gastric cancer physio
TRANSCRIPT

Gastric Cancer
By: Saeid Afshar
(Ph.D. student of molecular medicine )
November 2014
Hamadan university of medical science
Molecular medicine and genetic department

introduction
• Gastric cancer has been described as
early as 3000 BC in hieroglyphic
inscriptions and papyri manuscripts from
ancient Egypt. The first major statistical
analysis of cancer incidence and mortality
(using data gathered in Verona, Italy from
1760 to 1839) showed that gastric cancer
was the most common and lethal cancer.
http://www.uptodate.com/

INCIDENCE
• Gastric cancer is one of the most common
cancers worldwide
• Gastric cancer used to be the leading
cause of cancer deaths in the world until
the 1980s when it was overtaken by lung
cancer .
http://www.uptodate.com/

INCIDENCE
• The worldwide incidence of gastric cancer
has declined rapidly over the recent few
decades . Part of the decline may be
due to the recognition of certain risk
factors such as H. pylori and other
dietary and environmental risks.
http://www.uptodate.com/

GEOGRAPHICAL VARIATION
• The incidence of gastric cancer varies with
different geographic regions.
• Rates are highest in Eastern Asia, Eastern
Europe, and South America, while the
lowest rates are in North America and
parts of Africa .
http://www.uptodate.com/

• Over 70 percent of gastric cancers occur
in developing countries .
• Gastric cancer is more common in men
than in women, in both developed and
developing countries.
• There are also substantial differences in
incidence among different ethnic groups
within the same region .
http://www.uptodate.com/

GEOGRAPHICAL VARIATION
Geographical Variation in Gastric Cancer Incidence
Parkin DM. International variation. Oncogene 2004; 23: 6329-6340

Pathology
• The risk of gastric cancer is greater among
lower socioeconomic classes. Migrants
from high- to low-incidence nations
maintain their susceptibility to gastric
cancer, while the risk for their offspring
approximates that of the new homeland.
(Dan L. Longo,2012)

• These findings suggest that an
environmental exposure, probably
beginning early in life, is related to the
development of gastric cancer, with dietary
carcinogens considered the most likely
factor(s).
(Dan L. Longo,2012)

Pathology
• About 85% of stomach cancers are
adenocarcinomas, with 15% due to
lymphomas and gastrointestinal stromal
tumors (GIST) and leiomyosarcomas.
•
gastrointestinal stromal tumors Leiomyosarcoma
(Dan L. Longo,2012)

Pathology
• Gastric adenocarcinomas may be
subdivided into two categories: a diffuse
type , in which cell cohesion is absent, so
that individual cells infiltrate and thicken
the stomach wall without forming a
discrete mass; and an intestinal type ,
characterized by cohesive neoplastic cells
that form glandlike tubular structures.
(Dan L. Longo,2012)

Pathology
• Diffuse cancers have defective intercellular
adhesion, mainly as a consequence of loss of
expression of E-cadherin.
• Intestinal-type lesions are frequently
ulcerative, more commonly appear in the
antrum and lesser curvature of the stomach,
and are often preceded by a prolonged
precancerous process, often initiated by
Helicobacter pylori infection.
(Dan L. Longo,2012)

Pathology
• While the incidence of diffuse carcinomas
is similar in most populations, the intestinal
type tends to predominate in the high-risk
geographic regions and is less likely to be
found in areas where the frequency of
gastric cancer is declining. Thus, different
• etiologic factor(s) are likely involved in
these two subtypes.
(Dan L. Longo,2012)

Pathology
• In the United States
• , ~30% of gastric cancers originate in the distal stomach,
• ~20% arise in the midportion of the stomach,
• and ~37% originate in the proximal third of the stomach.
• The remaining 13%involve the entire stomach.
(Dan L. Longo,2012)

Pathology
A: the Endoscopic image of an ulcerating adenocarcinoma. B. Ulcerating
adenocarcinoma, pictorial representation. Picture courtesy: John Hopkins Medicine-
Gastroenterology and Hepatology department. ‘An introduction to Gastric cancer’, 2012.

Etiology
• The long-term ingestion of highconcentrations of nitrates in dried, smoked,and salted foods appears to be associatedwith a higher risk. The nitrates are thought tobe converted to carcinogenic nitrites bybacteria Such bacteria may be introducedexogenously through the ingestion of partiallydecayed foods, which are consumed inabundance worldwide by the lowersocioeconomic classes.
(Dan L. Longo,2012)

Etiology
• Bacteria such as H. pylori may also contribute to this effect by causing chronic gastritis, loss of gastric acidity, and bacterial growth in the stomach.
• Loss of acidity may occur when acid-producing cells of the gastric antrum have been removed surgically to control benign peptic ulcer disease or when achlorhydria, atrophic gastritis, and even pernicious anemia develop in the elderly.
(Dan L. Longo,2012)

Etiology
• H. pylori has not been associated with the
diffuse, more proximal form of gastric
carcinoma .
• Individuals with blood group A have a
higher incidence of gastric cancer than
persons with blood group O; this
observation may be related to differences
in the mucous secretion, leading to altered
mucosal protection from carcinogens.(Dan L. Longo,2012)

Etiology
• A germ-line mutation in the E-cadherin gene
( CDH1 ), inherited in an autosomal
dominant pattern and coding for a cell
adhesion protein, has been linked to a high
incidence of occult diffuse-type gastric
cancers in young asymptomatic carriers.
(Dan L. Longo,2012)

Etiology
• In keeping with the stepwise model of
carcinogenesis, K-ras mutations appear to be
early events in intestinal-type gastric cancer.
• C-met expression is amplified in about 1 in 5
cases and correlates with advanced stage.
(Dan L. Longo,2012)

Etiology
• About half of intestinal-type tumors have
mutations in tumor suppressor genes such
as TP53
• Epigenetic changes (especially increased
methylation) has been correlated with
higher risk of invasive disease.
(Dan L. Longo,2012)A genetic model for colorectal tumorigenesis.


Clinical features
• Gastric cancers, when superficial and surgically curable, usually produce no symptoms. As the tumor becomes more extensive, patients may complain of an insidious upper abdominal discomfort varying in intensity from a vague, postprandial fullness to a severe, steady pain.
• Anorexia, often with slight nausea, is very common but is not the usual presenting complaint.
(Dan L. Longo,2012)

Clinical features
• Weight loss may eventually be observed,
and nausea and vomiting are particularly
prominent with tumors of the pylorus
• Dysphagia and early satiety may be the
major symptoms caused by diffuse lesions
originating in the cardia. (Dan L. Longo,2012)

Risk Factors for Gastric
Cancer• Definite—surveillance suggested
• Familial adenomatous polyposis
• Gastric adenomas
• Gastric biopsy revealing high-grade dysplasia
• Definite
• Chronic atrophic gastritis
• Gastric metaplasia or biopsy
• Helicobacter pylori infection
• Hereditary nonpolyposis colorectal cancer
Downloaded from the American Family Physician Web site at www.aafp.org/afp. Copyright© 2004 American Academy of Family Physicians. For the private,
noncommercial use of one individual user of the Web site. All other rights reserved. Contact [email protected] for copyright questions and/or

Risk Factors for Gastric
Cancer• Possible
• Excess alcohol ingestion
• Hamartomas
• High intake of salted, pickled, or smoked foods
• Low intake of fruits and vegetables
• Ménétrier’s disease
• Peutz-Jeghers syndrome
• Tobacco smoking
• Probable
• History of subtotal gastrectomy (> 20 years)
• Pernicious anemia
• Tobacco smoking (adenocarcinoma of cardia)
Downloaded from the American Family Physician Web site at www.aafp.org/afp. Copyright© 2004 American Academy of Family Physicians. For the private,
noncommercial use of one individual user of the Web site. All other rights reserved. Contact [email protected] for copyright questions and/or

Diagnosis
• The initial diagnosis of gastric carcinoma
often is delayed because up to 80 percent
of patients are asymptomatic during the
early stages of stomach cancer.
• Unfortunately, in the United States, most
cases of gastric cancer are discovered
only after local invasion has advanced.
Downloaded from the American Family Physician Web site at www.aafp.org/afp. Copyright© 2004 American Academy of Family Physicians. For the private,
noncommercial use of one individual user of the Web site. All other rights reserved. Contact [email protected] for copyright questions and/or

Diagnostic
• A double-contrast radiographic (barium)
examination is the simplest diagnostic
procedure for the evaluation of a patient
with epigastric complaints.
Courtesy of Norman Joffe, MD.Graphic 61767 Version 5.0
(Dan L. Longo,2012)

Diagnostic
• Endoscopy provides the most specific and
sensitive means of diagnosis of gastric
cancers. Gastrointestinal endoscopy
allows the physician to visualize and
biopsy the mucosa of the esophagus,
stomach, duodenum, and most of the
jejunum.
http://www.hopkinsmedicine.org/kimmel_cancer_center/types_cancer/stomach_canc
er.html
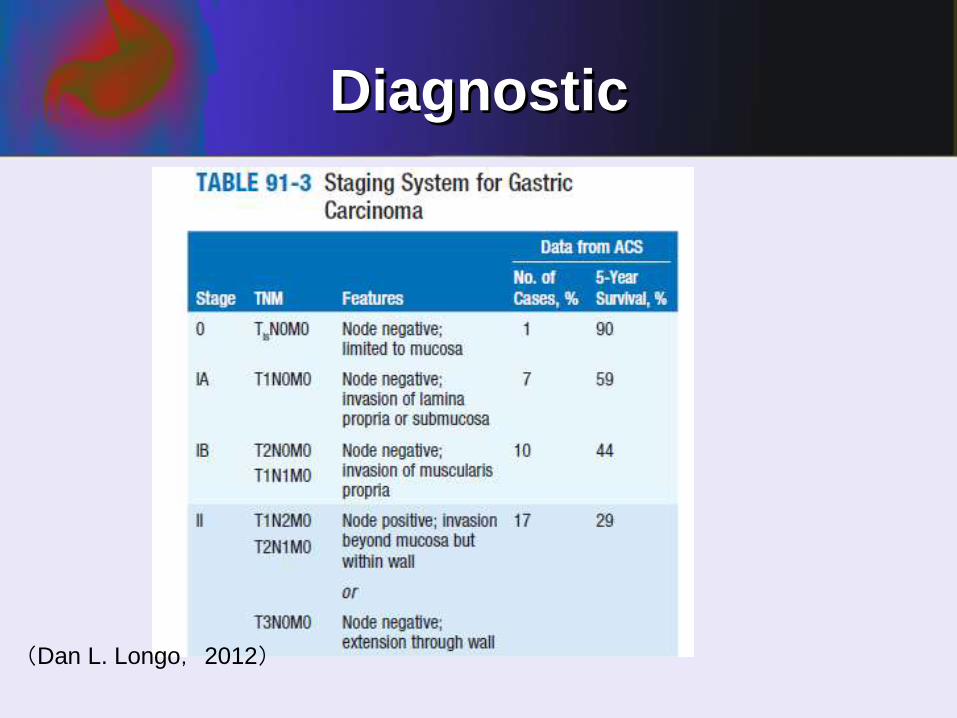
Diagnostic
(Dan L. Longo,2012)

Diagnostic
(Dan L. Longo,2012)

TREATMENT
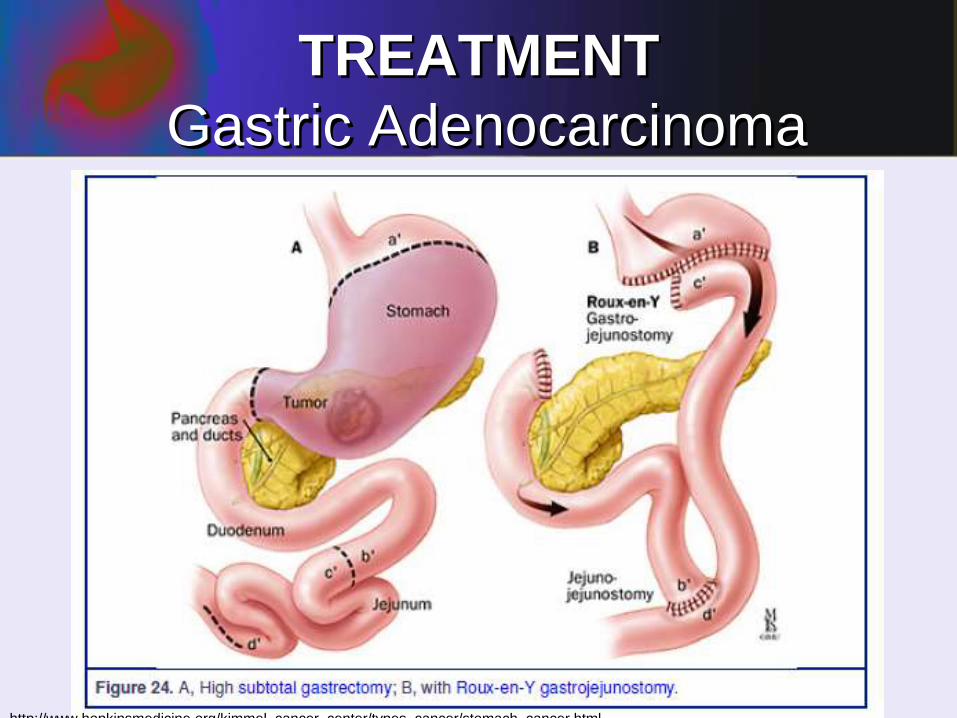
Gastric Adenocarcinoma• Complete surgical removal of the tumor
with resection of adjacent lymph nodes
offers the only chance for cure. However,
this is possible in less than a third of
patients. A subtotal gastrectomy is the
treatment of choice for patients with distal
carcinomas, while total or near-total
gastrectomies are required for more
proximal tumors.(Dan L. Longo,2012)

TREATMENT
Gastric Adenocarcinoma
http://www.hopkinsmedicine.org/kimmel_cancer_center/types_cancer/stomach_cancer.html
TREATMENT
Gastric Adenocarcinoma
http://www.hopkinsmedicine.org/kimmel_cancer_center/types_cancer/stomach_cancer.html

TREATMENT
Gastric Adenocarcinoma
http://www.hopkinsmedicine.org/kimmel_cancer_center/types_cancer/stomach_canc
er.html

http://www.hopkinsmedicine.org/kimmel_cancer_center/types_cancer/stomach_canc
er.html

TREATMENT
Gastric Adenocarcinoma
• Gastric adenocarcinoma is a relatively
radioresistant tumor, and adequate control
of the primary tumor requires doses of
external beam irradiation that exceed the
tolerance of surrounding structures, such
as bowel mucosa and spinal cord.
(Dan L. Longo,2012)

TREATMENT
Gastric Adenocarcinoma• As a result, the major role of radiation
therapy in patients has been palliation of
pain. Radiation therapy alone after a
complete resection does not prolong
survival. In the setting of surgically
unresectable disease limited to the
epigastrium, patients treated with 3500–
4000 cGy did not live longer than similar
patients not receiving radiotherapy;(Dan L. Longo,2012)
TREATMENT
Gastric Adenocarcinoma• however, survival was prolonged slightly
when 5-fluorouracil (5-FU) plus leucovorin
was given in combination with radiation
therapy (3-year survival 50% vs 41% for
radiation therapy alone). In this clinical
setting, the 5-FU may be functioning as a
radiosensitizer.
(Dan L. Longo,2012)

TREATMENT
Gastric Adenocarcinoma• The administration of combinations of
cytotoxic drugs to patients with advanced
gastric carcinoma has been associated with
partial responses in 30–50% of cases;
responders appear to benefit from treatment.
• Such drug combinations have generally
included cisplatin combined with epirubicin or
docetaxel and infusional 5-FU, or with
irinotecan.
(Dan L. Longo,2012)

TREATMENT
Gastric Adenocarcinoma• Despite this encouraging response rate,
complete remissions are uncommon, the partial responses are transient, and the overall influence of multidrug therapy on survival has been unclear.
• However, combination chemotherapy administered before and after surgery as well as postoperative chemotherapy combined with radiation therapy reduces the recurrence rate and prolongs survival.
(Dan L. Longo,2012)

metastasis
• When cancer spreads to another part of the body, it is called metastasis. Cancer cells break away from where they began (the primary tumor) and travel through the lymph system or blood.
• Lymph system. The cancer gets into the lymph system, travels through the lymph vessels, and forms a tumor (metastatic tumor) in another part of the body.
• Blood. The cancer gets into the blood, travels through the blood vessels, and forms a tumor (metastatic tumor) in another part of the body.
• The metastatic tumor is the same type of cancer as the primary tumor. For example, if thyroid cancer spreads to the lung, the cancer cells in the lung are actually thyroid cancer cells. The disease is metastatic thyroid cancer, not lung cancer.
http://www.cancer.gov/cancertopics/pdq/treatment/unusual-cancers-childhood/patient/

Thanks for your attention
