gas exchange chapter 44. learning objectives define physiological respiration, ventilation and...
TRANSCRIPT

Gas Exchange
Chapter 44

Learning Objectives
• Define Physiological Respiration, Ventilation and Perfusion
• Diagram the human respiratory tract and explain functions of the organs
• Define Tidal Volume, Vital Capacity and Residual Volume
• Compare and contrast negative and positive pressure breathing
• Describe how breathing is both a conscious and subconscious effort
• Describe the physiological gradient that allows for CO2 and O2 diffusion within the body
• Define COPD and health impact

Physiological Respiration
• Process by which animals exchange O2 and CO2 with the environment
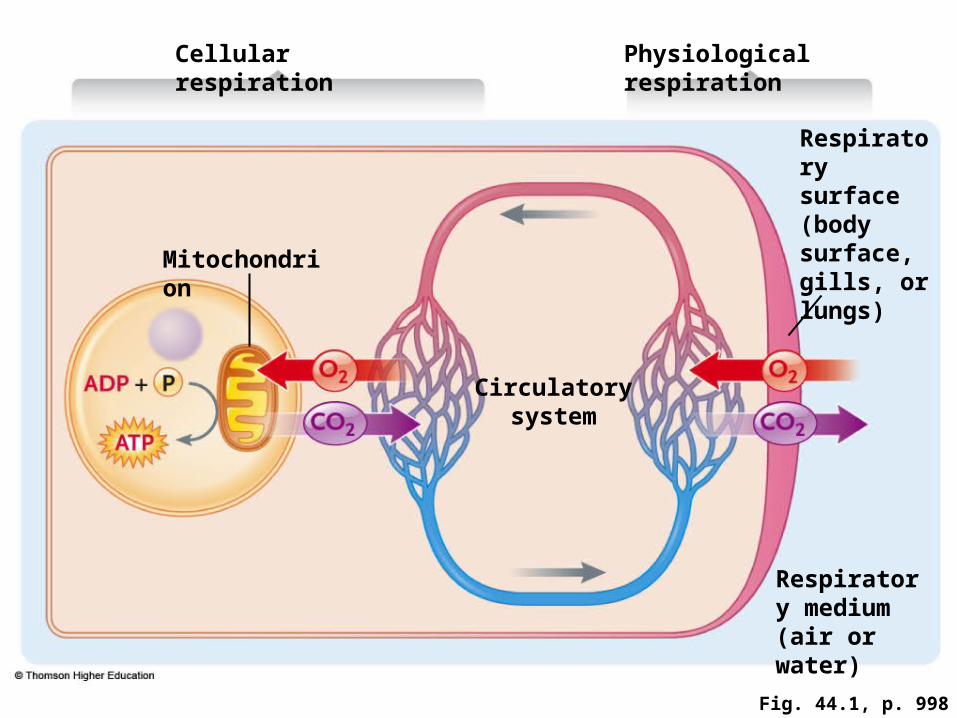
Fig. 44.1, p. 998
Cellular respiration Physiological respiration
Respiratory surface (body surface, gills, or lungs)
Mitochondrion
Circulatory system
Respiratory medium (air or water)

Breathing (Gas Exchange)
• Two primary operating features of gas exchange– The respiratory medium, either air or water– The respiratory surface, a wetted epithelium
over which gas exchange takes place

Respiratory Surfaces
• In some invertebrates, the skin is the respiratory surface
• In other invertebrates and all vertebrates, gills or lungs are the primary respiratory surfaces

Gas Exchange
• Simple diffusion of molecules drives exchange of gases across the respiratory surface– From regions of higher concentration to
regions of lower concentration
• Area of respiratory surface determines total quantity of gases exchanged by diffusion

Maximizing Gas Exchange
Concentration gradients of O2 and CO2 across respiratory surfaces are kept at optimal levels by ventilation and perfusion
Ventilation: Movement of respiratory media over the external respiratory surface
Perfusion: Movement of circulatory fluid over the internal respiratory surface

Air Breathers
• Air is high in O2 content
– Allows air-breathers to maintain higher metabolic levels than water breathers
• Air has lower density and viscosity than water– Allows air breathers to ventilate respiratory
surfaces with relatively little energy

Insects: Tracheal System
• Insects breathe by a tracheal system– Air-conducting tubes (trachea) lead from the
body surface (through spiracles) and branch to all body cells
• Gas exchange takes place in fluid-filled tips at ends of branches

Lungs (Air Breathers)
• Invaginations of the body surface– Allow air to become saturated with water
before it reaches the respiratory surface– Reduce water loss by evaporation

Lung Ventilation
• Positive pressure breathing– Air is forced into lungs by muscle contractions
• (Frogs do this)
• Negative pressure breathing– Muscle contractions expand lungs, lowering
air pressure inside– Allows air to be pulled into the lungs

Mammalian Respiratory System• Air enters the respiratory system through
the nose and mouth and passes through the pharynx, larynx, and trachea
• Trachea divides into two bronchi leading to lungs
• Within lungs, bronchi branch into bronchioles, leading into alveoli surrounded by networks of blood capillaries

Fig. 44.8, p. 1004
Nasal passages Chamber in which air is moistened, warmed, and filtered and in which sounds resonate
Pharynx (throat) Airway connecting nasal passages and mouth with larynx; enhances sounds; also connects with esophagus
Mouth Supplemental airway
Epiglottis Closes off larynx during swallowingLarynx (voice box) Airway where sound is produced; closed off during swallowing
Pleura Double-layered membrane that separates lungs from the wall of the thoracic cavity; fluid between its two layers lubricates breathing movementsTrachea (windpipe)
Airway connecting larynx with two bronchi that lead into the lungsLung Lobed, elastic organ of breathing exchanges gases between internal environment and outside air
Intercostal muscles Skeletal muscles between ribs that contract to fill and empty lungs
Bronchi Increasingly branched airways leading to alveoli of lung tissue
Diaphragm Muscle sheet between the chest cavity and abdominal cavity that contracts to fill lungs
Bronchiole
Alveoli (sectioned)
Alveoli
Alveoli
Pulmonary capillaries

Ventilation: Mammals
• Negative pressure mechanism
• Air is exhaled passively– Relaxation of diaphragm and external
intercostal muscles between ribs– Elastic recoil of lungs (pleural membranes)
• Deep and rapid breathing– Forceful expulsion of air driven by contraction
of internal intercostal muscles

Fig. 44.9, p. 1005
Inward bulk flow of air
Outward bulk flow of air
Internal intercostal muscles
External intercostal muscles
Diaphragm
Inhalation. Diaphragm contracts and moves down. The external intercostal muscles contract and lift rib cage upward and outward. The lung volume expands.
Exhalation during breathing or rest. Diaphragm and external intercostal muscles return to the resting positions. Rib cage moves down. Lungs recoil passively.

Measuring Lung Ventilation
• Tidal volume – Amount of air moved in and out of lungs during an
inhalation and exhalation
• Vital capacity – Total volume of air a person can inhale and exhale
by breathing as deeply as possible
• Residual volume– Air remaining in the lungs after as much air as
possible is exhaled

Control of Breathing
• Control mechanisms– Local chemical controls– Regulation centers in the brain stem
• Control functions – Match rate of air and blood flow in lungs– Link rate and depth of breathing to body’s
requirements for O2 uptake and CO2 release

Interneurons Regulate Breathing
• Basic rhythm of breathing – Produced by interneurons in the medulla
• When more rapid breathing is required– Other interneurons in the medulla reinforce
inhalation, produce forceful exhalation
• Fine-tuned breathing– Two interneuron groups in the pons stimulate
or inhibit the inhalation center in the medulla

Blood Gas Control
Sensory receptors in medulla detect changes in levels of O2 and CO2 in blood and body fluids (aortic and carotid, too)
• Control centers in medulla and pons adjust rate and depth of breathing to compensate for changes in blood gases

O2 Transport
• O2 diffuses from alveolar air into blood
– Partial pressure of O2 is higher in alveolar air than in blood in capillary networks surrounding alveoli
• Most O2 entering the blood combines with hemoglobin inside erythrocytes

Fig. 44.11, p. 1008
Dry inhaled air
Moist exhaled air Alveolar sacs
100 40
160 0.04 120 27Capillaries entering lungs
40 O2
46 CO2Pulmonary
veins100 40Pulmonary arteries
40 46O2
100 40
Alveolar sacs
CO2
Start of veins in body tissues
Start of capillaries in body tissues 40 46 Cell
100 40
Capillaries entering tissuesLess than 40 More than 46 100
O2
40 CO2
Cells of body tissues
40 46
O2
CO2

Hemoglobin and Oxygen
• One hemoglobin molecule can combine with four O2 molecules
• Large quantities of O2 combined with hemoglobin maintain a large partial pressure gradient between O2 in alveolar air and in blood

Fig. 44.12a, p. 1009
a. Hemoglobin saturation level in lungs
Saturation level in lungsHemoglobin
O2
Oxy
gen
sat
ura
tio
n (
%)
Body tissues PO2 (mm Hg)
Alveoli
In the alveoli, in which the PO2 is about 100 mm Hg and the pH is 7.4, most hemoglobin molecules are 100% saturated, meaning that almost all have bound four O2 molecules.

O2 Diffuses into Body Cells
• O2 concentration in interstitial fluid and body cells is lower than in blood plasma
• O2 diffuses from blood into interstitial fluid, and from interstitial fluid into body cells

CO2 Transfer: Body Tissues
• Partial pressure of CO2 is higher in tissues than in blood– About 10% of CO2 dissolves in blood plasma
– 70% is converted into H+ and HCO3-
(bicarbonate) ions – 20% combines with hemoglobin

Fig. 44.13a, p. 1009
a. Body tissuesBody cells
CO2
HCO3– + H+ Capillary
wall
In body tissues, some of the CO2 released into the blood combines with water in the blood plasma to form HCO3
– and H+. However, most of the CO2 diffuses into erythrocytes, where some combines directly with hemoglobin and some combines with water to form HCO3
– and H+. The H+ formed by this reaction combines with hemoglobin; the HCO3
– is transported out of erythrocytes to add to the HCO3
– in the blood plasma.
CO2 + H2OSlow
CO2 + H2O CO2
Erythrocyte
Fast
HCO3– + H+
Hemoglobin
Capillary

Fig. 44.13b, p. 1009
b. Lungs
HCO3– + H+ CO2 + H2O
SlowIn the lungs, the reactions are reversed. Some of the HCO3
– in the blood plasma combines with H+ to form CO2 and water. However, most of the HCO3
– is transported into erythrocytes, where it combines with H+ released from hemoglobin to form CO2 and water. CO2 is released from hemoglobin. The CO2 diffuses from the erythrocytes and, with the CO2 in the blood plasma, diffuses from the blood into the alveolar air.
HCO3– + H+
Hemoglobin
Fast
CO2 + H2O CO2
Capillary wall
Alveolar air
Alveolar wall
CO2
CO2

44.5 Respiration at High Altitudes and
in Ocean Depths
• High altitudes reduce the PO2 of air entering the lungs
• Diving mammals are adapted to survive the high partial pressures of gases at extreme depths

High Altitudes: PO2 Decreases
• When mammals move to high altitudes, the number of red cells and amount of hemoglobin per cell increase
• These changes are reversed if the animals return to lower altitudes

Adaptations to High Altitudes
• Humans living at higher altitudes from birth develop more alveoli and capillary networks in the lungs
• Some mammals and birds adapted to high altitudes have forms of hemoglobin with greater O2 affinity
– Allows saturation at lower PO2

Deep-Diving Marine Mammals
• Blood (compared to other mammals)– Contains more red blood cells – Has higher hemoglobin content – Greater blood volume per unit of body weight
• Muscles contain more myoglobin– Allows more O2 to be stored in muscle tissues

Adaptations for Deep-Diving
• During a dive– Heartbeat slows– Circulation is reduced to all parts of the body
except the brain

COPD
• Chronic Obstructive Pulmonary Disorder
• Number 4 leading cause of Death in US
• 24 million adults affected
• Causes include tobacco use and asthma
• Asthma- Percent of noninstitutionalized adults who currently have asthma: 7.3%
• Percent of children who currently have asthma: 9.4%