friends of msf uk and ireland agm report 2010
DESCRIPTION
A report on the FoMSF UK and Ireland AGM held on March 6th 2010TRANSCRIPT

…………………………………………………………………………….
March 2010
The Friends of Médecins Sans
Frontières (FoMSF) UK and Ireland
2010 AGM Report
AGM Report 2010 1
………………………………………………………………………….…
Contents
……………………………………………………………………….…… Title Page number
Introduction……….………………………………………………………………………………….…..…….2
AGM Agenda………………………………………………………………………..….…………….…………5
Access to Essential Medicines Report………………………………………………………………6
Winning Essay- FoMSF Essay Competition……………………………………………………….7
Living in Emergency report……………………………………………………………………………..15
Keynote speech by Mr. David Nott…………………………….……………………………………16
MSF Workshops:
1- ‘Acceptance is the best form of protection:
An out-dated concept?’- Paul Foreman..………………………….…………..…...19
2- ‘Challenges to Humanitarianism in 2010:
Changes in the Global Context’- Marc DuBois…………………..…………….…21
3- Field Staff Behaviours and Perceptions of MSF-
Argyris Georgopoulos …………………………………..……………………………….…24
4- Surgery in the Field- Mr. David Nott..………………………………….……….…..26
5- The Challenge of HIV Care in Resource Poor Settings:
Why it is an Emergency?’- Dr. Melanie Rosenvinge…………………………..28
FoMSF workshops:
1- New committees workshop- Julia Neely………………………….…………………30
2- Events workshop- Aya Taniguchi………………………..……………………….…..…32
3- Where to now?- Peter Siordet Scolding.................................................34
Plenary session……………………….……………………………………………………………..….…...36
Co-option motions and voting details……………………………………..…………….…..….…38
Feedback………………………………………………………………………………..…………….…..…….39
AGM Report 2010 2
………………………………………………………………………….…
Introduction
……………………………………………………………………….……
Dear all,
Welcome to the Friends of Médecins Sans Frontières (FoMSF) UK and Ireland 2010 Annual
General Meeting Report.
We held the 4th
FoMSF AGM at Imperial College University, London on 6th March, where
more than 120 students from 27 universities across Ireland and the UK attended.
Agenda
The day was split into two halves. The morning kicked off with individual group and national
committee updates. A talk on MSF’s 'Access to Essential Medicines' campaign was followed
by election presentations. The second half of the day saw the naming of the new
committee, a key note speech by Mr David Nott, and two rounds of workshops before a
plenary panel session. We also held our first post AGM Social which was very well attended.
Also new this year was the travel subsidies, available to representatives of those groups who
had to travel furthest. The level of uptake of these suggested that they were extremely
useful!
The registration fee was slightly increased to £5.00 this year to cover the costs of the social.
As in previous years we tried to keep this charge as low as possible (and the FoMSF AGM
remains, to our knowledge, one of the least expensive conference days in the UK or
Ireland!) as it is understandable that travel is already a significant expense.
Contents
This report will detail the day’s events, providing notes on the keynote presentation by Mr
David Nott, and the Access to Essential Medicines talk by Katy Athersuch. We uncover what
was discussed during each of the 5 MSF workshops held in the afternoon, and the 3 FoMSF
workshops. Also included are Piyush Sarmah’s winning essay from the very first FoMSF essay
competition, and some feedback from those who attended the AGM.
We will look forward to the coming year and discuss our plans and prospects. New paths to
venture along over this year include a continuing to expand the current FoMSF movement,
to set-up a ‘post-FoMSF’ group, and a new, much developed model of advocacy, in line with
MSF itself, as well as seeking to increase nationwide publicity of FoMSF events and projects.
‘Exporting the FoMSF idea’
We heard briefly of the spread of ‘the FoMSF idea’ in Ireland and Canada. After passing a
motion to allow the National Committee to annually co-opt members where there may be
an advantage (full text included in report), our first co-opted position, was the FoMSF

AGM Report 2010 3
……………………………………………………………………………
Ireland Liaison. The Ireland Liaison will help to provide better support and communication
as a focal point for the Irish groups collectively as they continue to develop and proliferate
as an integral part of the FoMSF movement
Contact Group Report
After almost a year of discussions, the FoMSF-MSF Contact group made its preliminary
report. It proposed the developing of a new model of advocacy and the initiation of a new
Post-FoMSF group, potentially open to all interested graduates. This group would have a
number of aims to build a community of members and to help them to continue engaging
with MSF in ways more appropriate to non-students. Attendees had the opportunity to
volunteer to be a part of the organising committee for both projects.
New National Committee Positions
Three new NC positions were elected to meet the needs of a growing movement. The Web
Liaison, who will be in charge of the FoMSF webpages and the a forthcoming new online
forum, the Communications Liaison who will put together the E-newsletter and FoMSF
documents and finally the Campaigns officer will take the lead in the development of
FoMSF’s advocacy work.
The year ahead
This year’s AGM covered many topics and threw up many indications for FoMSF to really
focus on next. The FoMSF “Where to Now?” workshop was extremely useful in airing some
of the problems, ideas and intentions FoMSF groups have worked with over the past year.
Several themes really stood out in all that was said, homing in on what makes us unique,
what inspires us, and how we can help each other remain as motivated and determined to
see success in 2010/2011.
Our efforts over will remain directed towards our three aims:
1. To raise awareness of Médecins Sans Frontières, and of humanitarian issues in general.
2. To encourage students to think about working for organisations such as MSF in the
future.
3. To raise funds for MSF.
Over the next year therefore, we suggest three emphases in the way we go about these
aims, deriving directly from the AGM. These are IDENTITY, CONSISTENCY and COMMUNITY.
Identity was a word recurrently mentioned throughout the day, both the identities
belonging to FoMSF and to MSF itself. There still much room for movement-wide
improvement in awareness of MSF’s work and its guiding principles and for familiarity with
FoMSF’s core aims and activities.
The latter point leads into the second emphasis of consistency. This has relevance both
within individual groups, and right across the movement. At the local group level, groups

AGM Report 2010 4
……………………………………………………………………………
can familiarise themselves with all the resources now available, so that (in theory) groups
throughout the UK and Ireland are able to work in similarly supported and resourced ways.
Where resources are not forthcoming or relevant, sharing of ideas and experience with
other groups and with the National Committee will help to work towards a consistently
inspired, active and well-supported network!
Lastly, community was a desire strongly expressed both during the day and at the social.
Meeting up once a year is not enough! Some suggestions included regional conferences and
workshops, and more joint events between FoMSF groups like the 2010 FoMSF London Fun
Run.
We hope that the 2010 FoMSF AGM was a day for forming relationships, sharing ideas and
making the most of opportunities for insight into and gaining inspiration from the work of
MSF itself. If we continue over the forthcoming year to work with the commitment, passion
and enjoyment shown by those attending then we will surely see another exciting year full
of opportunities and success. We thank you all for your contributions to the success of the
2010 AGM, and look forward to what the next 12 months have in store.
Almas Janjua, President, FoMSF National Committee 2010-11
Peter Siordet Scolding, President, FoMSF National Committee 2009-10
AGM Report 2010 5
……………………………………………………………………………
AGM 2010 – Agenda
…………………………………………………………………………… AM
09:00 – 10:00 – Registration
10:00 – 10:05 – Open
10:05 – 11:20 – Group Presentations – Parts I & II
11:20 – 11:45 – National Committee Updates
11:55 – 12:10 – Contact Group Update
12:10 – 12:15 – Living In Emergency – Film Trailer and talk – Polly Markandya
12:15 – 12:40 - Access to Essential Medicines Talk – Katy Athersuch
12:40 – 12:45 – Hosting Bids – AGM 2011
12:45 – 13:00 – National Committee Election presentations
LUNCH
13:00 – 14:00 – Lunch and voting (Votes in by 13:55)
PM
14:00 – 14:05 – NC Election and hosting results
14:05 – 14:10 – Winning Essay Presentation - FoMSF Essay Competition 2009-10
14:10 – 14:40 – ‘Haiti’ – Mr David Nott – Key Notes Speech
14:50 – 15:35 – MSF Workshops
15:40 – 16:20 – FoMSF Workshops or Break
16:20 – 16:45 – Reports from Workshops and Motions
16:45 – 17:25 – Plenary Panel session – questions and discussion
17:25 – 17:30 – Close
17:30 – LATE – SOCIAL
AGM Report 2010 6
……………………………………………………………………………
Access to Essential Medicines –
A talk by Katy Athersuch
…………………………………………………………………………… Report by Huanghuan Li
The talk raises the awareness about the need to campaign for increasing access to essential
medicine in parts of the world that is less developed. The aim of the campaign is to improve
access and stimulate development of the medical tools including drugs, diagnostics and
vaccines and to improve the medical care available to the population in developing
countries.
During the talk, Ms Athersuch effectively explained the two primary reasons for the
shortage of access to the medicine. One is the unavailability. The healthcare need for the
population from poor countries is not met by current research and development. Only one
percent of the drugs produced in the last 30 years targets tropical diseases such as
tuberculosis that are most prevalent in developing countries. This is simply the result of low
commercial intensive to direct the development of drugs for people in ‘resource-limited
settings’ as quoted from Ms Athersuch. Another reason is unaffordability. Annual cost of
HIV treatment in 1999 was $12,000 per patient per year. This is simply unfeasible for
developing nations to afford. Drug monopoly exercised by pharmaceutical companies does
not help that as well.
Through campaign for increasing access to essential medicines, there is one example of
major achievement since 1999. That is the drastic decrease in price in anti-retroviral drug
from $12,000 to $80 through competition from generic drugs. MSF had set up clinics in
Africa to prove that HIV treatment can be realistic and applicable even in poor settings.
Media pressure has also forced a pharmaceutical company to drop their case for their HIV
drug monopoly. In Doha declaration, governments have accepted that public health is the
primary goal.
All these achievement towards better access to essential medicines is achieved through
relentless public campaigning, lobbying, advocacy and negotiation.
In 2006, there was a strong campaign against lamivudine/zodovudine patent. In the end,
GSK withdrew the drug patent application in India under pressure and Thailand government
continued to import cheaper HIV drug from India. This allows HIV patients who could not
afford the patented, expensive new HIV drugs from these countries could still have access to
the generic drugs to be saved.
After the years of successful campaigning, MSF continues to work for new priories. They are
to address the concerns of eradicating tuberculosis, malnutrition and HIV, increasing access
to vaccination and lastly, to have more innovation and access by encouraging more generic
drug competitions.

AGM Report 2010 7
.……………………………………………………………………………
Friends of MSF Essay Competition 2009-10
Category 3- ‘Situations’
……………………………………………………………………………
Winning Essay 2009-10
Statelessness as illustrated with the ‘stranded Biharis’ – could there
be hope for all other stateless people?
Piyush Sarmah
On June 11th
2010 more than a billion pairs of eyes from across the globe will shift their gaze
to South Africa, where the fortunes of 32 countries competing in the FIFA World Cup ™ will
be followed eagerly by many fans. And yet even today in the 21st
century there are still
surprisingly large numbers of people who would not have anyone to support in such a
tournament because they are without a nation. These are the so-called ‘stateless people’,
some 6.6 million of whom the United Nations High Commissioner for Refugees (UNHCR)
identified in 58 countries worldwide in 2008. This is more than double the figure for 2007,
although it has been estimated that the true figure of stateless persons around the world
may actually be almost twice as large. 1
Nevertheless, ‘statelessness’ has been described by
Refugees International as an ‘international blind spot’ for it is a humanitarian issue that has
received relatively little attention, and progress on finding solutions has been slow.
A stateless person in broad terms is an individual who has neither nationality nor citizenship
of any country, either because their country does not exist or because the state which they
claim to be part of does not accept them as its citizens. According to the 1954 Convention
Relating to the Status of Stateless Persons, they have no legal bond of nationality with any
state. 2 As a result they are denied basic rights including work, education, property

AGM Report 2010 8
……………….……………………………………………………………
ownership, minimal healthcare from the state and free movement. There are some people
whose statelessness is better known: the plights of the Kurds in the Middle East, the Roma
in Europe and the Palestinians are known worldwide. But there are many lesser known
groups who find themselves marginalised and whose situations are virtually unknown. For
example, two million members of so-called ‘hill tribes’ in Thailand lack numerous legal rights
despite being born in the country, 1
and two million Rohingya Muslims in Burma were
stripped of their citizenship by the government in 1982 to try and force them to leave the
country. 3
The issues and problems that stateless people worldwide face can be illustrated in
the case of a large group of people who until very recently thought their struggle for
recognition would never cease.
On August 15th
1947, India gained its independence from the British Empire but was
partitioned along religious lines into modern-day India, composed of mainly Sikhs and
Hindus, and the Muslim state of Pakistan with two countries, East and West, situated on
either side of India. 4
The largest mass migration in human history occurred with
approximately 14.5 million people crossing the borders between India and Pakistan; Hindus
and Sikhs moved into India and Muslims travelled to East and West Pakistan, precipitated by
communal violence that had taken hold throughout the country. 4, 5, 6
One group of people
that migrated into East Pakistan from India were Urdu-speaking Muslims from the Indian
state of Bihar in the northeast of the country, lured by the promise of a Muslim homeland
but also fleeing from religious persecution in India. 7
At this point it is important to note that
within the South Asian countries there are many different people with their own cultures,
values and languages. This is why the Biharis in their new country found themselves to be a
minority amongst the majority Bengali population, but they identified more with the West
Pakistani elite that dominated both countries. 8

AGM Report 2010 9
…………………………………………………………………………….
In 1970 the Bengali population in East Pakistan declared independence from the West. In
the ensuing conflict that followed, in which many atrocities were committed by both sides,
the Biharis sided with West Pakistan in fighting to keep a united country. 9 However, after
the entry of India into the war, and the subsequent victory and independence that followed
in 1971 for the new nation of Bangladesh as it stands today, the Biharis were outcast
because of their collaboration with the ‘enemy’ of Pakistan and their identification as
‘Pakistani’. Incredibly though, the very state that the Biharis had supported throughout the
entire conflict, and whose very existence had brought them to migrate from India in the first
place, also refused to accept them, possibly for fears of heightening cultural and ethnic
tensions in an already fragile society. 10, 11
A promise was made to repatriate these
individuals and bring them to Pakistan, but although approximately 100000 people ended
up being repatriated, the rest of the process stalled and this promise was not realised. As a
result, approximately 250000-300000 people became stateless and have existed in this
manner for almost four decades. 1, 4, 12
To this day 66 refugee camps located throughout Bangladesh (the biggest one of which is
ironically named ‘Camp Geneva’) house the Biharis, who live in the squalid conditions
synonymous with these places: severe overcrowding, poor sanitation, lack of water supplies,
lack of an infrastructure and just abject poverty. ‘Accommodation’ for families is limited to
small spaces which may measure as little as ten by eight square feet and yet within the
same spaces families of up to 12 people, sometimes even more, somehow manage to sleep.
10 Sanitation is so poor that within some camps it has been reported that there is only one
toilet for 3000 people. With this lack of sanitation come infectious diseases and water-borne
illnesses and these are compounded by the lack of refuse collection and disposal in the
camps and co-habitation with animals. These conditions become even worse in a country
with a monsoon season, as rainwater gets through the inadequate roofing of many of the
refugees’ homes. The vast majority of children in the camps do not receive a proper
AGM Report 2010 10
……………………………………………………………………………
education, for example in Geneva Camp, which has an estimated population of more than
35000 inhabitants, there is one non-governmental school available to only 371 pupils. 13
These children are therefore unlikely to develop the skills and knowledge necessary for
future employment, if indeed they have any chance at all of acquiring this.
Despite the scale of the crisis and the seriousness of the conditions in the camps, medical
care is very limited, sometimes even non-existent. A quick search on MedLine for medical
articles on the Biharis does not even yield any results for papers reporting on the medical
conditions within the camps themselves in Bangladesh, only on the Bihari refugees that
were eventually repatriated to Pakistan. Not only have the world’s governments failed to
act for the Biharis in trying to end their statelessness, but likewise it seems that
international humanitarian organisations have also failed to provide the minimum standards
of the appropriate healthcare required in such disasters. 14 The UNHCR, although putting
pressure on the Governments of Bangladesh and Pakistan to find a solution, has not
properly addressed the plight of the Biharis, 15 and according to the terms of the 1951
United Nations Convention Relating to the Status of Refugees 16 does not actually recognise
them as ‘refugees’, thus depriving them of the benefits that are extended to refugee
populations. 12 Another problem lies in the fact that only 65 countries are party to the 1954
Convention, not including large nations such as the USA, Canada, India, Russia or China. 17
This only adds more fuel to the argument that not only have the Biharis’ problems, to a
huge extent, been ignored by the whole world, but also those of the other populations of
stateless people scattered globally. 18
Fortunately in recent times events have taken a turn for the better, raising hopes for an end
to the many years of suffering of the Biharis. In May of 2008 the Bangladesh High Court in
Dhaka ruled that any Urdu speaker born in Bangladesh, or whose father or grandfather were
born in Bangladesh, and who had permanently resided in the country since 1971 were

AGM Report 2010 11
……………………………………………………………………………
eligible for Bangladeshi citizenship. They also became eligible to register on the electoral roll
for the country’s general elections which took place in December of that year, and after
doing this to register in order to receive their national identity card and then a Bangladeshi
passport. 19, 20 The sudden passing of the judgement represented a breakthrough in the
Biharis’ struggle for recognition by a state, and for many of the young people living in the
camps it represented the chance to escape the complete misery that they had experienced
from birth. It also brought a modicum of hope to all stateless people around the world,
showing that positive and possibly decisive action had been brought about after much
persistence by the Biharis and those acting on behalf of their fight for recognition.
But despite the seemingly happy news there are many unanticipated matters. Firstly, the
ruling of the High Court does not apply to those Biharis who were adults at the time of
Bangladesh’s independence in 1971 but who were not born there, or who were born in
India and crossed the border into the former East Pakistan in 1947. 21
This creates a problem
for the younger generation seeking citizenship because they cannot simply abandon the
elder members of their families. Moreover, some of the older Biharis do not want
Bangladeshi citizenship at all and still pledge allegiance to Pakistan, clinging to the belief
that the latter will eventually repatriate them to their desired homeland. 16
In addition,
while the Biharis will gain many of the basic rights afforded with nationality to a specific
country, there is no guarantee that the existing prejudice and hatred directed towards them
from the Bengali population will cease. Their ambitions to work their way up through
Bangladeshi society may be abruptly halted by the discrimination against them that still
persists amongst Bengalis and which will take a long time to be eradicated. Integration into
Bangladeshi society is likely to be difficult, due in part to cultural differences as is found all
through the subcontinent. The refugees are also continuing to live in the camps; the
younger generation, those happiest about the ruling, may take many years to work and earn
enough money before they can leave, and even then finding significantly improved living

AGM Report 2010 12
……………………………………………………………………………
conditions in one of the poorest countries on Earth will prove to be a challenge for them.
The time and resources that Bangladesh can commit to ensuring successful integration of
more than 150 000 people are questionable, and it is to be expected that outside aid from
the UN and international donors will be required to achieve this.
All of the issues regarding the Biharis apply to stateless persons worldwide. It is important
to understand the history and complex political issues which lie at the heart of all cases of
statelessness, and unless these are resolved then no solution will ever be found.
Unfortunately there is no international organisation specifically representing stateless
people; while the UNHCR has set out plans to improve their identification, another large
stumbling block in finding solutions, 22
it is likely that neither it nor other humanitarian
organisations has sufficient resources and funds to bring about legal action against the
countries involved to force many rulings. While the Biharis may have scored a sizeable
victory, cynics can point to the extreme goodwill from the Bangladeshi government that
occurred without much external pressure, something unlikely to be exhibited in other
countries. For the time being, the least that the world’s governments can do is to speak out
to acknowledge the presence of the problem, its scale and to recognise that swift action is
needed. Pressure should be maintained on the nations concerned to bring about solutions
and ensure that people like the 103 000 Hindu-speaking Nepali Bhutanese, forced to leave
Bhutan in 1991 to ‘preserve its Buddhist character’ and now living in refugee camps in Nepal
where they are prohibited from working, 23
can finally end their torment - brought about by
political actions and events that many of them do not understand, and which have
prevented them from leading normal lives with the basic rights that should be afforded to
every human being, including that of nationality. 24

AGM Report 2010 13
………………………………………………………………….…………
References
1. United Nations High Commissioner for Refugees. Global Trends 2008: Refugees, Asylum-
seekers, Returnees, Internally Displaced and Stateless Persons. United Nations High
Commissioner for Refugees, 2009
2. United Nations. Convention Relating to the Status of Stateless Persons. United Nations
Economic and Social Council resolution 526 A (XVII), 1954
3. Garcia S, Olson C. Rohingya: Burma’s forgotten minority. Refugees International Field Report.
Washington: Refugees International, 2008
4. Berkeley B. Stateless people, violent states. World Policy Journal. 2009; 26(1): 3-15
5. French P. Liberty or Death: India’s journey to independence and division. London: Flamingo,
1997
6. Collins L, Lapirerre D. Freedom at Midnight. London: Harper Collins Publishers, 1997
7. Sen S. Stateless refugees and the right to return: the Bihari refugees of South Asia – part 1.
International Journal of Refugee Law. 1999; 11(4): 625-45
8. Rahman MDM, van Schendel W. ‘I am not a refugee’: rethinking partition migration. Modern
Asian Studies. 2003; 37(3): 551-84
9. Hashmi TU. The ‘Bihari’ minorities in Bangladesh: victims of nationalisms. [Online]. Available
from:
http://www.statelesspeopleinbangladesh.net/uploaded_files/articles/TheBihariMinoritiesIn
Bangladesh.pdf
10. Lynch M, Cook T. Stateless Biharis in Bangladesh: a humanitarian nightmare. Refugees
International Bulletin. Washington: Refugees International, 2004
11. U.S. Committee for Refugees and Immigrants. World Refugee Survey 2000. U.S. Committee
for Refugees and Immigrants, 2000
12. Farzana KF. The neglected stateless Bihari community in Bangladesh: victims of political and
diplomatic onslaught. Journal of Humanities and Social Sciences. 2008; 2(1): 1-19

AGM Report 2010 14
…………………………………………………………………………
13. Southwick K, Calabia D. Bangladesh: maintain momentum to guarantee citizenship rights.
Refugees International Bulletin. Washington: Refugees International, 2008
14. Steering Committee for Humanitarian Response I. The sphere project: humanitarian charter
and minimum standards in disaster response. Geneva: Sphere Project, 1998
15. Lynch M. Lives on Hold: the human cost of statelessness. Washington: Refugees
International, 2005
16. United Nations. Convention Relating to the Status of Refugees. United Nations General
Assembly resolution 429 (V), 1951
17. United Nations High Commissioner for Refugees. States Parties to the 1954 Convention
Relating to the Status of Stateless Persons. [Online]. Available from:
http://www.unhcr.org/3bbb0abc7.html
18. Frelick B, Lynch M. Statelessness: a forgotten human rights crisis. Forced Migration Review.
2005; 24: 65-6
19. Majumder A. Bangladesh citizenship right divides Biharis. Reuters India. [Online] May 20
2008. Available from:
http://in.reuters.com/article/southAsiaNews/idINIndia-33670220080520?sp=true
20. BBC News. Citizenship for Bihari refugees. BBC News. [Online] May 19 2008. Available from:
http://news.bbc.co.uk/1/hi/world/south_asia/7407757.stm
21. Aziz S. Stranded Biharis: saga of a forgotten people continues. Saudi Gazette. [Online]
December 16 2008. Available from:
http://www.saudigazette.com.sa/index.cfm?method=home.regcon&contentID=2009121657
192#
22. United Nations High Commissioner for Refugees. UNHCR Global Appeal 2010-2011 -
Addressing Statelessness. [Online]. Available from: http://www.unhcr.org/4b02c5e39.html
23. Spiegel PB, Qassim M. Forgotten refugees and other displaced populations. The Lancet.
2003; 362: 72-4
24. United Nations. The Universal Declaration of Human Rights. United Nations General
Assembly resolution 217 A (III), 1948

AGM Report 2010 15
……………………………………………………………………………
Living in Emergency- Introducing the MSF film
……………………………………………………………………………
Report by Jonathan Messing
Living in Emergency is a full length film shot commercially, but subsequently lost money,
and due to copyright issues, has been difficult to show until recently. Since 4th
February, the
film can be legally shown in educational institutions by Friends of MSF groups, however
guests must be invited – either through targeted posters in the educational environment or
through internet media such as facebook - and so should not pay a fee to watch. The film
demonstrates the extreme ends of the MSF experience; the joy of saving lives and genuinely
helping the natives, contrasted with volunteers folding under the pressure they are put
under. Consequently, the film was hailed as being incredibly realistic, and will throw up
many questions by the end of its hour and a half duration, leading to the strong
recommendation that when showing the film, an MSF speaker is present to answer
questions. From January 2011, the restrictions on its showing will be made even more lax.
AGM Report 2010 16
……………………………………………………………………………
‘Haiti’
Keynote Speech by Mr David Nott, MSF Surgeon
……………………………………………………………………………
Report by Joel Cunningham
Mr David Nott is a General and Vascular surgeon who is based in London. He spends one
month a year working for Médecins Sans Frontières (MSF) around the globe. Previously,
most of Mr Nott’s placements were in warzones. During his key note speech at this year’s
Friends of MSF AGM he discussed the challenges he met in Haiti as part of the MSF team in
the aftermath of the earthquake in January 2010.
Mr Nott first set the scene before the earthquake. Haiti has a colourful history, and since its
independence from France in 1804 the country has seen national debt, coups, revolts and
dictators, most recently in the form of ‘Papa Doc’ and ‘Baby Doc’. Its capital, Port-au-Prince,
was home to 3 million inhabitants.
The earthquake happened on January 12th 2010, with an epicentre approximately 30km
west of Port-au-Prince. It is estimated that around 190,000 people died within the first three
hours following the quake, rising to 270,000 within the first three days. Around 600,000
inhabitants were injured. Despite only being a ‘moderate’ earthquake on the Richter scale,
the ripple effect that spread out from the epicentre caused enormous damage to the
already poor infrastructure. There have been many notable catastrophic earthquakes in the
past decades all over the world, but this earthquake represented a “unique level of
awfulness”.
MSF sprang into action. The day after the earthquake in January, Mr Nott received the call
from Nell at the MSF UK office. It took a few days to sort out his surgical schedule in London,
but before long Mr Nott was on a plane to Haiti.
Mr Nott shared with us some of his pictures of the devastation he found on arrival in Haiti.
Collapsed houses were surrounded by survivors finding refuge in tents. One 20-storey
hospital had collapsed like a concertina into a pile of rubble barely 20ft tall. After only a few
days in the 40-50°C heat, decaying bodies were posing a large sanitation problem.
The rapid international aid effort had ensured that, after only a few days, water and food
supplies were reaching the areas in need. However, whatever healthcare was there
previously had been crippled. Before the quake, MSF had staff in four hospitals in Port-au-

AGM Report 2010 17
……………………………………………………………………………
Prince. Mr Nott described how one of these, “Trinity Hospital”, had collapsed, tragically
killing patients, nurses and an orthopaedic surgeon. These hospitals had to be replaced with
tents and canvas coverings on the roadside so that the injured could be treated. Severe
maxillofacial injuries were being sent out to the USNS Comfort, a United States hospital ship
with 1000 beds. Those staying on land were operated upon in makeshift surgical units inside
ship’s containers.
After the first four days of Mr Nott’s trip, MSF had delivered a new inflatable hospital and
work began to construct it on a football pitch in the middle of Port-au-Prince. Staff worked
day and night to pump the tents full of compressed air, constructing a hospital with wards,
two operating theatres and space for 200-300 patients. The inflatable tents alone cost €2
million. Local survivors volunteered to maintain the cleanliness of the hospital, vital given
the poor sanitation in the earthquake hit city.
MSF had managed to provide a digital X-ray machine and a range of equipment for the
theatres, including tools for skin grafting. However, the team were still aware they were
working in a fragile environment and were occasionally hampered by aftershocks.
A large portion of the surgical cases required orthopaedic surgery. Those unfortunate to
have serious crush injuries often had no alternative to an amputation. Mr Nott noted that
many patients had already been given ‘guillotine’ amputations before he even saw them.
Abdominal gunshot wounds were common, but Mr Nott explained that the presence of the
American GIs had seemed to minimise violence and gunshot wounds. Mr Nott worked with
a maxillofacial surgeon to repair some of the more difficult injuries, and the team were even
able to provide some plastic surgery to those patients who had suffered extremely
disfiguring trauma. There were also some non-trauma cases, including abdominal
perforations from typhoid fever and intestinal parasitic worms.
The media focus on Haiti was undeniably large in the aftermath of the earthquake. As well
as the positive media coverage of the humanitarian relief efforts, there was also questioning
by the media about the humanitarian aid action during the very first few days following the
quake. Mr Nott showed one French article which questioned the reasons behind the
enormous number of amputations that had taken place by a wide range of surgeons who
seemed to have set themselves up in Haiti. With no one overseeing the combined
humanitarian aid efforts, it will be difficult to ever know if these amputations were done for
the right reasons.

AGM Report 2010 18
……………………………………………………………………………
The large scale media interest drew the attention of a number of celebrities. The MSF team
received a visit from Angelina Jolie, and Mr Nott took great pleasure in showing us the
photo of him standing a mere four places away from the actress. Ms Jolie dug deep and
donated $1 million to MSF France for their operation in Haiti.
Mr Nott ended his talk with the story of Landina Seignon, a three month old girl with
missing parents. She had survived the earthquake but had undergone an amputation and
was at risk of an infection in her brain from a burn wound. Mr Nott found himself in a
difficult position where he couldn’t fulfil his duty to give her a proper ‘standard of care’ in
the environment in which he was based. He explained that the MSF team couldn’t
adequately treat her and the hospital ship wouldn’t take her. He felt he had to find
somewhere that could. Together with the ‘Facing The World’ charity, Mr Nott prepared for
Landina to be taken back to the UK for potentially life-saving specialist treatment. Aviation
Sans Frontières and British Airways worked together to transport Mr Nott, Landina and a
specialist paediatric anaesthetist back to the UK. Here, she has received lifesaving treatment
in the Great Ormond Street Hospital, and there are plans to repatriate her once she has
recovered. Ultimately, Mr Nott felt he couldn’t compromise his standard of care to Landina,
and despite the overwhelming conditions he strived to take Landina to a place where she
would get the care she deserved.
Mr Nott’s final words to us demonstrated how he dealt with working in Haiti following such
an appalling natural disaster.
“Keep Calm & Carry On”
Further reading:
https://www.facingtheworld.net/
http://www.msf.org.uk/video_inflatable_hospital_haiti_20100128.news
http://www.dailymail.co.uk/news/worldnews/article-1251524/Landina-Seignon-British-
doctors-prepare-operate-Haitian-baby-maimed-earthquake.html
AGM Report 2010 19
……………………………………………………………………………
MSF Workshops
……………………………………………………………………….……
1- ‘Acceptance is the best form of protection: an out-dated concept?’
Report by Richard Menzies-Wilson
Facilitator: Paul Foreman
Paul Foreman started professional life as a manager in the construction industry. He has
worked in the voluntary sector since 1994, having started in humanitarian relief in a small
NGO in Bosnia. He then worked in development in Eastern Europe, and relief in a number of
countries with UK charity Merlin. Paul joined MSF in 2002 and worked as head of mission in
Angola, Republic of Congo, Sudan, DRC & Iraq. He is currently on the board of MSF UK and
working as a business development advisor in the UK voluntary sector.
Workshop Focus: Theoretically, the ‘three pillars’ of an effective security strategy are
acceptance, avoidance and protection. The theory also states that you can use any mix of
emphasis, as long as each of the three pillars is present in some form. MSF chooses to put
itself in the front line in humanitarian crises, and so limits reliance on avoidance; to what
extent can it rely on its acceptance by the beneficiary community as the mainstay of its
security strategy?
Scenario Event: The earthquake in Haiti. MSF has been present in the country since 1991.
Context as described in the background reading – debate how to proceed....
Humanitarian security is based on 3 pillars:
1. Acceptance by the local community
2. Avoidance of inflammatory situations
3. Protection measures
Acceptance:
• Most important form of security for MSF
• By being seen to be independent, neutral and impartial, whilst delivering a good
service a great deal of protection is brought. Hence the ‘white land cruiser’
protection.

AGM Report 2010 20
……………………………………………………………………………
• Although this is being undermined by the ubiquitous adoption of white land cruisers
by all parties in conflicts.
• Participation of locals is essential to gaining their trust and acceptance
• By focusing on the medical needs of the population and maintaining impartiality,
NGOs gain more acceptance
• Involve all local parties in discussions and be aware of their needs when planning
interventions
• Make clear to rebel and fraction groups that looting medical facilities will have
repercussions on their image locally and internationally.
Avoidance:
• Avoid fraternising with any military groups for protection.
• Avoid inflammatory behaviour. In the case where bearing witness is deemed
worthwhile, be aware of repercussions.
Protection:
• Local security where necessary
• Be wary of militarised humanitarianism, through working with military
• Try and avoid using firearms for security, unless absolutely necessary.
Compromising MSF values:
• When adopting representatives from local populations it is sometimes necessary to
compromise impartiality. You want the best educated and most able to help you
with implementation. By very virtue, these often represent the most wealthy and
powerful within a society.
• Does the Hippocratic oath still apply in conflict/emergency situations? What
compromises do humanitarian medical workers have to take? Mr. Nott: “Do not
compromise your medical principles.”
• But some principles should never be compromised. For example neutrality should
not be compromised for the sake of ease, where one warring party offers protection
in return for treating their patients first.
• ICRC does not compromise on circumstances under any circumstances.
AGM Report 2010 21
……………………………………………………………………………
2- ‘Challenges to Humanitarianism in 2010: Changes in the Global Context’
Report by Katherine Fok
- Facilitator: Marc DuBois
Marc DuBois is Executive Director of MSF-UK. After spending 2 ½ years in Burkina Faso
with the Peace Corps, Marc worked for a time as a lawyer in the USA. He joined MSF in
the 1990s and after missions in Sudan and Angola, he spent six years working in
Amsterdam as advisor, researcher and later Head of the MSF-OCA Humanitarian Affairs
Department. He joined MSF-UK as Executive Director in 2008.
- Workshop Focus: Over the past decade, a number of global trends have affected the
context in which MSF works. From the Global War on Terror and changing patterns of
conflict to new relationships with actors in crises; from globalisation and ‘immediacy’ to
new diseases, new transmission routes and new health programmes; from climate
change and urbanisation to poverty and inequality, how is the world in which
humanitarians work is being shaped by these changing forces?
Our world is changing.
Marc divided the audience in two, with each section discussing some topics in small groups,
before bringing everyone back together.
Points from each topic included:
Globalisation - is everywhere
Oil prices increasing means more expensive travel costs, but ultimately impacts malnutrition
in urban centres
Global warming and climate change – some potential long term consequences were
discussed. Increasing number of natural disasters such as floods, tsunamis and earthquakes
would be evident. There would be a rise in the frequency of droughts and therefore famine.
Economies can be affected by changes in migration patterns.
Would a warm climate in the developed world finally result in a malaria cure?
Urbanisation
MSF is used to setting up in camps without authority figures or established services.
Urban centres require more organisation and co-ordination (and bureaucracy)
Cholera in Zimbabwe was exacerbated by transmission through an extensive water system.
AGM Report 2010 22
……………………………………………………………………………
As opposed to decontaminating one well and treating all the immediate cases, the entire
water supply had to be investigated.
Diseases - HIV, TB and some superbugs were mentioned. There is a requirement for long
term funding and resources. Research into treatment needs to be increased to support
these plans.
Does continuity of care fit with MSF's ethos?
Tackling disease on a global level may requires a sophisticated approach and more
experienced personnel - not MSF's demographic.
Verticalisation - A model that has been rising due to the changes in funding.
Well-funded organisations are able to provide comprehensive programmes from prevention
to end-care for one particular condition but does that lead to the redistribution of resources
away from basic healthcare? Would this worsen the situation for neglected diseases?
There would be a definite change in the pattern of morbidity in years to come.
Immediacy – A debate about the free flow of information
Some pros include the chance to find out about disasters/outbreaks sooner. For those
suffering from oppression of healthcare this can be very liberating.
But actions have far-reaching consequences.
We recall the time when MSF was expelled from Sudan and represented as spies and
thieves. This was broadcast in Arabic with implications on MSF’s work as far away as
Pakistan.
Currently MSF’s work in Palestine is watched all over the world and analysed. Because of
this MSF has to carefully plan whatever is said officially and by MSF workers and associates
informally online. There are far reaching influences on dynamics with other countries - visas
and permits are not an easy task anymore.
Strong State Capacity
Darfur, Sri Lanka, Pakistan, Ethiopia, Yemen have stopped or made MSF retract statements.
They are less reliant on western countries and therefore diplomacy from the West to
prevent MSF expulsion has less effect. Ministries within these countries are improving and
shrinking MSF's operational portfolio which is great but the standard of care is not
necessarily at the level that MSF would be providing. Does the level of access present
already mean a shifting in MSF's remit to chronic care?
Countries of operation want more control over NGOs - making restrictions on
qualification/registration, taxation, imports and exports, protocols (should MSF follow
substandard protocols from that country or go against it? Their ‘gold standard’ of treatment
is often different from MSF’s which is based on the very latest evidence)
Is this legitimate control of their people?
AGM Report 2010 23
……………………………………………………………………………
Western Powers Decline – In the recent geopolitical shifts.
We realised there is a possibility that countries who are no longer dependent on Western
aid and aid from newly developed countries may not have the same humanitarian provisos
attached.
Global War On Terror – how has it impacted humanitarian agencies like MSF?
NGOs are often funded by the same western powers who are occupying the country in
question, for this reason MSF has to be transparent about where funding is coming from. It
aims to be completely neutral and impartial but comments such as that of Colin Powell
calling MSF a "force multiplier" can impact on its work and ability to access politically
unstable areas.
Aid has become a part of the Afghanistan military strategy - "win over hearts and minds,"
building hospitals; making aid a part of the military weapon, what implications does this
have for MSF’s work?
At the end of the session, the discussion was opened up to all with people pulling apart the
above ideas and how best to deal with them as they become more prominent in MSF’s
work.
AGM Report 2010 24
…………………………………………………………………………….
3- ‘Field Staff Behaviour and Perceptions of MSF’
Report by Kirsty MacLeod
- Facilitator: Argyris Georgopoulos
Argyris Georgopoulos is the MSF UK Learning and Development Officer. He has over 3
years MSF experience delivering preparation courses for ‘first missioners’ and generally
looking after training matter in MSF.
- Workshop Focus: How does the behaviour of MSF staff affect perceptions of MSF in the
field and what is the impact on the programmes we manage?
Scenario Event: Several examples of different behaviours and voting/discussing whether
they are acceptable or not and why.
This workshop explored and challenged the ideas and perceptions that participant held
about MSF Staff and their roles and responsibilities in the field. From exploring team
dynamics and respecting local customs, the workshop gave participants the opportunity to
think about issues outside the traditional
Argyris Georgopoulos, a learning and development officer from MSF, who works with those
health professional and co-ordinators about to deploy out into the field for the first time,
gave an interesting and dynamic workshop. The following issues were discussed:
• Is it right to get angry with a local national or fellow team member, if a mistake is
made, in front of the rest of the hospital or clinical team?
An interesting variation of opinions existed. Whilst the majority felt that in every
circumstance shouting and getting angry was not the way to solve problems, creating a
blame culture and ineffective team dynamics, it was argued that for the safety of patients
and relying of risks, sometimes shouting is necessary. Despite differences it was
acknowledged by all that shouting generally is not effective and appears unprofessional.
• Is it right to remain silent about a colleagues excessive drinking, despite the fact that
their work remains unaffected?
There was unanimous agreement that it would both be irresponsible and unprofessional not
to tackle the issue of uncontrolled drinking, due to a concern for the mental wellbeing of the
person involved and the unresolved issues behind their drinking.
AGM Report 2010 25
……………………………………………………………………………
• Something has gone missing from the MSF office – should you go to the local police?
Whilst some believed that depending on the nature of the theft, the local police should be
involved, they were reminded of MSF’s impartiality and involvement of the local authorities
could, in some instances, affect their perceptions within the local population and cause the
charity to be seen and taking a non-neutral stance within the country’s politics.
• Is it right to have a relationship with someone when out in the field with MSF?
Although professionally team dynamics are adversely affected, relationships have and do
happen whilst out in the field. However, when they break down the lack of trust that can be
created, and the out of work politics, is always damaging to the team. Consideration must
also be given to local customs and relations with local nationals can be both dangerous to
personnel’s health and MSF’s reputation in an area, where some relationships with
Westerners are considered prostitution.
The workshop also dealt with the way MSF personnel should dress both when working and
socialising, with respect for local tradition and culture being paramount, as well as the issue
of the use of the MSF logo in the form of upholding the organisations reputation and
ensuring personal safety when working in the field.
The workshop was well thought through and raised important considerations about staff
behaviour in the field. It offered an alternative perspective to MSF’s work, often less
considered in light of the glossy “medicine in an austere environment”.
AGM Report 2010 26
…………………………………………………………………….………
4- ‘Surgery in the field’
Report by Rebecca Leo
- Facilitator: Mr David Nott
Mr David Nott has been a Consultant General Surgeon at the Chelsea & Westminster Hospital
and a Consultant Vascular Surgeon at both Charing Cross Hospital and The Royal Marsden &
Royal Brompton Hospitals for 16 years. David has a keen interest in war surgery and spends a
few months every year working for Médecins Sans Frontières and the International Committee
of the Red Cross. His experience with MSF goes back to the 1990s, from his first mission in
Sarajevo, through countries such as Sudan, Yemen, Afghanistan and Iraq. His work in the
Democratic Republic of Congo in 2008 received much media coverage; including operating on 75
gunshot wound victims in 24 hours and performing a life-saving amputation with instructions by
text message. He has very recently returned from a three week mission in Haiti.
This workshop was about MSF missions that required surgical skills. First, Mr. Nott talked about
some of his experiences in MSF. After this, we were able to raise questions and have an interactive
talk.
Some questions that were raised by workshop participants and topics of discussion were:
- Surgical protocol in Haiti
- What does it feel like when going back to the UK after a mission?
- Why do you get involved with MSF missions when they put you in such dangerous situations?
- What is the most memorable experience you have had?
- Is there a language barrier between surgeons in MSF missions?
- At what level is the training of local surgeons and how do MSF doctors help them?
- Why work for MSF one month a year and no longer?
- Why choose MSF over other organizations that undertake similar work?

AGM Report 2010 27
……………………………………………………………………………
Mr. Nott said that it was extremely hard to tune back into normal life when he returned to the UK
after missions, as the environment was totally different. However MSF provided the staff with a lot
of help and support in dealing with the stress and were very supportive overall. He mentioned that it
is very important to wear an MSF t-shirt all the time during a mission, as the situation is usually very
dangerous. Also, he emphasized the importance of ‘speaking fluent French’ if one would want to
consider getting involved with MSF in the future. This is because MSF France is responsible for
allocating most of the surgical jobs, and they prefer to communicate in French, as do many members
of MSF and the people they provide aid to. MSF is his ultimate choice as it provides the best
resources and is best equipped to help him work at his best, and he continues to work for MSF
simply because of his ‘love of doing it’.
Participants of this workshop expressed how they could sense his passion for MSF and learned a lot
about what it is like to be an MSF surgeon.

AGM Report 2010 28
……………………………………………………………………………
5- ‘The Challenge of HIV Care in Resource Poor Settings: Why it is an
Emergency?’
Report by Diane Pople
- Facilitator: Dr Melanie Rosenvinge
Dr Melanie Rosenvinge is a Specialist Registrar in Genito-Urinary/HIV medicine who has
an interest in Infectious Diseases. She currently works at St George’s Hospital, South
London but spent 9 months working for MSF in an HIV/TB/malnutrition project in
Epworth, just outside of Harare, Zimbabwe, returning in August 2009. Whilst there, Dr
Rosenvinge was interviewed in the recent MSF documentary, ‘The Positive Ladies Soccer
Club’.
- Workshop Focus: In 2008 the WHO estimated that approximately 33 million adults were
living with HIV/AIDS worldwide with 40% of those in need of antiretrovirals (ARVs)
receiving them and a significant proportion also being co-infected with TB. Most of the
infections are concentrated in resource-poor areas which lack the infrastructure to
provide even basic healthcare. This workshop aims to explore the challenges faced by
providing HIV/TB care in this context.
- Scenario Event: to be set in Zimbabwe during December 2008 where inflation was in
excess of 231 million percent and there was a near-total collapse of the healthcare
system, a life expectancy of 36 and an HIV prevalence estimated at 16%.
Background Reading: “What is the way forward for health in Zimbabwe?” (C. Todd et al,
Lancet 2010; 375: 606-609)
Dr Rosenvinge distributed a sheet with “HIV Basic Facts” to inform the discussion, which
included WHO guidelines for ARV treatment commencement (CD4 counts<350, or clinical
stage 3 or 4).
ARV treatment can prolong life and prevent opportunistic infections. Missing doses
(through patient non-adherence or interrupted supply) easily leads to resistance. Second-
line treatments have limited availability and are more expensive. This chronic nature of the
disease and its treatment appears to conflict with MSF’s usual operation in “emergencies”.
However in many of the countries where MSF works HIV/AIDS is the number one public
health problem and has a huge economic impact. In Zimbabwe there are further
complications due to the political situation, with corruption, violence and intimidation, and
AGM Report 2010 29
……………………………………………………………………………
the previously good infrastructure has deteriorated leading to poor access to utilities,
limited transportation, and a ‘Brain Drain’ of qualified healthcare workers. While Dr
Rosenvinge was in Zimbabwe this was exacerbated by a cholera outbreak, hyper-inflation
and a national strike.
So HIV care is an emergency – but MSF also needs to plan ahead for the eventual handover
of stable cases to the national services.
An added challenge in resource-poor settings is that there is limited treatment capacity. In
starting ARV there is a long-term commitment by MSF to that patient to provide a reliable
supply of the drugs, which is more difficult to guarantee (especially in large numbers) in the
climate of instability currently experienced in Zimbabwe. In the clinic where Dr Rosenvinge
worked there was a waiting list of >2000 for treatment, but they were only able to start
160/month on treatment.
Several case studies of HIV+ people approaching MSF for ARV treatment were discussed,
illustrating the challenging decisions that must be made when there is limited capacity:
• A pregnant woman, working as a prostitute to support her two other children
• A three year old orphan, already receiving treatment for malnourishment in a feeding
centre
• A nurse working for MSF
• A patient who also has TB, currently responding to treatment but possibly drug-resistant
TB
• A lady with political affiliations who is unable to obtain her ARVs from her normal
treatment centre
• A young single man, very ill with meningitis
• A man who was one of the first patients to be enrolled in the program and has attended
all his follow up appointments over the years and now has a low CD4 count
• A previous patient, who had left to care for family in another village, interrupting
treatment
• A mother of four, with an extremely low CD4 count and bed-bound
AGM Report 2010 30
……………………………………………………………………….……
FoMSF Workshops
…….………………………………………………………………………
FoMSF Workshop 1 – New Committees
Report by Ina Schim van der Loeff
- Facilitator: Julia Neely
Julia is the New Groups Officer on the Friends of MSF National Committee.
- Workshop Focus:
To discuss potential issues which may arise while launching a group and then encourage
groups to develop to meet local demands.
To engender confidence in new/ aspiring Friends committees to progress through the
early and often challenging phases of setting up a group
To inform new and aspiring members about Friends groups with respect to the purpose,
aims and national framework of Friends groups (including currently available resources
and role of New Groups officer) and relationship to MSF-UK
To gather feedback from newly-established groups about their concerns or problems
and collaboratively finding ways to overcome these
This was the first time we had run a workshop for new groups
Topics covered were:
FoMSF 3 core aims
Why start a FoMSF group? Some ideas volunteered were:
- large group of students interested in global health issues and in working for MSF in
the near future (St Andrews)
- follow-up travelling and experience different cultures from gap years (TCD?)
- personal/handful passionate individuals create/discover interest in wider student
community (Leicester)
Some ideas prepared by Julia were to:
- engage with issues
- become ‘global’
- exposure to volunteers from the field
- help in deciding how to go about career humanitarianism
- information about the various career options
- immediate involvement in campaigns

AGM Report 2010 31
……………………………………………………………………………
Liz Crawford in sBMJ: MSF makes you a ‘better clinician’ and a ‘better decision-maker’
We covered the basic process of starting a group:
- sign 3 core aims
- sent FoMSF handbook
- write group constitution
- registration with union
- elect committee members
2 scenarios passed around, number of issues raised:
- one person very much in charge and involved with setting up, if difficult to delegate
risk problems continuity
- becoming recognisable entity (retaining memory, remaining true to identity)
- Affiliation with other societies can be useful to maximise audiences, learn, gain
experience running events etc.
- clinical years and multiple campuses create logistical difficulties, especially difficult if
committee split into different campuses

AGM Report 2010 32
……………………………………………………………………………
FoMSF Workshop 2 – Events Workshop
Report by Charlotte Morris (Cardiff)
- Facilitator: Ayame Taniguchi
Ayame is the Events Liaison on the Friends of MSF National Committee.
- Workshop Focus: The weekend following this AGM sees the largest ever FoMSF joint
event, where almost 250 people from 5-10 universities will run together, aiming to raise
more than £10,000 for MSF. With almost 30 FoMSF groups around the UK and Ireland
now, the potential benefits of working together are massive! This workshop will aim to
gather some ideas together from participants, and then get groups from the same
region talking to each other to try and spark off the next joint event.
Present: Dipal Shah (Nottingham), Tom Conway (Kings), James Barnacle & Holly Kirk &
Charlotte Morris (Cardiff), Lisa Rennie (Aberdeen), Natasha Mistry (Sheffield), Olivia Corn &
Nicola Koo (Cambridge), Lucy Harvard & Marilyn Wan (Birmingham), Fran Butcher (BSMS),
Joel Cunningham (UCL), Himanshu Patel & Joanna Smith (Leicester), Samira Green (Barts,
Events coordinator 2010-2011), Ayame Taniguchi (Imperial, Events coordinator 2009-2010)
Joint Events Ideas
1. Pimms on Pitches – Aberdeen would like to recruit other FoMSF to join the sports
competition. Aberdeen to email around the other FoMSF for more information.
Event template will be useful for individual FoMSF events as well.
2. Sheffield – Northern Run – Sheffield to contact Nottingham, Manchester, Leeds, Hull
and York, Keele, Durham. Use template from South Charity Run?
3. Joint educational workshops – with speakers from different universities.
4. Kings - campaigns/awareness fundraising e.g. balloon race. No cost for transport
between universities involved (like World AIDS day). Kings to expand on this further,
along with all the other FoMSF groups.
5. Photography competition – again, involves organisation by individual FoMSF at each
university (no travelling required). Use event template? If possible, aim for
publication like Cambridge?
6. ‘X without borders’ joint events – competition between FoMSF and e.g. engineers
without borders. Compare scores across different universities.

AGM Report 2010 33
……………………………………………………………………………
Action Points
A) All to join facebook fan page
B) Aya to transfer the information from joint events page to fan page – create a joint
events section
C) Contact each other regarding the events and start planning – date of event, venue,
how to organise, main organiser(s). Samira to help and chase up the event planning
D) Keep communicating and keep up the motivation!
General issues with individual/joint FoMSF events
- Travel – includes meetings. Travel subsidy from FoMSF/sponsorship/any better ideas
- Communication – difficult communicating with some FoMSF through emails and
facebook only. Ask NC to contact as well. Any better ideas?
- Prize collecting – Ask Joanna Davies for endorsement letter. Target smaller
companies/shops.
Action Points
- Ask for help – Post on facebook page, email other FoMSF, email national committee
and Samira

AGM Report 2010 34
……………………………………………………………………………
FoMSF Workshop 3 – ‘Friends of MSF: Where to now?’
Report by Priya Rajesh Shah
- Facilitator: Peter Siordet Scolding:
Pete is ex-President of the FoMSF National Committee.
- Workshop Focus: It is five years since the first Friends of MSF groups began to take
shape. This workshop is a chance to discuss what you think about FoMSF. What makes it
good? What makes it unique? What should we be doing differently? Where are we going
next? Any firm ideas about future areas where FoMSF should be more active or for new
resources can be proposed as a motion, to give the next National Committee a good
idea of what really matters to you.
The session began with introductions from everyone; each person gave their name,
university and one positive or negative about their experiences with running and being part
of a Friends of MSF group. There were definitely some recurring themes, with many people
struggling with the real identity of Friends of MSF. Many commented that it is often unclear
to other students what exactly they get from Friends of MSF and many join with
expectations of going on MSF missions or having more hands on experience. We went
through the three core aims:
• Raise awareness of MSF’s work and humanitarian issues
• Encourage students to work for such organisations
• Raise funds for MSF.
We also discussed ways to overcome this issue, with some great ideas such as visits to the
London office to see what work happens there and how our efforts have an effect on MSF’s
work, as well as ensuring that the speaker events are led by a variety of medical and non-
medical MSF workers. In addition to this, workshops such as ‘Tropical First Aid’ were
reported to be very successful amongst students.
The difficulties with handing over to a new committee each year were also discussed and we
discussed the importance of a clear and guided handover to ensure all the good work of
previous years is not lost when less experienced committee members start out. The national
Friends of MSF handover guide can be particularly useful with this.
On a more positive note, everyone was very impressed to hear the number of FoMSF groups

AGM Report 2010 35
has doubled since last year’s AGM and lots of people were happy
with the cohesiveness of their individual university committees.
The main aims for the next year were to cement the role of FoMSF and what it offers to
students, consider its place within Global Health Forums and Medical societies, extend our
reach to non-medical students and keep up the good work with a particular focus on
publicity to spread the word!

AGM Report 2010 36
……………………………………………………………………………
Plenary Session
……………………………………………………………………………
MSF Plenary Question and Answer Session
Report by Sarah Law
1) The online blog situation?
The main issues with the online MSF Blogs – there is no capacity on the website to allow
public comments to be added to the discussions. However, due to the intense scrutiny of
communications in association with MSF, it is now very sensitive to address issues in the
most open and honest manner than previously.
2) Is it possible for students setting up skill days and weekend courses to have advice on
how to run them?
There are already existing courses such as RADAR in the communications sector. The most
highly demanded individuals are “French speaking medical coordinators.” Therefore it is
advisable to learn French or Arabic rather than just going on courses; and to improve your
clinical and logistical skills to their highest abilities.
3) It will be useful for applicants to know whether they are fully prepared, and allow time to
develop the areas in which they are lacking before applying.
Could MSF develop a specifications list indicating the mandatory skills that they are looking
for when choosing applications?
Yes, they will be looking into this. There are a few specifications already: such as having
prior clinical experience (completed FY2), acquiring a Diploma in Tropical Medicine,
experience working in a tropical environment, being able to demonstrate great
management skills and learning certain languages. You have to register on the website
before you can obtain this information.
AGM Report 2010 37
……………………………………………………………………………
4) Could there be an interagency network of placements, and training for workers in the UK
before going abroad?
MSF have already made links with certain institutions where you can complete Masters
Programmes; School of Tropical Medicine; University of Liverpool’s training courses;
Manchester’s Humanitarian and Conflict Response Institute. However without experience,
diplomas can be seen as useless. MSF is like a stepping stone providing the opportunity to
gain this invaluable experience. Therefore it is incredibly competitive to get an internship on
a study programme as well as an MSF job.
All NGOs would have to discuss this idea, as they don’t just want enthusiastic individuals,
but quality individuals who apply for jobs.
One thing that everyone agreed was important to consider was how to fit Diplomas or MSF
experience in with your training which will be difficult.
5) What are the most pressing issues for MSF today?
– Speak to politicians with evidence to support campaigns and put pressure on
pharmaceutical companies.
– Enhance NGO’s roles of supporting countries by helping them to sustain themselves in the
long term.
– Ensure that the individuals representing MSF have excellent language, management, and
clinical skills to ensure delivery of a high standard quality of care.
– Engage with the wider public about humanitarian issues. They could focus on self-
preservation tactics – stress the value of sharing in order to preserve the benefits we have
already.
– Communications: The struggle for freedom to talk about issues more openly. How do we
address a large organisation “to avoid gagging staff but also to not jeopardise the
operation?”
– Question whether MSF should still focus on the British media response or elsewhere?
Especially when certain governments now have less leverage over other countries.

AGM Report 2010 38
……………………………………………………………………………
Co-Option Motion
……………………………………………………………………………
Version passed by e-vote in March 2010
Title: ‘Co-Opted Members’ on the FoMSF National Committee
Motion proposed by: Peter Scolding, President, FoMSF National Committee 2009-10
Seconded by: Cork FoMSF, Trinity College Dublin FoMSF, Barts FoMSF, Leicester FoMSF
STATEMENT: There are many individuals who are not elected to the National Committee,
but who have experience, expertise or enthusiasm which would greatly benefit the FoMSF
movement.
Over the past year for example the non-National Committee members of the FoMSF-MSF
UK Contact Group, Tom Conway and Lizzie Crowther would have benefited from an official
mandate to represent the movement in the discussions of the Contact Group.
Over the coming year, it might be very useful to the developing movement in Ireland to
have a dedicated representative on the National Committee.
For these reasons I would like to propose a way to do this in the future.
PROPOSAL: We propose that the National Committee should temporarily be able to co-opt
individual students for a specific purpose, so that these individuals have an official mandate
to work for FoMSF.
Any ‘Co-opted Members’ should report in the FoMSF Newsletter and at the next National
AGM, so that they are accountable to all FoMSF groups.
The period of co-option would run until the next National AGM, and there should be a very
limited total number of ‘Co-opted Members'.
AGM Report 2010 39
……………………………………………………………………………
AGM Feedback
……………………………………………………………………………
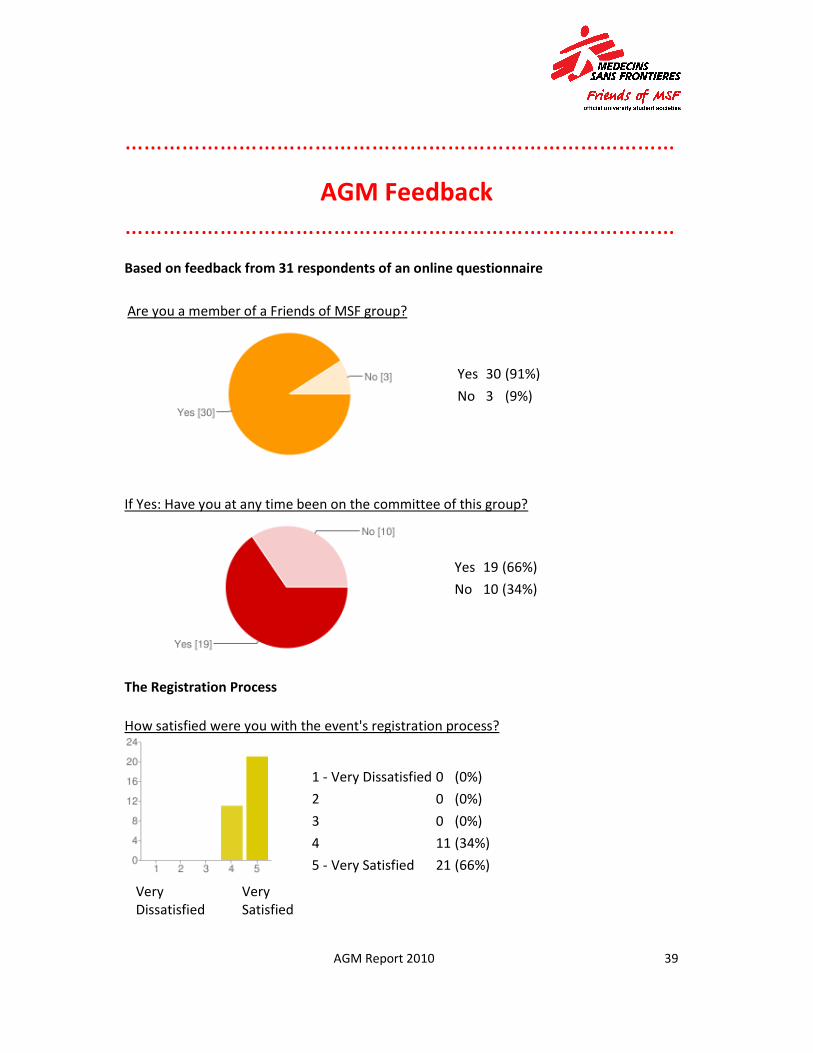
Based on feedback from 31 respondents of an online questionnaire
Are you a member of a Friends of MSF group?
Yes 30 (91%)
No 3 (9%)
If Yes: Have you at any time been on the committee of this group?
Yes 19 (66%)
No 10 (34%)
The Registration Process
How satisfied were you with the event's registration process?
Very
Dissatisfied
Very
Satisfied
1 - Very Dissatisfied 0 (0%)
2 0 (0%)
3 0 (0%)
4 11 (34%)
5 - Very Satisfied 21 (66%)

AGM Report 2010 40
……………………………………………………………………………
How could the registration process be improved?
• Done very efficiently
• Was fine but seemed a bit of a long process.
• I can't think of any improvements.
• Show who else has been registered.
Format and Agenda
How satisfied were you with the event's location?
Very
Dissatisfied
Very
Satisfied
1 - Very Dissatisfied 0 (0%)
2 1 (3%)
3 2 (6%)
4 11 (34%)
5 - Very Satisfied 18 (56%)
Considering the layout of this AGM, with the morning for FoMSF and the afternoon for MSF,
how would you prefer the layout for next year's AGM?
More focus on Friends of MSF, discussion, sharing of ideas, and developing joint
events! 5 (16%)
More focus on MSF, their dilemmas, and our questions answered! 10 (31%)
It was just about right this year. 16 (50%)
Other 1 (3%)
AGM Report 2010 41
……………………………………………………………………………
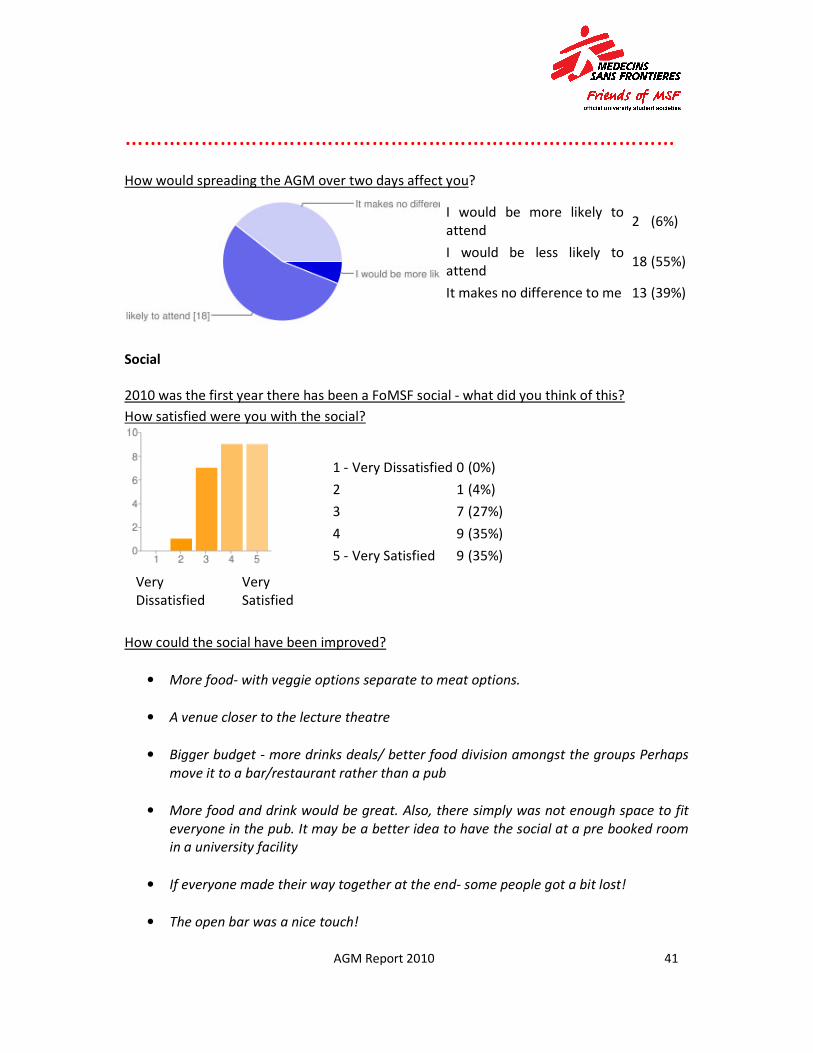
How would spreading the AGM over two days affect you?
I would be more likely to
attend 2 (6%)
I would be less likely to
attend 18 (55%)
It makes no difference to me 13 (39%)
Social
2010 was the first year there has been a FoMSF social - what did you think of this?
How satisfied were you with the social?
Very
Dissatisfied
Very
Satisfied
1 - Very Dissatisfied 0 (0%)
2 1 (4%)
3 7 (27%)
4 9 (35%)
5 - Very Satisfied 9 (35%)
How could the social have been improved?
• More food- with veggie options separate to meat options.
• A venue closer to the lecture theatre
• Bigger budget - more drinks deals/ better food division amongst the groups Perhaps
move it to a bar/restaurant rather than a pub
• More food and drink would be great. Also, there simply was not enough space to fit
everyone in the pub. It may be a better idea to have the social at a pre booked room
in a university facility
• If everyone made their way together at the end- some people got a bit lost!
• The open bar was a nice touch!
AGM Report 2010 42
…………………………………………………………………………
Overall - Reviewing the AGM
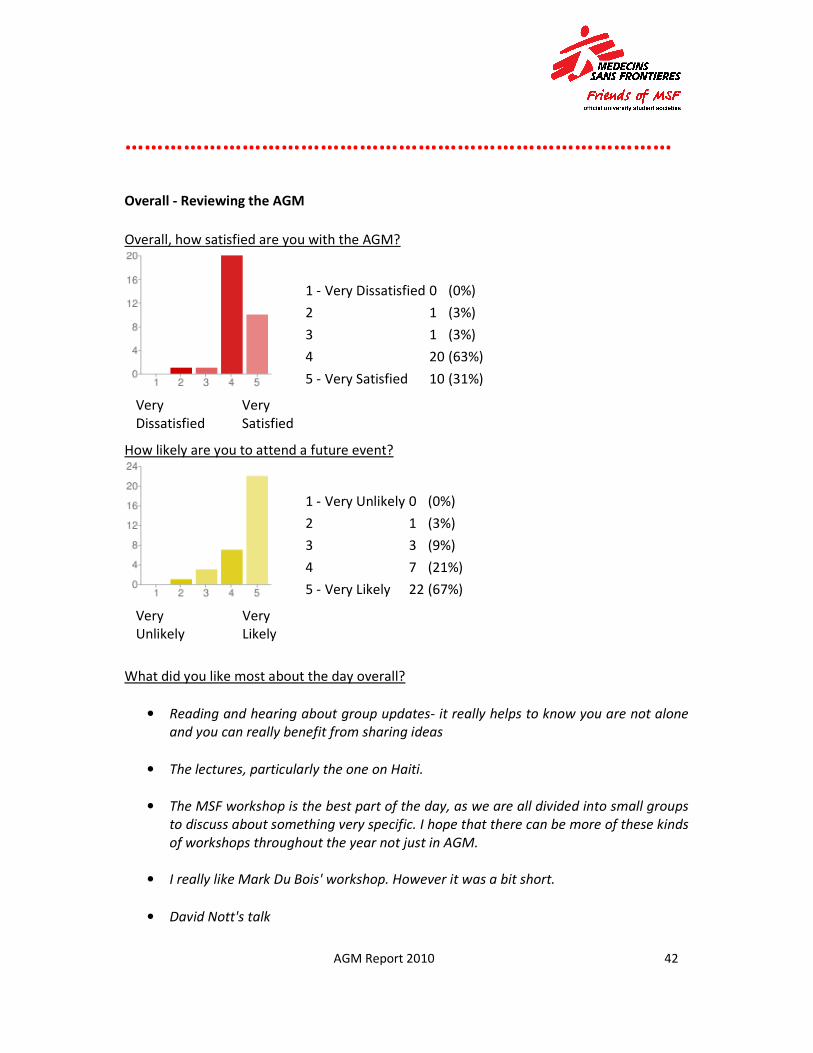
Overall, how satisfied are you with the AGM?
Very
Dissatisfied
Very
Satisfied
1 - Very Dissatisfied 0 (0%)
2 1 (3%)
3 1 (3%)
4 20 (63%)
5 - Very Satisfied 10 (31%)
How likely are you to attend a future event?
Very
Unlikely
Very
Likely
1 - Very Unlikely 0 (0%)
2 1 (3%)
3 3 (9%)
4 7 (21%)
5 - Very Likely 22 (67%)
What did you like most about the day overall?
• Reading and hearing about group updates- it really helps to know you are not alone
and you can really benefit from sharing ideas
• The lectures, particularly the one on Haiti.
• The MSF workshop is the best part of the day, as we are all divided into small groups
to discuss about something very specific. I hope that there can be more of these kinds
of workshops throughout the year not just in AGM.
• I really like Mark Du Bois' workshop. However it was a bit short.
• David Nott's talk

AGM Report 2010 43
………………………………………………………….………………
• MSF workshop was very interesting. (Marc Dubois)
• The surgeon's lecture about his experience in Haiti - fascinating.
• Mr Nott's presentation was fascinating -
great to see behind the headlines of such a recent, major event. Inspirational!
• The question and answer session with the MSF board members.
• The opportunity to meet other like-minded individuals.
• The talk from the surgeon who had been to Haiti, it was very interesting and
inspiring, seeing those photos first hand, not many people would have the chance to
see them and to see what was really going on
• Mr Nott’s speaking!
• The guest speaker (surgeon who worked in Haiti) was a really interesting insight
• Really enjoyed meeting everyone and seeing the enthusiasm
• Dr Nott's talk really inspired me, made me remember why i chose to study medicine,
and made me realise why i put so much effort into FoMSF events.
• It was a great opportunity to meet all the other groups and get ideas for future
events.
• Professor David Nott's keynote speech.
• Meeting and talking to people from other universities with similar interests is great.
The talk from the MSF doctor was fantastic.
• All of it. The keynote speaker and MSF workshops were particularly interesting.
• I liked the presentation from the surgeon from Haiti.
• Meeting other people. New ideas from other groups.
AGM Report 2010 44
………………………………………………………….………………
Are there any things in particular you think you learned or will take away from the day?
• Public speaking! We should not be afraid to speak our mind
• Really liked that the different groups talked a bit about what they have been up to.
Was able to get a lot of new ideas, but had no real opportunity to follow up and ask
them more questions.
• A better understanding of futures issues concerning MSF, how to improve career
potential for working with MSF (e.g. tropical disease course, managerial skills), and
new ideas for FoMSF events - either joint or solo!
• The principles the MSF and FOMSF. How that has impacted on what MSF do.
• The core principals of MSF
• A wider awareness of issues and raised interest in security (thanks to the talk with an
MSF worker in security)
• Further collaboration with other FoMSF societies to address any issues.
• Events ideas
• Ideas from other groups. Discussion from the workshops
• Possibly film showings, type of events, organising events
Is there anything different you would like to see, or something that can be improved upon
for at future events?
• Possibly some more workshops, some more practical/active ones included. such as
wilderness first aid, or scenario discussions etc
• I think the workshops can be longer, so to let us discuss problems in more depth.
• More time on the workshops, maybe more emphasis on getting the different groups
to talk to each other, sharing ideas.
• More time for inter-university group discussion.

AGM Report 2010 45
……………………………………………………………..……………
• Maybe one more guest speaker and less time spent on the individual updates from
FoMSF uni groups - it was very repetitive
• perhaps people could wear name badges to let others know who they are and where
they are from
• It would have been nice since people travelled to give us a free cup of coffee or
snacks during break. Also the directions to lunch were horrible for people from out of
town. Providing box lunches would have been nice and also helping more with funds
for people who travelled far distance.
.
Additional comments or suggestions
• Thanks for a great day!
• Unfortunately, owing to an urgent appointment, I was unable to attend this year,
having attended as an observer and supporter the previous year.
• Thanks a lot for your hard work.
• It was great to meet with other students from other FoMSFs :)-
AGM Report 2010 46
…………….………………………………………………………………
NEW - FoMSF Campaigns and Post-FoMSF Group
FoMSF Campaigns aims to explore how you can participate in highlighting areas of special
interest for MSF such as the Access to Essential Medicine Campaign. For more details email
Alison Arenas : [email protected]
Post-FoMSF will endeavour to maintain contact with FoMSF members once they graduate or
enter different fields of interest. For more details email Peter Scolding :
Your input on these new ideas presented in the Contact Group update will be key in
developing this area of the next year. Please let us know what you thought.
What do you think about the idea of 'FoMSF Campaigns'?
I like it, I think this is something FoMSF should be doing. 28 (93%)
I don't like it, this is not something FoMSF should be doing. 1 (3%)
I did not understand what FoMSF Campaigns might involve 1 (3%)
Other 0 (0%)
Are there any particular issues you think FoMSF should be involved in?
• Would like to hear more about climate change as it is responsible for a lot of the
recent major disasters and more to come.
• Access to health care in the UK
• I am not sure if there are enough resources or chances for this to be done, but i think
it would be a great idea if there can be voluntary works organized in the summer that
are organized by joined university FoMSF, this can get FoMSF members closer
together as a whole and have more interaction between this large society.
• I don't think that there is any one particular issue that we should focus on.
• Access to healthcare for undocumented migrants and failed asylum seekers -
in the UK and abroad
• Humanitarian disasters such as Palestine & the Gaza Strip, Haiti (with reference to
AGM Report 2010 47
…………………………………………..………………………………
its horrendous past and what could have been done to alleviate the suffering of some
of its people), the Democratic Republic of Congo, and scores of other such
circumstances around the globe.
What do you think about the idea of a Post-FoMSF group?
I like it, it would be something I would be interested in. 26 (90%)
I don't like it, I would not be interested in it. 0 (0%)
I did not understand what the group might be. 2 (7%)
Other 1 (3%)
Do you have any ideas or suggestions for what activities or opportunities this group might
facilitate?
• Graduation bash for FoMSF members- where we can meet some inspirational MSF
doctors who can further excite us about our new life!
• Continuing links between MSF and the students and young doctors who have been
part of FoMSF. Making junior doctors' training have some relevance to humanitarian
work.
• I think MSF made it patently clear during the day that they would much prefer
potential candidates focus on professional skills and learning a language, rather than
focus on these FoMSF groups long term
• Opportunities for going abroad.
• I feel that it would be beneficial, both financially and in publicity, for Friends of MSF t
o be extended to interested members of the general public.
• Not particularly, other than to emphasise the need for the Post-FoMSF to work
closely with the new FoMSF groups, so as not to eradicate any previous hard work,
and to pass on useful knowledge and experience.
• Campaigns, fundraising, recruiting health care workers, supporting FoMSF groups, or
ganising short courses and training days, holding events. Not hugely different from w
hat FoMSF does, but with a greater focus on skill-building.
• Skills required to get involved with MSF