giovanni scambia. caso clinico donna di 25 anni con cdi trattato con quart + ct. dopo 2 anni rimane...
TRANSCRIPT

Giovanni Scambia
Caso clinico
Donna di 25 anni con CDI trattato con QUART + CT. Dopo 2 anni rimane incinta e partorisce; dopo 7 anni sviluppa meta ossee multiple al rachide con pericolo di crollo vertebrale .

˜25% of breast cancer patients are pre-menopausal (15% pts <45 yrs) at the time of diagnosis
Breast cancer
Premenopausal26%
Postmenopausal74%
ER–46%
ER– 27%
ER+73%
Advanced: 19% Early: 81%
Decision Resources Epidemiology Data
ER+54%
Fattori di rischio, diagnosi e trattamento del BC nella donna giovane
Impatto del trattamento sulla fertilità

Breast Cancer in young women

C.Anders : J Clin Oncol. 2008 Jul 10;26(20):3324-30
Age is an important prognostic factor

C.Anders : J Clin Oncol. 2008 Jul 10;26(20):3324-30
“Breast cancer arising in young women correlates with inferior survival and higher incidence of negative clinical-pathologic features”
Fattori di rischio, diagnosi e trattamento del BC nella donna giovane
Impatto del trattamento sulla fertilità
Implicazioni circa la gravidanza
Most young women will no longer undergo surgical or radiation ovarian ablation but it is recognised that chemotherapy may cause premature ovarian failure,depending upon the woman’s age and the treatment regimen. Scottish Cancer Trials Breast Group ICRF Breast Unit. Lancet 1993: 341: 1293–8.
It has been also reported an increased chance of spontaneous abortions (25% of cases of pregnancy) in women with a history of breast cancer. Velentgas et al, 1999
It has been suggested that up to 7% of women who are fertile after treatment for breast cancer will subsequently have children. Saunders: J R Soc Med 1993: 86: 162–5.

Is pregnancy safe for women survival after a diagnosis of breast cancer?
Is chemotherapy detrimental for ovarian function?
Is LHRH-analogs treatment useful to preserve ovarian function?
What about other options about fertility preservations?

PREGNANCY AFTER BREAST CANCER AND PROGNOSIS
Available data show no adverse effect on survival of pregnancy after a diagnosis of breast cancer
Healthy mother effect !!
Is pregnancy safe for women survival after a diagnosis of breast cancer?
Is chemotherapy detrimental for ovarian function?
Is LHRH-analogs treatment useful to preserve ovarian function?
What about other options about fertility preservations?
Chemotherapy can compromise ovarian function resulting in premature ovarian failure (POF: defined as menopause before the age of 40 years or hypergonadotropic amenorrhea) and infertility (Byrne et al,
1999)
Dependending on the extent of damage to the ovaries, two forms of POF can be distinguished:
1. Acute Ovarian Failure (AOF) = loss of ovarian function during or shortly after the end of chemotherapy
2. Premature menopause = loss of ovarian function that occurs years after the end of chemotherapy (before age 40 yr)
Sklar et al, J Natl Cancer Inst 2005

• A constant number of resting primordial follicles enter the growth phase at any given time, independent of pituitary gonadotropins
• Later stages of maturation require FSH and LH
• Follicles either mature to ovulation or become atresic
Ovarian Structure

… due to a continual process of atresia, the ovarian reserve of primordial follicles is progressively eroded over time (Gosden et al, 1994)
Lobo, N Engl J Med 2005
Gonadotoxic chemotherapy causes marked follicle loss through, presumably, apoptotic cell death
(Ratts et al, 1995; Tilly et al, 2003)

Age of the patient
Type of the cytotoxic agent(s)
Cumulative dose
The likelihood of gonadal failure depend on:
Bines et al, 1996; Goodwin et al, 1999; Meirow et al, 1999
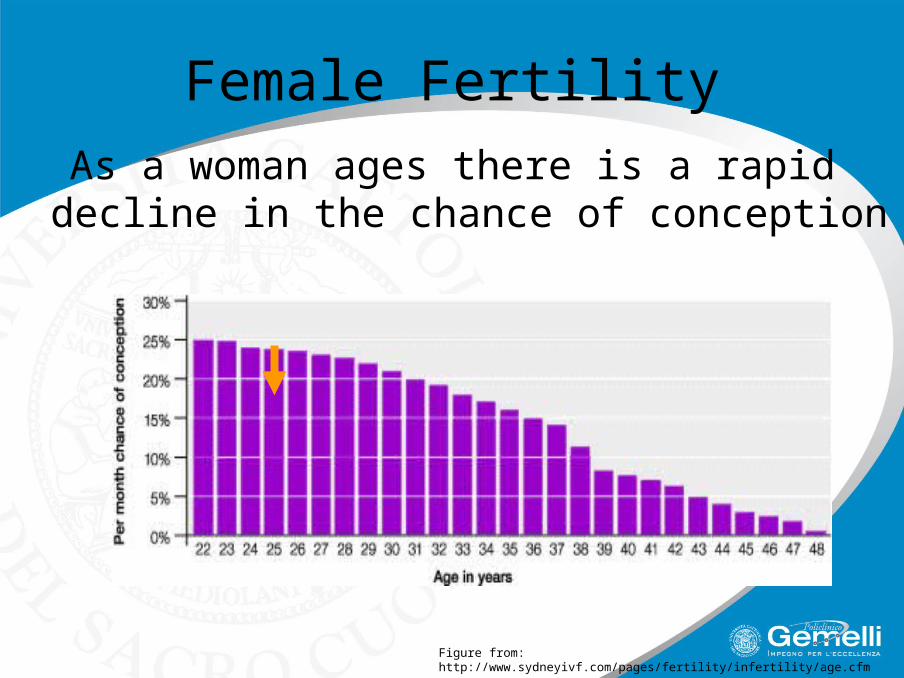
Female Fertility
Figure from: http://www.sydneyivf.com/pages/fertility/infertility/age.cfm
As a woman ages there is a rapid decline in the chance of conception

Treatment for Early Breast Cancer: Effect on Fertility
Graph adapted from Goodwin P, Ennis M, Pritchard K, Trudeau M, Hood N. Risk of menopause during the first year after breast cancer diagnosis. J Clin Oncol 1999;17(8):2365-2370.

• Adjuvant endocrine therapy does not cause permanent infertility
• but …. endocrine therapy usually entails years of treatment when pregnancy contraindicated and aging during that time may compromise fertility
Risk of Treatment induced Amenorrhea

Sonmezer, M. et al. Oncologist 2006;11:422-434
Alkylating agents are extremely gonadotoxic because they are not cell cycle-specific and can damage resting primordial follicles, whereas cycle-specific agents such as MTX and 5-FU do not have any effect on ovarian reserve
Degree of gonadal failure associated with chemotherapeutic agents
High riskCyclophoshamideMelphalanBusulfanChlorambucilProcarbazine
Intermediate riskCisplatinAdriamycin
Low or no riskMethotrexate5-FluorouracilVincristineBleomycinActinomycin D
Paclitaxel?

Copyright ©2006 AlphaMed Press Sonmezer, M. et al. Oncologist 2006;11:422-434
Degree of gonadotoxicity related to the most commonly used chemotherapy regimens in breast cancer

Studies assessing the impact of breast cancer chemotherapy on fertility issue, often use chemotherapy-induced amenorrhea as a surrogate marker for fertility
(Bines et al, 1996; Goodwin et al, 1999; Nabholtz et al, 2002)
BUT… Premenopausal levels of estradiol have been detected in amenorrheic pts after chemotherapy thus indicating persisting ovarian function despite mestrual activity cessation (Braverman et al, 2002)
On the other hand, resumption of menstruation after chemotherapy does not imply that also the fertility has been preserved (Schmidt et al, 2005)

Is chemotherapy detrimental for ovarian function?
Is LHRH-analogs treatment useful to preserve ovarian function?
What about other options about fertility preservations?
Is pregnancy safe for women with breast cancer?
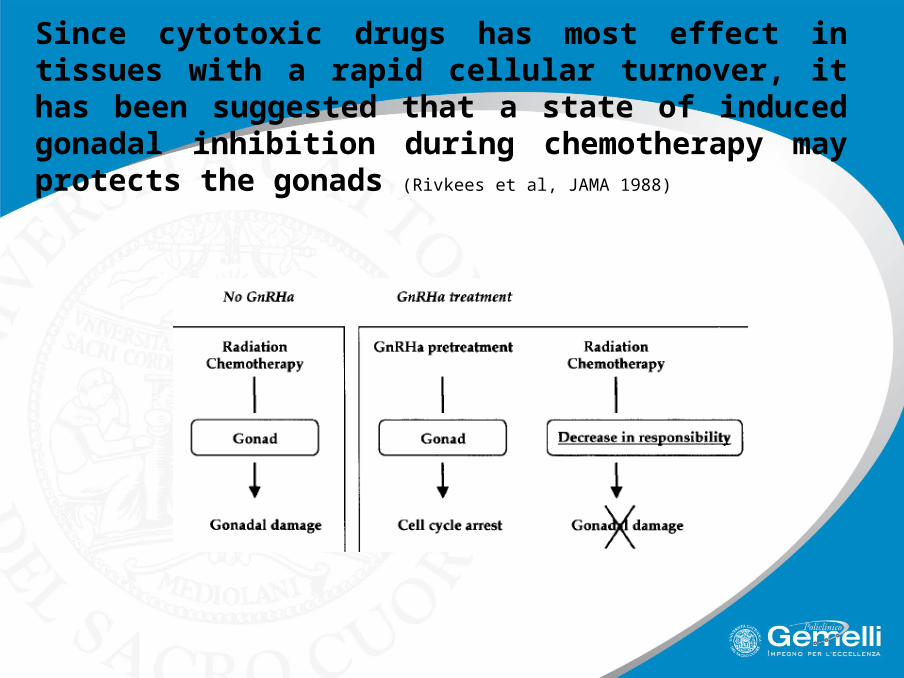
Since cytotoxic drugs has most effect in tissues with a rapid cellular turnover, it has been suggested that a state of induced gonadal inhibition during chemotherapy may protects the gonads (Rivkees et al, JAMA 1988)

18 women, 15-40 yrs, Hodgkin’s or non-Hodgkin’s lymphomas
Chemotherapy + LHRH-a
historical matched control group of 18 women (17-40 yrs) treated with chemotherapy alone
COMPARED TO:

94%
39%
…but the mean follow-up was only 1.7+1.0 years in the study group, compared with 7.0+4.9 years in the control group.
Incidence of amenorrhoea vs regular cyclic ovarian activity
Only 4 out of 16 pts in the study group received CTX (cumulative dose: 609-4500 mg/mq) vs 10 out of 18 in the control group (cumulative dose: 531-14531 mg/mq)
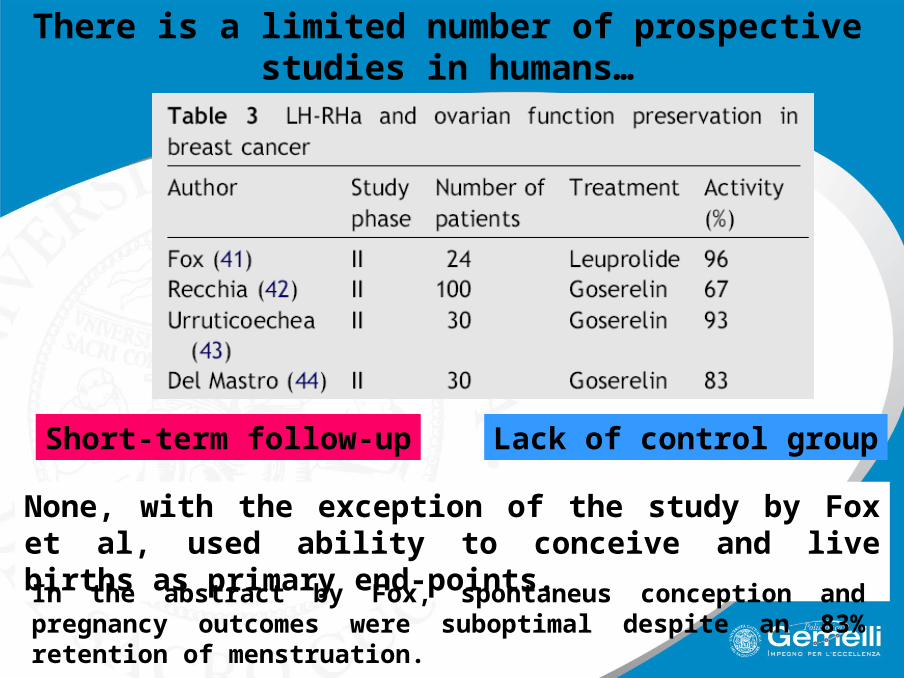
There is a limited number of prospective studies in humans…
Short-term follow-up Lack of control group
None, with the exception of the study by Fox et al, used ability to conceive and live births as primary end-points.
In the abstract by Fox, spontaneus conception and pregnancy outcomes were suboptimal despite an 83% retention of menstruation.

Single center, prospective, single arm, phase II study
29 pts with breast cancer (stage I-III)
GOSERELIN + CHEMOTHERAPYAll but one pt received FEC q21 for 6 cycles
Goserelin 3.6 mg s.c., at least 1 week before the first cycle of chtPts with HR+, received tamoxifen at the end of chemotherapy and if a resumption of menstrual activity was observed during the 12-month follow-up, they restarted goserelin and continued it for at least 2 yrs

RESULTS
Pts with resumption of menses 21 (72%)
Pts without menses but FSH <40 IU/l 24 (83%)
Expected rate of menses resumption with CEF regimens is nearly 40%
FSH <40 IU/l was not predictive of menses resumption
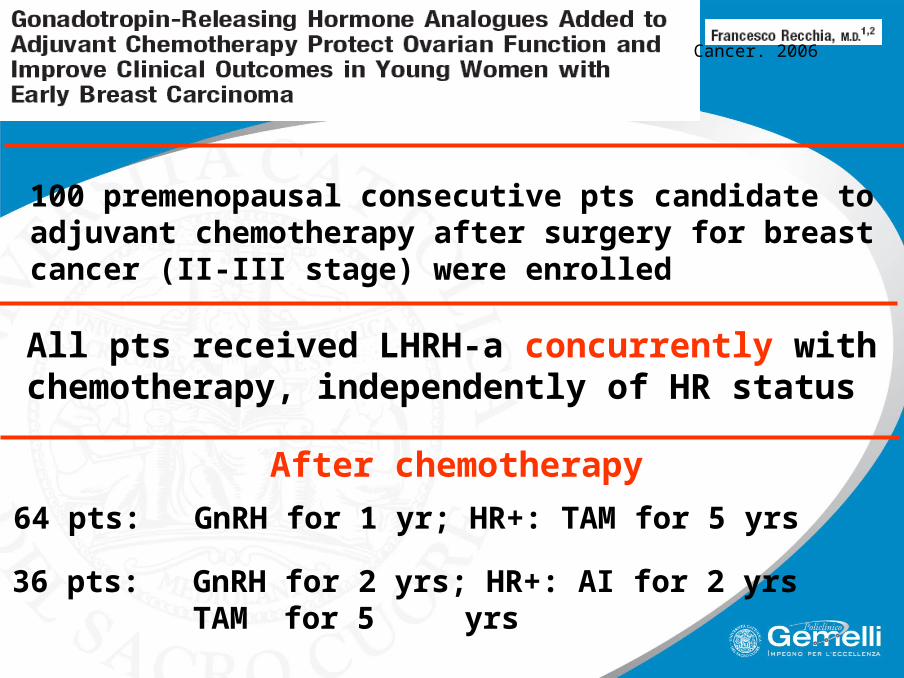
100 premenopausal consecutive pts candidate to adjuvant chemotherapy after surgery for breast cancer (II-III stage) were enrolled
All pts received LHRH-a concurrently with chemotherapy, independently of HR status
64 pts: GnRH for 1 yr; HR+: TAM for 5 yrs
36 pts: GnRH for 2 yrs; HR+: AI for 2 yrs TAM for 5 yrs
After chemotherapy
Cancer. 2006
RESULTS
After a median follow-up of 75 months, NORMAL MENSES were RESUMED by 67% of patients
(100% for pts <40 yr and 56% for pts >40 yr)
The addition of a GnRH analog to adjuvant chemotherapy and temporary estrogen suppression in pts with ER+ disease protected long-term ovarian function, and appeared to improve the expected clinical outcome

but …..
… treatment with LHRH-a has been continued for two yrs in ER- women …. ?
No planned sample size: this is an observational study rather than a phase II study
The lack of a study design and the small number of pts do not allow to draw valid conclusions on clinical outcome

ASCO Recommendations on Fertility Preservation in Cancer Patients
(Expert Panel, J Clin Oncol 2006)
At this time, since there is insufficient evidence regarding the safety and effectiveness of GnRH analogs and other means of ovarian suppression on female fertility preservation, women interested in ovarian suppression for this purpose are encouraged to partecipate in clinical trials

SWOG 0230 study
It is an ongoing phase III study, in which ER- and PR-negative young breast cancer pts are randomized to receive chemotherapy alone or chemotherapy plus LHRH-a to evaluate the role of LHRH-a in the ovarian function preservation

Prospective, multicenter, randomized, phase III study
PROMISE-GIM6
Premenopausal Women, 18-45 yrs, stage I-III breast cancer, HR+/-, candidate for adjuvant chemotherapy
Chemotherapy Chemotherapy +
TriptorelinPrimary endpoint
Incidence of chemotherapy-induced early menopause (at 1 year following the completion of cht, measured by FSH, E2, menses resumption)
Study start: Sept 2003Projected accrual: 280 pts
Is pregnancy safe for women survival after a diagnosis of breast cancer?
Is chemotherapy detrimental for ovarian function?
Is LHRH-analogs treatment useful to preserve ovarian function?
What about other options about fertility preservations?

Is chemotherapy detrimental for ovarian function?
Is LHRHa treatment useful to preserve ovarian function?
YES
YES
Waiting for phase III studies
Is pregnancy safe for women survival after a diagnosis of breast cancer?