frenulectomy presentation - emory bf conference.pptx ... · incidence 4.8%, m:f ratio 2.6:1 ... •...
TRANSCRIPT
3/7/2018
1
LatchingOnToaBetterUnderstandingofTongueandLipTies
ErikBauer,MDPediatricENTofAtlanta,P.C.
EmoryBreastfeedingConference
March12,2018
Tongue‐tie(Ankyloglossia)
AcademyofBreastfeedingMedicinedefinition
“asublingualfrenulum(bandunderneaththetongue)whichchangestheappearanceand/orfunctionoftheinfant’stonguebecauseofitsdecreasedlength,lackofelasticityorattachmenttoodistalbeneaththetongueortooclosetoorintothegingivalridge”
Doestonguetieaffectbreastfeeding?
1041infantsscreenedforankyloglossiaatWBC Incidence4.8%,M:Fratio2.6:1
Breastfeedingproblems(nipplepainlastinglongerthan6weeksand/ordifficultyofthebabylatchingontothebreast)reportedin: 25%ofinfantswithankyloglossia 3%ofcontrols
Conclusion:ankyloglossiaisassociatedwithBFdifficultyinselected infants,whileothersareabletocompensate…let’sexplorewhy.
Messner AH, Lalakea ML, Aby J, Macmahon J, Bair E.Arch Otolaryngol Head Neck Surg. 2000 Jan;126(1):36‐9. Ankyloglossia: incidence and associated feeding difficulties.

3/7/2018
2
TongueEmbryology
Tonguedevelopsbetween4‐7weeksofpregnancy
Contributionsfromall4pharyngealarchesandtheirnerves
Fusionofbilateraltissuebudsfromfloorofthemouth(musclelayerunderthetongue)
Budsfusefrombacktofront
Apoptosis(programmedcelldeath)separatestonguefromFOM
Thefrenulumisaremnantofthisprocesswithavariabledegreeofpersistence
MechanicsofBreastfeeding
Upperlipflangesabovenippletoreachareola,wideningthemouthgape
Theinfantmovesthetongueforwardtograspanddrawthenippleandareolaintothemouth
Fronttomid‐dorsaltongueliftsthenippleagainstthehardpalateandmustformanairtightsealwithminimalcompression
Tonguebasedropsdown,expandingthechambertocreatenegativepressureandextractingmilkfromthebreast
Someinfantswithlatchrestrictionareunabletograspthenipple/breast,whileothersattachpoorlycausingnipplepainordamage
Ultrasoundimagingofinfantswallowingduringbreast‐feeding.GeddesDT,ChadwickLM,KentJC,Garbin CP,HartmannPE.Dysphagia.2010Sep;25(3):183‐91.
AnatomyofBreastfeeding
3/7/2018
3
MechanicsofBreastfeeding:AnatomicConsequence
Mostimportantsinglemechanicalfactorforlatchingsuccess:Totalsurfaceareaofcontactbetweenbaby’smouthandnipple/areola
RestrictedLatchFeedingPattern
Consequenceoflossofsuctionwithinadequateseal
Troubleestablishinglatch,shallowlatch,frequentseparation
Biting,pinchingor“chomping”nipplewithgumridges
“Lipstick”compressionorblanchingofnipple
Nipplepain,crackingorblistering;pluggedductsormastitis
Clickingandairswallowing,gassyafterfeeds,frequentspitup
Ineffectivemilktransfer,breastnotdrainedafterfeed
Prolonged,frustratingfeedsandlittlerestbetweenfeedings
Frequentsuspectedthrushthatdoesnotrespondwelltotypicaltreatments
Poorweightgaininbaby,poormilkproductioninmother
MultifactorialElements
Manyfactorsotherthantongueandliptiesmaycontributetobreastfeedingdifficulties
InfantFactors Higharchedorcleftpalate Recessedjaw Coordination/strengthofsuck,tonguemuscle Oromotortone Airway/breathing(suck/swallow/breathecoordination)
MaternalFactors Decreasedmilksupply
Breasthypoplasia/insufficientglandulartissue(IGT) Stress/hormonalissuesaffectingletdown Short,flatorinvertednipple
3/7/2018
4
PregnancyandDeliveryImpactBreastfeeding
Notallcausesofpoorbreastfeedingarestructural/anatomic
Manycausesoflowmilkproductionorineffectivebreastfeedingcanbeidentifiedandmanaged hypothyroid Insulindysregulation PCOS Fertilitystruggles Alcoholandtobaccouse Postpartumdepression Medications,herbs,andnaturalremedies
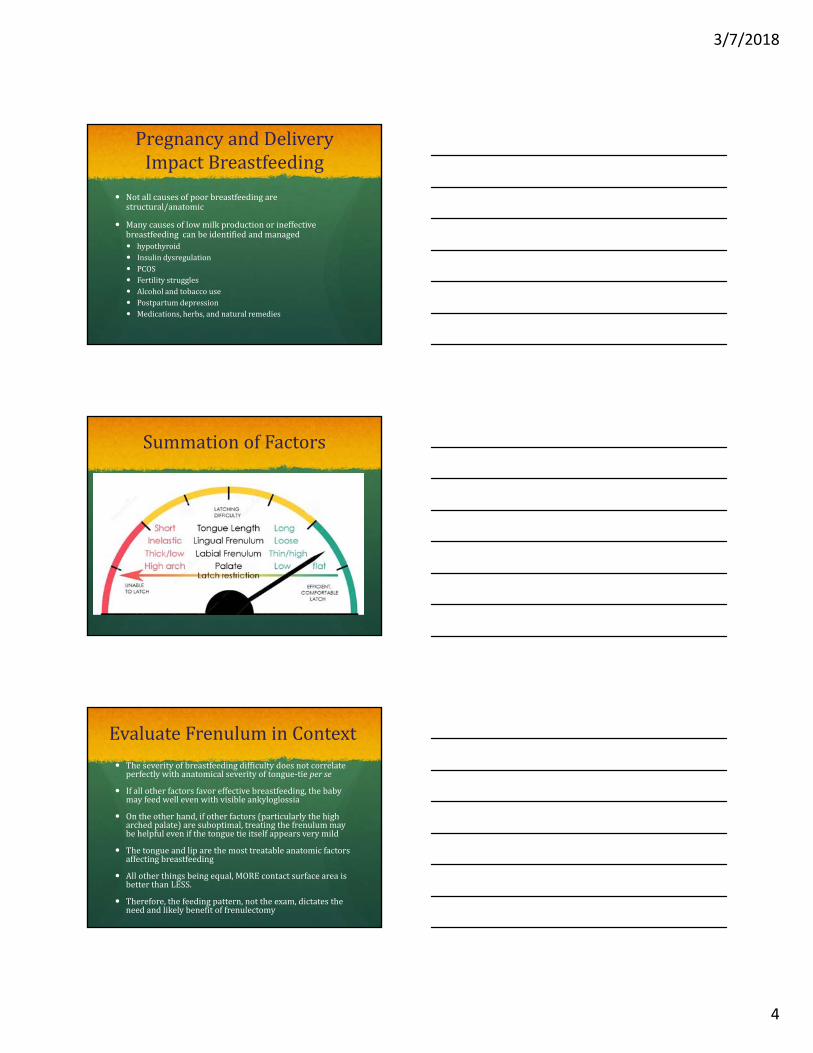
SummationofFactors
EvaluateFrenuluminContext Theseverityofbreastfeedingdifficultydoesnotcorrelateperfectlywithanatomicalseverityoftongue‐tieperse
Ifallotherfactorsfavoreffectivebreastfeeding,thebabymayfeedwellevenwithvisibleankyloglossia
Ontheotherhand,ifotherfactors(particularlythehigharchedpalate)aresuboptimal,treatingthefrenulummaybehelpfulevenifthetonguetieitselfappearsverymild
Thetongueandliparethemosttreatableanatomicfactorsaffectingbreastfeeding
Allotherthingsbeingequal,MOREcontactsurfaceareaisbetterthanLESS.
Therefore,thefeedingpattern,nottheexam,dictatestheneedandlikelybenefitoffrenulectomy
3/7/2018
5
SchematicofBFdifficulty
Breastfeedingdifficulty
Structurallatchrestriction
Classicalanteriorankyloglossia
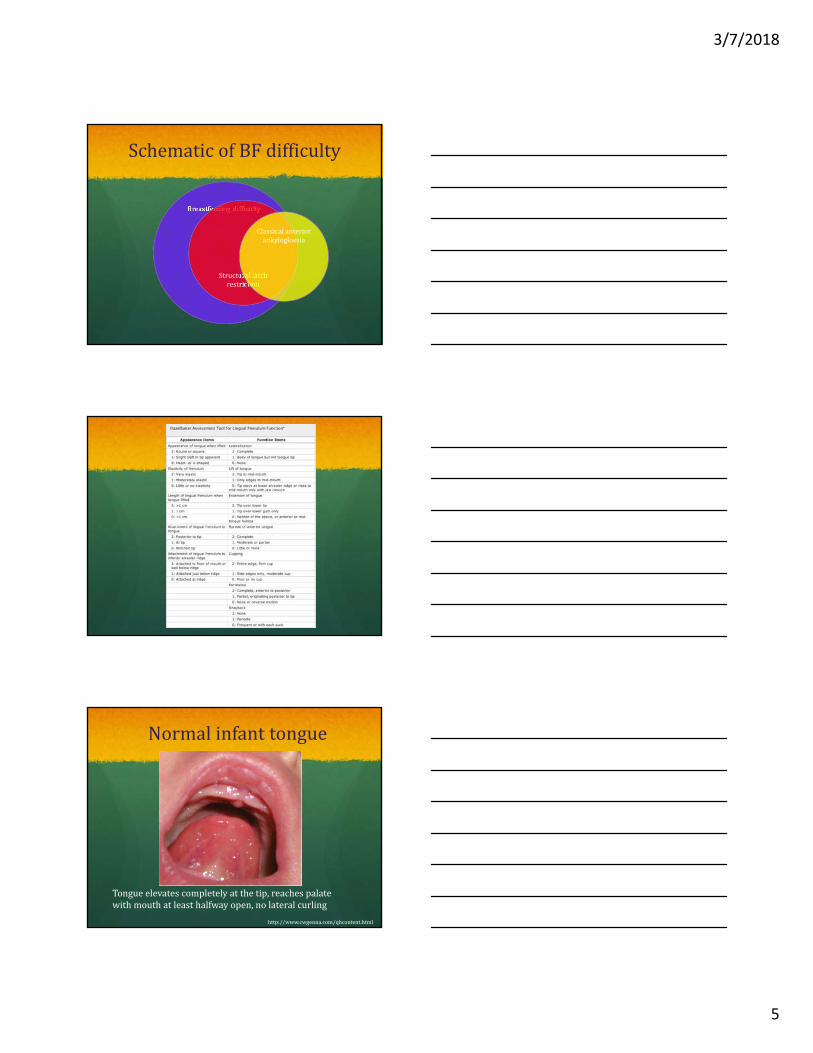
Normalinfanttongue
Tongueelevatescompletelyatthetip,reachespalatewithmouthatleasthalfwayopen,nolateralcurling
http://www.cwgenna.com/qhcontent.html
3/7/2018
6
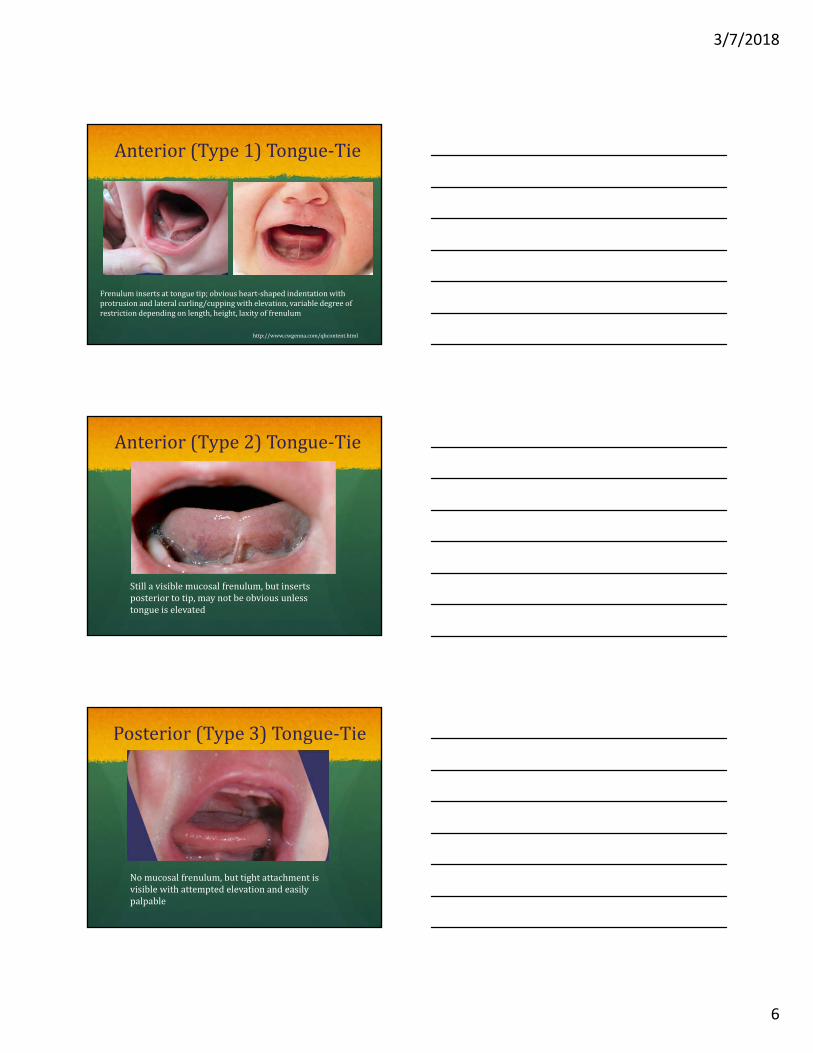
Anterior(Type1)Tongue‐Tie
Frenuluminsertsattonguetip;obviousheart‐shapedindentationwithprotrusionandlateralcurling/cuppingwithelevation,variabledegreeofrestrictiondependingonlength,height,laxityoffrenulum
http://www.cwgenna.com/qhcontent.html
Anterior(Type2)Tongue‐Tie
Stillavisiblemucosalfrenulum,butinsertsposteriortotip,maynotbeobviousunlesstongueiselevated
Posterior(Type3)Tongue‐Tie
Nomucosalfrenulum,buttightattachmentisvisiblewithattemptedelevationandeasilypalpable
3/7/2018
7
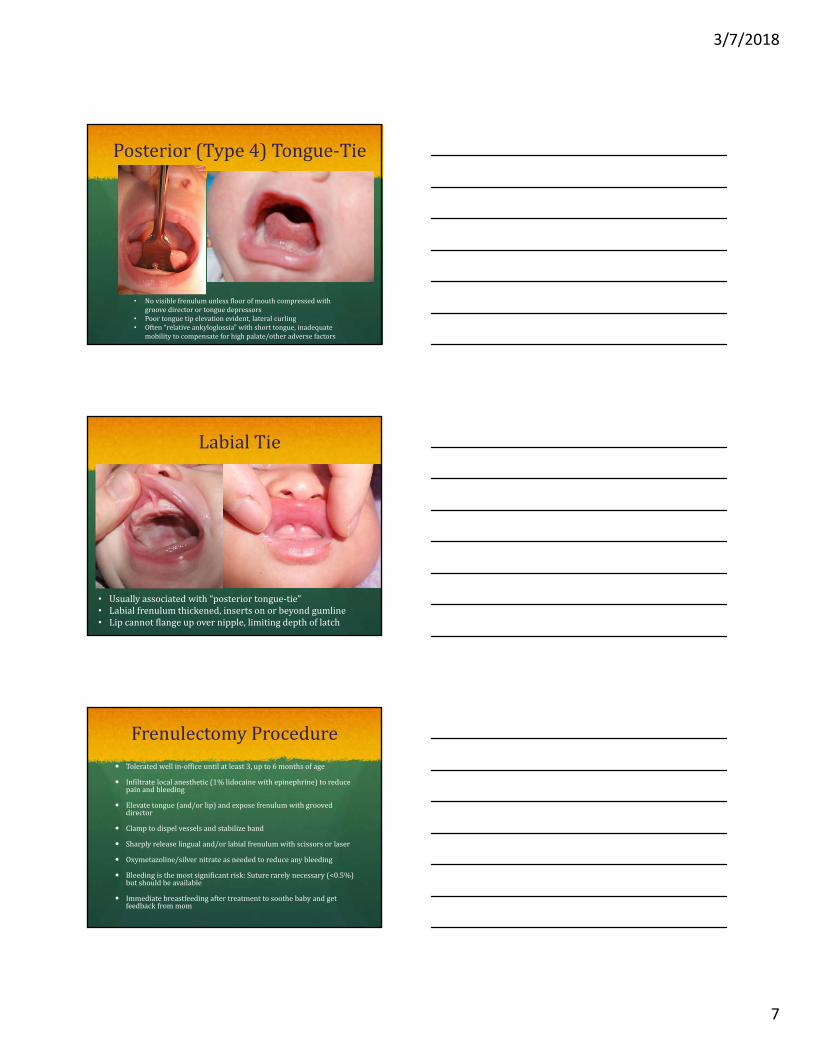
Posterior(Type4)Tongue‐Tie
• Novisiblefrenulumunlessfloorofmouthcompressedwithgroovedirectorortonguedepressors
• Poortonguetipelevationevident,lateralcurling• Often“relativeankyloglossia”withshorttongue,inadequate
mobilitytocompensateforhighpalate/otheradversefactors
LabialTie
• Usuallyassociatedwith“posteriortongue‐tie”• Labialfrenulumthickened,insertsonorbeyondgumline• Lipcannotflangeupovernipple,limitingdepthoflatch
FrenulectomyProcedure
Toleratedwellin‐officeuntilatleast3,upto6monthsofage
Infiltratelocalanesthetic(1%lidocainewithepinephrine)toreducepainandbleeding
Elevatetongue(and/orlip)andexposefrenulumwithgrooveddirector
Clamptodispelvesselsandstabilizeband
Sharplyreleaselingualand/orlabialfrenulumwithscissorsorlaser
Oxymetazoline/silvernitrateasneededtoreduceanybleeding
Bleedingisthemostsignificantrisk:Suturerarelynecessary(<0.5%)butshouldbeavailable
Immediatebreastfeedingaftertreatmenttosoothebabyandgetfeedbackfrommom
3/7/2018
8
Whentodoit Anatomyisnotirrelevantbutisnottheprimaryconcernintreatment
decision.Favorreleasewhenfeedingpattern(function)andexamaresuggestiveofstructurallatchrestriction,evenwhentongue‐tieisitselfnotobvious
Recommendedevenwithnormalfeedingiftightenoughtopotentiallyaffectspeech(i.e.anteriortype1‐2)
Noturgentunlessunabletobottlefeed,buttheearlierthebetter
maladaptivecompensatorymaneuvers
decreasedmilksupply
generalanesthesiarequiredinolderinfantsandchildren
Parentaloptionorwaitingperiod,especiallyinequivocalcases
Goalistoworkwiththebaby’sanatomytotreatthetreatablefactorsandachievemaximumsaferelease
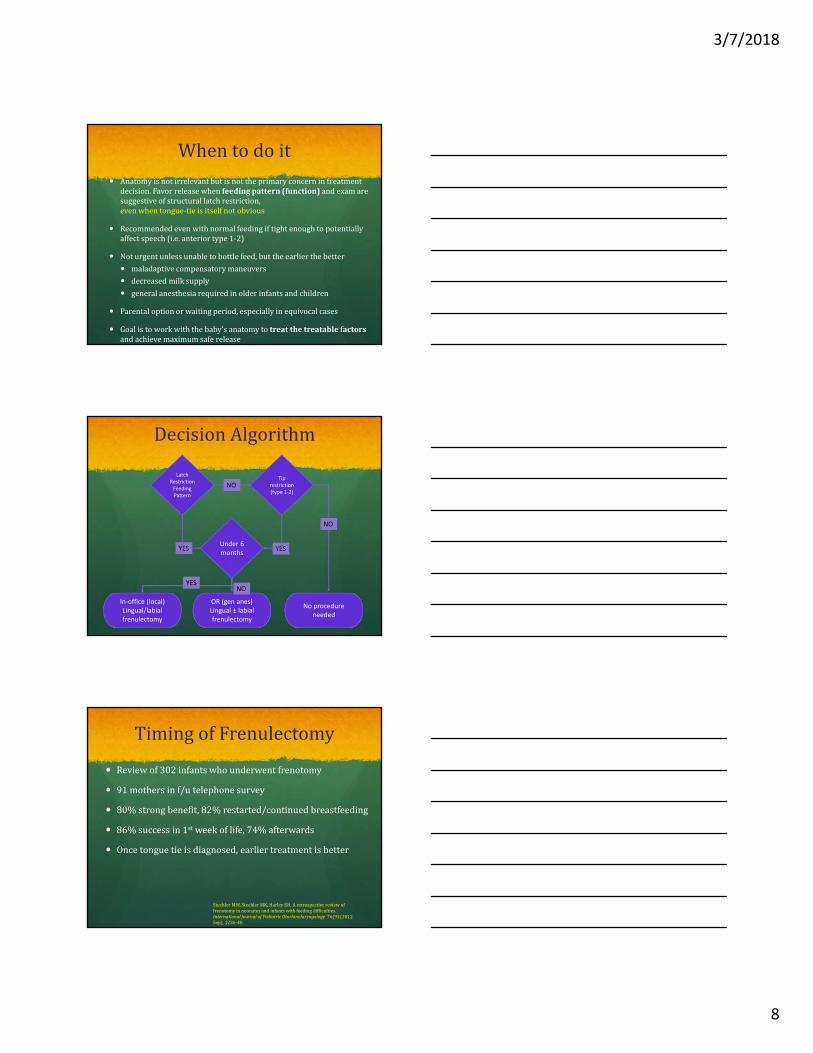
DecisionAlgorithm
Latch Restriction Feeding Pattern
Under 6 months
Tip restriction (type 1‐2)
YES
NO
YES
YES
In‐office (local) Lingual/labialfrenulectomy
OR (gen anes) Lingual ± labialfrenulectomy
No procedure needed
NO
NO
TimingofFrenulectomy
Reviewof302infantswhounderwentfrenotomy
91mothersinf/utelephonesurvey
80%strongbenefit,82%restarted/continuedbreastfeeding
86%successin1st weekoflife,74%afterwards
Oncetonguetieisdiagnosed,earliertreatmentisbetter
SteehlerMW,SteehlerMK,HarleyEH.Aretrospectivereviewoffrenotomyinneonatesandinfantswithfeedingdifficulties.InternationalJournalofPediatricOtorhinolaryngology 76(9)(2012Sep),1236‐40.
3/7/2018
9
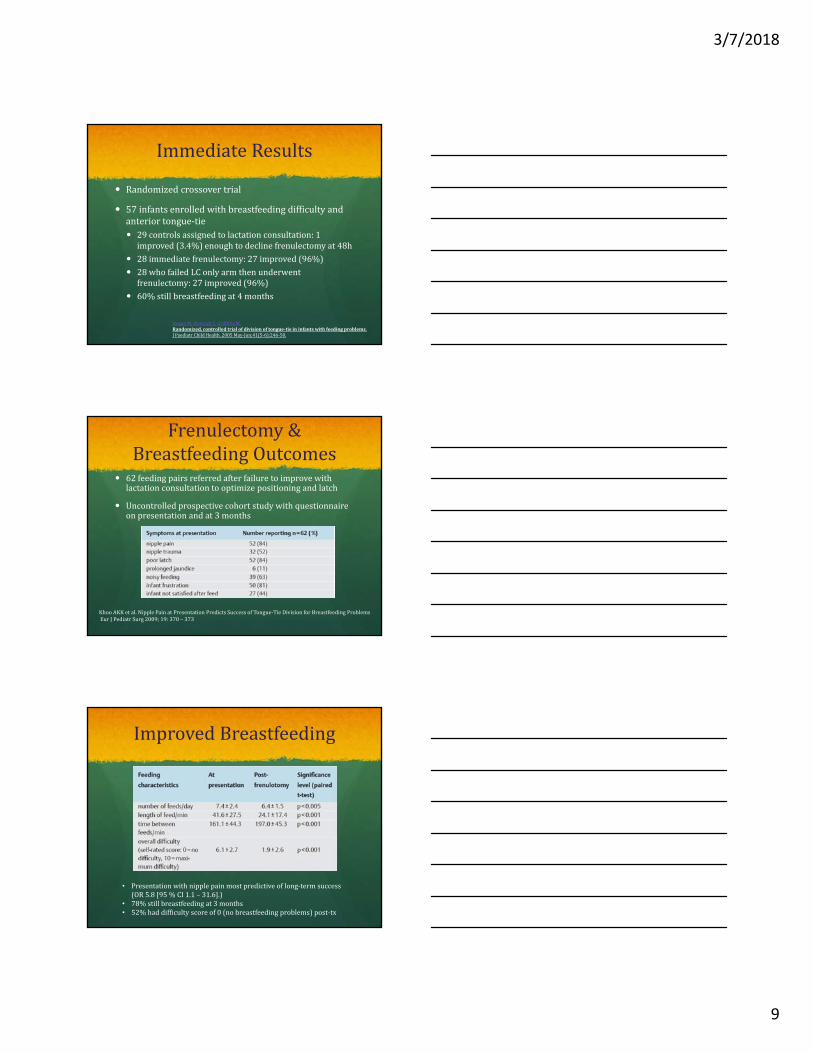
ImmediateResults
Randomizedcrossovertrial
57infantsenrolledwithbreastfeedingdifficultyandanteriortongue‐tie 29controlsassignedtolactationconsultation:1improved(3.4%)enoughtodeclinefrenulectomyat48h
28immediatefrenulectomy:27improved(96%)
28whofailedLConlyarmthenunderwentfrenulectomy:27improved(96%)
60%stillbreastfeedingat4months
HoganM,WestcottC,GriffithsM.Randomized,controlledtrialofdivisionoftongue‐tieininfantswithfeedingproblems.JPaediatrChildHealth.2005May‐Jun;41(5‐6):246‐50.
Frenulectomy&BreastfeedingOutcomes
62feedingpairsreferredafterfailuretoimprovewithlactationconsultationtooptimizepositioningandlatch
Uncontrolledprospectivecohortstudywithquestionnaireonpresentationandat3months
KhooAKKetal.NipplePainatPresentationPredictsSuccessofTongue‐TieDivisionforBreastfeedingProblemsEur JPediatr Surg 2009;19:370– 373
ImprovedBreastfeeding
• Presentationwithnipplepainmostpredictiveoflong‐termsuccess(OR5.8[95%CI1.1– 31.6].)
• 78%stillbreastfeedingat3months• 52%haddifficultyscoreof0(nobreastfeedingproblems)post‐tx
3/7/2018
10
UltrasoundConfirmation
24infantswithankyloglossiaexperiencingpersistentbreastfeedingdifficultiesdespitelactationadvice
Ultrasoundimagestakenfrombelowthejaw,beforeandafterfrenulectomy,showedimprovedbreastfeedingasdefinedby
Decreasedjawexcursion(i.e.lessbiting/chomping) Lesscompressionofthenipplebythetongue Betterattachmentwithlessfrequentseparation Increasedmilktransfer Alsoassociatedwithlessmaternalpain
GeddesDT,LangtonDB,GollowI,JacobsLA,HartmannPE,SimmerK.Frenulotomy forBreastfeedingInfantsWithAnkyloglossia:EffectonMilkRemovalandSuckingMechanismasImagedbyUltrasoundPediatrics2008;122:e188–e194
AdditionalReportedBenefits
Increasespost‐frenotomyin: meaninfantmilkintake(50.5ml→69.1ml) meanmilktransferrate(5.6ml/min→ 10.5ml/min)
meanmaternal24hr milkproduction(455ml→ 615ml)
GeddesDT,LangtonDB,GollowI,JacobsLA,HartmannPE,SimmerK.Frenulotomy forBreastfeedingInfantsWithAnkyloglossia:EffectonMilkRemovalandSuckingMechanismasImagedbyUltrasoundPediatrics2008;122:e188–e194
Anteriorvs.PosteriorTongue‐TieSuccessRates
311infantsevaluatedforfren,299(95%)treated
16%TypeI/II,36%TypeIII,49%TypeIV
37%alsolabial(21%TypeI/II,30%TypeIII,48%TypeIV)
Amongthosewiththesepre‐interventionproblems: Nopost‐interventionlatchdifficulty:100%ant,50%post
Nomaternalnipplepain:79%ant,60%post
Frenulectomycanbesuccessfulinbothgroupsbutmoreposteriortiemorelikelytoberefractorytotreatment
O’Callahan C,Macary S,ClementeS.Theeffectsofoffice‐basedfrenotomyforanteriorandposteriorankyloglossiaonbreastfeeding.InternationalJournalofPediatricOtorhinolaryngology77(2013)827–832
3/7/2018
11
LipTie/PosteriorTongueTie
Retrospectivereviewof618patientsfromadedicatedbreastfeedingdifficultyclinicin2014
47%‐ anteriorankyloglossiaalone19%‐ posteriorankyloglossia6%‐ bothanteriorankyloglossiaandupperlip‐tie5%‐ posteriorankyloglossiaandupper‐liptie2%‐ upper‐liptiealone.21%‐ “noanomaly”
Anteriorankyloglossia:78%reportedsomedegreeofimprovementinbreastfeedingafterfrenotomy.
Posteriorankyloglossia,91%reportedsomedegreeofimprovementinbreastfeedingafterfrenotomy.
Upperlip‐tiereleasealsoledtoimprovedbreastfeeding(100%).Pransky SM,LagoD.,HongP.Breastfeedingdifficultiesandoralcavityanomalies:Theinfluenceofposteriorankyloglossiaandupper‐lipties.InternationalJournalofPediatricOtorhinolaryngology79(2015)1714–1717
LipTie/PosteriorTongueTie
Prospectivecohortstudyof237dyadsfromadedicatedbreastfeedingdifficultyclinicin2014‐15
78%hadposteriortonguetie
75%lip/tonguerelease,25%tongueonly,0.4%liponly
3%requiredrevisionprocedures
Preop,1week,and1monthpostopsurveys BreastfeedingSelf‐Efficacy(BSES‐SF):42.9→52.3→56.5 Visualanalogscale(VAS)fornipplepainseverity:4.6→2.2→1.5 InfantGastroesophagealReflux(I‐GERQ‐R):16.5→13.2→11.6 Breastmilkintakeandtransferratepre‐ /1wk post3.4→4.9ml/min Allchangesstatisticallysignificantatp<0.001
Ghaheri BAetal. BreastfeedingImprovementFollowingTongue‐TieandLip‐TieRelease:AProspectiveCohortStudyLaryngoscope,127:1217–1223,2017
LipTieRecommendations
Morerecentlyrecognizedcontributortolatchrestriction
Nostudiesaddressinglabialfrenulectomyisolatedfromtreatmentoftonguetie,astheytypicallycoexistandaretreatedtogether
Improvedflangingofupperlipallowswidermouthopening,deeperpositionofnipple/areolawithinmouth,increasedcontactsurfacearea andmoreeffectivetonguefunction;“everylittlebithelps.”
5‐10secondsadditionalproceduretime;noadditionalriskorrecoverytime;avoidanceofpotentialsecondprocedure
ThereforeIfavorlipreleasealongwithlingualfrenulectomyunlesslipflangingisclearlyunrestricted

3/7/2018
12
Post‐treatmentcare
Firstfeednotalwayssuccessfulduetonumbnessand/orpain;firstgoalistosoothebaby
30‐50%immediateresponserate,80%willhaveimprovementwithinfirst3‐5days
Infantacetaminophenasneeded
Lip/tonguestretchingtohelpreducere‐scarring
Bottlesupplementationasneededtorestmomand/orbaby
LCvisitabout3‐7daysoutishelpfulinconsolidatingimprovementsandaddressingpositioningissues
Post‐treatmentCare
Skintoskintoreducepainandimprovecoordination
Laid‐backbreastfeeding
Kindnessduringstretches
Continuefollowupwiththerapists(especiallyLC,mayalsoincludeST/OT,somefindsuccesswithCST)
Expectprogresswithregressions(“twostepsforward,onestepback”)
ThankYou!