gastric analysis with fractional test meals (ethanol...
TRANSCRIPT

S. KWIECIEÑ, S. J. KONTUREK
GASTRIC ANALYSIS WITH FRACTIONAL TEST MEALS (ETHANOL,CAFFEINE, AND PEPTONE MEAL), AUGMENTED HISTAMINE OR PENTAGASTRIN TESTS, AND GASTRIC PH RECORDING
Department of Physiology, Jagiellonian University Medical College, Cracow, Poland
For centuries it was recognized that the stomach produces a juice, which has acidicproperties, however, it was not until 1824 when Prout demonstrated the presence ofhydrochloric acid in gastric juice. At the same time experiments on a patient withgastric fistula began by W. Beaumont showing alterations of acid secretion aftermeals and under various psychological conditions. After the discovery by L.Popielski in 1920 that histamine is a direct stimulant of oxyntic glands, histaminestarted to be used in the 1930s in gastric secretory tests. Then in 1949 the dose ofhistamine was established by K. Kowalewski to induce in humans maximal gastricsecretion and in 1953 Kay from UK, using a similar dose of histamine (0.04 mg/kg),introduced augmented histamine test to determine maximal acid output. Thedigestive period of gastric secretion can be divided into 3 phases: cephalic phase,gastric phase, and intestinal phase. When an acidified meal reaches the antrum orproximal part of the small intestine, the inhibitory autoregulatory mechanisms aretriggered. Using a peptone meal as a physiological stimulant of gastric secretion,Fordtran and Walsh designed in 1973 the intragastric titration method. Histaminestimulates H1 and H2 receptors, producing some side effects so Betazole (Histalog),an analogue of histamine was introduced, because of smaller side effects than withhistamine. In 1967, pentagastrin, which contains a C-terminal amino-acid sequenceof gastrin and does not exert serious side effects, was applied first in Poland as astimulant of gastric acid secretion instead of histamine. At the present time, a 12 or24 h pH-metry with a magnetic recording of gastric acidity using the Digitrapper wasfound to have a greater diagnostic value in assessment of gastric acid secretion undernatural conditions including meal than classic gastric secretory tests. This techniquehas been widely used in detecting the duodeno-gastric or gastro-esophageal reflux(GERD) and testing various drugs affecting gastric acid secretion and healing acid-pepsin disorders.
K e y w o r d s : gastric secretion, meal, histamine, pentagastrin, intragastric titration, pH-recording
JOURNAL OF PHYSIOLOGY AND PHARMACOLOGY 2003, 54, S3, 69�82
www.jpp.krakow.pl

INTRODUCTION
Archaic theories on gastric content
For centuries it was known that the stomach produces a juice, which has souror acidic properties. However, it was not clear what kind of acid was produced inthe stomach. The first hypotheses considered three possibilities: lactic acid, aceticacid, or butyric acid. Not until the XIX century, the detection of the presence ofhydrochloric acid in gastric juice was made. The controversy concluded with thediscovery of this acid in the stomach by Prout in 1824 (1).
Examination of gastric acid secretion in XIXth and XXth centuries
In 1822, Beaumont began his famous experiments on a wounded patient whodeveloped a chronic gastric fistula (2). During the next eleven years, he collectedgastric juice, obtained through a fistula from this patient and analyzed its content.He discovered the alterations in gastric secretion depending on the digestive stateof the patient. These investigations initiated gastric secretory testing in man (1).
The first studies related to the stimulation of gastric acid secretion took placein 1876, when Leube applied a standard meal 7 h before gastric juice aspiration.The concept of a fractional test meal was introduced in physiology after theexperiments of Ewald and Boas, Ehrenreich, as well as Rehfuss (2 - 4). Theirinvestigations were carried out in the second part of XIXth century and thebeginning of XXth century. They collected samples of gastric acid at frequentintervals after a standard meal.
Since 1930, the method of stimulated gastric secretion was developed. Pollandand Bloomfield in 1931 (5), and then Ihre in 1938 (6) used histamine, which wasknown since L. Popielski's discovery in 1920 to be a potent and direct gastricsecretagogue. Histamine was initially administered in a dose of 10 µg/kg tostimulate gastric acid secretion in humans. K. Kowalewski, working after WWIIin the Free University of Brussels, attempted to establish the optimal dose ofhistamine to achieve the maximal stimulation of acid secretion, by using a doseof 0.03-0.04 mg/kg. He concluded that this dose fulfills the criteria for themaximal histamine test. Kay, using an identical dose to that of Kowalewski, thatis 0.04 mg/kg, also reached maximal stimulation of acid secretion in humans in1953 (7). Because of the increased dose of secretagogue was used and maximalacid output was reached, this test was called by Kay the "augmented histaminetest". Kay attempted to explain the observed phenomenon of maximal histaminetests by correlating maximal acid output with parietal cell mass (number), whichwas subsequently confirmed in humans by Card and Marks in 1960 (8).
Pathological aspects of gastric acid secretion
In the 1920, when Pavlov's theories of nervism dominated in gastricphysiology, L. Popielski, Polish professor of pharmacology at University in Lvov,
70
found for the first time that histamine is a direct and potent non-nervous stimulantof gastric acid secretion and may be useful in testing gastric secretory activity inhumans. Basal acid secretion was thought at this time to be of neural origin (9).In 1932, Henning and Norjsoth (10) demonstrated for the first time that in patientswith duodenal ulcers, an increase of gastric acid secretion occurred. The reasonsof this enhancement of gastric secretion in ulcer patients remained unknown, untilthe discovery of Helicobacter pylori infection and its eradication in therapeuticregimen of ulcer disease starting in 1980s (11).
Phases of gastric secretion
Gastric secretion depends upon the intrinsic activity of gastric glands,autonomic innervation, gastrointestinal hormones and blood flow in the gastricmucosa. A meal appears to be the most potent, physiological stimulant of acidand pepsin secretion. The dual control of gastric secretion by vagus nerves andgastrin ensures optimal postprandial stimulation (12).
The digestive phase of gastric secretion can be classically divided into 3phases: cephalic, gastric and intestinal phase.
Cephalic phase of gastric secretion
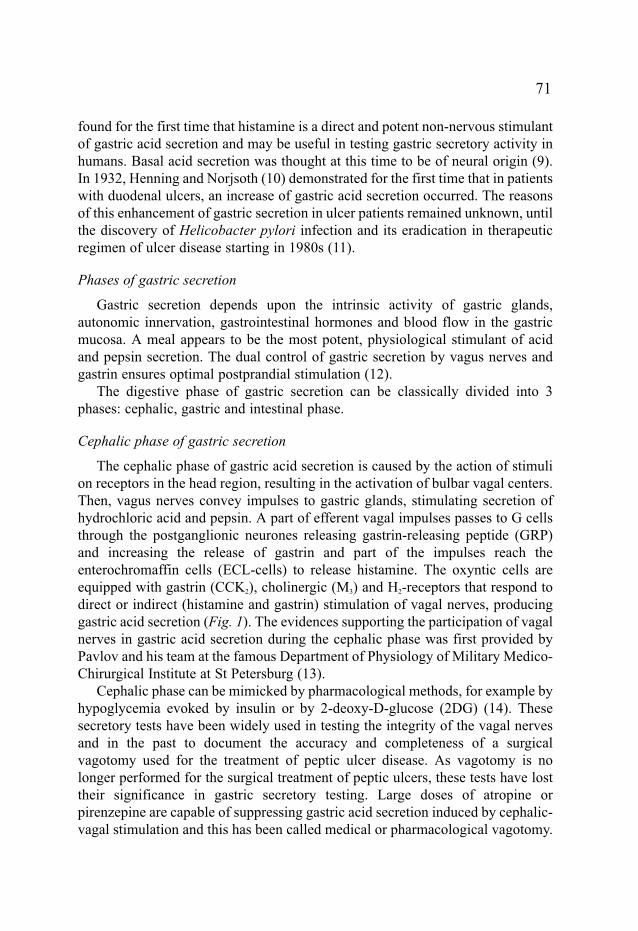
The cephalic phase of gastric acid secretion is caused by the action of stimulion receptors in the head region, resulting in the activation of bulbar vagal centers.Then, vagus nerves convey impulses to gastric glands, stimulating secretion ofhydrochloric acid and pepsin. A part of efferent vagal impulses passes to G cellsthrough the postganglionic neurones releasing gastrin-releasing peptide (GRP)and increasing the release of gastrin and part of the impulses reach theenterochromaffin cells (ECL-cells) to release histamine. The oxyntic cells areequipped with gastrin (CCK2), cholinergic (M3) and H2-receptors that respond todirect or indirect (histamine and gastrin) stimulation of vagal nerves, producinggastric acid secretion (Fig. 1). The evidences supporting the participation of vagalnerves in gastric acid secretion during the cephalic phase was first provided byPavlov and his team at the famous Department of Physiology of Military Medico-Chirurgical Institute at St Petersburg (13).
Cephalic phase can be mimicked by pharmacological methods, for example byhypoglycemia evoked by insulin or by 2-deoxy-D-glucose (2DG) (14). Thesesecretory tests have been widely used in testing the integrity of the vagal nervesand in the past to document the accuracy and completeness of a surgicalvagotomy used for the treatment of peptic ulcer disease. As vagotomy is nolonger performed for the surgical treatment of peptic ulcers, these tests have losttheir significance in gastric secretory testing. Large doses of atropine orpirenzepine are capable of suppressing gastric acid secretion induced by cephalic-vagal stimulation and this has been called medical or pharmacological vagotomy.
71
Gastric phase of gastric secretion
The gastric phase occurs during the presence of a meal in the stomach. A majorrole in this phase has gastrin released from G cells in the antral part of the stomach;however, short- and long vago-vagal reflexes initiated by the distention of thegastric wall and products of protein digestion also contribute to gastric acidsecretion. Gastrin was discovered by Edkins in 1905 (15). In the 1960's Gregoryand his colleagues purified gastrin from antral mucosal extract and from a tumorof Zollinger-Ellison syndrome (gastrinoma) and revealed the chemical structure ofgastrins (16, 17). The predominant form of gastrin in the antral mucosa and thecirculating blood is 17-amino acid gastrin ("little gastrin") and 34-amino acidpeptide ("big gastrin") with identical C-terminal sequence including Trp-Met-Asp-
72
ECL-cell
G-cell
Meal Enteric neurones
Parietal cell
HCl
Gastrin
Acetylcholine
H2
CCK2M3
Histamine
H2
Atropine
Atropine
Anacida
H2-blockers
Proton pumpinhibitors
Fig. 1. Physiological stimulation of gastric acid secretion by meal involves the release of gastrinfrom the G-cells and the release of acetylcholine from the gastric enteric neurons. Both gastrin andacetylcholine act via specific receptors on the mucosal ECL-cells to release of histamine that finallystimulates the parietal cells via activation of their H2-receptors. Blocking of receptors for gastrin(CCK2), acetylcholine (M3) or histamine inhibits gastric acid secretion. The most potent inhibitorsinclude histamine H2-receptors blockers and proton pump inhibitors, while antacids neutralize onlythe secreted acid into the gastric lumen. (Modlin I. et. al., 1998)

Phe-NH2, that by itself has similar acid stimulatory activity to the whole gastrinmolecule. In the beginning of the 1970's, Yalow and Berson (18,19) detected otherform of gastrins composed of larger molecule and naming it, "big big gastrin". Inthe case of gastrinoma, hypersecretion of gastrin results in a very potent andprolong stimulation of gastric acid secretion (Zollinger-Ellison syndrome). Therole of gastric secretory tests in this syndrome will be described later.
Intestinal phase of gastric secretion
When a meal reaches the proximal part of the small intestine, the last phase ofgastric secretion occurs - the intestinal phase. In the 1940's, Gregory and Ivy (20)proved the humoral nature of this phase. More recently, a hormone called'enterooxyntin' has been held responsible for this intestinal phase but the role ofgastrin released from duodenum cannot be excluded (21).
Sokolov, in 1904 (22), showed that the presence of acid in duodenum hasinhibitory influence on gastric secretion. This phenomenon was further investigatedby Konturek and Grossman (23) in 1965. They found that the upper duodenum isinvolved in the inhibition of gastric secretion, and found that the excision ofconsecutive parts of duodenum leads to a gradual increase in acid production by thestomach. A total excision of the duodenum completely abolished the inhibitoryeffect of acid in the intestines on gastric secretion. Subsequently, in 1971, Konturekand Johnson (24) explained this mechanism by inhibitory reflexes between theduodenum and the stomach (intramural and vago-vagal duodenogastric reflexes).H. pylori infection was reported to disturb the autoregulation of gastric acidsecretion, and this has been explained by the decrease in the number and thesecretory deficiency of the D-cells in the antral and duodenal mucosa whichcontrols the release of gastrin from G-cells (11, 12). There is no particular testdetecting the disturbance of gastric autoregulation due to H. pylori infection exceptthe finding of the enhanced plasma level of gastrin in infected patients (11).
Indications for gastric secretory testing
In the 1970s the usefulness of various secretory tests in detecting gastric acid-pepsin disorders was widely discussed and their application in the diagnosis ofsecretory alterations, especially in hyperchlorhydria in peptic ulcerations andgastrinoma (Zollinger-Ellison syndrome) was considered (Fig. 2). With wider useof upper endoscopy and the gastric pH-metry, the usefulness of gastric secretorytests markedly declined.
Diseases with gastric hypersecretion
An increase of gastric hydrochloric acid secretion in patients with dyspepsiaseems to be the most obvious indication to perform gastric secretory testing as adiagnostic procedure. The first ailment considered in this spectrum was duodenalulcer disease. There was an observed increment of gastric acid production related
73

to duodenal ulceration, accompanied by hypergastrinemia, indicating that thenormal control of gastrin release, by enhanced luminal acid concentration, isdisordered. Elevation of gastric acid content in the stomach is, however, notpathognomonic, because in some cases of duodenal ulcer disease, acidconcentration remained within normal limits (25, 26). The reason ofhypergastrinemia, accompanying peptic ulcerations was revealed in the 1990s(27), when the role of H. pylori in the antral regulatory processes was established.
The main area of usefulness for gastric secretory tests remains for detectinggastrinoma. The excessive gastric acid secretion in this syndrome was recognizedbefore and it was found to be accompanied by very high levels of plasma gastrin.An elevated level of basal acid output, near the maximal acid output, appeared tobe symptomatic for Zollinger-Ellison syndrome (Fig. 3). This property could bedetected by gastric secretory tests.
Diseases with gastric hyposecretion
A decrease of gastric acid secretion can also be easily revealed using secretorytests in certain diseases such as pernicious anemia, gastric atrophy or gastriccancer. In the 1970's, gastric secretory tests were useful in the study of thesecases. However, it is important to emphasize that these tests were performed forresearch purposes rather than for routine clinical practice.
Fractional test meals. The intragastric titration method
A meal is commonly known as a potent, physiological stimulant of gastricsecretion. In 1973, Fordtran and Walsh (28) designed the intragastric titrationmethod to measure the postprandial (gastric phase) of gastric acid secretion.
74
Control Gastriculcer
Duodenalulcer
Atrophicgastritis
Gastriccancer
10
20
30
40`
H+(mmol/h)
Fig. 2. Maximal acidoutput in response tohistamine in healthycontrols and patients withgastric ulcer, duodenalulcer, atrophic gastritisand gastric cancer.(Konturek S.J. et. al.,1976)

Under normal conditions, the intragastric pH gradually decreases in response to aliquid, usually peptone meal. The first step of this test was ingestion of a meal.Then small samples of gastric content were aspirated at intervals every fewminutes and the pH of the samples was determined. This procedure allowedmeasurement of intragastric pH and whenever this pH fell below pH 5.5, sodiumbicarbonate ( 0.15 mmol/L ) was added to the gastric liquid meal (usually 10%liver extract) in order to maintain a constant intragastrical pH at the original valueof pH 5.5. The amounts of sodium bicarbonate solution instilled into the stomach,corresponded to the amount of hydrochloric acid secreted by the stomach aftermeal ingestion.
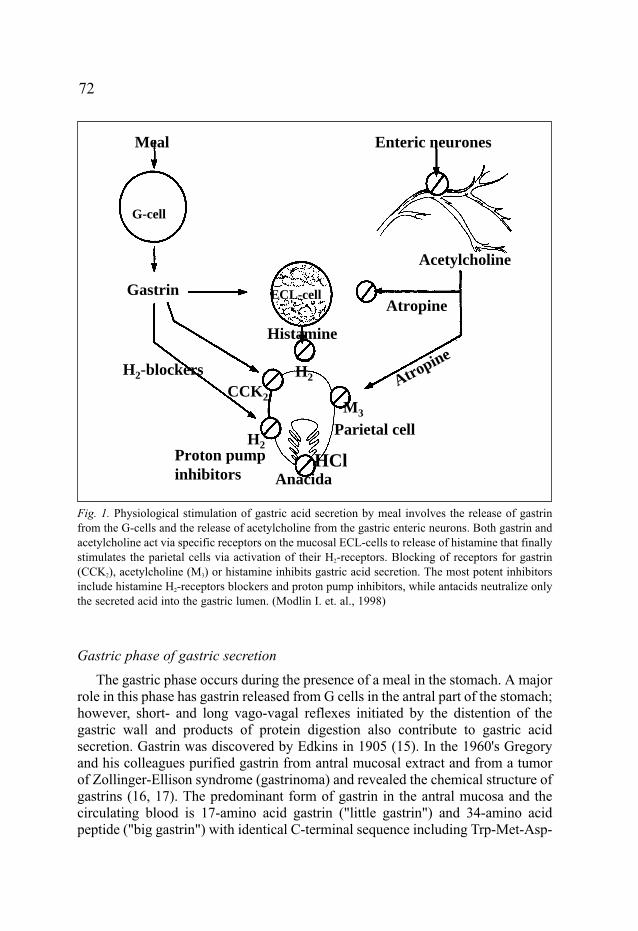
In 1974 Konturek et al. (29), at the Institute of Physiology Academy ofMedicine in Cracow, modified this method, using a barostat to maintain aconstant intragastric pressure and gastric emptying rate. The gastric acid secretionmeasured with this technique reached the value of augmented histamine orpentagastrin tests and was accompanied by a marked rise in plasma gastrin level.The peak acid secretory output obtained with liver extract meal was about twiceas high as that induced by sham-feeding but comparable to that obtained withpentagastrin or histamine. This technique was very useful in detecting thealterations in gastric acid secretion induced by the addition of gastric inhibitorssuch as H2-receptor antagonist or proton pump inhibitors (Fig. 4).
Other methods
In the 1970's, Go et al. (30) and Malagelada et al. (31) described other methodfor measuring of gastric acid secretion. This method required placement of 2tubes: one in the stomach and another in the duodenum. The basis of thistechnique differed from intragastric titration in that the pH of the liquid meal in
75
Control
GUDU
Gastrinoma
BAO MAO BAO /MAO
30
50
70
90
H+
(mm
ol/h
)
Fig. 3. Values of basal (BAO)and maximal acid output (MAO)and the ratio of BAO to MAO inhealthy controls, gastric ulcer(GU), duodenal ulcer (DU) andgastrinoma patients. (KonturekS.J. et. al., 1976)
the stomach was not maintained at its constatnt and original value. Instead, theintragastric pH was allowed to reach its natural level in response to gastric acidsecretion. A series of equations were necessary to calculate gastric acid secretion.It should be mentioned that in 1976 MacGregor et al. (32) independentlydescribed a comparable method.
Rune (33) had a different approach for measuring of meal-stimulated acidsecretion. He determined arterial pH and pCO2, at frequent intervals after a mealto calculate base excess resulting from the acid secretion into the lumen of thestomach.
Ethanol and caffeine tests
Ethanol and caffeine were previously employed as stimulators for gastric acidsecretion. However, the response of a stomach to ethanol or caffeine was muchsmaller, as compared to pentagastrin, histamine or a meal. Therefore, ethanol andcaffeine are no longer used for routine gastric secretory testing in humans (34).
76
Sham-Feeding
LEMeal
Penta-gastrin
Histamine
Fig. 4. Ranitidine or cimetidine (upper panel) or omeprazole (lower panel) on gastric acid response to S-F, meal, P-gastrin or histamine
ControlCimet.Ranit.
ControlOmeprazol
Fig. 4. Effects of therapeuticdose of cimetidine, ranitidineor omeprazole used in lower(20 mg) or higher dose (40mg) on gastric acid secretionin duodenal ulcer patientsfollowing sham-feeding, liverextract meal, pentagastrin orhistamine.(Konturek S.J. et.al., 1976)
AUGMENTED (MAXIMAL) GASTRIC SECRETORY TESTS
Histamine or Histalog secretory tests
Since the discovery of histamine as gastric secretagogue by L. Popielski, it iswell known as potent stimulant of parietal cells to produce hydrochloric acid. Itacts entirely through the activation of H2 receptors on these cells. However,histamine also stimulates H1 receptors, producing severe side effects, such ashypotension, dizziness, nausea, palpitations, and headache. To avoid the abovementioned side-effects, antihistamine drugs (e.g. promethasine), which block H1
receptors, should be administered prior to examination. A patient's position playsan important role during testing, because of the risk of hypotension. The mostappropriate position is a recumbent one or, at least, a sitting position during thehistamine secretory test (35).
Following its description by Kowalewski in 1949 and then by Kay in 1953, theaugmented histamine test was introduced into routine clinical practice. Histaminewas administered in a dose of 40 µg/kg in this test. Previously histamine wasapplied in lower doses but this did not produce maximal acid output. Afterintravenous or subcutaneous administration of dose 40 µg/kg/h, histamine can
77
��
��������
��
������
���µ������ ���� ��
����µ���������������� �
� ���� �������� �
�� ����������� � �� ���������
�
��
����
��
��
��
��
��������������� �����!��"������� ���� �����#� ��������� �
$���%� �� ����
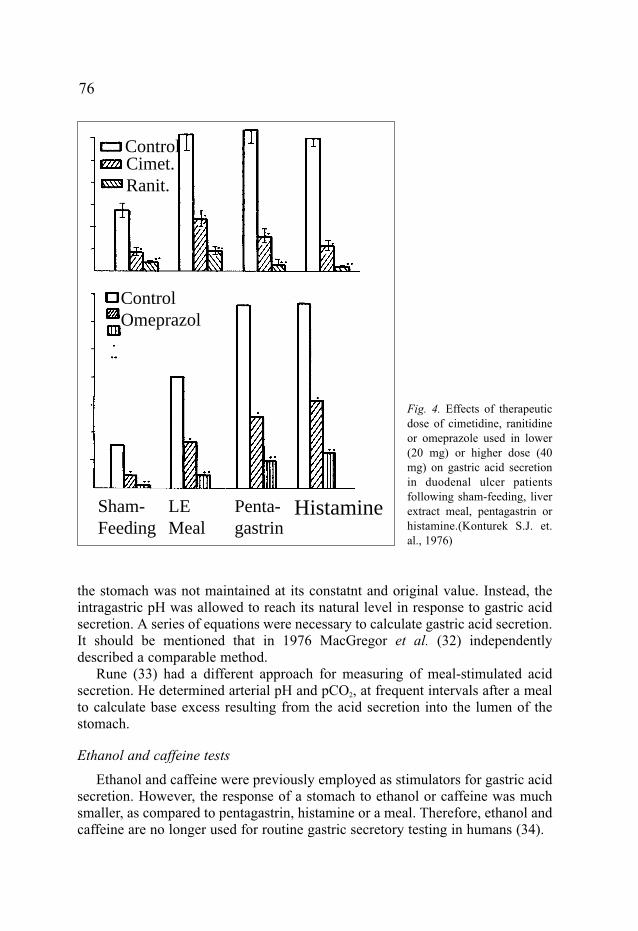
Fig. 5. Effects of graded doses of histamine (10-40 µg/kg) or pentagastrin (0.24 - 6 µg/kg) on gastricacid secretion in patients with duodenal ulcers. (Konturek S.J. et. al., 1976)
induce acid secretion reaching maximal acid output. This dose was established asa standard in further investigations. After histamine administration the peaksecretory effect usually occurred during the first postinjection hour. Nevertheless,because of danger for patients, caused by side effects, a derivate of histamine,betazole, replaced native histamine in secretory stimulation.
Betazole, an analogue of histamine, is better known as Histalog. It wasadministered in higher doses than histamine, i.e. 2 mg/kg (36). It produced thepeak effect later than histamine, i.e. during 2nd hour. It was reasonable to replacehistamine by betazole in gastric secretory testing due to lower rate of side effectsof betazole (37). Therefore, in this case, administration of the antihistaminicdrugs is not necessary. However, when at the end of the 1960's, pentagastrinbegan to be used in gastric secretory tests, the histamine and its analogue werequickly replaced by pentagastrin for gastric secretory testing (38). The reason forthis situation was a markedly lower intensity of side effects, a faster productionof peak secretory response, and a lower dose required to produce a maximalsecretory response.
Pentagastrin secretory test
As mentioned above, in 1967, pentagastrin was approved as a stimulant ofgastric acid secretion instead of histamine. Pentagastrin appeared to be safer forpatients and the secretory response to pentagastrin was found to be identical tothat of gastrin and histamine.
It is commonly known, that gastrin stimulates specific receptors on ECL cellsto release histamine, which then acts on H2-receptors of parietal cells to stimulateacid secretion. There may be some gastrin receptors on the parietal cells but themajor pathway of the stimulation of gastric acid is through the release ofhistamine from ECL cells and activation of H2-receptors of parietal cells (12).With isolation and purification of gastrin by Gregory, it was conceivable to usenative gastrin in order to stimulate gastric acid secretion. However, native gastrinis a 17 or 34 amino acid containing peptide, which is rather expensive. In 1976,when gastrin was already synthesized, Walsh et al. (39) used it as a secretagoguein gastric secretory testing in humans, however, its production was too expensiveto be employed in routine clinical investigations.
Because of these problems, it was necessary to find an analogue of gastrinwhich would possess the same biological activity as native gastrin. The mosteffective was found to be a 5-amino acid peptide containing the C-terminalportion of the gastrin molecule which produced a maximal response of gastricacid secretion. Therefore, it was enough to synthesize a peptide composed ofthese 5 C-terminal amino acid sequence of natural gastrin in order to obtain apotent stimulation of parietal cells. Due to the structure of this substance, it wascalled pentagastrin (38, 40). In 1966, the usefulness of pentagastrin andtetragastrin was thoroughly examined as gastric secretagogues in our institute in
78
Cracow (41). It was established that tetragastrin had the same physiologicalproperties as pentagastrin and it also produced minimal side effects (42).
Pentagastrin has a property of inducing of maximal gastric secretory responsesimilar to that evoked by histamine, betazole, or native gastrin. Therefore, it canbe used in testing maximal gastric acid secretion. Pentagastrin was administeredeither subcutaneously or intravenously as a single bolus or as continuous infusionof graded doses. A range of effective doses was from 0.24 to 6 µg/kg (38, 40). Itwas established that the standard dose in intravenous infusion of pentagastrinproducing maximal gastric acid secretion was about 1.2 µg/kg/h (Fig. 5) (12, 41).After pentagastrin application, the peak secretory effect took place within 45 to60 minutes (43). To summarize we can conclude, that pentagastrin hasadvantages, as compared to histamine and its analogue, i.e. smaller side effectsand an earlier stimulatory peak response. However, after pentagastrinadministration rarely side effects can also be observed, such as nausea,diaphoresis, hypotension, even syncope. It is important to emphasize thathypotension after pentagastrin application rarely occurs as compared after ahistamine injection (44). Pentagastrin-dependent side effects increase with anelevated dose of this peptide and they often take place after rapid intravenousinjection of pentagastrin.
79
Lunch
pH
10
9
8
7
6
5
4
3
2
109 11 13 15 17 19 21 23 01 03 05 07
Time (h)
24 h record of intragastric pH before and after administration of omeprazole
Dinner
Control
Omeprazole
Breakfast
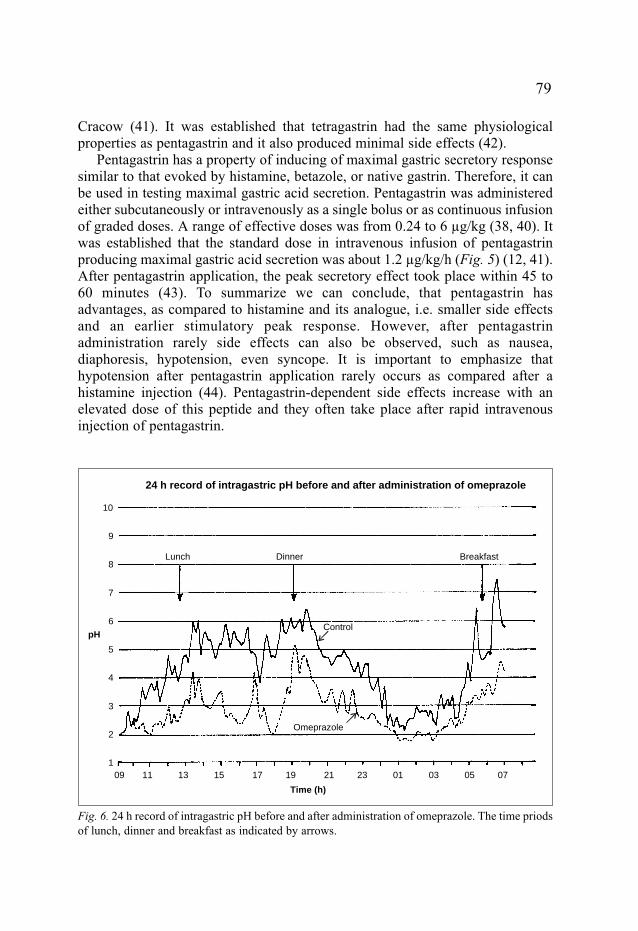
Fig. 6. 24 h record of intragastric pH before and after administration of omeprazole. The time priodsof lunch, dinner and breakfast as indicated by arrows.

The pentagastrin-stimulated gastric secretory test maintains its clinical valueuntil present time. It is useful, as an additional examination, in diagnosticprocedures, in the case of diseases with hypochlorhydria or hyperchlorhydria.
At present time
Gastric analysis with fractional test meals, histamine or pentagastrinadministration were performed predominantly from 1960s to 1980s. They were,at that time, experimental methods, which were tested in order to assess theirusefulness in the diagnostic regimen related to gastric diseases. However,improvement in gastroscopy, led to a decrease in the practical value of gastricsecretory tests in clinical circumstances. Introduction of novel techniques, such as12 or 24 h intragastric pH-metry, gave the possibility of accurately measuringgastric circadian pH changes (Fig. 6). It appears to be undoubtedly better tomeasure acidity in the stomach under natural conditions than by the classic gastricsecretory tests. The pH-metry allows the determination of intragastric acidityunder normal daily and nocturnal conditions that is in the interdigestive periods,such as, after food intake, and at night when in some patients, despite gastricinhibition, periods of acid production occurs, resulting in nocturnal pain andgastroesophageal reflux.
CONCLUDING REMARKS
1. Gastric acid secretory testing serves to determine the secretory capacity of thegastric glands to produce acid that depends upon the number of active parietalcells;
2. Most popular secretory tests are induced by histamine and pentagastrin, whichare used to determine the gastric secretory activity in various gastric diseases,especially in peptic ulcer and gastrinoma;
3. At present these secretory tests are replaced by 12 or 24 h gastric pH-metrywhich allows for the examination of the gastric secretion under naturalconditions without any risk of side effects which have been described both intests with histamine or pentagastrin.
REFERENCES
1. Beaumont W. Experiments and observations on the gastric juice and physiology of digestion.New York, Dover Publications, Inc. 1959.
2. Ewald C, Boas J. Aspects of physiology and secretion. Archiv Path Anat Physiol 1885; 101: 325.
3. Ehrenreich M. Examination of digestion by gastric tube. Z Klin Med 1912; 75: 231.4. Rehfuss ME. Diseases of the stomach. Philadelphia, WB Saunders Co. 1927.5. Polland WS, Bloomfield AL. Normal standards of gastric functions. J Clin Invest 1931; 9: 651.
80
6. Ihre BJE. Human gastric secretion. Acta Med Scand 1938; 95 (suppl.): 1.7. Kay AW. Effect of large doses of histamine on gastric secretion of HCl. An augmented
histamine test. Brit Med J 1953; 2: 77-80.8. Card WI, Marks IN. The relationship between the acid output of the stomach following
"maximal" histamine stimulation and parietal cell mass. Clin Sci 1960; 19: 147-163.9. Hollander F, Penner A. History and development of gastric analysis procedure. Amer J Dig Dis
1993; 7: 739-786.10. Henning N, Norjsoth L: Observation of gastric secretion. Deutsche Arch Klin Med 1932;
172: 558.11. Konturek PCh, Konturek SJ, Konturek JW. Gastric secretion and the pathogenesis of peptic
ulcer in Helicobacter pylori infection. J Physiol Pharmacol 1996; 47: 1: 5-19.12. Konturek SJ. Physiology of digestive system. PZWL, Warsaw 1976.13. Konturek SJ. Mechanisms of gastric glands secretion. Acta Physiol Pol 1976; 12: 63.14. Szafran H, Popiela T, Szafran Z. The effect of 2-deoxy-D-glucose and insulin stimulation on the
secretion of gastric lipase. Scand J Gastroenterol 1971; 6: 55-58.15. Edkins JS. On the chemical mechanism of gastric secretion. Proc Roy Soc London 1905;
76: 376.16. Gregory RA, Tracy HJ. Constitution and properties of two gastrins extracted from hog antral
mucosa. Gut 1964; 46: 103-114. 17. Gregory RA, Tracy HJ: A review of recent progress in the chemistry of gastrin. Amer J Dig Dis
1966; 11: 97-102.18. Yalow RS, Berson SA And now "big", "big" gastrin. Biochim Res Commun 1972; 48: 391-395.19. Yalow RS, Wu N. Additional studies on the nature of big big gastrin. Gastroenterology 1973;
65: 19-27.20. Gregory RA, Ivy AC. The hormonal stimulation of gastric secretion. Quart J Physiol 1941;
31:111.21. Grossman MI: Candidate hormons of the gut. I. Introduction. Gastroenterology 1974; 67:
730-731.22. Sokolov AP. Thesis. St Petersburg 1904.23. Konturek SJ, Grossman MI. Localization of the mechanism for inhibition of gastric secretion
by acid in the intestine. Gastroenterology 1965; 49: 74-78.24. Konturek SJ, Johnson LR. Evidence for an enterogastric reflex for the inhibition of acid
secretion. Gastroenterology 1971; 61: 667-674.25. Wormsley KG, Grossman MI. Maximal Histalog test in control subjects and patients with peptic
ulcer. Gut 1965; 6: 427-435.26. Isenberg JI, Grossman MI, Maxwell V et al: Increased sensitivity to stimulation of acid
secretion by pentagastrin in duodenal ulcer. J Clin Invest 1975; 55: 330-337.27. Konturek JW. Cholecystokinin in the control of gastric acid and plasma gastrin and somatostatin
secretion in healthy subjects and duodenal ulcer patients before and after eradication ofHelicobacter pylori. J Physiol Pharmacol 1994; 45 (Suppl. 1): 4-59.
28. Fordtran JS, Walsh JH. Gastric acid secretion rate and buffer content of the stomach after eating.Results in normal subjects and in patients with duodenal ulcer. J Clin Invest 1973; 52: 645-657.
29. Konturek SJ, Biernat J, Oleksy J. Serum gastrin and gastric acid responses to meals at variouspH levels in man. Gut 1974; 15: 526-530.
30. Go VL, Hoffman AF, Summerskill WH. Simultaneous measurement of total pancreatic, biliaryand gatric outputs in man using a perfusion technique. Gastroenterology 1970; 58: 321-328.
31. Malagelada JR, Longstreth GF, Summerskill WHJ et al. Measurement of gastric functionsduring digestion of ordinary solid meals in man. Gastroenterology 1976; 70: 203-210.
81

32. MacGregor IL, Deveney C, Way LW et al. The effect of acute hyperglycemia on meal-stimulated gatric, biliary and pancreatic secretion and serum gastrin. Gastroenterology 1976,70, 197-202.
33. Rune SJ. Comparison of the rates of gastric acid secretion in man after ingestion of food andafter maximal stimulation with histamine. Gut 1966; 7: 344-350.
34. Cohen MM, Debas HT, Holubitsky IB et al. Caffeine and pentagastrin stimulation of humangastric secretion. Gastroenterology 1971; 61: 440-444.
35. Hector RM. Improved technique of gastric aspiration. Lancet 1968; 1: 15-16.36. Laudano OM, Roncoroni EL. Determination of the dose of Histalog that provokes maximal
secretory response. Gastroenterology 1965; 49: 372-374.37. Goldenberg J, Cummins AJ, Gompertz MJ. A clinical evaluation of the maximal Histalog test.
Amer J Dig Dis 1967; 12: 468-474.38. Multicentre Pilot Study. Pentagastrin as a stimulant of maximal gastric acid response in man.
Lancet 1967; 1: 291.39. Walsh JH, Isenberg JI, Ansfield J et al. Clearance and acid-stimulating action of human big and
little gastrins in duodenal ulcer subjects. J Clin Invest 1976; 57, 1125-1131.40. Johnston D, Jepson K. Use of pentagastrin in a test of gastric acid secretion. Lancet 1967; 2:
585-588.41. Konturek SJ, Król W. The influence of gastrin-related peptides on HCl secretion in man and in
cats with gastric fistulas and Heidenhain pouches. Gastroenterologia 1966; 106: 281-294.42. Köster KH, Rödbro P, Petersen HJ. Comparative effects of tetragastrin and histamine on acid
and intrinsic factor secretion in man. Scand J Gastroenterol 1968; 3: 23-35.43. Isenberg IJ, Brooks AM, Grossman MI. Pentagastrin vs betazole as stimulant of gastric
secretion. JAMA 1968; 206: 2897-2898.44. Prugh MF, Schorr BA, Vlahevic ZR et al. Intravenous pentagastrin as a partial agonist of gastric
secretion in man. Evidence in favor of the existence of hormonal inhibitory sites.Gastroenterology 1975; 68: 45-49.
R e c e i v e d : November 15, 2003A c c e p t e d : December 15, 2003
Author's address: S. Kwiecien, Department of Physiology, Jagiellonian University MedicalCollege, 16 Grzegorzecka St., 31-531 Cracow, Poland. Phone: (12) 421 1006; fax: (12) 4211578
82