goal-directed resuscitation in sepsis; a case-based … · goal-directed resuscitation in sepsis; a...
TRANSCRIPT

1
Goal-directed resuscitation insepsis; a case-based
approach
Jorge A Guzman, MD, FCCM
Head, Section Critical Care Medicine
Respiratory Institute
Cleveland Clinic Foundation
The challenges to managing septicshock are to find the right
parameters to monitor and the end-points for adequate resuscitation
• The hemodynamic status of critically illpatients is complex
• Complicating co-morbidities
• Conflicting therapeutic goals(hemodynamic instability and ALI/ARDS)

2
Resp
on
se
Days After Injury
Pro
gre
ssiv
eO
rgan
Dysfu
ncti
on
Injury
1 3 10 14 21
Primary OrganDysfunction
Secondary OrganDysfunction
Sh
oc
k
Resu
scit
ati
on
Reco
very
Reco
very
SIRS
Early GoalDirectedTherapy
AppropriateAntibiotics
Management of shock
Glucose control
Ventilatory support
aPC
Earlyrecognition
Beal, AL. JAMA 1994 271;226-33.
Goal-directed resuscitation
Identify circulatory failureMAP < 65 mm Hg – Lactate > 2 mmol/L
Global macrocirculatory goals• MAP > 65 mm Hg• Adequate preload
• Adequate urine output
Microcirculatory goals• ScvO2 > 65-70%
• Lactate < 2 mmol/L• Base excess
• Microcirculation assessment• PCO2 gap
• NIRS• OPS
Tim
ing UPSTREAM
DOWNSTREAM

3
A 72 y/o male presented to the ED with increasing SOB, feverand cough. He has no significant PMH. His initial BP was 85/55mm Hg. Mechanical ventilation was started due to poorresponse to O2 supplementation via VM. He was resuscitatedwith 2 L on NS and sent to the MICU. An hour later his SBPremains in the 90s, he is making some urine, and he hasreceived 3.5 L of NS thus far
Physicians in the ICU continue
administering intravenous fluids
SSC guidelines for initial resuscitation
Central venous pressure 8-12 mm Hg
Mean arterial pressure (MAP) ≥65 mm Hg
Urine output ≥0.5 mL·kg-1·hr-1
Central venous (superior vena cava) or mixed venousoxygen saturation ≥70% or ≥65%, respectively (grade1C)
If ScvO2 or SvO2 of 70% or 65%, respectively, is notachieved with fluid resuscitation to the CVP target, thentransfusion of PRBC to achieve a Htc of ≥30% and/oradministration of a dobutamine infusion (up to amaximum of 20 μg·kg-1·min-1) be used to achieve thisgoal (grade 2C).
Crit Care Med 2008; 36:296-327

4
Central venous andarterial catherization
Sedation, paralysis (ifintubated), or both
Hospital admission
Crystalloid
Colloid
Vasoactive agents
Transfusion of red cellsuntil hematocrit 30%
Inotropic agents
CVP
Goalsachieved
ScvO2
< 8 mm Hg
8 - 12 mm Hg
65 and 90 mm Hg
70 mm Hg
No
Yes
< 65 mm Hg
> 90 mm Hg
< 70%
< 70%
70%
Supplemental oxygen ±endotracheal intubation and
mechanical ventilation
MAP
Engl J Med. 2001;345:1368-1377.
Volume resuscitation was sufficient
to restore ScvO2 of >70%
in 36% of all patients
In-hospital mortality
30.5
46.5
0
20
40
60
80
100
Protocol
Controls
28-day mortality
33
49
0
20
40
60
80
100
Protocol
Controls
60-day mortality
4457
0
20
40
60
80
100
Mortality (%)
Protocol
Controls
*
*
*
EGDT; administered treatments
*
Rivers E. NEJM 2001; 345:1368-1377
IV Fluids
5
3.5
0
2
4
6
8
10
12
6 hr pRx 7-72 hr pRx
IVflu
ids
(L)
EGDT
Controls
PRBC
0
20
40
60
80
100
6 hr pRx 7-72 hr pRx
Pa
tie
nts
(%)
EGDT
Controls 0
10
20
30
40
50
60
Press
ors0-
6
Press
ors7-
72
Dobuta
0-6
Dobuta
7-12
MV
0-6
MV
7-72
PAC
0-6
PAC
7-72
Pe
rce
nt
(%)
EGDT
Standard
*
*
9% of EGDT ptsgot nitroglycerin!
5
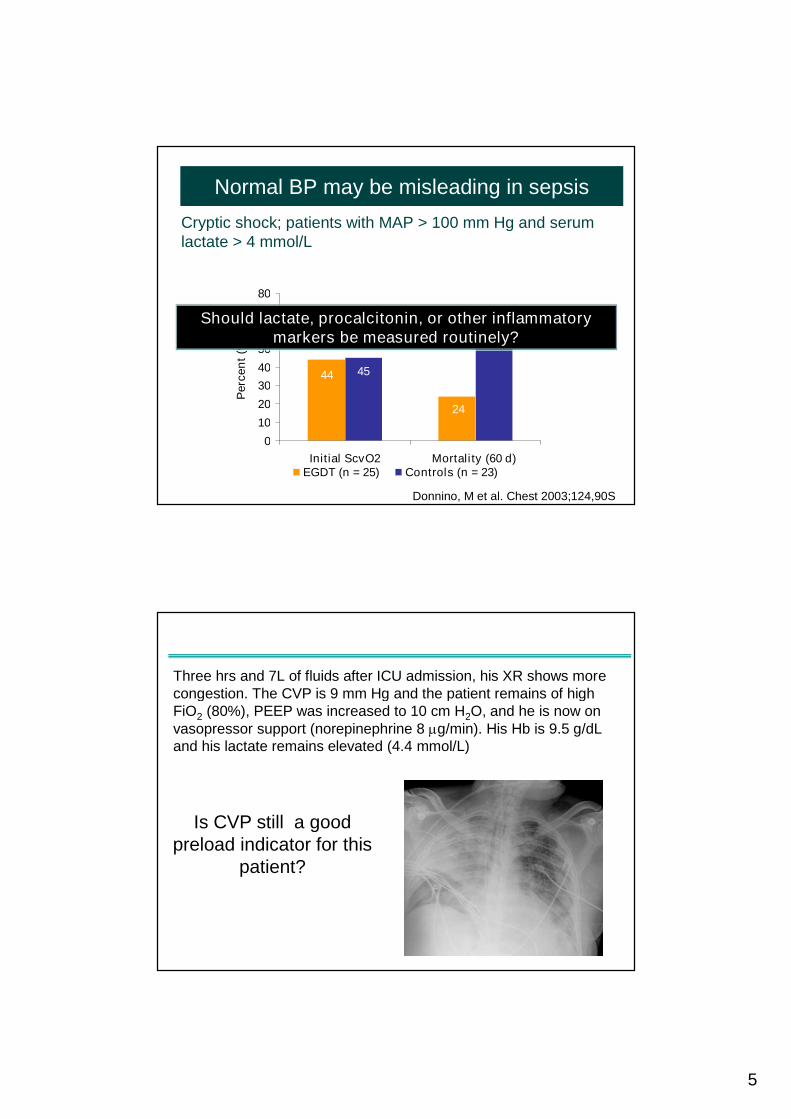
Normal BP may be misleading in sepsis
24
44
70
45
0
10
20
30
40
50
60
70
80
Initial ScvO2 Mortality (60 d)
Perc
en
t(%
)
EGDT (n = 25) Controls (n = 23)
Cryptic shock; patients with MAP > 100 mm Hg and serumlactate > 4 mmol/L
Donnino, M et al. Chest 2003;124,90S
*
Should lactate, procalcitonin, or other inflammatorymarkers be measured routinely?
Three hrs and 7L of fluids after ICU admission, his XR shows morecongestion. The CVP is 9 mm Hg and the patient remains of highFiO2 (80%), PEEP was increased to 10 cm H2O, and he is now onvasopressor support (norepinephrine 8 g/min). His Hb is 9.5 g/dLand his lactate remains elevated (4.4 mmol/L)
Is CVP still a goodpreload indicator for this
patient?

6
What to monitor? Preload
• Preload is defined as the load before contraction of theventricle starts
• Static measures of preload– CVP/RAP – right ventricular preload
– PAOP – left ventricular preload
– EDV - usually by echo
• Dynamic measures of preload– Examine CV response to respiratory changes in pleural
pressure, mainly in ventilated patients
– Give a fluid bolus and see what changes- the classical fluidchallenge…
Static measures of preloadThere is NO correlation between blood volume and CVP

7
0
2
4
6
8
10
12
CVP
mm
Hg
Responders
Non responders
Intensive Care Med 2004; 30:1740Crit Care Med 2007; 35; 64
32/66 VLS (48%)500 mL HES27>15% SVISeptic shockMichard F (2003)
20 (53%)500 ml NS38>15% in ABF(Doppler)
Critically ill w/circulatory failure
Monnet X (2005)
20 (39%)4 ml/kg colloid x251>10% in SVICritically ill w/circulatory failure
Vallee F (2005)
9 (43%)1 L Ringer or 500mL HES
21>15% in COCritically ill w/circulatory failure
Heenan S (2006)
RespondersChallengeNDefinition ofResponders
Patients
4 (40%)25 mL/Kg ofRinger
10Increase in COSepsis w/circulatory failure
Swensen CH(2006)
21/35 VLS (60%)500-1000mL15>15% SVISepsisw/circulatory
failure
Tavernier B(1998)
16 (40%)500 mL HES40>15%Septic shockcirculatory failure
Michard F (2000)
13/22 VLS (59%)8 ml/kg HES20>15% CISeptic shockFessel M (2005)
10 (15%)PLR & 500 ml NS22>15% in ABF(Doppler)
Critically ill w/circulatory failure
Lafanechère A(2006)
Hofer CK (2005)
Preisman S(2005)
21 (60%)10 mL/kg (IBS) 6% HES
35>35% SVIAbdominalsurgery
32/70 VLS (46%)250 mL colloids18>15% SVCardiac surgery
50% of critically ill patients may be loaded with fluidsunnecessarily!
He
mo
dyn
am
icre
sp
on
seto
fluid
load
ing

8
Ann Surg 2003; 238:641
Fluid balance and outcomes
CCM- 2006;12:219
NEJM 2006; 354:2564
If CVP is not the answer, then what?
Arterial pressure variations during mechanical ventilation
Reverse pulsus paradoxus
Anesthesiology 2005; 103:419

9
Small scale-high speed
Large scale-slow speed
Quick bedside trick
• Drawbacks
– No spontaneous breathing efforts
– Need larger tidal volumes (> 8mL/kg)
– Arrhythmias
– Assure accurate line recording (avoid bubbles, kinks,clots, etc)
– Does not work in patients with cor pulmonale - RVF
– Caution in CHF
What to monitor?Dynamic measures of preload- Arterial pressure variations
10
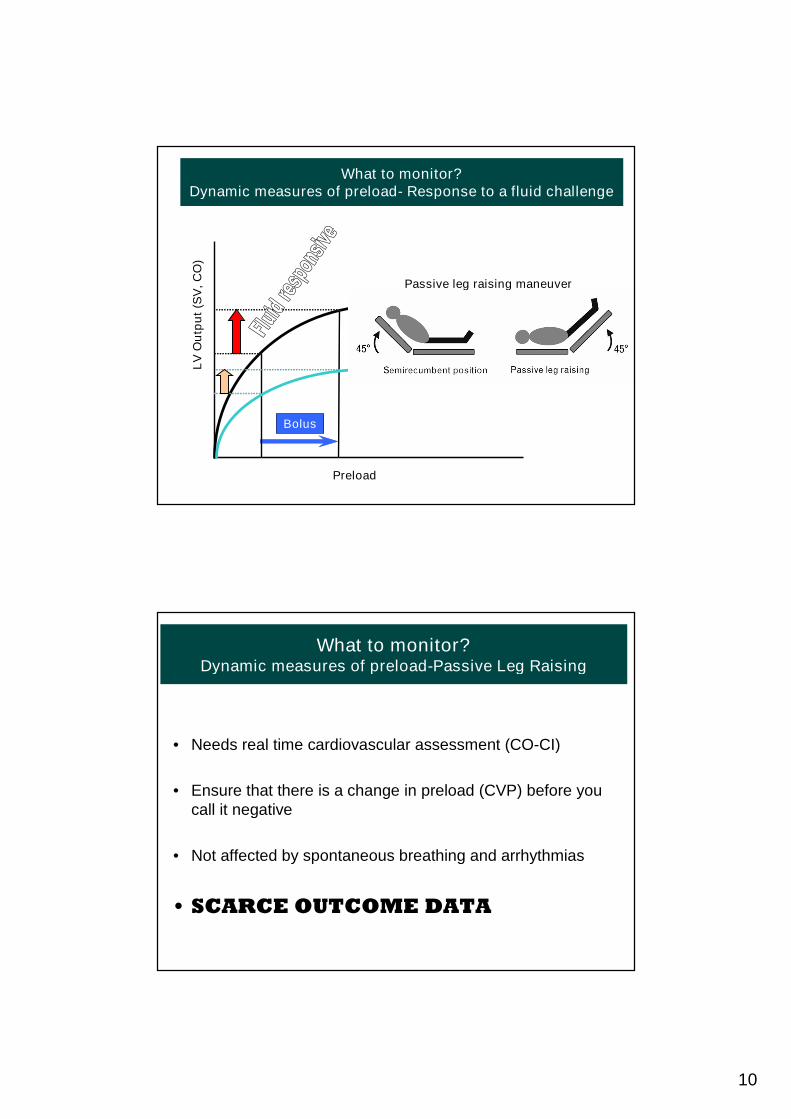
What to monitor?Dynamic measures of preload- Response to a fluid challenge
Preload
LV
Ou
tpu
t(S
V,
CO
)
Normal Contractility
Bolus
Decreased Contractility
Passive leg raising maneuver
What to monitor?Dynamic measures of preload-Passive Leg Raising
• Needs real time cardiovascular assessment (CO-CI)
• Ensure that there is a change in preload (CVP) before youcall it negative
• Not affected by spontaneous breathing and arrhythmias
• SCARCE OUTCOME DATA

11
Five hours after ICU admission, MAP is 60 mm Hg on 30mcg/min of NE. His CVP is 10 mm Hg and no longer fluidresponsive. He remains mechanically ventilated requiringhigh FiO2 (0.6) and high PEEP and has minimal urine output.
ScvO2 is 62% and serum lactate is 4.2 mmol/L
Is it time to know his cardiac output?

12
• Misuse of CO may worsen outcomes– Hayes et al. Elevation of Systemic Oxygen Delivery in the Treatment of
Critically Ill Patients. NEJM 1994;330:1717
• It would be of value if it guided therapies toimprove outcomes…
What to monitor?Stroke volume and cardiac output
CVP goals in Sepsis Trials
0
1
2
3
4
4 6 8 10 12 14 16 18
Trial CVP goal
Nu
mb
er
of
tria
ls
MAP goals in Sepsis Trials
0
1
2
3
4
60 65 70 75 80 85 90 95 100
Trial MAP goal
Nu
mb
er
of
tria
ls
CI goals in Sepsis Trials
0
1
2
3
4
2 3 4 5 6 7
Trial CI goal
Nu
mb
er
of
tria
ls
PAOP goals in Sepsis Trials
0
1
2
3
4
10 11 12 13 14 15 16 17 18
Trial PAOP goal
Nu
mb
er
of
tria
ls
Crit Care 2007; 11 R67
To Swan or not to Swan?

13
What to monitor?Stroke volume and cardiac output
Cardiacoutput
Electricimpedance/reactance
Arterial waveformanalysis-
Pulse contour(can also get SVV)
Lithium indicatordilution
Transpulmonarythermodiluton(can also getSVV-EVLW)
Indirect Fick
Partial CO 2
rebreathing
Transthoracic-transesophageal
Echocardiography
Thermodilution(PAC)
The future:Intensivists assessing LVF
using hand-held echo
• 6 hr of US training
• Blinded to the patient’s clinical condition
Severe failureMild-Moderate
71%69%Correct interpretation-Degree of LV failure
80%92%Correct interpretation
Abnormal LVFNormal LVF
Melamed R et al. Chest 2009; 135:1416

14
Six hours after ICU admission, MAP is 62 mm Hg on22 mcg/min of NE and 5 mcg/min dobutamine. HisCVP is 12 mm Hg and no longer fluid responsive.He remains mechanically ventilated with an FiO2 of0.6. Lactate is 3.5 mmoL/L. Cardiac output obtainedby pulse contour is 6.0 L/min
Should we now focus on ScvO2 and/or lactates asend-points of resuscitation?

15
Understanding ScvO2
92
92
72
71
9975
97
66
88
7578
The difference between ScvO2 and SvO2
changes in shock
ScvO2 > SvO2 by 5-8 %units
What to monitor?Central venous oxygen saturation
Oxygen Delivery
Oxyg
en
Co
nsu
mp
tio
nL
acta
teS
VO
2(S
cV
O2) VO2 (SvO2 - ScvO2)
Lactic acidosis
Critical OxygenDelivery Threshold
If Hb and SaO2 are
normal a lowScvO2/SvO2
reflects a LOWOUTPUT state
BUT IT DOES NOTTELL YOU THE REASON

16
Since metabolic demands vary widelyin critically patients,
there is NO NORMAL CARDIAC
OUTPUT for critically ill patients
ScvO2 may help decide whetheradditional interventions are
necessary
Oxygen Delivery
Oxyg
en
Co
nsu
mp
tio
nL
acta
teS
VO
2(S
cV
O2)
A normal ScvO2 does not indicateadequate perfusion in sepsis
Treciak S et al. Critical Care 2008;9(suppl):S20

17
Crit Care Med 1988; 16: 655-658
Low venous oxygen saturation wasinfrequent in a Dutch study
• Mean ScvO2 74.0 ± 10.2%; mean lactate 2.7 ±2.2 mmol/L. Mean CVP 9.8 ± 5.4 mm Hg. Only1% (of septic shock pts) had a ScvO2 < 50% van
Beest et al. Critical Care 2008; 12:R33
• Baseline ScvO2 in patients with septic shock (n79) was 71 ± 12.3 % Shapiro NI et al, Crit Care Med 2006;34:1025-32
Venous saturation was high amongpatients in the Multiple Urgent Sepsis
Therapies (MUST) protocol
18
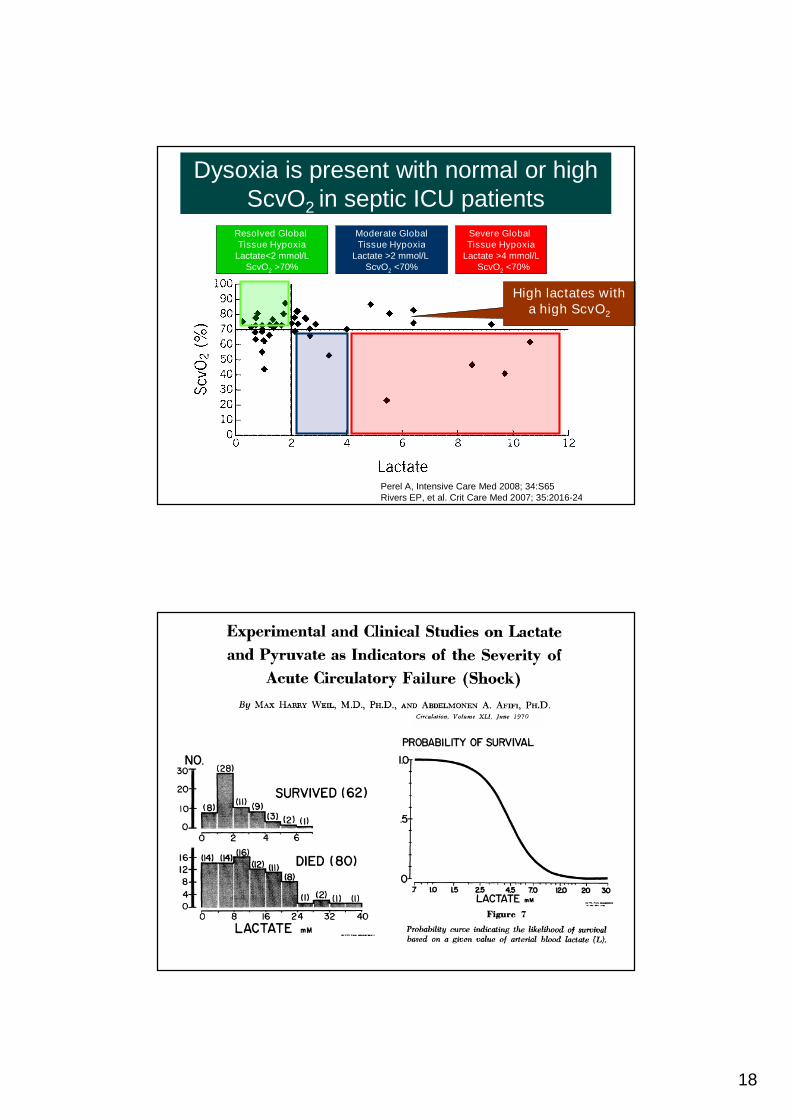
Dysoxia is present with normal or highScvO2 in septic ICU patients
Perel A, Intensive Care Med 2008; 34:S65Rivers EP, et al. Crit Care Med 2007; 35:2016-24
Severe GlobalTissue Hypoxia
Lactate >4 mmol/LScvO2 <70%
Moderate GlobalTissue Hypoxia
Lactate >2 mmol/LScvO2 <70%
Resolved GlobalTissue Hypoxia
Lactate<2 mmol/LScvO2 >70%
High lactates witha high ScvO2

19
Am J Surg 1996;171:221
Ann Emerg Med 2005; 45:524-8
Hyperlactatemia; aerobic etiologyrelevant to sepsis
• Increased aerobic glycolysis bycatecholamine stimulated Na+-K+ ATPasehyperactivity (Lancet 2005; 365:871)
• Mitochondrial dysfunction (Lancet 2002; 360:219)
• Impaired pyruvate dehydrogenase activity(Shock 1996; 6:89)
• Sepsis-induced impaired lactate clearance(Am J Resp Crit Care Med 1998;157:1021)
Paradigm shiftHyperlactatemia due to tissue hypoxiamay be the exception and not the rule
May explain failed trials aimingat supranormal DO2

20
• Failure to normalize lactate carried a 100% mortality• Clearing between 48-96 hrs had a 42.5% mortality• Patients clearing in <24 hr had a mortality of 4%
Am J Surg 2001; 182;481-5
Crit Care Med 2004; 32:1637-62
The selection of hemodynamic parameters tomonitor and end-points for resuscitation during
septic shock is rarely straightforward!
The complexity of critical illness and the presence oftherapeutic conflicts (heart vs. lungs) necessitates
monitoring of a combination of parameters
Preload&
Fluid responsiveness
Cardiac function
CO-SV- echo
ScvO2
Lactate
Hemodynamic management in shock
Macrocirculation Microcirculation

21
• Protocol driven early aggressive goal-directedresuscitation improve the outcome of patients in septicshock IF INITIATED EARLY
• Monitoring techniques that couple measurement of COwith ventilatory variations of systolic arterial pressure,pulse pressure, and SV enhance the ability to predictfluid responsiveness in circulatory failure
• Agreeing on end-points for resuscitation is difficult, but acombination of macro and microcirculatory targetsseems likely to yield better results
In summary…