g. a. salles, j. f. seymour, p. feugier, f. offner, a. lopez-guillermo, r. bouabdallah,
DESCRIPTION
Rituximab Maintenance for 2 Years in Patients with Untreated High Tumor Burden Follicular Lymphoma After Response to Immunochemotherapy. G. A. Salles, J. F. Seymour, P. Feugier, F. Offner, A. Lopez-Guillermo, R. Bouabdallah, - PowerPoint PPT PresentationTRANSCRIPT
Rituximab Maintenance for 2 Years in Patients with Untreated High Tumor Burden Follicular Lymphoma After Response to Immunochemotherapy
G. A. Salles, J. F. Seymour, P. Feugier, F. Offner, A. Lopez-Guillermo, R. Bouabdallah,
L. M. Pedersen, P. Brice, D. Belada, L. Xerri on behalf of the PRIMA investigators
Gilles Salles Hospices Civils de Lyon
& Université Claude Bernard, Lyon, France

• Although FL remains incurable, patients may benefit from prolonged remission intervals; recent progress in response rate and response duration have translated into an improved survival
• Previous studies have demonstrated a significant clinical benefit using rituximab maintenance:
– In relapsing patients after chemo or R-chemo
– In first line patients after chemo alone or rituximab alone
– … but the role of rituximab after R-chemo in first line remains unknown
• PRIMA: an international and intergroup study Phase III randomized study
– Coordinated by GELA, in collaboration with European and Australian study groups and individual centers in Europe, Middle East, South America, and Asia, who collected, cleaned and analyzed the data
– With support from Roche
Primary RItuximab and MAintenance (PRIMA): Rationale

PRIMA: study design
PD/SDoff study
Rituximab maintenance375 mg/m2
every 8 weeks for 2 years‡
Observation‡
CR/CRuPR
Random 1:1*
Immunochemotherapy8 x Rituximab
+8 x CVP or
6 x CHOP or6 x FCM
High tumor burden
untreated follicular lymphoma
INDUCTION MAINTENANCE
Registration
* Stratified by response after induction, regimen of chemo, and geographic region‡ Frequency of clinical, biological and CT-scan assessments identical in both armsFive additional years of follow-up

PRIMA: Inclusion criteria
• Patients over 18 years previously untreated with histologically confirmed follicular lymphoma grade 1, 2 or 3a
• Patients with at least one of the following symptoms requiring initiationof treatment:
– Bulky disease at study entry (nodal or extranodal mass > 7cm)– Involvement of ≥ 3 nodal sites (each > 3 cm) – Symptomatic splenic enlargement, compressive syndrome,
pleural/peritoneal effusion – B symptoms presence– Elevated serum LDH (> ULN) or 2-microglobulin (> 3mg/L)
• ECOG performance status < 2• Written informed consent
ClinicalTrials.gov: NCT00140582

PRIMA: Exclusion criteria
• Transformation to high-grade lymphoma or Grade 3b follicular lymphoma• Regular corticosteroids during the last 4 weeks (> 20 mg/day prednisone)• Prior or concomitant malignancies• Serious underlying medical conditions or poor renal or hepatic function• Known HIV infection; active HBV or HCV infection• Known sensitivity or allergy to murine products
ClinicalTrials.gov: NCT00140582

• Primary endpoint:
– Progression-free survival (PFS) from randomization (to rituximab maintenance or observation)
• Secondary endpoints:
– event-free survival (EFS), overall survival (OS)
– time to next anti-lymphoma treatment (TTNLT), time to next chemotherapy (TTNCT)
– response rates at end of maintenance
– safety and toxicity
– quality of life (QoL) (FACT-G and EORTC scales)
• An Independent Review Committee (IRC) also examined all response and progression data (CT scans + clinical/biological findings)
PRIMA: Study endpoints
ClinicalTrials.gov: NCT00140582

• Sample size calculation:
– Based on a 45% increase in median PFS, with a power of 80% to detect this difference (type I alpha risk - 2-sided - of 5%)
– 1200 patients registered at induction, estimated response rate of 75%:
• 900 randomized to maintenance or observation (1:1)
• Full analysis after 344 events
• Interim analysis planned after 258 events:
– Stopping rules: two-sided O’Brien-Fleming boundary of 2.3397 with type I of 5% (nominal p = 0.0193)
– Analyzed by a third party statistician and submitted to an independent Data Safety Monitoring Committee (DSMC)
PRIMA: Statistical assumptions
ClinicalTrials.gov: NCT00140582

R-CHOPN = 885
Randomized N = 769
* 15 pts in 3 sites closed prematurely
Patients evaluable (N = 1202)*
R-CVPN = 272
Patients registered: N = 1217
R-FCMN = 45
RandomizedN = 222
Randomized N = 28
ObservationN = 513
RituximabN = 505
‡ 1 pt died during the randomization process
Ind
uct
ion
Mai
nte
nan
ce
9 pts did not receive chemo
147 pts withdrew during or at the end of induction (failure to respond; toxicity)
28 pts failed to be randomized
Patient disposition
Patients randomized: N = 1018‡
Pat
ien
ts (
%)
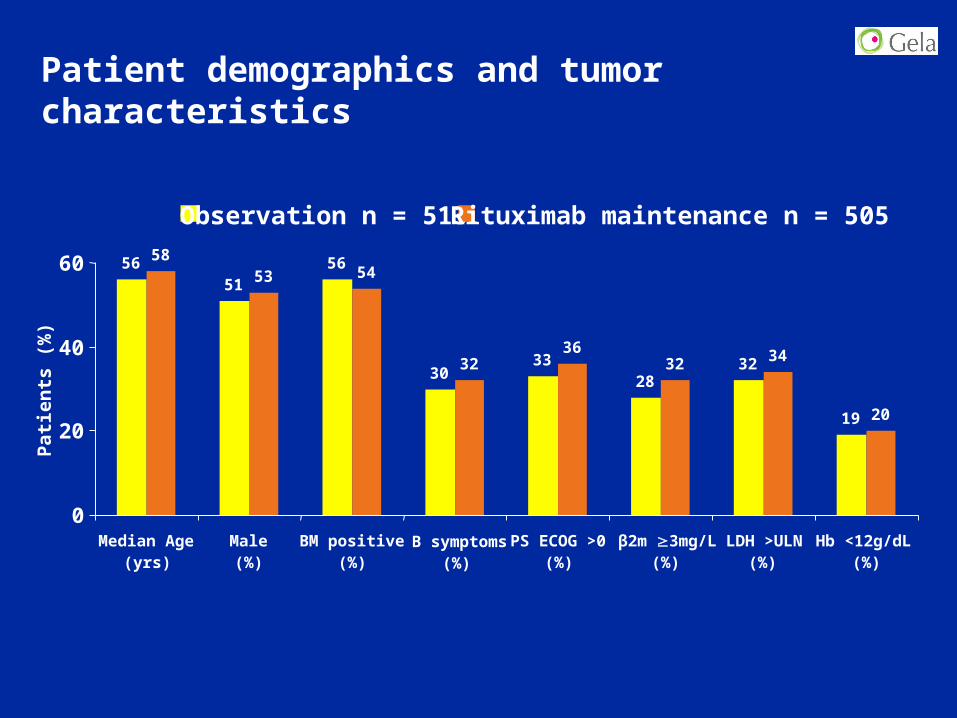
Patient demographics and tumor characteristics
5156
3033
2832
19
5853 54
3236
32 34
20
56
0
20
40
60
Median Age(yrs)
Male BM positive(%)
B symptoms(%)
PS ECOG >0(%)
β2m 3mg/L (%)
LDH >ULN(%)
Hb <12g/dL(%)
Observation n = 513 Rituximab maintenance n = 505
(%)

(2) (≥3)
Induction chemotherapy Response to inductionFLIPI at registration
(≤1)
Patient demographics and tumor characteristics (cont)
21
3642
75
22
3
3832
29
1
36
43
76
22
3
40
3128
2
21
0
10
20
30
40
50
60
70
80
Low Intermediate High R-CHOP R-CVP R-FCM CR CRu PR SD/Notevaluated
Observation n = 513 Rituximab maintenance n = 505
Pat
ien
ts (
%)

Primary endpoint (PFS) met at the planned interim analysis
Rituximab maintenance significantly reduced the risk of progression by 50%
stratified HR=0.50 95% CI 0.39; 0.64p<.0001
Time (months)
Rituximab maintenanceN=505
ObservationN=513
60 12 18 24 30 36
Pro
gre
ssio
n-f
ree
rate 0.8
0.6
0.4
0.2
0
1.0
82%
66%
Patients at risk
505
513
472 443 336 230 103 18
469 411 289 195 82 15

Benefits of rituximab maintenance seen in all major sub-groups evaluated
Subgroup Hazard ratioCategory 95% CIsHazard ratio*N
1018
624
394
216
370
431
768
222
28
721
290
0.38–0.64
0.33–0.62
0.39–0.90
0.19–0.77
0.25–0.61
0.43–0.67
0.31–0.59
0.44–1.08
0.13–2.07
0.38–0.70
0.29–0.72
0.49
0.45
0.59
0.38
0.39
0.61
0.43
0.69
0.51
0.52
0.45
All
< 60≥ 60
FLIPl = 2
FLIPl ≤ 1
FLIPl ≥ 3
R-CHOPR-CVP
R-FCM
CR/CRuPR
0 1 2 3
Response to Induction
Induction Chemotherapy
FLIPl Index
Age
All
* Non-stratified analysis
Favors maintenance Favors observation

Consistent results across secondary endpoints
513
505
487 447 327 218 87 15
483 453 349 235 103 18
Time (months)
60 12 18 24 30 360
Eve
nt-
free
rat
e 0.8
0.6
0.4
0.2
0
1.0
Patients at risk
513
505
492 454 332 225 91 17
484 457 351 243 108 19
Time (months)
60 12 18 24 30 360E
ven
t-fr
ee r
ate 0.8
0.6
0.4
0.2
0
1.0
Time to nextanti-lymphoma treatment
Time to nextchemotherapy treatment
HR = 0.61p = 0.0003
Rituximabmaintenance
ObservationHR = 0.60p = 0.0011
Observation
Rituximabmaintenance
ObservationObservation

Response status at end of maintenance
Observationn = 398 *
Rituximabn = 389 *
Progressive disease (PD) 162 (40.7%) 79 (20.3%)
Stable disease (SD) 1 (0.3%) 0 (0%)
Partial response (PR) 29 (7.3%) 28 (7.2%)
Complete response (CR/CRu) 190 (47.7%) 260 (66.8%)
* Patients not evaluated/missing data: respectively 16 and 22 pts‡ not evaluated in the rituximab maintenance arm: 2 pts
Response: end of Induction → Maintenance n = 190 n = 258 ‡
Patients remaining in CR/CRu 153 (56%) 209 (75%)
Patients converting from PR/SD to CR/CRu 37 (30%) 49 (45%)

Rituximab maintenance (n = 501)
Observation (n = 508)
Safety during rituximab maintenance
52
37
Any adverseevent
Grade 3/4neutropenia
Grade 3/4infections
Grade ≥2infections
Pat
ien
ts (
%)
100
80
60
40
20
0<1 4 <1 4
23
Grade 3/4adverse events
<1
3522
16

• At the time of analysis:
– Few patients withdrew for toxicity-related reasons during rituximab maintenance
• 1 patient in the observation arm• 10 patients in the maintenance arm
– 18 and 13 deaths*, respectively, had occurred in the observation and rituximab maintenance arms
• 12 related to lymphoma in the observation• 10 related to lymphoma in the maintenance arm
Safety during rituximab maintenance (cont)
(*) 3 additional deaths in the maintenance arm in patients that did not receive rituximab

Summary
• Rituximab maintenance for 2 years significantly improved PFS for patients with previously untreated FL who responded to induction with chemotherapy plus rituximab
• Benefits of rituximab maintenance seen in all major sub-groups
• Consistent improvements in secondary endpoints including EFS, TNLT, TNCT, ORR and CR rate at the end of maintenance
• IRC-assessed endpoints were consistent (not shown)
• Safety of maintenance was consistent with the known safety profile of rituximab, with no new or unexpected findings
• Additional follow-up will allow evaluation of a possible effect on overall survival

Conclusions
• The benefit of rituximab maintenance in first line appears superior to that described in relapsing patients:
– After R-CHOP in the EORTC study* HR = 0.69
– After R-CHOP in PRIMA HR = 0.43
• R-chemo followed by 2 years of rituximab maintenance
– Represents a new standard of care for FL patients in need of treatment
– Constitutes a new platform to further develop more efficient(and well tolerated) strategies
* van Oers MHJ, et al. J Clin Oncol 2010; ePub ahead of print.

Ackowledgements
• All the investigators and their staff from 223 centers in 25 countries
• Other cooperative groups in Australia/New Zealand, Spain, Czech Republic, UK and the Netherlands and several key investigators in various countries that made this study possible
• The GELA and GELA-RC teams for organization, monitoring, data cleaning and statistics
Latin America 76
France 624
Belgium 75Portugal 16Spain 54
Czech Republic 36
Denmark 48
U.K / Netherlands 34
Croatia / Serbia 16
Finland 24
India / China / Thailand 40
Australia / New Zaeland 158
Israel / Turkey 16
• Pathology review: L Xerri, N Brousse, D Canioni, F Charlotte, C Chassagne-Clément,P Dartigues, B Fabiani, L Deleval, E Campos, D DeJong
• DMSC members: J Armitage, D Hasenclever, M Ghielmini
• Roche team for their support, especially C Berge, J Maurer, M Mendila, M Wenger,O Manzke & S Zurfluh

Backup slides

PRIMA: Cox multivariate analysis
Covariate included in the modelHazard
Ratio95% CI for
Hazard Ratiop-value
Randomization treatment (R vs. O) 0.50 [0.39;0.64] <.0001
Age (>60 years vs. <60 years) 0.54 [0.49;0.83] .0010
FLIPI (low vs. intermediate/high) 0.62 [0.42;0.90] .0117
FLIPI (high vs. low/intermediate) 1.42 [1.08;1.87] .0121
Induction treatment (R-CHOP vs R-CVP/R-FCM) 0.63 [0.48;0.81] .0004
PFS, Stepwise Backward Selection Procedure, n=1018

Patient demography at induction
R-CHOPn = 881
R-CVPn = 268
R-FCMn = 44
Male 463 (53%) 137 (51%) 22 (50%)
Female 418 (47%) 131 (49%) 22 (50%)
Age (years) at registration
Mean (min–max) 55.4 (22–80) 57 (22–87) 51.3 (29–74)
Median 56 57.5 50
FLIPI score
0–1 193 (22%) 54 (21%) 7 (16%)
2 312 (35%) 91 (34%) 20 (45%)
3–5 375 (43%) 122 (45%) 17 (39%)
n 880 267 44

Patient demography at induction (cont)
R-CHOPn = 881
R-CVPn = 268
R-FCMn = 44
Performance status (ECOG scale)
0 574 (65%) 161 (60%) 24 (55%)
1 272 (31%) 94 (35%) 16 (36%)
2 35 (4%) 13 (5%) 4 (9%)
Ann Arbor stage
I 19 (2%) 4 (1%) -
II 68 (8%) 22 (8%) 5 (11%)
III 167 (19%) 53 (20%) 7 (16%)
IV 627 (71%) 189 (71%) 32 (73%)
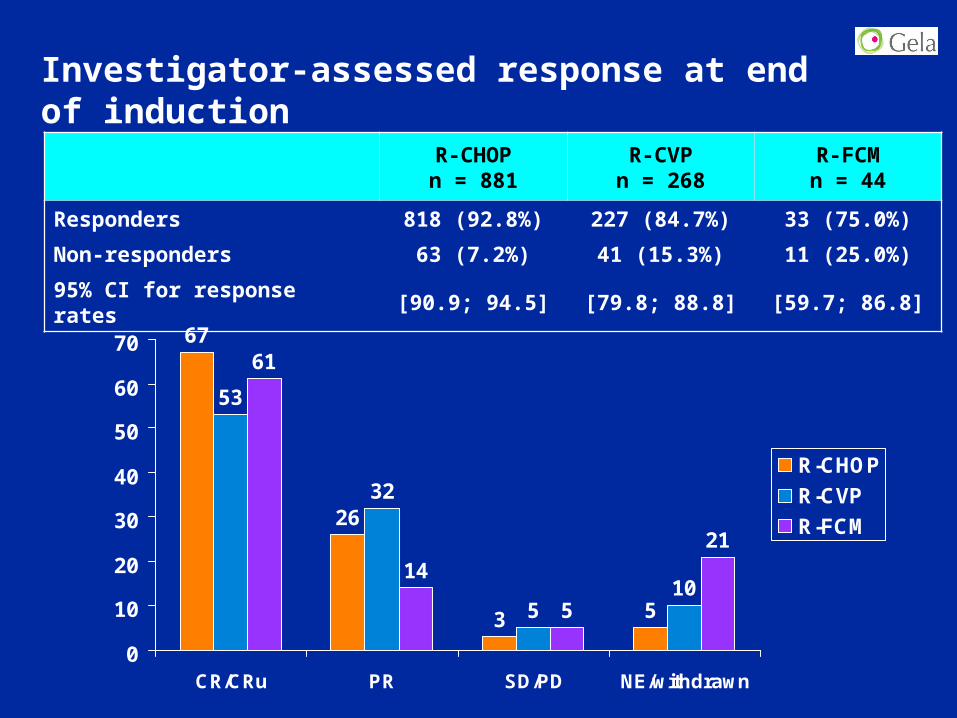
Investigator-assessed response at end of induction
R-CHOPn = 881
R-CVPn = 268
R-FCMn = 44
Responders 818 (92.8%) 227 (84.7%) 33 (75.0%)
Non-responders 63 (7.2%) 41 (15.3%) 11 (25.0%)
95% CI for response rates [90.9; 94.5] [79.8; 88.8] [59.7; 86.8]
67
26
3 5
53
32
510
61
14
5
21
0
10
20
30
40
50
60
70
CR/CRu PR SD/PD NE/withdrawn
R-CHOP
R-CVP
R-FCM

PFS followingR-CHOP induction
Time (months)
Rituximab maintenance
Observation
60 12 18 24 30 36
Ev
en
t-fr
ee
ra
te
0.8
0.6
0.4
0.2
0
1.0
42
Time (months)
Rituximab maintenance
Observation
60 12 18 24 30 36E
ve
nt-
fre
e r
ate
0.8
0.6
0.4
0.2
0
1.0
42
Observation 388 385 361 321 222 153 64 18 113 113 99 87 63 44 19 0
Number left
Rituximabmaintenance 383 383 362 344 262 154 84 17 109 109 97 90 69 46 20 2
PFS followingR-CVP induction
Benefits of rituximab maintenance seen in major sub-groups evaluated
88%
68%
71%
61%

Rituximab maintenance does not adversely affect quality of life
Rituximab maintenance Observation
0
10
20
30
40
50
60
70
80
90
100
Glo
bal
Hea
lth
Sta
tus
scal
e
BL AI +1YEOT1Y BL AI +1YEOT1Y
BL =baselineAI = after induction1Y = 1 year of treatment
n 374 337 174 146 5304 341 218 177 13
EOT = end of treatment+1Y = 1 year after end of treatment
304 341 218 177 13

Immunoglobulin levels during maintenance / observation
IgG IgA
IgM
Imm
un
og
lob
ulin
G (
G/L
) 12
10
8
6
4
Baseline Visit 3 Visit 6 Visit 12 Assess end trt
Imm
un
og
lob
ulin
A (
G/L
) 6
3
0
-3
Observation / n = 508 Rituximab / n = 501
Imm
un
og
lob
ulin
M (
G/L
)
0.0
0.3
0.6
0.9
1.2
1.5
Baseline Visit 3 Visit 6 Visit 12 Assess end trt
Baseline Visit 3 Visit 6 Visit 12 Assess end trt

Laboratory values during maintenance/observation
Neutrophils Platelets
Lymphocytes
Neu
trop
hils (
10
**9
/L)
12
Base-line
11109876543210
2 3 4 5 6 7 8 9 10 11 12 Endtrt
Pla
tele
ts (
10
**9
/L)
0
100
200
300
400
500600
700
800
900
1000
Lym
ph
ocyte
s (
10
**g
/L)
0
1
2
3
4
5
6
7
8
Observation / n = 508 Rituximab / n = 501
VISIT
Base-line
2 3 4 5 6 7 8 9 10 11 12 EndtrtVISIT
Base-line
2 3 4 5 6 7 8 9 10 11 12 EndtrtVISIT