glsg/osho study group - kompetenznetz- · pdf fileglsg/osho study group study concepts •...
TRANSCRIPT

Supported by
Deutsche Krebshilfe
GLSG/OSHO Study Group
GLSG/OSHO Study Group
Study Concepts
• Follicular Lymphomas
• Mantel Cell Lymphomas
• Waldenstroem s Disease

Palliation
of Symptomes
Prolongation
of Life
Cure
Key Steps in Improving Treatment for
Follicular Lymphoma
until mid 1990ies
Cytostatic Drugs
Radiation
since mid 1990ies
Antibodies
ASCT

CVP 64 % 14 mo 83 %
R-CVP 87 % (p<0.0001)
38 mo (p<0.001)
89 % (p=0.022)
Marcus et al. 2008
CHOP 90 % 31 mo 90 %
R-CHOP 96 % (p=0.011)
n.r. (p=0.0006)
95 % (p=0.016)
Hiddemann et al. 2005
MCP 75 % 26 mo 74 %
R-MCP 92 % (p=0.0009)
n.r. (p<0.0001)
87 % (p=0.0096)
Herold et al. 2007
CHVP+IFN 72 % 35 mo 79 %
R-CHVP+IFN 81 % (p<0.0001)
n.r. (p<0.0001)
84 % (p=0.029)
Salles et al. 2008
OR PFS OS
Rituximab – Chemotherapy Combinations

Time to Treatment Failure

Comparison of Two Consecutive Study
Generations of the GLSG Overall Survival

Future Strategies in
Follicular Lymphomas
Induction Therapy in Remission
Rituximab Maintenance
=> Lymphoma Control => Lymphoma Reduction
Chemotherapy plus Rituximab

Follicular Lymphomas
Questions for the Next Steps of Therapy
• Best Chemotherapy to be combined with Rituximab
• Value of Radio-Immuno Therapy
• Value of Stem Cell Transplantation after R Chemo
• Improvement of Rituximab Application
• Improvement of Rituximab Maintenance
• New Antibodies
• New Agents

Adapted from Press. Cancer J Sci Am. 1998;4(suppl 2):S19.
CD22
HLA-DR
CD20
slg
CD19 B Cell
CD37
CD25
CD52
Antibody Therapy for B - Cell Lymphomas
• Targeting agent
– Monoclonal antibody
– Engineered antibody
– Recombinant toxin
• Modifications
– None
– Conjugation
• Radioisotopes
• Drugs
• Toxins
B-Cell

GA101 Mechanisms of Action
*Mössner E, et al. Blood. 2010; June 3; 115:4393-4402; Roche data on file
Lower CDC activity Type II vs. Type I antibody
B cell
Effector
cell
Increased direct cell death Type II vs. Type I antibody
Enhanced ADCC Glycoengineering for increased
affinity to FcγRIIIa
CD20 FcγRIIIa
Complement GA101
10

GALLIUM Phase III - Study Design
Experimental arm GA101 1000 mg d1, d8, d15 cycle 1; d1 cycles 2–6/8 +
CHOP q 21d / CVP q 21 d / Bendamustine 90 mg/m2 d1, d2 q28d
Control arm Rituximab 375 mg/m2 d1 cycles 1-6/8 +
CHOP q 21d / CVP q 21 d / Bendamustine 90 mg/m2 d1, d2 q28d
Patient population 1200 fNHL and 200 MZL
Primary endpoint PFS of 1200 fNHL patients
Maintenance treatment Patients achieving CR or PR continue therapy every
2 months for up to 2 years
Maintenance rituximab q2m 2 years
Maintenance GA101 q2m 2 years
CR/PR Previously untreated
indolent NHL (n=1400)
GA101 1000 mg x 6-8 cycles +
CHOP/CVP/Bendamustine x 6-8 cycles
Rituximab 375 mg/m2 x 6-8 cycles +
CHOP/CVP/Bendamustine x 6-8 cycles CR/PR
Source: www.clinicaltrials.gov

GALLIUM Global Recruitment
February 2013
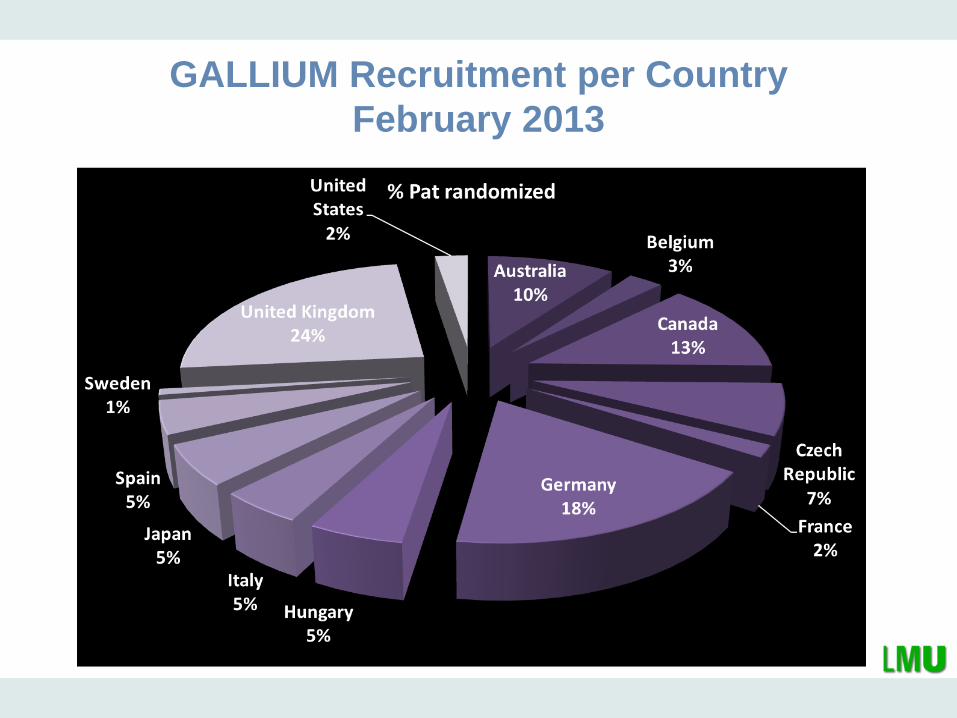
GALLIUM Recruitment per Country
February 2013

GALLIUM - Lymphoma Subtypes
February 2013

GALLIUM - Chemotherapy chosen by Center for FL

GALLIUM (BO21223):
Timelines for Futility Analysis
FA data availability
IA data availability
Futility 2010 2011 2012 2013 2014 2015 2016 2017 2018 2019 2020
GALLIUM (BO21223) – Phase III G-chemo vs. R-chemo in 1st line iNHL w/maintenance
L
Futility CR
(Feb ’13)
Futility PFS
(May ’15) (Nov ‘19) IA PFS
(Jan ’17)
FA
(Jun ’18)
Futility analysis based on first 170 patients’ response at end of induction

Follicular Lymphomas
Questions for the Next Steps of Therapy
• Best Chemotherapy to be combined with Rituximab
• Value of Radio-Immuno therapy
• Value of Stem Cell Transplantation after R Chemo
• Improvement of Rituximab Application
• Improvement of Rituximab Maintenance
• New Antibodies
• New Agents

Lenalidomide
Mechanism of Action

SLL (N=24)
Marginal (N=24)*
Follicular (N=45)*
All Patients
Eval (N=93)
ITT (N=100)
ORR, n (%) 20(83) 21(88) 44(98) 85(91) 85(85)
CR/Cru 6(25) 16(67) 38(85) 60(65) 60(60)
PR 14(59) 5(21) 6(13) 25(27) 25(25)
SD, n (%) 2(8) 3(13) 1(2) 6(6) 6(6)
PD, n (%) 2(8) 0 0 2(2) 2(2)
Fowler, N. et al. ICML 2011. Abst#137.
Lenalidomide plus Rituximab
First Line Therapy of Follicular Lymphoma

R
1st line
FL
n = 1000
R2 Maintenance
2 Years Rituximab Maintenance
R2
R-Chemo
CR, CRu, PR
CR, CRu, PR
R-Chemo
R-CHOP (6x), R-CVP (8x), R-B (6x)
International, multi-centre, randomised study
R2 maintenance
2 Years of Rituximab
Maintenance
1 Year of Lenalidomide
Maintenance
R2 Induction
Lenalidomide 20 mg d 2-22 for 6 Cycles
Ritux 4xCycle 1, 1x Cycles 2-6
RELEVANCE : Phase 3 Study Design (Rituximab and LEnalidomide Versus ANy ChEmotherapy, FL-001)

Therapy of follicular Lymphomas:
GLSG/OSHO Gruppe 1
„Fit patient“
Organfunktion
Funktioneller
Status
Lebenserwartung
Komorbidität
Toxizitätsrisiko
Gruppe 3
„Frail patient“
Organfunktion
Funktioneller Status
Lebenserwartung
Komorbidität
Toxizitöätsrisiko
Gruppe 2
„Compromised
patient“
Organfunktion
Funktioneller Status
Lebenserwartung
Komorbidität
Toxizitätsrisiko
„Go go“
Intensive
Chemotherapie
=> anhaltende
Remissionen
„Slow go“
Weniger
belastende
Chemotherapie
=> Zurückdrängen
des Lymphoms
„No go“
„supportive“
Therapie
=> Syptomkontrolle
GALLIUM
CHOP/Benda-R
Rituximab
Maintenance
GA 101
Maintenance
CHOP/Benda-G
RELEVANCE
R- Chemo R- 2
Rituximab
Maintenance
R - 2
Maintenance

Therapy of follicular Lymphomas:
GLSG/OSHO/StiL
Gruppe 1
„Fit patient“
Organfunktion
Funktioneller Status
Lebenserwartung
Komorbidität
Toxizitätsrisiko
Gruppe 3
„Frail patient“
Organfunktion
Funktioneller Status
Lebenserwartung
Komorbidität
Toxizitöätsrisiko
Gruppe 2
„Compromised patient“
Organfunktion
Funktioneller Status
Lebenserwartung
Komorbidität
Toxizitätsrisiko
„Go go“
Intensive Chemotherapie
=> anhaltende
Remissionen
„Slow go“
Weniger belastende
Chemotherapie
=> Zurückdrängen des
Lymphoms
„No go“
„supportive“ Therapie
=> Syptomkontrolle


Off study
4 x Rituximab
+ 1x Rituximab
A
B
R
A
N
D
O
M
I
S
A
T
I
O
N
4x R - Bendamustine
+ 1 x Rituximab
CR
PR
SD
PD
Re -
Staging
Week 16
Rituximab
375 mg/m²
every 8 weeks
week 2 1 , 29 , 3 7
Induction
CR
PR
SD
Rituximab
375 mg/m²
every 8 weeks
week 2 1 , 29 , 3 7
Observation
Observation
Study Design – Medically Non-Fit
GLSG/OSHO Study Group
Study Concepts
• Follicular Lymphomas
• Mantel Cell Lymphomas
• Waldenstroem s Disease
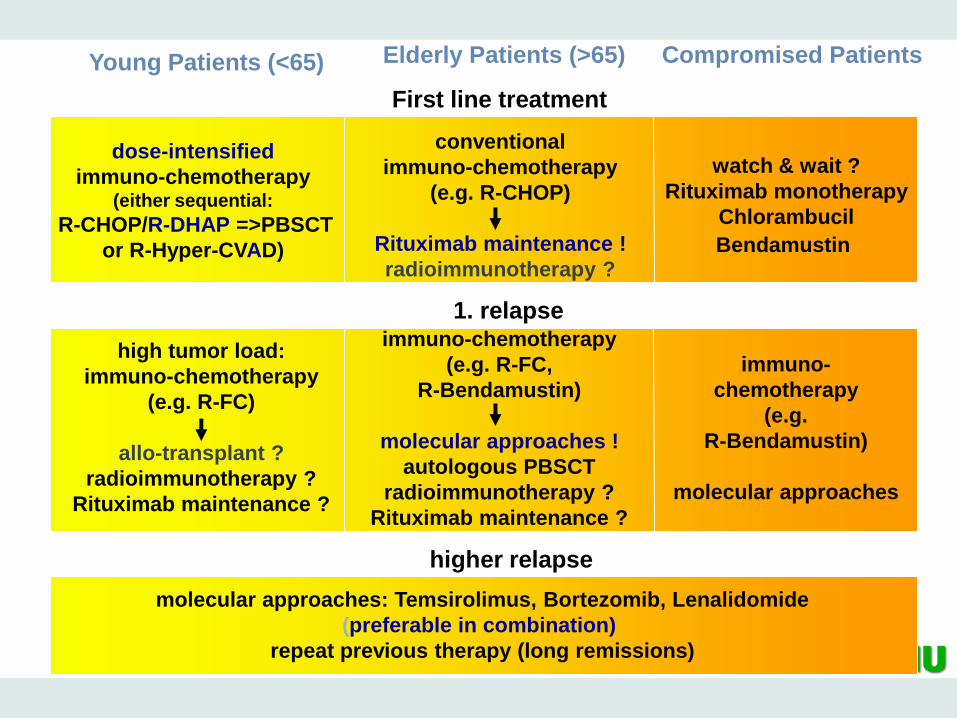
Young Patients (<65) Elderly Patients (>65) Compromised Patients
First line treatment
conventional
immuno-chemotherapy
(e.g. R-CHOP)
Rituximab maintenance !
radioimmunotherapy ?
watch & wait ?
Rituximab monotherapy
Chlorambucil
Bendamustin
1. relapse
high tumor load:
immuno-chemotherapy
(e.g. R-FC)
allo-transplant ?
radioimmunotherapy ?
Rituximab maintenance ?
immuno-chemotherapy
(e.g. R-FC,
R-Bendamustin)
molecular approaches !
autologous PBSCT
radioimmunotherapy ?
Rituximab maintenance ?
immuno-
chemotherapy
(e.g.
R-Bendamustin)
molecular approaches
higher relapse
molecular approaches: Temsirolimus, Bortezomib, Lenalidomide
(preferable in combination)
repeat previous therapy (long remissions)
dose-intensified
immuno-chemotherapy (either sequential:
R-CHOP/R-DHAP =>PBSCT
or R-Hyper-CVAD)

European MCL Network
Patients <65 Years
PR, CR!
Cyclo 120mg/kg
+ TBI 12 Gray
PBSCT
PR, CR!
3 x R-CHOP
3 x R-DHAP
alternating
(stem cell
mobilization after
course 4)
PBSCT
TBI 10 Gray
Ara-C 4 x 1.5 g/m2
Melphalan 140 mg/m2
3 x R-CHOP
DexaBEAM (stem cell mobilization)
3 x R-CHOP
Hermine, ASH 2012
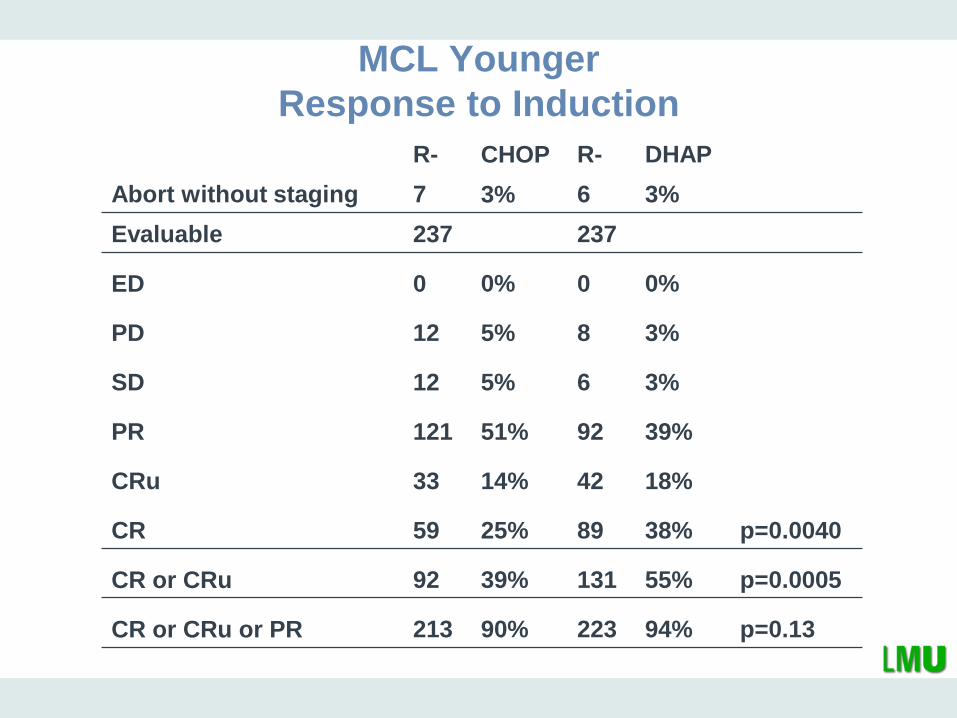
MCL Younger
Response to Induction
R- CHOP R- DHAP
Abort without staging 7 3% 6 3%
Evaluable 237 237
ED 0 0% 0 0%
PD 12 5% 8 3%
SD 12 5% 6 3%
PR 121 51% 92 39%
CRu 33 14% 42 18%
CR 59 25% 89 38% p=0.0040
CR or CRu 92 39% 131 55% p=0.0005
CR or CRu or PR 213 90% 223 94% p=0.13

MCL younger
Time to Treatment Failure
Hermine, ASH 2012

MCL younger
Overall Survival
Hermine, ASH 2012

Young Patients (<65) Elderly Patients (>65) Compromised Patients
First line treatment
conventional
immuno-chemotherapy
(e.g. R-CHOP)
Rituximab maintenance !
radioimmunotherapy ?
watch & wait ?
Rituximab monotherapy
Chlorambucil
Bendamustin
1. relapse
high tumor load:
immuno-chemotherapy
(e.g. R-FC)
allo-transplant ?
radioimmunotherapy ?
Rituximab maintenance ?
immuno-chemotherapy
(e.g. R-FC,
R-Bendamustin)
molecular approaches !
autologous PBSCT
radioimmunotherapy ?
Rituximab maintenance ?
immuno-
chemotherapy
(e.g.
R-Bendamustin)
molecular approaches
higher relapse
molecular approaches: Temsirolimus, Bortezomib, Lenalidomide
(preferable in combination)
repeat previous therapy (long remissions)
dose-intensified
immuno-chemotherapy (either sequential:
R-CHOP/R-DHAP =>PBSCT
or R-Hyper-CVAD)

European MCL Network
Patients >60 Years
4 x R-CHOP
PR, CR
IFN-α maintenance
(3 x 3 M IU/week)
or Peg-IFN (1mg/kg week)
4 x R-CHOP
PR, CR
3 x R-FC
Rituximab
maintenance (all 2 months)
3 x R-FC
Kluin-Nelemans, NEJM 2012

MCL Elderly: Response to Induction
R-CHOP R-FC All
Documented 274 276 550
Premature stop 7 3% 11 4% 18
Evaluable 267 265 532
ED 12 4% 8 3%
PD 15 6% 36 14%
SD 17 6% 13 5%
PR 100 37% 73 28%
CRu 37 14% 33 12%
CR 86 32% 102 38% p=0.15
CR/CRu 123 46% 135 51% p=0.30
CR/CRu/PR 223 84% 208 78% p=0.15

MCL Elderly: Toxicity of Induction
R-CHOP
(n 261)
R-FC (n
272)
Toxicity p Grade freq % freq %
Hemoglobin 0.059 1/2 175 67 160 60
3/4 33 13 54 20
Leukocytes 0.002 1/2 75 29 50 18
3/4 153 59 199 73
Granulocytes 0.097 1/2 48 19 42 17
3/4 150 60 168 69
Platelets <0.001 1/2 82 32 107 40
3/4 49 19 110 41
Lymphocytes 0.004 1/2 47 19 22 9
3/4 169 69 193 78
R-CHOP
R-FC
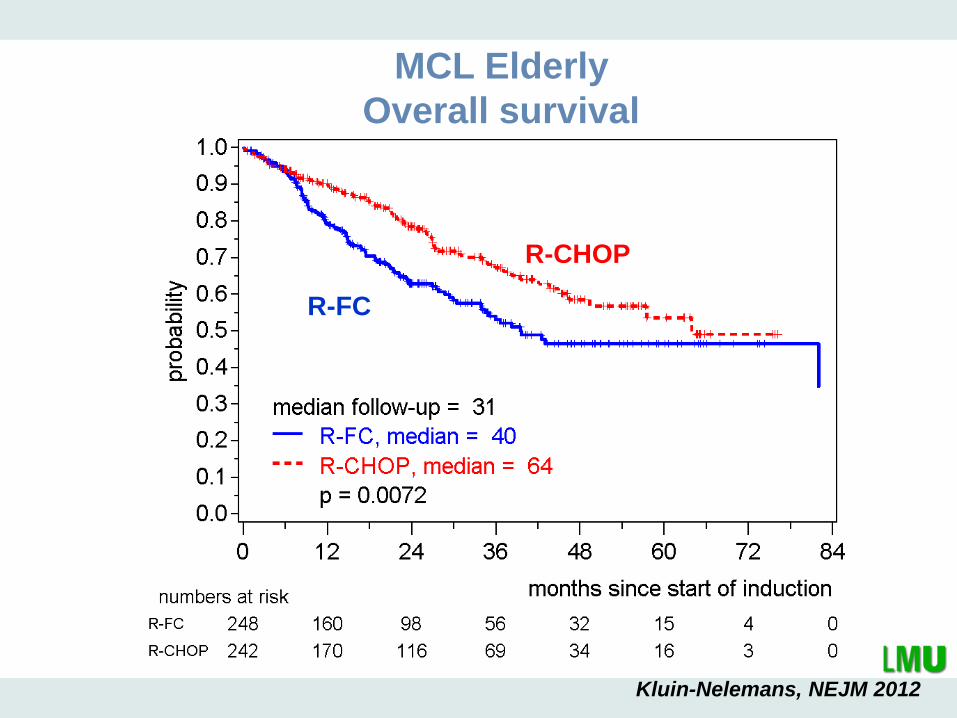
MCL Elderly
Overall survival
Kluin-Nelemans, NEJM 2012

European MCL Network
Patients >60 Years
4 x R-CHOP
PR, CR
IFN-α maintenance
(3 x 3 M IU/week)
or Peg-IFN (1mg/kg week)
4 x R-CHOP
PR, CR
3 x R-FC
Rituximab
maintenance (all 2 months)
3 x R-FC
Kluin-Nelemans, ASH 2011
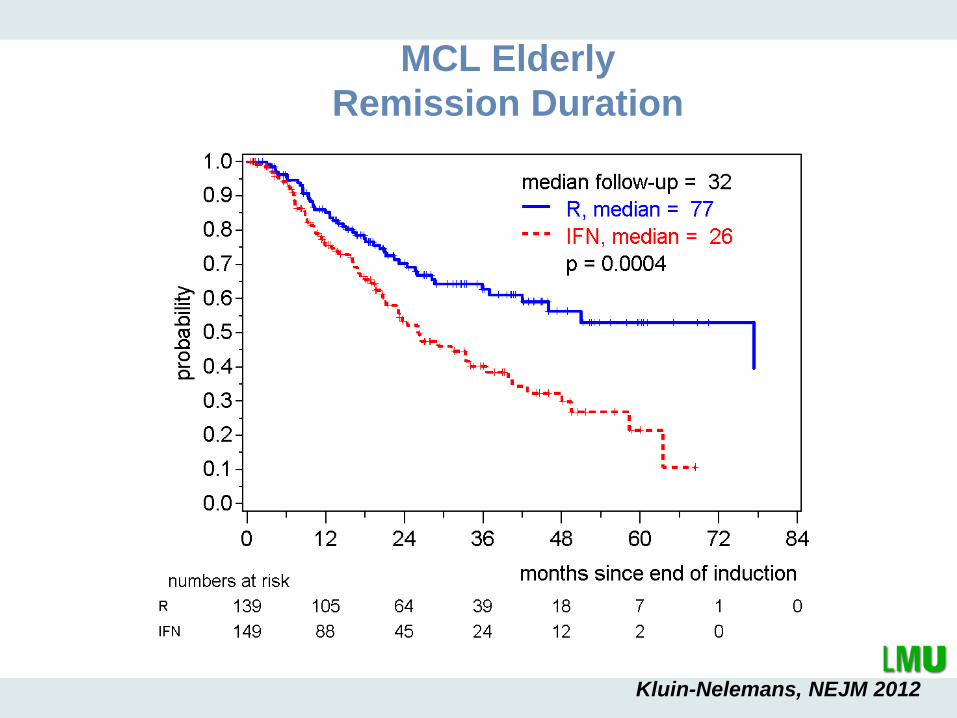
MCL Elderly
Remission Duration
Kluin-Nelemans, NEJM 2012

MCL Elderly
Response Duration
After R-CHOP After R-FC
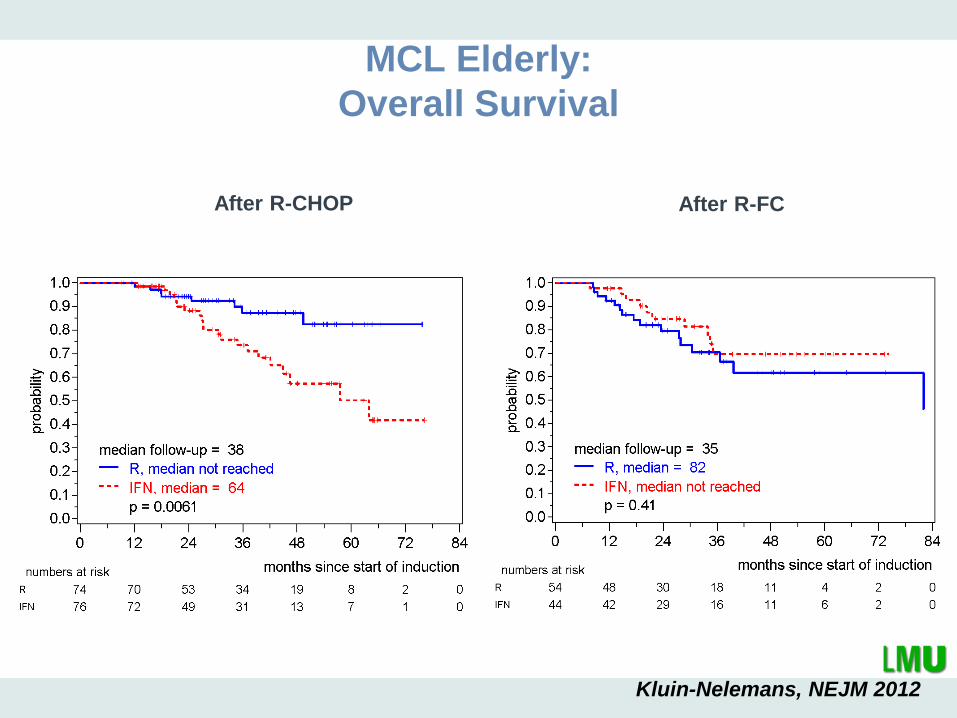
MCL Elderly:
Overall Survival
After R-CHOP After R-FC
p=0.055 for interaction of induction and maintenance
Kluin-Nelemans, NEJM 2012

< 65 years > 65 years
R-HAD +/- Bortezomib
1. Relapse
European MCL Network: new studies 2013
2. Relapse (or not qualifying for R-HAD)
First line
BeRT BR-Temsirolimus
Ibrutinib vs
Temsirolimus
MCL elderly R2:
R-CHOP vs R-CHOP/Ara-C
=> Rituximab M
+/-Lenalidomide
MCL younger:
R-CHOP/DHAP
=> low risk: ASCT vs. I .
high risk: ASCT-> R vs I
MCL elderly I:
BR +/- Ibrutinib
=> Rituximab M
+/- Ibrutinib

GLSG/OSHO Study Group
• Follicular Lymphomas
• Mantel Cell Lymphomas
• Waldenstroem s Disease