gastric acid secretion 1. acid synthesis – regulated by 3 transporters lumen plasma parietal cell
TRANSCRIPT

Gastric Acid Secretion1. Acid synthesis – regulated by 3 transporters
LumenPlasma
Parietal cell

2. Action of secretagogues
Cholinergic nerve Mast-like cell Blood vessel
Parietal cell
Acetylcholine Histamine Gastrin

• The defensive forces– Bicarbonate– Mucus layer– Mucosal blood flow– Prostaglandins– Growth factors
• The aggressive forces– Helicobacter pylori– HCl acid– Pepsins– NSAIDs– Bile acids– Ischemia and hypoxia. – Smoking and alcohol
• When the aggressive factors increase or the defensive factors decrease, mucosal damage will result, leading to erosions and ulcerations.
Gastric Mucosa & Secretions

Structural Considerations
Mechanisms that maintain mucosal integrity

• The two most common causes of PUD are:
– Helicobacter pylori infection– Non-steroidal anti-inflammatory drugs (NSAIDS)
• Other uncommon causes include:
– Gastrinoma (Gastrin secreting tumor)– Stress ulceration (trauma, burns, critical illness)– Viral infections– Vascular insufficiency
Etiology

Etiology – Helicobacter pylori
Helicobacter pylori

Helicobacter pylori as a cause of PUD
• The majority of PUD patients are H. pylori infected.
• Studies show that about 95% of patients with DU and 85% with GU are infected with H. pylori
• Cure of H. pylori infection reduces ulcer recurrence.
Etiology – Helicobacter pylori

Helicobacter pylori as a cause of PUD
• Over a 10 year period 1 out of 133 (0.75%) individuals without H. pylori developed a peptic ulcer, compared with 35 out of 321 (11%) with H. pylori infection.
• The incidence of peptic ulcers in H.pylori infected people is about 1% per year.
Etiology – Helicobacter pylori

Non-steroidal anti-inflammatory drugs (NSAIDs)
• Symptomatic GI ulceration occurs in 2% to 4% of patients treated with NSAIDs for 1 year.
• In view of the million of people who take NSAIDs annually, these small percentages translate into a large number of symptomatic ulcers.
• The effects of aspirin and NSAIDs on the gastric mucosa ranges from mucosal hemorrhages to erosions and acute ulcers.
Etiology – NSAIDs

Etiology – NSAIDS
Effect of NSAIDS
• All NSAIDs reduce the mucosal production of prostaglandins from precursor membrane fatty acids.
• The drugs also generate oxygen-free radicals and products of the lipoxygenase pathway that may contribute to ulceration.

Etiology – NSAIDS
• Users of NSAIDs are at approximately 3 times greater relative risk of serious adverse gastrointestinal events than nonusers.
• Additional risk factors include: – Age greater than 60 years– Smoking – Previous history of GI events – Concomitant corticosteroid use. In terms of serious
complications, the combination of steroids and NSAIDs leads to a 10-fold increase in GI bleeding and a 20-fold increase in GI-related death.

Etiology – NSAIDS
Type of NSAID and Risk of Ulcer
Risk Group Drug Relative Risk
Low Ibuprofen 2.0Diclofenac 4.2
Medium Naproxen 9.1Indomethacin 11.3Piroxicam 13.7
High Ketoprofen 23.7Azapropazone 31.5

Tests for Helicobacter pylori
Non-invasive• C13 or C14 Urea Breath Test• Stool antigen test• H. pylori IgG titer (serology)
Invasive• Gastric mucosal biopsy• Rapid Urease test
Diagnosis of H. pylori

• Gastric Ulcer on Endoscopy
Peptic Ulcer Disease - Diagnosis
Chronic Gastric Ulcers

Complications of PUD
• Bleeding
• Perforation
• Gastric outlet or duodenal obstruction
• Chronic anemia
PUD – Complications

• Complications of PUD on Endoscopy
Peptic Ulcer Disease - Complications
Bleeding DU Perforated GU Duodenal stricture
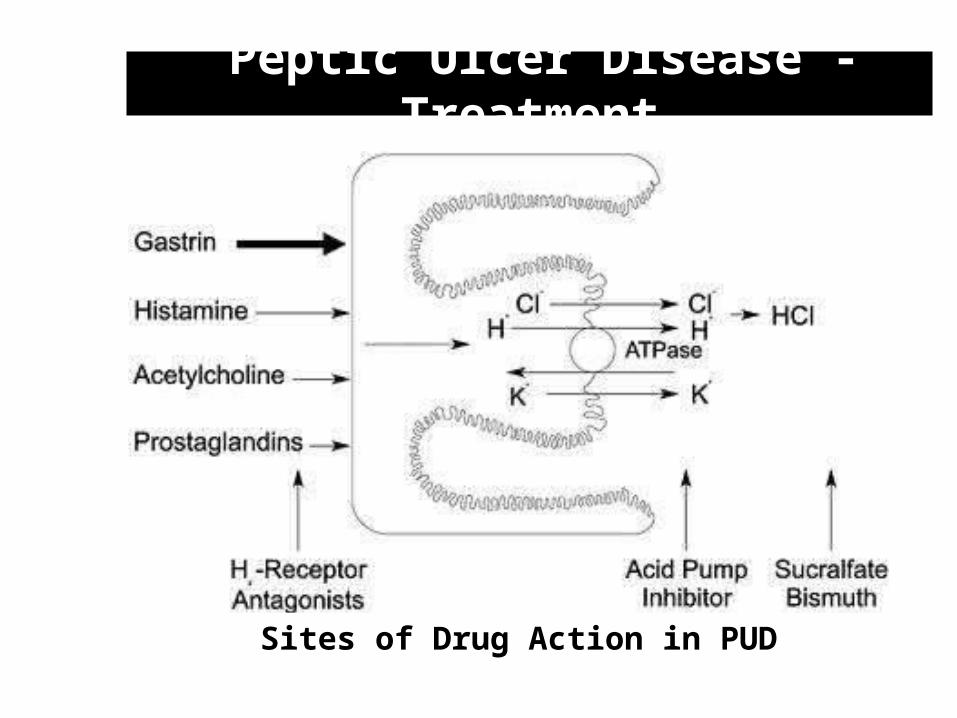
Peptic Ulcer Disease - Treatment
Sites of Drug Action in PUD
1. Neutralise secreted acid – Antacids
Bases that raise GI tract pH
Primarily salts of calcium, magnesium and aluminium• Aluminium hydroxide• Calcium carbonate• Magnesium hydroxide or trisilicate

2. Drugs that inhibit acid secretion
Cholinergic nerve Mast-like cell Blood vessel
Parietal cell
Acetylcholine Histamine Gastrin 1. H2R antagonists[Ranitadine]
3. Arachidonic acidagonists[Misoprostol]
2. Proton pump inhibitors[Pantoprazole

3. Protect mucosa from damage
Agents that coat the mucosa and protect from acid irritation
- Bismuth subcitrate (colloidal suspension)- Sucralfate (complex of aluminium hydroxide and sucrose)
Peptic Ulcer + sucralfate After 5 days of treatment

4. Eradicate causative agent (H. pylori)
• Most common cause of gastric ulcers.• Infects ~ 30% population.• Readily detected with ‘urea breath test’, bloodtest (for antibodies).
H. Pylori invades the stomachand duodenal lining, weakens theresistance of the lining to acidand stimulates acid secretion.Local inflammation can also beobserved.

Treatment of NSAID-induced gastric ulcers
1. Stop NSAID, if possible.2. If NSAID required, use lowest effective dose, for shortest period.3. Effective treatment with proton pump inhibitor (Pantoprazole).
Guide to minimising NSAID gastric ulcer risk:
Low vascular
Risk
High vascular
Risk
Low NSAID risk High NSAID risk
Non-selective NSAID COX2-selective NSAIDor
Non-selective NSAID + PPI
Non-selective NSAIDwith/without PPI
Non-selective NSAID + PPI
[Always check for H. pylori involvement]

Regimen for eradication of H pylori:
TRIPLE THERAPY X 14 DAYS:
[PPI + Clarithromycin 500 mg + ( Metronidazole 500 mg or amoxicillin 1 g)] twice a day. (Tetracycline 500 mg can be substituted for amoxicillin or metronidazole.)
QUADRUPLE THERAPY x 14 DAYS:
PPI twice daily + Metronidazole 500 mg three times daily + (Bismuth subsalicylate 525 mg + tetracycline 500 mg four times daily)
OR
H2 receptor antagonist twice a day + ( Bismuth subsalicylate 525 mg + Metronidazole 250 mg + tetracyclione 500 mg) four times daily