general surgeon workforce in tennessee in the era of the affordable care act
TRANSCRIPT
ww.sciencedirect.com
j o u r n a l o f s u r g i c a l r e s e a r c h 1 8 4 ( 2 0 1 3 ) 2 6e3 0
Available online at w
journal homepage: www.JournalofSurgicalResearch.com
Association for Academic Surgery
General surgeon workforce in Tennessee in the era of theAffordable Care Act
Michael G. Jerkins, BA, MEd, Ben L. Zarzaur, MD, MPH,* and Timothy C. Fabian, MD
The Department of Surgery, University of Tennessee Health Science Center, Memphis, Tennessee
a r t i c l e i n f o
Article history:
Received 5 January 2013
Received in revised form
12 April 2013
Accepted 1 May 2013
Available online 23 May 2013
Keywords:
Surgeon workforce
Affordable Care Act
Health care reform
* Corresponding author. University of Tenne448 8140.
E-mail address: [email protected] (B.L.0022-4804/$ e see front matter ª 2013 Elsevhttp://dx.doi.org/10.1016/j.jss.2013.05.005
a b s t r a c t
Background: The Affordable Care Act of (ACA) 2010 may result in an increase in demand for
surgery and may exacerbate any existing surgeon shortage. The purpose of this study was
to examine factors associated with general surgeon workforce within counties in Ten-
nessee in light of the ACA.
Materials and methods: The Area Resource File for 2011 was utilized for this study. Counties
with less than 3 active surgeons/100,000 persons were classified as shortage counties (SC).
Counties with more than 6 active surgeons/100,000 persons were considered over-supply
counties (OC). Demographic factors for each county were determined. Univariate and
multivariable analysis was used to determine factors associated with SC.
Results: There are 95 counties in the state and 45.3% were SC and 33.7% were OC. Sixty-nine
(72.6%) of the counties had at least one hospital and 57 (60%) were in non-metro counties.
Multivariable logistic regression analysis revealed that increasing percent uninsured in
a county was positively associated with a SC. No other factors were associated with SC. To
meet the cutoff of three surgeons per 100,000 in SC 23 general surgeons would be required.
There was an excess of 219 general surgeons in OCs.
Conclusions: There appears to be an adequate supply of general surgeons but a maldis-
tribution exists, particularly if demand increases with the implementation of the ACA. If
redistribution of surgeons does not occur through natural changes in supply and demand,
careful policy changes may be considered to encourage redistribution of surgeon resources
to meet demand in counties that are currently underserved.
ª 2013 Elsevier Inc. All rights reserved.
1. Introduction surgery, the projected surgeon shortage is likely the result
Healthcare delivery is highly sensitive to the availability of
physicians. Without the necessary number of physicians to
meet demand, access to healthcare can be limited. Currently,
there is an imbalance in physician supply in the United States.
This imbalance in supply and demand is especially true for
primary care and general surgery [1,2]. Regarding general
ssee Health Science Cent
Zarzaur).ier Inc. All rights reserved
of a multitude of factors. A declining number of medical
students choosing surgery, an increase of subspecilization of
general surgery, and an inadequate amount of funding for
training general surgeons are but a few [3,4].
The demand for general surgeons is likely to increase given
the recent Supreme Court decision upholding the Affordable
Care Act of 2010 (ACA). Through this legislation, an increase in
er, 910 Madison Bldg, 2nd Floor, Memphis, TN 38163. Tel.: þ1 901
.
j o u r n a l o f s u r g i c a l r e s e a r c h 1 8 4 ( 2 0 1 3 ) 2 6e3 0 27
those with insurance can be expected, although the rates will
vary by state [5]. Furthermore, portions of the population that
may not have had access to elective procedures will now
be able to afford such procedures, increasing demand for
surgeons. Through health care reform, the shortage of sur-
geons may be exacerbated by a sudden rise in demand and
could cause a crisis in this nation’s health care system. The
lack of access to surgeons could cost lives as has been shown
for those who suffer a major injury [6]. Exacerbating the issue
of access to surgery is the fact that having fewer general
surgeons has a negative impact on the financial viability
of rural hospitals, which could lower the access to even
nonsurgical health services in rural populations [7].
In light of the problems associated with areas that have
a shortage of general surgeons, we set out to further under-
stand the dilemma. The purpose of this study was to deter-
mine factors associated with a shortage of general surgeons
within counties in a single state and to determine if there are
enough active surgeons to meet an immediate increase in
demand.
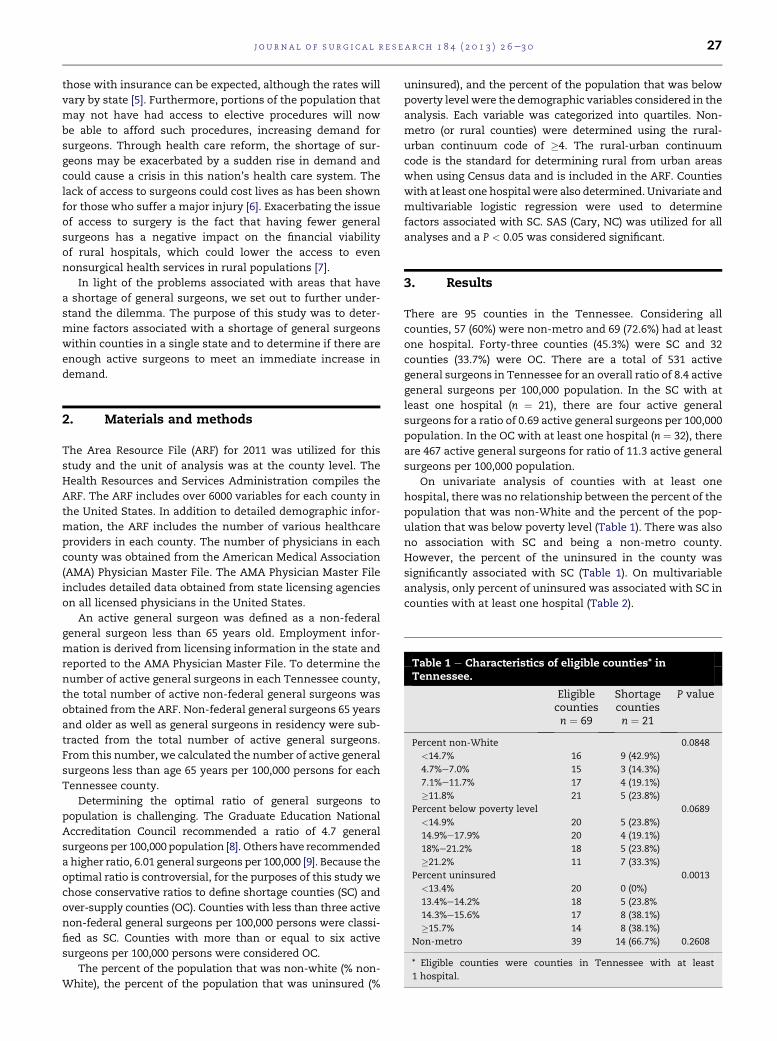
Table 1 e Characteristics of eligible counties* inTennessee.
Eligiblecountiesn ¼ 69
Shortagecountiesn ¼ 21
P value
Percent non-White 0.0848
<14.7% 16 9 (42.9%)
4.7%e7.0% 15 3 (14.3%)
7.1%e11.7% 17 4 (19.1%)
�11.8% 21 5 (23.8%)
Percent below poverty level 0.0689
<14.9% 20 5 (23.8%)
14.9%e17.9% 20 4 (19.1%)
18%e21.2% 18 5 (23.8%)
�21.2% 11 7 (33.3%)
Percent uninsured 0.0013
<13.4% 20 0 (0%)
13.4%e14.2% 18 5 (23.8%
14.3%e15.6% 17 8 (38.1%)
�15.7% 14 8 (38.1%)
Non-metro 39 14 (66.7%) 0.2608
* Eligible counties were counties in Tennessee with at least
1 hospital.
2. Materials and methods
The Area Resource File (ARF) for 2011 was utilized for this
study and the unit of analysis was at the county level. The
Health Resources and Services Administration compiles the
ARF. The ARF includes over 6000 variables for each county in
the United States. In addition to detailed demographic infor-
mation, the ARF includes the number of various healthcare
providers in each county. The number of physicians in each
county was obtained from the American Medical Association
(AMA) Physician Master File. The AMA Physician Master File
includes detailed data obtained from state licensing agencies
on all licensed physicians in the United States.
An active general surgeon was defined as a non-federal
general surgeon less than 65 years old. Employment infor-
mation is derived from licensing information in the state and
reported to the AMA Physician Master File. To determine the
number of active general surgeons in each Tennessee county,
the total number of active non-federal general surgeons was
obtained from the ARF. Non-federal general surgeons 65 years
and older as well as general surgeons in residency were sub-
tracted from the total number of active general surgeons.
From this number, we calculated the number of active general
surgeons less than age 65 years per 100,000 persons for each
Tennessee county.
Determining the optimal ratio of general surgeons to
population is challenging. The Graduate Education National
Accreditation Council recommended a ratio of 4.7 general
surgeons per 100,000 population [8]. Others have recommended
a higher ratio, 6.01 general surgeons per 100,000 [9]. Because the
optimal ratio is controversial, for the purposes of this study we
chose conservative ratios to define shortage counties (SC) and
over-supply counties (OC). Counties with less than three active
non-federal general surgeons per 100,000 persons were classi-
fied as SC. Counties with more than or equal to six active
surgeons per 100,000 persons were considered OC.
The percent of the population that was non-white (% non-
White), the percent of the population that was uninsured (%
uninsured), and the percent of the population that was below
poverty level were the demographic variables considered in the
analysis. Each variable was categorized into quartiles. Non-
metro (or rural counties) were determined using the rural-
urban continuum code of �4. The rural-urban continuum
code is the standard for determining rural from urban areas
when using Census data and is included in the ARF. Counties
with at least one hospital were also determined. Univariate and
multivariable logistic regression were used to determine
factors associated with SC. SAS (Cary, NC) was utilized for all
analyses and a P < 0.05 was considered significant.
3. Results
There are 95 counties in the Tennessee. Considering all
counties, 57 (60%) were non-metro and 69 (72.6%) had at least
one hospital. Forty-three counties (45.3%) were SC and 32
counties (33.7%) were OC. There are a total of 531 active
general surgeons in Tennessee for an overall ratio of 8.4 active
general surgeons per 100,000 population. In the SC with at
least one hospital (n ¼ 21), there are four active general
surgeons for a ratio of 0.69 active general surgeons per 100,000
population. In the OC with at least one hospital (n ¼ 32), there
are 467 active general surgeons for ratio of 11.3 active general
surgeons per 100,000 population.
On univariate analysis of counties with at least one
hospital, there was no relationship between the percent of the
population that was non-White and the percent of the pop-
ulation that was below poverty level (Table 1). There was also
no association with SC and being a non-metro county.
However, the percent of the uninsured in the county was
significantly associated with SC (Table 1). On multivariable
analysis, only percent of uninsured was associated with SC in
counties with at least one hospital (Table 2).

Table 2 e Multivariable analysis of eligible counties* inTennessee.
Or (95% CI) P value
Percent non-White 0.9677
<14.7% REF
4.7%e7.0% 0.75 (0.15, 3.66)
7.1%e11.7% 0.99 (0.23, 4.29)
�11.8% 1.07 (0.23, 4.95)
Percent below poverty level 0.0661
<14.9% REF
14.9%e17.9% 0.80 (0.18, 3.51)
18%e21.2% 1.04 (0.20, 5.47)
�21.2% 6.92 (1.0, 47.53)
Percent uninsured 0.0331
<13.4% REF
13.4%e14.2% 2.40 (0.44, 13.07)
14.3%e15.6% 5.67 (1.08, 29.72)
�15.7% 13.03 (2.09, 81.40)
Non-metro 0.46 (0.13, 1.66) 0.2361
* Eligible counties were counties in Tennessee with at least
1 hospital.
j o u r n a l o f s u r g i c a l r e s e a r c h 1 8 4 ( 2 0 1 3 ) 2 6e3 028
The number of active general surgeons needed to bring SC
up to at least three per 100,000 persons regardless of whether
the county had at least one hospital was calculated using the
following equation:
Additional Surgeons Needed per SC
¼ ðð3� Surgerons per 100; 000 populationÞ� SC PopulationÞO100; 0000
Twenty-three active general surgeons would be needed to
reach this threshold in the 43 SC. If only SC with at least one
hospital are considered, 13 active general surgeons would be
needed to bring the SC up to at least three active general
surgeons per 100,000 persons. The 32 counties in the state
with at least six active general surgeons per 100,000 persons
had an excess of 219 general surgeons. All OCwere in counties
with at least one hospital. The equation used to calculate the
number of excess surgeons follows:
Excess Surgeons per OC ¼ ððSurgeonsper 1000;000 population� 6Þ� OC PopulationÞO100; 000
4. Discussion
There is increasing evidence that a shortage in general
surgeons is looming in the United States [10,11]. Several
factors are thought to play a role in intensifying the general
surgeon shortage. Etzioni and colleagues estimated that due
the aging population in the United States, demand for surgical
services will increase from 14% to 47% [12]. While the demand
for services is increasing, there is also evidence that physi-
cians of all specialties are working less hours currently
compared with the 1990s [13]. Increasing specialization of
general surgeons is also contributing to the surgeon shortage
[3,4]. However, no studies have modeled the impact of the
ACA on surgeon availability on a national scale.
The effect of the ACA on the number of insured in Ten-
nessee has been recently reported [14]. It is projected that
61.3% of currently uninsured Tennesseans, or over 558,000
people, will gain health insurance as a result of the ACA.
Demand for all hospital and ambulatory services is expected
to increase with the exception of visits to the emergency
department, which are expected to decline by 9.6%. Ambula-
tory visits to surgeons are projected to increase by 175,226
extra visits per year. The increase in number of ambulatory
visits is likely to result in increased surgical volume.
As the current study indicates, in Tennessee over 30% of
counties with at least one hospital are already enduring
a general surgeon shortage. However, over 40% of counties
with at least one hospital were found to have more than six
general surgeons per 100,000. To fill the gap in general surgeon
supply in the SC, only 23 active general surgeons would be
needed. In OC, there are 219 more active general surgeons
than potentially needed. A sudden increase in demand in OC
could potentially be met. On the other hand, if the demand in
SC suddenly increases, it is possible that residents of SC in
Tennessee will have to travel further to find an active surgeon
to address their surgical problems. It is a distinct possibility
in a state that boarders eight other states, that persons in
Tennessee may go to other states to get their healthcare
needs met. This may already be happening. Ten of the SC are
boarder counties. Patients may already be going to other
states to obtain care.
A sudden surge in demand for surgical services in SC of
Tennessee could potentially be absorbed if there were not
a maldistribution of general surgeons in the state. Rickets and
colleagues have discussed the maldistribution of general
surgeons. In their study, surgeons tended to move to areas
that already had a high concentration of practicing surgeons
potentially further concentrating surgical services [15]. This is
particularly true for areas with higher rates of uninsured, like
rural counties [16]. Other issues contributing to surgeon
shortages in rural areas are related to a retiring surgical
workforce and an increase in preference of surgeons to prac-
tice in urban areas [17e19].
Another key finding of this study was that the percent
uninsured in a county was the only demographic factor
analyzed that was associated with being a SC. As the percent of
uninsured in the county increased, so did the odds of being
a SC. Previous work regarding physician migration demon-
strated that areas with few number of insured, higher health
maintenance organization penetrance, and high percent of
Medicaid were associated with fewer physicians. The findings
in this study are consistent with the previous studies [20e22].
Lack of a payer sourcemaymake it more difficult for a surgeon
to support a practice, resulting in a maldistribution of active
surgeons in Tennessee. As the provisions of the ACA come into
effect and the insured population in Tennessee increases, there
may be an incentive for surgeons to relocate and service the
newly insured, particularly in counties with at least one
hospital. On the other hand, it is possible that demand for
services from the uninsured will not change and that the
uninsured are already seeking care despite havingno insurance
coverage. Further, it is possible that patients may have insur-
ance as a result of the ACA, but have high deductibles pushing
these patients away from procedures or expensive tests.

j o u r n a l o f s u r g i c a l r e s e a r c h 1 8 4 ( 2 0 1 3 ) 2 6e3 0 29
As mentioned previously, rural areas tend to have a higher
concentration of uninsured compared with urban areas. It is
possible that the observation in this study that surgeons
aggregate in counties with a higher percent of insured might
actually be an epiphenomenon. It may be that surgeons, and
physicians in general, prefer to live in more urban areas for
reasons of lifestyle. Limited entertainment options, fewer
restaurants, less school choice among others may lead phy-
sicians to choose urban areas to live. Recent work regarding
the surgeon shortage indicates that this may be occurring in
the United States [17e19]. However, in this study there was no
relationship between rural counties and SC on univariate or
multivariable analysis.
The findings of this study should be tempered by the study’s
limitations. Because this study focused on a single state, it may
not be applicable to other states or regions in the country. Also,
only a few factorswere available for study in each county to see
if there was an association with general surgeon shortages.
There are clearly others that could potentially impact the
distribution of surgeons that were unmeasured in this study.
Another limitation of the study was that the complex issue of
demand for services was largely unaddressed because there is
no demand information in the database. In particular, it is
possible that because of established referral patterns, patients
from shortage or rural areas are sent for care at referral centers
in larger counties. Because of the large impact of demand on
how general surgeons are dispersed in counties within the
state, examining our findings in light of demandvariationsmay
shed new light on the distribution of surgeons Data from the
AMA Physician Master File may have some inaccuracies
because of the lags in reporting new physician data and errors
in reporting physicians who have recently left clinical practice
[23]. It is also possible that some general surgeons are mis-
classified. The AMA Physician Master File includes an area for
self-designation of practice type. This field was utilized in this
study. However, General Surgery is broad and it is possible that
some surgeons have limited their practices to just a few areas
of General Surgery. There was also no data in the dataset
regarding the number of surgeons taking calls in an emergency
department. Thus, it is possible there was an overestimation of
the number of surgeons available to serve a county’s
population.
Another area of limitation of this study has to do with
differentiation between emergency surgery and elective
surgery. The ideal ratio of general surgeons was derived taking
into account both elective and emergency surgery. However,
the lack of demandfiguresmakes it difficult to comment on the
effect of a surgeon shortage on patients needing emergency
surgery in SC in Tennessee. It is possible that patients needing
emergency surgery in SC would have to travel great distances
to have their surgical needs met. This could have an adverse
impact on outcomes. In a study by Chang and colleagues, the
authors found that increasing surgeon density was associated
with decreased death from motor vehicle crashes [24].
Despite the limitations of the study, it is clear that there
are some factors that are associated with areas that
have a shortage of general surgeons. The trend towards
increased consolidation and regionalization of healthcare
may be one potential solution to workforce issues. Also, this
study suggests that increasing the potential for a surgeon to be
compensated for his or her services plays a role in where
a surgeon decides to practice. It is possible that a natural
migration of surgeons to shortage areas may result from an
increase in the insured population in these areas as a result of
the ACA. Future studies should examine this possibility. Going
forward, careful policy changes may be considered to help
mitigate the effects of surgeon shortages. For example, loan
forgiveness programs for primary care physicians have been
shown to be effective in recruiting physicians to shortage
areas [25]. Further studies should examine effects of growing
potential earnings of general surgeons through increasing not
only the number of insured patients in underserved areas but
also the rate of compensation for services provided to insured
patients in underserved areas. This would effectively do what
loan forgiveness does in using financial reward to encourage
migration to these areas but may offer a long-term incentive
for surgeons to not onlymove to underserved areas but to stay
in these areas.
r e f e r e n c e s
[1] MacDowell M, Glasser M, Fitts M, Nielsen K, Hunsaker M.A national view of rural health workforce issues in the USA.J Rural Remote Health 2010;10:1531:(Online).
[2] Dill MJ, Salsberg ES. The Complexities of physician supplyand demand: projections through 2025. Washington, DC:AAMC Center for Workforce Studies; 2008.
[3] Sanchez M, Sariego J. The general surgeon shortage: causes,consequences, and solutions. South Med J 2009;102:291.
[4] Williams TE Jr, Satiani B, Thomas A, Ellison EC. Theimpending shortage and the estimated cost of training thefuture surgical workforce. AnnSurg 2009;250:590.
[5] Buettgens M, Holahan J, Carroll C. Health reform across thestates:Increased insurance coverage and federal spending onthe exchanges and Medicaid. Princeton: Robert WoodJohnson Foundation: State Coverage Initiatives; 2011.
[6] Aston G. Closing the gaps in the nation’s trauma system.Hosp Health Network 2012;86:49.
[7] Cofer JB, Burns RP. The developing crisis in the nationalgeneral surgery workforce. J Am Coll Surg 2008;206:790.
[8] Graduate Medical Education National Advisory Committee(1980). Report to the Secretary, Department of Health andHuman Services, Geographic Distribution Technical PanelVol. III. HRA 81e653. Washington, DC.
[9] Solucient (2004). Physician Community Requirements in The21st Century: the 2003 Physicians to Population ratios.
[10] Williams TE, Ellison EC. Population analysis predicts a futurecritical shortage of general surgeons. Surgery 2008;144:548.
[11] Physician Supply and Demand: Projections to 2020. USDepartment of Health and Human Services. Available at:http://bhpr.hrsa.gov/healthworkforce/reports/physwfissues.pdf. Accessed December 26, 2012.
[12] Etzioni DA, Liu JH, Maggard MA, et al. The aging populationand its impact on the surgery workforce. Ann Surg 2003;238:170.
[13] Staiger DO, Auerbach DI, Buerhaus PI. Trends in the workhours of physicians in the United states. JAMA 2010;303:747.
[14] Chang A, Mirvis D, Gnuschke J, et al. Impacts of health reformin Tennessee: an examination of changes in health insurance,use of health care resources, and the implications on healthcare manpower. Memphis: University of Memphis Press; 2012.
[15] Rickets T. The migration of surgeons. Ann Surg 2010;251:363.[16] Bolin J, Gamm L. Access to quality health services in
rural areas e insurance: a literature review. In: Gamm LD,

j o u r n a l o f s u r g i c a l r e s e a r c h 1 8 4 ( 2 0 1 3 ) 2 6e3 030
Hutchison LL, Dabney BJ, Dorsey AM, editors. Rural HealthyPeople 2010: A companion document to Healthy People 2010,Vol. 2. College Station, TX: Texas A&M University Press;2003. p. 15.
[17] Thompson M, Lynge D. Characterizing the general surgeryworkforce in rural America. Arch Surg 2005;140:74.
[18] Valentine RJ, Jones A, Biester TW, et al. General surgeryworkloads and practice patterns in the United States, 2007 to2009: a 10-year update from the American Board of Surgery.Ann Surg 2011;254:520.
[19] Polk HC Jr, Bland KI, Ellison EC, et al. A proposal forenhancing the general surgical workforce and access tosurgical care. Ann Surg 2012;255:611.
[20] Simon CJ, Dranove D, White WD. The impact of Managedcare on the physician Marketplace. Public Health Rep 1997;112:222.
[21] Jiang HJ, Begun JW. Dynamics of change in local physiciansupply: an ecological perspective. Soc Sci Med 2002;54:1525.
[22] Brown TT, Coffman JM, Quinn BC, Scheffler RM,Schwalm DD. Do physicians always flee HMOs? New resultsusing dynamic panel estimation methods. Health Serv Res2006;41:357.
[23] Rittenhouse DR, Mertz E, Keane D, Grumbach K. No exit: anevaluation of measures of physician attrition. Health ServRes 2004;39:1571.
[24] Chang DC, Eastman B, Talamini MA, Osen HB, Tran Cao HS,Coimbra R. Density of surgeons is significantly associatedwith reduced risk of deaths frommotor vehicle crashes in UScounties. J Am Coll Surg 2011;212:862.
[25] Pathman DE, Konrad TR, King TS, Taylor DH Jr, Koch GG.Outcomes of states’ scholarship, loan repayment, andrelated programs for physicians. Med Care 2004;42:560.