g2 cindy van wicklin - gateby care center's quality improvement team presents engaging staff
TRANSCRIPT

Gateby Care Center’s Quality Improvement Team
presents
Engaging Staff
Acknowledgement
• Interior Health Authority
• Gateby Care Center
• SCOPE (Safer Care of Older Persons in Residential Care Environment)
Gateby Care Center • Located in Vernon B.C. • Part of the Interior Health Authority • 75 bed Residential Care Home • 2nd Floor is our Dementia Unit • 3rd Floor is complex and convalescent care • 1st Floor houses Vernon’s Adult Daycare
Center and (EAST) Elderly Assessment and Treatment Program

• Team Leader: Cindy V.W. (Residential Care Attendant) • Core Team: Celia (RCA) Candra (RCA) Trent (RCA) Cindy Mc (RCA) Bev A. (RCA) Carrie (LPN) Brenda (LPN) Carolyn (RN) Rhonda (RN) Representative Members: Donna (Gateby Manager) Lorrianne (Residential Care Coordinator) Marijon (Program Service Manager) Jan (Food Service Manager) Associate Members: members who join our team for 1 specific problem or goal
Our Journey to the Quality Improvement Team
-Our bus ride has had many bumps and stops along the way
-To keep the bus moving we needed to: - load the bus - keep on the bus - deal departures
• The Quality Improvement Model of Problem Solving
• Engaging RCA’s to realize the difference they can make
• Greater quality and safety of care for residents
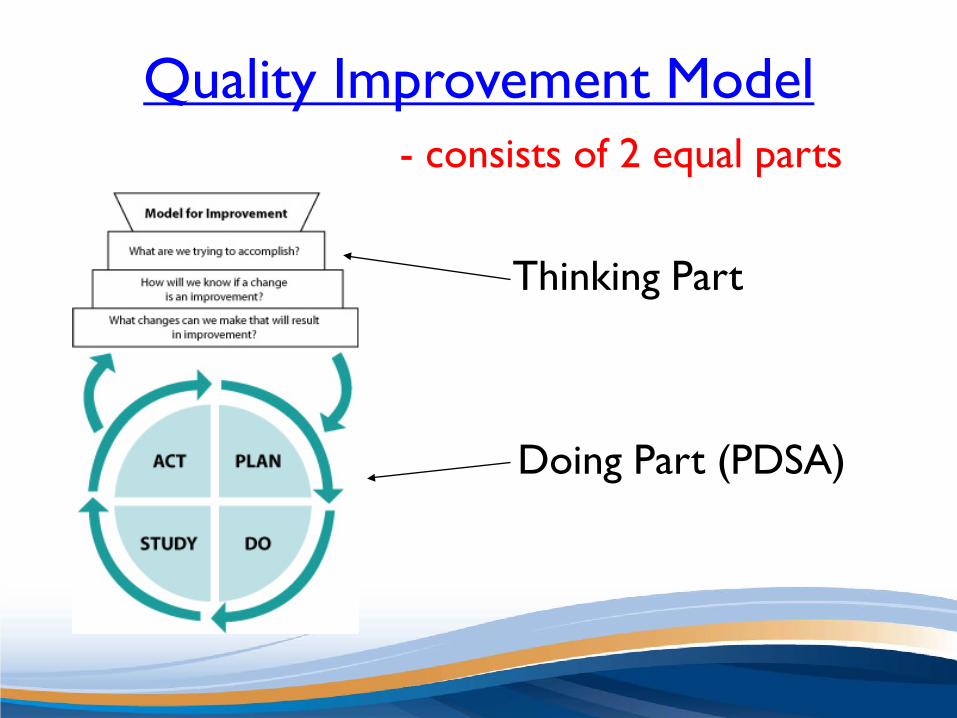
Quality Improvement Model - consists of 2 equal parts Thinking Part Doing Part (PDSA)
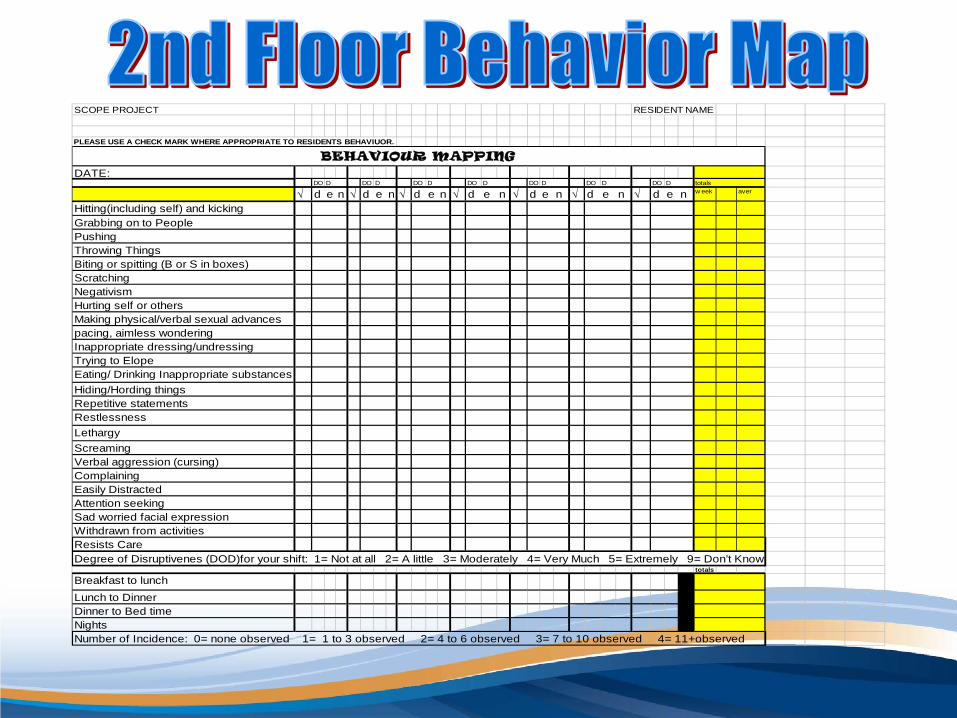
SCOPE PROJECT RESIDENT NAME
PLEASE USE A CHECK MARK WHERE APPROPRIATE TO RESIDENTS BEHAVIUOR.
DATE:DO DO DO DO DO DO DO totals
√ d e n √ d e n √ d e n √ d e n √ d e n √ d e n √ d e n w eek aver
Hitting(including self) and kicking Grabbing on to PeoplePushingThrowing ThingsBiting or spitting (B or S in boxes) ScratchingNegativism Hurting self or othersMaking physical/verbal sexual advancespacing, aimless wonderingInappropriate dressing/undressingTrying to Elope Eating/ Drinking Inappropriate substancesHiding/Hording thingsRepetitive statements Restlessness LethargyScreamingVerbal aggression (cursing)ComplainingEasily DistractedAttention seeking Sad worried facial expression Withdrawn from activities Resists CareDegree of Disruptivenes (DOD)for your shift: 1= Not at all 2= A little 3= Moderately 4= Very Much 5= Extremely 9= Don’t Know
totals
Breakfast to lunch Lunch to DinnerDinner to Bed timeNights Number of Incidence: 0= none observed 1= 1 to 3 observed 2= 4 to 6 observed 3= 7 to 10 observed 4= 11+observed
BEHAVIOUR MAPPING
D D D D D D D
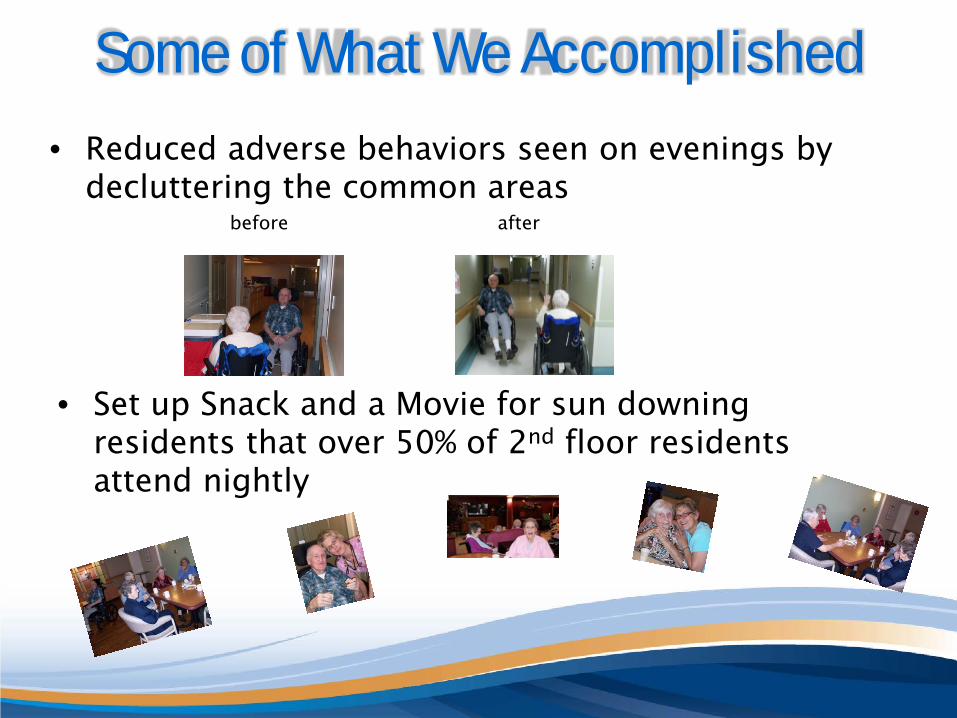
Some of What We Accomplished • Reduced adverse behaviors seen on evenings by
decluttering the common areas before after
• Set up Snack and a Movie for sun downing residents that over 50% of 2nd floor residents attend nightly

• Decreased Adverse Behaviours • Decreased Pre-bath Medication use • Increased Resident care quality • Increased resident and staff safety
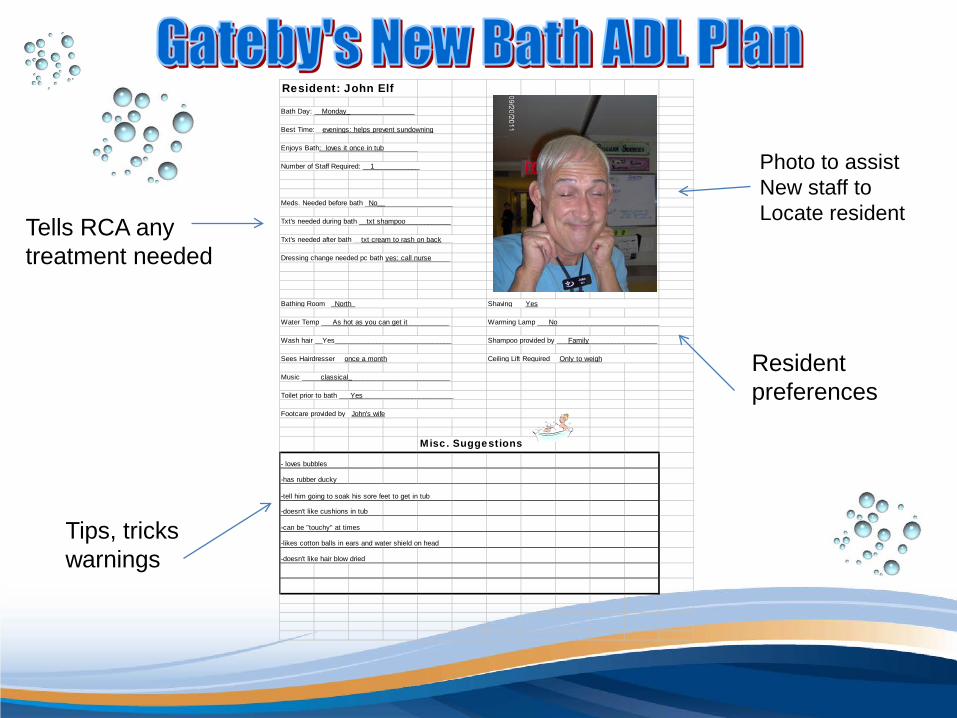
Resident: John Elf
Bath Day: __Monday__________________
Best Time:__evenings: helps prevent sundowning
Enjoys Bath: loves it once in tub_________
Number of Staff Required: __1____________
Meds. Needed before bath _No____________________
Txt's needed during bath __txt shampoo____________
Txt's needed after bath __txt cream to rash on back___
Dressing change needed pc bath yes: call nurse_____
Bathing Room __North___________________________ Shaving ___Yes________________________________
Water Temp ___As hot as you can get it___________ Warming Lamp ___No___________________________
Wash hair __Yes_______________________________ Shampoo provided by ___Family__________________
Sees Hairdresser __once a month_________________ Ceiling Lift Required __Only to weigh_______________
Music _____classical___________________________
Toilet prior to bath ___Yes________________________
Footcare provided by _John's wife__________________
Misc. Suggestions
- loves bubbles
-has rubber ducky
-tell him going to soak his sore feet to get in tub
-doesn't like cushions in tub
-can be "touchy" at times
-likes cotton balls in ears and water shield on head
-doesn't like hair blow dried
Tells RCA any treatment needed
Tips, tricks warnings
Photo to assist New staff to Locate resident
Resident preferences
• Changing dementia behaviors vs non dementia behaviors
• Our first 3rd floor individual trial
• Involving the resident
• Taking what worked on one shift and adapting for the other shifts
• Taking what worked on one resident and adapting for other residents
• Set a stretchable goal • You need to collect data to see where or if change is needed, but only
the data you require • Make behavioral mapping staff friendly • Keep staff involved and informed
• There is a difference between dementia and non-dementia behavior

Contacts: Cindy VanWicklin – team leader Gateby Care Center’s Quality Improvement Team
[email protected] Celia Foster – core team member Gateby Care Center’s Quality Improvement Team