glucose and cv disease and glucose • how common is diabetes? • diabetes as a risk for cvd •...
TRANSCRIPT
Glucose and CV disease
Copyright © 2017 by Sea Courses Inc.
All rights reserved. No part of this document may be
reproduced, copied, stored, or transmitted in any form
or by any means – graphic, electronic, or mechanical,
including photocopying, recording, or information
storage and retrieval systems without prior written
permission of Sea Courses Inc. except where
permitted by law.
Sea Courses is not responsible for any speaker or
participant’s statements, materials, acts or omissions.
Diabetes and glucose
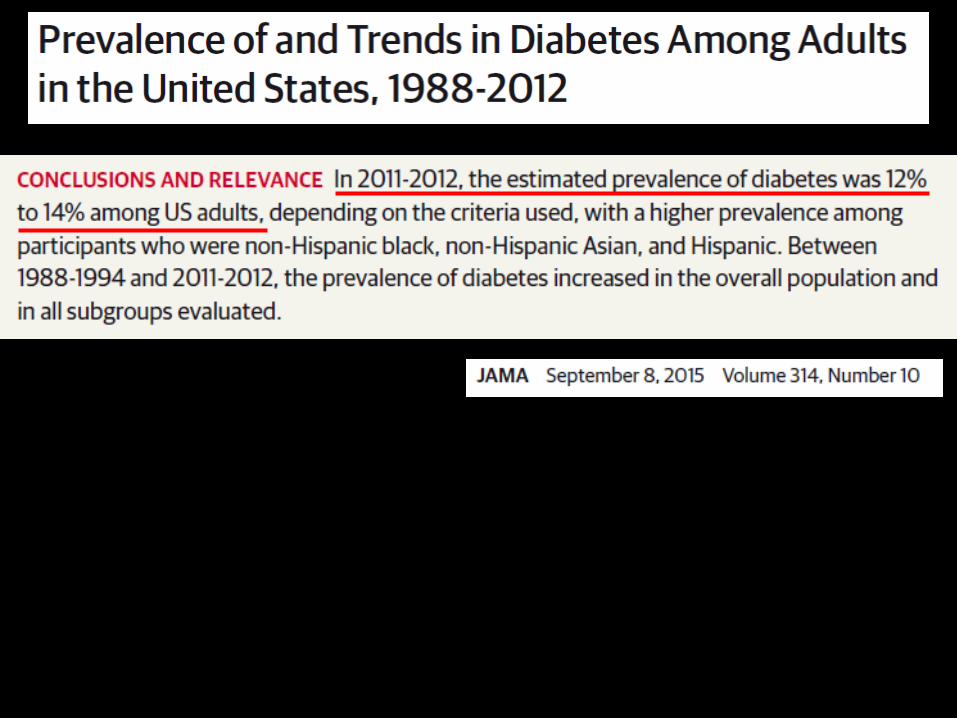
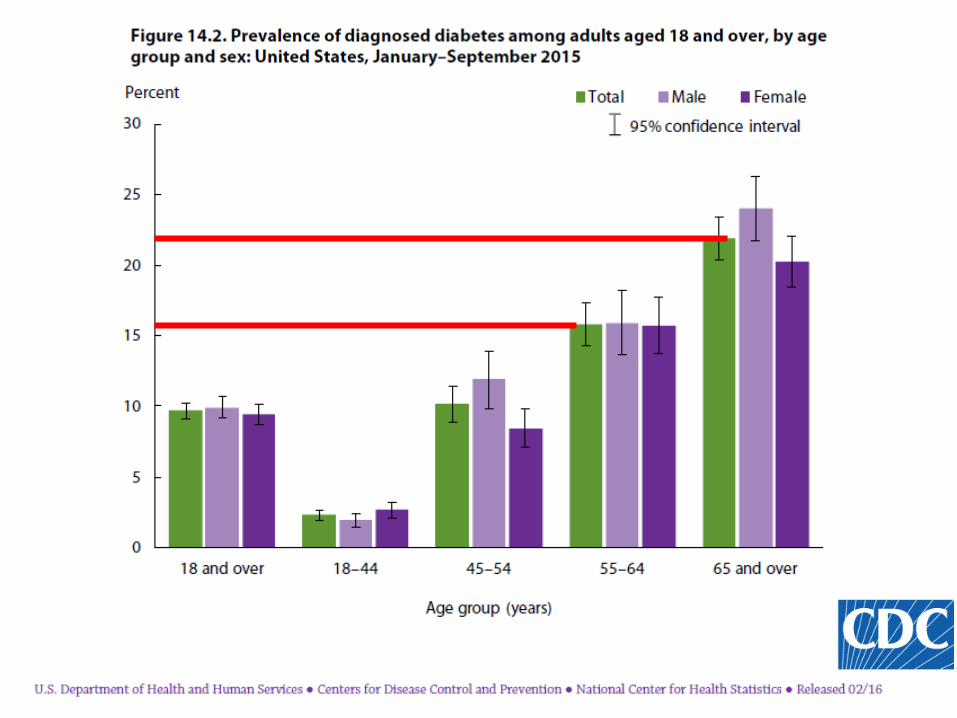
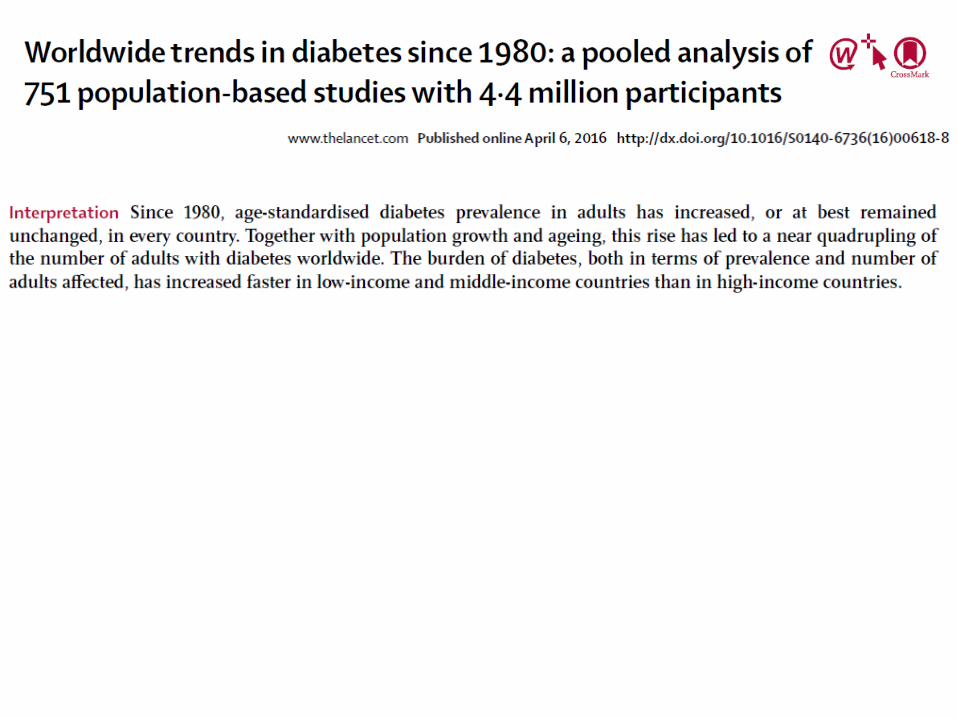
• How common is diabetes?
• Diabetes as a risk for CVD
• Does improving glucose control prevent complications?
• Does too tight glucose control cause death?
• Glucose vs glycation
– Hemoglobin Glycation Index
• What should our A1c target be?
Diabetes and glucose
• How common is diabetes?
• Diabetes as a risk for CVD
• Does improving glucose control prevent complications?
• Does too tight glucose control cause death?
• Glucose vs glycation
– Hemoglobin Glycation Index
• What should our A1c target be?

Diabetes-related complications in the USA, 1990-2010Acute myocardial infarction
Adapted from Gregg EW, et al. N Engl J Med 2014;370:1514–1523. Presented at the American Diabetes Association 76th Scientific Sessions, Session 3-CT-SY24. June 13 2016, New Orleans, LA, USA.

Diabetes and glucose
• How common is diabetes?
• Diabetes as a risk for CVD.
• Does improving glucose control prevent complications?
• Does too tight glucose control cause death?
• Glucose vs glycation
• Hemoglobin Glycation Index
• What should our A1c target be?
Diabetes and glucose
• How common is diabetes?
• Diabetes as a risk for CVD. Does A1c make a difference?
• Does improving glucose control prevent complications?
• Does too tight glucose control cause death?
• Glucose vs glycation
• Hemoglobin Glycation Index
• What should our A1c target be?
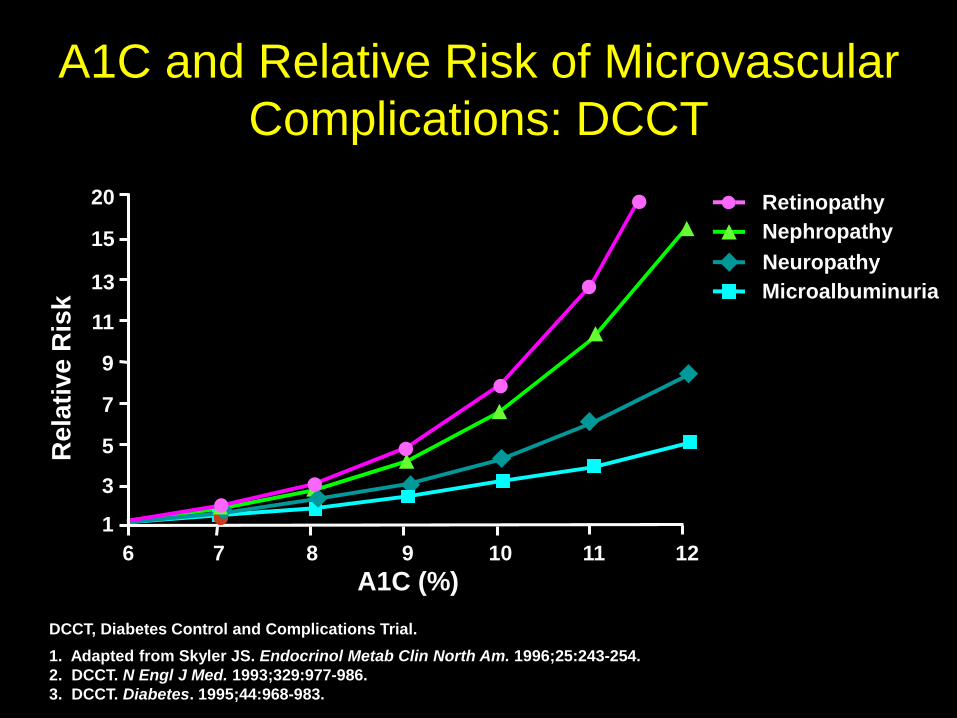
DCCT, Diabetes Control and Complications Trial.
1. Adapted from Skyler JS. Endocrinol Metab Clin North Am. 1996;25:243-254.
2. DCCT. N Engl J Med. 1993;329:977-986.
3. DCCT. Diabetes. 1995;44:968-983.
Re
lati
ve
Ris
k
A1C (%)
15
13
11
9
7
5
3
1
6 7 8 9 10 11 12
A1C and Relative Risk of Microvascular
Complications: DCCT
Retinopathy
Nephropathy
Neuropathy
Microalbuminuria
20
17
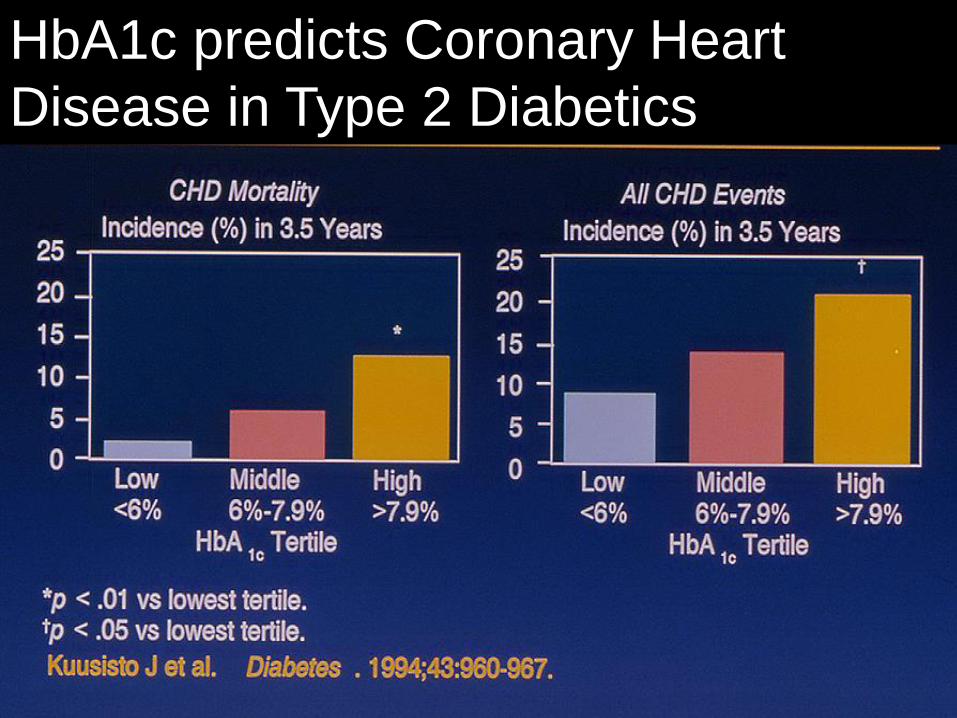
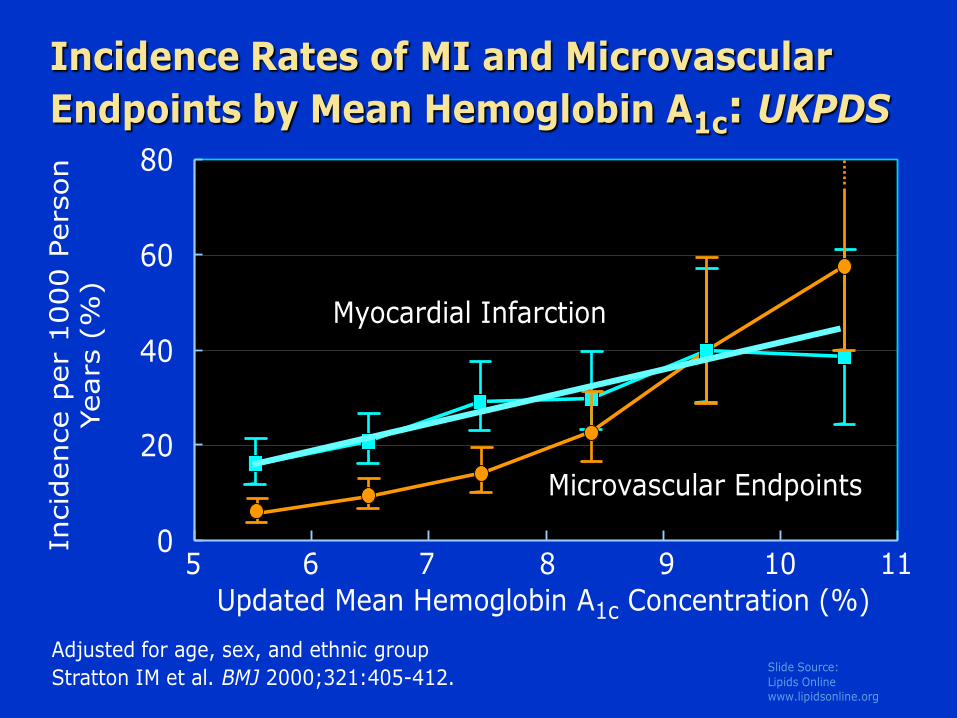
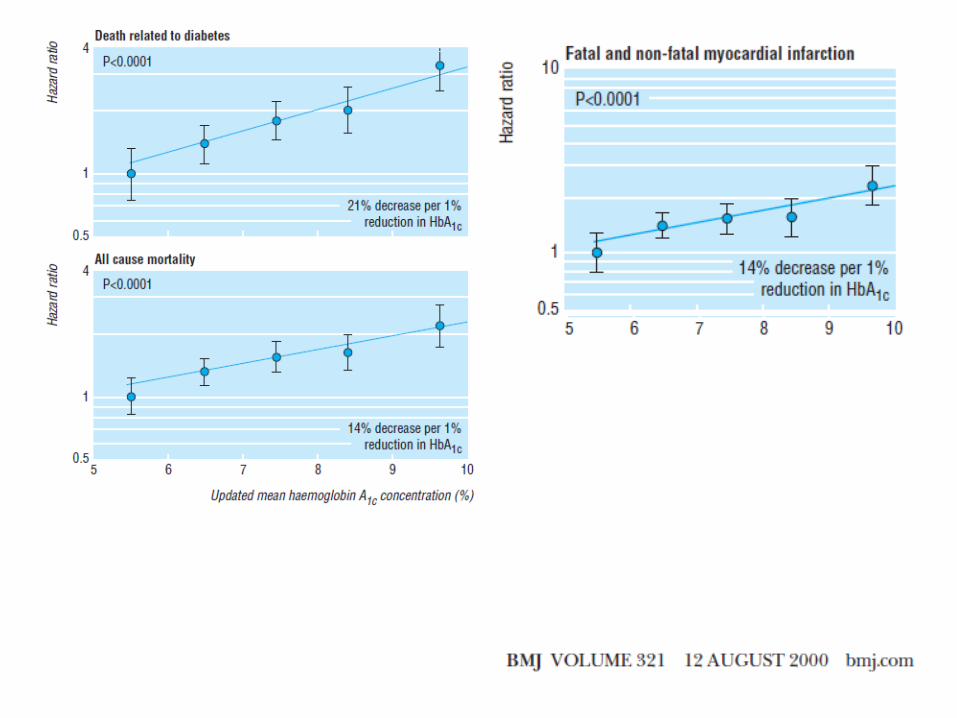
HbA1c predicts Coronary Heart
Disease in Type 2 Diabetics
ukpdsSlide Source:
Lipids Onlinewww.lipidsonline.org
0
20
40
60
80
Incidence Rates of MI and Microvascular
Endpoints by Mean Hemoglobin A1c: UKPDS
5 6 7 8 9 10 11
Incid
ence p
er
1000 P
ers
on
Years
(%
)
Stratton IM et al. BMJ 2000;321:405-412.
Updated Mean Hemoglobin A1c Concentration (%)
Adjusted for age, sex, and ethnic group
Myocardial Infarction
Microvascular Endpoints
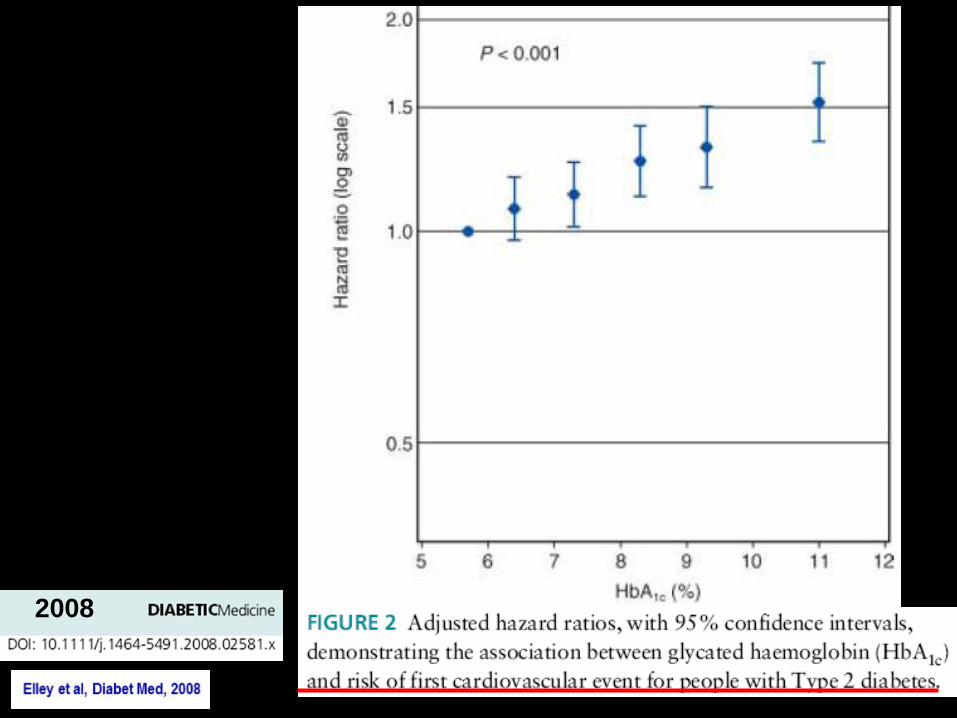
2008
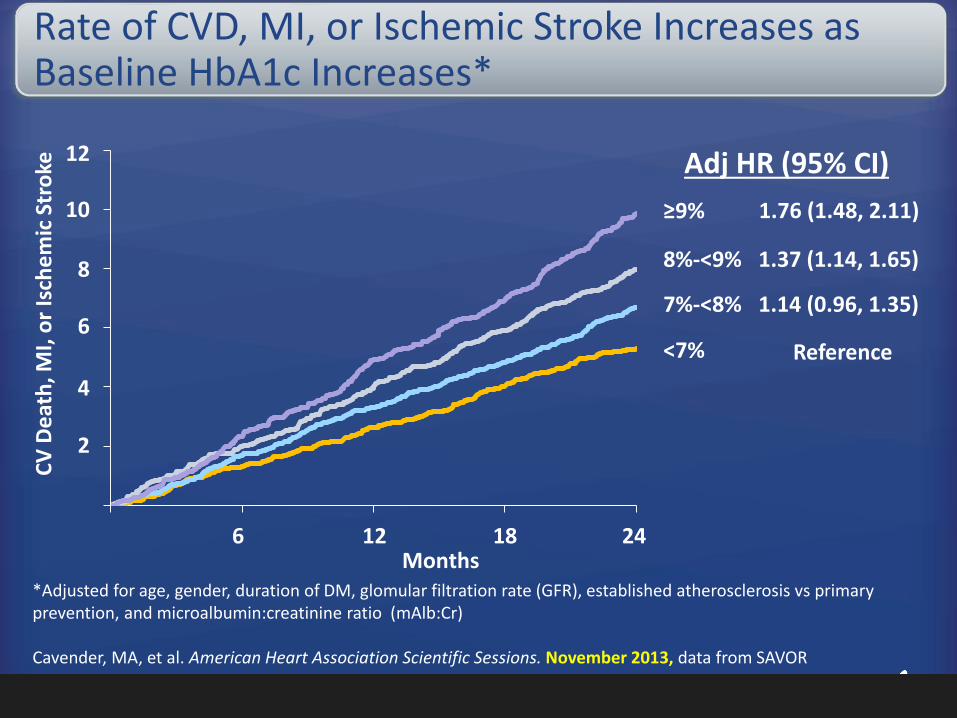
Rate of CVD, MI, or Ischemic Stroke Increases as Baseline HbA1c Increases*
*Adjusted for age, gender, duration of DM, glomular filtration rate (GFR), established atherosclerosis vs primary prevention, and microalbumin:creatinine ratio (mAlb:Cr)
Cavender, MA, et al. American Heart Association Scientific Sessions. November 2013, data from SAVOR
6 12 18 24
<7%
7%-<8%
8%-<9%
≥9%
Months
Adj HR (95% CI)
1.76 (1.48, 2.11)
1.37 (1.14, 1.65)
1.14 (0.96, 1.35)
Reference
2
4
6
8
10
12
CV
De
ath
, MI,
or
Isch
em
ic S
tro
ke
21
Diabetes and glucose
• How common is diabetes?
• Diabetes as a risk for CVD. Does A1c make a difference?
• Does improving glucose control prevent complications?
• Does too tight glucose control cause death?
• Glucose vs glycation
• Hemoglobin Glycation Index
• What should our A1c target be?
Diabetes and glucose
• How common is diabetes?
• Diabetes as a risk for CVD. Does A1c make a difference?
• Does improving glucose control prevent complications?
• Does too tight glucose control cause death?
• Glucose vs glycation
• Hemoglobin Glycation Index
• What should our A1c target be?
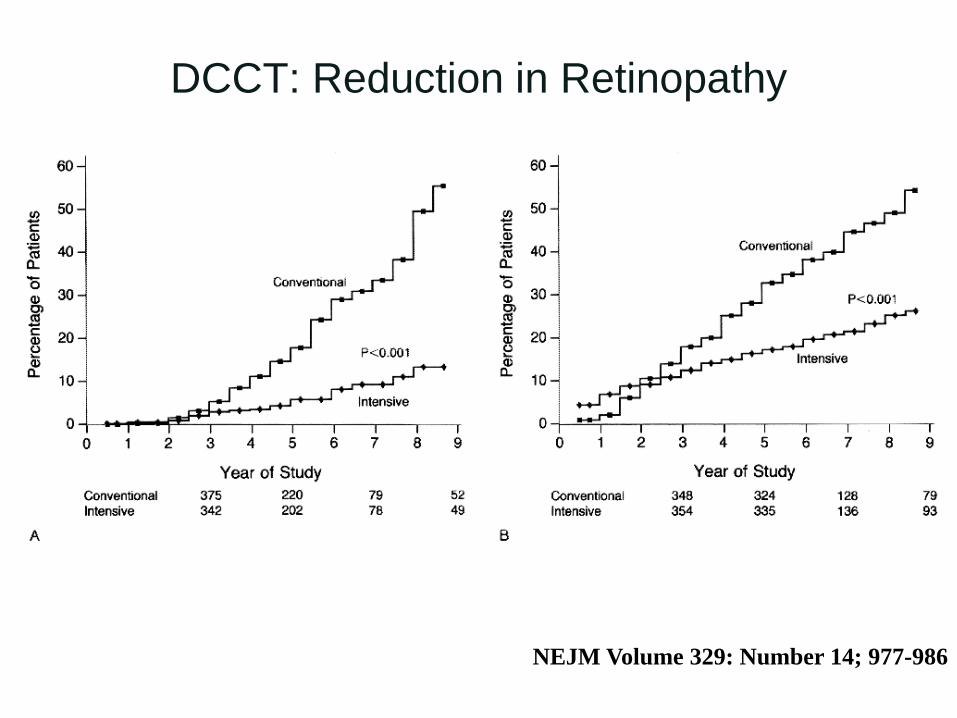
NEJM Volume 329: Number 14; 977-986
DCCT: Reduction in Retinopathy
ukpds
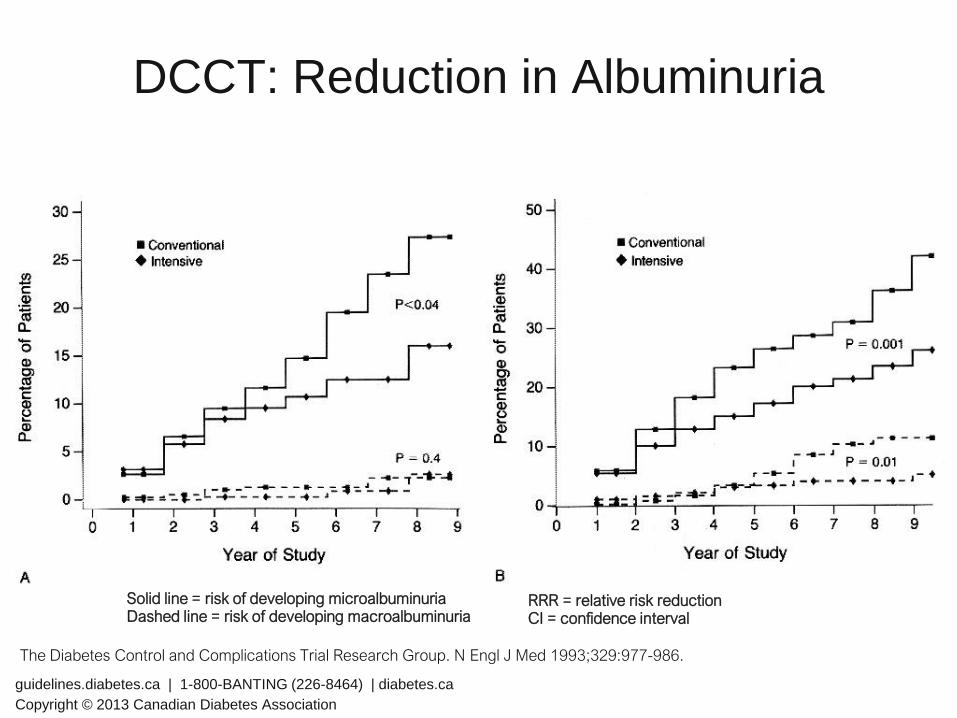
Solid line = risk of developing microalbuminuriaDashed line = risk of developing macroalbuminuria
DCCT: Reduction in Albuminuria
The Diabetes Control and Complications Trial Research Group. N Engl J Med 1993;329:977-986.
34% RRR (p<0.04)
43% RRR(p=0.001)
56% RRR(p=0.01)
Primary Prevention Secondary Intervention
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.ca
Copyright © 2013 Canadian Diabetes Association
RRR = relative risk reductionCI = confidence interval
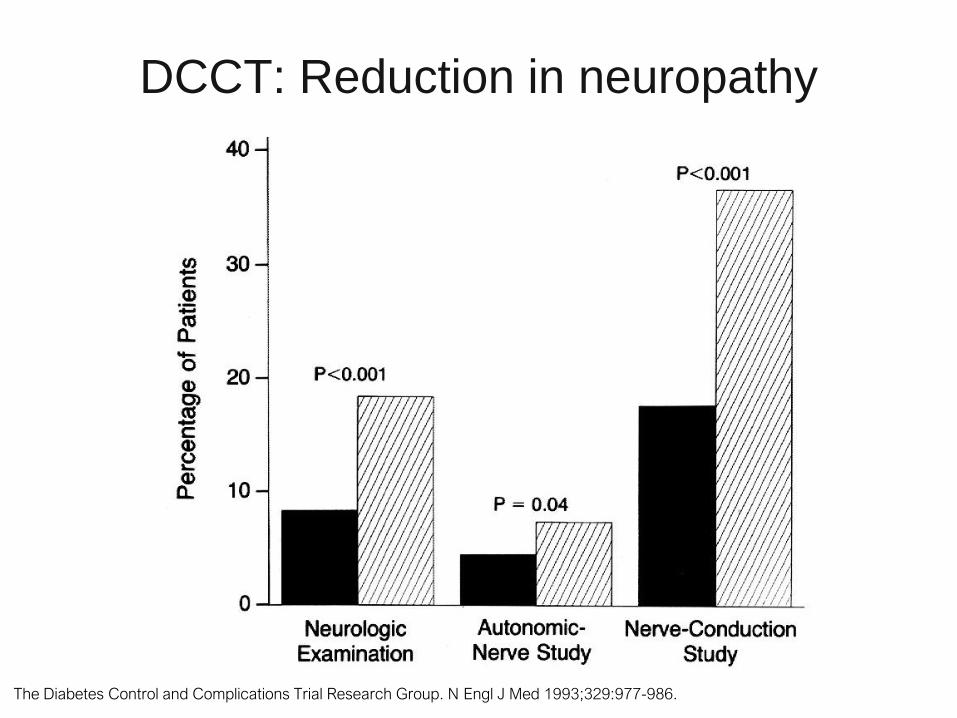
ukpdsThe Diabetes Control and Complications Trial Research Group. N Engl J Med 1993;329:977-986.
DCCT: Reduction in neuropathy
ukpds
Does tighter glycemic
control offer CV benefits?
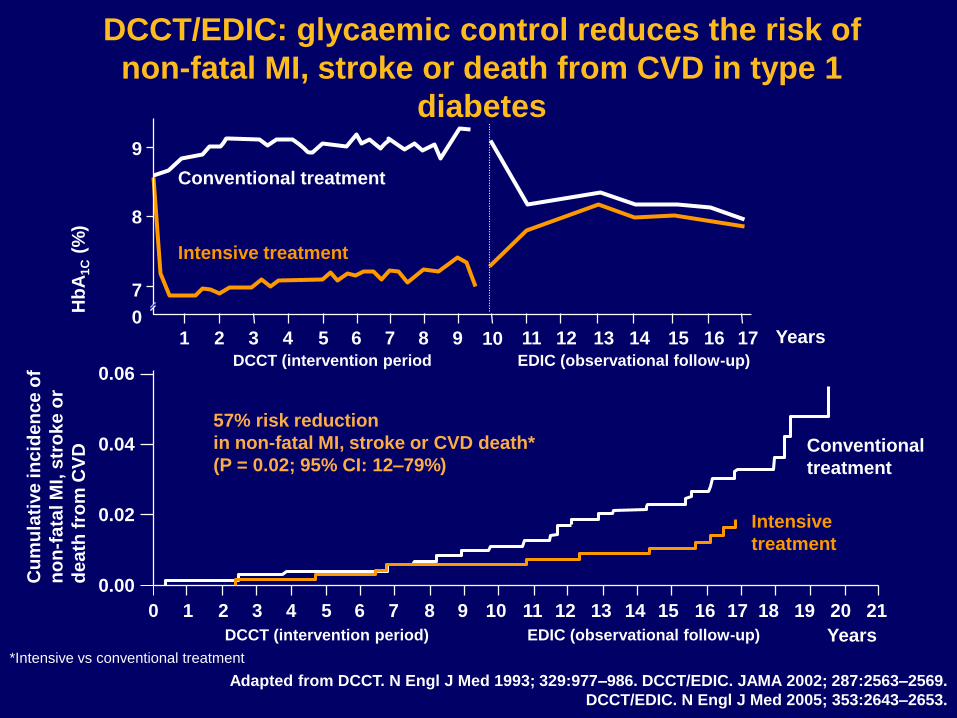
57% risk reduction
in non-fatal MI, stroke or CVD death*
(P = 0.02; 95% CI: 12–79%)
Cu
mu
lati
ve
in
cid
en
ce
of
no
n-f
ata
l M
I, s
tro
ke
or
de
ath
fro
m C
VD Conventional
treatment
Intensive
treatment
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
Years
0.06
0.04
0.02
0.00
Adapted from DCCT. N Engl J Med 1993; 329:977–986. DCCT/EDIC. JAMA 2002; 287:2563–2569.
DCCT/EDIC. N Engl J Med 2005; 353:2643–2653.
DCCT/EDIC: glycaemic control reduces the risk of
non-fatal MI, stroke or death from CVD in type 1
diabetes
0
7
1 6
Hb
A1C
(%)
9
8
2 3 4 5 7 8 9
Conventional treatment
Intensive treatment
11 12 13 14 15 16 1710
*Intensive vs conventional treatment
DCCT (intervention period EDIC (observational follow-up)
DCCT (intervention period) EDIC (observational follow-up)
Years
3 major studies that are referred to,
ADVANCE, ACCORD, VADT to provide
answers• All studies of “Intensive glucose control” vs “looser
glucose control”
• All were in very high risk patients who had their diabetes
for 8-11 years
– Either had documented vascular disease or
– Very high risk based on risk factors
3 major studies that are referred to,
ADVANCE, ACCORD, VADT to provide
answers• All studies of “Intensive glucose control” vs “looser
glucose control”
• All were in very high risk patients who had their diabetes
for 8-11 years
– Either had documented vascular disease or
– Very high risk based on risk factors
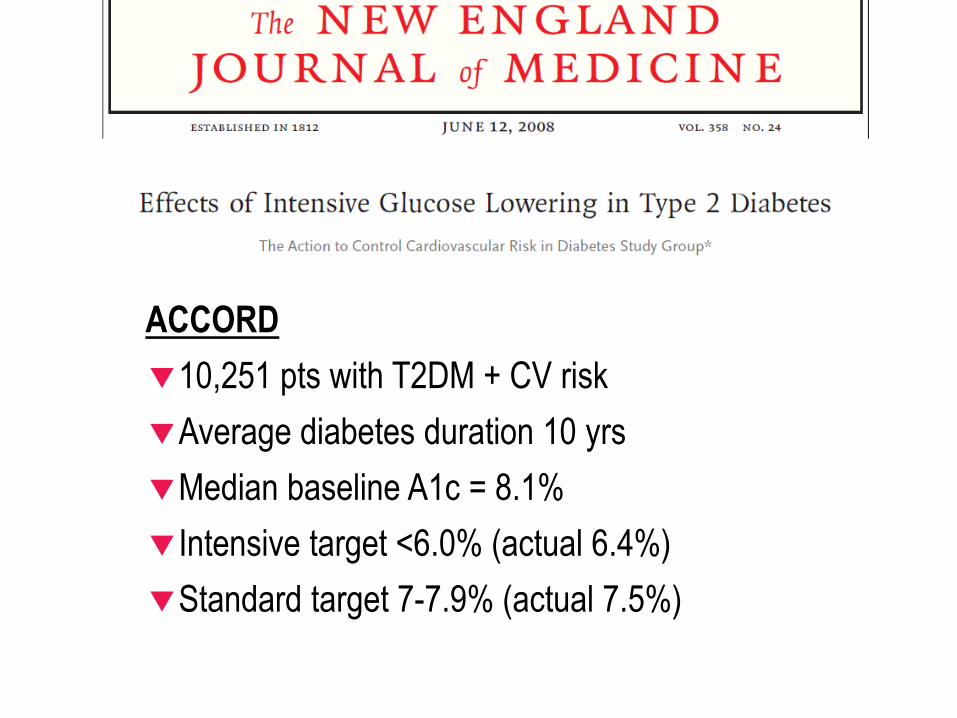
ACCORD
10,251 pts with T2DM + CV risk
Average diabetes duration 10 yrs
Median baseline A1c = 8.1%
Intensive target <6.0% (actual 6.4%)
Standard target 7-7.9% (actual 7.5%)
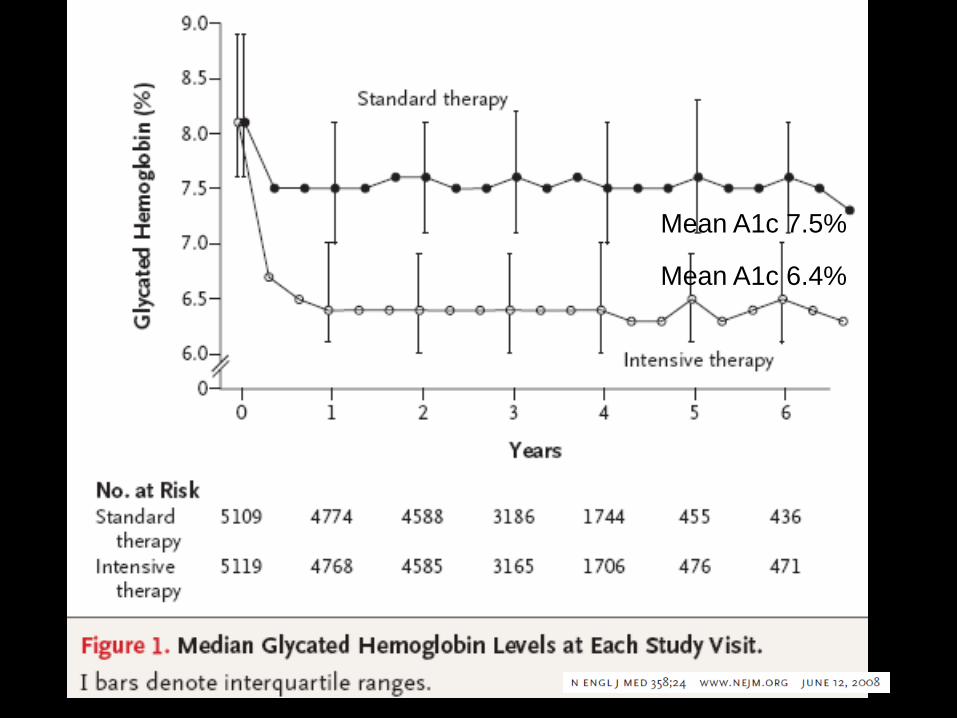
Mean A1c 7.5%
Mean A1c 6.4%
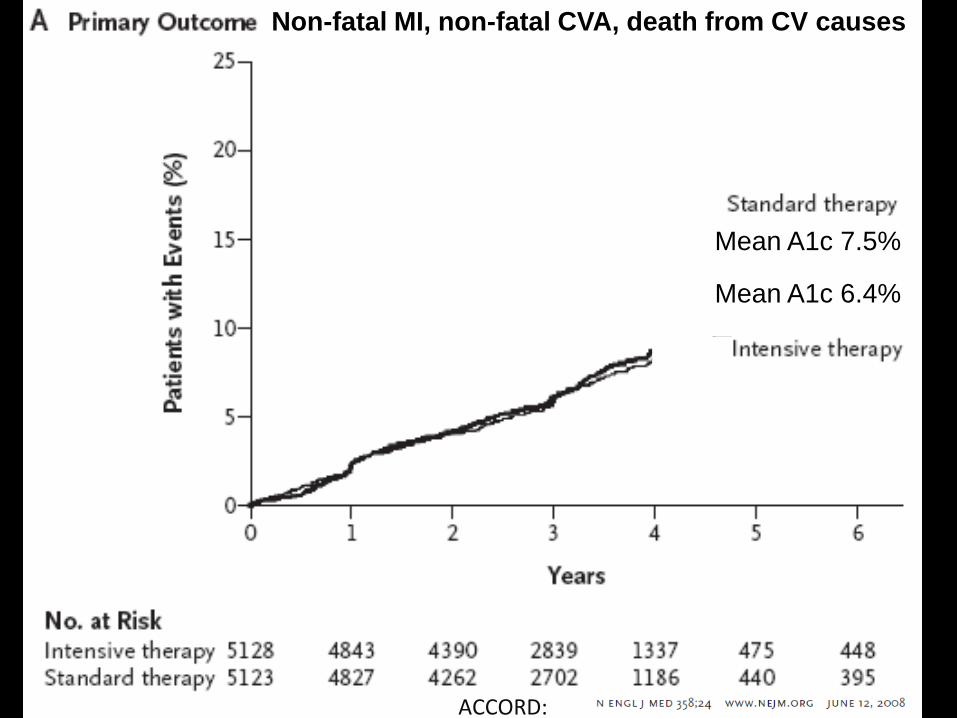
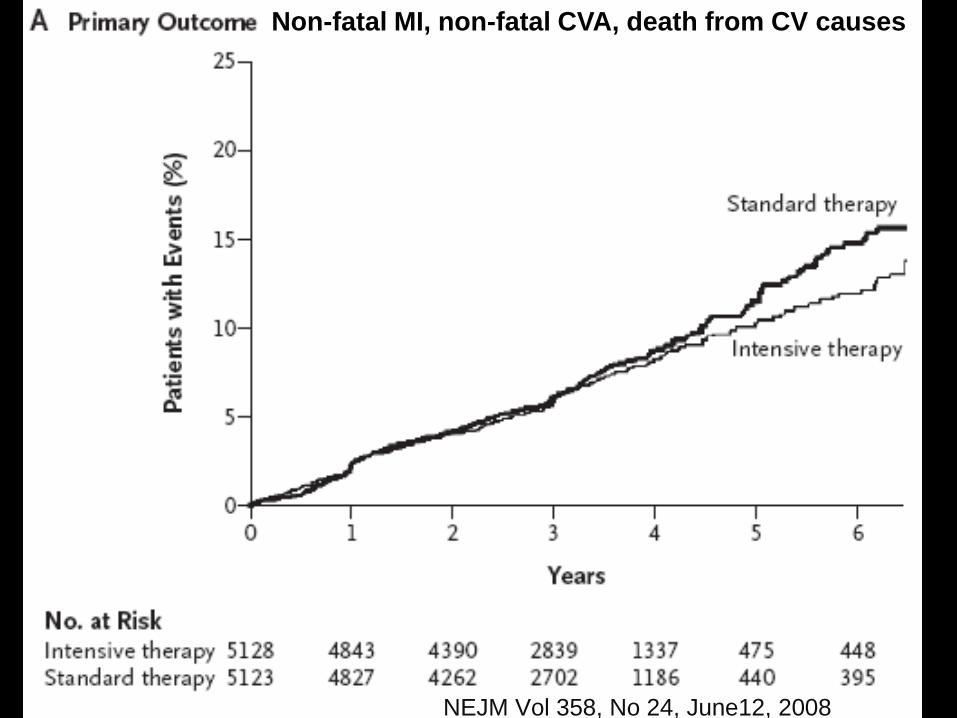
Non-fatal MI, non-fatal CVA, death from CV causes
ACCORD:
Mean A1c 7.5%
Mean A1c 6.4%
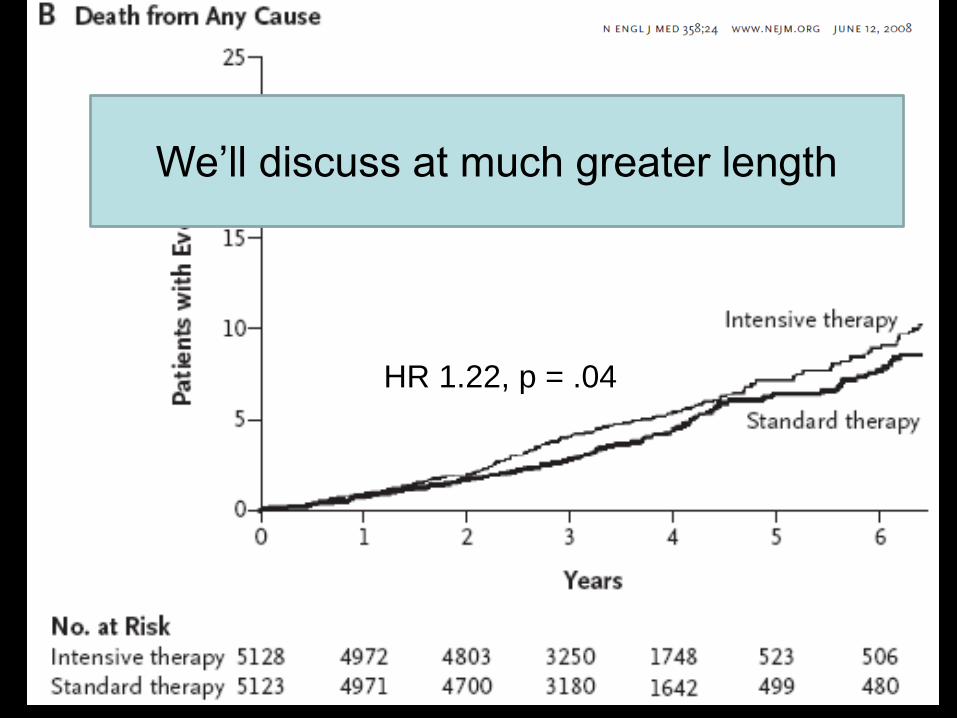
HR 1.22, p = .04
We’ll discuss at much greater length
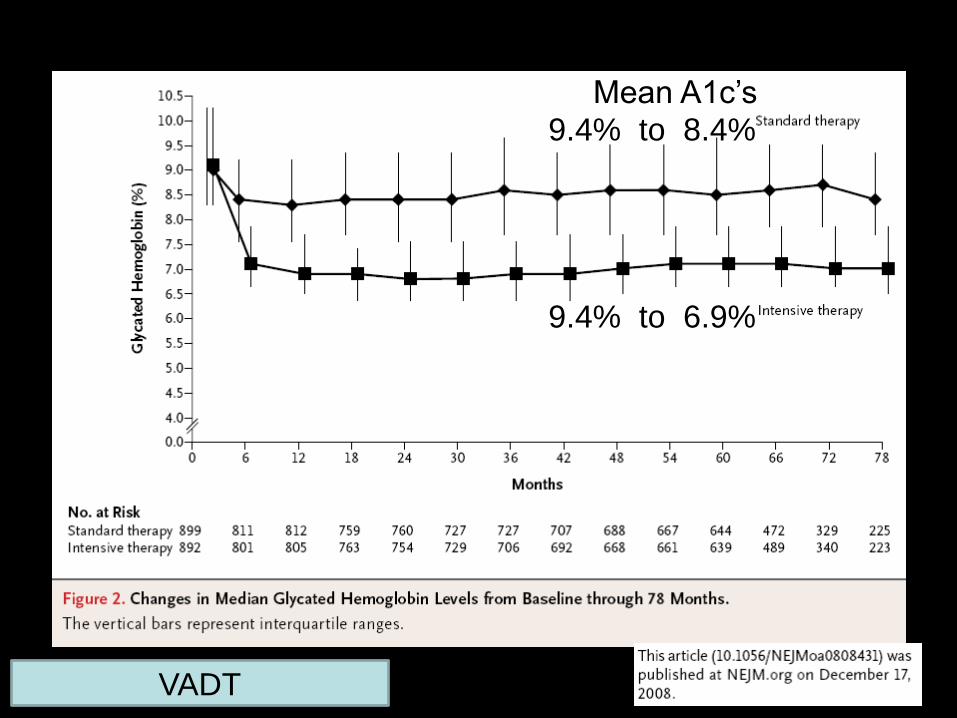
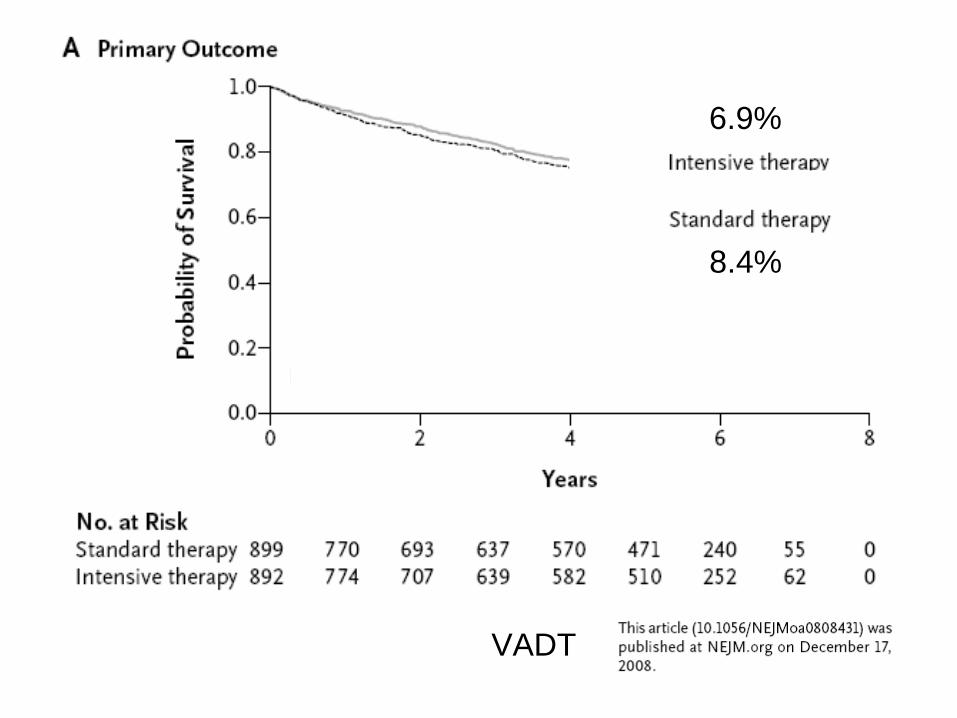
9.4% to 8.4%
9.4% to 6.9%
Mean A1c’s
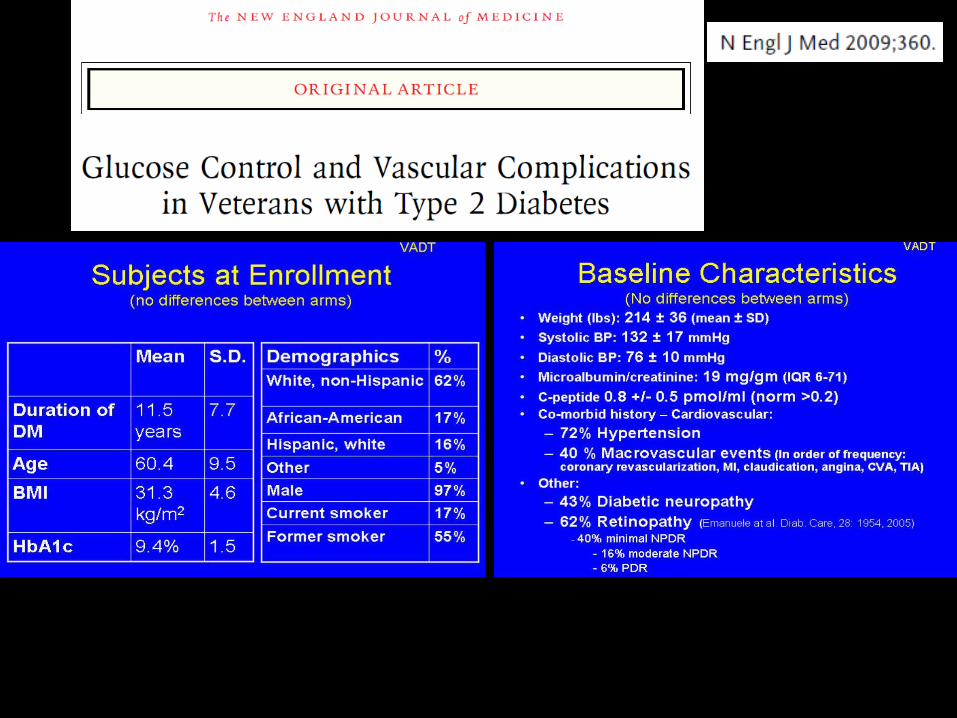
VADT
And
VADT
hazard ratio in the intensive-therapy group of 0.88
(95% confidence interval [CI], 0.74 to 1.05).
8.4%
6.9%
Does VADT tell us anything?
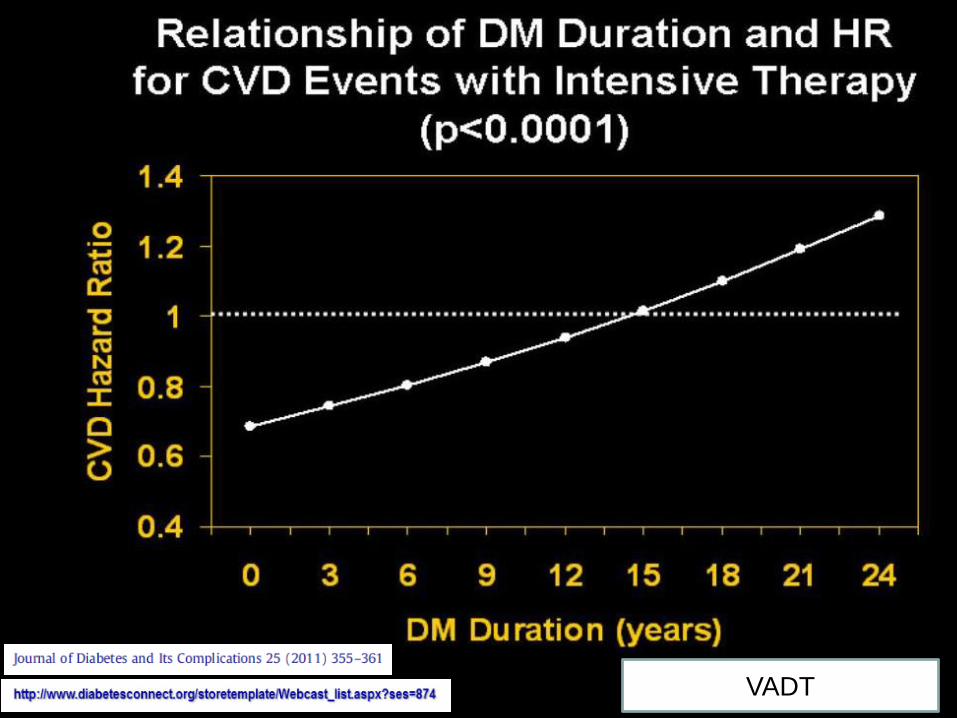
VADT
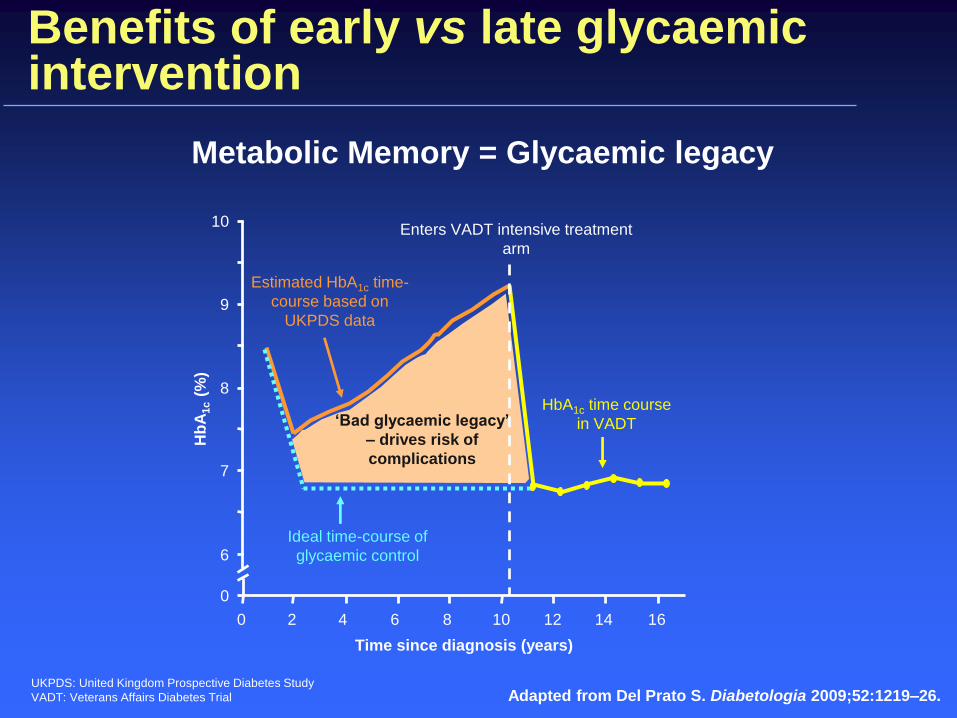
Benefits of early vs late glycaemic intervention
Adapted from Del Prato S. Diabetologia 2009;52:1219–26.
Metabolic Memory = Glycaemic legacy
UKPDS: United Kingdom Prospective Diabetes Study
VADT: Veterans Affairs Diabetes Trial
Enters VADT intensive treatment
arm
1614121086420
0
6
7
9
8
10
Time since diagnosis (years)
Hb
A1c
(%)
‘Bad glycaemic legacy’
– drives risk of
complications
Estimated HbA1c time-
course based on
UKPDS data
Ideal time-course of
glycaemic control
HbA1c time course
in VADT

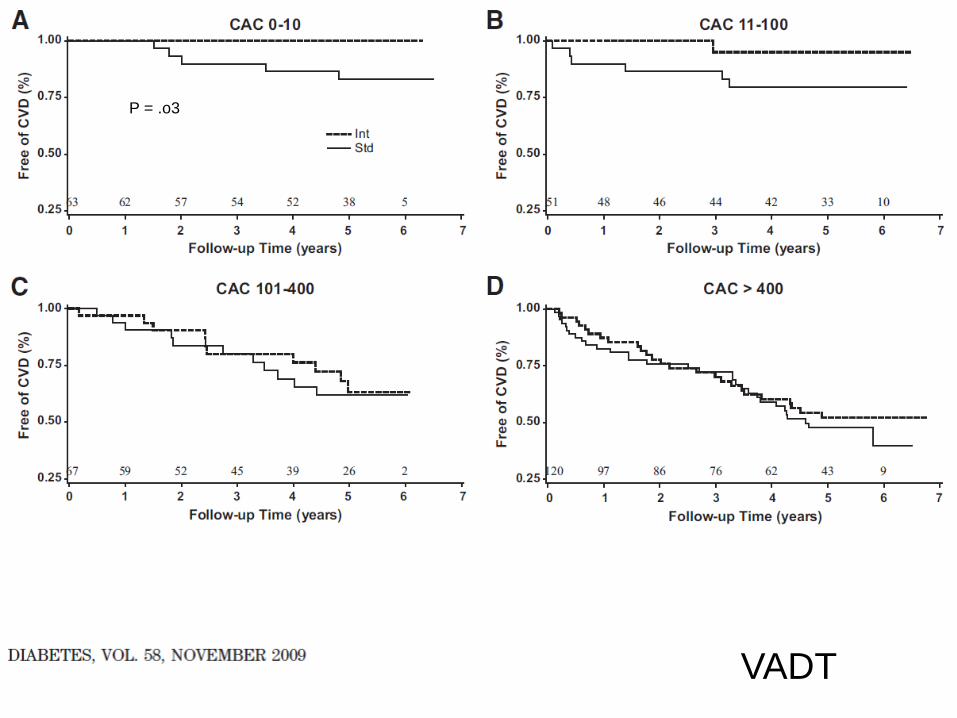
P = .o3
VADT
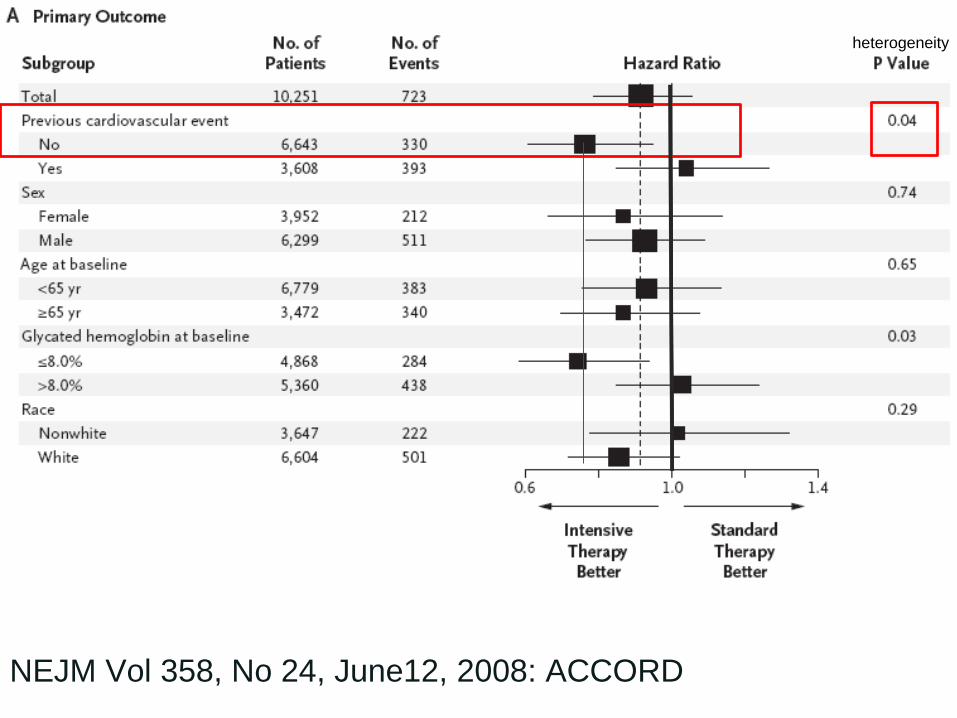
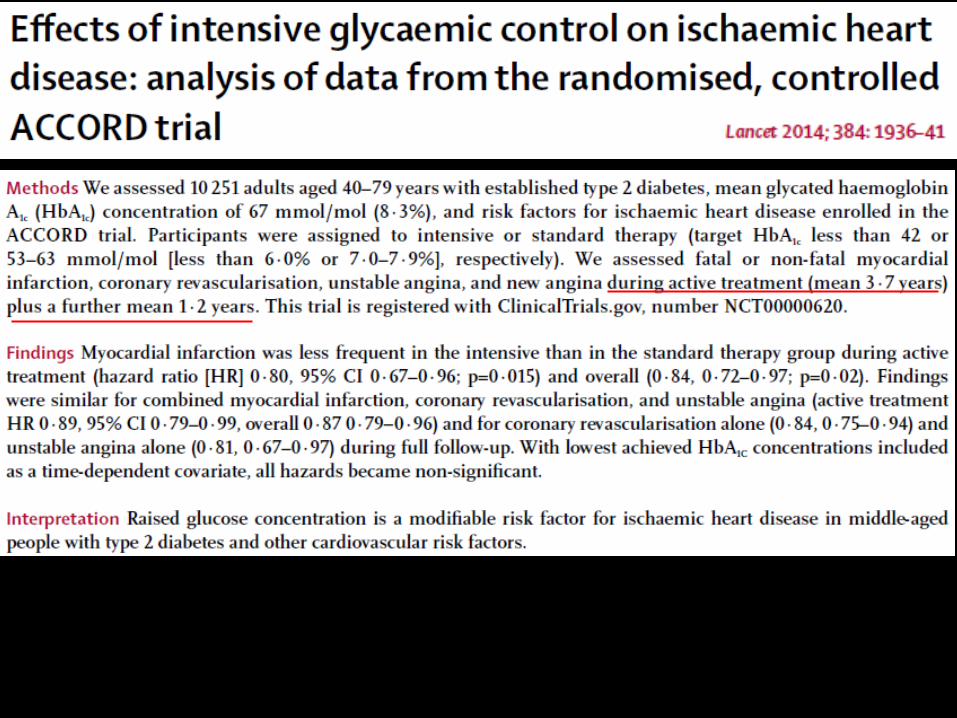
NEJM Vol 358, No 24, June12, 2008: ACCORD
heterogeneity
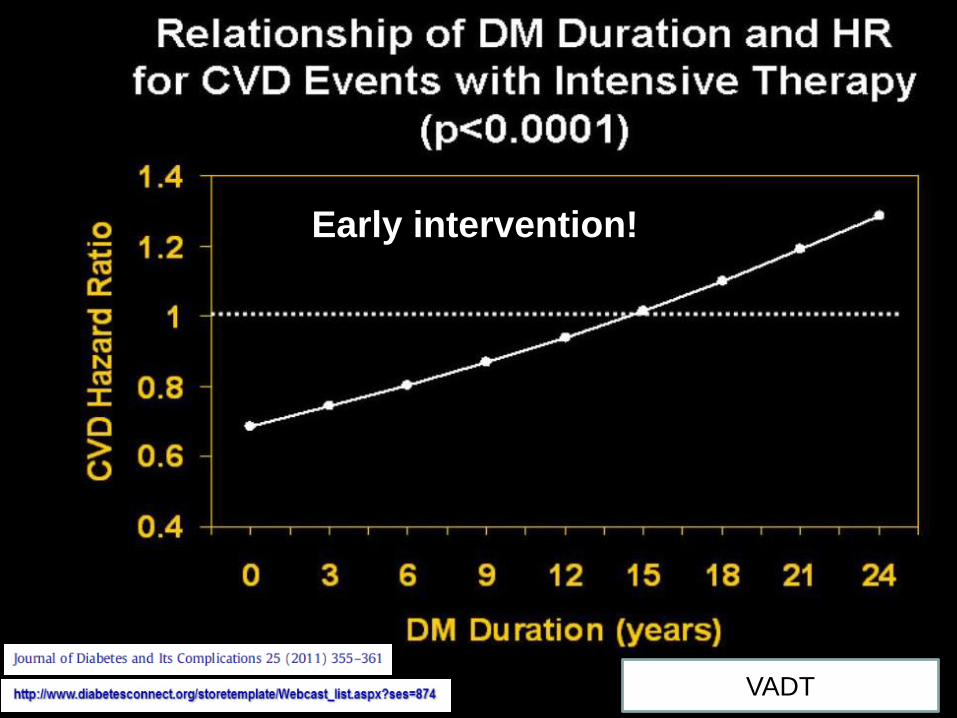
VADT
Early intervention!
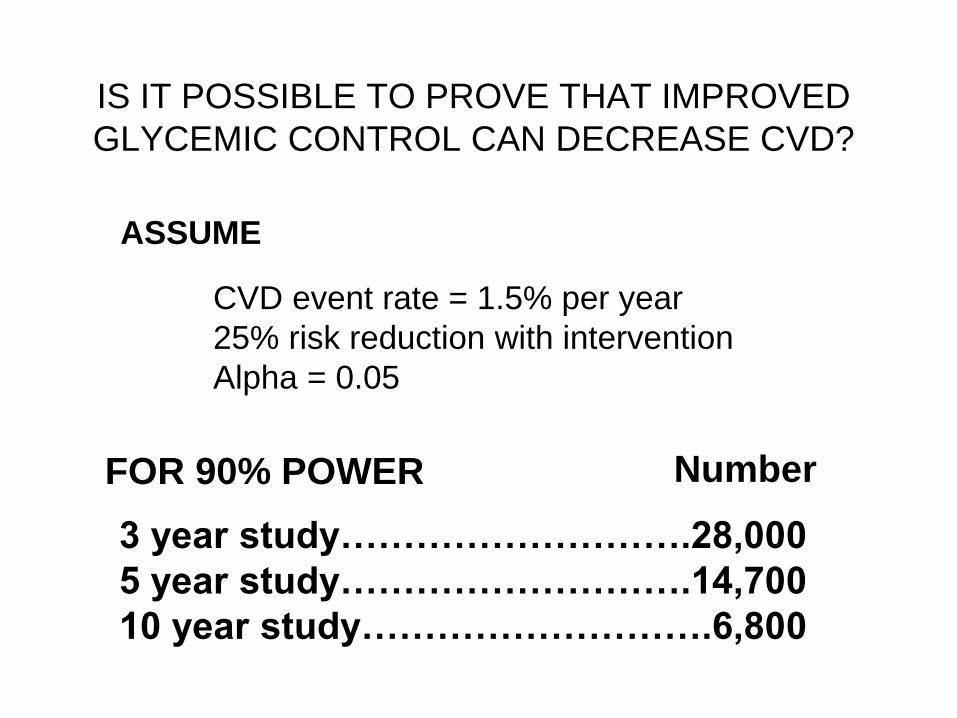
IS IT POSSIBLE TO PROVE THAT IMPROVED
GLYCEMIC CONTROL CAN DECREASE CVD?
• CVD event rate = 1.5% per year
• 25% risk reduction with intervention
• Alpha = 0.05
3 year study……………………….28,000
5 year study……………………….14,700
10 year study……………………….6,800
FOR 90% POWER Number
ASSUME
Are there any studies looking at
glucose control early in the course of
the diabetes?
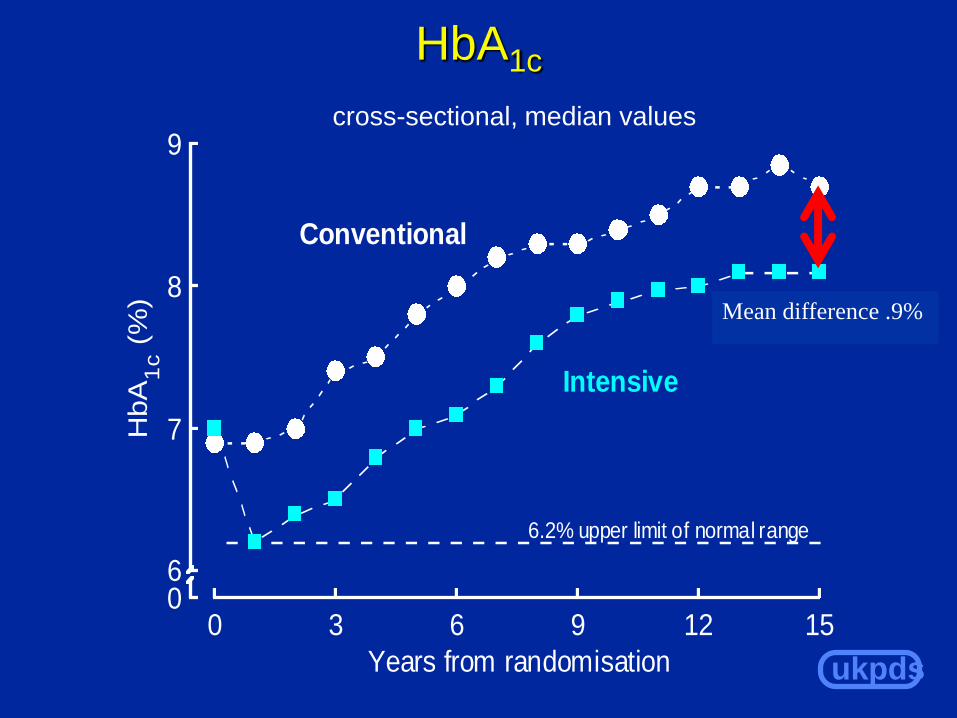
ukpds
HbA1c
cross-sectional, median values
06
7
8
9
0 3 6 9 12 15
HbA
1c (
%)
Years from randomisation
Conventional
Intensive
6.2% upper limit of normal range
Mean difference .9%
ukpds
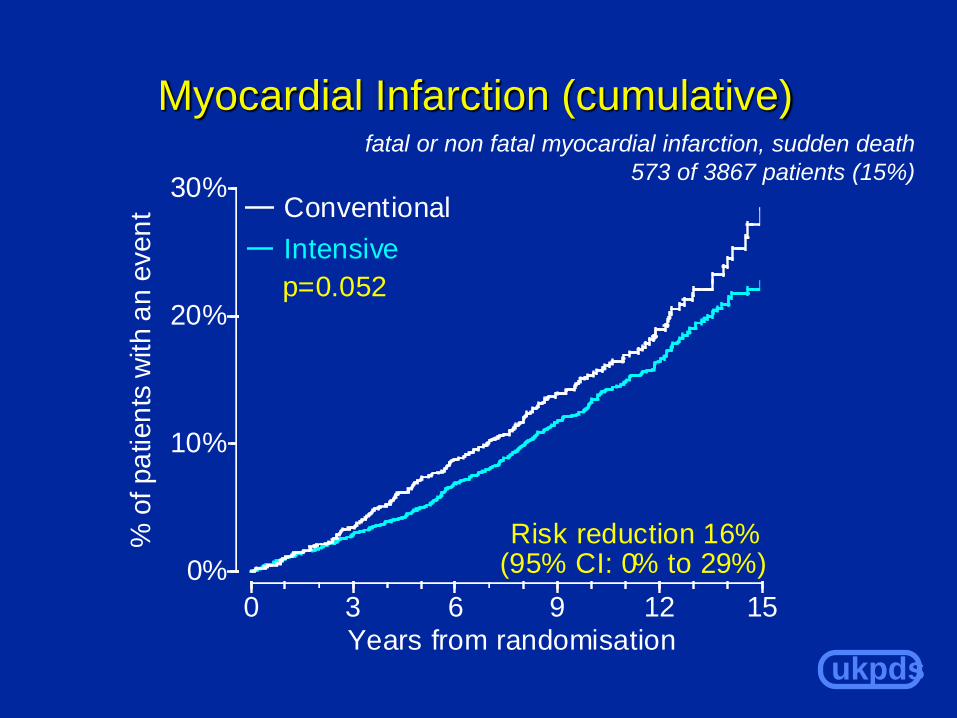
Myocardial Infarction (cumulative)
0%
10%
20%
30%
0 3 6 9 12 15
% o
f pa
tien
ts w
ith a
n e
ven
t
Years from randomisation
Intensive
Conventional
p=0.052
Risk reduction 16%(95% CI: 0% to 29%)
fatal or non fatal myocardial infarction, sudden death
573 of 3867 patients (15%)
ukpds
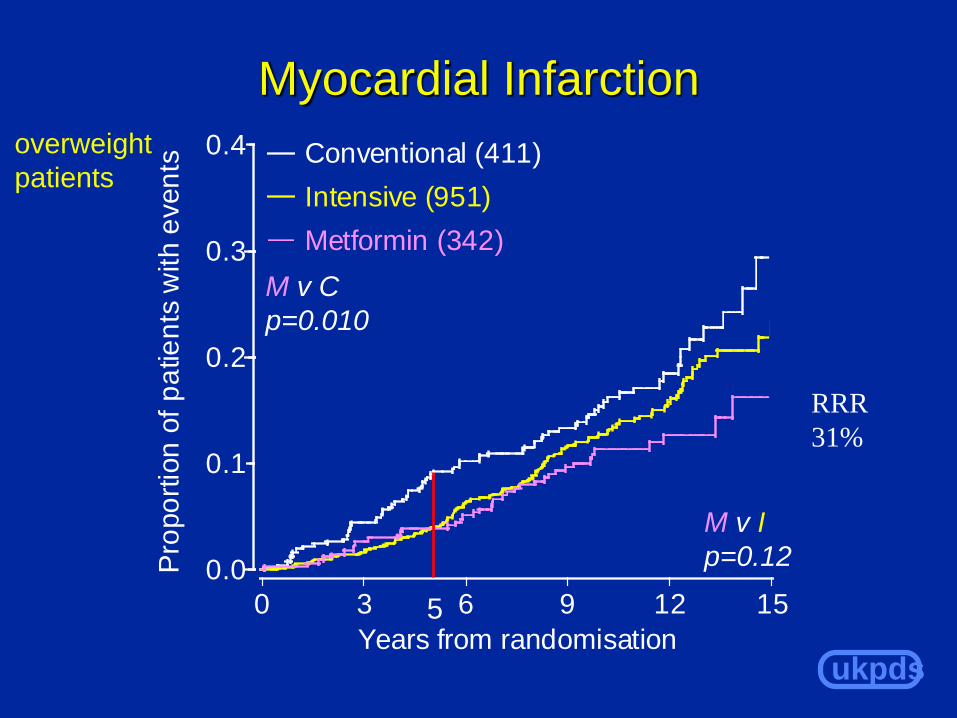
Myocardial Infarction
M v I
p=0.12
overweight
patients
0.0
0.1
0.2
0.3
0.4
0 3 6 9 12 15
Pro
po
rtio
n o
f p
atie
nts
with e
ven
ts
Years from randomisation
Conventional (411)
Intensive (951)
Metformin (342)
M v C
p=0.010
RRR
31%
5

Abstract 1338
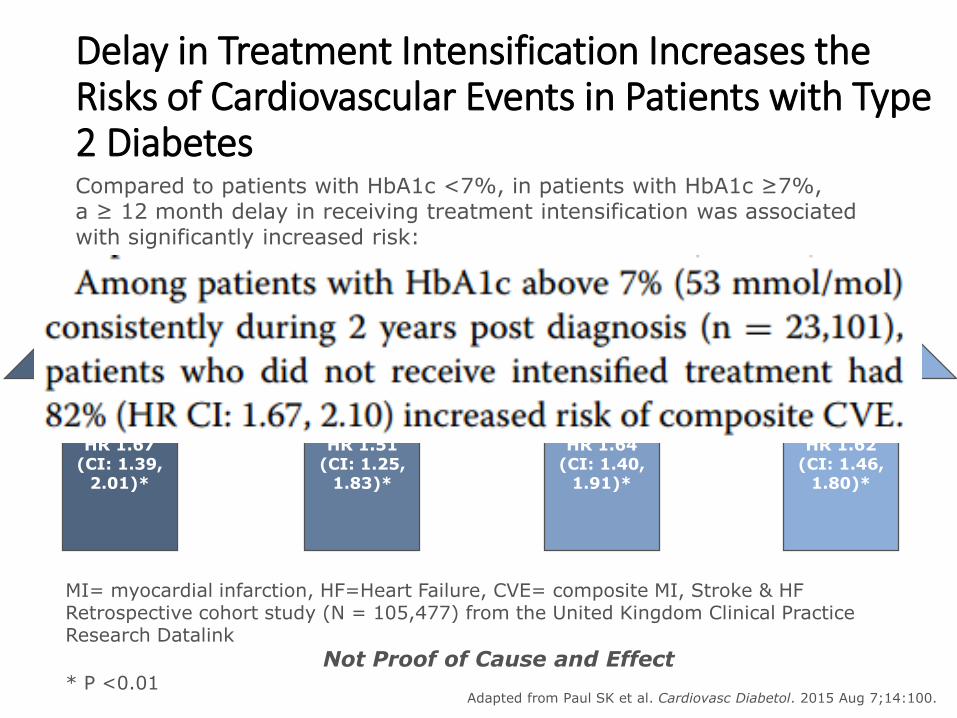
Delay in Treatment Intensification Increases the Risks of Cardiovascular Events in Patients with Type 2 Diabetes
Adapted from Paul SK et al. Cardiovasc Diabetol. 2015 Aug 7;14:100.
Compared to patients with HbA1c <7%, in patients with HbA1c ≥7%, a ≥ 12 month delay in receiving treatment intensification was associated with significantly increased risk:
MI 67%
HR 1.67 (CI: 1.39,
2.01)*
51%
HR 1.51 (CI: 1.25,
1.83)*
HF 64%
HR 1.64 (CI: 1.40,
1.91)*
CVE 62%
HR 1.62 (CI: 1.46,
1.80)*
MI= myocardial infarction, HF=Heart Failure, CVE= composite MI, Stroke & HFRetrospective cohort study (N = 105,477) from the United Kingdom Clinical Practice Research Datalink
Not Proof of Cause and Effect * P <0.01
STROKE
• The earlier you start while the blood vessels are clean, the more benefit you expect from tighter glucose control
Diabetes and glucose
• How common is diabetes?
• Diabetes as a risk for CVD. Does A1c make a difference?
• Does improving glucose control prevent complications?
• Does too tight glucose control cause death?
• Glucose vs glycation
• Hemoglobin Glycation Index
• What should our A1c target be?
Diabetes and glucose
• How common is diabetes?
• Diabetes as a risk for CVD. Does A1c make a difference?
• Does improving glucose control prevent complications?
• Does too tight glucose control cause death?
• Glucose vs glycation
• Hemoglobin Glycation Index
• What should our A1c target be?
Diabetes and glucose
• How common is diabetes?
• Diabetes as a risk for CVD. Does A1c make a difference?
• Does improving glucose control prevent complications?
• Does too tight glucose control cause death?
• Glucose vs glycation
• Hemoglobin Glycation Index
• What should our A1c target be?
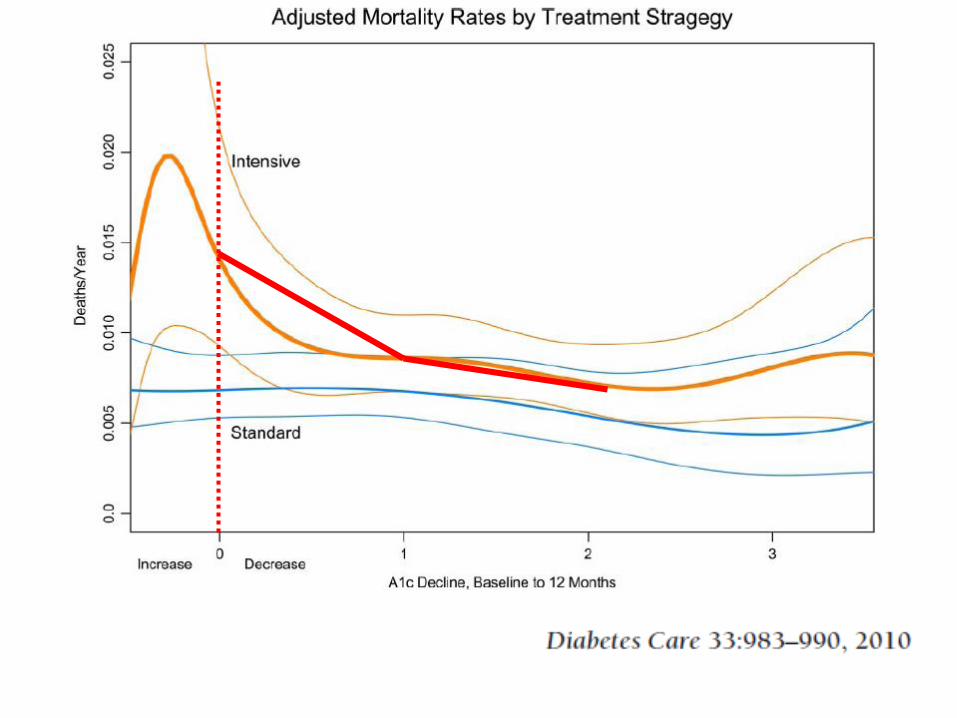
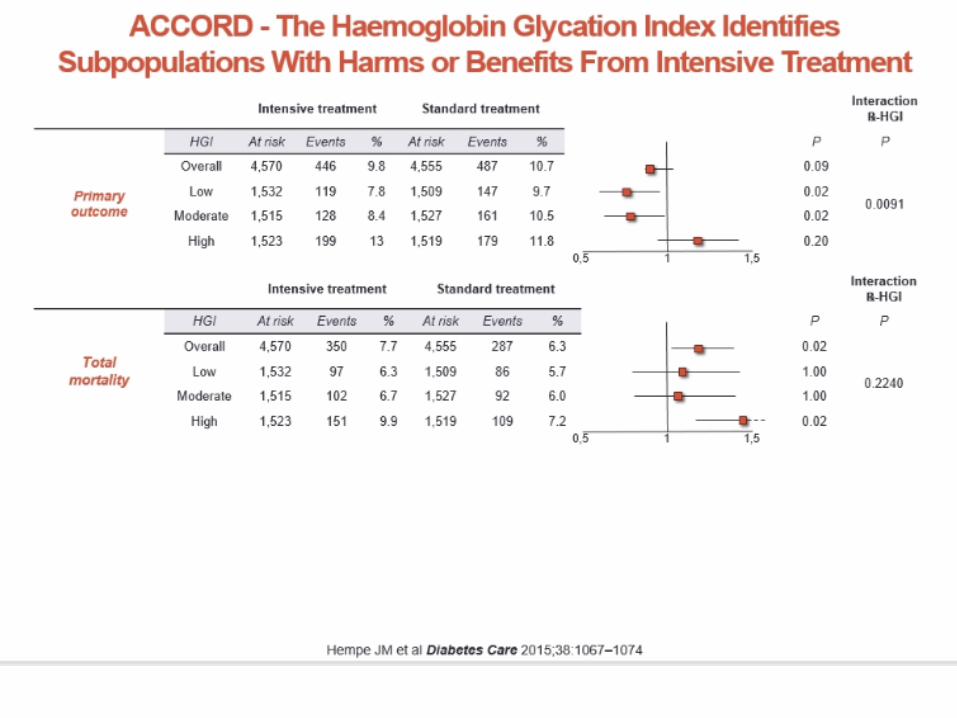
Who died in ACCORD?
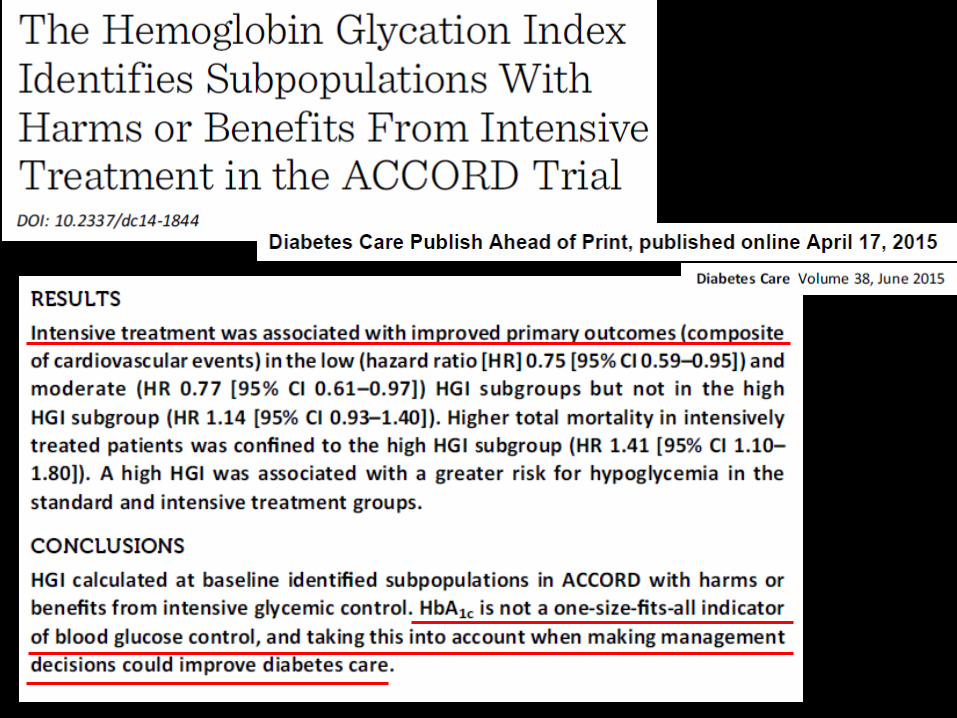
What does ACCORD really tell us?
• Tight glycemic control shows CV benefit after
5 years
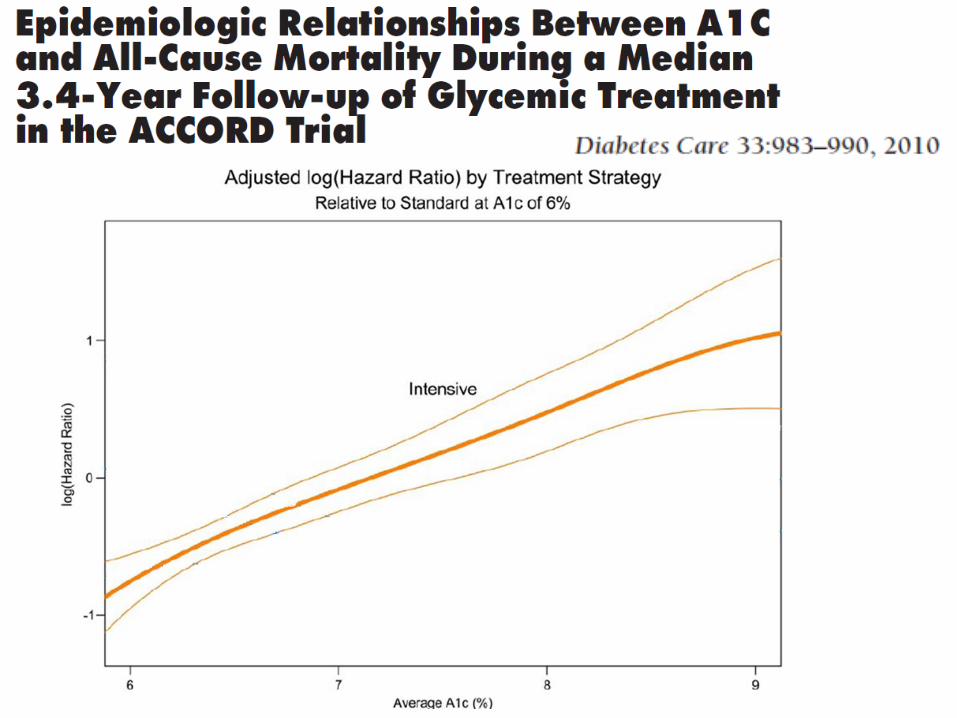
• People who died had higher A1c’s
• People who died were people in whom it was
not possible to lower their A1c’s
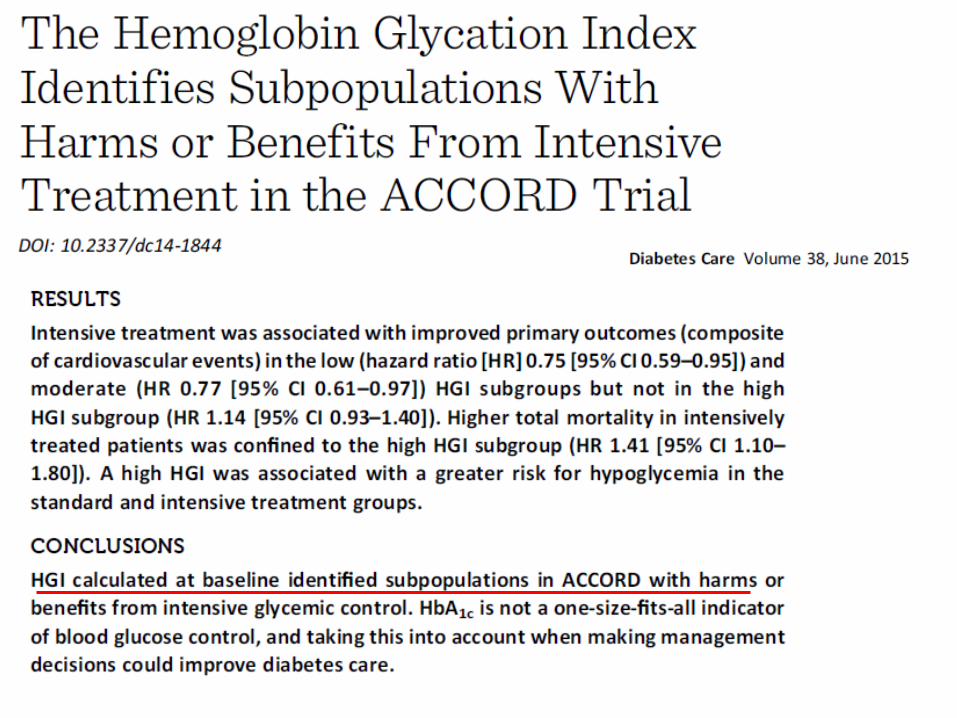
• People who died had a high “Hemoglobin
Glycation Index”
• People who died tended not to be on beta
blockers
What does ACCORD really tell us?
• Tight glycemic control shows CV benefit after
5 years
• People who died had higher A1c’s
• People who died were people in whom it was
not possible to lower their A1c’s
• People who died had a high “Hemoglobin
Glycation Index”
• People who died tended not to be on beta
blockers
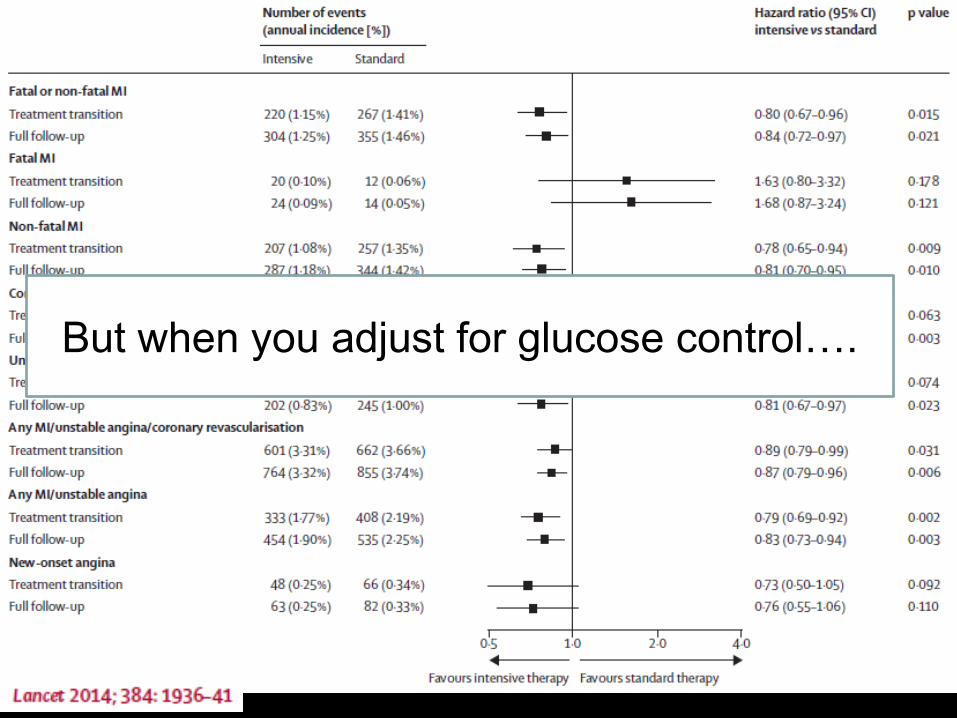
But when you adjust for glucose control….

What does ACCORD really tell us?
• Tight glycemic control shows CV benefit after
5 years
• People who died had higher A1c’s
• People who died were people in whom it was
not possible to lower their A1c’s
• People who died had a high “Hemoglobin
Glycation Index”
• People who died tended not to be on beta
blockers
What does ACCORD really tell us?
• Tight glycemic control shows CV benefit after
5 years
• People who died had higher A1c’s
• People who died were people in whom it was
not possible to lower their A1c’s
• People who died had a high “Hemoglobin
Glycation Index”
• People who died tended not to be on beta
blockers
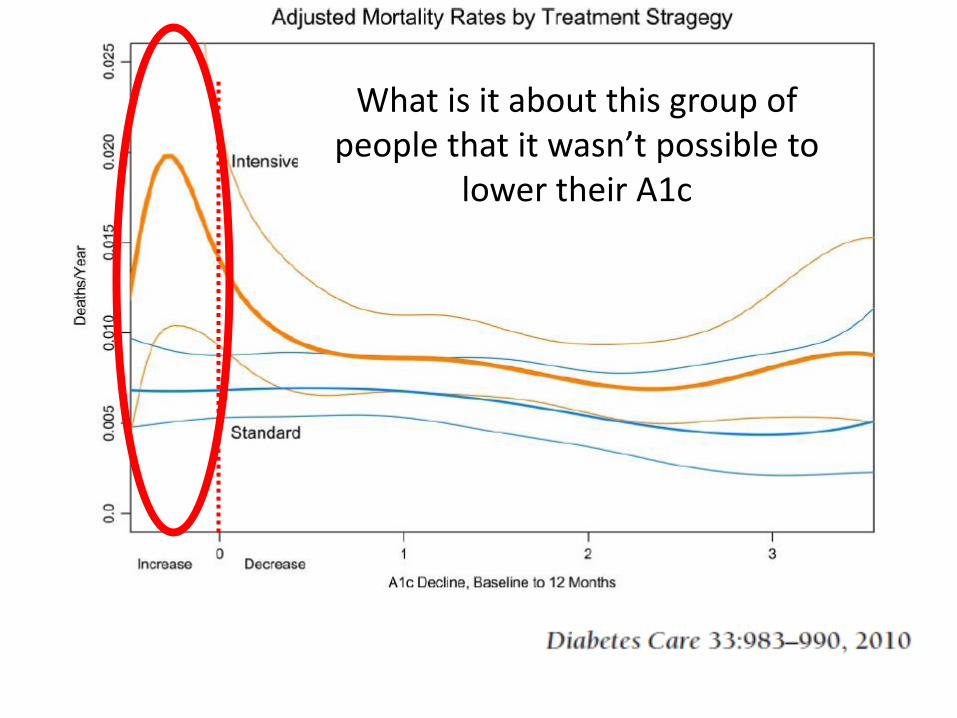
What is it about this group of people that it wasn’t possible to
lower their A1c
What does ACCORD really tell us?
• Tight glycemic control shows CV benefit after
5 years
• People who died had higher A1c’s
• People who died were people in whom it was
not possible to lower their A1c’s
• People who died had a high “Hemoglobin
Glycation Index”
• People who died tended not to be on beta
blockers
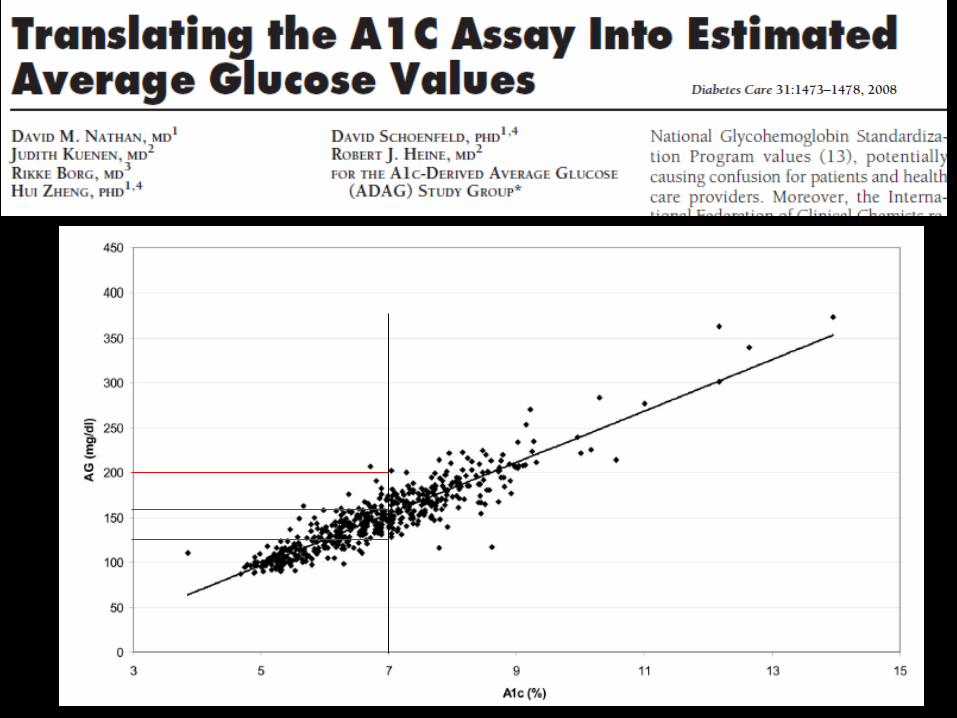
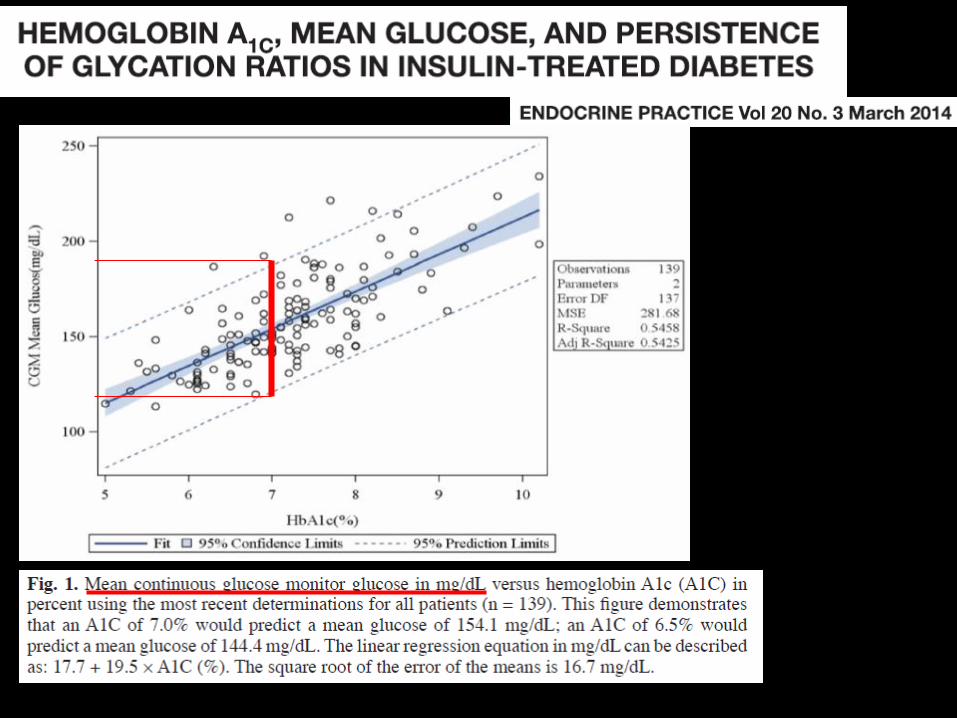
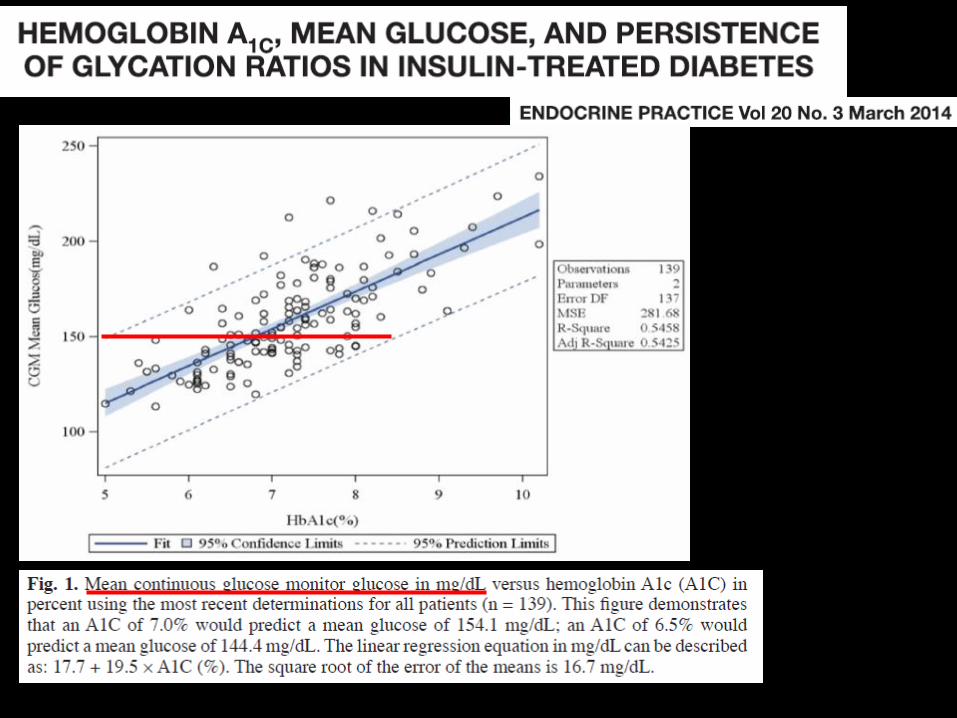
A1c’s do not accurately describe glucose
profiles in ALL people
(Even excluding people with
hemoglobinopathy, hemolysis, anemia, etc
which are known to affect A1c)
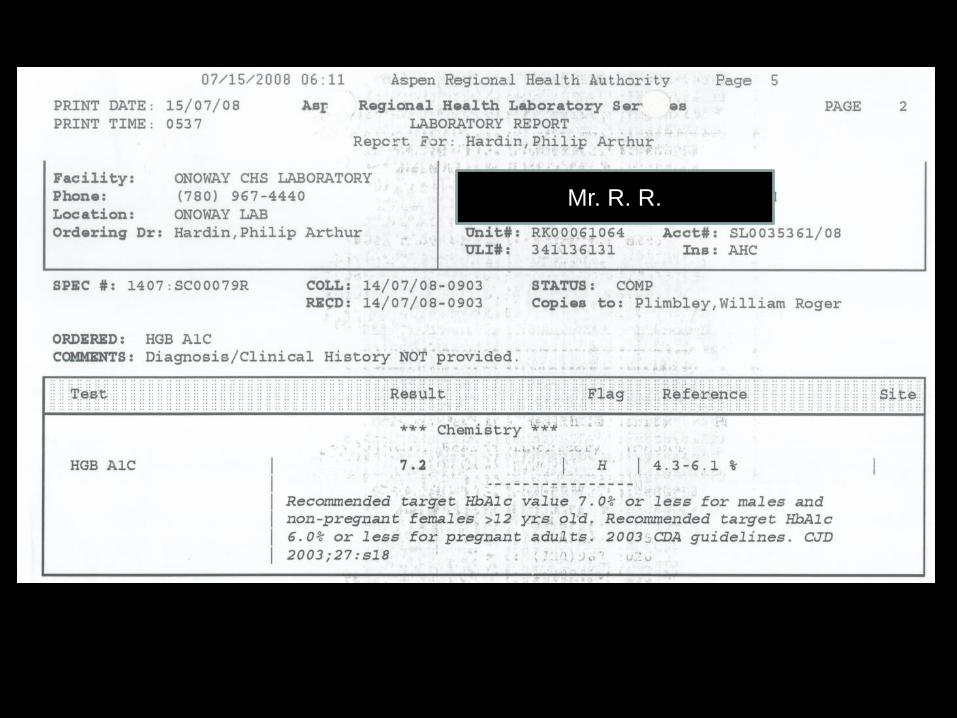
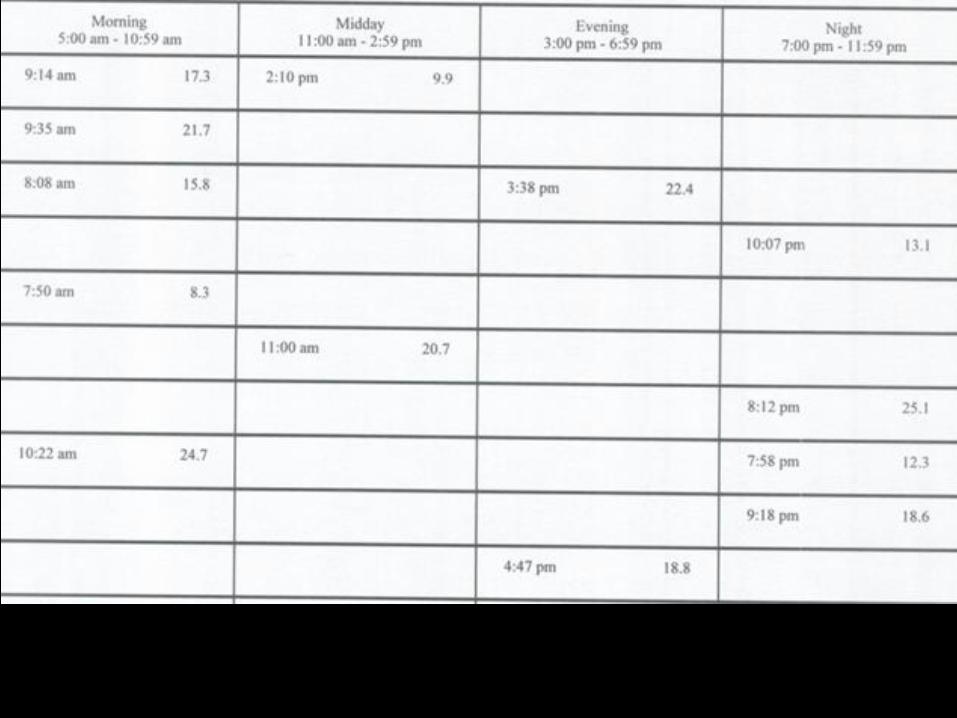
Mr. R. R.
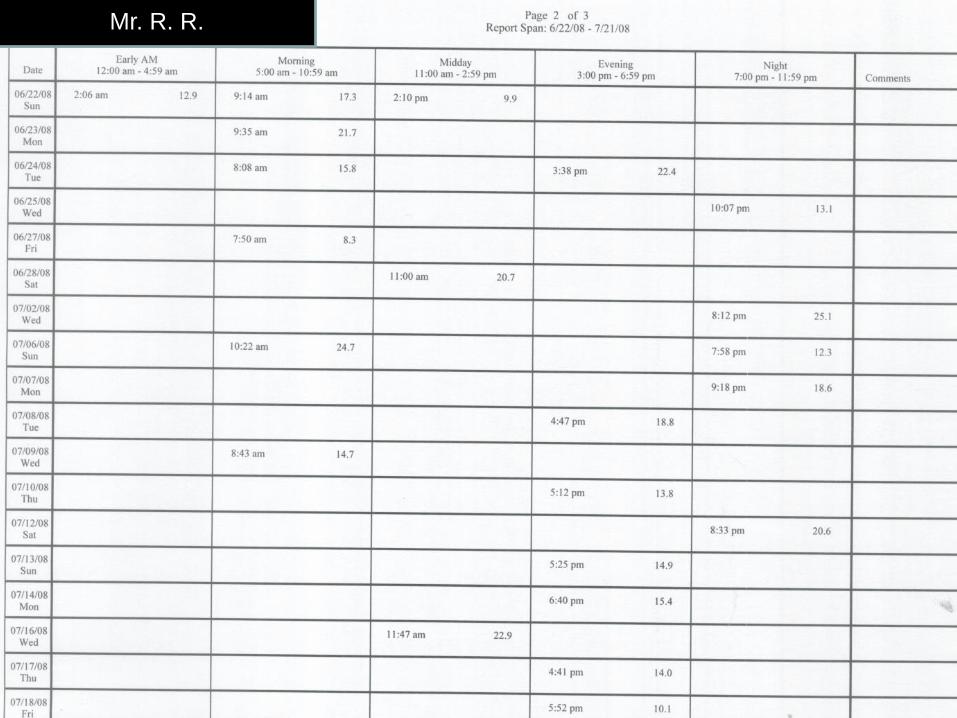
Mr. R. R.
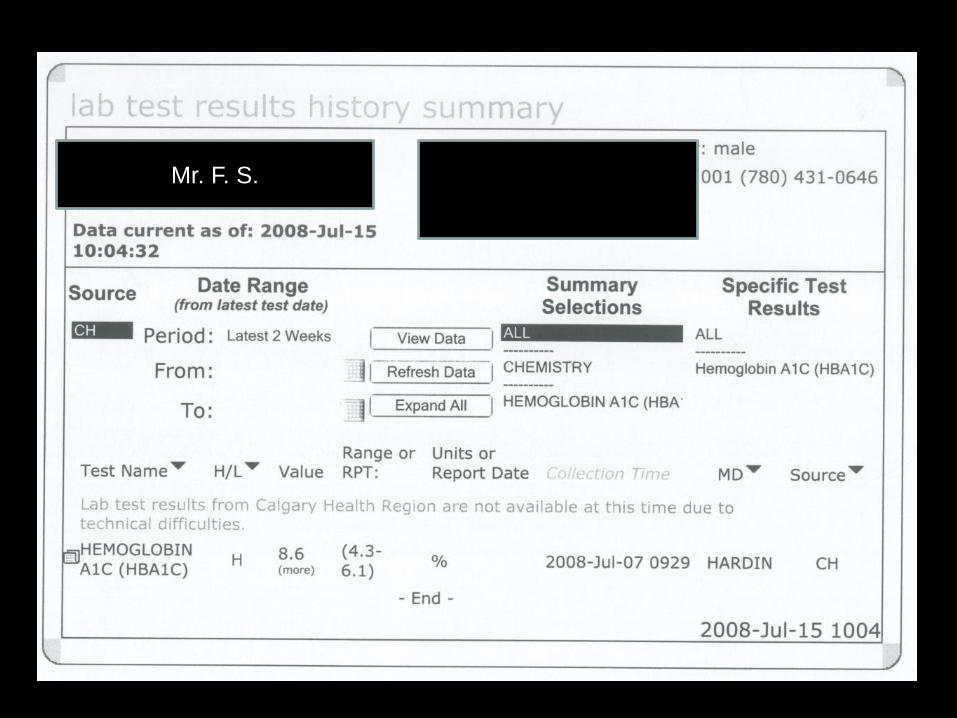
Mr. F. S.
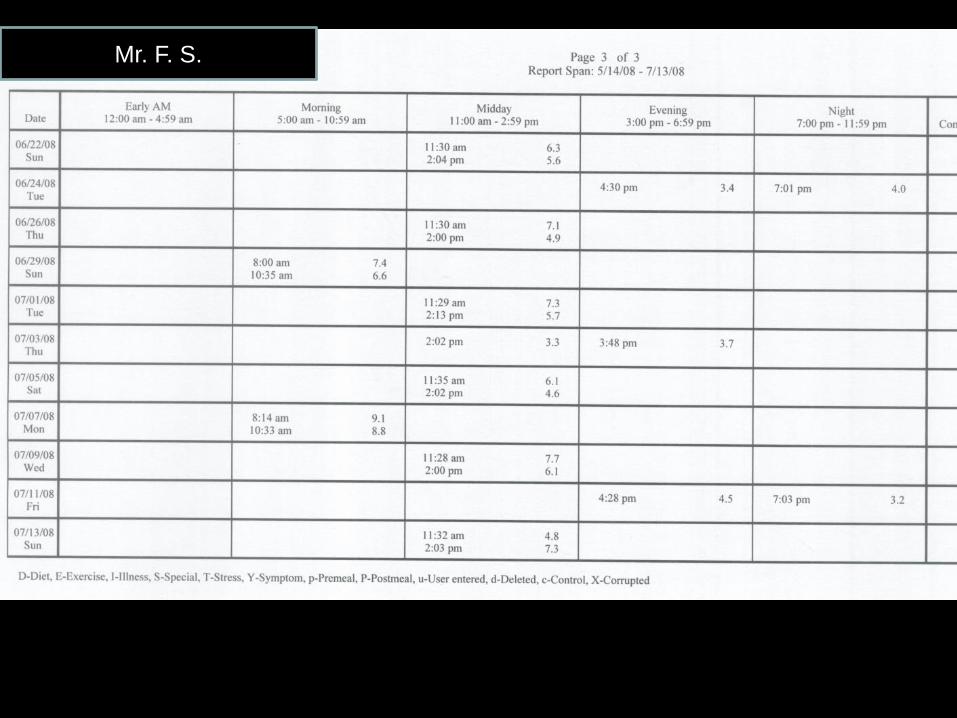
Mr. F. S.
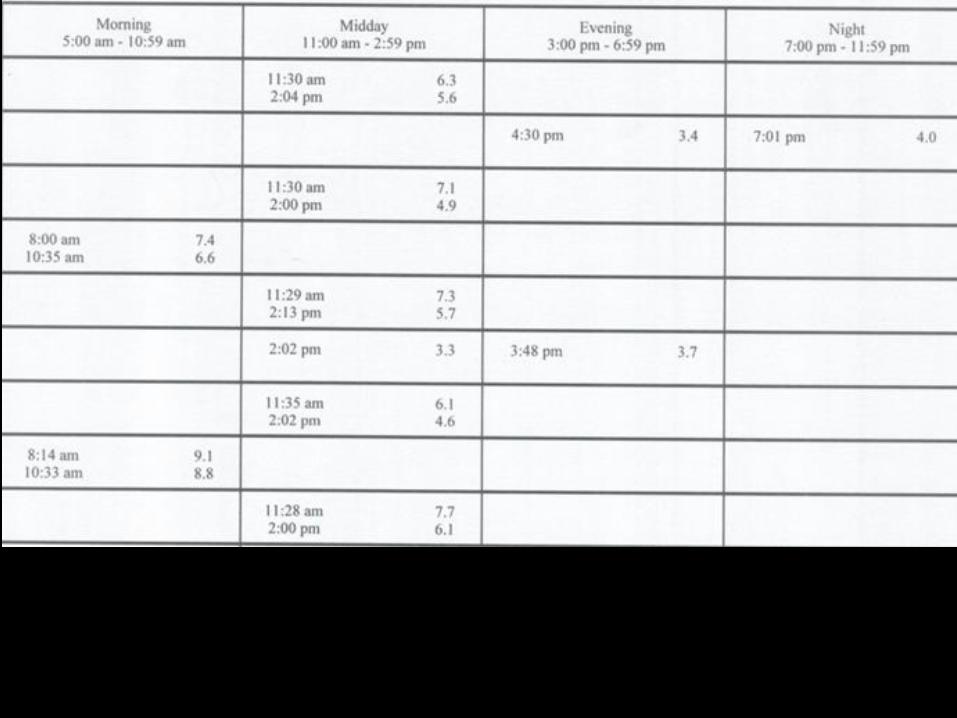
• (Actual A1c) minus (Predicted A1c based on glucose
values)
• Someone has a high HGI, (i.e., rapid glycator) if their
glucoses are good but their A1c is high
• Someone has a low HGI, (i.e., slow glycator) if their
glucoses are high but their A1c is low
Hemoglobin Glycation Index (HGI)
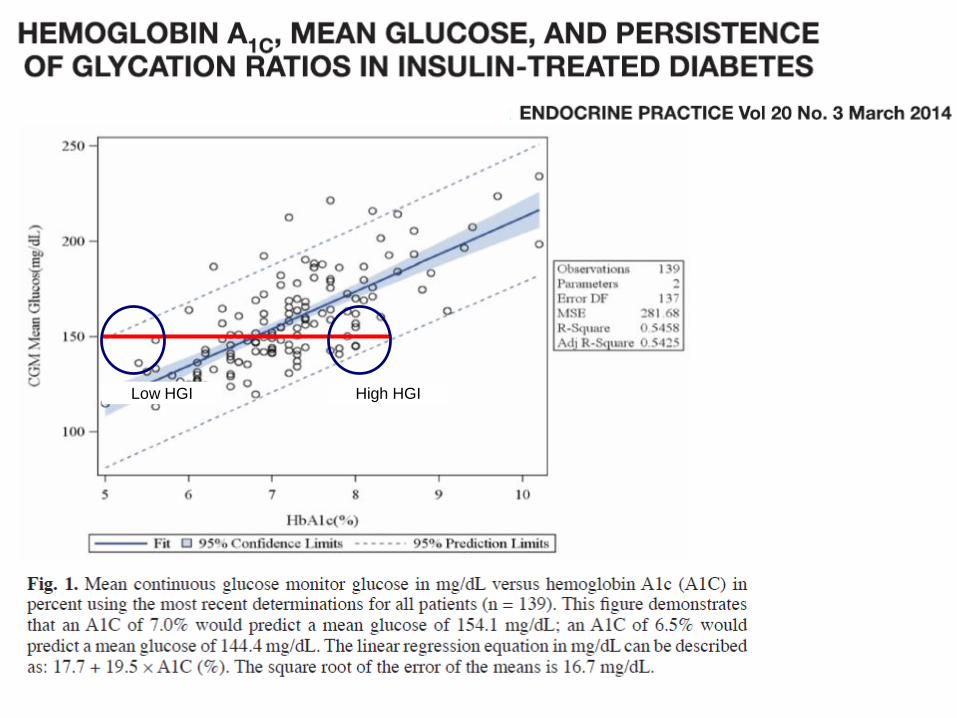
High HGILow HGI
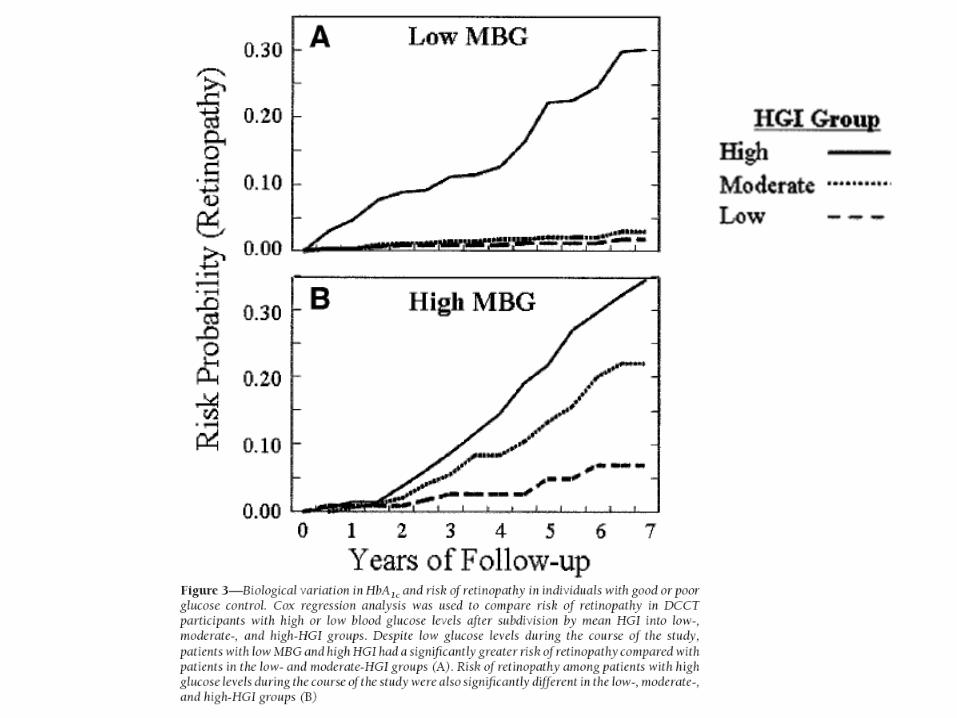
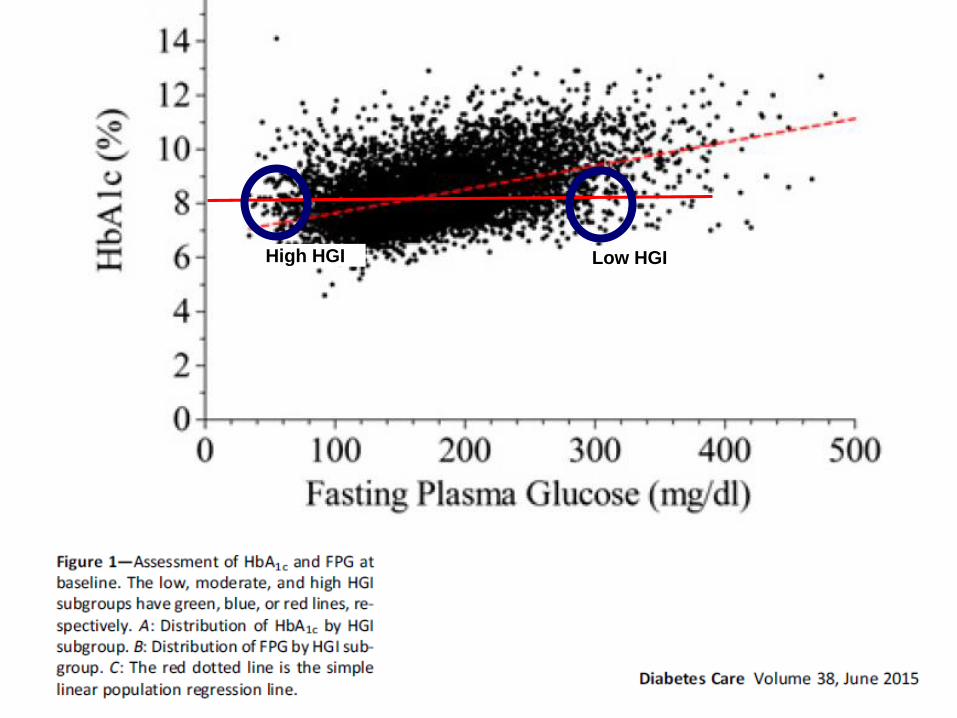
High HGI Low HGI
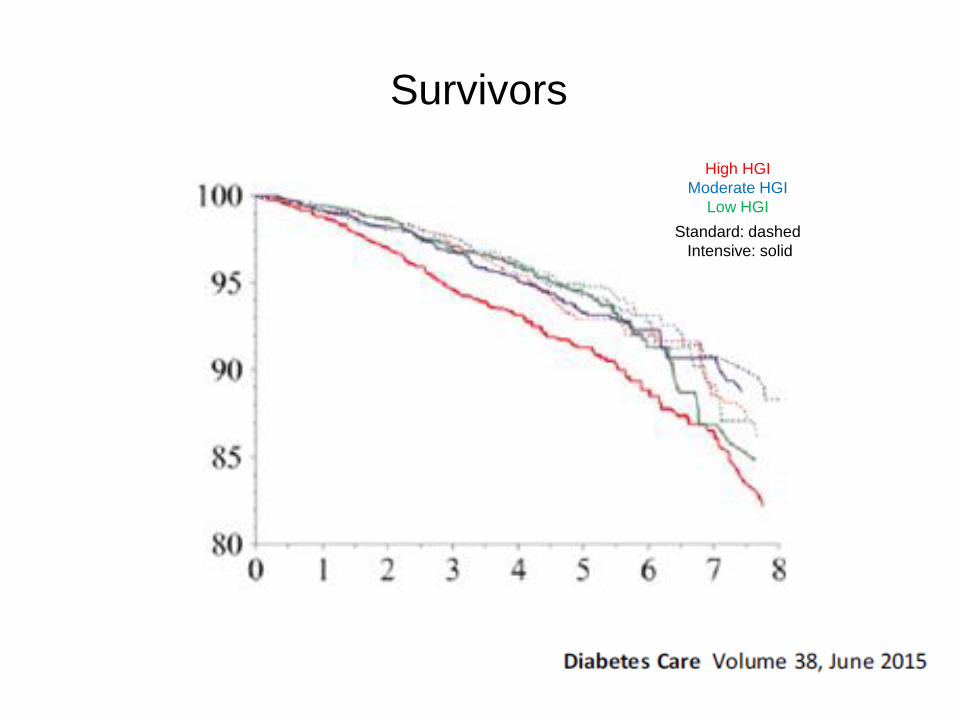
Survivors
Standard: dashed
Intensive: solid
High HGI
Moderate HGI
Low HGI
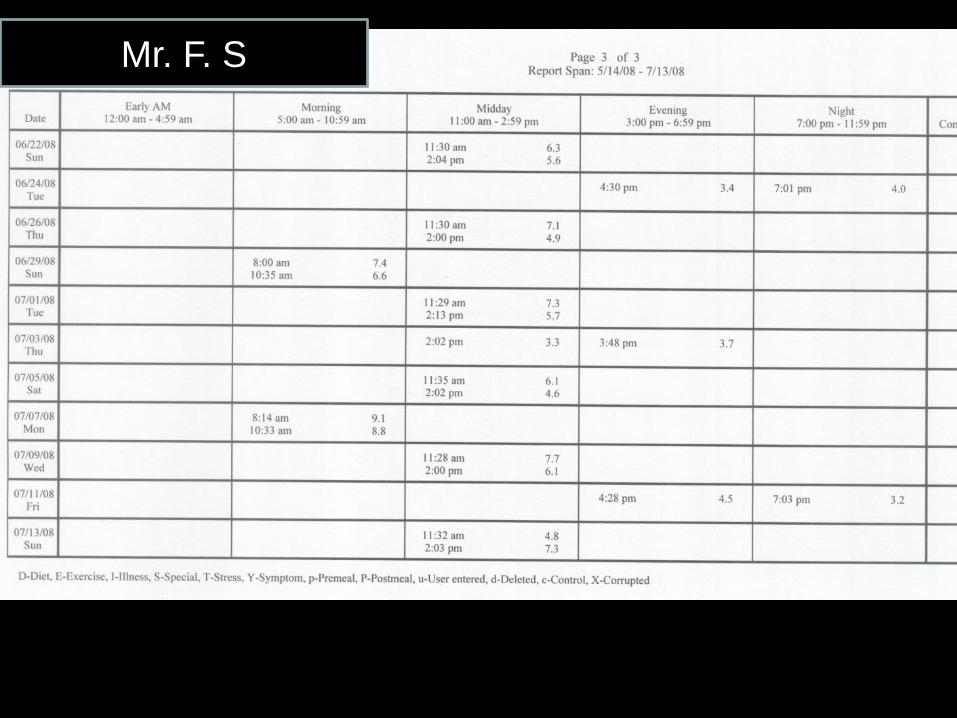
Mr. F. S
What does ACCORD really tell us?
• Tight glycemic control shows CV benefit after
5 years
• People who died had higher A1c’s
• People who died were people in whom it was
not possible to lower their A1c’s
• People who died had a high “Hemoglobin
Glycation Index”
• People who died tended not to be on beta
blockers
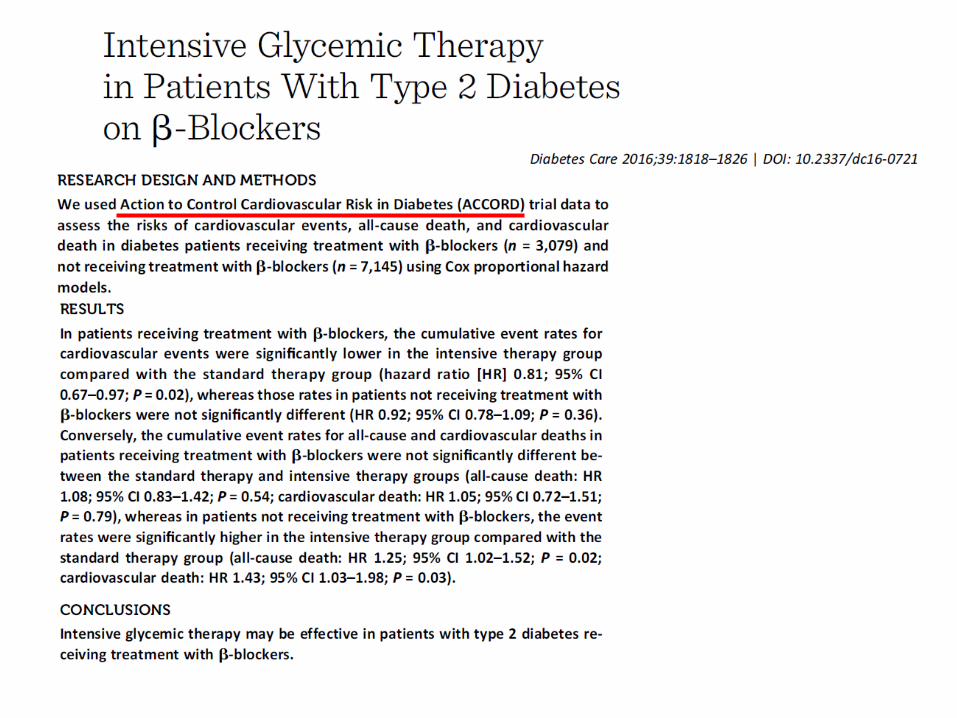
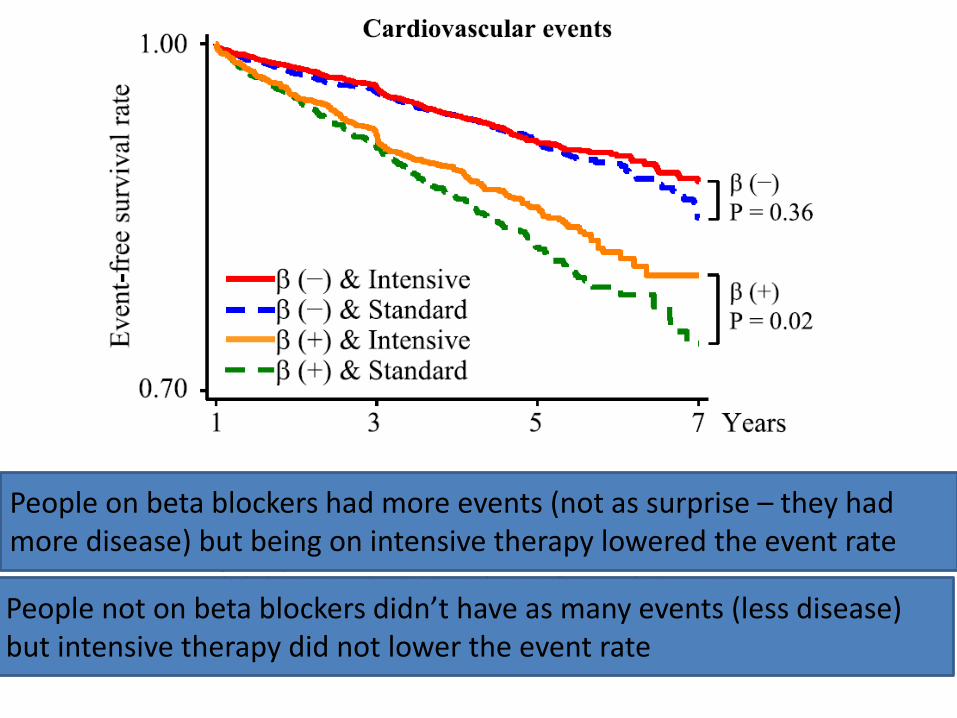
People on beta blockers had more events (not as surprise – they had more disease) but being on intensive therapy lowered the event rate
People not on beta blockers didn’t have as many events (less disease) but intensive therapy did not lower the event rate
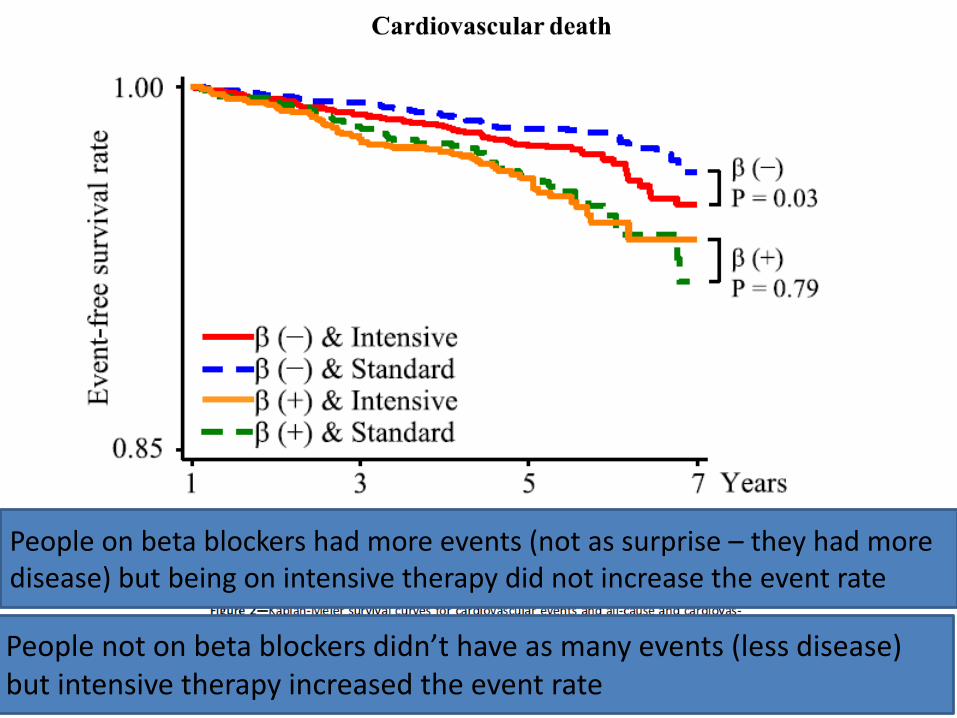
People on beta blockers had more events (not as surprise – they had more disease) but being on intensive therapy did not increase the event rate
People not on beta blockers didn’t have as many events (less disease) but intensive therapy increased the event rate
Summary and Conclusions (1):
• Good glycemic control lowers risk of
microvascular disease
• Aggressive glucose control early in the course of
diabetes seems to be the best strategy
• Aggressive glucose control prior to the
development of a large atherosclerotic burden
seems to be best strategy
• This does not mean that if an individual has had
their diabetes for a long period or has had a CV
event that they won’t benefit – will take more time
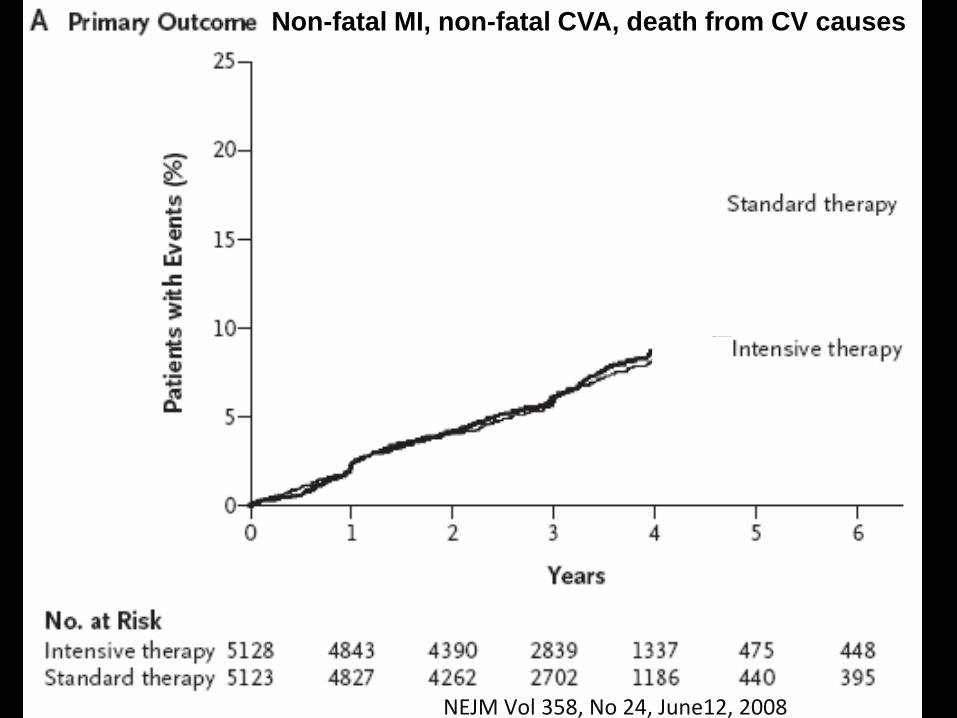
Non-fatal MI, non-fatal CVA, death from CV causes
NEJM Vol 358, No 24, June12, 2008
Non-fatal MI, non-fatal CVA, death from CV causes
NEJM Vol 358, No 24, June12, 2008
Summary and Conclusions (2):
• A1c does not always tell the whole story. Look at
the glucoses – Look at the Pt’s glucose meter!!!
– If A1c is high but glucoses are good, this
patient is a rapid glycator with a high HGI.
• This is a higher risk patient
• There seems no gain in pushing his
glucoses down further to lower his A1c
–It won’t happen
– It would increase risk of hypoglycemia
• Concentrate on other risk factors
• In people with vascular disease, beta blockers appear to
be synergistic with tightening glucose control to lessen
CV complications
– Protection for adrenergic stimulation from either
• Hypoglycemia?
• Further hyperinsulinemia????
Summary and Conclusions (3):
Diabetes and glucose
• How common is diabetes?
• Why do we treat it?
• Does glycemic control predict complications?
• Does improving glucose control prevent complications?
• Does too tight glucose control cause death?
• Glucose vs glycation
• Hemoglobin Glycation Index
• What should our A1c target be?
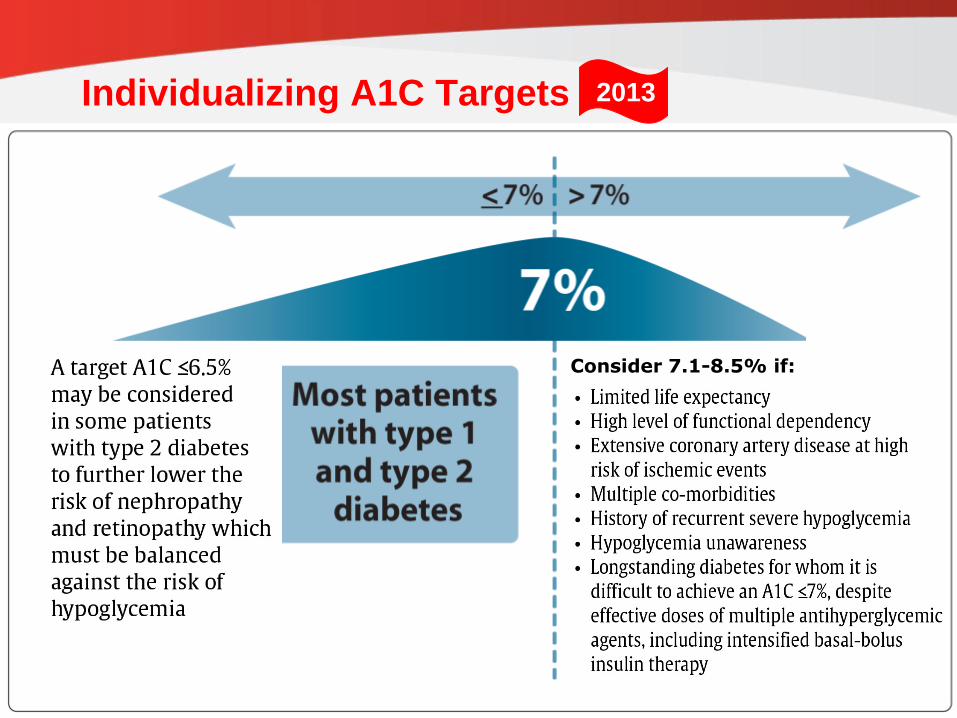
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.ca
Copyright © 2013 Canadian Diabetes Association
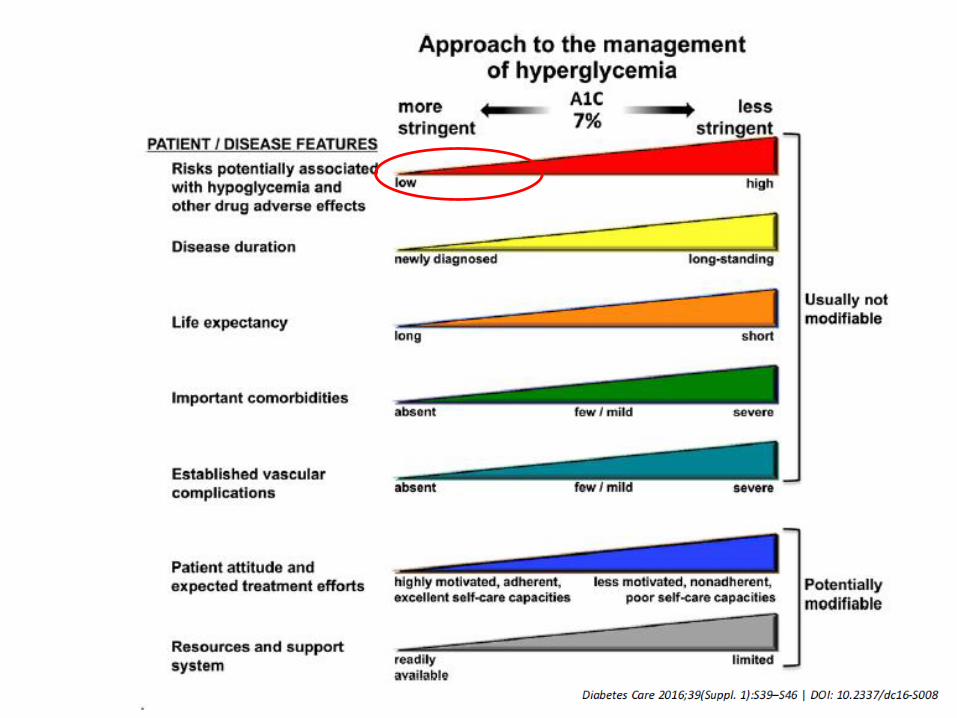
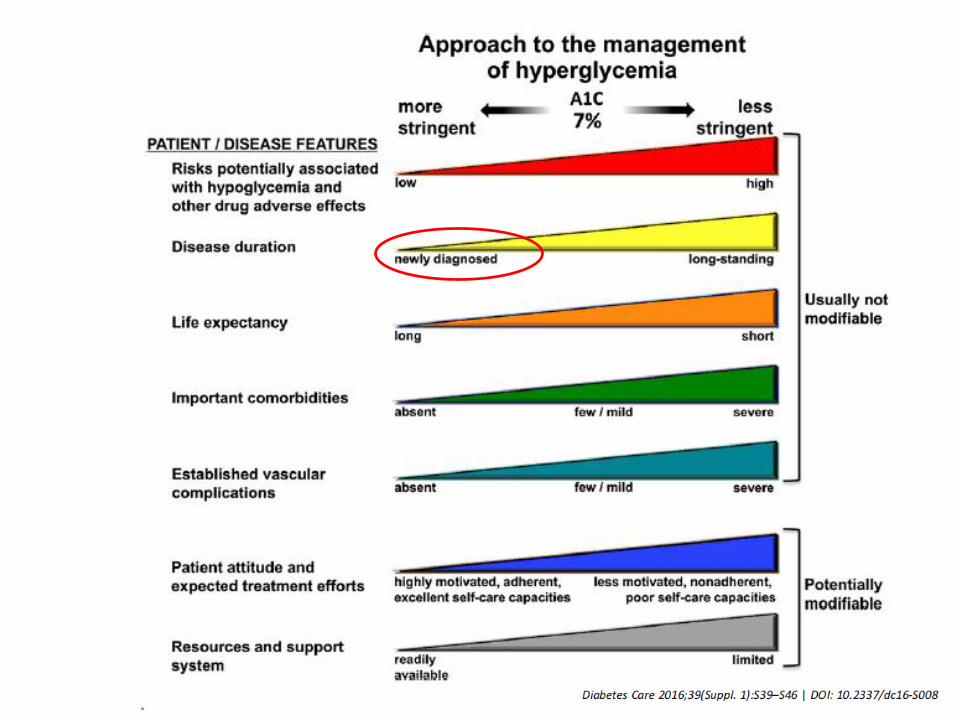
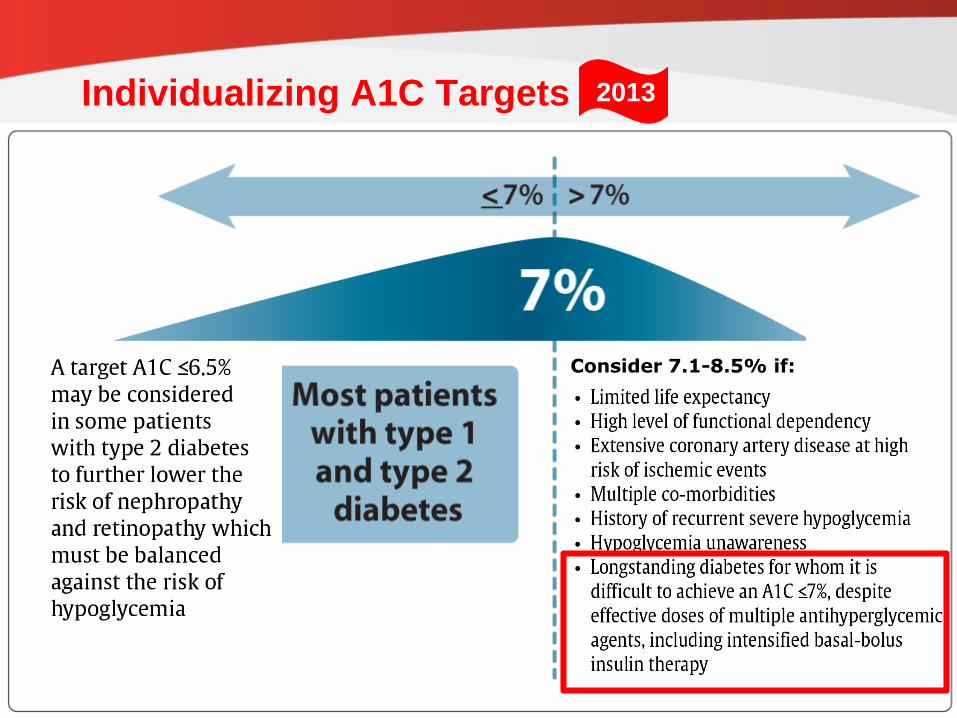
Individualizing A1C Targets
which must be balanced against the risk of hypoglycemia
Consider 7.1-8.5% if:
2013

• Keep the above targets in mind, but …
• Try to achieve the lowest A1c possible with the best
balance of minimal highs and minimal lows
• The determination of “best balance of minimal lows”
depends on risk of hypoglycemia and other general
factors
– To do this, you must look at the meter and the
logbook
Hardin’s suggestion for A1c target:
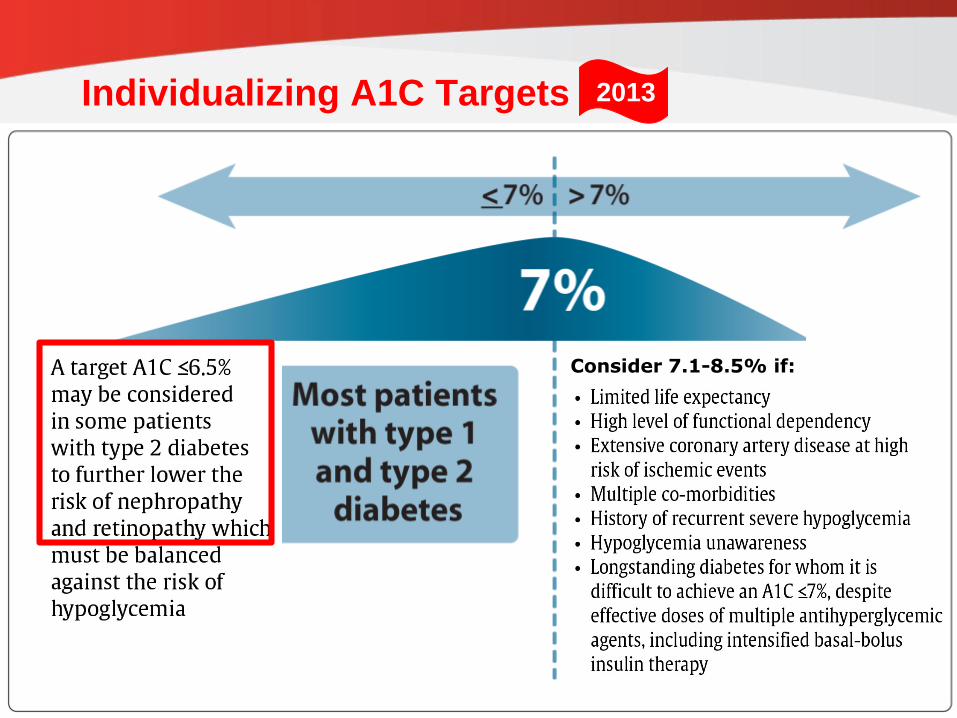
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.ca
Copyright © 2013 Canadian Diabetes Association
Individualizing A1C Targets
which must be balanced against the risk of hypoglycemia
Consider 7.1-8.5% if:
2013
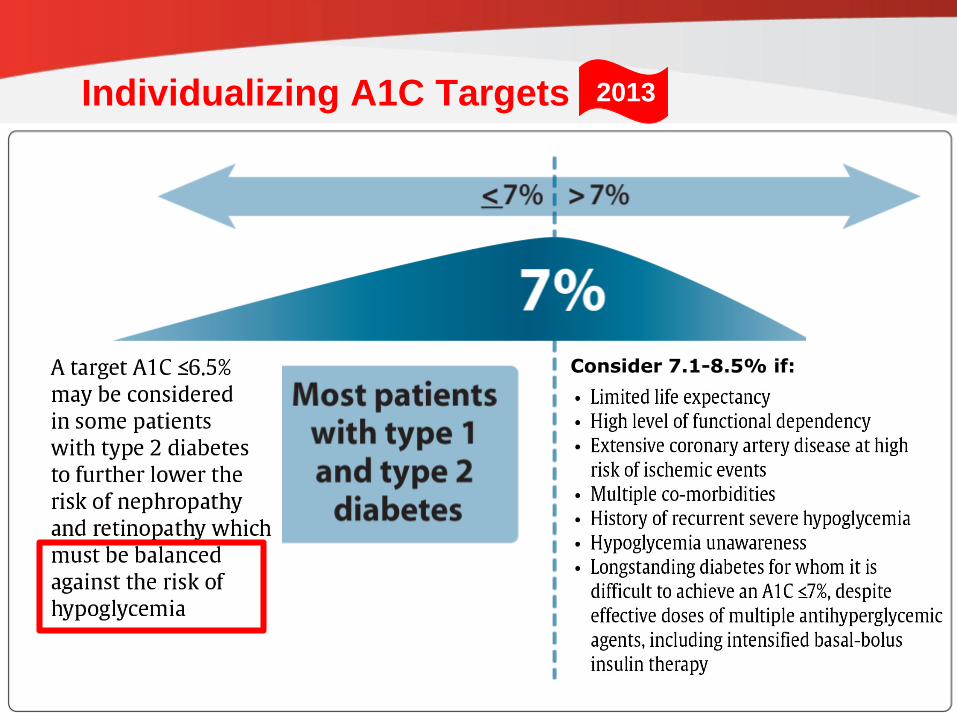
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.ca
Copyright © 2013 Canadian Diabetes Association
Individualizing A1C Targets
which must be balanced against the risk of hypoglycemia
Consider 7.1-8.5% if:
2013
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.ca
Copyright © 2013 Canadian Diabetes Association
Individualizing A1C Targets
which must be balanced against the risk of hypoglycemia
Consider 7.1-8.5% if:
2013