gastrointestinal bleeding g muthukumarasamy specialist registrar in general surgery
TRANSCRIPT

Gastrointestinal Bleeding
G MuthukumarasamySpecialist Registrar in General Surgery

Anatomy and Physiology

Oesophagus

Stomach

Duodenum

History taking
• Complaints Haematemesis Malena Haemotochezia Pain Light-headedness, syncope, dyspnoea, altered mental status (blood loss symptoms) occult blood loss (anaemia)

Malena and Coffee ground vomiting

Clinical Indicator Probability of Upper GI Source
Probability of Lower GI Source
Hematemesis Almost certain Rare
Melena Probable Possible
Hematochezia Possible Probable
Blood-streaked stool Rare Almost certain
Occult blood in stool Possible Possible
Contd.,
• H/o Drug intake – Aspirin, Anticoagulants (warfarin), NSAIDS, Clopidogrel, steroids
• H/o Alcohol intake, smoking• H/o Weight loss
Past History :Chronic liver disease, peptic ulcer, bleedingDisorders

Examination
• General ExaminationMental statusEyes – Pallor, JaundiceLiver disease – caput medusae, spider angiomas,
ascites, palmar erythema, flapBleeding disorders – Petechia, echymosis
Vital Signs – BP, HR, SaO2, RR, T⁰, CRF Urine output

Jaundice and Anaemia

Liver disease

Petechiae/Echymosis

Examination – contd.,
• Abdominal Inspection – Shape, symmetry, Dilated Veins, signs
of liver failure Palpation – tenderness, Splenomegaly, hepatomegaly Percussion – Shifting dullness, Fluid thrill Auscultation – BS, Bruit Rectal Examination – Fresh blood, MalenaCVS, RS, Neurological Examination

Investigation
• FBC, Coagulation profile, U&ES, LFT, CRP, Calcium• Type and Crossmatch Blood• ECG• CXR• OGD• Angiogram CT or Catheter• Nasogastric lavage• USS/CT (to assess liver disease)• Tc-99m-labeled erythrocyte scans (rarely)

Management
• RESUSCITATION – ABCDE• Fluid and BLOOD Replacement• Medical Management - PPIs, Vasoactive agents,
B-blocker, ISMN (to prevent re-bleeding)• Endoscopic management – Adrenaline,
coagulation, banding, clipping• Interventional Angiography – coiling, TIPS• Surgical Management

Haemorrhagic ShockEstimated Fluid and Blood Losses in Shock
Class 1 Class 2 Class 3 Class 4
Blood Loss, mL
Up to 750 750-1500 1500-2000 >2000
Blood Loss,% blood volume
Up to 15% 15-30% 30-40% >40%
Pulse Rate, bpm
<100 >100 >120 >140
Blood Pressure
Normal Normal Decreased Decreased
Respiratory Rate
Normal or Increased
Decreased Decreased Decreased
Urine Output, mL/ h
14-20 20-30 30-40 >35
CNS/ Mental Status
Slightly anxious
Mildly anxious
Anxious, confused
Confused, lethargic
Fluid Replacement, 3-for-1 rule
Crystalloid Crystalloid Crystalloid and blood
Crystalloid and blood

UpperGI Bleeding
Non variceal Upper GI bleeding 90% Variceal bleeding 10%

Causes




Esophageal Varices Bleeding esophageal varices
Oesophageal varices

Oesophagitis

Angiodysplasia

Gastric varices Mallory Weiss Tear Esophagitis
Other causes

Glasgow-Blatchford Score
Scores of 6 or more were associated with a greater than 50% risk of needing an intervention






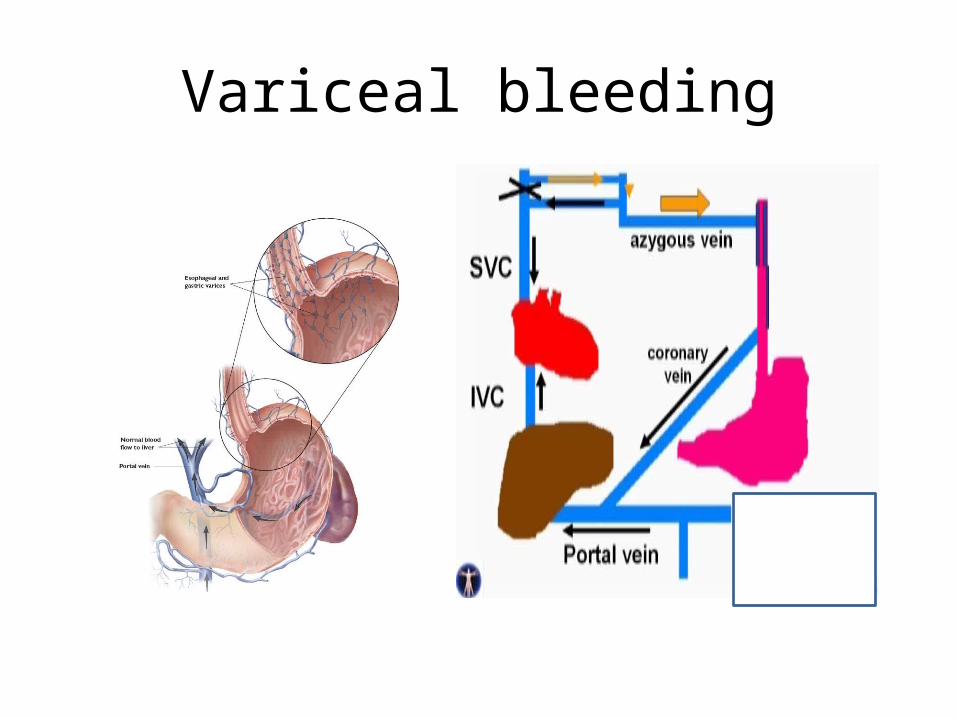
Variceal bleeding










Further reading/References
• Clinical Anatomy: Applied Anatomy for Students and Junior Doctors by Prof H Ellis
• Review Of Medical Physiology by W F Ganong• Guidelines - http://guidance.nice.org.uk/CG141 - http://www.sign.ac.uk/guidelines/fulltext/105
