forsvarets logistikkorganisasjon norwegian armed...
TRANSCRIPT

16/10/10 1 Forfatter Prosjektittel
FORSVARET Forsvarets logistikkorganisasjon
16/10/10 1
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services
Health for fighting strength
Crystalloids and colloids in RDCR
Christian Medby Anaestesiologist
Norwegian Armed Forces Medical Services
& St Olav University Hospital
16/10/10 2
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services
What is Remote DCR?
• Far forward • Prehospital • No/limited surgical capability
16/10/10 3
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services
What is Remote DCR?
• Life-saving interventions • Use of hemostatic agents • Blood transfusions • Hypotensive fluid resuscitation
16/10/10 4
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services
”Lethal triad” Coagulopathy Hypothermia
Acidosis

16/10/10 5
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services
• Very little room for colloids and crystalloids in RDCR

16/10/10 6
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services
In fact, most clinical evidence suggests that we are better off giving no fluids..

16/10/10 7
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services
”For hypotensive patients with penetrating torso injuries, delay of aggressive fluid resuscitation until
operative intervention improves the outcome.”
Bickell, W. H., Wall, M. J., Pepe, P. E., Martin, R. R., Ginger, V. F., Allen, M. K., & Mattox, K. L. (1994). Immediate versus delayed fluid resuscitation for hypotensive patients with penetrating torso injuries. New Eng J Med, 331(17), 1105–9

16/10/10 8
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services
5
Prehospital Intravenous Fluid Administra5on Is Associated With Higher Mortality in Trauma Pa5ents: A Na5onal Trauma Data Bank Analysis. Haut, Ellio,; Kalish, Brian; Co,on, Bryan; MD, MPH; Efron, David; Haider, Adil; MD, MPH; Stevens, Kent; MD, MPH; Kieninger, Alicia; Cornwell, Edward; Chang, David; MBA, MPH Annals of Surgery. 253(2):371-‐377, February 2011. DOI: 10.1097/SLA.0b013e318207c24f
MulUple logisUc regression showing odds raUo of death for trauma paUents with prehospital IV fluid administraUon-‐subset analyses.
16/10/10 9
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services
”The review found no evidence to suggest that prehospital IV fluid
resuscitation is beneficial, and some evidence that it may be harmful.”
Dretzke J, Sandercock J, Bayliss S, Burls A. Clinical effectiveness and cost-effectiveness of prehospital intravenous fluids in trauma patients. Health Technol Assess 2004;8(23).

16/10/10 10
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services
• Restrict prehospital fluid resuscitation in patients with a radial pulse and normal mental status
• Hypotension, coagulation and vasospasm will limit blood loss
Hypotensive fluid resuscitation

16/10/10 11
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services
The concept of hypotensive resuscitation is extrapolated from ‘delayed resuscitation’ and mostly supported by animal studies

16/10/10 12
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services
Mor
talit
y
Amount of fluid infused
HAHN, R. G. (2012). Fluid therapy in uncontrolled hemorrhage - what experimental models have taught us. Acta Anaesthesiologica Scandinavica, 57(1), 16–28.
16/10/10 13
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services
”Titration of initial fluid therapy to a lower than normal SBP during active hemorrhage did not affect mortality
in this study.”
Dutton, R. P., Mackenzie, C. F., & Scalea, T. M. (2002). Hypotensive resuscitation during active hemorrhage: impact on in-hospital mortality. J Trauma, 52(6), 1141–6.

16/10/10 14
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services
”Hypotensive resuscitation is a safe strategy for use in the trauma population and results in a significant reduction in blood product transfusions and overall IV fluid administration. (…) lowers the risk of early postoperative death and coagulopathy.” Morrison, C. A., Carrick, M. M., Norman, M. A., Scott, B. G., Welsh, F. J., Tsai, P., et al. (2011). Hypotensive resuscitation strategy reduces transfusion requirements and severe postoperative coagulopathy in trauma patients with hemorrhagic shock: preliminary results of a randomized controlled trial. J Trauma, 70(3), 652–63.
16/10/10 15
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services
Colloids or crystalloids?
Blood

16/10/10 16
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services
Crystalloids/colloids vs blood
Blood: • Expands blood volume • Risk of transmission of pathogens • Transports oxygen • Contains platelets and coagulation factors
Crystalloids/colloids • Expands blood volume • No risk of disease transmission • No oxygen carrying capacity • Dilutes platelets and coagulation factors

16/10/10 17
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services
Crystalloids or colloids? • Colloids have the advantage of staying
longer in circulation • Less colloids needed for same expansion
of intravascular volume • Colloids cause less edema
However…
16/10/10 18
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services
Colloids cause coagulopathy

16/10/10 19
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services
Sorensen, B., & Fries, D. (2011). Emerging treatment strategies for trauma-induced coagulopathy. Br J Surg, 99(S1), 40–50.
16/10/10 20
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services
Comparisons of lactated Ringer’s and Hextend resuscitationon hemodynamics and coagulation following femur injury
and severe hemorrhage in pigs
Wenjun Z. Martini, PhD, Michael A. Dubick, PhD, and Lorne H. Blackbourne, MD, Fort Sam Houston, Texas
BACKGROUND: This study compared coagulation function after resuscitation with Hextend and lactated Ringer’s (LR) solution in pigs with tissue injuryand hemorrhagic shock.
METHODS: Pigs were randomized into control (n = 7 each), LR, and Hextend groups. Femur fracture was induced using the captive bolt stunner atmidshaft of the pigs’ left legs, followed by hemorrhage of 60% total blood volume and resuscitation with either Hextend (equal to bledvolume) or LR to reach the same mean arterial pressure. Pigs in the control group were not bled or resuscitated. Hemodynamics wasmonitored hourly for 6 hours. Blood samples were taken at baseline (BL), after hemorrhage, 15 minutes, 3 hours, and 6 hours afterresuscitation for blood and coagulation measurements.
RESULTS: Mean arterial pressure decreased to 50% of BL by the 60% hemorrhage but returned to near BL within 1 hour after LR or Hextendresuscitation. Heart rate was increased (from 91 T 4 beats per minute to 214 T 20 beats per minute) by hemorrhage and decreased afterresuscitation but remained elevated above BL in both groups. Resuscitation with Hextend (42 mL/kg) or LR (118 T 3 mL/kg) reducedhematocrit, total protein, fibrinogen, and platelet counts, with greater decreases shown in the Hextend group. Clot strength was lower butreturned to BL by 3 hours in the LR group, whereas it remained reduced for the 6-hour period after Hextend. The overall clottingcapacity after LR was decreased after hemorrhage and resuscitation but returned to BL by 3 hours, whereas it remained low afterHextend for the 6-hour experiment period.
CONCLUSION: After traumatic hemorrhage, coagulation function was restored within 6 hours with LR resuscitation but not with Hextend. The lack ofrecovery after Hextend is likely caused by greater hemodilution and possible effects of starches on coagulation substrates and furtherdocuments the need to restrict the use of high-molecular-weight starch in resuscitation fluids for bleeding casualties. (J Trauma AcuteCare Surg. 2013;74: 732Y740. Copyright * 2013 by Lippincott Williams & Wilkins)
KEY WORDS: Hemorrhagic shock; Hextend; lactated Ringer’s (LR) solution; thrombelastography; pig.
Hemorrhage is the leading cause of potentially survivabledeath in the battlefield and amajor cause of death in civilian
trauma.1 Blood loss is also commonly encountered during sur-gical intervention.2 To restore tissue perfusion and hemody-namics, fluid resuscitation is a routine clinical practice to treathypovolemia. A variety of resuscitation fluids have been usedaround the globe, with selections depending on availability, cost,and clinical experience.3 Crystalloids, such as isotonic sodiumchloride solution and lactated Ringer’s (LR) solution, are inex-pensive and have been widely used at prehospital and hospitalsettings. Colloids, such as albumin, gelatin, and hydroxyethylstarch (HES), are highly effective in increasing intravascularvolume with small volume increase in interstitial space (com-pared with crystalloids). Different colloid products have beenused in clinical practice.4Y7As one of theHESproducts, Hextend
(BioTime, Berkeley, CA) was developed and approved for use asa plasma volume expander in the United States in 1999 and wasrecommended for use in the military by the committee on Tac-tical Combat Casualty Care.8 It contains 6% hetastarch with amean molecular weight (MW) of 670 kD and a degree ofhydroxyethyl group substitution of 0.75 (HES 670/0.75) in aphysiologically balanced solution of electrolytes, glucose, andlactate. The newest starch product,Voluven (FreseniusKabi, BadHomburg, Germany), was developed and approved in Europeand recently in the United States and contains 6% Hetastarchwith a MW of 130 kD and a degree of hydroxyethyl groupsubstitution of 0.4 (HES 130/0.4) in saline medium. A growingnumber of studies have been undertaken to investigate resusci-tative effects of colloids.5,6,9Y14 Although effective volume ex-pansion and positive clinical outcomes have been reported inclinical trials and animal studies,7,15Y16 colloid infusion has beenshown to be associated with reductions of coagulation factors,17
platelet dysfunction,18Y20 anaphylactic reactions,21 and hemor-rhagic complications.22Y24
Limited information is available comparing Hextend withcrystalloid LR after hemorrhage in vivo. In a swine model, Toddet al.25 investigated effects of LR and Hextend on coagulationchanges and blood loss after severe liver injury. However, sincethe only coagulation data shown were at the end of the study,25
it is difficult to evaluate the time course changes in coagula-tion from either LR or Hextend resuscitation or compare theeffects between LR andHextend from that study. In patients who
AAST 2012 PLENARY PAPER
J Trauma Acute Care SurgVolume 74, Number 3732
Submitted: September 20, 2012, Revised: November 14, 2012, Accepted: November20, 2012.
From the US Army Institute of Surgical Research, Fort Sam Houston, Texas.This study was presented at the 71st annual meeting of the American Association
for the Surgery of Trauma, September 12Y15, 2012, in Kauai, Hawaii.The opinions or assertions contained herein are the private views of the authors and
are not to be construed as official or as reflecting the views of the USDepartmentof the Army or the US Department of Defense.
Address for reprints: Wenjun Z. Martini, PhD, US Army Institute of Surgical Re-search, 3698 Chambers Pass, Fort Sam Houston, TX 78234; email: [email protected].
DOI: 10.1097/TA.0b013e31827f156d
Copyright © 2013 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

16/10/10 21
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services
Dextran > HES > Gelatins
Dextran: platelet dysfunction (acquired von Willebrand’s state)
HES: coating of platelets Gels: impaired fibrinogen polymerization
16/10/10 22
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services
2
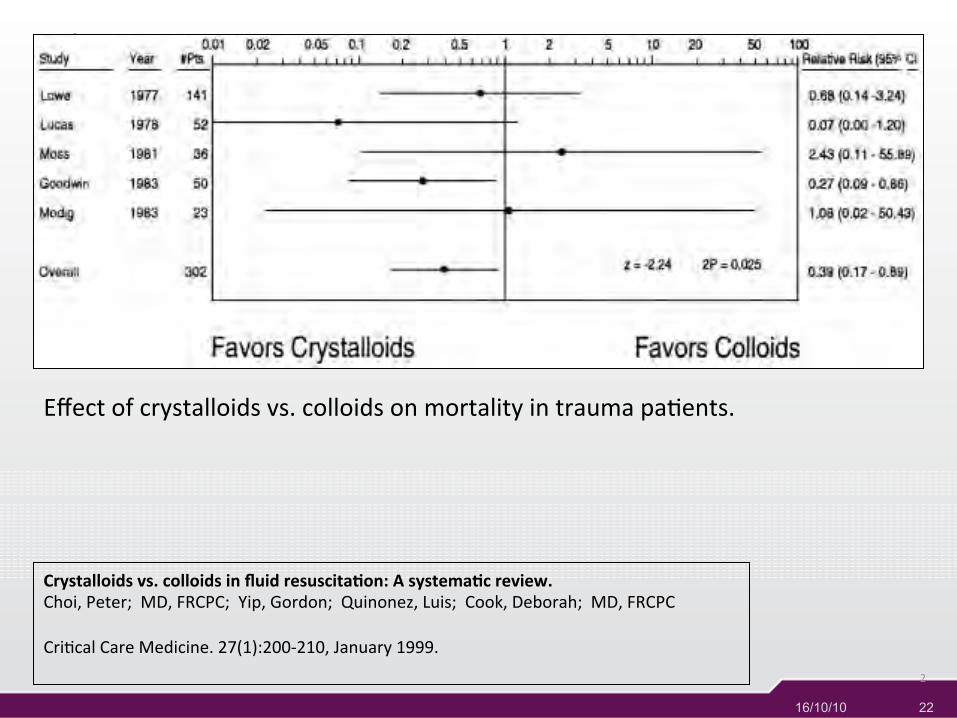
Crystalloids vs. colloids in fluid resuscita5on: A systema5c review. Choi, Peter; MD, FRCPC; Yip, Gordon; Quinonez, Luis; Cook, Deborah; MD, FRCPC CriUcal Care Medicine. 27(1):200-‐210, January 1999.
Effect of crystalloids vs. colloids on mortality in trauma paUents.
16/10/10 23
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services
Colloids
Conclusions: Overall, there is no apparent difference in pulmonary edema, mortality, or length of stay between isotonic crystalloid and colloid resuscitation. Crystalloid resuscitation is associated with a lower mortality in trauma patients. Methodologic limitations preclude any evidence-based clinical recommendations. Larger well-designed randomized trials are needed to achieve sufficient power to detect potentially small differences in treatment effects if they truly exist.
(Crit Care Med 1999;27:200-210)

16/10/10 24
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services
Colloids versus crystalloids for fluid resuscitation in criticallyill patients (Review)
Perel P, Roberts I
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library2012, Issue 11
http://www.thecochranelibrary.com
Colloids versus crystalloids for fluid resuscitation in critically ill patients (Review)
Copyright © 2012 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

16/10/10 25
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services
There is no evidence from RCTs that resuscitation with colloids reduces the risk of death, compared to resuscitation with crystalloids, in patients with trauma, burns or following surgery. As colloids are not associated with an improvement in survival, and as they are more expensive than crystalloids, it is hard to see how their continued use in these patients can be justified outside the context of RCTs.

16/10/10 26
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services
Hypertonic saline Hypertonic resuscitation of hypovolemic shock after blunt
trauma: a randomized controlled trial.
Bulger EM, Jurkovich GJ, Nathens AB, Copass MK, Hanson S, Cooper C, Liu PY, Neff M, Awan AB, Warner K, Maier RV.
Arch Surg. 2008 Feb;143(2):139-48; discussion 149.
…stopped for safety reasons
16/10/10 27
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services
My opinion:
The only reason to choose colloids is logistical: less volume, less weight.
Choose colloids if you have to carry it
yourself.

16/10/10 28
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services
What about crystalloids?
• Edema • ARDS • Hyperchloraemic acidosis (NS) • Compartment syndromes • Dilution coagulopathy

16/10/10 29
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services
What crystalloid?
• ‘Balanced’ crystalloids cause less hyperchloraemic acidosis
• Less electrolyte disturbances

16/10/10 30
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services
What are the alternatives?
16/10/10 31
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services
Blood?

16/10/10 32
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services

16/10/10 33
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services
Thrombin generation after dilution. Thrombin generation patterns in platelet-poor plasma are shown before and after dilution to about 40% of baseline. The patterns are similar between baseline and dilution with fresh frozen plasma (FFP).
33
Bolliger, D., Görlinger, K., & Tanaka, K. A. (2010). Pathophysiology and treatment of coagulopathy in massive hemorrhage and hemodilution. Anesthesiology, 113(5), 1205–19.

16/10/10 34
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services
Hess JR et al. The coagulopathy of trauma: a review of mechanisms. J Trauma. 2008 Oct;65(4):748-54.
16/10/10 35
NORWEGIAN ARMED FORCES Norwegian Armed Forces Medical Services
Questions?