gene therapy review - american society of radiologic ... · 156 ce directed reading radologc...
TRANSCRIPT

155
CEDirected Reading
This article is a Directed Reading. Your access to Directed Reading quizzes for continuing education credit is determined by your membership status and CE preference.
RADIOLOGIC TECHNOLOGY, November/December 2014, Volume 86, Number 2
Gene Therapy Review
Joseph Anthony Moss, MS
After completing this article, the reader should be able to:Understand basic gene therapy methodologies.Describe current modes of therapeutic delivery.List key diseases that are targeted using gene therapy.Identify the role of medical imaging in gene therapy research and clinical application.Discuss current and future challenges and ethical issues associated with gene therapy.
The use of genes to treat disease, more commonly known as gene therapy, is a valid and promising tool to manage and treat diseases that conventional drug therapies cannot cure. Gene therapy holds the potential to control a wide range of diseases, including cystic fibrosis, heart disease, diabetes, cancer, and blood diseases. This review assesses the current status of gene therapy, highlighting therapeutic methodologies and applications, terminology, and imaging strategies. This article presents an overview of roadblocks associated with each therapeutic methodology, along with some of the scientific, social, and ethical issues associated with gene therapy.
This idea of gene therapy was concep-tualized in the early 1970s1 but was not applied until the 1990s.2 With knowledge now available about the human genome and the discovery of genes responsible for medical conditions, along with develop-ment of gene transfer vector and delivery systems, physicians can target particular genes and pathways that play key roles in how the human body functions.
The Human Genome Project,3 a large-scale international research program that started in 1990, was designed to document and understand sequences that make up human DNA. Information learned from mapping the human genome supported many goals in molecular medicine, including improved understanding and management of can-cer and rare diseases. The field of gene therapy therefore is rapidly expanding; however, the biology and strategy of gene therapy is complex and diverse.
In one sense, the goal of gene thera-py is to modify a gene or genetic path-way to prevent or reduce effects of dis-ease. In addition to modifying a gene or pathway, approaches can include:
Medical and health sciences have experienced pro-nounced advances in recent decades. Genetic
research has progressed, and now sci-entists can attempt to modify human genes for therapeutic purposes. By modifying defects in genes that mani-fest into serious diseases, physicians can, in effect, treat or cure the disease. This particular branch of applied genetic research is known as gene therapy, and although still in its infancy after nearly 3 decades, the discipline is quickly gaining momentum in the medical sciences.
The concept of gene therapy evolved from confirmation that certain diseases are caused when an individual inher-its a single gene that is functionally defective. Further, researchers realized that diseases could be managed or potentially cured by the insertion and expression of an operational copy of the mutant or deleted gene. An operational copy of a gene is one that has had its deformities and defects corrected or repaired for use in therapy.

156
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2014, Volume 86, Number 2
Gene Therapy Review
Replacing a mutated gene with a functional copy of the gene.
Inactivating a mutated gene that is functioning improperly or introducing an entirely new gene to help fight a disease.
Repairing an abnormal gene through selective reverse mutation.
Regulating the degree to which a gene is turned on or off.
Of the more than 14 000 known diseases,4 more than 10 000 are known to be monogenic, or controlled by a single gene.5 Each disease varies in how rare and serious it manifests in humans, and each year the num-ber of known genetic diseases increases. Generally, 10% of people will, at some point in their lives, have a type of genetic mutation, activated by environmental, dietary, or lifestyle factors that cause a disease.6
Gene therapy research and clinical trials are ongoing in the United States and around the world. More than half of the research has occurred in the past decade and most clinical trials (approximately 90%) are concentrat-ed in just 10 countries.7 The United States and Europe account for 90% of all clinical trials worldwide, the majority of which target cancer-related disease. Many of these trials still are in the early clinical phases. Multiple conditions and diseases have been targeted for gene therapy, many of which are listed in Table 1.
Commercial development of gene therapy is quickly gaining momentum. Hundreds of millions of dollars have been raised by biotechnology companies toward gene therapy.8 In fall 2013, the Children’s Hospital of Philadelphia invested $50 million in a new biotech-nology start-up that aims to be the nation’s first com-mercial provider of gene therapy.9 In early 2013, a gene
Table 1
Conditions and Diseases Targeted for Gene Therapy7
Monogenic disorders
Cystic fibrosis, severe combined immunodeficiency, -1 antitrypsin deficiency, hemophilia A and B, Hurler syndrome, Hunter syndrome, Huntington chorea, Duchenne muscular dystrophy, Becker muscular dystrophy, canavan disease, chronic granulomatous disease, sickle cell disease, familial hypercholesterolemia, Gaucher disease, Fanconi anemia, purine nucleoside phosphorylase deficiency, ornithine transcarbamylase deficiency, leukocyte adherence deficiency, gyrate atrophy, Fabry disease, familial amyotrophic lateral sclerosis, junctional epidermolysis bullosa, Wiskott-Aldrich syndrome, lipoprotein lipase deficiency, late infantile neuroal ceroid lipofuscinosis, retinal disease, and mucopolysacchraridosis
Cancers Breast cancer, ovarian cancer, cervical cancer, glioblastoma, leptomeningeal carcinomatosis, glioma, astrocytoma, neuroblastoma, colon cancer, colorectal cancer, liver metastases, posthepatitis liver cancer, pancreatic cancer, prostate cancer, renal cancer, melanoma, nasopharyngeal carcinoma, adenocarcinoma, mesothelioma, leukemia, lymphoma, sarcoma, and multiple myeloma
Infectious diseases
HIV/AIDS, tetanus, Human herpesvirus 4 (Epstein-Barr virus), Human herpesvirus 5 (cytomegalovirus), adenovirus, Japanese encephalitis virus, Hepatitis B virus and Hepatitis C virus, and influenza viruses
Cardiovascular disease
Peripheral vascular disease, intermittent claudication, critical limb ischemia, myocardial ischemia, coronary artery stenosis, stable and unstable angina, venous ulcers, diabetes-derived vascular complications, pulmonary hypertension, and heart failure
Neurological conditions
Alzheimer disease, carpal tunnel syndrome, cubital tunnel syndrome, diabetic neuropathy, epilepsy, multiple sclerosis, myasthenia gravis, Parkinson disease, and peripheral neuropathy
Ocular diseases Diabetic macular edema, Leber congenital amaurosis, glaucoma, retinitis pigmentosa, superficial corneal opacity, wet age-related macular degeneration, Stargardt disease, Usher syndrome 1B, and age-related macular degeneration
Other diseases and conditions
Inflammatory bowel disease, rheumatoid arthritis, chronic renal disease, fractures, erectile dysfunction, anemia of end-stage renal disease, parotid salivary hypofunction, type I diabetes, detrusor overactivity, Down syndrome, Rett syndrome, and graft vs host disease
157
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2014, Volume 86, Number 2
Moss
therapy company in Cambridge, Massachusetts, raised more than $100 million in an initial public offering.10 Recently, another company agreed to develop and mar-ket a potential gene therapy to treat hemophilia B that was in a phase 1/2 trial at a cost of nearly $25 million.8
However, completion of various clinical trials provides no guarantee that all or even many of the currently funded technologies will become accepted or widely used. Only about 5% of trials to date are in later (phase 3 and 4) clinical stages.7 In 2012, however, the European Union approved alipogene tiparvovec after years of research.11 The therapy, which targets the genetic disorder lipoprotein lipase deficiency, has provided a significant boost to the gene therapy field. This came well after the first U.S. Food and Drug Administration (FDA)–approved gene therapy trial in 1990 for adenosine deaminase deficiency, an inherited disorder that compromises an individual’s immune sys-tem and causes severe combined immunodeficiency.2
Neither alipogene tiparvovec nor any other gene ther-apy has been approved by the FDA to date. Worldwide, recombinant adenovirus-p53 was the first gene therapy product approved. The adenovirus vector carrying the p53 gene as a treatment for cancer was first approved in China in 2003 for clinical use. There have been claims that large numbers of patients already have been treated.12 In the United States, several gene therapies in late-phase testing or near late-phase testing are contending to be the first FDA-approved therapy. Currently, 8 to 10 clinical trials are nearing final stages of testing.13 These late-phase trials include therapies targeting genes involved in various cancers, cardiovascular disease, and blindness.
Radiologic technology has played a continual role in gene therapy administration and will remain essential. Molecular imaging, a specialized branch of radiology, is consequently emerging. The radiologic sciences are becoming increasingly complex in equipment and meth-odology. Imaging professionals are expected to master new terms and concepts related to gene therapy delivery to targeted cells and to monitoring cellular function.
Gene Therapy FundamentalsGenes
Gene therapy typically involves substituting cor-rectly functioning genes for defective ones. In terms of
basic biology, genes are “a locatable region of genomic sequence, corresponding to a unit of inheritance, which is associated with regulatory regions, transcribed regions, and/or other functional sequence regions.”14,15 In simpler terms, genes are the physical and func-tional units of heredity. Humans are estimated to have between 20 000 and 25 000 genes.16
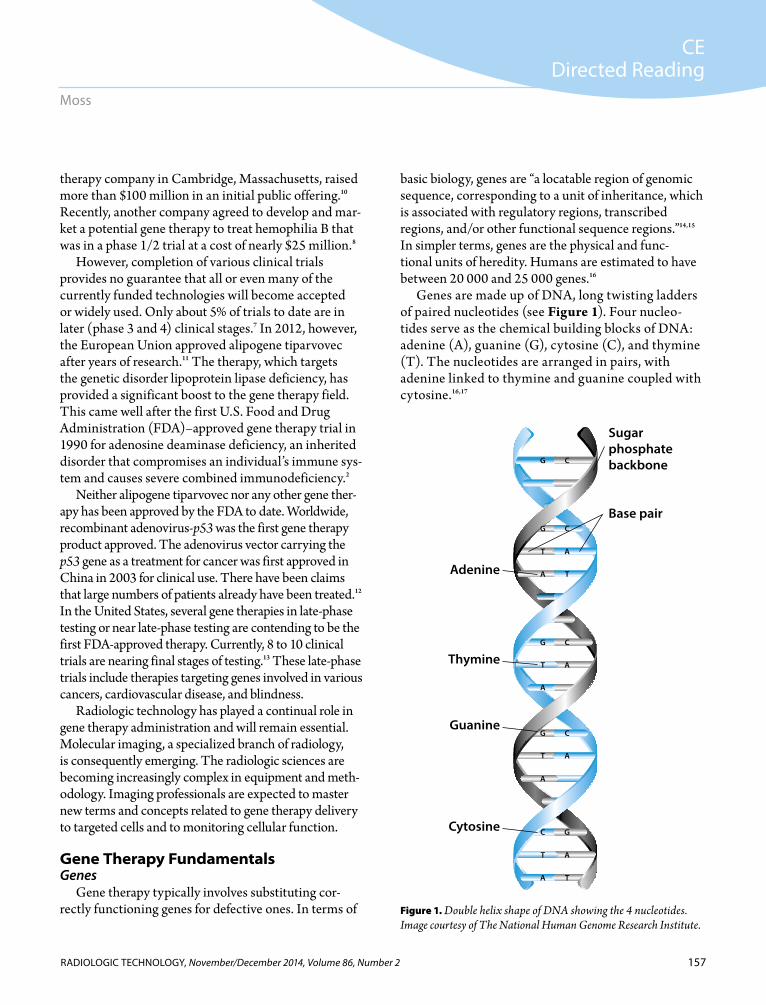
Genes are made up of DNA, long twisting ladders of paired nucleotides (see Figure 1). Four nucleo-tides serve as the chemical building blocks of DNA: adenine (A), guanine (G), cytosine (C), and thymine (T). The nucleotides are arranged in pairs, with adenine linked to thymine and guanine coupled with cytosine.16,17
Figure 1. Double helix shape of DNA showing the 4 nucleotides. Image courtesy of The National Human Genome Research Institute.
G C
G C
T A
A T
G C
T A
A
G C
T A
A
GC
T A
A T
Sugar phosphate backbone
Base pair
Adenine
Thymine
Cytosine
Guanine

158
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2014, Volume 86, Number 2
Gene Therapy Review
The combination and sequence of these nucleotides provide the instructions for manufacturing the thou-sands of proteins needed by the human body. A small percentage of genes (about 1%) are alleles. Their unique base pair coding helps account for the traits passed from parents to offspring. Genes vary in size from a few hun-dred nucleotide pairs to more than 2 million base pairs, and there are approximately 3 billion base pairs in the human genome.16,17
Genes become functional through a chain of bio-chemical events. A gene’s DNA sequence, or code, is arranged in a string of nucleotide triplets known as codons. For example, the string CATATCATT would be arranged CAT ATC ATT. The codons specify, or code for, any one of the 20 different amino acids used to manufacture proteins.
To make a protein, the coded DNA information is copied, or transcribed, into messenger ribonucleic acid (mRNA), a single-stranded molecule. The mRNA then travels from the nucleus to the cytoplasm of the cell (see Figure 2). Once in the cytoplasm, tiny units known as ribosomes read the mRNA code and use the infor-mation to transform amino acids into proteins (see Figure 3).18,19
Proteins are monitored and regulated by a number of mecha-nisms such as repressor proteins that prevent excessive production and activator proteins that stimu-late production. In addition, any change or modification to genetic DNA can affect the structure and quantity of proteins produced by the body.20,21
In principle, a faulty gene can create a malfunctioning meta-bolic pathway that can manifest as a disease. If the building blocks of DNA are altered or mutated in such a way that the genetic blue-print is changed, the resulting protein could be altered. Most mutations are neutral or silent, only affecting regions of DNA that have no known function.19
Figure 3. Following DNA transcription, the messenger RNA then enters the cytoplasm where ribosomes translate the mRNA code and use the information to make proteins. Image courtesy of The National Human Genome Research Institute.
CellNucleus
Sense strand
Nucleus
Cytoplasm
RNA transcript
Antisense strand RNA polymerase3’
5’3’
5’
Messenger RNA (mRNA) an RNA version of the gene that leaves the cell nucleus and moves to the cytoplasm
mRNA
Figure 2. During transcription, a DNA segment is “unzipped” and used as a template to build the single strand of RNA. Image courtesy of The National Human Genome Research Institute.
Nucleus
Cytoplasm
DNA
Ribosome
ProteinAmino acids
GCG
mRNA

159
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2014, Volume 86, Number 2
Moss
In some cases, a mutation is beneficial and can improve the function of an important protein enzyme.22 However, in a hereditary disease, a mutation in the DNA code can cause a vital protein to malfunction or cease functioning; occasionally the mutation is so acute that the protein is not synthesized at all. Because some proteins are more crucial to a cell’s normal function, the severity of a disease often reflects the importance of the protein.
CategoriesGene therapy generally has been classified into 2
categories: somatic cell (nongerm/nonstem cell) therapy and reproductive cell, or “germ-line,” therapy. The cells targeted for somatic cell therapy are corrective only for the specific patient receiving treatment. The genetic therapy or responding traits and outcomes are not inher-ited.23 Germ-line therapy is based on the Weismann theory of heredity, which states that all inheritable characteristics are transmitted by the reproductive cells (eg, ova or sperm, also called a gamete). Therefore, any therapeutic alteration to the germ cells of the patient will be passed on to his or her descendants.23,24
ApproachesTypically, there are 2 main approaches to gene thera-
py. One approach, the in vivo approach, is the introduc-tion of a gene into a vector that is administered directly into the patient via injection or intravenously. This vector transfers the therapeutic gene into the target tissue to produce the therapeutic protein. The second approach, the ex vivo approach, involves the transfer of vectors carrying the therapeutic gene into cultured cells that have been extracted from the patient. The geneti-cally engineered cells are reintroduced into the patient, where they express the necessary therapeutic protein. In vitro procedures normally occur outside the body and often use artificial media such as test tubes in labora-tory conditions.
Clinicians must consider several key aspects when designing a gene therapy approach, including: Choice of therapeutic gene. Route of administration. Choice of an animal model in which to test the
approach.
For monogenic diseases, such as most muscular dys-trophies caused by the dysfunction of a single gene or lack of a single protein, choosing a gene for therapy is made simpler. However, multifactorial diseases such as diabetes, cancer, spina bifida, Alzheimer disease, and congenital heart defects have more complex origins. Interactions of more than one gene, associated environmental causes, or both, lead to the disease processes. In these instances, choosing a therapeutic gene is more challenging.
In addition, clinicians must focus on finding the right regulatory sequences that determine exactly when and where on the gene encoding of a therapeu-tic protein takes place. These regulatory sequences are called promoters and are positioned in front of the therapeutic gene to be expressed. Some promoters direct gene expression to specific cell types such as cardiomyocytes (heart cells) and hepatocytes (liver cells). Other promoters, known as ubiquitous promot-ers, allow gene expression simultaneously to multiple tissues.
Gene DeliveryGene therapy often requires delivery of a gene into
a target cell’s chromosome. Treatment success depends largely on the agent or vector available to deliver thera-peutic genes. A vector is a vehicle that packages the therapeutic gene of interest. Vectors have several func-tions, including protecting the gene from degradation, facilitating entry into target cells, and securing stable gene transcription upon arrival in the nucleus.25 Ideally, a vector should be efficient in gene transfer and be safe. Safe transfer means that the vector introduces zero to minimal risk of infection or immunogenicity (immune response). In addition, a safe vector causes no mutation in the host cell or patient-to-patient transmission of a virus or other pathogen.25,26
In recent years, a number of vectors have been researched or developed, each with unique character-istics. No universal vector currently exists, so when choosing a vector, researchers must weigh factors such as which target therapy to use and whether short-term or chronic treatment is necessary. More than 40 vari-ants of vectors have been evaluated or implemented in gene therapy clinical trials as of spring 2014. These vec-tors fall into the 2 main categories of viral or nonviral
160
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2014, Volume 86, Number 2
Gene Therapy Review
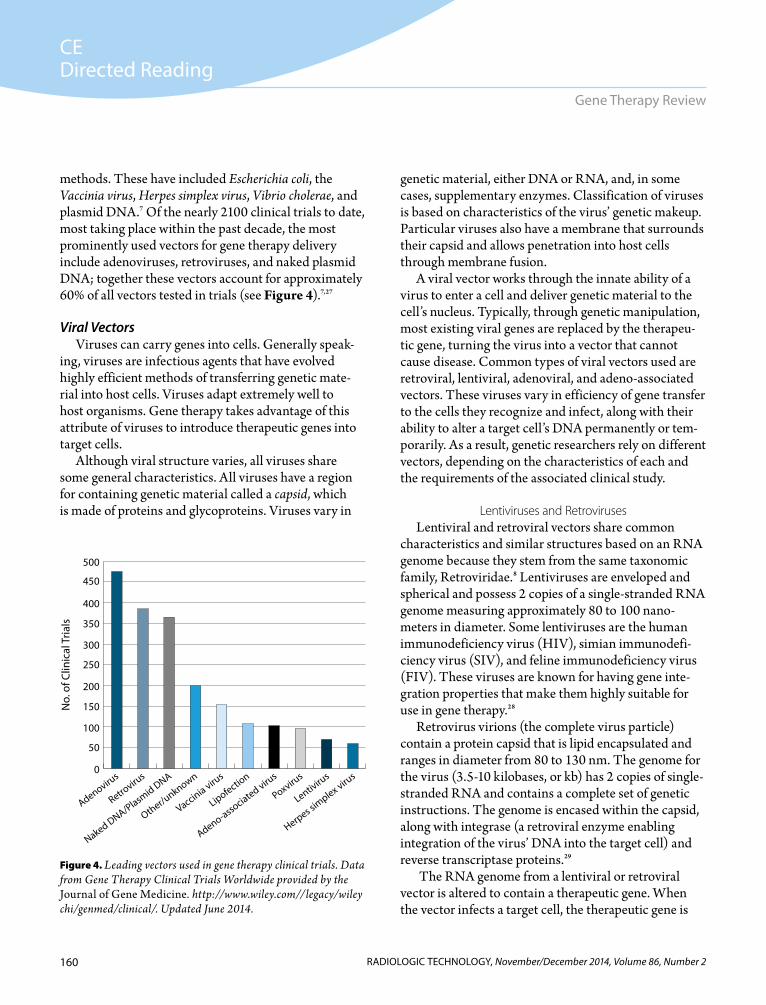
methods. These have included Escherichia coli, the Vaccinia virus, Herpes simplex virus, Vibrio cholerae, and plasmid DNA.7 Of the nearly 2100 clinical trials to date, most taking place within the past decade, the most prominently used vectors for gene therapy delivery include adenoviruses, retroviruses, and naked plasmid DNA; together these vectors account for approximately 60% of all vectors tested in trials (see Figure 4).7,27
Viral VectorsViruses can carry genes into cells. Generally speak-
ing, viruses are infectious agents that have evolved highly efficient methods of transferring genetic mate-rial into host cells. Viruses adapt extremely well to host organisms. Gene therapy takes advantage of this attribute of viruses to introduce therapeutic genes into target cells.
Although viral structure varies, all viruses share some general characteristics. All viruses have a region for containing genetic material called a capsid, which is made of proteins and glycoproteins. Viruses vary in
genetic material, either DNA or RNA, and, in some cases, supplementary enzymes. Classification of viruses is based on characteristics of the virus’ genetic makeup. Particular viruses also have a membrane that surrounds their capsid and allows penetration into host cells through membrane fusion.
A viral vector works through the innate ability of a virus to enter a cell and deliver genetic material to the cell’s nucleus. Typically, through genetic manipulation, most existing viral genes are replaced by the therapeu-tic gene, turning the virus into a vector that cannot cause disease. Common types of viral vectors used are retroviral, lentiviral, adenoviral, and adeno-associated vectors. These viruses vary in efficiency of gene transfer to the cells they recognize and infect, along with their ability to alter a target cell’s DNA permanently or tem-porarily. As a result, genetic researchers rely on different vectors, depending on the characteristics of each and the requirements of the associated clinical study.
Lentiviruses and RetrovirusesLentiviral and retroviral vectors share common
characteristics and similar structures based on an RNA genome because they stem from the same taxonomic family, Retroviridae.8 Lentiviruses are enveloped and spherical and possess 2 copies of a single-stranded RNA genome measuring approximately 80 to 100 nano-meters in diameter. Some lentiviruses are the human immunodeficiency virus (HIV), simian immunodefi-ciency virus (SIV), and feline immunodeficiency virus (FIV). These viruses are known for having gene inte-gration properties that make them highly suitable for use in gene therapy.28
Retrovirus virions (the complete virus particle) contain a protein capsid that is lipid encapsulated and ranges in diameter from 80 to 130 nm. The genome for the virus (3.5-10 kilobases, or kb) has 2 copies of single-stranded RNA and contains a complete set of genetic instructions. The genome is encased within the capsid, along with integrase (a retroviral enzyme enabling integration of the virus’ DNA into the target cell) and reverse transcriptase proteins.29
The RNA genome from a lentiviral or retroviral vector is altered to contain a therapeutic gene. When the vector infects a target cell, the therapeutic gene is
Figure 4. Leading vectors used in gene therapy clinical trials. Data from Gene Therapy Clinical Trials Worldwide provided by the Journal of Gene Medicine. http://www.wiley.com//legacy/wiley chi/genmed/clinical/. Updated June 2014.
0
100
200
300
400
500
450
350
250
150
50
Adenovirus
Retroviru
s
Naked DNA/Plasmid DNA
Other/unknown
Vaccinia virus
Lipofection
Adeno-associated viru
s
Poxvirus
Lentiviru
s
Herpes sim
plex virus
No.
of C
linic
al T
rials

161
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2014, Volume 86, Number 2
Moss
reverse transcribed to DNA in the target cell’s cyto-plasm through a reverse transcriptase enzyme carried by the vector. Once transcribed, the DNA with the therapeutic gene enters the nucleus of the cell, where it integrates into the genome of the target cell.30 In simple terms, this means the viral vector copies its genetic material by inserting the material into the target cell’s DNA.
Lentiviral vectors are highly successful in crossing the nuclear membrane of the target cell and perma-nently changing the cell. This advantage potentially increases the efficacy and longevity of therapeutic treat-ment. When therapeutic genes are integrated into a tar-get cell’s genome, new cells are created through mitosis. In mitosis, or nuclear division, the daughter cells are genetically identical to the parent cell. Daughter cells from a target cell infected by a lentiviral vector also contain the therapeutic gene, which allows for the stable and long-term expression of the therapeutic gene.
All types of retroviruses efficiently integrate into the target cell’s genome, potentially allowing persistent gene transfer. A disadvantage associated with most lentiviral vectors is that the largest genome that can be inserted is 5 kb, whereas some classes of retroviruses have cloning capacities between 7 and 10 kb.31 However, retroviruses generally are difficult to grow in large quantities.
The main difference between the lentiviral and ret-roviral vectors is that lentiviruses can infect both quies-cent (nondividing) and mitotically active cells, whereas retroviruses can infect target cells only during division. As a result, retroviral vectors only can be used for ex vivo gene therapy methodologies.32 Lentiviral vectors can be used in both ex vivo and in vivo gene therapy method-ologies. Lentiviral vectors can infect a broader variety of cell types and sustain gene delivery through stable vec-tor integration into the target cell’s genome. In addition, the lentiviral vector’s viral envelope protein can interact with a broad number of receptors at the target cell sur-face, a characteristic called viral tropism.33
The first clinical trial for lentiviral gene therapy was in 2006 and involved treatment of the cerebral form of X-chromosomal linked adrenoleukodystrophy, a demy-elinating disease of the central nervous system. Since then, lentiviral vectors have been used in approximately
4% of clinical trials.7,34 Conversely, as of 2013, retrovi-ral vectors had been used in approximately 20% of the nearly 2000 trials conducted around the world, repre-senting the second-most-often-used therapeutic vehicles after adenoviral vectors.7
AdenovirusesAdenoviral vectors are derived from adenoviruses
and contain a double-stranded DNA genome measur-ing about 36 kb. More than 55 different variations or serotypes have been identified to date and have been classified according to their characteristics and differ-ences in capsid structure and receptor use.35
Following cell contact, the vector enters the target cell via endosomes, a type of coated vesicle, or mem-branous pouch inside the target cell. This process is called endocytosis. After release from the endosome, the adenoviral DNA enters the target cell’s nucleus where it remains in an extra-chromosomal form.35 Adenoviral vectors have high transfection efficiency, meaning they are effective at adding DNA to target cells. Adenoviral vectors are similar to lentiviral vectors in that they also can infect both actively dividing and quiescent cells.
An advantage of adenoviral delivery of therapeutic genes over lentiviral delivery is the intrinsic charac-teristic of adenovirus DNA not to integrate into the target cell. This characteristic avoids the addition of extraneous DNA bases and the possibility of induc-ing mutation.36 Adenoviral vectors also are more easily manipulated genetically, so the virus cannot continue to replicate. These replication-deficient vectors ultimately reduce unwanted adverse effects. However, producing adenoviral particles takes longer than for other viruses. It takes several weeks to produce an adenoviral virus vector vs several days to produce retroviruses.37
Initially, there were problems associated with adeno-virus vectors. Only a portion of the adenovirus genes were removed, and target cells proved to be capable of recognizing the remaining viral proteins and destroying the newly introduced foreign genes, or transduced, ther-apeutic genes shortly after infection.38 This resulted in short-term expression of the therapeutic gene. However, use of vectors in which all of the viral genes have been removed has made long-term expression of the thera-peutic gene possible with adenoviruses.39 Innovative

162
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2014, Volume 86, Number 2
Gene Therapy Review
adenovirus production schemes have been developed that allow for scaling up production of adenoviruses, facilitating their use in human clinical trials.
Adeno-Associated VirusesAdeno-associated (Parvoviridae family) vectors are
derived from particularly small (approximately 20 nm), replication defective, nonenveloped viruses. The adeno-associated virus genome consists of a single-stranded DNA, which is about 4.7 kb long.40 Adeno-associated viruses are among the most promising viral vectors for human gene therapy and are becoming progressively common as a vector for clinical use. With approximately 12 serotypes,41 most have a variety of tropism, meaning they can respond or orient to different types of tissue. Adeno-associated viruses can infect several types of cells, ranging from skeletal muscle cells to vascular muscle cells.
As with lentiviral vectors, adeno-associated viral vec-tors can infect both dividing and quiescent cells. The virus persists outside the chromosome and has the abil-ity to integrate with stability at a site-specific point with-in the genome. Adeno-associated viruses integrate with stability at a specific point within the human genome.42
After entry into the target cell’s nucleus, the vector follows 1 of 2 distinct, interchangeable pathways of its life cycle: the lytic or lysogenic. The lytic pathway develops in target cells infected with a helper virus, such as adenovirus or herpes simplex virus. Once the adeno-associated virus attaches to and infects the target cell, it makes copies. In the lysogenic pathway, the virus, in absence of a helper virus, becomes established in a target cell and transmits DNA directly from the virus genome into a region of human chromosome 19.43,44
Adeno-associated viruses have been shown to have low immunogenicity45-47 and have no known roles in disease. These vectors have demonstrated efficiency for gene transfer to the retina48,49 and also have been implemented as vectors in gene therapy for lipoprotein lipase deficiency.50 Adeno-associated vector’s clon-ing capacity is relatively limited because the virus has only a 4.7 kb genome. New technologies might allow for expanding vector capacity in the future.51 Further research into the use of adeno-associated viruses likely will continue because of the vector’s promise as a gene therapy delivery method.52-55
Risks of Using Viral VectorsViruses typically can infect more than one type
of cell; therefore, viral vectors can potentially infect healthy cells along with target cells. Once recognized by the body, or if the vaccine or therapy fails, effective use of a viral vector in the patient a second time proves difficult. The same viral vector most likely cannot be used in the patient for a different future vaccine or gene therapy.56,57 Furthermore, some patients may have pre-existing immunity to a viral vector, ultimately rendering the gene therapy ineffective.56,57
Viral vectors that require cells to be actively dividing for transduction (the insertion of genetic material) have drawbacks because some cells are highly resistant to infection and transduction by retroviruses. Transferred genes also can become overexpressed and produce too much of the necessary protein, which can lead to harm-ful effects such as inflammation or an immune reaction. In addition, the integrase enzyme has the innate abil-ity to insert genetic material in arbitrary spots within the target cell’s genome. If genetic material is inserted in the wrong location, insertional mutagenesis can occur. This has been demonstrated in clinical trials for X-linked severe combined immunodeficiency patients in which hematopoietic (blood) stem cells were trans-duced and led to development of T-cell leukemia in a few patients.58 The induced mutation problem can be addressed by inserting sequences to control site integra-tion and using engineered DNA-binding proteins that create a double-stranded break in DNA at user-specified locations.59
Nonviral MethodsNonviral gene vectors have been routinely used in
gene therapy, partly because of concerns regarding the safety of viral vectors. Nonviral gene therapy can be performed by administering plasmid DNA that encodes a transferred gene, or transgene, locally or systemi-cally (eg, injection into arteries). This procedure yields expression of a therapeutic protein to amend a disease state. Clinical applications of nonviral gene delivery have included peripheral arterial occlusive disease,60 arthritis,61 and cancer.62
Using plasmid vectors is one of many approaches that can be used to insert therapeutic genes at preselected

163
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2014, Volume 86, Number 2
Moss
target sites. Most often found in bacteria and archaea (single-celled microbes) plasmids are small circular double-stranded DNA molecules. In nature, plasmids transmit genes that support an organism’s survival, such as antibiotic resistance. Plasmids frequently can be transmitted between bacteria via nonreproductive hori-zontal gene transfer allowing exchange of genetic mate-rial with neighboring bacteria. The plasmids contain a gene for acquiring antibiotic resistance, and after gene transfer, the gene can then be used by the bacteria.
Natural and artificial plasmids are essential tools in genetics and biotechnology labs, where the molecules are routinely used for the genetic cloning of small DNA fragments and genes and for mass production of various proteins. Many plasmids are commercially available for such uses.
Plasmid DNA can be injected alone and yield thera-peutic gene expression. This was first discovered by intramuscular injection using a reporter gene used as a marker to verify and measure gene expression, resulting in the marking of muscle cells at the site of injection. Reporter genes also are called marker genes.63 Recent late-stage clinical applications have taken advantage of this type of plasmid-based gene delivery. Methodologies have been applied to peripheral vascular disease by expressing a therapeutic gene that encodes for angiogenic growth factors, basic fibroblast growth factor, or hepatocyte growth factor.64,65
The development of genetic vaccines is another active area of plasmid DNA therapy. Genetic vaccines using plasmid DNA alone are being developed for pandemic f lu, HIV, and hepatitis C.66-68 Obstacles to full implementation have included reduced and limited transgenic transcription through their use.69 Once the plasmid vector DNA enters the target cell’s nucleus, efficient transcription of the DNA must occur for effec-tive cell division and transgene expression. Therapeutic DNA introduced into target cells must remain func-tional to obtain a permanent cure. Further, the rap-idly dividing nature of various cells might necessitate patients undergoing multiple sessions of gene therapy.
In addition, a patient’s immune system is stimulated when a foreign object, including a gene therapy vector, is introduced. The immune system can reduce therapeutic effectiveness, especially for recurring therapy. The protein
must be purified before the vector is used, usually with a commercially available preparation that strips it of DNA. Antigens can be problematic with regard to the yield and purity, often giving rise to antibody responses to the impurity. There is also a limit to the size of inserts (30-40 kb pairs). Proteins have isoelectric points, and molecular charges might cause electrostatic repulsion of therapeutic DNA at the cell surface. Use of cationic liposomes to enclose the therapeutic DNA can improve endocytosis.70-72
Clinical TargetsInitially, gene therapy was established to cure
patients with hereditary diseases caused by single-gene defects, or monogenic disorders (dominant, recessive, or x-linked). Examples of monogenic disorders include cystic fibrosis, muscular dystrophy, and hemophilia. For many years, gene therapy has been considered most suc-cessful when applied to diseases caused by defects on a single gene or the absence of a single gene. At present, however, much gene therapy research and development is focused on diseases caused by polygenic and nonin-herited diseases. Some of these diseases include hepati-tis C, retinitis pigmentosa, and various types of cancer and cardiovascular diseases. In recent years, the focus has shifted from the conceptual stage through technol-ogy development and laboratory research to present clinical translational trials.
CancerEarly gene therapy clinical trials targeted severe
diseases with minimal therapeutic options and asso-ciated substantial morbidity and mortality, such as severe combined immunodeficiency with bone marrow transplant. To date, more than 60% of trials world-wide are focused on cancer7 with formidable results. For instance, in 2012, a sizable percentage (. 70%) of patients treated for multiple myeloma, a cancer related to plasma cells, showed signs of remission after being treated with genetically engineered T-cells to target specific proteins NY-ESO-1 and LAGE-1 that exist in cancerous myeloma cells.73
Current gene therapy approaches for cancer are less hindered by complications. Many current approaches are designed to elicit increased tumor cell immunogenicity

164
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2014, Volume 86, Number 2
Gene Therapy Review
or to enhance cell death by replacing a gene. In addi-tion, many efforts for cancer therapy do not require sustained and closely regulated gene expression.74 Most gene therapy trials have used adenoviral and retrovi-ral vectors to deliver therapeutic genes to target sites. Adeno-associated viral-based vectors also are proving to be suitable for cancer gene therapy.
Ongoing research involves the application of gene-directed enzyme prodrug therapy in addition to, or as a replacement for, standard chemotherapy for cancer treatment. Essentially, “suicide” genes are directed at cancer cells to make tumors more susceptible to radiation therapy and chemotherapy. These directed genes cause an inactive drug, or prodrug, to become toxic only when the prodrug is metabolized by pro-teins produced by the directed genes injected into the tumor. For example, a directed suicide gene encodes an enzyme that converts a nontoxic prodrug such as ganci-clovir into highly toxic metabolites.
The herpes simplex virus type 1 thymidine kinase (HSVtk) gene is the driving agent that makes trans-duced cells sensitive to the antiviral medication ganciclovir. Gene-directed enzyme prodrug therapy introduces viral or bacterial genes into tumor cells and has successfully been used in several in vitro and in vivo studies.75-78 Use of the prodrug therapy with the HSVtk gene has been thoroughly investigated.79-82 Induction of HSVtk into tumor cells makes cells sensi-tive to various drug regimens.83,84 The therapy’s poten-tial has been demonstrated in animal studies, often with results that include complete eradication of the tumor.85-87
Gene therapy offers potential for targeted destruc-tion of tumor cells in patients and can be used to delin-eate new targets or investigate the role of specific genes in carcinogenesis or cancer progression. In 2013, highly positive results were shown in subjects who had acute lymphoblastic leukemia, a cancer of the blood and bone marrow, and were treated with genetically modified T-cells that attacked cells with CD19 genes on their surface.88
Glioblastoma multiforme is highly invasive and the most common brain tumor occurring in adults.89 The gene therapy approach most often used for treating glio-blastoma multiforme relies on various adenoviral and
retroviral vectors, as well as nonviral vectors. The viral and nonviral vectors are genetically modified to express genes for an enzyme that transfigures a prodrug tar-geted at the tumor sites and ultimately destroys tumor cells. Several enzyme-prodrug systems have been evalu-ated in phase 1, 2, and 3 trials,90 with the HSVtk gene as the most extensively investigated.
To date, only modest successes have been recorded.91,92 Unfortunately, anatomical and physiological aspects associated with the brain reduce transduction effi-ciency and effect overall vector targeting and delivery. Researchers continue to review limitations and poten-tial strategies.90,93,94
Cardiovascular DiseaseTargeted gene therapy also is being investigated for
the management of cardiovascular disease. The use of gene therapy is currently being studied for several cardiac diseases, including heart failure and coronary artery disease. Heart failure is one of the leading causes of morbidity and mortality in the United States.95 Several preclinical and clinical studies have shown some efficacy in administering genes that upregulate enzymes, notably a transporting gene involved in myocardial contraction and relaxation to treat advanced heart failure.96-101
Jessup et al conducted a study on calcium upregula-tion using gene therapy in patients with heart failure. Low levels of calcium uptake have been identified in striated heart muscle cells of patients with heart failure. Further, the deficient levels have been associated with low expression and activity of an enzyme that triggers reloading of calcium while the sarcoplasmic reticulum is at rest, the sarcoplasmic reticulum adenosine triphos-phatase, calcium 2 ion. In phase 1 and 2 clinical trials investigators restored levels of the associated enzyme in patients who had advanced heart failure using gene transfer via an adeno-associated viral vector. Patients who received intracoronary administration of the gene therapy had significant improvement in functional capacity and symptoms from heart failure.96
Coronary artery disease is another leading cause of mortality in the United States95 and is currently the most common cause of death in the world.102 Alternative options to conventional pharmacologics and revascular-ization methodologies are being developed. One option

165
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2014, Volume 86, Number 2
Moss
is therapeutic angiogenesis, which involves administer-ing certain genes for angiogenic growth factors to aug-ment collateral vessel development and increase new blood cell formation.
Recent clinical studies have investigated a number of angiogenic growth factors, including fibroblastic growth factor, vascular endothelial growth factor, and hepatocyte and platelet-derived growth factors.103-108 However, angiogenesis is a highly complex mecha-nism requiring the organization of multiple growth factors acting on receptors to stimulate and sustain growth, thereby complicating therapeutic applica-tions. Moreover, positive and encouraging effects of gene therapy on initiating heart impulse activity have been shown in several arrhythmia investigations.109-111 Selective expression of certain genes producing ion-stimulated enzymes could ultimately be used to initiate and regulate heartbeats, thereby establishing genetic alternatives to electrical pacemakers.
VisionGene therapy offers great promise for treating vision
loss from a variety of causes. Significant advances in understanding disease processes of human retinopathy and the development of efficient retinal gene transfer using adeno-associated vectors or lentivirus-based vec-tors have led to proof-of-concept studies of gene replace-ment therapy.112,113 The potential of gene therapy has been demonstrated in the treatment of degenerative diseases such as retinitis pigmentosa, which is characterized by a slow, progressive loss of photoreceptors and caused by defects specific to the retinal epithelium, a pigmented cell layer just outside the neurosensory retina.114
In 2011, the first gene therapy clinical trial was initi-ated for Stargardt disease, a form of juvenile macular degeneration that affects 30 000 to 50 000 people in the United States alone.115,116 The trials are designed to work by delivering healthy copies of the protein coding gene ABCA4 to cells in the retina. Another example of progress is the reconstitution of vision following adeno-associated viral vector gene therapy in patients with Leber congenital amaurosis, a hereditary disorder that leads to retinal dysfunction and visual impairment at an early age.117, 118 To date, 19 genes have been identified with mutations that lead to the disease.119
In 2007, positive effects were reported concerning subretinal delivery of recombinant adeno-associated viral vectors carrying the RPE65 gene for inherited retinal disease.120 Several modes of therapy are currently in varying stages of development, including a human clinical trial for gene replacement for the retinal pigment epithelial gene RPE65 Leber congenital amaurosis muta-tion. A 2009 phase 1 clinical trial reported substantial restoration of vision to patients, 50% of whom improved enough to be declassified as legally blind.121 More recently, stable reversal of congenital blindness was dem-onstrated using injections of the adeno-associated viral vector with the RPE65 gene.122
Noninherited DiseasesMany genetic syndromes are not inherited. A form
of Down syndrome called Trisomy 21 is one of the most common noninherited genetic syndromes. The syndrome occurs in approximately 1 of every 700 births.123 Early research has shown that insertion of the X-inactive nonprotein coding gene XIST can silence the extra copy of chromosome 21 that causes Down syn-drome.124 In in vitro experiments, chromosome 21, the extra chromosome in cells of individuals with Down syndrome, has been removed via a type of genetic modification that uses stem cells to naturally remove the third copy.125
Parkinson disease is another example of a disease in which not all cases are directly inherited; only a fraction (15%-25%) of people with Parkinson disease report having a relative with the disease. A gene ther-apy product using adeno-associated viral vectors car-rying neurturin (NTN), a gene encoding for a neuro-trophic growth factor, was well tolerated and appeared to reduce symptoms in about 40% of subjects with advanced Parkinson disease in a 2006 phase 1 study. Neurturin is the protein responsible for the survival and function of neurons. Instead of simply treating symptoms of Parkinson disease, helping to preserve neurons could halt degeneration associated with the disease.126
Studies by Muramatsu et al and During et al using adeno-associated viral vectors have shown promise in treating Rett syndrome, a serious brain disorder caused by mutations in the protein-coding MECP2 gene. Fewer

166
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2014, Volume 86, Number 2
Gene Therapy Review
than 1% of cases are inherited and the disorder affects mostly young girls. In the Muramatsu study, the vec-tors carried genes encoding for the aromatic L-amino acid decarboxylase, which is required for synthesis of the neurotransmitters dopamine and serotonin, and in the During study, vectors carried genes encoding for glutamic acid decarboxylase, an enzyme involved in producing neurotransmitters.127,128
Participants in the Muramatsu study showed signs of improvement after 2 years, while those in the During study improved after 3 years of treatment. For many years, Rett syndrome was widely regarded as incur-able. Recently, using an animal (mouse) model, it was demonstrated that Rett syndrome could be reversed by restoring the function of the MECP2 gene,129 providing some hope for future management.
Recent reports have been made of promising and long-term results in canines chemically induced to have diabetes that were given single shots of an adeno-associated viral vector. The vector carried genes for insulin and glucokinase in skeletal muscle, making it possible for the dogs’ bodies to produce insulin and glucokinase.130,131
Medical Imaging in Gene TherapyGene therapy offers great promise for various dis-
eases and conditions and for managing several cancer types. Medical imaging plays a key role in implement-ing and advancing strategies for successful delivery and function of desired genes. These strategies comprise both traditional and new molecular imaging technolo-gies using reporter probes. In medical imaging, reporter probes are radiopharmaceuticals that help detect or identify disease biomarkers.132
Imaging techniques used in gene therapy have included ultrasonography, magnetic resonance (MR) imaging, computed tomography (CT), positron emis-sion tomography (PET), and single-photon emission computed tomography (SPECT), and optical imaging. Each imaging modality offers unique advantages and limitations related to sensitivity or spatial resolution. For example, MR imaging offers superior contrast for soft tissue and high spatial resolution for anatomical information, yet has lower sensitivity for detecting reporter probes compared with PET scanning.133
Monitoring Gene ExpressionAn objective in gene therapy is to ensure as rapidly
as possible that the administered therapeutic gene is being expressed in the target cells. Most current in vivo molecular imaging strategies use a reporter gene with a complementary reporter probe. By coupling a reporter, or marker, gene with a therapeutic gene, molecular imaging techniques in particular can be used to evalu-ate gene expression. The marker gene might serve no therapeutic role but only act in reporting gene expres-sion, providing an indirect measure of the location and magnitude of the expression of the therapeutic gene.
Reporter genes and probes have been developed mostly for PET and MR imaging. MR imaging relies on measuring magnetization of nuclei (eg, carbon 13, f luorine 19, sodium 23, and phosphorous 31) subjected to radiofrequency radiation, which offers several strategies for use of markers with MR imaging. These strategies include enzyme-based markers using enzyme-catalyzed chemical modification that exploit various enzymes based on contrast agents with cova-lent bonds. A covalent bond refers to sharing of elec-trons between compounds. Other strategies include bond cleavage, or splitting of bonds, and iron-based strategies in which protein accumulation of iron can act as a contrast agent.
Depending on the protein structure and oxidation state, iron can act as a paramagnetic reactive metal. Manipulation of iron concentration yields detectable contrast and has been implemented for monitoring therapeutic gene expression in which an engineered transferrin receptor134 was expressed as part of a vec-tor that carried several genes, among them a prodrug therapy gene.135
Chemical exchange saturation transfer (CEST) can be monitored using a variety of compounds (eg, organic, organometallic, or both) with suitable chemical exchange rates and resonance frequencies. The tech-nique works by chemical exchange between protons in solutes such as contrast agents with those in water.136,137 An advantage of using MR reporter genes is that the specific signal can be recorded for both soft-tissue anat-omy and functional tissue information, providing data on gene expression along with anatomic and functional information.138,139

167
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2014, Volume 86, Number 2
Moss
PET is one of the most exacting approaches to imaging for detection and quantification of picomolar amounts of radiolabeled materials in vivo. A further advantage of PET is its accuracy regardless of the depth of the tissue of interest. Reporter probes labeled with positron-emitting isotopes, such as f ludeoxyglucose F 18, oxygen O 15, and copper Cu 64, are taken up by target cells, binding to specific receptors. The recep-tors are phosphorylated, which means that a chemical reaction or transfer occurs in a phosphate group that is catalyzed by a substrate-specific enzyme that can be detected on PET images.
A number of PET reporter genes have been found suitable for imaging vector-mediated gene delivery and expression in both preclinical and clinical situations. The findings have been based on the radiolabeled substrates that interact with specific transgenic proteins. Much like MR-based markers, these reporter genes enable noninva-sive analysis of the location, level, and kinetics of trans-genic activity. The PET methodology has optimum char-acteristics, however, in terms of sensitivity and quantifi-cation of in vivo gene expression. In addition, increased availability of and familiarity with PET equipment has helped define the modality as an applicable method for analyzing gene therapy in patients.140
As with vectors for gene delivery, reporter genes and probes should have certain characteristics, such as inability to induce immune responses, accumulation of probes only at the site of reporter gene expression, sta-bility and lack of cytotoxicity, and the ability to fit into selected vectors.140 In addition, no single combination of marker genes and probes is suitable for all imaging applications.
A few strategies are used to facilitate imaging of the reporter gene and probe using PET or SPECT. Intracellular or enzyme-based strategies involve phos-phorylation of a radiotracer substrate by the imaging reporter enzyme, in which cells expressing the imaging reporter gene ensnare the probe. For example, the enzy-matic activity of HSV1-tk has been used widely for in vivo imaging of gene expression via various radioisotope-labeled substrates. Surface-based (receptor-based) strate-gies involve the delivery of membrane receptors such as a dopamine-2 receptor or somatostatin receptor to target cells that bind specifically to radiolabeled tracers such as
F18 (fluroethyl) spiperone or radiolabeled somatostatin analogues. The technique results in the trapping of the probe on or in cells expressing the gene.
Transporter-based strategies using radiopharmaceu-ticals with half-lives averaging about 110 minutes are time-sensitive approaches that deliver membrane trans-porters to target cells that facilitate uptake of the report-er probe. The major advantages of surface-expressed receptors are satisfactory kinetics, or chemical changes, and the fact that synthetic reporters can be manufac-tured to recognize probes already approved for use by the FDA. Advantages of intracellular strategies include their simple design and lower immune responses com-pared with surface-based strategies. HSV1-tk (and vari-ants of the gene) is the most frequently used reporter gene. The gene is imaged by both PET and SPECT.141 In addition, HSV1-tk conceptually can be used both as a therapeutic gene and a reporter gene.142
Gene DeliveryA leading challenge in gene therapy is the release
of a therapeutic gene to the precise desired location. Research in cancer gene therapy is focused on how to improve gene delivery to malignant tumors. Medical imaging can play a critical role when combined with medical biology and oncology in the delivery of suicide genes that can help destroy malignant cells. The tar-geted delivery of therapeutic genes helps limit potential adverse effects from drug toxicity. Vascular and inter-ventional radiology techniques are particularly suited for marginally invasive and readily monitored gene delivery. Some medical imaging techniques in gene therapy delivery are already implemented or undergo-ing evaluation in clinical trials.
UltrasoundExposure of cells to ultrasound waves increases
membrane permeability and assists with intentional introduction of nucleic acids or transfection into cells. The first applied demonstration of ultrasonog-raphy in gene transfer took place in 1987.143 Local administration of naked plasmid DNA results in a small amount of gene transfer to cells at the site of injec-tion. Cells are known to spontaneously uptake nucleic acids.144 However, gene transfer efficiency can be

168
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2014, Volume 86, Number 2
Gene Therapy Review
increased by applying electroporation or sonoporation. Electroporation is use of electrical pulses to permeate a cell membrane with tiny holes, and sonoporation devel-ops temporary pores in the membrane using sound waves. Applying electrical or ultrasound energy in a series of pulses (lasting microseconds) allows for cell entry and results in increased gene expression.145-150
When oncologists use liposomes for gene therapy, focused ultrasound can implode the liposomes, prompting them to release their genetic contents. Liposomes are artificial vesicles made from lipids. The lipids encapsulate microbubbles generally filled with gas and contrast agents. Success of the therapy depends on effective delivery of the plasmid DNA and adequate acoustic energy. In addition, clinicians must select the most suitable plasmid to maximize delivery.151 The magnitude and duration of pulses must be optimized to maximize gene transfer and minimize damage to cell membranes. Several studies have shown that ultra-sound can be used to enhance gene expression from liposomal transfection.152
Transfection rates have recently increased several orders of magnitude in in vitro studies using ultrasound exposure on various tissue cells.152-154 In addition, in vitro transfection rates using ultrasound are generally much higher than those recorded for in vivo studies.155-157 These methods result in increased uptake by cells and therefore an increase in gene expression. Still, nonviral vectors con-tinue to offer lower levels of gene transfection and subse-quent cellular expression than do viral vectors.
Computed TomographyImaging methods such as CT have been used for
decades for gene therapy monitoring and for precise needle guidance for therapeutic gene delivery. Use of micro-CT imaging assists in evaluating healing responses of allografts. The gene therapy is delivered by adeno-associated viral vectors with the protein carrying the ALK2 gene.158 Micro-CT also has been used to eval-uate articular fracture healing following mesenchymal stem cell-mediated delivery of a gene encoding for bone morphogenetic protein-2.159
In a laboratory study, investigators used micro-CT to evaluate progression of pulmonary fibrosis in mice fol-lowed by intertracheal administration of an adenoviral
gene vector encoding for the transforming growth factor-1 gene.160 In human trials, CT imaging has guided intratumoral injection of plasmid DNA in trials directed at treating melanoma.161 CT scanning also has been used to safely steer gene-therapy injections direct-ly into the tumor when treating patients with metastatic kidney cancer.162 Several therapeutic agents have been developed that improve the use of interleukin-2, an approved treatment for metastatic kidney cancer.
In addition, in phase 1 and 2 clinical trials for treat-ment of pancreatic cancer, CT was used to evaluate liver lesions following administration of targeted gene therapy.163 Attempts also have been made to correlate CT images with gene expression, although the meth-ods have been indirect, occurring by means of imaging patterns.164,165
Positron Emission TomographyPET is a specialized nuclear medicine procedure
used to examine various body tissues and to isolate molecular activity in the body to evaluate function and disease. PET scanning can detect chemical substances such as glucose (usually f ludeoxyglucose), which is used naturally by organs or tissues during metabolic processes. Because of this feature, PET scans can dis-play the metabolism of a particular organ or tissue to provide information about the physiology, anatomy, and biochemical properties of the organ or tissue.
PET scans can identify the onset of a disease process before anatomical changes related to the disease can be seen on other structurally based imaging scans, such as CT and MR. PET has been used to evaluate conditions such as Alzheimer, Parkinson, and Huntington disease, and cardiac disease, and is a useful tool in evaluating cancer and cancer therapy.
In gene therapy, PET scanning is a noninvasive tool for diagnosing the pathology, biology, and safety of vectors. In addition, PET scanning is useful for imag-ing biochemical effects of gene therapy; quantitatively monitoring the site, scale, and continuity of gene expression; and to better understand vector biology and safety.
Conceptually, combined use of PET with reporter genes and probes could be used to noninvasively moni-tor all aspects of transgene and cell kinetics in virtually

169
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2014, Volume 86, Number 2
Moss
all types of living mammals. Its usefulness has been shown in animal trials166 and in human patients. For example, Jacobs et al demonstrated that a combination of PET and a specific marker substrate (I-124-labeled 2-fluoro-2-deoxy-1-D-arabino-furanosyl-5-iodo-uracil, or 124I-FIAU) could be used to monitor gene therapy response in a phase 1/2 clinical trial for recurrent glioblastoma in 5 patients.167
PET scanning is not without limitations. Minimizing exposure to ionizing radiation and signal loss from leakage into nontarget signal cells are goals for improve-ment. In addition, radiotracers have relatively short half-lives, and PET scanning has limited ability to track signals longitudinally and long term. Combined CT and PET imaging has become more commonplace. The fusing of structural and functional imaging in a single instrument substantially increases the utility and applicability of imaging in gene therapy patient manage-ment.168 For example, PET-CT has been evaluated for use in gene delivery and for monitoring of gene expres-sion using animal models.169
Magnetic ResonanceMR imaging generates high-contrast and high-
resolution 3-D images and assists in diagnostic evalua-tion of organ function and morphology. Recent efforts have focused on using MR technology and methodolo-gies for monitoring gene therapy delivery, enhancing gene transfection and transduction, and for tracking gene expression.
Various markers have been evaluated for use with MR scanning to display transgene expression.170-173 Rehemtulla et al followed patients who had intratu-moral injection of adenoviral vectors carrying thera-peutic genes into gliomas.174 The investigators recorded anatomical and diffusion-weighted MR images every 2 or 3 days over a period of 4 to 6 weeks to determine therapeutic efficacy and spatial heterogeneity of cancer cell destruction.174
MR spectroscopy has been used in laboratory stud-ies involving mice to evaluating transgenic expression.175 MR also was used in test studies for therapeutic treat-ment of brain tumors in rats, documenting the disap-pearance of large tumors by detecting 5-bromodeoxy-uridine−labeled progenitor (neural stem) cells after the
injection.166 More recently, in a phase 2 trial, MR neu-roimaging was used to monitor participants in which lentiviral vectors containing functional protein coding ARSA genes were delivered as therapy for metachro-matic leukodystrophy, a neurodegenerative lysosomal storage disease caused by arylsulfatase A (ARSA) defi-ciency.176 Neurosurgeons at the University of California San Diego School of Medicine and Moores Cancer Center used real-time MR navigational technology to deliver genes carrying an investigational anticancer drug (Toca 511) directly to brain malignancies.177
A new method of using MR/CEST imaging may be implemented to monitor the effectiveness of gene thera-py for cancer. MR/CEST is considered an alternative to relaxivity-based contrast protocols that is better suited for molecular imaging. The technique involves detect-ing proton exchange when certain chemotherapy com-pounds such as glutamate are broken down.178 Unlike nuclear imaging, MR provides multiple image planes with no ionizing radiation. However, MR sensitivity is limited in some studies.
Challenges and EthicsGene therapy researchers must answer several ques-
tions to gain approval for gene therapy trials in humans. They must determine whether the disease being treated is a good candidate for gene therapy, and be certain that the gene they introduce will be correctly inserted and regulated so that it is clinically expressed in the patient. Researchers also must explain technical details of the DNA and the vector they will use. Even if these questions are answered, human gene therapy experi-ments can be delayed because of the technical aspects involved, risks to study participants and future patients, and the fear of human genetic engineering.179
The future of gene therapy has been riddled with both overly optimistic claims and overly exaggerated statements of risk. Whether future research and applica-tion will remain constrained or open to wider possibili-ties remains to be seen. Ethical and moral issues implicit in gene therapy have drawn notice from several govern-mental and religious organizations. Debate regarding use of genetically engineered material in human subjects has been complex, with viewpoints from the fields of law, medicine, politics, biology, philosophy, and religion.

170
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2014, Volume 86, Number 2
Gene Therapy Review
During the 1980s, when gene therapy was in its infancy, representatives of government agencies and government-appointed groups debated the topic exten-sively, resulting in a succession of guidelines that legiti-mized gene therapy clinical trials.180,181 The emergence of a scientific discipline of gene therapy in the 1990s stimulated mixed reviews within and outside of the scientific community, episodes of public excitement, and, subsequently, some ill-conceived and unsuccessful clinical trials.182
Gene therapy manipulates cells in the human body. Therefore, its use is accompanied by several unique ethical and moral concerns. Gene therapy is initiated for patients who have serious diseases and conditions. However, clinicians, ethics committees, patients, and family members must draw lines between which traits constitute a unique disorder in an individual and which constitute advancement of common human traits. Further, society must address which governing body will oversee determining and enforcing these lines. Inevitably, issues regarding affordability and economic fairness will arise.
Current therapeutic research has focused on treating patients by targeting therapy to body cells such as blood cells. Somatic gene therapy cannot be passed on genera-tionally. In the future, however, germ-line gene therapy could potentially target reproductive cells sparing a family’s future generations from a particular genetic dis-order. On the other hand, the therapy could affect the development of a fetus in unexpected ways or have long-term adverse effects that are yet unknown.
Individuals who would be most affected by germ-line gene therapy are not yet born, so they cannot choose whether to have the treatment. Because of these ethical concerns, the U.S. government does not allow federal funds to be used for research on germ-line gene therapy in humans. The idea of germ-line gene therapy is quite controversial, and acceptance may take years or decades.
Despite the dramatic increase of gene therapy fund-ing and clinical trials over the past decade, as well as recent successes, attitudes toward gene therapy vary. In a recent study, a sizable proportion of European Union opinions favored regulation, and European public opinion was mixed, with residents weighing the risk vs
usefulness of gene therapy to society.183 People in several countries in the European Union knew little about the subject.183 In the United States, public opinion is gener-ally favorable, though citizens have expressed concerns about eugenics and control of genetic information.184
New DiscoveriesNew molecular methodologies and technologies can
accomplish much good but could cause great harm. These issues arise whenever powerful new technologies are developed. Genetic sequencing, for example, has been established as a powerful diagnostic and prognos-tic tool, but it is not yet fully clear how useful sequenc-ing will be for disease prevention or health promotion and the role of regulation and ethics in those uses of the technology. Current high-throughput sequencing technology is extremely powerful and has led to an increase in sequencing projects in laboratories around the world. The cost and accuracy of genome sequenc-ing have improved dramatically. Genomics is no longer seen as the expensive venture that the initial $2.7 billion human genome mapping project cost in 2003.3
If and when genome sequencing becomes a clinical mainstay, it is uncertain whether scientists and physi-cians will know enough about how genes code for health to make genomic data useful for preventing disease. In addition, physicians are unclear specifically what genetic findings they should reveal to patients, and whether the answer differs based on the patient’s age and health. Ownership of privacy of genetic data for research is questionable. Current gene therapy research is focused on correcting genetic f laws and curing life-threatening disease. Although regulations have been developed for conducting these types of studies, the techniques of gene therapy will likely become more refined and more widely available in the future. At that point, more com-plex issues should be addressed.185
There is a distinction, of course, between repara-tion of genetic damage and efforts to make genetic “enhancements.” Some also have concerns that genetic therapy technologies could be abused to improve ath-letic performance (gene doping), even at risk to an ath-lete’s own health or the health of others.186 Moreover, decisions might need to be made regarding whether and when it is appropriate for society to intervene on

171
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2014, Volume 86, Number 2
Moss
behalf of anyone who abuses or could be harmed by gene therapy or doping. Decisions about ethical issues, commercial interests, political choices, intellectual property, and patient rights might be necessary and some rules might need to be enforced, including in what circumstances it is morally acceptable to manipu-late human genes. In 1990 the Ethical, Legal, and Social Implications research program was established to address basic and applied research on the ethical, legal, and social implications of genetic and genomic research.187
It has been argued that correcting a gene’s func-tion is merely a further extension of medicine. As our understanding of the human body has increased, we
can now envisage treating patients at the genetic level. In effect, somatic gene therapy does not represent a major departure from established medical practice. Instead of injecting a necessary, yet deficient, protein into a patient, the gene that normally would regulate the body’s production of that protein could have its normal function restored. These viewpoints have been expressed with regard to the ethics of somatic gene therapy.188
Current laws in the United States and United Kingdom prohibit early embryonic and germ-line gene therapy, which is in part because of our current state of genetic knowledge. It is possible that enough information might never be obtained. Concerns about cost and debates regarding the benefit of eradicating genetic diseases vs the justification of making genetic decisions on behalf of future generations are potentially irrevo-cable decisions.
RegulationRegulation of gene therapy is intended to assess
potential risks and to ensure a measure of safety. Although gene therapy holds much promise, a few seri-ous adverse events have occurred in its use, including death of a patient from an inflammatory reaction to use of an adenovirus-based vector in 1991,189 development of leukemialike symptoms following successful gene therapy,190 and death from disseminated histoplasmosis following a gene therapy trial. After a subsequent inves-tigation of the trial participant’s death from histoplas-mosis, however, it was concluded that the gene therapy treatment was not the cause of death.191 With these examples in mind, investigators must consider how safe a therapeutic approach must be before it is ethical to try it on humans, and whether the review process is suffi-cient to determine clinical safety.
In the United Kingdom, genetic research and its applications in gene therapy are controlled by organi-zations such as the national Gene Therapy Advisory Committee and regional and local ethics committees for hospitals, universities, and research institutes.192 In the European Union, the European Medicines Agency is responsible for the conduct of clinical trials and vigilance of pharmaceutical development activities.193 Numerous steps must be followed for approval.
Box
Resources on Genomics and Gene Therapy
For information on genes, chromosomes, and conditions:National Human Genome Research Institute Talking Glossary of Genetic Termshttp://www.genome.gov/glossary/index.cfm
National Library of Medicine Genetics Home Referencehttp://ghr.nlm.nih.gov
To search active gene therapy clinical trials:The Journal of Gene Medicine Databasehttp://www.abedia.com/wiley
National Cancer Institute Clinical Trialshttp://www.cancer.gov/clinicaltrials
For information on gene therapy:Gene Therapy Nethttp://www.genetherapynet.com/viral-vectors.html
For information on plasmid cell vectors:Pinto UM, KM Pappas, S Winans. The ABCs of plasmid replica-tion and segregation. Nature Reviews Microbiol. 2012;10:755-765. doi:10.1038/nrmicro2882.
For information about issues regarding genetics:National Human Genome Research Institutehttp://www.genome.gov/Issues

172
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2014, Volume 86, Number 2
Gene Therapy Review
In the United States, gene therapy is regulated by a myriad of governmental departments and organizations. Since 1976, the Department of Health and Human Services has overseen most gene therapy activities. The Department of Health and Human Services has super-vision of clinical trials, and the National Institutes of Health, which has considerable oversight of research for drug development, testing, and safety, is under the aus-pices of the Department of Health and Human Services.
Also within the Department of Health and Human Services are the Office for Human Research Protections and the FDA.194 The FDA is the essential agency for protecting the health of U.S. citizens by ensuring the safety of drugs, medical devices, and biological products before their commercial use. All research involving human subjects must undergo review and approval from an institutional review board195 and additional require-ments made by the National Institutes of Health must be met in addition to those specified in the Code of Federal Regulations. Furthermore, the Center for Biologics Evaluation and Research, a center within the FDA that was created by the Federal Food, Drug, and Cosmetic Act and the Public Health Service Act, regulates cellular therapy products, human gene therapy products, and certain devices related to cell and gene therapy.
A manufacturer considering developing and selling a gene therapy product must first inform the FDA. Before implementing human trials, the manufacturer must obtain special permission, called an investigational new drug application, from the FDA. Manufacturers must meet rigorous FDA requirements for safety, purity, and potency from the FDA and additional agencies such as the National Institutes of Health before marketing a new product.196
The process for obtaining an investigational drug license is more difficult for gene therapy products than for standard chemical or biological drugs for several reasons. The distinctive nature of the products and the fact that early trials using gene therapy have resulted in some unexpected outcomes have led to extra caution on the part of regulators. Other concerns involve questions regarding drug dosage and toxicity, drug persistence in the patient, and ensuring quality in manufacturing and preservation of the therapeutic products.197
ConclusionGene therapy is a complicated subject of research, and
questions remain to be answered. Nonetheless, the field of gene therapy has been marked by astounding progress despite early pitfalls. Medical researchers are develop-ing more accurate and proficient methods of diagnos-ing and managing several diseases and disorders, and these advancements will only become more impressive. (See the Box for resources about genomics and gene therapy.) Recent developments in gene therapies and the ability to pharmacologically target and administer these therapies to infected cells suggest that new cura-tive treatments will soon prove applicable to a broader range of diseases and patients.
In the future, gene therapy will provide an exciting new therapeutic option, particularly for disorders with no available treatment. It remains to be seen how near or distant this future lies or the potentially expanding role of medical imaging in gene therapy.
Joseph Anthony Moss, MS, is a research associate with the Center for Environmental Diagnostics and Bioremediation at the University of West Florida in Pensacola. He has worked as a molecular biologist for nearly a decade and is the author of several research articles and literature reviews involving molecular biology and microbiology. Much of his current research focuses on the detection of waterborne pathogens and the evaluation of microbial communities in the Gulf of Mexico.
Reprint requests may be mailed to the American Society of Radiologic Technologists, Communications Department, at 15000 Central Ave SE, Albuquerque, NM 87123-3909, or e-mailed to [email protected].
© 2014 American Society of Radiologic Technologists
References1. Friedmann T, Roblin R. Gene therapy for human genetic
disease? Science. 1972;175(4025):949-955. doi:10.1126 /science.175.4025.949.
2. Blaese R, Culver KW, Miller AD, et al. T lymphocyte- directed gene therapy for ADA−SCID: initial trial results after 4 years. Science. 1995;270(5235):475-480. doi:10.1126 /science.270.5235.475.
3. An overview of the human genome project. National Human Genome Research Institute Web site. http://www.genome .gov/12011238. Accessed September 11, 2013.

173
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2014, Volume 86, Number 2
Moss
4. International classification of diseases (ICD). World Health Organization Web site. http://www.who.int/classifications /icd/en/. Accessed October 12, 2013.
5. Genes and human disease. Monogenic diseases. World Health Organization Web site. http://www.who.int /genomics/public/geneticdiseases/en/index2.html. Accessed October 12, 2013.
6. Jorde LB. Genes, environment, lifestyle and common diseas-es. In: McCance KL, Huether SE, eds. Pathophysiology: The Biologic Basis for Disease in Adults and Children. 5th ed. St Louis: Elsevier Mosby; 2006:157-174.
7. Gene Therapy Clinical Trials Worldwide. John Wiley and Sons Ltd. http://www.abedia.com/wiley/. Accessed September 13, 2013.
8. Wilson JM. Is this gene therapy’s breakout moment? Genetic Engineering & Biotechology. News. http://www.geneng news.com/gen-articles/is-this-gene-therapy-s-breakout -moment/4761/. Published March 5, 2013. Accessed October 17, 2013.
9. Avril T. Children’s Hospital of Phila. funds gene therapy com-pany. Inquirer. http://articles.philly.com/2013-10-24 /news/43327514_1_gene-therapy-treatment-gene -therapy-gene-therapy-company. Published October 24, 2013. Accessed October 19, 2013.
10. Gene therapy company bluebird bio (BLUE) files $86M IPO. Street Insider.com Web site. http://www.streetinsider.com /IPOs/Gene+Therapy+Company+bluebird+bio+(BLUE) +Files+$86M+IPO/8338375.html. Published May 14, 2013. Accessed October 19, 2013.
11. Richards S. Gene therapy arrives in Europe. Scientist. http://www.the-scientist.com/?articles.view/article No/33166/title/Gene-Therapy-Arrives-in-Europe/. Published November 6, 2012. Accessed October 18, 2013.
12. Guo G, Xin H. Chinese gene therapy: splicing out the West? Science. 2006;314(5803):1232-1235.
13. Rojahn SY. When will gene therapy come to the U.S.? MIT Technology Review Web site. http://www.technologyreview.com/news/519071/when-will-gene-therapy-come-to-the-us/. Published September 30, 2013. Accessed October 15, 2013.
14. Pearson H. Genetics: what is a gene? Nature. 2006;441:398-401. doi:10.1038/441398a.
15. Pennisi E. DNA study forces rethink of what it means to be a gene. Science. 2007;316(5831):1556-1557. doi:10.1126 /science.316.5831.1556.
16. A guide to your genome. National Human Genome Research Institute. http://www.genome.gov/Pages/Education /AllAbouttheHumanGenomeProject/GuidetoYour Genome07.pdf. Published October 2007. Accessed September 19, 2013.
17. Ridley M. Genome: The Autobiography of a Species in 23 Chapters. New York, NY: HarperCollins; 2013:12-22.
18. The New Genetics. Chapter 1: How genes work. National Institute of General Medical Sciences Web site. http://publications.nigms.nih.gov/thenewgenetics/chapter1.html. Accessed October 14, 2013.
19. How do genes work? The Tech Museum of Innovation Web site. http://genetics.thetech.org/about-genetics/how-do -genes-work. Accessed October 14, 2013.
20. Gagniuc P, Ionescu-Tirgoviste C. Gene promoters show chromosome-specificity and reveal chromosome territories in humans. BMC Genomics. 2013;14:278. doi:10.1186/1471 -2164-14-278.
21. Smale ST, Kadonaga JT. The RNA polymerase II core pro-moter. Ann Rev Biochem. 2003;72: 449-479. doi:10.1146 /annurev.biochem.72.121801.161520.
22. Daugherty PS, Chen G, Iverson BL, Georgiou G. Quantitative analysis of the effect of the mutation frequency on the affinity maturation of single chain Fv antibodies. Proc Natl Acad Sci USA. 2000;97(5):2029-2034.
23. Sabour D, Schöler HR. Reprogramming and the mamma-lian germline: the Weismann barrier revisited [published online ahead of print September 1, 2012]. Curr Opin Cell Biol. 2012;24(6):716-723. doi:10.1016/j.ceb.2012.08.006.
24. MA Handel, ed. Meiosis and Gametogenesis. San Diego, CA: Academic Press; 1997:2-12.
25. Walther W, Stein U. Viral vectors for gene transfer: a review of their use in the treatment of human diseases. Drugs. 2000;60(2):249-271.
26. Peng KW. Strategies for targeting therapeutic gene delivery. Mol Med Today. 1999;5(10):448-453.
27. Ginn SL, Alexander IE, Edelstein ML, Abedi MR, Wixon J. Gene therapy clinical trials worldwide to 2012 – an update. J Gene Med. 2013;15(2):65-77. doi:10.1002/jgm.2698.
28. Campbell RS, Robinson WF. The comparative pathology of the lentiviruses. J Comp Pathol. 1998;119(4):333-395.
29. The place of retroviruses in biology. In: Coffin JM, Hughes SH, Varmus HE, eds. Retroviruses. Cold Spring Harbor, NY: Cold Spring Harbor Laboratory Press; 1997. http://www .ncbi.nlm.nih.gov/books/NBK19382/. Accessed August 22, 2014.
30. Nisole S, Saib A. Early steps of retrovirus replicative cycle. Retrovirology. 2004;1:9. doi:10.1186/1742-4690-1-9.
31. Miller AD. Principles of retroviral vector design. In: Coffin JM, Hughes SH, Varmus HE, eds. Retroviruses. Cold Spring Harbor, N.Y: Cold Spring Harbor Laboratory Press; 1997. http://www.ncbi.nlm.nih.gov/books/NBK19423/. Accessed August 22, 2014.

174
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2014, Volume 86, Number 2
Gene Therapy Review
32. Cooray S, Howe SJ, Thrasher AJ. Retrovirus and lentivirus vector design and methods of cell conditioning. Methods Enzymol. 2012;507:29-57. doi:10.1016/B978-0-12-386509 -0.00003-X.
33. Sakuma T, Barry MA, Ikeda Y. Lentiviral vectors: back to translational. Biochem J. 2012; 443(3):603-618. doi:10.1042 /BJ20120146.
34. Cartier N, Hacein-Bey-Abina S, Bartholomae CC, et al. Hematopoietic stem cell gene therapy with a lenti-viral vector in X-linked adrenoleukodystrophy. Science. 2009;326(5954):818-823.
35. Shenk TE. Adenoviridae: the viruses and their replica-tion. In: Knipe DM and Howley PM, eds. Fields Virology. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2001:2265-2300.
36. Mitani K, Kubo S. Adenovirus as an integrating vector. Curr Gene Ther. 2002;2(2):135-144.
37. Dormond E, Kamen AA. Manufacturing of adenovirus vec-tors: production and purification of helper dependent adeno-virus. Methods Mol Biol. 2011;737:139-156. doi:10.1007/978 -1-61779-095-9_6.
38. Danthinne X, Imperiale MJ. Production of first generation adenovirus vectors: a review. Gene Ther. 2000;7(20):1707-1714.
39. Alba R, Bosch A, Chillon M. Gutless adenovirus: last-gener-ation adenovirus for gene therapy. Gene Ther. 2005;12 Suppl 1:S18-S27.
40. Srivastava A, Lusby EW, Berns KI. Nucleotide sequence and organization of the adeno-associated virus 2 genome. J Virol. 1983;45(2):555-564.
41. Mori S, Wang L, Takeuchi T, Kanda T. Two novel adeno-associated viruses from cynomolgus monkey: pseudotyping characterization of capsid protein. Virology. 204;330(2):375-383. doi:10.1016/j.virol.2004.10.012.
42. Surosky RT, Urabe M, Godwin SG, et al. Adeno-associated virus Rep proteins target DNA sequences to a unique locus in the human genome. J Virol. 1979;71(10):7951-7959.
43. Kotin RM, Siniscalco M, Samulski RJ, et al. Site-specific inte-gration by adeno-associated virus. Proc Natl Acad Sci USA. 1990;87(6):2211-2215.
44. Samulski RJ, Zhu X, Xiao X, et al. Targeted integration of adeno-associated virus (AAV) into human chromosome 19. EMBO J. 1991;10(12):3941-3950.
45. Chirmule N, Propert K, Magosin S, Qian Y, Qian R, Wilson J. Immune responses to adenovirus and adeno-associated virus in humans. Gene Ther. 1999;6(9):1574-1583. doi:10.1038 /sj.gt.3300994.
46. Hernandez YJ, Wang J, Kearns WG, Loiler S, Poirier A, Flotte TR. Latent adeno-associated virus infection elicits humoral but not cell-mediated immune responses in a non-human primate model. J Virol. 1999;73(10):8549-8558.
47. Zaiss AK, Liu Q , Bowen GP, Wong NC, Bartlett JS, Muruve DA. Differential activation of innate immune responses by adenovirus and adeno-associated virus vectors. J Virol. 2002;76(9):4580-4590.
48. Ali RR, Reichel MB, Thrasher AJ, et al. Gene transfer into the mouse retina mediated by an adeno-associated viral vector. Hum Mol Genet. 1996;5(5):591-594.
49. Rabinowitz, JE, Samulski RJ. Building a better vector: the manipulation of AAV virions. Virology. 2000;278(2):301-308.
50. Gaudet D, Méthot GD, J Déry, et al. Efficacy and long-term safety of alipogene tiparvovec (AAV1-LPLS447X) gene therapy for lipoprotein lipase deficiency: an open-label trial [published online ahead of print June 21, 2012]. Gene Ther. 2013;20(4):361-9. doi:10.1038/gt.2012.43.
51. Yan Z, Zhang Y, Duan D, Engelhardt JF. Trans-splicing vec-tors expand utility of adeno-associated virus for gene therapy. Proc Natl Acad Sci USA. 2000;97(12):6716-6721.
52. Grieger JC, Choi VW, Samulski RJ. Production and char-acterization of adeno-associated viral vectors. Nat Protoc. 2006;1(3):1412-1428.
53. McClure C, Cole KLH, Wulff P, Klugmann M, Murray AJ. Production and titering of recombinant adeno-associated viral vectors. J Vis Exp. 2011;(57):e3348. doi:10.3791/3348.
54. Weitzman MD, Linden RM. Adeno-associated virus biology. Methods Mol Biol. 2011;807:1-23. doi:10.1007/978-1-61779 -370-7_1.
55. Daya S, Berns KI. Gene therapy using adeno-associated virus vectors. Clin Microbiol Rev. 2008;21(4):583-593. doi:10.1128 /CMR.00008-08.
56. Nayak S, Herzog RW. Progress and prospects: immune responses to viral vectors [published online ahead of print November 12, 2009]. Gene Ther. 2009;17(3):295-304. doi:10.1038/gt.2009.148.
57. Zhou HS, Liu DP, Liang CC. Challenges and strategies: the immune responses in gene therapy. Med Res Rev. 2004;24(6):748-761. doi:10.1002/med.20009.
58. Thrasher AJ, Gaspar HB, Baum C, et al. Gene ther-apy: X-SCID transgene leukaemogenicity. Nature. 2006;443(7109):E5-6; discussion E6-7.
59. Urnov FD, Miller JC, Lee Y-L, et al. Highly efficient endogenous human gene correction using designed zinc-finger nucleases. Nature. 2005;435:646-651. doi:10.1038/nature03556.
60. Comerota AJ, Throm RC, Miller KA, et al. Naked plas-mid DNA encoding fibroblast growth factor type 1 for the treatment of end-stage unreconstructible lower extremity ischemia: preliminary results of a phase I trial. J Vasc Surg. 2002;35(5):930-936.
61. Bloquel C, Bessis N, Boissier MC, Scherman D, Bigey P. Gene therapy of collagen-induced arthritis by electrotransfer of

175
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2014, Volume 86, Number 2
Moss
human tumor necrosis factor-alpha soluble receptor I vari-ants. Hum Gene Ther. 2004;15(2):189-201.
62. Daugimont L, Vandermeulen G, Defresne F. Antitumoral and antimetastatic effect of antiangiogenic plasmids in B16 melanoma: higher efficiency of the recombinant disintegrin domain of ADAM 15 [published online ahead of print February 18, 2011]. Eur J Pharm Biopharm. 2011;78(3):314-319. doi:10.1016/j.ejpb.2011.02.001.
63. Wolff JA, Malone RW, Williams P, et al. Direct gene transfer into mouse muscle in vivo. Science. 1990;247(4949 Pt 1):1465-1468.
64. Nikol S, Baumgartner I, Van Belle E, et al. Therapeutic angiogenesis with intramuscular NV1FGF improves ampu-tation-free survival in patients with critical limb ischemia [published online ahead of print April 1, 2008]. Mol Ther. 2008;16(5):972-978. doi:10.1038/mt.2008.33.
65. Powell RJ, Simons M, Mendelsohn FO, et al. Results of a double-blind, placebo-controlled study to assess the safety of intramuscular injection of hepatocyte growth factor plas-mid to improve limb perfusion in patients with critical limb ischemia [published online ahead of print June 16, 2008]. Circulation. 2008;118(1):58-65. doi:10.1161/CIRCULA TIONAHA.107.727347.
66. Seaman MS, Xu L, Beaudry K, et al. Multiclade human immunodeficiency virus type 1 envelope immunogens elicit broad cellular and humoral immunity in rhesus monkeys. J Virol. 2005;79(5):2956-2963.
67. Gudmundsdotter L, Sjödin A, Boström AC, et al. Therapeutic immunization for HIV [published online ahead of print October 10, 2006]. Springer Semin Immunopathol. 2006;28(3):221-230.
68. Sandstrom E, Nilsson C, Hejdeman B, et al. Broad immu-nogenicity of a multigene, multiclade HIV-1 DNA vaccine boosted with heterologous HIV-1 recombinant modified vaccinia virus Ankara. J Infect Dis. 2008;198(10):1482-1490. doi:10.1086/592507.
69. Li S, Huang L. Nonviral gene therapy: promises and chal-lenges. Gene Ther. 2000;7(1):31-34.
70. del Solar G, Giraldo R, Ruiz-Echevarría MJ, Espinosa M, Díaz-Orejas R. Replication and control of circular bacterial plasmids. Microbiol Mol Biol Rev. 1998;62(2):434-464.
71. Vivian A, Murillo J, Jackson RW. The roles of plasmids in phytopathogenic bacteria: mobile arsenals? Microbiol. 2001;147(pt 4):763-780.
72. Pinto UM, Pappas KM, Winans S. The ABCs of plasmid rep-lication and segregation. Nat Rev Microbiol. 2012;10(11):755-765. doi:10.1038/nrmicro2882.
73. Coghlan A. Souped-up immune cells force leukaemia into remission. New Scientist Web site. http://www.newscientist
.com/article/dn22613-soupedup-immune-cells-force-leuka emia-into-remission.html. Published December 11, 2012. Accessed October 20, 2013.
74. Anklesaria P. Gene therapy: a molecular approach to cancer treatment. Curr Opin Mol Ther. 2000;2(4):426-432.
75. Duarte S, Carle G, Faneca H, de Lima MC, Pierrefite-Carle V. Suicide gene therapy in cancer: where do we stand now? [published online ahead of print May 24, 2012]. Cancer Lett. 2012;324(2):160-170. doi:10.1016/j.can-let.2012.05.023.
76. Kong H, Huang ZH, Li Q , Yang LC, Yu JL, Li Z. Adenovirus-mediated double suicide gene selectively kills breast cancer MCF-7 cells in vitro. Nan Fang Yi Ke Da Xue Xue Bao. 2008;28(6):907-910.
77. Preuss E, Muil A, Weber K, Otte J, von Laer D, Fehse B. Cancer suicide gene therapy with TK.007: superior killing efficiency and bystander effect [published online ahead of print June 23, 2011]. J Mol Med. 2011;89(11):1113-1124. doi:10.1007/s00109-011-0777-8.
78. Okino T, Onda M, Matsukura N, et al. Sequential histopatho-logical changes in vivo after suicide gene therapy of gastric cancer induced by N-methyl-N’-nitro-N-nitrosoguanidine in rats. Jpn J Cancer Res. 2001;92(6):673-679.
79. Wan LB, Parysek LM, Warnick R, Stambrook PJ. In vitro evidence that metabolic cooperation is responsible for the bystander effect observed with HSV tk retroviral gene thera-py. Human Gene Therapy. 1993;4(6):725-731. doi:10.1089 /hum.1993.4.6-725.
80. Kanazawa T, Mizukami H, Okada T, et al. Suicide gene therapy using AAV-HSVtk/ganciclovir in combination with irradiation results in regression of human head and neck cancer xenografts in nude mice. Gene Ther. 2003;10(1):51-58. doi:10.1038/sj.gt.3301837.
81. Greco O, Dachs GU. Gene directed enzyme/prodrug therapy of cancer: historical appraisal and future prospectives. J Cell Physiol. 2001;187(1):22-36.
82. Nicholas TW, Read SB, Burrows FJ, Kruse CA. Suicide gene therapy with Herpes simplex virus thymidine kinase and gan-ciclovir is enhanced with connexins to improve gap junctions and bystander effects. Histol Histopathol. 2003;18(2): 495-507.
83. Balzarini J, Bohman C, De Clercq E. Differential mechanism of cytostatic effect of (E)-5-(2-bromovinyl)-2-deoxyuridine, 9-(1,3-dihydroxy-2-propoxymethyl)guanine, and other anti-herpetic drugs on tumor cells transfected by the thymidine kinase gene of herpes simplex virus type 1 or type 2. J Biol Chem. 1993;268(9):6332-6337.
84. Springer CJ, Niculescu-Duvaz I. Prodrug-activating systems in suicide gene therapy. J Clin Invest. 2000;105(9):1161-1167. doi:10.1172/JCI10001.

176
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2014, Volume 86, Number 2
Gene Therapy Review
85. Culver KW, Ram Z, Wallbridge S, Ishii H, Oldfield EH, Blaese RM. In vivo gene transfer with retroviral vector-producer cells for treatment of experimental brain tumors. Science. 1992;256(5063):1550-1552.
86. Freeman SM, Abboud CN, Whartenby KA, et al. The “bystander effect”: tumor regression when a fraction of the tumor mass is genetically modified. Cancer Res. 53(21):5274-5283.
87. Malecki M. Frontiers in suicide gene therapy of cancer. J Genet Syndr Gene Ther. 2012; 2012(3). pii: e114.
88. Coghlan A. Gene therapy cures leukaemia in eight days. The New Scientist Web site. http://www.newscientist.com /article/mg21729104.100-gene-therapy-cures-leukaemia-in -eight-days.html. Published March 26, 2103. Accessed April 15, 2013.
89. Wen PY, Kesari S. Malignant gliomas in adults. New Engl J Med. 2008;359:492-507. doi:10.1056/NEJMra0708126.
90. Tobias A, Ahmed A, Moon KS, Lesniak MS. The art of gene therapy for glioma: a review of the challenging road to the bedside [published online ahead of print September 19, 2012]. J Neurol Neurosurg Psychiatry. 2013;84(2):213-222. doi:10.1136/jnnp-2012-302946.
91. Kroeger KM, Muhammad AK, Baker GJ, et al. Gene therapy and virotherapy: novel therapeutic approaches for brain tumors. Discov Med. 2010;10(53):293-304.
92. Iwami K, Natsume A, Wakabayashi T. Gene therapy for high-grade glioma. Neurol Med Chir (Tokyo). 2010;50(9):727-736.
93. Bansal K, Engelhard HH. Gene therapy for brain tumors. Curr Oncol Rep. 2000;2(5):463-472.
94. Roth JA, Cristiano RJ. Gene therapy for cancer: what have we done and where are we going? J Natl Cancer Inst. 1997;89(1):21-39.
95. Go AS, Mozaffarian D, Roger VL, et al. Executive sum-mary: heart disease and stroke statistics – 2013 update: a report from the American Heart Association. Circulation. 2013;127(1):143-152. doi:10.1161/CIR.0b013e318282ab8f.
96. Jessup M, Greenberg B, Mancini D, et al. Calcium upregu-lation by percutaneous administration of gene therapy in cardiac disease (CUPID): a phase 2 trial of intracoronary gene therapy of sarcoplasmic reticulum ca2+-ATPase in patients with advanced heart failure [published online ahead of print June 27, 2011]. Circulation. 2011;124(3):304-313. doi:10.1161/CIRCULATIONAHA.111.022889.
97. Penn MS, Mendelsohn FO, Schaer GL, et al. An open-label dose escalation study to evaluate the safety of administra-tion of nonviral stromal cell-derived factor-1 plasmid to treat symptomatic ischemic heart failure [published online ahead of print February 21, 2013]. Circ Res. 2013;112(5):816-825. doi:10.1161/CIRCRESAHA.111.300440.
98. Rebolledo B, Lai NC, Gao MH, et al. Adenylylcyclase gene transfer increases function of the failing heart. Hum Gene Ther. 2006;17(10):1043-1048.
99. Roth DM, Bayat H, Drumm JD, et al. Adenylyl cyclase increases survival in cardiomyopathy. Circulation. 2002;105(16):1989-1994.
100. Takahashi T, Tang T, Lai NC, et al. Increased cardiac adeny-lyl cyclase expression is associated with increased survival after myocardial infarction [published online ahead of print July 24, 2006]. Circulation. 2006;114(5):388-396.
101. Williams ML, Hata JA, Schroder J, et al. Targeted beta-adrenergic receptor kinase (betaARK1) inhibition by gene transfer in failing human hearts [published online ahead of print March 29, 2004]. Circulation. 2004;109(13):1590-1593.
102. Finegold JA, Asaria P, Francis DP. Mortality from ischaemic heart disease by country, region, and age: statistics from World Health Organisation and United Nations [published online ahead of print December 4, 2012]. Int J Cardiol. 2012;168(2):934-945. doi:10.1016/j.ijcard.2012.10.046.
103. Li J, Wei Y, Liu K, et al. Synergistic effects of FGF-2 and PDGF-BB on angiogenesis and muscle regeneration in rabbit hindlimb ischemia model [published online ahead of print January 4, 2010]. Microvasc Res. 2010;80(1):10-17. doi:10.1016/j.mvr.2009.12.002.
104. Kilian EG, Sadoni S, Vicol C, et al. Myocardial transfection of hypoxia inducible factor-1 alpha via an adenoviral vector during coronary artery bypass grafting: a multicenter phase I and safety study [published online ahead of print March 10, 2010]. Circ J. 2010;74(5):916-924. doi:10.1253/circj .CJ-09-0594.
105. Yang ZJ, Chen B, Sheng Z, et al. Improvement of heart function in postinfarct heart failure swine models after hepatocyte growth factor gene transfer: comparison of low-, medium- and high-dose groups [published online ahead of print August 13, 2009]. Mol Biol Rep. 2010;37(4):2075-2081. doi:10.1007/s11033-009-9665-5.
106. Jin YN, Inubushi M, Masamoto K, et al. Long-term effects of hepatocyte growth factor gene therapy in rat myocardial infarct model [published online ahead of print September 15, 2011]. Gene Ther. 2012;19(8):836-843. doi:10.1038 /gt.2011.128.
107. Rosengart TK, Patel SR, Crystal RG. Therapeutic angiogen-esis: protein and gene therapy delivery strategies. J Cardiovasc Risk. 1999;6(1):29-40.
108. Symes JF, Losordo DW, Vale PR, et al. Gene therapy with vascular endothelial growth factor for inoperable coronary artery disease. Ann Thorac Surg. 1999;68(3):830-836.
109. Mattick P, Parrington J, Odia E, Simpson A, Collins T, Terrar D. Ca2+-stimulated adenylyl cyclase isoform AC1 is

177
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2014, Volume 86, Number 2
Moss
preferentially expressed in guinea-pig sino-atrial node cells and modulates the I(f) pacemaker current [published online ahead of print May 31, 2007]. J Physiol. 2007;582 (Pt 3):1195-1203.
110. Ruhparwar A, Kallenbach K, Klein G, et al. Adenylate-cyclase VI transforms ventricular cardiomyocytes into bio-logical pacemaker cells. Tissue Eng Part A. 2010;16(6):1867-1872. doi:10.1089/ten.tea.2009.0537.
111. Boink GJ, Duan L, Nearing BD, et al. HCN2/SkM1 gene transfer into canine left bundle branch induces stable, auto-nomically responsive biological pacing at physiological heart rates [published online ahead of print February 6, 2013]. J Am Coll Cardiol. 2013;61(11):1192-1201. doi:10.1016/j .jacc.2012.12.031.
112. Pawlyk BS, Smith AJ, Buch PK, et al. Gene replacement therapy rescues photoreceptor degeneration in a murine model of Leber congenital amaurosis lacking RPGRIP. Invest Ophthalmol Vis Sci. 2005;46(9):3039-3045.
113. Pang JJ, Chang B, Kumar A, et al. Gene therapy restores vision-dependent behavior as well as retinal structure and function in a mouse model of RPE65 Leber congenital amaurosis [published online ahead of print October 11, 2005]. Mol Ther. 2006;13(3):565-572.
114. Tschernutter M, Schlichtenbrede FC, Howe S, et al. Long-term preservation of retinal function in the RCS rat model of retinitis pigmentosa following lentivirus-mediated gene therapy. Gene Ther. 2005;12(8):694-701. doi:10.1038 /sj.gt.3302460.
115. Gene therapy clinical trials underway for Stargardt disease and AMD. Foundation Fighting Blindness Web site. http://www.blindness.org/index.php?option=com_content&view=article&id=2719%3Agene-therapy-clin ical-trials-underway-for-stargardt-disease-and-amd &catid=66%3Astargardt-disease&Itemid=122. Published June 22, 2011. Accessed August 25, 2014.
116. What is macular degeneration: Stargardt disease. American Macular Degeneration Foundation Web site. https://www.macular.org/stargardt-disease. Accessed August 21, 2014.
117. Bainbridge JW, Smith AJ, Barker SS, et al. Effect of gene therapy on visual function in Leber’s congenital amauro-sis. N Engl J Med. 2008;358:2231-2239. doi:10.1056/NEJ Moa0802268.
118. Maguire AM, Simonelli F, Pierce EA. Safety and effi-cacy of gene transfer for Leber’s amaurosis. N Engl J Med. 2008;358:2240-2248. doi:10.1056/NEJMoa0802315.
119. Foundation for Retinal Research (FRR). Gene Mutations that Cause LCA. http://www.tfrr.org/index.php/about -lca/113-nike-free-run-2-0-id-odio-vestibulum. Accessed September 21, 2013.
120. Gosh P. Gene therapy first for poor sight. BBC News Web site. http://news.bbc.co.uk/2/hi/health/6609205.stm. Published May 1, 2007. Accessed October 21, 2013.
121. Maguire AM, High KA, Auricchio A, et al. Age-dependent effects of RPE65 gene therapy for Leber’s congenital amau-rosis: a phase 1 dose-escalation trial [published online ahead of print October 23, 2009]. Lancet. 2009;374(9701):1597-1605. doi:10.1016/S0140-6736(09)61836-5.
122. Bennett JM, Ashtari M, Wellman J, et al. AAV2 gene ther-apy readministration in three adults with congenital blind-ness. Sci Transl Med. 2012;4(120):120ra15. doi:10.1126 /scitranslmed.3002865.
123. Facts about Down syndrome. Centers for Disease Control and Prevention Web site. http://www.cdc.gov/ncbddd /birthdefects/DownSyndrome.html. Updated August 7, 2014. Accessed October 6, 2014.
124. Jiang J, Jing Y, Cost GJ, et al. Translating dosage compensa-tion to trisomy 21 [published online ahead of print July 17, 2013]. Nature. 2013;500:296-300. http://dx.doi.org /10.1038/nature12394.
125. Li LB, Chang KH, Wang PR, Hirata RK, Papayannopoulou T, Russell DW. Trisomy correction in Down syndrome induced pluripotent stem cells [published online ahead of print October 18, 2012]. Cell Stem Cell. 2012;11(5):615-619. doi:10.1016/j.stem.2012.08.004.
126. Rush University Medical Center and UCSF research-ers found gene therapy appeared to reduce symptoms of Parkinson’s disease by 40 percent [press release]. Chicago, IL: Rush University Medical Center; October 16, 2006. http://www.rush.edu/webapps/MEDREL/servlet/News Release?ID=802. Accessed August 19, 2014.
127. Muramatsu S, Fujimoto K, Kato S, et al. A phase I study of aromatic L-amino acid decarboxylase gene therapy for Parkinson’s disease [published online ahead of print July 6, 2010]. Mol Ther. 2010;18(9):1731-1735. doi:10.1038/mt .2010.135.
128. During MJ, Feigin A, Eidelberg D, et al. Subthalamic GAD gene transfer improves brain metabolism associated with clinical recovery in Parkinson’s disease. Abstracts from Neuroscience 2006: The 36th Annual Meeting of the Society for Neuroscience; No. 510.9.
129. Garg SK, Lioy DT, Cheval H, et al. Systemic deliv-ery of MeCP2 rescues behavioral and cellular deficits in female mouse models of Rett syndrome. Neurosci. 2013;33(34):13612-136120. doi:10.1523/JNEURO SCI.1854-13.2013.
130. Murray P. Scientists cure diabetes with gene therapy in dogs – will it work on humans? SinglularityHUB Web site. http://singularityhub.com/2013/03/06/scientists-cure -diabetes-with-gene-therapy-in-dogs-will-it-work-on

178
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2014, Volume 86, Number 2
Gene Therapy Review
-humans/. Published March 6, 2013. Accessed October 14, 2013.
131. Callejas D, Mann CJ, Ayuso E, et al. Treatment of diabe-tes and long-term survival after insulin and glucokinase gene therapy [published online ahead of print February 1, 2013]. Diabetes. 2013;62(5):1718-1729. doi:10.2337/db12-1113.
132. What is molecular imaging? UC Davis Biomedical Engineering Web site. http://bme.ucdavis.edu/cmgi/over view-2/what-is-molecular-imaging/. Accessed August 25, 2014.
133. Catana C, Guimaraes AR, Rosen BR. PET and MRI: The odd couple or a match made in heaven? J Nucl Med. 2013; 54(5):815-824.
134. Högemann-Savellano D, Bos E, Blondet C, et al. The trans-ferrin receptor: a potential molecular imaging marker for human cancer. Neoplasia. 2003;5(6):495-506.
135. Ichikawa T, Högemanny D, Saeki Y, et al. 2002. MRI of transgene expression: correlation to therapeutic gene expression. Neoplasia. 2002;4(6):523-530. doi:10.1038 /sj.neo.7900266.
136. Sherry AD, Woods M. Chemical exchange saturation trans-fer contrast agents for magnetic resonance imaging. Annu Rev Biomed Eng. 2008;10:391-411. doi:10.1146/annurev.bio eng.9.060906.151929.
137. Hingorani DV, Randtke EA, Pagel MD. A catalyCEST MRI contrast agent that detects the enzyme catalyzed creation of a covalent bond. J Am Chem Soc. 2013;135(17):6396-6398. doi:10.1021/ja400254e.
138. Gilad AA, Ziv K, McMah MT, et al. MRI reporter genes. J Nuc Med. 2008;49:1905-1908. doi:10.2967/jnumed .108.053520.
139. Liu G, Gilad, AA. MRI of CEST-based reporter gene. Meth Mol Biol. 2011;771:733-746. doi:10.1007/978-1-61779-219 -9_36.
140. Radiopharmaceuticals for cancer imaging: nature, mecha-nisms of localization, and molecular targets. In: Ell PJ, Gambhir SS, eds. Nuclear Medicine in Clinical Diagnosis and Treatment. 3rd ed. London, UK: Churchill Livingstone; 2004.
141. Chuang K, Cheng T. Noninvasive imaging of reporter gene expression and distribution in vivo. Fooyin J Health Sci. 2010;2(1):1-11. doi:10.1016/S1877-8607(10)60007-0.
142. Min JJ, Gambhir SS. Molecular imaging of PET reporter gene expression. Handb Exp Pharmacol. 2008;(185 Pt 2): 277-303. doi:10.1007/978-3-540-77496-9_12.
143. Fechheimer M, Boylan JF, Parker S, Sisken JE, Patel GL, Zimmer SG. Transfection of mammalian cells with plasmid DNA by scrape loading and sonication loading. Proc Natl Acad Sci USA. 1987;84(23):8463-8467.
144. Davis HL, Whalen RG, Demeneix BA. Direct gene transfer into skeletal muscle in vivo: factors affecting efficiency of transfer and stability of expression. Hum Gene Ther. 1993;4(2):151-159.
145. Unger EC, McCreery TP, Sweitzer RH. Ultrasound enhanc-es gene expression of liposomal transfection. Invest Radiol. 1997;32(12):723-727.
146. Rizzuto G, Cappelletti M, Maione D, et al. Efficient and regulated erythropoietin production by naked DNA injec-tion and muscle electroporation. Proc Natl Acad Sci USA. 1999;96(11):6417-6422.
147. Huber PE, Pfisterer P. In vitro and in vivo transfection of plasmid DNA in the Dunning prostate tumor R3327-AT1 is enhanced by focused ultrasound. Gene Ther. 2000;7(17):1516-1525.
148. Daud AI, DeConti RC, Andrews S, et al. Phase I trial of interleukin-12 plasmid electroporation in patients with metastatic melanoma [published online ahead of print November 24, 2008]. J Clin Oncol. 2008; 26(36):5896-5903. doi:10.1200/JCO.2007.15.6794.
149. Takeuchi D, Sato N, Shimamura M, et al. Alleviation of Abeta-induced cognitive impairment by ultrasound-mediated gene transfer of HGF in a mouse model [pub-lished online ahead of print February 21, 2008]. Gene Ther. 2008;15(8):561-571. doi:10.1038/sj.gt.3303094.
150. Ziadloo A, Jianwu X, Frenkel V. Pulsed focused ultra-sound exposures enhance locally administered gene therapy in a murine solid tumor model. J Acoust Soc Am. 2013;133(3):1827-1834. doi:10.1121/1.4789390.
151. Wang DS, Panje C, Pysz MA, et al. Cationic versus neutral microbubbles for ultrasound-mediated gene delivery in cancer [published online ahead of print June 21, 2012]. Radiology. 2012;264(3):721-732. doi:10.1148/radiol .12112368.
152. Guo DP, Li XY, Sun P, et al. Ultrasound-targeted microbub-ble destruction improves the low density lipoprotein recep-tor gene expression in HepG2 cells [published online ahead of print March 10, 2006]. Biochem Biophys Res Commun. 2006;343(2):470-474.
153. Zhou QH, Miller DL, Carlisle RC, Seymour LW, Oupicky D. Ultrasound-enhanced transfection activity of HPMA-stabilized DNA polyplexes with prolonged plasma circula-tion. J Control Release. 2005;106(3):416-427.
154. Rahim AA, Taylor SL, Bush NL, ter Haar GR, Bamber JC, Porter CD. Physical parameters affecting ultrasound/microbubble-mediated gene delivery efficiency in vitro. Ultrasound Med Biol. 2006;32(8):1269-1279.
155. Pislaru SV, Pislaru C, Kinnick RR, et al. Optimization of ultrasound-mediated gene transfer: comparison
179
CEDirected Reading
RADIOLOGIC TECHNOLOGY, November/December 2014, Volume 86, Number 2
Moss
of contrast agents and ultrasound modalities. Eur Heart J. 2003;24(18):1690-1698. doi:10.1016/S0195 -668X(03)00469-X.
156. Guo DP, Li XY, Sun P, et al. Ultrasound/microbubble enhances foreign gene expression in ECV304 cells and murine myocardium. Acta Biochim Biophys Sin. 2004;36(12):824-831.
157. Sakakima Y, Hayashi S, Yagi Y, Hayakawa A, Tachibana K, Nakao A. Gene therapy for hepatocellular carcinoma using sonoporation enhanced by contrast agents. Cancer Gene Ther. 2005;12(11):884-889.
158. Awad HA, Zhang X, Reynolds DG, Guldbuerg RE, O’Keefe RJ, Schwarz EM. Recent advances in gene delivery for struc-tural bone allografts. Tissue Eng. 2007;13(8):1973-1985.
159. Zachos TA, Weisbrode SE, Bertone AL. Mesenchymal stem cell-mediated gene delivery of bone morphogenetic protein-2 in alginate in an articular fracture model. Mol Ther. 2006;13:S400-S400. doi:10.1016/j.ymthe.2006 .08.1140.
160. Rodt T, von Falck C, Dettmer S, et al. Micro-computed tomography of pulmonary fibrosis in mice induced by adenoviral gene transfer of biologically active transforming growth factor-1. Resp Res. 2010;11:181-189.
161. Waddill W 3rd, Wright W, Unger E, et al. Human gene therapy for melanoma: CT-guided interstitial injection. AJR Am J Roentgenol. 1997;169(1):63-67.
162. Schmidt E. UCLA radiologists use CT-scans to inject gene therapy into tumors; method could improve cancer patients’ survival rate. UCLA Newsroom Web site. http://newsroom.ucla.edu/portal/ucla/UCLA-Radiologists-Use-CT-Scans -5156.aspx. Published May 4, 2004. Accessed November 26, 2013.
163. Hall FL, Levy JP, Reed RA, et al. Pathotropic targeting advances clinical oncology: tumor-targeted localization of therapeutic gene delivery. Oncol Rep. 2010;24(4):829-833.
164. Dross. Correlating gene expression with CT scan imaging [online forum]. CancerFocus Web site. http://cancerfocus .net/correlating_gene_expression_with_ct_scan_imaging /45. Published May 22, 2007. Accessed November 24, 2013.
165. Maran A, Khosla S, Riggs BL, Zhang M, Ritman EL, Turner RT. Measurement of gene expression following cryo-genic mu-CT scanning of human iliac crest biopsies. J Musculoskelet Neuron Interact. 2003;3(1):83-88.
166. Benedetti S, Pirola B, Pollo B, et al. Gene therapy of experi-mental brain tumors using neural progenitor cells. Nat Med. 2000;6(4):447-450. doi:10.1038/74710.
167. Jacobs A, Voges J, Reszka R, et al. Positron-emission tomography of vector-mediated gene expression in gene therapy for gliomas. Lancet. 2001;358(9283):727-729.
168. Beyer T, Townsend DW, Blodgett TM. Dual-modality PET/CT tomography for clinical oncology. Q J Nucl Med. 2002;46:24-34.
169. Rodriguez-Porcel M, Brinton TJ, Chen IY, et al. Reporter gene imaging following percutaneous delivery in swine moving toward clinical applications. J Am Coll Cardiol. 2008;51(5):595-597. doi:10.1016/j.jacc.2007.08.063.
170. Louie AY, Hüber MM, Ahrens ET, et al. In vivo visualization of gene expression using magnetic resonance imaging. Nat Biotechnol. 2000;18:321-325. doi:10.1038/73780.
171. Weissleder R, Moore A, Mahmood U, et al. In vivo mag-netic resonance imaging of transgene expression. Nat Med. 2000;6(3):351-355.
172. Genove G, DeMarco U, Xu H, Goins WF, Ahrens ET. A new transgene reporter for in vivo magnetic resonance imaging [published online ahead of print March 20, 2005]. Nat Med. 2005;11(4):450-454. doi:10.1038/nm1208.
173. Bar-Shir A, Lui G, MM Greenberg, Bulte JW, Gilad AA. Synthesis of a probe for monitoring HSV1-tk reporter gene expression using chemical exchange saturation transfer MRI [published online ahead of print October 31, 2013]. Nat Protoc. 2013;8(12):2380-2391. doi:10.1038 /nprot.2013 .140.
174. Rehemtulla A, Hall DE, Stegman LD, et al. Molecular imag-ing of gene expression and efficacy following adenoviral-mediated tumor gene therapy. Mol Imaging. 2002;1:43-55.
175. Kristensen CA, Askenasy N, Jain RK, Koretsky AP. Creatine and cyclocreatine treatment of human colon ade-nocarcinoma xenografts: 31P and 1H magnetic resonance spectroscopic studies. Br J Cancer. 1999;79(2):278-285. doi:10.1038/sj.bjc.6690045.
176. Biffi B, Montini E, Lorioli L, et al. Lentiviral hematopoietic stem cell gene therapy benefits metachromatic leukodystro-phy [published online ahead of print July 11, 2013]. Science. 2013;341(6148): 1233158. doi:10.1126/science.1233158.
177. Whiteman H. Brain cancer: ground breaking MRI-guided gene therapy. Medical News Today Web site. http://www .medicalnewstoday.com/articles/264500.php. Published August 8, 2013. Accessed November 4, 2013.
178. Innovative MRI scan monitors cancer gene therapy. The Institute of Cancer Research Web site. http://www.icr .ac.uk/research/new_research_highlights/research_high lights/24036.shtml. Published September 26, 2013. Accessed November 19, 2013.
179. Bergeson ER. The ethics of gene therapy. http://www.ndsu .edu/pubweb/~mcclean/plsc431/students/bergeson.htm. Accessed September 30, 2014.
180. Fletcher JC. Evolution of ethical debate about human gene therapy. Hum Gene Ther. 1990;1(1):55-68.
180 RADIOLOGIC TECHNOLOGY, November/December 2014, Volume 86, Number 2
Gene Therapy Review
181. Walters L. Human gene therapy: ethics and public policy. Hum Gene Ther. 1991;2(2):115-122.
182. Wilson JM. Bulls, bubbles, and biotech. Hum Gene Ther. 2013;24(8):715-716. doi:10.1089/hum.2013.2509.
183. Hudson J, Orviska M. European attitudes to gene therapy and pharmacogenetics. Drug Discovery Today. 2011;16 (19-20):843-847. doi:10.1016/j.drudis.2011.06.008.
184. Condit CM. Public attitudes and beliefs about genet-ics. Annu Rev Genomics Hum Genet. 2010;11: 339-359. doi:10.1146/annurev-genom-082509-141740.
185. Gene therapy for cancer. GeoSalud Web site. http://www .geosalud.com/gene_therapy/cancer.html. Accessed October 6, 2014.
186. WADA gene doping. World Anti-Doping Agency Web site. https://elb.wada-ama.org/en/what-we-do/science-medical/. Accessed October 14, 2013.
187. Policy, legal and ethical issues in genetic research. National Human Genome Research Institute Web site. http://www .genome.gov/Issues/. Accessed November 8, 2013.
188. Report of the committee on the ethics of gene therapy (Cecil Clothier, chair). Hum Gene Ther. 1992:3(5):519-523.
189. Raper SE, Chirmule N, Lee FS, et al. Fatal systemic inflam-matory response syndrome in a ornithine transcarbamylase deficient patient following adenoviral gene transfer. Mol Genet Metab. 2003;80(1-2):148-158.
190. Hacein-Bey-Abina S, von Kalle C, Schmidt M, et al. A serious adverse event after successful gene therapy for X-linked severe combined immunodeficiency. N Engl J Med. 2003;348:255-256. doi:10.1056/NEJM200301163480314.
191. Frank KM, Hogarth DK, Miller JL, et al. Investigation of the cause of death in a gene-therapy trial. N Engl J Med. 2009;361:161-169. doi:10.1056/NEJMoa0801066.
192. Determine which review body approvals are required. Health Research Authority Web site. http://www.hra.nhs .uk/research-community/before-you-apply/determine -which-review-body-approvals-are-required/. Accessed October 3, 2014.
193. Advanced-therapy medicinal products. European Medicines Agency Web site. http://www.ema.europa.eu /ema/index .jsp?curl=pages/regulation/general/general _content_000294.jsp&mid=WC0b01ac05800241e0. Accessed October 3, 2014.
194. Code of Federal Regulations (annual edition). http://www.gpo.gov/fdsys/browse/collectionCfr.action ?collectionCode=CFR. Accessed October 20, 2013.
195. Code of Federal Regulations Title 45 Public Welfare Department of Health and Human Services Part 46 Protection of Human Subjects. U.S. Department of Health and Human Services. http://www.hhs.gov/ohrp/human
subjects/guidance/45cfr46.html. Accessed October 20, 2013.
196. Wolf SM, Gupta R, Kohlhepp P. Gene therapy over-sight: lessons for nanobiotechnology. J Law Med Ethics. 2009;37(4):659-684. doi:10.1111/j.1748-720X .2009.00439.x.
197. Gaffney A. Safety main challenge to preparing INDs for cellular and gene therapy products, says FDA. Regulatory Affairs Professional Society Web site. http://www.raps.org /focus-online/news/news-article-view/article/3734/safety -main-challenge-to-preparing-inds-for-cellular-and-gene -therapy-products.aspx. Published July 3, 2013. Accessed September 14, 2013.
CEDirected Reading

181RADIOLOGIC TECHNOLOGY, November/December 2014, Volume 86, Number 2
Directed Reading Quiz
continued on next page
Gene Therapy Review
1. The United States and ______ account for most gene therapy trials worldwide, and most trials focus on ______.a. Canada; HIV/AIDS b. Europe; cancerc. Europe; Parkinson diseased. Canada; noninherited diseases
2. The first European Union–approved gene therapy product was developed to treat:a. smallpox. b. Huntington disease.c. lipoprotein lipase deficiency.d. retinitis pigmentosa.
3. Which of the following diseases was first targeted for genetic therapeutic trials?a. AIDS b. adenosine deaminase deficiencyc. Parkinson diseased. retinitis pigmentosa
4. Which country was first to approve a gene therapy product for clinical use?a. United States b. United Kingdomc. Chinad. Germany
5. The chemical building blocks of DNA comprise:a. amino acids.b. adenine, guanine, cytosine, and thymine.c. RNA and simple proteins.d. complex proteins.
6. A gene’s DNA sequence or code is arranged in a string of nucleotide triplets known as:a. codons. b. bases.c. micro-RNA.d. alleles.
Read the preceding Directed Reading and choose the answer that is most correct based on the article.
Renewed through Jan. 1, 2020*
To earn continuing education credit: Take this Directed Reading quiz online at asrt.org/drquiz. Or, transfer your responses to the answer sheet on Page 186 and mail to:
Processing Center, 2908 Stewart Creek Blvd., Charlotte, NC 28216.
New and rejoining members are ineligible to take DRs from journal issues published prior to their most recent join date unless they have purchased access to the quiz from the ASRT. To purchase access to other quizzes, go to asrt.org/store.
* Your answer sheet for this Directed Reading must be received in the ASRT office on or before this date. Some quizzes are renewed and the expiration date extended. Check online at asrt.org/drquiz or call Member Services at 800-444-2778.
14806-01 2.0 Category A+ creditsOriginal Expiration Date: Oct. 31, 2016*Approved by MDCB. Check MDCB.org for details.

RADIOLOGIC TECHNOLOGY, November/December 2014, Volume 86, Number 2
Directed Reading Quiz
continued on next page
182
7. Before translation into proteins, DNA normally is:a. modified into alleles.b. transcribed into vectors.
c. transcribed into messenger RNA.d. amplified via polymerase chain reaction.
8. Which of the following statements is not true about germ-line theory?a. It is based on the Weismann theory of heredity. b. Therapeutic alteration of germ cells cannot be
passed on to a descendant.c. Inheritable characteristics are passed on by
reproductive cells.d. Reproductive cells include ova and sperm.
9. A gene delivery approach in which the therapeutic gene is administered directly into the patient via injection or intravenously is known as an ______ approach.a. in vitro b. ex vivoc. in vivod. intra vivo
10. What are the 2 main categories of therapeutic gene delivery?a. somatic and plasmidb. viral and nonviralc. plasmid and germ line d. gene-gun and ultrasound
11. Approximately how many gene therapy trials have been approved to date?a. 250b. 200c. 2100d. 22 000
12. The following is not among the commonly used viral vectors for gene therapy.a. adenovirus b. adeno-associated virusc. amur virusd. retrovirus
13. Lentiviruses and retroviruses both have a ______ genome.a. single-stranded RNAb. single-stranded DNAc. double-stranded RNAd. double-stranded DNA
14. A main difference between retroviral and lentiviral vectors is the fact that lentiviral virus vectors can infect ______ cells.a. only mitotically active b. both mitotically active and quiescentc. only somaticd. both somatic and germ-line
15. The adeno-associated virus genome consists of a:a. single-stranded RNA.b. single-stranded DNA.c. double-stranded RNA.d. double-stranded DNA.
16. Which of the following statements is true regarding the lytic pathway of a viral vector life cycle?a. The lytic pathway is the only pathway a viral
vector can follow once it enters a target cell’s nucleus.
b. The virus transmits DNA directly into a region of chromosome 19.
c. Once attached and infecting the target cell, the virus makes copies.
d. The lytic pathway does not develop in cells infected with a helper virus.

RADIOLOGIC TECHNOLOGY, November/December 2014, Volume 86, Number 2
Directed Reading Quiz
continued on next page
183
17. Which of the following might be a risk associated with use of viral vectors?
1. potential infection of healthy cells 2. preexisting, inherent immunity 3. low yield and purity
a. 1 and 2b. 1 and 3c. 2 and 3d. 1, 2, and 3
18. A gene that is overexpressed can:a. insert DNA in the wrong location.b. produce too much of the necessary protein.c. produce no protein.d. produce the incorrect protein.
19. Plasmids are most often found in:a. cells of patients who have bleeding disorders.b. liver cells.c. somatic cells.d. archaea and bacteria.
20. Plasmids are natural and cannot be made artificially. a. true b. false
21. Which of the following factors are a complication associated with use of a nonviral vector?
1. limited transgenic transcription2. limited size of gene insert3. electrostatic repulsion at cell surface
a. 1 and 2b. 1 and 3c. 2 and 3d. 1, 2, and 3
22. Which of the following is an example of a monogenic disorder?a. hepatitis Cb. spina bifidac. cystic fibrosisd. retinitis pigmentosa
23. Clinical trials have shown that gene therapy can restore vision in some patients who have a congenital mutation to the point that the patients are declassified as legally blind.a. trueb. false
24. In vitro experiments have been successful in using stem cells to naturally remove the third copy of chromosome 21 in individuals who have:a. spina bifida.b. muscular dystrophy.c. hydrocephalus.d. Down syndrome.
25. A covalent bond refers to:a. sharing of electrons between compounds.b. sharing of proteins between cells.c. bond splitting.d. iron-based transfer.
26. Ideally, characteristics of reporter genes should include:
1. a fit into the selected vectors. 2. inability to induce immune response.3. stability and lack of cytotoxicity.
a. 1 and 2b. 1 and 3c. 2 and 3d. 1, 2, and 3

RADIOLOGIC TECHNOLOGY, November/December 2014, Volume 86, Number 2
Directed Reading Quiz
184
27. Exposure of cells to ultrasound waves increases:a. resolution of viral vectors.b. viral vector tropism.c. membrane permeability.d. transcription.
28. According to the article, computed tomography (CT) imaging has been used in human trials to:
1. evaluate progression of pulmonary fibrosis following administration of an adenoviral gene vector.
2. guide intratumoral injection of plasmid DNA for treating melanoma.
3. steer gene-therapy injections into tumors of patients with metastatic kidney cancer.
a. 1 and 2b. 1 and 3c. 2 and 3d. 1, 2, and 3
29. In gene therapy, ______ is a noninvasive tool for diagnosing the pathology, biology, and safety of vectors.a. ultrasonographyb. CTc. magnetic resonance imagingd. positron emission tomography
30. In the United States, a manufacturer considering developing and selling a gene therapy product must first inform the:a. Gene Therapy Advisory Committee.b. U.S. Food and Drug Administration.c. National Institutes of Health.d. Institutional Review Board.