from pathophysiology to clinical management€¦ · vascularization of anorectal region, rectal...
TRANSCRIPT

Medicographia
www.medicographia.com
ISSN 0243-3397Vol 41, No. 2, 2019
Quarterly Thematic Journalof Clinical and Therapeutic Research
A Servier Publication
“C hancef a vo r s on l yt he p repa red m ind”
Pa s teu r
19 M
P 0
428
BA
Prin
ted
in F
ranc
e
Servier - 50, rue Carnot - 92284 SureSneS Cedex (FranCe)
www.servier.com
Hemorrhoids: an updatefrom pathophysiology
to clinical management

50
52
56
64
71
77
85
92
EDITORIAL P. Godeberge, France
THEMED ARTICLESV. Lohsiriwat, Thailand
Y. A. Shelygin, Russian Federation
P. Sheikh, India
F. Seow-Choen, Singapore
M. Wunderlich, Austria
CONTROVERSIAL QUESTIONJ. Bocobo, Philippines -M. L. Esquivel Herrera, Mexico - A. Karimuddin, A. Farooq,Canada - K. Madbouly, Egypt - C. Tohme, Lebanon - D. Voiculescu, Romania
THERAPEUTIC OUTLOOK H. P. Yaltirik, France
A S e r v i e r p u b l i c a t i o n
Vol 41, No. 2, 2019
139Hemorrhoids: an update
from pathophysiologyto clinical management
MEDICOGRAPHIA, Vol 41, No. 2, 2019 Hemorrhoidal disease: a very common medical condition – Godeberge50
H
Address for correspondence:
www.medicographia.com
by P. Godeberge, France
EDITORIALThe treatment paradigm needs
to change. Definitive resolution ofall symptoms or complete anatom-ical correction is not a realistic aim.Disease progression varies andthe pattern of treatments must beadapted to each individual to main-tain everyday comfort without ini-tiating a more aggressive proce-dure.”
Hemorrhoidal disease:a very common medicalcondition in the general
population
Philippe GODEBERGE,

E D I T O R I A L
Hemorrhoidal disease: a very common medical condition – Godeberge MEDICOGRAPHIA, Vol 41, No. 2, 2019 51
Keywords: disease progression; hemorrhoidal disease; symptoms; treatment paradigm
MEDICOGRAPHIA, Vol 41, No. 2, 2019 Hemorrhoids: pathophysiology and risk factors – Lohsiriwat52
H emorrhoids are a very common anorectal condition defined as thesymptomatic enlargement and distal displacement of the normal analcushions. However, the exact pathophysiology of hemorrhoids remains
unknown. The current theories surrounding hemorrhoid development involvemechanical injury to the anal mucosa, vascular abnormalities and the hyper-vascularization of anorectal region, rectal redundancy, tissue inflammation,and any combination thereof. The different pathophysiologies may result indifferent approaches to hemorrhoids. Nevertheless, an improvement in ourunderstanding of the pathophysiology of hemorrhoids will prompt the devel-opment of better pharmacological and nonpharmacological approaches tohemorrhoids in the future. This article comprehensively reviews the currentpathophysiology and risk factors of hemorrhoids.
Medicographia. 2019;41:52-55
Introduction
S
Pathophysiology of hemorrhoidsMechanical injury to the anal cushions
Address for correspondence:
www.medicographia.com
H E M O R R H O I D S : A N U P D AT E F R O M PAT H O P H Y S I O L O G Y
TO C L I N I C A L M A N A G E M E N T
The exact pathophysiology ofhemorrhoid development remainsunknown, but it is most likely to bemultifactorial. The different patho-physiologies may result in differ-ent approaches to treating hem-orrhoids.
Hemorrhoids:pathophysiology and
risk factors
by V. Lohs i r iwat , Thai land
Varut LOHSIRIWAT,

H E M O R R H O I D S : A N U P D AT E F R O M PAT H O P H Y S I O L O G Y
TO C L I N I C A L M A N A G E M E N T
Hemorrhoids: pathophysiology and risk factors – Lohsiriwat MEDICOGRAPHIA, Vol 41, No. 2, 2019 53
Vascular abnormalities
Tissue inflammation

H E M O R R H O I D S : A N U P D AT E F R O M PAT H O P H Y S I O L O G Y
TO C L I N I C A L M A N A G E M E N T
MEDICOGRAPHIA, Vol 41, No. 2, 2019 Hemorrhoids: pathophysiology and risk factors – Lohsiriwat54
Rectal redundancy
Risk factors for hemorrhoids
Table I
Strong risk factors (odds ratio >2)
Modest risk factors (odds ratio, 1.1-2.0)
Table I. Risk factors* for hemorrhoids.*Note:The designation of risk categories is arbitrary and regarded as semiquantitative.
Figure 1. Schematic diagram of hemorrhoid development.

H E M O R R H O I D S : A N U P D AT E F R O M PAT H O P H Y S I O L O G Y
TO C L I N I C A L M A N A G E M E N T
Hemorrhoids: pathophysiology and risk factors – Lohsiriwat MEDICOGRAPHIA, Vol 41, No. 2, 2019 55
Conclusions(Fi-gure 1).
Keywords: hemorrhoid disease; inflammation; pathophysiology; risk factors
References1. World J Gastroenterol.
2. Postgrad Med J.
3. Zhonghua Wei Chang Wai Ke Za Zhi.
4. Am Surg.
5. Colorectal Dis.
6. Tech Coloproctol.
7. Br J Surg.
8. Int J Colorectal Dis.
9. J Gas-trointest Surg.
10. Curr Vasc Pharmacol.
11. N Engl J Med.
12. Phlebology.
13. Eur J Clin Invest.
14. Dis Colon Rectum.
15. Ann Nucl Med Sci.
16. Dis Colon Rectum.
17. AmJ Dig Dis.
18. CochraneDatabase Syst Rev.
19. PLoS One.
20. Gastroenterol Clin Biol.
21. BJOG.
22. Dis Colon Rectum.
23. Korean J Fam Med.
24. Am J Gastroenterol.
25. Int J Colorectal Dis.
MEDICOGRAPHIA, Vol 41, No. 2, 2019 Diagnosis and classification of hemorrhoids – Shelygin 56
I n most cases, diagnosing hemorrhoids is not a problem. A typical clinicalpresentation, accessibility for physical examination, and the absence ofthe necessity to perform complex and expensive examinations allow a doc-
tor to quickly establish the diagnosis and determine a treatment approach.However, it is essential to recall the diversity of clinical forms of hemorrhoids,take a thorough patient history, and identify the pathogenetic aspects of theoccurrence and development of each symptom. Hemorrhoids can be both acause and a consequence of the development of serious complications, suchas anemia, or occur on top of systemic diseases, often masking their clinicalpicture. Only a thorough assessment of all aspects of the disease and con-ducting a reasonable differential diagnosis with diseases that have a similarclinical picture can help doctors avoid diagnostic and treatment errors. Inorder to establish the correct diagnosis, determine the treatment strategy, andanalyze the problem in a consistent manner, it is extremely important to havea unified global approach to systematizing the information obtained after study-ing all aspects of the disease. Therefore, the role of the unified adequate clas-sification of the disease is unequivocal.
Medicographia. 2019;41:56-63
Introduction
T
Diagnosis
Address for correspondence:
www.medicographia.com
H E M O R R H O I D S : A N U P D AT E F R O M PAT H O P H Y S I O L O G Y
T O C L I N I C A L M A N A G E M E N T
Differentiated approachesto each patient, an introduction ofnew modern methods of treat-ment, and the possibility of theircombined use, including tradition-al surgical methods for hemor-rhoids, substantiate the need forrevision and modification of thecurrent classifications.
Diagnosis andclassification of hemorrhoids
by Y. A . Shelyg in , Russ ian Federat ion
Yury A. SHELYGIN,

H E M O R R H O I D S : A N U P D AT E F R O M PAT H O P H Y S I O L O G Y
T O C L I N I C A L M A N A G E M E N T
Diagnosis and classification of hemorrhoids – Shelygin MEDICOGRAPHIA, Vol 41, No. 2, 2019 57
Complaints and medical history(Table I).
(Figure 1).
(Figure 2).
Figure 1.Prolapse of
internal hemorrhoids.
Figure 2.Thrombosisof externalhemorrhoid.
Table I. The cardinal symptoms of hemorrhoids. The information is based on a study of 1025 patients with hemorrhoids.
Initial Symptoms at the Symptoms symptoms (%) visit to the doctor (%)

H E M O R R H O I D S : A N U P D AT E F R O M PAT H O P H Y S I O L O G Y
T O C L I N I C A L M A N A G E M E N T
MEDICOGRAPHIA, Vol 41, No. 2, 2019 Diagnosis and classification of hemorrhoids – Shelygin 58
Table I
Physical examination
(Figure 3).
Additional methods of examination

H E M O R R H O I D S : A N U P D AT E F R O M PAT H O P H Y S I O L O G Y
T O C L I N I C A L M A N A G E M E N T
Diagnosis and classification of hemorrhoids – Shelygin MEDICOGRAPHIA, Vol 41, No. 2, 2019 59
(Table II, page 60).
Classification
(Table III, page 61). Rectal Disorders (Table III). (TableIII)(Table III). (Table III).
Coloproctology and the PelvicFloor,
Figure 3.Anoscopy (in the leftside position). Panel A. Internal hemor-rhoid at 3 o’clock position.Panel B. Internal hemor-rhoid at 7 o’clock position.
A B

H E M O R R H O I D S : A N U P D AT E F R O M PAT H O P H Y S I O L O G Y
T O C L I N I C A L M A N A G E M E N T
MEDICOGRAPHIA, Vol 41, No. 2, 2019 Diagnosis and classification of hemorrhoids – Shelygin 60
(Table III). (Table III)
Surgery of the Anus,Rectum and Colon.
Degrees of hemorrhoid formation
Table II. Differential diagnosis of hemorrhoids.
Possible diseases
Complaints
Anorectal bleeding
Hemorrhoidal prolapse
Pain syndrome
Anal itching
Mucous or purulentdischarge from theanal canal
Perianal edema

H E M O R R H O I D S : A N U P D AT E F R O M PAT H O P H Y S I O L O G Y
T O C L I N I C A L M A N A G E M E N T
Diagnosis and classification of hemorrhoids – Shelygin MEDICOGRAPHIA, Vol 41, No. 2, 2019 61
Gabriel39
Hemorrhoids, the veins of the anal canal are increased in number and size, and they may bleed at the time of defecation. They do not prolapse, but merely project into the lumen
Hemorrhoids present to the outside of the anal canal during defecation, but return spontaneously into the anal canal where they remain the rest of the time
Hemorrhoids protrude outside the anal canal and require manual reductionHemorrhoids are irreducible and constantly remain in the prolapsed state
Braytsev40
Internal hemorrhoid prolapse during defecation, but spontaneously reduce into the anal canalInternal hemorrhoid prolapse during defecation or straining, but cannot reduce spontaneously into the anal canalInternal hemorrhoid prolapse during physical exertion, but cannot reduce spontaneously into the anal canal and remain outside
Beique and Siward41
Bleeding, development of anemiaInternal hemorrhoid prolapse during defecation, development of a fissureInternal hemorrhoid prolapse during defecation that requires manual reduction, development of the hemorrhoidal thrombosis
Ryzhikh42
External hemorrhoidsExternal hemorrhoids in the form of a nodeExternal hemorrhoids with thrombosisExternal hemorrhoids in the form of fringes
Internal hemorrhoidsInternal hemorrhoids with bleedingInternal hemorrhoids with recurrences (or in the acute phase)Internal hemorrhoids with hemorrhoidal prolapseInternal hemorrhoids with prolapse of the mucosa of the rectum
Combined (external and internal) hemorrhoids
Smith43 (American classification of hemorrhoids I)Internal hemorrhoids do not protrude from the anal canalProlapse of internal hemorrhoids during defecation with their spontaneous reduction into the anal canalProlapse of internal hemorrhoids during defecation with the need for their manual reduction into the anal canalProlapsed internal hemorrhoids, often with symptoms of thrombosis
Salvati44 (American classification of hemorrhoids II)Bleeding, without internal hemorrhoids prolapseProlapse of internal hemorrhoids with their spontaneous reduction into the anal canal and bleedingProlapse of internal hemorrhoids with the need for their manual reduction into the anal canal and bleedingProlapsed internal hemorrhoids
HenryHemorrhoid maintained with proper level in the anal canalProlapse with bowel movements, but spontaneously reduceProlapse out of the anal canal and require manual reductionProlapsed and incarcerated
BanovInternal hemorrhoids bulge into the anus without prolapseInternal hemorrhoids prolapse during defecation, but spontaneously reduceInternal hemorrhoids prolapse requiring manual reductionHemorrhoids prolapsed and irreducible
State Scientific Centre of Coloproctology, RussiaBleeding only, no prolapseInternal hemorrhoids prolapse, but reduce into the anal canal spontaneously, with or without bleedingInternal hemorrhoids prolapse, but require manual reduction into the anal canal, with or without bleedingPermanently prolapsed hemorrhoids that cannot be reduced into the anal canal, with or without bleeding; the dentate line is visualizedPermanently prolapsed hemorrhoids that cannot be reduced into the anal canal, with or without bleeding; the dentate line is not visualized
Deg
ree
Sta
geD
egre
eS
tage
Deg
ree
Deg
ree
Sta
geG
rade
Sta
geS
tage
1
2
34
123
123
123
1234
1234
1234
1234
1234
1234A4B
Table III. Classification systems for hemorrhoids.

H E M O R R H O I D S : A N U P D AT E F R O M PAT H O P H Y S I O L O G Y
T O C L I N I C A L M A N A G E M E N T
MEDICOGRAPHIA, Vol 41, No. 2, 2019 Diagnosis and classification of hemorrhoids – Shelygin 62
(Ta-ble III)
References1. Surgery of the Anus,Rectum and Colon.
2. Colon and rectal surgery.
3. Hemorrhoids
4. The ASCRS Textbook of Colon and Rec-tal Surgery.
5. Koloproktologia.
6. Am J Gastroenterol.
7. Dis Co-lon Rectum.
8. Gastroenterol Clin.Biol.
9. Dis ColonRectum.
10. PLoSOne.
11. Dis Colon Rectum.
12. Cochrane Database Syst Rev.
13. Am J Gastroenterol.
14. Mi-nerva Gastroenterol Dietol.
15. PLoS One.
16. J Gastroenterol Hepatol.
17. Am J Gastroenterol.
18. Gastrointest Endosc.
19. Biomed Res Int.
20. JAMA.
21. Lancet.
22. Tech Coloproctol.
23. Tech Coloproctol.
24. DisColon Rectum.
25. Am J Surg.
26. Dis Colon Rectum.
27. Gut.
28. Dis Colon Rectum.
29. Br J Surg.

H E M O R R H O I D S : A N U P D AT E F R O M PAT H O P H Y S I O L O G Y
T O C L I N I C A L M A N A G E M E N T
Diagnosis and classification of hemorrhoids – Shelygin MEDICOGRAPHIA, Vol 41, No. 2, 2019 63
30. Br J Surg.
31. Br J Surg.
32. Tech Coloproctol.
33. World J Gastroenterol.
34. Gut.
35. Colorectal Dis.
30. CochraneDatabase Syst Rev.
37. Dis Colon Rectum.
38. Clin Colon Rectal Surg. 39.
Ann Ital Chir. 40. The Principles and
Practice of Rectal Surgery. 41. Diseases of the rectum.
42.
L Union Med du Canada. 43. Surgery of the rectum.
44. Geriatrics.
45. Dis Colon Rectum.
46. Dis Colon Rectum.
47. Coloproctology and the pelvic floor: pathophysiology and manage-ment.
48. J S C Med Assoc.
49. Gastroenterology.
50. J Evid Based ComplementaryAltern Med.
51. IntJ Colorectal Dis.
52. Curr Gastroenterol Rep.
50. Dis ColonRectum.
54. Koloproktologia.
55. Pirogov Russian Journal of Surgery/Khirurgiya. Zhurnal imeni N.I. Piro-gova.
Keywords: classification; diagnosis; hemorrhoid

MEDICOGRAPHIA, Vol 41, No. 2, 2019 Medical management of hemorrhoids – Sheikh64
O nly between 5% to 10% of patients with hemorrhoidal disease will re-quire a formal excision or hemorrhoidectomy. The majority of patientsare treated satisfactorily with medical management. Medical man-
agement has essentially two components – lifestyle/dietary changes and oralphlebotonic drugs. Dietary modification consists of adequate fluid and fiberintake and counseling regarding defecation habits. Topical creams containinglidoocaine steroids, phenylephrine, and herbal extracts have been used forsymptomatic relief, but there is very little evidence to support their use. Flavo-noids are the most common oral phlebotonic drugs used for treating hemor-rhoids. They increase vascular tone, reduce venous capacity, decrease cap-illary permeability, facilitate lymphatic drainage, and have anti-inflammatoryeffects. The commonly used flavonoids are diosmin and oxerutins. Among allthe flavonoids, micronized purified flavonoid fraction (MPFF), an oral phlebo-tropic drug, has proven to be the most effective, particularly due to microniza-tion of the particles with a diameter <2 m. In acute hemorrhoids, MPFF giv-en in a dose of 3000 mg per day for 4 days, followed by 2000 mg per day for3 days has been shown to reduce bleeding and inflammation. Continuing MPFFfor 2 to 3 months can prevent a relapse of symptoms. Using MPFF in the pe-rioperative period can reduce both the duration and extent of postoperativesymptoms and wound bleeding following an hemorrhoidectomy. MPFF canalso be used safely in the third trimester of pregnancy to relieve the symp-toms of hemorrhoids.
Medicographia. 2019;41:64-70
Introduction
H
Address for correspondence:
www.medicographia.com
H E M O R R H O I D S : A N U P D AT E F R O M PAT H O P H Y S I O L O G Y
T O C L I N I C A L M A N A G E M E N T
Drug therapy is the mainstayin the medical management ofhemorrhoids, with oral flavonoidsbeing the preferred drugs. MPFF,due to its micronization, is themost effective flavonoid and it hasbeen shown to decrease almostall symptoms of hemorrhoids.
Managementof hemorrhoidal disease:
medical management
by P. Sheikh, India
Parvez SHEIKH,

H E M O R R H O I D S : A N U P D AT E F R O M PAT H O P H Y S I O L O G Y
T O C L I N I C A L M A N A G E M E N T
Medical management of hemorrhoids – Sheikh MEDICOGRAPHIA, Vol 41, No. 2, 2019 65
Medical management Dietary and lifestyle modification
P
Topical therapy
ABBREVIATIONS
MPFF
OR
RR

H E M O R R H O I D S : A N U P D AT E F R O M PAT H O P H Y S I O L O G Y
T O C L I N I C A L M A N A G E M E N T
MEDICOGRAPHIA, Vol 41, No. 2, 2019 Medical management of hemorrhoids – Sheikh66
Oral phlebotonic drugs
PPPP P PPP
Diosmin
Micronized purified flavonoid fraction
PP

H E M O R R H O I D S : A N U P D AT E F R O M PAT H O P H Y S I O L O G Y
T O C L I N I C A L M A N A G E M E N T
Medical management of hemorrhoids – Sheikh MEDICOGRAPHIA, Vol 41, No. 2, 2019 67
(Fi-gure 1).
PP
Figure 1. Algorithm for the management of hemorrhoids by the Association of Colon and Rectal Surgeons of India practice guidelines. Abbreviations: DGHL, Doppler-guided hemorrhoidal artery ligation; MPFF, micronized purified flavonoid fraction; PPH, procedure for prolapse and hemorrhoids.From reference 18: Agarwal N et al. Indian J Surg. 2017;79(1):58-61. © 2017, Association of Surgeons of India.
H E M O R R H O I D S : A N U P D AT E F R O M PAT H O P H Y S I O L O G Y
T O C L I N I C A L M A N A G E M E N T
MEDICOGRAPHIA, Vol 41, No. 2, 2019 Medical management of hemorrhoids – Sheikh68
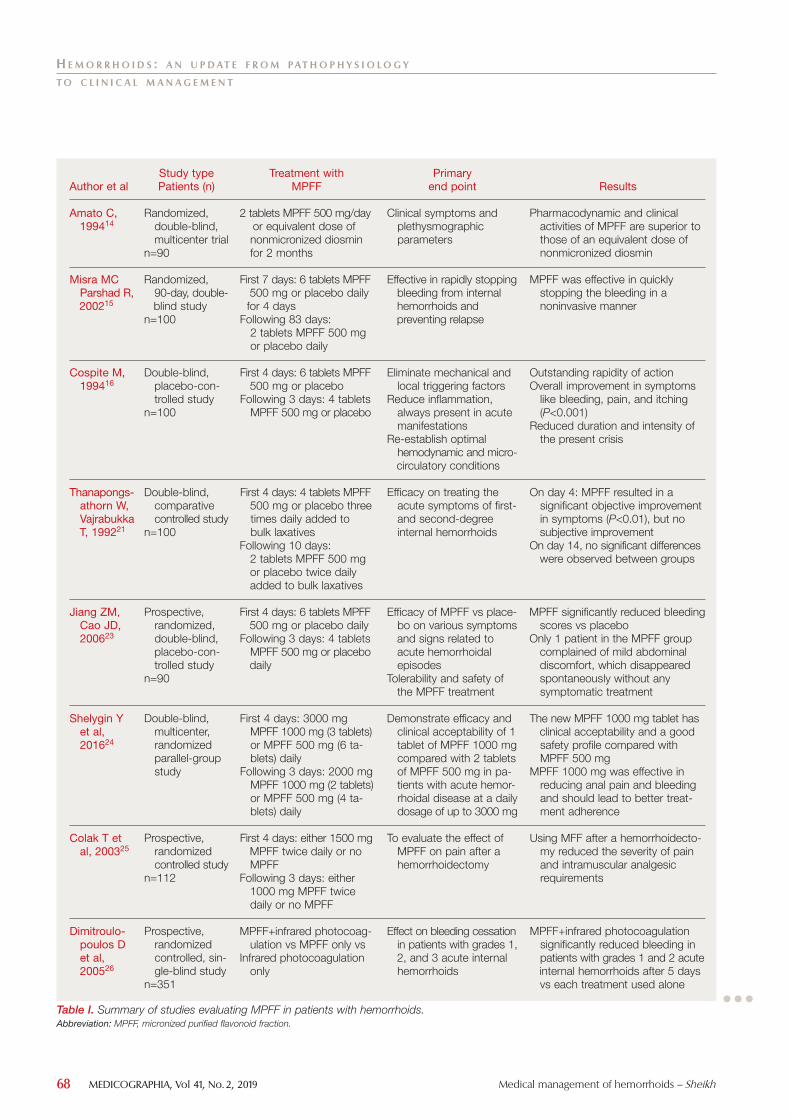
Primary end point
Results
P
P
Author et al
Amato C, 199414
Misra MC Parshad R,200215
Cospite M, 199416
Thanapongs-athorn W, VajrabukkaT, 199221
Jiang ZM, Cao JD, 200623
Shelygin Y et al, 201624
Colak T et al, 200325
Dimitroulo-poulos D et al, 200526
Study type Patients (n)
Randomized, double-blind, multicenter trial
n=90
Randomized, 90-day, double-blind study
n=100
Double-blind, placebo-con-trolled study
n=100
Double-blind, comparative controlled study
n=100
Prospective, randomized,double-blind, placebo-con-trolled study
n=90
Double-blind, multicenter, randomized parallel-group study
Prospective, randomized controlled study
n=112
Prospective, randomized controlled, sin-gle-blind study
n=351
Treatment with MPFF
Table I. Summary of studies evaluating MPFF in patients with hemorrhoids.Abbreviation: MPFF, micronized purified flavonoid fraction.

H E M O R R H O I D S : A N U P D AT E F R O M PAT H O P H Y S I O L O G Y
T O C L I N I C A L M A N A G E M E N T
Medical management of hemorrhoids – Sheikh MEDICOGRAPHIA, Vol 41, No. 2, 2019 69
P
Table I
Other phlebotonic drugs
Primary end point
Results
Author et al
Godeberge P, 199427
Ho YH et al, 199528
Ho YH et al, 200029
Meshikhes AW, 200230
Meshikhes AW, 200431
Navadiya Set al, 201332
Study type Patients (n)
Double-blind, placebo-con-trolled trial
n=120
Prospective, randomized controlled trial
n=228
Randomized controlled trial
n=162
Prospective clinical study
n=105
Multicenter, non-randomized, observational study with no placebo
n=268
Prospective randomized clinical study
n=200
Treatment with MPFF
H E M O R R H O I D S : A N U P D AT E F R O M PAT H O P H Y S I O L O G Y
T O C L I N I C A L M A N A G E M E N T
MEDICOGRAPHIA, Vol 41, No. 2, 2019 Medical management of hemorrhoids – Sheikh70
Summary
Keywords: flavonoid; hemorrhoid; hemorrhoidectomy; MPFF; phlebotonic drugs
References1. Dis Co-lon Rectum.
2. Dis Colon Rectum.
3. Cochrane Database of Syst Rev.
4. Hepatogastroenterology.
5. Am J Gas-troenterol.
6. Drugs. 7. Minerva GastroenterolDietol.
8. Am J Gastroenterol.
9. World J Gastroenterology.
10. Dis Colon Rectum.
11. World J Gastroenterol.
12. CochraneDatabase of Syst Rev.
13. Br J Surg.
14. Angiology.
15. Br J Surg.
16. Angiology.
17. Adv Ther.
18. Indian J Surg.
19. Dis Colon Rectum.
20. World J Gastroenterology.
21. Dis Colon Rectum.
22. Int J Gynaecol Obstet.
23. Curr Med Res Opin.
24. Curr Med Res Opin.
25. Surg Today.
26. Clin Ther.
27. Angiology.
28. Br J Surg.
29. Dis Colon Rectum.
30. Saudi Med J.
31. Surgeon.
32. Int J Med SciPublic Health.
33. CurrMed Res Opin.
34. J Visc Surg.
35. Dis Colon Rectum.
36. Eur J Clin Pharmacol.

Outpatient interventions for hemorrhoidal disease – Seow-Choen MEDICOGRAPHIA, Vol 41, No. 2, 2019 71
H emorrhoids are normal arteriovenous bulges on the wall of the anorec-tum concerned with fine tuning anal continence. Hemorrhoids are nota disease entity unless they cause symptoms. Patients should only be
treated if hemorrhoids are causing problems, but not all patients, even thosewith prolapsed hemorrhoids, need treatment, as many prolapsed hemorrhoidsare asymptomatic. Straining, especially severe straining, when constipatedresults in a shearing force that breaks the suspension of hemorrhoidal tissuewithin the anorectal wall, allowing hemorrhoidal prolapse to occur. Excessivedietary fiber, normal vaginal delivery, and squatting for defecation are impor-tant causative factors of prolapsing hemorrhoids. Symptomatic hemorrhoidsshould be treated according to the presenting symptoms and not on a “one-size-fits-all” basis. Important aspects for the initial treatment of symptomatichemorrhoids are to decrease dietary fiber, stop using toilet paper, use waterto wash after defecation, use posterior perineal support, and take flavonoids.Other serious symptoms, such as bleeding together with prolapse, may re-quire outpatient interventional procedures. Rubber band ligation is a testedtechnique that is safe, cheap, and effective. A laser hemorrhoid procedure isa new procedure that holds some promise, but it is still too expensive for rou-tine usage for most patients.
Medicographia. 2019;41:71-76
Introduction
C
Consultation
Address for correspondence:
www.medicographia.com
H E M O R R H O I D S : A N U P D AT E F R O M PAT H O P H Y S I O L O G Y
TO C L I N I C A L M A N A G E M E N T
Patients should only be treat-ed if hemorrhoids are causingproblems, but not all patients,even those with prolapsed hem-orrhoids, need treatment, as manyprolapsed hemorrhoids are asymp-tomatic.
Managementof hemorrhoidal disease:
a practical approachto outpatient interventions
by F. Seow-Choen, S ingapore
Francis SEOW-CHOEN

H E M O R R H O I D S : A N U P D AT E F R O M PAT H O P H Y S I O L O G Y
TO C L I N I C A L M A N A G E M E N T
MEDICOGRAPHIA, Vol 41, No. 2, 2019 Outpatient interventions for hemorrhoidal disease – Seow-Choen72
十男九痔,十女十痔
Dietary adjustments

H E M O R R H O I D S : A N U P D AT E F R O M PAT H O P H Y S I O L O G Y
TO C L I N I C A L M A N A G E M E N T
Outpatient interventions for hemorrhoidal disease – Seow-Choen MEDICOGRAPHIA, Vol 41, No. 2, 2019 73
Toilet habit and toilet training
Posterior perineal support
Management of pruritis ani

H E M O R R H O I D S : A N U P D AT E F R O M PAT H O P H Y S I O L O G Y
TO C L I N I C A L M A N A G E M E N T
MEDICOGRAPHIA, Vol 41, No. 2, 2019 Outpatient interventions for hemorrhoidal disease – Seow-Choen74
Management of hemorrhoidal bleeding
Table I Table I
Managing painful hemorrhoids
H E M O R R H O I D S : A N U P D AT E F R O M PAT H O P H Y S I O L O G Y
TO C L I N I C A L M A N A G E M E N T
Outpatient interventions for hemorrhoidal disease – Seow-Choen MEDICOGRAPHIA, Vol 41, No. 2, 2019 75
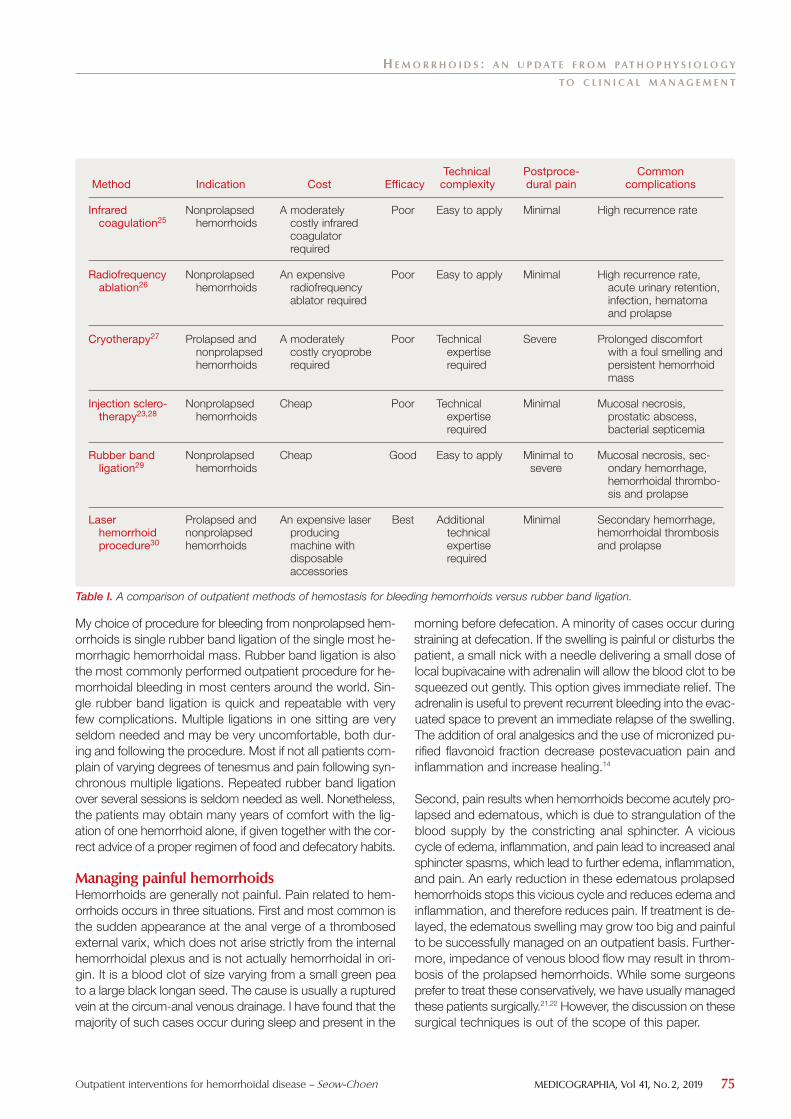
Efficacy
Technicalcomplexity
Postproce-dural pain
Common complications
Method
Infrared coagulation25
Radiofrequencyablation26
Cryotherapy27
Injection sclero-therapy23,28
Rubber band ligation29
Laser hemorrhoid procedure30
Indication
Nonprolapsed hemorrhoids
Nonprolapsed hemorrhoids
Prolapsed and nonprolapsedhemorrhoids
Nonprolapsed hemorrhoids
Nonprolapsed hemorrhoids
Prolapsed andnonprolapsedhemorrhoids
Cost
Table I. A comparison of outpatient methods of hemostasis for bleeding hemorrhoids versus rubber band ligation.

Conclusion
H E M O R R H O I D S : A N U P D AT E F R O M PAT H O P H Y S I O L O G Y
TO C L I N I C A L M A N A G E M E N T
MEDICOGRAPHIA, Vol 41, No. 2, 2019 Outpatient interventions for hemorrhoidal disease – Seow-Choen76
Keywords: arteriovenous bulges; hemorrhoid
References1.
World J Gastroenterol. 2. Proc R Soc Med.
3. World J Gas-troenterol.
5. Dis Colon Rectum.
6. World J Gastroenterol.
6. Br J Surg. 7. Am J Gastroenterol.
8. Tech Coloproctol.
9. The Straits Times.
10. Zhonghua Weichang Waike Zazhi.
11. J Biochem Mol Biol.
12. Eur J Clin Invest.
13. echColoproct.
14. Angiology.
15. Surgical Treatment of Hemorrhoids.
16. Surgical Treatment of Hemorrhoids.
17. World J Gas-troenterol.
18. Br J Nutr.
19. J Am Diet Assoc.
20. Br J Surg.
21. Br J Surg.
22. Colorectal Dis.
23. Br J Surg.
24. BMJ Case Rep.
25. Braz J Med Biol Res.
26. Medicina (Kaunas).
27. Dis Colon Rectum.
28. J R Soc Med.
29. J Med Assoc Thai.
30. Dis Colon Rectum.

Surgery for hemorrhoids – Wunderlich MEDICOGRAPHIA, Vol 41, No. 2, 2019 77
S urgery for hemorrhoids is indicated in the presence of long-standing se-vere symptoms and for when conservative therapy has failed. The ob-ject is to reduce the blood supply and the size of the hemorrhoids. The
procedures mostly in use at present are conventional hemorrhoidectomy (withor without minor modifications), hemorrhoidal artery ligation/transanal he-morrhoidal dearterialization/rectoanal repair, tailored hemorrhoidectomy, andstapled anopexy (ie, procedure for prolapse and hemorrhoids). No operationis free from drawbacks, as recurrence of symptoms and pain are often seenas mere problems. Complications are severe and include long-lasting pain,urgency, postoperative bleeding, anal incontinence, abscess, or fistula in theoperative field, and pelvic sepsis, which may be life-threatening and even lethal.Patients have to be informed extensively about the risks before surgery, par-ticularly when a seemingly harmless and safe method, such as procedure forprolapse and hemorrhoids, is offered. The future seems to lie in operationsthat, instead of extensive excision, are based on ligatures (hemorrhoidal arteryligation/rectoanal repair) and are, if necessary, combined with excision of thelargest and prolapsing pile—a concept that is tailored to every patient's in-dividual situation.
Medicographia. 2019;41:77-83
Introduction
S
(Figure 1, page 78).
Address for correspondence:
www.medicographia.com
H E M O R R H O I D S : A N U P D AT E F R O M PAT H O P H Y S I O L O G Y
T O C L I N I C A L M A N A G E M E N T
The future seems to lie in op-erations that, instead of extensiveexcision, are based on ligaturesand are, if necessary, combinedwith excision of the largest andprolapsing pilea concept that istailored to every patient’s individ-ual situation.
Managementof hemorrhoidal disease:
surgical treatments
by M. Wunder l ich , Aust r ia
Max WUNDERLICH,

H E M O R R H O I D S : A N U P D AT E F R O M PAT H O P H Y S I O L O G Y
T O C L I N I C A L M A N A G E M E N T
MEDICOGRAPHIA, Vol 41, No. 2, 2019 Surgery for hemorrhoids – Wunderlich78
General considerations
Conventional hemorrhoidectomy
Figure 1. The targets of surgery for hemorrhoids. Abbreviations: HAL, hemorrhoidal artery ligation; HE, conventional hemorrhoidectomy; MISSH,minimally invasive subanodermal submucosal hemorrhoidoplasty; PPH, procedure for prolapseand hemorrhoids; RAR, rectoanal repair; THD, transanal hemorrhoidal dearterialization.

H E M O R R H O I D S : A N U P D AT E F R O M PAT H O P H Y S I O L O G Y
T O C L I N I C A L M A N A G E M E N T
Surgery for hemorrhoids – Wunderlich MEDICOGRAPHIA, Vol 41, No. 2, 2019 79
Hemorrhoidal artery ligation, transanal hemorrhoidaldearterialization, and rectoanal repair
Minimally invasive subanodermal submucosal hemorrhoidoplasty
Laser hemorrhoidectomy
Tailored hemorrhoidectomy
Stapled anopexy

H E M O R R H O I D S : A N U P D AT E F R O M PAT H O P H Y S I O L O G Y
T O C L I N I C A L M A N A G E M E N T
MEDICOGRAPHIA, Vol 41, No. 2, 2019 Surgery for hemorrhoids – Wunderlich80
(Table I). (Table II).
(Table III)
Discussion
(see Table II)
Procedure for prolapse andhemorrhoids
Comment
Author
Cheetham et al31
Ortiz et al32
Ho, Ho33
Martinsons et al34
Pescatori, Gagliardi35
Giordano et al36
Infantino et al37
Porrett et al38
Aly39
Watson et al40
Carvajal López20
Year
2000
2005
2006
2007
2008
2009
2012
2015
2015
2016
2019
Conventional hemorrhoid-
ectomy
Table I. Pain after surgery for hemorrhoids.

(see Table I)
(see Table III),
H E M O R R H O I D S : A N U P D AT E F R O M PAT H O P H Y S I O L O G Y
T O C L I N I C A L M A N A G E M E N T
Surgery for hemorrhoids – Wunderlich MEDICOGRAPHIA, Vol 41, No. 2, 2019 81
Table III. Severe complications after procedure for prolapse and hemorrhoids.
Procedure forprolapse and hemorrhoids
Comment
Author
Ortiz et al32
Jayaraman et al41
Giordano et al36
Porrett et al38
Aly39
Watson et al40
Carvajal López et al20
Year
2005
2006
2009
2015
2015
2016
2019
Conventional hemorrhoid-
ectomy
Reviews
Author
Pescatori, Gagliardi35
Cirocco44
Naldini42
Faucheron et al45
Porrett et al38
Year
2008
2009
2011
2012
2015
Table II. Recurrence after surgery for hemorrhoids.

H E M O R R H O I D S : A N U P D AT E F R O M PAT H O P H Y S I O L O G Y
T O C L I N I C A L M A N A G E M E N T
MEDICOGRAPHIA, Vol 41, No. 2, 2019 Surgery for hemorrhoids – Wunderlich82
References1. Die Punkte Gynäkologie/Prokto-logie.
2. Br Med J.
3. Lancet.
4. Dis Colon Rectum.
5. Surg Clin North Am.6. Surgery.
7. Updates Surg.
8. Ann Coloproc-tol.
9. Tech Coloproctol.
10. ANZ J Surg.
11. Dis Colon Rectum.
12. Chirurgie. 13. World J Gastroenterol.
14.
Wien Klin Wochenschr. 15.
Dis Colon Rectum.
16. Am J Surg.
17. Dis Colon Rectum.
18. Br J Surg.
19. J Visc Surg.
20. Surg Innov.
21. Tech Coloproctol.
22. Coloproctology.
23. Colorectal Dis.
24. Ann Surg.
25. Patient Saf Surg.
26. Ann Ital Chir.
27.
28. Dis Colon Rectum.
29. Langenbecks Arch Surg.
30. Tech Coloproctol.

31. Lancet.
32. Dis Colon Rectum.
33. Tech Coloproctol.
34. Colorectal Dis.
35. Tech Coloproctol.
36. Arch Surg.
37. Colorectal Dis.
38. Int Surg.
39. Ann R Coll Surg Engl.
40. Lancet.
41. Cochrane Database Syst Rev.
42. Colorectal Dis.
43. Chirurgie.
44. Surgery.
45. Br J Surg.
46. World J Gastroenterol.
47. Angiology.
48. Asian J Surg.
49. Colorectal Dis.
50. Int J Colorectal Dis.
H E M O R R H O I D S : A N U P D AT E F R O M PAT H O P H Y S I O L O G Y
T O C L I N I C A L M A N A G E M E N T
Surgery for hemorrhoids – Wunderlich MEDICOGRAPHIA, Vol 41, No. 2, 2019 83
Keywords: complications; hemorrhoids; hemorrhoidal artery ligation; hemorrhoidectomy; procedure for prolapse andhemorrhoids; rectoanal repair; transanal hemorrhoidal dearterialization


1. J. Bocobo, Philippines
2. M. L. Esquivel Herrera, Mexico
3. A. Karimuddin, A. Farooq, Canada
4. K. Madbouly, Egypt
5. C. Tohme, Lebanon
6. D. Voiculescu, Romania
Which clinical practice and medical treatments for hemorrhoidal patients? MEDICOGRAPHIA, Vol 41, No. 2, 2019 85
C O N T R O V E R S I A L Q U E S T I O N
In your clinical practice,when, in which type
of hemorrhoidal patients,and how do you usemedical treatments?
THE QUESTION
Hemorrhoidal disease is acommon and benign ano-rectal condition. Treatment
of hemorrhoids depends on thenature of the clinical presentation,and the type of treatment shouldbe tailored to each patient. In thisarticle, experts discuss the typesof patients they see, as well aswhen and how these patients aretreated.

C O N T R O V E R S I A L Q U E S T I O N
MEDICOGRAPHIA, Vol 41, No. 2, 2019 Which clinical practice and medical treatments for hemorrhoidal patients?86
Joseph BOCOBO, MD
Institute of Digestive and Liver Diseases
St. Luke's Medical Center
Quezon City, 1100
PHILIPPINES
(email: [email protected])
H emorrhoidal disease is a common disorder that I usu-ally encounter in my daily clinical practice. I see pa-tients complaining of fresh blood during defecation,
either dripping or staining the toilet paper, especially if thestool is hard and they strain. Many of them would undergo acolonoscopy, which, most of the time, confirms the diagnosisof internal hemorrhoids, upon exclusion of other possible caus-es of bleeding, or the colon is identified to be unremarkableor normal. Several patients who would go through the aboveprocedure for other indications (eg, screening for colon can-cer and suspected inflammatory bowel disease), would havean incidental finding of engorged internal hemorrhoids. Onthe other hand, very few patients will come complaining ofpainful lump(s) or swelling in the distal anal canal aggravat-ed by a bowel movement, and, on perianal examination, theidentification of thrombosed external hemorrhoids would beestablished. Most of these individuals of either type of he-morrhoidal disease have not self-medicated, and a few willhave taken an underdosed oral drug, applied a topical oint-ment or cream, or used a suppository.
In my experience, more than 95% of the patients with symp-tomatic internal hemorrhoids are grade 1, the others aregrade 2. These patients are the best candidates to receivemedical management. My treatment protocol consists of a
high-fiber diet, such as fruits, vegetables, wheat, and oats, andmicronized purified flavonoid fraction (MPFF) diosmin and hes-peridin 500 mg tablets, 2 tablets three times a day for 4 days,then 2 tablets twice a day for 3 days, then 2 tablets once a dayfor 1 to 3 months. The recurrent bleeding rate is approximate-ly less than 10%, which is normally among patients noncom-pliant with the prescribed treatment regimen. However, forthose who thoroughly follow the instituted medical care, theoutcome is a lot better. Relief of hemorrhoidal symptoms, suchas pain and bleeding, is experienced promptly, improving moresignificantly day after day, as they proceed with their courseof therapy, leading to total control of the hemorrhage.
I have yet to come across patients with the more severe gradesof hemorrhoidal disease though. In the Philippines, these pa-tients go directly to our surgeon colleagues for operative pro-cedures. However, for those patients I encounter with throm-bosed external hemorrhoids, I give my usual treatment regimenwith the addition of a hot sitz bath for 5 minutes twice a dayuntil the discomfort is gone. Moist heat is convincingly an-other factor that alleviates pain due to its ability to decreaseanal canal pressure. I do find this management effective sinceat least 5 of those patients that I can recall have successfullyresponded, with adequate follow-up postmedication, and sofar no recurrence, saving them from an excisional procedure.To date, none of my patients to whom I have prescribed MPFFhas ever reported any adverse reaction or untoward side ef-fect with the medication.
In conclusion, my personal experience confirms the efficacyof medical management, particularly with MPFF diosmin andhesperidin 500 mg, among patients with grades 1 and 2 in-ternal hemorrhoids, as well as those with thrombosed exter-nal hemorrhoidal disease. ■
1. J. Bocobo, Philippines

C O N T R O V E R S I A L Q U E S T I O N
Which clinical practice and medical treatments for hemorrhoidal patients? MEDICOGRAPHIA, Vol 41, No. 2, 2019 87
A lthough the actual prevalence of hemorrhoidal diseaseis difficult to identify by different factors, it fluctuatesaround 40% in the US population and it is very similar
in Western countries. Of the three hundred and thirty-onemillion Americans, about one hundred and forty million aresuffering from some degree of the disease and only about10% to 20% will require surgical treatment. The universe ofpatients who will require conservative treatment is very vast.The treatment is then divided into conservative and surgical;the latter in turn into noninvasive and invasive.1-7 Based onGoligher’s classification, grade 1 patients will require the mostbasic measures, including a high fiber diet and/or bolus for-mers (eg, psyllium plantago), adequate fluid intake, a reduc-tion in the intake of possible irritants, an increase in physicalactivity, and a modification in their evacuation habits. Thesemeasures also apply to all grades of the disease in stages ofexacerbation. Additional measures could include a sitz bath(at a temperature of 40°C) in order to decrease edema and torelax sphincter contractions (2018 American Society of Colonand Rectal Surgeons guideline recommendation grade 1B).In some cases, conservative medical treatment, ie, topicaltreatments, such as oils, creams, and suppositories with anes-thetics and/or anti-inflammatories, for short periods of time.The time duration is short due to the risk of skin sensitization,the discomfort of its application, and the usefulness only asa symptomatic treatment. For many patients, Preparation H ®
is the most used treatment. It is available as a cream, a re-freshing gel, suppositories, and even wipes, with most con-taining anti-inflammatory ingredients and/or hydrocortisone.Preparation H is elaborated with petrolatum, mineral oil,phenylephrine chloride, and shark liver oil; phenylephrine chlo-ride has a vasoconstrictive effect, while the other components
are skin protectors. This treatment will not cure the disease,but it is commonly used for relieving the most frequent man-ifestations.
In addition, stool softeners and flavonoids are frequently usedin cases of exacerbation. Among flavonoids, micronized pu-rified flavonoid fraction (MPFF) has been the best studied.The active components of MPFF include diosmin, diosmetin,hesperidin, linarin, isorhoifolin. The synergy between the com-ponents plus the micronization of its particles (<2 mm) im-proves drug absorption two fold vs other available flavonoids.MPFF improves vascular tone, and, at the microcirculatory lev-el, reinforces capillary resistance, decreases capillary perme-ability, and improves microlymphatic flow. Another action in-cludes an effect on venous inflammatory processes througha reduction in the inflammatory cascade. These effects makeMPFF an initial step in treating all patients with pruritus, analbleeding, pain during and after defecation, prolapse, and whenhemorrhoids are detected during a proctological screening.The dosage is 1000 mg per day in one or two doses untilthe symptomatology disappears and for a period of up to 3months. The American Society of Colorectal Surgeons ap-proves its use with a IIB grade of recommendation, mainlyfor improving anal bleeding, pruritus, and recurrence. ■
References1. Hnátek L. Therapeutic potential of micronized purified flavonoid fraction (MPFF)
of diosmin and hesperidin in treatment chronic venous disorder [in Czech]. VnitrLek. 2015;61(9):807-814.
2. Giannini I, Amato A, Basso L, et al. Flavonoids mixture (diosmin, troxerutin, hes-
peridin) in the treatment of acute hemorrhoidal disease: a prospective, random-
ized, triple-blind, controlled trial. Tech Coloproctol. 2015;19(6):339-345.
3. Perera N, Liolitsa D, Iype S, et al. Phlebotonics for haemorrhoids. CochraneDatabase Syst Rev. 2012;8:CD004322.
4. Davis BR, Lee-Kong SA, Migaly J, Feingold DL, Steele SR. The American Society
of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management
of Hemorrhoids. Dis Colon Rectum. 2018;61(3):284-292.
5. Alonso-Coello P, Zhou Q, Martinez-Zapata MJ, et al. Meta-analysis of flavonoids
for the treatment of haemorrhoids. Br J Surg. 2006;93(8):909-920.
6. Ba-bai-ke-re MM, Huang HG, Re WN, et al. How we can improve patients’ com-
fort after Milligan-Morgan open haemorrhoidectomy. World J Gastroenterol.2011;17(11):1448-1456.
7. Zagriadskiĭ EA, Bogomazov AM, Golovko EB. Conservative treatment of hem-
orrhoids: results of an observational multicenter study. Adv Ther. 2018;35(11):
1979-1992.
Miguel Luis ESQUIVEL HERRERA, MD
Past President of the Mexican Society of
Surgeons of Recto, Colon and Anus A.C.
Professor of Coloproctology and
General Surgery
La Salle University
Queretaro, MEXICO
(email: [email protected])
2. M. L. Esquivel Herrera, Mexico

C O N T R O V E R S I A L Q U E S T I O N
MEDICOGRAPHIA, Vol 41, No. 2, 2019 Which clinical practice and medical treatments for hemorrhoidal patients?88
H emorrhoidal disease is a common anorectal condi-tion presenting to general practitioners, gastroen-terologists, and general and colorectal surgeons. In
fact, sufferers of hemorrhoidal disease have their own patronsaint: St Fiacre, patron saint of gardeners and hemorrhoidsufferers.1 It is important for physicians to have an algorith-mic approach to dealing with hemorrhoidal disease, whichincludes nonsurgical options. The American Society of Colonand Rectal Surgeons (ASCRS) recently published clinical prac-tice guidelines on the management of hemorrhoids.2 Themainstays of therapy for the majority of patients includes in-creased fiber and water intake.2 A 2005 Cochrane review foundthat fiber supplementation was associated with a 53% im-provement in symptoms.3 Fiber intake reduces symptoms bybulking up stool and reducing straining. When recommend-ing fiber intake, patients should be aware that the goal of dailyfiber intake is 25 g to 30 g. Generally, this will require fiber sup-plementation, usually in the form of psyllium. A sometimesoverlooked detail of prescribing fiber supplementation is en-suring adequate fluid intake, usually recommended as twoglasses of water with the fiber.4,5 Fiber taken before bed orwithout enough water can paradoxically lead to colonic sta-sis and worsen constipation.5
Flavonoids, such as diosmin, are phenolic dietary supplementsthat are derived from plants.2 Also known as venotonics, flavo-noids are thought to be vasoactive, reduce inflammation, andincrease venous return.6 Flavonoids are much more popularin Europe than in the UK or North America, with France rep-resenting 70% of the world’s market.5 A Cochrane reviewby Alonso-Coello et al found that flavonoids were associatedwith a 50% relative risk reduction in symptoms, with little tono harm from the treatment,5 which has led to a recommen-dation by both ASCRS and Italian hemorrhoid guidelines forthe routine use of oral flavonoids to help manage hemorrhoidsymptoms related to bleeding and discomfort.
There are other commonly available over-the-counter creamsand topical ointments; most include a combination of agents,usually a barrier cream and steroids.4 The evidence for mostof these agents is very limited. In particular, the use of cortico-steroid creams, such as proctosol, should be discouraged,as they will thin the perianal skin and potentially aggravate
symptoms related to bleeding and itching.4 Patients general-ly present with one of two main symptoms: bleeding or pro-lapse. All patients should have a complete history and phys-ical exam. The physical exam typically involves anoscopicevaluation and rigid proctoscopy, with colonoscopy as indi-cated. Once it is clear that the bleeding is indeed outlet typebleeding from hemorrhoids, then we base our therapy on thegrade of hemorrhoids. Our first-line approach is fiber supple-mentation and flavonoids for at least 6 to 8 weeks, with re-evaluation if symptoms persist.
Grade 1 and 2 hemorrhoids usually respond to conservativetherapy,6 ie, a combination of fiber, fluids, and oral flavonoids.Grade 3 hemorrhoids will often respond, although they willoften require rubber band ligation. Grade 4 hemorrhoids willsometimes respond to conservative therapy, but many of thesepatients will require an excisional hemorrhoidectomy. Whilesymptoms may not be completely obviated, the symptomburden may be reduced enough with medical managementthat the patient can cope and have an improved quality of life,despite the presence of grade 3 or 4 hemorrhoids. In the caseof prolapse, our approach is similar. Grade 1 and 2 hemorrhoidstypically respond to conservative measures. Grade 3 hemor-rhoids will often require rubber band ligation. Grade 4 hem-orrhoids generally require an excisional hemorrhoidectomy.Therapy is driven by patient symptoms and their impact on thepatient’s quality of life rather than the grade of hemorrhoids.
Hemorrhoidal disease is a common and benign anorectal con-dition that is presented to many general practitioners and sur-geons. We have outlined the commonly accepted medicaltherapies, as well as our approach. All patients should have atrial of conservative therapy, which may sometimes requiremultiple office visits. This trial period is important to build rap-port with the patient and to gain a greater understanding of theirexpectations and main symptoms. In our experience, many pa-tients are looking for reassurance, amelioration of their difficultsymptoms, with only a small proportion of patients with he-morrhoidal disease ultimately going on to require surgery. ■
References1. Senagore AJ. Surgical management of hemorrhoids. J Gastrointest Surg Off J
Soc Surg Aliment Tract. 2002;6(3):295-298.
2. Davis BR, Lee-Kong SA, Migaly J, Feingold DL, Steele SR. The American So-
ciety of Colon and Rectal Surgeons Clinical Practice Guidelines for the Man-
agement of Hemorrhoids. Dis Colon Rectum. 2018;61(3):284-292.
3. Alonso-Coello P, Mills E, Heels-Ansdell D, et al. Fiber for the treatment of hem-
orrhoids complications: a systematic review and meta-analysis. Am J Gastro-enterol. 2006;101(1):181-188.
4. Garg P. Conservative treatment of hemorrhoids deserves more attention in guide-
lines and clinical practice. Dis Colon Rectum. 2018;61(7):e348.
5. Steele SR, Hull TL, Read TE, Saclarides TJ, Senagore AJ, Whitlow CB, eds. TheASCRS Textbook of Colon and Rectal Surgery. 3rd ed. New York, NY: Springer;
2016.
6. Alonso-Coello P, Zhou Q, Martinez-Zapata MJ, et al. Meta-analysis of flavonoids
for the treatment of haemorrhoids. Br J Surg. 2006;93(8):909-920.
3. A. Karimuddin, A. Farooq, Canada
Ahmer KARIMUDDIN, MD
Ameer FAROOQ, MD
St. Paul’s Hospital, Department of Surgery
University of British Columbia
Vancouver, BC, Canada
(email: [email protected])
▲

C O N T R O V E R S I A L Q U E S T I O N
Which clinical practice and medical treatments for hemorrhoidal patients? MEDICOGRAPHIA, Vol 41, No. 2, 2019 89
H emorrhoidal disease is common in both Eastern andWestern communities. More than 50% of individu-als over the age of 50 years have, at some point, ex-
perienced symptoms related to hemorrhoids. Medical treat-ment of hemorrhoids depends on the nature of the clinicalpresentation. The most common presenting complaint is brightred bleeding. With worsening disease, internal hemorrhoidsstart to prolapse through the anal canal, and they might re-duce spontaneously (grade 2), require manual reduction(grade 3), or remain chronically prolapsed (grade 4) with mu-coid discharge and/or perianal irritation. If bleeding is relatedto straining or diarrhea, treatment should be directed to thecause of the bleeding. Changes in lifestyle behaviors, as wellas using oral and topical medications to decrease symptomsare usually applied. The goal of behavioral, oral, and topicalapproaches is to relieve symptoms, not to cure hemorrhoids.
Alonso-Coello et al1 performed a meta-analysis of 378 pa-tients from 7 randomized trials to analyze the effect of usingfiber supplements on symptomatic hemorrhoids. In the fibergroup, there was a 47% decrease in overall symptoms, a50% decrease in bleeding, and no significant improvement inprolapse, pain, or itching.
Flavonoids have been used for decades in the treatment ofbleeding hemorrhoids. Corsale et al 2 used flavonoids in aprospective, double-blind trial on 154 patients with hemor-rhoidal bleeding. Bleeding improved after 1 and 6 months inboth the study and control groups, with no significant be-tween-group differences. Yet, the degree of satisfaction af-ter 6 months was statistically greater in the patients who re-ceived flavonoids (P=0.003). In addition, Alonso-Coello et al 3
conducted a meta-analysis on 1514 patients from 14 trials. They suggested that flavonoids decrease the risk of symp-toms that persist or do not improve by 58% and showed anapparent reduction in the risk of bleeding (relative risk, 0.33).
Many creams and suppositories are used to stop the bleed-ing. The active ingredients usually include a vasoconstrictorand soothing agents that may lead to temporary relief ofburning and itching. Symptoms of pruritus ani may be ame-liorated, yet the hemorrhoids do not shrink. Sitz baths leadto a symptomatic improvement in hemorrhoids. Dodi et al4
performed anorectal manometry on volunteers and on pa-tients with anorectal problems. A statistically significant de-crease in resting pressure was observed after immersion inthe warm water, which is why patients with hemorrhoids andelevated anal pressures could benefit from Sitz baths.
Patients with thrombosed external hemorrhoids usually pres-ent with a painful, tender mass at the anal verge. If the patientis seen after more than 2 days, medical management in theform of sitz baths, stool softeners, and a mild analgesic shouldbe offered. Topical nifedipine and lidocaine ointment havebeen demonstrated to cause excellent pain relief comparedwith local anesthetic alone in a randomized clinical trial.5
Hemorrhoidal complaints are not uncommon in patients withinflammatory bowel disease. In patients with ulcerative colitis,the general guidelines for treatment are followed and surgerycan be offered, as there are few complications. However, inCrohn’s disease, conservative measures are better and surgeryshould be avoided because of the high rate of complications.
Medical treatment of hemorrhoids ranges from dietary andlifestyle changes to topical and oral medications, with initialmanagement usually being medical and preventative. Timingand type of medical treatment should be tailored case bycase. ■
References1. Alonso-Coello P, Mills E, Heels-Ansdell D, et al. Fiber for the treatment of hem-
orrhoids complications: a systematic review and meta-analysis. Am J Gastroen-terol. 2006;101:181-188.
2. Corsale I, Carrieri P, Martellucci J, et al. Flavonoid mixture (diosmin, troxerutin,
rutin, hesperidin, quercetin) in the treatment of I-III degree hemorroidal disease:
a double-blind multicenter prospective comparative study. Int J Colorectal Dis.2018;33(11):1595-1600.
3. Alonso-Coello P, Zhou Q, Martinez-Zapata MJ, et al. Meta-analysis of flavonoids
for the treatment of haemorrhoids. Br J Surg. 2006;93:909-920.
4. Dodi G, Bogoni F, Infantino A, et al. Hot or cold in anal pain? A study of the changes
in internal anal sphincter pressure profiles. Dis Colon Rectum. 1986;29:248-251.
5. Perrotti P, Antropoli C, Molino D, et al. Conservative treatment of acute throm-
bosed external hemorrhoids with topical nifedipine. Dis Colon Rectum. 2001;
44:405-409.
Khaled MADBOULY, MD, MS, PhD, FRCS
(Glasg), FACS, FASCRS, FISUCRS, MBA
Professor of Colorectal Surgery, Department
of Surgery, University of Alexandria, Egypt
Associate Secretary General of the International
Society of University of Colon & Rectal Surgeons
Vice President of the Egyptian Board of Colon
& Rectal Surgery
President-elect of the Egyptian Society of
Colon & Rectal Surgeons, EGYPT
(email: [email protected])
4. K. Madbouly, Egypt

C O N T R O V E R S I A L Q U E S T I O N
MEDICOGRAPHIA, Vol 41, No. 2, 2019 Which clinical practice and medical treatments for hemorrhoidal patients?90
N o matter how bad the hemorrhoids look, they shouldnot be treated unless they are symptomatic. Varioustreatments are available; they depend mainly on the
type and severity of hemorrhoids, patient preferences, andthe expertise of the physician. Not all people will require anoffice procedure or surgery. First-line treatment of all first- andsecond-degree and many third-degree internal hemorrhoidsshould be conservative. Initial treatment of symptomatic hem-orrhoids consists of warm sitz baths (twice or three times dai-ly), dietary modifications (high fiber diet, adequate fluid in-take), stool softeners, topical analgesic or steroid cream, andphlebotonics.1
Constipation and abnormal bowel habits (straining, prolongedsitting) play a significant role in patients with symptomatichemorrhoids. Increased fiber and fluid intake with or withouta stool softener or a laxative should be recommended andhave been shown to improve symptoms of mild and moder-ate prolapse and to minimize the risk of bleeding by approx-imately 50% when applied for up to 6 weeks. A Cochranereview that included 7 randomized trials (378 patients) com-pared fiber with a no fiber control and showed that fiber had abeneficial effect in the treatment of symptomatic hemorrhoids.Fiber supplementation had a significant effect on bleeding withno effect on prolapse, pain, or itching.2 Patients should also beadvised to exercise regularly and to maintain proper bowelhabits, such as avoidance of straining and sitting on the toi-let for a long period of time. Decreasing straining (and con-stipation) shrinks internal hemorrhoids and decreases theirsymptoms.
Topical applications of ointments containing local anesthetic,antibiotics, steroids, or emollients are commonly used. Thereis no strong scientific evidence regarding their efficacy. Littlehigh-quality data exist regarding their use in patients with symp-tomatic hemorrhoids. Topical steroids can be used to decrease
symptoms of pruritus, inflammation, and sometimes bleed-ing, but they are not to be used longer than 10 to 14 days.Their prolonged use may be detrimental and should be avoid-ed because of the associated side effects, such as mucos-al atrophy, local allergic reaction, or sensitization of the skin.
Phlebotonics are a group of treatment options that can beoffered with expectations of minimal harm and a decent po-tential for relief. These drugs are used in early grades whereprolapse is not significant, as a primary control of acute bleed-ing until definitive office procedures or surgery is done if nec-essary or in stage III and IV as a bridge-to-surgery. They areassociated with strengthening of blood vessel walls, increas-ing venous tone and lymphatic drainage, and normalizing cap-illary permeability.3 In a Cochrane review of 24 randomizedcontrolled trials with 2234 patients that compared phleboton-ics with a control, phlebotonics demonstrated a statisticallysignificant effect on pruritus, bleeding, discharge, and leak-age, as well as overall symptom improvement. Although ben-eficial, they did not show a beneficial effect on pain.4 Flavonoids(diosmin, micronized purified flavonoid fraction, troxerutin, andrutosides) are the most commonly used agents and werenoted to decrease bleeding by 67%, pruritus by 35%, per-sistent pain by 65%, and recurrence by 47% in a meta-analy-sis reviewing 14 randomized controlled trials (1514 patients)comparing flavonoids with placebo or no therapy, but themethodological quality of the studies was moderate with a riskof bias.5 They are usually used for a period of 4 to 6 weeks.
In conclusion, many patients see improvement or completeresolution of their symptoms with this treatment. Hemorrhoidscan recur in 25% of the patients after medical treatment. Ag-gressive therapy is reserved for patients who have persist-ent symptoms after 1 month of conservative treatment. ■
References1. Wald A, Bharucha AE, Cosman BC, Whitehead WE. ACG clinical guideline: man-
agement of benign anorectal disorders. Am J Gastroenterol. 2014;109:1141-
1157.
2. Alonso-Coello P, Guyatt G, Heels-Ansdell D, et al. Laxatives for the treatment of
hemorrhoids. Cochrane Database Syst Rev. 2005;4:CD004649.
3. Davis BR, Lee-Kong SA, Migaly J, Steele SR. The American Society of Colon
and Rectal Surgeons Clinical Practice Guidelines for the Management of Hem-
orrhoids. Dis Colon Rectum. 2018;61:284-292.
4. Perera N, Liolitsa D, Iype S, et al. Phlebotonics for haemorrhoids. CochraneDatabase Syst Rev. 2012;8:CD004322.
5. Alonso-Coello P, Zhou Q, Martinez-Zapata MJ, et al. Meta-analysis of flavonoids
for the treatment of haemorrhoids. Br J Surg. 2006;93:909-920.
5. C. Tohme, Lebanon
Cyril TOHME, MD, MHHM
Lebanese Hospital Geitaoui
University Hospital, Beirut, LEBANON
(email: [email protected])

C O N T R O V E R S I A L Q U E S T I O N
Which clinical practice and medical treatments for hemorrhoidal patients? MEDICOGRAPHIA, Vol 41, No. 2, 2019 91
H emorrhoidal disease is the most common cause ofanorectal complaints and this condition has an in-creased incidence. Trying to find a perfect solution for
treatment has been a concern for the medical world over time,without getting a true consensus so far. What is clearly es-tablished is that curative treatment is the interventionist one(classic or minimally invasive surgery). From this point of view,can we consider that medical treatment still finds a place,and if so, what would it be?
The answer to this question is clearly affirmative because med-ical treatment remains an effective adjuvant for all stages ofevolution of symptomatic hemorrhoidal disease. I highlightsymptomatic because it is currently considered almost unan-imous that a diagnosed hemorrhoidal disease, in the absenceof symptomatology, does not require treatment, even if theanoscopically assessed lesion is obviously significant.1 Thismedical treatment primarily consists of the systemic use ofmicronized purified flavonoid fraction (diosmin/hesperidin) byoral administration. This combination is the largest used veno-tonic; there are numerous studies offering data on the way itworks and the safety profile of this medication.2 The mech-anisms by which such medication is useful are complex andinclude: increasing vascular tone, reducing venous capaci-ty, the anti-inflammatory effect on the venous wall, reducingcapillary permeability, and increasing lymphatic drainage.3,4
I have emphasized the role of oral medication not in the pur-pose of undermining local medication (ointments, supposi-tories), but for the simple reason that this last group of reme-dies generates a strictly local effect that actually does notinterfere with the venous pathophysiological mechanismsresponsible for the occurrence of symptomatology. Oral med-ication can be used in all circumstances of hemorrhoidal dis-ease: symptomatic hemorrhoids, acute complications of hem-orrhoids, or in the recovery period after invasive hemorrhoidaldisease treatment (banding, photocoagulation, sclerotherapy,hemorrhoidal artery ligation, Milligan-Morgan resection, etc).
In the first and second stages of hemorrhoidal disease, drugtreatment can be used to relieve symptoms, such as bleed-ing, pain, pruritus. It can be used in chronic administrationuntil the patient decides to undergo a specific treatment. Inthe third and fourth stages, medical treatment retains the samerole of alleviating symptoms, but with slightly reduced effica-cy. The used doses are the usual ones for chronic mainte-nance treatment and are administered over long periods oftime.4-6
For acute complications of hemorrhoidal disease, primarily wespeak of hemorrhoidal thrombosis, oral drug therapy is ap-propriately adapted by increasing the dose, being associat-ed with heparin ointments. This type of therapy can replacesurgical treatment in the situations when the patient cannothave access to the therapy, has temporary or absolute con-traindications (for example, Crohn disease7), or refuses the ther-apy. The results are quite satisfactory, although in many cases,in the absence of a surgical excision, the healing process willleave skin tags. Medical treatment necessarily accompaniesall of the therapeutic procedures that remove hemorrhoidaldilations. Its role is to prevent, reduce, or ameliorate the post-intervention symptoms: bleeding, local pain, local edema, andlocal venous plexus thrombosis. The doses used in thesesituations for oral administration are similar to those used inthe treatment of acute complications of the disease.
In conclusion, the medical treatment of hemorrhoidal diseasealways remains of interest, having clear indications and beingthe most important adjuvant in controlling the symptoms ofhemorrhoids in situations of both symptomatic disease andconvalescence after specific therapeutic procedures. ■
References1. Thornton SC, Perry KR, Rosh AJ, Talavera F, Gossman WF. Hemorrhoids. https://
emedicine.medscape.com/article/775407-overview. Updated Jan 18, 2017.
Accessed May 24, 2019.
2. Shelygin Y, Krivokapic Z, Frolov S, et al. Clinical acceptability study of micronized
purified flavonoid fraction 1000 mg tablets versus 500 mg tablets in patients suf-
fering acute hemorrhoidal disease. Curr Med Res Opin. 2016;32(11):1821-1826.
3. Cerera N, Liolitsa D, Iype S, et al. Phlebotonics for haemorrhoids. CochraneDatabase Syst Rev. 2012;8:CD004322.
4. Lohsiriwat V. Treatment of hemorrhoids: a coloproctologist’s view. World J Gas-troenterol. 2015;21(31):9245-9252.
5. Brown SR. Haemorrhoids: an update on management. Ther Adv Chronic Dis.2017;8(10):141-147.
6. Altomare D, Giuratrabocchetta S. Conservative and surgical treatment of haem-
orrhoids. Nat Rev Gastroenterol Hepatol. 2013;10(9):513-521.
7. D’Ugo S, Franceschilli L, Cadeddu F, et al. Medical and surgical treatment of
haemorrhoids and anal fissure in Crohn’s disease: a critical appraisal. BMCGastroenterol. 2013;13:47.
Daniel VOICULESCU, MD, PhD
Assistant Professor 1st Surgery Clinic
Universitary Emergency Hospital
Bucharest University of Medicine and
Pharmacy “Carol Davila”
Bucharest, ROMANIA
(email: [email protected])
6. D. Voiculescu, Romania
T H E R A P E U T I C O U T L O O K
MEDICOGRAPHIA, Vol 41, No. 2, 2019 Association of hemorrhoidal disease with chronic venous disease – Yaltirik92
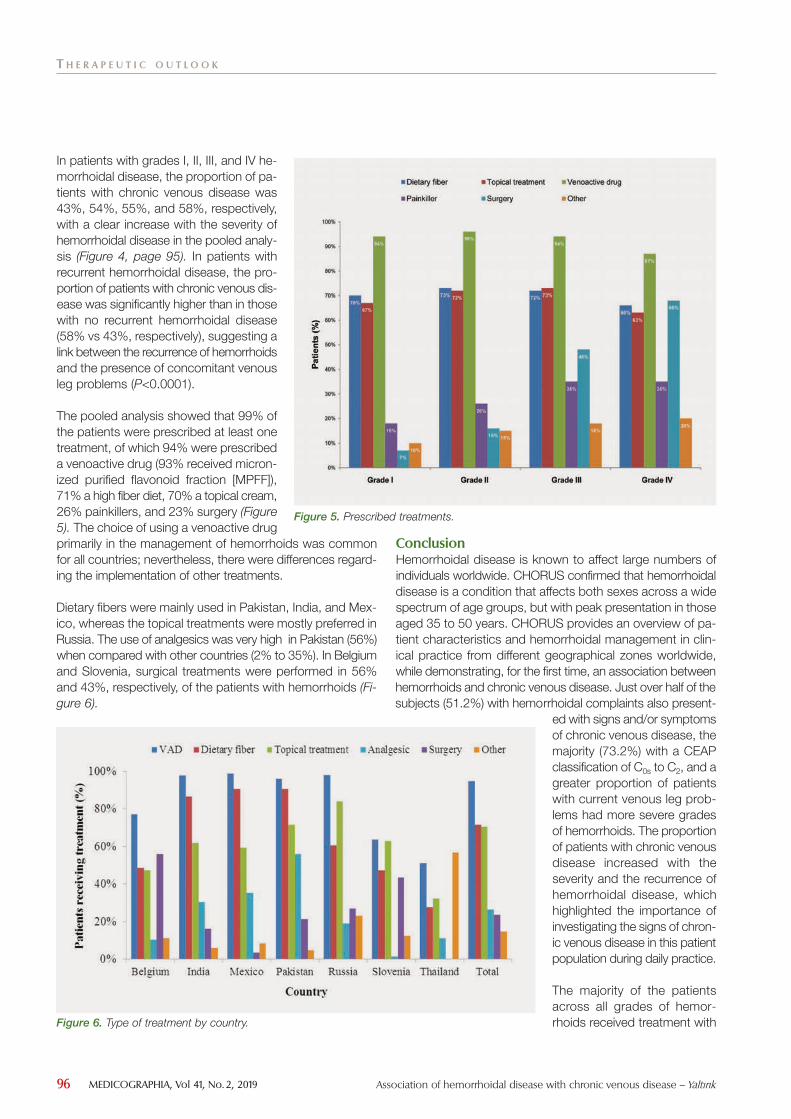
H emorrhoidal disease is known to affect large numbers of individualsworldwide, thus there are limited recent data on the profile of affect-ed patients in different continents and on the associated conditions.
The CHORUS study (Chronic venous and HemORrhoidal diseases evalUationand Scientific research), a multicenter, observational study, has addressed thisshortfall by providing up-to-date information on the characteristics of patientswith hemorrhoidal disease in clinical practice in different regions of the world,and, for the first time, the frequency with which it coexists with chronic venousdisease and associated risk factors. This report focuses on new data show-ing the coexistence of hemorrhoidal disease and chronic venous disease.Just over half the subjects (51.2%) with hemorrhoidal complaints also pre-sented with signs and/or symptoms of chronic venous disease, the majority(73.2%) with a clinical, etiological, anatomical, and pathophysiological (CEAP)classification of C0s to C2, and a greater proportion of patients with currentvenous leg problems had more severe grades of hemorrhoids. These out-comes should be considered in daily practice for optimizing the diagnosisand treatment.
Medicographia. 2019;41:92-97
Background and objective
H
Hurrem Pelin YALTIRIK,
Address for correspondence:
www.medicographia.com
Up-to-date data from theCHORUS survey: association
of hemorrhoidal diseasewith chronic venous disease
by H. P. Ya l t i r ik , France
The use of early pharmaco-logical treatment with a venoac-tive agent, particularly with MPFF,may play a significant role in pre-venting or slowing the develop-ment and recurrence of the signsand symptoms of both hemor-rhoidal disease and chronic ve-nous disease.

Methods (Fi-gure 1)
T H E R A P E U T I C O U T L O O K
Association of hemorrhoidal disease with chronic venous disease – Yaltirik MEDICOGRAPHIA, Vol 41, No. 2, 2019 93
Figure 1. Countries that participated in the CHORUS study.

t P P
T H E R A P E U T I C O U T L O O K
MEDICOGRAPHIA, Vol 41, No. 2, 2019 Association of hemorrhoidal disease with chronic venous disease – Yaltirik94
Hemorrhoid grade
Grade I Grade II Grade III Grade IVn (%) n (%) n (%) n (%)
Belgium 102 (24.06%) 166 (39.15%) 137 (32.31%) 19 (4.48%)
India 417 (27.62%) 723 (47.88%) 320 (21.19%) 50 (3.31%)
Mexico 245 (52.69%) 163 (35.05%) 51 (10.97%) 6 (1.29%)
Pakistan 185 (29.46%) 234 (37.26%) 170 (27.07%) 39 (6.21%)
Russia 613 (25.95%) 1047 (44.33%) 563 (23.84%) 139 (5.88%)
Slovenia 36 (27.91%) 39 (30.23%) 35 (27.13%) 19 (14.73%)
Thailand 33 (33.33%) 26 (26.26%) 25 (25.25%) 15 (15.15%)
Total 1631 (29.04%) 2398 (42.69%) 1301 (23.16%) 287 (5.11%)
Patients characteristics Patients (n=5617)
SexMale, n (%) 3020 (53.8%) Female, n (%) 2597 (46.2%)
Age (years), mean±SD 45.3±13.8
Body mass index (kg/m²), mean±SD 26.7±4.8
Hemorrhoid grade, n (%)I 1631 (29.0%) II 2398 (42.7%)III 1301 (23.2%)IV 287 (5.1%)
Previous consultation for hemorrhoids, n (%) 3176 (56.5%)
Table I. Patient demographics and baseline characteristics foranalysis population.
Patients (n=5617)
n %
Belgium 424 7.55%
India 1510 26.88%
Mexico 465 8.28%
Pakistan 628 11.18%
Russia 2362 42.05%
Slovenia 129 2.30%
Thailand 99 1.76%
Table II. Repartition of the patients per country.
Table III. Repartition of the grades of hemorrhoidal disease by country.
Figure 2. Frequency of hemorrhoidal complaints according to hemorrhoid grades.
T H E R A P E U T I C O U T L O O K
Association of hemorrhoidal disease with chronic venous disease – Yaltirik MEDICOGRAPHIA, Vol 41, No. 2, 2019 95
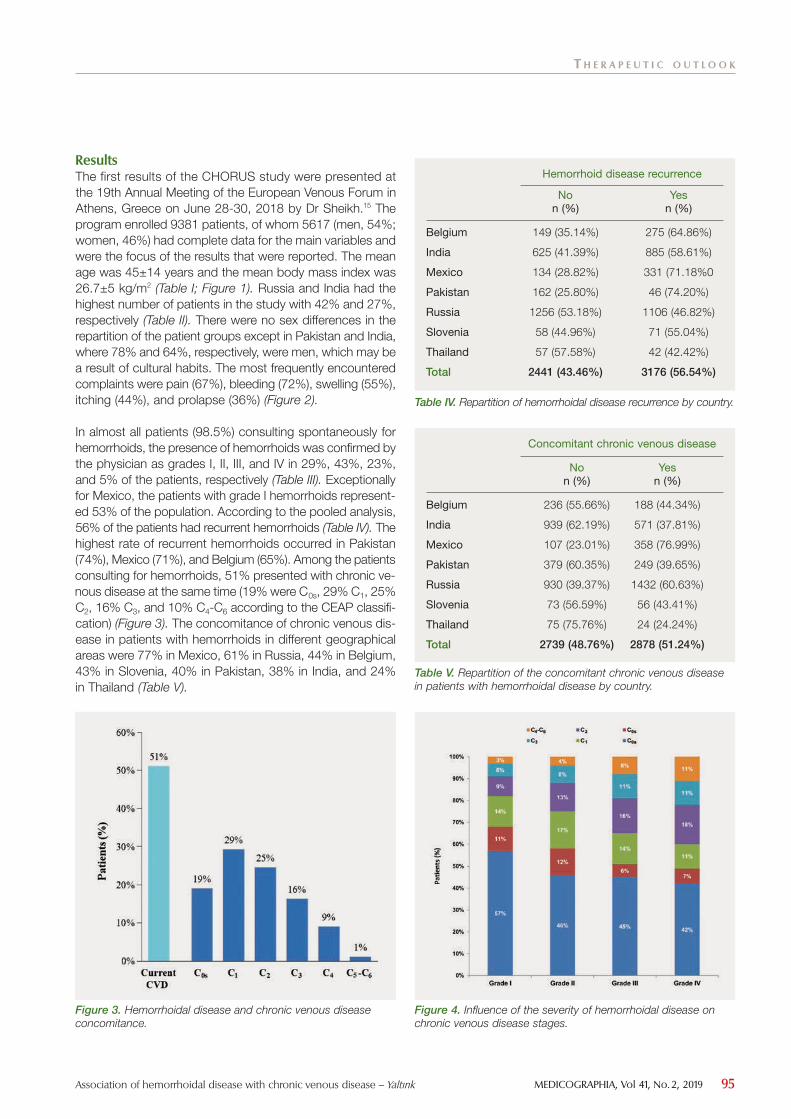
Results (Table I; Figure 1). (Table II). (Figure 2).
(Table III). (Table IV). (Figure 3). (Table V).
Hemorrhoid disease recurrence
No Yesn (%) n (%)
Belgium 149 (35.14%) 275 (64.86%)
India 625 (41.39%) 885 (58.61%)
Mexico 134 (28.82%) 331 (71.18%0
Pakistan 162 (25.80%) 46 (74.20%)
Russia 1256 (53.18%) 1106 (46.82%)
Slovenia 58 (44.96%) 71 (55.04%)
Thailand 57 (57.58%) 42 (42.42%)
Total 2441 (43.46%) 3176 (56.54%)
Table IV. Repartition of hemorrhoidal disease recurrence by country.
Concomitant chronic venous disease
No Yesn (%) n (%)
Belgium 236 (55.66%) 188 (44.34%)
India 939 (62.19%) 571 (37.81%)
Mexico 107 (23.01%) 358 (76.99%)
Pakistan 379 (60.35%) 249 (39.65%)
Russia 930 (39.37%) 1432 (60.63%)
Slovenia 73 (56.59%) 56 (43.41%)
Thailand 75 (75.76%) 24 (24.24%)
Total 2739 (48.76%) 2878 (51.24%)
Table V. Repartition of the concomitant chronic venous diseasein patients with hemorrhoidal disease by country.
Figure 3. Hemorrhoidal disease and chronic venous diseaseconcomitance.
Figure 4. Influence of the severity of hemorrhoidal disease onchronic venous disease stages.
T H E R A P E U T I C O U T L O O K
MEDICOGRAPHIA, Vol 41, No. 2, 2019 Association of hemorrhoidal disease with chronic venous disease – Yaltirik96
(Figure 4, page 95). P
(Figure5).
(Fi-gure 6).
Conclusion
Figure 5. Prescribed treatments.
Figure 6. Type of treatment by country.

T H E R A P E U T I C O U T L O O K
Association of hemorrhoidal disease with chronic venous disease – Yaltirik MEDICOGRAPHIA, Vol 41, No. 2, 2019 97
References1. Eur J Gen Pract.
2. BMC Fam Pract.
3. Dis Colon Rectum.
4. Gastroenterology.
5. FP Es-sent.
6. Int J Colorectal Dis.
7. World J Gastroenterol.
8. Dis Colon Rectum.
9. Am J Gastroenterol.
10.
Clin Gastroenterol Hepatol. 11.
Gastroenterol Clin Biol.
12. Gut.
13. Surgery of the Anus, Rectum and Colon.
14. J Vasc Surg.
15. Phlebology.
16. Indian J Surgery.
17. Int Angiol.
Keywords: chronic venous disease; hemorrhoidal disease; management; micronized purified flavonoid fraction; venoactivedrugs