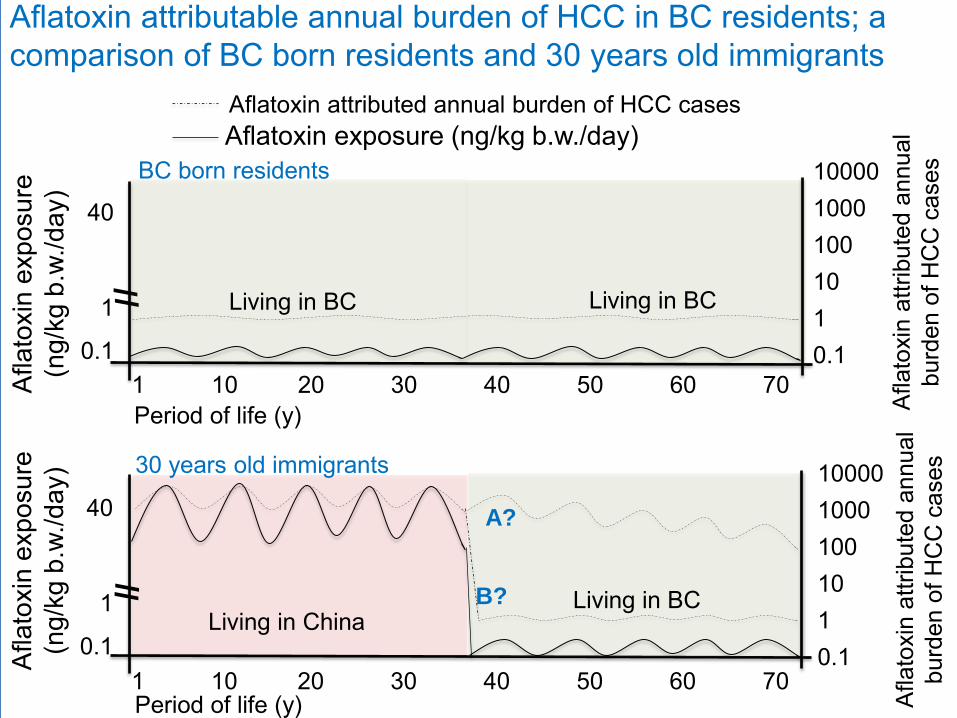
Aflatoxin attributable annual burden of HCC in BC residents; a comparison of BC born residents and 30 years old immigrants
Aflatoxin attributed annual burden of HCC cases
BC born residents
40
1
0.1 1 10 20 30 40 50 60 70 Period of life (y)
/ /
Afla
toxi
n ex
posu
re
(ng/
kg b
.w./d
ay)
Living in BC
10000 1000 100 10 1 0.1
Living in BC
Afla
toxi
n at
tribu
ted
annu
al
burd
en o
f HC
C c
ases
Aflatoxin exposure (ng/kg b.w./day)
Aflatoxin attributable annual burden of HCC in BC residents; a comparison of BC born residents and 30 years old immigrants
1 10 20 30 40 50 60 70 Period of life (y)
/ /
Afla
toxi
n ex
posu
re
(ng/
kg b
.w./d
ay)
Living in BC Living in China
40
1
0.1
10000 1000 100 10 1 0.1
A?
B?
Aflatoxin attributed annual burden of HCC cases
Afla
toxi
n at
tribu
ted
annu
al
burd
en o
f HC
C c
ases
BC born residents
30 years old immigrants

GBD; 2010, Population; 2005
Population Illnesses Deaths DALYS
Total 7 000 000 000 338 611 19 736 1 012 362
AMR 884 408 678 -- -- --
Canada-Total 35 200 000 1701 99 5087
BC-Total 4 600 000 222 13 665
BC-AMR 4 600 000 15+23* 0.34+0.28* 102
CB-27.5% immigrant (2006) 61 4 183 AMR calculation suffers; All America (population of 884 408 678) included and allergies were not included ** Allergies
Four chemicals (aflatoxin, dioxin, cyanide in cassava & peanut allergen) were globally responsible for 339,000 illnesses, 20,000 deaths and 1,012,000 DALYs in 2010. Assuming similar distribution of these problems in BC, chemical food poisoning accounts for 222 illnesses and 13 deaths (overestimated). For 27.5% population of BC immigrants, food poisoning would be accounted for 61 illnesses and 4 deaths.

.
Based on Norovirus
Cases Deaths DALYS N
orov
irus
Cam
pylo
bact
er s
sp.
Sal
mon
ella
s ss
p. (n
on
Afla
toxi
n C
yani
de/C
assa
va
Dio
xin
Pea
nut a
llerg
ies
Nor
oviru
s C
ampy
loba
cter
ssp
. S
alm
onel
las
ssp.
(non
A
flato
xin
Cya
nide
/Cas
sava
--
P
eanu
t alle
rgie
s
Nor
oviru
s C
ampy
loba
cter
ssp
. S
alm
onel
las
ssp.
(non
A
flato
xin
Cya
nide
/Cas
sava
D
ioxi
n --
Relative size of the problem Global

Data related to Canada • 6 major pathogens; Estimation from Thomas M.K. et al • 4 chemicals; Estimated numbers for 27% immigrants

Source-Pathway-Receptor Model in Toxicology Source Pathway Receptor
Bioclinical Marker Subclinical
Illness Death
Food Water
Air Soil
Aflatoxin Nuts HCC
Acute/Sub-acute Chronic Delayed
In Canada HHRA is not needed ?

Source-Pathway-Receptor Model in Toxicology
Customising for new Canadians
Current exposure
Previous exposure
In Canada HHRA IS NEEDED

In British Colombia (Canada) - I
1. Chemical foodborne diseases are less frequent illnesses in
comparison to pathogens foodborne diseases. Taking 27.5%
immigrants, however, they are similarly fatal.
2. Despite the fact that food in Canada is effectively monitored for
Aflatoxin, New Canadians have already been heavily exposed in
their country of origin.
Although chemical foodborne diseases are not a matter of “food
safety”, but they are a matter of “human health” in new
Canadians.
Chemical foodborne diseases deserve to receive as much if not
more scrutiny than Pathogen foodborne diseases.

In British Colombia (Canada) - II
3. New Canadians are coming from AFR, SEAR and WPR.
They have been exposed to aflatoxin for a long time in their
country of origin. They are at high risk of developing
hepatocellular carcinoma (HCC) similar to the findings of
FERG-WHO.
Highly fatal HCC is Secondary to viral hepatitis B or C and
Cirrhosis (alcoholism), aflatoxin exposure. Epidemiological
studies and animal models suggest synergism for HCC.

In British Colombia (Canada) - III
The following recommendations for New Canadians from West Pacific Region (China) could be discussed. • Physicians should be notified of their potential risks. • Diet advise (↓ nuts, ↓ non alcoholic fatty liver (obesity and
diabetes), ↓ heavy alcohol consumption, ↓ iron overload, … . (Coffee, vitamin K, Vit E, cilymarin, selenium…. may have preventive effect).
• Screening for other risk factors. • Screening for biomarkers and hemochromatosis…
(treatment depends on tumour size and staging) • Preventing “spread of the HCV” via safe injection practices. • Prevention via vaccination against hepatitis B • Perhaps secondary prevention (antiviral therapy) could
also be discussed in certain circumstances.

In British Colombia (Canada) - III
• Prevention via vaccination against hepatitis B Currently in BC [new suggestions that could be discussed] • All newcomers below age of 12 from regions of regions of
high Hep B prevalence [high aflatoxin exposed] (Asia and Africa) provided free.
• Individual with chronic liver disease (cirrhosis, liver damage with hemochromatosis [long time aflatoxin exposure] provided free.
• Persons visiting high HBV endemicity [high aflatoxin exposure >=6 years?] countries and staying >=6 months (not provided free)
• Communities in which HBV is highly endemic [long term exposure to aflatoxin] (not provided free)

In British Colombia (Canada) - IV
4. The following recommendations for New Canadians from South East Asia Region (India) could be seemed reasonable. In addition to Aflatoxin, they have been exposed to dioxin prior to their immigration. This exposure may lead to increase the risk of Hypo-thyroidism and low sperm counts. • Physicians should be notified for their potential risk.

In British Colombia (Canada) - V
5. Health policy decision making could and should be customised for new Canadians.
Available international data (such as this report by WHO FERG) related to different WHO regions [which are reliable and free] could [and probably should] be used as surrogate sources for health policy decision making for new comers, as health data are not available for them.

.
Raw data is available at http://dx.doi.org/10.5256/f1000research.7340.d107254
Special thanks to Dr Tom Kosatsky for his inputs in developing this presentation.