genetic testing - uhcprovider.com home · a. genetic disorders (e.g., mongolism) in a fetus b. ......
TRANSCRIPT

Page 1 of 25
UHC MA Coverage Summary: Genetic Testing
Proprietary Information of UnitedHealthcare. Copyright 2018 United HealthCare Services, Inc.
Coverage Summary
Genetic Testing
Policy Number: G-003 Products: UnitedHealthcare Medicare Advantage Plans Original Approval Date: 02/14/2008
Approved by: UnitedHealthcare Medicare Benefit Interpretation Committee Last Review Date: 04/17/2018
Related Medicare Advantage Policy Guidelines:
Molecular Pathology/Molecular Diagnostics/Genetic
Testing
Cytogenic Studies (190.3)
This information is being distributed to you for personal reference. The information belongs to UnitedHealthcare and
unauthorized copying, use, and distribution are prohibited. This information is intended to serve only as a general reference
resource and is not intended to address every aspect of a clinical situation. Physicians and patients should not rely on this
information in making health care decisions. Physicians and patients must exercise their independent clinical discretion and
judgment in determining care. Each benefit plan contains its own specific provisions for coverage, limitations, and
exclusions as stated in the Member’s Evidence of Coverage (EOC)/Summary of Benefits (SB). If there is a discrepancy
between this policy and the member’s EOC/SB, the member’s EOC/SB provision will govern. The information contained in
this document is believed to be current as of the date noted.
The benefit information in this Coverage Summary is based on existing national coverage policy, however Local Coverage
Determinations (LCDs) may exist and compliance with these policies is required where applicable.
INDEX TO COVERAGE SUMMARY
I. COVERAGE
1. Tumor Markers
2. Cytogenetic Studies
3. Molecular Diagnostic Tests included in the Palmetto MolDX Program
4. Other Diagnostic Genetic Tests
a. Hereditary Angioedema (HAE) Treatment
b. MyPRS™ Test for Multiple Myeloma Gene Expression Profile
c. Cytological Examination of Breast Fluids for Cancer Screening
d. APC and MYH Gene Testing for Familial Adenomatous Polyposis (FAP),
Attenuated FAP (AFAP), or MYH-associated polyposis
e. PancraGEN® (powered by Pathfinder TG)
f. Ovarian Cancer Biomarker Panels (OVA1™, ROMA™)
g. VeriStrat®
Assay
h. Next Generation Sequencing (NGS)
II. DEFINITIONS
III. REFERENCES
IV. REVISION HISTORY
I. COVERAGE
Coverage Statement: Genetic testing and counseling are covered when Medicare coverage
criteria are met.

Page 2 of 25
UHC MA Coverage Summary: Genetic Testing
Proprietary Information of UnitedHealthcare. Copyright 2018 United HealthCare Services, Inc.
Note: Screening services, such as predictive and pre-symptomatic genetic tests and services, are
those used to detect an undiagnosed disease or disease predisposition, and as such are not a
Medicare benefit and not covered by Medicare. However, Medicare does cover a broad range
of legislatively mandated preventive services to prevent disease, detect disease early when it is
most treatable and curable, and manage disease so that complications can be avoided. These
services can be found on the CMS website at
http://www.cms.hhs.gov/prevntiongeninfo/01_overview.asp. (Accessed April 11, 2018)
Guidelines/Notes:
1. Tumor markers are covered when criteria are met; refer to the following NCDs:
a. Tumor Antigen by Immunoassay - CA 125 (190.28) (Accessed April 11, 2018)
b. Tumor Antigen by Immunoassay - CA 19-9 (190.30) (Accessed April 11, 2018)
c. Tumor Antigen by Immunoassay - CA 15-3/CA 27.29 (190.29) (Accessed April 11,
2018)
d. Carcinoembryonic Antigen (190.26) (Accessed April 11, 2018)
2. Cytogenetic Studies
Cytogenetic studies is used to describe the microscopic examination of the physical
appearance of human chromosomes.
Cytogenetic studies are covered when reasonable and necessary for the diagnosis or
treatment of the following conditions:
a. Genetic disorders (e.g., mongolism) in a fetus
b. Failure of sexual development;
c. Chronic myelogenous leukemia;
d. Acute leukemias lymphoid (FAB L1-L3), myeloid (FAB M0-M7), and unclassified; or
e. Myodysplasia
See the NCD for Cytogenetic Studies (190.3). (Accessed April 11, 2018)
3. Molecular Diagnostic Tests included in the Palmetto MolDX Program
For tests Covered by MolDX Program; refer to Attachment A
For tests Excluded by MolDX Program; refer to Attachment B.
4. Other Diagnostic Genetic Tests
a. Hereditary Angioedema (HAE) Treatment (HCPCS codes J0596, J0597, J0598
and J1290)
Medicare does not have a National Coverage Determination (NCD) for
Hereditary Angioedema (HAE) treatment.
Local Coverage Determinations (LCDs)/Local Coverage Articles (LCAs) do not
exist at this time.
For coverage guidelines, refer to the UnitedHealthcare Drug Policy for
Hereditary Angioedema (HAE), Treatment and Prophylaxis. (IMPORTANT
NOTE: After searching the Medicare Coverage Database, if no state LCD/LCA is
found, then use the above referenced policy.)
Committee approval date: April 17, 2018

Page 3 of 25
UHC MA Coverage Summary: Genetic Testing
Proprietary Information of UnitedHealthcare. Copyright 2018 United HealthCare Services, Inc.
Accessed April 11, 2018
b. MyPRS™ Test for Multiple Myeloma Gene Expression Profile (CPT code 81479)
Medicare does not have a National Coverage Determination (NCD) for MyPRS™
test for multiple myeloma gene expression profile.
Local Coverage Determinations (LCDs)/Local Coverage Article (LCAs) exist and
compliance with these policies is required where applicable. For state-specific
LCDs/LCAs, refer to the LCD Availability Grid (Attachment C).
For states with no LCDs/LCAs, see the UnitedHealthcare Medical Policy for
Molecular Oncology Testing for Cancer Diagnosis, Prognosis, and Treatment
Decisions for coverage guidelines. (IMPORTANT NOTE: After checking the
LCD Availability Grid and searching the Medicare Coverage Database, if no state
LCD/LCA is found, then use the above referenced policy.)
Committee approval date: April 17, 2018
Accessed June 7, 2018
c. Cytological Examination of Breast Fluids for Cancer Screening (Breast Ductal
Lavage, HALO® Breast Pap Test and Fiberoptic ductoscopy, with or without
Ductal Lavage)
Medicare does not have a National Coverage Determination (NCD) for
Cytological Examination of Breast Fluids for Cancer Screening.
Local Coverage Determinations (LCDs)/Local Coverage Articles (LCAs) do not
exist at this time.
For coverage guidelines, refer to the UnitedHealthcare Medical Policy for
Cytological Examination of Breast Fluids for Cancer Screening. (IMPORTANT
NOTE: After searching the Medicare Coverage Database, if no state LCD/LCA is
found, then use the above referenced policy.)
Committee approval date: April 17, 2018
Accessed April 11, 2018
d. APC and MYH Gene Testing for Familial Adenomatous Polyposis (FAP),
Attenuated FAP (AFAP), or MYH-associated polyposis (CPT codes 81201, 81202,
81203)
Medicare does not have a National Coverage Determination (NCD) for APC and
MYH gene testing for familial adenomatous polyposis.
Local Coverage Determinations (LCDs)/Local Coverage Article (LCAs) exist for
all 50 states and compliance with these policies is required where applicable. For
state-specific LCDs/LCAs, refer to the LCD Availability Grid (Attachment D).
Committee approval date: April 17, 2018
Accessed June 7, 2018
e. PancraGEN® (powered by Pathfinder TG) (CPT code 81479)
Medicare does not have a National Coverage Determination (NCD) for
PancraGEN®.
Only one contractor has Local Coverage Determinations (LCDs) which address,
i.e., Novitas Solutions, Inc., for the following states: AR, CO, DC, DE, LA, MD,
MS, NJ, NM, OK, PA, and TX. Compliance with these LCDs is required where
applicable. See the LCD for Loss-of-Heterozygosity Based Topographic

Page 4 of 25
UHC MA Coverage Summary: Genetic Testing
Proprietary Information of UnitedHealthcare. Copyright 2018 United HealthCare Services, Inc.
Genotyping with PathfinderTG®
(L34864). This test is provided to Medicare
beneficiaries throughout the United States by Interpace Diagnostics in
Pittsburg, PA.
For coverage and payment information for all 50 states, refer to the LCD for
Loss-of-Heterozygosity Based Topographic Genotyping with PathfinderTG®
(L34864).
Committee approval date: April 17, 2018
Accessed June 7, 2018
Note: For additional Medicare guidance, see the Medicare Managed Care Manual
Chapter 4, §90.4.1 – MAC with Exclusive Jurisdiction over a Medicare Item or
Service. (Accessed April 11, 2018)
f. Ovarian Cancer Biomarker Panels [OVA1™
(CPT code 81503), ROMA™ (CPT
code 84999)]
Medicare does not have a National Coverage Determination (NCD) for ovarian
cancer biomarker panels.
Local Coverage Determinations (LCDs)/Local Coverage Article (LCAs) exist for
all 50 states and compliance with these policies is required where applicable. For
state-specific LCDs/LCAs, refer to the LCD Availability Grid (Attachment E).
Committee approval date: April 17, 2018
Accessed June 7, 2018
g. VeriStrat®
Assay (CPT Code 81538)
Medicare does not have a National Coverage Determination (NCD) for VeriStrat®
Assay.
Local Coverage Determinations (LCDs)/Local Coverage Article (LCAs) exist for
all 50 states and compliance with these policies is required where applicable. For
state-specific LCDs/LCAs, refer to the LCD Availability Grid (Attachment F).
Committee approval date: April 17, 2018
Accessed June 7, 2018
h. Next Generation Sequencing (NGS)
On March 16, 2018, the Centers for Medicare & Medicaid Services (CMS) issued a
decision memo stating it Next Generation Sequencing (NGS) as a diagnostic
laboratory test is reasonable and necessary and covered nationally, when performed in
a CLIA-certified laboratory, when ordered by a treating physician and when all of the
following requirements are met.
For additional information see the Decision Memo for Next Generation Sequencing
(NGS) for Medicare Beneficiaries with Advanced Cancer (CAG-00450N). (Accessed
April 11, 2018)
Local Coverage Articles (LCAs) exist and compliance with these LCAs is required
where applicable. For state-specific LCAs, see the LCA Availability Grid (Attachment
G). (Accessed June 7, 2018)
II. DEFINITIONS
III. REFERENCES

Page 5 of 25
UHC MA Coverage Summary: Genetic Testing
Proprietary Information of UnitedHealthcare. Copyright 2018 United HealthCare Services, Inc.
See above
IV. REVISION HISTORY
04/17/2018 Annual review with the following updates:
Guideline 3 (Molecular Diagnostic Tests included in the Palmetto MolDX
Program)
Attachment A – Palmetto MolDX Program COVERED Tests
- Combined the following tests :BRACAnalysis® Rearrangement Test
(BART), BRCA1 Analysis, BRCA1/2, BRCAssureSM, BRCAvantage,
Comprehensive, Comprehensive BRACAnalysis® and
- Integrated BRAC Analysis ® into guideline 6 “BRCA1 and BRCA2
Genetic Testing”.
- Deleted “Vysis ALK Break Apart Fish Probe Kit”.
Guideline 4.b [MyPRS™ Test for Multiple Myeloma Gene Expression
Profile (CPT code 81479)] – Updated default for states without LCDs title
name from “UnitedHealthcare Medical Policy for Gene Expression Tests” to
“UnitedHealthcare Medical Policy for Molecular Oncology Testing for
Cancer Diagnosis, Prognosis, and Treatment Decisions” (no changes to
actual guidelines)
Guideline 4.h. [Next Generation Sequencing (NGS)] – Added applicable
coverage guidelines (new to policy)
02/20/2018 Re-review with the following updates:
Guideline 3 (Molecular Diagnostic Tests included in the Palmetto MolDX
Program) – updated the applicable LCDs to include the most recent website links
and effective dates related to the Cahaba-Palmetto jurisdiction transition; no
change in guideline.
Guideline 4.d [APC and MYH Gene Testing for Familial Adenomatous Polyposis
(FAP), Attenuated FAP (AFAP), or MYH-associated polyposis (CPT codes
81201, 81202, 81203)] – updated the applicable LCDs to include the most recent
website links and effective dates related to the Cahaba-Palmetto jurisdiction
transition; no change in guideline.
Guideline 4.f [Ovarian Cancer Biomarker Panels [OVA1™
(CPT code 81503),
ROMA™
(CPT code 84999)] – updated the applicable LCDs to include the most
recent website links and effective dates related to the Cahaba-Palmetto
jurisdiction transition; no change in guideline.
Guideline 4.g [VeriStrat® Assay (CPT Code 81538)] – updated the applicable
LCDs to include the most recent website links and effective dates related to the
Cahaba-Palmetto jurisdiction transition; no change in guideline.
07/17/2017 Re-review with the following updates:
Guideline 4.e [Loss-of-Heterozygosity Based Topographic Genotyping with
PathfinderTG® PancraGEN® (powered by Pathfinder TG) (CPT code 81479)]
updated test name; from PathfinderTG® to new test name, PancraGen®
updated provider name from RedPath Pathology Services to Interpace

Page 6 of 25
UHC MA Coverage Summary: Genetic Testing
Proprietary Information of UnitedHealthcare. Copyright 2018 United HealthCare Services, Inc.
Diagnostics
05/16/2017 Re-review with the following updates:
Guideline 4.e (Loss-of-Heterozygosity Based Topographic Genotyping with
PathfinderTG® )
No change in guideline; will continue to default to the Novitas LCD for Loss-
of-Heterozygosity Based Topographic Genotyping with PathfinderTG®
(L34864). Test is only available and provided by one provider, RedPath
Integrated Pathology (Pittsburg, PA).
Added reference link to the Medicare Managed Care Manual Chapter 4,
§90.4.1 – MAC with Exclusive Jurisdiction over a Medicare Item or Service
04/18/2017 Annual review with the following updates:
Guideline 3 (Molecular Diagnostic Tests included in the Palmetto MolDX
Program) – format changes to Attachment A (Palmetto MolDX Program Covered
Tests and Attachment B (Palmetto MolDX Program Excluded Tests); will
continue to default to the applicable avaialalble Palmetto MolDX Program
Guideline for states with no LCDs.
Guideline 4.d [APC and MYH Gene Testing for Familial Adenomatous Polyposis
(FAP), Attenuated FAP (AFAP), or MYH-associated polyposis] - update
guideline to state that LCDs exist for all 50 states; delete reference to the MCG™
Care Guidelines, 21st edition, 2017, Familial Adenomatous Polyposis - APC Gene
ACG: A-0534 (AC) as default for states with no LCDs.
Guideline 4.f [Ovarian Cancer Biomarker Panels (OVA1™, ROMA™)] - update
guideline to state that LCDs exist for all 50 states; delete statement to refer to the
UnitedHealthcare Medical Policy for Genetic Testing for coverage guidelines.
Guideline 4.g (VeriStrat® Assay) - update guideline to state that LCDs exist for all
50 states; delete statement to refer to the UnitedHealthcare Medical Policy for
Omnibus Codes for coverage guidelines.
03/21/2017 Re-review with the following update:
Guideline 4.d [APC and MYH Gene Testing for Familial Adenomatous Polyposis
(FAP), Attenuated FAP (AFAP), or MYH-associated polyposis] - Updated the
MCG™ Care Guidelines title and reference from 20th
edition 2016 to 21st edition
2017.
05/17/2016 Guideline 3 (Molecular Diagnostic Tests) – Attachment A (Palmetto MolDX
Program Covered Tests) updated to include CPT codes update, i.e., CPT code
81479 replaced with CPT code 81162 for the following tests: BRCA1/ 2,
BRCAssureSM; BRCAvantage, Comprehensive; and Integrated BRAC
Analysis®. New available LCDs also added.
04/19/2016 Annual review with the following updates:
Guideline 2 (Cytogenetic Studies) – removed reference to the LCDs (no
longer available)
Guideline 3 (Molecular Diagnostic Tests included in the Palmetto MolDX
Program)
Attachment A – Palmetto MolDX Program COVERED Tests

Page 7 of 25
UHC MA Coverage Summary: Genetic Testing
Proprietary Information of UnitedHealthcare. Copyright 2018 United HealthCare Services, Inc.
- Deleted duplicate information that’s also available in the Palmetto MolDX
website
- Added separate columns for LCDs/LCAs for Noridian and CGS
- Updated test names as needed
- Removed references to manufacturer; available in the MolDX website
- Add new available LCDs
- Updated codes as needed
- Updated reference links as needed; delete links that are no longer available
- Removed LCD titles; leave LCD numbers only to make grid less busy and
more user friendly
- Deleted from the last column “Not Included in the MolDX Program and”
Attachment B – Palmetto MolDX Program EXCLUDED Tests
- Deleted duplicate information that’s also available in the Palmetto MolDX
website
- Added separate columns for LCDs/LCAs for Noridian and CGS
- Updated test names as needed
- Removed reference to manufacturer; available in the MolDX website
- Updated reference links as needed; delete links that are no longer available
- Removed LCD titles; leave LCD numbers only to make grid less busy and
more user friendly
- Deleted from the last column “Not Included in the MolDX Program and”
- Deleted the following as these are no longer listed in the Palmetto MolDX
Program Excluded Test List):
BRCA1 and BRCA2 genetic testing for a familial mutation
Lipoprotein-associated phospho-lipase A2 (Lp-PLA2) Assay
MPL gene mutations
Pervenio Lung RS assay
Guideline 4 (Other Genetic Tests) – added the word “Diagnostic” to read as
“Other Diagnostic Genetic Tests”
Guideline 4.e (Loss-of-Heterozygosity Based TopographicGenotyping with
PathfinderTG®) – changed CPT code from 84999 to 81479
Guideline 4.g (VeriStrat) – changed code from 84999 to 81538
03/15/2016 Guideline 4.d [APC and MYH Gene Testing for Familial Adenomatous Polyposis
(FAP), Attenuated FAP (AFAP), or MYH-associated polyposis] - Updated the
MCG™ Care Guidelines title and reference from 19th
edition 2015 to 20th
edition
2016.
Updated reference link(s) of the applicable LCDs to reflect the condensed link.
11/17/2015 Guideline 3 (Molecular Diagnotic Tests; Attachment B Excluded Tests) – updated
to include Lipoprotein-associated phospho-lipase A2 (Lp-PLA2) Assay; moved
from the Laboratory Test and Services Coverage Summary.
Guideline 4.e (Loss-of-Heterozygosity Based TopographicGenotyping with
PathfinderTG®) – guideline added; moved from the Laboratory Tests and Services
Coverage Summary; continue to default to the only available LCD, LCD for Loss-
of-Heterozygosity Based Topographic Genotyping with PathfinderTG®
(L34864)
for all 50 states.

Page 8 of 25
UHC MA Coverage Summary: Genetic Testing
Proprietary Information of UnitedHealthcare. Copyright 2018 United HealthCare Services, Inc.
Guideline 4.f Biomarkers for Oncology (e.g., OVA1™ Assay, VeriStrat®
Assay) –
guideline added; moved from the Laboratory Tests and Services Coverage
Summary; changed default guideline for states with no LCDs from Novitas LCD
for Biomarkers for Oncology (L35396) to the UnitedHealthcare Medical Policy
for Genetic Testing.
Guideline 4.g (VeriStrat® Assay) – guideline added; moved from the Laboratory
Tests and Services Coverage Summary; changed default guideline for states with
no LCDs from L Novitas LCD for Biomarkers for Oncology (L35396) to the
UnitedHealthcare Medical Policy for Omnibus Codes.
10/20/2015 Annual review with the following updates:
Guideline 1.a (Cystic Fibrosis Carrier Testing) - Removed guideline; already
addressed in the Laboratory Tests and Services Coverage Summary
Guideline 1.b (General Coverage Rules) - Removed general guideline;
specific test guideline addressed under Guideline 3 (Molecular Diagnostic
Tests included in the MolDX Program) or Guideline 4 (Other Genetic Tests)
Guideline 1.b.1) (Hereditary Breast and Ovarian Cancer Syndromes - BRCA1
and BRCA2) – Moved to Guideline 3 (Molecular Diagnostic Tests included in
the MolDX Program)
Guideline 1.b.2).a) hMLH1, hMSH2, and hMSH6 Gene Tests - Moved to
Guideline 3 (Molecular Diagnostic Tests included in the MolDX Program)
Guideline 1.b.2).b) [APC and MYH Gene Testing for Familial Adenomatous
Polyposis (FAP), Attenuated FAP (AFAP), or MYH-associated polyposis -
Moved to Guideline 4 (Other Genetic Tests)
Guideline 1.b.2).c) (HLA-B*5701 Testing) - Moved to Guideline 3
(Molecular Diagnostic Tests included in the MolDX Program)
Guideline 1.b.2).d).i [KRAS Testing (v-Ki-ras2 Kirsten rat sarcoma viral
oncogene homolog)] - Moved to Guideline 3 (Molecular Diagnostic Tests
included in the MolDX Program)
Guideline 1.b.2)..d).ii [JAK2 (Janus Kinase 2) Testing] - Moved to Guideline
3 (Molecular Diagnostic Tests included in the MolDX Program)
Guideline 1.b.2).d).iii (BCR/ABL fusion gene) - Moved to Guideline 3
(Molecular Diagnostic Tests included in the MolDX Program)
Guideline 1.b.2).e) (Molecular Testing of Lymphoma) - Removed guideline;
reference LCD, Noridian L24308 was retired on 9/30/2015; replaced by
Noridian L34101 which was also retired 10/1/2015. No other available LCD
reference.
Guideline 1.b.2).).f) (Genetic Counseling) - Removed guideline.; no specific
Medicare source/reference.
Guideline 1.c (Tumor markers) - Re-numbered to Guideline 1; no change in
guideline
Guideline 1.d (Cytogenetic Studies) - Re-numbered to Guideline 2; language
updated based on reference NCD to state: “Cytogenetic studies is used to
describe the microscopic examination of the physical appearance of human
chromosomes.”
Guideline 1.e [Hereditary Angioedema (HAE) Treatment] - Moved to
Guideline 4 (Other Genetic Tests)

Page 9 of 25
UHC MA Coverage Summary: Genetic Testing
Proprietary Information of UnitedHealthcare. Copyright 2018 United HealthCare Services, Inc.
Guideline 1.f (MyPRS™ Test for Multiple Myeloma Gene Expression Profile)
- Moved to Guideline 4 (Other Genetic Tests)
Guideline 2.a (Genetic testing that does not meet criteria) - Removed
guideline; no specific Medicare reference/source
Guideline 2.b [Genetic testing for the sole purpose of determining the sex of a
fetus (not reasonable or necessary)] - Removed guideline; no specific
Medicare reference/source
Guideline 2.c (Genetic testing for non-UnitedHealthcare Medicare Advantage
members) - Removed guideline; no specific Medicare reference/source
Guideline 2.d (Cytological Examination of Breast Fluids for Cancer
Screening) Moved to Guideline 4 (Other Genetic Tests)
Guideline 3 (Molecular Diagnostic Tests included in the MolDX Program)
Moved from the Laboratory Tests and Services Coverage Summary; added
guideline (new to the policy) with individual test guidelines listed in 2
attachments: Attachment A (MolDX Program COVERED Tests) and
Attachment B (MolDX Program EXCLUDED Tests)
Guideline 4.a [Hereditary Angioedema (HAE) Treatment] - Moved from
Guideline 1.e; added HCPCS codes J0597, J0598 and J1290; changed default
policy from First Coast LCD for Selective Treatment of HAE with Cinryze,
Berinert and Ecallantide (L31475) to UnitedHealthcare Drug Policy for
Hereditary Angioedema (HAE) Treatment and Prophylaxis
Guideline 4.b (MyPRS™ Test for Multiple Myeloma Gene Expression
Profile) Moved from Guideline 1.f; added CPT code 81479; changed default
policy from Novitas Solutions, Inc. LCD for My PRS Genetic Expression
Profile Testing (L32636) to UnitedHealthcare Medical Policy for Gene
Expression Tests
Guideline 4.c (Cytological Examination of Breast Fluids for Cancer Screening
- Moved from Guideline #2.d; added to the section title “Breast Ductal
Lavage, HALO®
Breast Pap Test and Fiberoptic ductoscopy, with or without
Ductal Lavage”; no change in guideline
Guideline 4.d [APC and MYH Gene Testing for Familial Adenomatous
Polyposis (FAP), Attenuated FAP (AFAP), or MYH-associated polyposis] -
Moved from Guideline 1.b.2).b); added CPT codes 81201, 81202, 81203;
changed default policy from Noridian Healthcare Solutions LCD for Genetic
Testing (L24308) to MCG™ Care Guidelines, 19th
edition, 2015, Familial
Adenomatous Polyposis - APC and MUTYH Genes, and Gene Panels ACG:
A-0534 (AC)
04/15/2014 Annual review with the following updates:
Guideline #1.e [Hereditary Angioedema (HAE) Treatment)]- Removed
reference to ICD-9-CM code 277.6
Definitions
o Cystic Fibrosis (removed; no CMS reference available)
o Cytogenetic Studies (removed; already defined in Guideline #1.d)
o Genetic Counseling (removed; no CMS reference available)
o Genetic Testing (removed; already defined in Guideline #1.b)
04/29/2013 Annual review with the following updates:

Page 10 of 25
UHC MA Coverage Summary: Genetic Testing
Proprietary Information of UnitedHealthcare. Copyright 2018 United HealthCare Services, Inc.
Guidelines #1.b.1 (BRCA1 and BRCA2)-Default guidelines for states with no
LCDs replaced with the direct link to the Noridian LCD for Genetic Testing
(L24308)
Guidelines 1.b.2.a (hMLH1, hMSH2, and hMSH6 Gene Tests)-Default
guidelines for states with no LCDs replaced with the direct link to the Noridian
LCD for Genetic Testing (L24308)
Guidelines 1.b.2.b (APC and MYH Gene Testing for Familial Adenomatous
Polyposis, Attenuated FAP, or MYH-associated polyposis)-Default guidelines
for states with no LCDs replaced with the direct link to the Noridian LCD for
Genetic Testing (L24308)
Guidelines 1.b.2.c (HLA-B*5701 Testing)-Added applicable coverage
guidelines (new to policy)
Guidelines 1.b.2.d.i (KRAS Testing)-Default guidelines for states with no
LCDs replaced with the direct link to the Palmetto LCD for K-ras Testing
Required before Epidermal Growth Factor Receptor Antibody Use in
Colorectal Cancer (L31766)
Guidelines 1.b.2.d.ii (JAK2 Testing)-Default guidelines for states with no
LCDs replaced with the direct link to the Noridian LCD for Genetic Testing
(L24308)
Guidelines 1.b.2.d.iii (BCR/ABL fusion gene)-Added applicable coverage
guidelines (new to policy)
Guidelines 1.b.2.e (Molecular Testing of Lymphoma)-Added applicable
coverage guidelines (new to policy)
10/08/2012 Guidelines #9 MyPRS™ Test for Multiple Myeloma Gene Expression Profile–
updated the default LCDs for states with no LCDs to Novitas L23636
The default LCDs, Pinnacle L32060 and L32066 were retired on 8/12/2012
due to MAC transition from Pinnacle to Novitas for the states of AR, LA and
MS
New LCD is Novitas L23636 (effective 8/20/2012); no change in LCD
coverage guidelines
08/20/2012 The following guidelines were deleted from this Coverage Summary and moved
to Coverage Summary for Laboratory Services:
Gene Expression Test Oncotype DX®
MammaPrint Genetic Expression Profiling Test
Molecular Profiling for Unknown Primary Cancers (UPC) Cancers (i.e.,
Pathwork® Tissue of Origin and biotheranostics Cancer TYPE ID
®)
04/23/2012 Annual review with the following updates:
Guidelines #1.b (Genetic Testing for Hereditary Breast , Ovarian, Colorectal
and Polyposis Cancer) was updated, i.e., deleted reference to L23664 as this
LCD was retired; only default LCD is now L24308; no change in guidelines as
these 2 LCDs are identical
Guidelines #1.d (MammaPrint Genetic Expression Profiling Test) updated to
include sections for Documentation Requirements and Utilization Review
Guidelines
Added the following guidelines:
o (1) Guidelines #1.e (Molecular Profiling for Unknown Primary

Page 11 of 25
UHC MA Coverage Summary: Genetic Testing
Proprietary Information of UnitedHealthcare. Copyright 2018 United HealthCare Services, Inc.
Cancers);
o (2) Guidelines #1.h Hereditary Angioedema Treatment; and
o (3) Guidelines #1.i MyPRS™ Test for Multiple Myeloma Gene
Expression Profile
Guidelines #2.b (Genetic testing for the sole purpose of determining the sex of
a fetus) updated to include the language “not reasonable and necessary”
10/07/2011 Updated Guidelines #1.b.5 (Therapy-Directing Testing - KRAS Testing), i.e.,
changed CIGNA L30200 to Palmetto L31766 as one of the default LCDs for
states with no LCDs as L30200 was retired due to MAC transition from CIGNA
to Palmetto; no change in guidelines
04/26/2011 Annual review; updated to include Guidelines #1.d (MammaPrint Genetic
Expression Profiling Test)
10/21/2010 Updated the LCD links and UHC Medical Policy links
V. ATTACHMENT(S)
Attachment A – Palmetto MolDX Program COVERED Tests Committee Approval Date: April 17, 2018
Accessed June 7, 2018
The following is a list, but not all-inclusive, of tests that have completed the MolDX Technical Assessment Process. For the most current
MolDX information, refer to the MolDX Program website at http://www.palmettogba.com/palmetto/MolDX.nsf/DocsCatHome/MolDx.
Important Note:
For states with no LCDs/LCAs, refer to the applicable Palmetto MolDX Program Guideline for coverage guideline.
Test Code(s) Palmetto MolDX Program
Guideline
States
LCDs/LCAs
Noridian
States
CGS
States
Wisconsin
States
Novitas
States
NGS
States
First
Coast
States
1. Afirma
81545
L35025 Afirma Assay by
Veracyte Coding and Billing
Guidelines (M00015)
L35160
L36256
L36021
L36807 L35396
L35000
2. Allomap
81595 L35025 AlloMap Coding
and Billing Guidelines
(M00016)
L35160
L36256
L36021
L36807
3. Avise PG
84999
L35025 Avise PG Assay
Coding and Billing
Guidelines (M00026)
L35160
L36256
L36021
L36807
4. BCR-ABL
Negative Myelo-
proliferative
Disease
81206
81207
81206
81207
and
81208
L36044 BCR-ABL Coding
and Billing Guidelines
(M00044)
L36180
L36186
L36021
L36807 L35396 L35000 L34519
5. Bladder Tumor
Marker FISH
88120
or
88121
L33420 Bladder Tumor
Marker FISH Coding and
Coding Guidelines
(M00001)
L33965
6. BRCA1 and
BRCA2 Genetic
Testing
81162
81211
to
81217
L36082
L36161
L36163
L36456
A55248
L35062
L35000 L36499

Page 12 of 25
UHC MA Coverage Summary: Genetic Testing
Proprietary Information of UnitedHealthcare. Copyright 2018 United HealthCare Services, Inc.
Attachment A – Palmetto MolDX Program COVERED Tests Committee Approval Date: April 17, 2018
Accessed June 7, 2018
The following is a list, but not all-inclusive, of tests that have completed the MolDX Technical Assessment Process. For the most current
MolDX information, refer to the MolDX Program website at http://www.palmettogba.com/palmetto/MolDX.nsf/DocsCatHome/MolDx.
Important Note:
For states with no LCDs/LCAs, refer to the applicable Palmetto MolDX Program Guideline for coverage guideline.
Test Code(s) Palmetto MolDX Program
Guideline
States
LCDs/LCAs
Noridian
States
CGS
States
Wisconsin
States
Novitas
States
NGS
States
First
Coast
States
81432
7. Breast Cancer
Index Genetic
Assay
81479 L35631
L36314
L36316
L36458 L36785
8. Cobas 4800
BRAF V600
81210 L35025 FDA-Approved
BRAF Tests (M00111)
L35160
L36256
L36021
L36807 L35396 L35000 L34912
L34519
9. Short Tandem
Repeat (STR)
Markers and
Chimerism
Testing
81265
to
81268
L35025 Short Tandem
Repeat (STR) CDMarkers
and Chimerism Coding and
Billing Guidelines
(M00129)
L35160
L36256
L36021
L36807 L35062
L35000 L34519
10. cobas EGFR
Mutation Test
81235 L35025 FDA-Approved
EGFR Tests (M00110)
L35160
L36256
L36021
L36807 L35396
L35000 L34519
11. cobas KRAS
81275 L35025 FDA-Approved
KRAS Tests (M00121)
L35160
L36256
L36021
A54688
L36807 L35396
L35000 L34519
12. BRACAnalysis
CDx
81479 A54338 Myriad's
BRACAnalysis CDx Coding
and Billing Guidelines
(M00120)
A55294
A55295
A54689 A55224
13. Confirm MDX
81551 L35632
L36327
L36329
L36006 L37005
14. Corus CAD
81493 L35025 L35160
L36256
L36021 L36807 L36713
15. CTID
CancerTYPE ID®
81540 L35025 bioTheranostics
Cancer TYPE ID (M00027)
L35160
L36256
L36021
L36807
16. Decipher®
prostate cancer
classifier assay
81479 L35868 L36343
L36345
L36656 L36791
17. GeneSight®
Psychotropic
81479 L35633 L36323
L36325
L35443 L36799
18. HERmark Assay
by Monogram
81479 L35025 HERmark Assay by
Monogram Coding and
Billing Guidelines
(M00028)
L35160
L36256
L36021
L36807
19. HLA-B*15:02
Genetic Testing
81381 L36033 L36145
L36149
L36048
L36021
L36807 L35062
L34518

Page 13 of 25
UHC MA Coverage Summary: Genetic Testing
Proprietary Information of UnitedHealthcare. Copyright 2018 United HealthCare Services, Inc.
Attachment A – Palmetto MolDX Program COVERED Tests Committee Approval Date: April 17, 2018
Accessed June 7, 2018
The following is a list, but not all-inclusive, of tests that have completed the MolDX Technical Assessment Process. For the most current
MolDX information, refer to the MolDX Program website at http://www.palmettogba.com/palmetto/MolDX.nsf/DocsCatHome/MolDx.
Important Note:
For states with no LCDs/LCAs, refer to the applicable Palmetto MolDX Program Guideline for coverage guideline.
Test Code(s) Palmetto MolDX Program
Guideline
States
LCDs/LCAs
Noridian
States
CGS
States
Wisconsin
States
Novitas
States
NGS
States
First
Coast
States
20. hMLH1, hMSH2,
and hMSH6 Gene
Tests
81288
81292
81293
81294
81295
to
81300
L35024
L36370
L36374
L35349
L36807 L35062
L34519
21. JAK2 V617F
JAK2 exon 12
81270
81403
L36044 L36180
L36186
L36807 L35396
L35000 L34519
22. MammaPrint
81521 L35025 MammaPrint
Billing and Coding
Guidelines Update
(M00029)
L35160
L36256
L36021
L36807 L33586
23. Oncotype DX
Breast Cancer
Assay
81519 L35025 Oncotype DX
Breast Cancer Assay Coding
and Billing Guidelines
(M00003)
L35160
L36256
L36021
A55248 L33586
24. Oncotype DX
Colon Cancer
Assay
81525 L35025 Oncotype DX
Colon Cancer Assay Coding
and Billing Guidelines
(M0002)
L35160
L36256
L36021
L36807
25. PreciseType™
HEA BeadChip
81403 L36074 L36167
L36171
L36021 A55248
26. Progensa PCA3
Assay
81313 L35025 Progensa PCA3
Assay Coding and Billing
Guidelines (M00013)
L35160
L36256
L36021
L36807
27. Prolaris™
Prostate Cancer
Assay
(Myriad Genetics)
81541 L35869
L37043
L36348
L36350
L37080
L37082
L36002
L37142
L36787
L37226
28. therascreen EGFR
RGQ PCR
81235 L35025 FDA-Approved
EGFR Tests (M00110)
L35160
L36256
L36021
L36807 L35396
L35000 L34519
29. Therascreen
KRAS Kit
81275 L35025 FDA-Approved
KRAS Tests (M00121)
L35160
L36256
L36021
L36807 L35396
L35000 L34519
30. ThxID™ BRAF
V600/K Test
81210 L35025 FDA-Approved
BRAF Tests (M00111)
L35160
L36256
L36021
L36807 L35396
L35000 L34912
31. Tissue of Origin
(ResponseDx)
81504 L35025 ResponseDX Tissue
of Origin Coding and
Billing Guidelines
(M00034)
L35160
L36256
L36021
L36807
L35000 L33777

Page 14 of 25
UHC MA Coverage Summary: Genetic Testing
Proprietary Information of UnitedHealthcare. Copyright 2018 United HealthCare Services, Inc.
Attachment A – Palmetto MolDX Program COVERED Tests Committee Approval Date: April 17, 2018
Accessed June 7, 2018
The following is a list, but not all-inclusive, of tests that have completed the MolDX Technical Assessment Process. For the most current
MolDX information, refer to the MolDX Program website at http://www.palmettogba.com/palmetto/MolDX.nsf/DocsCatHome/MolDx.
Important Note:
For states with no LCDs/LCAs, refer to the applicable Palmetto MolDX Program Guideline for coverage guideline.
Test Code(s) Palmetto MolDX Program
Guideline
States
LCDs/LCAs
Noridian
States
CGS
States
Wisconsin
States
Novitas
States
NGS
States
First
Coast
States
32. Ventana ALK
(D5F3) CDx
Assay
88342 L35922
L36351
L36353
L35986
L36805 L36234
L33261
L34912
33. Vectra-DA
81479 L35025 Vectra DA Coding
and Billing Guidelines
(M00031)
L35160
L36256
L36021
L36807
End of Attachment A
^Back to Top Attachment A
Attachment B – Palmetto MolDX Program EXCLUDED Tests Committee Approval Date: April 17, 2018
Accessed June 4, 2018
The following is a list, but not all-inclusive, of tests that have completed the MolDX Technical Assessment process.For the most current
MolDX information, refer to the MolDX Program website at http://www.palmettogba.com/palmetto/MolDX.nsf/DocsCatHome/MolDx.
Important Note:
For states with no LCDs/LCAs, refer to the applicable Palmetto MolDX Program Guideline for coverage guideline.
Test Code
(s)
Palmetto MolDX Program
Guideline
States
LCDs/ LCAs
Noridian
States
CGS
States
Wisconsin
States
Novitas
States
NGS
States
First Coast
States
1. 4q25-AF Risk
Genotype Coding
81479 L35025
A53457
4q25-AF Risk Genotype
Coding and Billing Guidelines
(M00004)
A55090
A55091
A54241 A55137
2. 9p21 Genotype
Test
81479 L35025
A53657
9p21 Genotype Test Coding
and Billing Guidelines
(M00082)
A55092
A55093
A54242
A55138
3. Apolipo- protein
(Apo) E genotype
81401 L35025
A53652
ApoE Genotype Coding and
Billing Guidelines (M00083)
A55094
A55095
A54244 A55141 L35000
4. Arrhythmogenic 81479 L35025 A54975
A54976
A54685 A55235

Page 15 of 25
UHC MA Coverage Summary: Genetic Testing
Proprietary Information of UnitedHealthcare. Copyright 2018 United HealthCare Services, Inc.
Attachment B – Palmetto MolDX Program EXCLUDED Tests Committee Approval Date: April 17, 2018
Accessed June 4, 2018
The following is a list, but not all-inclusive, of tests that have completed the MolDX Technical Assessment process.For the most current
MolDX information, refer to the MolDX Program website at http://www.palmettogba.com/palmetto/MolDX.nsf/DocsCatHome/MolDx.
Important Note:
For states with no LCDs/LCAs, refer to the applicable Palmetto MolDX Program Guideline for coverage guideline.
Test Code
(s)
Palmetto MolDX Program
Guideline
States
LCDs/ LCAs
Noridian
States
CGS
States
Wisconsin
States
Novitas
States
NGS
States
First Coast
States
Right Ventricular
Dysplasia/Cardiom
yopathy (ARVD/C)
Testing
A53605
Arrhythmogenic Right
Ventricular
Dysplasia/Cardiomyopathy
(ARVD/C) Testing Coding
and Billing Guidelines
(M00067)
5. Aspartoacyclase 2
Deficiency (ASPA)
Testing
81200 L35025
A53602
Aspartoacyclase 2
Deficiency(ASPA) Testing
Coding and Billing Guidelines
(M00068)
A55088
A55089
A54253 A55142
L35062
L35000
L34519
6. ATP7B Gene Tests 81406 L35025
A53550
ATP7B Gene Tests Coding
and Billing Guidelines
(M00052)
A55097
A55098
A54254 A55143 L35000
7. BCKDHB Gene
Test
81205
81206
L35025
A53600
BCKDHB Gene Test Coding
and Billing Guidelines
(M00069)
A55099
A55100
A54255 A55145
8. Biocept’s
OncoCee,
Circulating Tumor
Cell (CTC) Assay
88346
88313
88361
88346
88313
88361
88346
88313
88361
88346
88313
88361
A53112
OncoCee Coding and Billing
Guidelines (M00036)
A55598
A55593
A54292 A55245
9. BLM Gene 81209 L35025 A55113
A55114
A54256
A55148

Page 16 of 25
UHC MA Coverage Summary: Genetic Testing
Proprietary Information of UnitedHealthcare. Copyright 2018 United HealthCare Services, Inc.
Attachment B – Palmetto MolDX Program EXCLUDED Tests Committee Approval Date: April 17, 2018
Accessed June 4, 2018
The following is a list, but not all-inclusive, of tests that have completed the MolDX Technical Assessment process.For the most current
MolDX information, refer to the MolDX Program website at http://www.palmettogba.com/palmetto/MolDX.nsf/DocsCatHome/MolDx.
Important Note:
For states with no LCDs/LCAs, refer to the applicable Palmetto MolDX Program Guideline for coverage guideline.
Test Code
(s)
Palmetto MolDX Program
Guideline
States
LCDs/ LCAs
Noridian
States
CGS
States
Wisconsin
States
Novitas
States
NGS
States
First Coast
States
Analysis A53540
BLM Gene Analysis Coding
and Billing Guidelines
(M00049)
10. BluePrint®, a
molecular
subtyping assay
81479 L35025
A53484
BluePrint Coding and Billing
Guidelines (M00010)
A55115
A55116
A54257 A55146
11. CDH1 Genetic
Testing
81406 L35025
A54835
CDH1 Genetic Testing Coding
and Billing Guidelines
(M00087)
A54878 A55622
12. CFTR Gene
Analysis
81220
81221
81222
81223
81224
81479
L35025
A53615
CFTR Gene Analysis Coding
and Billing Guidelines
(M00076)
A55117
A55118
A54258 A55156
13. CHD7 Gene
Analysis
81407 L35025
A53565
CHD7 Gene Analysis Coding
and Billing Guidelines
(M00058)
A55085
A55086
A54243 A55157
14. Coenzyme Q10 82542 L37022
Coenzyme Q10 (Q10) Coding
and Billing Guideline
(M00146)
A55715
15. CYP2B6 Test 81479 L35025
A53556
CYP2B6 Test Coding and
Billing Guidelines (M00054)
A55177
A55178
A54260 A55234
16. Cytogenomic
Constitutional
Microarray
81228
81229
L35025
L35160
MolDX
Excluded
Tests
L36021
L36807
L35062 L35000 L34519

Page 17 of 25
UHC MA Coverage Summary: Genetic Testing
Proprietary Information of UnitedHealthcare. Copyright 2018 United HealthCare Services, Inc.
Attachment B – Palmetto MolDX Program EXCLUDED Tests Committee Approval Date: April 17, 2018
Accessed June 4, 2018
The following is a list, but not all-inclusive, of tests that have completed the MolDX Technical Assessment process.For the most current
MolDX information, refer to the MolDX Program website at http://www.palmettogba.com/palmetto/MolDX.nsf/DocsCatHome/MolDx.
Important Note:
For states with no LCDs/LCAs, refer to the applicable Palmetto MolDX Program Guideline for coverage guideline.
Test Code
(s)
Palmetto MolDX Program
Guideline
States
LCDs/ LCAs
Noridian
States
CGS
States
Wisconsin
States
Novitas
States
NGS
States
First Coast
States
Analysis
L36256
MolDX
Excluded
Tests
17. RPS19 Gene Tests 81403
81405
81479
L35025
A53587
RPS19 Gene Tests Coding and
Billing Guidelines (M00062)
A55610
A55614
A54299 A55205
18. FANCC Genetic
Testing
81242 L35025
A53628
FANCC Genetic Testing
Coding and Billing Guidelines
(M00073)
A55183
A55184
A54263 A55160
19. Fragile X 81243
81244
L35025
A53638
Fragile X Coding and Billing
Guidelines (M00077)
A55241
A55242
A54264 A55163
20. GBA Genetic
Testing
81251 L35025
A53542
GBA Genetic Testing Coding
and Billing Guidelines
(M00050)
A55244
A55243
A54265 A55164
21. HAX1 Gene
Sequencing
81479 L35025
A53619
HAX1 Gene Sequencing
Coding and Billing Guidelines
(M00074)
A55249
A55252
A54266 A55165
22. HBB Full Gene
Sequencing
81401
81403
81404
L35025
A53493
HBB Full Gene Sequencing
Coding and Billing Guidelines
(M00020)
A55253
A55254
A54267 A55166
23. ENG and ACVRL1
Gene Tests
81403
81405
81406
81479
L35025
A53536
ENG and ACVRL1 Gene
Tests Coding and Billing
A55182
A55181
A54262 A55159

Page 18 of 25
UHC MA Coverage Summary: Genetic Testing
Proprietary Information of UnitedHealthcare. Copyright 2018 United HealthCare Services, Inc.
Attachment B – Palmetto MolDX Program EXCLUDED Tests Committee Approval Date: April 17, 2018
Accessed June 4, 2018
The following is a list, but not all-inclusive, of tests that have completed the MolDX Technical Assessment process.For the most current
MolDX information, refer to the MolDX Program website at http://www.palmettogba.com/palmetto/MolDX.nsf/DocsCatHome/MolDx.
Important Note:
For states with no LCDs/LCAs, refer to the applicable Palmetto MolDX Program Guideline for coverage guideline.
Test Code
(s)
Palmetto MolDX Program
Guideline
States
LCDs/ LCAs
Noridian
States
CGS
States
Wisconsin
States
Novitas
States
NGS
States
First Coast
States
Guidelines (M00046)
24. HEXA Gene
Analysis
81255
81406
L35025
A53598
HEXA Gene Analysis Coding
and Billing Guidelines
(M00070)
A55255
A55256
A54268 A55168
25. IKBKAP Genetic
Testing
81260 L35025
A53596
IKBKAP Genetic Testing
Coding and Billing Guidelines
(M00071)
A55612
A55613
A54270 A55170
26. KIF6 Genotype 81479 L35025
A53576
KIF6 Genotype Coding and
Billing Guidelines (M00017)
A54272
A55171
27. LPA-Aspirin
Genotype
81479 L35025
A53467
LPA-Aspirin Genotype
Coding and Billing Guidelines
(M00006)
A54275 A55173
28. LPA-Intron 25
Genotype
81479 L35025
A53468
LPA-Intron 25 Genotype
Coding and Billing Guidelines
(M0007)
A54276
A55174
29.
L1CAM Gene
Sequencing
81704 L35025
A53659
L1CAM Gene Sequencing
Coding and Billing Guidelines
(M00078)
A55277
A55278
A54274 A55192
30. MCOLN1 Genetic
Testing
81290 L35025
A53630
MCOLN1 Genetic Testing
Coding and Billing Guidelines
(M00075)
A55283
A55284
A54277 A55176

Page 19 of 25
UHC MA Coverage Summary: Genetic Testing
Proprietary Information of UnitedHealthcare. Copyright 2018 United HealthCare Services, Inc.
Attachment B – Palmetto MolDX Program EXCLUDED Tests Committee Approval Date: April 17, 2018
Accessed June 4, 2018
The following is a list, but not all-inclusive, of tests that have completed the MolDX Technical Assessment process.For the most current
MolDX information, refer to the MolDX Program website at http://www.palmettogba.com/palmetto/MolDX.nsf/DocsCatHome/MolDx.
Important Note:
For states with no LCDs/LCAs, refer to the applicable Palmetto MolDX Program Guideline for coverage guideline.
Test Code
(s)
Palmetto MolDX Program
Guideline
States
LCDs/ LCAs
Noridian
States
CGS
States
Wisconsin
States
Novitas
States
NGS
States
First Coast
States
31.
MMACHC Test 81404 L35025
A54035
MMACHC Test Coding and
Billing Guidelines (M00089)
A55288
A55289
A54209 A55191
32. Mitochondrial
Nuclear Gene Tests
81440 L35025
A53669
Mitochondrial Nuclear Gene
Tests Coding and Billing
Guidelines (M00079)
A55290
A55291
A54288 A55190
33.
PTCH1 Gene
Testing
81479 L35025
A53567
PTCH1 Gene Testing Coding
and Billing Guidelines
(M00059)
A55608
A55618
A54297
A55203
34 PAX6 Gene
Sequencing
81479 L35025
A53664
PAX6 Gene Sequencing
Coding and Billing Guidelines
(M00080)
A55625
A55632
A54293 A55199
35. PIK3CA Gene
Tests
81403 L35025
A53558
PIK3CA Gene Tests Coding
and Billing Guidelines
(M00056)
A55597
A55602
A54295 A55200
36.
PreDx® 81403 L35025
A53489
PreDx Coding and Billing
Guidelines (M00011)
A55594
A55599
A54296
A55201
37. MECP2 Genetic
Testing
81302
81303
81304
81479
L35025
A53574
MECP2 Genetic Testing
Coding and Billing Guidelines
(M00066)
A55285
A55286
A54278 A55189

Page 20 of 25
UHC MA Coverage Summary: Genetic Testing
Proprietary Information of UnitedHealthcare. Copyright 2018 United HealthCare Services, Inc.
Attachment B – Palmetto MolDX Program EXCLUDED Tests Committee Approval Date: April 17, 2018
Accessed June 4, 2018
The following is a list, but not all-inclusive, of tests that have completed the MolDX Technical Assessment process.For the most current
MolDX information, refer to the MolDX Program website at http://www.palmettogba.com/palmetto/MolDX.nsf/DocsCatHome/MolDx.
Important Note:
For states with no LCDs/LCAs, refer to the applicable Palmetto MolDX Program Guideline for coverage guideline.
Test Code
(s)
Palmetto MolDX Program
Guideline
States
LCDs/ LCAs
Noridian
States
CGS
States
Wisconsin
States
Novitas
States
NGS
States
First Coast
States
38. SEPT9 Gene Test 81401 L35025
A53702
SEPT9 Gene Test Coding and
Billing Guidelines (M00093)
A55623
A55628
A54300 A55206
39. HTTLPR Gene
Testing
81479 L35025
A53480
HTTLPR Gene Testing
Coding and Billing Guidelines
(M00008)
A54269
A55169
40. SLCO1B1
Genotype
81400 L35025
A53698
SLCO1B1 Genotype Coding
and Billing Guidelines
(M00091)
A55626
A55630
A54286 A55207
41. NSD1 Gene Tests 81403
81405
81406
81479
L35025
A53585
NSD1 Gene Tests Coding and
Billing Guidelines (M00061)
A55609
A55615
A54291
A55198
42. SMPD1 Genetic
Testing
81330
81403
L35025
A53624
SMPD1 Genetic Testing
Coding and Billing Guidelines
(M00072)
A55627
A55631
A54285 A55208
43.
STAT3 Gene
Testing
81405 L35025
A53562
STAT3 Gene Testing Coding
and Billing Guidelines
(M00057)
A55480
A55481
A54284 A55209
44.
SULT4A1 Genetic
Testing
81479 L35025
A53538
SULT4A1 Genetic Testing
Coding and Billing Guidelines
(M00048)
A55596
A55601
A54283 A55210
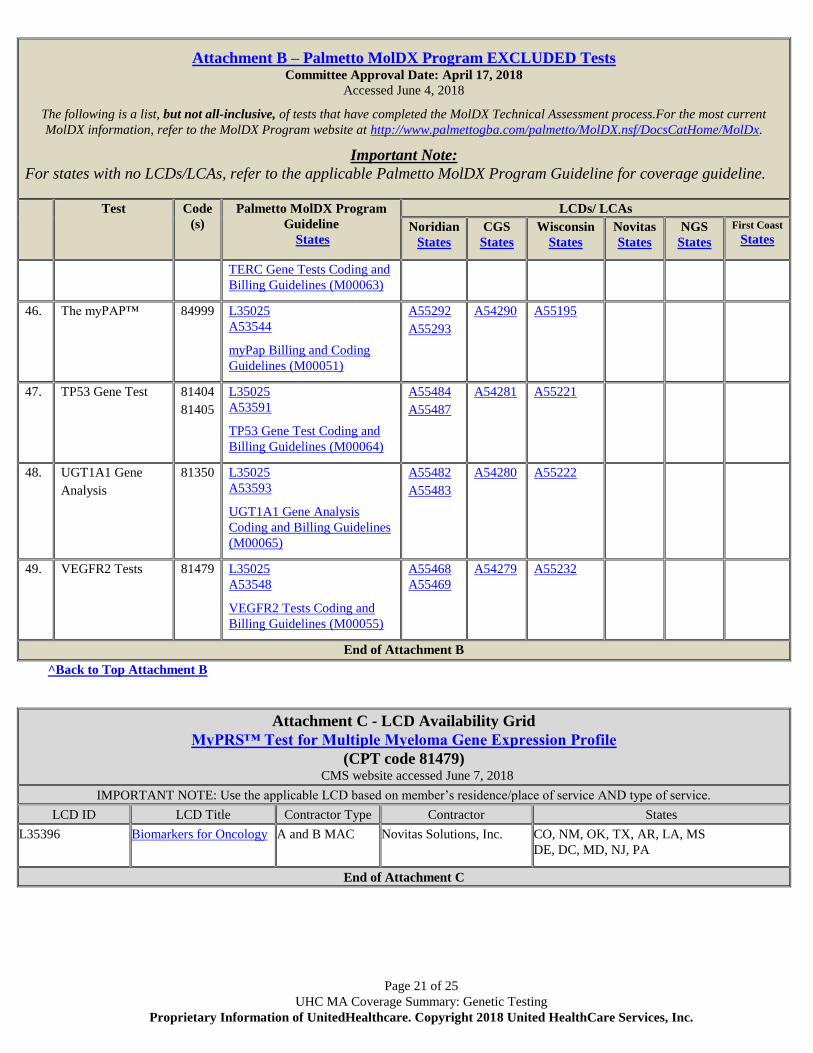
45. TERC Gene Tests 81479 L35025
A53589
A55611
A55616
A54282 A55611
Page 21 of 25
UHC MA Coverage Summary: Genetic Testing
Proprietary Information of UnitedHealthcare. Copyright 2018 United HealthCare Services, Inc.
Attachment B – Palmetto MolDX Program EXCLUDED Tests Committee Approval Date: April 17, 2018
Accessed June 4, 2018
The following is a list, but not all-inclusive, of tests that have completed the MolDX Technical Assessment process.For the most current
MolDX information, refer to the MolDX Program website at http://www.palmettogba.com/palmetto/MolDX.nsf/DocsCatHome/MolDx.
Important Note:
For states with no LCDs/LCAs, refer to the applicable Palmetto MolDX Program Guideline for coverage guideline.
Test Code
(s)
Palmetto MolDX Program
Guideline
States
LCDs/ LCAs
Noridian
States
CGS
States
Wisconsin
States
Novitas
States
NGS
States
First Coast
States
TERC Gene Tests Coding and
Billing Guidelines (M00063)
46. The myPAP™ 84999 L35025
A53544
myPap Billing and Coding
Guidelines (M00051)
A55292
A55293
A54290
A55195
47. TP53 Gene Test 81404
81405
L35025
A53591
TP53 Gene Test Coding and
Billing Guidelines (M00064)
A55484
A55487
A54281 A55221
48. UGT1A1 Gene
Analysis
81350 L35025
A53593
UGT1A1 Gene Analysis
Coding and Billing Guidelines
(M00065)
A55482
A55483
A54280
A55222
49.
VEGFR2 Tests 81479 L35025
A53548
VEGFR2 Tests Coding and
Billing Guidelines (M00055)
A55468
A55469
A54279 A55232
End of Attachment B
^Back to Top Attachment B
Attachment C - LCD Availability Grid
MyPRS™ Test for Multiple Myeloma Gene Expression Profile
(CPT code 81479) CMS website accessed June 7, 2018
IMPORTANT NOTE: Use the applicable LCD based on member’s residence/place of service AND type of service.
LCD ID LCD Title Contractor Type Contractor States
L35396 Biomarkers for Oncology A and B MAC Novitas Solutions, Inc. CO, NM, OK, TX, AR, LA, MS
DE, DC, MD, NJ, PA
End of Attachment C

Page 22 of 25
UHC MA Coverage Summary: Genetic Testing
Proprietary Information of UnitedHealthcare. Copyright 2018 United HealthCare Services, Inc.
Attachment D - LCD Availability Grid
APC and MYH Gene Testing for Familial Adenomatous Polyposis (FAP), Attenuated FAP (AFAP), or MYH-
associated Polyposis
(CPT codes 81201, 81202, 81203) CMS website accessed June 7, 2018
IMPORTANT NOTE: Use the applicable LCD based on member’s residence/place of service AND type of service.
LCD ID LCD Title Contractor Type Contractor States
L35062 Biomarkers Overview
A and B MAC Novitas Solutions, Inc. AR, CO, DC, DE, LA, MD, MS, NJ, NM,
OK, PA, TX
L36827 MolDX: APC and MUTYH Gene
Testing
A and B MAC Palmetto GA AL, GA, SC, TN, VA, WV, NC
L35025 MolDX: Molecular Diagnostic
Tests (MDT)
A and B MAC Palmetto GBA AL, GA, SC, TN, VA, WV, NC
L35160
MolDX: Molecular Diagnostic
Tests (MDT)
A and B MAC Noridian Healthcare Solutions,
LLC
AS, CA, GU, HI, MP, NV
L36256
MolDX: Molecular Diagnostic
Tests (MDT)
A and B MAC Noridian Healthcare Solutions,
LLC
AK, AZ, ID, MT, ND, OR, SD, WA, UT, WY
L36882 MolDX: APC and MUTYH Gene
Testing
A and B MAC Noridian Healthcare Solutions,
LLC
AS, CA, GU, HI, MP, NV
L36884 MolDX: APC and MUTYH Gene
Testing
A and B MAC Noridian Healthcare Solutions,
LLC
AK, AZ, ID, MT, ND, OR, SD, WA, UT, WY
L36021 Molecular Diagnostic Tests
(MDT)
MAC Part A & B CGS Administrators, LLC KY, OH
L36910 MolDX: APC and MUTYH Gene
Testing
MAC Part A & B CGS Administrators, LLC KY, OH
L36807
MolDX: Molecular Diagnostic
Tests (MDT)
MAC - Part A and
B
Wisconsin Physicians Service
Insurance Corporation
IA, IN, KS, MI, MO, NE
L36807
MolDX: Molecular Diagnostic
Tests (MDT)
MAC - Part A Wisconsin Physicians Service
Insurance Corporation
AK, AL, AR, AZ, CT, FL, GA, IA, ID, IL, IN,
KS, KY, LA, MA, ME, MI, MN, MO, MS,
MT, NC, ND, NE, NH, NJ, OH, OR, RI, SC,
SD, TN, UT, VA, VI, VT, WA, WI, WV, WY
L37224 MolDX: APC and MUTYH Gene
Testing
MAC - Part A and
B
Wisconsin Physicians Service
Insurance Corporation
IA, IN, KS, MI, MO, NE
L37224 MolDX: APC and MUTYH Gene
Testing
MAC - Part A Wisconsin Physicians Service
Insurance Corporation
AK, AL, AR, AZ, CT, FL, GA, IA, ID, IL, IN,
KS, KY, LA, MA, ME, MI, MN, MO, MS,
MT, NC, ND, NE, NH, NJ, OH, OR, RI, SC,
SD, TN, UT, VA, VI, VT, WA, WI, WV, WY
L35000 Molecular Pathology Procedures A and B MAC National Government
Services, Inc.
CT, IL, MA, ME, MN, NH, NY, RI, VT, WI
L34519 Molecular Pathology Procedures A and B MAC First Coast Service Options,
Inc.
FL, PR, VI
End of Attachment D
Attachment E - LCD Availability Grid
Ovarian Cancer Biomarker Panels
[OVA1™ (CPT code 81503) , ROMA™ (CPT code 84999)] CMS website accessed June 7, 2018
IMPORTANT NOTE: Use the applicable LCD based on member’s residence/place of service AND type of service.
LCD ID LCD Title Contractor Type Contractor States

Page 23 of 25
UHC MA Coverage Summary: Genetic Testing
Proprietary Information of UnitedHealthcare. Copyright 2018 United HealthCare Services, Inc.
Attachment E - LCD Availability Grid
Ovarian Cancer Biomarker Panels
[OVA1™ (CPT code 81503) , ROMA™ (CPT code 84999)] CMS website accessed June 7, 2018
IMPORTANT NOTE: Use the applicable LCD based on member’s residence/place of service AND type of service.
LCD ID LCD Title Contractor Type Contractor States
L35396 Biomarkers for Oncology A and B MAC Novitas Solutions, Inc. AR, CO, DC, DE, LA, MD, MS, NJ, NM,
OK, PA, TX
L35160 MolDX: Molecular Diagnostic
Tests (MDT)
A and B MAC Noridian Healthcare Solutions,
LLC
AS, CA, GU, HI, MP, NV
L36256 MolDX: Molecular Diagnostic
Tests (MDT)
A and B MAC Noridian Healthcare Solutions,
LLC
AK, AZ, ID, MT, ND, OR, SD, WA, UT, WY
L35025 MolDX: Molecular Diagnostic
Tests (MDT)
A and B MAC Palmetto GBA AL, GA, SC, TN, VA, WV, NC
L36807
MolDX: Molecular Diagnostic
Tests (MDT)
MAC Part A & B Wisconsin Physicians Service
Insurance Corporation
IA, IN, KS, MI, MO, NE
L36807
MolDX: Molecular Diagnostic
Tests (MDT)
MAC Part A Wisconsin Physicians Service
Insurance Corporation
AK, AL, AR, AZ, CT, FL, GA, IA, ID, IL, IN,
KS, KY, LA, MA, ME, MI, MN, MO, MS,
MT, NC, ND, NE, NH, NJ, OH, OR, RI, SC,
SD, TN, UT, VA, VI, VT, WA, WI, WV, WY
L36021 Molecular Diagnostic Tests
(MDT)
MAC Part A & B CGS Administrators, LLC KY, OH
L35000
Molecular Pathology
Procedures
MAC Part A & B
A and B MAC
National Government
Services, Inc.
CT, IL, ME, MA, MN, NH, NY, RI, VT, WI
L33629 Non-covered Services MAC Part A & B
A and B MAC
National Government
Services, Inc.
CT, IL, ME, MA, MN, NH, NY, RI, VT, WI
End of Attachment E
Attachment F - LCD Availability Grid
VeriStrat® Assay
(CPT Code 81538) CMS website accessed June 7, 2018
IMPORTANT NOTE: Use the applicable LCD based on member’s residence/place of service AND type of service.
LCD ID LCD Title Contractor Type Contractor States
L35396 Biomarkers for Oncology A and B MAC Novitas Solutions, Inc. AR, CO, DC, DE, LA, MD, MS, NJ, NM,
OK, PA, TX
L35160 MolDX: Molecular Diagnostic
Tests (MDT)
A and B MAC Noridian Healthcare Solutions,
LLC
AS, CA, GU, HI, MP, NV
L36256 MolDX: Molecular Diagnostic
Tests (MDT)
A and B MAC Noridian Healthcare Solutions,
LLC
AK, AZ, ID, MT, ND, OR, SD, WA, UT, WY
L35025 MolDX: Molecular Diagnostic
Tests (MDT)
A and B MAC Palmetto GBA AL, GA, SC, TN, VA, WV, NC
L36807 MolDX: Molecular Diagnostic
Tests (MDT)
MAC Part A & B Wisconsin Physicians Service
Insurance Corporation
IA, IN, KS, MI, MO, NE
L36807
MolDX: Molecular Diagnostic
Tests (MDT)
MAC Part A Wisconsin Physicians Service
Insurance Corporation
AK, AL, AR, AZ, CT, FL, GA, IA, ID, IL, IN,
KS, KY, LA, MA, ME, MI, MN, MO, MS,
MT, NC, ND, NE, NH, NJ, OH, OR, RI, SC,
SD, TN, UT, VA, VI, VT, WA, WI, WV, WY

Page 24 of 25
UHC MA Coverage Summary: Genetic Testing
Proprietary Information of UnitedHealthcare. Copyright 2018 United HealthCare Services, Inc.
Attachment F - LCD Availability Grid
VeriStrat® Assay
(CPT Code 81538) CMS website accessed June 7, 2018
IMPORTANT NOTE: Use the applicable LCD based on member’s residence/place of service AND type of service.
LCD ID LCD Title Contractor Type Contractor States
L36021 Molecular Diagnostic Tests
(MDT)
MAC Part A & B CGS Administrators, LLC KY, OH
L35000
Molecular Pathology
Procedures
MAC Part A & B
A and B MAC
National Government
Services, Inc.
CT, IL, ME, MA, MN, NH, NY, RI, VT, WI
End of Attachment F
Attachment G - LCA Availability Grid
Next Generation Sequencing (NGS)
(CPT code 81479) CMS website accessed June 7, 2018
IMPORTANT NOTE: Use the applicable LCD based on member’s residence/place of service AND type of service.
LCD ID LCD Title Contractor Type Contractor States
A55624 MolDX: Next Generation
Sequencing Billing and
Coding Guidelines
A and B MAC Noridian Healthcare
Solutions, LLC
AS, CA, GU, HI, MP, NV
A55629 MolDX: Next Generation
Sequencing Billing and
Coding Guidelines
A and B MAC Noridian Healthcare
Solutions, LLC
AK, AZ, ID, MT, ND, OR, SD, WA, UT, WY
A54901 MolDX: Next Generation
Sequencing Billing and
Coding Guidelines
MAC Part A & B CGS Administrators, LLC KY, OH
A54795 MolDX: Next Generation
Sequencing Billing and
Coding Guidelines
A and B MAC Palmetto GBA AL, GA, SC, TN, VA, WV, NC
A55197 MolDX: Next Generation
Sequencing Billing and
Coding Guidelines
MAC Part A & B Wisconsin Physicians
Service Insurance
Corporation
IA, IN, KS, MI, MO, NE
A55197 MolDX: Next Generation
Sequencing Billing and
Coding Guidelines
MAC Part A Wisconsin Physicians
Service Insurance
Corporation
AK, AL, AR, AZ, CT, FL, GA, IA, ID, IL, IN,
KS, KY, LA, MA, ME, MI, MN, MO, MS,
MT, NC, ND, NE, NH, NJ, OH, OR, RI, SC,
SD, TN, UT, VA, VI, VT, WA, WI, WV, WY
End of Attachment G
MAC and States
Attachment A and Attachment B - Addendum
Palmetto AL, GA, NC, SC, TN, VA, WV
<Back to Attachment A – Covered
Noridian AK, AZ, ID, MT, ND, OR, SD, UT, WA, WY
Noridian AS, CA, HI, NV, No. Mariana Islands
CGS KY, OH

Page 25 of 25
UHC MA Coverage Summary: Genetic Testing
Proprietary Information of UnitedHealthcare. Copyright 2018 United HealthCare Services, Inc.
Wisconsin AK, AL, AR, AZ, CT, FL, GA, IA, ID, IL, IN, KS, KY, LA, MA, ME, MI, MN,
MO, MS, MT, NC, ND, NE, NH, NJ, OH, OR, RI, SC, SD, TN, UT, VA, VI,
VT, WA, WI, WV, WY
Tests Grid>
<Back to Attachment B – Excluded
Tests Grid> Novitas AR, CO, DE, LA, MD, MS, NJ, NM, OK, PA, TX
First Coast FL, PR, VI
NGS CT, IL, ME, MA, MN, NH, NY, RI, VT, WI