format 2015: food allergy and the brain
TRANSCRIPT

Food Allergy and the Brain
Attilio BonerUniversity ofVerona, Italy
Introduction
Micronutrients and Behaviour
Immunity & Ipersensitivity
Food Allergy&Ipersensitivity and Brain
Not only Food Allergy
Which came first?
Possible Mechanisms
Food-based Therapies
Conclusions

Clinically, allergy is characterized by
symptoms that, by in large, are secondary to
an altered nervous system
itchy and red eyes;
rhinorrhea, nasal congestion, and sneezing;
urge to cough, dyspnea, airway mucus secretion, and episodic reflex bronchospasm;
dysphagia, alteredgastrointestinal motility;
cutaneous itching and flare responses.
Allergy as an Immune-Neuronal Disorder

Clinically, allergy is characterized by
symptoms that, by in large, are secondary to
an altered nervous system
itchy and red eyes;
rhinorrhea, nasal congestion, and sneezing;
urge to cough, dyspnea, airway mucus secretion, and episodic reflex bronchospasm;
dysphagia, alteredgastrointestinal motility;
cutaneous itching and flare responses.
Allergy as an Immune-Neuronal Disorder
the immune-driveninflammation associated with allergic reactions might in some cases betrivial unless transduced
into the neurogenicsymptoms of suffering
(eg, itch, cough, bronchospasm,
motility disturbance,pain, sneeze,
skin conditions).

Neuromodulationduring the allergic reaction.Undem BJ,JACI 2014;133:1521
1) sensory (afferent) nerves sense the local
tissue environment.
2) in the centralnervous system the
signal induces
3) neurotransmitter release at
nerve’s synapse

Neuromodulationduring the allergic reaction.Undem BJ,JACI 2014;133:1521
1) sensory (afferent) nerves sense the local
tissue environment.
2) in the centralnervous system the
signal induces
3) neurotransmitter release at
nerve’s synapse
These symptoms occur because
mediators released during an allergic reaction can interact with sensory nerves,
change processing in the central
nervous system, and alter
transmission in sympathetic,
parasympathetic, and enteric
autonomic nerves.

Neuromodulation during the allergic reaction.Undem BJ, JACI 2014;133:1521
The allergic response comprises changes at all 3 levels of the neural arc:
These changes can be subdivided into:1) acute changes (overt activation of nerves that lasts only as long as
the stimulus is present),2) longer-lasting changes in neuroexcitability that can outlast the
stimulus by hours or days, and 3) the more persistent phenotypic changes that can last
for weeks and perhaps, when one considers the idea of developmental ‘‘critical periods,’’ for years.
sensory nerve function, CNS integration, andautonomic/enteric neuroeffector cell function.

C, Mast cells (green) near MrgA3 expressing
‘‘afferent itch nerves’’ (orange) in mouse skin
Mast cells are found in close proximity to nerves in virtually all organs. Undem BJ, JACI 2014;133:1521
A, Mast cell tryptase–positive cells (red) near PGP9.5-positive nerves
(green) in human intestinal submucosal plexus.
B, Mast cells (red) near synapsin-positive neurons
(green) in rat cardiac ventricle.
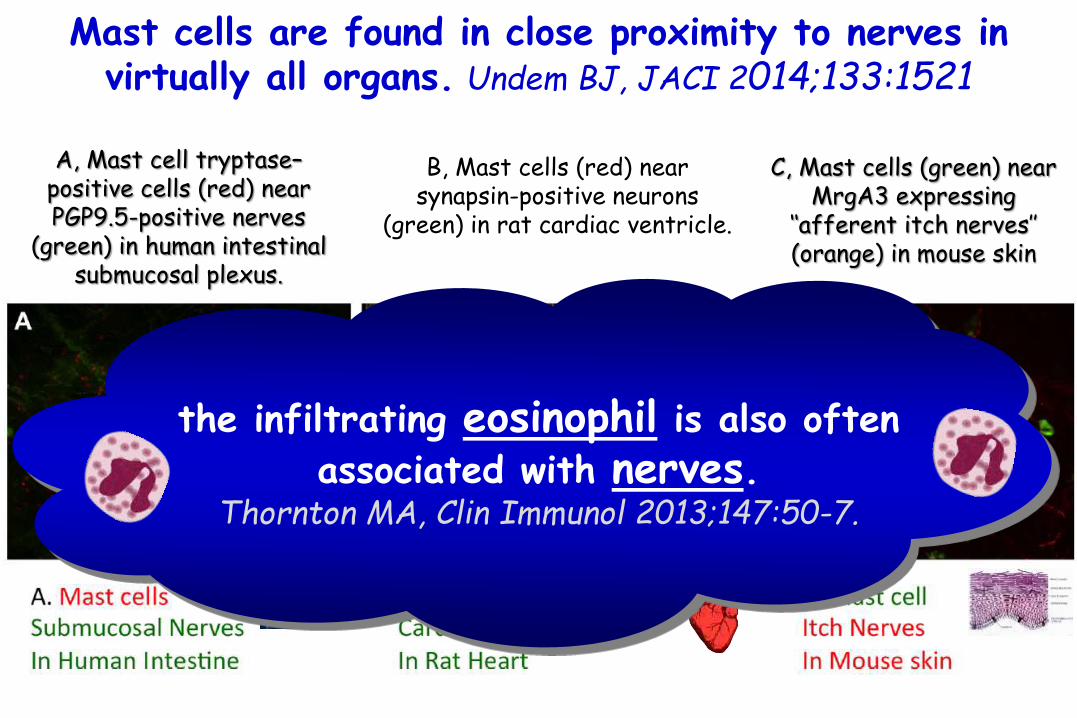
C, Mast cells (green) near MrgA3 expressing
‘‘afferent itch nerves’’ (orange) in mouse skin
Mast cells are found in close proximity to nerves in virtually all organs. Undem BJ, JACI 2014;133:1521
A, Mast cell tryptase–positive cells (red) near PGP9.5-positive nerves
(green) in human intestinal submucosal plexus.
B, Mast cells (red) near synapsin-positive neurons
(green) in rat cardiac ventricle.
the infiltrating eosinophil is also often
associated with nerves.Thornton MA, Clin Immunol 2013;147:50-7.

C, Mast cells (green) near MrgA3 expressing
‘‘afferent itch nerves’’ (orange) in mouse skin
Mast cells are found in close proximity to nerves in virtually all organs. Undem BJ, JACI 2014;133:1521
A, Mast cell tryptase–positive cells (red) near PGP9.5-positive nerves
(green) in human intestinal submucosal plexus.
B, Mast cells (red) near synapsin-positive neurons
(green) in rat cardiac ventricle.
fine nerve terminals in various tissues are also commonly associated also with other bone marrow–
derived cells, such as plasma cells.Arizono N, Lab Invest 1990;62:626-34.

Already in 400 B.C., Hippocrates described the importance of the gastrointestinal tract in health and disease, by stating
‘bad digestion is the root of all evil’
The enteric nervous system (ENS) discovered around 1900 is often described as the ‘second brain’ since it consists of a complexity comparable to the CNS.Costa M, Gut 2000;47(Suppl. 4):iv15–9.De Theije CGM, Pediatr Allergy Imm 2014;25:218

Gut feelings: the emerging biology of gut-brain communication.
Mayer EA. Nat Rev Neurosci2011:12:453–66
a | Endocrine, immune and neuronal afferent signalling from the gut to the CNS.
•Information about luminal factors and conditions of the gut are signalled through extrinsic vagal and spinal afferents to the brain stem and spinal cord, respectively. •Different stimuli can activate spinal, vagal and intrinsic primary afferents directly, withoutintermediary cells such as the enteroendocrine (EE) cells which act both in an endocrine and paracrinefashion. •Enterochromaffin (EC) cells signal to both intrinsic primary afferents and vagal afferents troughsecretion of serotonin (5-hydroxytryptamine; 5-HT).
Enteroendocrinecell

La funzione della serotonina è molteplice in quanto regola l’umore, induce al rilassamento, al piacere ed al benessere, interagisce con il ciclo sonno-veglia, stimola l’interesse sessuale, aumenta la sensibilità al dolore e condiziona l’aggressività.
La serotonina (neurotrasmettitore) interessa anche il sistema cardio-circolatorio, l’apparato respiratorio, regola l’attività gastrointestinale (la sua mancanza provoca stitichezza o la presenza eccessiva diarrea) e la temperatura corporea.
La serotonina (neurotrasmettitore) è implicata nelle emicranie e nelle cefalee, provocate dalla sua assenza.
La dopamina crea le sensazioni di soddisfazione, gratificazione sessuale, motivazione (o della punizione), stimolando l’attenzione, la memoria, l’apprendimento (legato al lavoro), il comportamento, la cognizione ed il movimento volontario. La dopamina Agisce sul sistema simpatico (sistema nervoso autonomo), causando l’aumento della pressione sanguigna e del battito cardiaco.

Gut feelings: the emerging biology of gut-brain communication.
Mayer EA. Nat Rev Neurosci2011:12:453–66
a | Endocrine, immune and neuronal afferent signalling from the gut to the CNS.
•Information about luminal factors and conditions of the gut are signalled through extrinsic vagal and spinal afferents to the brain stem and spinal cord, respectively. •Mechanical stimuli (stretch, pressure, distortion and shearing forces) can activate spinal, vagal and intrinsic primary afferents (IPANs) directly, withoutintermediary cells such as the enteroendocrine (EE) cells. •Signalling molecules (including proteases, histamine, serotonin and cytokines) that are produced by immunecells in Peyer's patches and within the gut epithelium can activate their respective receptors on vagal and spinal afferents.

Gut feelings: the emerging biology of gut-brain communication.
Mayer EA. Nat Rev Neurosci2011:12:453–66
a | Endocrine, immune and neuronal afferent signalling from the gut to the CNS.
•Similarly, neuropeptides and hormones (gut peptides) that are released from enteroendocrine(EE) cells in response to other luminal factors, such as nutrients, toxins or antigens, can act both in an endocrine fashion, reaching targets in the brain (area postrema, dorsal vagal complex and hypothalamus), and through receptor activation on spinal and vagal afferents, in a paracrine fashion.
•Enterochromaffin (EC) cells signal to both intrinsic primary afferents (IPANs) and vagal afferents trough secretion of serotonin(5-hydroxytryptamine; 5-HT).
Enteroendocrinecell

Gut feelings: the emerging biology of gut-brain communication.
Mayer EA. Nat Rev Neurosci2011:12:453–66
b | Encoding of multiple luminal signals by enteroendocrine (EE) cells.
•Different classes of enterochromaffin (EE) cells are interspersed between gut epithelial cells throughout the gastrointestinal tract.
•Upon luminal stimulation (or upon activation by postganglionic sympathetic or vagal nerves), these cells can release up to 20 different gut peptides from their basolateral (and possibly luminal) surface.
•Released peptides can activate closely adjacent vagalafferent nerve terminals in a paracrine fashion, or when released into the circulation they can exert an endocrine effect, signalling to various sites in the brain and other parts of the gastrointestinal tract. Enteroendocrine
cell
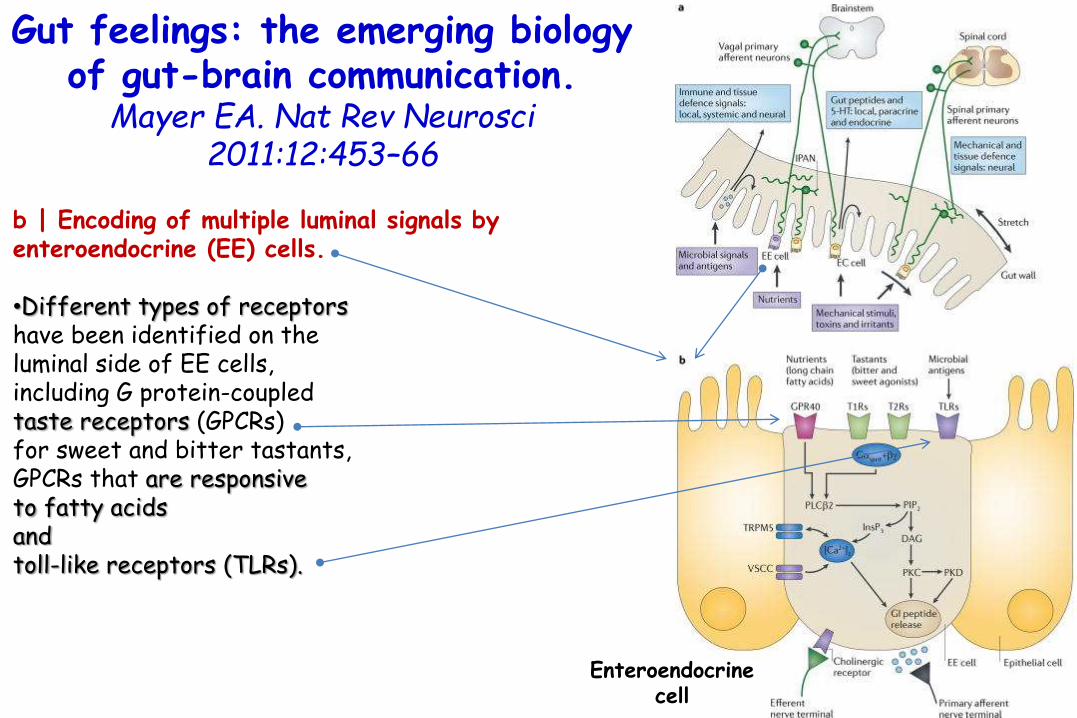
Gut feelings: the emerging biology of gut-brain communication.
Mayer EA. Nat Rev Neurosci2011:12:453–66
b | Encoding of multiple luminal signals by enteroendocrine (EE) cells.
•Different types of receptorshave been identified on the luminal side of EE cells, including G protein-coupledtaste receptors (GPCRs) for sweet and bitter tastants, GPCRs that are responsiveto fatty acidsand toll-like receptors (TLRs).
Enteroendocrinecell

Gut feelings: the emerging biology of gut-brain communication.
Mayer EA. Nat Rev Neurosci2011:12:453–66
b | Encoding of multiple luminal signals by enteroendocrine (EE) cells.
•The intestinal taste receptors that are shown are coupled to a specific Gα protein subunit, gustducin(Gαgust), and receptor-induced increases in intracellularcalcium result in peptide release from the basolateralmembrane. [Ca2+]i, intracellular calcium concentration; DAG, diacylglycerol; GI peptide, gastrointestinal peptide; GPR40, G protein-coupled receptor 40; InsP3, Inositol-1,4,5-trisphosphate;. PIP2, aquaporin PIP2 member; PKC, proteinkinase C; PLCβ2, phospholipase Cβ; T1R, taste receptor type 1 member; TRPM5, transient receptor potential cation channelsubfamily M member 5 (specifically linked to taste receptor signalling); VSCC, voltage-sensitive Ca2+ channel. Enteroendocrine
cell

Gut feelings: the emerging biology of gut-brain communication.
Mayer EA. Nat Rev Neurosci2011:12:453–66
Gut–brain signalling related to food intake•Nutrient-related signals reach the CNS through spinal, vagal and endocrine signalling pathways. •Endocrine signalling of gut peptides that are released into the systemic circulation reach the dorsal vagal complex through the area postrema where they modulate the transmission of afferent vagal signals to the dorsal motor nucleus. •These gut peptides also reach specialized neurons within the hypothalamus. •Paracrine signals activate function-specific vagal afferent fibres that ultimately signal to subregions of the anterior insula (aINS). area postrema

Gut feelings: the emerging biology of gut-brain communication.
Mayer EA. Nat Rev Neurosci2011:12:453–66
Gut–brain signalling related to food intake
•The sensory aspect of taste is primarily encoded in the anterior insula (aINS), but the multimodal integration of satiety signals with the sensory properties of food (including its flavour, palatability and reward value) as well as the context of food intake (including food related visual and auditory signals) occurs in the orbitofrontal cortex (OFC).

Gut feelings: the emerging biology of gut-brain communication.
Mayer EA. Nat Rev Neurosci2011:12:453–66
Gut–brain signalling related to food intake
•Further integration with inputs from the reward system and with interoceptivememories of previous food ingestiongenerates a multidimensionalfood-related experience that ultimatelydetermines ingestive behaviour.
•Prefrontal regions exert cognitive control over ingestive behaviours.
•Learning about food-related experiencesand the formation of interoceptivememories is an important aspect of the cortical circuitry that is involved in thisprocess.
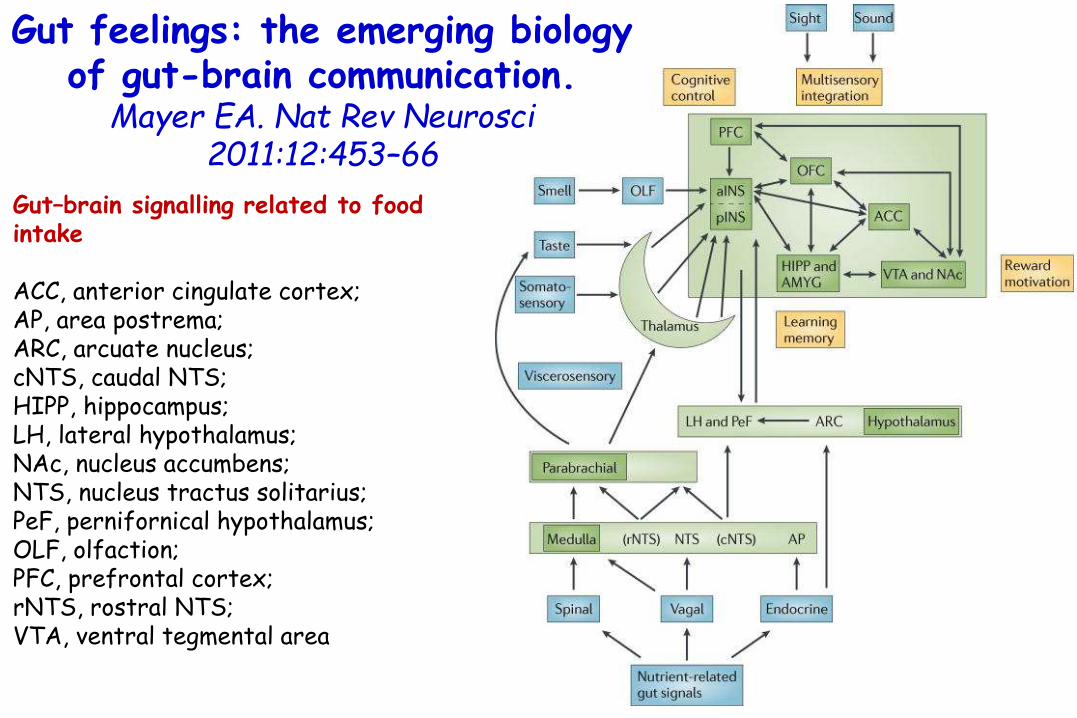
Gut feelings: the emerging biology of gut-brain communication.
Mayer EA. Nat Rev Neurosci2011:12:453–66
Gut–brain signalling related to food intake
ACC, anterior cingulate cortex; AP, area postrema; ARC, arcuate nucleus; cNTS, caudal NTS; HIPP, hippocampus; LH, lateral hypothalamus;NAc, nucleus accumbens; NTS, nucleus tractus solitarius; PeF, pernifornical hypothalamus; OLF, olfaction; PFC, prefrontal cortex; rNTS, rostral NTS; VTA, ventral tegmental area

Paracrine signaling is a form of cell-cell communication in which a cell produces a signal to induce changes in nearby cells, altering the behavior or differentiation of those cells.
Signaling molecules known as paracrine factors diffuse over a relatively short distance (local action), as opposed to endocrine factors (hormones which travel considerably longer distances via the circulatory system), juxtacrine interactions, and autocrine signaling.
Cells that produce paracrine factors secrete them into the immediate extracellular environment. Factors then travel to nearby cells in which the gradient of factor received determines the outcome.
Paracrine and Endocrine Signaling

Bidirectional communications between the brain and the gutoccur via various pathways, involving the vagus nerve, autonomic nervous system and neuroimmune interactions both in the GI tract and in the brain.Kennedy PJ, Neurosci Biobehav Rev2012: 36: 310–40.
Over the past few decades, strong correlations have been observed between the occurrence of GI problems and psychiatric disorders.Cryan JF, Neurogastroenterol Motil2011: 23: 187–92

Allergen challenge is often associated with the overt activation of afferent nerve terminals leading to action
potential discharge of afferent C-fibers
C-fibers(pain, cough, itch)
are known to express receptorsfor many chemical mediators that, present in the
allergicallyinflamed tissue,
lead to nervemembrane
depolarization.
1° mediators
2°receptors
3°depolarization

Neuromodulation takes place also at the level of gene expression.
The allergic reaction can lead to production and release of neurotrophic factors from mast cells in the local environment of the nerve terminals where they influence nerves’ gene expression.
‘‘nerves phenotypic switch’’
an intense quantitative increase in action potential volleys at the
central terminals of afferent C-fibers to the CNS
Undem BJ, JACI 2014;133:1521
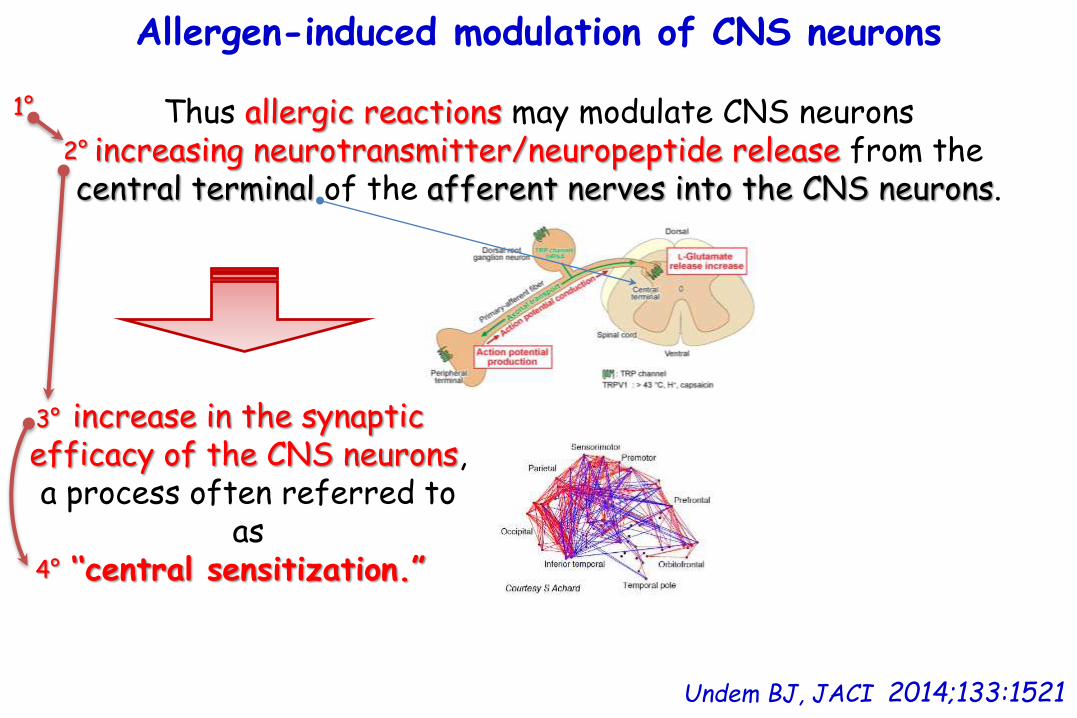
Allergen-induced modulation of CNS neurons
Undem BJ, JACI 2014;133:1521
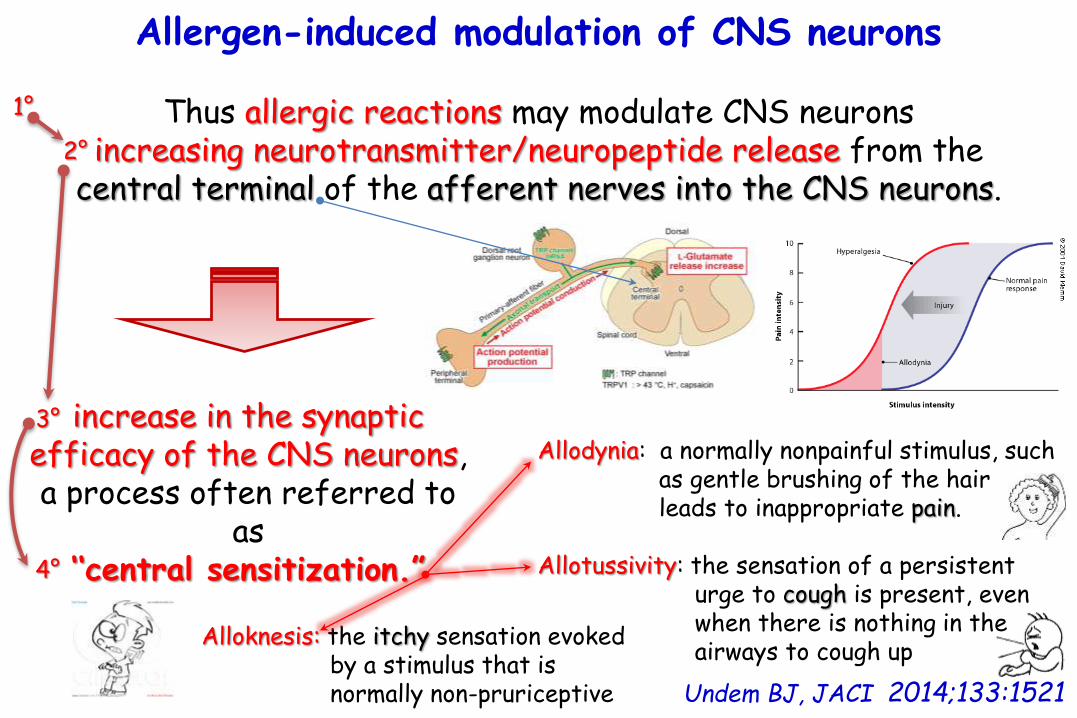
Thus allergic reactions may modulate CNS neuronsincreasing neurotransmitter/neuropeptide release from the
central terminal of the afferent nerves into the CNS neurons.
increase in the synaptic efficacy of the CNS neurons, a process often referred to
as ‘‘central sensitization.”
1°
2°
3°
4°
Allergen-induced modulation of CNS neurons
Undem BJ, JACI 2014;133:1521
Thus allergic reactions may modulate CNS neuronsincreasing neurotransmitter/neuropeptide release from the
central terminal of the afferent nerves into the CNS neurons.
increase in the synaptic efficacy of the CNS neurons, a process often referred to
as ‘‘central sensitization.”
Allodynia: a normally nonpainful stimulus, such as gentle brushing of the hair leads to inappropriate pain.
Allotussivity: the sensation of a persistent urge to cough is present, even when there is nothing in the airways to cough up
Alloknesis: the itchy sensation evoked by a stimulus that is normally non-pruriceptive
1°
2°
3°
4°

Alloknesis: the itchy sensation evoked by a stimulus that is normally non-pruriceptive
Allergen-induced modulation of CNS neurons
Undem BJ, JACI 2014;133:1521
Thus allergic reactions may modulate CNS neuronsincreasing neurotransmitter/neuropeptide release from the
central terminal of the afferent nerves into the CNS neurons.
increase in the synaptic efficacy of the CNS neurons, a process often referred to
as ‘‘central sensitization.”
Allodynia: a normally nonpainful stimulus, such as gentle brushing of the hair leads to inappropriate pain.
Allotussivity: the sensation of a persistent urge to cough is present, even when there is nothing in the airways to cough up
A clinically relevant aspect of central sensitization is that it provides a
mechanism whereby an allergic reaction in
one location can influence the physiology of a disparate location.
1°
2°
3°
4°

Alloknesis: the itchy sensation evoked by a stimulus that is normally non-pruriceptive
Allergen-induced modulation of CNS neurons
Undem BJ, JACI 2014;133:1521
Thus allergic reactions may modulate CNS neuronsincreasing neurotransmitter/neuropeptide release from the
central terminal of the afferent nerves into the CNS neurons.
increase in the synaptic efficacy of the CNS neurons, a process often referred to
as ‘‘central sensitization.”
Allodynia: a normally nonpainful stimulus, such as gentle brushing of the hair leads to inappropriate pain.
Allotussivity: the sensation of a persistent urge to cough is present, even when there is nothing in the airways to cough up
1) stimulation of C-fibers in the larynx can enhance
parasympathetic drive to the peripheral airways.
2) C-fiber activation in the esophagus (eg, during acid
reflux) can lead to the urge to cough through enhancing synaptic
activity of A-fibersin the trachea.
1°
2°
3°
4°

Alloknesis: the itchy sensation evoked by a stimulus that is normally non-pruriceptive
Allergen-induced modulation of CNS neurons
Undem BJ, JACI 2014;133:1521
Thus allergic reactions may modulate CNS neuronsincreasing neurotransmitter/neuropeptide release from the
central terminal of the afferent nerves into the CNS neurons.
increase in the synaptic efficacy of the CNS neurons, a process often referred to
as ‘‘central sensitization.”
Allodynia: a normally nonpainful stimulus, such as gentle brushing of the hair leads to inappropriate pain.
Allotussivity: the sensation of a persistent urge to cough is present, even when there is nothing in the airways to cough up
Allergen challenge in the nose can lead to central sensitization of lower airway cough nerves.
This raises the possibility that cough associated with gastroesophageal reflux is
not secondary to microaspiration of substances into the airways and that cough
associated with nasal allergy is not necessarily secondary to ‘‘postnasal drip’’
and the direct activation of cough nerves, as much as it is due to central sensitization of the cough pathway by converging esophageal
and nasal nociceptors.
1°
2°
3°
4°

Allergen-induced modulation of CNS neurons
Central sensitization in allergy is supported by studies with young adult rhesus monkeys.
After sensitization to house dust mite, monkeys were repeatedly challenged with house dust mite–containing aerosol.
Approximately 5 to 6 months later, the electrical excitability ofneurons in the nucleus of the solitary tract were found to be strongly upregulated; their responsiveness to a given input stimulus was much stronger than that seen with similar neurons from nonallergic monkeys.
Extended allergen exposure in asthmatic monkeys induces neuroplasticity in nucleus tractus solitarius. Chen CY, J Allergy Clin Immunol 2001;108:557-62.

Allergen-induced modulation of CNS neurons
Central sensitization
Extended allergen exposure in asthmatic monkeys induces neuroplasticity in nucleus tractus solitarius. Chen CY, J Allergy Clin Immunol 2001;108:557-62.
monkeys sensitized to house dust mite and repeatedly challenged with house
dust mite–containing aerosol
5 to 6 months laterstrongly upregulation of excitability of neurons
in the nucleus of the solitary tract their responsiveness to a given input stimulus
was much stronger than that seen with similar neurons from nonallergic monkeys.

Extended allergen exposure in asthmatic monkeys induces neuroplasticity in nucleus tractus solitarius. Chen CY, J Allergy Clin Immunol 2001;108:557-62.
A, Photomicrograph of a patch-clamped neuron in a brain slice from the caudomedial nucleus of the solitary tract, which is where the vagal sensory afferents terminate.
B, recordings of depolarizing
current pulses C, Increasedactionpotential discharge in response to depolarizing stimulus

Allergic modulation of efferent enteric nerves
Of particular relevance to food allergy, immunologic activation of mast cells in the gut is commonly associated with alterations inneurotransmission within the enteric ganglia, thereby increasing the synaptic activity of submucosal neurons.

Allergic modulation of efferent enteric nerves
There is evidence that mast cell activation leads to more neurotransmitter (typically acetylcholine) released from the presynaptic terminals per givenamount of stimulus.
Allergen challenge can also lead to an increase in autonomic neurotransmitter release from the postganglionic peripheral terminals per a given amount of stimulus.
(+)
(+)Undem BJ, JACI 2014;133:1521
Concept of modulation in critical periods: early life
Undem BJ, JACI 2014;133:1521
There may be a potential role of ‘‘critical periods’’ in allergen-induced neuromodulation because these changes can persist for years or even a lifetime.
It is well established that the development of sensory systemsoften requires use-dependent activity early in life(experience-dependent plasticity). Berardi N, Curr Opin Neurobiol 2000;10:138.
Thus, for example, if a young animal is deprived of vision by lid closure, changes occur in the neural circuitry of the visual cortex, leading to severe and permanent loss in visual acuity.
Even prolonged vision deprivation after the critical period is withoutan effect on visual acuity.

Undem BJ, JACI 2014;133:1521
Allergic (or infectious)inflammation in critical periods therefore raises the possibility that the inflammatory response might leave behind a nervous system that is subtly altered many years later, such that a mildinflammatory insult could lead to overly exaggerated responses.
Concept of modulation in critical periods: early life

Undem BJ, JACI 2014;133:1521
Allergic inflammation in critical periods
nervous system subtly altered many years later,
such that a mildinflammatory insult could
lead to overly exaggerated responses.
Concept of modulation in critical periods: early life
first 1000 days

Undem BJ, JACI 2014;133:1521
Allergic inflammation in critical periods
nervous system subtly altered many years later,
such that a mildinflammatory insult could
lead to overly exaggerated responses.
Concept of modulation in critical periods: early life
first 1000 days
The prevalence of food allergy peaks in
the first 2 years of life.
Berin MC, Sampson HA. Food allergy:
an enigmatic epidemic. Trends Immunol. 2013; 8:390–397.

Bidirectional communications between the brain and the gutoccur via various pathways, involving the vagus nerve, autonomic nervous system and neuroimmune interactions both in the GI tract and in the brain.Kennedy PJ, Neurosci Biobehav Rev2012: 36: 310–40.
Over the past few decades, strong correlations have been observed between the occurrence of GI problems and psychiatric disorders.Cryan JF, Neurogastroenterol Motil2011: 23: 187–92
Food allergy is suggested to be one of the GI triggers
for various psychologic
and psychiatric conditions

Bidirectional communications between the brain and the gutoccur via various pathways, involving the vagus nerve, autonomic nervous system and neuroimmune interactions both in the GI tract and in the brain.Kennedy PJ, Neurosci Biobehav Rev2012: 36: 310–40.
Over the past few decades, strong correlations have been observed between the occurrence of GI problems and psychiatric disorders.Cryan JF, Neurogastroenterol Motil2011: 23: 187–92
Allergic reactions to food are primarily
observed in children, and an association with
neurodevelopmentaldisorders has therefore been
proposed.de Theije CG,
Pediatr Allergy Immunol. 2014;25(3):218-26

Food Allergy and the Brain
Attilio BonerUniversity ofVerona, Italy
Introduction
Micronutrients and Behaviour
Immunity & Ipersensitivity
Food Allergy&Ipersensitivity and Brain
Not only Food Allergy
Which came first?
Possible Mechanisms
Food-based Therapies
Conclusions
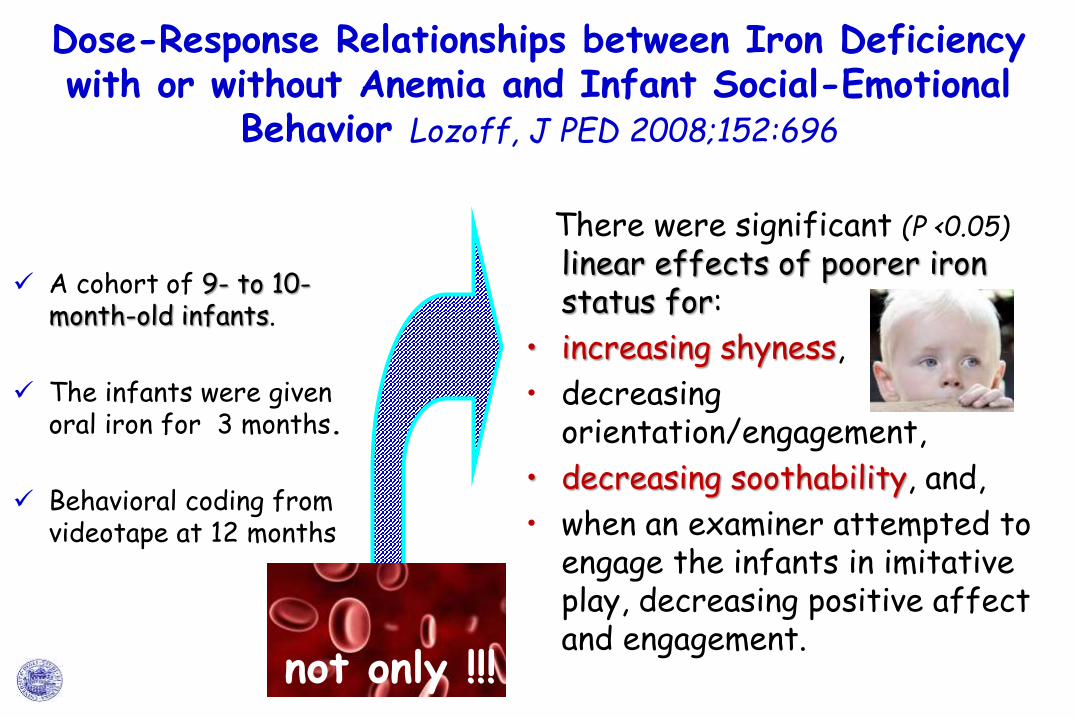
A cohort of 9- to 10-month-old infants.
The infants were givenoral iron for 3 months.
Behavioral coding fromvideotape at 12 months
Dose-Response Relationships between Iron Deficiency with or without Anemia and Infant Social-Emotional
Behavior Lozoff, J PED 2008;152:696
There were significant (P <0.05)
linear effects of poorer ironstatus for:
• increasing shyness,
• decreasingorientation/engagement,
• decreasing soothability, and,
• when an examiner attempted toengage the infants in imitative play, decreasing positive affectand engagement.
not only !!!

A cohort of 9- to 10-month-old infants.
The infants were givenoral iron for 3 months.
Behavioral coding fromvideotape at 12 months
Dose-Response Relationships between Iron Deficiency with or without Anemia and Infant Social-Emotional
Behavior Lozoff, J PED 2008;152:696
There were significant (P <0.05)
linear effects of poorer ironstatus for:
• increasing shyness,
• decreasingorientation/engagement,
• decreasing soothability, and,
• when an examiner attempted toengage the infants in imitative play, decreasing positive affectand engagement.
not only !!!
Infant social-emotional behavior appears to be adversely affected by Iron
Deficiency with or without
anemia.

Iron Deficiency Anemia and Cognitive Function in Infancy Carter Pediatrics 2010;126;e427
Effects of iron deficiency anemia (IDA) on specific domains of infant cognitive function
IDA was defined as hemoglobin level<110 g/L with/or ≥2 abnormal iron deficiency indicators (mean corpuscular volume, red cell distribution width, zinc protoporphyrin, transferrin saturation, ferritin)
At 9 and 12 months, the Fagan Test of Infant Intelligence (FTII); A-not-B task; Emotionality, Activity, and Sociability Temperament Survey; and Behavior Rating Scale
Infants with IDA showed poorer recognition memory
The Behavior Rating Scale orientation/engagement measure partially mediated these effects

Iron-Deficiency Anemia in Infancy and Social Emotional Development in Preschool-Aged Chinese Children
Chang Pediatrics 2011;127:e927
Children with iron-deficiency anemia (IDA) in infancy whose anemia was not corrected before 24 months (chronic IDA) (n=27).
Children with IDA in infancy whose anemia was correctedbefore 24 months (corrected IDA) (n=70).
Children who were non-anemic in infancy and at 24 months (n =64).
Children who had chronic IDA in infancy at age 4 yrs displayed: 1.less positive affect
and frustration tolerance;
2.more passive behavior and physical self-soothing in the stranger approach;
3.delay of gratification.

Iron-Deficiency Anemia in Infancy and Social Emotional Development in Preschool-Aged Chinese Children
Chang Pediatrics 2011;127:e927
In contrast,the behavior and affect
of children whoseanemia was correctedbefore 24 mo of age
were comparableto those of children who
were non-anemic throughout infancy.
Children with iron-deficiency anemia (IDA) in infancy whose anemia was not corrected before 24 months (chronic IDA) (n=27).
Children with IDA in infancy whose anemia was correctedbefore 24 months (corrected IDA) (n=70).
Children who were non-anemic in infancy and at 24 months (n =64).
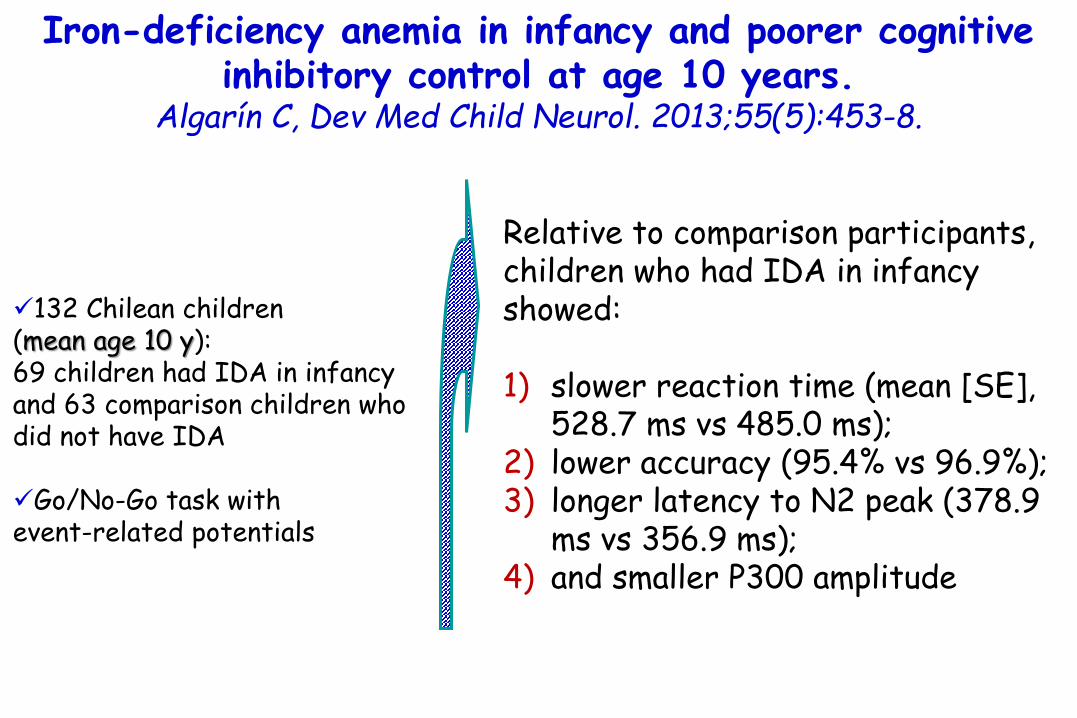
Iron-deficiency anemia in infancy and poorer cognitive inhibitory control at age 10 years.
Algarín C, Dev Med Child Neurol. 2013;55(5):453-8.
132 Chilean children (mean age 10 y): 69 children had IDA in infancy and 63 comparison children who did not have IDA
Go/No-Go task with event-related potentials
Relative to comparison participants, children who had IDA in infancy showed:
1) slower reaction time (mean [SE], 528.7 ms vs 485.0 ms);
2) lower accuracy (95.4% vs 96.9%); 3) longer latency to N2 peak (378.9
ms vs 356.9 ms); 4) and smaller P300 amplitude

Functional Significance of Early-Life Iron Deficiency: Outcomes at 25 Years Lozoff J Ped 2013;163:1260
At 25 years, 33 subjects with chronic iron deficiency in infancy vs 89 who were iron-sufficient before and/or after iron therapy.
Education, employment, marital status, and physical and mental health.
•Anemia was defined as Hb ≤105 g/L non-anemia as Hb ≥120 g/L, Hb concentration 106-119 g/L considered intermediate.
•Iron deficiency was defined as - serum ferritin <12 ng/mL and - free erythrocyte protoporphyrin
≥1.77 µmol/L (100 µg/dL) of red blood cells and/or
- transferrin saturation <10%

Functional Significance of Early-Life Iron Deficiency: Outcomes at 25 Years Lozoff J Ped 2013;163:1260
% subjects who did not complete secondary school
58.1%
chronic irondeficiency
iron sufficient
60 –
50 –
40 –
30 –
20 –
10 –
0
19.8%
p=0.003
At 25 years, 33 subjects with chronic iron deficiency in infancy vs 89 who were iron-sufficient before and/or after iron therapy.
Education, employment, marital status, and physical and mental health.
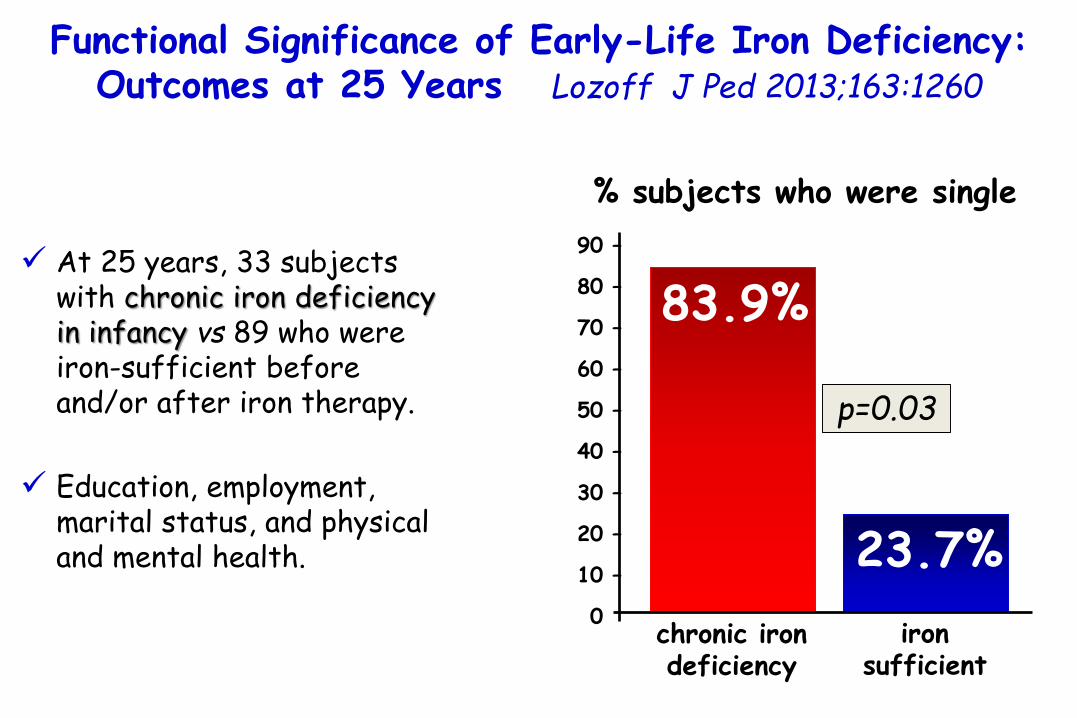
Functional Significance of Early-Life Iron Deficiency: Outcomes at 25 Years Lozoff J Ped 2013;163:1260
% subjects who were single
83.9%
chronic irondeficiency
iron sufficient
23.7%
90 –
80 –
70 –
60 –
50 –
40 –
30 –
20 –
10 –
00
p=0.03
At 25 years, 33 subjects with chronic iron deficiency in infancy vs 89 who were iron-sufficient before and/or after iron therapy.
Education, employment, marital status, and physical and mental health.

Functional Significance of Early-Life Iron Deficiency: Outcomes at 25 Years Lozoff J Ped 2013;163:1260
83.9%
chronic irondeficiency
iron sufficient
23.7%
90 –
80 –
70 –
60 –
50 –
40 –
30 –
20 –
10 –
00
p=0.03
They reported poorer emotional health and more negative emotions and
feelings of dissociation/detachment.
At 25 years, 33 subjects with chronic iron deficiency in infancy vs 89 who were iron-sufficient before and/or after iron therapy.
Education, employment, marital status, and physical and mental health.
% subjects who were single

Functional Significance of Early-Life Iron Deficiency: Outcomes at 25 Years Lozoff J Ped 2013;163:1260
indirect paths for chronic iron deficiency and not completing
secondary school via
poorer cognitive functioning in early adolescence
more negative emotions via behavior problems in adolescence, indicating a cascade of adverse outcomes.
At 25 years, 33 subjects with chronic iron deficiency in infancy vs 89 who were iron-sufficient before and/or after iron therapy.
Education, employment, marital status, and physical and mental health.

Neuropsychosocial Deficits Associated with Iron Deficiency: How Long Do They Last? Editorial
Trimm J Ped 2013;163:1242
Iron deficiency anemia (IDA) is more prevalent in pregnant women and young children.
Brain development in utero through early childhood requires adequate availability of iron.
Insufficient quantities of iron interfere with neuronal and glialdevelopment, neurotransmitter production, and myelination.
The consequences of these disturbances include cognitive, motor, and emotional dysfunction.
From studies that focus on early and prompt treatment of iron deficiency anemia . It is not evident that iron supplementation reverses the disruption to brain development.
The persistence of cognitive, motor, emotional, academic, and social concerns suggests long-term or permanent disruption.
A recent systematic review of daily iron supplementation in 2-to 5- year-old children identified increases in hemoglobin and ferritin. However, improvement in clinically important outcomes like cognitive development was not found.
Neuropsychosocial Deficits Associated with Iron Deficiency: How Long Do They Last? Editorial
Trimm J Ped 2013;163:1242
What has to be done
Promoting access to and intake of adequate nutrition by women prior to and during pregnancy.
Once born, children at risk of developing iron deficiency should be identified as soon as possible.
1) inadequate access to age-appropriate balanced diet, 2) low intake of protein paired with high intake of cereals/legumes, 3) preterm delivery or 4) low birth weight.
Neuropsychosocial Deficits Associated with Iron Deficiency: How Long Do They Last? Editorial
Trimm J Ped 2013;163:1242

Iron supplementation in infancy contributes to more adaptive behavior at 10 years of age.
Lozoff B, J Nutr. 2014 Jun;144:838-45.
Healthy Chilean infants free of Iron Deficiency Anemia at age 6 mo were randomly assigned to iron supplementation or no added iron (formula with iron/powdered cow milk, vitamins with/without iron) from ages 6 to 12 mo.
Follow-up at age 10 yrs
Compared with the no-added-iron group children in the iron-supplemented group were:
1) more cooperative, confident, persistent after failure, coordinated, 2) direct and reality-oriented
in speech, 3) working harder after praise, 4) spent more time laughing and smiling together with their mothers and started smiling more quickly.

Iron supplementation in infancy contributes to more adaptive behavior at 10 years of age.
Lozoff B, J Nutr. 2014 Jun;144:838-45.
Healthy Chilean infants free of Iron Deficiency Anemia at age 6 mo were randomly assigned to iron supplementation or no added iron (formula with iron/powdered cow milk, vitamins with/without iron) from ages 6 to 12 mo.
Follow-up at age 10 yrs
Compared with the no-added-iron group children in the iron-supplemented group were:
1) more cooperative, confident, persistent after failure, coordinated, 2) direct and reality-oriented
in speech, 3) working harder after praise, 4) spent more time laughing and smiling together with their mothers and started smiling more quickly.
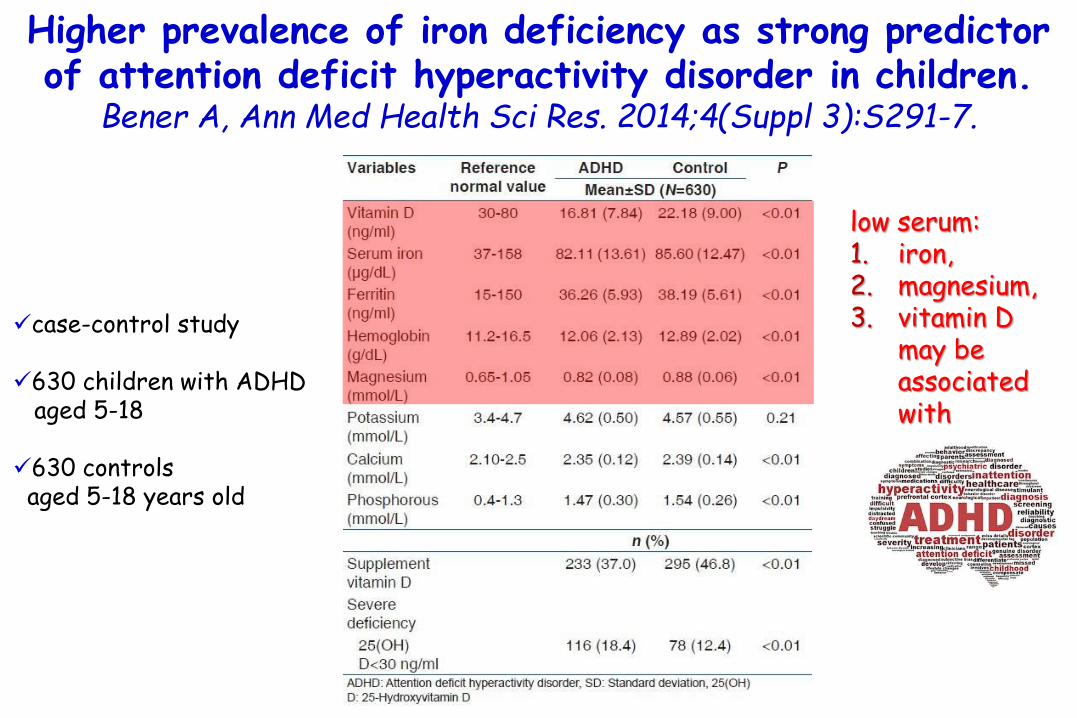
Higher prevalence of iron deficiency as strong predictor of attention deficit hyperactivity disorder in children.
Bener A, Ann Med Health Sci Res. 2014;4(Suppl 3):S291-7.
case-control study
630 children with ADHD aged 5-18
630 controls aged 5-18 years old
low serum: 1. iron,2. magnesium, 3. vitamin D
may be associated with
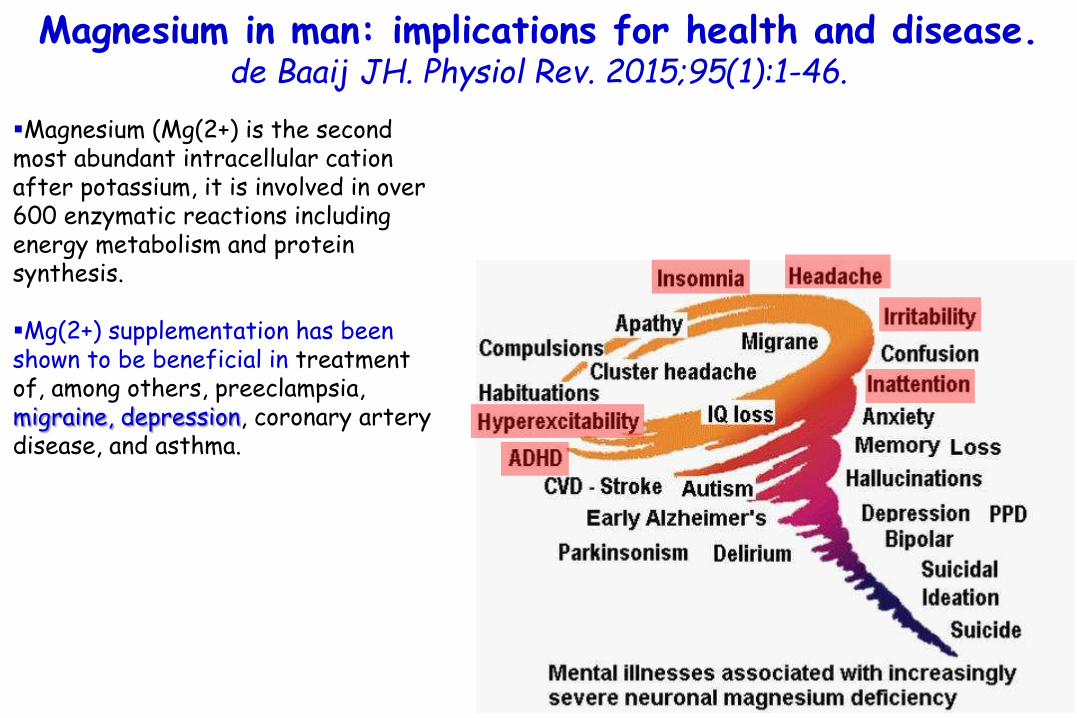
Magnesium in man: implications for health and disease.de Baaij JH. Physiol Rev. 2015;95(1):1-46.
Magnesium (Mg(2+) is the second most abundant intracellular cationafter potassium, it is involved in over 600 enzymatic reactions including energy metabolism and protein synthesis.
Mg(2+) supplementation has been shown to be beneficial in treatment of, among others, preeclampsia, migraine, depression, coronary artery disease, and asthma.
Maternal Long-Chain Polyunsaturated Fatty Acid Status during Early Pregnancy and Children's Risk of
Problem Behavior at Age 5-6 Years Loomans EM, J Ped 2014;164;762-768
•Essential fatty acids and particularly their long-chain polyunsaturatedderivatives eicosapentaenoic acid (EPA; omega-3), docosahexaenoic acid (DHA; omega-3), and arachidonic acid (AA; omega-6) are important toneurodevelopmental processes such as neurogenesis, cell proliferation, membrane functioning, and, potentially, myelination.
•To enable optimal fetal brain development, both a sufficient and balanced supply of omega-3 and omega-6 long-chain polyunsaturated fatty acids (LCPUFAs) from the maternal circulation (ie, placental transfer) are crucial.
•Hence, deficiencies in maternal LCPUFA or an imbalance in the omega-6:omega-3 LCPUFA (ie, AA/[DHA + EPA]) during gestationmight affect fetal brain development and influence subsequent long-term behavioral outcomes.

Maternal long-chain polyunsaturated fatty acid (LCPUFA) status and ratio during pregnancy (4336 women)
Children’s risk of problem behavior at 5 years of age rated by their mother (n = 2502) and teacher (n = 2061)
0.75
Greater concentrations of Ώ-3fatty acid docosahexaenoic acid
OR for children’semotional symptoms
at age 5 years1.0 –
0.5 –
0.0
Maternal Long-Chain Polyunsaturated Fatty Acid Status during Early Pregnancy and Children's Risk of
Problem Behavior at Age 5-6 Years Loomans EM, J Ped 2014;164;762-768

Maternal long-chain polyunsaturated fatty acid (LCPUFA) status and ratio during pregnancy (4336 women)
Children’s risk of problem behavior at 5 years of age rated by their mother (n = 2502) and teacher (n = 2061)
0.75
1.0 –
0.5 –
0.0
Maternal Long-Chain Polyunsaturated Fatty Acid Status during Early Pregnancy and Children's Risk of
Problem Behavior at Age 5-6 Years Loomans EM, J Ped 2014;164;762-768
Lower eicosapentaenoicacid (EPA) and a greateromega-6:omega-3 LCPUFA tended to increase the risk
for emotional symptomsand the risk ofhyperactivity/
inattention problems
Greater concentrations of Ώ-3fatty acid docosahexaenoic acid
OR for children’semotional symptoms
at age 5 years

Dietary long chain n-3 polyunsaturated fatty acidsprevent impaired social behaviour and normalize brain
dopamine levels in food allergic mice.de Theije CG, Neuropharmacology 2015;90:15-22
Whey sensitive mouse
Whey
Impaired social behaviour
X

Dietary long chain n-3 polyunsaturated fatty acidsprevent impaired social behaviour and normalize brain
dopamine levels in food allergic mice.de Theije CG, Neuropharmacology 2015;90:15-22
Impaired social behaviourWhey sensitive mouse
Whey
n-3 LCPUFA-enriched diet before and during
sensitization with whey(-)
X

Dietary long chain n-3 polyunsaturated fatty acidsprevent impaired social behaviour and normalize brain
dopamine levels in food allergic mice.de Theije CG, Neuropharmacology 2015;90:15-22
Impaired social behaviourWhey sensitive mouse
Whey
n-3 LCPUFA-enriched diet before and during
sensitization with whey(-)
n-3 LCPUFA supplementation
increased docosahexaenoic acid (DHA) incorporation into the brain and
restored reduced levels of prefrontal dopamine
(DA) and its metabolites
(reward-motivatedbehavior).
X

Dietary long chain n-3 polyunsaturated fatty acidsprevent impaired social behaviour and normalize brain
dopamine levels in food allergic mice.de Theije CG, Neuropharmacology 2015;90:15-22
Impaired social behaviourWhey sensitive mouse
Whey
n-3 LCPUFA-enriched diet before and during
sensitization with whey(-)
In addition to these brain effects, n-3 LCPUFA
supplementation reduced the allergic skin response and restored decreased
intestinal levels of serotoninmetabolite
(regulation of mood, appetite, and sleep).
X

High Folate Intake Is Related to Better AcademicAchievement in Swedish Adolescents
Nilsson, Pediatrics 2011;128:e358
An increased plasma total homocysteine (tHcy) serves as a marker for functional deficiency of certain B vitamins, such as B12, B6, riboflavin, and, in particular, folate.
The genetic model disease homocystinuria is characterized by high plasma tHcy levels, mental retardation, and a range of psychiatric symptoms, in addition to premature atherosclerosis.
In more recent studies, links have been found between impaired homocysteine metabolism and a wide range of neuropsychiatric conditions such as depression, cognitive impairment, and dementia in adult populationsand in the elderly.

High Folate Intake Is Related to Better AcademicAchievement in Swedish Adolescents
Nilsson, Pediatrics 2011;128:e358
386 Swedish adolescentsaged 15 yrs.
The sum of school grades in10 core subjects obtainedin the final semester ofcompulsory 9 years ofschooling used as outcomemeasure of academicachievement.
Adolescents are vulnerableto increased plasma totalhomocysteine (tHcy) and toinsufficient folate status.
Academic achievement was
strongly correlated to tertiles of tHcy
(negatively; P=0.023)
and to
tertiles of folate intake (positively; P<0.001).

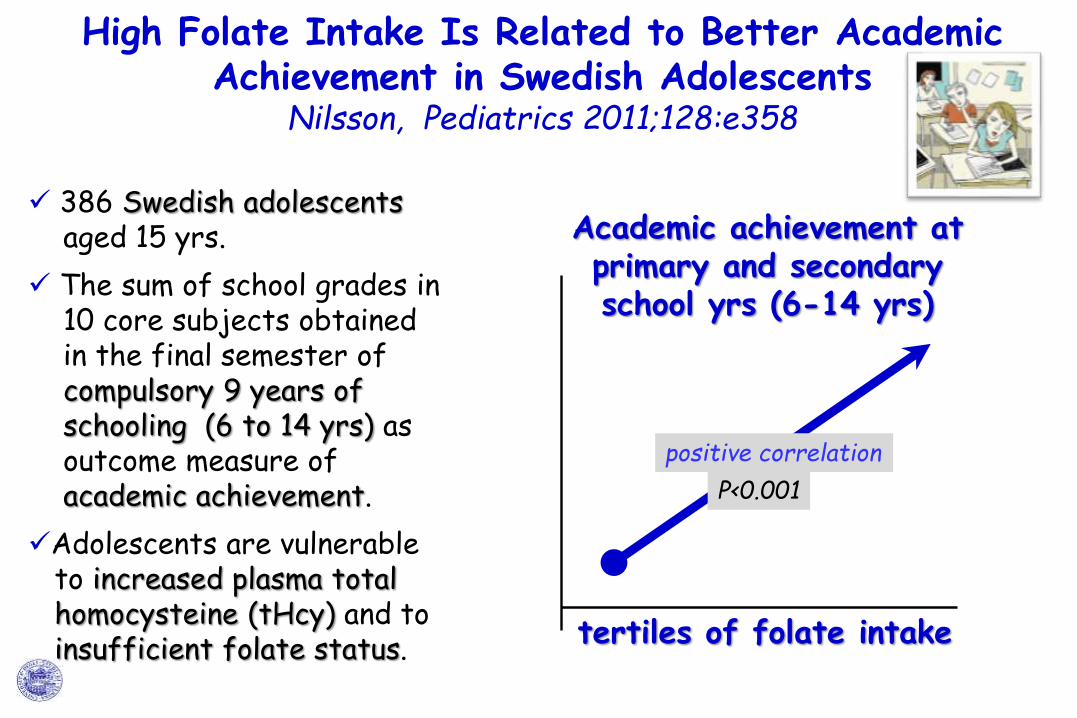
High Folate Intake Is Related to Better AcademicAchievement in Swedish Adolescents
Nilsson, Pediatrics 2011;128:e358
High Folate Intake Is Related to Better AcademicAchievement in Swedish Adolescents
Nilsson, Pediatrics 2011;128:e358
386 Swedish adolescentsaged 15 yrs.
The sum of school grades in10 core subjects obtainedin the final semester ofcompulsory 9 years ofschooling (6 to 14 yrs) as outcome measure of academic achievement.
Adolescents are vulnerableto increased plasma totalhomocysteine (tHcy) and toinsufficient folate status. tertiles of folate intake
Academic achievement atprimary and secondary school yrs (6-14 yrs)
P<0.001
positive correlation

Plasma nutrient status of patients with Alzheimer's disease: Systematic review and meta-analysis.Lopes da Silva S, Alzheimers Dement. 2014;10(4):485-502
≥ 5 studies for folate, vitamin A, vitamin B12, vitamin C, vitamin D, vitamin E, copper, iron, and zinc
< 5 studies for vitaminsB1 and B6, long-chainomega-3 fatty acids, calcium, magnesium, manganese, and selenium
in AD patients.significantly lower plasma levels of:1) Folate, 2) vitamin A, 3) vitamin B12, 4) vitamin C, 5) vitamin E.
nonsignificantly lower levels of:1) zinc (P = 0.050) 2) vitamin D (P = 0.075)
P < 0.001

Plasma nutrient status of patients with Alzheimer's disease: Systematic review and meta-analysis.Lopes da Silva S, Alzheimers Dement. 2014;10(4):485-502
≥ 5 studies for folate, vitamin A, vitamin B12, vitamin C, vitamin D, vitamin E, copper, iron, and zinc
< 5 studies for vitaminsB1 and B6, long-chainomega-3 fatty acids, calcium, magnesium, manganese, and selenium
in AD patients.significantly lower plasma levels of:1) Folate, 2) vitamin A, 3) vitamin B12, 4) vitamin C, 5) vitamin E.
nonsignificantly lower levels of:1) zinc (P = .050) 2) vitamin D (P = .075)
P < .001
No significant differences were
observed for plasma levels of
copper
and
iron.

Plasma nutrient status of patients with Alzheimer's disease: Systematic review and meta-analysis.Lopes da Silva S, Alzheimers Dement. 2014;10(4):485-502
≥ 5 studies for folate, vitamin A, vitamin B12, vitamin C, vitamin D, vitamin E, copper, iron, and zinc
< 5 studies for vitaminsB1 and B6, long-chainomega-3 fatty acids, calcium, magnesium, manganese, and selenium
in AD patients.significantly lower plasma levels of:1) Folate, 2) vitamin A, 3) vitamin B12, 4) vitamin C, 5) vitamin E.
nonsignificantly lower levels of:1) zinc (P = .050) 2) vitamin D (P = .075)
P < .001
The lower plasma nutrient levels indicate that patients
with AD have impaired systemic availability of
several nutrients.
This difference appears to be unrelated to the classic malnourishment that is well known to be common in AD, suggesting that compromised
micronutrient status may precede protein and energy malnutrition

Food Allergy and the Brain
Attilio BonerUniversity ofVerona, Italy
Introduction
Micronutrients and Behaviour
Immunity & Ipersensitivity
Food Allergy&Ipersensitivity and Brain
Not only Food Allergy
Which came first?
Possible Mechanisms
Food-based Therapies
Conclusions
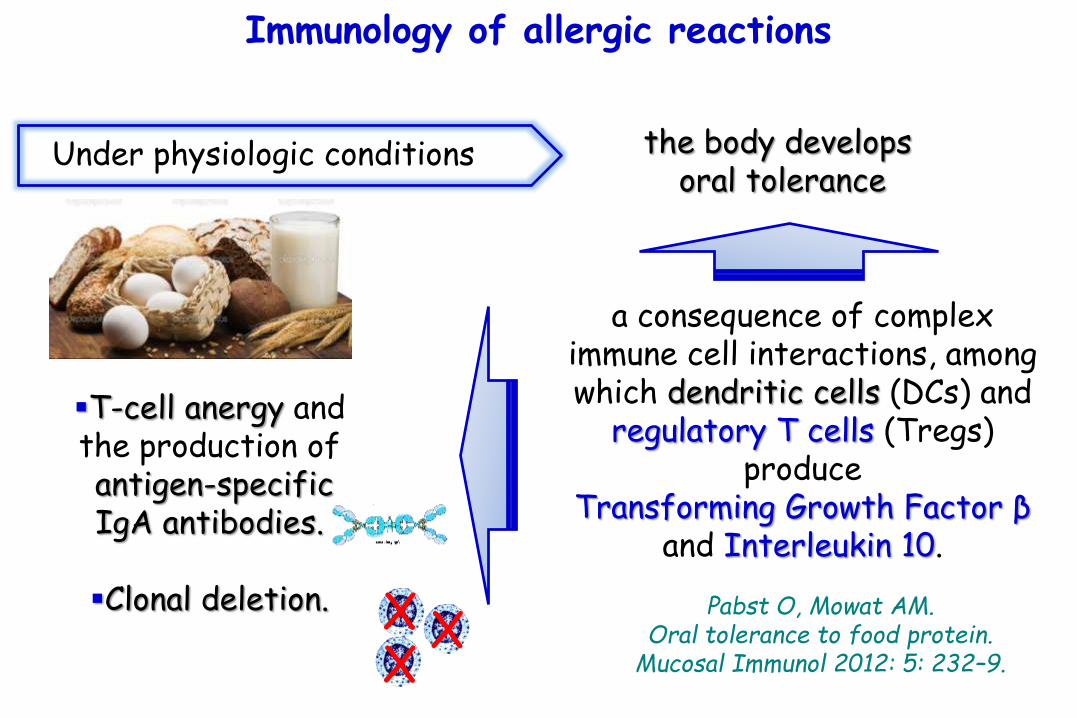
Immunology of allergic reactions
Under physiologic conditions the body develops oral tolerance
a consequence of complex immune cell interactions, among which dendritic cells (DCs) and
regulatory T cells (Tregs) produce
Transforming Growth Factor β and Interleukin 10.
Pabst O, Mowat AM. Oral tolerance to food protein.
Mucosal Immunol 2012: 5: 232–9.
T-cell anergy and the production of antigen-specific IgA antibodies.
Clonal deletion. X XX

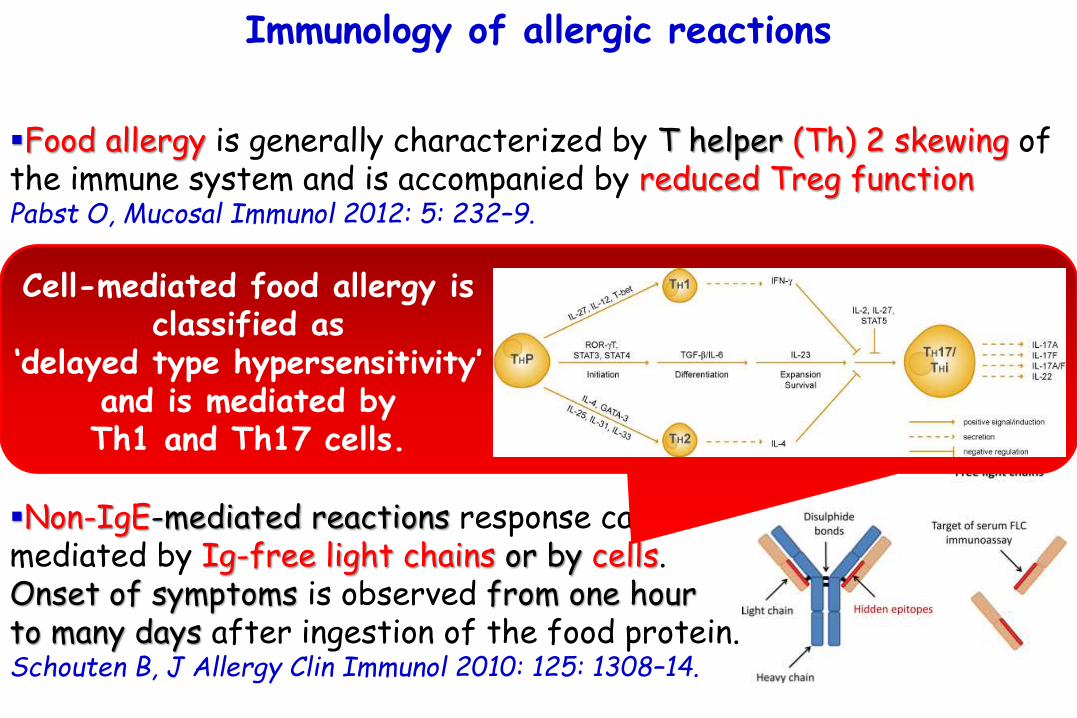
Food allergy is generally characterized by T helper (Th) 2 skewing of the immune system and is accompanied by reduced Treg functionPabst O, Mucosal Immunol 2012: 5: 232–9.
The majority of food-allergic reactions is mediated by IgE inducing mast cell degranulation and secretion of inflammatory mediators such as cytokines, histamine, leukotrienes, and prostaglandin. Onset of symptoms evolves within several minutes to several hours after contact with the allergen
Non-IgE-mediated reactions response can be mediated by Ig-free light chains or by cells. Onset of symptoms is observed from one hour to many days after ingestion of the food protein.Schouten B, J Allergy Clin Immunol 2010: 125: 1308–14.
Immunology of allergic reactions
Food allergy is generally characterized by T helper (Th) 2 skewing of the immune system and is accompanied by reduced Treg functionPabst O, Mucosal Immunol 2012: 5: 232–9.
The majority of food-allergic reactions is mediated by IgE inducing mast cell degranulation and secretion of inflammatory mediators such as cytokines, histamine, leukotrienes, and prostaglandin. Onset of symptoms evolves within several minutes to several hours after contact with the allergen
Non-IgE-mediated reactions response can be mediated by Ig-free light chains or by cells. Onset of symptoms is observed from one hour to many days after ingestion of the food protein.Schouten B, J Allergy Clin Immunol 2010: 125: 1308–14.
Immunology of allergic reactions
Cell-mediated food allergy is classified as
‘delayed type hypersensitivity’ and is mediated by Th1 and Th17 cells.

Immunology of allergic reactions
For systemic clinical symptoms to occur, food allergens must first cross from the lumen through the epithelial barrier to the intestinal mucosa.Kim JS, Curr Opin Gastroenterol. 2012;28:99–103.
During IgE-mediated reactions, allergens crossing the epithelial barrier then bind to IgE found on mast cells, causing them to degranulate and release allergic mediators, such as histamines.
Conversely, non–IgE-mediated reactions likely involve antigens being presented to Th1, Th17 cells in the intestinal mucosa. These in turn release cytokines that can lead to long-term changes to epithelial cells and the intestinal mucosa.Jyonouchi H. Inflamm Allergy Drug Targets. 2008;7:173–180.
Immunology of allergic reactions
IgE-mediated food allergy can be diagnosed by skin prick test and allergen-sIgE levels.
Unfortunately, no standardized test is available for detection of non-IgE-mediated food allergy, and diagnosis is based on elimination of the suspected allergenic food for weeks.
A challenge test can be used to confirm the diagnosis.
Clinical symptoms of food-allergic reactions are not restricted to the GI tract, but also involve the skin and airways. In addition to these non-GI symptoms, it has also been suggested that behavioral and psychologic symptoms can be evoked by allergic reactions
Costa-Pinto FA, Neural and behavioral correlates of food allergy. Chem Immunol Allergy 2012: 98: 222–39.

Certain foods contain pharmacologically active substances, such as caffeine, histamine, serotonin, and tyramine, which can affect
behavior in all individuals to a greater or lesser extent.
•Ingestion of the amino acids glutamic acid and tryptophan have been known to cause the disturbances of cognition and myalgia characteristic of the Chinese restaurant syndrome and the eosinophilia myalgia syndrome, respectively. •Certain ingested foods and food substances, such as strawberries, tomatoes, pineapple, and alcohol, produce an increase in circulating histamine that is known to be associated with hyperactive behavior. •Excessive intake of sugar or highenergy foods, e.g., “squash,” leads to the development of reactive hypoglycemia several hours after ingestion, which, in turn, produces an aberration in behavior and cognitive performance.
Bellanti JA, Allergy Asthma Proc. 2005;26(1):19-28

'exorphins' are derived from the incomplete digestive breakdown of dairy and grain derived foods.
Exorphins are small protein or peptides that have an action like morphine.
Endorphins, exorphins and morphine all work by way of opioid receptors.
Five exorphins have been discovered in digests of gluten and eight others in digests of milk.
The discovery of these psychoactive exorphins offers a possible explanation for some of the reported psychiatric reactions to these proteins including the sense of "brain fog" that often accompanies immune reactions to dairy and grain foods.
Exorphins may also modulate mood by depressing serotonin, dopamine and norepinephrine in the central nervous system.

Chinese restaurant syndromeChinese restaurant syndrome is a set of symptoms that some people have after eating Chinese food. A food additive called monosodium glutamate (MSG) has been blamed for the condition. However, this has not been proven to be the cause.
Symptoms include:Chest painFlushingHeadacheNumbness or burning in or around the mouthSense of facial pressure or swellingSweating
The following signs may also be used to aid in diagnosis:Abnormal heart rhythm observed on an electrocardiogramDecreased air entry into the lungsRapid heart rate

Food Allergy and the Brain
Attilio BonerUniversity ofVerona, Italy
Introduction
Micronutrients and Behaviour
Immunity & Ipersensitivity
Food Allergy&Ipersensitivity and Brain
Not only Food Allergy
Which came first?
Possible Mechanisms
Food-based Therapies
Conclusions

The psychosocial impact of food allergy and food hypersensitivity in children, adolescents and their
families: a review. Cummings AJ, Allergy. 2010;65:933–945.
psychological distress, including anxiety, depression and stress in the both the sufferer and the parents.
Food allergy orhypersensitivity
•Assessment of quality of life in children with peanut allergy. Avery NJ, Pediatr Allergy Immunol 2003;14:378–382.
•Impact of peanut allergy on quality of life, stress and anxiety in the family. King RM, Allergy 2009;64:461–468.
•Food allergy in young adults: perceptions and psychological effects. Lyons AC, J Health Psychol 2004;9:497–504.
•The impact of childhood food allergy on quality of life. Sicherer SH, Ann Allergy Asthma Immunol 2001;87:461–464

Self-reported allergies and their relationship to several Axis I disorders in a community sample. Patten SB, Int J Psychiatry Med 2007;37:11–22
Axis I refers broadly to the principal disorder that needs immediate attention; e.g., a major depressive episode, an exacerbation of schizophrenia, or a flare-up of panic disorder. It is usually (though not always) the Axis I disorder that brings the person "through the office door."
Axis II lists any personality disorder that may be shaping the current response to the Axis I problem. Axis II also indicates any developmental disorders, such as mental retardation or a learning disability, which may be predisposing the person to the Axis I problem. For example, someone with severe mental retardation or a paranoid personality disorder may be more likely to be "bowled over" by a major life stressor, and succumb to a major depressive episode.
Axis III lists any medical or neurological problems that may be relevant to the individual's current or past psychiatric problems; for example, someone with severe asthma may experience respiratory symptoms that are easily confused with a panic attack, or indeed, which may precipitate a panic attack.
Axis IV codes the major psychosocial stressors the individual has faced recently; e.g., recent divorce, death of spouse, job loss, etc.
Axis V codes the "level of function" the individual has attained at the time of assessment, and, in some cases, is used to indicate the highest level of function in the past year. This is coded on a 0-100 scale, with 100 being nearly "perfect" functioning (none of us would score that high!).

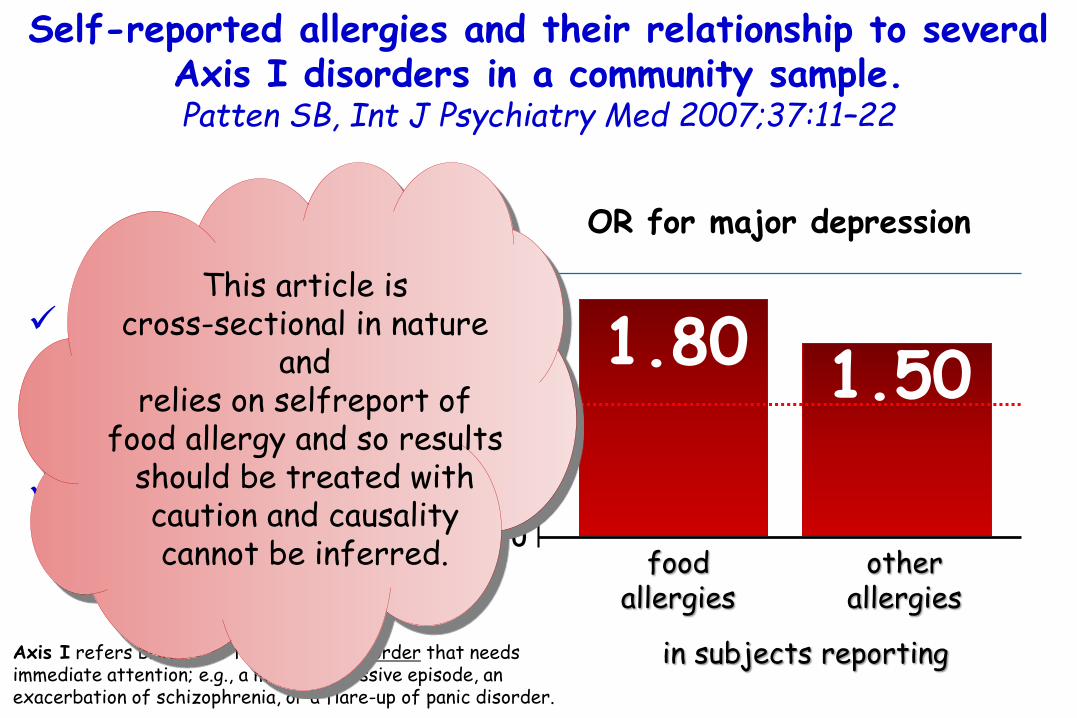
Self-reported allergies and their relationship to several Axis I disorders in a community sample. Patten SB, Int J Psychiatry Med 2007;37:11–22
Canadian Community Health Study in 2002.
Self-report data about food allergies.
food allergies
1.802.0 –
1.5 –
1.0 –
0.5 –
0.0
OR for major depression
Axis I refers broadly to the principal disorder that needs immediate attention; e.g., a major depressive episode, an exacerbation of schizophrenia, or a flare-up of panic disorder.
in subjects reporting
otherallergies
1.50

Self-reported allergies and their relationship to several Axis I disorders in a community sample. Patten SB, Int J Psychiatry Med 2007;37:11–22
2002 Canadian Community Health Study.
Self-report data about food allergies.
food allergies
1.802.0 –
1.5 –
1.0 –
0.5 –
0.0
OR for major depression
Axis I refers broadly to the principal disorder that needs immediate attention; e.g., a major depressive episode, an exacerbation of schizophrenia, or a flare-up of panic disorder.
in subjects reporting
otherallergies
1.50
Associations of comparable strength were observed for bipolar disorder and for panic disorder/agoraphobia.
The association with social phobia was statistically significant, but not as strong.
Self-reported allergies and their relationship to several Axis I disorders in a community sample. Patten SB, Int J Psychiatry Med 2007;37:11–22
2002 Canadian Community Health Study.
Self-report data about food allergies.
food allergies
1.802.0 –
1.5 –
1.0 –
0.5 –
0.0
OR for major depression
Axis I refers broadly to the principal disorder that needs immediate attention; e.g., a major depressive episode, an exacerbation of schizophrenia, or a flare-up of panic disorder.
in subjects reporting
otherallergies
1.50
This article is cross-sectional in nature
and relies on selfreport of
food allergy and so results should be treated with caution and causality cannot be inferred.

The psychosocial impact of food allergy and food hypersensitivity in children, adolescents and their
families: a review. Cummings AJ, Allergy. 2010;65:933–945.
Changes in distress over time
1) A great deal of anxiety is experienced by patients and families around the time of diagnosis of food allergy.Primeau MN, Clin Exp Allergy 2000;30:1135–1143.
2) Following diagnosis, parents and children will often follow a period of psychosocial adjustment. Mandell D, Health Soc Work 2005;30:325–335.
3) Once parents understand the risks associated with their child’s food allergy, fear begins to emerge as a predominant emotion.Gillespie CA, J Pediatr Nurs 2007;22:30–42.
The psychosocial impact of food allergy and food hypersensitivity in children, adolescents and their
families: a review. Cummings AJ, Allergy. 2010;65:933–945.
Changes in distress over time
1) A great deal of anxiety is experienced by patients and families around the time of diagnosis of food allergy.Primeau MN, Clin Exp Allergy 2000;30:1135–1143.
2) Following diagnosis, parents and children will often follow a period of psychosocial adjustment. Mandell D, Health Soc Work 2005;30:325–335.
3) Once parents understand the risks associated with their child’s food allergy, fear begins to emerge as a predominant emotion.Gillespie CA, J Pediatr Nurs 2007;22:30–42.
It is likely to be this fear that promotes patients and parents to develop coping strategies
to manage allergy and minimize risk.

The psychosocial impact of food allergy and food hypersensitivity in children, adolescents and their
families: a review. Cummings AJ, Allergy. 2010;65:933–945.
The period of starting school is also a concern for parents.
Mothers often find it difficult to completely relax when their children are attending school, away from their supervision.Gillespie CA, J Pediatr Nurs 2007;22:30–42.
As children grow into teenagers, parents have reported anxietyin handing over the responsibility to their child for their riskassessment, avoidance strategies and management of theirfood allergy, and it is suggested there is a risk that they maytransfer their anxieties to their children. Akeson N, Clin Exp Allergy 2007;37:1213–1220.

The psychosocial impact of food allergy and food hypersensitivity in children, adolescents and their
families: a review. Cummings AJ, Allergy. 2010;65:933–945.
parental modelling of anxious behaviour to activities such as
administering emergency treatment
increasedanxiety in the child.
high levels of anxiety experienced by food allergic children,although impacting adversely upon QoL, could be interpretedas protective if it encourages them to comply with adequateavoidance measures and management plans.Mandell D, Health Soc Work 2005;30:325–335.

The psychosocial impact of food allergy and food hypersensitivity in children, adolescents and their
families: a review. Cummings AJ, Allergy. 2010;65:933–945.
parental modelling of anxious behaviour to activities such as
administering emergency treatment
increasedanxiety in the child.
high levels of anxiety experienced by food allergic children,although impacting adversely upon QoL, could be interpretedas protective if it encourages them to comply with adequateavoidance measures and management plans.Mandell D, Health Soc Work 2005;30:325–335.
However, high levels of anxiety may bemaladaptive, for example, if it places
unrealistic restrictionson an individual’s life

Anxiety and depression: a common feature of health care seeking patients with irritable bowel syndrome and foodallergy. Addolorato G, Hepatogastroenterology 1998:45:1559–64
The % of subjects with high levels of state anxiety, trait anxiety and depression was significantly higher in IBS than in both LI and healthy controls.
Psychological findings in patients with FA were very similar to those of IBS.
66 pts with irritable bowelsyndrome (IBS).
44 with food allergy (FA).
48 with lactose intolerance (LI).
52 healthy controls
State and Trait Anxiety Inventory and the Zung depression scale.

Association between childhood allergic disease, psychological comorbidity, and injury requiring medical
attention.Garg N, Ann Allergy Asthma Immunol. 2014;112(6):525-32
Conduct/oppositionaldefiant disorder
2.973.0 –
2.0 –
1.0 –
00
In children with allergicdisorders OR for
2.49
Learning delay
Data from the 2007 to 2008 National Survey of Children's Health (27,556 children 0 to 5 years old).
(angry and irritable mood, argumentative or vindictiveness)

Association between childhood allergic disease, psychological comorbidity, and injury requiring medical
attention.Garg N, Ann Allergy Asthma Immunol. 2014;112(6):525-32
Conduct/oppositionaldefiant disorder
2.973.0 –
2.0 –
1.0 –
00
In children with allergicdisorders OR for
2.49
Learning delay
Data from the 2007 to 2008 National Survey of Children's Health (27,556 children 0 to 5 years old).
(angry and irritable mood, argumentative or vindictiveness)
Children with food allergies, had higher odds of sustaining
injuries (OR = 2.0).

Association between childhood allergic disease, psychological comorbidity, and injury requiring medical
attention.Garg N, Ann Allergy Asthma Immunol. 2014;112(6):525-32
In children withallergic disorders OR for
Data from the 2007 to 2008 National Survey of Children's Health (27,556 children 0 to 5 years old).
Depression Anxiety ADHD
6.03
7.0 –
6.0 –
5.0 –
4.0 –
3.0 –
2.0 –
1.0 –
0.0
5.544.75

Are children and adolescents with food allergies at increased risk for psychopathology?
Shanahan L, J Psychosom Res. 2014;77(6):468-73.
Adolescents (N=1420) were recruited from the community, and interviewed up to 6 times between ages 10 and 16 years.
N=5165 pairs of interviews.
Cross-sectionally, food allergies were associated with more symptoms of:1) separation and generalized
anxiety2) attention deficit and
hyperactivity disorder (ADHD),
Longitudinally, adolescents with food allergy experienced increases in symptoms of:1) generalized anxiety disorder 2) depressionfrom one assessment to the next.

Are children and adolescents with food allergies at increased risk for psychopathology?
Shanahan L, J Psychosom Res. 2014;77(6):468-73.
Adolescents (N=1420) were recruited from the community, and interviewed up to 6 times between ages 10 and 16 years.
N=5165 pairs of interviews.
Food allergies were not, however,
associated with a higher likelihood of meeting diagnostic
criteria for a psychiatric disorder.
Cross-sectionally, food allergies were associated with more symptoms of:1) separation and generalized
anxiety2) attention deficit and
hyperactivity disorder (ADHD),
Longitudinally, adolescents with food allergy experienced increases in symptoms of:1) generalized anxiety disorder 2) depressionfrom one assessment to the next.

Are children and adolescents with food allergies at increased risk for psychopathology?
Shanahan L, J Psychosom Res. 2014;77(6):468-73.
Adolescents (N=1420) were recruited from the community, and interviewed up to 6 times between ages 10 and 16 years.
N=5165 pairs of interviews.
adolescents' increased symptoms of psychopathology in the context of food allergy likely
reflects an adaptive increase in vigilance
rather than cohesive syndromes of psychopathology.
Cross-sectionally, food allergies were associated with more symptoms of:1) separation and generalized
anxiety2) attention deficit and
hyperactivity disorder (ADHD),
Longitudinally, adolescents with food allergy experienced increases in symptoms of:1) generalized anxiety disorder 2) depressionfrom one assessment to the next.

Are children and adolescents with food allergies at increased risk for psychopathology?
Shanahan L, J Psychosom Res. 2014;77(6):468-73.
Adolescents (N=1420) were recruited from the community, and interviewed up to 6 times between ages 10 and 16 years.
N=5165 pairs of interviews.
Support and guidance from health care
providers is needed to help adolescents with food allergies and their caregivers
achieve an optimal balance between
necessary vigilance and hypervigilanceand unnecessary
restriction.
Cross-sectionally, food allergies were associated with more symptoms of:1) separation and generalized
anxiety2) attention deficit and
hyperactivity disorder (ADHD),
Longitudinally, adolescents with food allergy experienced increases in symptoms of:1) generalized anxiety disorder 2) depressionfrom one assessment to the next.

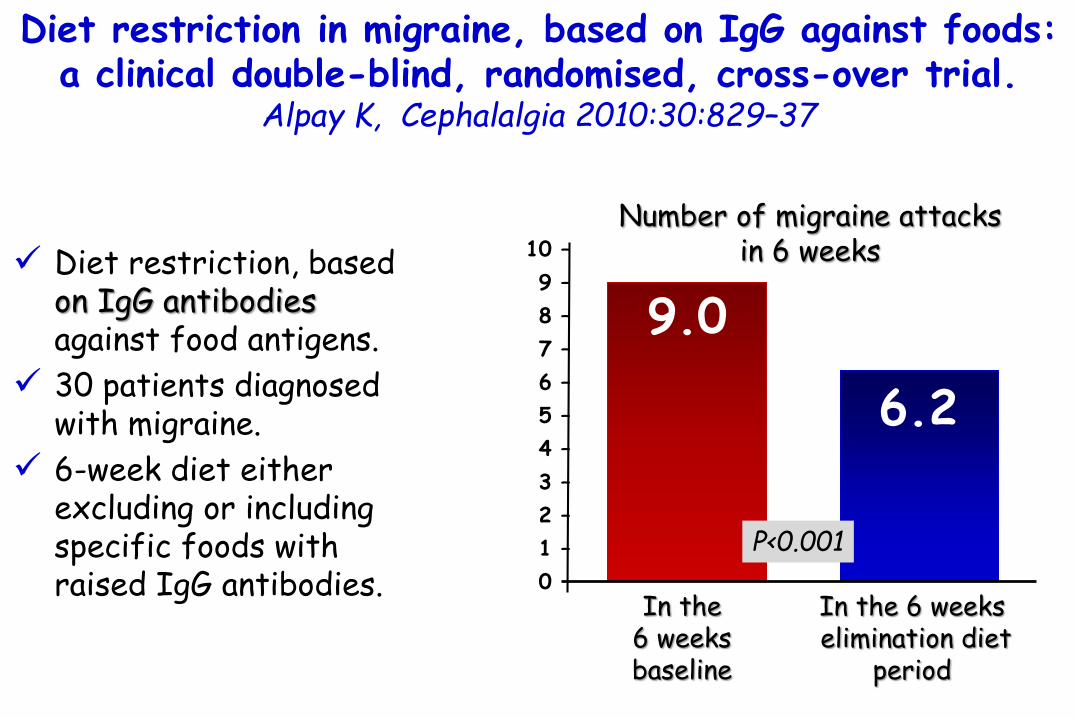
Diet restriction in migraine, based on IgG against foods: a clinical double-blind, randomised, cross-over trial.
Alpay K, Cephalalgia 2010:30:829–37
1) There is evidence of a profound role of meningeal inflammation in migraine pathogenesis.
2) Many contributing factors may trigger the occurrence of migraine attacks and foodis one of the most well-known.
3) IgE-specific food allergy has been shown to be related with migraine supported by the success of individualised diet in controlling migraine attacks.
4) IgG mediated hypersensitivity to foods is also possible.
Diet restriction in migraine, based on IgG against foods: a clinical double-blind, randomised, cross-over trial.
Alpay K, Cephalalgia 2010:30:829–37
In the 6 weeksbaseline
9.0
Number of migraine attacksin 6 weeks
6.2
Diet restriction, based on IgG antibodies against food antigens.
30 patients diagnosed with migraine.
6-week diet either excluding or including specific foods with raised IgG antibodies.
In the 6 weekselimination diet
period
10 –
09 –
08 –
07 –
06 –
05 –
04 –
03 –
02 –
01 –
00
P<0.001

Diet restriction in migraine, based on IgG against foods: a clinical double-blind, randomised, cross-over trial.
Alpay K, Cephalalgia 2010:30:829–37
9.0
6.2
Diet restriction, based on IgG antibodies against food antigens.
30 patients diagnosed with migraine.
6-week diet either excluding or including specific foods with raised IgG antibodies.
10 –
09 –
08 –
07 –
06 –
05 –
04 –
03 –
02 –
01 –
00
P<0.001
Diet restriction based on IgG
antibodies is an effective strategy in reducing the frequency of
migraine attacks.
In the 6 weeksbaseline
In the 6 weekselimination diet
period
Number of migraine attacksin 6 weeks

Diet restriction in migraine, based on IgG against foods: a clinical double-blind, randomised, cross-over trial.
Alpay K, Cephalalgia 2010:30:829–37
The food categories from most frequent IgG positivity to least
(+)
(-)

Non coeliac gluten sensitivity –A new disease with gluten intolerance.
Czaja-Bulsa G. Clin Nutr. 2014 Aug 29. pii: S0261-5614(14)00218-0.
Non-celiac gluten sensitivity (NCGS) is a new syndrome of gluten intolerance. In literature some other names have been suggested for this disorder, such as gluten sensitivity (GS), gluten hypersensitivity or non-celiac gluten intolerance.
The typical presentation of NCGS is a combination of:
- IBS-like symptoms: abdominal pain, nausea, bloating, flatulence, diarrhoea or constipation, and
-systemic manifestations such as: headache, joint and muscle pain, muscle contractions, leg or arm numbness, chronic fatigue, “foggy mind”, body mass loss and anaemia or they can include behaviourdisturbances such as the disturbance inattention and depression.

Non coeliac gluten sensitivity –A new disease with gluten intolerance.
Czaja-Bulsa G. Clin Nutr. 2015;34:189-194.
Symptoms of non-celiac gluten sensitivity disorders (NCGS).
Gluten is comprised of the proteins
gliadin and glutelin
a 347 patients treated at the Center for Celiac Research University of Maryland in
2004e2010

Characteristics of gluten-dependent disorders.
The diagnosis by elimination diet cannot be made until Coeliac Disease and Wheat Allergy have been eliminated.
The diagnosis is confirmed by a food provocation test.
Non coeliac gluten sensitivity –A new disease with gluten intolerance.
Czaja-Bulsa G. Clin Nutr. 2015;34:189-194.

Non coeliac gluten sensitivity –A new disease with gluten intolerance.
Czaja-Bulsa G. Clin Nutr. 2015;34:189-194.
Pathogenesis
Aetiologically NCGS is a disorder with poorly recognised pathogenesis. It has not been determined yet what grain ingredients are responsible for the symptoms of the disease.A major role as triggers of the innate immune response leading to NCGS can be played by the poorly absorbed carbohydrates in wheat grains - fructo-oligosaccharides, fructans.During fermentation gas is produced and short-chain fatty acid are formed. What is more, changes in microbiota take place resulting in gastrointestinal symptoms.In the NCGS patients TGFβ1 and the FoxP3 markers for regulatory lymphocytes 3 are significantly reduced, which indicates the likelihood of the recruitment of the regulatory T lymphocytes to the small intestine to be smaller than in healthy people.

Classification of gluten-related
disorders.
Non coeliac gluten sensitivity –A new disease with gluten intolerance.
Czaja-Bulsa G. Clin Nutr. 2015;34:189-194.

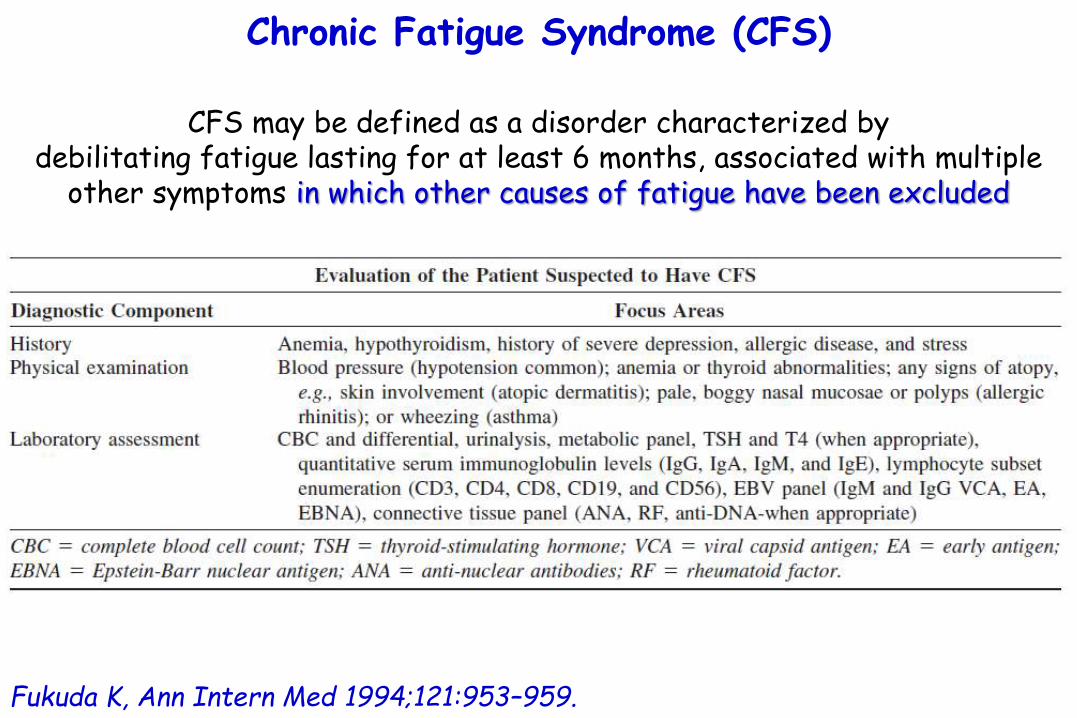
Chronic Fatigue Syndrome (CFS)
CFS may be defined as a disorder characterized by debilitating fatigue lasting for at least 6 months, associated with multiple
other symptoms in which other causes of fatigue have been excluded
feverishness,
chills and night sweats,
recurrent sore throat,
lymph node pain and enlargement,
myalgia, arthralgia,
headache,
postexertional weakness and fatigability,
sleep disorders, and
various neuropsychological complaints.
Fukuda K, Ann Intern Med 1994;121:953–959.
Chronic Fatigue Syndrome (CFS)
CFS may be defined as a disorder characterized by debilitating fatigue lasting for at least 6 months, associated with multiple
other symptoms in which other causes of fatigue have been excluded
Fukuda K, Ann Intern Med 1994;121:953–959.
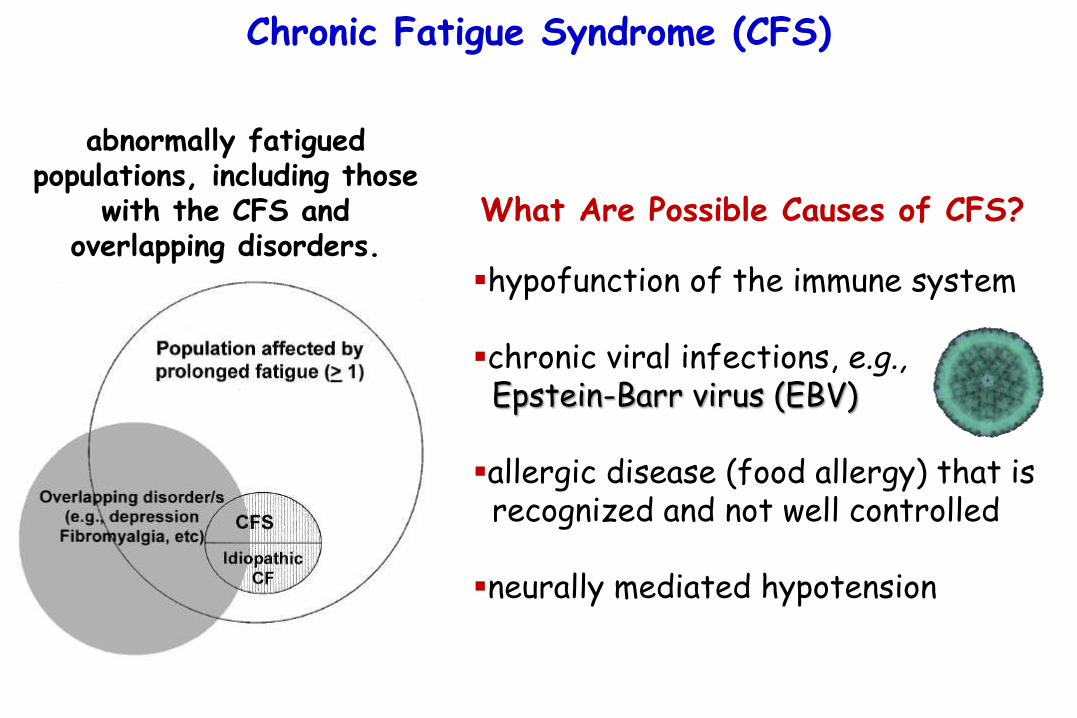
Chronic Fatigue Syndrome (CFS)
hypofunction of the immune system
chronic viral infections, e.g.,Epstein-Barr virus (EBV)
allergic disease (food allergy) that is recognized and not well controlled
neurally mediated hypotension
What Are Possible Causes of CFS?
abnormally fatiguedpopulations, including those
with the CFS and overlapping disorders.

Fibromyalgia (FM)
FM currently is defined as a disorder with many of the features of Chronic Fatigue Syndrome but with the presence of both chronic widespread pain and the finding of 11/18 tender points on examination.
Clauw DJ, Best Pract Res Clin Rheumatol 2003;17:685–701.
Examples of chronic regional pain syndromes where ‘peripheral’ factors (e.g. inflammation or damage to tissues) play
a minor or no role in pain.Patients have pain that is “central” (i.e., not caused by inflammation
or damage of structures) rather than peripheral in nature.

Fibromyalgia (FM)
Examples of overlapping systemic
syndromes characterized by
otherwise unexplained chronic pain and
fatigue.
Clauw DJ, Best Pract Res Clin Rheumatol 2003;17:685–701.

Are attention deficit hyperactivity disorder and chronicfatigue syndrome allergy related? what is fibromyalgia?
Bellanti JA, Allergy Asthma Proc. 2005;26(1):19-28
There are a group of diseases that the allergist immunologist may be called on to manage in which their precise etiologies have not been identified but that appear to be initiated or exacerbated by allergic mechanisms.
Attention deficit hyperactivity disorder (ADHD), chronic fatigue syndrome (CFS), and fibromyalgia (FM) fall into this category of disorders.
Although the precise etiology of ADHD still remains unknown, the mostprevalent theory is that it represents a developmental disability leading to inadequate production of the neurotransmitter dopamine.
In patients with CFS, there appears to be a fundamental dysfunction of the neuroendocrine-immunological system with deficiencies of immunological and neurological function, which, together with chronic viral infection, may lead to a sequence of events responsible for the symptoms of this disorder.

Gastrointestinal inflammation and associated immune activation in schizophrenia.
Severance EG, Schizophr Res 2012:138:48–53
IgG antibodies toSaccharomyces cerevisiae(ASCA, a marker of intestinalinflammation), bovine milk casein, wheat-derived gluten.
193 with non-recentonset schizophrenia(Non-RO SZ).
67 with recent onsetschizophrenia (RO SZ)
207 non-psychiatric controls.
Quantitative ASCA IgG levelsin individuals with schizophrenia
compared to controls.

Gastrointestinal inflammation and associated immune activation in schizophrenia.
Severance EG, Schizophr Res 2012:138:48–53
IgG antibodies toSaccharomyces cerevisiae(ASCA, a marker of intestinalinflammation), bovine milk casein, wheat-derived gluten.
193 with non-recentonset schizophrenia(Non-RO SZ).
67 with recent onsetschizophrenia (RO SZ)
207 non-psychiatric controls.
Quantitative ASCA IgG levelsin individuals with schizophrenia
compared to controls. ASCA markers were significantly elevated and correlated with
food antigen antibodies in recent onset and non-recent onset
schizophrenia compared
to controls.

Gastrointestinal inflammation and associated immune activation in schizophrenia.
Severance EG, Schizophr Res 2012:138:48–53
IgG antibodies toSaccharomyces cerevisiae(ASCA, a marker of intestinalinflammation), bovine milk casein, wheat-derived gluten.
193 with non-recentonset schizophrenia(Non-RO SZ).
67 with recent onsetschizophrenia (RO SZ)
207 non-psychiatric controls.
Quantitative ASCA IgG levelsin individuals with schizophrenia
compared to controls. Gastrointestinal inflammation is a relevant pathology in schizophrenia.

Food allergy in autism spectrum disorder
Autism spectrum disorder is a heterogeneous cluster of neurodevelopmental disorders
characterized by impairments in communication
and social interaction and by repetitive behavior .
American-Psychiatric-Association.Diagnostic and Statistical Manual of
Mental Disorders (4th ed). Washington, DC:
American-Psychiatric-Association, 2000
De Theije CGM, Pediatr Allergy Imm 2014;25:218

Food allergy in autism spectrum disorder
Autism spectrum disorder is a heterogeneous cluster of neurodevelopmental disorders
characterized by impairments in communication
and social interaction and by repetitive behavior .
American-Psychiatric-Association.Diagnostic and Statistical Manual of
Mental Disorders (4th ed). Washington, DC:
American-Psychiatric-Association, 2000
De Theije CGM, Peditr Allergy Imm 2014;25:218
The gut-brain axis is an emerging
field ofresearch on
ASD.

The diagnostic category pervasive developmental disorders (PDD), as opposed to specific developmental disorders (SDD), refers to a group of five disorders characterized by delays in
the development of multiple basic functions including socialization and communication.
PDD-NOS: Pervasive Developmental Disorder, Not Otherwise Specified

Symptoms of PDD may include behavioral and communication problems such as:
1) Difficulty using and understanding language2) Difficulty relating to people, objects, and events; for example, lack
of eye contact, pointing behavior, and lack of facial responses3) Unusual play with toys and other objects4) Difficulty with changes in routine or familiar surroundings5) Repetitive body movements or behavior patterns, such as hand
flapping, hair twirling, foot tapping, or more complex movements6) Inability to cuddle or be comforted7) Difficulty regulating behaviors and emotions, which may result in
temper tantrums, anxiety, and aggression.


Autistic-like behavioural and neurochemical changesin a mouse model of food allergy.
de Theije CG, Behav Brain Res. 2014;261:265-74.
Food allergic reaction to cow's milk protein, induced
shortly after weaning
1) Reduced social behaviour
2) Increased repetitive behaviour
Xincreased levels of serotonin in the intestine
reduced dopaminergic activity in the prefrontal cortex

1) This food allergic reaction increased levels of serotonin (5-hydroxytryptamine; 5-HT) and the number of 5-HT positive cells, and decreased levels of 5-hydroxyindoleacetic acid (5-HIAA) in the intestine.
2) Behavioural changes in food allergic mice were accompanied by reduced dopaminergic activity in the prefrontal cortex. The dopamine system is strongly associated with the reward system of the brain.
3) Neuronal activation (c-Fos expression) was increased in the prefrontal cortex and reduced in the paraventricular nucleus of the hypothalamus after exposure to a social target.
Autistic-like behavioural and neurochemical changesin a mouse model of food allergy.
de Theije CG, Behav Brain Res. 2014;261:265-74.

1) This food allergic reaction increased levels of serotonin (5-hydroxytryptamine; 5-HT) and the number of 5-HT positive cells, and decreased levels of 5-hydroxyindoleacetic acid (5-HIAA) in the intestine.
2) Behavioural changes in food allergic mice were accompanied by reduced dopaminergic activity in the prefrontal cortex. The dopamine system is strongly associated with the reward system of the brain.
3) Neuronal activation (c-Fos expression) was increased in the prefrontal cortex and reduced in the paraventricular nucleus of the hypothalamus after exposure to a social target.
Autistic-like behavioural and neurochemical changesin a mouse model of food allergy.
de Theije CG, Behav Brain Res. 2014;261:265-74.
We hypothesize that an intestinal allergic response regulates complex, but critical,
neuroimmune interactions, thereby affecting brain circuits involved in social interaction,
repetitive behaviour and cognition.

How do we measure permeability?It is easy to measure one's intestinal permeability by way of simply measuring the passive permeability using a dual sugar technique utilising lactulose and mannitol.The IP test may well be the most useful, precise and low-invasive way for assessing mucosal integrity in the small bowel. Mannitol (a monosaccharide) and lactulose (a disaccharide) are water soluble molecules that are not metabolised by the body. Mannitol is readily absorbed, and lactulose is only absorbed slightly.Testing procedureThe patient is given an oral dose containing 5gr of lactulose and 3gr of mannitol in a base of 10gr of glycerol. A timed urine sample is analysed and the ratios are assessed for the permeation of the water-soluble molecules (lactulose and mannitol) through the intestinal mucosa. Accurate information is obtained regarding gut integrity and function.What do the results mean?The permeation of the sugars through the intestinal mucosa can occur either through cells or between cells lining the small intestine wall. Small molecules (mannitol) readily penetrate cells and passively diffuse through them. Larger molecules (lactulose) normally are excluded by the cells in a normal, healthy functioning gut. The rate limiting barrier in this case is the "tight junction" between cells, which are only one layer thick. Tight junctions are important to maintain healthy epithelial integrity.Lactulose, being only slightly absorbed, serves as a marker for mucosal integrity.Mannitol is readily absorbed and serves as a marker for trans-cellular uptake.Low levels of mannitol and lactulose indicate malabsorption.Elevated levels of mannitol and lactulose indicate general increased permeability and are indicative of "leaky gut"syndrome.The lactulose/mannitol ratio is a useful parameter.Elevated ratios indicate that the effective pore size of the gut mucosa has increased, allowing access (to the body) of larger, and possibly antigenic molecules.

Food allergy in autism spectrum disorder
Parents of autistic children report more often that their child suffered from food allergies than parents of healthy children or children with special education needs.Gurney JG, Arch Pediatr Adolesc Med 2006:160:825–30.Chandler S, J Autism Dev Disord 2013;43(12):2737-47
Indeed, serum levels of immunoglobulins IgA, IgG, and IgM specificfor cow’s milk derived allergens and total IgE are increased in children with ASD compared with healthy controls.Lucarelli S, Panminerva Med 1995:37:137–41.
De Theije CGM, Pediatr Allergy Imm 2014;25:218

Parental report of health conditions and health care use among children with and without autism: National Survey of Children’s Health.
Gurney JG, Arch Pediatr Adolesc Med 2006:160:825–30
Cross-sectional analysis of the 2003 to 2004 National Survey of Children's Health.
More than 100 000 parents.
Response to the question: "Has a doctor or health professional ever told you that your child has autism?“.
Autism prevalence among children aged 3 to 17 years
5.3 per 1000

4.5
5.0 –
4.0 –
3.0 –
2.0 –
1.0 –
0.0
OR for food allergy
in childrenwith autism
Parental report of health conditions and health care use among children with and without autism: National Survey of Children’s Health.
Gurney JG, Arch Pediatr Adolesc Med 2006:160:825–30
Cross-sectional analysis of the 2003 to 2004 National Survey of Children's Health (NSCH).
More than 100 000 parents.
Response to the question: "Has a doctor or health professional ever told you that your child has autism?“.
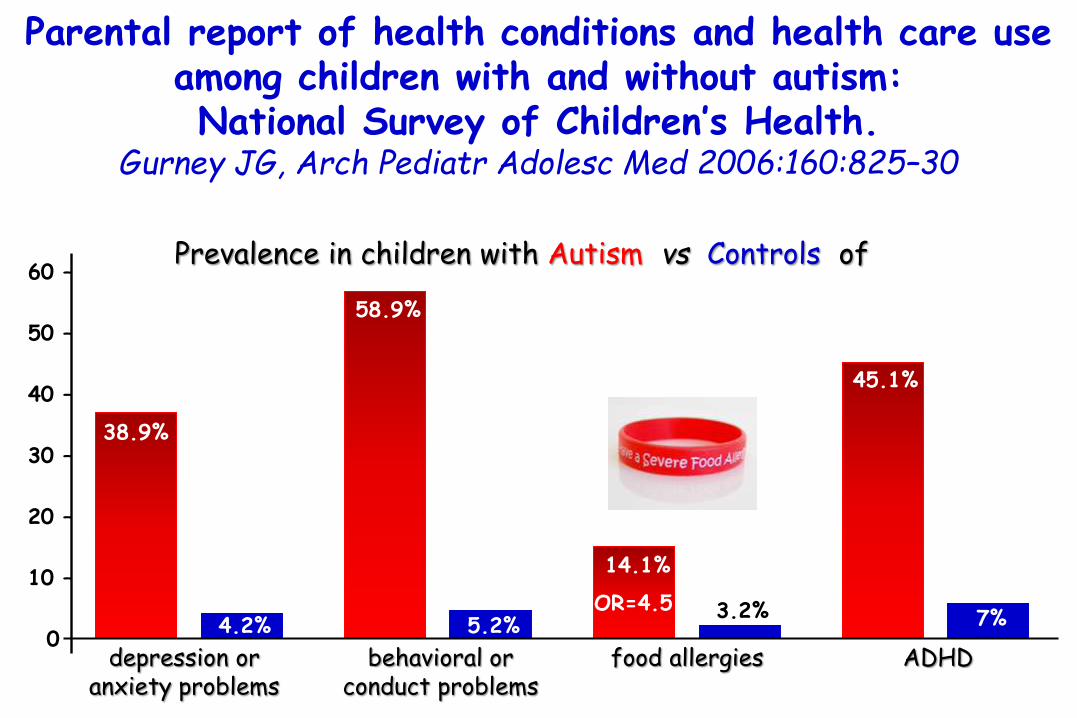
Parental report of health conditions and health care use among children with and without autism: National Survey of Children’s Health.
Gurney JG, Arch Pediatr Adolesc Med 2006:160:825–30
depression or anxiety problems
behavioral or conduct problems
food allergies ADHD
Prevalence in children with Autism vs Controls of
38.9%
45.1%
14.1%
58.9%
60 –
50 –
40 –
30 –
20 –
10 –
04.2%
3.2%5.2% 7%
OR=4.5

Shared heritability of attention-deficit/hyperactivitydisorder and autism spectrum disorder.
Rommelse NN, Eur Child Adolesc Psychiatry 2010:19:281–95
1) Attention-deficit/hyperactivity disorder (ADHD) and autism spectrum disorder (ASD) are both highly heritable neurodevelopmental disorders.
2) Evidence indicates both disorders co-occur with a high frequency.
meeting criteria for ASD
50 –
40 –
30 –
20 –
10 –
00
children with ADHD
20%
50%
meeting criteria for ADHD
80 –
70 –
60 –
50 –
40 –
30 –
20 –
10 –
00
children with ASD
30%
80%
ADHD
ASD

Food allergy and infantile autism.Lucarelli S, Panminerva Med 1995:37:137–41
Efficacy of a cow's milk free diet (or other foods which gave a positive result after a skin test).
36 autistic patients.
20 healthy children.
1) Levels of sIgA for casein, lactalbumin and β lactoglobulinand IgG and IgM for casein higher than in healthy controls.
2) A marked improvement in the behavioural symptoms of patients after 8 weeks on an elimination diet.

Food allergy and infantile autism.Lucarelli S, Panminerva Med 1995:37:137–41
Efficacy of a cow's milk free diet (or other foods which gave a positive result after a skin test).
36 autistic patients.
20 healthy children.
1) Levels of sIgA for casein, lactalbumin and β lactoglobulinand IgG and IgM for casein higher than in healthy controls.
2) A marked improvement in the behavioural symptoms of patients after 8 weeks on an elimination diet.
Our results lead us to hypothesisea relationship between
food allergy and infantile autism as has already been suggested for other disturbances of the central nervous
system.

Food allergy in autism spectrum disorder
Peripheral blood mononuclear cells of ASD children produce moreTNF-a and IL-12 in response to cow’s milk-derived allergens than those from control subjects. Jyonouchi H. J Pediatr 2005:146:605–10.
Milk intake by autistic patients was a significant predictor of constipation and led to the worsening of some of the behavioral symptoms specific for ASD. Afzal N, Pediatrics 2003:112:939–42.
Lucarelli S, Panminerva Med 1995:37:137–41.
Gluten intake has also been suggested to exacerbate autistic behavior although no association between gluten sensitivity or celiac disease and ASD has been reported. Barcia G, J Autism Dev Disord 2008:38:407–8
Genuis SJ, J Child Neurol 2010:25: 114–9. Batista IC, Arq Neuropsiquiatr 2012:70:28–33.
De Theije CGM, Pediatr Allergy Imm 2014;25:218

Evaluation of an association between gastrointestinalsymptoms and cytokine production against common dietary
proteins in children with autism spectrum disorders. Jyonouchi H. J Pediatr 2005:146:605–10
PBMCs from ASD children with gastrointestinal
symptoms
Peripheral blood mononuclear cells (PBMCs) from 109 autism spectrum disorders(ASD) children with or without GI symptoms (GI [+] ASD, N = 75 and GI (-) ASD, N = 34], from children with non-allergic food hypersensitivity(NFH) (N = 15), and control subjects (N = 19).
cow's milk and gliadin
more TNF-α and IL-12

Evaluation of an association between gastrointestinalsymptoms and cytokine production against common dietary
proteins in children with autism spectrum disorders. Jyonouchi H. J Pediatr 2005:146:605–10
PBMCs from ASD children with gastrointestinal
symptoms
Peripheral blood mononuclear cells (PBMCs) from 109 autism spectrum disorders(ASD) children with or without GI symptoms (GI [+] ASD, N = 75 and GI (-) ASD, N = 34], from children with non-allergic food hypersensitivity(NFH) (N = 15), and control subjects (N = 19).
cow's milk and gliadin
more TNF-α and IL-12
A high prevalence of elevated TNF-α/IL-12
production by GI (+) ASD PBMCs with cow's milk proteins and its major components indicates
a role of non-allergic foodhypersensitivity in GI symptoms observed in children with ASD.

Parent-reported gastro-intestinal symptoms in children with autism spectrum disorders.
Chandler S, J Autism Dev Disord 2013;43(12):2737-47
132 children with autismspectrum disorders (ASD) and 81 with special educational needs (SEN) but no ASD, aged 10-14 years.
82 typically developing (TD) children.
% children with past and current gastro-intestinal (GI) symptoms
46.5%
29.2%
21.8%
50 –
40 –
30 –
20 –
10 –
.0
ASD SEN TD
autismspectrumdisorders
typically developing
special educational
needs
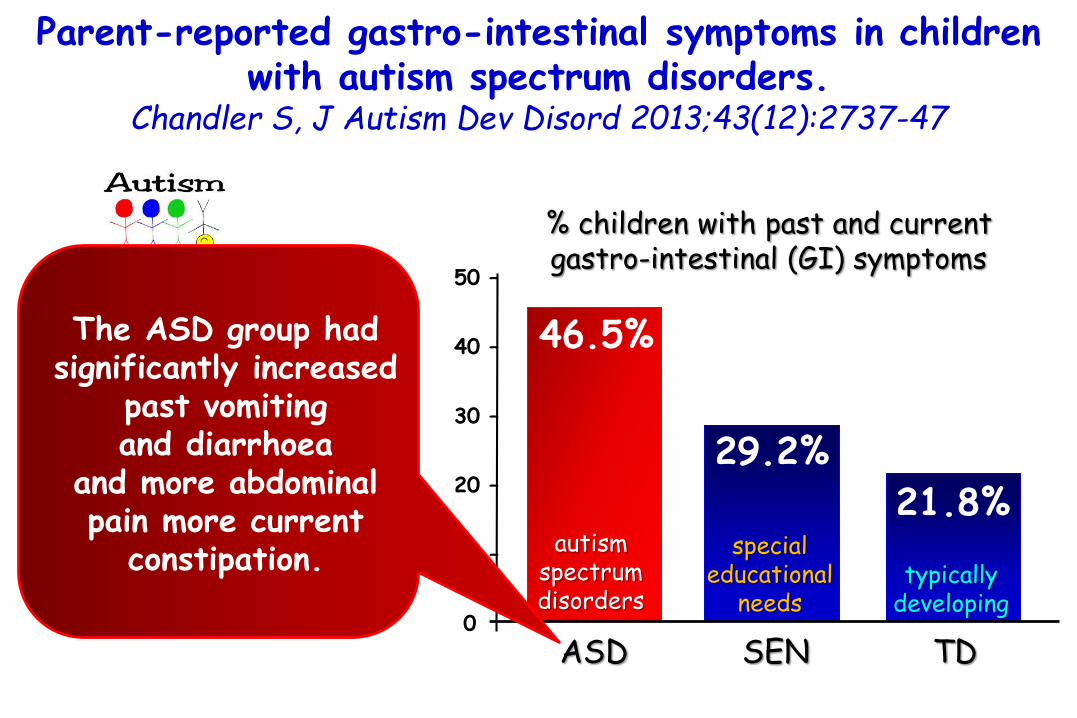
Parent-reported gastro-intestinal symptoms in children with autism spectrum disorders.
Chandler S, J Autism Dev Disord 2013;43(12):2737-47
132 children with autismspectrum disorders (ASD) and 81 with special educational needs (SEN) but no ASD, aged 10-14 years.
82 typically developing (TD) children.
% children with past and current gastro-intestinal (GI) symptoms
46.5%
29.2%
21.8%
50 –
40 –
30 –
20 –
10 –
.0
ASD SEN TD
The ASD group had significantly increased
past vomiting and diarrhoea
and more abdominal pain more current
constipation.autism
spectrumdisorders
typically developing
special educational
needs

Constipation with acquired megarectum in children with autism. Afzal N, Pediatrics 2003:112:939–42
103 autistic children referred for gastroenterological assessment.
29 control radiographs from referred to the emergency department, with abdominal pain.
Radiographs and a radiologist. The severity of constipation was determined using a validated index.
Autistic
36%
% children with moderate or severe constipation
10%
Controls
p=0.011
40 –
30 –
20 –
10 –
.0

Constipation with acquired megarectum in children with autism. Afzal N, Pediatrics 2003:112:939–42
103 autistic children referred for gastroenterological assessment.
29 control radiographs from referred to the emergency department, with abdominal pain.
Radiographs and a radiologist. The severity of constipation was determined using a validated index.
Autistic
36%
% children with moderate or severe constipation
10%
Controls
p=0.011
40 –
30 –
20 –
10 –
.0
Multivariate regression analysis showed
consumption of milk to be the strongest
predictor of constipation in the
autistic group.

Constipation with acquired megarectum in children with autism. Afzal N, Pediatrics 2003:112:939–42
Autistic
54.4%
% children with moderate/severe
rectosigmoid loading or acquired megarectum
21.1%
Controls
p<0.001
60 –
50 –
40 –
30 –
20 –
10 –
.0
103 autistic children referred for gastroenterological assessment.
29 control radiographs from referred to the emergency department, with abdominal pain.
Radiographs and a radiologist. The severity of constipation was determined using a validated index.

Accumulating evidence strongly suggests that Gastro Intestinal dysfunctions and abdominal pain are often present in children withASD.
The reported prevalence of gastrointestnal symptoms ranges from 9% to 91%, an immense range probably due to varying interpretations of GI problems, inability of ASD children to express their discomfort and the heterogeneity of the disorder.
Pathways underlying the gut-to-brain connection in autism spectrum disorders as future targets for diseasemanagement.de Theije CG, Eur J Pharmacol 2011: 668:S70–80.
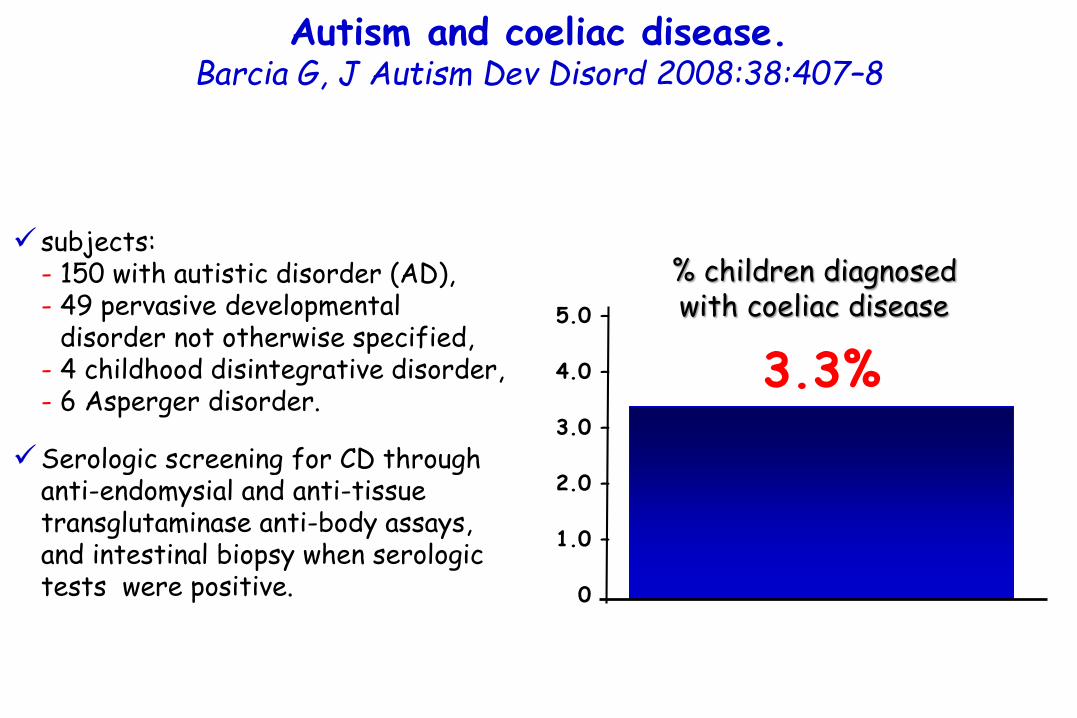
Autism and coeliac disease.Barcia G, J Autism Dev Disord 2008:38:407–8
subjects: - 150 with autistic disorder (AD), - 49 pervasive developmental- disorder not otherwise specified, - 4 childhood disintegrative disorder, - 6 Asperger disorder.
Serologic screening for CD throughanti-endomysial and anti-tissuetransglutaminase anti-body assays, and intestinal biopsy when serologictests were positive.
3.3%5.0 –
4.0 –
3.0 –
2.0 –
1.0 –
0.0
% children diagnosed with coeliac disease

Autism and coeliac disease.Barcia G, J Autism Dev Disord 2008:38:407–8
subjects: - 150 with autistic disorder (AD), - 49 pervasive developmental- disorder not otherwise specified, - 4 childhood disintegrative disorder, - 6 Asperger disorder.
Serologic screening for CD throughanti-endomysial and anti-tissuetransglutaminase anti-body assays, and intestinal biopsy when serologictests were positive.
The diagnostic category pervasive developmental disorders (PDD), as opposed to specific developmental disorders (SDD), refers to a group of five disorders characterized by delays in the development of multiple basic functions including socialization and communication.
The pervasive developmental disorders are:1) Pervasive developmental disorder not otherwise specified (PDD-NOS), which includes atypical autism, and is the most common;2) Autism, the best-known, now understood to be part of a spectrum;3) Asperger syndrome;4) Rett syndrome; and5) Childhood disintegrative disorder (CDD).

Autism and coeliac disease.Barcia G, J Autism Dev Disord 2008:38:407–8
subjects: - 150 with autistic disorder (AD), - 49 pervasive developmental- disorder not otherwise specified, - 4 childhood disintegrative disorder, - 6 Asperger disorder.
Serologic screening for CD throughanti-endomysial and anti-tissuetransglutaminase anti-body assays, and intestinal biopsy when serologictests were positive.
3.3%5.0 –
4.0 –
3.0 –
2.0 –
1.0 –
0.0
% children diagnosed with coeliac disease
This is significantly higher (p = 0.014) in comparison to
CD prevalence for the general paediatric population
of 0.94% (1:106).
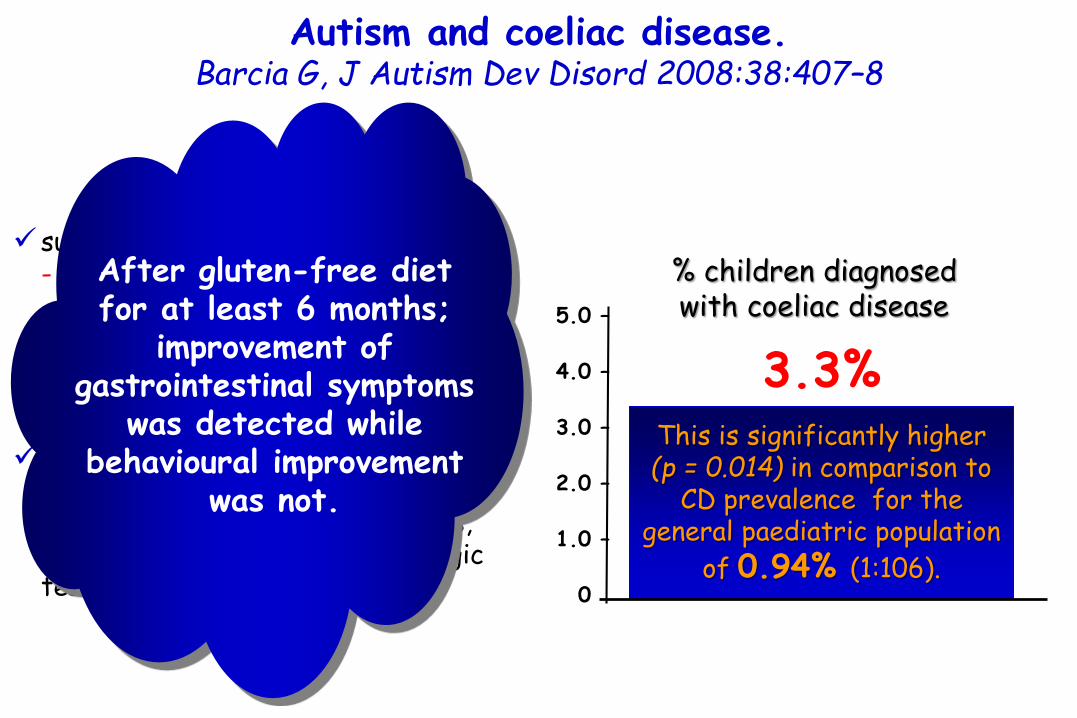
Autism and coeliac disease.Barcia G, J Autism Dev Disord 2008:38:407–8
subjects: - 150 with autistic disorder (AD), - 49 pervasive developmental- disorder not otherwise specified, - 4 childhood disintegrative disorder, - 6 Asperger disorder.
Serologic screening for CD throughanti-endomysial and anti-tissuetransglutaminase anti-body assays, and intestinal biopsy when serologictests were positive.
3.3%5.0 –
4.0 –
3.0 –
2.0 –
1.0 –
0.0
% children diagnosed with coeliac disease
This is significantly higher (p = 0.014) in comparison to
CD prevalence for the general paediatric population
of 0.94% (1:106).
After gluten-free diet for at least 6 months;
improvement of gastrointestinal symptoms
was detected while behavioural improvement
was not.

Autism and coeliac disease.Barcia G, J Autism Dev Disord 2008:38:407–8
subjects: - 150 with autistic disorder (AD), - 49 pervasive developmental- disorder not otherwise specified, - 4 childhood disintegrative disorder, - 6 Asperger disorder.
Serologic screening for CD throughanti-endomysial and anti-tissuetransglutaminase anti-body assays, and intestinal biopsy when serologictests were positive.
3.3%5.0 –
4.0 –
3.0 –
2.0 –
1.0 –
0.0
% children diagnosed with coeliac disease
This is significantly higher (p = 0.014) in comparison to
CD prevalence for the general paediatric population
of 0.94% (1:106).
Screening for CD is recommended in all
children with autism, even if no
gastrointestinal symptoms are present.

Celiac disease presenting as autism. Genuis SJ, J Child Neurol 2010:25: 114–9
Investigations revealed inadequate levels of fat-soluble vitamins, including notable deficiencies of vitamins A, D, and E as well as low coenzyme Q10 and folate. Plasma levels of Ώ-3 fatty acids including a-linolenic acid and docosahexanoic acid were also very low. In addition, polyunsaturated Ώ-6 fatty acids including linoleic acid and γ-linolenic acid were noted to be markedly deficient. Amino acid status and mineral status were unremarkable other than a low zinc level.
These findings along with low saturated fat status (despite regular consumption of saturated fats in his diet)
were suggestive of difficulty with fat absorption.

Autism spectrum disorder and celiac disease: no evidencefor a link. Batista IC, Arq Neuropsiquiatr 2012:70:28–33.
Occurrences of CD determined in a group of children and adolescents affected by ASD and, conversely, occurrences of ASD assessed in a group of biopsy-proven celiac patients.
levels of antigliadin antibodies to asses gluten sensitivity (GS) in ASD patients compared with the levels in a group of non-celiac children.
1) The prevalence of CoeliacDisease or Gluten Sensitivity in ASD patients was not greater than in groups originating from the same geographical area.
2) Similarly the prevalence of ASD was not greater than in a group of biopsy-proven CD patients.
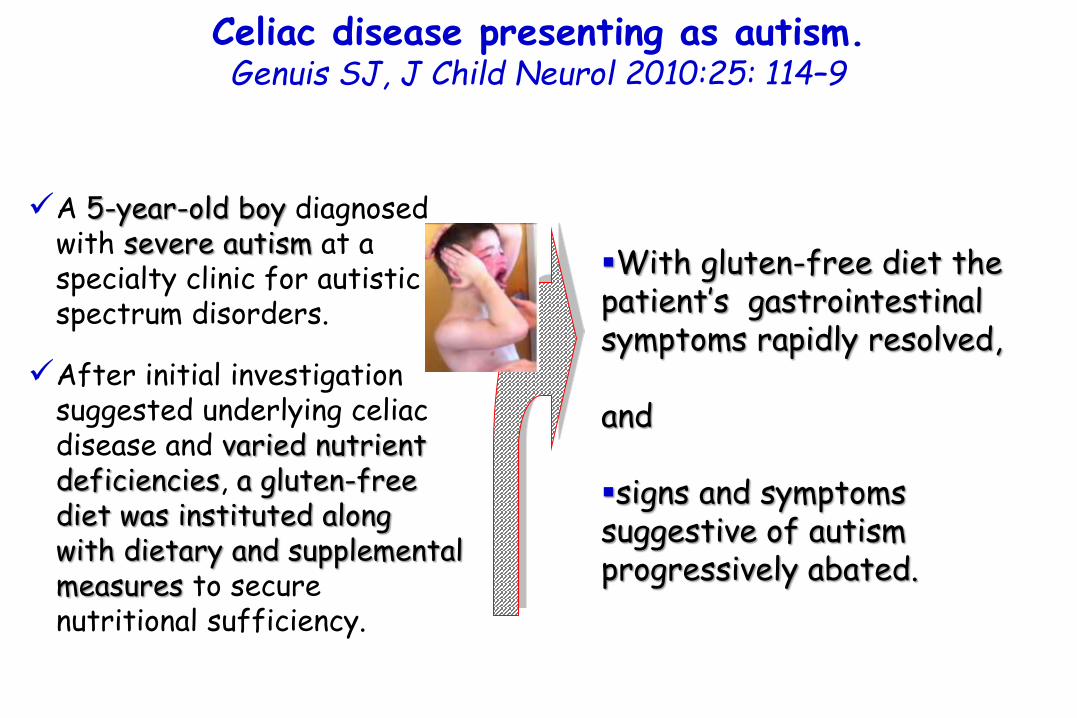
Celiac disease presenting as autism. Genuis SJ, J Child Neurol 2010:25: 114–9
A 5-year-old boy diagnosed with severe autism at a specialty clinic for autistic spectrum disorders.
After initial investigation suggested underlying celiac disease and varied nutrient deficiencies, a gluten-free diet was instituted along with dietary and supplemental measures to secure nutritional sufficiency.
With gluten-free diet the patient’s gastrointestinal symptoms rapidly resolved,
and
signs and symptoms suggestive of autism progressively abated.
Celiac disease presenting as autism. Genuis SJ, J Child Neurol 2010:25: 114–9
This case is an example of a common malabsorptionsyndrome associated with central nervous system dysfunction and suggests that in some contexts, nutritional deficiency may be a determinant of developmental delay.
A 5-year-old boy diagnosed with severe autism at a specialty clinic for autistic spectrum disorders.
After initial investigation suggested underlying celiac disease and varied nutrient deficiencies, a gluten-free diet was instituted along with dietary and supplemental measures to secure nutritional sufficiency.

Celiac disease presenting as autism. Genuis SJ, J Child Neurol 2010:25: 114–9
This case is an example of a common malabsorptionsyndrome associated with central nervous system dysfunction and suggests that in some contexts, nutritional deficiency may be a determinant of developmental delay.
A 5-year-old boy diagnosed with severe autism at a specialty clinic for autistic spectrum disorders.
After initial investigation suggested underlying celiac disease and varied nutrient deficiencies, a gluten-free diet was instituted along with dietary and supplemental measures to secure nutritional sufficiency.
It is recommended that all children with
neurodevelopmentalproblems be assessed
for nutritional deficiency
and malabsorptionsyndromes.

Alterations of the intestinal barrier in patients with autism spectrum disorders and in their first-degree relatives.
de Magistris L, J Pediatr Gastroenterol Nutr 2010:51:418–24
Intestinal permeability(IPT) by means of the lactulose/mannitol test.
Faecal calprotectin in patients with autism, either with or without gastrointestinal symptoms, and in their first-degree relatives.
Mannitol is a small molecule that normally passes through easily and serves as a marker of how well nutrients are being absorbed.
Lactulose is a larger molecule that doesn't normally pass through very well and serves as a marker for whether there are large holes in the lining.
To perform the test, the patient mixes pre-measured amounts of lactulose and mannitoland drinks it.
The test measures the amount of lactuloseand mannitol recovered in a 6-hour urine sample.

Alterations of the intestinal barrier in patients with autism spectrum disorders and in their first-degree relatives.
de Magistris L, J Pediatr Gastroenterol Nutr 2010:51:418–24
patients withautism
36.7%
21.2%
4.8%their
relativesnormal
subjects
40 –
30 –
20 –
10 –
.0
% subjects with abnormal intestinal permeability
Intestinal permeability(IPT) by means of the lactulose/mannitol test.
Faecal calprotectin in patients with autism, either with or without gastrointestinal symptoms, and in their first-degree relatives.
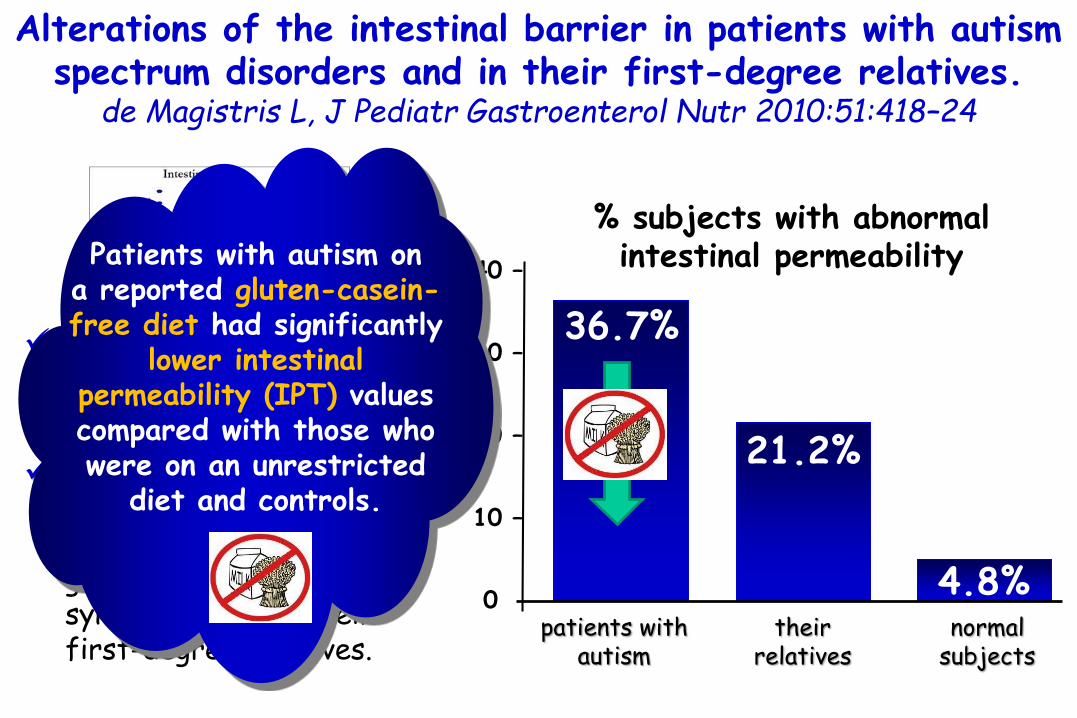
Intestinal permeability(IPT) by means of the lactulose/mannitol test.
Faecal calprotectin in patients with autism, either with or without gastrointestinal symptoms, and in their first-degree relatives.
Alterations of the intestinal barrier in patients with autism spectrum disorders and in their first-degree relatives.
de Magistris L, J Pediatr Gastroenterol Nutr 2010:51:418–24
patients withautism
36.7%
21.2%
4.8%their
relativesnormal
subjects
40 –
30 –
20 –
10 –
.0
Patients with autism on a reported gluten-casein-free diet had significantly
lower intestinal permeability (IPT) values compared with those who were on an unrestricted
diet and controls.
% subjects with abnormal intestinal permeability

Intestinal permeability(IPT) by means of the lactulose/mannitol test.
Faecal calprotectin in patients with autism, either with or without gastrointestinal symptoms, and in their first-degree relatives.
Alterations of the intestinal barrier in patients with autism spectrum disorders and in their first-degree relatives.
de Magistris L, J Pediatr Gastroenterol Nutr 2010:51:418–24
patients withautism
36.7%
21.2%
4.8%their
relativesnormal
subjects
40 –
30 –
20 –
10 –
.0
The results obtained support the leaky gut
hypothesis and indicate that measuring IPT
could help to identify a subgroup of patients with autism who could
benefit from a gluten-free diet.
% subjects with abnormal intestinal permeability

Alterations of the intestinal barrier in patients with autism spectrum disorders and in their first-degree relatives.
de Magistris L, J Pediatr Gastroenterol Nutr 2010:51:418–24
Intestinal permeability(IPT) by means of the lactulose/mannitol test.
Faecal calprotectin in patients with autism, either with or without gastrointestinal symptoms, and in their first-degree relatives.
% of children with autismand gastrointestinal symptoms
constipation
45.5%
34.1%
15.9%
diarrhoea alternatingdiarrhoea-
constipation, abdominal pain
50 –
40 –
30 –
20 –
10 –
.0

Alterations of the intestinal barrier in patients with autism spectrum disorders and in their first-degree relatives.
de Magistris L, J Pediatr Gastroenterol Nutr 2010:51:418–24
Intestinal permeability(IPT) by means of the lactulose/mannitol test.
Faecal calprotectin in patients with autism, either with or without gastrointestinal symptoms, and in their first-degree relatives.
constipation
45.5%
34.1%
15.9%
diarrhoea alternatingdiarrhoea-
constipation, abdominal pain
50 –
40 –
30 –
20 –
10 –
.0
Faecal calprotectinwas elevated in 24.4%
of patients with autism
and in 11.6% of their relatives; it was not, however, correlated
with abnormal IPT values.
% of children with autismand gastrointestinal symptoms
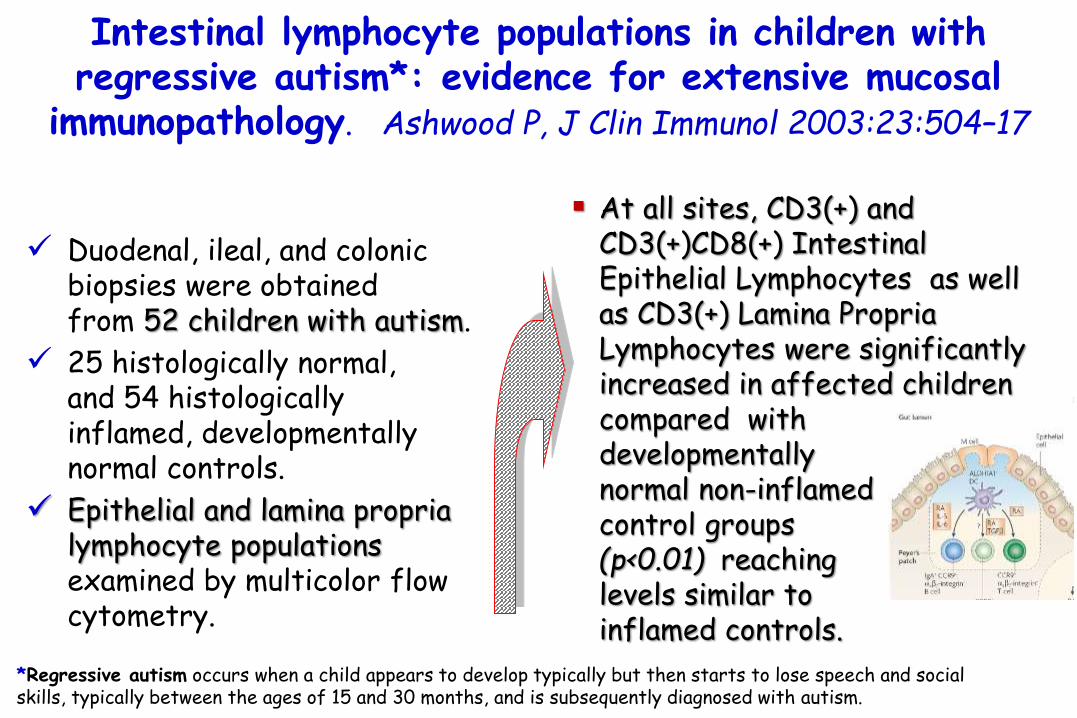
Intestinal lymphocyte populations in children with regressive autism*: evidence for extensive mucosal
immunopathology. Ashwood P, J Clin Immunol 2003:23:504–17
Duodenal, ileal, and colonic biopsies were obtained from 52 children with autism.
25 histologically normal, and 54 histologicallyinflamed, developmentally normal controls.
Epithelial and lamina proprialymphocyte populations examined by multicolor flow cytometry.
At all sites, CD3(+) and CD3(+)CD8(+) Intestinal Epithelial Lymphocytes as well as CD3(+) Lamina PropriaLymphocytes were significantly increased in affected children compared with developmentally normal non-inflamed control groups (p<0.01) reaching levels similar to inflamed controls.
*Regressive autism occurs when a child appears to develop typically but then starts to lose speech and social skills, typically between the ages of 15 and 30 months, and is subsequently diagnosed with autism.

Intestinal lymphocyte populations in children with regressive autism: evidence for extensive mucosal
immunopathology. Ashwood P, J Clin Immunol 2003:23:504–17
Comparison of T-cell populations within the lamina propria (A)
and epithelial (B) compartments of duodenal biopsy
*p < 0.05 ; ** p < 0.01 compared with ASD patients
Detection of lymphocyte populations within lamina propria (A)
and epithelial (B) compartmentsfrom terminal ileum biopsy
*p < 0.05 ; ** p < 0.01 compared with ASD patients
* *
*
*
*
*
*
*
*
* *
*
*
*
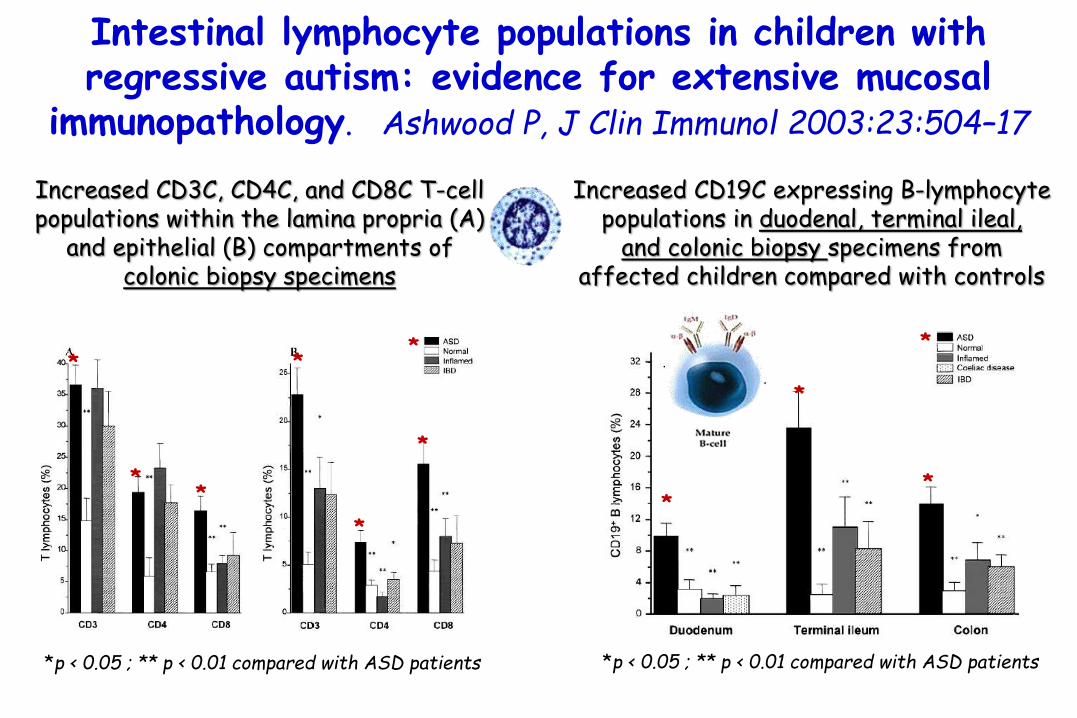
Intestinal lymphocyte populations in children with regressive autism: evidence for extensive mucosal
immunopathology. Ashwood P, J Clin Immunol 2003:23:504–17
Increased CD3C, CD4C, and CD8C T-cell populations within the lamina propria (A)
and epithelial (B) compartments of colonic biopsy specimens
*p < 0.05 ; ** p < 0.01 compared with ASD patients
Increased CD19C expressing B-lymphocyte populations in duodenal, terminal ileal,
and colonic biopsy specimens from affected children compared with controls
*p < 0.05 ; ** p < 0.01 compared with ASD patients
* **
**
*
*
*
*
*
*

Intestinal lymphocyte populations in children with regressive autism: evidence for extensive mucosal
immunopathology. Ashwood P, J Clin Immunol 2003:23:504–17
Increased CD3C, CD4C, and CD8C T-cell populations within the lamina propria (A)
and epithelial (B) compartments of colonic biopsy specimens
*p < 0.05 ; ** p < 0.01 compared with ASD patients
Increased CD19C expressing B-lymphocytepopulations in duodenal, terminal ileal,
and colonic biopsy specimens from affected children compared with controls
*p < 0.05 ; ** p < 0.01 compared with ASD patients
* **
**
*
*
*
*
*
*
The data provide further evidence of a pan-enteric mucosal immunopathologyin children with autism
that is apparently distinct from other inflammatory
bowel diseases.

Food allergy in autism spectrum disorder
De Theije CGM, Peditr Allergy Imm 2014;25:218
An imbalance in T-cell subsets has been suggested in ASD patients.
Low numbers of Th1- type INF-y and IL-2 positive cells were observed in blood of ASD children compared with healthy controls. Gupta S, J Neuroimmunol 1998:85:106–9.
Significant increase was observed in Th2 cytokine production by PBMC (IL-4, IL-5, and IL-13) from autistic children when compared to age-matched controls regarding. Molloy CA, J Neuroimmunol 2006:172:198–205.
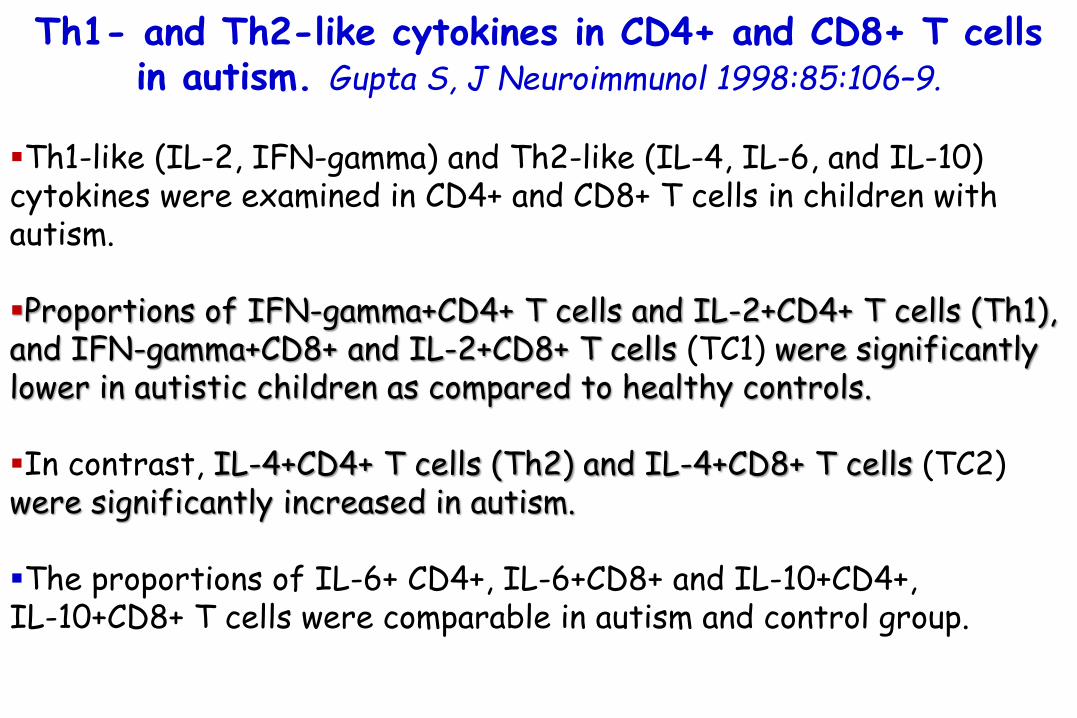
Th1- and Th2-like cytokines in CD4+ and CD8+ T cellsin autism. Gupta S, J Neuroimmunol 1998:85:106–9.
Th1-like (IL-2, IFN-gamma) and Th2-like (IL-4, IL-6, and IL-10) cytokines were examined in CD4+ and CD8+ T cells in children with autism.
Proportions of IFN-gamma+CD4+ T cells and IL-2+CD4+ T cells (Th1), and IFN-gamma+CD8+ and IL-2+CD8+ T cells (TC1) were significantly lower in autistic children as compared to healthy controls.
In contrast, IL-4+CD4+ T cells (Th2) and IL-4+CD8+ T cells (TC2) were significantly increased in autism.
The proportions of IL-6+ CD4+, IL-6+CD8+ and IL-10+CD4+, IL-10+CD8+ T cells were comparable in autism and control group.

Th1- and Th2-like cytokines in CD4+ and CD8+ T cellsin autism. Gupta S, J Neuroimmunol 1998:85:106–9.
Th1-like (IL-2, IFN-gamma) and Th2-like (IL-4, IL-6, and IL-10) cytokines were examined in CD4+ and CD8+ T cells in children with autism.
Proportions of IFN-gamma+CD4+ T cells and IL-2+CD4+ T cells (Th1), and IFN-gamma+CD8+ and IL-2+CD8+ T cells (TC1) were significantly lower in autistic children as compared to healthy controls.
In contrast, IL-4+CD4+ T cells (Th2) and IL-4+CD8+ T cells (TC2) were significantly increased in autism.
The proportions of IL-6+ CD4+, IL-6+CD8+ and IL-10+CD4+, IL-10+CD8+ T cells were comparable in autism and control group.
These data suggest that an imbalance of Th1- and Th2-like cytokines in autism may play a role in the pathogenesis of
autism.

Elevated cytokine levels in children with autism spectrum disorder. Molloy CA, J Neuroimmunol 2006:172:198–205
20 children with autism spectrum disorder and matched controls.
Levels of all Th2 cytokines were significantly higher in cases.
Cases had significantly higher IL-13/IL-10 and IFN-γ/IL-10 than controls.
(+)
(+)

Elevated cytokine levels in children with autism spectrum disorder. Molloy CA, J Neuroimmunol 2006:172:198–205
20 children with autism spectrum disorder and matched controls.
Levels of all Th2 cytokines were significantly higher in cases.
Cases had significantly higher IL-13/IL-10 and IFN-γ/IL-10 than controls.
(+)
(+)
Children with ASD had increased activation of both Th2 and Th1 arms of the adaptive immune
response, with a Th2 predominance, and without the
compensatory increase in the regulatory cytokine IL-10.

Food allergy in autism spectrum disorder
De Theije CGM, Peditr Allergy Imm 2014;25:218
Concerning regulatory T-cellresponses, reduced levels of IL-10 and TGF-β were observed in children with ASD, indicating reduced tolerance to antigens.Ashwood P, J Neuroimmunol2008:204:149–53.Okada K, Prog Neuro BiolPsychiatry 2007:31:187–90.
Furthermore, these low TGF-β levels correlated with worse behavioral scores, suggesting that reduced regulatory T-cell responses could be involved in the regulation of autistic behavior.Ashwood P, J Neuroimmunol 2008:204:149–53.

Decreased serum levels of transforming growth factor-beta 1 in patients with autism.
Okada K, Prog Neuropsychopharmacol Biol Psychiatry 2007:31:187–90
BACKGROUND:
The neurobiological basis for autism remains poorly understood.
Given the key role of transforming growth factor-β1 (TGF-β1) in brain development, we hypothesized that TGF-β1 plays a role in the pathophysiology of autism.
In this study, we studied whether serum levels of TGF-β1 are altered in patients with autism.

Decreased serum levels of transforming growth factor-beta 1 in patients with autism.
Okada K, Prog Neuropsychopharmacol Biol Psychiatry 2007:31:187–90
TGF-β1 in 19 male adult patients with autism
21 age-matched male healthy subjects.
Patients withautism
7.34
Serum levels (ng/mL) of TGF- β1
14.48
Normal controls
p<0.001
15 –
10 –
05 –
…0

Decreased serum levels of transforming growth factor-beta 1 in patients with autism.
Okada K, Prog Neuropsychopharmacol Biol Psychiatry 2007:31:187–90
TGF-β1 in 19 male adult patients with autism
21 age-matched male healthy subjects.
Patients withautism
7.34
Serum levels (ng/mL) of TGF- β1
14.48
Normal controls
p<0.001
15 –
10 –
05 –
…0
However, there were no marked or significant
correlations between serumTGF-β1 levels and other clinical
variables, including: Autism Diagnostic Interview-
Revised (ADI-R) scores, Yale-Brown Obsessive-
Compulsive Scale (Y-BOCS), aggression, and
Intellectual Quotient
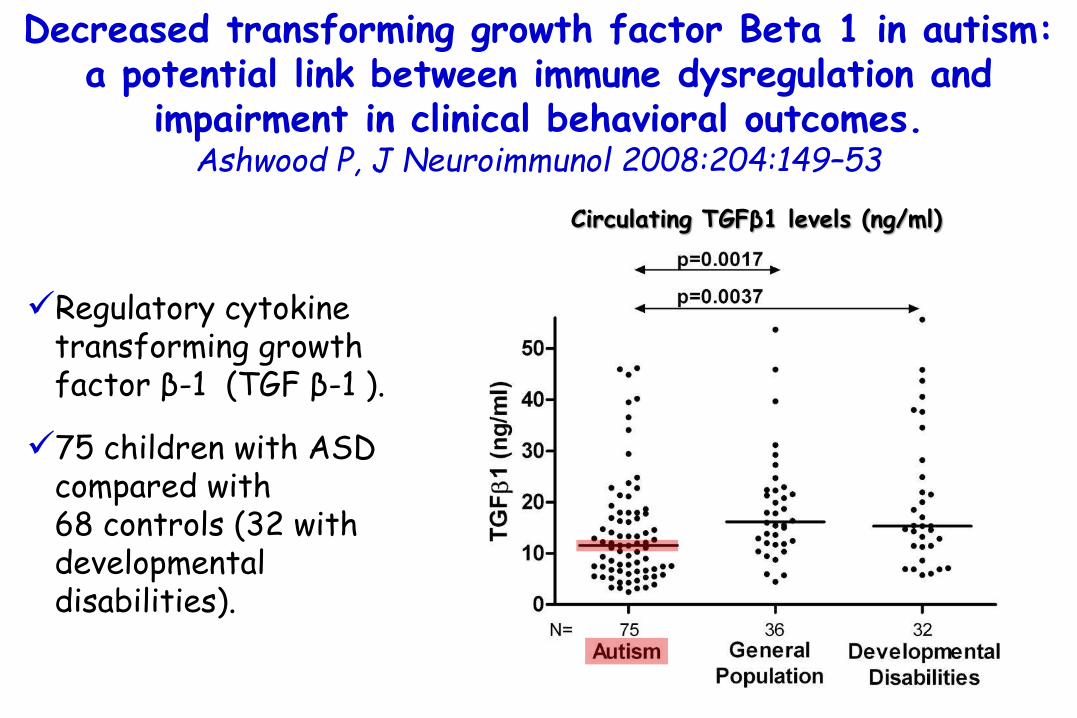
Decreased transforming growth factor Beta 1 in autism: a potential link between immune dysregulation and
impairment in clinical behavioral outcomes.Ashwood P, J Neuroimmunol 2008:204:149–53
Regulatory cytokine transforming growth factor β-1 (TGF β-1 ).
75 children with ASD compared with 68 controls (32 with developmental disabilities).
Circulating TGFβ1 levels (ng/ml)

Decreased transforming growth factor Beta 1 in autism: a potential link between immune dysregulation and
impairment in clinical behavioral outcomes.Ashwood P, J Neuroimmunol 2008:204:149–53
Regulatory cytokine transforming growth factor β-1 (TGF β-1 ).
75 children with ASD compared with 68 controls (32 with developmental disabilities).
Circulating TGFβ1 levels (ng/ml)
TGF β-1 levels were significantly decreased in
children with autism compared with typically
developing general population controls
(p=0.0017) and children with other developmental disabilities (p=0.0037).

Decreased transforming growth factor Beta 1 in autism: a potential link between immune dysregulation and
impairment in clinical behavioral outcomes.Ashwood P, J Neuroimmunol 2008:204:149–53
Regulatory cytokine transforming growth factor β-1 (TGF β-1 ).
75 children with ASD compared with 68 controls (32 with developmental disabilities).
Circulating TGFβ1 levels (ng/ml)
There were significant correlations between
psychological measures and TGF β-1 levels, such that lower TGF β-1 levels
were associated with lower adaptive behaviors
and worse behavioral symptoms.

Decreased transforming growth factor Beta 1 in autism: a potential link between immune dysregulation and
impairment in clinical behavioral outcomes.Ashwood P, J Neuroimmunol 2008:204:149–53
Regulatory cytokine transforming growth factor β-1 (TGF β-1 ).
75 children with ASD compared with 68 controls (32 with developmental disabilities).
Circulating TGFβ1 levels (ng/ml)
Such immune dysregulationmay predispose to the development of possible autoimmune responses
and/or adverse neuroimmuneinteractions during critical windows in development.

Decreased transforming growth factor Beta 1 in autism: a potential link between immune dysregulation and
impairment in clinical behavioral outcomes.Ashwood P, J Neuroimmunol 2008:204:149–53
Regulatory cytokine transforming growth factor β-1 (TGF β-1 ).
75 children with ASD compared with 68 controls (32 with developmental disabilities).
Circulating TGFβ1 levels (ng/ml)
TGF-β is required for the development of
microglia
microglia are absent in the CNS of TGF-β1-deficient
mice.
Butovsky O, Nat Neurosci. 2014 ;17(1):131-43.
Microglia cells are the resident macrophages of the brain and act as the first
and main form of active immune defense in the central nervous system

Emerging roles for TGF-β1 in nervous system development Gomes FCA, Int J Dev Neurosci 2005;23:413–24.
TGF-betas family is represented by three isoforms: TGF-beta1, -beta 2 and -beta 3, all produced by both glial and neuronal cells.
They are involved in essential tissue functions, including cell-cycle control, regulation of early development and differentiation, neuron survival and astrocyte differentiation.
TGF-beta1 might be a crucial regulator of CNS development.
Expression of TGF-b1 and TGFRII by neurons and astrocytes of the
cerebral cortex

Emerging roles for TGF-β1 in nervous system development Gomes FCA, Int J Dev Neurosci 2005;23:413–24.
TGF-β1 network as mediatorof astrocyte interactions.
1) Neurons increase production and release of TGF-b1 by astrocytes, which in turn protects neighboring neurons against excitotoxic death. 2) Additionally, TGF-b1 secreted by neurons modulates neuronal migration along radial glia fibers and might be involved in radial glia differentiation. 3) In addition to promoting neuronal survival, TGF-b1 modulates several events in astrocytes such as:gene expression and differentiation; inhibition of proliferation and modulation of secretion of extracellular matrix proteins (ECM).

The role of immune dysfunction in the pathophysiology of autism. Onore C, Brain Behav Immun. 2012;26:383–392.
Neurobiological research in ASD has highlighted pathways involved in neural development, synapse plasticity, structural brain abnormalities, cognition and behavior. Several lines of evidence point to altered immune dysfunction in ASD that directly impacts some or all these neurological processes. Extensive alterations in immune function have now been described in both children and adults with ASD, including ongoing inflammation in brain specimens, elevated pro-inflammatory cytokine profiles in the CSF and blood, increased presence of brain-specific auto-antibodies and altered immune cell function. Furthermore, these dysfunctional immune responses are associated with increased impairments in behaviors characteristic of core features of ASD, in particular, deficits in social interactions and communication.

The role of immune dysfunction in the pathophysiology of autism. Onore C, Brain Behav Immun. 2012;26:383–392.
Immune dysfunction in ASD involves a network of interactions between several cell types, from the innate and adaptive arms of the immune system.
Increased cytokine production, such TNF-α and IL-1β inhibit neurogenesis and promote neuron death, while IL-6 may promote the growth and proliferation of neurons and oligodendrocytes.
Increased levels of complement proteins can participate in synaptic scaling, opsonizing synapses and targetingthem for removal by phagocytic microglia.
Activated microglia may additionally mediate synaptic pruning via MHCI interactions.

Does the human gut microbiota contribute to the etiology of autism spectrum disorders? Louis P. Dig Dis Sci 2012:57:1987–9.
The rapid increase in autism in recent years is unlikely to be explained by an increase in awareness and diagnosis of the condition alone, which also points to the environment as a contributing factor.
Environmental factors that may contribute to the etiology of ASD include pre- or postnatal exposure to certain environmental chemicals and drugs, stress, maternal infection, and dietary factors.
A subset of patients experience gastrointestinal symptoms,pointing to a role of the gut microbiota in ASD.
Changes in microbiota composition in subjects with ASD compared tohealthy control subjects have been identified in several studies, both based on bacterial culture and molecular methods.

Does the human gut microbiota contribute to the etiology of autism spectrum disorders? Louis P. Dig Dis Sci 2012:57:1987–9.

Does the human gut microbiota contribute to the etiology of autism spectrum disorders? Louis P. Dig Dis Sci 2012:57:1987–9.
Autistic subjects often receive frequent medication with antibiotics and are often on special diets or have repetitive dietary behaviors, both of which may alter
microbiota composition.
Difference in microbiota are cause or effect?

Does the human gut microbiota contribute to the etiology of autism spectrum disorders? Louis P. Dig Dis Sci 2012:57:1987–9.
A role of the microbiota in ASD is supported by the fact that interventions with antibiotics have led to an improvement of behavior and communication in ASD
subjects, and probiotic interventions have resulted in positive effects on neuropsychological symptoms
(such as mood and anxiety) in other study populations.
Critchfield JW, Gastroenterol Res Pract. 2011: 2011:161358

Does the human gut microbiota contribute to the etiology of autism spectrum disorders? Louis P. Dig Dis Sci 2012:57:1987–9.
Total short-chain fatty acid (SCFA) levels as well as all individual SCFA, were elevated in ASD subjects, pointing towards a general increase in microbiota population or
activity rather than a major shift in composition, which would more likely lead to more specific changes in
fermentation product profiles.

Does the human gut microbiota contribute to the etiology of autism spectrum disorders? Louis P. Dig Dis Sci 2012:57:1987–9.
in contrast to these results, Adams reported lower levels of several SCFA in autistic subjects.
Adams JB, BMC Gastroenterol. 2011;11:22.

Does the human gut microbiota contribute to the etiology of autism spectrum disorders? Louis P. Dig Dis Sci 2012:57:1987–9.
The short-chain fatty acids propionate and butyratehave been shown to elicit behavioral changes in rodents,
with propionate inducing changes similar to autism.
Differences in the microbiota may also result in altered microbial metabolism of aromatic amino acids,
which could lead to neurological symptoms.
Clayton TA, FEBS Lett. 2012;586:956

ADHD was first described in 1902 by a British pediatrician, G.F. Still, who first defined hyperactive behavior in children as a “defect of moral control.” However, he also believed that a medical cause and not a spiritual one was at the root of this yet-to-be-discovered entity (Lancet 1902).

In the 1930s, the etiology ofthis disorder was attributed to minimal brain damage referredto as “minimal brain dysfunction.” In 1937, doctorsmade the astounding discovery that amphetamines had aparadoxical effect
and could be used to reduce hyperactive and impulsive behaviors. The term hyperactive child syndrome was introduced in the early 1950s at which time these stimulant medications (i.e., amphetamines and methylphenidate) became regularly used as therapy for hyperactivity and impulsive disorders.

Epidemiology of ADHD
Affects 4–12% of all school-aged children
Most commonly diagnosed behavioral disorder in children
9 to 18% of school-aged children with mental retardation meet criteria for ADHD (comorbidity is high in ADHD)
Male/female ratio in childhood ranges from 4:1 to 9:1 depending on the setting (clinic or general population; DSM-IV, 1994); in adults, no male predominance is seen (1:1 ratio)
Occurs in all cultures, with prevalent findings in Western cultures (due to diagnostic methods; DSM-IV)
Mood and anxiety, learning, substance-related, and antisocial personality disorders are more prevalent in ADHD and in family members of those with ADHD (high rate of comorbidity; DSM-IV)
Estimated 30–60% persistence into adulthood; in USA estimated 9.5 million adults are suffering from ADHD
Bellanti JA, All Asthma Proc 2005;26:19

The precise etiology of ADHD still remains unknown;however, current research points strongly to a neurologically based cause. Many theories concerning the causesof ADHD are attributed to neuroanatomicand neurochemical disorders, genetic origins, central nervous system insults,and environmental factorsaffecting the production of the neurotransmitterdopamine.

Schematic representation of production of dopamine in the
presynaptic neuron and released into the synaptic
cleft where it next attaches to dopamine receptors on a postsynaptic neuron after which a neural stimulus is
initiated.
The excess dopamine istaken up by a transporter
molecule to adjust dopamine concentrations in the cleft to physiological concentrations.
In ADHD it is thought that there is an abnormal
transporter molecule that takes up excessive quantities of dopamine leaving deficient
levels in the cleft.
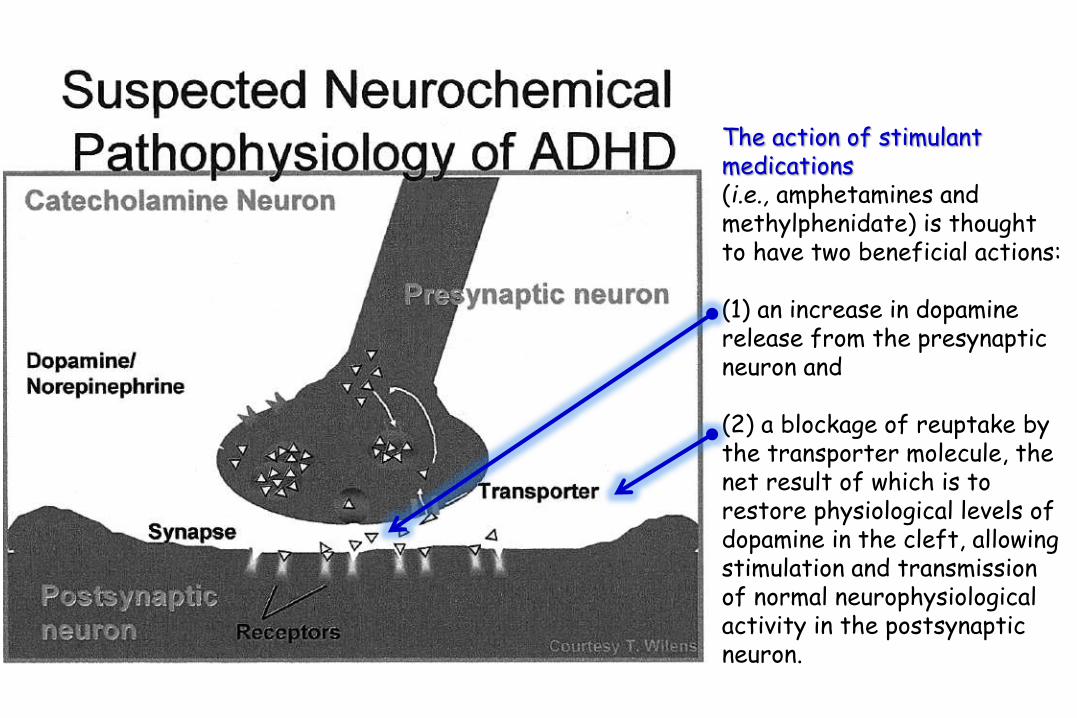
The action of stimulant medications (i.e., amphetamines and methylphenidate) is thought to have two beneficial actions:
(1) an increase in dopamine release from the presynapticneuron and
(2) a blockage of reuptake by the transporter molecule, the net result of which is to restore physiological levels of dopamine in the cleft, allowing stimulation and transmission of normal neurophysiologicalactivity in the postsynapticneuron.
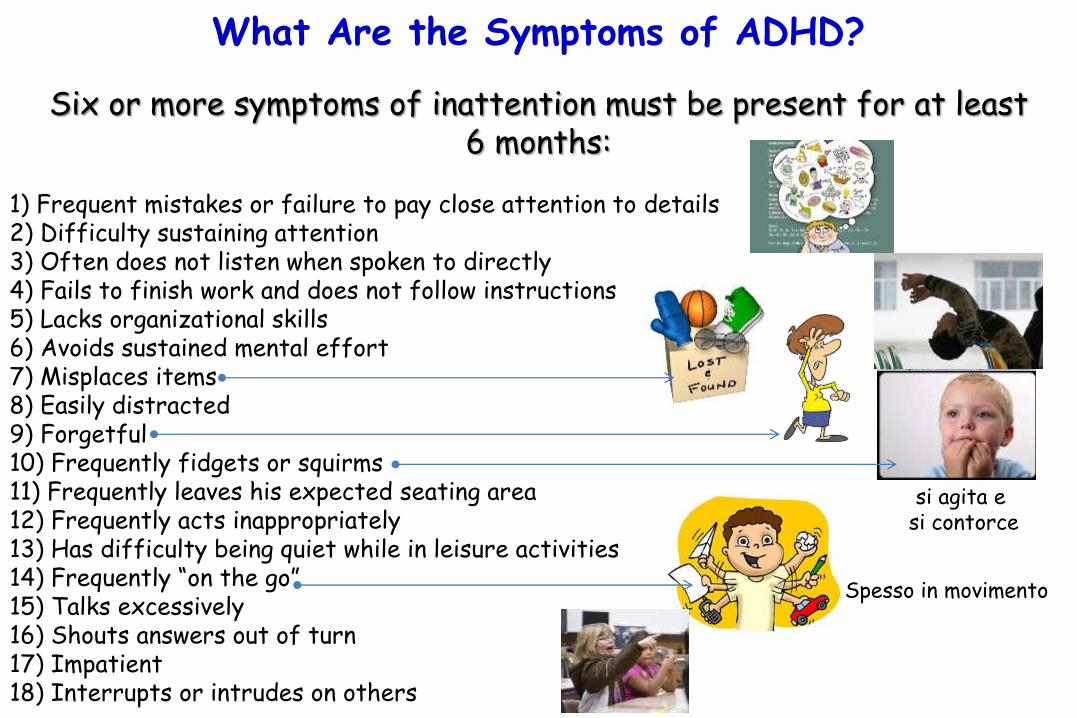
What Are the Symptoms of ADHD?
Six or more symptoms of inattention must be present for at least6 months:
1) Frequent mistakes or failure to pay close attention to details2) Difficulty sustaining attention3) Often does not listen when spoken to directly4) Fails to finish work and does not follow instructions5) Lacks organizational skills6) Avoids sustained mental effort7) Misplaces items8) Easily distracted9) Forgetful10) Frequently fidgets or squirms11) Frequently leaves his expected seating area12) Frequently acts inappropriately13) Has difficulty being quiet while in leisure activities14) Frequently “on the go”15) Talks excessively16) Shouts answers out of turn17) Impatient18) Interrupts or intrudes on others
si agita e si contorce
Spesso in movimento

De Theije CGM, Peditr Allergy Imm 2014;25:218
Food allergy in Attention-Deficit Hyperactivity Disorder
Attention deficit hyperactivity disorder (ADHD) is a neurodevelopmental disorder that is characterized by inappropriate symptoms ofinattention, impulsiveness, and hyperactivity. Diagnostic and Statistical Manual of MentalDisorders (4th ed). Washington, DC:American-Psychiatric-Association, 2000.
The relationship between allergic diseases and ADHD has been a matter of debate ever since Geschwind and Behan hypothesized on an association between left-handedness, immune disease, and developmental learning disorders.Geschwind N, Behan P. Proc Natl Acad Sci U S A 1982:79:5097–100
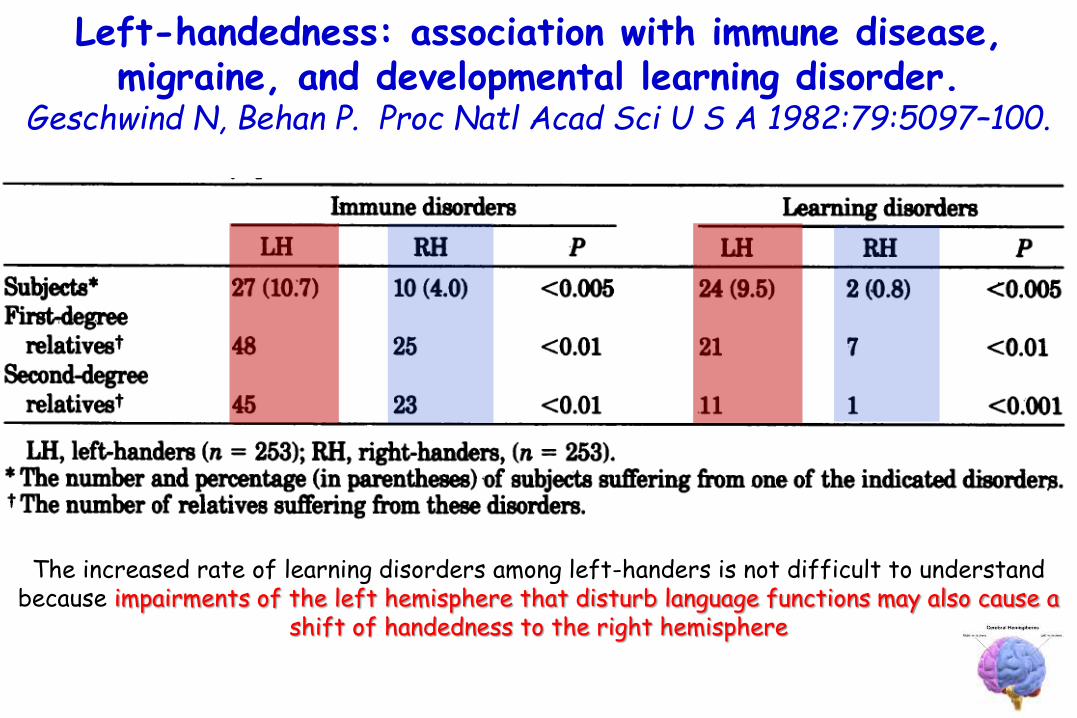
Left-handedness: association with immune disease, migraine, and developmental learning disorder.
Geschwind N, Behan P. Proc Natl Acad Sci U S A 1982:79:5097–100.
The increased rate of learning disorders among left-handers is not difficult to understand because impairments of the left hemisphere that disturb language functions may also cause a
shift of handedness to the right hemisphere
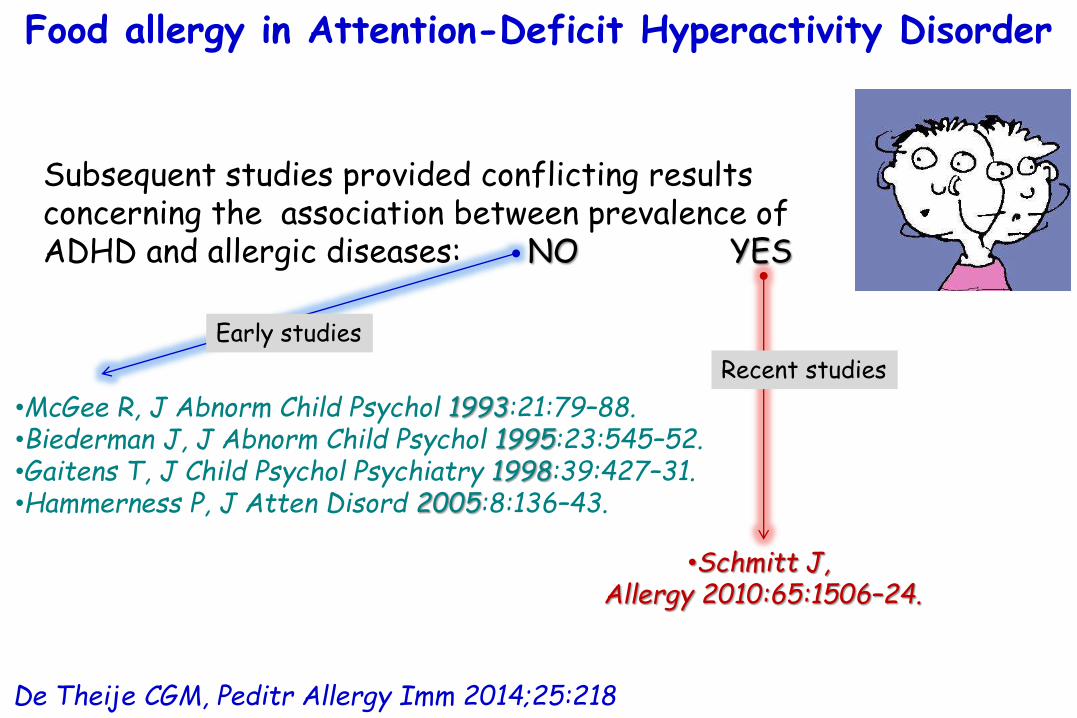
De Theije CGM, Peditr Allergy Imm 2014;25:218
Subsequent studies provided conflicting results concerning the association between prevalence of ADHD and allergic diseases: NO YES
•McGee R, J Abnorm Child Psychol 1993:21:79–88.•Biederman J, J Abnorm Child Psychol 1995:23:545–52.•Gaitens T, J Child Psychol Psychiatry 1998:39:427–31.•Hammerness P, J Atten Disord 2005:8:136–43.
•Schmitt J, Allergy 2010:65:1506–24.
Early studies
Recent studies
Food allergy in Attention-Deficit Hyperactivity Disorder

Allergic disorders and attention deficit disorder in children. McGee R, J Abnorm Child Psychol 1993:21:79–88.
It has been suggested that children with attention deficit disorder-hyperactivity (ADDH) are likely to show allergic disorders, and that both ADDH and allergic disorders may share a common biological background. In a large sample of children from the general population we found no association between parent, teacher, and self-reports of ADDH behaviors and a history of allergic disorders (asthma, eczema, rhinitis, and urticaria) at ages 9 or 13 years. Similarly, reports of ADDH behaviors at age 13 years were not related to level of atopic responsiveness by skin test or serum IgElevels. Our findings call into question the hypothesis that there is a relationship between ADDH and allergic disorder.

No confirmation of Geschwind’s hypothesis of associationsbetween reading disability, immune disorders, and motor
preference in ADHD. Biederman J, J Abnorm Child Psychol 1995:23:545–52.
Subjects were 6- to 17-year-old boys with DSM-III-R ADHD (n = 140) and normal controls (n = 120).
Information on reading disability, asthma, and motor preference was obtained in a standardized manner blind to the proband's clinical status.
Neither ADHD nor reading disability was associated with either asthma or left motor preference nor was asthma and left motor preference associated with one another.
Our results are not consistent with Geschwind's hypothesis linking reading disability, immune disorder, and left motor preference.
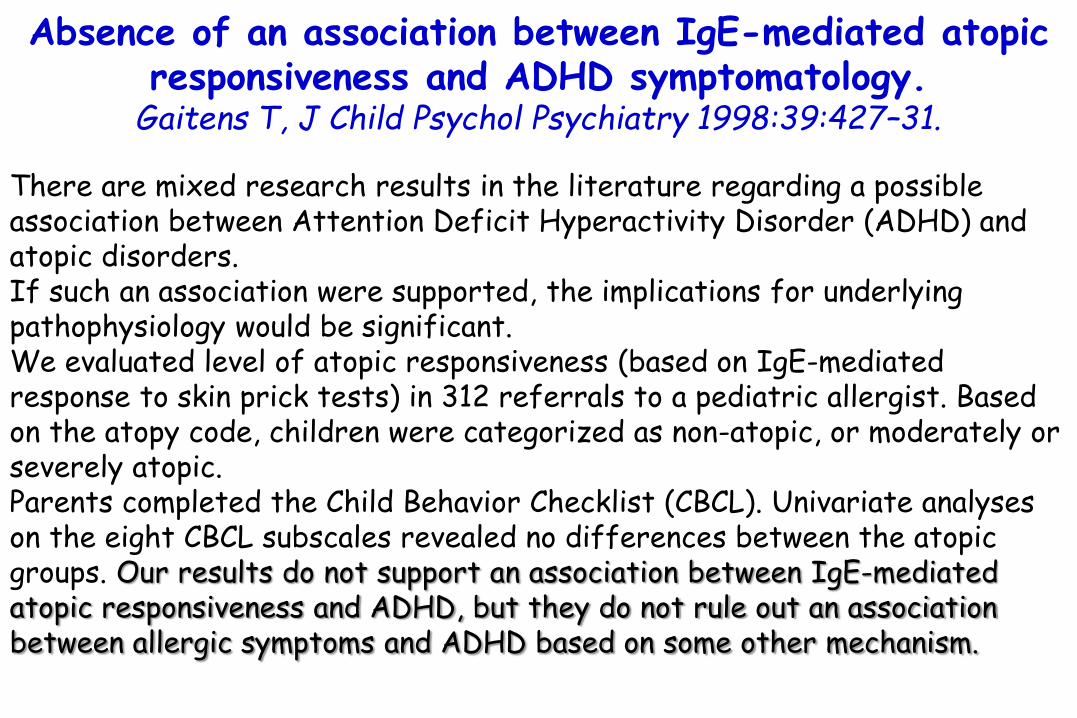
Absence of an association between IgE-mediated atopicresponsiveness and ADHD symptomatology.
Gaitens T, J Child Psychol Psychiatry 1998:39:427–31.
There are mixed research results in the literature regarding a possible association between Attention Deficit Hyperactivity Disorder (ADHD) and atopic disorders. If such an association were supported, the implications for underlying pathophysiology would be significant. We evaluated level of atopic responsiveness (based on IgE-mediated response to skin prick tests) in 312 referrals to a pediatric allergist. Based on the atopy code, children were categorized as non-atopic, or moderately or severely atopic. Parents completed the Child Behavior Checklist (CBCL). Univariate analyses on the eight CBCL subscales revealed no differences between the atopic groups. Our results do not support an association between IgE-mediated atopic responsiveness and ADHD, but they do not rule out an association between allergic symptoms and ADHD based on some other mechanism.
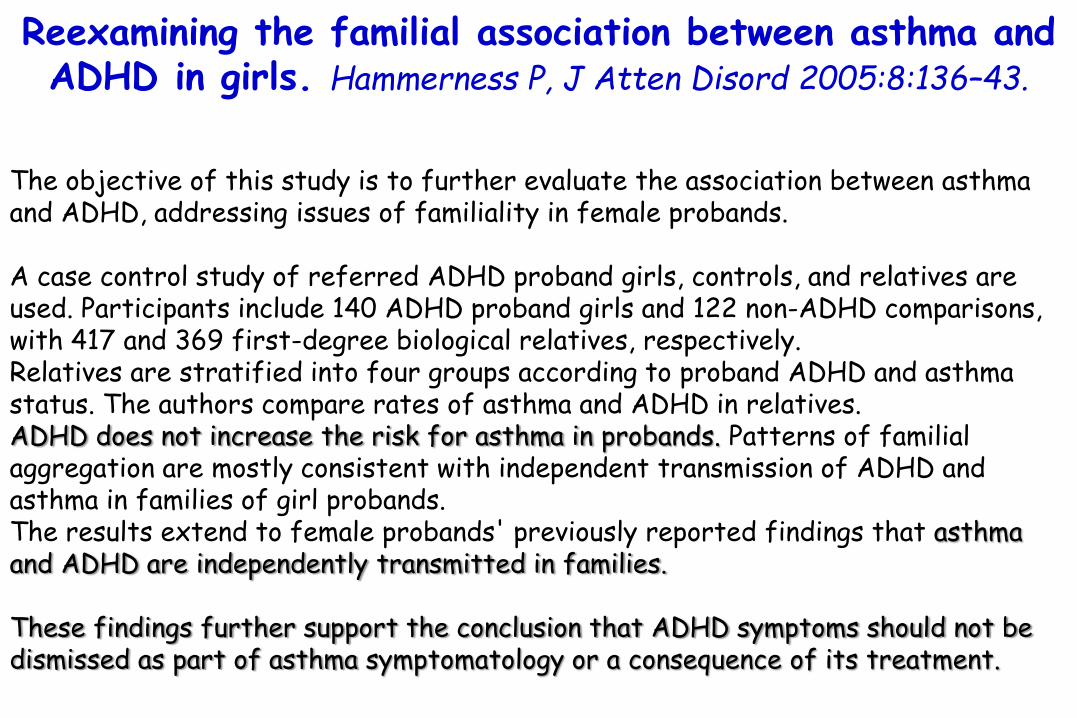
Reexamining the familial association between asthma and ADHD in girls. Hammerness P, J Atten Disord 2005:8:136–43.
The objective of this study is to further evaluate the association between asthma and ADHD, addressing issues of familiality in female probands.
A case control study of referred ADHD proband girls, controls, and relatives are used. Participants include 140 ADHD proband girls and 122 non-ADHD comparisons, with 417 and 369 first-degree biological relatives, respectively. Relatives are stratified into four groups according to proband ADHD and asthma status. The authors compare rates of asthma and ADHD in relatives. ADHD does not increase the risk for asthma in probands. Patterns of familial aggregation are mostly consistent with independent transmission of ADHD and asthma in families of girl probands. The results extend to female probands' previously reported findings that asthma and ADHD are independently transmitted in families.
These findings further support the conclusion that ADHD symptoms should not be dismissed as part of asthma symptomatology or a consequence of its treatment.

Is atopic disease a risk factor for attention-deficit/hyperactivity disorder? A systematic review.
Schmitt J, Allergy 2010:65: 1506–24.
20 relevantstudies
170 175 individuals.
6 studies consistently reported a (+) association between eczema and ADHD with one study suggesting effect modification by sleeping problems.
12 studies consistently found a (+) association between asthma and ADHD, which, however, appeared to be at least partly explained by concurrent or previous eczema.

Is atopic disease a risk factor for attention-deficit/hyperactivity disorder? A systematic review.
Schmitt J, Allergy 2010:65: 1506–24.
20 relevantstudies
170 175 individuals.
6 studies consistently reported a (+) association between eczema and ADHD with one study suggesting effect modification by sleeping problems.
12 studies consistently found a (+) association between asthma and ADHD, which, however, appeared to be at least partly explained by concurrent or previous eczema.
Rhinitis and serum-IgE level were not related
to ADHD symptomatology.

Is atopic disease a risk factor for attention-deficit/hyperactivity disorder? A systematic review.
Schmitt J, Allergy 2010:65: 1506–24.
20 relevantstudies
170 175 individuals.
6 studies consistently reported a (+) association between eczema and ADHD with one study suggesting effect modification by sleeping problems.
12 studies consistently found a (+) association between asthma and ADHD, which, however, appeared to be at least partly explained by concurrent or previous eczema.
eczema appears to be
independently related to ADHD.

Association between allergic sensitization and attention deficit hyperactivity disorder (ADHD).
Suwan P, Asian Pac J Allergy Immunol 2011:29:57–65
40 patients with ADHD.
40 controls.
SPTs to common allergens.
ADHD
67.5%
% subjects with (+) SPTs
45.0%
Controls
p=0.043
70 –
60 –
50 –
40 –
30 –
20 –
10 –
0

Association between allergic sensitization and attention deficit hyperactivity disorder (ADHD).
Suwan P, Asian Pac J Allergy Immunol 2011:29:57–65
40 patients with ADHD.
40 controls.
SPTs to common allergens.
ADHD
67.5%
% subjects with (+) SPTs
45.0%
Controls
p=0.043
70 –
60 –
50 –
40 –
30 –
20 –
10 –
0
The most common sensitizing allergens
were D. farinae(42.5%),
D. pteronyssinus(40.0%), and
cockroach (35.0%)

Association between allergic sensitization and attention deficit hyperactivity disorder (ADHD).
Suwan P, Asian Pac J Allergy Immunol 2011:29:57–65
ADHD
30%
% subjects with (+) SPTs to Johnson grass
10%
Controls
p<0.0530 –
20 –
10 –
0
40 patients with ADHD.
40 controls.
SPTs to common allergens.
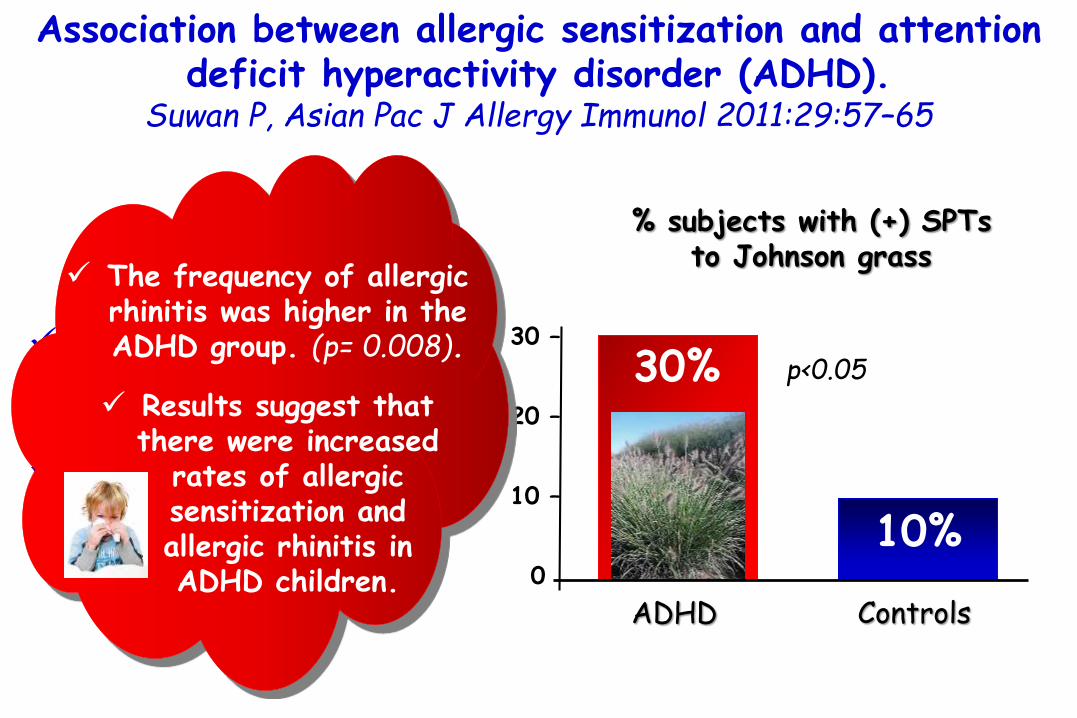
Association between allergic sensitization and attention deficit hyperactivity disorder (ADHD).
Suwan P, Asian Pac J Allergy Immunol 2011:29:57–65
ADHD
30%
% subjects with (+) SPTs to Johnson grass
10%
Controls
p<0.0530 –
20 –
10 –
0
40 patients with ADHD.
40 controls.
SPTs to common allergens.
The frequency of allergic rhinitis was higher in the ADHD group. (p= 0.008).
Results suggest that there were increased
rates of allergic sensitization and allergic rhinitis in ADHD children.
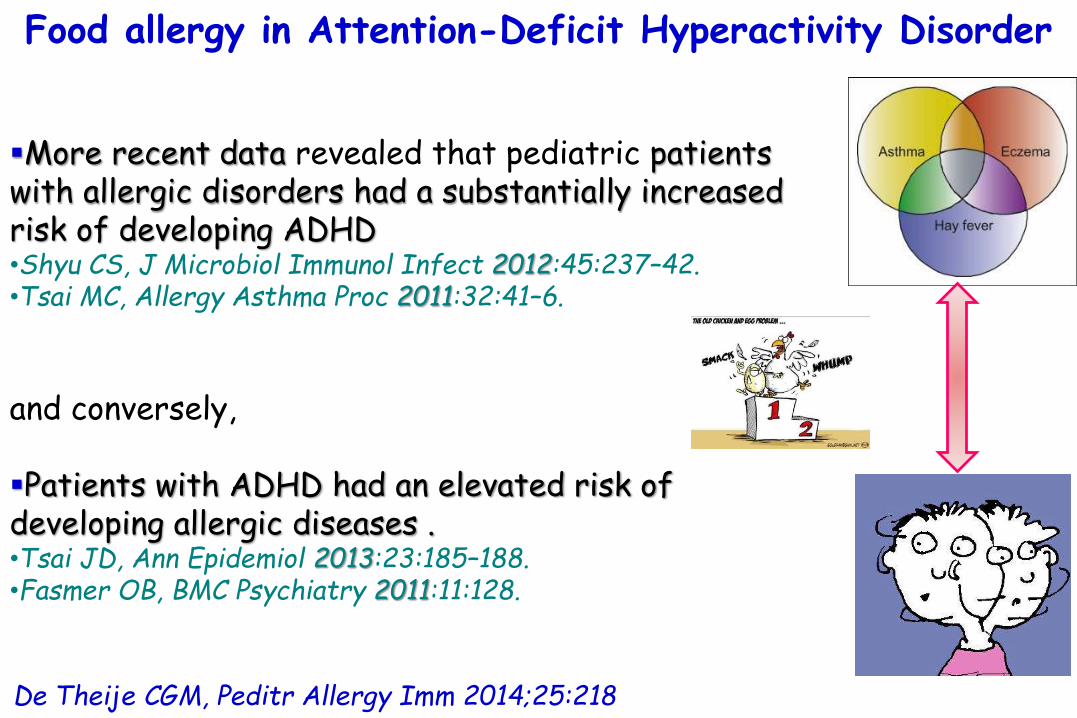
De Theije CGM, Peditr Allergy Imm 2014;25:218
Food allergy in Attention-Deficit Hyperactivity Disorder
More recent data revealed that pediatric patients with allergic disorders had a substantially increased risk of developing ADHD •Shyu CS, J Microbiol Immunol Infect 2012:45:237–42.•Tsai MC, Allergy Asthma Proc 2011:32:41–6.
and conversely,
Patients with ADHD had an elevated risk of developing allergic diseases .•Tsai JD, Ann Epidemiol 2013:23:185–188.•Fasmer OB, BMC Psychiatry 2011:11:128.

Prevalence of attention-deficit/hyperactivity disorder in patients with pediatric allergic disorders:
a nationwide, population-based study.Shyu CS, J Microbiol Immunol Infect 2012:45:237–42.
Allergicdisorders
21.5%
Prevalence rates of
226,550 pediatric patients < 18 yrs of age.
Prevalence (proportion of a population found to have a condition) ofallergic diseases and ADHD.
ADHD
25 –
20 –
15 –
10 –
5 –
000.6%

Prevalence of attention-deficit/hyperactivity disorder in patients with pediatric allergic disorders:
a nationwide, population-based study.Shyu CS, J Microbiol Immunol Infect 2012:45:237–42.
1.38
<6 6-11 12-17
1.86
2.5 –
2.0 –
1.5 –
1.0 –
0.5 –
0.0
2.16
AGE (YRS)
p=0.005 p<0.001 p<0.001
OR for ADHD in subjectswith allergic disorders
226,550 pediatric patients < 18 yrs of age.
Prevalence (proportion of a population found to have a condition) ofallergic diseases and ADHD.

Prevalence of attention-deficit/hyperactivity disorder in patients with pediatric allergic disorders:
a nationwide, population-based study.Shyu CS, J Microbiol Immunol Infect 2012:45:237–42.
1.38
<6 6-11 12-17
1.86
2.5 –
2.0 –
1.5 –
1.0 –
0.5 –
0.0
2.16
AGE (YRS)
p=0.005 p<0.001 p<0.001
OR for ADHD in subjectswith allergic disorders
226,550 pediatric patients < 18 yrs of age.
Prevalence (proportion of a population found to have a condition) ofallergic diseases and ADHD.
Bronchial asthma (BA) and allergic rhinitis (AR),
but not atopic dermatitis (AD), were risk factors for
ADHD.

Prevalence of attention deficit/hyperactivity disorder in pediatric allergic rhinitis: a nationwide population-based
study. Tsai MC, Allergy Asthma Proc 2011:32:41–6
226,550 pediatric patients <18 years old.
Prevalence of allergicdiseases and ADHD.
2.0
<6 6-11 12-17
1.9
2.5 –
2.0 –
1.5 –
1.0 –
0.5 –
0.0
2.2
AGE (YRS)
In subjects with allergic rhinitisOR for ADHD

Prevalence of attention deficit/hyperactivity disorder in pediatric allergic rhinitis: a nationwide population-based
study. Tsai MC, Allergy Asthma Proc 2011:32:41–6
226,550 pediatric patients <18 years old.
Prevalence of allergicdiseases and ADHD.
2.0
<6 6-11 12-17
1.9
2.5 –
2.0 –
1.5 –
1.0 –
0.5 –
0.0
2.2
AGE (YRS)
In subjects with allergic rhinitisOR for ADHD
Neither comorbidityof atopic dermatitis nor bronchial asthma carried high risk for
ADHD in AR patients.
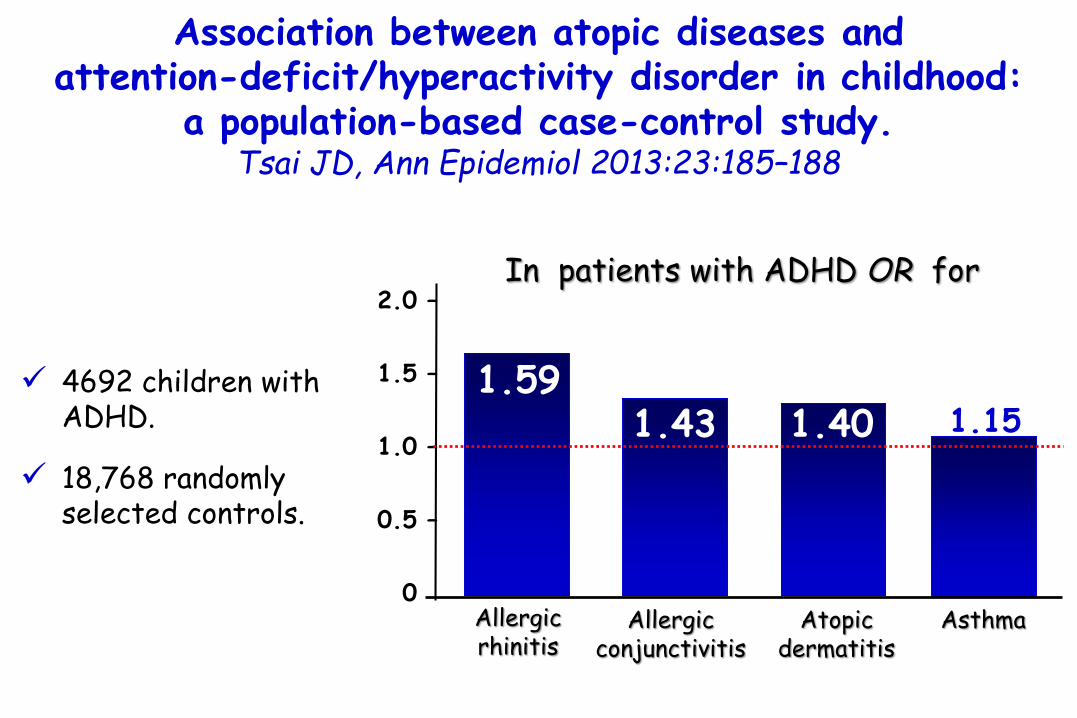
Association between atopic diseases and attention-deficit/hyperactivity disorder in childhood:
a population-based case-control study. Tsai JD, Ann Epidemiol 2013:23:185–188
4692 children with ADHD.
18,768 randomly selected controls.
1.59
Allergic rhinitis
2.0 –
1.5 –
1.0 –
0.5 –
0.0
In patients with ADHD OR for
1.43 1.151.40
Allergic conjunctivitis
Atopicdermatitis
Asthma

Association between atopic diseases and attention-deficit/hyperactivity disorder in childhood:
a population-based case-control study. Tsai JD, Ann Epidemiol 2013:23:185–188
4692 children with ADHD.
18,768 randomly selected controls. 1.0
3.0 –
2.5 –
2.0 –
1.5 –
1.0 –
0.5 –
0.0
OR for ADHD
1.63
2.79
2.25
0 1 2 ≥3
n° of allergic disease
p<001 for trend

Adult attention deficit hyperactivity disorder is associated with asthma. Fasmer OB, BMC Psychiatry 2011:11:128
Controls
24.4%
Prevalence of asthma
594 adult patients with ADHD.
719 persons from the general population.
ADHDpatient group
25 –
20 –
15 –
10 –
05 –
00
11.3%
OR =2.54
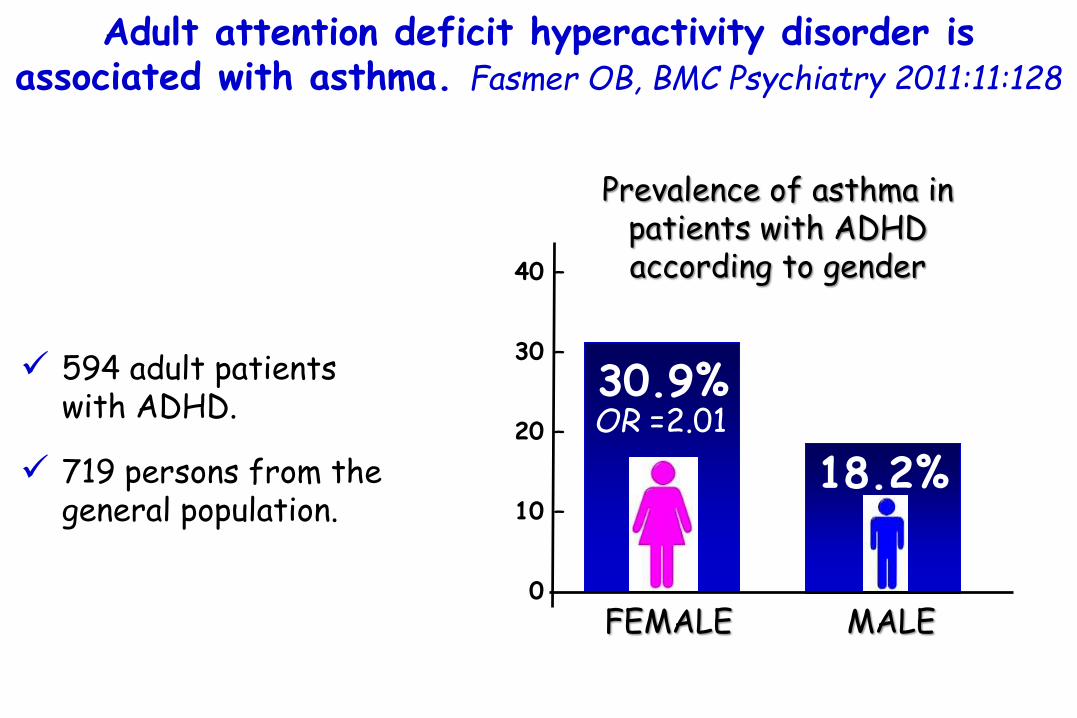
Adult attention deficit hyperactivity disorder is associated with asthma. Fasmer OB, BMC Psychiatry 2011:11:128
30.9%
Prevalence of asthma in patients with ADHD according to gender
594 adult patients with ADHD.
719 persons from the general population.
FEMALE MALE
40 –
30 –
20 –
10 –
00
18.2%OR =2.01

De Theije CGM, Peditr Allergy Imm 2014;25:218
Food allergy in Attention-Deficit Hyperactivity Disorder
More recent data revealed that pediatric patients with allergic disorders had a substantially increased risk of developing ADHD •Shyu CS, J Microbiol Immunol Infect 2012:45:237–42.•Tsai MC, Allergy Asthma Proc 2011:32:41–6.
and conversely,
Patients with ADHD had an elevated risk of developing allergic diseases .•Tsai JD, Ann Epidemiol 2013:23:185–188.•Fasmer OB, BMC Psychiatry 2011:11:128.
Research on atopic diseases in ADHD patients is predominately
focused on asthma, eczema, and rhinitis,
but findingsregarding food allergy
are limited.

a dietary intervention that:
1) Lowered IgG antibodies 2) was accompanied by
improvement in behavior
Case study: the effectiveness of a dietary supplement regimen in reducing IgG-mediated food sensitivity in
ADHD. Ritz BW, Altern Ther Health Med 2005:11:72–5.
a 7-year-old boy with ADHD and severe IgG-mediated foodallergy

Association between allergic sensitization and attention deficit hyperactivity disorder (ADHD).
Suwan P, Asian Pac J Allergy Immunol 2011:29:57–65
37.5%
% subjects with (+) SPTs to food allergens
40 patients with ADHD.
40 controls.
SPTs to common allergens.
40 –
30 –
20 –
10 –
00
25%
ControlsADHD
ns

Association between allergic sensitization and attention deficit hyperactivity disorder (ADHD).
Suwan P, Asian Pac J Allergy Immunol 2011:29:57–65
40 patients with ADHD.
40 controls.
SPTs to common allergens.

Association between allergic sensitization and attention deficit hyperactivity disorder (ADHD).
Suwan P, Asian Pac J Allergy Immunol 2011:29:57–65
37.5%
% subjects with (+) SPTs to food allergens
40 patients with ADHD.
40 controls.
SPTs to common allergens.
40 –
30 –
20 –
10 –
00
25%
ControlsADHD
nsA different
approach to test the importance of food allergens in ADHD children is a food challenge.

Recognition of food additives as a cause of symptoms of allergy. Feingold BF. Ann Allergy. 1968;26(6):309-13.
raising the whole issue of the relationship between food allergy and disturbances of
central nervous system function, e.g., ADHD
Feingold introduced the concept that food additives could be responsible for behavioral disturbances in children,
Chief of Allergy and Chairman of the Central Research Committee, Kaiser Foundation Hospitals of Northern California
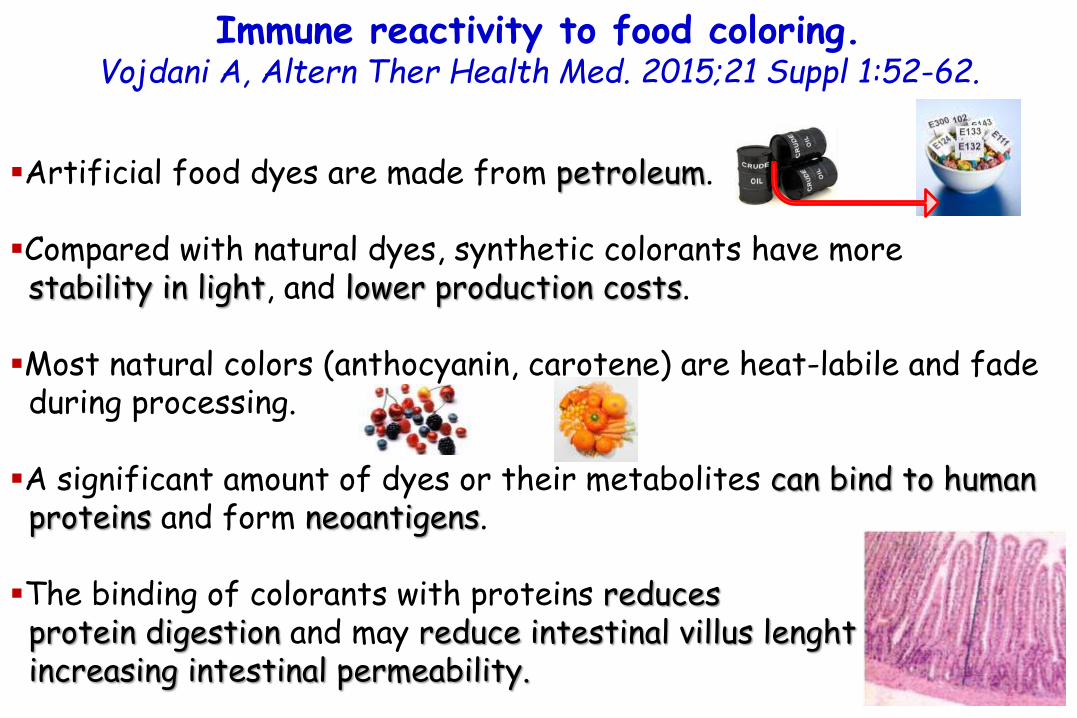
Immune reactivity to food coloring.Vojdani A, Altern Ther Health Med. 2015;21 Suppl 1:52-62.
Artificial food dyes are made from petroleum.
Compared with natural dyes, synthetic colorants have more stability in light, and lower production costs.
Most natural colors (anthocyanin, carotene) are heat-labile and fade during processing.
A significant amount of dyes or their metabolites can bind to human proteins and form neoantigens.
The binding of colorants with proteins reducesprotein digestion and may reduce intestinal villus lenghtincreasing intestinal permeability.

The effect of artificial food colors on childhood behavior. Pollock I, and Warner JO. Arch Dis Child 1990:65:74 –77.
The trial consisted of double blind placebo controlled challenges with artificial foodcolours:Tartrazine (E102) 50 mg, sunset yellow (EIIO) 25 mg,carmoisine (E122) 25 mg, amaranth (E123) 25 mg.
Food colours were effectively disguised in gelatin capsules.
One capsule was swallowed with breakfast throughout the 7 weeks of the trial.
39 children with parents’ report of improved behaviour on an artificial foodadditive free diet and deterioration with dietary lapses.
19 children completed a double blind placebo controlled challenge study with artificial food colours.
daily Conners' rating ofbehaviour > 15 = Hypereactivity

The effect of artificial food colors on childhood behavior. Pollock I, and Warner JO. Arch Dis Child 1990:65:74 –77.
39 children with parents’ report of improved behaviour on an artificial foodadditive free diet and deterioration with dietary lapses.
19 children completed a double blind placebo controlled challenge study with artificial food colours.
daily Conners' rating ofbehaviour > 15 = Hypereactivity
The mean daily Conners' behaviour score during the 14 active days and
21 or 28 placebo days.
P<0.01

The effect of artificial food colors on childhood behavior. Pollock I, and Warner JO. Arch Dis Child 1990:65:74 –77.
39 children with parents’ report of improved behaviour on an artificial foodadditive free diet and deterioration with dietary lapses.
19 children completed a double blind placebo controlled challenge study with artificial food colours.
daily Conners' rating ofbehaviour > 15 = Hypereactivity
The mean daily Conners' behaviour score during the 14 active days and
21 or 28 placebo days.
P<0.01
a daily intake of 125 mg of a mixture of 'artificial' food colourscan produce a measurable change in the behaviour scores of a group
of children.
We suggest that a pharmacological mechanism of food additive
intolerance is likely as many food additives can cause histamine
release from basophils.

The effects of a double blind placebo controlled artificial food colorings and benzoate preservatives challenge on
hyperactivity in a general population sample of pre-school children. Bateman B, and Warner JO, Arch Dis Child 2004:89:506–511.
1873 children were screened in their 4th
year for the presence of hyperactivity at baseline (HA), 1246 had SPTs to identify atopy (AT). Children were selected to form the following groups: HA/AT, not-HA/AT,HA/not-AT, and not-HA/not-AT
Following a diet eliminating artificial colourings and benzoate preservatives for one week; in the subsequent three week dietary challenge with a drink containing artificial colourings (20 mg daily) and sodium benzoate (45 mg daily) (active period), or placebo
1) significant reductions in hyperactive behaviour during the 1 week withdrawal phase.
2) significantly greater increases in hyperactive behaviour during the active than the placebo period based on parental reports.
These effects were not influenced by the presence or absence of
hyperactivity, nor by the presence or absence of atopy.

The effects of a double blind placebo controlled artificial food colorings and benzoate preservatives challenge on
hyperactivity in a general population sample of pre-school children. Bateman B, and Warner JO, Arch Dis Child 2004:89:506–511.
1873 children were screened in their 4th
year for the presence of hyperactivity at baseline (HA), 1246 had SPTs to identify atopy (AT). Children were selected to form the following groups: HA/AT, not-HA/AT,HA/not-AT, and not-HA/not-AT
Following a diet eliminating artificial colourings and benzoate preservatives for one week; in the subsequent three week dietary challenge with a drink containing artificial colourings (20 mg daily) and sodium benzoate (45 mg daily) (active period), or placebo
These effects were not influenced by the presence or absence of
hyperactivity, nor by the presence or absence of atopy.
The study clearly needs confirmation but the findings indicate that
potentially considerable public health benefits could be gained by the withdrawal
of these artificial food colorings and preservatives
from youngchildren’s diets.
1) significant reductions in hyperactive behaviour during the 1 week withdrawal phase.
2) significantly greater increases in hyperactive behaviour during the active than the placebo period based on parental reports.

The effects of a double blind placebo controlled artificial food colorings and benzoate preservatives challenge on
hyperactivity in a general population sample of pre-school children. Bateman B, and Warner JO, Arch Dis Child 2004:89:506–511.
1873 children were screened in their 4th
year for the presence of hyperactivity at baseline (HA), 1246 had SPTs to identify atopy (AT). Children were selected to form the following groups: HA/AT, not-HA/AT,HA/not-AT, and not-HA/not-AT
Following a diet eliminating artificial colourings and benzoate preservatives for one week; in the subsequent three week dietary challenge with a drink containing artificial colourings (20 mg daily) and sodium benzoate (45 mg daily) (active period), or placebo
There is a general adverse effect of artificial food colouring and benzoate preservatives on the behaviourof 3 year old children which is detectable by parents.
Subgroups are not made more vulnerable to this effect by their prior levels of hyperactivity or by atopy.

Synthetic food coloring and behavior: A dose response effect in a double blind placebo controlled repeated measures study. Rowe KS. J Pediatr 1994:125:691– 698.
200 children referred to the Royal Children's Hospital (Melbourne) for assessment of suspected hyperactivity
a 6-week open trial of a diet free of synthetic food coloring.
Placebo, or one of six dose levels of tartrazine (1, 2, 5, 10, 20, 50 mg), administered randomly each morning,
behavioral ratings recorded by parents at the end of each 24 hours.
80 –
70 –
60 –
50 –
40 –
30 –
20 –
10 –
0
75%
% children with behavioral improvement with the diet free
of synthetic food coloring

Synthetic food coloring and behavior: A dose response effect in a double blind placebo controlled repeated measures study. Rowe KS. J Pediatr 1994:125:691– 698.
200 children referred to the Royal Children's Hospital (Melbourne) for assessment of suspected hyperactivity
a 6-week open trial of a diet free of synthetic food coloring.
Placebo, or one of six dose levels of tartrazine (1, 2, 5, 10, 20, 50 mg), administered randomly each morning,
behavioral ratings recorded by parents at the end of each 24 hours.
80 –
70 –
60 –
50 –
40 –
30 –
20 –
10 –
0
44.5%
% children with a clear reaction after tartrazine challenge
A dose response effect was obtained.
With a dose increase > 10 mg, the duration of effect was
prolonged.

Food additives and hyperactive behaviour in 3-year-old and 8/9-year-old children in the community:
a randomised, double-blinded, placebo-controlled trial.McCann D, Lancet 2007; 370:1560–67.
153 (3-year-old)
144 (8/9-year-old children)
challenge drink containigsodium benzoate and one of 2 artificial food colour and additives (AFCA) mixes (A or B) or a placebo mix.
behaviours ratings by teachers and parentsa
computerised test of attention
Mix A for 3-year-old children included 20 mg of artificial food colourings(5 mg sunset yellow [E110], 2⋅5 mg carmoisine [E122], 7⋅5 mg tartrazine[E102], and 5 mg ponceau 4R [E124, Forrester Wood, Oldham, UK]) and 45 mg of sodium benzoate [E211, Sigma Aldridge, Gillingham, UK]).
Mix B included 30 mg of artificial food colourings (7⋅5 mg sunset yellow, 7⋅5 mgcarmoisine, 7⋅5 mg quinoline yellow [E110], and 7⋅5 mg allura red AC [E129]) and 45 mg of sodium benzoate.

Food additives and hyperactive behaviour in 3-year-old and 8/9-year-old children in the community:
a randomised, double-blinded, placebo-controlled trial.McCann D, Lancet 2007; 370:1560–67.
153 (3-year-old)
144 (8/9-year-old children)
challenge drink containigsodium benzoate and one of 2 artificial food colour and additives (AFCA) mixes (A or B) or a placebo mix.
behaviours ratings by teachers and parents
computerised test of attention
8/9-year-old children showed a significantly adverse effect on
global hyperactivity score when given mix A (p=0.023)
or mix B (p=0.001)
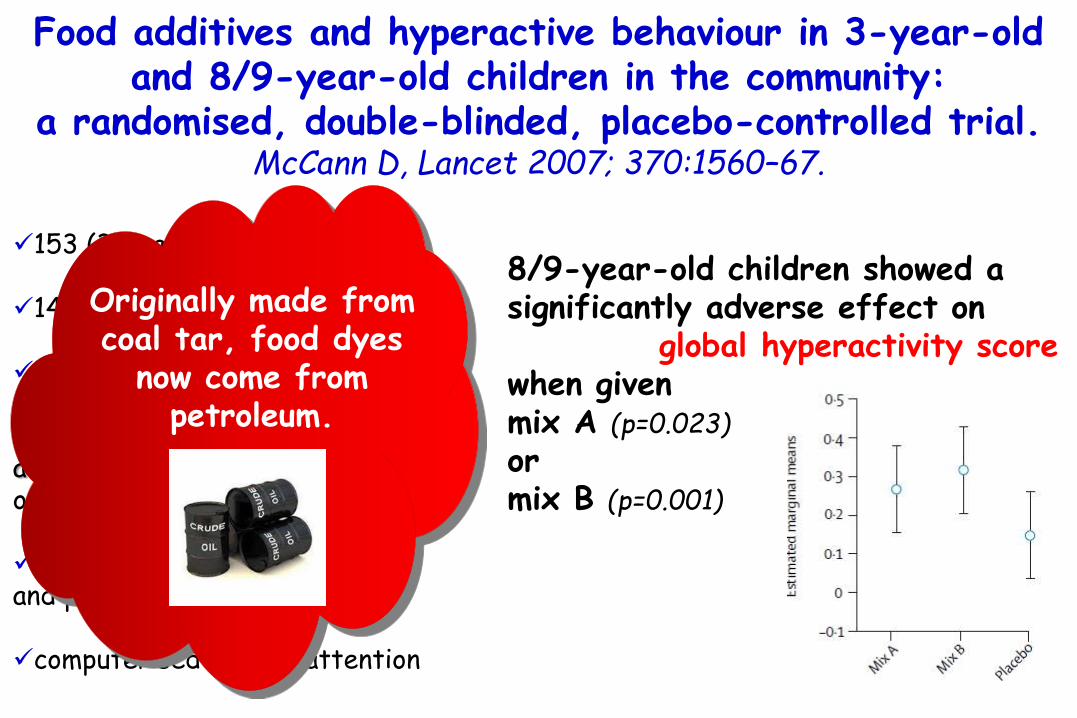
Food additives and hyperactive behaviour in 3-year-old and 8/9-year-old children in the community:
a randomised, double-blinded, placebo-controlled trial.McCann D, Lancet 2007; 370:1560–67.
153 (3-year-old)
144 (8/9-year-old children)
challenge drink containigsodium benzoate and one of 2 artificial food colour and additives (AFCA) mixes (A or B) or a placebo mix.
behaviours ratings by teachers and parents
computerised test of attention
8/9-year-old children showed a significantly adverse effect on
global hyperactivity score when given mix A (p=0.023)
or mix B (p=0.001)
Originally made from coal tar, food dyes
now come from petroleum.
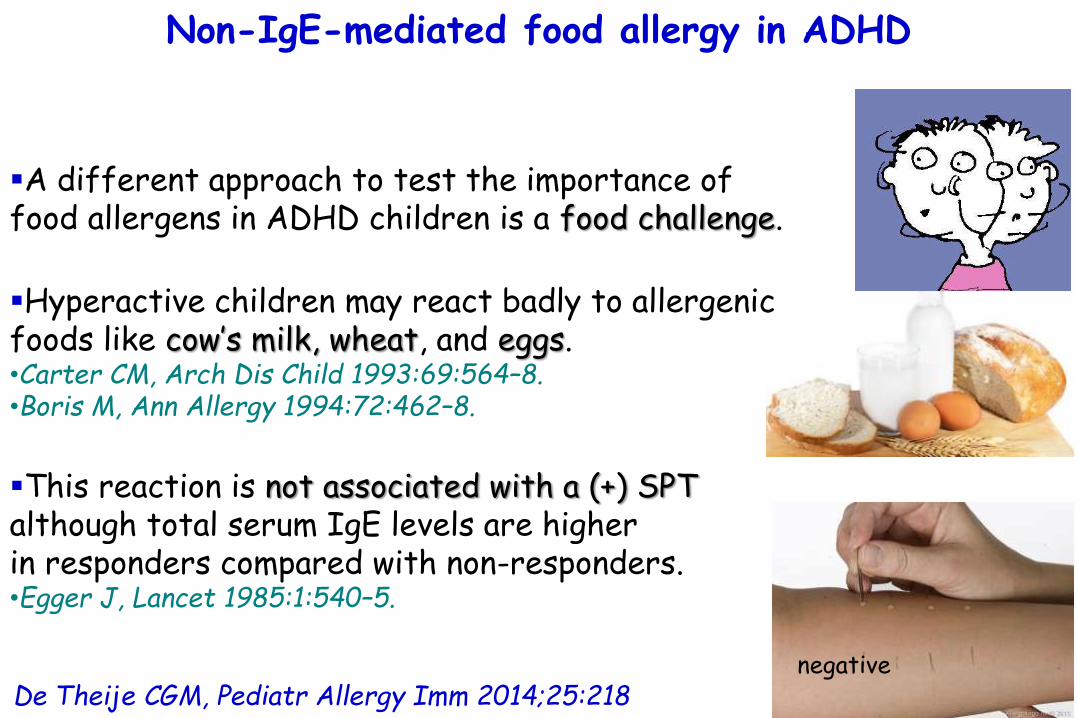
De Theije CGM, Pediatr Allergy Imm 2014;25:218
Non-IgE-mediated food allergy in ADHD
A different approach to test the importance of food allergens in ADHD children is a food challenge.
Hyperactive children may react badly to allergenic foods like cow’s milk, wheat, and eggs.•Carter CM, Arch Dis Child 1993:69:564–8.•Boris M, Ann Allergy 1994:72:462–8.
This reaction is not associated with a (+) SPT although total serum IgE levels are higher in responders compared with non-responders.•Egger J, Lancet 1985:1:540–5.
negative

ADHD as a (non) allergic hypersensitivity disorder: a hypothesis. Pelsser LM, Pediatr Allergy Immunol 2009:20:107–12.
ADHD may not be caused by the allergic response, but
ADHD may be a (non-) allergic hypersensitivity disorder itself.
Food-derived allergens trigger a hypersensitivity reaction that causes ADHD symptoms, possibly via an IgE or non-IgE allergicresponse or a non-allergic mechanism.

ADHD as a (non) allergic hypersensitivity disorder: a hypothesis. Pelsser LM, Pediatr Allergy Immunol 2009:20:107–12.
The underlying mechanisms of asthma,
eczema and ADHDcan be based on allergic
sensitization, resulting in immunoglobulin E (IgE) or
non-IgE-mediated mechanisms, or upon
nonallergicmechanisms.
Triggers and mechanisms of asthma, eczema and attention deficit hyperactivity disorder (ADHD) according to the old hypothesis (dashed arrow) and
the new hypothesis (solid arrow).

ADHD as a (non) allergic hypersensitivity disorder: a hypothesis. Pelsser LM, Pediatr Allergy Immunol 2009:20:107–12.
The underlying mechanisms of asthma,
eczema and ADHDcan be based on allergic
sensitization, resulting in immunoglobulin E (IgE) or
non-IgE-mediated mechanisms, or upon
nonallergicmechanisms.
Triggers and mechanisms of asthma, eczema and attention deficit hyperactivity disorder (ADHD) according to the old hypothesis (dashed arrow) and
the new hypothesis (solid arrow).
According to the hypothesis, ADHD can be subdivided in hypersensitive and non-hypersensitive ADHD, derived from different pathophysiologies.

ADHD as a (non) allergic hypersensitivity disorder: a hypothesis. Pelsser LM, Pediatr Allergy Immunol 2009:20:107–12.
The underlying mechanisms of asthma,
eczema and ADHDcan be based on allergic
sensitization, resulting in immunoglobulin E (IgE) or
non-IgE-mediated mechanisms, or upon
nonallergicmechanisms.
Triggers and mechanisms of asthma, eczema and attention deficit hyperactivity disorder (ADHD) according to the old hypothesis (dashed arrow) and
the new hypothesis (solid arrow).
This would provide opportunities for nutritional interventions or elimination diets for a subset of children with ADHD.
Food Allergy and the Brain
Attilio BonerUniversity ofVerona, Italy
Introduction
Micronutrients and Behaviour
Immunity & Ipersensitivity
Food Allergy&Ipersensitivity and Brain
Not only Food Allergy but also…
Which came first?
Possible Mechanisms
Food-based Therapies
Conclusions
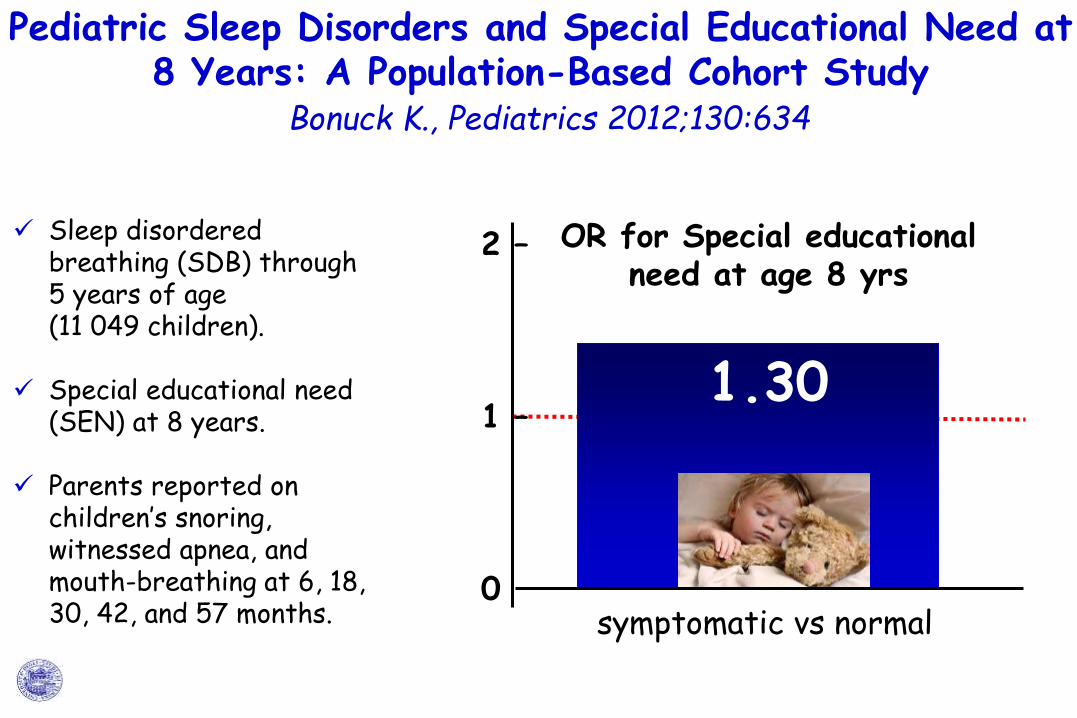
Pediatric Sleep Disorders and Special Educational Need at 8 Years: A Population-Based Cohort Study
Bonuck K., Pediatrics 2012;130:634
2 –
1 –
0
1.30
symptomatic vs normal
OR for Special educational need at age 8 yrs
Sleep disordered breathing (SDB) through 5 years of age (11 049 children).
Special educational need (SEN) at 8 years.
Parents reported on children’s snoring, witnessed apnea, and mouth-breathing at 6, 18, 30, 42, and 57 months.

Pediatric Sleep Disorders and Special Educational Need at 8 Years: A Population-Based Cohort Study
Bonuck K., Pediatrics 2012;130:634
2 –
1 –
0
1.38
6mo
1.311.43
18mo 30-57mo
Age of peak of symptoms
OR for Special educational need at age 8 yrs
Sleep disordered breathing (SDB) through 5 years of age (11 049 children).
Special educational need (SEN) at 8 years.
Parents reported on children’s snoring, witnessed apnea, and mouth-breathing at 6, 18, 30, 42, and 57 months.
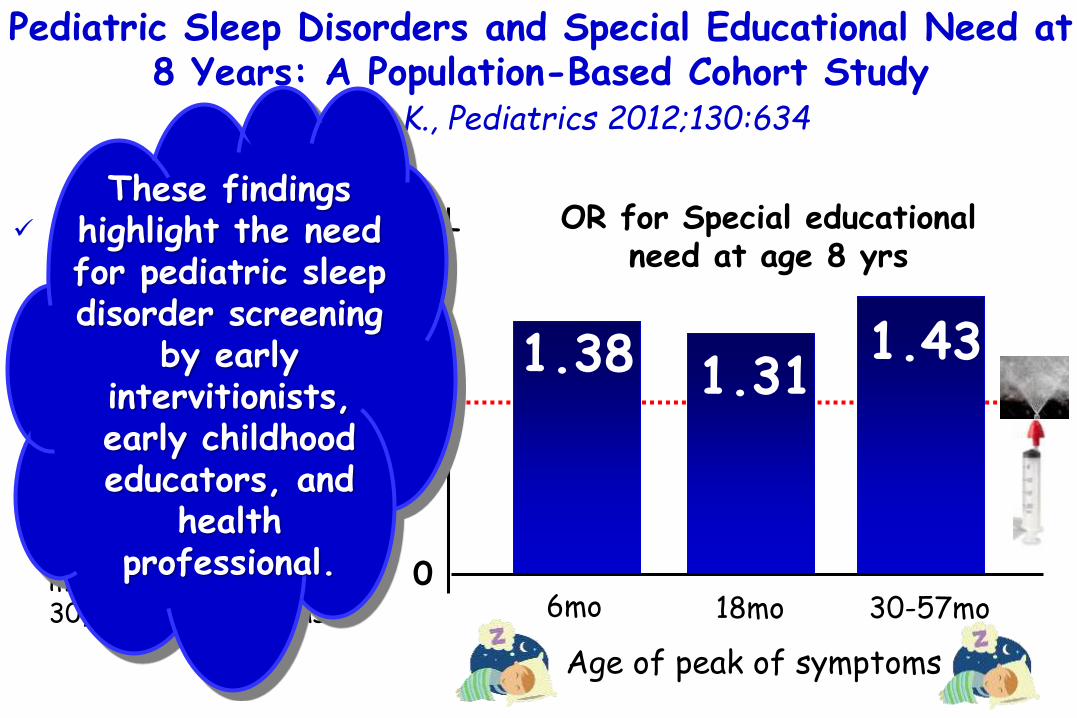
Sleep disordered breathing (SDB) through 5 years of age (11 049 children).
Special educational need (SEN) at 8 years.
Parents reported on children’s snoring, witnessed apnea, and mouth-breathing at 6, 18, 30, 42, and 57 months.
Pediatric Sleep Disorders and Special Educational Need at 8 Years: A Population-Based Cohort Study
Bonuck K., Pediatrics 2012;130:634
2 –
1 –
0
1.38
6mo
1.311.43
18mo 30-57mo
Age of peak of symptoms
OR for Special educational need at age 8 yrs
These findingshighlight the needfor pediatric sleepdisorder screening
by earlyintervitionists, early childhoodeducators, and
health professional.

Rhinitis as a risk factor for depressive mood in pre-adolescents: a new approach to this relationship
Audino P. Pediatr Allergy Immunol. 2014;25:360-5
40 –
20 –
0
% subjects with
Rhinitis
1283 subjectsaged 10–13 yrs
Questionnairerelevant tosocioeconomicstatus (HCI)
Test fordepression and anxiety
16.0%13.6%
7.7%
33.4%
Depressive mood
Anxious mood
Both depressive and anxious
mood
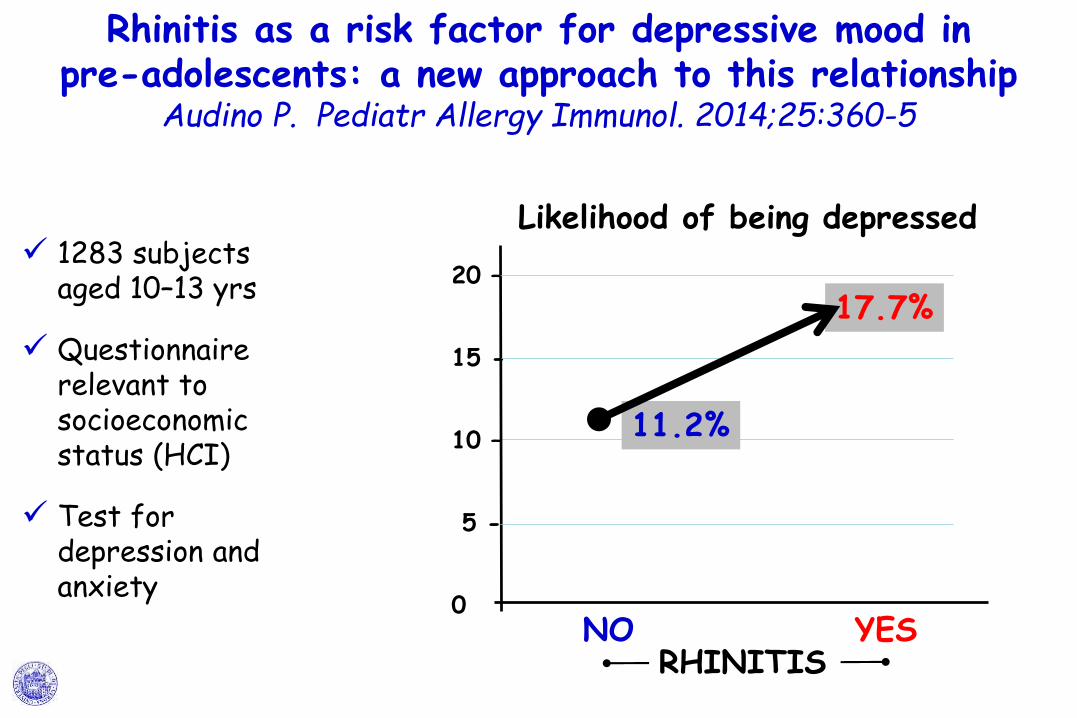
11.2%
17.7%20 –
15 -
10 –
5 -
0
Likelihood of being depressed
NO YESRHINITIS
Rhinitis as a risk factor for depressive mood in pre-adolescents: a new approach to this relationship
Audino P. Pediatr Allergy Immunol. 2014;25:360-5
1283 subjectsaged 10–13 yrs
Questionnairerelevant tosocioeconomicstatus (HCI)
Test fordepression and anxiety
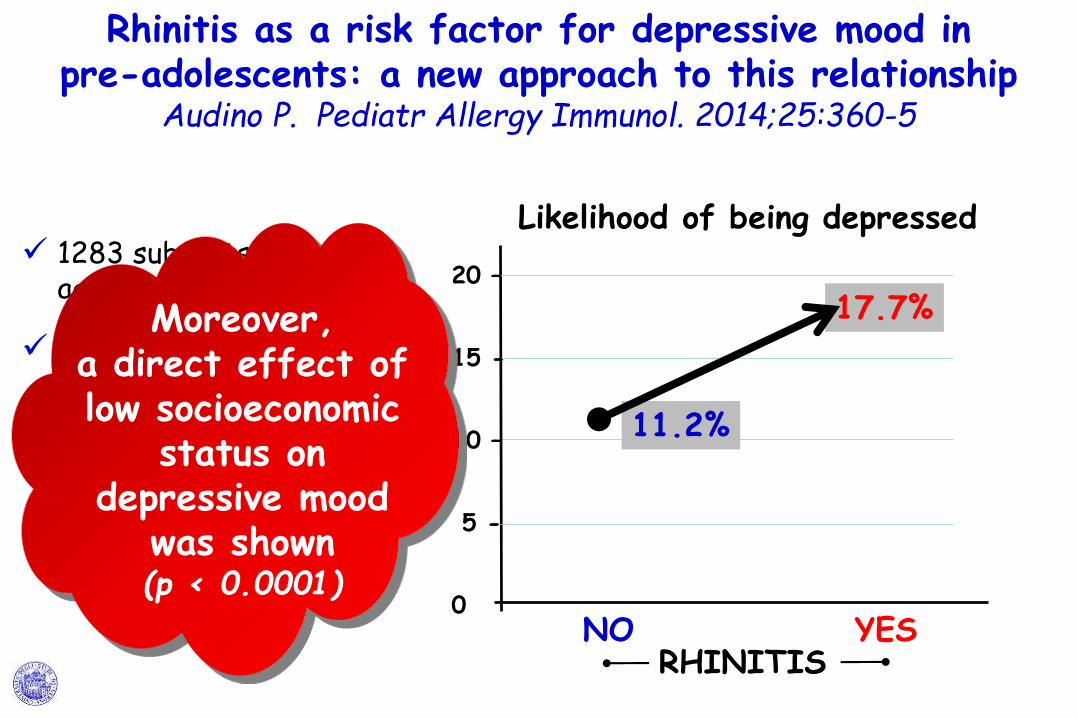
11.2%
17.7%20 –
15 -
10 –
5 -
0
Likelihood of being depressed
NO YESRHINITIS
Rhinitis as a risk factor for depressive mood in pre-adolescents: a new approach to this relationship
Audino P. Pediatr Allergy Immunol. 2014;25:360-5
1283 subjectsaged 10–13 yrs
Questionnairerelevant tosocioeconomicstatus (HCI)
Test fordepression and anxiety
Moreover, a direct effect of low socioeconomic
status on depressive mood
was shown(p < 0.0001)

Early wheezing phenotypes and cognitive developmentof 3-yr-olds. Community-recruited birth cohort
study Jedrychowski PAI 2010;21:550
Birth cohort.Wheezing symptoms over first two years.Cognitive status of children at the age of 3 yr with the Bayley Mental Development Index (MDI).
90 –
80 –
70 –
60 –
50 –
40 –
30 –
20 –
10 –
0
100 –
110 –
Persistent0-24 mo
Never Only in months 0-12
or 13-24
104.3101.6 97.5
WHEEZING
Mental Development Indexat age 3 yrs
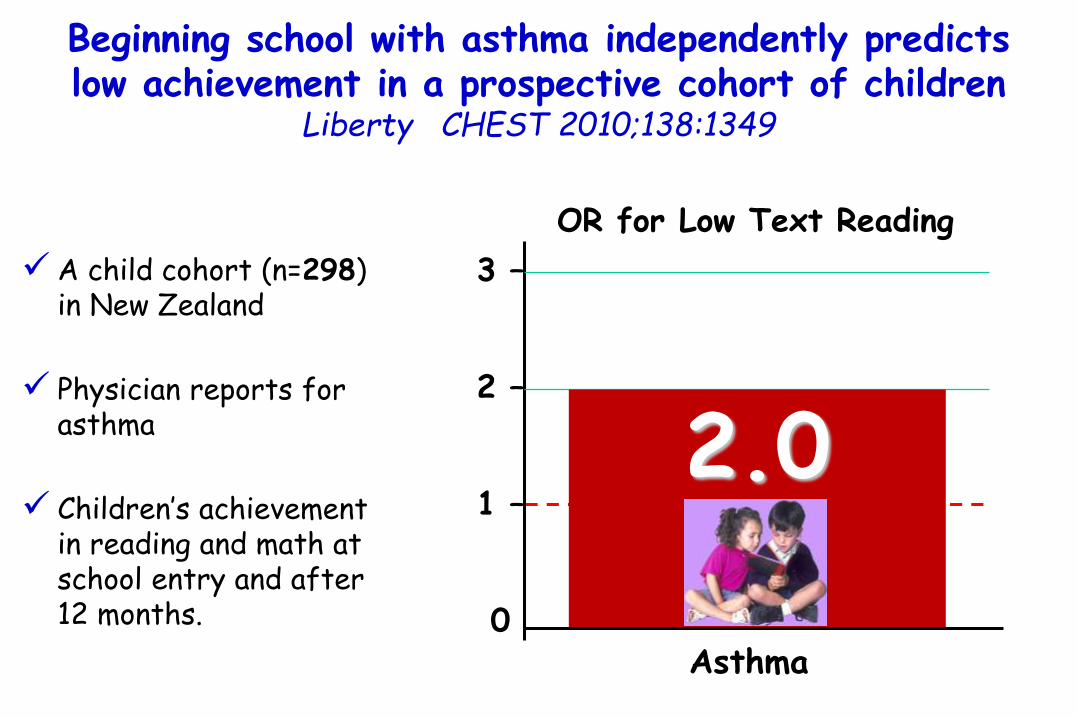
A child cohort (n=298) in New Zealand
Physician reports for asthma
Children’s achievement in reading and math at school entry and after 12 months.
OR for Low Text Reading
3 –
2 –
1 –
0
2.0
Asthma
Beginning school with asthma independently predicts low achievement in a prospective cohort of children
Liberty CHEST 2010;138:1349

A child cohort (n=298) in New Zealand
Physician reports for asthma
Children’s achievement in reading and math at school entry and after 12 months.
OR for Low Text Reading
3 –
2 –
1 –
0
2.0
Asthma
Beginning school with asthma independently predicts low achievement in a prospective cohort of children
Liberty CHEST 2010;138:1349
there is now good evidence that the immune system plays a critical role in the establishment
of synaptic networks in the developing brain, and that the
balance of cytokine levels in the hippocampus is important for
learning and memory. •Kettenmann H, Neuron 2013;77:10-8.•Aguzzi A, Science 2013;339:156-61.•Bilbo SD, Front Neuroendocrinol
2012;33:267-86.

Developmental and behavioral comorbidities of asthmain children. Blackman JA, J Dev Behav Pediatr 2007:28:92–9.
102,353 randomly selected children ages 0-17 years.
Associations between asthma and rates of developmental and behavioral problems.
1.82
Mild Moderate Severe
3.15
5.0 –
4.0 –
3.0 –
2.0 –
1.0 –
0.0
4.47
Asthma Severity
OR for depression/anxiety
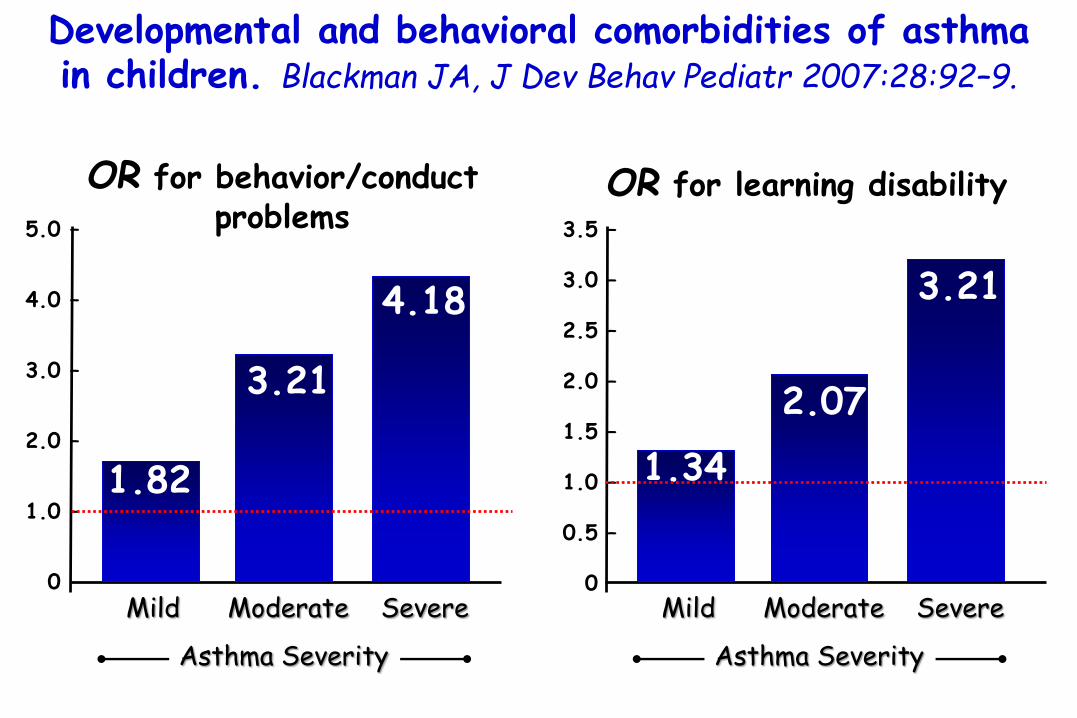
Developmental and behavioral comorbidities of asthmain children. Blackman JA, J Dev Behav Pediatr 2007:28:92–9.
1.82
Mild Moderate Severe
5.0 –
4.0 –
3.0 –
2.0 –
1.0 –
0.0
Asthma Severity
OR for behavior/conductproblems
3.21
4.18
1.34
Mild Moderate Severe
3.5 –
3.0 –
2.5 –
2.0 –
1.5 –
1.0 –
0.5 –
0.0
Asthma Severity
OR for learning disability
2.07
3.21

Developmental and behavioral comorbidities of asthmain children. Blackman JA, J Dev Behav Pediatr 2007:28:92–9.
102,353 randomly selected children ages 0-17 years.
Associations between asthma and rates of developmental and behavioral problems.
1.61
Mild Moderate Severe
2.45
3.0 –
2.5 –
2.0 –
1.5 –
1.0 –
0.5 –
0.0
2.93
Asthma Severity
OR for ADHD

Behavioral adjustment in children with asthma: a meta-analysis. McQuaid EL, J Dev Behav Pediatr 2001:22:430.
26 studies reflecting data on nearly 5,000 children with asthma (mean age = 8.4 years; 40% female).
Children with asthma have more behavioral difficulties than do healthy children, with the effect for internalizing behaviors being greater than that for externalizing behaviors (d(mn) = 0.73 vs 0.40).
>Comportamenti internalizzanti > comportamenti esternalizzanti

Behavioral adjustment in children with asthma: a meta-analysis. McQuaid EL, J Dev Behav Pediatr 2001:22:430.
26 studies reflecting data on nearly 5,000 children with asthma (mean age = 8.4 years; 40% female).
Increased asthma severity was
associated with greater behavioral
difficulties.
Children with asthma have more behavioral difficulties than do healthy children, with the effect for internalizing behaviors being greater than that for externalizing behaviors (d(mn) = 0.73 vs 0.40).
Comportamenti internalizzanti > comportamenti esternalizzanti
>

Changes over time in reducing developmental and behavioral comorbidities of asthma in children.
Blackman JA, J Dev Behav Pediatr 2012:33:24–31
Asthma rates remained stable between the 2 surveys,
but
there was a shift from moderate to mild and, to a lesser extent, severe asthma.
Rates of asthma, asthma severity, and developmental and behavioral problems among children with asthma
two surveys performed in 2003 and 2007 National Surveys of Children's Health.

Changes over time in reducing developmental and behavioral comorbidities of asthma in children.
Blackman JA, J Dev Behav Pediatr 2012:33:24–31
Comorbid rates of developmental and
behavioral problems were about 2x as high among children with
asthma compared with those without asthma.
Rates of asthma, asthma severity, and developmental and behavioral problems among children with asthma
two surveys performed in 2003 and 2007 National Surveys of Children's Health.

Rates of asthma, asthma severity, and developmental and behavioral problems among children with asthma
two surveys performed in 2003 and 2007 National Surveys of Children's Health.
Changes over time in reducing developmental and behavioral comorbidities of asthma in children.
Blackman JA, J Dev Behav Pediatr 2012:33:24–31
All problems increased for both groups between
the surveys but at a significantly greater pace
for repeated grades among children with
asthma.
Comorbid rates of developmental and
behavioral problems were about 2x as high among children with
asthma compared with those without asthma.

Rates of asthma, asthma severity, and developmental and behavioral problems among children with asthma
two surveys performed in 2003 and 2007 National Surveys of Children's Health.
Changes over time in reducing developmental and behavioral comorbidities of asthma in children.
Blackman JA, J Dev Behav Pediatr 2012:33:24–31
Children with asthma continue to have high rates of comorbiddevelopmental and
behavioral problems.
Comorbid rates of developmental and
behavioral problems were about 2x as high among children with
asthma compared with those without asthma.

Association between childhood asthma and ADHD symptoms in adolescence – a prospective
population-based twin study. Mogensen N, Allergy 2011;66:1224
4 –
3 –
2 –
1 –
00
3.2
OR for ≥3 symptoms ofhyperactivity–impulsivity
at age 13-14 years
2.73
Questionnaires at ages 8–9 and 13–14 yrs.(American Psychiatric Association. Diagnosticand statistical manual of mental disorders, 4th edn. Washington, DC: American PsychiatricAssociation; 1994.)
1480 Swedish twin pairs.
Association between asthma at age 8–9 and ADHD symptoms at age 13–14.
Children with asthma at age 8–9 years
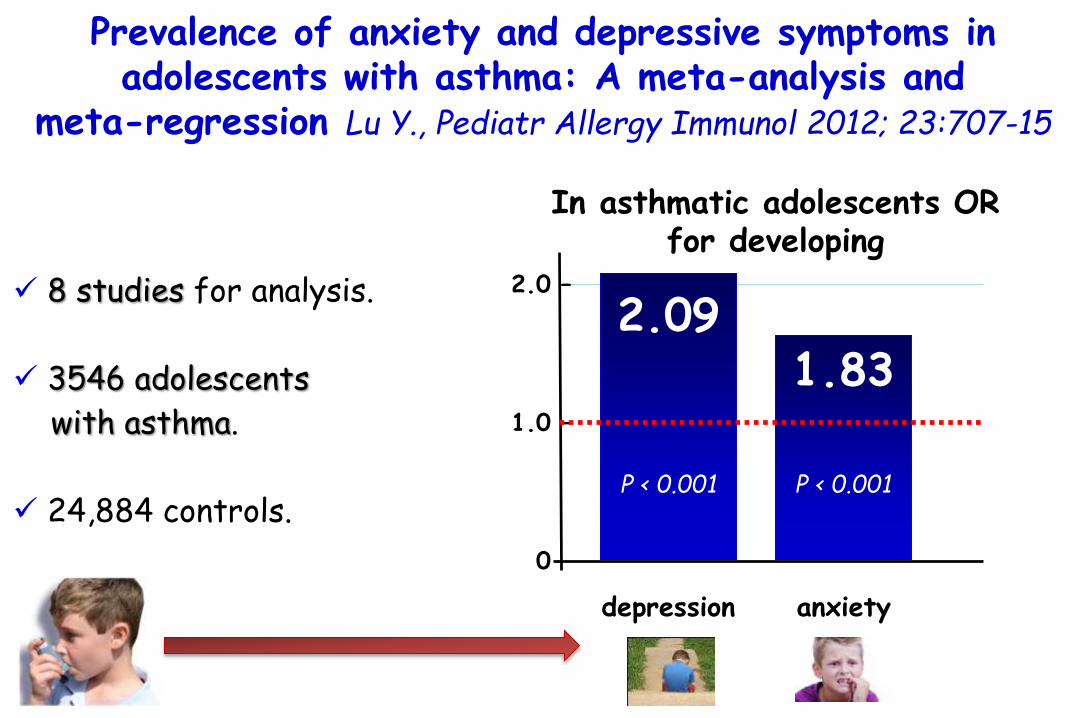
Prevalence of anxiety and depressive symptoms inadolescents with asthma: A meta-analysis and
meta-regression Lu Y., Pediatr Allergy Immunol 2012; 23:707-15
8 studies for analysis.
3546 adolescents
with asthma.
24,884 controls.
In asthmatic adolescents OR for developing
2.092.0 –
1.0 –
0.0
1.83
P < 0.001 P < 0.001
depression anxiety

Mental health comorbidity in patients with atopic dermatitis Yaghmaie P, JACI 2013;131:428-33
92642 noninstitutionalizedchildren aged 0 to 17 years.
Lifetime prevalence of provider-diagnosedmental health conditionsfor those with and withouta history of AD.
OR of having AttentionDeficit Hyperactivity
Disorder
1.87
In children with AD
2 –
1 –
0
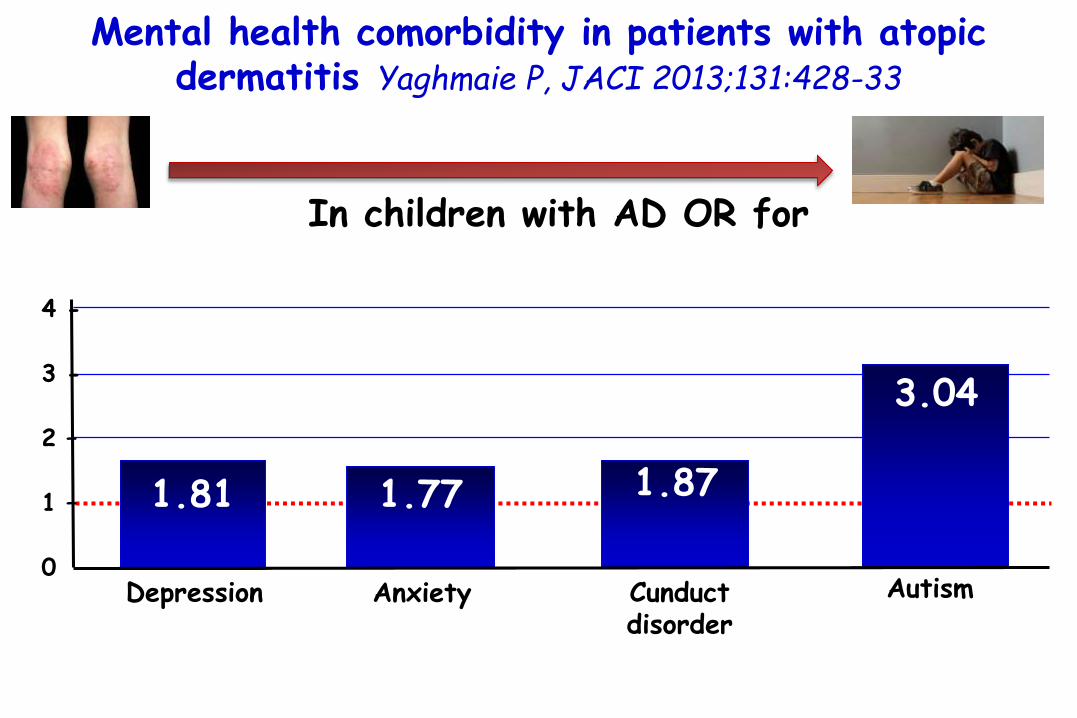
Mental health comorbidity in patients with atopic dermatitis Yaghmaie P, JACI 2013;131:428-33
1.81
Depression
1.87
3.04
1.77
Anxiety Cunductdisorder
Autism
4 -
3 -
2 –
1 –
0
In children with AD OR for

Mental health comorbidity in patients with atopic dermatitis Yaghmaie P, JACI 2013;131:428-33
1.81
Depression
1.87
3.04
1.77
Anxiety Cunductdisorder
Autism
4 -
3 -
2 –
1 –
0
In children with AD OR for
A clear dose-dependent relationshipwas observed between the prevalence of a mental health disorder and the reported
severity of the skin disease.
Mental health comorbidity in patients with atopic dermatitis Yaghmaie P, JACI 2013;131:428-33
1.81
Depression
1.87
3.04
1.77
Anxiety Cunductdisorder
Autism
4 -
3 -
2 –
1 –
0
In children with AD OR for
The mechanisms underlyingmental health disorders and AD are unknown.
1a.The sleep disturbance that accompanies AD might be one mechanism by which children with
AD could theoretically be predisposed to concomitant
mental health conditions.

Mental health comorbidity in patients with atopic dermatitis Yaghmaie P, JACI 2013;131:428-33
1.81
Depression
1.87
3.04
1.77
Anxiety Cunductdisorder
Autism
4 -
3 -
2 –
1 –
0
In children with AD OR for
1b Disrupted sleep patterns have well-knownnegative effects on the mental state of
children, including effects on behavior, schoolfunctioning, attention, and mood.

Mental health comorbidity in patients with atopic dermatitis Yaghmaie P, JACI 2013;131:428-33
1.81
Depression
1.87
3.04
1.77
Anxiety Cunductdisorder
Autism
4 -
3 -
2 –
1 –
0
In children with AD OR for
2.Another theoretical mechanismexplaining the association between mentalhealth and AD could be the wide-ranging
effects of inflammation.AD and mental conditions might result,in part, from shared disturbances in
inflammatory pathways.

Prevalence of at least 1 allergic disease
30 –
25 –
20 –
15 –
10 –
0
Association between childhood allergic disease, psychological comorbidity, and injury requiring medical
attention Garg Ann Allergy 2014;112:525
Data from the 2007 to 2008 National Survey of Children’s Health.
27,556 children ≤ 5 years old.
29.4%• 6.6% with
asthma,
• 15.0% with eczema,
• 11.6% with hay fever,
• 6.1% with food allergy.

In children with allergic disorders OR for7 –
6 –
5 –
4 –
3 –
2 –
1 –
0
2.93
4.75
6.035.54
2.972.49
1.89
at least 1 comorbid
psychiatric and behavioral
disorder
ADHD depression anxiety conduct/ oppositional
defiantdisorder
learningdelay
autism/ Asperger disorder
Association between childhood allergic disease, psychological comorbidity, and injury requiring medical
attention Garg Ann Allergy 2014;112:525

In children with allergic disorders OR for7 –
6 –
5 –
4 –
3 –
2 –
1 –
0
2.93
4.75
6.035.54
2.972.49
1.89
at least 1 comorbid
psychiatric and behavioral
disorder
ADHD depression anxiety conduct/ oppositional
defiantdisorder
learningdelay
autism/ Asperger disorder
Association between childhood allergic disease, psychological comorbidity, and injury requiring medical
attention Garg Ann Allergy 2014;112:525
Children with at least 1 allergic disorder had higher odds of sustaining injuries
even after controlling for comorbid psychiatric disorders.

A. The association between allergic and psychiatric disorders, including ADHD, conduct disorder, depression, and anxiety, has recently been increasingly recognized.
B. Multiple mechanisms underlying this association have been proposed, including sleep deprivation and chronic inflammation.
Yaghmaie J Allergy Clin Immunol 2013;131:428Chang Allergy Asthma Immunol Res 2013;5:315Slattery J Allergy Clin Immunol 2011;128:668
Chen J Child Psychol Psychiatry. 2013;54:1208Slattery J Psychiatr Res. 2011;45:788
Infante J Clin Psychiatry. 2007;68:1419
Association between childhood allergic disease, psychological comorbidity, and injury requiring medical
attention Garg Ann Allergy 2014;112:525

C. Sleep disturbances accompanying allergic disorders may predispose to psychiatric disorders and strengthen the association between allergic disorders and mental healthconditions.
D. Yaghmaie et al suggested that the association between allergic and psychiatric disorders is secondary to the wide-ranging effects of inflammation, because eczema, depression, and anxiety are characterized by an increase in proinflammatory cytokines.
Slattery J Allergy Clin Immunol 2011;128:668Romanos J Epidemiol Community Health 2010;64:269
Yaghmaie J Allergy Clin Immunol 2013;131:428
Association between childhood allergic disease, psychological comorbidity, and injury requiring medical
attention Garg Ann Allergy 2014;112:525

C. Sleep disturbances accompanying allergic disorders may predispose to psychiatric disorders and strengthen the association between allergic disorders and mental healthconditions.
D. Yaghmaie et al suggested that the association between allergic and psychiatric disorders is secondary to the wide-ranging effects of inflammation, because eczema, depression, and anxiety are characterized by an increase in proinflammatory cytokines.
Slattery J Allergy Clin Immunol 2011;128:668Romanos J Epidemiol Community Health 2010;64:269
Yaghmaie J Allergy Clin Immunol 2013;131:428
Together, these studies show that the association between
allergic and psychiatric diseaseis multifactorial.
Association between childhood allergic disease, psychological comorbidity, and injury requiring medical
attention Garg Ann Allergy 2014;112:525

Allergic disease in the first year of life is associated with differences in subsequent neurodevelopment and
behaviour. Meldrum SJ, Early Hum Dev 2012:88:567–73.
Relationship between early allergic disease and sensitisation at 12 mo. of age and neurodevelopmentaloutcomes at 18 months.
Infants with a maternal history of allergic disease (n=324).
Children with any diagnosed allergic disease at 12 months had evidence of reduced motor scores (p = 0.016), and this was most apparent for a diagnosis of eczema (p = 0.007).
(-)
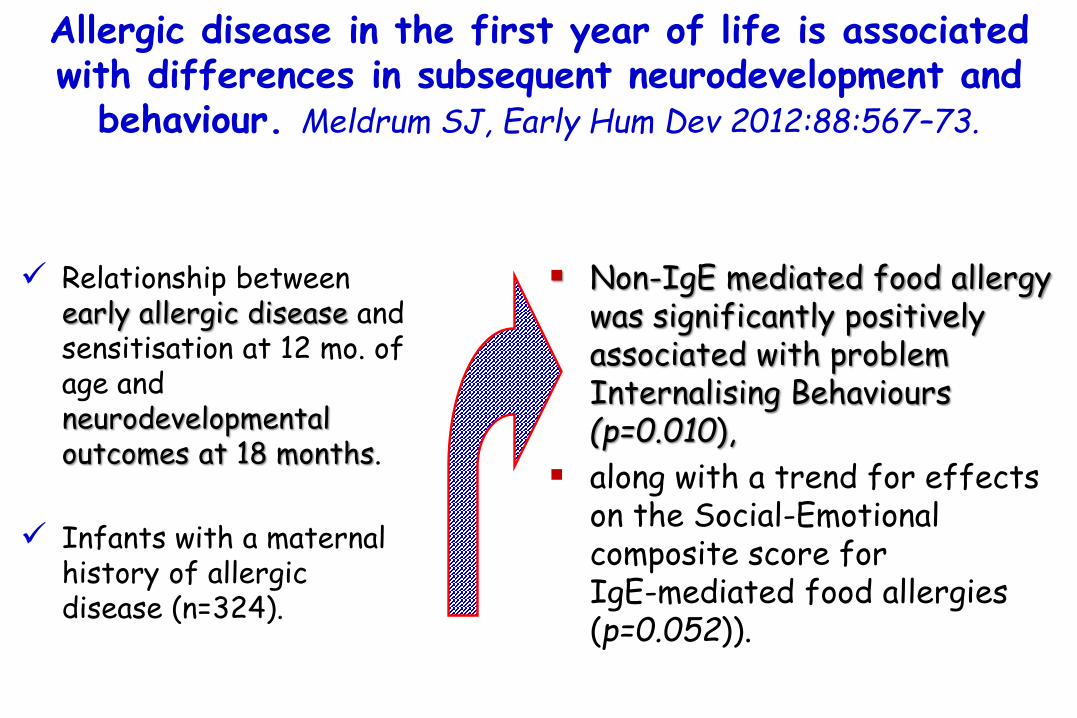
Allergic disease in the first year of life is associated with differences in subsequent neurodevelopment and
behaviour. Meldrum SJ, Early Hum Dev 2012:88:567–73.
Non-IgE mediated food allergy was significantly positively associated with problem Internalising Behaviours(p=0.010),
along with a trend for effects on the Social-Emotional composite score for IgE-mediated food allergies (p=0.052)).
Relationship between early allergic disease and sensitisation at 12 mo. of age and neurodevelopmentaloutcomes at 18 months.
Infants with a maternal history of allergic disease (n=324).

Allergic disease in the first year of life is associated with differences in subsequent neurodevelopment and
behaviour. Meldrum SJ, Early Hum Dev 2012:88:567–73.
Relationship between early allergic disease and sensitisation at 12 mo. of age and neurodevelopmentaloutcomes at 18 months.
Infants with a maternal history of allergic disease (n=324).
This study provides evidence that an allergic phenotype
in infancy is associated with effects on
neurodevelopment.
Non-IgE mediated food allergy was significantly positively associated with problem Internalising Behaviours(p=0.010),
along with a trend for effects on the Social-Emotional composite score for IgE-mediated food allergies (p=0.052)).

Allergic disease in the first year of life is associated with differences in subsequent neurodevelopment and
behaviour. Meldrum SJ, Early Hum Dev 2012:88:567–73.
lower social emotional scoresand internalizing behaviors.
lower behavioral outcomes Children suffering from allergic diseases in the 1st year of life
allergic diseases during infancy predict later neurodevelopmental scores
children with eczema in the 1st year of life
poorer gross motor skills
food allergy in the 1st year of life

Allergic disease in the first year of life is associated with differences in subsequent neurodevelopment and
behaviour. Meldrum SJ, Early Hum Dev 2012:88:567–73.
lower social emotional scoresand internalizing behaviors.
lower behavioral outcomes Children suffering from allergic diseases in the 1st year of life
allergic diseases during infancy predict later neurodevelopmental scores
children with eczema in the 1st year of life
poorer gross motor skills
food allergy in the 1st year of life
Internalizing behaviors are negative, problematic behaviors that are directed toward the self.
People with internalizing behaviors have difficulty coping with negative emotions or stressful situations, so they direct their
feelings inward:
Social withdrawalFeelings of loneliness or guilt
Unexplained physical symptoms, i.e., headaches and stomach aches, not due to a medical conditionNot talking to or interacting with others
Food Allergy and the Brain
Attilio BonerUniversity ofVerona, Italy
Introduction
Micronutrients and Behaviour
Immunity & Ipersensitivity
Food Allergy&Ipersensitivity and Brain
Not only Food Allergy but also…
Which came first?
Possible Mechanisms
Food-based Therapies
Conclusions

Brain and Food Allergywhich came first?
acute and chronic stress exposures
in early life inrat models
1) increases epithelial permeability in the rat intestine,
2) shifts the intestinal mucosa toward a more inflammatory state towords TH-2 that have long-lasting effects,
3) reduce the number of lactobacilli and bifidobacteria in the intestinal microbiota,
Stress and food allergy: mechanistic considerations.Schreier HM, Wright RJ, Ann Allergy Asthma Immunol. 2014;112:296-301

Neonatal maternal deprivation triggers long termalterations in colonic epithelial barrier and mucosal
immunity in rats. Barreau F, Gut. 2004;53:501–506.
Male Wistar rat pups wereseparated during postnatal days2-14 or left undisturbed with theirdam.
At 12 weeks of age, colonicparacellular permeability, bacterialtranslocation, myeloperoxidase(MPO) activity, mucosal mast celldensity, IL-1 β, IL-2, IL-4, IL-10, and IFN-γ mRNA expression, and macroscopic damage.
maternal separationafter birth is associated
with increased colonic permeability
>

Neonatal maternal deprivation triggers long termalterations in colonic epithelial barrier and mucosal
immunity in rats. Barreau F, Gut. 2004;53:501–506.
Effect of neonatal stress (maternal separation) on total gut (A) and colonic (B)
paracellular permeability in 12 week old rats.
Effect of neonatal stress on colonic myeloperoxidase (MPO) activity (A) and
mucosal mast cell number (B) in 12 week old rats.
total gut colon PMN PMN

Neonatal maternal deprivation triggers long termalterations in colonic epithelial barrier and mucosal
immunity in rats. Barreau F, Gut. 2004;53:501–506.
Effect of neonatal stress (maternal separation) on total gut (A) and colonic (B)
paracellular permeability in 12 week old rats.
Effect of neonatal stress on colonic myeloperoxidase (MPO) activity (A) and
mucosal mast cell number (B) in 12 week old rats.
total gut colon PMN PMN
In animal models exposure to psychosocial stressors may increase the transepithelial passage of food antigens into
the intestinal mucosa, thereby increasing the risk of adverse reactions to these foods.

Brain and Food Allergywhich came first?
acute and chronic stress exposures
in early life inrat models
1) increases epithelial permeability in the rat intestine,
2) shifts the intestinal mucosa toward a more inflammatory state towords TH-2 that have long-lasting effects,
3) reduce the number of lactobacilli and bifidobacteria in the intestinal microbiota,
4) no information on microbioma are avalable.
Stress and food allergy: mechanistic considerations.Schreier HM, Wright RJ, Ann Allergy Asthma Immunol. 2014;112:296-301

A bidirectional relationship between psychosocial factorsand atopic disorders: a systematic review and
meta-analysis. Chida Y, Psychosom Med 2008:70:102–16
34 studies evaluated the effect of psychosocial factors on atopic disorders.
9 studies evaluated the effect of atopic disorders on mental health.
The overall meta-analysis exhibited
a positive association between:
1) psychosocial factors
and future atopic disorder (r= 0.024; p < 0.001)
2) atopic disorders
and future poor mental health (r = 0.044; p < 0.001).
1
1
2
2
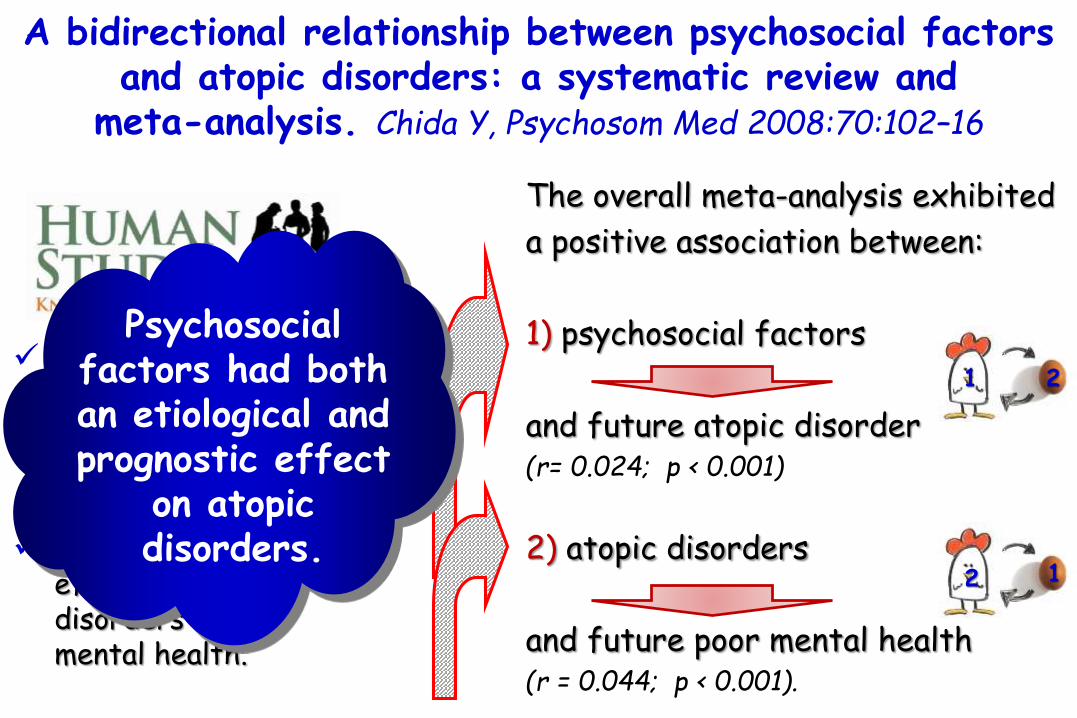
A bidirectional relationship between psychosocial factorsand atopic disorders: a systematic review and
meta-analysis. Chida Y, Psychosom Med 2008:70:102–16
34 studies evaluated the effect of psychosocial factors on atopic disorders.
9 studies evaluated the effect of atopic disorders on mental health.
The overall meta-analysis exhibited
a positive association between:
1) psychosocial factors
and future atopic disorder (r= 0.024; p < 0.001)
2) atopic disorders
and future poor mental health (r = 0.044; p < 0.001).
1
1
Psychosocial factors had both an etiological and prognostic effect
on atopic disorders.
2
2

Food Allergy and the Brain
Attilio BonerUniversity ofVerona, Italy
Introduction
Micronutrients and Behaviour
Immunity & Ipersensitivity
Food Allergy&Ipersensitivity and Brain
Not only Food Allergy but also…
Which came first?
Possible Mechanisms
Food-based Therapies
Conclusions

Atopic disease as a risk factor for ADHD possible explanations. Schmitt J, Allergy 2010:65: 1506–24.
Children with atopic eczema are exposed to increased levels of proinflammatory cytokines and during early infancy.
Inflammatory cytokines released during the atopic response may pass the blood brain barrier and activate neuroimmune mechanisms that involve behaviorally and emotionally relevant circuits.
The prefrontal cortex is known to subserve executive cognitive functions such as planned behavior, decision making, motivation and attention.
Structural and functional alterations in prefrontal cortex regions have been linked to various cognitive disturbances including ADHD symptomatology.
1° explanation
2° explanation
Eczema is associated early in infancy with high levels of psychological stress that may include dysfunctional mother-child relationship, sleep disturbances, less bodily contact,as well as later stigmatization and bullying by the peer group.
Studies in animals and humans clearly suggest that during early life the brain is particularly sensitive to stress probably because of its profound developing changes during this period.
Animal data show that adverse rearing behavior during infancy lead to increased fear behavior, an exaggerated startle response (a defensive response to sudden or threatening stimuli) or changes in prefrontal cortex regions.
Atopic disease as a risk factor for ADHD possible explanations. Schmitt J, Allergy 2010:65: 1506–24.

3° explanation
Sleep disturbances are common in the eczematous child and sleep is vital for the brain development.
Night waking and sleeplessness during early infancy are correlated with difficult temperament, higher irritability and lower approachability in childhood.
Increased stress exposure, i.e. adverse parenting or malfunctioning sleep patterns, during early infancy may affect neurotransmitter and neuroendocrine systems leading to long-term alterations of the behavioral and physiological repertoire in children with eczema increasing their vulnerability to psychopathological conditions, such as ADHD.
Atopic disease as a risk factor for ADHD possible explanations. Schmitt J, Allergy 2010:65: 1506–24.

It is possible that both prenatal and postnatal allergic immune activation regulates complex, but critical, neuroimmuneinteractions and therefore affects neurodevelopment and brain function.
Together with a genetic pre-disposition and multiple environmental factors, these effects of allergic immune activation might contribute to the development of Autism Spectrum Disorders and ADHD
Development of the brain from 25 days to 9 months
of fetal life
Multifactorial etiology of neurodevelopmental disorders.
De Theije CGM, Peditr Allergy Imm 2014;25:218
(+)
≈

Multifactorial etiology of neurodevelopmental disorders.
De Theije CGM, Peditr Allergy Imm 2014;25:218
In additionmaternal immune activation can causeepigenetic changes
deficits inneurodevelopment
ASP and ADHD

Multifactorial etiology of neurodevelopmental disorders.
De Theije CGM, Peditr Allergy Imm 2014;25:218
Maternal allergic immune reactions might enhance such epigenetic changes.
Furthermore, also during postnatal development, (food) allergic immune activation is thought to affect brainfunction via neuroimmune interactions that affect the enteric nervous system and central nervous system.
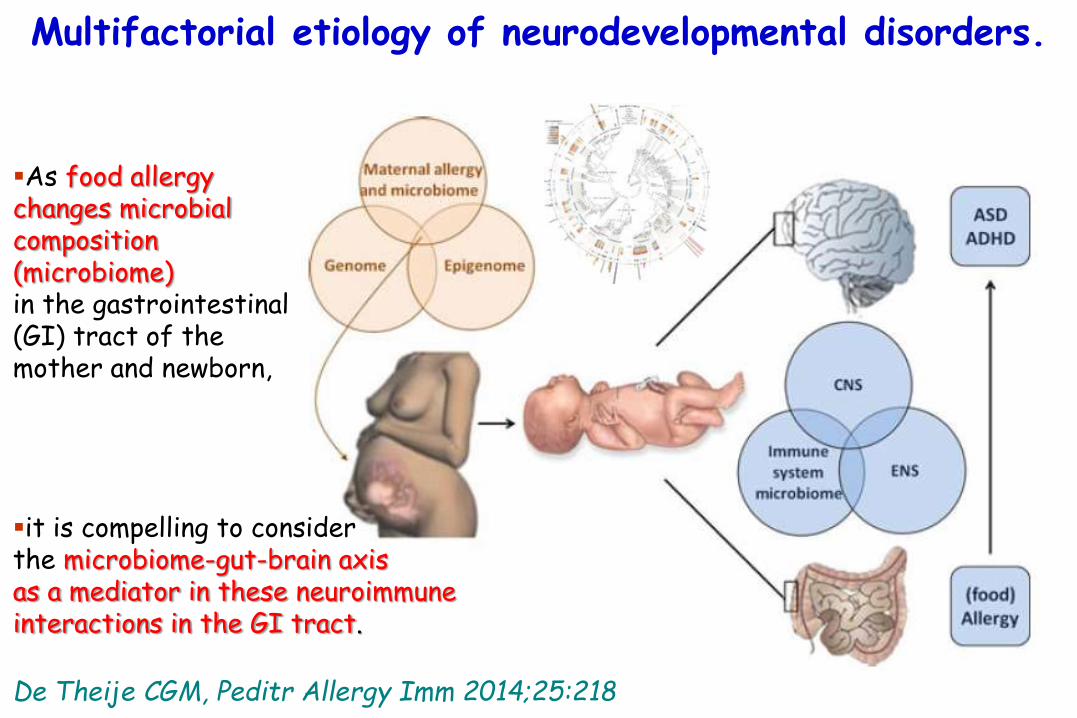
Multifactorial etiology of neurodevelopmental disorders.
De Theije CGM, Peditr Allergy Imm 2014;25:218
As food allergy changes microbialcomposition (microbiome) in the gastrointestinal (GI) tract of the mother and newborn,
it is compelling to consider the microbiome-gut-brain axisas a mediator in these neuroimmuneinteractions in the GI tract.
The gut microbiota influences blood–brain barrierpermeability in mice.
Braniste V. Sci. Transl. Med. 2014;6(263):263ra158.
Pivotal to brain development and function is an intact blood-brain barrier (BBB), which acts as a gatekeeper to control the passage and exchange of molecules and nutrients between the circulatory system and the brain parenchyma.
The BBB also ensures homeostasis of the central nervous system (CNS).
Germ-free mice, beginning with intrauterine life, displayed increased BBB permeability compared to pathogen-free mice with a normal gut flora.
The increased BBB permeability was maintained in germ-free mice after birth and during adulthood and was associated with reduced expression of the tight junction proteins occludin and claudin-5, which are known to regulate barrier function in endothelial tissues. Exposure of germ-free adult mice to a pathogen-free gut microbiota decreased BBB permeability and up-regulated the expression of tight junction proteins. Our results suggest that gut microbiota-BBB communication is initiated during gestation and propagated throughout life.

The gut microbiota influences blood–brain barrierpermeability in mice.
Braniste V. Sci. Transl. Med. 2014;6(263):263ra158.
Pivotal to brain development and function is an intact blood-brain barrier (BBB), which acts as a gatekeeper to control the passage and exchange of molecules and nutrients between the circulatory system and the brain parenchyma.
The BBB also ensures homeostasis of the central nervous system (CNS).
Germ-free mice, beginning with intrauterine life, displayed increased BBB permeability compared to pathogen-free mice with a normal gut flora.
The increased BBB permeability was maintained in germ-free mice after birth and during adulthood and was associated with reduced expression of the tight junction proteins occludin and claudin-5, which are known to regulate barrier function in endothelial tissues. Exposure of germ-free adult mice to a pathogen-free gut microbiota decreased BBB permeability and up-regulated the expression of tight junction proteins. Our results suggest that gut microbiota-BBB communication is initiated during gestation and propagated throughout life.
Germ-free mice

Mechanisms: Maternal factors
Maternal allergic response affects the immune system of thedeveloping fetus in utero.
Chronic maternal stress affects behavioral and cognitive functions later in life, Talge NM, J Child Psychol Psychiatry 2007:48:245–61.
Buitelaar JK, Neurobiol Aging 2003:24 (Suppl. 1):S53–60
Maternal infection during pregnancy is a significant risk factor for the development schizophrenia in offspring.
Brown AS, Schizophr Bull 2011:37:284–90.
Maternal viral infection in the first trimester and bacterial infection in the second trimester were found to increase the risk of ASD in the offspring. Atladottir HO, J Autism Dev Disord 2010:40:1423–30.
Mechanisms: Maternal factors
Maternal allergic response affects the immune system of thedeveloping fetus in utero.
Chronic maternal stress affects behavioral and cognitive functions later in life, Talge NM, J Child Psychol Psychiatry 2007:48:245–61.
Buitelaar JK, Neurobiol Aging 2003:24 (Suppl. 1):S53–60
Maternal infection during pregnancy is a significant risk factor for the development schizophrenia in offspring.
Brown AS, Schizophr Bull 2011:37:284–90.
Maternal viral infection in the first trimester and bacterial infection in the second trimester were found to increase the risk of ASD in the offspring. Atladottir HO, J Autism Dev Disord 2010:40:1423–30.
In addition, animals prenatally exposed to infections display features relevant to autism in humans, suggesting
a causal link between maternal immune activation and autistic behavior.
Schwartzer JJ, Transl Psychiatry 2013:3:e240.

Antenatal maternal stress and long-term effects on child neurodevelopment: how and why?
Talge NM, J Child Psychol Psychiatry 2007:48:245–61
Several prospective studies.
1) If a mother is stressed while pregnant, her child is substantially more likely to have emotional or cognitive problems, including an increased risk of attentionaldeficit/hyperactivity, anxiety, and language delay.
2) These findings are independent of effects due to maternal postnatal depression and anxiety.
3) The attributable load of emotional/behavioral problems due to antenatal stress and/or anxiety is approximately 15%.

Antenatal maternal stress and long-term effects on child neurodevelopment: how and why?
Talge NM, J Child Psychol Psychiatry 2007:48:245–61
Under stimulatory conditions neurons of the hypothalamus secrete corticotropin releasing hormone (CRH).
In the anterior pituitary, CRH induces production of adrenocorticotropin (ACTH), to stimulate release of glucocorticoids from the adrenal cortex .
Elevated serum glucocorticoids provide the physiologic milieu required for an adaptive stress response, but also immediately begin to interact with corticoid receptors to inhibit the stress response via negative feedback.
Antenatal maternal stress and long-term effects on child neurodevelopment: how and why?
Talge NM, J Child Psychol Psychiatry 2007:48:245–61
Under stimulatory conditions neurons of the hypothalamus secrete corticotropin releasing hormone (CRH).
In the anterior pituitary, CRH induces production of adrenocorticotropin (ACTH), to stimulate release of glucocorticoids from the adrenal cortex .
Elevated serum glucocorticoids provide the physiologic milieu required for an adaptive stress response, but also immediately begin to interact with corticoid receptors to inhibit the stress response via negative feedback.
Deleterious consequences of chronic exposure to stress or high levels of
glucocorticoids are well characterized, including structural damage to key brain
regions such as the hippocampus.

Antenatal maternal stress and long-term effects on child neurodevelopment: how and why?
Talge NM, J Child Psychol Psychiatry 2007:48:245–61
A model to show how antenatal stress may affect the function of the HPA axis, by a reduction in glucocorticoid receptors in the hippocampus, causing reduced negative feedback.

Prenatal stress and cognitive development and temperament in infants.
Buitelaar JK, Neurobiol Aging 2003: 24 (Suppl. 1):S53–60.
Self-report data about daily hassles and pregnancy-specific anxiety.
Salivary cortisol levels collected in nulliparouspregnant women.
Bayley Scales of Infant Development and on temperamental questionnaires at 3 and 8 months.
Psychomotor developmental scores infants at 3 and 8 mo. whose mother had salivary cortisol levels in the upper quartile and in the bottom quartile in late pregnancy.
*
*

Prenatal stress and cognitive development and temperament in infants.
Buitelaar JK, Neurobiol Aging 2003: 24 (Suppl. 1):S53–60.
Self-report data about daily hassles and pregnancy-specific anxiety.
Salivary cortisol levels collected in nulliparouspregnant women.
Bayley Scales of Infant Development and on temperamental questionnaires at 3 and 8 months.
Psychomotor developmental scores infants at 3 and 8 mo. whose mother had salivary cortisol levels in the upper quartile and in the bottom quartile in late pregnancy.
*
*
chronic exposure to stress or high levels of glucocorticoids
structural damage to key brain regions such as the
hippocampus.
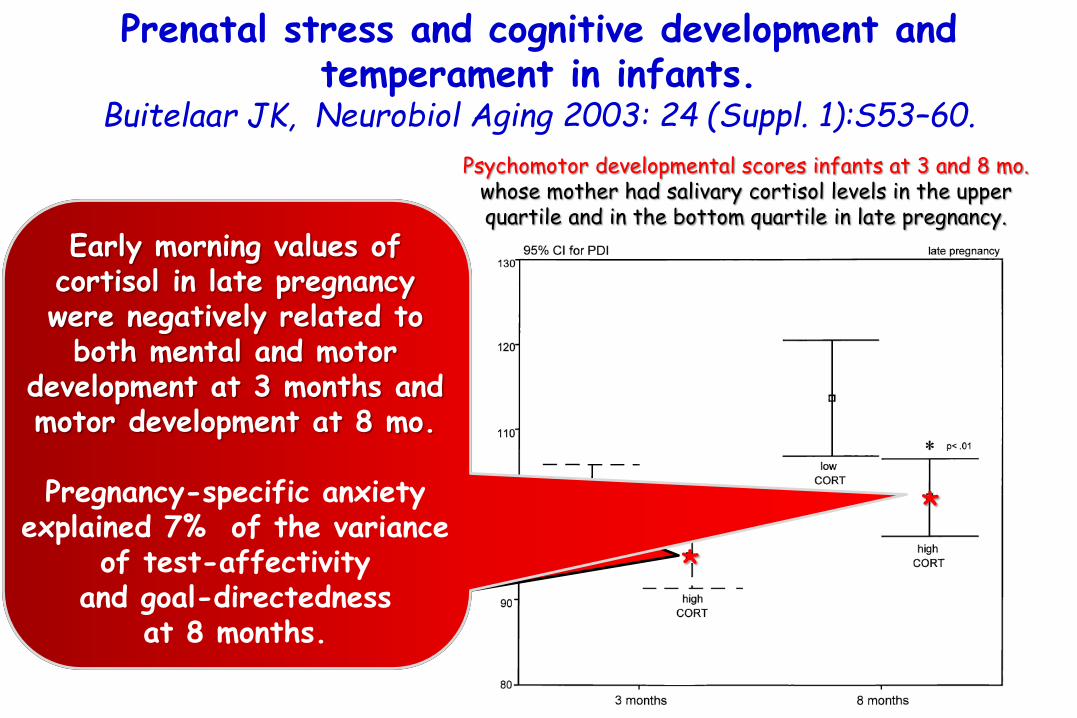
Prenatal stress and cognitive development and temperament in infants.
Buitelaar JK, Neurobiol Aging 2003: 24 (Suppl. 1):S53–60.
Self-report data about daily hassles and pregnancy-specific anxiety.
Salivary cortisol levels collected in nulliparouspregnant women.
Bayley Scales of Infant Development and on temperamental questionnaires at 3 and 8 months.
Psychomotor developmental scores infants at 3 and 8 mo. whose mother had salivary cortisol levels in the upper quartile and in the bottom quartile in late pregnancy.
*
*
Early morning values of cortisol in late pregnancy were negatively related to
both mental and motor development at 3 months and motor development at 8 mo.
Pregnancy-specific anxiety explained 7% of the variance
of test-affectivity and goal-directedness
at 8 months.

Maternal infection and schizophrenia: implications for prevention. Brown AS, Schizophr Bull 2011:37:284–90.
Accumulating evidence suggests that maternal infection is a risk factor for schizophrenia. Prospective epidemiological studies indicate that maternal influenza, toxoplasmosis, and genital/reproductive infection are associated with this disorder in offspring. Preclinical models of maternal immune activation have supported the neurobiological plausibility of these microbes in schizophrenia.
Previous studies suggest that treatment or prophylactic efforts targeting these and other infections could have significant effects on reducing the incidence of schizophrenia, given that they are common in the population and the effect sizes derived from epidemiological studies of these and other microbial pathogens and schizophrenia, to date, are not small.

Maternal infection requiring hospitalization duringpregnancy and autism spectrum disorders.
Atladottir HO, J Autism Dev Disord 2010:40:1423–30
2.98
HR of ASDs in the offspring
Admission to hospital due to maternal viral infection in
the first trimester
3.0 –
2.5 –
2.0 –
1.5 –
1.0 –
0.5 –
0.0
1.42
All children born in Denmark from 1980, through 2005.
Diagnoses of autism spectrum disorders (ASDs) and maternal infection obtained through nationwide registers. Maternal bacterial
infection in the second trimester
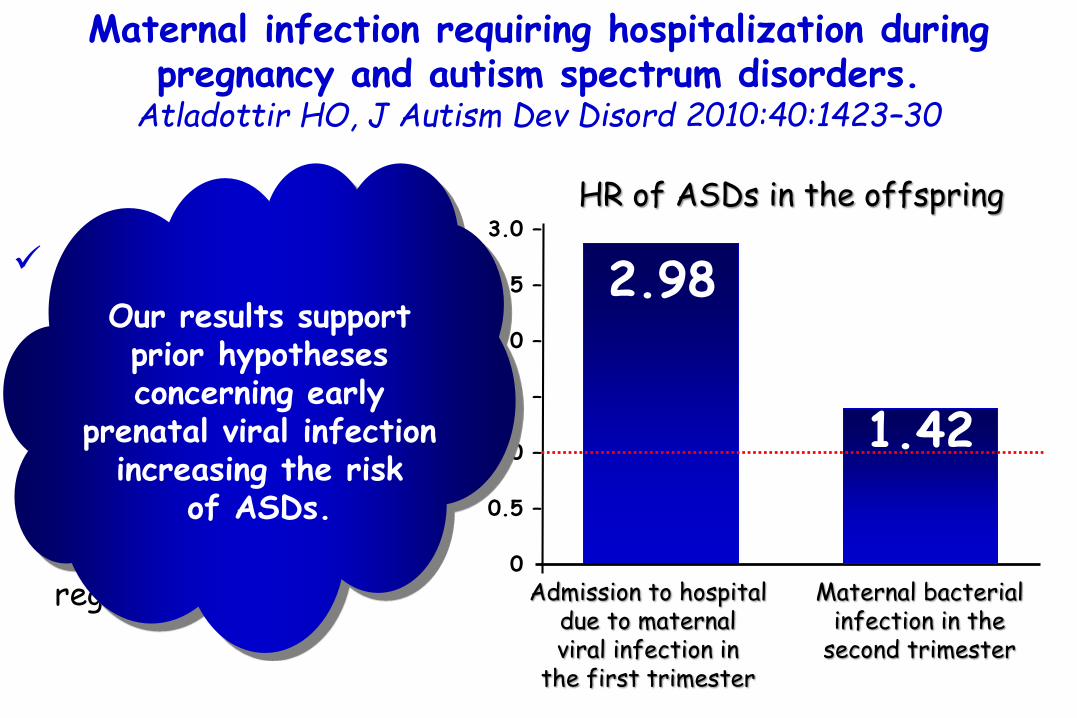
Maternal infection requiring hospitalization duringpregnancy and autism spectrum disorders.
Atladottir HO, J Autism Dev Disord 2010:40:1423–30
2.98
HR of ASDs in the offspring
Admission to hospital due to maternal viral infection in
the first trimester
3.0 –
2.5 –
2.0 –
1.5 –
1.0 –
0.5 –
0.0
1.42
All children born in Denmark from 1980, through 2005.
Diagnoses of autism spectrum disorders (ASDs) and maternal infection obtained through nationwide registers. Maternal bacterial
infection in the second trimester
Our results support prior hypotheses concerning early
prenatal viral infection increasing the risk
of ASDs.

Maternal immune activation and strain specific interactions in the development of autism-like behaviors
in mice. Schwartzer JJ, Transl Psychiatry 2013:3:e240
1) It is becoming increasingly apparent that the causes of autism spectrum disorders (ASD) are due to both genetic and environmental factors.
2) Animal studies have demonstrated a link between maternal immune activation and the expression of ASD-like behaviors.
3) It is hypothesized that the severity of effects of maternal immune activation on ASD-like phenotypes is influenced by the genetic background in mice.
4) To test this, pregnant dams of two inbred strains (that is, C57BL/6J and BTBR T(+)tf/J) were exposed to the viral mimic polyinosinic-polycytidylic acid (polyI:C), and their offspring were tested for the presence and severity of ASD-like behaviors.

5) To identify differences in immune system regulation, spleens were processed and measured for alterations in induced cytokine responses.
6) Strain-treatment interactions were observed in social approach, ultrasonic vocalization, repetitive grooming and marble burying behaviors.
7) Interestingly, persistent dysregulation of adaptive immune system function was only observed in BTBR mice.
8) behavioral and immunological effects of maternal immune activation are strain-dependent in mice.
Maternal immune activation and strain specific interactions in the development of autism-like behaviors
in mice. Schwartzer JJ, Transl Psychiatry 2013:3:e240

Mechanisms: Maternal Factors
Viral rashes during pregnancy increased the risk of developing ADHDin the offspring. Arpino C, Eur J Paediatr Neurol 2005:9:363–5.
Maternal allergies are also implicated to put the offspring at risk of developing ASD. In a large study population, a greater than 2X elevated risk of ASD was observed for maternal asthma and allergy diagnosed during the second trimester, but not for maternal autoimmune diseases. Croen LA, Arch Pediatr Adolesc Med 2005:159:151–7.
Mothers with mastocytosis during pregnancy, characterized by increased number of mast cells in many organs, had a higher risk of delivering a child with ASD.Theoharides TC. Int J Immunopathol Pharmacol 2009:22:859–65.

Exanthematic diseases during pregnancy and attention-deficit/hyperactivity disorder (ADHD).
Arpino C, Eur J Paediatr Neurol 2005:9:363–5
A case-control study conducted to evaluate risk factors for ADHD.
The viral rash during pregnancy(i.e. measles, varicella, or rubella) was reported by 4 of 71 mothers of children with ADHD and none of the 118 controls' mothers (p<0.01).

Exanthematic diseases during pregnancy and attention-deficit/hyperactivity disorder (ADHD).
Arpino C, Eur J Paediatr Neurol 2005:9:363–5
A case-control study conducted to evaluate risk factors for ADHD.
The viral rash during pregnancy(i.e. measles, varicella, or rubella) was reported by 4 of 71 mothers of children with ADHD and none of the 118 controls' mothers (p<0.01).
High rate of viraldisease found among ADHD cases' mothers
suggest a role for viral diseases
occurring during pregnancy in the
development of ADHD.

Maternal autoimmune diseases, asthma and allergies, and childhood autism spectrum disorders: a case-control study. Croen LA, Arch Pediatr Adolesc Med 2005:159:151–7.
2.9
Psoriasis Asthma Eczema
3.0 –
2.5 –
2.0 –
1.5 –
1.0 –
0.5 –0.
0
maternal
OR for autism spectrumdisorder (ASD) in children
1.6 1.8
A case-control study of infants born between January 1995 and June 1999.
Cases (n = 420) werechildren with at least1 diagnosis of an autismspectrum disorder (ASD)
Controls (n = 2100) werechildren without an ASD diagnosis.
Frequencies of maternalimmunologic disorders.
IL-6

Maternal autoimmune diseases, asthma and allergies, and childhood autism spectrum disorders: a case-control study. Croen LA, Arch Pediatr Adolesc Med 2005:159:151–7.
2.93.0 –
2.5 –
2.0 –
1.5 –
1.0 –
0.5 –0.
0
OR for autism spectrumdisorder (ASD) in children
1.6 1.8
A case-control study of infants born between January 1995 and June 1999.
Cases (n = 420) werechildren with at least1 diagnosis of an autismspectrum disorder (ASD)
Controls (n = 2100) werechildren without an ASD diagnosis.
Frequencies of maternalimmunologic disorders.
After adjustment for maternal
factors, only 1 autoimmune condition,
psoriasis, was significantly
associated with ASDs.
IL-6
Psoriasis Asthma Eczema
maternal

Maternal autoimmune diseases, asthma and allergies, and childhood autism spectrum disorders: a case-control study. Croen LA, Arch Pediatr Adolesc Med 2005:159:151–7.
2.93.0 –
2.5 –
2.0 –
1.5 –
1.0 –
0.5 –0.
0
OR for autism spectrumdisorder (ASD) in children
1.6 1.8
A case-control study of infants born between January 1995 and June 1999.
Cases (n = 420) werechildren with at least1 diagnosis of an autismspectrum disorder (ASD)
Controls (n = 2100) werechildren without an ASD diagnosis.
Frequencies of maternalimmunologic disorders.
There is strong evidence that the inflammatory cytokine
interleukin 6 (IL-6) can cross the
placenta, and dysregulation of IL-6 has been implicated in
the pathology of nervous system disturbances.
IL-6
Psoriasis Asthma Eczema
maternal

Maternal autoimmune diseases, asthma and allergies, and childhood autism spectrum disorders: a case-control study. Croen LA, Arch Pediatr Adolesc Med 2005:159:151–7.
2.93.0 –
2.5 –
2.0 –
1.5 –
1.0 –
0.5 –0.
0
OR for autism spectrumdisorder (ASD) in children
1.6 1.8
A case-control study of infants born between January 1995 and June 1999.
Cases (n = 420) werechildren with at least1 diagnosis of an autismspectrum disorder (ASD)
Controls (n = 2100) werechildren without an ASD diagnosis.
Frequencies of maternalimmunologic disorders.
Recent data indicate that T cells and
proinflammatory cytokines, including IL-6, are of
major importance in the pathophysiology of
psoriasis.IL-6
Psoriasis Asthma Eczema
maternal

Mechanisms: Maternal Factors
Elevated levels of proinflammatory cytokine IL-6 have been claimed as a mechanism underlying the effect of maternal immune activationon neurodevelopment.

Mechanisms: Maternal Factors
Indeed, prenatal exposure to IL-6 alone is sufficient to initiate abnormal behavior and neurodegeneration in the hippocampus of rodents. Smith SE, Neurosci 2007:27:10695–702.
IL-6, which is able to cross the placenta and the blood brain barrier, has been shown to affect developing serotonergic and dopaminergic neurons in vitro.Banks WA, Neurosci Lett 1994:179:53–6.Jarskog LF, Int J Dev Neurosci 1997:15:711–6.

Maternal immune activation alters fetal brain development through interleukin-6. Smith SE, Neurosci 2007:27:10695–702
Maternal immune activation
Pregnant rodents
Offspring with abnormalities in behavior, histology,
and gene expression that are reminiscent of schizophrenia
and autism.

Maternal immune activation alters fetal brain development through interleukin-6. Smith SE, Neurosci 2007:27:10695–702
Maternal immune activation
Pregnant rodents
Offspring with abnormalities in behavior, histology,
and gene expression that are reminiscent of schizophrenia
and autism.
IL-6 is critical for mediating the behavioral and transcriptional
changes in the offspring.

Maternal immune activation alters fetal brain development through interleukin-6. Smith SE, Neurosci 2007:27:10695–702
Pregnant rodents
A single maternal injection of IL-6 on day 12.5 of
mouse pregnancy.
Prepulse inhibition (PPI) and latent inhibition (LI)
deficits in the adult offspring.

Maternal immune activation alters fetal brain development through interleukin-6. Smith SE, Neurosci 2007:27:10695–702
Prepulse Inhibition (PPI) is a neurological phenomenon in which a weaker prestimulus (prepulse) inhibits the reaction of an organism to a subsequent strong startling stimulus (pulse). The stimuli are usually acoustic, but tactile stimuli (e.g. via air puffs onto the skin) [1] and light stimuli [2] are also used
Latent inhibition is a technical term used in classical conditioning to refer to the observation that a familiar stimulus takes longer to acquire meaning (as a signal or conditioned stimulus) than a new stimulus.

Maternal immune activation alters fetal brain development through interleukin-6. Smith SE, Neurosci 2007:27:10695–702
Pregnant rodents
A single maternal injection of IL-6 on day 12.5 of
mouse pregnancy.
Prepulse inhibition (PPI) and latent inhibition (LI)
deficits in the adult offspring.
Coadministration of an anti-IL-6 antibody prevents the PPI, LI, deficits and normalizes the associated changes in gene expression in
the brains of adult offspring.

Penetration of interleukin-6 across the murine blood-brain barrier. Banks WA, Neurosci Lett 1994:179:53–6.
Peripheral administrationof IL-6
Approximately 0.2% of the dose injected i.v. entered each gram of brain.
Most of the IL-6 taken up by brain entered the parenchyma.

Cytokine regulation of embryonic rat dopamine and serotonin neuronal survival in vitro.
Jarskog LF, Int J Dev Neurosci 1997:15:711–6.
IL-1β, IL-6, andTNF-α are cytokines with pleiotropic effects in the central nervous system including an emerging role in neurodevelopment
The survival of 5-hydroxytryptamine (5-HT) neurons was significantly
reduced by 20-30%
Embryonic day 14
rat brain
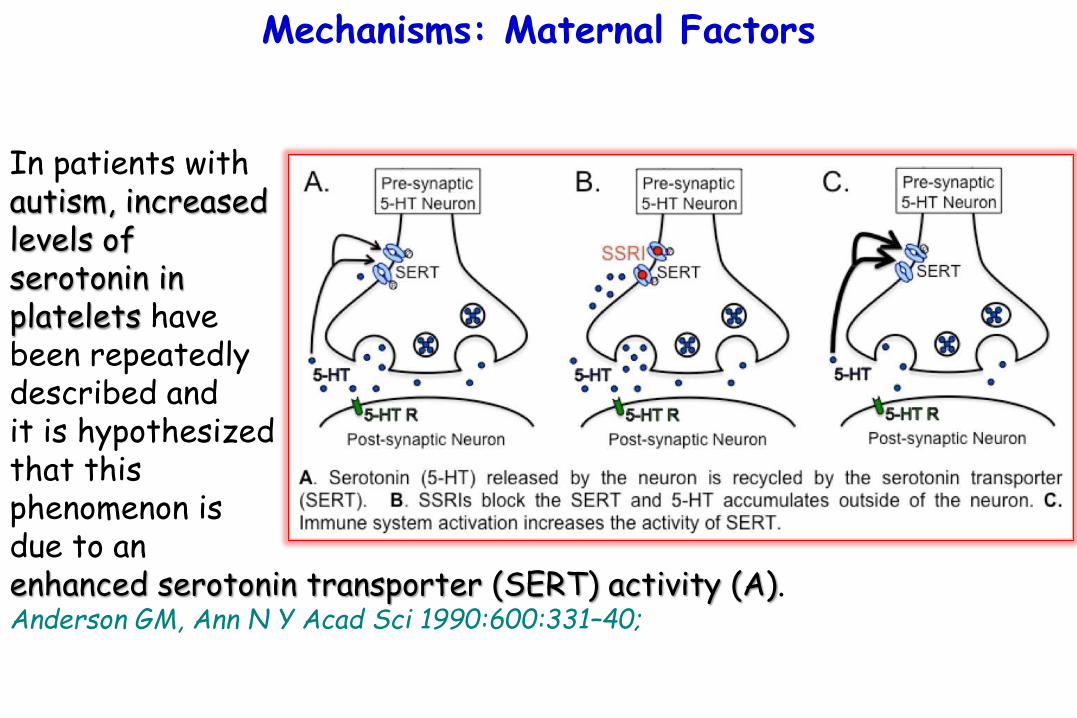
Mechanisms: Maternal Factors
In patients withautism, increasedlevels of serotonin in platelets have been repeatedly described and it is hypothesizedthat this phenomenon is due to an enhanced serotonin transporter (SERT) activity (A). Anderson GM, Ann N Y Acad Sci 1990:600:331–40;

The hyperserotonemia of autism.Anderson GM, Ann N Y Acad Sci 1990:600:331–40.
The identification of the platelet alteration which is responsible for the hyperserotonemia of autism should prove useful in several ways:
1) It would be expected that assessment of the altered function would provide a marker with less overlap with the normal population than the multidetermined measure of blood 5-HT.
2) Determination of the specific protein(s) involved in the altered platelet should lead directly to gene probes and chromosomal location. These, in turn, should prove useful for neonatal screening, subtyping, and more powerful genetic and family studies.
3) Work of this sort might also allow early intervention and improved treatment.
4) Finally, characterization of the physiological alteration would provide a basis for focusing studies of brain neurochemistry and should, as well, suggest modes of neuropharmacologicalintervention.

Mechanisms: Maternal Factors
Treatment with selective serotonin reuptake inhibitors (SRRIs)has favorable effects in some children (B).Kumar B, Pharmacol Rep 2012:64:1291–304.

Drug therapy in autism: present and future perspective. Kumar B, Pharmacol Rep 2012:64:1291–304.
Autism is is traditionally considered a "static" encephalopathicdisorder without any specific cure and few effective biomedical interventions.
There are various factors which are involved in the etiopathogenesisof autism or autism spectrum disorder (ASD) such as impaired immune responses, neuroinflammation, abnormal neurotransmission, oxidative stress, mitochondrial dysfunction, environmental toxins and stressors.
The autism is often associated with a number of genetic disorders such as fragile X syndrome, tuberous sclerosis, epilepsy and Down syndrome.

Mechanisms: Maternal Factors
Furthermore, associations with important genes in the dopaminergicpathway have also been reported in both ASD and ADHD, including the dopamine transporter gene DAT1.Rommelse NN, Eur ChildAdolescPsychiatry 2010:19:281–95.
Dopamine (contracted from 3,4-dihydroxyphenethylamine) is a hormone and neurotransmitter and of the catecholamine and phenethylamine families. The brain includes several distinct dopamine systems, one of which plays a major role in reward-motivated behavior. Other brain dopamine systems are involved in motor control and in controlling the release of several other important hormones.

Mechanisms: Maternal Factors
Cytokines in the CNS can activate monoamine transporters, Zhu CB, Neuropsychopharmacology 2006:31:2121–31.
resulting in reduced neurotransmission, which may lead to symptoms observed in ADHD and ASDMadras BK, Biol Psychiatry 2005:57:1397–409.

The proinflammatory cytokines IL-1β and TNF-αactivate serotonin transporters.
Zhu CB, Neuropsychopharmacology 2006:31:2121–31.
Activation of p38 mitogen-activatedprotein kinase (MAPK) induces a catalyticactivation of the serotonin transporter(SERT) arising from a reduction in the SERT for 5 hydroxytryptamine (5-HT).
As inflammatory cytokines can activatep38 MAPK, we hypothesized that theymight also activate neuronal SERT.
The proinflammatory cytokines IL-1β and TNF-αactivate serotonin transporters.
Zhu CB, Neuropsychopharmacology 2006:31:2121–31.
Interleukin-1beta (IL-1beta) and tumor necrosis factor alpha
(TNF-alpha) stimulated
serotonin uptake in both the ratembryonic cell line,
and in mouse midbrain and striatal synaptosomes.
proinflammatory cytokines can acutely regulate neuronal SERT activity via
p38 MAPK-linked pathways.

The dopamine transporter and attention-deficit/hyperactivity disorder.
Madras BK, Biol Psychiatry 2005:57:1397–409.
Currently, the majority of specific genes implicated in ADHD encode components of catecholamine signaling systems.
Of these, the dopamine transporter (DAT) is a principal target of the most widely used antihyperactivity medications (amphetamine and methylphenidate).
The DAT gene is associated with ADHD, and some studies have detected abnormal levels of the DAT in brain striatum of ADHD subjects

The dopamine transporter and attention-deficit/hyperactivity disorder.
Madras BK, Biol Psychiatry 2005:57:1397–409.
Medications for ADHD interfere with dopamine transport by brain-region- and drug-specific mechanisms, indirectly activating dopamine- and possibly norepinephrine-receptor subtypes that are implicated in enhancing attention and experiential salience.
The most commonly used dopamine transporter (DAT)-selective ADHD medications raise extracellular dopamine levels in DAT-rich brain regions.

Mechanisms: Maternal Factors
Maternal immune activation ( IL-6) in animal models cause defects in dopaminergic development in the offspring, Aguilar-Valles A, PLoS ONE 2010:5:e10967.Bitanihirwe BK, Neuropsychopharmacology 2010:35:2462–78.Vuillermot S, J Neurosci 2010:30:1270–87.
and neutralization of IL-6 in pregnant dams prevented the dopaminergic and behavioral alterations induced by maternal immune activation . Aguilar-Valles A, Psychoneuroendocrinology 2012:37:956–69.

Prenatal inflammation-induced hypoferremia altersdopamine function in the adult offspring in rat: relevance for schizophrenia. Aguilar-Valles A, PLoS ONE 2010:5:e10967.
1) Maternal infection during pregnancy has been associated with increased incidence of schizophrenia in the adult offspring.
2) Mechanistically, this has been partially attributed to neurodevelopmental disruption of the dopamine neurons, as a consequence of exacerbated maternal immunity.
3) Hypoferremia, a cytokine-induced reduction of serum non-heme iron, is common to all types of infections.
4) Adequate iron supply to the fetus is fundamental for the development of the mesencephalic dopamine neurons.
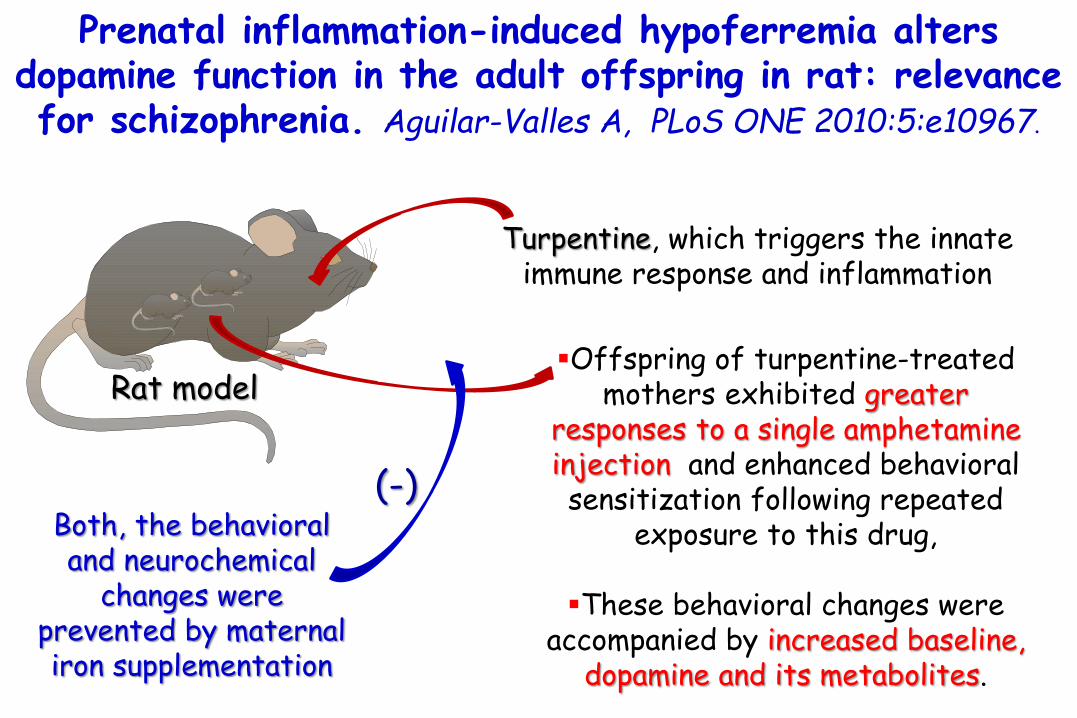
Turpentine, which triggers the innate immune response and inflammation
Rat model
Both, the behavioral and neurochemical
changes were prevented by maternal iron supplementation
Prenatal inflammation-induced hypoferremia altersdopamine function in the adult offspring in rat: relevance for schizophrenia. Aguilar-Valles A, PLoS ONE 2010:5:e10967.
Offspring of turpentine-treated mothers exhibited greater
responses to a single amphetamine injection and enhanced behavioral sensitization following repeated
exposure to this drug,
These behavioral changes were accompanied by increased baseline,
dopamine and its metabolites.
(-)
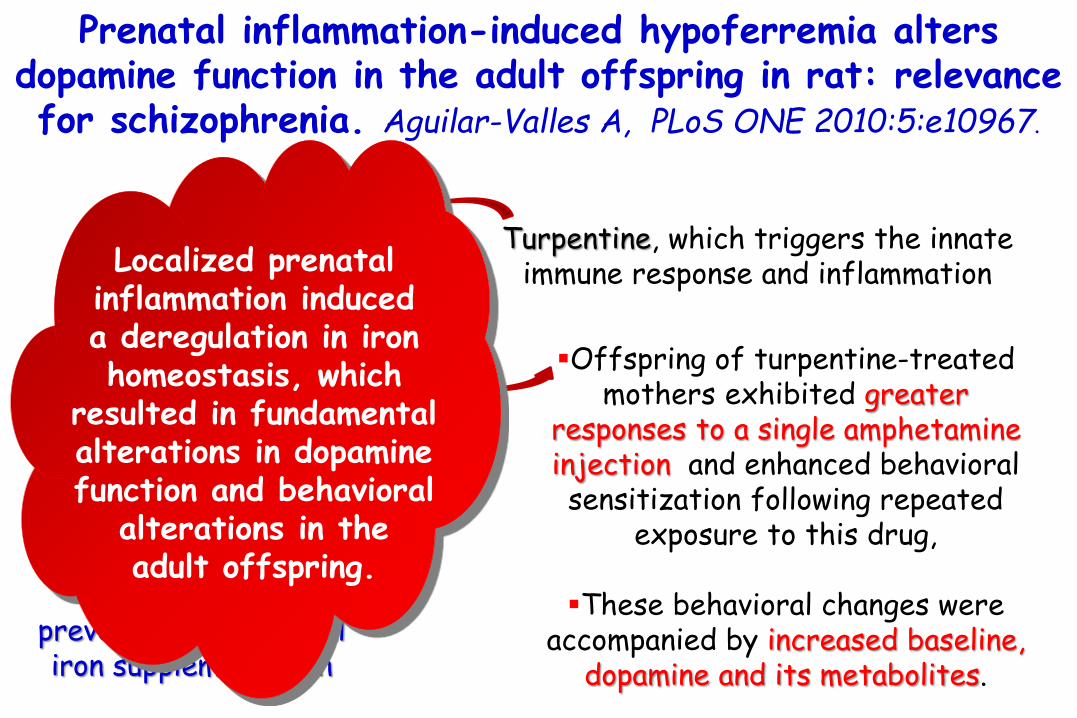
Turpentine, which triggers the innate immune response and inflammation
Rat model
Both, the behavioral and neurochemical
changes were prevented by maternal iron supplementation
Prenatal inflammation-induced hypoferremia altersdopamine function in the adult offspring in rat: relevance for schizophrenia. Aguilar-Valles A, PLoS ONE 2010:5:e10967.
Offspring of turpentine-treated mothers exhibited greater
responses to a single amphetamine injection and enhanced behavioral sensitization following repeated
exposure to this drug,
These behavioral changes were accompanied by increased baseline,
dopamine and its metabolites.
(-)
Localized prenatal inflammation induced a deregulation in iron homeostasis, which
resulted in fundamental alterations in dopamine function and behavioral
alterations in the adult offspring.
Late prenatal immune activation in mice leads to behavioral and neurochemical abnormalities
relevant to the negative symptoms of schizophrenia. Bitanihirwe BK, Neuropsychopharmacology 2010:35:2462–78.
prenatal exposure to the viral mimic polyriboinosinic-polyribocytidilic acid (Poly-I:C; 5 mg/kg, i.v.) on gestation day (GD) 17 led to significant deficits in social interaction, anhedonicbehavior, and alterations in the locomotor and stereotyped behavioral responses to acute apomorphine (APO) treatment in both male and female offspring. In addition, male but notfemale offspring born to immune challenged mothers displayed behavioral/cognitive inflexibility as indexed by the presence of an abnormally enhanced latent inhibition (LI) effect. Prenatal immune activation in late gestation also led to numerous, partly sex-specificchanges in basal neurotransmitter levels, including reduced dopamine (DA) and glutamatecontents in the prefrontal cortex and hippocampus, as well as reduced γ-aminobutyric acid (GABA) and glycine contents in the hippocampus and prefrontal cortex, respectively.

A longitudinal examination of the neurodevelopmentalimpact of prenatal immune activation in mice reveals
primary defects in dopaminergic development relevant to schizophrenia. Vuillermot S, J Neurosci 2010:30:1270–87.
Prenatal exposure to infection is a significant environmental risk factor in the development of schizophrenia and related disorders.
Recent evidence indicates that disruption of functional and structural dopaminergicdevelopment may be at the core of the developmental neuropathology associated with psychosis-related abnormalities induced by prenatal exposure to infection.
Using a mouse model of prenatal immune challenge by the viral mimic polyriboinosinic-polyribocytidilic acid, we showed that prenatal immune challenge leads to dopaminergicmaldevelopment starting as early as in the fetal stages of life and produces a set of postnatal dopaminergic abnormalities that is dependent on postnatal maturational processes.
Furthermore, our longitudinal investigations reveal a striking developmental correspondencebetween the ontogeny of specific dopaminergic neuropathology and the postnatal onset ofdistinct forms of dopamine-dependent functional abnormalities implicated in schizophrenia.

Leptin and IL-6 alter the function of mesolimbic dopamine neurons in a rodent model of prenatal inflammation. Aguilar-Valles A, Psychoneuroendocrinology 2012:37:956–69.
Increased activity of mesolimbic dopamine (DA) neurons, a hallmark of psychosis, is found in offspring of rodents exposed to a prenatal inflammatory challenge but it is unclear how this effect is elicited.
Using an experimental model of localized aseptic inflammation with turpentine oil (TURP) we sought to establish whether circulating interleukin-6 (IL-6) and leptin play a role in the effects of prenatal inflammation on DA neurons.
Both mediators are involved in the systemic inflammatory response to immunogens, with IL-6 mediating the early phase, followed by leptin in the late phase of the response.
Maternal treatment with TURP at gestational day (GD) 15 enhanced the locomotor response to the DA indirect agonist, amphetamine (AMPH), increased the expression of tyrosine hydroxylase (TH), an enzyme involved in DA synthesis, DA levels and the expression of the post-synaptic protein spinophilin in the nucleus accumbens (NAcc) in the adult offspring.
All of these alterations were totally abolished by co-treating the pregnant dams with a neutralizing
IL-6 antiserum.

Mechanisms: Maternal Factors
Maternal immune activation ( IL-6) in animal models cause defects in dopaminergic development in the offspring, Aguilar-Valles A, PLoS ONE 2010:5:e10967.Bitanihirwe BK, Neuropsychopharmacology 2010:35:2462–78.Vuillermot S, J Neurosci 2010:30:1270–87.
and neutralization of IL-6 in pregnant dams prevented the dopaminergic and behavioral alterations induced by maternal immune activation . Aguilar-Valles A, Psychoneuroendocrinology 2012:37:956–69.
These findings suggest that prenatalimmune activation disturbs neurodevelopment via IL-6,
leading to behavioral abnormalities as found in ADHD and ASD.

Autism spectrum disorders and mastocytosis. Theoharides TC. Int J Immunopathol Pharmacol 2009:22:859–65
1) The number of ASD cases have increased over the last decade to 1/100 up to 1/68.
2) The apparent prevalence of ASD in patients with mastocytosis, is about 1/10 or 10 times higher than the general population.
Allergic, infectious, neuroimmune and environmental triggers may activate mast cells to release vasoactive, inflammatory and neurotoxic molecules.
These could disrupt the gut-blood-brain-barriers, and/or activate susceptibility genes, thus contributing to brain inflammation and ASD.

Autism spectrum disorders and mastocytosis. Theoharides TC. Int J Immunopathol Pharmacol 2009:22:859–65
1) The number of ASD cases have increased over the last decade to 1/100.
2) The apparent prevalence of ASD in patients with mastocytosis, is about 1/10 or 10 times higher than the general population.
Allergic, infectious, neuroimmune and environmental triggers may activate mast cells to release vasoactive, inflammatory and neurotoxic molecules.
These could disrupt the gut-blood-brain-barriers, and/or activate susceptibility genes, thus contributing to brain inflammation and ASD.

Mechanisms: Mast cells
Not only IgE, but also several neuropeptides can trigger mast cell activation, including:•substance P,•nerve growth factor (NGF), •vasoactive intestinalpeptide (VIP), and•neurotensin.Angelidou A, J Neuroinflammation2010:7:48.
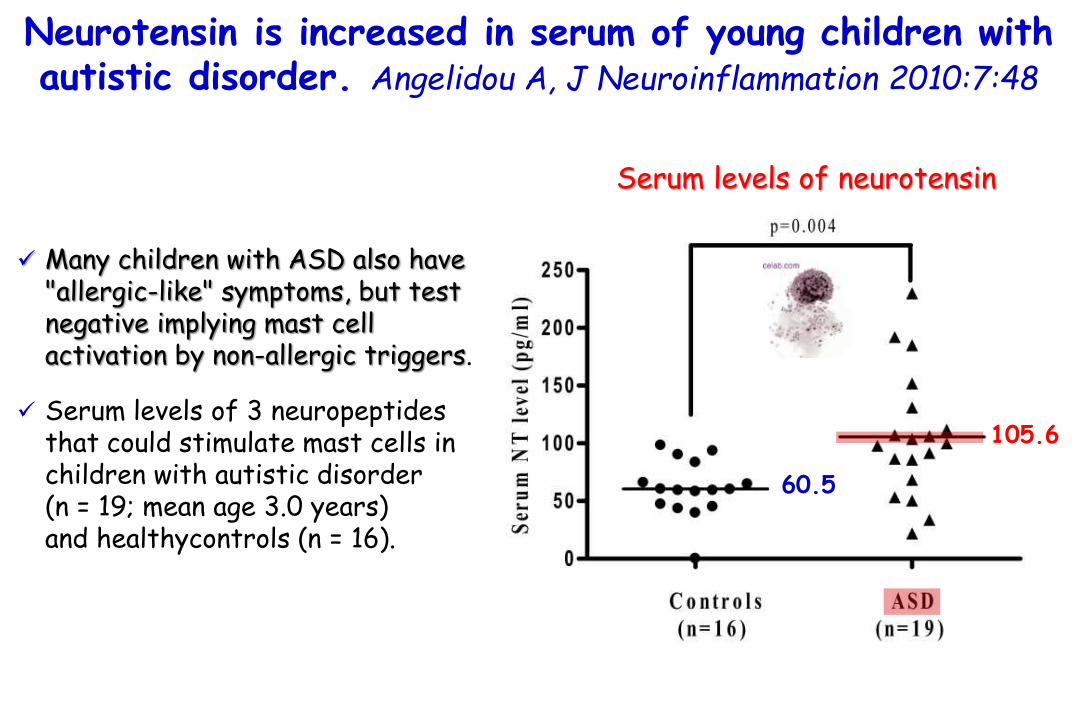
Neurotensin is increased in serum of young children with autistic disorder. Angelidou A, J Neuroinflammation 2010:7:48
Many children with ASD also have "allergic-like" symptoms, but test negative implying mast cell activation by non-allergic triggers.
Serum levels of 3 neuropeptidesthat could stimulate mast cells in children with autistic disorder (n = 19; mean age 3.0 years) and healthycontrols (n = 16).
Serum levels of neurotensin
60.5
105.6

Neurotensin is increased in serum of young children with autistic disorder. Angelidou A, J Neuroinflammation 2010:7:48
Many children with ASD also have "allergic-like" symptoms, but test negative implying mast cell activation by non-allergic triggers.
Serum levels of 3 neuropeptidesthat could stimulate mast cells in children with autistic disorder (n = 19; mean age 3.0 years) and healthycontrols (n = 16).
Serum levels of neurotensin
60.5
105.6
Only neurotensin was significantly increased in
autistic disorder (p = 0.004).
There was no statistically significant difference in the
serum levels of β-endorphin or substance P.

Neurotensin is increased in serum of young children with autistic disorder. Angelidou A, J Neuroinflammation 2010:7:48
Many children with ASD also have "allergic-like" symptoms, but test negative implying mast cell activation by non-allergic triggers.
Serum levels of 3 neuropeptidesthat could stimulate mast cells in children with autistic disorder (n = 19; mean age 3.0 years) and healthycontrols (n = 16).
Serum levels of neurotensin
60.5
105.6
Neurotensin could stimulate immune cells, especially mast cells, and/or have direct effects on brain
inflammation and ASD.

NT is a peptide originally isolated from the brain. It is present also in the gastrointestinal tract,where it can induce intestinal inflammation.
Neurotensin can: 1) stimulate lymphocyte proliferation, 2) activate T cells, 3) enhance IL-1 production from macrophages4) trigger of mast cells.
These effects are relevant to the findings that many children with ASD also present with gastrointestinal and “allergic-like” symptoms
Gurney JG, Arch Pediatr Adolesc Med. 2006;160(8):825-30.
Neurotensin is increased in serum of young children with autistic disorder. Angelidou A, J Neuroinflammation 2010:7:48
macrophage
IL-1
IL-1IL-1
IL-1IL-1
*
*
*
*
*
*
*
*
**
**

NT is a peptide originally isolated from the brain. It is present also in the gastrointestinal tract,where it can induce intestinal inflammation.
Neurotensin can: 1) stimulate lymphocyte proliferation, 2) activate T cells, 3) enhance IL-1 production from macrophages4) trigger of mast cells.
These effects are relevant to the findings that many children with ASD also present with gastrointestinal and “allergic-like” symptoms
Gurney JG, Arch Pediatr Adolesc Med. 2006;160(8):825-30.
Neurotensin is increased in serum of young children with autistic disorder. Angelidou A, J Neuroinflammation 2010:7:48
macrophage
IL-1
IL-1IL-1
IL-1IL-1
*
*
*
*
*
*
*
*
**
**
Such “allergic symptoms” often occur in the absence of elevated serum IgE or positive skin prick tests,
suggesting mast cell activation by non-immune triggers .Theoharides TC, Ann NY Acad Sci 2006, 1088:78-99.

Mast cells and nerves tickle in the tummy: implications for inflammatory bowel disease and irritable bowelsyndrome. Rijnierse A, Pharmacol Ther 2007:116:207–35.
Mast cells are well known as versatile cells capable of releasing and producing a variety of inflammatory mediators upon activation and are often found in close proximity of neurons.
In addition, inflammation leads to local activation of neurons resulting in the release neuropeptides, which also play an important immune modulatory role by stimulation of immune cells.
In intestinal disorders like inflammatory bowel disease (IBD) and irritable bowel syndrome (IBS), the number of mast cells is known to be much higher than in the normal intestine. Moreover, both these disorders are also reported to be associated with alterations in neuropeptide content and in neural innervation.
Mutual association between mast cells and enteric nerves has been demonstrated to be increased in pathophysiological conditions and contribute to spreading and amplification of the response in IBD and IBS.

Mast cells and nerves tickle in the tummy: implications for inflammatory bowel disease and irritable bowelsyndrome. Rijnierse A, Pharmacol Ther 2007:116:207–35.
bidirectional receptor expression by mast cells and nerves of their
respective mediators.

Mechanisms: Mast cells
In theory, an allergic reaction in the gut might therefore influence behavior via intestinal mast cells, which are able to trigger enteric neurons to conveyinformation through afferent sensory pathways to the CNS.
Although there is very little direct evidence suggesting thatmast cells are involved in neurodevelopmental disorders, apreliminary report indicated ASD to be more prevalent amongchildren with mastocytosis. Theoharides TC. Int J Immunopathol Pharmacol 2009:22:859.

Mechanisms: Mast cells
Activated Th2 and mast cells produce IL-6, which promotes B cell differentiation and production of immunoglobulinsand inhibits Tregs, leading to an enhanced allergic reaction.Lin G, J Immunother 2012: 35: 337–43.
The production of IL-6 by activated mast cells is mediated bythe mammalian target of rapamycin(mTOR) pathway.Kim MS, J Immunol 2008: 180: 4586–95.
Deficiency of PTEN, a negative regulatory molecule of mTOR, causes mastocytosis in mice and increased mast cell degranulation and IL-6 production, leading to a higher allergic response. Furumoto Y, Blood 2011:118:5466–75.

Mechanisms: Mast cells
Activated Th2 and mast cells produce IL-6, which promotes B cell differentiation and production of immunoglobulinsand inhibits Tregs, leading to an enhanced allergic reaction.Lin G, J Immunother 2012: 35: 337–43.
The production of IL-6 by activated mast cells is mediated bythe mammalian target of rapamycin(mTOR) pathway.Kim MS, J Immunol 2008: 180: 4586–95.
Deficiency of PTEN, a negative regulatory molecule of mTOR, causes mastocytosis in mice and increased mast cell degranulation and IL-6 production, leading to a higher allergic response. Furumoto Y, Blood 2011:118:5466–75.
besides the effect on the allergic response, PTEN-deficient mice also
developed autistic features in behaviorZhou J, J Neurosci 2009:29:1773–83.
Pharmacological inhibition of mTORC1 suppressesanatomical, cellular, and behavioral abnormalities in
neural-specific Pten knock-out mice. Zhou J, J Neurosci 2009:29:1773–83.
PTEN (phosphatase and tensin homolog deleted on chromosome ten) is a lipid phosphatase that counteracts the function of phosphatidylinositol-3 kinase (PI3K).
Loss of function of PTEN results in constitutive activation of AKT and downstream effectors and correlates with various brain disorders, including macrocephaly, seizures, Lhermitte-Duclos disease, and autism.
A Pten knock-out mouse line with Pten-null neurons developed neuronal hypertrophy and loss of neuronal polarity.
The mutant mice exhibited macrocephaly and behavioral abnormalities reminiscent of certain features of human autism.
Pharmacological inhibition of mTORC1 suppressesanatomical, cellular, and behavioral abnormalities in
neural-specific Pten knock-out mice. Zhou J, J Neurosci 2009:29:1773–83.
PTEN (phosphatase and tensin homolog deleted on chromosome ten) is a lipid phosphatase that counteracts the function of phosphatidylinositol-3 kinase (PI3K).
Loss of function of PTEN results in constitutive activation of AKT and downstream effectors and correlates with various brain disorders, including macrocephaly, seizures, Lhermitte-Duclos disease, and autism.
A Pten knock-out mouse line with Pten-null neurons developed neuronal hypertrophy and loss of neuronal polarity.
The mutant mice exhibited macrocephaly and behavioral abnormalities reminiscent of certain features of human autism.
rapamycin, a specific inhibitor of mammalian target of rapamycincomplex 1 (mTORC1), can prevent and reverse neuronal hypertrophy, resulting in the amelioration of a subset of PTEN-associated abnormal behaviors, providing evidence that the mTORC1 pathway downstream
of PTEN is critical for this complex phenotype.

Mechanisms: Mast cells
Indeed, increased mTOR signaling has been suggested to be involved in neurodevelopmental disorders.
For example, tuberous sclerosis, a genetic disorder of mutations in tuberoussclerosis complex (Tsc) 1 or Tsc2 genes that negatively regulate mTOR, is associated with ASD and ADHD.Numis AL, Neurology 2011:76:981–7.Muzykewicz DA, Epilepsy Behav 2007:11:506–13.
(+)

Identification of risk factors for autism spectrum disorders in tuberous sclerosis complex.
Numis AL, Neurology 2011:76:981–7
40%40 –
30 –
20 –
10 –
.0
% Patients with TSC
Diagnosed with an ASD
103 patients withtuberous sclerosiscomplex (TSC).
Evaluated for ASD.

Identification of risk factors for autism spectrum disorders in tuberous sclerosis complex.
Numis AL, Neurology 2011:76:981–7
40%40 –
30 –
20 –
10 –
.0
% Patients with TSC
Diagnosed with an ASD
103 patients withtuberous sclerosiscomplex (TSC).
Evaluated for ASD.
Patients with ASD also had an earlier age at seizure onset and more frequent
seizures.
On EEG, those with ASD had a significantly greater
amount of intercriticalepileptiform features in the left temporal
lobe only.

Psychiatric comorbid conditions in a clinic population of 241 patients with tuberous sclerosis complex.
Muzykewicz DA, Epilepsy Behav 2007:11:506–13
Psychiatric symptoms retrospectively assessed.
241 children and adults with tuberous sclerosis complex (TSC). Mood
disorderAnxietydisorder
History of attention-
deficit hyperactivity
disorder
Aggressive-disruptive behaviordisorder
27%
30 –
25 –
20 –
15 –
10 –
05 –.
00
30% 28%
% subjects with
27%
SYMPTOMS

Psychiatric comorbid conditions in a clinic population of 241 patients with tuberous sclerosis complex.
Muzykewicz DA, Epilepsy Behav 2007:11:506–13
Psychiatric symptoms retrospectively assessed.
241 children and adults with tuberous sclerosis complex (TSC). Mood
disorderAnxietydisorder
History of attention-
deficit hyperactivity
disorder
Aggressive-disruptive behaviordisorder
27%
30 –
25 –
20 –
15 –
10 –
05 –.
00
30% 28%
% subjects with
27%
SYMPTOMS
Citalopramdemonstrated
efficacy in treating anxiety and
depression, and risperidone, in
treating problematic behaviors.

Mechanisms: Mast cells
higher IL-6 production by mast cells and mastocytosis,
a higher allergic response.
neurodevelopmental disorders
behavioral deficits.
In mice increased activity of the mTOR-signaling pathway

Mechanisms: Mast cells
The effects of mTOR activity on behavior are partially mediated by IL-6, as enhanced mTOR activation results in IL-6 production, and IL-6 has beenshown to induce behavioral deficits and is enhanced in postmortem brains of patients with ASD.Vargas DL, Ann Neurol2005: 57:67–81.Li X, J Neuroimmunol 2009:207:111–6.

Neuroglial activation and neuroinflammation in the brain of patients with autism. Vargas DL, Ann Neurol 2005:57:67–81
Immunocytochemistry, cytokine protein arrays, and enzyme-linkedimmunosorbent assays tostudy brain tissues and cerebrospinal fluid (CSF) from autistic patients.
Brain tissues fromcerebellum, midfrontal, and cingulate gyrusobtained at autopsy from11 patients with autism.
CSF from six living autistic patients.
We demonstrate an active neuroinflammatory process in the cerebral cortex, white matter, and notably in cerebellum of autistic patients.

Neuroglial activation and neuroinflammation in the brain of patients with autism. Vargas DL, Ann Neurol 2005:57:67–81
Immunocytochemical studiesshowed marked activation ofmicroglia and astroglia,
and cytokine profiling indicatedthat macrophagechemoattractant protein (MCP)-1
and TGF-β1, derived fromneuroglia, werethe most prevalentcytokines in brain tissues.
Immunocytochemistry, cytokine protein arrays, and enzyme-linkedimmunosorbent assays tostudy brain tissues and cerebrospinal fluid (CSF) from autistic patients.
Brain tissues fromcerebellum, midfrontal, and cingulate gyrusobtained at autopsy from11 patients with autism.
CSF from six living autistic patients.

Neuroglial activation and neuroinflammation in the brain of patients with autism. Vargas DL, Ann Neurol 2005:57:67–81
Cerebrospinal fluid showed a unique proinflammatoryprofile of cytokines, including a marked increase in macrophagechemoattractant proteinMCP-1.
Immunocytochemistry, cytokine protein arrays, and enzyme-linkedimmunosorbent assays tostudy brain tissues and cerebrospinal fluid (CSF) from autistic patients.
Brain tissues fromcerebellum, midfrontal, and cingulate gyrusobtained at autopsy from11 patients with autism.
CSF from six living autistic patients.

Neuroglial activation and neuroinflammation in the brain of patients with autism. Vargas DL, Ann Neurol 2005:57:67–81
Cerebrospinal fluid showed a unique proinflammatoryprofile of cytokines, including a marked increase in macrophagechemoattractant proteinMCP-1.
Immunocytochemistry, cytokine protein arrays, and enzyme-linkedimmunosorbent assays tostudy brain tissues and cerebrospinal fluid (CSF) from autistic patients.
Brain tissues fromcerebellum, midfrontal, and cingulate gyrusobtained at autopsy from11 patients with autism.
CSF from six living autistic patients.
Innate neuroimmune
reactions play a pathogenic role in an proportion
of autistic patients.

Neuroglial activation and neuroinflammation in the brain of patients with autism. Vargas DL, Ann Neurol 2005:57:67–81
Cerebellar pathology in autism (autoptic biopsy)
Marked activation of microglia (immunostainedwith anti–HLA-DR) in the cerebellar folia in autism
Normal cerebellar foliain a control brain
Patchy loss of Purkinjecell layer and granular
cell layer in autism
an active neuroinflammatory process in the cerebral cortex, white matter, and notably in cerebellum of autistic patients.

Neuroglial activation and neuroinflammation in the brain of patients with autism. Vargas DL, Ann Neurol 2005:57:67–81
Neuroinflammatorydamage in ASD

Neuroglial activation and neuroinflammation in the brain of patients with autism. Vargas DL, Ann Neurol 2005:57:67–81
Neuroglial reactions in the cerebral cortex of autistic patients
Autistic Normal Autistic Normal
Microglia staining Astroglia staining
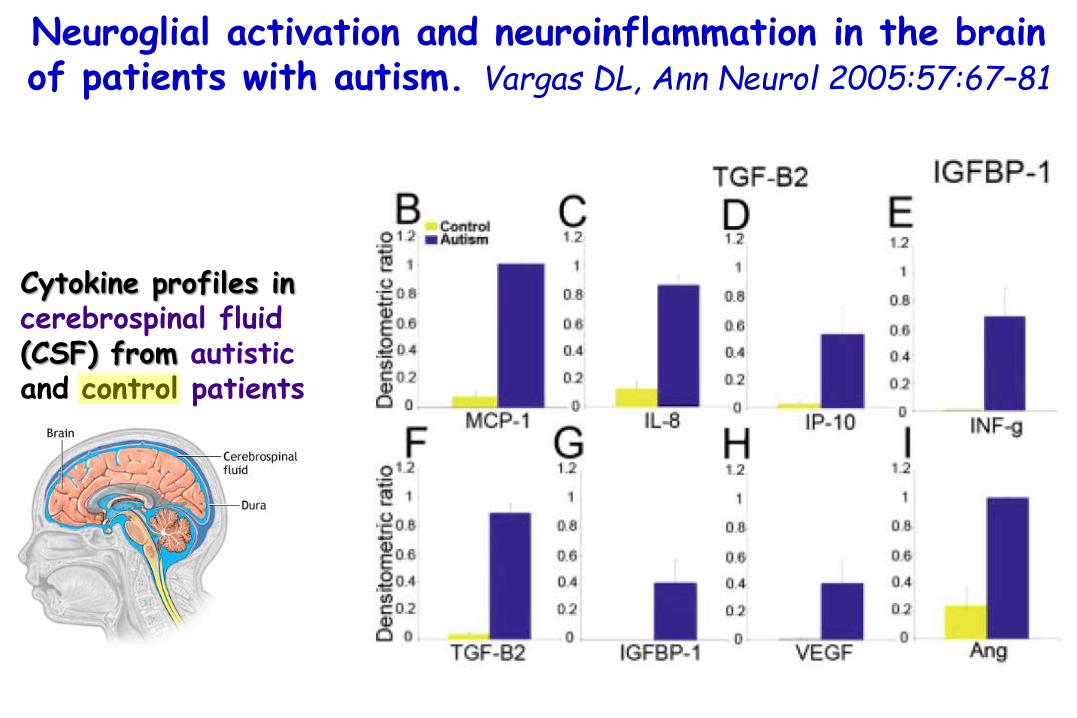
Neuroglial activation and neuroinflammation in the brain of patients with autism. Vargas DL, Ann Neurol 2005:57:67–81
Cytokine profiles in cerebrospinal fluid (CSF) from autisticand control patients
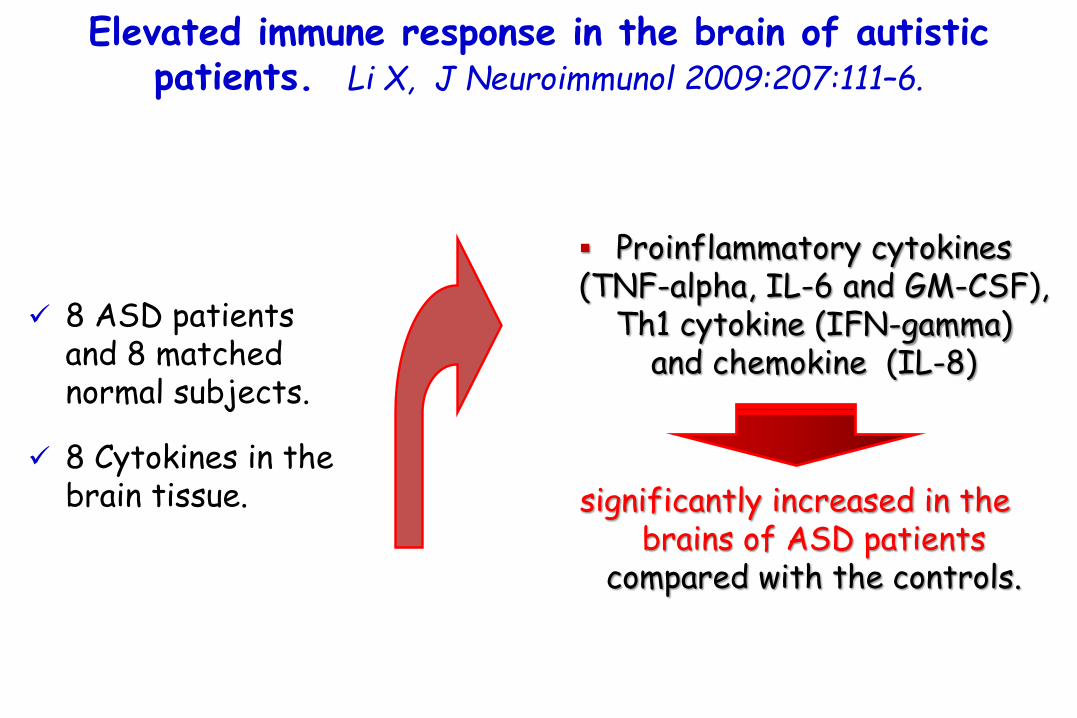
Elevated immune response in the brain of autisticpatients. Li X, J Neuroimmunol 2009:207:111–6.
8 ASD patients and 8 matched normal subjects.
8 Cytokines in the brain tissue.
Proinflammatory cytokines (TNF-alpha, IL-6 and GM-CSF),
Th1 cytokine (IFN-gamma) and chemokine (IL-8)
significantly increased in the brains of ASD patients
compared with the controls.

Elevated immune response in the brain of autisticpatients. Li X, J Neuroimmunol 2009:207:111–6.
8 ASD patients and 8 matched normal subjects.
8 Cytokines in the brain tissue.
Proinflammatory cytokines (TNF-alpha, IL-6 and GM-CSF),
Th1 cytokine (IFN-gamma) and chemokine (IL-8)
significantly increased in the brains of ASD patients
compared with the controls.
Th2 cytokines (IL-4, IL-5
and IL-10) showed no significant difference.

Elevated immune response in the brain of autisticpatients. Li X, J Neuroimmunol 2009:207:111–6.
Pro-inflammatory cytokines profile in the brain cortex of ASD patients
p<0.001p<0.05
p<0.01
ns

Elevated immune response in the brain of autisticpatients. Li X, J Neuroimmunol 2009:207:111–6.
Th1/Th2 cytokine ratio increases in the brain of ASD patients
Chemokine profile in the brain cortex of ASD patients
p<0.05
p<0.01

Mechanisms: Microbiome
microglia (the resident macrophages of the brain), are very sensitive
to any inflammatory triggers
high fat, low fibre ‘western’ diet
change in the gut microbiome,
effects on gut barrier function,
increasing systemic antigenic load and low-grade endotoxaemia
higher levels of:
CRP IL-1β, TNF-α, IL-6.
low-gradesystemic inflammation

Mechanisms: Microbiome
microglia (the resident macrophages of the brain), are very sensitive
to any inflammatory triggers
high fat, low fibre ‘western’ diet
change in the gut microbiome,
effects on gut barrier function,
increasing systemic antigenic load and low-grade endotoxaemia
higher levels of:
CRP IL-1β, TNF-α, IL-6.
low-gradesystemic inflammation
Natural environments, ancestral diets, and microbial ecology:
is there a modern "paleo-deficit disorder"? Logan AC, J Physiol Anthropol. 2015;34(1):9
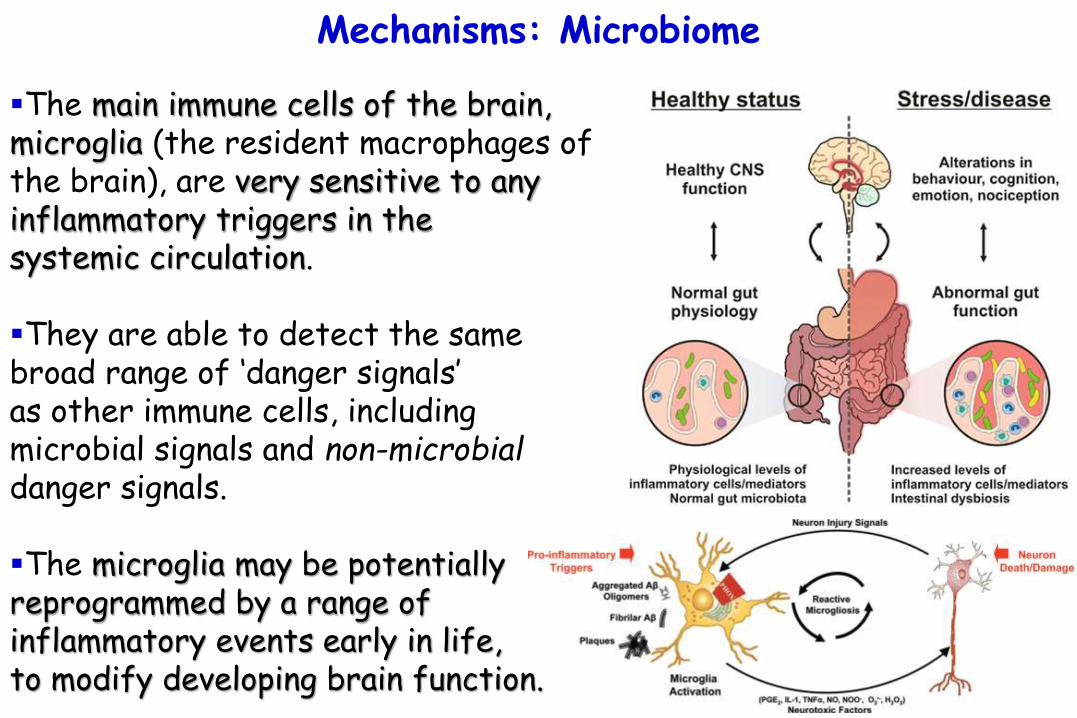
Mechanisms: Microbiome
The main immune cells of the brain, microglia (the resident macrophages of the brain), are very sensitive to any inflammatory triggers in the systemic circulation.
They are able to detect the samebroad range of ‘danger signals’ as other immune cells, including microbial signals and non-microbialdanger signals.
The microglia may be potentially reprogrammed by a range of inflammatory events early in life, to modify developing brain function.
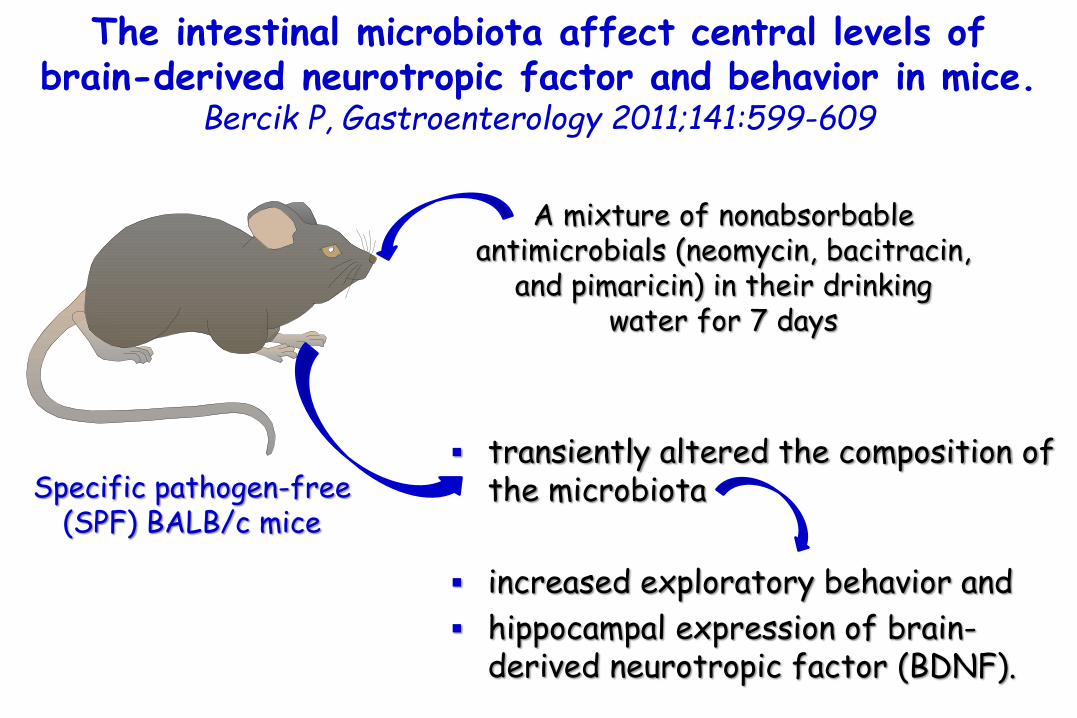
The intestinal microbiota affect central levels of brain-derived neurotropic factor and behavior in mice.
Bercik P, Gastroenterology 2011;141:599-609
Specific pathogen-free (SPF) BALB/c mice
A mixture of nonabsorbableantimicrobials (neomycin, bacitracin,
and pimaricin) in their drinking water for 7 days
transiently altered the composition of the microbiota
increased exploratory behavior and
hippocampal expression of brain-derived neurotropic factor (BDNF).

The intestinal microbiota affect central levels of brain-derived neurotropic factor and behavior in mice.
Bercik P, Gastroenterology 2011;141:599-609
Specific pathogen-free (SPF) BALB/c mice
A mixture of nonabsorbableantimicrobials (neomycin, bacitracin,
and pimaricin) in their drinking water for 7 days
transiently altered the composition of the microbiota
increased exploratory behavior and
hippocampal expression of brain-derived neurotropic factor (BDNF).
The intestinal microbiota
influences brain chemistry
and behavior.

The intestinal microbiota affect central levels of brain-derived neurotropic factor and behavior in mice.
Bercik P, Gastroenterology 2011;141:599-609
Germ-freeBALB/c mice
Colonization of germ-free BALB/c mice with microbiota from NIH
Swiss mice increased exploratory behavior and hippocampal levels of brain-derived neurotropic factor
A mixture of nonabsorbableantimicrobials (neomycin, bacitracin, and pimaricin) in their drinking water for 7 days and
Microbiota from Specific pathogen-free (SPF) NIH Swiss mice.

Postnatal microbial colonization programs the hypothalamic-pituitary-adrenal system for stress response in mice. Sudo N, J Physiol 2004;558:263-75
Germfree (GF) Specific pathogen free (SPF)
Gnotobiotic mice
Higher Plasma ACTH and corticosterone
than
Hypothalamic-pituitary-adrenal (HPA) reaction to restraint stress

Postnatal microbial colonization programs the hypothalamic-pituitary-adrenal system for stress response in mice. Sudo N, J Physiol 2004;558:263-75
Germfree (GF) Specific pathogen free (SPF)
Gnotobiotic mice
Higher Plasma ACTH and corticosterone
than
Hypothalamic-pituitary-adrenal (HPA) reaction to restraint stress
GF mice also exhibited reduced brain-derived neurotrophic factor expression levels in the cortex and hippocampus relative to SPF mice.
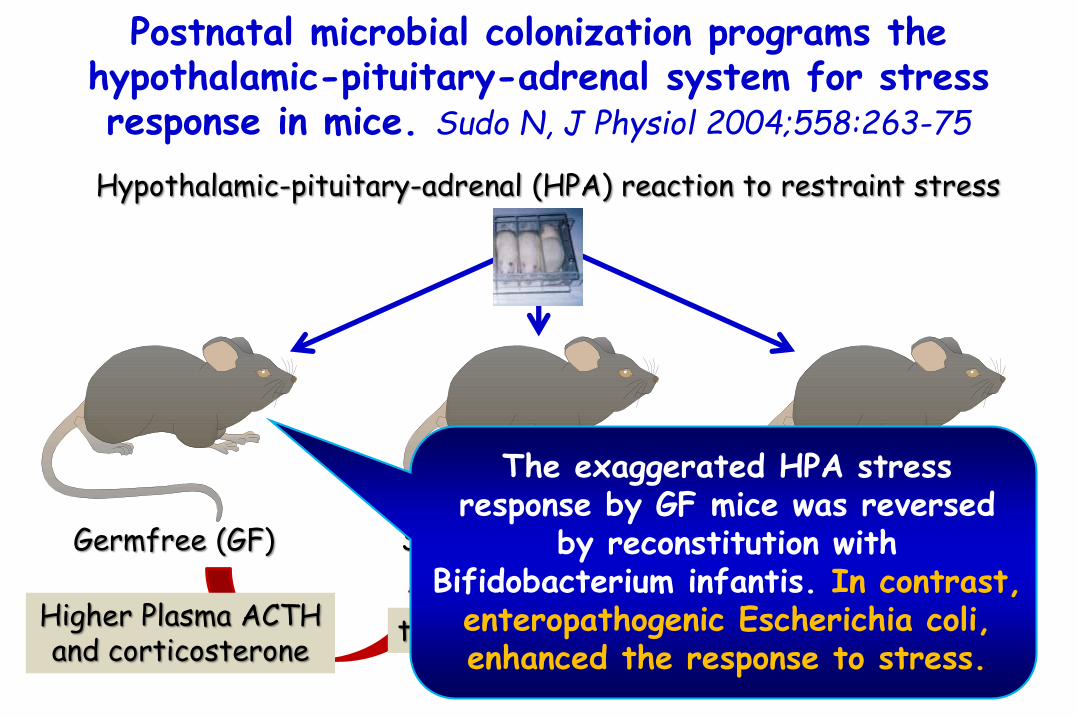
Postnatal microbial colonization programs the hypothalamic-pituitary-adrenal system for stress response in mice. Sudo N, J Physiol 2004;558:263-75
Germfree (GF) Specific pathogen free (SPF)
Gnotobiotic mice
Higher Plasma ACTH and corticosterone
than
Hypothalamic-pituitary-adrenal (HPA) reaction to restraint stress
The exaggerated HPA stress response by GF mice was reversed
by reconstitution with Bifidobacterium infantis. In contrast,
enteropathogenic Escherichia coli, enhanced the response to stress.

Postnatal microbial colonization programs the hypothalamic-pituitary-adrenal system for stress response in mice. Sudo N, J Physiol 2004;558:263-75
Germfree (GF) Specific pathogen free (SPF)
Gnotobiotic mice
Higher Plasma ACTH and corticosterone
than
Hypothalamic-pituitary-adrenal (HPA) reaction to restraint stress
The enhanced HPA response of GF mice was partly corrected by reconstitution with SPF faecesat an early stage, but not by
any reconstitution exerted at a later stage.

Postnatal microbial colonization programs the hypothalamic-pituitary-adrenal system for stress response in mice. Sudo N, J Physiol 2004;558:263-75.
Essentially, in germ-free animals showed reduced expression of the neuronal growth factor BDNF in the cortex and hippocampus, and heightened cortisol stress responses,consistent with patterns seen in depression and anxiety.
This shows that without normal bacteria, ‘germ free’ animals develop not only immune and metabolic dysregulation, but also maladaptive changes in brain function and in regulation of the HPA axis.
Critically, these effects can all be reverse by either giving probiotic bacteria, or by ‘faecaltransplant’ from a normally colonized mouse.Critically, and just as for immune development, timing was critical reversal was only possible at an early stage of development. Once the responses patterns become established with age, they cannot be readily changed.
This is consistent with what we know about ‘critical early periods’ for both immune and neural development and the declining plasticity of neural networks with age. Even in mature animals, disrupting the established normal gut flora with antibiotics can resultin changes in BDNF in the brain and altered behaviour.
Mechanisms: Microbiome
The microbiome has been a major point of attention in research on the gut-brain axis.
Recently, it has been shown that gut bacteria influence CNS development and therefore behavioral and cognitive responses.
For example, germ-free mice expressed decreased anxiety-like behavior, while colonization of these mice early in life, but not as adults, normalized these behavioral deficits.Diaz Heijtz R, Proc Natl Acad Sci U S A 2011:108:3047–52.

Normal gut microbiota modulates brain development and behavior.Diaz Heijtz R, Proc Natl Acad Sci U S A 2011:108:3047–52
Germ free (GF) mice
Increased motor activity and reduced anxiety
than
mice with a normal gut microbiota
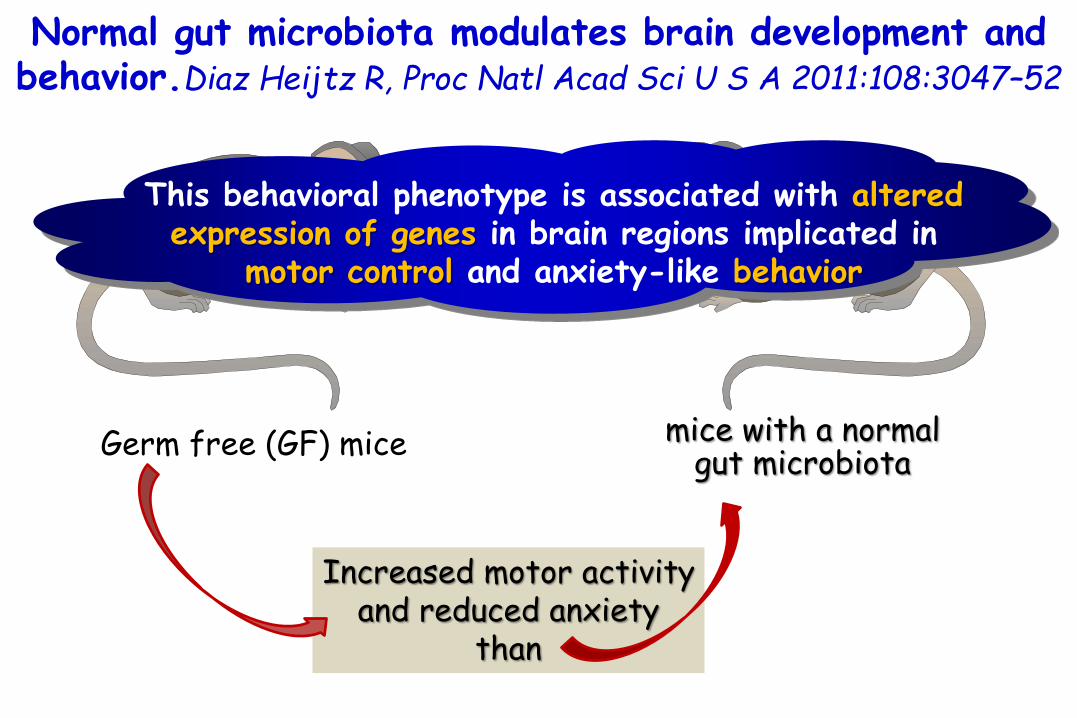
Normal gut microbiota modulates brain development and behavior.Diaz Heijtz R, Proc Natl Acad Sci U S A 2011:108:3047–52
Germ free (GF) mice
Increased motor activity and reduced anxiety
than
This behavioral phenotype is associated with altered expression of genes in brain regions implicated in
motor control and anxiety-like behavior
mice with a normal gut microbiota

Germ free (GF) mice
Exposed to gut microbiota early in life
Normal gut microbiota modulates brain development and behavior.Diaz Heijtz R, Proc Natl Acad Sci U S A 2011:108:3047–52
Display similar characteristics as Specific Pathogen Free mice, including reduced expression of:
PSD-95 and
synaptophysin in the striatum

Germ free (GF) mice
Exposed to gut microbiota early in life
Normal gut microbiota modulates brain development and behavior.Diaz Heijtz R, Proc Natl Acad Sci U S A 2011:108:3047–52
The intestinal microbiota
influences brain chemistry
and behavior.
Display similar characteristics as Specific Pathogen Free mice, including reduced expression of:
PSD-95 and
synaptophysin in the striatum

Germ free (GF) mice
Exposed to gut microbiota early in life
Normal gut microbiota modulates brain development and behavior.Diaz Heijtz R, Proc Natl Acad Sci U S A 2011:108:3047–52
Microbial colonization process initiates signaling mechanisms that affect neuronal circuits involved in motor control
and anxiety behavior.
Display similar characteristics as Specific Pathogen Free mice, including reduced expression of:
PSD-95 and
synaptophysin in the striatum

The impact of microbiota on brain and behavior: mechanisms & therapeutic potential.
Borre YE, Adv Exp Med Biol. 2014;817:373-403.
Alterations in gut microbial composition is associated with marked changes in behaviors relevant to mood, pain and cognition, establishing the critical importance of the bi-directional pathway of communication between the microbiota and the brain in health and disease.
Dysfunction of the microbiome-brain-gut axis has been implicated in stress-related disorders such as depression, anxiety and irritable bowel syndrome and neurodevelopmental disorders such as autism.
Bacterial colonization of the gut is central to postnatal development and maturation of key systems that have the capacity to influence central nervous system (CNS) programming and signaling, including the immune and endocrine systems.
Moreover, there is now expanding evidence for the view that enteric microbiotaplays a role in early programming and later response to acute and chronic stress.

Gut-brain axis: how the microbiome influences anxietyand depression. Foster JA, Trends Neurosci. 2013;36(5):305-12.
Within the first few days of life, humans are colonized by commensalintestinal microbiota.
Microbiota are important in normal healthy brain function and alterations in microbiota influence stress-related behaviors.
Bacteria, including commensal, probiotic, and pathogenic bacteria, in the gastrointestinal (GI) tract can activate neural pathways and central nervous system (CNS) signaling systems.
Ongoing and future animal and clinical studies aimed at understanding the microbiota-gut-brain axis may provide novel approaches for prevention and treatment of mental illness, including anxiety and depression.

Mechanisms: Microbiome
The microbiome has been a major point of attention in research on the gut-brain axis.
Recently, it has been shown that gut bacteria influence CNS development and therefore behavioral and cognitive responses.
For example, germ-free mice expressed decreased anxiety-like behavior, while colonization of these mice early in life, but not as adults, normalized these behavioral deficits.Diaz Heijtz R, Proc Natl Acad Sci U S A 2011:108:3047–52.
This indicates that the microbiome contributes toneurodevelopment, and it is compelling to consider its
influence on ASD and ADHD.

Mechanisms: Microbiome
Several groups have studied the intestinal microbiota of the autistic human population and found differences in composition of Ruminococcus, Bacteroides, and Desulfovibrio genera from the Clostridia, Bacteroidetes, and Proteobacteria classes, respectively.Finegold SM, Clin Infect Dis 2002:35:S6–16.Finegold SM, Anaerobe 2010:16:444–53Parracho HMRT, J Med Microbiol 2005:54:987–91Song Y, Appl Environ Microbiol 2004:70:6459–65.
A recent study demonstrated lower levels of Bifidobacterium and higher levels of Lactobacillus in ASD, both considered to be beneficial bacteria.Adams JB, BMC Gastroenterol 2011:11:22.

Gastrointestinal microflora studies in late-onset autism. Finegold SM, Clin Infect Dis 2002:35:S6–16
Some cases of late-onset (regressive) autism may involve abnormal flora because oral vancomycin, which is poorly absorbed, may lead to significant improvement in these children.
Fecal flora of children with regressive autism compared with that of control children.
The number of clostridialspecies found in the stools of children with autism was greater than in the stools of control children.
Children with autism had 9 species of Clostridium not found in controls, whereas controls yielded only 3 species not found in children with autism.

Gastrointestinal microflora studies in late-onset autism. Finegold SM, Clin Infect Dis 2002:35:S6–16
Possible pathways for bacteria-related autism

Pyrosequencing study of fecal microflora of autistic and control children. Finegold SM, Anaerobe 2010:16:444–53
33 subjects with variousseverities of autism withgastrointestinal symptoms.
7 siblings not showingautistic symptoms(sibling controls).
8 non-sibling controlsubjects.
Bacterial tag encoded FLX amplicon pyrosequencing(bTEFAP) procedure.
Bacteroidetes was found at high levels in the severely autistic group, while
Firmicutes were more predominant in the control group.
Gastrointestinal symptoms
+
-

Pyrosequencing study of fecal microflora of autistic and control children. Finegold SM, Anaerobe 2010:16:444–53
Bacterial composition at the phylum level of all autistic, control and sibling control samples
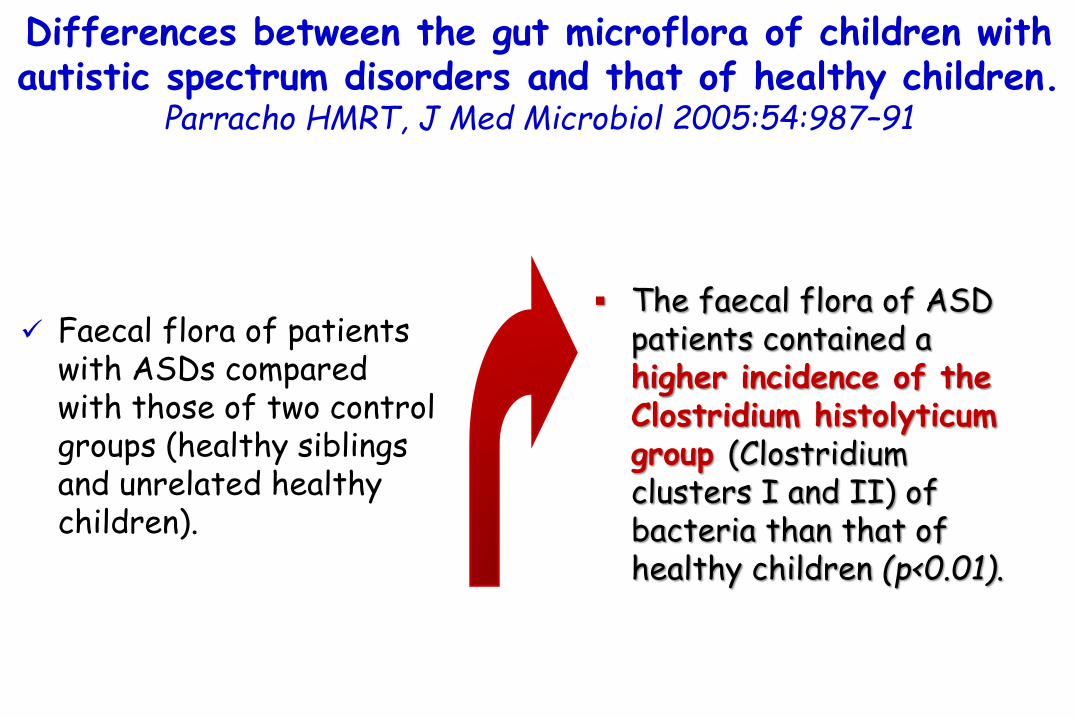
Differences between the gut microflora of children with autistic spectrum disorders and that of healthy children.
Parracho HMRT, J Med Microbiol 2005:54:987–91
Faecal flora of patients with ASDs compared with those of two control groups (healthy siblings and unrelated healthy children).
The faecal flora of ASD patients contained a higher incidence of the Clostridium histolyticumgroup (Clostridium clusters I and II) of bacteria than that of healthy children (p<0.01).

Differences between the gut microflora of children with autistic spectrum disorders and that of healthy children.
Parracho HMRT, J Med Microbiol 2005:54:987–91
Faecal flora of patients with ASDs compared with those of two control groups (healthy siblings and unrelated healthy children).
The faecal flora of ASD patients contained a higher incidence of the Clostridium histolyticumgroup (Clostridium clusters I and II) of bacteria than that of healthy children (p<0.01).
Members of the C. histolyticum group are
recognized toxin-producers and may contribute
towards gut dysfunction, with their metabolic
products also exerting systemic effects.

Differences between the gut microflora of children with autistic spectrum disorders and that of healthy children.
Parracho HMRT, J Med Microbiol 2005:54:987–91
Faecal flora of patients with ASDs compared with those of two control groups (healthy siblings and unrelated healthy children).
However, the non-autistic sibling group had an intermediate level of the C. histolyticum group, which was not significantly different from either of the other subject groups.

Differences between the gut microflora of children with autistic spectrum disorders and that of healthy children.
Parracho HMRT, J Med Microbiol 2005:54:987–91
Faecal flora of patients with ASDs compared with those of two control groups (healthy siblings and unrelated healthy children).
However, the non-autistic sibling group had an intermediate level of the C. histolyticum group, which was not significantly different from either of the other subject groups.
Strategies to reduce clostridial population
levels harboured by ASD patients or to improve their gut microflora
profile through dietary modulation may help to alleviate gut disorders
common in such patients.

Differences between the gut microflora of children with autistic spectrum disorders and that of healthy children.
Parracho HMRT, J Med Microbiol 2005:54:987–91.
GI problems were associated with high levels of clostridia (P < 0.001)
in patients with ASD compared with the unrelated healthy children group, i.e. a significant link was observed between the levels of the C. histolyticum group and GI problems in ASD patients.
Most ASD patients were consuming probiotics (86 %). This suggested that clostridial populations did not appear to be affected by probiotic ingestion.
Clostridia are recognized toxin-producers, including neurotoxins.
Anecdotal reports from parents of autistic children report worsening of behavioural symptoms coinciding with bouts of GI problems.

Differences between the gut microflora of children with autistic spectrum disorders and that of healthy children.
Parracho HMRT, J Med Microbiol 2005:54:987–91.
Previous studies have reported increased resistance of clostridia to severalantimicrobial agents but significant improvements in ASD was demonstrated in children given vancomycin orally.
However, the benefit was short term, with regression noted approximately 2 weeksafter treatment ceased.
These findings may be explained by vancomycin treatment reducing the Clostridium population, but due to the persistence of spores the clostridial levels return once treatment has stopped.
Since orally administered vancomycin is only minimally absorbed, it is likely that theeffect is mediated, in some way, through vancomycin activity on intestinal bacteria.
Thus, it has been suggested that the short-termbenefit from vancomycin treatment might be due to the temporary elimination of neurotoxin-producing micro-organisms.

Gastrointestinal flora and gastrointestinal status in children with autism–comparisons to typical children and
correlation with autism severity. Adams JB, BMC Gastroenterol 2011:11:22.
Autism severity was assessed with the Autism TreatmentEvaluation Checklist (ATEC), an instrument which was designed to provide a quantitative assessment ofautism severity.
It is composed of four subscales:
1) speech/language/communication, 2) sociability, 3) sensory/cognitive awareness, and 4) health/physical behavior.The sum of the scores for each subscale gives the total ATEC score.Rimland B, Edelson S: Autism Treatment Evaluation Checklist: Statistical Analyses. Autism Research Institute, San Diego, CA; 2000.

Gastrointestinal flora and gastrointestinal status in children with autism–comparisons to typical children and
correlation with autism severity. Adams JB, BMC Gastroenterol 2011:11:22.
Gastrointestinal symptoms were assessed using a modifiedversion of the GI Severity Index.
Specifically, we included only the first six items (constipation, diarrhea, stool consistency, stool smell, flatulence, andabdominal pain), but did not include “unexplained daytime irritability”, “nighttime awakening,” or “abdominal tenderness.”
We call this shortened version the 6-GI Severity Index (6-GSI).Schneider CK, Journal Autism Developmental Disorders 2006, 36(8):1053-64.
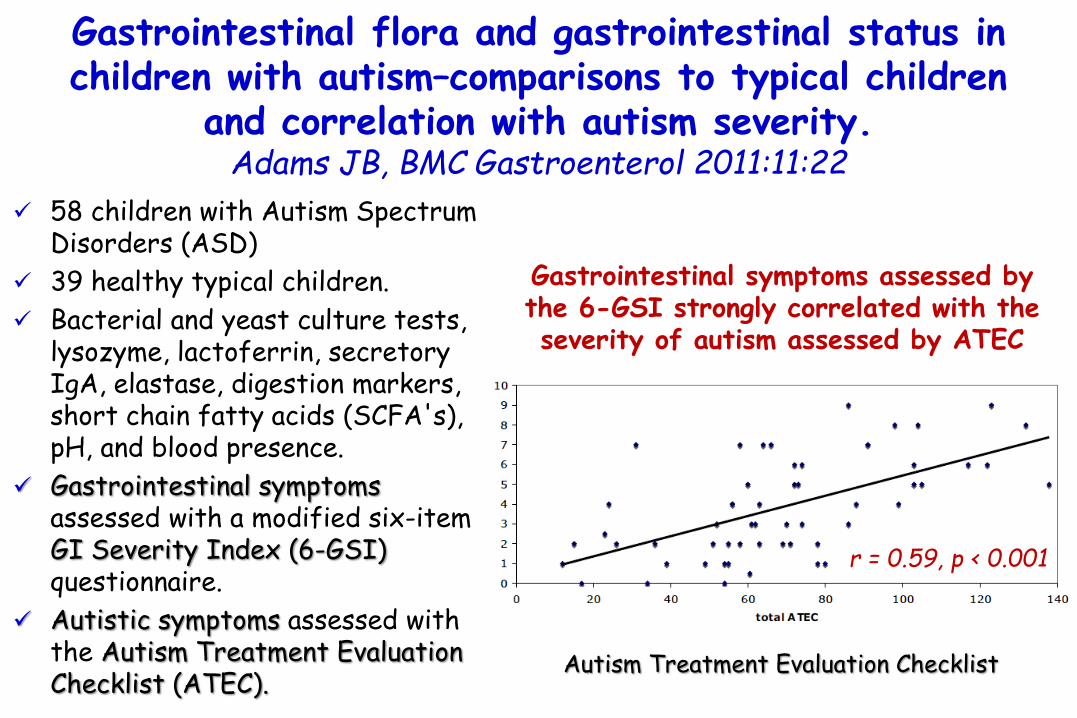
58 children with Autism SpectrumDisorders (ASD)
39 healthy typical children.
Bacterial and yeast culture tests, lysozyme, lactoferrin, secretoryIgA, elastase, digestion markers, short chain fatty acids (SCFA's), pH, and blood presence.
Gastrointestinal symptomsassessed with a modified six-itemGI Severity Index (6-GSI) questionnaire.
Autistic symptoms assessed withthe Autism Treatment EvaluationChecklist (ATEC).
Gastrointestinal flora and gastrointestinal status in children with autism–comparisons to typical children
and correlation with autism severity. Adams JB, BMC Gastroenterol 2011:11:22
Gastrointestinal symptoms assessed by the 6-GSI strongly correlated with the severity of autism assessed by ATEC
r = 0.59, p < 0.001
Autism Treatment Evaluation Checklist

Gastrointestinal flora and gastrointestinal status in children with autism–comparisons to typical children
and correlation with autism severity. Adams JB, BMC Gastroenterol 2011:11:22
children withautism
Species of Bifidobacter-20
-10 –
-20 –
-30 –
-40 –
-50 –
p=0.002
-43%
58 children with Autism SpectrumDisorders (ASD)
39 healthy typical children.
Bacterial and yeast culture tests, lysozyme, lactoferrin, secretoryIgA, elastase, digestion markers, short chain fatty acids (SCFA's), pH, and blood presence.
Gastrointestinal symptomsassessed with a modified six-itemGI Severity Index (6-GSI) questionnaire.
Autistic symptoms assessed withthe Autism Treatment EvaluationChecklist (ATEC).
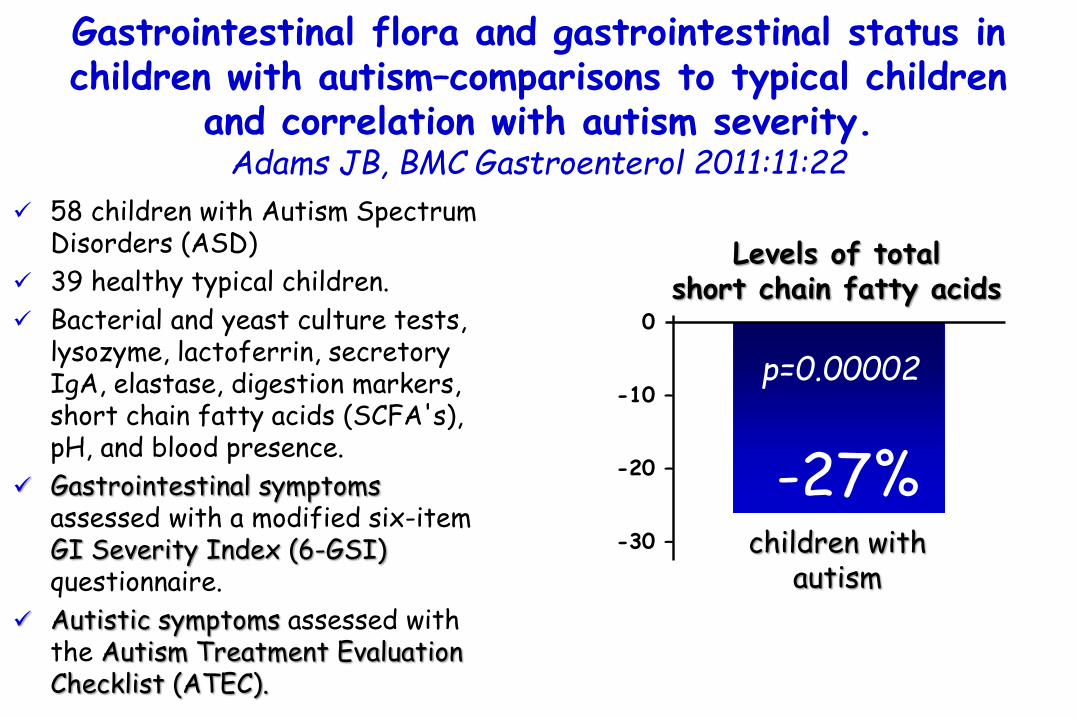
Gastrointestinal flora and gastrointestinal status in children with autism–comparisons to typical children
and correlation with autism severity. Adams JB, BMC Gastroenterol 2011:11:22
children withautism
-20
-10 –
-20 –
-30 –
p=0.00002
-27%
Levels of total short chain fatty acids
58 children with Autism SpectrumDisorders (ASD)
39 healthy typical children.
Bacterial and yeast culture tests, lysozyme, lactoferrin, secretoryIgA, elastase, digestion markers, short chain fatty acids (SCFA's), pH, and blood presence.
Gastrointestinal symptomsassessed with a modified six-itemGI Severity Index (6-GSI) questionnaire.
Autistic symptoms assessed withthe Autism Treatment EvaluationChecklist (ATEC).

58 children with Autism SpectrumDisorders (ASD)
39 healthy typical children.
Bacterial and yeast culture tests, lysozyme, lactoferrin, secretoryIgA, elastase, digestion markers, short chain fatty acids (SCFA's), pH, and blood presence.
Gastrointestinal symptomsassessed with a modified six-itemGI Severity Index (6-GSI) questionnaire.
Autistic symptoms assessed withthe Autism Treatment EvaluationChecklist (ATEC).
Gastrointestinal flora and gastrointestinal status in children with autism–comparisons to typical children
and correlation with autism severity. Adams JB, BMC Gastroenterol 2011:11:22
children withautism
-20
-10 –
-20 –
-30 –
p=0.00002
-27%
The low level of short chain fatty
acids was partly due to either lower
production and/or lower intake of soluble fiber.
Levels of total short chain fatty acids
Mechanisms: Microbiome
Interestingly, antibiotic treatment for ASD children not only led to GI improvements, but also improvements in cognitive skills.Sandler RH, J Child Neurol 2000:15:429–35.
However, more research on the microbiome of children with ASD is required to understand the role of a microbial factor in ASD.
De Theije CGM, Pediatr Allergy Imm 2014;25:218

Short-term benefit from oral vancomycin treatment of regressive-onset autism.
Sandler RH, J Child Neurol 2000:15:429–35
Short-term improvement was noted using multiple pre- and post-therapy evaluations (videotapes scored by a clinical psychologist).
Unfortunately, these gains had largely waned at follow-up.
In most cases symptoms of autism begin in early infancy.
However, a subset of children appears to develop normally until a clear deterioration is observed ("regressive"-onset autism).
11 children with regressive-onset autism.
a minimally absorbed oral antibiotic Vancomicin(500 mg/6ml = 2 ml x 3 times/day)

Mechanisms: Microbiome
To our knowledge, no studies have been published on the microbial status of children with ADHD.
Investigating the microbial composition of children with ADHD could lead to new insights on the effects of food or food allergy on behavior in these patients.
Interestingly and very recent, the first proof in human showing that the microbiome–gut–brain axis exists has been reported.
De Theije CGM, Pediatr Allergy Imm 2014;25:218

FMPP intake (Bifidobacterium animalis subsp
Lactis, Streptococcus thermophiles, Lactobacillus bulgaricus, and
Lactococcus lactis subsp Lactis)
was associated with reduced task-related response of a
distributed functional network
(49% cross-block covariance; P = 0.004) containing affective,
viscerosensory, and somatosensory cortices.
Healthy women with no gastrointestinal or psychiatric symptoms were randomly assigned to groups given: 1)fermented milk product with probiotic(FMPP) (n = 12), 2)a nonfermented milk product (n = 11, controls), or 3)no intervention (n = 13) twice daily for 4 weeks.
Functional magnetic resonance imaging before and after the intervention to measure brain response to an emotional faces attention task and resting brain activity.
Consumption of fermented milk product with probiotic(FMPP) modulates brain activity.
Tillisch K, Gastroenterology 2013:144:1394–401.

Alterations in intrinsic activity of resting brain
indicated that ingestion of FMPP was associated with
changes in midbrain connectivity, which could
explain the observed differences in activity
during the task.
Healthy women with no gastrointestinal or psychiatric symptoms were randomly assigned to groups given: 1)fermented milk product with probiotic(FMPP) (n = 12), 2)a nonfermented milk product (n = 11, controls), or 3)no intervention (n = 13) twice daily for 4 weeks.
Functional magnetic resonance imaging before and after the intervention to measure brain response to an emotional faces attention task and resting brain activity.
Consumption of fermented milk product with probiotic(FMPP) modulates brain activity.
Tillisch K, Gastroenterology 2013:144:1394–401.

Healthy women with no gastrointestinal or psychiatric symptoms were randomly assigned to groups given: 1)fermented milk product with probiotic(FMPP) (n = 12), 2)a nonfermented milk product (n = 11, controls), or 3)no intervention (n = 13) twice daily for 4 weeks.
Functional magnetic resonance imaging before and after the intervention to measure brain response to an emotional faces attention task and resting brain activity.
Alterations in intrinsic activity of resting brain
indicated that ingestion of FMPP was associated with
changes in midbrain connectivity, which could
explain the observed differences in activity
during the task.
Four-week intake of an FMPP by healthy women
affected activity of brain regions that control central
processing of emotion and sensation.
Consumption of fermented milk product with probiotic(FMPP) modulates brain activity.
Tillisch K, Gastroenterology 2013:144:1394–401.

FMPP was a fermented milk containing Bifidobacterium animalis subsplactis (strain number I-2494 in French National Collection of Cultures of Micro-organisms
(CNCM, Paris, France), referred as DN-173 010 in a previous publication,23 together with the 2 classical yogurt starters, Streptococcus thermophilus (CNCM strain
number I-1630) and Lactobacillus bulgaricus (CNCM strain numbers I-1632 and I-
1519), and Lactococcus lactis subsp lactis (CNCM strain number I-1631). The test product contains 1.25 × 1010 colonyforming units of B lactis CNCM I-2494/DN-173 010 per cup and 1.2 × 109 colony-forming units/cup of S thermophilus and L bulgaricus. The nonfermented Control milk product was a milk-based nonfermented dairy product without probiotics and with a lactose content of <4 g/cup, which is similar to the content of lactose in the test product. The Control product was matched for color, texture, taste, calories, protein, and lipid content to the FMPP. Both products were provided in 125-g pot, consumed twice daily.
The product was prepared at Danone Research facilities
Consumption of fermented milk product with probiotic(FMPP) modulates brain activity.
Tillisch K, Gastroenterology 2013:144:1394–401.

Healthy women with no gastrointestinal or psychiatric symptoms were randomly assigned to groups given: 1) fermented milk product with probiotic
(FMPP) (n = 12), 2) a nonfermented milk product
(n = 11, controls), or 3) no intervention (n = 13) twice daily for 4 weeks.
Functional magnetic resonance imaging before and after the intervention to measure brain response to an emotional faces attention task and resting brain activity.
in healthy women, chronic ingestion of
several strains of gut bacteria by fermented
milk, including Bifidobacterium
and Lactobacillus, reduced activity of
brain regionsinvolved in processing
of emotion and sensation.
Consumption of fermented milk product with probiotic(FMPP) modulates brain activity.
Tillisch K, Gastroenterology 2013:144:1394–401.

A distributed network of brain regions showing decreases in the FMPP group during the emotional faces attention task is shown in the shaded regions.
Three regions of interest selected from the network for study in the resting state are highlighted inpink (insula), green(periaqueductal gray), blue (somatosensoryregions).
Consumption of fermented milk product with probiotic(FMPP) modulates brain activity.
Tillisch K, Gastroenterology 2013:144:1394–401.

Brain regions showing reduced activity in response to an
emotional faces attention taskafter fermented milk product
with probiotic (FMPP) intervention are shown, with
significant regions demarcated.
Consumption of fermented milk product with probiotic(FMPP) modulates brain activity.
Tillisch K, Gastroenterology 2013:144:1394–401.

A resting-state midbrain centered network has strong positive correlation with midbrain emotional reactivity after No-Intervention, is not engaged after Control, and is negatively correlated with midbrain activity after FMPP. This suggests
a shift away from an arousal based resting-state network and toward a regulatory network. Network regions are depicted in (A). Red regions show areas that are positively correlated with midbrain activity in the No-Intervention group and
negatively correlated in the FMPP group. Green regions are negatively correlated with midbrain activity in the No-Intervention group and are positively correlated in the FMPP group. (B)
Consumption of fermented milk product with probiotic(FMPP) modulates brain activity.
Tillisch K, Gastroenterology 2013:144:1394–401.

A resting-state midbrain centered network has strong positive correlation with midbrain emotional reactivity after No-Intervention, is not engaged after Control, and is negatively correlated with midbrain activity after FMPP. This suggests a shift away from an arousal based resting-state network and toward
a regulatory network. Network regions are depicted in (A). Red regions show areas that are positively correlated with midbrain activity in the No-Intervention group and negatively correlated in the FMPP
group. Green regions are negatively correlated with midbrain activity in the No-Intervention group and are positively correlated in the FMPP group. (B)
Consumption of fermented milk product with probiotic(FMPP) modulates brain activity.
Tillisch K, Gastroenterology 2013:144:1394–401.

Mechanisms: Microbiome
Several possible mechanisms have been proposed in which the microbiomecan modulate brain activity.
Preclinical models indicate that themicrobiome can signal to the brain via vagal afferent nerves and the nucleus tractus solitarius (NTS). Mayer EA. Nat Rev Neurosci 2011:12:453–66.
This signaling could be mediated by direct communication of microbiota with the intestinal epithelium and serotonin producingenterochromaffin cells, affecting the Enteric Nervous System and immune system.
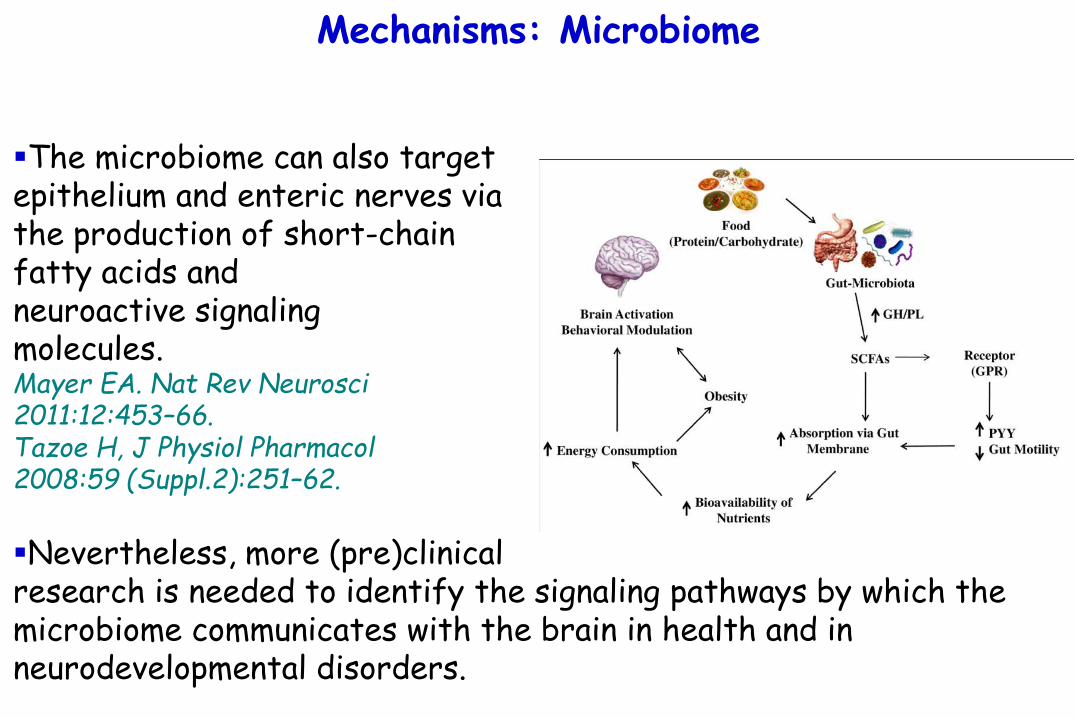
Mechanisms: Microbiome
The microbiome can also target epithelium and enteric nerves via the production of short-chain fatty acids and neuroactive signaling molecules.Mayer EA. Nat Rev Neurosci2011:12:453–66.Tazoe H, J Physiol Pharmacol2008:59 (Suppl.2):251–62.
Nevertheless, more (pre)clinical research is needed to identify the signaling pathways by which the microbiome communicates with the brain in health and in neurodevelopmental disorders.

Food Allergy and the Brain
Attilio BonerUniversity ofVerona, Italy
Introduction
Micronutrients and Behaviour
Immunity & Ipersensitivity
Food Allergy&Ipersensitivity and Brain
Not only Food Allergy but also…
Which came first?
Possible Mechanisms
Food-based Therapies
Conclusions

Food-based therapies
If children with a genetic pre-disposition are more susceptible to develop ASD or ADHD when exposed to an allergic immune challenge, allergen-free diets and immunomodulatory dietary interventions could be beneficial for the treatment of behavior.
Indeed, many ASD patients and ADHD patients are using complementary and alternative medicine (CAM).
Levy SE, Pediatr Ann 2003:32:685–91.Sinha D, J Paediatr Child Health 2005:41:23–6.
De Theije CGM, Pediatr Allergy Imm 2014;25:218

Food allergy and autism spectrum disorders: is there a link? Jyonouchi H. Curr Allergy Asthma Rep 2009:9:194–201
Gastrointestinal (GI) symptoms are common comorbidities in children with autism spectrum disorders (ASDs). Parents often attribute these GI symptoms to food allergy (FA), although an evaluation for IgE-mediated FA is often unrevealing. Our previous studies indicated a high prevalence of non-IgE-mediated FA in young children with ASDs. Therefore, non-IgE-mediated FA may account for some but not all GI symptoms observed in children with ASDs. This raises the question of what treatment measures are applicable to ASD children with GI symptoms. A wide variety of dietary supplements and dietary intervention measures for ASD children have been promoted by medical professionals practicing complementary and alternative medicine despite the lack of rigorous scientific validation in most instances. This review summarizes possible (or proposed) etiologies of GI symptoms in ASD children and discusses risks and possible benefits of intervention measures promoted by complementary and alternative practitioners, with emphasis on FA
Use of complementary and alternative treatments for children with autistic spectrum disorders is increasing.
Levy SE, Pediatr Ann 2003:32:685–91.
A recent web search using "autism and detoxification“ resulted in almost 8,000 sites.
The Defeat Autism Now! (DAN!) Project arose in 1995 from collaboration of members of the Autism Research Institute.
The DAN! Project advocates a specific and extensive protocol for diagnosis and treatment and can be viewed at http://www.autism.com/ari/#dan.
The scientific validation and support for many interventions is incomplete and disparate from the recommendation in the American Academy of Pediatrics Policy Statement.

Use of complementary and alternative treatments for children with autistic spectrum disorders is increasing.
Levy SE, Pediatr Ann 2003:32:685–91.
A recent web search using "autism and detoxification“ resulted in almost 8,000 sites.
The Defeat Autism Now! (DAN!) Project arose in 1995 from collaboration of members of the Autism Research Institute.
The DAN! Project advocates a specific and extensive protocol for diagnosis and treatment and can be viewed at http://www.autism.com/ari/#dan.
The scientific validation and support for many interventions is incomplete and disparate from the recommendation in the American Academy of Pediatrics Policy Statement.
Families should be encouraged to discuss all proposed investigations or treatments they wish to
try with their primary care provider

Complementary and alternative medicine use in children with attention deficit hyperactivity disorder.
Sinha D, J Paediatr Child Health 2005:41:23–6
Current or past CAM use
67.6%
% families reporting
64% CAM use in a clinical
sample of children with ADHD.
75 patients aged5-17 years.
Informed their paediatrician of their CAM use
70 –
60 –
50 –
40 –
30 –
20 –
10 –
0
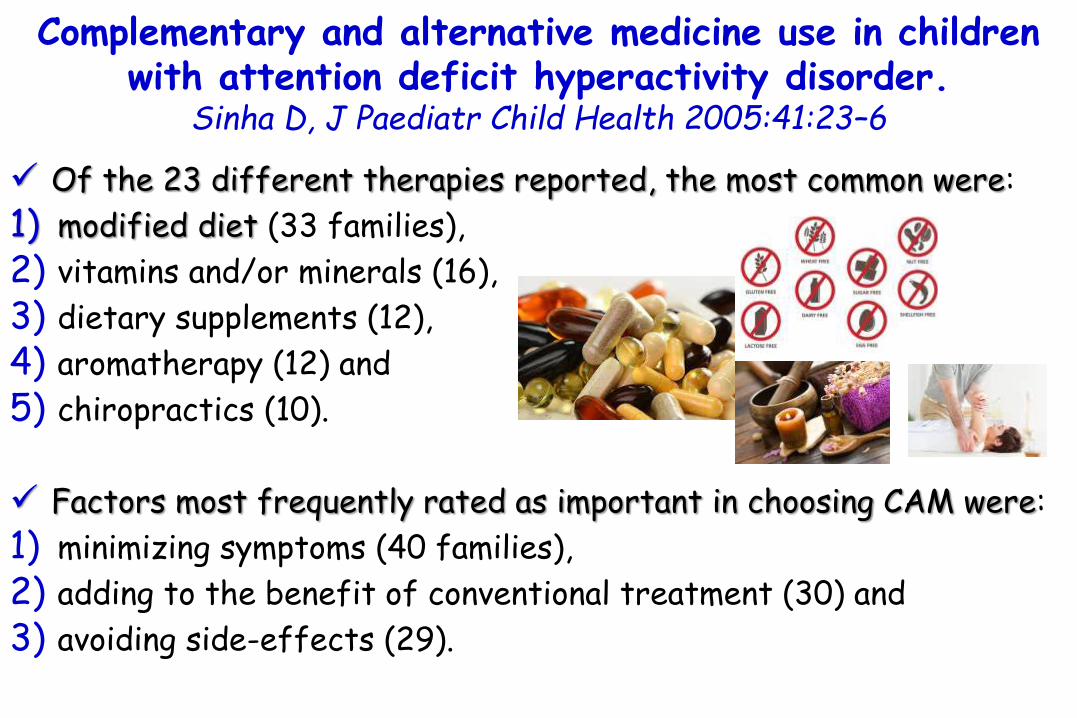
Complementary and alternative medicine use in children with attention deficit hyperactivity disorder.
Sinha D, J Paediatr Child Health 2005:41:23–6
Of the 23 different therapies reported, the most common were:
1) modified diet (33 families),
2) vitamins and/or minerals (16),
3) dietary supplements (12),
4) aromatherapy (12) and
5) chiropractics (10).
Factors most frequently rated as important in choosing CAM were:
1) minimizing symptoms (40 families),
2) adding to the benefit of conventional treatment (30) and
3) avoiding side-effects (29).

Food-based therapies
If children with a genetic pre-disposition are more susceptible to develop ASD or ADHD when exposed to an allergic immune challenge, allergen-free diets and immunomodulatory dietary interventions could be beneficial for the treatment of behavior.
Indeed, approximately 30% of ASD patients and 12% of ADHD patients are using complementary and alternative medicine (CAM).Levy SE, Pediatr Ann 2003:32:685–91.Sinha D, J Paediatr Child Health 2005:41:23–6.
Examples of such treatmentsinclude the exclusion of
hyperallergenic foods and use ofpolyunsaturated fatty acids
(PUFAs), vitamins, and mineralsupplements.

Food-based therapies
Both in ASD and ADHD, elimination diets have received most attention.
still under debate!
exclusion ofhyperallergenic foods
was claimed to be beneficial in multiple studies
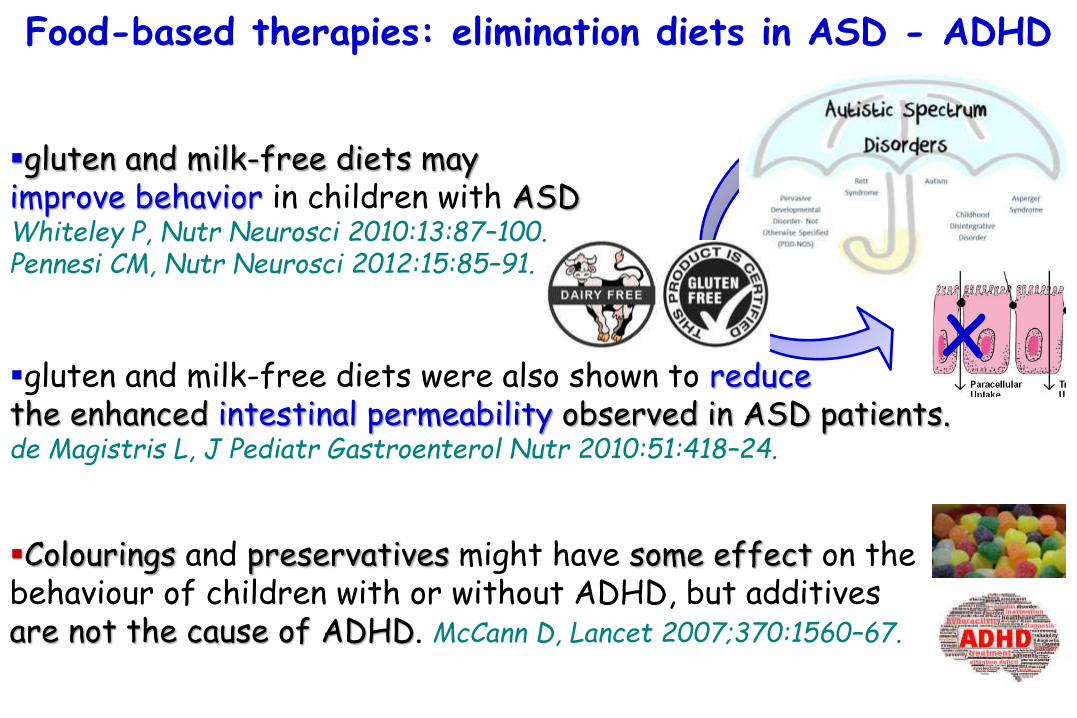
Food-based therapies: elimination diets in ASD - ADHD
gluten and milk-free diets mayimprove behavior in children with ASDWhiteley P, Nutr Neurosci 2010:13:87–100.Pennesi CM, Nutr Neurosci 2012:15:85–91.
gluten and milk-free diets were also shown to reducethe enhanced intestinal permeability observed in ASD patients.de Magistris L, J Pediatr Gastroenterol Nutr 2010:51:418–24.
Colourings and preservatives might have some effect on the behaviour of children with or without ADHD, but additives are not the cause of ADHD. McCann D, Lancet 2007;370:1560–67.
x

The ScanBrit randomised, controlled, single-blind study of a gluten- and casein free dietary intervention for
children with autism spectrum disorders. Whiteley P, Nutr Neurosci 2010:13:87–100
72 Danish children (aged 4 years to 10 years) assigned to diet (n=26) or non-diet (n=29).
Autism Diagnostic Observation Schedule (ADOS) and the Gilliam Autism Rating Scale (GARS) to assess core autism behaviours.
Vineland Adaptive Behaviour Scales (VABS) to ascertain developmental level, and Attention-Deficit Hyperactivity Disorder - IV scale (ADHD-IV) to determine inattention and hyperactivity.

The ScanBrit randomised, controlled, single-blind study of a gluten- and casein free dietary intervention for
children with autism spectrum disorders. Whiteley P, Nutr Neurosci 2010:13:87–100
At 12 months there was a significant improvement in the diet group on sub-domains of:
1) ADOS,
2) GARS and
3) ADHD-IV measures.
55 Danish children (4-10 years) assigned to diet (n=26) or non-diet (n=29).
Autism Diagnostic Observation Schedule (ADOS) and the Gilliam Autism Rating Scale (GARS) to assess core autism behaviours.
Vineland Adaptive Behaviour Scales (VABS) to ascertain developmental level, and Attention-Deficit Hyperactivity Disorder - IV scale (ADHD-IV) to determine inattention and hyperactivity.
X

The ScanBrit randomised, controlled, single-blind study of a gluten- and casein free dietary intervention for
children with autism spectrum disorders. Whiteley P, Nutr Neurosci 2010:13:87–100
At 12 months there was a significant improvement in the diet group on sub-domains of:
1) ADOS,
2) GARS and
3) ADHD-IV measures.
55 Danish children (4-10 years) assigned to diet (n=26) or non-diet (n=29).
Autism Diagnostic Observation Schedule (ADOS) and the Gilliam Autism Rating Scale (GARS) to assess core autism behaviours.
Vineland Adaptive Behaviour Scales (VABS) to ascertain developmental level, and Attention-Deficit Hyperactivity Disorder - IV scale (ADHD-IV) to determine inattention and hyperactivity.
Our results suggest that dietary
intervention may positively affect
developmental outcome for some children
diagnosed with ASD.
X

The ScanBrit randomised, controlled, single-blind study of a gluten- and casein free dietary intervention for
children with autism spectrum disorders. Whiteley P, Nutr Neurosci 2010:13:87–100
At 12 months there was a significant improvement in the diet group on sub-domains of:
1) ADOS,
2) GARS and
3) ADHD-IV measures.
55 Danish children (4-10 years) assigned to diet (n=26) or non-diet (n=29).
Autism Diagnostic Observation Schedule (ADOS) and the Gilliam Autism Rating Scale (GARS) to assess core autism behaviours.
Vineland Adaptive Behaviour Scales (VABS) to ascertain developmental level, and Attention-Deficit Hyperactivity Disorder - IV scale (ADHD-IV) to determine inattention and hyperactivity.
In the absence of a placebo condition to the current investigation, we are, however, unable to
disqualify potential effects derived from intervention outside of
dietary changes.
X
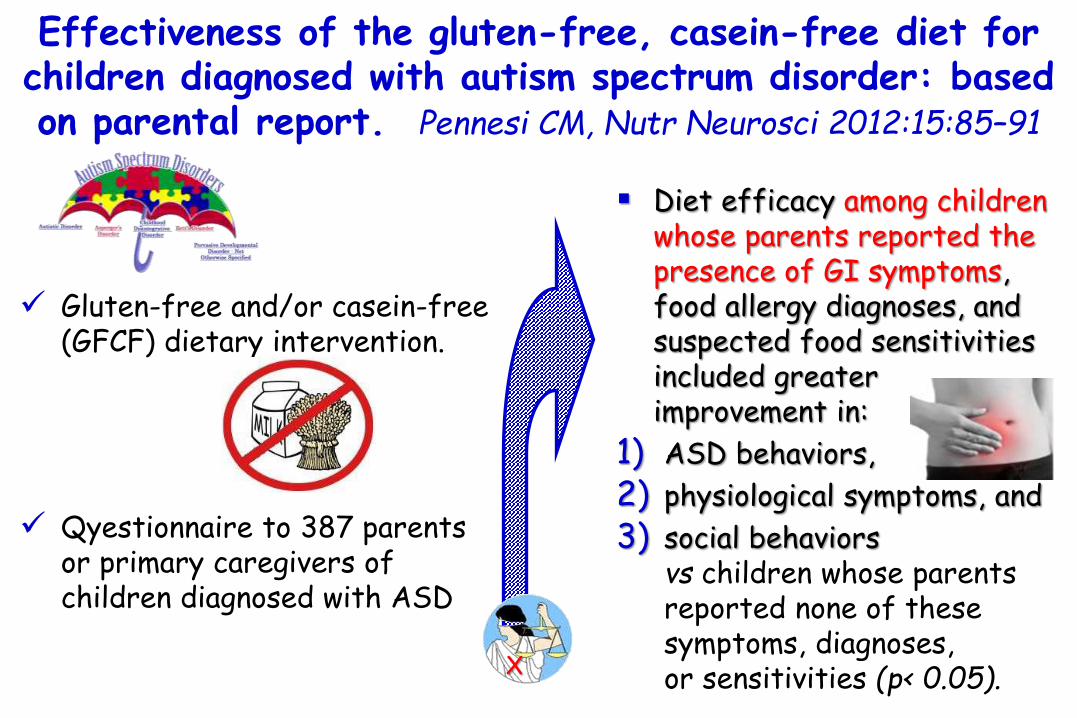
Effectiveness of the gluten-free, casein-free diet for children diagnosed with autism spectrum disorder: basedon parental report. Pennesi CM, Nutr Neurosci 2012:15:85–91
Diet efficacy among children whose parents reported the presence of GI symptoms, food allergy diagnoses, and suspected food sensitivities included greater improvement in:
1) ASD behaviors,
2) physiological symptoms, and
3) social behaviors vs children whose parents reported none of these symptoms, diagnoses, or sensitivities (p< 0.05).
Gluten-free and/or casein-free (GFCF) dietary intervention.
Qyestionnaire to 387 parents or primary caregivers of children diagnosed with ASD
X

Effectiveness of the gluten-free, casein-free diet for children diagnosed with autism spectrum disorder: basedon parental report. Pennesi CM, Nutr Neurosci 2012:15:85–91
Diet efficacy among children whose parents reported the presence of GI symptoms, food allergy diagnoses, and suspected food sensitivities included greater improvement in:
1) ASD behaviors,
2) physiological symptoms, and
3) social behaviors vs children whose parents reported none of these symptoms, diagnoses, or sensitivities (p< 0.05).
Gluten-free and/or casein-free (GFCF) dietary intervention.
Qyestionnaire to 387 parents or primary caregivers of children diagnosed with ASD
X
GI and immune factors may play a role in differentiating diet responders from
diet non-responders.

Alterations of the intestinal barrier in patients with autism spectrum disorders and in their first-degree relatives.
de Magistris L, J Pediatr Gastroenterol Nutr 2010:51:418–24
Constipation
45.5%
% gastrointestinal symptomsin children with autism
Intestinal symptoms & permeability (IPT) in patients with autism as well as in their first-degree relatives.
To investigate leaky gut hypothesis.
Faecal calprotectin(FC). Diarrhoea
50 –
40 –
30 –
20 –
10 –
00 Abdominalpain
34.1%
15.9%

Alterations of the intestinal barrier in patients with autism spectrum disorders and in their first-degree relatives.
de Magistris L, J Pediatr Gastroenterol Nutr 2010:51:418–24
Patients withautism
24.4%
% subjects with elevated Fecal Calprotectin
11.6%
Their relatives
25 –
20 –
15 –
10 –
05 –
00
Intestinal symptoms & permeability (IPT) in patients with autism as well as in their first-degree relatives.
To investigate leaky gut hypothesis.
Faecal calprotectin(FC).

Alterations of the intestinal barrier in patients with autism spectrum disorders and in their first-degree relatives.
de Magistris L, J Pediatr Gastroenterol Nutr 2010:51:418–24
Patients withautism
24.4%
% subjects with elevated Fecal Calprotectin
11.6%
Their relatives
25 –
20 –
15 –
10 –
05 –
00
Intestinal symptoms & permeability (IPT) in patients with autism as well as in their first-degree relatives.
To investigate leaky gut hypothesis.
Faecal calprotectin(FC).
FC elevated was not, correlated with abnormal
intestinalpermeability
values.
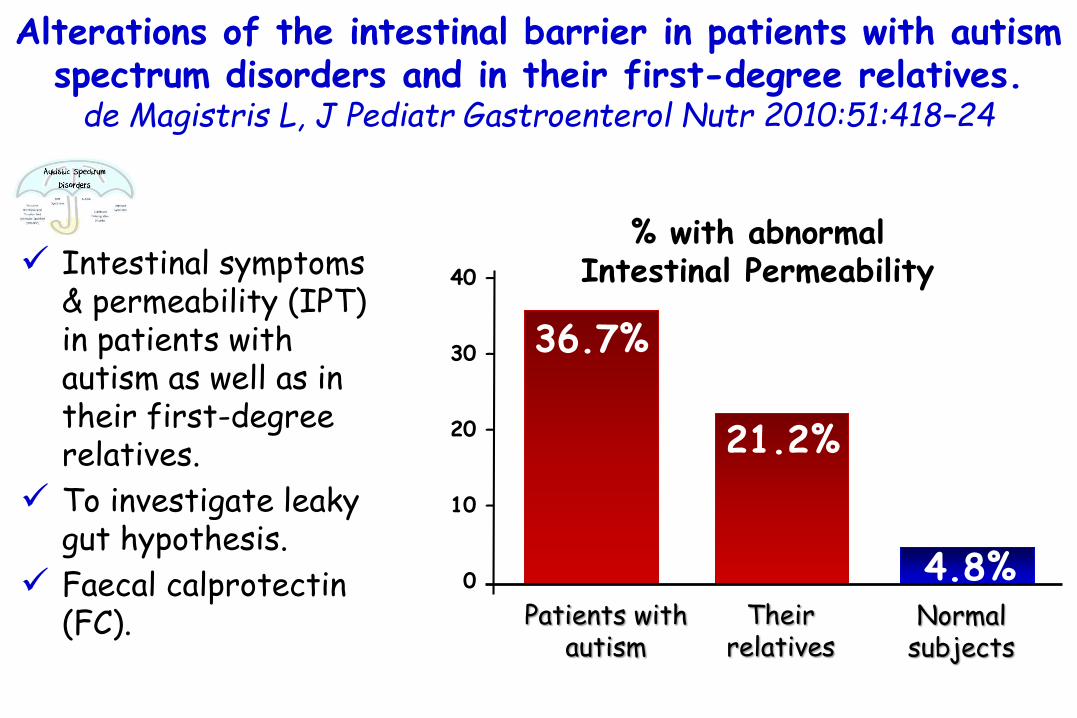
Alterations of the intestinal barrier in patients with autism spectrum disorders and in their first-degree relatives.
de Magistris L, J Pediatr Gastroenterol Nutr 2010:51:418–24
Patients withautism
36.7%
% with abnormal Intestinal Permeability
Theirrelatives
40 –
30 –
20 –
10 –
00
Normalsubjects
21.2%
4.8%
Intestinal symptoms & permeability (IPT) in patients with autism as well as in their first-degree relatives.
To investigate leaky gut hypothesis.
Faecal calprotectin(FC).

Alterations of the intestinal barrier in patients with autism spectrum disorders and in their first-degree relatives.
de Magistris L, J Pediatr Gastroenterol Nutr 2010:51:418–24
Patients withautism
36.7%
% with abnormal Intestinal Permeability
Theirrelatives
40 –
30 –
20 –
10 –
00
Normalsubjects
21.2%
4.8%
Intestinal symptoms & permeability (IPT) in patients with autism as well as in their first-degree relatives.
To investigate leaky gut hypothesis.
Faecal calprotectin(FC).
Patients with autism on a
gluten-casein-free diet had significantly
lower IPT values compared with those
who were on an unrestricted diet and
controls.

Food-based therapies: elimination diets in ASD - ADHD
gluten and milk-free diets mayimprove behavior in children with ASD Whiteley P, Nutr Neurosci 2010:13:87–100.Pennesi CM, Nutr Neurosci 2012:15:85–91.
gluten and milk-free diets were also shown to reduce the enhanced intestinal permeability observed in ASD patients.de Magistris L, J Pediatr Gastroenterol Nutr 2010:51:418–24.
Colourings and preservatives might have some effect on the behaviour of children with or without ADHD, but additives are not the cause of ADHD. McCann D, Lancet 2007;370:1560–67.
However, large double-blind and well-controlled trials are required to strengthen these observations.

Food-based therapies: elimination diets in ADHD
1) cow’s milk,
2) wheat,
3) egg,
4) chocolate,
5) cheese,
6) nuts, and
7) citrus fruits.
8) Food additives
Foods that are often
eliminated are
De Theije CGM, Pediatr Allergy Imm 2014;25:218

Food-based therapies: elimination diets in ADHD
Two early studies reported that behavioral symptoms improved in children with ADHD (1, 2).
1) Egger J, Lancet 1985:1:540–5 . 2) Carter CM, Arch Dis Child 1993:69:564–8.

Controlled trial of oligoantigenic treatment in the hyperkinetic syndrome. Egger J, Lancet 1985:1:540–5.
Improved
81.5%
28%
Reached a normalrange of behaviour
76 selected overactive children.
Treated with an oligoantigenic diet.
(62/76) (21/76)
90 –
80 –
70 –
60 –
50 –
40 –
30 –
20 –
10 –
00
% children who
of the children who improved completed a double-blind, crossover, placebo-controlled challenge in which foods thought to provoke symptoms were reintroduced.
Symptoms returned or were exacerbated much more often when patients were on active material than on placebo.
48 foods were incriminated.
Artificial colorants and preservatives were the commonest provoking substances, but no child was sensitive to these alone.
Controlled trial of oligoantigenic treatment in the hyperkinetic syndrome. Egger J, Lancet 1985:1:540–5.

The children were put on a restricted (or 'few foods') diet for a period of 3 to 4 weeks.
The foods allowed were typically two meats (often lamb and turkey), two carbohydrate sources (rice and potato), two fruits (often banana and pear), a range of root and green vegetables, bottled water, sunflower oil, and milk free margarine.
Carter CM, Human Nutrition: Applied Nutrition1985; 39A: 294-303
If there was no improvement by the end of the 2° week the diet was changed or further restricted for the last week.
Effects of a few food diet in attention deficit disorder. Carter CM, Arch Dis Child 1993:69:564–8.
?

Effects of a few food diet in attention deficit disorder. Carter CM, Arch Dis Child 1993:69:564–8.
78 children referred because of hyperactive behaviour.
Placed on a 'few foods' elimination diet.
Conners’ behaviouralrating scale of parents.
80 –
70 –
60 –
50 –
40 –
30 –
20 –
10 –
00
% children improving in behaviourduring this open trial
75.6%(59/78)

Effects of a few food diet in attention deficit disorder. Carter CM, Arch Dis Child 1993:69:564–8.
75.6%
80 –
70 –
60 –
50 –
40 –
30 –
20 –
10 –
00
(59/78)
in 19/59 (32%) of these children it was possible to disguise foods and/or additives that
reliably provoked behaviouralproblems in a placebo controlled
double blind challenge.
% children improving in behaviourduring this open trial 78 children referred
because of hyperactive behaviour.
Placed on a 'few foods' elimination diet.
Conners’ behaviouralrating scale of parents.
X

≥ 1 Additive containing
foods
Foods most commonly implicated during open reintroduction% children reacting adversely to
Chocolate Cows' milk
Orange Cows‘ cheese
Wheat Otherfruits
Tomato Egg
70%70 –
60 –
50 –
40 –
30 –
20 –
10 –
00
64%
57%
45% 45%
36%
22%18%
64%
Effects of a few food diet in attention deficit disorder. Carter CM, Arch Dis Child 1993:69:564–8.

Foods and additives are common causes of the attention deficit hyperactive disorder in children.
Boris M, Ann Allergy 1994:72:462–8
73% 26 children with ADHD
Treatment with a multiple item elimination diet.
80 –
70 –
60 –
50 –
40 –
30 –
20 –
10 –
00
% children improvingwith elimination diet
(19/26)
p<0.001

Foods and additives are common causes of the attention deficit hyperactive disorder in children.
Boris M, Ann Allergy 1994:72:462–8
73% 26 children with ADHD
Treatment with a multiple item elimination diet.
80 –
70 –
60 –
50 –
40 –
30 –
20 –
10 –
00
% children improvingwith elimination diet
(19/26)
p<0.001
On open challenge, all 19 children reacted to many foods, dyes, and/or preservatives.
A double-blind placebo controlled food
challenge (DBPCFC) was completed in
16 children.

Foods and additives are common causes of the attention deficit hyperactive disorder in children.
Boris M, Ann Allergy 1994:72:462–8
73% 26 children with ADHD
Treatment with a multiple item elimination diet.
80 –
70 –
60 –
50 –
40 –
30 –
20 –
10 –
00
% children improvingwith elimination diet
(19/26)
p<0.001
There was a significant
improvement on placebo days compared with challenge days
(P = 0.003).

Foods and additives are common causes of the attention deficit hyperactive disorder in children.
Boris M, Ann Allergy 1994:72:462–8
73% 26 children with ADHD
Treatment with a multiple item elimination diet.
80 –
70 –
60 –
50 –
40 –
30 –
20 –
10 –
00
% children improvingwith elimination diet
(19/26)
p<0.001
Atopic children with ADHD had a
significantly higher response rate than the nonatopic group.

Effects of food on physical and sleep complaints in children with ADHD: a randomised controlled pilot study.
Pelsser LM, Eur J Pediatr 2010;169:1129–38.
27 children (3.8-8.5 years) with ADHD
2-week baseline diet in which they adhered to their normal diet;
then a diet group (15/27)[rice, turkey, lamb, a range of vegetables (lettuce, carrots, cauliflower, cabbage and beet), pears and water] or a control group (12/27) for 5 weeks
% decrease in total number of complaints, including sleep complaints
p<0.001
-00
-10 –
-20 –
-30 –
-40 –
-50 –
-60 –
-70 –
-80 –-77%
-17%
diet group control group

Effects of food on physical and sleep complaints in children with ADHD: a randomised controlled pilot study.
Pelsser LM, Eur J Pediatr 2010;169:1129–38.
% decrease in total number of complaints, including sleep complaints
p<0.001
-00
-10 –
-20 –
-30 –
-40 –
-50 –
-60 –
-70 –
-80 –-77%
-17%
diet group control group The odds of having complaints at the end of the trial is 13.25-fold higher in the control
group compared to the diet group
27 children (3.8-8.5 years) with ADHD
2-week baseline diet in which they adhered to their normal diet;
then a diet group (15/27)[rice, turkey, lamb, a range of vegetables (lettuce, carrots, cauliflower, cabbage and beet), pears and water] or a control group (12/27) for 5 weeks

Effects of food on physical and sleep complaints in children with ADHD: a randomised controlled pilot study.
Pelsser LM, Eur J Pediatr 2010;169:1129–38.
Effect of the interventions on physical and sleep complaints
The odds of having complaints at the end of the trial is 13.25-fold higher in the control group compared to the diet group

Effects of food on physical and sleep complaints in children with ADHD: a randomised controlled pilot study.
Pelsser LM, Eur J Pediatr 2010;169:1129–38.
27 children (3.8-8.5 years) with ADHD
2-week baseline diet in which they adhered to their normal diet;
then a diet group (15/27)[rice, turkey, lamb, a range of vegetables (lettuce, carrots, cauliflower, cabbage and beet), pears and water] or a control group (12/27) for 5 weeks
% decrease in total number of complaints, including sleep complaints
p<0.001
-00
-10 –
-20 –
-30 –
-40 –
-50 –
-60 –
-70 –
-80 –-77%
-17%
diet group control group
The reduction did not differ between children with or without an atopic
constitution (p = 0.7).

Food-based therapies: elimination diets in ADHD
More recently, Pelsser and colleagues observed improvements in behavior in 62% of ADHD patients using an eliminationdiet (3).
3) Pelsser LM, Ned Tijdschr Geneeskd 2002:146:2543–7.

Favourable effect of a standard elimination diet on the behavior of young children with attention deficit hyperactivity disorder (ADHD): a pilot study.Pelsser LM, Ned Tijdschr Geneeskd 2002:146:2543–7.
40 children, 36 boys and 4 girls, aged 3-7 years, with the DSM-IV-criteria for ADHD,usual diet for two weeks and thereafter for two weeks an elimination diet, based on the few foods diet (rice, turkey, pear and lettuce).Behaviour evaluated at study entry, after the baseline period and at the end of the diet. Parents completed the 10-item Conners list, the ADHD Rating Scale and a physical complaints list. Teachers completed the 10-item Conners list and the ADHD Rating Scale, at the beginning and at the end of the diet.
% children with improvement in behaviour of at least 50% on both the Conners list and
the ADHD Rating
according to the parent-ratings,
70 –
60 –
50 –
40 –
30 –
20 –
10 –
0
62%
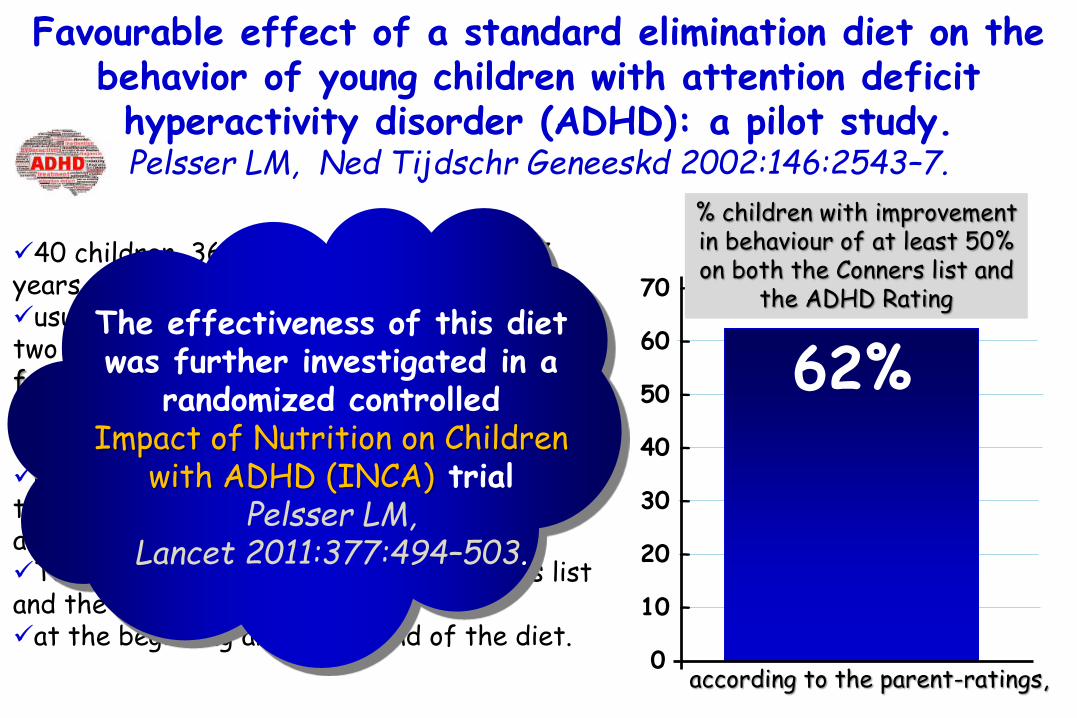
Favourable effect of a standard elimination diet on the behavior of young children with attention deficit hyperactivity disorder (ADHD): a pilot study.Pelsser LM, Ned Tijdschr Geneeskd 2002:146:2543–7.
40 children, 36 boys and 4 girls, aged 3-7 years, with the DSM-IV-criteria for ADHD,usual diet for two weeks and thereafter for two weeks an elimination diet, based on the few foods diet (rice, turkey, pear and lettuce).Behaviour evaluated at study entry, after the baseline period and at the end of the diet. Parents completed the 10-item Conners list, the ADHD Rating Scale and a physical complaints list. Teachers completed the 10-item Conners list and the ADHD Rating Scale, at the beginning and at the end of the diet.
according to the parent-ratings,
70 –
60 –
50 –
40 –
30 –
20 –
10 –
0
62%The effectiveness of this diet was further investigated in a
randomized controlled Impact of Nutrition on Children
with ADHD (INCA) trialPelsser LM,
Lancet 2011:377:494–503.
% children with improvement in behaviour of at least 50% on both the Conners list and
the ADHD Rating

Total IgE, food-specifi c IgE(to chicken egg, peanut, soy, milk, fi sh, and wheat), and food-specifi c total IgG
levels to 270 diff erent foods were assessed with ELISA.
We postulated that ADHD might be an allergic or non-allergic hypersensitivity
disorder in some children. IgE is implicated in typical food allergies.
In reactions to food that are notmediated by IgE, assessment of IgG levels might be useful, and IgG blood tests are
offered—especially in complementary care—with the aim of establishing arelation between foods and ADHD.
Effects of a restricted elimination diet on the behaviourof children with attention-deficit hyperactivity disorder
(INCA study): a randomised controlled trial. Pelsser LM, Lancet 2011:377:494–503.
100 children aged 4-8 years diagnosed with ADHD
randomly assigned to 5 weeks of a restricted elimination diet based on sIgG for foods (diet group, n=50) or to instructions for a healthy diet (control group, n=50).
In the following 4 weeks double blind food challenge.

Effects of a restricted elimination diet on the behaviourof children with attention-deficit hyperactivity disorder
(INCA study): a randomised controlled trial. Pelsser LM, Lancet 2011:377:494–503.
Measurement points during baseline, and the fi rst and second phases
Masking (paediatrician only) during the first phase (diet group and control group) is for group assignment, masking(paediatrician, researcher, parent, and teacher) during the second phase (diet group only) is for challenge assignment.
ACS=abbreviated Conners’ scale. ARS=attention-defi cit hyperactivity disorderrating scale. SPI=structured psychiatricinterview. LP=researcher assessor. P=parent. T=teacher. JT=paediatrician assessor. SDQ=strengths and diffi cultiesquestionnaire.
*Diet group responders only. †Responders who relapsed only. ‡Those who had not relapsed at 11 weeks.

Effects of a restricted elimination diet on the behaviourof children with attention-deficit hyperactivity disorder
(INCA study): a randomised controlled trial. Pelsser LM, Lancet 2011:377:494–503.
Between baseline and the end of the first phase, the difference between the diet group and the
control group in the mean ADHD rating scale [ARS]
total score was 23.7 (p<0·0001)
100 children aged 4-8 years diagnosed with ADHD
randomly assigned to 5 weeks of a restricted elimination diet based on sIgG for foods (diet group, n=50) or to instructions for a healthy diet (control group, n=50).
In the following 4 weeks double blind food challenge.

Effects of a restricted elimination diet on the behaviourof children with attention-deficit hyperactivity disorder
(INCA study): a randomised controlled trial. Pelsser LM, Lancet 2011:377:494–503.
Between baseline and the end of the first phase, the difference between the diet group and the
control group in the meanabbreviated Conners' scale (ACS) score was
11.8 (p<0·0001).
100 children aged 4-8 years diagnosed with ADHD
randomly assigned to 5 weeks of a restricted elimination diet based on sIgG for foods (diet group, n=50) or to instructions for a healthy diet (control group, n=50).
In the following 4 weeks double blind food challenge.

Effects of a restricted elimination diet on the behaviourof children with attention-deficit hyperactivity disorder
(INCA study): a randomised controlled trial. Pelsser LM, Lancet 2011:377:494–503.
Distribution of behaviour scores at start and end of the diet phase according to masked paediatrician ratings
ARSatt=ADHD rating scale inattention score (maximum score 27). ARShyp=ADHD rating scale hyperactivity and impulsivity score (maximum score 27).
ODD=oppositional defiant disorder (maximum score 8).
100 children aged 4-8 years diagnosed with ADHD
randomly assigned to 5 weeks of a restricted elimination diet based on sIgG for foods (diet group, n=50) or to instructions for a healthy diet (control group, n=50).
In the following 4 weeks double blind food challenge.

Effects of a restricted elimination diet on the behaviourof children with attention-deficit hyperactivity disorder
(INCA study): a randomised controlled trial. Pelsser LM, Lancet 2011:377:494–503.
Distribution of behaviour scores at start and end of the diet phase according to unmasked teacher ratings.
100 children aged 4-8 years diagnosed with ADHD
randomly assigned to 5 weeks of a restricted elimination diet based on sIgG for foods (diet group, n=50) or to instructions for a healthy diet (control group, n=50).
In the following 4 weeks double blind food challenge.
ARSatt=ADHD rating scale inattention score (maximum score 27). ARShyp=ADHD rating scale hyperactivity and impulsivity score (maximum score 27).
ODD=oppositional defiant disorder (maximum score 8).

Effects of a restricted elimination diet on the behaviourof children with attention-deficit hyperactivity disorder
(INCA study): a randomised controlled trial. Pelsser LM, Lancet 2011:377:494–503.
abbreviatedConners’ scale
Inattention
hyperactivity and impulsivity scores
ADHD=attention-deficit hyperactivity disorder. ACS=abbreviated Conners’ scale. ARSall=ADHD rating scale total score (maximum score 54). ARSatt=ADHD rating scale inattention score (maximum score 27). ARShyp=ADHD rating scale hyperactivity and impulsivity score (maximum score 27).
challenge challenge
challengechallenge
100 children aged 4-8 years diagnosed with ADHD
randomly assigned to 5 weeks of a restricted elimination diet based on sIgG for foods (diet group, n=50) or to instructions for a healthy diet (control group, n=50).
In the following 4 weeks double blind food challenge.
ADHD rating total score

Effects of a restricted elimination diet on the behaviourof children with attention-deficit hyperactivity disorder
(INCA study): a randomised controlled trial. Pelsser LM, Lancet 2011:377:494–503.

Effects of a restricted elimination diet on the behaviourof children with attention-deficit hyperactivity disorder
(INCA study): a randomised controlled trial. Pelsser LM, Lancet 2011:377:494–503.
The ADHD rating scale [ARS] total score increased in clinical responders after the challenge by 20.8 (p<0·0001) and the abbreviated Conners' scale (ACS) score increased by 11.6 (p<0·0001).
100 children aged 4-8 years diagnosed with ADHD
randomly assigned to 5 weeks of a restricted elimination diet based on sIgG for foods (diet group, n=50) or to instructions for a healthy diet (control group, n=50).
In the following 4 weeks double blind food challenge.
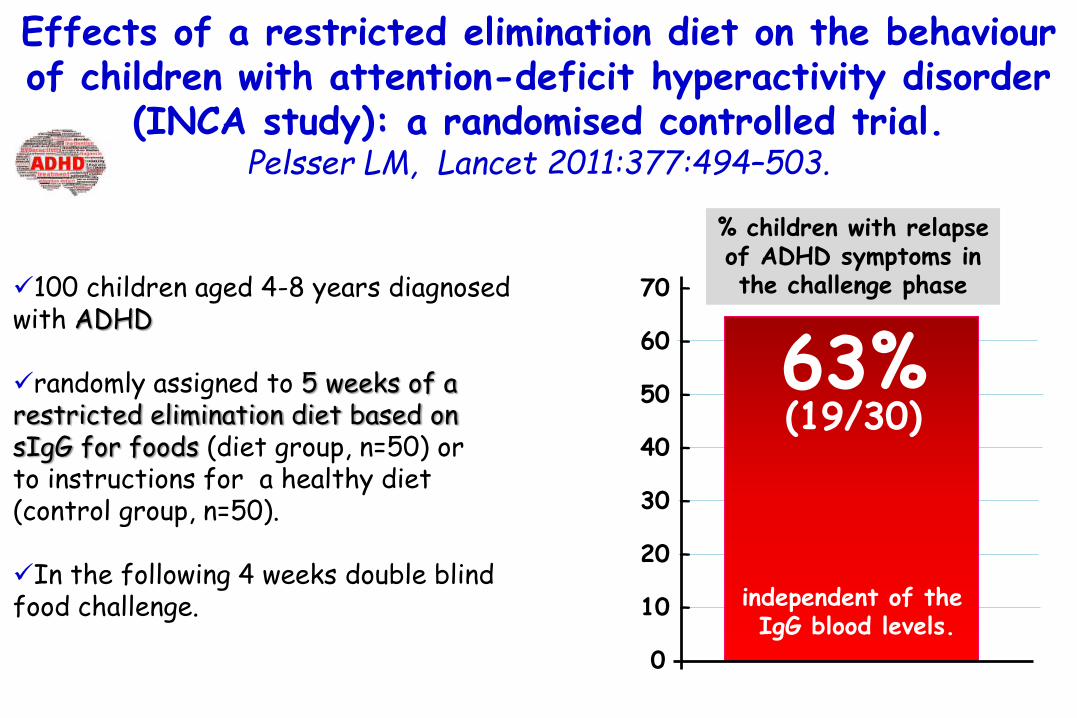
Effects of a restricted elimination diet on the behaviourof children with attention-deficit hyperactivity disorder
(INCA study): a randomised controlled trial. Pelsser LM, Lancet 2011:377:494–503.
70 –
60 –
50 –
40 –
30 –
20 –
10 –
0
(19/30)63%63%
% children with relapse of ADHD symptoms in the challenge phase
independent of the IgG blood levels.
100 children aged 4-8 years diagnosed with ADHD
randomly assigned to 5 weeks of a restricted elimination diet based on sIgG for foods (diet group, n=50) or to instructions for a healthy diet (control group, n=50).
In the following 4 weeks double blind food challenge.

100 children aged 4-8 years diagnosed with ADHD
randomly assigned to 5 weeks of a restricted elimination diet based on sIgG for foods (diet group, n=50) or to instructions for a healthy diet (control group, n=50).
In the following 4 weeks double blind food challenge.
Effects of a restricted elimination diet on the behaviourof children with attention-deficit hyperactivity disorder
(INCA study): a randomised controlled trial. Pelsser LM, Lancet 2011:377:494–503.
70 –
60 –
50 –
40 –
30 –
20 –
10 –
0
(19/30)63%63%
independent of the IgG blood levels.
Elimination diet was selectedon the basis of high IgG
levels to foods,
serum levels of food-specificIgE and total IgE did not differ between responders
and nonresponders.
% children with relapse of ADHD symptoms in the challenge phase

100 children aged 4-8 years diagnosed with ADHD
randomly assigned to 5 weeks of a restricted elimination diet based on sIgG for foods (diet group, n=50) or to instructions for a healthy diet (control group, n=50).
In the following 4 weeks double blind food challenge.
Effects of a restricted elimination diet on the behaviourof children with attention-deficit hyperactivity disorder
(INCA study): a randomised controlled trial. Pelsser LM, Lancet 2011:377:494–503.
70 –
60 –
50 –
40 –
30 –
20 –
10 –
0
(19/30)63%63%
independent of the IgG blood levels.
These findings suggest that ingested foods can affect
behavior in a subset of children with ADHD through a mechanism
that involves a non-IgG, non-IgE-mediated,
cell-mediated, ornon-allergic response.
% children with relapse of ADHD symptoms in the challenge phase
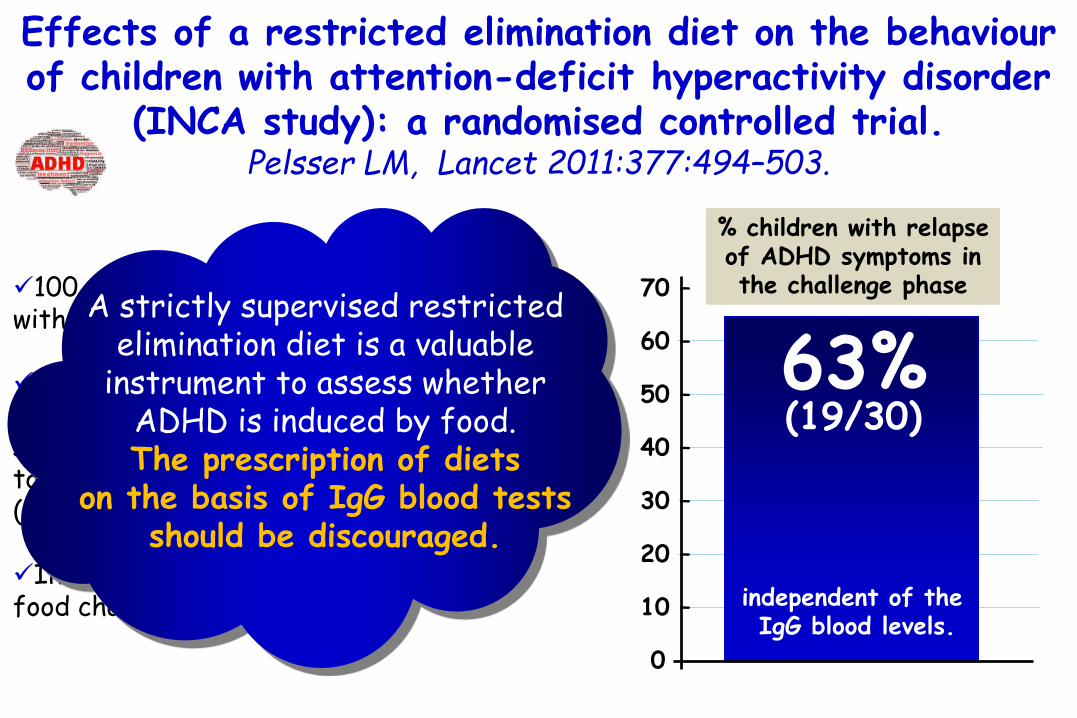
100 children aged 4-8 years diagnosed with ADHD
randomly assigned to 5 weeks of a restricted elimination diet based on sIgG for foods (diet group, n=50) or to instructions for a healthy diet (control group, n=50).
In the following 4 weeks double blind food challenge.
Effects of a restricted elimination diet on the behaviourof children with attention-deficit hyperactivity disorder
(INCA study): a randomised controlled trial. Pelsser LM, Lancet 2011:377:494–503.
70 –
60 –
50 –
40 –
30 –
20 –
10 –
0
(19/30)63%63%
independent of the IgG blood levels.
A strictly supervised restricted elimination diet is a valuable
instrument to assess whether ADHD is induced by food. The prescription of diets
on the basis of IgG blood tests should be discouraged.
% children with relapse of ADHD symptoms in the challenge phase

Food-based therapies: supplementation in ADHD ans ASD
Decreased levels of incorporated omega-3PUFAs have been observed in peripheral blood cells of ASD and ADHD patients.Meguid NA, Clin Biochem 2008:41:1044–8.
Nutritional supplementation with omega-3was observed to be beneficial in both ASD and ADHD.Richardson AJ. Int Rev Psychiatry 2006:18:155–72.

Role of polyunsaturated fatty acids in the management of Egyptian children with autism.
Meguid NA, Clin Biochem 2008:41:1044–8.
30 autistic children aged 3-11 years.
30 healthy children.
Free PUFAs from dried blood spot.
Before and after taking fish oil (Efalex).
-71% -65%
-32%
-45%
polyunsaturated fatty acid (PUFA) levels in autistic children before treatment
and control group *
* *
**

Role of polyunsaturated fatty acids in the management of Egyptian children with autism.
Meguid NA, Clin Biochem 2008:41:1044–8.
30 autistic children aged 3-11 years.
30 healthy children.
Free PUFAs from dried blood spot.
Before and after taking fish oil (Efalex).
-71% -65%
-32%
-45%
polyunsaturated fatty acid (PUFA) levels in autistic children before treatment
and control group *
* *
**
Before taking Efalex, linolenic acid showed a
significant reduction (71%), followed by docosahexaenoic
acid (65%) and arachidonic acid (45%),
while linoleic acid was the least affected
PUFA (32%).

Role of polyunsaturated fatty acids in the management of Egyptian children with autism.
Meguid NA, Clin Biochem 2008:41:1044–8.
30 autistic children aged 3-11 years.
30 healthy children.
Free PUFAs from dried blood spot.
Before and after taking fish oil (Efalex).
PUFA levels in autistic children before and after treatment
*
*
*
**

Role of polyunsaturated fatty acids in the management of Egyptian children with autism.
Meguid NA, Clin Biochem 2008:41:1044–8.
30 autistic children aged 3-11 years.
30 healthy children.
Free PUFAs from dried blood spot.
Before and after taking fish oil (Efalex).
PUFA levels in autistic children before and after treatment
*
*
*
**
After taking Efalex, 66% of autistic children
showed clinical and biochemical improvement,
linolenic acid and docosahexaenoic acid showed the highest levels
after Efalexsupplementation.

Role of polyunsaturated fatty acids in the management of Egyptian children with autism.
Meguid NA, Clin Biochem 2008:41:1044–8.
Comparison between Childhood Autism Rating Scale (CARS) score before and after treatment with fish oil (DHA, EPA)
CARS = Childhood Autism Rating ScaleSchopler E, Reichler RJ, Renner BR. The Childhood Autism Rating Scale(CARS) for diagnostic screening and classification of autism. New York:Irvington; 1993.

Role of polyunsaturated fatty acids in the management of Egyptian children with autism.
Meguid NA, Clin Biochem 2008:41:1044–8.
The supplement studied was Efalex® (supplied by Efamol Ltd., UK) a blend of high DHA fish oil and evening primrose oil. Each capsule contained:
– 60 mg of docosahexaenoic acid– 12 mg of gamma-linolenic acid– 13 mg of eicosapentaenoic acid– 5 mg of arachidonic acid.
Efalex® was chosen as, compared to other preparations, it contains both omega 3 and omega 6 fatty acids whichare important for the autistic children.

Omega-3 fatty acids in ADHD and relatedneurodevelopmental disorders.
Richardson AJ. Int Rev Psychiatry 2006:18:155–72.
Omega-3 fatty acids are dietary essentials, and are critical to brain development and function.
Increasing evidence suggests that a relative lack of omega-3 may contribute to many psychiatric and neurodevelopmental disorders.
Theory and experimental evidence support a role for omega-3 in ADHD, dyslexia, developmental coordination disorder (DCD) and autism.
Dietary supplementation with fish oils (providing EPA and DHA) appears to alleviate ADHD-related symptoms in at least some children, and one study of DCD children also found benefits for academic achievement.

Omega-3 fatty acids in ADHD and relatedneurodevelopmental disorders.
Richardson AJ. Int Rev Psychiatry 2006:18:155–72.
Omega-3 fatty acids are dietary essentials, and are critical to brain development and function.
Increasing evidence suggests that a relative lack of omega-3 may contribute to many psychiatric and neurodevelopmental disorders.
Theory and experimental evidence support a role for omega-3 in ADHD, dyslexia, developmental coordination disorder (DCD) and autism.
Dietary supplementation with fish oils (providing EPA and DHA) appears to alleviate ADHD-related symptoms in at least some children, and one study of DCD children also found benefits for academic achievement.
Omega-3 is not supported by current evidence as a primary treatment for ADHD or related conditions, but further research in this area is clearly warranted. Given their relative safety and general health benefits, omega-3 fatty acids offer a promising
complementary approach to standard treatments.

Food-based therapies: supplementation in ADHD ans ASD
PUFAs are present in neuronal membranousphospholipids, where they modulate membrane fluidity and thereby affect receptor function, resulting in changes in neurotransmitterrelease and uptake.Murphy MG. J Nutr Biochem 1990:1:68–79.
Omega-3 PUFAs can be incorporated in themembrane of immune cells, where they modulate intracellular pathways, such as NFkB) and peroxisome proliferator-activated receptor (PPAR)-γ, leading to an antiinflammatoryresponse through the production of resolvinsand inhibition of leukotrienes, prostaglandins, proinflammatory cytokines, and adhesion molecules. Calder PC. Proceedings of the Nutrition Society 2010:69:565–73.

Dietary fatty acids and membrane protein function. Murphy MG. J Nutr Biochem 1990:1:68–79.
There has been growing public awareness of the potential health benefits of dietary fatty acids, and of the distinction between the effects of the Ώ-6 and Ώ-3 polyunsaturated fatty acids that are concentrated in vegetable and fish oils, respectively.
A part of the biologic effectiveness of the two families of polyunsaturated fatty acids resides in their relative roles as precursors of the eicosanoids.
However, we are also beginning to appreciate that as the major components of the hydrophobic core of the membrane bilayer, they can interact with and directly influence the functioning of select integral membrane proteins.
Fatty acid affects the "fluidity" and/or thickness of the membrane

Rationale and use of n-3 fatty acids in artificial nutrition.
Calder PC. Proceedings of the Nutrition Society 2010:69:565–73.
Lipids traditionally used in artificial nutrition are based on n-6 fatty acid-rich vegetable oils like soyabean oil. This may not be optimal because it may present an excessive supply of linoleic acid.
One alternative to the use of soyabean oil is its partial replacement by fish oil, which contains n-3 fatty acids. These fatty acids influence inflammatory and immune responses and so may be useful in particular situations where those responses are not optimal.
Fish oil-containing lipid emulsions have been used in parenteral nutrition in adult patients post-surgery (mainly gastrointestinal). This has been associated with alterations in patterns of inflammatory mediators and in immune function and, in some studies, a reduction in length of intensive care unit (ICU) and hospital stay. Perioperative administration of fish oil may be superior to post-operative.
A formula including fish oil, borage oil and antioxidants has demonstrated marked benefits on gas exchange, ventilation requirement, new organ failures, ICU stay and mortality in patients with acute respiratory distress syndrome, acute lung injury or severe sepsis.

Food-based therapies: supplementation in ADHD ans ASD
PUFAs are present in neuronal membranousphospholipids, where they modulate membrane fluidity and thereby affect receptor function, resulting in changes in neurotransmitterrelease and uptake.Murphy MG. J Nutr Biochem 1990:1:68–79.
Omega-3 PUFAs can be incorporated in themembrane of immune cells, where they modulate intracellular pathways, such as NFkB) and peroxisome proliferator-activated receptor (PPAR)-γ, leading to an antiinflammatoryresponse through the production of resolvinsand inhibition of leukotrienes, prostaglandins, proinflammatory cytokines, and adhesion molecules. Calder PC. Proceedings of the Nutrition Society 2010:69:565–73.
Therefore, supplementation of omega-3
PUFAs could be beneficial for patients with ASD and ADHD,
either by acting directly on neuronal responses
or indirectly via the immune system and
GI tract.
Human milk oligosaccharides are resistant to enzymatic hydrolysis in the upper gastrointestinal tract.
Engfer MB, Am J Clin Nutr 2000:71:1589–96.
Human milk oligosaccharides (HMOs) show a complexity and variety not found in milk of any other species.
As a prerequisite for biological activity in infant metabolism, HMOs have to resist enzymatic hydrolysis in the gastrointestinal tract.
A majority of human milk HMOs reach the large intestine, where they serve as substrates for bacterial metabolism.
Therefore, HMOs might be considered the soluble fiber fraction of human milk.

Food-based therapies: supplementation in ADHD ans ASD
De Theije CGM, Pediatr Allergy Imm 2014;25:218
The effects of non-digestible oligosaccharides (prebiotics) and beneficial bacterial strains (probiotics) in the treatment for neurodevelopmental disorders have not been studied.
Nondigestible oligosaccharides consist of naturally occurring sugar base units that are not hydrolyzed in the upper small intestine and reach the large intestine intact to serve as substrates for bacterial metabolism.

Food-based therapies: supplementation in ADHD ans ASD
De Theije CGM, Peditr Allergy Imm 2014;25:218
Non-digestible oligosaccharides are suggested to selectively stimulate growth and/or activityof Bifidobacteria and lactic acid bacteria in the colon, which are important markers of a healthy gut microbiota .Costalos C, Early Hum Dev 2008:84:45–9.Langlands SJ, Gut 2004:53:1610–6.
Regarding allergic diseases,non-digestible oligosaccharides were shown to be beneficial fordisease progression and immune status.Schouten B, Pediatr Allergy Immunol 2011:22:537–42. van Hoffen E, Allergy 2009:64:484–7.
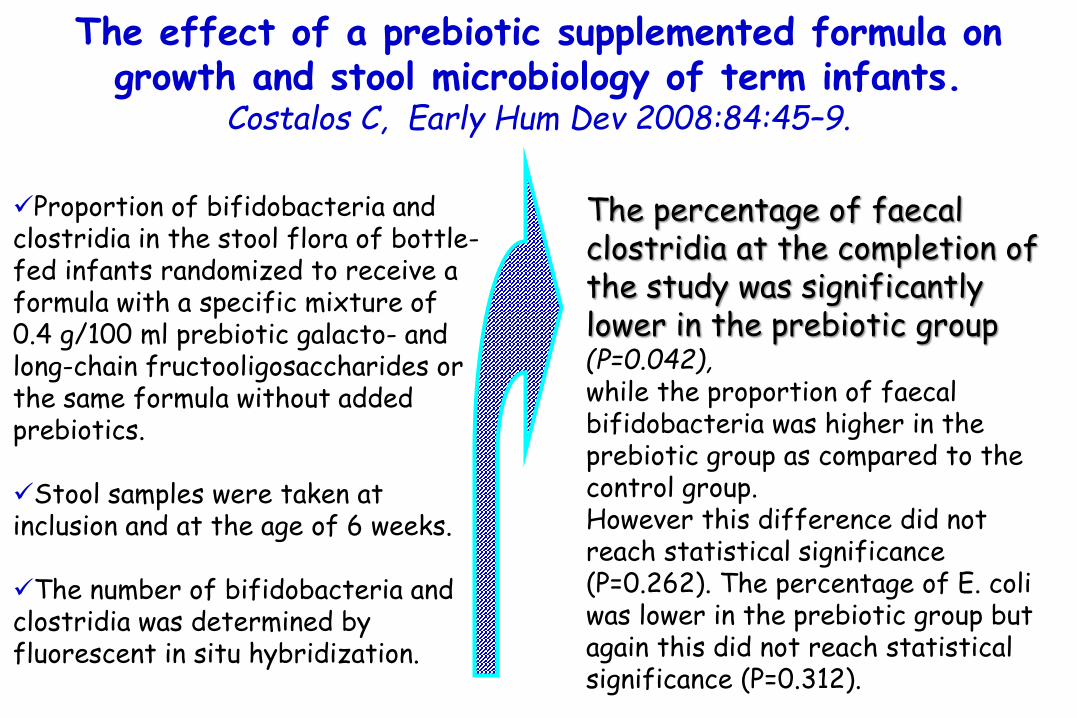
The effect of a prebiotic supplemented formula on growth and stool microbiology of term infants.
Costalos C, Early Hum Dev 2008:84:45–9.
Proportion of bifidobacteria and clostridia in the stool flora of bottle-fed infants randomized to receive a formula with a specific mixture of 0.4 g/100 ml prebiotic galacto- and long-chain fructooligosaccharides or the same formula without added prebiotics.
Stool samples were taken at inclusion and at the age of 6 weeks.
The number of bifidobacteria and clostridia was determined by fluorescent in situ hybridization.
The percentage of faecalclostridia at the completion of the study was significantly lower in the prebiotic group (P=0.042), while the proportion of faecalbifidobacteria was higher in the prebiotic group as compared to the control group. However this difference did not reach statistical significance (P=0.262). The percentage of E. coli was lower in the prebiotic group but again this did not reach statistical significance (P=0.312).

Prebiotic carbohydrates modify the mucosa associated microflora of the human large bowel.
Langlands SJ, Gut 2004:53:1610–6
Prebiotics increased mucosal bifidobacteriain both the proximal
and distal colon.
14 subjects.
Supplemented their diet for two weeks with a mix of 7.5 g of oligofructoseand 7.5 g inulin.

Prebiotic carbohydrates modify the mucosa associated microflora of the human large bowel.
Langlands SJ, Gut 2004:53:1610–6
14 subjects.
Supplemented their diet for two weeks with a mix of 7.5 g of oligofructoseand 7.5 g inulin.
Prebioticcarbohydrates can change the
composition of the mucosa associated flora significantly
(p = 0.02)
Prebiotics increased mucosal bifidobacteriain both the proximal
and distal colon.

Non-digestible oligosaccharides reduce immunoglobulinfree light-chain concentrations in infants at risk for allergy. Schouten B, Pediatr Allergy Immunol 2011:22:537–42
A special prebiotic mixture (Immunofortis®) of short-chaingalacto-oligosaccharides (scGOS) and long-chain fructo-oligosaccharides (lcFOS).
Infants at risk for allergy.
A hypoallergenic whey formula containing 8 g/l of the scGOS/lcFOS mixture (n = 34) or maltodextrin as a placebo (n=40) for 6 months.

Non-digestible oligosaccharides reduce immunoglobulinfree light-chain concentrations in infants at risk for allergy. Schouten B, Pediatr Allergy Immunol 2011:22:537–42
Oral supplementation with a mixture of short-chain galacto-oligosaccharides (scGOS)/long-chain fructo-oligosaccharides (lcFOS) prevents the increase in plasma concentrations of both(a) kappa and (b) lambda immunoglobulin free light-chains in infants at high risk for allergy at
6 months of age
p<0.001 p<0.001
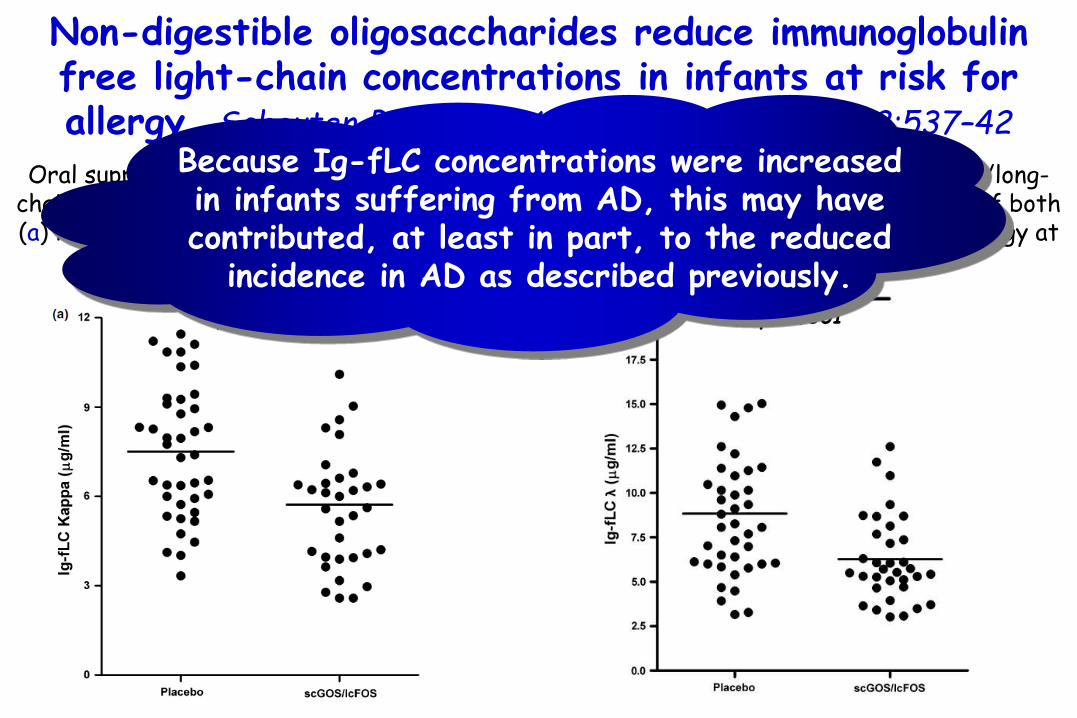
Non-digestible oligosaccharides reduce immunoglobulinfree light-chain concentrations in infants at risk for allergy. Schouten B, Pediatr Allergy Immunol 2011:22:537–42
Oral supplementation with a mixture of short-chain galacto-oligosaccharides (scGOS)/long-chain fructo-oligosaccharides (lcFOS) prevents the increase in plasma concentrations of both(a) kappa and (b) lambda immunoglobulin free light-chains in infants at high risk for allergy at
6 months of age
p<0.001 p<0.001
Because Ig-fLC concentrations were increased in infants suffering from AD, this may have contributed, at least in part, to the reduced
incidence in AD as described previously.

A specific mixture of short-chain galactooligosaccharidesand long-chain fructooligosaccharides induces a beneficialimmunoglobulin profile in infants at high risk for allergy.
van Hoffen E, Allergy 2009:64:484–7
Infants received a hypoallergenic whey formula with either 8 g/l GOS/FOS in a 9 : 1 ratio (IMMUNOFORTIS) or 8 g/l maltodextrine (placebo) for 6 months.
At 3 months of age, childrenwere vaccinated with Hexavacagainst a.o. diphteria, tetanus, polio.
At 6 months of age, plasma samples were collected.
p<0.01
Total IgE levels at 6 months

A specific mixture of short-chain galactooligosaccharidesand long-chain fructooligosaccharides induces a beneficialimmunoglobulin profile in infants at high risk for allergy.
van Hoffen E, Allergy 2009:64:484–7
Infants received a hypoallergenic whey formula with either 8 g/l GOS/FOS in a 9 : 1 ratio (IMMUNOFORTIS) or 8 g/l maltodextrine (placebo) for 6 months.
At 3 months of age, childrenwere vaccinated with Hexavacagainst a.o. diphteria, tetanus, polio.
At 6 months of age, plasma samples were collected.
p<0.01
Total IgE levels at 6 months
GOS/FOS supplementation led to a significant reduction in the plasma level of
total IgE.
DTP-specific Ig levels were not affected.

Food-based therapies: supplementation in ADHD ans ASD
De Theije CGM, Peditr Allergy Imm 2014;25:218
Non-digestible oligosaccharides are suggested to selectively stimulate growth and/or activityof Bifidobacteria and lactic acid bacteria in the colon, which are important markers of a healthy gut microbiota .Costalos C, Early Hum Dev 2008:84:45–9.Langlands SJ, Gut 2004:53:1610–6.
Regarding allergic diseases,non-digestible oligosaccharides were shown to be beneficial fordisease progression and immune status.Schouten B, Pediatr Allergy Immunol 2011:22:537–42. van Hoffen E, Allergy 2009:64:484–7.
Considering the increased recognition of a microbial role in the regulation of behavioral responses and
neurodevelopment,children with ASD and ADHD
may benefit from dietarysupplementation with
non-digestible oligosaccharidesor
beneficial bacterial strains.

Food-based therapies: supplementation in ADHD ans ASD
De Theije CGM, Peditr Allergy Imm 2014;25:218
Non-digestible oligosaccharides are suggested to selectively stimulate growth and/or activityof Bifidobacteria and lactic acid bacteria in the colon, which are important markers of a healthy gut microbiota .Costalos C, Early Hum Dev 2008:84:45–9.Langlands SJ, Gut 2004:53:1610–6.
Regarding allergic diseases,non-digestible oligosaccharides were shown to be beneficial fordisease progression and immune status.Schouten B, Pediatr Allergy Immunol 2011:22:537–42. van Hoffen E, Allergy 2009:64:484–7.
Beneficial bacterial strainsare thought to reduce intestinal
permeability and restore a‘healthy’ gut, which could be of
specific importance inthe treatment for
GI disturbances and behavioral deficits of
ASD patients.Reid G, Nat Rev Microbiol
2011:9:27–38.

Microbiota restoration: natural and supplementedrecovery of human microbial communities.
Reid G, Nat Rev Microbiol 2011:9:27–38.
Known sites of natural microbiota restoration.

Microbiota restoration: natural and supplementedrecovery of human microbial communities.
Reid G, Nat Rev Microbiol 2011:9:27–38.
a | Co-aggregation of non-pathogens and pathogens interferes with the ability of the pathogenic species to infect the host. b | Biosurfactants produced by lactobacilli help prevent the adhesion of pathogens to mucosal surfaces. c | In addition to host immunoglobulin defences, it has been suggested that bacteriocins and hydrogen peroxide produced by lactobacilli can inhibit or kill pathogens.d | Signalling between bacteria can lead to downregulation of toxin production in pathogens. e | By competing for nutrients and surface receptors, non-pathogenic bacteria can competitively exclude pathogens from host surfaces.f | The regulation of immune responses by the microbiota can result in: the production of host factors such as antimicrobial peptides (for example, defensins), lactoferrin and lysozyme, which can kill pathogens; the production of alkaline phosphatases, which bind to lipopolysaccharide and negate its toxicity; and the deregulation of nuclear factor-κB (NF-κB) signalling in host epithelia (whether this is influenced by lactobacilli, as indicated, remains to be confirmed).g | Upregulation of tight junction proteins might help to limit the damage that is caused to epithelia by inflammatory processes or pathogens. The damage disrupts the cell linkages and induces a host response, shown here as a macrophage, which further induces local damage. The lactobacilli-coated surface retains an intact junction.
Possible mechanisms contributing to restoration of the microbiota.

Microbiota restoration: natural and supplementedrecovery of human microbial communities.
Reid G, Nat Rev Microbiol 2011:9:27–38.
Possible mechanisms contributing to restoration of the microbiota.

The potential role of probiotics in the management of childhood autism spectrum disorders.
Critchfield JW, Gastroenterol Res Pract. 2011:161358.
a substantial number of children with autism
spectrum disorders (ASD)
Activation of the mucosal immune response
Presence of abnormal gut microbiota
Gastrointestinal (GI) dysfunction
irritability, tantrums, (collera, malumore, bizza)
aggressive behaviour, sleep disturbances.

The potential role of probiotics in the management of childhood autism spectrum disorders.
Critchfield JW, Gastroenterol Res Pract. 2011:161358.
a substantial number of children with autism
spectrum disorders (ASD)
Activation of the mucosal immune response
Presence of abnormal gut microbiota
Gastrointestinal (GI) dysfunction
irritability, tantrums, aggressive behaviour, sleep disturbances.
modulating gut bacteria with short-term antibiotic treatment can lead to temporary improvement in behavioral symptoms in some individuals with ASD.

The potential role of probiotics in the management of childhood autism spectrum disorders.
Critchfield JW, Gastroenterol Res Pract. 2011:161358.
Probiotics can influence microbiota composition and intestinal barrier function and alter mucosal immune responses.
The administration of probiotic bacteria to address changes in the microbiota might, therefore, be a useful novel therapeutic tool with which to restore normal gut microbiota, reduce inflammation, restore epithelial barrier function, and potentially ameliorate behaviouralsymptoms associated with some children with ASD.
In this review of the literature, support emerges for the clinical testing of probiotics in ASD, especially in the context of addressing GI symptoms.

However, preclinical studies in disease models of ASD and ADHD are requiredto study the benefits and safety of supplementation with non-digestible oligosaccharides andbeneficial bacterial strains in the treatment of behavior.
Food-based therapies: supplementation in ADHD ans ASD
lino
tarassaco
As prenatal (immune) factors are thought to have detrimental effects on behavior of the offspring later in life, it may be even more interesting to provide genetically or environmentally predisposed mothers with beneficial diets during pregnancy.
Food-based therapies: supplementation in ADHD ans ASD

Food supplementation during pregnancy for the prevention of ADHD ans ASD
Preclinical murine studies showed that a maternal diet rich in omega-6 during gestation and lactation induced autism-likebehavior in offspring. Jones KL, Behav Brain Res 2013:238:193–9.
Omega-3-rich fish consumption during pregnancy was shown to be protective of ADHD related behavior in children. Sagiv SK, Arch Pediatr Adolesc Med 2012:166:1123–31.
Furthermore, a traditional Dutch diet during pregnancy was positively associated with externalizing behaviors in children, while a Mediterranean diet was negatively associated.Sagiv SK, Arch Pediatr Adolesc Med 2012:166:1123–31.

Maternal diet rich in omega-6 polyunsaturated fatty acids during gestation and lactation produces autistic like
sociability deficits in adult offspring.Jones KL, Behav Brain Res 2013:238:193–9
An environmental factor that may contribute to the etiology of autism is diet. One dietary variable that has received recent attention is polyunsaturated fatty acids (PUFAs), particularly the decline in omega-3 PUFAs in the modern Western diet. Currently, modern Western diets are rich in omega-6 (n-6) PUFAs and deficient in omega-3 (n-3) PUFAs. The ratio of n-6 to n-3 in the traditional hunter-gatherer diet was approximately 2:1 to 3:1, whereas the ratio in a modern Western diet is approximately 15:1 to 17:1. In extreme cases, the ratio may even reach 50:1, caused by an excess of n-6 PUFAs and a severe deficiency in n-3 PUFAs. As long-chain PUFAs (LC-PUFAs) are not endogenously made in humans, they must be obtained from the diet. While the level of the n-6 PUFA arachidonic acid (AA) is relatively consistent worldwide, n-3 PUFAs DHA and eicosapentaenoic acid (EPA) are more variable, resulting in the n-6:n-3ratio imbalance.Omega-3 polyunsaturated fatty acids (PUFAs), specifically docosahexaenoic acid (DHA), play a central role in the functioning and development of the brain and central nervous system.

Maternal diet rich in omega-6 polyunsaturated fatty acids during gestation and lactation produces autistic like
sociability deficits in adult offspring.Jones KL, Behav Brain Res 2013:238:193–9
Either chronic stress or no stress, and also placed on a control diet or a
diet rich in omega-6 PUFAs
Maternal diet rich in omega-6 PUFAs during gestation and lactation produce changes in sociability consistent with
those observed in ASD.
Pregnant C57BL/6J dams
Maternal diet rich in omega-6 polyunsaturated fatty acids during gestation and lactation produces autistic like
sociability deficits in adult offspring.Jones KL, Behav Brain Res 2013:238:193–9
Pregnant C57BL/6J dams
Additionally, offspring exposed to a diet rich in omega-6 PUFAs during gestation and lactation had increased levels of anxiety
Either chronic stress or no stress, and also placed on a control diet or a
diet rich in omega-6 PUFAs

Maternal diet rich in omega-6 polyunsaturated fatty acids during gestation and lactation produces autistic like
sociability deficits in adult offspring.Jones KL, Behav Brain Res 2013:238:193–9
Pregnant C57BL/6J dams
Additionally, offspring exposed to a diet rich in omega-6 PUFAs during gestation and lactation had increased levels of anxiety
Either chronic stress or no stress, and also placed on a control diet or a
diet rich in omega-6 PUFAs
Prenatal stress had no effect on offspring
behaviour.These findings provide
evidence for a possible
environmental risk factor that contributes to the
production of autistic-like
behavior in mice.

Prenatal exposure to mercury and fish consumption duringpregnancy and attention-deficit/hyperactivity disorder
related behavior in children. Sagiv SK, Arch Pediatr Adolesc Med 2012:166:1123–31
Children examined at age 8 years with peripartummaternal hair mercury measures (n = 421) or maternal report of fish consumption during pregnancy (n = 515).
Inattentive and impulsive/hyperactive behaviors were assessed using a teacher rating scale and neuropsychological testing.
Association of perinatal maternal hair mercury levels with total scores from the Conners Rating Scale–Teachers
for 8-year-old

Prenatal exposure to mercury and fish consumption duringpregnancy and attention-deficit/hyperactivity disorder
related behavior in children. Sagiv SK, Arch Pediatr Adolesc Med 2012:166:1123–31
Children examined at age 8 years with peripartummaternal hair mercury measures (n = 421) or maternal report of fish consumption during pregnancy (n = 515).
Inattentive and impulsive/hyperactive behaviors were assessed using a teacher rating scale and neuropsychological testing.
Association of perinatal maternal hair mercury levels with total scores from the Conners Rating Scale–Teachers
for 8-year-old
There was a protective association for fish consumption
(>2 servings per week) with ADHD-related behaviors,
particularly impulsive/hyperactive
behaviors (relative risk = 0.4).

Prenatal exposure to mercury and fish consumption duringpregnancy and attention-deficit/hyperactivity disorder
related behavior in children. Sagiv SK, Arch Pediatr Adolesc Med 2012:166:1123–31
Mild/markedlyatypical inattentive
1.4
In maternal hair mercury level at ≥ 1 μg/g, for an interquartile range (0.5 μg/g) mercury increase; RR for
1.7
Children examined at age 8 years with peripartummaternal hair mercury measures (n = 421) or maternal report of fish consumption during pregnancy (n = 515).
Inattentive and impulsive/hyperactive behaviors were assessed using a teacher rating scale and neuropsychological testing.
2.0 –
1.5 –
1.0 –
0.5 –
0.0Impulsive-
hyperactive
BEHAVIORS
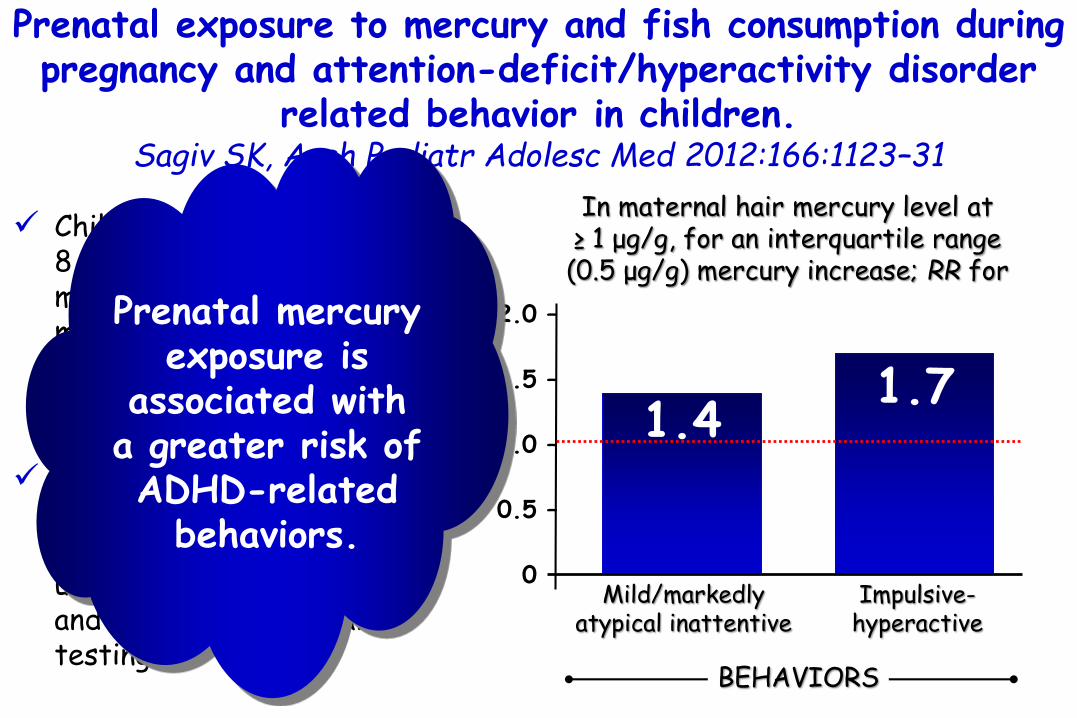
Prenatal exposure to mercury and fish consumption duringpregnancy and attention-deficit/hyperactivity disorder
related behavior in children. Sagiv SK, Arch Pediatr Adolesc Med 2012:166:1123–31
Mild/markedlyatypical inattentive
1.4
In maternal hair mercury level at ≥ 1 μg/g, for an interquartile range (0.5 μg/g) mercury increase; RR for
1.7
Children examined at age 8 years with peripartummaternal hair mercury measures (n = 421) or maternal report of fish consumption during pregnancy (n = 515).
Inattentive and impulsive/hyperactive behaviors were assessed using a teacher rating scale and neuropsychological testing.
2.0 –
1.5 –
1.0 –
0.5 –
0.0Impulsive-
hyperactive
BEHAVIORS
Prenatal mercury exposure is
associated with a greater risk of ADHD-related
behaviors.

Maternal dietary patterns during pregnancy and childinternalising and externalising problems.
The Generation R Study. Steenweg-de Graaff J, Clin Nutr. 2014;33:115-21
The pattern labelled ‘Mediterranean’, because of its high loadings on vegetables, fish & shellfish, vegetable oil, fruit, and eggs, and relatively high negative loading on processed meat.
The 'Traditionally Dutch’ was characterized by high intakes of fresh and processed meat and potatoes, a relatively high intake of margarines and a very low intake of soy and diet products.

Maternal dietary patterns during pregnancy and childinternalising and externalising problems.
The Generation R Study. Steenweg-de Graaff J, Clin Nutr. 2014;33:115-21
per SD increase in
Mediterraneandiet score
0.90
OR for child externalising problems
1.11
Food frequency questionnaire.
Child internalising(emotionally reactive, anxious/depressed or withdrawn, having somatic complaints) and externalisingproblems (inattention, aggression) assessed with the Child BehaviourChecklist at 1.5, 3 and 6 yrs in 3104 children.
1.5 –
1.0 –
0.5 –
0.0per SD
inncrease in Traditionally Dutch score

Maternal dietary patterns during pregnancy and childinternalising and externalising problems.
The Generation R Study. Steenweg-de Graaff J, Clin Nutr. 2014;33:115-21
per SD increase in
Mediterraneandiet score
0.90
1.11
Food frequency questionnaire.
Child internalising(emotionally reactive, anxious/depressed or withdrawn, having somatic complaints) and externalisingproblems (inattention, aggression) assessed with the Child BehaviourChecklist at 1.5, 3 and 6 yrs in 3104 children.
1.5 –
1.0 –
0.5 –
0.0per SD
inncrease in Traditionally Dutch score
Neither diet was associated with internalisingproblems.
OR for child externalising problems

Maternal folic acid supplement use in early pregnancy and child behavioural problems: the Generation R Study.
Roza SJ, Br J Nutr 2010:103:445–52
Total problems
1.44
In children of mothers who did not use folic acid supplements in the first
trimester OR for 4214 toddlers.
Child behaviouraland emotional problems assessed with the Child Behaviour Checklist at the age of 18 months
Internalising Externalising
1.65
2.0 –
1.5 –
1.0 –
0.5 –
0.0
1.45
PROBLEMS

Maternal folic acid supplement use in early pregnancy and child behavioural problems: the Generation R Study.
Roza SJ, Br J Nutr 2010:103:445–52
Total problems
1.44
In children of mothers who did not use folic acid supplements in the first
trimester OR for 4214 toddlers.
Child behaviouraland emotional problems assessed with the Child Behaviour Checklist at the age of 18 months
Internalising Externalising
1.65
2.0 –
1.5 –
1.0 –
0.5 –
0.0
1.45
PROBLEMS
Inadequate use of folic acid
supplements during early pregnancy
may be associated with a higher risk
of behaviouralproblems in the
offspring.

Maternal periconceptional folic acid intake and risk of autism spectrum disorders and developmental delay in the
CHARGE (CHildhood Autism Risks from Geneticsand Environment) case-control study.
Schmidt RJ, Am J Clin Nutr 2012:96:80–9
TD
779
μg of folic acid intake in the first month of pregnancy
655
Children with autism spectrum disorder (ASD) (n=429) and developmental delay (DD) (n=130) or typical development (TD; n = 278).
Average daily folic acid quantified for each mother.
ASDCHILDREN WITH
800 –
700 –
600 –
500 –
400 –
300 –
200 –
100 –
000
P<0.01

Maternal periconceptional folic acid intake and risk of autism spectrum disorders and developmental delay in the
CHARGE (CHildhood Autism Risks from Geneticsand Environment) case-control study.
Schmidt RJ, Am J Clin Nutr 2012:96:80–9
Children with autism spectrum disorder (ASD) (n=429) and developmental delay (DD) (n=130) or typical development (TD; n = 278).
Average daily folic acid quantified for each mother.
In children of mother with a mean daily folic acid intake of ≥600 μg(compared with <600 μg) during
the 1st month of pregnancy OR for
0.62P=0.02
1.0 –
0.5 –
0.0autism spectrum disorder

Maternal periconceptional folic acid intake and risk of autism spectrum disorders and developmental delay in the
CHARGE (CHildhood Autism Risks from Geneticsand Environment) case-control study.
Schmidt RJ, Am J Clin Nutr 2012:96:80–9
Children with autism spectrum disorder (ASD) (n=429) and developmental delay (DD) (n=130) or typical development (TD; n = 278).
Average daily folic acid quantified for each mother.
In children of mother with a mean daily folic acid intake of ≥600 μg(compared with <600 μg) during
the 1st month of pregnancy OR for
0.62P=0.02
1.0 –
0.5 –
0.0
and risk estimates decreased with
increased folic acid (P-trend =0.001).
ASD
folic acid intake
autism spectrum disorder

Maternal periconceptional folic acid intake and risk of autism spectrum disorders and developmental delay in the
CHARGE (CHildhood Autism Risks from Geneticsand Environment) case-control study.
Schmidt RJ, Am J Clin Nutr 2012:96:80–9
Children with autism spectrum disorder (ASD) (n=429) and developmental delay (DD) (n=130) or typical development (TD; n = 278).
Average daily folic acid quantified for each mother.
In children of mother with a mean daily folic acid intake of ≥600 μg(compared with <600 μg) during
the 1st month of pregnancy OR for
0.62P=0.02
1.0 –
0.5 –
0.0autism spectrum disorder
A minimum of 400 up to 800 micrograms
of folic acid or folatesuppletion per day
from 4 weeks before conception to 8 weeks
thereafter is reccomended

Folate concentrations during pregnancy and autistic traitsin the offspring. The Generation R Study.
Steenweg-de Graaff J, Eur J Public Health. 2014 [Epub ahead of print
maternal plasma folateconcentrations at 13 weeks of gestation and prenatal folic acid supplement use
autistic traits in the offspring at the age of 6 years.
parent-reported autistic traits were assessed using the Social Responsiveness Scale short form.
1. Maternal folate was not associated with autistic traits in the offspring.
2. In contrast, prenatal folic acid use was associated with less child autistic traits.
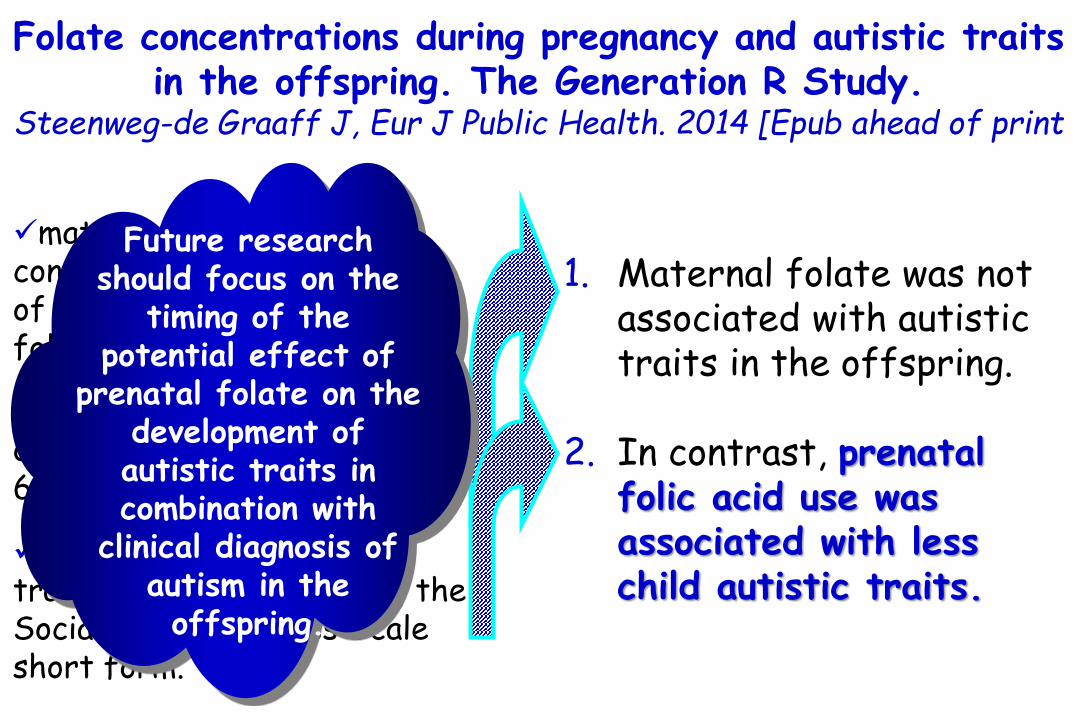
Folate concentrations during pregnancy and autistic traitsin the offspring. The Generation R Study.
Steenweg-de Graaff J, Eur J Public Health. 2014 [Epub ahead of print
maternal plasma folateconcentrations at 13 weeks of gestation and prenatal folic acid supplement use
autistic traits in the offspring at the age of 6 years.
parent-reported autistic traits were assessed using the Social Responsiveness Scale short form.
1. Maternal folate was not associated with autistic traits in the offspring.
2. In contrast, prenatal folic acid use was associated with less child autistic traits.
Future research should focus on the
timing of the potential effect of
prenatal folate on the development of autistic traits in combination with
clinical diagnosis of autism in the offspring.
Food Allergy and the Brain
Attilio BonerUniversity ofVerona, Italy
Introduction
Micronutrients and Behaviour
Immunity & Ipersensitivity
Food Allergy&Ipersensitivity and Brain
Not only Food Allergy
Which came first?
Possible Mechanisms
Food-based Therapies
Conclusions

Neuro – Gastoenteric – Endocrine – Immunologic Network

Conclusions
Several micronutrients are important for normal developmentincluding behavior
Foods can act troughout animmunologic or troughout a pharmacologic mechanism
Anxiety and depression as well asbehavioral problem such as ADHDand ASD are more common in allergic subjects and pediatric allergologists need to think of the presenceof these disturbances when early symptoms occur.
Chronic fatigue syndrome and fibromyalgia can also have animmunologic component.

Conclusions
do not cause but may aggravate
ASD
ADHD
Conclusions
Gluten-free and/or casein-free (GFCF) dietary intervention may be offered to children with ASD and gastrointestinal symptoms and/or increased gastrointestinal permeablity.
Additive containing foods should be avoidedby children with ADHD and probably by all.
Every dietetic intervention should be evalutedin order to exclude its placebo effect and after animprovment during the elimination dieta challenge should be performed.
Conclusions
Nutritional supplementation with omega-3 was observed to be beneficial in both children with ASD and ADHD.
More studies are needed on probiotics but in meanwhile a diet rich in natural prebiotics (fruits & vegetables) can be reasonably suggested.
Correct nutrition and eventual micronutrientsupplementation must be advocated before conception, during pregnancy, and always in children particularly in the first two years of life

ADHD, ASD, and Chronic Fatigue Syndrome and Fibromialgiarepresent a group of diseases that the allergist-immunologist may be called on to manage in which its precise etiologies have not been identified but which appear to be exacerbated by allergic mechanisms.
Now, it is generally accepted that the immunological system is part of a broader tripartite system referred to as the NEI system, which represents a network of interdependent and interrelated responses of the neurological, endocrine, and immunological systems in response to external and internal stimuli.
An understanding of these interactive responses is essential for a comprehension of the pathophysiology of these disorders as well as their diagnosis and management.
Conclusions

There appears to be mounting evidence that high doses ofartificial food coloring may produce minimal but significantadverse effects on some children with behavior disorders,whether they have true hyperkinetic syndrome or conductdisorders, i.e., ADD.

there is emergingevidence to suggest that adverse reactions to foods orfood components also may be associated with behavioraldisturbances.
There have been unsubstantiated claims, primarily madein the lay media rather than in scientific channels, that“debilitating and chronic symptoms of ill health resultingfrom an intolerance to certain foods”2 exist and these havetended to direct medical opinion against the concept thatfoods might play a role in affecting behavior. The profession’srejection of such claims neither provide help forindividual patients nor recognize that there are some provenassociations between ingestion of food and aberrations inbehavior.


Both prenatal and postnatal allergic immune activation regulate complex, but critical, neuroimmune interactions and therefore affect neurodevelopment and brain function.
Pathways involved in allergy-mediated effects on neurodevelopment and behavior could include neuroimmune interactions induced by mast cells and cytokines such as IL-6, as these mediators have beenshown to induce behavioral deficits inpreclinical models and are enhanced in ASD patients.
Conclusions

Conclusions
Based on clinical and preclinical observations, it seems feasible to hypothesize that allergic reactions to foods indeed trigger orworsen the manifestation of neurodevelopmentaldisorders in at least a subset of pediatric patients.
In children with ASD, these allergic reactions could be both IgE as non-IgE-mediated, while in ADHD, it is more likely that non-IgE-mediated, cell-mediated, or non-allergic responses to foods are involved.

Conclusions
Changes in the microbiome and subsequent signalingto the brain could also be involved in the behavioral Consequences of an allergic response.
Nevertheless, very little preclinical research is conducted on the prenatal and postnatal effect of an allergic response on neurodevelopment and behavior related to ASD and ADHD.
Untangling the mechanisms underlying the effects of hyperallergenicfoods and food-allergic reactions on neurodevelopmental impairmentscould lead to new targets for the treatment of children withASD or ADHD.



“Grazie per la vostra
attenzione alla storia che vi ha
raccontato mio nonno.”
Mia Charlize Powell

18° FORMAT Verona 6-7/05/2016