governing body - nhs doncaster ccg marco pieri – locality lead, north west locality dr niki seddon...
TRANSCRIPT
Governing Body
To be held on Thursday 18
th May 2017
From 1pm until 4pm
in the Boardroom, Sovereign House, Heavens Walk, Doncaster DN4 5HZ

Governing Body
To be held on Thursday 18 May 2017 Commencing at 1pm – 4pm
In the Boardroom, Sovereign House, Heavens Walk, Doncaster, DN4 5HZ
PUBLIC AGENDA
Presenter Enc
1. Welcome and Introductions
Chair Verbal
2. Apologies
Chair Verbal
3. Declarations of Interest
Chair Verbal
4. Questions from Members of the Public (See our website for how to submit questions – required in advance)
Chair Verbal
5. Minutes of the previous meeting held on 20 April 2017
Chair Enc A
6. Matters Arising
Chair Verbal
Assurance
7. Quality & Performance Report
• Spotlight report on Planned Care Delivery Plan
• Spotlight report on and Primary Care Delivery Plan
Mr Russell & Mr Fitzgerald
Enc B
8. Finance Report
Mrs Tingle Enc C
9. Corporate Assurance Report Quarter 4 2016/2017
Mrs Atkins Whatley
Enc D
Standing Items
10. Chair & Chief Officer Report
Dr Crichton & Mrs Pederson
Enc E
11. Locality Feedback
Locality Leads Verbal
12. Receipt of Minutes
• Audit Committee – Minutes of the meeting held on 9 March
2017. • Quality & Patient Safety Committee – Minutes of the
meeting held on 2 March 2017. • Working Together Joint Committee of Clinical
Commissioning Groups – Minutes of the meetings held
on 21 March 2017.
Chair Enc F
13. Any Other Business
Chair Verbal
14. Date and Time of Next Meeting Thursday 15 June 2016 at 1pm in the Boardroom, Sovereign House, Heavens Walk, Doncaster, DN4 5HZ
Chair Verbal
To resolve that representatives of the press, and other members of the public, be excluded from the remainder of this meeting having regard to the confidential nature of the business to be transacted, publicity on which would be prejudicial to the public interest Section 1(2) Public Bodies (Admission to Meetings) Act 1960.
Chair
Verbal
Item 1
Welcome & Introductions

Verbal
Item 2
Apologies for Absence

Verbal
Item 3
Declarations of Interest

Verbal
Item 4
Questions from Members of the Public

Enc A
Item 5
Minutes of the previous meeting

1
Minutes of the Governing Body Held on Thursday 20th April 2017 commencing at 1pm
In the Boardroom, Sovereign House, Heavens Walk, Doncaster, DN4 5HZ Members Present:
Dr David Crichton – NHS Doncaster CCG Chairman (Chair) Miss Anthea Morris – Lay Member and Vice Chair of the Governing Body Mrs Sarah Whittle – Lay Member Dr Emyr Wyn Jones – Secondary Care Doctor Member Dr Nick Tupper – Locality Lead, Central Locality Dr Jeremy Bradley – Locality Lead, North East Locality Dr Marco Pieri – Locality Lead, North West Locality Dr Niki Seddon – Locality Lead, North West Locality Dr Pat Barbour – Locality Lead, South East Locality Dr Khaimraj Singh – Locality Lead, South East Locality Dr Karen Wagstaff – Locality Lead, South West Locality Mrs Jackie Pederson – Chief Officer Mrs Hayley Tingle – Chief Finance Officer Mr Andrew Russell – Chief Nurse
Formal Attendees present
Mrs Sarah Atkins Whatley – Chief of Corporate Services Mrs Laura Sherburn – Chief of Partnerships Commissioning and Primary Care Mr Anthony Fitzgerald – Chief of Strategy & Delivery Dr Rupert Suckling – Director of Public Health (from item 7)
In attendance:
Mrs Jayne Satterthwaite – PA (Taking Minutes) Mr Ian Carpenter, Head of Communications & Engagement Mr Lee Golze, Head of Strategy & Delivery Children & Maternity, (Item7)
Mrs Amy Coggan, Head of Performance and Intelligence – Acute Care, (Item 9) Mr Andrew Goodall – Healthwatch (Attending on behalf of Mrs Debbie Hilditch) (Item 8)
ACTION
1. Welcome and Introductions Dr Crichton welcomed everyone to the Governing Body meeting. There were 4 members of the public and 2 members of NHS Doncaster CCG staff in attendance at the meeting.
2. Apologies Apologies for absence were received from:
• Mrs Linda Tully – Lay Member
2
• Dr Lindsey Britten – Locality Lead, South West Locality
• Mr Damian Allen – DMBC Representative
• Mrs Deborah Hilditch – Healthwatch Representative
3. Declarations of Interest The Chair reminded members of their obligations to declare any interest they may have on any issues arising at meetings which might conflict with the business of NHS Doncaster Clinical Commissioning Group. Declarations declared by members are listed in the CCG’s register of Interests. The Register is available either via the secretary to the Governing Body or the CCG website at the following link www.doncasterccg.nhs.uk The meeting was noted as quorate. Declarations of interest from sub-committee/working groups: None declared. Declarations of interest from today’s meeting: None declared.
4. Questions from Members of the Public/ Patient Stories Questions from Members of the Public Mrs Atkins Whatley informed the Governing Body that the following questions regarding Due Regard Statements has been received from Mr Wright:
• Has the Due Regard Statement changed since 2015? Mrs Atkins Whatley stated that Equality analysis is a way of considering the effect (or in legal terms giving ‘due regard’) to different groups protected from discrimination by the Equality Act 2010, such as people of different ages, or people with disabilities. It involves using equality information, and the results of engagement with protected groups and others, to understand the actual effect or the potential effect of our functions, policies of decisions. We use a standard template for CCG equality analysis. This has not changed since 2015 except to update our corporate logo. We have recently refreshed and re-published our Equality & Diversity Strategy which includes our approach to equality analysis and our commitment both to our population and our staff members.
• If so what are the changes?
3
Not applicable.
• Is it likely to be changes before 2021? We regularly review corporate templates, including our equality analysis form. We may start to consider changes as we work more closely with other commissioners.
• If so when will it be changed? Not applicable.
Dr Crichton highlighted that a review of public questions had been undertaken by the Governing Body at strategy and are available on the website, he also highlighted that there are other mediums which the Public may ask questions of the Governing Body and NHS Doncaster CCG. These include formal letters, Healthwatch and via our enquiries email address [email protected]. Patient Story It was noted that there was no patient story.
5. Minutes of the Previous Meeting held on 16th March 2017 The minutes of the meeting held on 16th March 2017 were agreed as an accurate record.
6. Matters Arising Declarations of Interest Dr Crichton informed the Governing Body that he would liaise with Dr Britten outside of the meeting regarding the completion of a new Declaration of Interest form to reflect that Dr Britten had ceased practising at the Scott Practice and commenced at the Church View Practice. Quality & Performance Report Dr Seddon advised that the 50% target for Improving Access to Psychological Therapies has been set nationally. Delivery of the CCG Commissioning Strategy Mr Fitzgerald advised that the Delivery Plans and Dashboard will be exclusive of acronyms going forward. Mrs Whittle reported that she had commenced meetings with
Dr Crichton
4
Commissioning Managers to discuss the introduction of patient engagement methodologies within the Delivery Plans. Primary Care Delivery Plan Mrs Sherburn reported that the Primary Care Commissioning Committee will discuss GP consultation times at a future meeting. Quality & Performance Report Mr Fitzgerald reported that NHS Doncaster CCG is working with the Trust to find ways to improve the response rate of the Friends and Family Test (FFT) in A&E. Mr Russell stated that the Clinical Quality Review Group (CQRG) has discussed numerous options to improve the response rate and will now look at alternative ways to obtain patient views. The A&E response rate is positive albeit low. Out of Hours Home Visits Mr Fitzgerald reported that the Out of Hours Home Visits are not currently completed within 1 hour and work is ongoing with Fylde Coast Medical Service (FCMS) to address this and will managed through the monthly contract meetings. Chair and Chief Officer Report Mrs Atkins Whatley advised that the removal of the Terms of Reference for each Committee from our Constitution is currently out to consultation with the Membership.
7. Children & Young People Plan Presentation Mr Golze attended the Governing Body to give a presentation on the Children & Young People Plan and explained that the plan is a statutory requirement of the Borough. Mr Golze highlighted the following points:
• The interim Children & Young People (CYP) plan expired on 31st March 2016 and an Interim Executive Group was established to lead on developing a new plan.
• The plan sets out the overall ambition for CYP that translates into action and how we monitor impact. The new three year plan was agreed at full Cabinet on 28th March 2017.
• There are 12 priorities, set out under four key themes.
• These are drawn from intelligence, Joint Strategic Needs Assessment (JSNA) and the voice of CYP.
• To complement the voice of CYP, there was a collation of socio- economic and health data and the analysis looked at emerging trends and what the need is.
• Doncaster has been awarded funding for social mobility.
• The findings were categorised under the four thematic headings;
5
Safe, Healthy and Happy, Achievement and Equality.
• There are a number of key priorities as follows: o Children have access to the right services at the earliest
opportunity. o Domestic abuse practice is transformed across Doncaster. o No child suffers significant harm as a result of neglect. o Keeping teenagers and young people safe. o Children and Young People are healthy, have a sense of
wellbeing and are resilient. o Children have the best start in life. o Children and young people’s development is underpinned
through a healthy lifestyle. o Ensure all children are school ready. o All children attend a good or better setting and aspirations are
raised to ensure they reach their full potential. o Young people are equipped to access education, employment or
training in a way that supports future social mobility. o Diminish the difference between disadvantage and non-
disadvantaged children and young people. o Fewer children live in poverty.
• There is a comprehensive action plan that sits underneath the plan. The governance arrangements around this have been reviewed with subsequent recommendations. An outcomes framework will be developed and we will measure the impact we are having. Mr Golze is involved in the development of the outcomes framework.
• An analysis of the total spend will be undertaken in line with statutory responsibilities and priorities.
• Our ambition is to be the most child friendly borough in the country. We need to work in partnership and agree a set of principles.
• The voice of the Children & Young People (CYP) is at the heart of what we do.
• To deliver a partnership will involve joint commissioning, performance management and responsibility & accountability.
Dr Suckling joined the meeting at this point. Dr Barbour acknowledged that it will be challenging to join plans together to support the most vulnerable Children and Young People in the Borough however hoped that partners will work collaboratively to improve the plan and make it more integrated in the future and ensure opportunities are available for children to make the best of their talents. Mrs Whittle queried why the plan had not yet been presented to the Governing Body despite being agreed at the Cabinet in March 2017 and commented that those Children & Young People who had Special Educational Needs, who access Child Adolescent and Mental Health Services (CAMHS) and Looked after Children should be included within the plan. Mr Golze stated that although this cohort of children may not be explicitly referenced in the overarching strategic plan, work will still be undertaken to address their needs.
6
Mrs Pederson highlighted that the plan was further developed than those in other areas and more collective for Doncaster. There will be bold steps to take on integrated commissioning. Dr Crichton thanked Mr Golze for attending the Governing Body meeting.
8. Outcome of the consultations on the Hyper Acute Stroke Unit and Children’s Surgery & Anaesthesia Mr Goodall attended the Governing Body meeting to inform Members of the outcome of the public consultations on Hyper Acute Stroke Unit Services and Children’s Surgery & Anaesthesia. In 2016, Commissioners Working Together (CWT) carried out a review of Children’s Surgery and Anaesthesia services and Hyper Acute Stroke services across the region. Pre-consultation engagement took place between January and April 2016 as part of this review, during which CWT gathered the views of key stakeholders, including patients and the public, to inform plans for the future of services. Following this engagement, CWT proposed changes for both Children’s Surgery and Anaesthesia and Hyper Acute Stroke services that aim to use what is available in the best possible way to get the best services for everyone. For Children’s Surgery and Anaesthesia, three options have been developed and put forward for consideration, including CWT’s preferred option. For Hyper Acute Stroke services, one option has been developed and put forward for consideration. The consultation to get the views of patients, public and others with an interest in these issues was launched on 3rd October 2016 and ran until 14th February 2017. The original closing date for the consultation of 20th January 2017 was extended to take account of the Christmas period and to allow as many people as possible to take part in the consultation. The consultation process The following channels were provided for people to respond to each of the consultations throughout the consultation period:
• Online consultation questionnaire hosted on the Commissioners Working Together website http://www.smybndccgs.nhs.uk. The survey included some closed questions to measure levels of support around the service options proposed and a number of open questions around the proposals to allow respondents to express views in their own words. Information about demographics and the context in which people were responding to the consultation were also asked for sub-group analysis.
• Paper surveys were also available which contained the same questions as the online survey with a freepost return option. There
7
were no requests for translation into additional languages. Easy Read versions of the survey were also available.
• Meetings and events – A number of public events, stakeholder meetings, staff meetings and discussion groups were held during the consultation period.
• Submissions in the form of letters and petitions could be submitted to the consultation by post or by email.
• Representative telephone survey – A telephone survey of 740 local residents, broadly representative by geography and demographics, was conducted across South and Mid Yorkshire, Bassetlaw and North Derbyshire.
• Online poll – A short poll was devised at the mid-point stage (following analysis that the narrative was complex and it was difficult to engage people on the issues). The results do not inform the main survey analysis and are simply intended to provide further data on people’s opinions.
Communications and engagement activity Commissioners Working Together (CWT), each of the CCGs and provider organisations developed tailored communications and engagement plans for the consultations in their local areas. North Derbyshire CCG and Hardwick CCG agreed to conduct joint engagement activities. Children’s Surgery and Anaesthesia services Respondents were asked whether they agreed or disagreed with the proposal to change the way Children’s Surgery and Anaesthesia services and were asked to explain the reasons behind their expressed view. Respondents tended to agree with the proposed changes (63% of telephone survey respondents agree and 43% of self-selecting survey respondents agree). However, there are over a third of self-selecting respondents (39%) who disagree with the proposals compared to 13% of randomly selected telephone survey respondents. Hyper Acute Stroke Services Respondents were asked whether they agreed or disagreed with the three centre option to change the way Hyper Acute Stroke services were provided. There is a mixed response to this question; 54% of self-selecting consultation survey respondents disagrees with this option and 50% of telephone survey responses agree with it. As with all public consultations, the response cannot be seen as representative of the population but it is representative of interested parties who were made aware of the consultation and were motivated to respond. Within the analysis we cannot be clear the extent to which responses are informed by the supporting information that has been provided. The telephone survey was undertaken with a randomly selected and representative cross-section of residents to ensure that
8
the consultation process accurately captured the views of the wider population of South and Mid Yorkshire, Bassetlaw and North Derbyshire. The members of the Joint Committee of CCGs will review the evidence and considerations that have emerged during consultation while also taking account of all the other relevant evidence that will help them make their final decisions. The independent analysis is being shared with relevant steering groups, the Joint Overview and Scrutiny Committee and will also be widely available to the public, staff and stakeholders on the CWT website. The Joint Committee of CCGs will be asked to consider the independent analysis in advance of the Business Case. Mr Goodall requested that the Governing Body note the update. Dr Tupper queried if there was any rationale of how the consultation had influenced change and the direction of travel, if there was any feedback in respect of cost and what was learned regarding future public consultation and engagement sessions. Mr Goodall stated that he was unsure of the cost and would need to clarify this with Commissioners Working Together Team. Low attendance was noted at the consultation sessions and the Commissioners Working Together Team is exploring options of how this may be improved in the future. Mrs Pederson commented that the consultation sessions are resource intensive and that future consultations will be focused on the broader plans rather than individual areas. The Governing Body noted the update on the Outcome of the consultations on the Hyper Acute Stroke Unit and Children’s Surgery & Anaesthesia
Mr Goodall
9. Quality & Performance Report Mr Russell and Mr Fitzgerald stated that the Quality and Performance Report was for noting by the Governing Body however wished to highlight the following points: Doncaster and Bassetlaw Teaching Hospitals NHS Foundation Trust (DBTHFT)
• 18 week Referral to Treatment Times - The position for incomplete pathways in February improved slightly to 90.5% in line with the trajectory but remained below standard (92% of patients waiting under 18 weeks).
• There was a 52 week wait reported for February. This patient was treated in March.
• March 2017 A&E performance improved to 92.7% against the agreed aim of 90%, but remained below the national standard of 95%. The 5 Year Forward View details increased focus on achieving target in A&E. the Trust has committed to attaining a 95% target by March 2018 and this has been documented within contracts.
9
• Handovers over 60 minutes deteriorated to 66 during January 2017.
• Two cancer standards were not met during January 2017, 2 week wait from referral to date first seen: all urgent cancer referrals and 62 day wait for first treatment from NHS cancer screening service referral.
• The number of hospital acquired Clostridium Difficile cases, pressure ulcers and falls has reduced significantly during the last year.
Rotherham, Doncaster & South Humber NHS Foundation Trust (RDASH)
• The Improving Access to Psychological Therapies (IAPT) Recovery Rate achieved target at 56.2% for the 7th consecutive month during February 2017.
Mr Russell informed the Governing Body that the national survey regarding Care Quality Commission (CQC) performance data has been published and it has been noted that Doncaster has performed well with a 20% reduction in Care Homes ‘requiring improvement’. This is attributed to the significant amount of work which has been undertaken in partnership with our care homes. Mr Fitzgerald informed the Governing Body that the May report will include the performance Dashboard with a spotlight report on the Primary Care and Planned Care Delivery Plans. Dr Jones raised the continuing issues relating to delayed admissions to the Stroke Unit and Dr Tupper highlighted that there are issues relating to late diagnosis of stroke. Mr Russell reported that a ‘walk through’ of the Stroke Unit has been undertaken. The outcome for Doncaster patients is good with patients also receiving a level of care in Outreach however he would discuss this further with the Trust.
Spotlight Report on Cancer 62 day wait Dr Pieri and Mrs Coggan gave a presentation on the Cancer 62 day waits and highlighted the following points:
• Incidence of Cancer in Doncaster is higher than the national average, and has been increasing. One Year Survival has improved each year, and under 75 mortality, whilst above the national average, has also reduced over time.
• Over 10,000 2week wait referrals have been made each year for Doncaster patients since 2014/15, and over 1800 patients had a first treatment in 2015/16. 2 week wait referrals including Breast Symptomatic increased up to 2015/16, however they have reduced by 108 in 2016/17 compared to the same period last year. First treatments have also reduced in 2016/17 compared to the same period last year by 188, and are 46 lower than 2014/15 and 26 lower than 2013/14.
• NHS Doncaster CCG’s 62 day performance has not met the standard since Quarter 3 2013/14 and is currently below the England average performance. However Doncaster patients treated
Mr Russell
10
by DBTHFT have met the 62 day standard every quarter back to Quarter 1 2015/16. Doncaster patients treated by Sheffield Teaching Hospital Foundation Trust (STHFT) are not treated within the standard, and this has deteriorated.
• Analysis of breaches shows the largest reported reason was due to referrals for treatment being made late in the pathway from DBTHFT to STHFT (63 patients (53% of breaches) year to date). To improve this, the South Yorkshire & Bassetlaw Cancer Alliance is in the process of agreeing an Inter Provider Transfer Policy. The policy sets out the process and content of a referral to the tertiary centre. This aims to clarify what work is needed for each tumour group in the referring Trust, to make the referral more streamlined and efficient, and by what day in the pathway the referral will be made. It is supplemented with new national breach allocation guidance which better incentivises both the referring and treating provider to ensure the patient is treated within 62 days. The policy is expected tobe signed off by Medical Directors.
• More detailed breach analysis has identified that delays within DBTHFT mainly relate to first outpatient appointment and diagnostic waits.
• When looking at specific tumour groups, Doncaster patients with Breast, Gynaecological, Skin, Upper Gastro-Intestinal and other tumour groups are being treated within the standard. Patients with the following tumour groups are the lowest proportion treated in 62 days Quarters 1-3 2016/17 - Head and Neck, Lung, Urology and Lower Gastro-IntestinaI.
• Issues within the tumour groups with the longest waits include: o Head & Neck - Late referrals to Tertiary Provider due to pathway
delays. Complex treatment pathways due to nature of tumour site.
o Lung – Waiting times for Endo-bronchial ultrasounds at STHFT. Waiting times for Positron Emission Tomography (PET) scans and complexity of diagnosis.
o Urology - MRI demand versus capacity available, outpatient and Elective capacity at both DBTHFT and STHFT.
o Lower Gastro-Intestinal - Delays for Endoscopy and Histology.
• A large number of actions have already been undertaken to improve the timeliness of pathways and will be monitored continuously.
• DBTHFT is currently developing a business case for a new scanner. Mrs Pederson commented that the presentation was very helpful. As an exemplar, there may be changes going forward and a move to commissioning for outcomes in the future. Dr Jones acknowledged the move to a commissioning for outcomes model and asked what levers we may apply. Mrs Pederson stated that as an exemplar there will be more flexibility on payment mechanisms. Dr Barbour queried if there are financial penalties applied if targets have not been met and if they have been enacted. Mrs Coggan explained that the contract is quite complex and penalties have been on hold as a result of the Sustainability & Transformation Plan. Dr Barbour asked if there may be capacity within the private sector.
11
Mrs Coggan reported that there are a range of potential options. Dr Crichton reported that conversations are being held in respect of support for current services and establishing the correct skill mix of staff. The Cancer Detection Trust continues to raise funds for the necessary equipment. Mrs Sherburn reported that notification has been received that urgent bids are being requested by Friday 19th April 2017, for capital in respect of estates and DBTHFT has submitted a bid for a scanner. Dr Crichton thanked Dr Pieri and Mrs Coggan.
10. Finance Report Mrs Tingle reported that the Finance Report which provided an update on the financial position for February 2017 was for noting by the Governing Body. NHS Doncaster CCG is forecasting to achieve all of its financial targets for 2016/17. The year to date position reflects a surplus of £7,107k which is consistent with the year to date target of £7,079k. The annual target is a surplus of £7,722 which the CCG is forecasting to achieve. Mrs Tingle informed the Governing Body that the next report will be the Annual Accounts. Dr Bradley queried if there was any information relating to Category M drugs. Mrs Tingle reported that a saving of £1m is as a result of price reductions and a £2.4m achievement on efficiency savings is due to national savings on other drugs. Mrs Pederson highlighted the hard work of the Finance Team throughout the year and extended her thanks to the team. The Governing Body noted the report.
11. Assurance Framework Report Quarter 4 and 2017/2018 starting position Governing Body Assurance Framework Refresh 2017/18 Mrs Atkins Whatley explained that, alongside the last Quarter’s Assurance Framework update, Members noted the formal feedback report from a Governing Body Assurance Framework Timeout session run by our Internal Auditors, which resulted in revised corporate objectives against which the Governing Body Assurance Framework is mapped, and a list of current and emerging strategic risks to the achievement of these objectives. A new template recommended by our Internal Auditors has been developed, populated with the risks identified at the Timeout. Existing risks being treated at year-end on our old Assurance Framework have been mapped across to the new Assurance Framework. In summary, the risks are:
12
CO 1 - Ensure an effective, well led, and well governed organisation.
• 1.1 Organisational change: If we do we not have the right skill mix and resource within the organisation, supported by our Organisational Development Strategy, we may not achieve both our local commissioning strategy and our wider collaborative commissioning commitments.
CO 2- Commission high quality, continually improving, cost effective healthcare which meets the needs of the Doncaster population.
• 2.1 Quality impact: Financial resource reductions could potentially affect our ability to commission for continually improving quality.
• 2.2. Urgent Care: If we fail to commission effective, resilient and sustainable urgent & emergency care services, the quality of care delivered to patients and the achievement of associated quality and performance targets could be adversely affected.
• 2.3 Primary Care: If we fail to commission effective, resilient and sustainable primary medical care services, the quality of care delivered to patients and the achievement of associated quality and performance targets could be adversely affected, and the full vision contained within the Place Plan could potentially be adversely affected.
• 2.4 Provider Workforce: Providers in Doncaster may not have access to a sufficiently skilled workforce to meet the outcomes identified in our commissioning intentions.
CO 3 - Ensure that the healthcare system in Doncaster is sustainable.
• 3.1 Transformation: If our transformation delivery plans are not sufficiently ambitious to respond to the expected growth in activity and reduction in financial allocation, we could fail to deliver the efficiency savings required to maintain financial balance across the local health system.
• 3.2 Efficiencies: If we do not maximise efficiency opportunities presented by areas such as Prescribing and RightCare, we may be forced to consider decommissioning services from elsewhere in order to achieve the required savings.
• 3.3. System affordability: If the overall Doncaster healthcare system is not affordable given the impact of external controls on CCG allocations leading to increasingly limited financial resource, this may require the CCG to undertake greater prioritisation of resource to meet the identified needs of our population.
• 3.4. Control total: If we do not meet our CCG control total due to the impact of external controls on CCG allocations and/or the impact of unpredicted in-year cost pressures, then we will be in breach of our statutory duties to commission efficiently, effectively and to achieve value for money, and we may not be able to commission all the services which we have identified that our population needs.
CO 4 - Work collaboratively with partners to improve health and reduce inequalities in well governed and accountable
13
partnerships.
• 4.1 Dual partnership focus: We have dual areas of partnership commissioning focus - our local focus on Doncaster as a place delivering the ambition described in the Doncaster Place Plan, and our collaborative commissioning commitments within areas such as the South Yorkshire & Bassetlaw Sustainability & Transformation Plan. If these dual areas of focus dilute our local system leadership as CCG as resource is aligned both locally and across a wider collaborative footprint, this could potentially impact upon our organisational independence of decision making.
• 4.2 Engagement & prevention: If, across the Doncaster Place Plan footprint, we do not achieve cultural change away from a more dependant medicalised model of healthcare towards greater self-care, prevention, patient engagement & empowerment, and building on the existing strengths within communities, we may not deliver the vision contained within the Place Plan, or the efficiencies.
• 4.3 STP non-delivery: If the South Yorkshire & Bassetlaw Sustainability & Transformation Plan does not deliver the expected savings, greater savings will need to be identified at a Place level, and we may not be able to commission all the services which we have identified that our population needs.
Assurance Framework closing position – Quarter 4 In light of the above fundamental refresh of the Assurance Framework during Quarter 4, the existing format of the Assurance Framework has been refreshed at a relatively high level during the last Quarter and the position is presented for Governing Body approval as at quarter-end. The key updates to which attention is particularly drawn are detailed below.
• Health inequalities (Risk 1.3): changed from “treat” to “tolerate”.
• Efficiency programme (Risk 1.4): continues to be treated.
• Commissioning collaborations (Risk 4.4): continues to be treated.
• NHS Number in commissioning (Risk 5.5): closed. Mrs Atkins Whatley requested that the Governing Body consider and approve the year-end position of the 2016/17 Governing Body Assurance Framework and the 2017/18 starting position of the new Assurance Framework following the Governing Body timeout in January 2017. Dr Tupper and Mr Goodall commented that the new format was excellent and Mr Goodall queried if the documents were available to the public. Mrs Atkins Whatley confirmed that they are available on a quarterly basis within the Governing Body papers. The highest risks are included within the Annual Report. Dr Crichton asked if they could be available on the NHS Doncaster CCG website. Mrs Atkins Whatley agreed to include the documents within the Publication Scheme section on the website. Miss Morris queried if Internal Audit has had sight of the documents.
Mrs Atkins Whatley

14
Mrs Atkins Whatley stated that Mr Kevin Watkins of Internal Audit had undertaken a review on the basis of the recommendations from the Time Out session. Dr Jones enquired if the Governing Body will receive an all in one Executive Summary. It was confirmed that this is the case. Dr Suckling highlighted that most risks were closely controlled and queried if this was reflected in the every-day challenging environment. Mrs Pederson stated that the risks are viewed by the Executive Team. We are taking a more pragmatic but optimistic view for 2017/2018 The Governing Body considered and approved the year-end position of the 2016/17 Governing Body Assurance Framework and the 2017/18 starting position of the new Assurance Framework.
12. Chair and Chief Officer Report Mrs Pederson stated that the joint report was for noting by the Governing Body however wished to highlight the following: NHS Doncaster CCG Stakeholder Survey Report 2017 – Analysis - NHS Doncaster Clinical Commissioning Group (CCG) needs to have strong relationships with a range of health and care partners in order to be successful as commissioners within the local system. Our relationships provide us with ongoing information, advice and knowledge to help us make the best possible commissioning decisions. The CCG 360o Stakeholder Survey is a key part of ensuring these strong relationships are in place. NHS England commissioned Ipsos Mori to conduct the 2017 CCG 360o Stakeholder Survey. The survey allows stakeholders to provide feedback on working relationships with CCGs. Our overall response rate to the survey in 2017 was 57%, which is a 10% improvement in our response rate from 2016. The average response rate across all CCGs within the survey was 62%. We had a better than national average response rate from all stakeholders with the exception of our Member Practices and wider stakeholders, although a significant improvement in response rate from our Member Practices compared to 2016. The full nationally-produced outcome report from the survey is available on our website. NHS England Assurance Review – Quarter 4 - On 12th April 2017 we had our Annual Assurance Review with NHS England. With representation from our Senior Management Team and Chair, key areas discussed were:
• CCG key achievements and issues from 2016/17
• Operational and financial plans for 2017/18: formal sign-off / identification of key issues
• CCG Place Based Strategy
• Wider Sustainability & Transformation Plan implementation
15
The outcome letter from NHS England will be presented to the Governing Body when received. Constitutional change proposal – The Phoenix Practice - The Phoenix Practice has made a formal request to NHS Doncaster CCG for them as a Member Practice to move from the South East Locality to the Central Locality. The rationale given is due to the geographic patient base (for the purposes of commissioning) and also with a view to the future emerging local NHS landscape in Doncaster. The process for consideration of this change is detailed below: a) Consult the Locality which the Practice is wishing to leave to
ascertain if they have any objections to the Practice leaving the Locality (via Practice Representatives at the Locality meeting).
b) Consult the Locality which the Practice is wishing to join to ascertain if they have any objections to the Practice joining the Locality (via Practice Representatives at the Locality meeting).
c) Present the change to the Governing Body for approval (within the April 2017 Chair & Chief Officer Report).
d) Consult the Membership to ascertain if they have any objections to the change (via the established process as this will require a Constitutional change).
e) Submit the Constitutional change request to NHS England. The South East and Central Localities have been consulted during early April 2017 on the proposed change, and have supported the change. Governing Body members are asked to consider this Constitutional change request and recommend the change to our Member Practices. The Governing Body considered the Constitutional change request and recommended the change to our Member Practices. Information Governance Toolkit - On 27th March 2017 we published our 2016/17 Information Governance (IG) Toolkit. We attained an overall IG Toolkit score of 77%, improving on the score achieved for 2015/16 by 1%. The IG Toolkit scores result in one of 2 outcomes – “satisfactory” or “unsatisfactory”. Our score of 77% with a minimum score of 2 across all the standards means that our Toolkit outcome is “satisfactory”. The Toolkit was also subject to Internal Audit review in the last Quarter, which resulted in an outcome of significant assurance. The Governing Body noted the report.
13. Locality Feedback Locality Leads gave the following feedback from their Locality meetings:
16
North East Locality – Dr Bradley reported the following items were discussed:
• Mrs Sam Butcher attended the meeting to discuss Rapid Response.
• A prescribing update was given.
• The opportunities available in respect of Care Navigator training. South East Locality – Dr Barbour reported the following items were discussed:
• Rapid Response.
• GP Matrix and GPFind website.
• 2 week wait electronic referrals.
• The destruction of hard copies of medical records. Dr Barbour reported that this had been discussed at the Primary Care Commissioning Committee meeting on 13th March 2017 where it was agreed that the medical records could be scanned electronically onto the system then destroyed. The Lloyd George envelope however would be retained.
• The Phoenix Practice request to move Localities. South West Locality – Dr Wagstaff reported that the following items were discussed:
• Rapid Response.
• Tier 2 provision.
• Savings to be made in respect of Pregablin prescribing.
• Mrs Zara Head attended to discuss the Issues Log and improvements in feedback.
• National Reporting Learning System (NRLS). North West Locality – Dr Seddon reported that the following items were discussed:
• Mrs Sarah Atkins Whatley attended the meeting to give feedback from the CCG particularly Primary Care.
• The Locality discussed the role and job description of the Pharmacists in the Medicines Management Team. There have been capacity issues within the team due to sickness absence. Mr Russell stated that, if the situation continues, then resource will need to be shared equally however it will be limited.
Central Locality – Dr Tupper reported that the following items were discussed:
• Intermediate Care and Rapid Response.
• Electronic referrals.
• Meaningful feedback from the Issues Log. The Governing Body noted the feedback.
14. Receipt of Minutes The following minutes were received and noted by the Governing
17
Body:
• Engagement & Experience Committee – Minutes from the meetings held on 2 February and 2 March 2017.
• Executive Committee – Minutes from the meeting held on 1 March 2017.
• Working Together Joint Committee of CCGs – Minutes from the meeting held on 21 February 2017.
• Working Together Joint Committee of CCGs Terms of Reference.
• South Yorkshire & Bassetlaw Sustainability and transformation Plan Collaborative Partnership Board – Minutes from the meetings held on 13 January and 17 March 2017.
Mrs Pederson informed the Governing Body that there had been an amendment to the Working Together Joint Committee of CCGs Terms of Reference to reflect that Hardwick CCG will now be included within the Derbyshire footprint. The Governing Body noted this change.
15. Any Other Business Dr Crichton informed the Governing Body that Dr Singh had been awarded a Fellowship from the Royal College of General Practitioners and congratulated Dr Singh on his achievement.
16. Date and Time of Next Meeting Thursday 18th May 2017 at 1:00pm.

18
Verbal
Item 6
Matters Arising

Enc B
Item 7
Quality & Performance Report

Meeting name Governing Body
Meeting date 18 May 2017
Title of paper
Quality & Performance Report
Executive / Clinical Lead(s)
Mr Andrew Russell, Chief Nurse Mr Anthony Fitzgerald, Chief of Strategy & Delivery
Author(s) Performance and Intelligence Team Quality Team
Purpose of Paper - Executive Summary
This report sets out the key quality and performance issues to be noted by the NHS Doncaster Clinical Commissioning Group (NHS Doncaster CCG) Governing Body on an exception basis. The performance rating, indicated by Red, Amber, Green or Blue status, denotes the current month performance and does not reflect the historic trends. The report structure has been updated from the May 2017 meeting of the Governing Body to the following sections: Section 1: Doncaster CCG Delivery Plan Highlights/Issues Section 2: Doncaster CCG NHS Constitution Indicator Performance Section 3: Provider Exception Report Within Section 1 the report includes a highlight and issue summary of all twelve Delivery Plans, plus a focus on two of the twelve CCG Delivery Plans in depth each month. The key areas of change, both positive and negative, to note since the last report are: NHS Doncaster Clinical Commissioning Group (CCG)
The Improvement and Assessment Framework quarterly dashboard from NHS England that was due to be published in April has been delayed and is now expected in June. Doncaster CCG’s quarter 4 checkpoint meeting with NHS England on 12 April 2017 was very positive
The two Delivery Plan focus areas this month are Primary Care and Planned Care. The Planned Care Delivery Plan update can be found on pages 6-9. The Primary Care Delivery Plan update can be found on pages 10-12.
90.93% of patients waiting on an 18 week Referral to Treatment pathway were waiting less than 18 weeks at the end of February 2017, which is a slight improvement from January.
98.66% of patients waiting for a diagnostic test were waiting less than 6 weeks at the end of February which is a slight improvement from January.
Two week wait cancer performance deteriorated in February to 86.43%, and failed for the second month running, however all 31 day treatment standards were met.
62 day referral to treatment performance for cancer improved in February, despite being below target, to 80% as did 62 day Screening to 87.5%.
People waiting 18 weeks or less from referral to treatment for IAPT missed target for the first time since September at 93%, as did the Recovery Rate, at 49.11%.
People starting treatment for Early in Intervention Psychosis within 2 weeks deteriorated in February 2017 but continues to meet target.
Doncaster & Bassetlaw Teaching Hospitals NHS Foundation Trust (DBTHFT)
There was one 52 week breach during March 2017 who is a Bassetlaw CCG patient.
A number of stroke indicators deteriorated in January.
62 day wait for first treatment from NHS cancer screening service referral increased during February and reached target at 90.0%
Rotherham, Doncaster & South Humber NHS Foundation Trust (RDASH)
Section 117 (adults) – performance slightly decreased to 92.1% in March 2017 (45 breaches) which is below the 95% target.
Recommendation(s)
The Governing Body is asked to:
Note the key quality performance areas for attention.
Impact analysis
Quality impact Positive quality impact from a consistent focus on quality outcomes.
Specific quality impact as identified in the report.
Equality impact
Neutral
Sustainability impact
Nil
Financial implications
As identified in the report.
Legal implications
Nil
Management of Conflicts of
Interest
The report is for information – no conflicts of interest identified. It should be noted that some Governing Body members may be
employed in secondary employment by organisations referenced in this report: please see Register of Interests for details.
Consultation / Engagement
(internal departments,
clinical, stakeholder & public/patient)
N/A
Report previously
presented at N/A
Risk analysis
Risks are captured in the Executive Summary.
Assurance Framework
2.1, 2.2, 2.3, 2.4, 3.1
Measures Actions
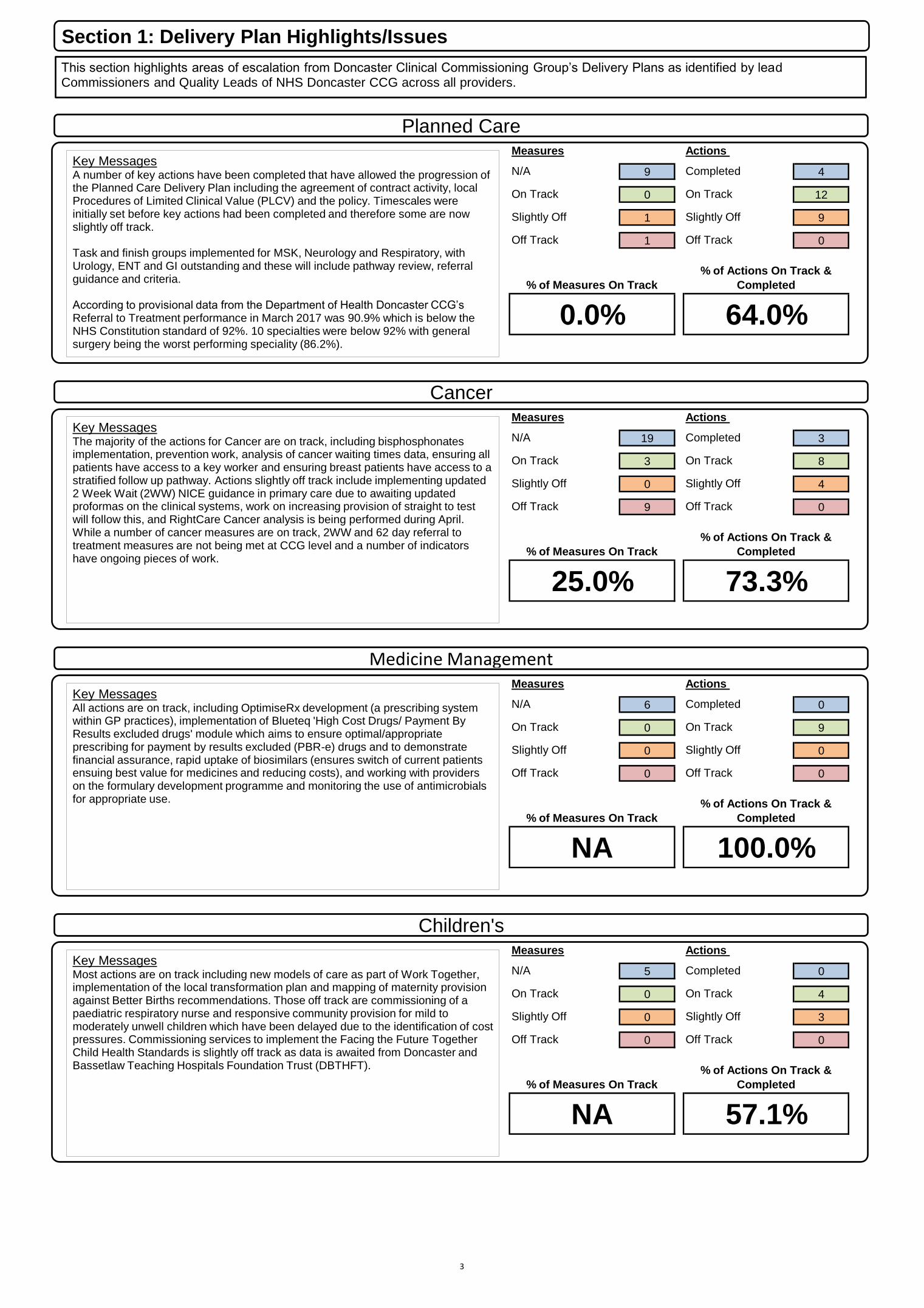
N/A 9 Completed 4
On Track 0 On Track 12
Slightly Off 1 Slightly Off 9
Off Track 1 Off Track 0
Measures Actions
N/A 19 Completed 3
On Track 3 On Track 8
Slightly Off 0 Slightly Off 4
Off Track 9 Off Track 0
Measures Actions
N/A 6 Completed 0
On Track 0 On Track 9
Slightly Off 0 Slightly Off 0
Off Track 0 Off Track 0
Measures Actions
N/A 5 Completed 0
On Track 0 On Track 4
Slightly Off 0 Slightly Off 3
Off Track 0 Off Track 0
% of Measures On Track
% of Actions On Track &
Completed
NA 57.1%
25.0% 73.3%
% of Measures On Track
% of Actions On Track &
Completed
NA 100.0%
0.0%
% of Measures On Track
% of Actions On Track &
Completed
% of Measures On Track
% of Actions On Track &
Completed
64.0%
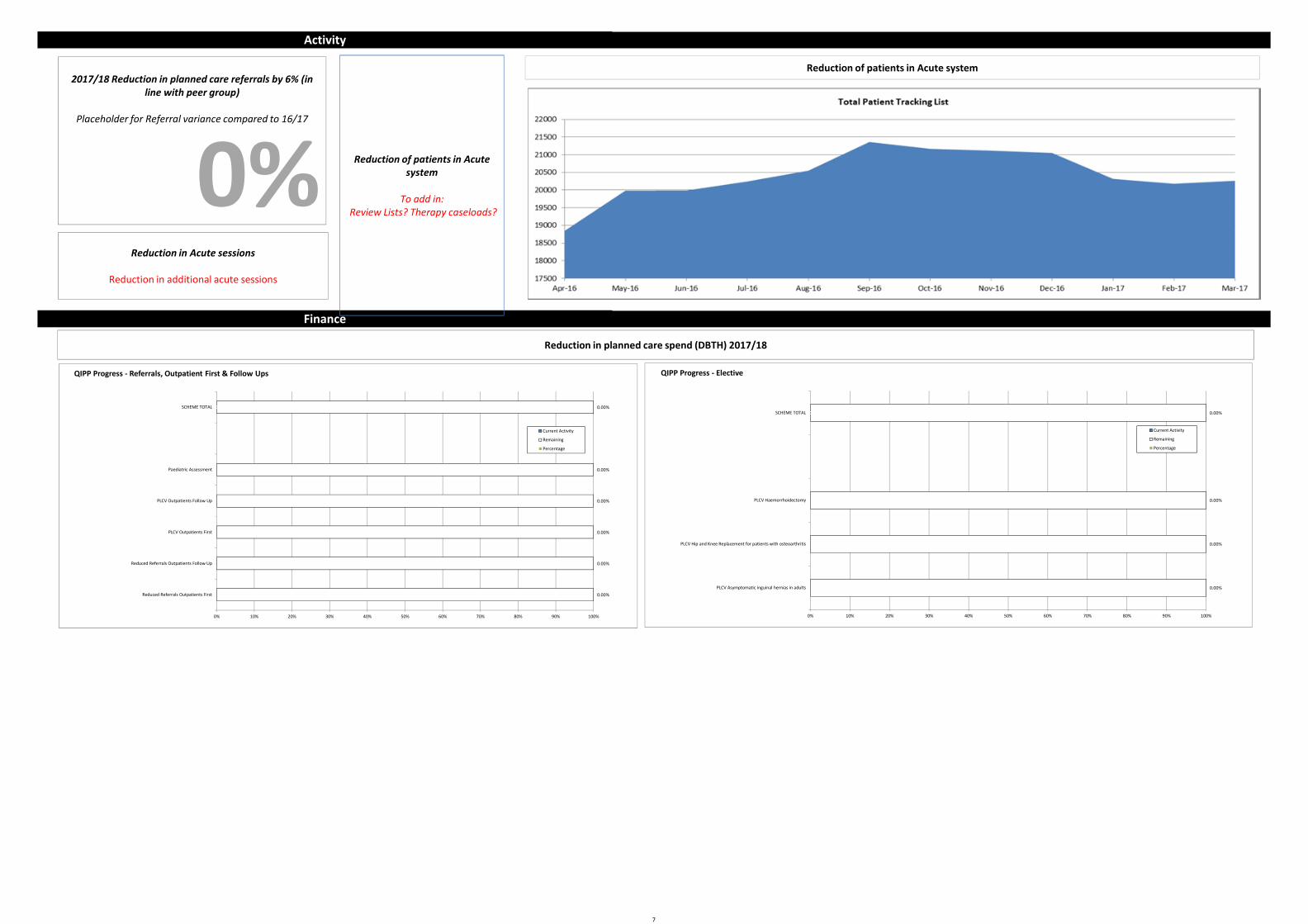
Planned Care
Key Messages A number of key actions have been completed that have allowed the progression of the Planned Care Delivery Plan including the agreement of contract activity, local Procedures of Limited Clinical Value (PLCV) and the policy. Timescales were initially set before key actions had been completed and therefore some are now slightly off track. Task and finish groups implemented for MSK, Neurology and Respiratory, with Urology, ENT and GI outstanding and these will include pathway review, referral guidance and criteria. According to provisional data from the Department of Health Doncaster CCG’s Referral to Treatment performance in March 2017 was 90.9% which is below the NHS Constitution standard of 92%. 10 specialties were below 92% with general surgery being the worst performing speciality (86.2%).
Section 1: Delivery Plan Highlights/Issues
Cancer
Key Messages The majority of the actions for Cancer are on track, including bisphosphonates implementation, prevention work, analysis of cancer waiting times data, ensuring all patients have access to a key worker and ensuring breast patients have access to a stratified follow up pathway. Actions slightly off track include implementing updated 2 Week Wait (2WW) NICE guidance in primary care due to awaiting updated proformas on the clinical systems, work on increasing provision of straight to test will follow this, and RightCare Cancer analysis is being performed during April. While a number of cancer measures are on track, 2WW and 62 day referral to treatment measures are not being met at CCG level and a number of indicators have ongoing pieces of work.
Medicine Management
Key Messages All actions are on track, including OptimiseRx development (a prescribing system within GP practices), implementation of Blueteq 'High Cost Drugs/ Payment By Results excluded drugs' module which aims to ensure optimal/appropriate prescribing for payment by results excluded (PBR-e) drugs and to demonstrate financial assurance, rapid uptake of biosimilars (ensures switch of current patients ensuing best value for medicines and reducing costs), and working with providers on the formulary development programme and monitoring the use of antimicrobials for appropriate use.
Children's
Key Messages Most actions are on track including new models of care as part of Work Together, implementation of the local transformation plan and mapping of maternity provision against Better Births recommendations. Those off track are commissioning of a paediatric respiratory nurse and responsive community provision for mild to moderately unwell children which have been delayed due to the identification of cost pressures. Commissioning services to implement the Facing the Future Together Child Health Standards is slightly off track as data is awaited from Doncaster and Bassetlaw Teaching Hospitals Foundation Trust (DBTHFT).
This section highlights areas of escalation from Doncaster Clinical Commissioning Group’s Delivery Plans as identified by lead Commissioners and Quality Leads of NHS Doncaster CCG across all providers.
3
Measures Actions
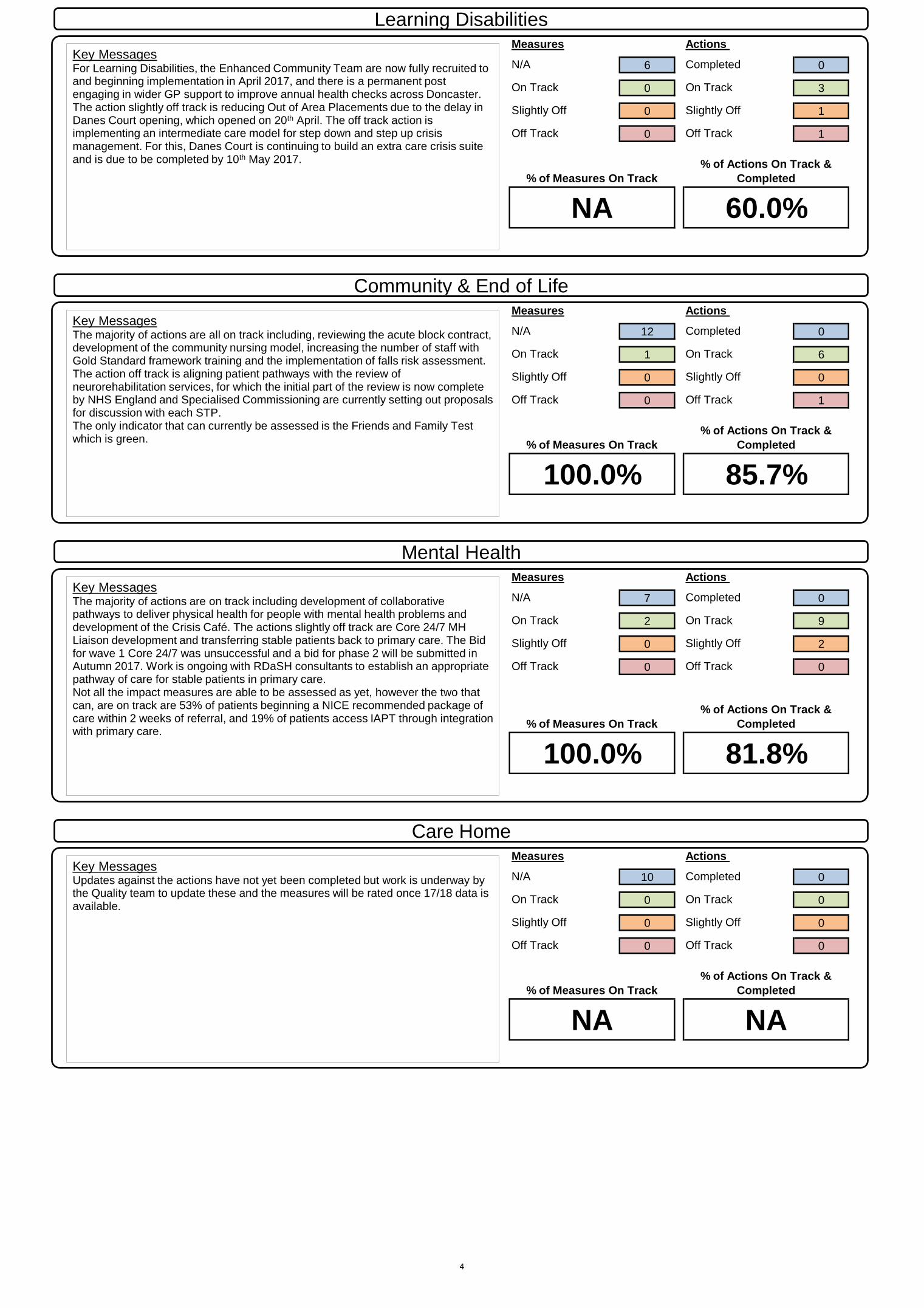
N/A 6 Completed 0
On Track 0 On Track 3
Slightly Off 0 Slightly Off 1
Off Track 0 Off Track 1
Measures Actions
N/A 12 Completed 0
On Track 1 On Track 6
Slightly Off 0 Slightly Off 0
Off Track 0 Off Track 1
Measures Actions
N/A 7 Completed 0
On Track 2 On Track 9
Slightly Off 0 Slightly Off 2
Off Track 0 Off Track 0
Measures Actions
N/A 10 Completed 0
On Track 0 On Track 0
Slightly Off 0 Slightly Off 0
Off Track 0 Off Track 0
NA NA
% of Measures On Track
% of Actions On Track &
Completed
100.0% 81.8%
% of Measures On Track
% of Actions On Track &
Completed
NA 60.0%
% of Measures On Track
% of Actions On Track &
Completed
100.0% 85.7%
% of Measures On Track
% of Actions On Track &
Completed
Learning Disabilities
Key Messages For Learning Disabilities, the Enhanced Community Team are now fully recruited to and beginning implementation in April 2017, and there is a permanent post engaging in wider GP support to improve annual health checks across Doncaster. The action slightly off track is reducing Out of Area Placements due to the delay in Danes Court opening, which opened on 20th April. The off track action is implementing an intermediate care model for step down and step up crisis management. For this, Danes Court is continuing to build an extra care crisis suite and is due to be completed by 10th May 2017.
Community & End of Life
Key Messages The majority of actions are all on track including, reviewing the acute block contract, development of the community nursing model, increasing the number of staff with Gold Standard framework training and the implementation of falls risk assessment. The action off track is aligning patient pathways with the review of neurorehabilitation services, for which the initial part of the review is now complete by NHS England and Specialised Commissioning are currently setting out proposals for discussion with each STP. The only indicator that can currently be assessed is the Friends and Family Test which is green.
Mental Health
Key Messages The majority of actions are on track including development of collaborative pathways to deliver physical health for people with mental health problems and development of the Crisis Café. The actions slightly off track are Core 24/7 MH Liaison development and transferring stable patients back to primary care. The Bid for wave 1 Core 24/7 was unsuccessful and a bid for phase 2 will be submitted in Autumn 2017. Work is ongoing with RDaSH consultants to establish an appropriate pathway of care for stable patients in primary care. Not all the impact measures are able to be assessed as yet, however the two that can, are on track are 53% of patients beginning a NICE recommended package of care within 2 weeks of referral, and 19% of patients access IAPT through integration with primary care.
Care Home
Key Messages Updates against the actions have not yet been completed but work is underway by the Quality team to update these and the measures will be rated once 17/18 data is available.
4
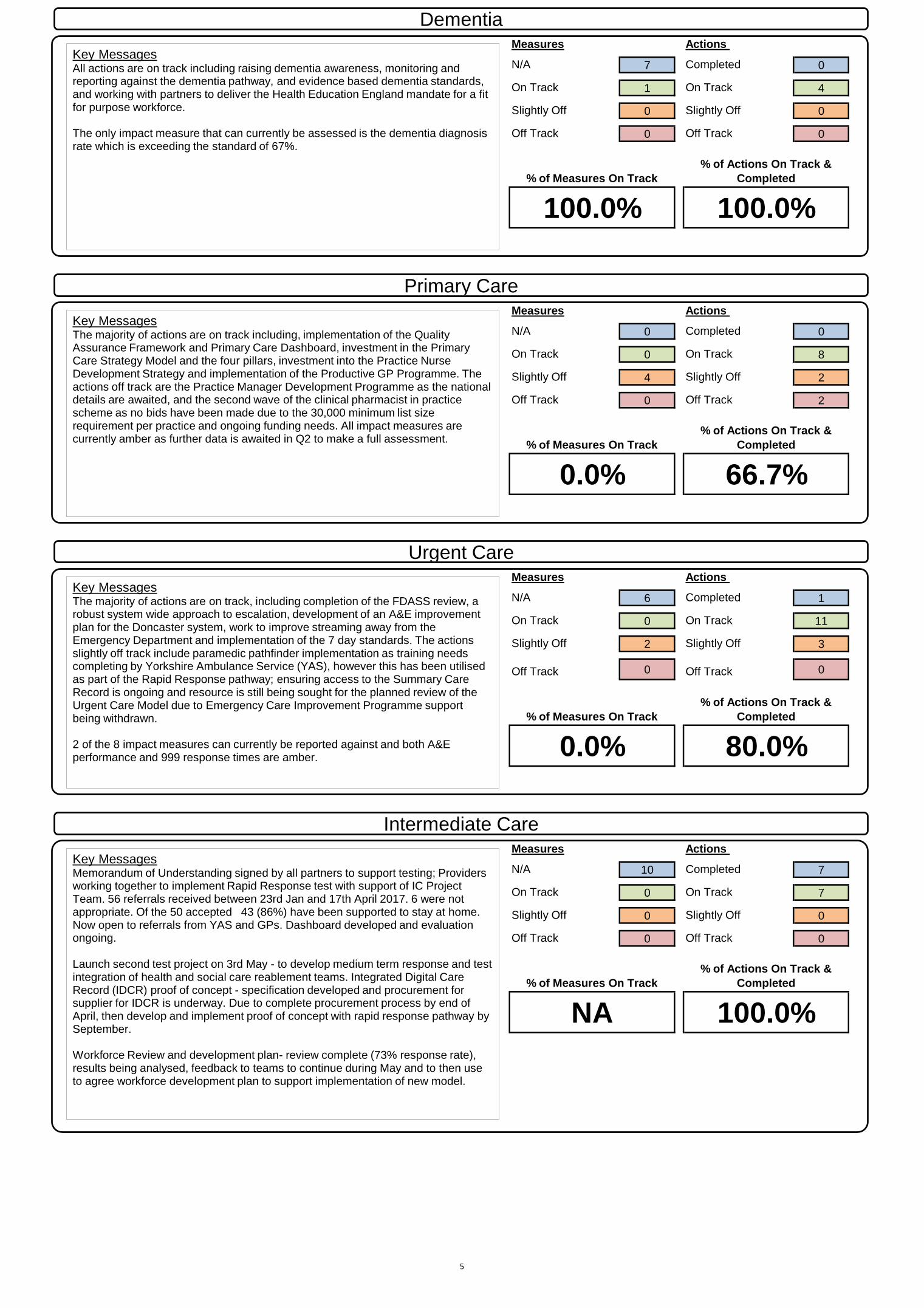
Measures Actions
N/A 7 Completed 0
On Track 1 On Track 4
Slightly Off 0 Slightly Off 0
Off Track 0 Off Track 0
Measures Actions
N/A 0 Completed 0
On Track 0 On Track 8
Slightly Off 4 Slightly Off 2
Off Track 0 Off Track 2
Measures Actions
N/A 6 Completed 1
On Track 0 On Track 11
Slightly Off 2 Slightly Off 3
Off Track 0 Off Track 0
Measures Actions
N/A 10 Completed 7
On Track 0 On Track 7
Slightly Off 0 Slightly Off 0
Off Track 0 Off Track 0
0.0% 80.0%
% of Measures On Track
% of Actions On Track &
Completed
NA 100.0%
% of Measures On Track
% of Actions On Track &
Completed
0.0% 66.7%
% of Measures On Track
% of Actions On Track &
Completed
% of Measures On Track
% of Actions On Track &
Completed
100.0% 100.0%
Dementia
Key Messages All actions are on track including raising dementia awareness, monitoring and reporting against the dementia pathway, and evidence based dementia standards, and working with partners to deliver the Health Education England mandate for a fit for purpose workforce. The only impact measure that can currently be assessed is the dementia diagnosis rate which is exceeding the standard of 67%.
Primary Care
Key Messages The majority of actions are on track including, implementation of the Quality Assurance Framework and Primary Care Dashboard, investment in the Primary Care Strategy Model and the four pillars, investment into the Practice Nurse Development Strategy and implementation of the Productive GP Programme. The actions off track are the Practice Manager Development Programme as the national details are awaited, and the second wave of the clinical pharmacist in practice scheme as no bids have been made due to the 30,000 minimum list size requirement per practice and ongoing funding needs. All impact measures are currently amber as further data is awaited in Q2 to make a full assessment.
Urgent Care
Key Messages The majority of actions are on track, including completion of the FDASS review, a robust system wide approach to escalation, development of an A&E improvement plan for the Doncaster system, work to improve streaming away from the Emergency Department and implementation of the 7 day standards. The actions slightly off track include paramedic pathfinder implementation as training needs completing by Yorkshire Ambulance Service (YAS), however this has been utilised as part of the Rapid Response pathway; ensuring access to the Summary Care Record is ongoing and resource is still being sought for the planned review of the Urgent Care Model due to Emergency Care Improvement Programme support being withdrawn. 2 of the 8 impact measures can currently be reported against and both A&E performance and 999 response times are amber.
Intermediate Care
Key Messages Memorandum of Understanding signed by all partners to support testing; Providers working together to implement Rapid Response test with support of IC Project Team. 56 referrals received between 23rd Jan and 17th April 2017. 6 were not appropriate. Of the 50 accepted 43 (86%) have been supported to stay at home. Now open to referrals from YAS and GPs. Dashboard developed and evaluation ongoing. Launch second test project on 3rd May - to develop medium term response and test integration of health and social care reablement teams. Integrated Digital Care Record (IDCR) proof of concept - specification developed and procurement for supplier for IDCR is underway. Due to complete procurement process by end of April, then develop and implement proof of concept with rapid response pathway by September. Workforce Review and development plan- review complete (73% response rate), results being analysed, feedback to teams to continue during May and to then use to agree workforce development plan to support implementation of new model.
5
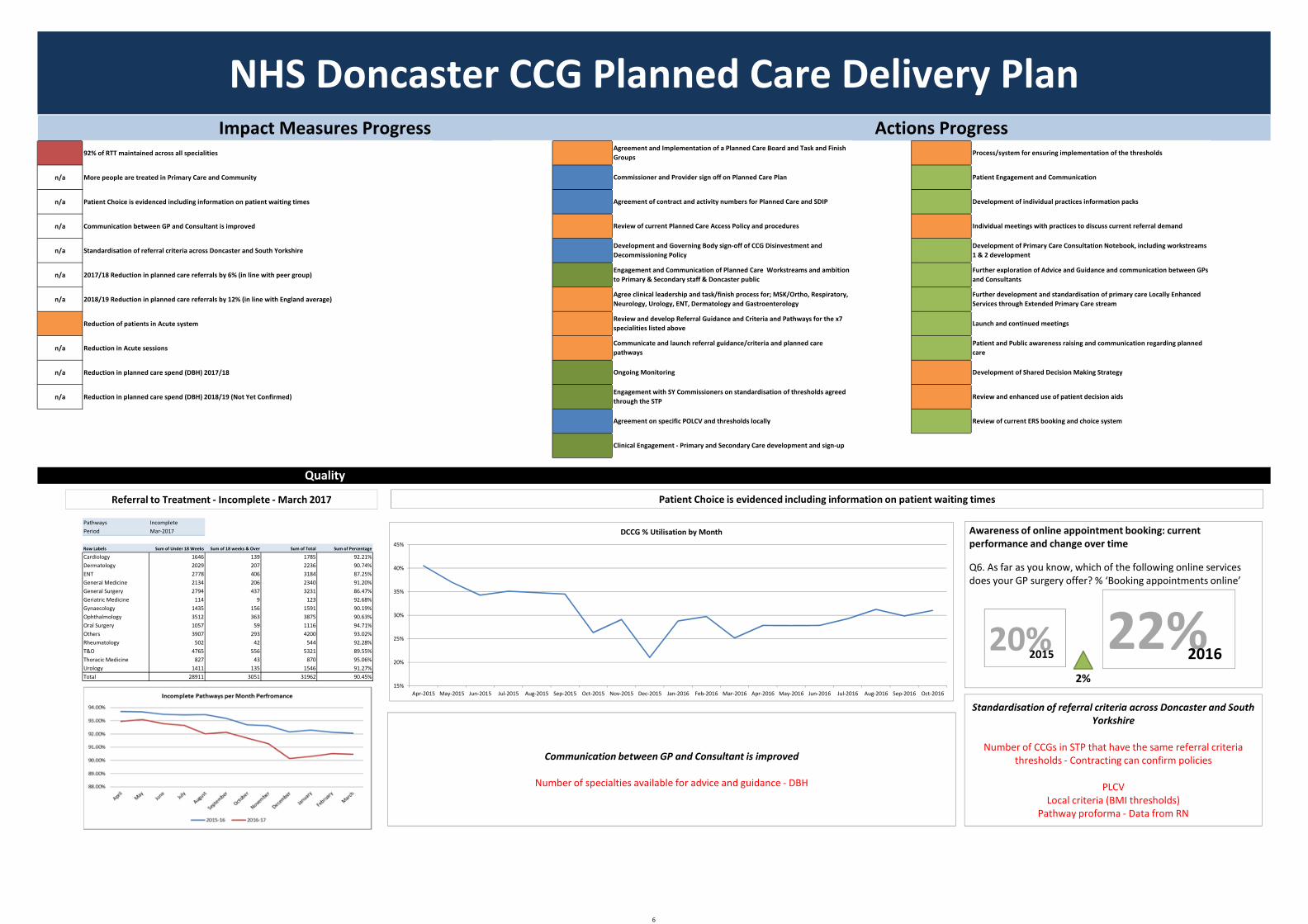
92% of RTT maintained across all specialities
n/a More people are treated in Primary Care and Community
n/a Patient Choice is evidenced including information on patient waiting times
n/a Communication between GP and Consultant is improved
n/a Standardisation of referral criteria across Doncaster and South Yorkshire
n/a 2017/18 Reduction in planned care referrals by 6% (in line with peer group)
n/a 2018/19 Reduction in planned care referrals by 12% (in line with England average)
Reduction of patients in Acute system
n/a Reduction in Acute sessions
n/a Reduction in planned care spend (DBH) 2017/18
n/a Reduction in planned care spend (DBH) 2018/19 (Not Yet Confirmed)
Pathways IncompletePeriod Mar‐2017
Row Labels Sum of Under 18 Weeks Sum of 18 weeks & Over Sum of Total Sum of Percentage
Cardiology 1646 139 1785 92.21%Dermatology 2029 207 2236 90.74%ENT 2778 406 3184 87.25%General Medicine 2134 206 2340 91.20%General Surgery 2794 437 3231 86.47%Geriatric Medicine 114 9 123 92.68%Gynaecology 1435 156 1591 90.19%Ophthalmology 3512 363 3875 90.63%Oral Surgery 1057 59 1116 94.71%Others 3907 293 4200 93.02%Rheumatology 502 42 544 92.28%T&O 4765 556 5321 89.55%Thoracic Medicine 827 43 870 95.06%Urology 1411 135 1546 91.27%Total 28911 3051 31962 90.45%
Agreement on specific POLCV and thresholds locally Review of current ERS booking and choice system
Clinical Engagement ‐ Primary and Secondary Care development and sign‐up
Engagement with SY Commissioners on standardisation of thresholds agreed through the STP
Review and enhanced use of patient decision aids
Development of Shared Decision Making Strategy
Process/system for ensuring implementation of the thresholds
Patient Engagement and Communication
Development of individual practices information packs
Individual meetings with practices to discuss current referral demand
Development of Primary Care Consultation Notebook, including workstreams 1 & 2 development
Agree clinical leadership and task/finish process for; MSK/Ortho, Respiratory, Neurology, Urology, ENT, Dermatology and Gastroenterology
Review and develop Referral Guidance and Criteria and Pathways for the x7 specialities listed above
Communicate and launch referral guidance/criteria and planned care pathways
Further exploration of Advice and Guidance and communication between GPs and Consultants
Further development and standardisation of primary care Locally Enhanced Services through Extended Primary Care stream
Launch and continued meetings
Patient and Public awareness raising and communication regarding planned care
NHS Doncaster CCG Planned Care Delivery Plan
Quality
Impact Measures Progress Actions ProgressAgreement and Implementation of a Planned Care Board and Task and Finish Groups
Commissioner and Provider sign off on Planned Care Plan
Agreement of contract and activity numbers for Planned Care and SDIP
Review of current Planned Care Access Policy and procedures
Ongoing Monitoring
Development and Governing Body sign‐off of CCG Disinvestment and Decommissioning Policy
Engagement and Communication of Planned Care Workstreams and ambition to Primary & Secondary staff & Doncaster public
Referral to Treatment ‐ Incomplete ‐March 2017 Patient Choice is evidenced including information on patient waiting times
Communication between GP and Consultant is improved
Number of specialties available for advice and guidance ‐ DBH
Standardisation of referral criteria across Doncaster and South Yorkshire
Number of CCGs in STP that have the same referral criteria thresholds ‐ Contracting can confirm policies
PLCVLocal criteria (BMI thresholds)
Pathway proforma ‐ Data from RN
15%
20%
25%
30%
35%
40%
45%
Apr‐2015 May‐2015 Jun‐2015 Jul‐2015 Aug‐2015 Sep‐2015 Oct‐2015 Nov‐2015 Dec‐2015 Jan‐2016 Feb‐2016 Mar‐2016 Apr‐2016 May‐2016 Jun‐2016 Jul‐2016 Aug‐2016 Sep‐2016 Oct‐2016
DCCG % Utilisation by Month Awareness of online appointment booking: current performance and change over time
Q6. As far as you know, which of the following online services does your GP surgery offer? % ‘Booking appointments online’
22%201620%2015
2%
6
Activity
Finance
Reduction in planned care spend (DBTH) 2017/18
2017/18 Reduction in planned care referrals by 6% (in line with peer group)
Placeholder for Referral variance compared to 16/17
Reduction in Acute sessions
Reduction in additional acute sessions
Reduction of patients in Acute system
0
0.00%
0.00%
0.00%
0.00%
0.00%
0.00%
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Reduced Referrals Outpatients First
Reduced Referrals Outpatients Follow Up
PLCV Outpatients First
PLCV Outpatients Follow Up
Paediatric Assessment
SCHEME TOTAL
QIPP Progress ‐ Referrals, Outpatient First & Follow Ups
Current Activity
Remaining
Percentage
0
0.00%
0.00%
0.00%
0.00%
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
PLCV Asymptomatic inguinal hernias in adults
PLCV Hip and Knee Replacement for patients with osteoarthritis
PLCV Haemorrhoidectomy
SCHEME TOTAL
QIPP Progress ‐ Elective
Current Activity
Remaining
Percentage
0% Reduction of patients in Acute system
To add in:Review Lists? Therapy caseloads?
7
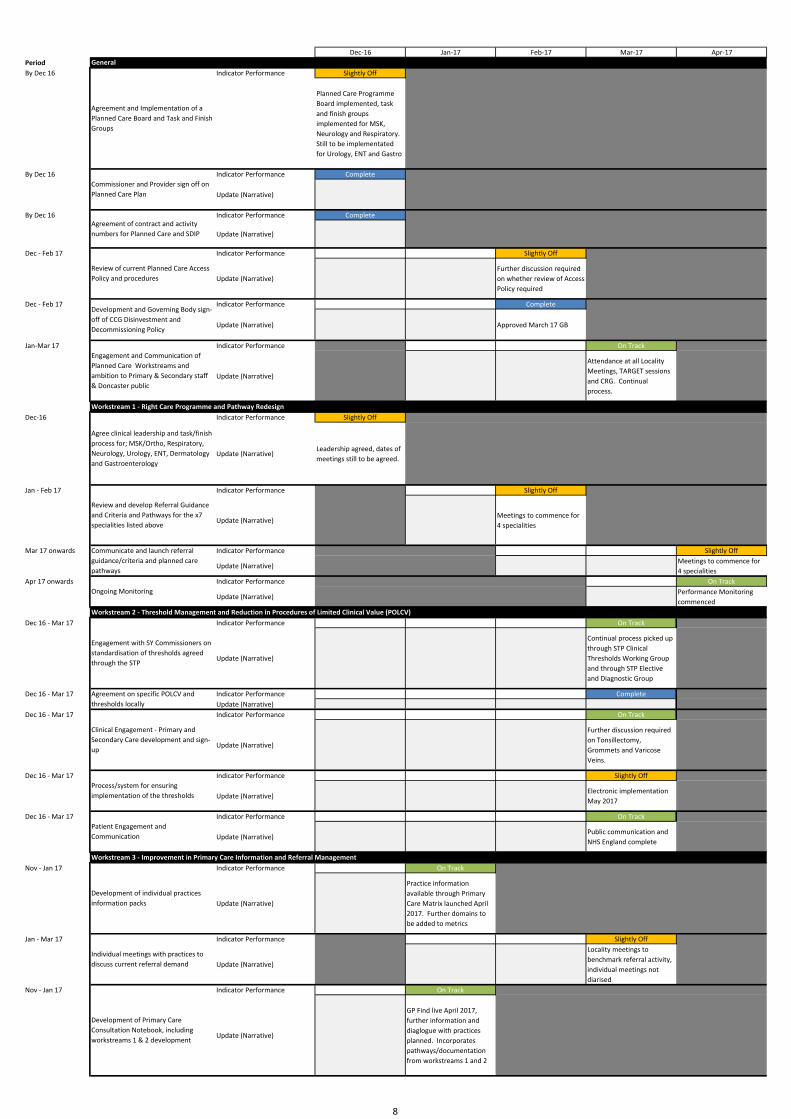
Dec‐16 Jan‐17 Feb‐17 Mar‐17 Apr‐17PeriodBy Dec 16 Indicator Performance Slightly Off
Planned Care Programme Board implemented, task and finish groups implemented for MSK, Neurology and Respiratory. Still to be implementated for Urology, ENT and Gastro
By Dec 16 Indicator Performance Complete
Update (Narrative)
By Dec 16 Indicator Performance Complete
Update (Narrative)
Dec ‐ Feb 17 Indicator Performance Slightly Off
Update (Narrative)Further discussion required on whether review of Access Policy required
Dec ‐ Feb 17 Indicator Performance Complete
Update (Narrative) Approved March 17 GB
Jan‐Mar 17 Indicator Performance On Track
Update (Narrative)
Attendance at all Locality Meetings, TARGET sessions and CRG. Continual process.
Dec‐16 Indicator Performance Slightly Off
Update (Narrative)Leadership agreed, dates of meetings still to be agreed.
Jan ‐ Feb 17 Indicator Performance Slightly Off
Update (Narrative)Meetings to commence for 4 specialities
Mar 17 onwards Indicator Performance Slightly Off
Update (Narrative)Meetings to commence for 4 specialities
Apr 17 onwards Indicator Performance On Track
Update (Narrative)Performance Monitoring commenced
Dec 16 ‐ Mar 17 Indicator Performance On Track
Update (Narrative)
Continual process picked up through STP Clinical Thresholds Working Group and through STP Elective and Diagnostic Group
Dec 16 ‐ Mar 17 Indicator Performance CompleteUpdate (Narrative)
Dec 16 ‐ Mar 17 Indicator Performance On Track
Update (Narrative)
Further discussion required on Tonsillectomy, Grommets and Varicose Veins.
Dec 16 ‐ Mar 17 Indicator Performance Slightly Off
Update (Narrative)Electronic implementation May 2017
Dec 16 ‐ Mar 17 Indicator Performance On Track
Update (Narrative)Public communication and NHS England complete
Nov ‐ Jan 17 Indicator Performance On Track
Update (Narrative)
Practice information available through Primary Care Matrix launched April 2017. Further domains to be added to metrics
Jan ‐ Mar 17 Indicator Performance Slightly Off
Update (Narrative)
Locality meetings to benchmark referral activity, individual meetings not diarised
Nov ‐ Jan 17 Indicator Performance On Track
Update (Narrative)
GP Find live April 2017, further information and diaglogue with practices planned. Incorporates pathways/documentation from workstreams 1 and 2
Engagement and Communication of Planned Care Workstreams and ambition to Primary & Secondary staff & Doncaster public
General
Workstream 1 ‐ Right Care Programme and Pathway Redesign
Agreement and Implementation of a Planned Care Board and Task and Finish Groups
Commissioner and Provider sign off on Planned Care Plan
Agreement of contract and activity numbers for Planned Care and SDIP
Review of current Planned Care Access Policy and procedures
Development and Governing Body sign‐off of CCG Disinvestment and Decommissioning Policy
Workstream 3 ‐ Improvement in Primary Care Information and Referral Management
Development of individual practices information packs
Development of Primary Care Consultation Notebook, including workstreams 1 & 2 development
Clinical Engagement ‐ Primary and Secondary Care development and sign‐up
Process/system for ensuring implementation of the thresholds
Patient Engagement and Communication
Individual meetings with practices to discuss current referral demand
Agree clinical leadership and task/finish process for; MSK/Ortho, Respiratory, Neurology, Urology, ENT, Dermatology and Gastroenterology
Review and develop Referral Guidance and Criteria and Pathways for the x7 specialities listed above
Communicate and launch referral guidance/criteria and planned care pathways
Ongoing Monitoring
Agreement on specific POLCV and thresholds locally
Workstream 2 ‐ Threshold Management and Reduction in Procedures of Limited Clinical Value (POLCV)
Engagement with SY Commissioners on standardisation of thresholds agreed through the STP
8
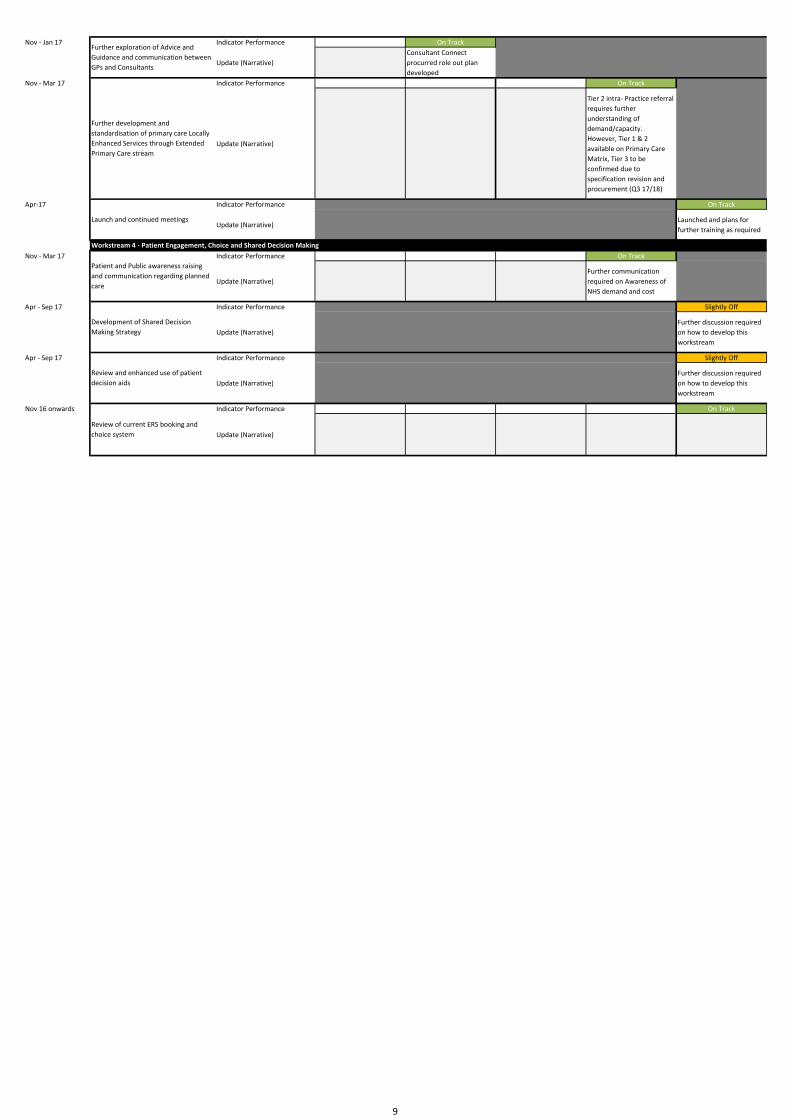
Nov ‐ Jan 17 Indicator Performance On Track
Update (Narrative)Consultant Connect procurred role out plan developed
Nov ‐ Mar 17 Indicator Performance On Track
Update (Narrative)
Tier 2 intra‐ Practice referral requires further understanding of demand/capacity. However, Tier 1 & 2 available on Primary Care Matrix, Tier 3 to be confirmed due to specification revision and procurement (Q3 17/18)
Apr‐17 Indicator Performance On Track
Update (Narrative)Launched and plans for further training as required
Nov ‐ Mar 17 Indicator Performance On Track
Update (Narrative)Further communication required on Awareness of NHS demand and cost
Apr ‐ Sep 17 Indicator Performance Slightly Off
Update (Narrative)Further discussion required on how to develop this workstream
Apr ‐ Sep 17 Indicator Performance Slightly Off
Update (Narrative)Further discussion required on how to develop this workstream
Nov 16 onwards Indicator Performance On Track
Update (Narrative)
Review of current ERS booking and choice system
Further exploration of Advice and Guidance and communication between GPs and Consultants
Further development and standardisation of primary care Locally Enhanced Services through Extended Primary Care stream
Launch and continued meetings
Development of Shared Decision Making Strategy
Review and enhanced use of patient decision aids
Workstream 4 ‐ Patient Engagement, Choice and Shared Decision Making
Patient and Public awareness raising and communication regarding planned care
9
On Track
On Track
On Track
On Track
Off Track
Off Track
On Track
On Track
On Track
On Track
Slightly Off Track
Slightly Off Track
Y Y Y Y N Y Y Y Y Y N Y Y Y Y Y N YY Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y YY Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y YY Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y YY Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y YY Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y YY Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y YY Y Y
Y Y Y Y N Y Y Y Y Y N Y Y Y Y Y N YY Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y YY Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y YY Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y YY Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y YY Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y YY Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y Y YY Y Y
Y Y Y Y N YY Y Y Y Y YY Y Y Y Y YY Y Y Y Y YY Y Y Y Y YY Y Y Y Y YY Y Y Y Y YY
9.07 ‐ Investment into the General Practice Nurse Development Strategy.
9.06 ‐ Second wave of the Clinical Pharmacist in Practice scheme.
C86002 ‐ The Ransome Practice
C86621 ‐ West End Clinic
C86029 ‐ St Vincent PracticeC86021 ‐ Whitehouse Farm Medical Centre
C86026 ‐ Dr Zaidi and PartnersC86020 ‐ St John’s Group PracticeC86014 ‐ Princess Medical CentreC86006 ‐ Regent Square Group Practice
C86623 ‐ Dr SheikhC86609 ‐ Auckley SurgeryC86034 ‐ The New Surgery
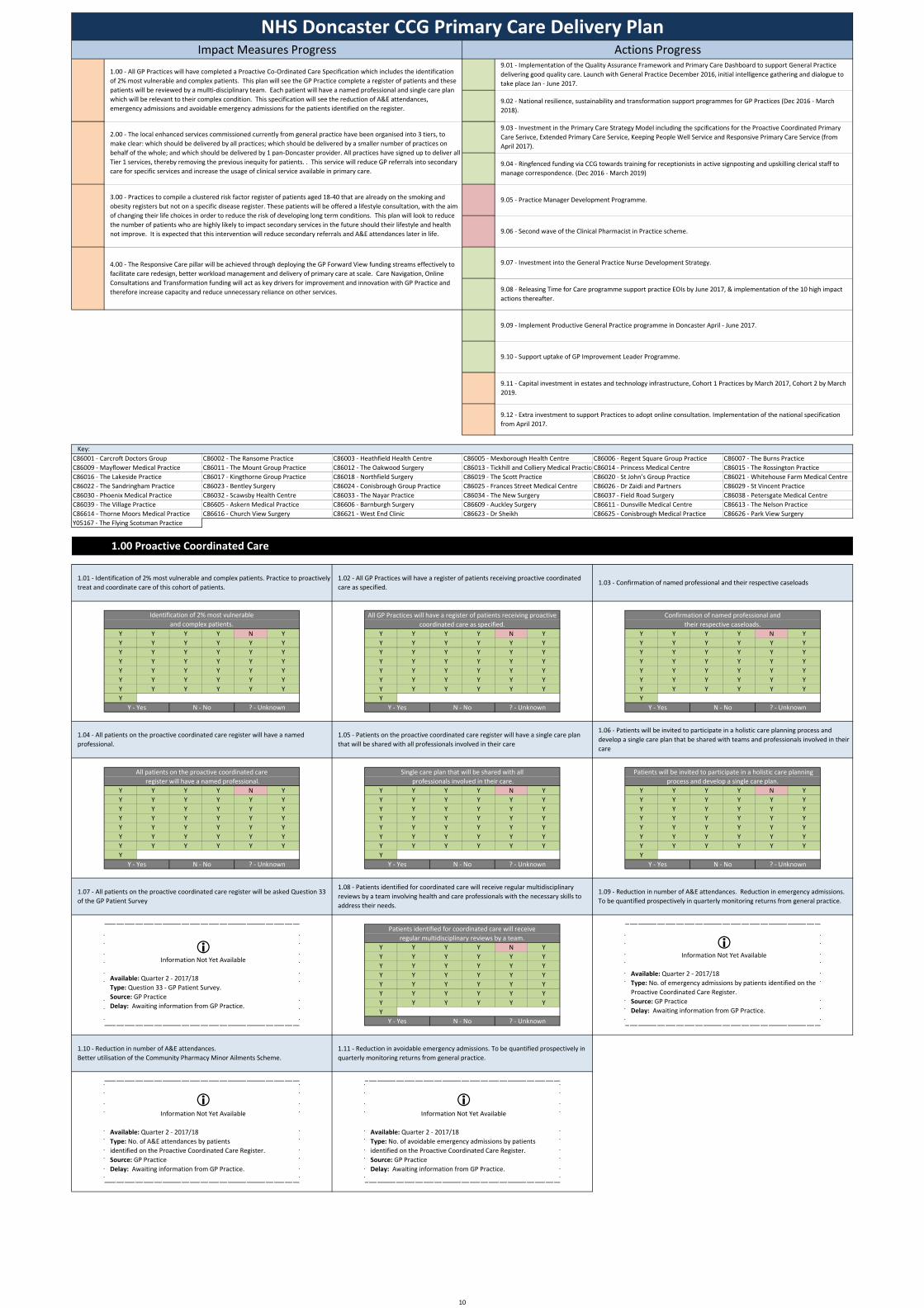
1.00 Proactive Coordinated Care
C86038 ‐ Petersgate Medical Centre
C86614 ‐ Thorne Moors Medical PracticeC86039 ‐ The Village Practice
C86625 ‐ Conisbrough Medical Practice
9.12 ‐ Extra investment to support Practices to adopt online consultation. Implementation of the national specification from April 2017.
9.11 ‐ Capital investment in estates and technology infrastructure, Cohort 1 Practices by March 2017, Cohort 2 by March 2019.
9.10 ‐ Support uptake of GP Improvement Leader Programme.
C86019 ‐ The Scott Practice
C86037 ‐ Field Road SurgeryC86030 ‐ Phoenix Medical PracticeC86022 ‐ The Sandringham Practice
C86616 ‐ Church View SurgeryC86605 ‐ Askern Medical Practice
C86013 ‐ Tickhill and Colliery Medical PracticeC86005 ‐ Mexborough Health Centre
C86626 ‐ Park View SurgeryC86613 ‐ The Nelson Practice
? ‐ Unknown
9.05 ‐ Practice Manager Development Programme.
9.04 ‐ Ringfenced funding via CCG towards training for receptionists in active signposting and upskilling clerical staff to manage correspondence. (Dec 2016 ‐ March 2019)
9.03 ‐ Investment in the Primary Care Strategy Model including the spcifications for the Proactive Coordinated Primary Care Serivce, Extended Primary Care Service, Keeping People Well Service and Responsive Primary Care Service (from April 2017).
9.02 ‐ National resilience, sustainability and transformation support programmes for GP Practices (Dec 2016 ‐ March 2018).
9.01 ‐ Implementation of the Quality Assurance Framework and Primary Care Dashboard to support General Practice delivering good quality care. Launch with General Practice December 2016, initial intelligence gathering and dialogue to take place Jan ‐ June 2017.
NHS Doncaster CCG Primary Care Delivery PlanImpact Measures Progress Actions Progress
C86015 ‐ The Rossington PracticeC86007 ‐ The Burns Practice
Key:
C86012 ‐ The Oakwood SurgeryC86003 ‐ Heathfield Health Centre
C86011 ‐ The Mount Group Practice
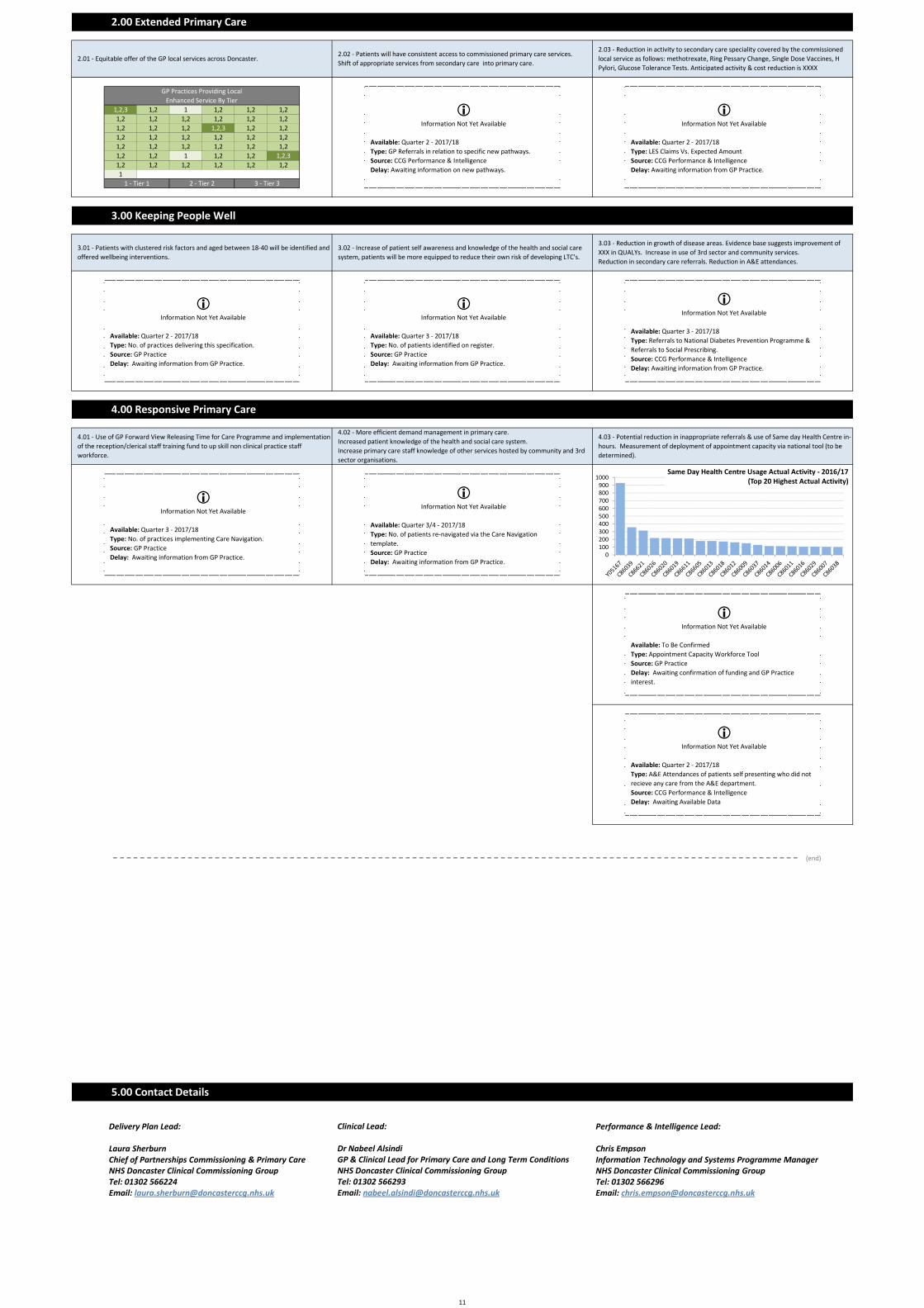
1.00 ‐ All GP Practices will have completed a Proactive Co‐Ordinated Care Specification which includes the identification of 2% most vulnerable and complex patients. This plan will see the GP Practice complete a register of patients and these patients will be reviewed by a mullti‐disciplinary team. Each patient will have a named professional and single care plan which will be relevant to their complex condition. This specification will see the reduction of A&E attendances, emergency admissions and avoidable emergency admissions for the patients identified on the register.
2.00 ‐ The local enhanced services commissioned currently from general practice have been organised into 3 tiers, to make clear: which should be delivered by all practices; which should be delivered by a smaller number of practices on behalf of the whole; and which should be delivered by 1 pan‐Doncaster provider. All practices have signed up to deliver all Tier 1 services, thereby removing the previous inequity for patients. . This service will reduce GP referrals into secondary care for specific services and increase the usage of clinical service available in primary care.
A
3.00 ‐ Practices to compile a clustered risk factor register of patients aged 18‐40 that are already on the smoking and obesity registers but not on a specific disease register. These patients will be offered a lifestyle consultation, with the aim of changing their life choices in order to reduce the risk of developing long term conditions. This plan will look to reduce the number of patients who are highly likely to impact secondary services in the future should their lifestyle and health not improve. It is expected that this intervention will reduce secondary referrals and A&E attendances later in life.
A
4.00 ‐ The Responsive Care pillar will be achieved through deploying the GP Forward View funding streams effectively to facilitate care redesign, better workload management and delivery of primary care at scale. Care Navigation, Online Consultations and Transformation funding will act as key drivers for improvement and innovation with GP Practice and therefore increase capacity and reduce unnecessary reliance on other services.
A
9.09 ‐ Implement Productive General Practice programme in Doncaster April ‐ June 2017.
9.08 ‐ Releasing Time for Care programme support practice EOIs by June 2017, & implementation of the 10 high impact actions thereafter.
Y05167 ‐ The Flying Scotsman Practice
1.10 ‐ Reduction in number of A&E attendances.Better utilisation of the Community Pharmacy Minor Ailments Scheme.
1.11 ‐ Reduction in avoidable emergency admissions. To be quantified prospectively in quarterly monitoring returns from general practice.
Information Not Yet Available
Available: Quarter 2 ‐ 2017/18Type: No. of A&E attendances by patients identified on the Proactive Coordinated Care Register.Source: GP PracticeDelay: Awaiting information from GP Practice.
Information Not Yet Available
Available: Quarter 2 ‐ 2017/18Type: No. of avoidable emergency admissions by patients identified on the Proactive Coordinated Care Register.Source: GP PracticeDelay: Awaiting information from GP Practice.
Y ‐ Yes N ‐ No ? ‐ Unknown
Information Not Yet Available
Available: Quarter 2 ‐ 2017/18Type: Question 33 ‐ GP Patient Survey.Source: GP PracticeDelay: Awaiting information from GP Practice.
C86611 ‐ Dunsville Medical CentreC86032 ‐ Scawsby Health CentreC86023 ‐ Bentley SurgeryC86017 ‐ Kingthorne Group Practice
C86025 ‐ Frances Street Medical CentreC86016 ‐ The Lakeside PracticeC86009 ‐ Mayflower Medical PracticeC86001 ‐ Carcroft Doctors Group
C86606 ‐ Barnburgh SurgeryC86033 ‐ The Nayar PracticeC86024 ‐ Conisbrough Group PracticeC86018 ‐ Northfield Surgery
Single care plan that will be shared with all professionals involved in their care.
All patients on the proactive coordinated care register will have a named professional.
Patients identified for coordinated care will receive regular multidisciplinary reviews by a team.
Y ‐ Yes N ‐ No ? ‐ Unknown Y ‐ Yes N ‐ No ? ‐ Unknown
Y ‐ Yes N ‐ No ? ‐ Unknown Y ‐ Yes N ‐ No
Y ‐ Yes N ‐ No ? ‐ Unknown
A
1.01 ‐ Identification of 2% most vulnerable and complex patients. Practice to proactively treat and coordinate care of this cohort of patients.
1.02 ‐ All GP Practices will have a register of patients receiving proactive coordinated care as specified.
1.03 ‐ Confirmation of named professional and their respective caseloads
1.04 ‐ All patients on the proactive coordinated care register will have a named professional.
1.05 ‐ Patients on the proactive coordinated care register will have a single care plan that will be shared with all professionals involved in their care
1.06 ‐ Patients will be invited to participate in a holistic care planning process and develop a single care plan that be shared with teams and professionals involved in their care
1.07 ‐ All patients on the proactive coordinated care register will be asked Question 33 of the GP Patient Survey
1.08 ‐ Patients identified for coordinated care will receive regular multidisciplinary reviews by a team involving health and care professionals with the necessary skills to address their needs.
1.09 ‐ Reduction in number of A&E attendances. Reduction in emergency admissions. To be quantified prospectively in quarterly monitoring returns from general practice.
Information Not Yet Available
Available: Quarter 2 ‐ 2017/18Type: No. of emergency admissions by patients identified on the Proactive Coordinated Care Register.Source: GP PracticeDelay: Awaiting information from GP Practice.
Identification of 2% most vulnerable and complex patients.
All GP Practices will have a register of patients receiving proactive coordinated care as specified.
Confirmation of named professional and their respective caseloads.
Patients will be invited to participate in a holistic care planning process and develop a single care plan.
Y ‐ Yes N ‐ No ? ‐ Unknown
10
1,2,3 1,2 1 1,2 1,2 1,21,2 1,2 1,2 1,2 1,2 1,21,2 1,2 1,2 1,2,3 1,2 1,21,2 1,2 1,2 1,2 1,2 1,21,2 1,2 1,2 1,2 1,2 1,21,2 1,2 1 1,2 1,2 1,2,31,2 1,2 1,2 1,2 1,2 1,21
Information Not Yet Available
Available: Quarter 2 ‐ 2017/18Type: GP Referrals in relation to specific new pathways.Source: CCG Performance & IntelligenceDelay: Awaiting information on new pathways.
Information Not Yet Available
Available: Quarter 2 ‐ 2017/18Type: LES Claims Vs. Expected AmountSource: CCG Performance & IntelligenceDelay: Awaiting information from GP Practice.
2.01 ‐ Equitable offer of the GP local services across Doncaster.2.02 ‐ Patients will have consistent access to commissioned primary care services.Shift of appropriate services from secondary care into primary care.
2.03 ‐ Reduction in activity to secondary care speciality covered by the commissioned local service as follows: methotrexate, Ring Pessary Change, Single Dose Vaccines, H Pylori, Glucose Tolerance Tests. Anticipated activity & cost reduction is XXXX
5.00 Contact Details
3.02 ‐ Increase of patient self awareness and knowledge of the health and social care system, patients will be more equipped to reduce their own risk of developing LTC's.
Information Not Yet Available
Available: Quarter 3 ‐ 2017/18Type: No. of patients identified on register.Source: GP PracticeDelay: Awaiting information from GP Practice.
3.03 ‐ Reduction in growth of disease areas. Evidence base suggests improvement of XXX in QUALYs. Increase in use of 3rd sector and community services. Reduction in secondary care referrals. Reduction in A&E attendances.
Information Not Yet Available
Available: Quarter 3 ‐ 2017/18Type: Referrals to National Diabetes Prevention Programme & Referrals to Social Prescribing.Source: CCG Performance & IntelligenceDelay: Awaiting information from GP Practice.
Information Not Yet Available
Available: To Be ConfirmedType: Appointment Capacity Workforce ToolSource: GP PracticeDelay: Awaiting confirmation of funding and GP Practice interest.
Information Not Yet Available
Available: Quarter 3/4 ‐ 2017/18Type: No. of patients re‐navigated via the Care Navigation template.Source: GP PracticeDelay: Awaiting information from GP Practice.
Currently Under Discussion
3.00 Keeping People Well
3.01 ‐ Patients with clustered risk factors and aged between 18‐40 will be identified and offered wellbeing interventions.
3 ‐ Tier 32 ‐ Tier 21 ‐ Tier 1
GP Practices Providing Local Enhanced Service By Tier
2.00 Extended Primary Care
4.02 ‐ More efficient demand management in primary care.Increased patient knowledge of the health and social care system. Increase primary care staff knowledge of other services hosted by community and 3rd sector organisations.
4.03 ‐ Potential reduction in inappropriate referrals & use of Same day Health Centre in‐hours. Measurement of deployment of appointment capacity via national tool (to be determined).
Information Not Yet Available
Available: Quarter 2 ‐ 2017/18Type: No. of practices delivering this specification.Source: GP PracticeDelay: Awaiting information from GP Practice.
Information Not Yet Available
Available: Quarter 3 ‐ 2017/18Type: No. of practices implementing Care Navigation.Source: GP PracticeDelay: Awaiting information from GP Practice.
Information Not Yet Available
Available: Quarter 2 ‐ 2017/18Type: A&E Attendances of patients self presenting who did not recieve any care from the A&E department.Source: CCG Performance & IntelligenceDelay: Awaiting Available Data
4.00 Responsive Primary Care
4.01 ‐ Use of GP Forward View Releasing Time for Care Programme and implementation of the reception/clerical staff training fund to up skill non clinical practice staff workforce.
0100200300400500600700800900
1000Same Day Health Centre Usage Actual Activity ‐ 2016/17
(Top 20 Highest Actual Activity)
Performance & Intelligence Lead:
Chris EmpsonInformation Technology and Systems Programme ManagerNHS Doncaster Clinical Commissioning GroupTel: 01302 566296Email: [email protected]
Clinical Lead:
Dr Nabeel AlsindiGP & Clinical Lead for Primary Care and Long Term ConditionsNHS Doncaster Clinical Commissioning GroupTel: 01302 566293Email: [email protected]
Delivery Plan Lead:
Laura SherburnChief of Partnerships Commissioning & Primary CareNHS Doncaster Clinical Commissioning GroupTel: 01302 566224Email: [email protected]
(end)
11
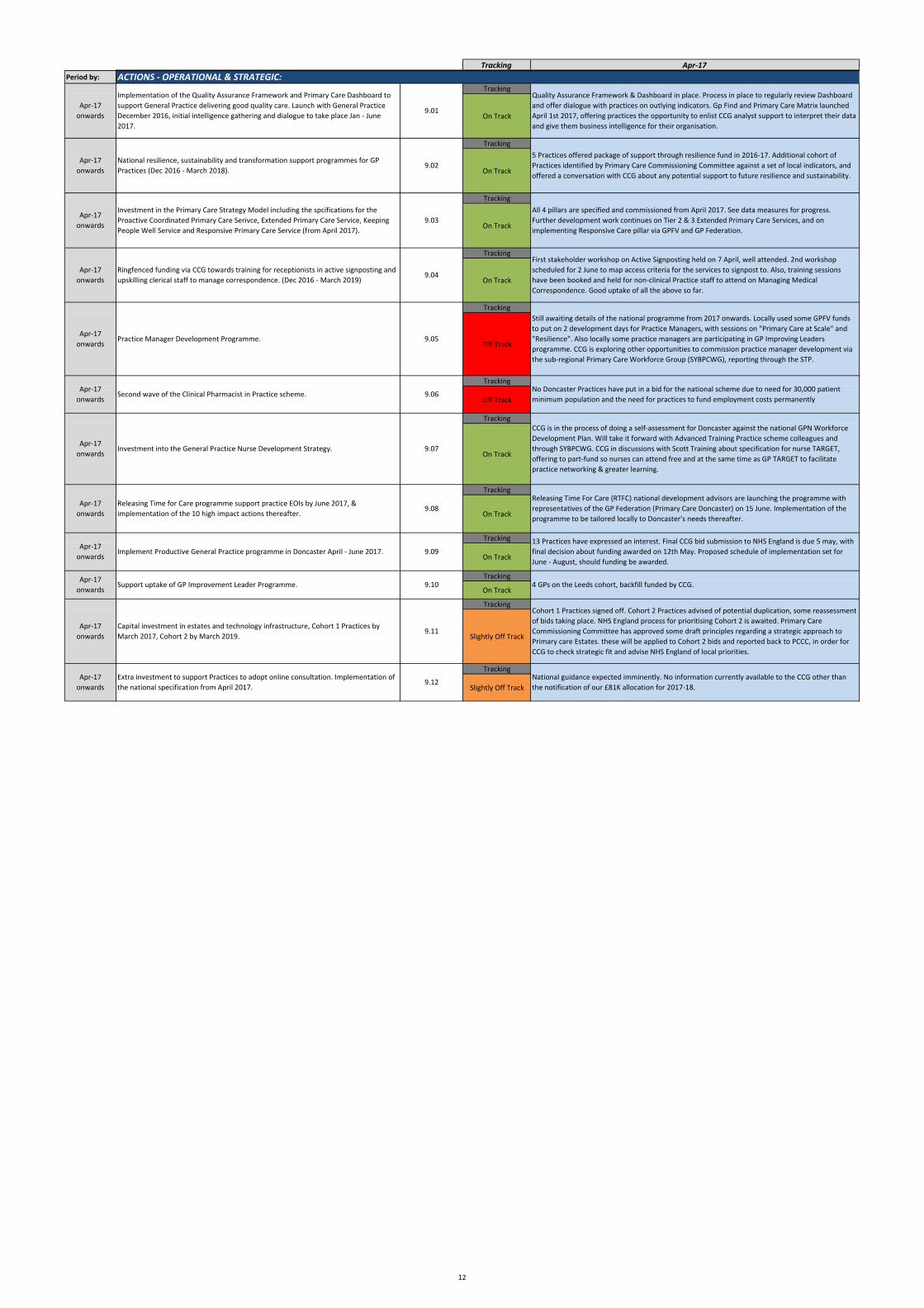
Tracking Apr‐17Period by:
Tracking
On Track
Tracking
On Track
Tracking
On Track
Tracking
On Track
Tracking
Off Track
Tracking
Off Track
Tracking
On Track
Tracking
On Track
Tracking
On Track
Tracking
On Track
Tracking
Slightly Off Track
Tracking
Slightly Off TrackNational guidance expected imminently. No information currently available to the CCG other than the notification of our £81K allocation for 2017‐18.
Cohort 1 Practices signed off. Cohort 2 Practices advised of potential duplication, some reassessment of bids taking place. NHS England process for prioritising Cohort 2 is awaited. Primary Care Commissioning Committee has approved some draft principles regarding a strategic approach to Primary care Estates. these will be applied to Cohort 2 bids and reported back to PCCC, in order for CCG to check strategic fit and advise NHS England of local priorities.
4 GPs on the Leeds cohort, backfill funded by CCG.
13 Practices have expressed an interest. Final CCG bid submission to NHS England is due 5 may, with final decision about funding awarded on 12th May. Proposed schedule of implementation set for June ‐ August, should funding be awarded.
Releasing Time For Care (RTFC) national development advisors are launching the programme with representatives of the GP Federation (Primary Care Doncaster) on 15 June. Implementation of the programme to be tailored locally to Doncaster's needs thereafter.
CCG is in the process of doing a self‐assessment for Doncaster against the national GPN Workforce Development Plan. Will take it forward with Advanced Training Practice scheme colleagues and through SYBPCWG. CCG in discussions with Scott Training about specification for nurse TARGET, offering to part‐fund so nurses can attend free and at the same time as GP TARGET to facilitate practice networking & greater learning.
No Doncaster Practices have put in a bid for the national scheme due to need for 30,000 patient minimum population and the need for practices to fund employment costs permanently
Still awaiting details of the national programme from 2017 onwards. Locally used some GPFV funds to put on 2 development days for Practice Managers, with sessions on "Primary Care at Scale" and "Resilience". Also locally some practice managers are participating in GP Improving Leaders programme. CCG is exploring other opportunities to commission practice manager development via the sub‐regional Primary Care Workforce Group (SYBPCWG), reporting through the STP.
First stakeholder workshop on Active Signposting held on 7 April, well attended. 2nd workshop scheduled for 2 June to map access criteria for the services to signpost to. Also, training sessions have been booked and held for non‐clinical Practice staff to attend on Managing Medical Correspondence. Good uptake of all the above so far.
Apr‐17 onwards
Ringfenced funding via CCG towards training for receptionists in active signposting and upskilling clerical staff to manage correspondence. (Dec 2016 ‐ March 2019)
Apr‐17 onwards
Investment in the Primary Care Strategy Model including the spcifications for the Proactive Coordinated Primary Care Serivce, Extended Primary Care Service, Keeping People Well Service and Responsive Primary Care Service (from April 2017).
All 4 pillars are specified and commissioned from April 2017. See data measures for progress. Further development work continues on Tier 2 & 3 Extended Primary Care Services, and on implementing Responsive Care pillar via GPFV and GP Federation.
ACTIONS ‐ OPERATIONAL & STRATEGIC:
Apr‐17 onwards
Implementation of the Quality Assurance Framework and Primary Care Dashboard to support General Practice delivering good quality care. Launch with General Practice December 2016, initial intelligence gathering and dialogue to take place Jan ‐ June 2017.
Apr‐17 onwards
National resilience, sustainability and transformation support programmes for GP Practices (Dec 2016 ‐ March 2018).
Quality Assurance Framework & Dashboard in place. Process in place to regularly review Dashboard and offer dialogue with practices on outlying indicators. Gp Find and Primary Care Matrix launched April 1st 2017, offering practices the opportunity to enlist CCG analyst support to interpret their data and give them business intelligence for their organisation.
5 Practices offered package of support through resilience fund in 2016‐17. Additional cohort of Practices identified by Primary Care Commissioning Committee against a set of local indicators, and offered a conversation with CCG about any potential support to future resilience and sustainability.
Apr‐17 onwards
Extra investment to support Practices to adopt online consultation. Implementation of the national specification from April 2017.
Apr‐17 onwards
Practice Manager Development Programme.
Apr‐17 onwards
Second wave of the Clinical Pharmacist in Practice scheme.
Apr‐17 onwards
Capital investment in estates and technology infrastructure, Cohort 1 Practices by March 2017, Cohort 2 by March 2019.
Apr‐17 onwards
Releasing Time for Care programme support practice EOIs by June 2017, & implementation of the 10 high impact actions thereafter.
Apr‐17 onwards
Support uptake of GP Improvement Leader Programme.
Apr‐17 onwards
Implement Productive General Practice programme in Doncaster April ‐ June 2017.
Apr‐17 onwards
Investment into the General Practice Nurse Development Strategy.
9.04
9.03
9.02
9.01
9.12
9.11
9.10
9.09
9.08
9.07
9.06
9.05
12
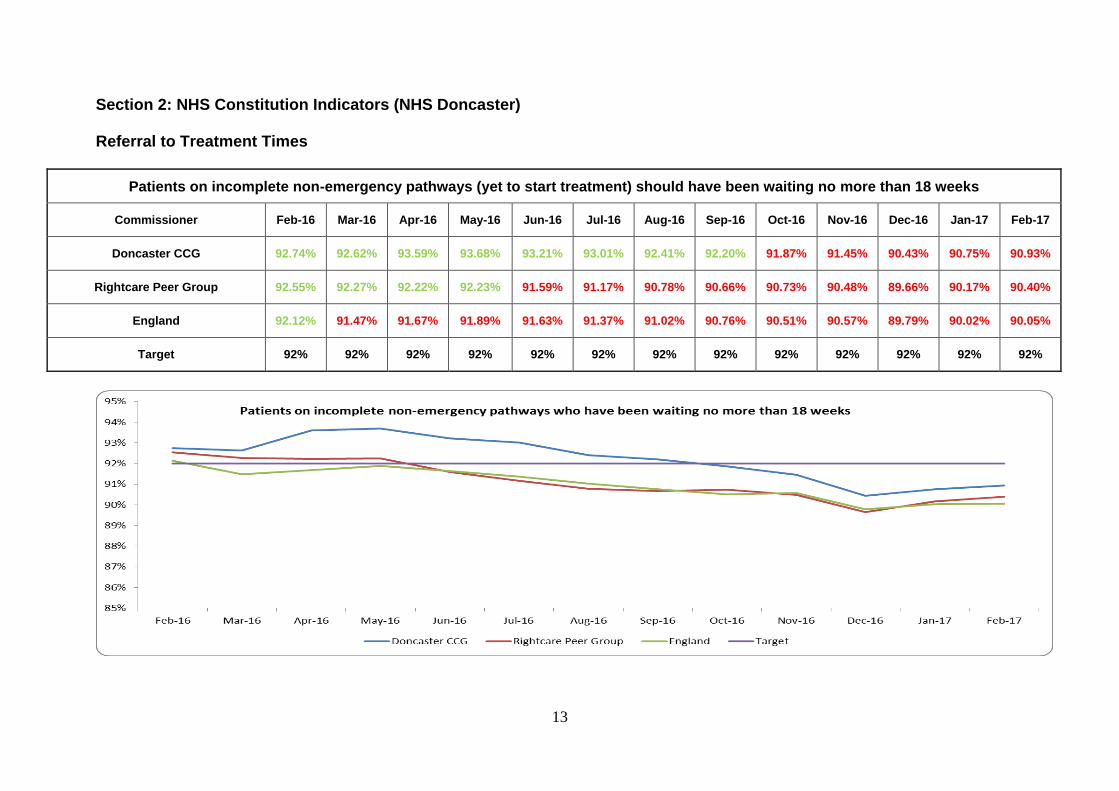
13
Section 2: NHS Constitution Indicators (NHS Doncaster) Referral to Treatment Times
Patients on incomplete non-emergency pathways (yet to start treatment) should have been waiting no more than 18 weeks
Commissioner Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17
Doncaster CCG 92.74% 92.62% 93.59% 93.68% 93.21% 93.01% 92.41% 92.20% 91.87% 91.45% 90.43% 90.75% 90.93%
Rightcare Peer Group 92.55% 92.27% 92.22% 92.23% 91.59% 91.17% 90.78% 90.66% 90.73% 90.48% 89.66% 90.17% 90.40%
England 92.12% 91.47% 91.67% 91.89% 91.63% 91.37% 91.02% 90.76% 90.51% 90.57% 89.79% 90.02% 90.05%
Target 92% 92% 92% 92% 92% 92% 92% 92% 92% 92% 92% 92% 92%
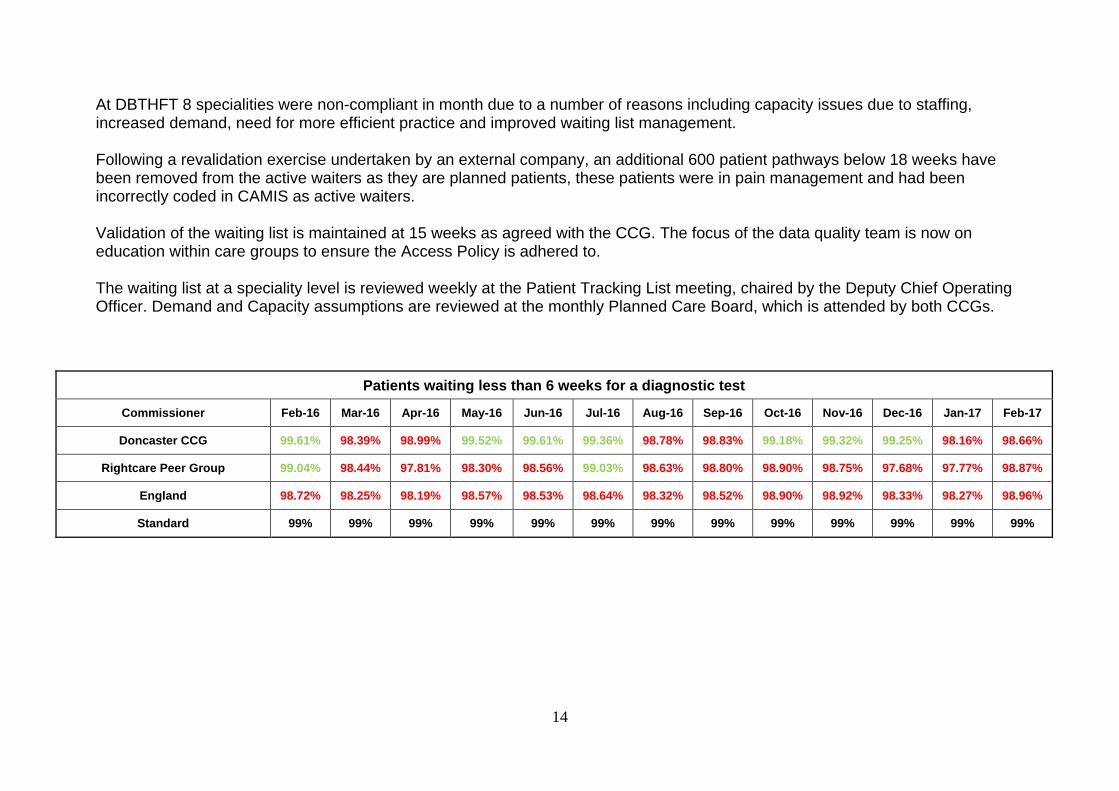
14
At DBTHFT 8 specialities were non-compliant in month due to a number of reasons including capacity issues due to staffing, increased demand, need for more efficient practice and improved waiting list management. Following a revalidation exercise undertaken by an external company, an additional 600 patient pathways below 18 weeks have been removed from the active waiters as they are planned patients, these patients were in pain management and had been incorrectly coded in CAMIS as active waiters. Validation of the waiting list is maintained at 15 weeks as agreed with the CCG. The focus of the data quality team is now on education within care groups to ensure the Access Policy is adhered to. The waiting list at a speciality level is reviewed weekly at the Patient Tracking List meeting, chaired by the Deputy Chief Operating Officer. Demand and Capacity assumptions are reviewed at the monthly Planned Care Board, which is attended by both CCGs.
Patients waiting less than 6 weeks for a diagnostic test
Commissioner Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17
Doncaster CCG 99.61% 98.39% 98.99% 99.52% 99.61% 99.36% 98.78% 98.83% 99.18% 99.32% 99.25% 98.16% 98.66%
Rightcare Peer Group 99.04% 98.44% 97.81% 98.30% 98.56% 99.03% 98.63% 98.80% 98.90% 98.75% 97.68% 97.77% 98.87%
England 98.72% 98.25% 98.19% 98.57% 98.53% 98.64% 98.32% 98.52% 98.90% 98.92% 98.33% 98.27% 98.96%
Standard 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% 99% 99%
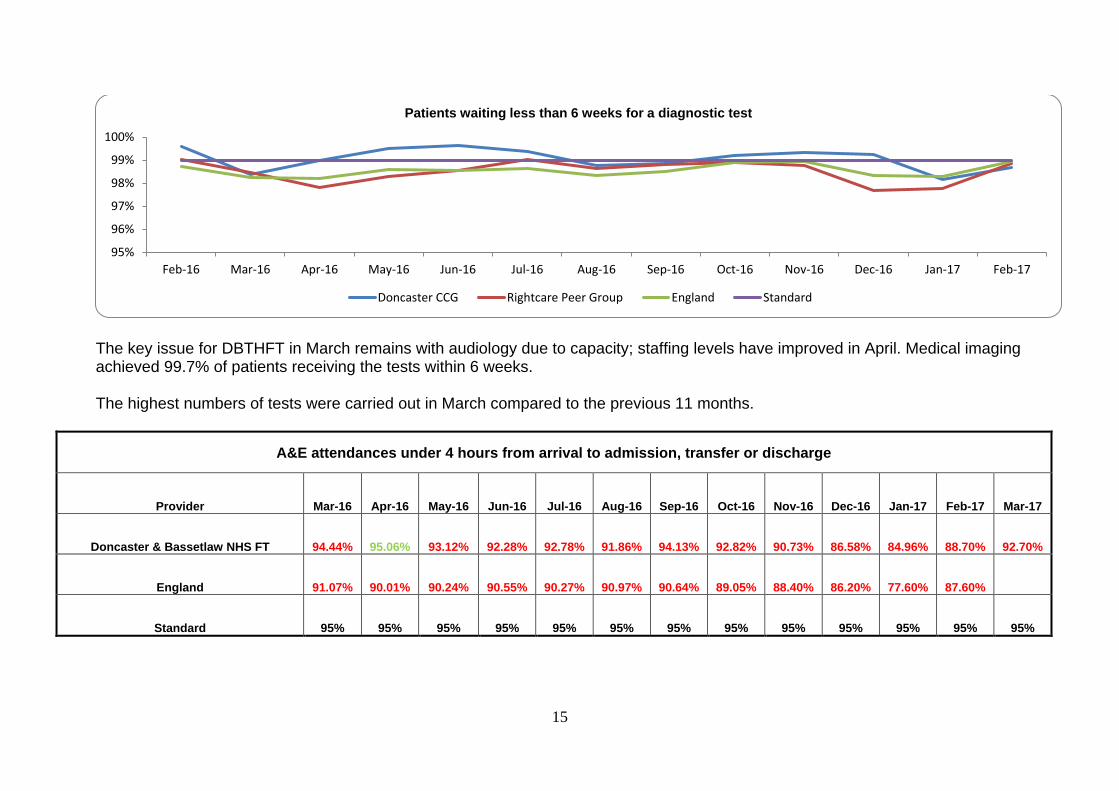
15
The key issue for DBTHFT in March remains with audiology due to capacity; staffing levels have improved in April. Medical imaging achieved 99.7% of patients receiving the tests within 6 weeks. The highest numbers of tests were carried out in March compared to the previous 11 months.
A&E attendances under 4 hours from arrival to admission, transfer or discharge
Provider Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17
Doncaster & Bassetlaw NHS FT 94.44% 95.06% 93.12% 92.28% 92.78% 91.86% 94.13% 92.82% 90.73% 86.58% 84.96% 88.70% 92.70%
England 91.07% 90.01% 90.24% 90.55% 90.27% 90.97% 90.64% 89.05% 88.40% 86.20% 77.60% 87.60%
Standard 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95%
95%
96%
97%
98%
99%
100%
Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17
Patients waiting less than 6 weeks for a diagnostic test
Doncaster CCG Rightcare Peer Group England Standard
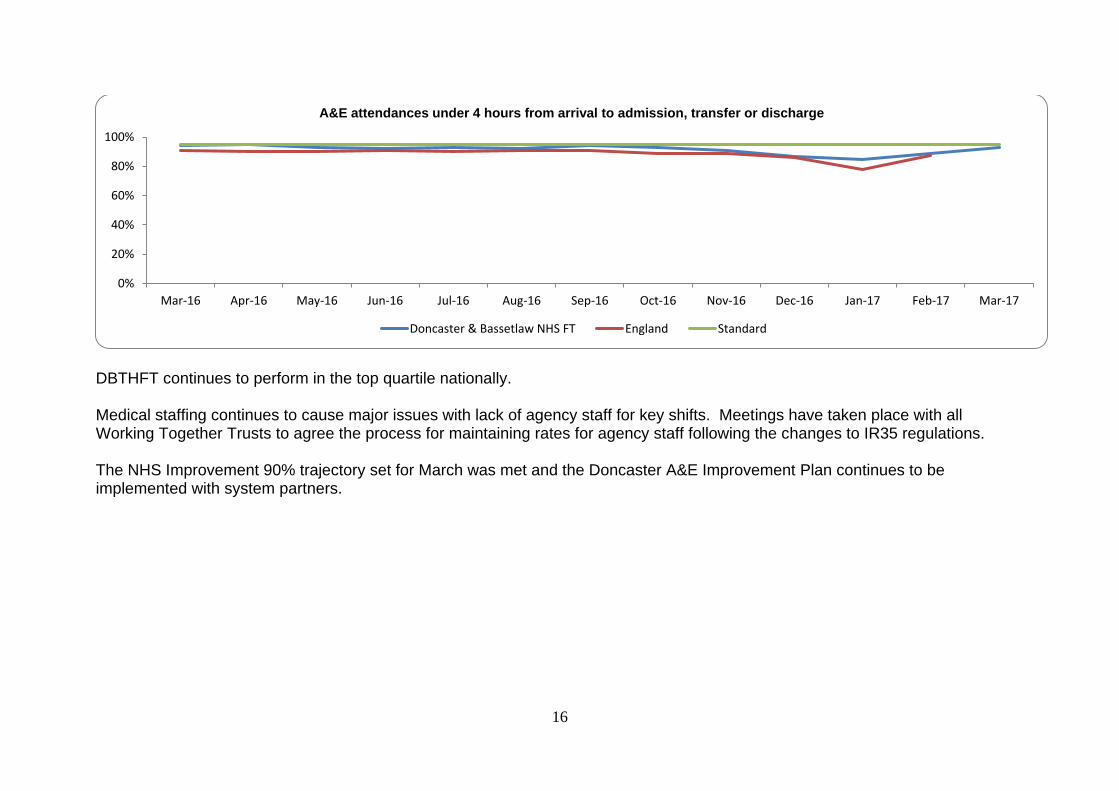
16
DBTHFT continues to perform in the top quartile nationally. Medical staffing continues to cause major issues with lack of agency staff for key shifts. Meetings have taken place with all Working Together Trusts to agree the process for maintaining rates for agency staff following the changes to IR35 regulations. The NHS Improvement 90% trajectory set for March was met and the Doncaster A&E Improvement Plan continues to be implemented with system partners.
0%
20%
40%
60%
80%
100%
Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17
A&E attendances under 4 hours from arrival to admission, transfer or discharge
Doncaster & Bassetlaw NHS FT England Standard
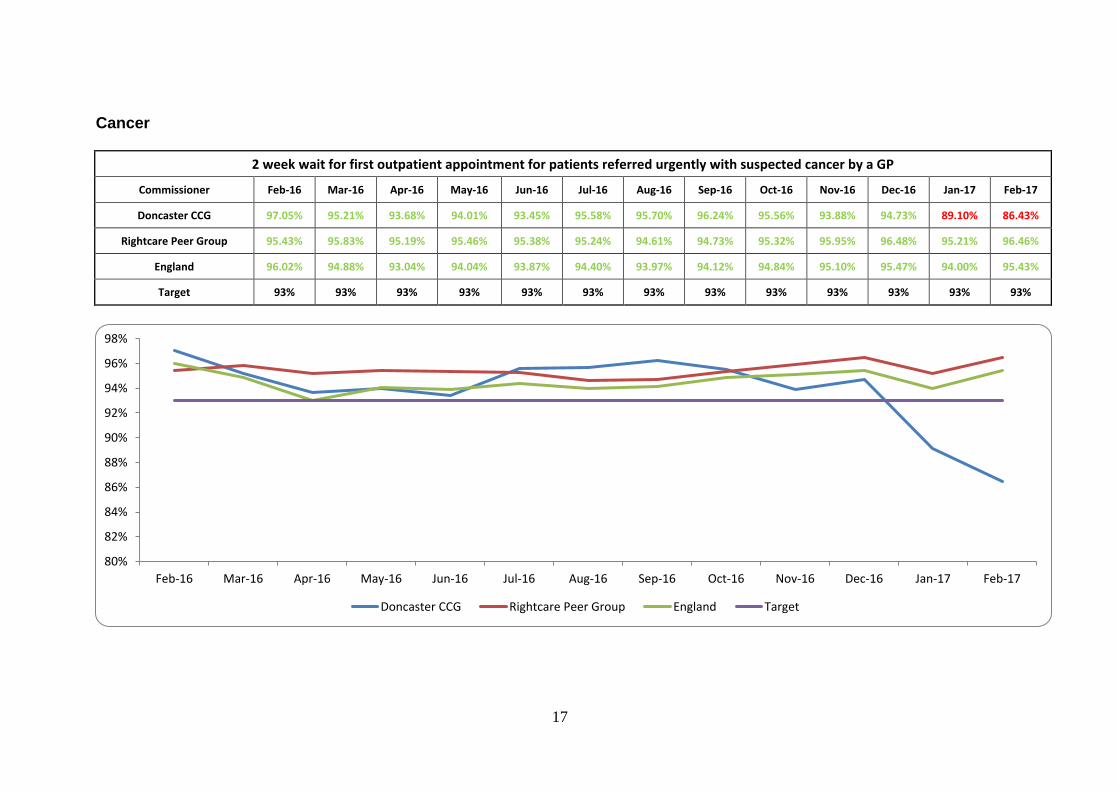
17
Cancer
2 week wait for first outpatient appointment for patients referred urgently with suspected cancer by a GP
Commissioner Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17
Doncaster CCG 97.05% 95.21% 93.68% 94.01% 93.45% 95.58% 95.70% 96.24% 95.56% 93.88% 94.73% 89.10% 86.43%
Rightcare Peer Group 95.43% 95.83% 95.19% 95.46% 95.38% 95.24% 94.61% 94.73% 95.32% 95.95% 96.48% 95.21% 96.46%
England 96.02% 94.88% 93.04% 94.04% 93.87% 94.40% 93.97% 94.12% 94.84% 95.10% 95.47% 94.00% 95.43%
Target 93% 93% 93% 93% 93% 93% 93% 93% 93% 93% 93% 93% 93%
80%
82%
84%
86%
88%
90%
92%
94%
96%
98%
Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17
Doncaster CCG Rightcare Peer Group England Target
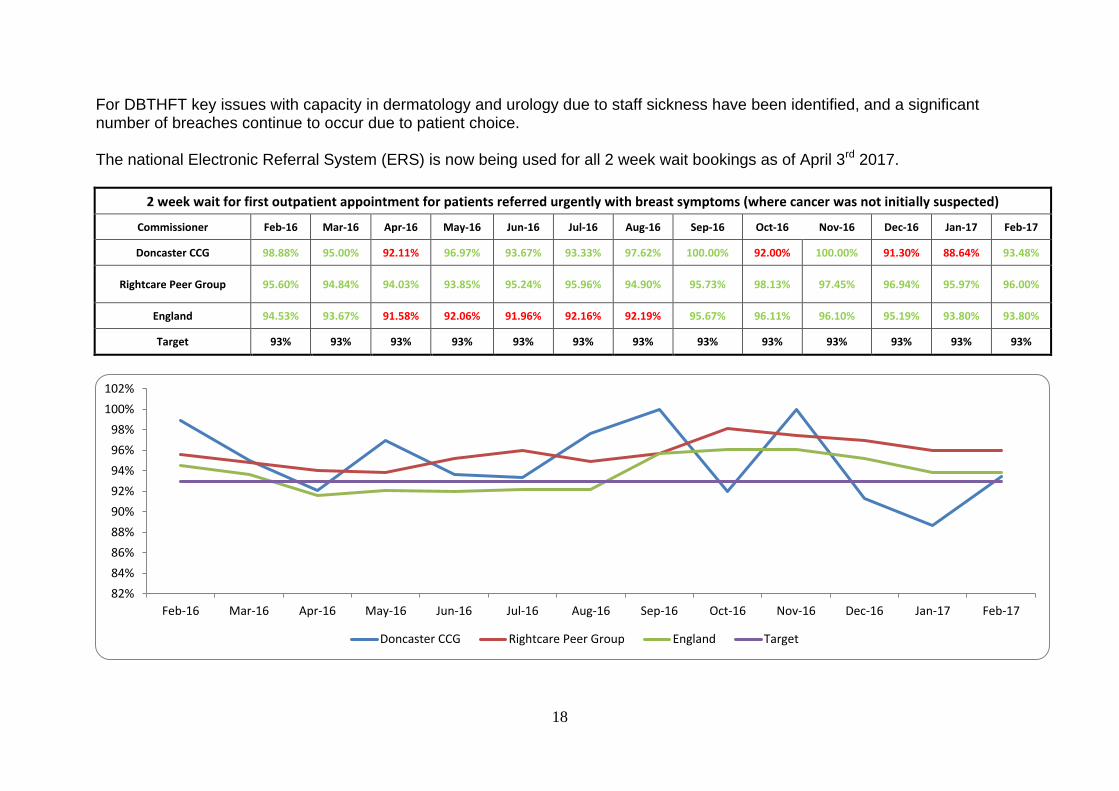
18
For DBTHFT key issues with capacity in dermatology and urology due to staff sickness have been identified, and a significant number of breaches continue to occur due to patient choice. The national Electronic Referral System (ERS) is now being used for all 2 week wait bookings as of April 3rd 2017.
2 week wait for first outpatient appointment for patients referred urgently with breast symptoms (where cancer was not initially suspected)
Commissioner Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17
Doncaster CCG 98.88% 95.00% 92.11% 96.97% 93.67% 93.33% 97.62% 100.00% 92.00% 100.00% 91.30% 88.64% 93.48%
Rightcare Peer Group 95.60% 94.84% 94.03% 93.85% 95.24% 95.96% 94.90% 95.73% 98.13% 97.45% 96.94% 95.97% 96.00%
England 94.53% 93.67% 91.58% 92.06% 91.96% 92.16% 92.19% 95.67% 96.11% 96.10% 95.19% 93.80% 93.80%
Target 93% 93% 93% 93% 93% 93% 93% 93% 93% 93% 93% 93% 93%
82%
84%
86%
88%
90%
92%
94%
96%
98%
100%
102%
Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17
Doncaster CCG Rightcare Peer Group England Target
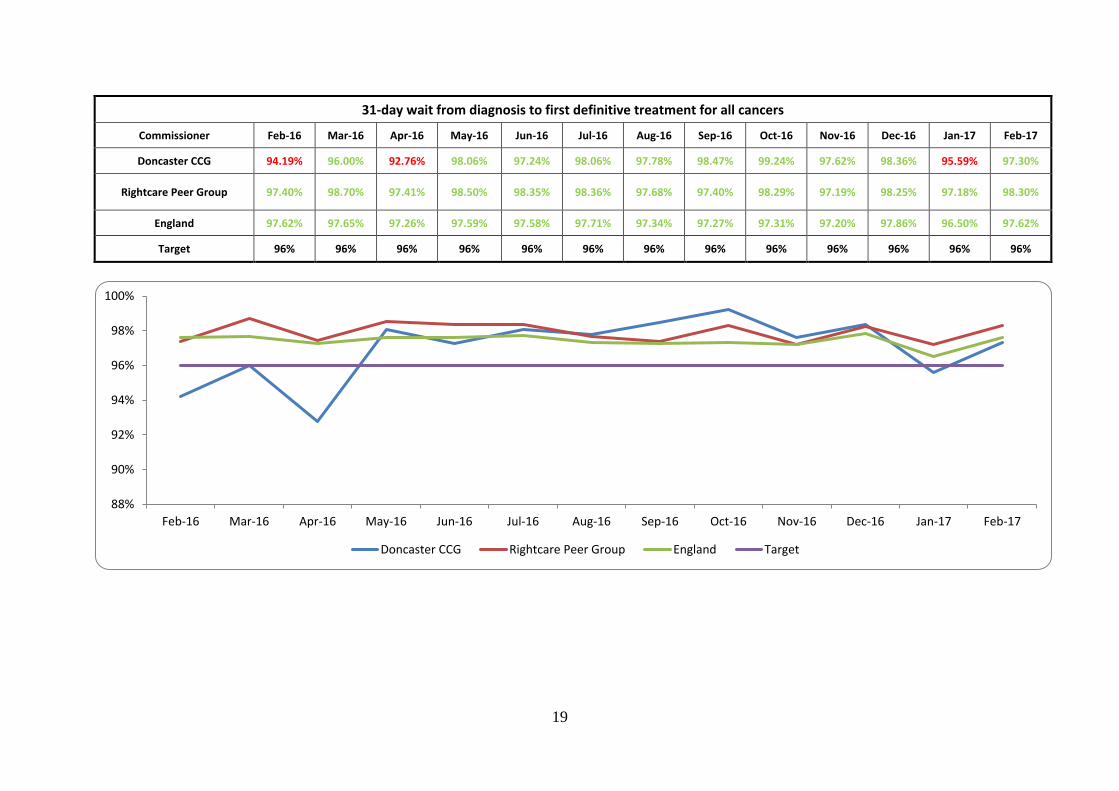
19
31-day wait from diagnosis to first definitive treatment for all cancers
Commissioner Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17
Doncaster CCG 94.19% 96.00% 92.76% 98.06% 97.24% 98.06% 97.78% 98.47% 99.24% 97.62% 98.36% 95.59% 97.30%
Rightcare Peer Group 97.40% 98.70% 97.41% 98.50% 98.35% 98.36% 97.68% 97.40% 98.29% 97.19% 98.25% 97.18% 98.30%
England 97.62% 97.65% 97.26% 97.59% 97.58% 97.71% 97.34% 97.27% 97.31% 97.20% 97.86% 96.50% 97.62%
Target 96% 96% 96% 96% 96% 96% 96% 96% 96% 96% 96% 96% 96%
88%
90%
92%
94%
96%
98%
100%
Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17
Doncaster CCG Rightcare Peer Group England Target
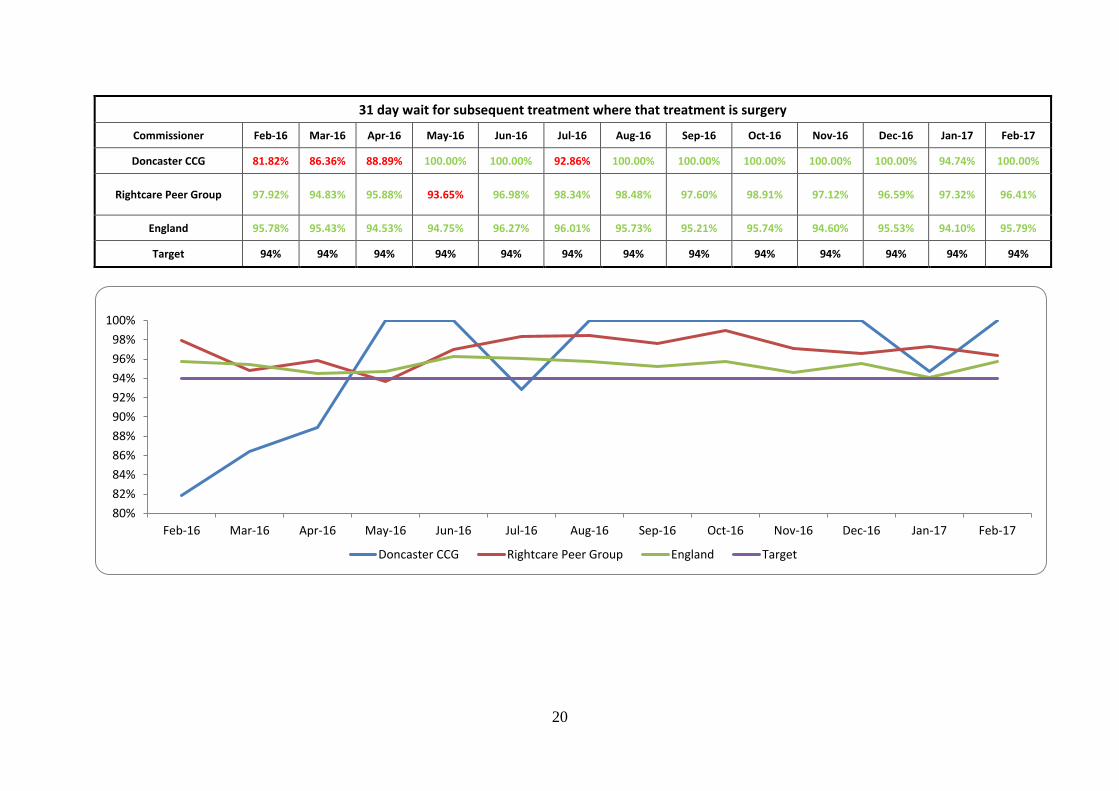
20
31 day wait for subsequent treatment where that treatment is surgery
Commissioner Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17
Doncaster CCG 81.82% 86.36% 88.89% 100.00% 100.00% 92.86% 100.00% 100.00% 100.00% 100.00% 100.00% 94.74% 100.00%
Rightcare Peer Group 97.92% 94.83% 95.88% 93.65% 96.98% 98.34% 98.48% 97.60% 98.91% 97.12% 96.59% 97.32% 96.41%
England 95.78% 95.43% 94.53% 94.75% 96.27% 96.01% 95.73% 95.21% 95.74% 94.60% 95.53% 94.10% 95.79%
Target 94% 94% 94% 94% 94% 94% 94% 94% 94% 94% 94% 94% 94%
80%
82%
84%
86%
88%
90%
92%
94%
96%
98%
100%
Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17
Doncaster CCG Rightcare Peer Group England Target
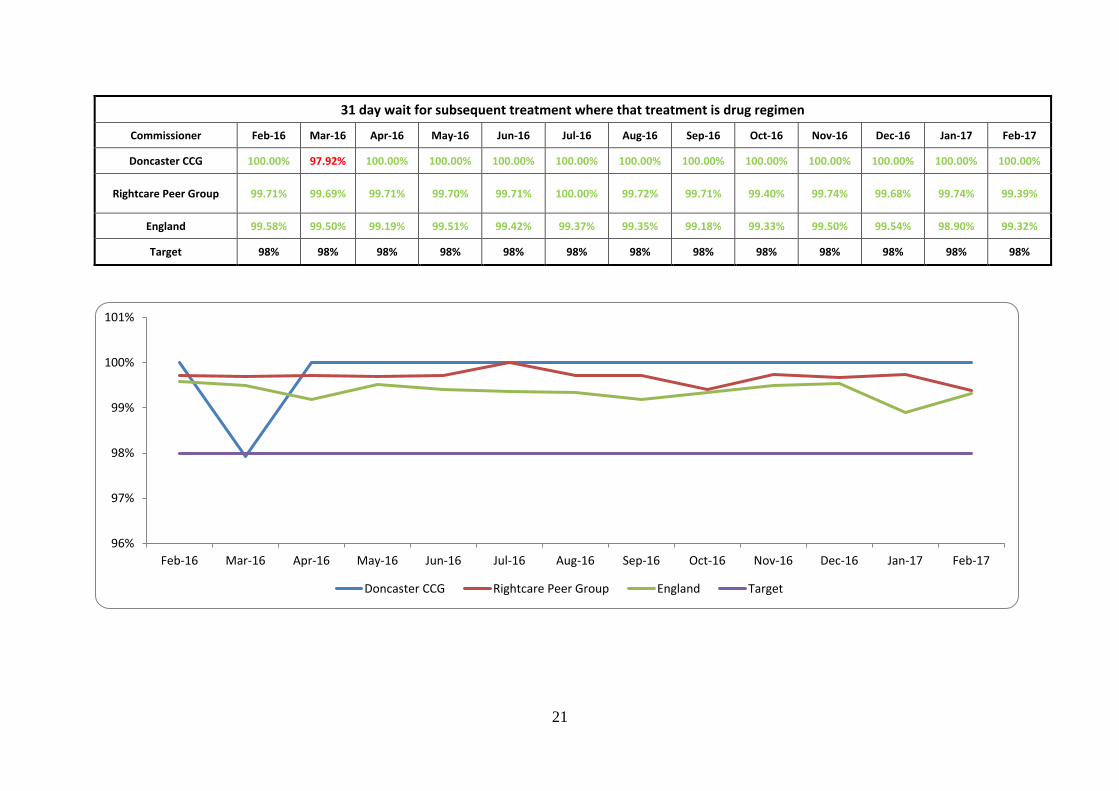
21
31 day wait for subsequent treatment where that treatment is drug regimen
Commissioner Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17
Doncaster CCG 100.00% 97.92% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00%
Rightcare Peer Group 99.71% 99.69% 99.71% 99.70% 99.71% 100.00% 99.72% 99.71% 99.40% 99.74% 99.68% 99.74% 99.39%
England 99.58% 99.50% 99.19% 99.51% 99.42% 99.37% 99.35% 99.18% 99.33% 99.50% 99.54% 98.90% 99.32%
Target 98% 98% 98% 98% 98% 98% 98% 98% 98% 98% 98% 98% 98%
96%
97%
98%
99%
100%
101%
Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17
Doncaster CCG Rightcare Peer Group England Target
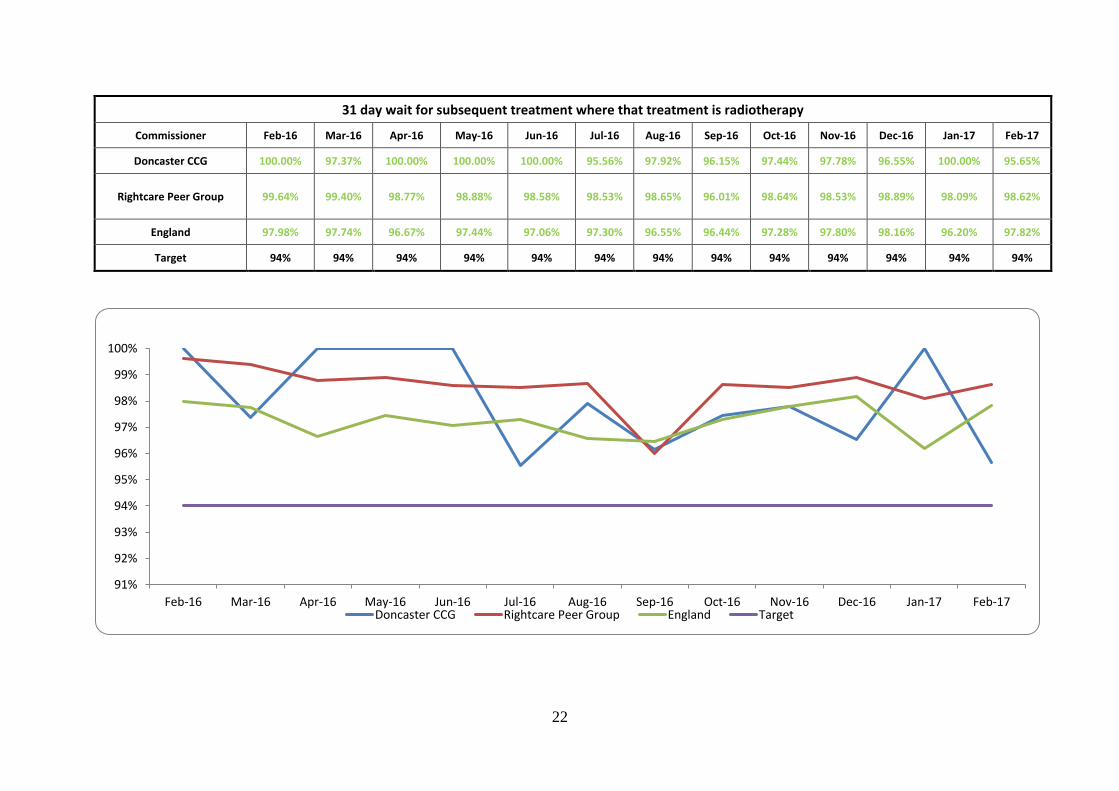
22
31 day wait for subsequent treatment where that treatment is radiotherapy
Commissioner Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17
Doncaster CCG 100.00% 97.37% 100.00% 100.00% 100.00% 95.56% 97.92% 96.15% 97.44% 97.78% 96.55% 100.00% 95.65%
Rightcare Peer Group 99.64% 99.40% 98.77% 98.88% 98.58% 98.53% 98.65% 96.01% 98.64% 98.53% 98.89% 98.09% 98.62%
England 97.98% 97.74% 96.67% 97.44% 97.06% 97.30% 96.55% 96.44% 97.28% 97.80% 98.16% 96.20% 97.82%
Target 94% 94% 94% 94% 94% 94% 94% 94% 94% 94% 94% 94% 94%
91%
92%
93%
94%
95%
96%
97%
98%
99%
100%
Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17Doncaster CCG Rightcare Peer Group England Target
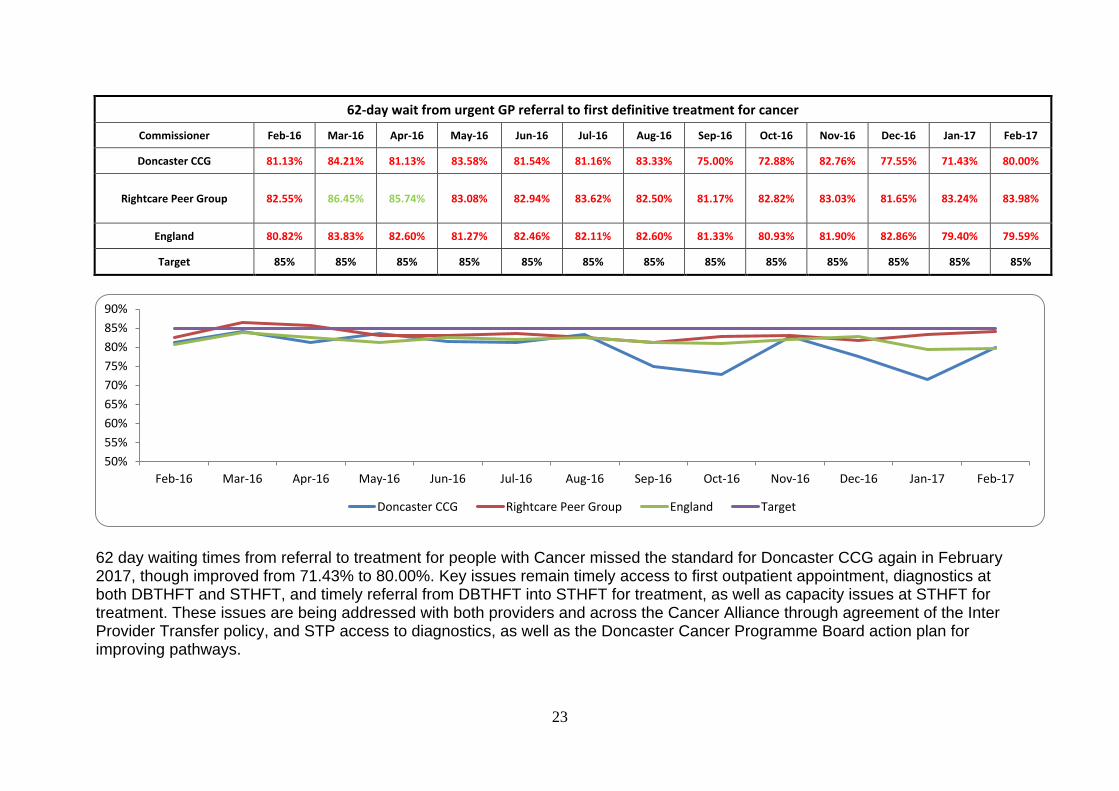
23
62-day wait from urgent GP referral to first definitive treatment for cancer
Commissioner Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17
Doncaster CCG 81.13% 84.21% 81.13% 83.58% 81.54% 81.16% 83.33% 75.00% 72.88% 82.76% 77.55% 71.43% 80.00%
Rightcare Peer Group 82.55% 86.45% 85.74% 83.08% 82.94% 83.62% 82.50% 81.17% 82.82% 83.03% 81.65% 83.24% 83.98%
England 80.82% 83.83% 82.60% 81.27% 82.46% 82.11% 82.60% 81.33% 80.93% 81.90% 82.86% 79.40% 79.59%
Target 85% 85% 85% 85% 85% 85% 85% 85% 85% 85% 85% 85% 85%
62 day waiting times from referral to treatment for people with Cancer missed the standard for Doncaster CCG again in February 2017, though improved from 71.43% to 80.00%. Key issues remain timely access to first outpatient appointment, diagnostics at both DBTHFT and STHFT, and timely referral from DBTHFT into STHFT for treatment, as well as capacity issues at STHFT for treatment. These issues are being addressed with both providers and across the Cancer Alliance through agreement of the Inter Provider Transfer policy, and STP access to diagnostics, as well as the Doncaster Cancer Programme Board action plan for improving pathways.
50%
55%
60%
65%
70%
75%
80%
85%
90%
Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17
Doncaster CCG Rightcare Peer Group England Target
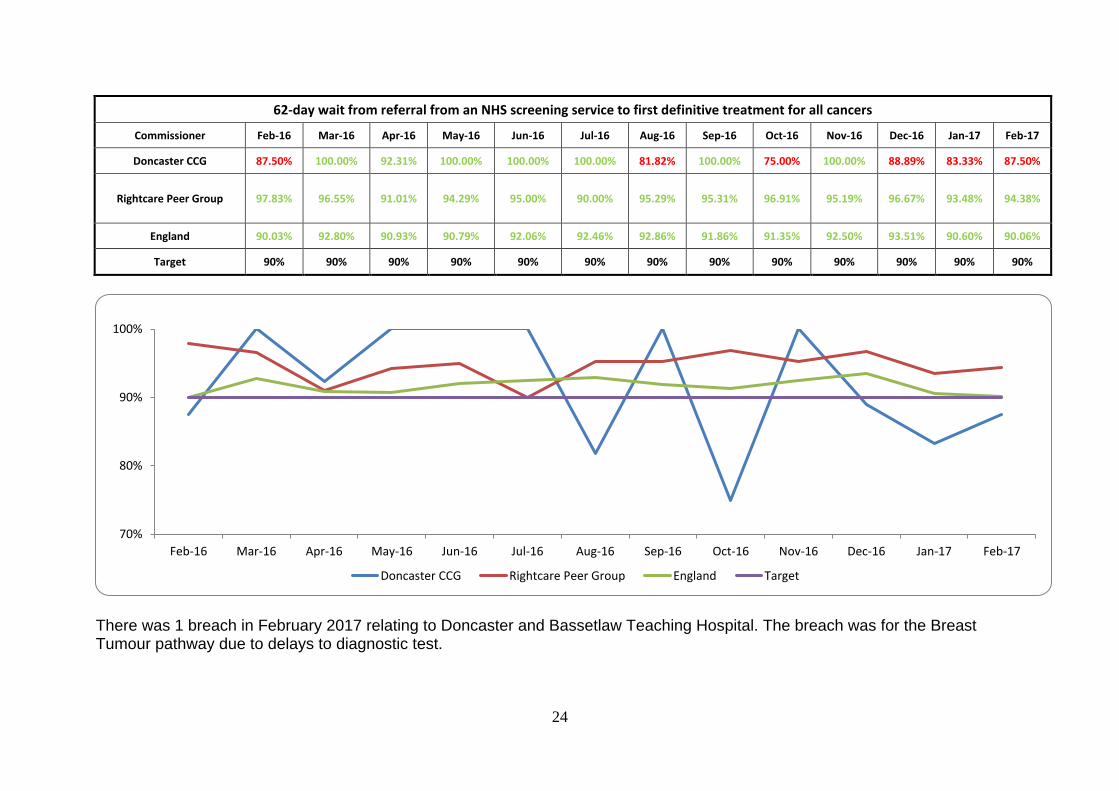
24
62-day wait from referral from an NHS screening service to first definitive treatment for all cancers
Commissioner Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17
Doncaster CCG 87.50% 100.00% 92.31% 100.00% 100.00% 100.00% 81.82% 100.00% 75.00% 100.00% 88.89% 83.33% 87.50%
Rightcare Peer Group 97.83% 96.55% 91.01% 94.29% 95.00% 90.00% 95.29% 95.31% 96.91% 95.19% 96.67% 93.48% 94.38%
England 90.03% 92.80% 90.93% 90.79% 92.06% 92.46% 92.86% 91.86% 91.35% 92.50% 93.51% 90.60% 90.06%
Target 90% 90% 90% 90% 90% 90% 90% 90% 90% 90% 90% 90% 90%
There was 1 breach in February 2017 relating to Doncaster and Bassetlaw Teaching Hospital. The breach was for the Breast Tumour pathway due to delays to diagnostic test.
70%
80%
90%
100%
Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17
Doncaster CCG Rightcare Peer Group England Target
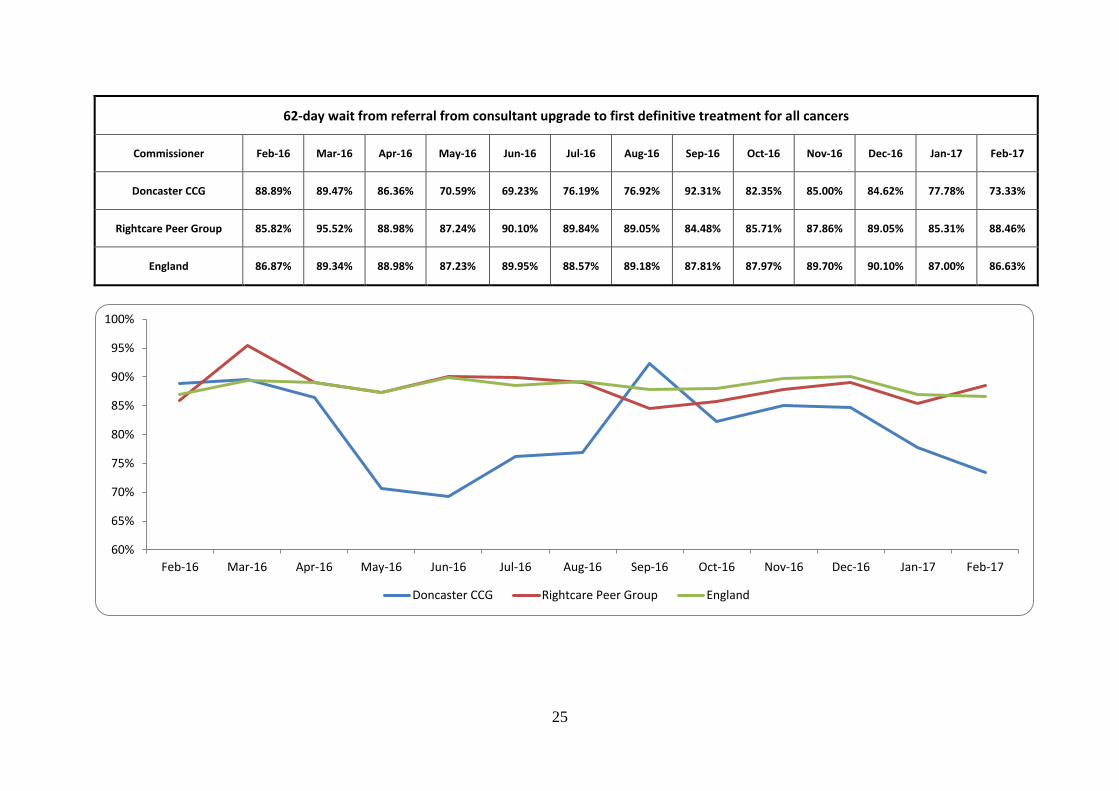
25
62-day wait from referral from consultant upgrade to first definitive treatment for all cancers
Commissioner Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17
Doncaster CCG 88.89% 89.47% 86.36% 70.59% 69.23% 76.19% 76.92% 92.31% 82.35% 85.00% 84.62% 77.78% 73.33%
Rightcare Peer Group 85.82% 95.52% 88.98% 87.24% 90.10% 89.84% 89.05% 84.48% 85.71% 87.86% 89.05% 85.31% 88.46%
England 86.87% 89.34% 88.98% 87.23% 89.95% 88.57% 89.18% 87.81% 87.97% 89.70% 90.10% 87.00% 86.63%
60%
65%
70%
75%
80%
85%
90%
95%
100%
Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17
Doncaster CCG Rightcare Peer Group England
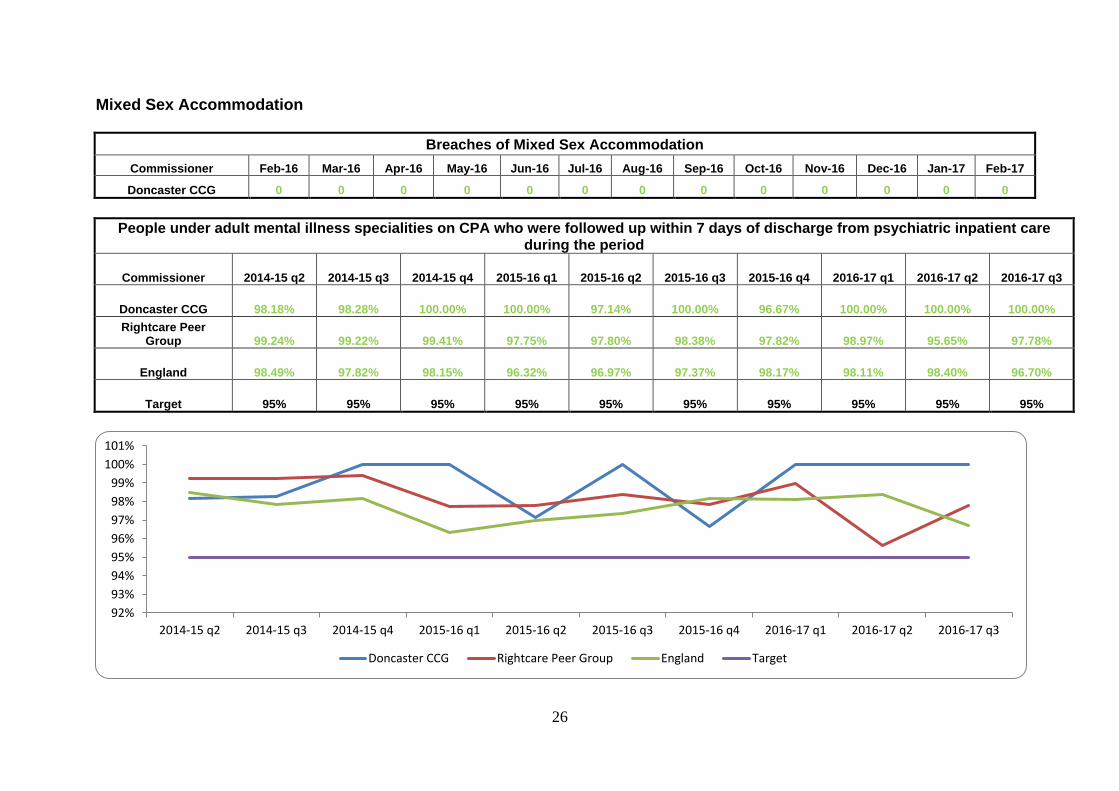
26
Mixed Sex Accommodation
Breaches of Mixed Sex Accommodation
Commissioner Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17
Doncaster CCG 0 0 0 0 0 0 0 0 0 0 0 0 0
People under adult mental illness specialities on CPA who were followed up within 7 days of discharge from psychiatric inpatient care during the period
Commissioner 2014-15 q2 2014-15 q3 2014-15 q4 2015-16 q1 2015-16 q2 2015-16 q3 2015-16 q4 2016-17 q1 2016-17 q2 2016-17 q3
Doncaster CCG 98.18% 98.28% 100.00% 100.00% 97.14% 100.00% 96.67% 100.00% 100.00% 100.00%
Rightcare Peer Group 99.24% 99.22% 99.41% 97.75% 97.80% 98.38% 97.82% 98.97% 95.65% 97.78%
England 98.49% 97.82% 98.15% 96.32% 96.97% 97.37% 98.17% 98.11% 98.40% 96.70%
Target 95% 95% 95% 95% 95% 95% 95% 95% 95% 95%
92%
93%
94%
95%
96%
97%
98%
99%
100%
101%
2014-15 q2 2014-15 q3 2014-15 q4 2015-16 q1 2015-16 q2 2015-16 q3 2015-16 q4 2016-17 q1 2016-17 q2 2016-17 q3
Doncaster CCG Rightcare Peer Group England Target

27
Improving Access to Psychological Therapies (IAPT)
People waiting 6 weeks or less from referral to entering a course of IAPT treatment (Completed)
Commissioner Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17
Doncaster CCG 30.00% 41.38% 45.45% 54.90% 60.00% 66.10% 72.00% 68.00% 80.00% 82.00% 83.00% 87.00% 78.00%
England 84.35% 83.41% 83.65% 84.56% 84.29% 84.82% 85.18% 86.98% 87.83% 87.71% 88.80% 89.40% 90.21%
Target 75% 75% 75% 75% 75% 75% 75% 75% 75% 75% 75% 75% 75%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17
People waiting 6 weeks or less from referral to entering a course of IAPT treatment - Completed
Doncaster CCG England Target
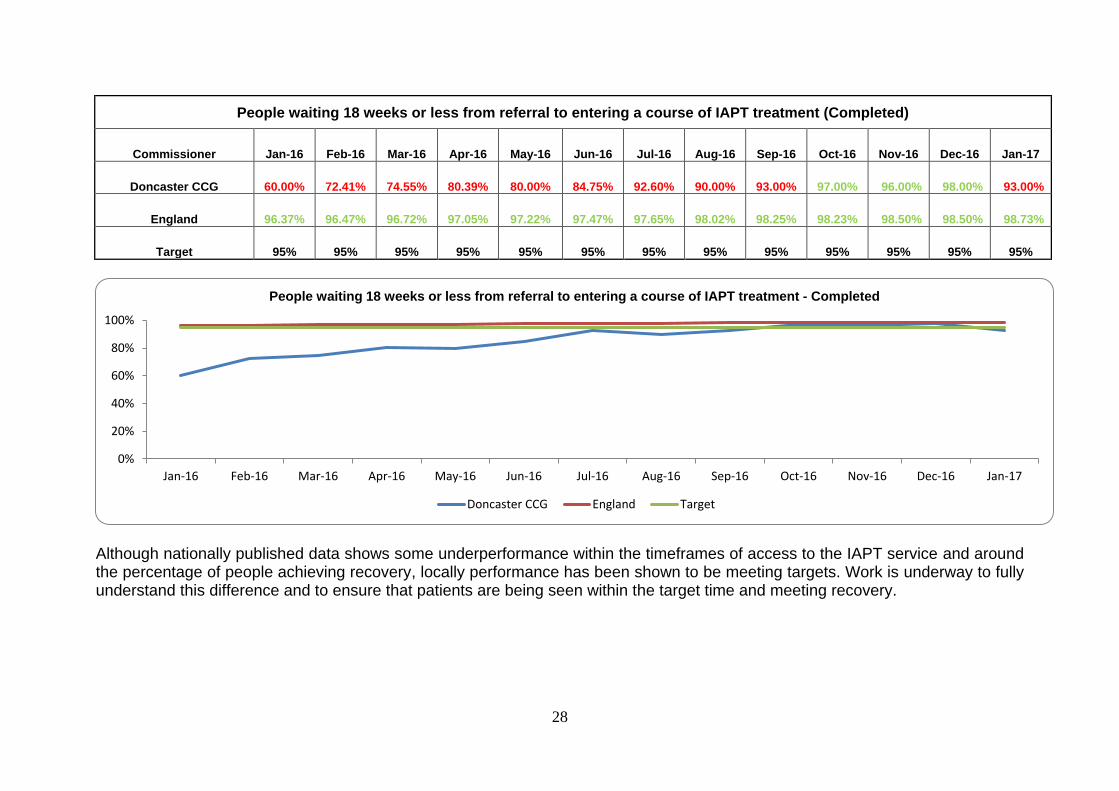
28
People waiting 18 weeks or less from referral to entering a course of IAPT treatment (Completed)
Commissioner Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17
Doncaster CCG 60.00% 72.41% 74.55% 80.39% 80.00% 84.75% 92.60% 90.00% 93.00% 97.00% 96.00% 98.00% 93.00%
England 96.37% 96.47% 96.72% 97.05% 97.22% 97.47% 97.65% 98.02% 98.25% 98.23% 98.50% 98.50% 98.73%
Target 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95%
Although nationally published data shows some underperformance within the timeframes of access to the IAPT service and around the percentage of people achieving recovery, locally performance has been shown to be meeting targets. Work is underway to fully understand this difference and to ensure that patients are being seen within the target time and meeting recovery.
0%
20%
40%
60%
80%
100%
Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17
People waiting 18 weeks or less from referral to entering a course of IAPT treatment - Completed
Doncaster CCG England Target
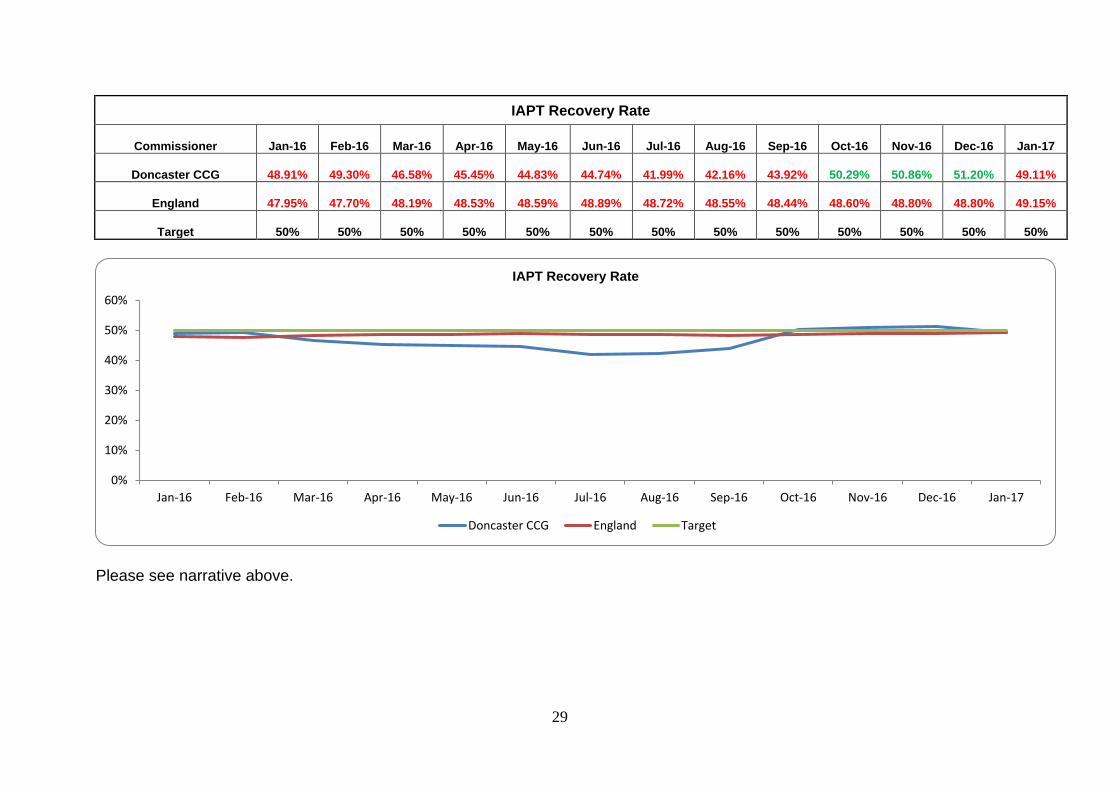
29
IAPT Recovery Rate
Commissioner Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17
Doncaster CCG 48.91% 49.30% 46.58% 45.45% 44.83% 44.74% 41.99% 42.16% 43.92% 50.29% 50.86% 51.20% 49.11%
England 47.95% 47.70% 48.19% 48.53% 48.59% 48.89% 48.72% 48.55% 48.44% 48.60% 48.80% 48.80% 49.15%
Target 50% 50% 50% 50% 50% 50% 50% 50% 50% 50% 50% 50% 50%
Please see narrative above.
0%
10%
20%
30%
40%
50%
60%
Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17
IAPT Recovery Rate
Doncaster CCG England Target
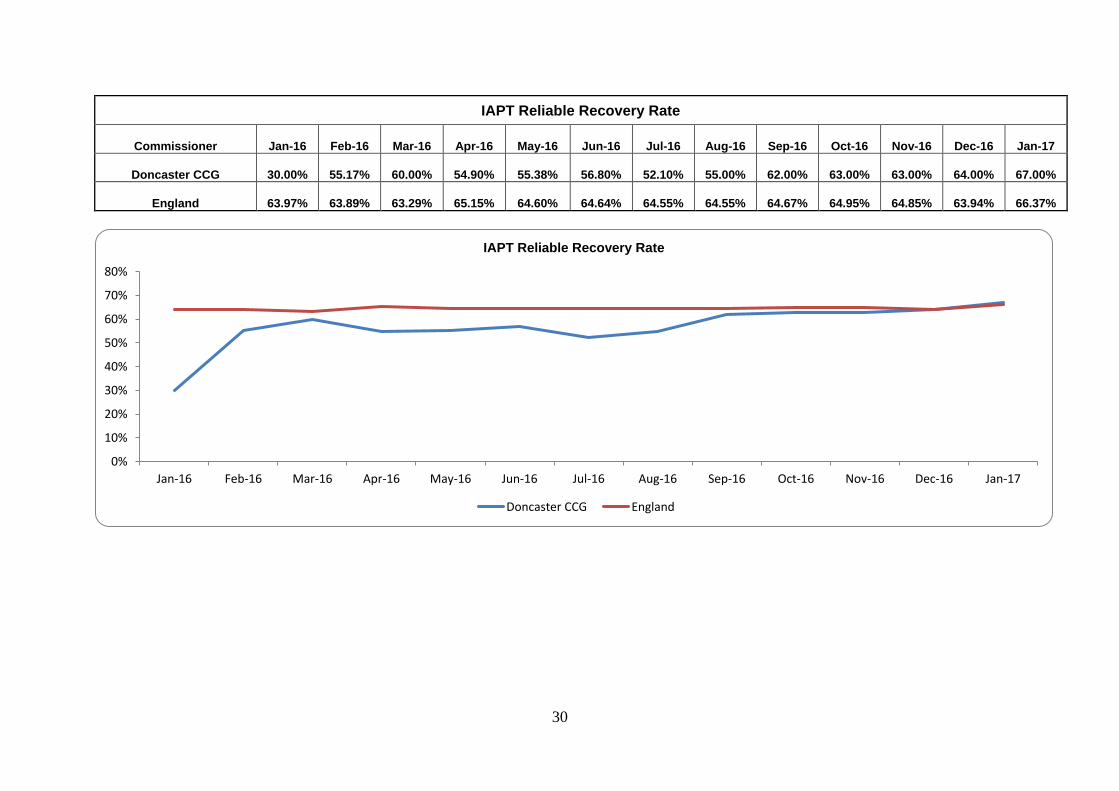
30
IAPT Reliable Recovery Rate
Commissioner Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17
Doncaster CCG 30.00% 55.17% 60.00% 54.90% 55.38% 56.80% 52.10% 55.00% 62.00% 63.00% 63.00% 64.00% 67.00%
England 63.97% 63.89% 63.29% 65.15% 64.60% 64.64% 64.55% 64.55% 64.67% 64.95% 64.85% 63.94% 66.37%
0%
10%
20%
30%
40%
50%
60%
70%
80%
Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17
IAPT Reliable Recovery Rate
Doncaster CCG England
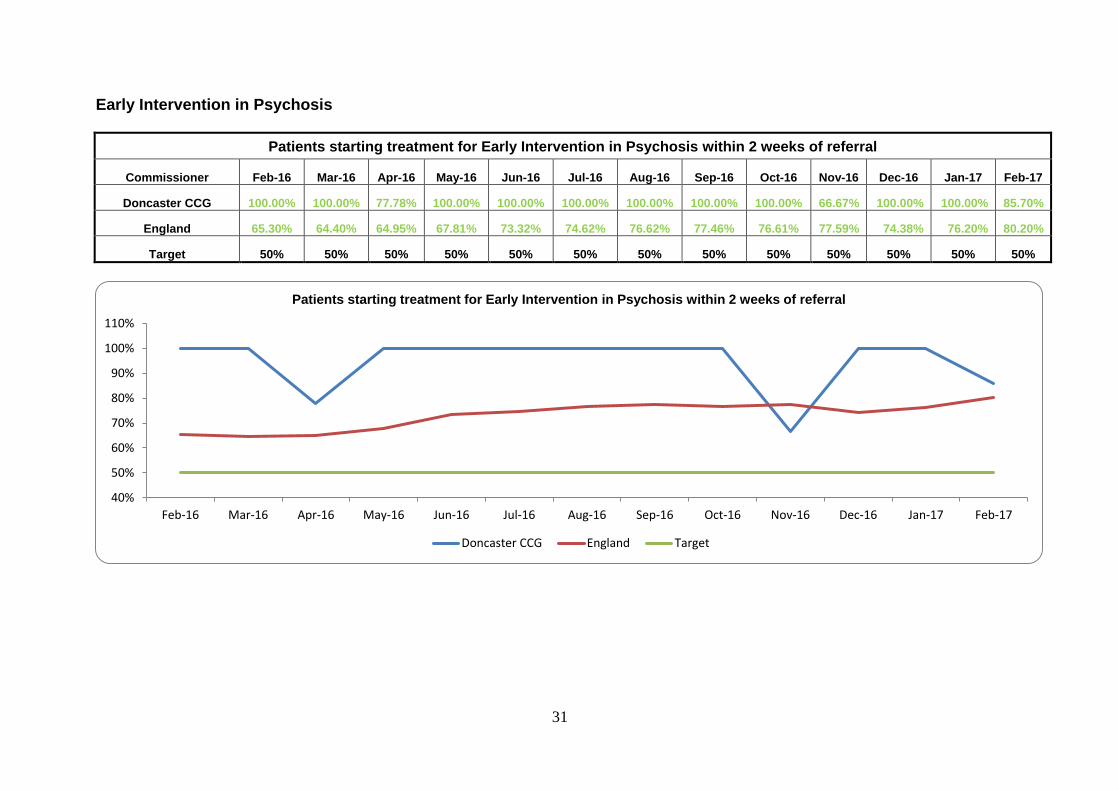
31
Early Intervention in Psychosis
Patients starting treatment for Early Intervention in Psychosis within 2 weeks of referral
Commissioner Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17
Doncaster CCG 100.00% 100.00% 77.78% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 66.67% 100.00% 100.00% 85.70%
England 65.30% 64.40% 64.95% 67.81% 73.32% 74.62% 76.62% 77.46% 76.61% 77.59% 74.38% 76.20% 80.20%
Target 50% 50% 50% 50% 50% 50% 50% 50% 50% 50% 50% 50% 50%
40%
50%
60%
70%
80%
90%
100%
110%
Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17
Patients starting treatment for Early Intervention in Psychosis within 2 weeks of referral
Doncaster CCG England Target
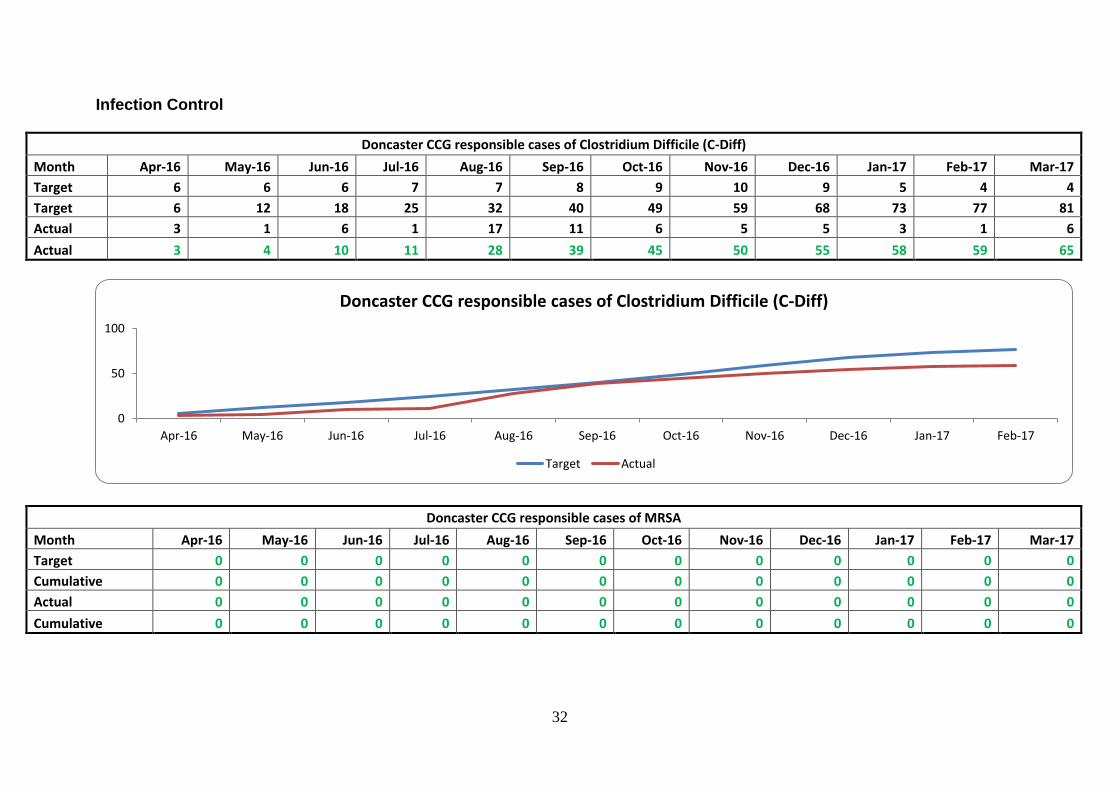
32
Infection Control
Doncaster CCG responsible cases of Clostridium Difficile (C-Diff)
Month Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17
Target 6 6 6 7 7 8 9 10 9 5 4 4
Target 6 12 18 25 32 40 49 59 68 73 77 81
Actual 3 1 6 1 17 11 6 5 5 3 1 6
Actual 3 4 10 11 28 39 45 50 55 58 59 65
Doncaster CCG responsible cases of MRSA
Month Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17
Target 0 0 0 0 0 0 0 0 0 0 0 0
Cumulative 0 0 0 0 0 0 0 0 0 0 0 0
Actual 0 0 0 0 0 0 0 0 0 0 0 0
Cumulative 0 0 0 0 0 0 0 0 0 0 0 0
0
50
100
Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17
Doncaster CCG responsible cases of Clostridium Difficile (C-Diff)
Target Actual
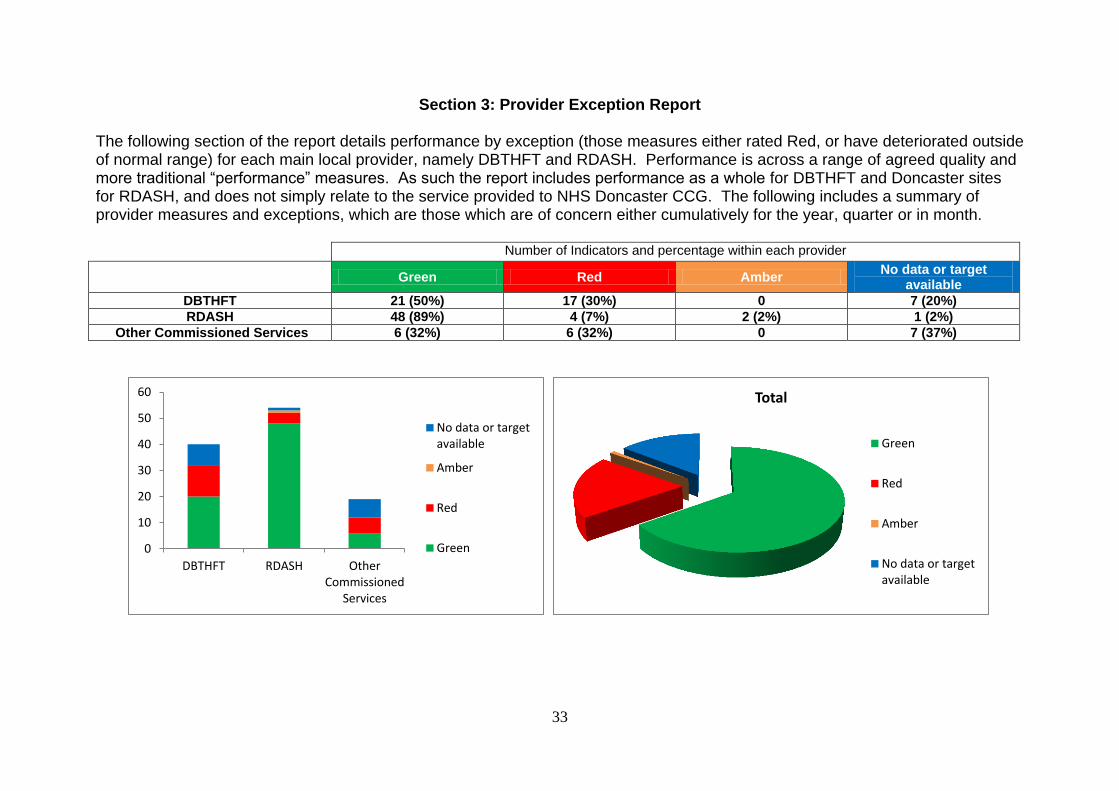
33
Section 3: Provider Exception Report
The following section of the report details performance by exception (those measures either rated Red, or have deteriorated outside of normal range) for each main local provider, namely DBTHFT and RDASH. Performance is across a range of agreed quality and more traditional “performance” measures. As such the report includes performance as a whole for DBTHFT and Doncaster sites for RDASH, and does not simply relate to the service provided to NHS Doncaster CCG. The following includes a summary of provider measures and exceptions, which are those which are of concern either cumulatively for the year, quarter or in month.
Number of Indicators and percentage within each provider
Green Red Amber
No data or target available
DBTHFT 21 (50%) 17 (30%) 0 7 (20%)
RDASH 48 (89%) 4 (7%) 2 (2%) 1 (2%)
Other Commissioned Services 6 (32%) 6 (32%) 0 7 (37%)
0
10
20
30
40
50
60
DBTHFT RDASH OtherCommissioned
Services
No data or targetavailable
Amber
Red
Green
Total
Green
Red
Amber
No data or targetavailable

34
3.1 Doncaster & Bassetlaw Teaching Hospitals NHS Foundation Trust: Exception Report
This section only includes those measures in the DBTHFT contract currently not meeting target, which are not covered by the constitution measures in Section 2. Handovers (ambulance to A&E) – no person waiting over 60 min
Handovers (ambulance to A&E) – no person waiting over 60 min
Provider Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17
DBTHFT 11 12 11 4 15 28 5 8 12 66 13 10
Target 0 0 0 0 0 0 0 0 0 0 0 0
Ambulance handovers over 60 minutes continued to improve during March 2017 with just 3 over an hour. Issues were down to both resuscitation patients and lack of medical staffing to handover to in ED.
0
10
20
30
40
50
60
70
Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17
Handovers (ambulance to DBTHFT A&E) – numbers waiting over 60 min
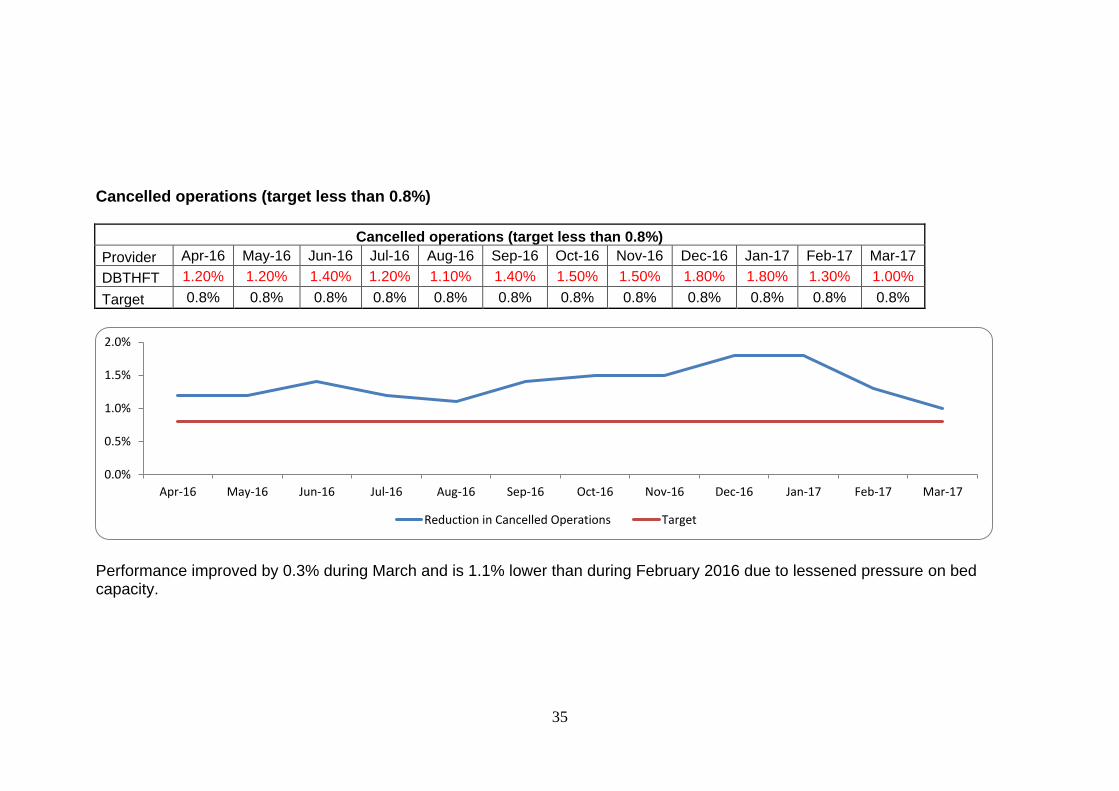
35
Cancelled operations (target less than 0.8%)
Cancelled operations (target less than 0.8%)
Provider Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17
DBTHFT 1.20% 1.20% 1.40% 1.20% 1.10% 1.40% 1.50% 1.50% 1.80% 1.80% 1.30% 1.00%
Target 0.8% 0.8% 0.8% 0.8% 0.8% 0.8% 0.8% 0.8% 0.8% 0.8% 0.8% 0.8%
Performance improved by 0.3% during March and is 1.1% lower than during February 2016 due to lessened pressure on bed capacity.
0.0%
0.5%
1.0%
1.5%
2.0%
Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17
Reduction in Cancelled Operations Target
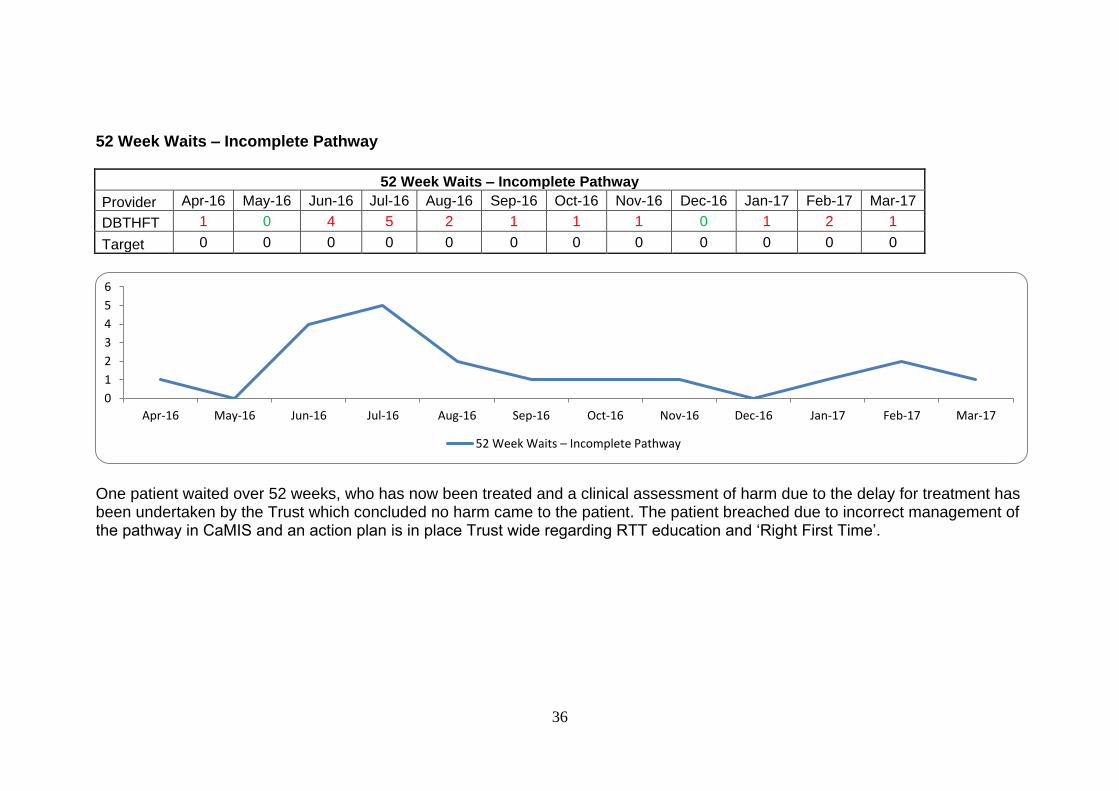
36
52 Week Waits – Incomplete Pathway
52 Week Waits – Incomplete Pathway
Provider Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17
DBTHFT 1 0 4 5 2 1 1 1 0 1 2 1
Target 0 0 0 0 0 0 0 0 0 0 0 0
One patient waited over 52 weeks, who has now been treated and a clinical assessment of harm due to the delay for treatment has been undertaken by the Trust which concluded no harm came to the patient. The patient breached due to incorrect management of the pathway in CaMIS and an action plan is in place Trust wide regarding RTT education and ‘Right First Time’.
0
1
2
3
4
5
6
Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17
52 Week Waits – Incomplete Pathway
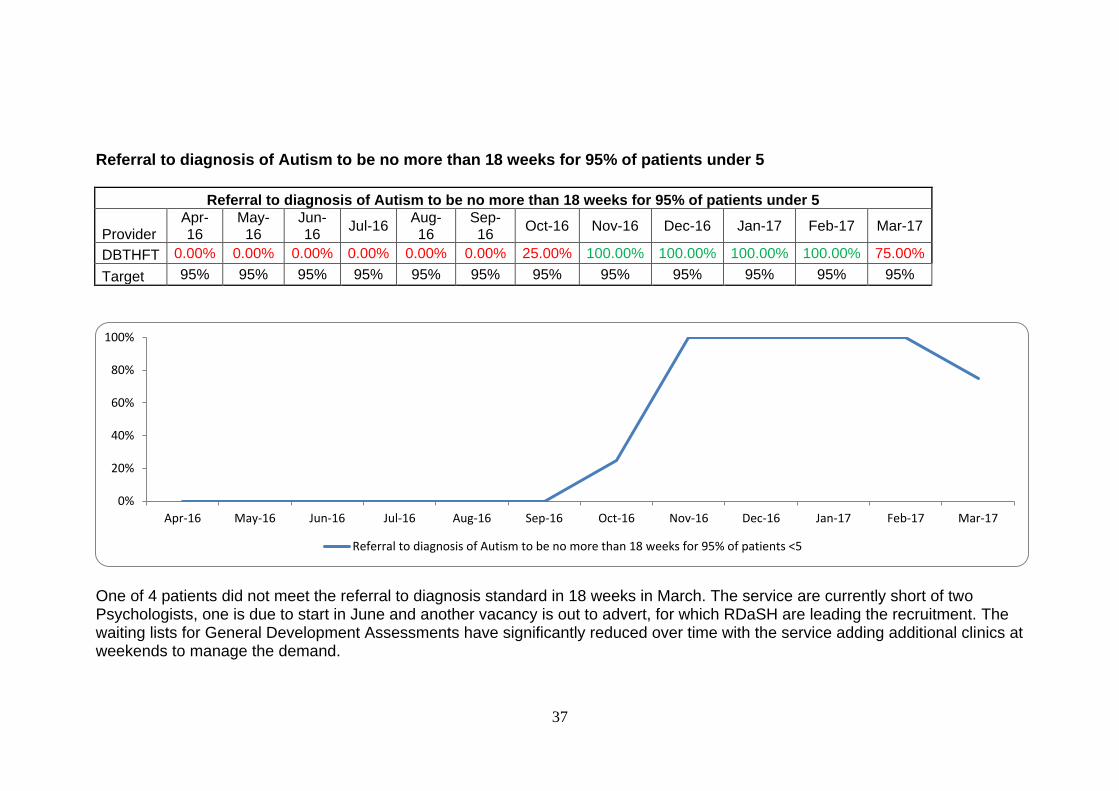
37
Referral to diagnosis of Autism to be no more than 18 weeks for 95% of patients under 5
Referral to diagnosis of Autism to be no more than 18 weeks for 95% of patients under 5
Provider Apr-16
May-16
Jun-16
Jul-16 Aug-16
Sep-16
Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17
DBTHFT 0.00% 0.00% 0.00% 0.00% 0.00% 0.00% 25.00% 100.00% 100.00% 100.00% 100.00% 75.00%
Target 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95%
One of 4 patients did not meet the referral to diagnosis standard in 18 weeks in March. The service are currently short of two Psychologists, one is due to start in June and another vacancy is out to advert, for which RDaSH are leading the recruitment. The waiting lists for General Development Assessments have significantly reduced over time with the service adding additional clinics at weekends to manage the demand.
0%
20%
40%
60%
80%
100%
Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17
Referral to diagnosis of Autism to be no more than 18 weeks for 95% of patients <5
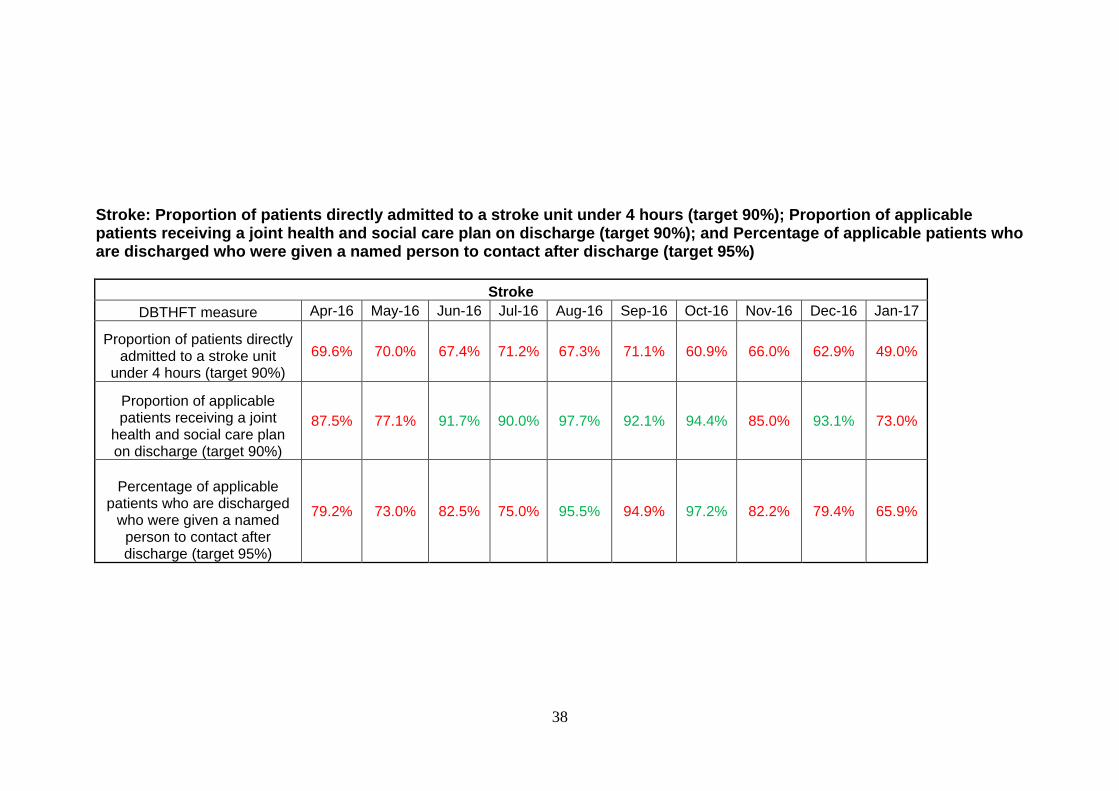
38
Stroke: Proportion of patients directly admitted to a stroke unit under 4 hours (target 90%); Proportion of applicable patients receiving a joint health and social care plan on discharge (target 90%); and Percentage of applicable patients who are discharged who were given a named person to contact after discharge (target 95%)
Stroke
DBTHFT measure Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17
Proportion of patients directly admitted to a stroke unit
under 4 hours (target 90%)
69.6% 70.0% 67.4% 71.2% 67.3% 71.1% 60.9% 66.0% 62.9% 49.0%
Proportion of applicable patients receiving a joint
health and social care plan on discharge (target 90%)
87.5% 77.1% 91.7% 90.0% 97.7% 92.1% 94.4% 85.0% 93.1% 73.0%
Percentage of applicable patients who are discharged
who were given a named person to contact after discharge (target 95%)
79.2% 73.0% 82.5% 75.0% 95.5% 94.9% 97.2% 82.2% 79.4% 65.9%
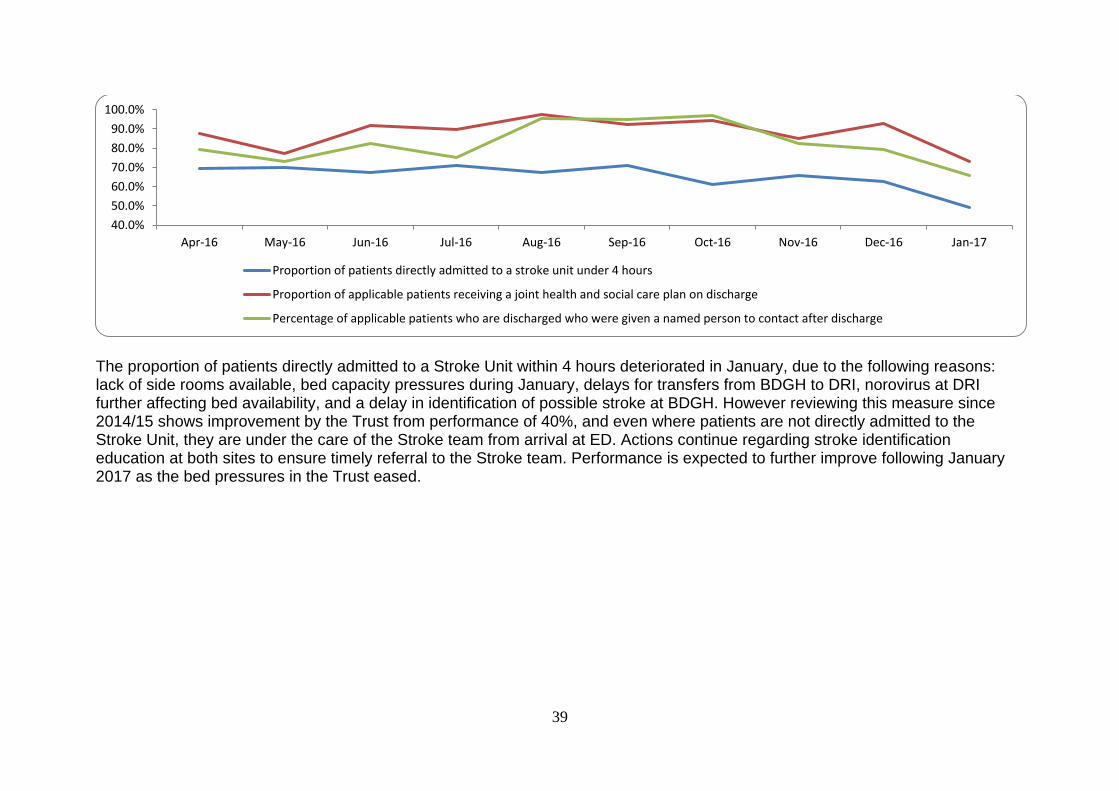
39
The proportion of patients directly admitted to a Stroke Unit within 4 hours deteriorated in January, due to the following reasons: lack of side rooms available, bed capacity pressures during January, delays for transfers from BDGH to DRI, norovirus at DRI further affecting bed availability, and a delay in identification of possible stroke at BDGH. However reviewing this measure since 2014/15 shows improvement by the Trust from performance of 40%, and even where patients are not directly admitted to the Stroke Unit, they are under the care of the Stroke team from arrival at ED. Actions continue regarding stroke identification education at both sites to ensure timely referral to the Stroke team. Performance is expected to further improve following January 2017 as the bed pressures in the Trust eased.
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17
Proportion of patients directly admitted to a stroke unit under 4 hours
Proportion of applicable patients receiving a joint health and social care plan on discharge
Percentage of applicable patients who are discharged who were given a named person to contact after discharge
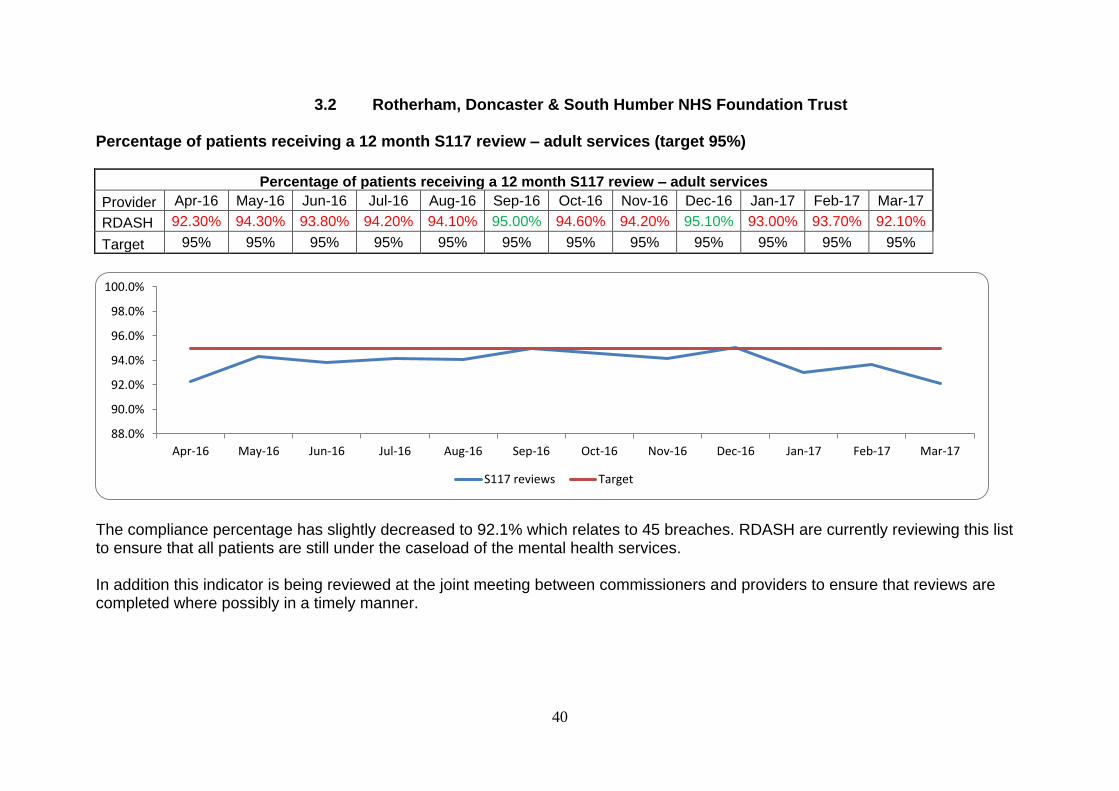
40
3.2 Rotherham, Doncaster & South Humber NHS Foundation Trust
Percentage of patients receiving a 12 month S117 review – adult services (target 95%)
Percentage of patients receiving a 12 month S117 review – adult services
Provider Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17
RDASH 92.30% 94.30% 93.80% 94.20% 94.10% 95.00% 94.60% 94.20% 95.10% 93.00% 93.70% 92.10%
Target 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95% 95%
The compliance percentage has slightly decreased to 92.1% which relates to 45 breaches. RDASH are currently reviewing this list to ensure that all patients are still under the caseload of the mental health services. In addition this indicator is being reviewed at the joint meeting between commissioners and providers to ensure that reviews are completed where possibly in a timely manner.
88.0%
90.0%
92.0%
94.0%
96.0%
98.0%
100.0%
Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17
S117 reviews Target
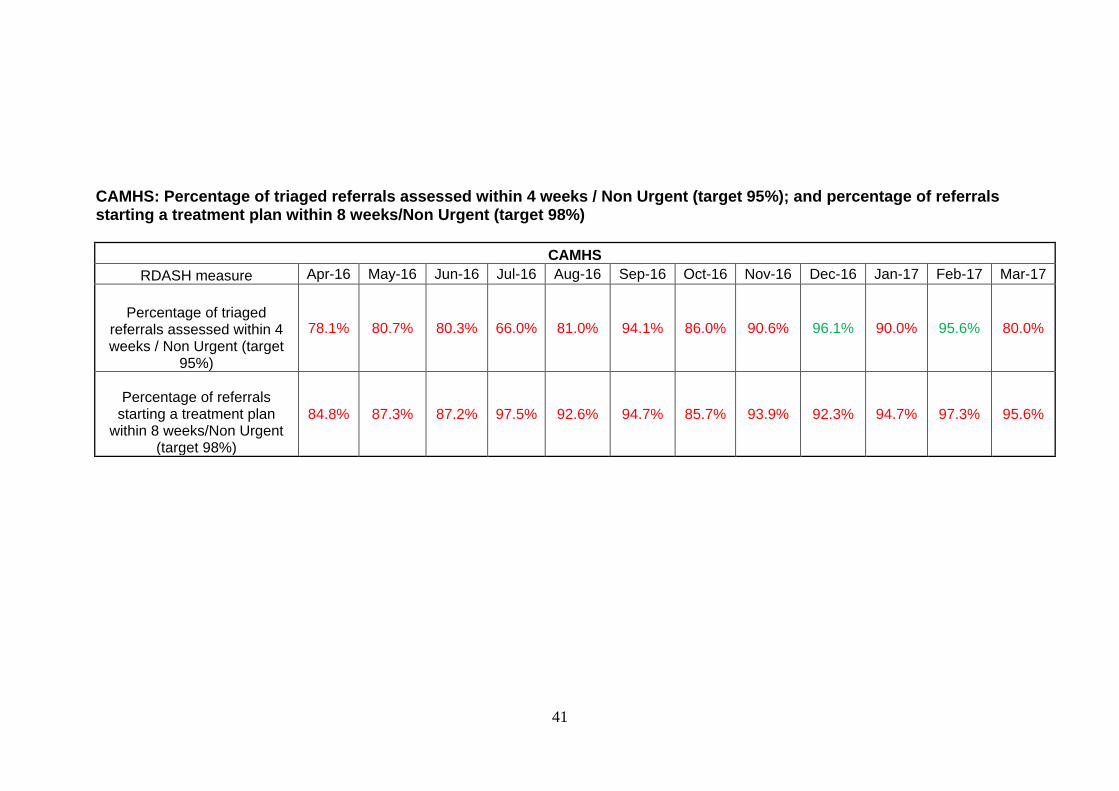
41
CAMHS: Percentage of triaged referrals assessed within 4 weeks / Non Urgent (target 95%); and percentage of referrals starting a treatment plan within 8 weeks/Non Urgent (target 98%)
CAMHS
RDASH measure Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17
Percentage of triaged referrals assessed within 4 weeks / Non Urgent (target
95%)
78.1% 80.7% 80.3% 66.0% 81.0% 94.1% 86.0% 90.6% 96.1% 90.0% 95.6% 80.0%
Percentage of referrals starting a treatment plan
within 8 weeks/Non Urgent (target 98%)
84.8% 87.3% 87.2% 97.5% 92.6% 94.7% 85.7% 93.9% 92.3% 94.7% 97.3% 95.6%
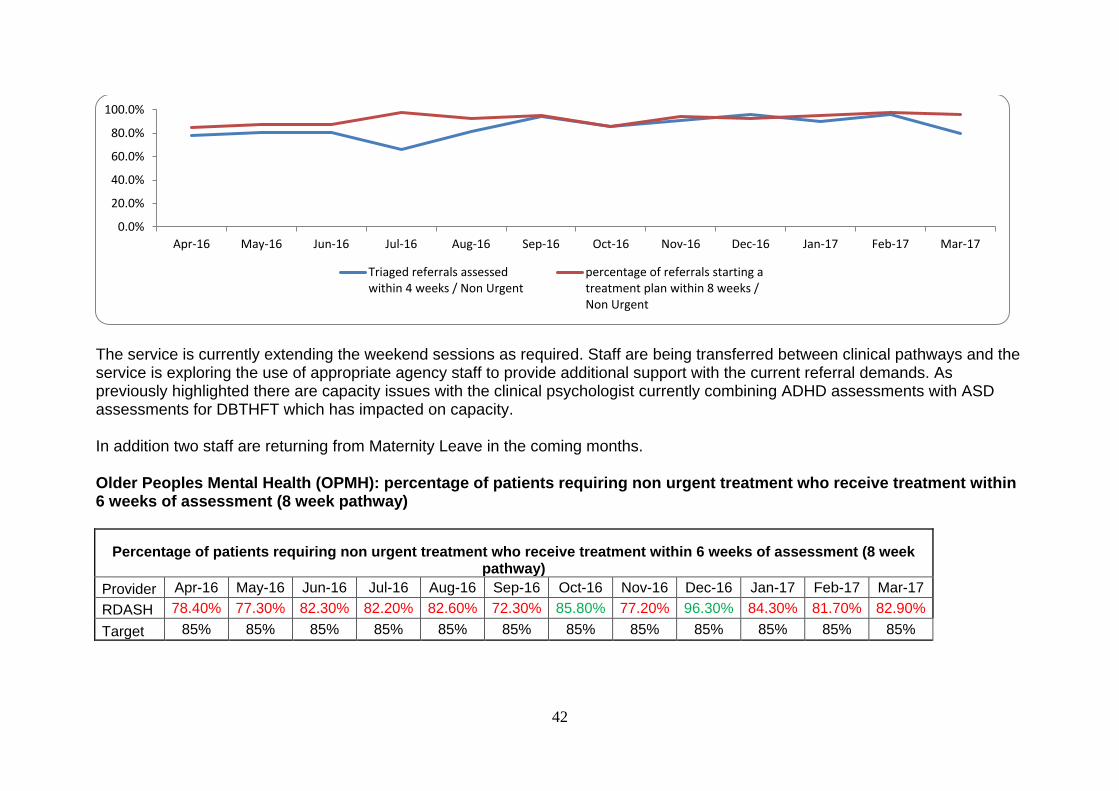
42
The service is currently extending the weekend sessions as required. Staff are being transferred between clinical pathways and the service is exploring the use of appropriate agency staff to provide additional support with the current referral demands. As previously highlighted there are capacity issues with the clinical psychologist currently combining ADHD assessments with ASD assessments for DBTHFT which has impacted on capacity. In addition two staff are returning from Maternity Leave in the coming months. Older Peoples Mental Health (OPMH): percentage of patients requiring non urgent treatment who receive treatment within 6 weeks of assessment (8 week pathway)
Percentage of patients requiring non urgent treatment who receive treatment within 6 weeks of assessment (8 week pathway)
Provider Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17
RDASH 78.40% 77.30% 82.30% 82.20% 82.60% 72.30% 85.80% 77.20% 96.30% 84.30% 81.70% 82.90%
Target 85% 85% 85% 85% 85% 85% 85% 85% 85% 85% 85% 85%
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17
Triaged referrals assessedwithin 4 weeks / Non Urgent
percentage of referrals starting atreatment plan within 8 weeks /Non Urgent
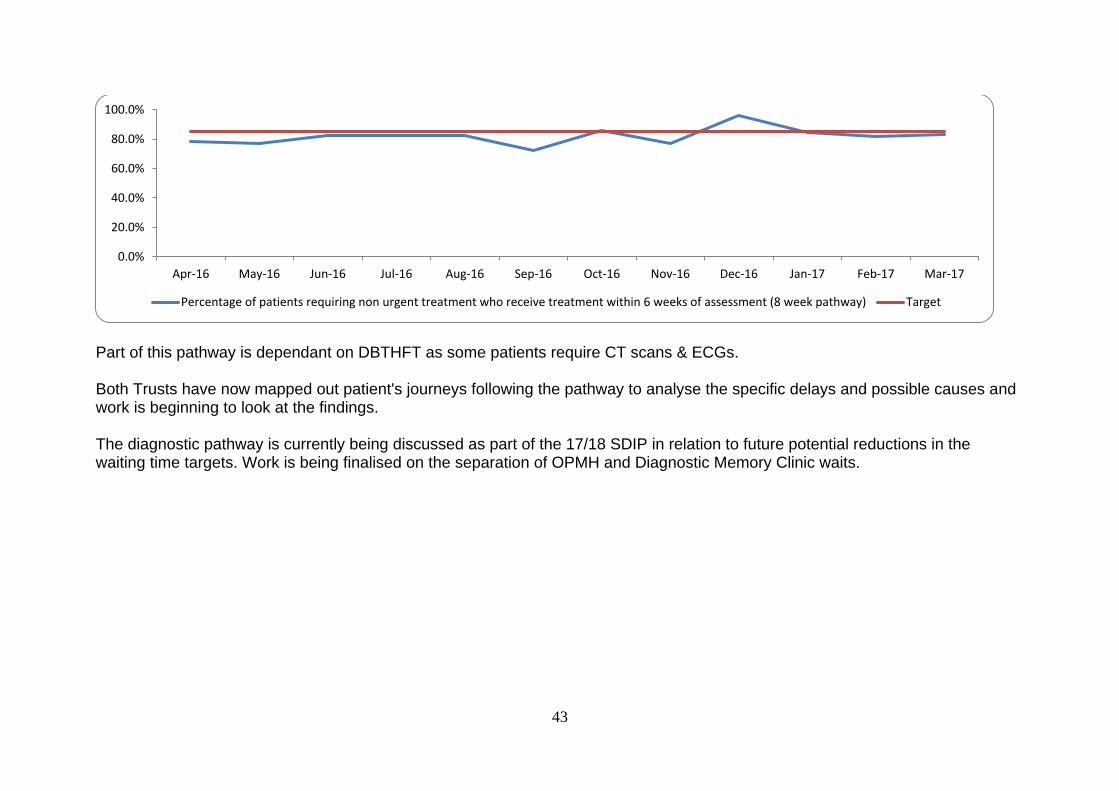
43
Part of this pathway is dependant on DBTHFT as some patients require CT scans & ECGs. Both Trusts have now mapped out patient's journeys following the pathway to analyse the specific delays and possible causes and work is beginning to look at the findings. The diagnostic pathway is currently being discussed as part of the 17/18 SDIP in relation to future potential reductions in the waiting time targets. Work is being finalised on the separation of OPMH and Diagnostic Memory Clinic waits.
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17
Percentage of patients requiring non urgent treatment who receive treatment within 6 weeks of assessment (8 week pathway) Target
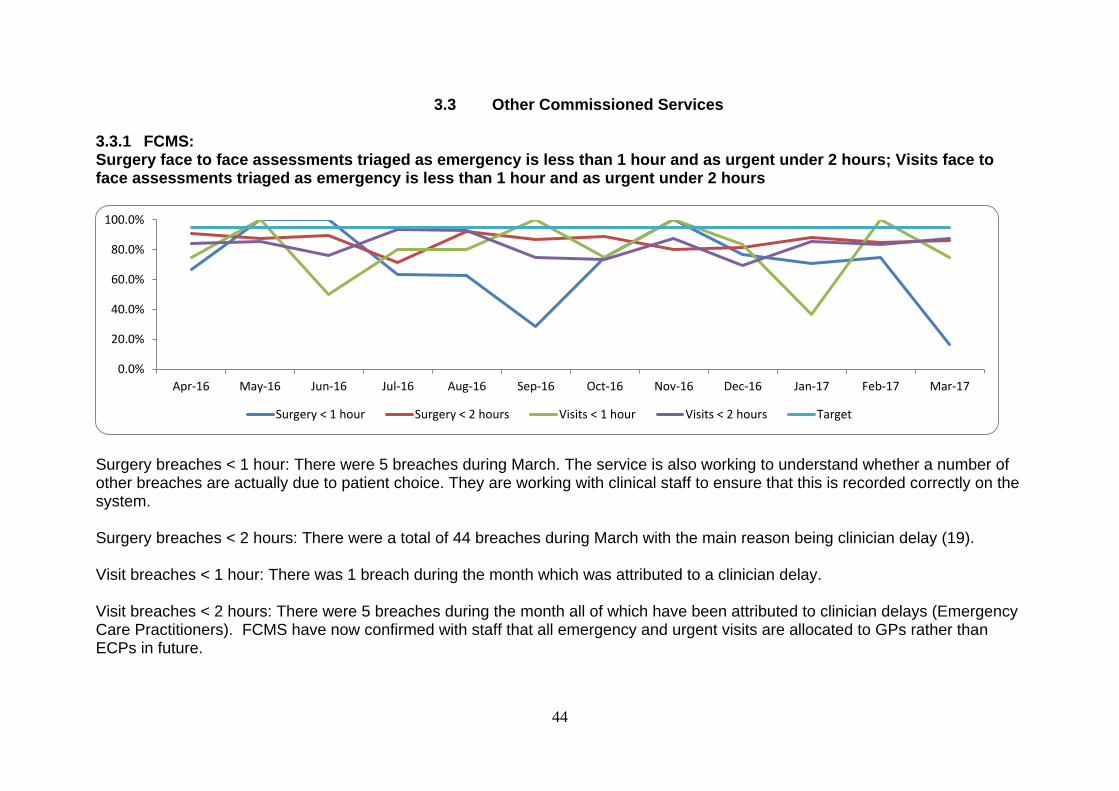
44
3.3 Other Commissioned Services
3.3.1 FCMS: Surgery face to face assessments triaged as emergency is less than 1 hour and as urgent under 2 hours; Visits face to face assessments triaged as emergency is less than 1 hour and as urgent under 2 hours
Surgery breaches < 1 hour: There were 5 breaches during March. The service is also working to understand whether a number of other breaches are actually due to patient choice. They are working with clinical staff to ensure that this is recorded correctly on the system. Surgery breaches < 2 hours: There were a total of 44 breaches during March with the main reason being clinician delay (19). Visit breaches < 1 hour: There was 1 breach during the month which was attributed to a clinician delay. Visit breaches < 2 hours: There were 5 breaches during the month all of which have been attributed to clinician delays (Emergency Care Practitioners). FCMS have now confirmed with staff that all emergency and urgent visits are allocated to GPs rather than ECPs in future.
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17
Surgery < 1 hour Surgery < 2 hours Visits < 1 hour Visits < 2 hours Target
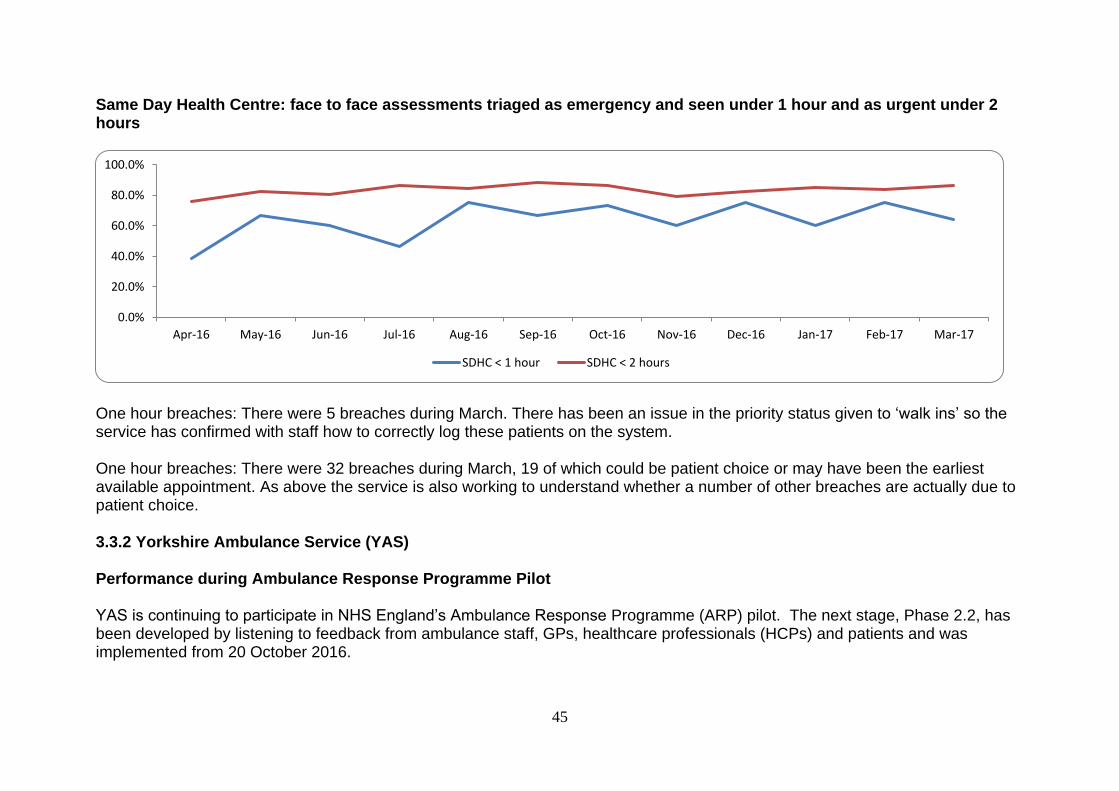
45
Same Day Health Centre: face to face assessments triaged as emergency and seen under 1 hour and as urgent under 2 hours
One hour breaches: There were 5 breaches during March. There has been an issue in the priority status given to ‘walk ins’ so the service has confirmed with staff how to correctly log these patients on the system.
One hour breaches: There were 32 breaches during March, 19 of which could be patient choice or may have been the earliest available appointment. As above the service is also working to understand whether a number of other breaches are actually due to patient choice.
3.3.2 Yorkshire Ambulance Service (YAS) Performance during Ambulance Response Programme Pilot
YAS is continuing to participate in NHS England’s Ambulance Response Programme (ARP) pilot. The next stage, Phase 2.2, has been developed by listening to feedback from ambulance staff, GPs, healthcare professionals (HCPs) and patients and was implemented from 20 October 2016.
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17
SDHC < 1 hour SDHC < 2 hours
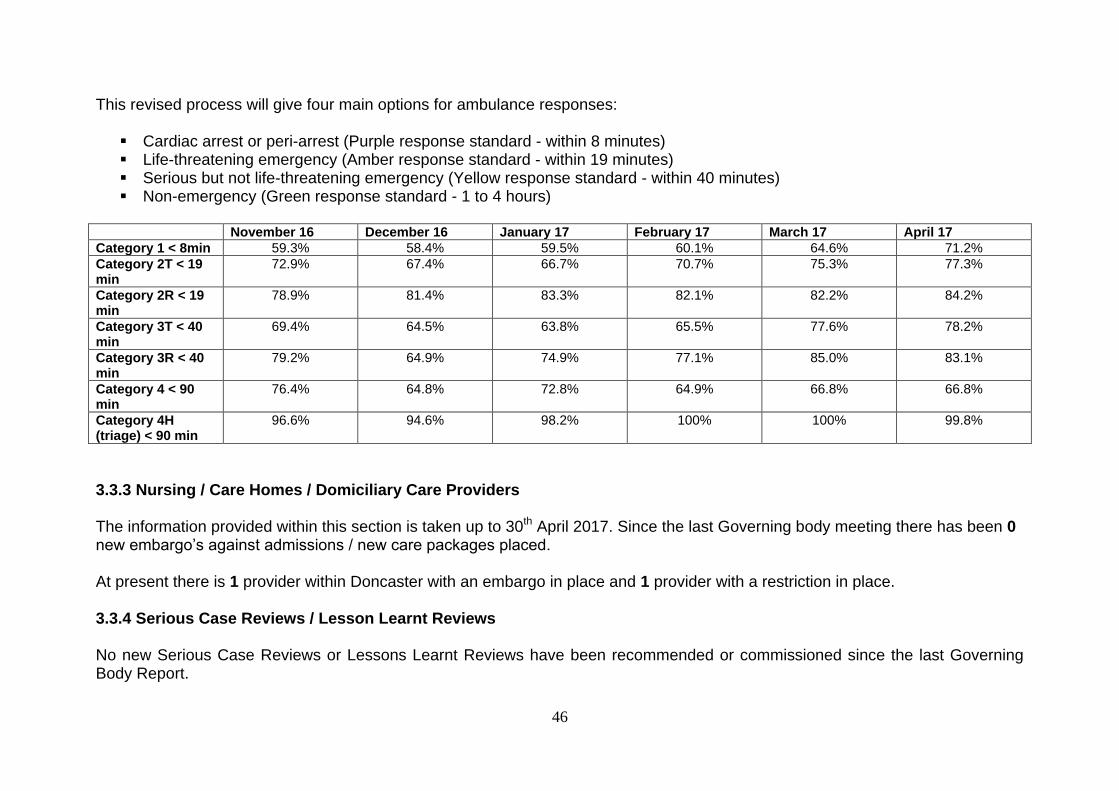
46
This revised process will give four main options for ambulance responses:
Cardiac arrest or peri-arrest (Purple response standard - within 8 minutes) Life-threatening emergency (Amber response standard - within 19 minutes) Serious but not life-threatening emergency (Yellow response standard - within 40 minutes) Non-emergency (Green response standard - 1 to 4 hours)
November 16 December 16 January 17 February 17 March 17 April 17
Category 1 < 8min 59.3% 58.4% 59.5% 60.1% 64.6% 71.2%
Category 2T < 19 min
72.9% 67.4% 66.7% 70.7% 75.3% 77.3%
Category 2R < 19 min
78.9% 81.4% 83.3% 82.1% 82.2% 84.2%
Category 3T < 40 min
69.4% 64.5% 63.8% 65.5% 77.6% 78.2%
Category 3R < 40 min
79.2% 64.9% 74.9% 77.1% 85.0% 83.1%
Category 4 < 90 min
76.4% 64.8% 72.8% 64.9% 66.8% 66.8%
Category 4H (triage) < 90 min
96.6% 94.6% 98.2% 100% 100% 99.8%
3.3.3 Nursing / Care Homes / Domiciliary Care Providers
The information provided within this section is taken up to 30th April 2017. Since the last Governing body meeting there has been 0 new embargo’s against admissions / new care packages placed.
At present there is 1 provider within Doncaster with an embargo in place and 1 provider with a restriction in place.
3.3.4 Serious Case Reviews / Lesson Learnt Reviews No new Serious Case Reviews or Lessons Learnt Reviews have been recommended or commissioned since the last Governing Body Report.
47
3.3.5 Domestic Homicide Reviews
There was a Domestic Homicide Review commissioned in November 2016. The initial meeting for this review has been held and an independent chair has been commissioned. The GP records for this review have now been obtained from Capita. The health input into this case is minimal therefore a summary is required rather than a full Individual Management Review. The deadline for completion is the end of June 2017.
A further Domestic Homicide Review was commissioned in March 2017. The initial meeting has been held and an independent chair has been commissioned. It has been agreed that the chair for both Domestic Homicide Reviews will be the same person in order for the reviews to run in parallel. The GP records for this review have been received. The health input into this case is minimal therefore a summary is required rather than a full Individual Management Review. The deadline for completion is the end of June 2017.

Enc C
Item 8
Finance Report

1
Meeting name Governing Body
Meeting date 18 May 2017
Title of paper
2016/17 Finance Report March 2017 (Month 12)
Executive / Clinical Lead(s)
Hayley Tingle, Chief Finance Officer
Author(s) Tracy Wyatt, Deputy Chief Finance Officer
Purpose of Paper - Executive Summary
This report sets out the financial position as at the end of March 2017. The CCG has achieved all of its financial targets for 2016/17. The report also outlines:
The key risk areas identified for 2016/17
A summary of the CCG Efficiency Savings for 2016/17 (Appendix 2)
A summary of the CCG’s Resource Allocation (Appendix 3)
A summary of the CCG’s Reserve position (Appendix 4)
Recommendation(s)
Members are asked to:
Receive the report and note the financial position for 2016/17
2
Impact analysis
Quality impact
None identified
Equality impact
None identified
Sustainability impact
Nil
Financial implications
As highlighted within the report
Legal implications
None identified
Management of Conflicts of Interest
None Identified
Consultation /
Engagement (internal
departments, clinical, stakeholder
& public/patient)
N/A
Report previously
presented at None
Risk analysis
The CCG identified a number of risks as part of the Financial planning for 2016/17. These included:
Prescribing and High Cost Drugs Expenditure
Over performance against the main acute contracts
Individual Placements
Non delivery of parts of the Efficiency Savings programme
A small contingency fund which equated to 0.5% of the CCG’s allocation was set aside to mitigate against these risks as required by the business rules. It has not been possible to flex investment reserves due to the national ring fencing of the 1% headroom. The CCG has managed to contain the risks within its allocation and achieved all of its financial targets.
Assurance Framework
3.2, 3.3, 3.4
3
NHS DONCASTER CCG 2016/17 FINANCE REPORT MONTH 12 – MARCH 2017 1. Introduction
This report provides the financial position for NHS Doncaster CCG for 2016/17 as at the end of March (Month 12). The CCG has achieved all of its financial targets for 2016/17. 2. Current Position The year end position reflects a surplus of £12,580k which is £4,858k greater than the target of £7,722k. As set out in the 2016/17 NHS Planning Guidance, CCGs were required to hold a 1 per cent reserve uncommitted from the start of the year, created by setting aside the monies that CCGs were otherwise required to spend non-recurrently. This was intended to be released for investment in Five Year Forward View transformation priorities to the extent that evidence emerged of risks not arising or being effectively mitigated through other means. In the event, the national position across the provider sector has been such that NHS England has been unable to allow CCGs’ 1% non-recurrent monies to be spent. Therefore, to comply with this requirement, NHS Doncaster CCG has released its 1% reserve to the bottom line, resulting in the additional surplus for the year of £4.8m. This additional surplus will be carried forward for drawdown in future years. The final year end position is summarised in the Operating Cost Statement included at Appendix 1. 3. Key Messages and Risks
The largest financial risks identified as part of the Financial Planning process were Prescribing and High Cost Drugs. Work to address the variations in both outcomes and costs were taken forward as part of the Primary Care Strategy, specifically the medicine optimisation work. A prior approval process was initiated with the Acute Trust and implemented from 1st April 2016; this was to address any non-compliance with NICE guidance and correct charging through the PbR tariff mechanism. This has had a positive impact on costs. Other risks identified include the over performance on acute contracts, increased Individual placements ( including Continuing Healthcare , Specialist Placement and Section 117 packages) and the non-delivery of parts of the efficiency savings. The pressures around Emergency and A&E activity have continued within the DBTH contract, and the contract over performed by £1.2m. This reflected a reduction to the forecast position due to a technical year end adjustment in relation to Antenatal Work in progress.
4
Some of the smaller contracts also over performed including Sheffield Teaching Hospitals (£640k), Sheffield Children’s (£150k) and Leeds Teaching Hospitals (£138k). There have also been pressures in relation to S117 and Specialist Placement activity due to increased activity levels and cases being stepped down from NHS England, however some of this has been offset by a reduction in Continuing Healthcare costs. An additional risk arose in year in relation to the nationally agreed rates for Funded Nursing Care (FNC) which caused an additional cost pressure of approximately £600k. Following a national review, the rate increased by 39% from £112 per week to £156.25 per week; the CCG has had no choice but to implement this rate. The further national review on the agency element of the FNC has now been completed and had no further impact in 2016/17. However a slight reduction to the rate has been agreed with effect from 1st April 2017 to £155.05. To help manage and offset the risks a small contingency fund of £2.2m was established as part of planning. This equated to 0.5% of the CCG’s allocation and was in line with planning guidance. In previous years flexing of investment funds have supported mitigation to manage unexpected risks however this was not an option for 2016/17. Despite the above risks the CCG has managed to contain the pressures outlined above within its allocation. 4. Efficiency Savings Programme
All contract values negotiated with providers were net of efficiency saving targets Appendix 2. The Prescribing LES scheme was launched earlier in the year and all practices signed up to the scheme which started in August. The scheme aimed to reduce overall spend across several areas of prescribing and rewarded practices with a percentage of the savings made. Information is not yet available for March due to the two month delay in BSA reporting, however information received so far indicates that savings are minimal. A final report will be taken to the Primary Care Committee and detailed practice level information will be shared in June. Savings have materialised overall in the prescribing budget as it was set net of a £5.1m efficiency target and overspent of £2.4m at year end. However most of these savings are fortuitous and are linked to the nationally determined Cat M prices and also other national price changes. The volume of items prescribed has actually increased by 3% on last year. Savings have also materialised in the DBH contract in relation to High Cost Drugs due to the impact of transferring patients onto bio-similars and the prior approval processes. There are also some savings against other elements of the contract due to activity being lower than expected in some areas, mainly outpatients, audiology and critical care. This equates to approximately £1.5m for the year.
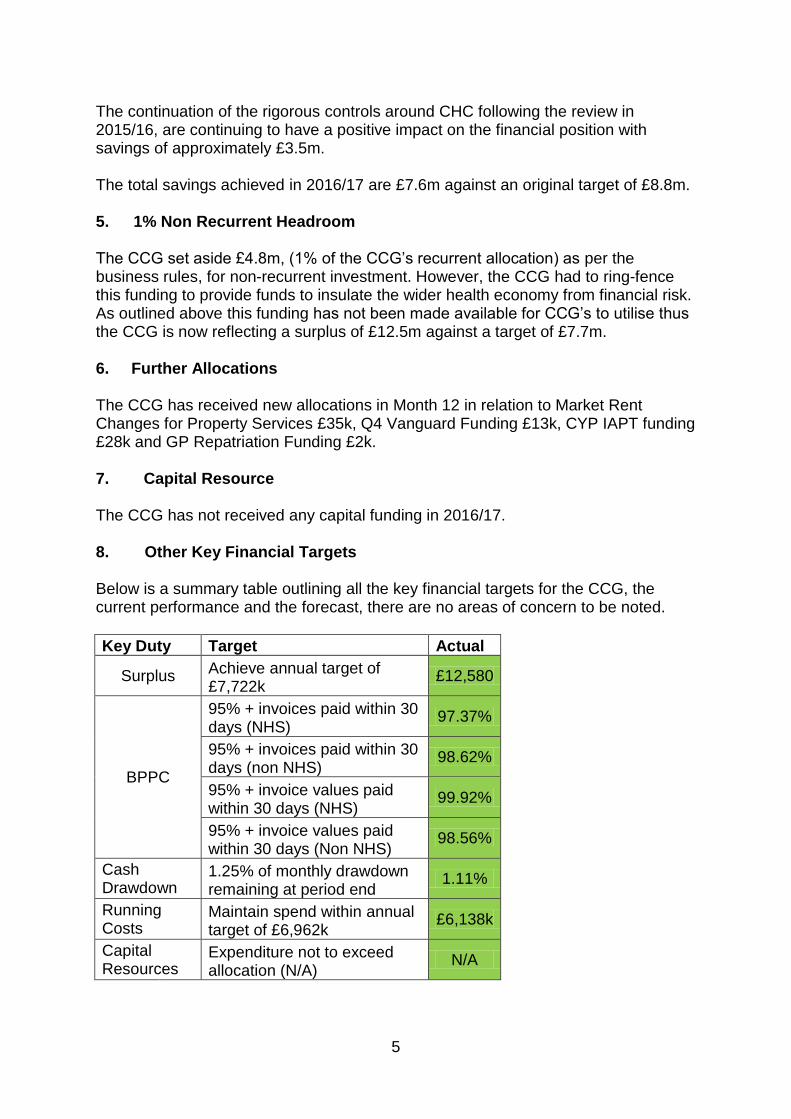
5
The continuation of the rigorous controls around CHC following the review in 2015/16, are continuing to have a positive impact on the financial position with savings of approximately £3.5m. The total savings achieved in 2016/17 are £7.6m against an original target of £8.8m. 5. 1% Non Recurrent Headroom The CCG set aside £4.8m, (1% of the CCG’s recurrent allocation) as per the business rules, for non-recurrent investment. However, the CCG had to ring-fence this funding to provide funds to insulate the wider health economy from financial risk. As outlined above this funding has not been made available for CCG’s to utilise thus the CCG is now reflecting a surplus of £12.5m against a target of £7.7m. 6. Further Allocations The CCG has received new allocations in Month 12 in relation to Market Rent Changes for Property Services £35k, Q4 Vanguard Funding £13k, CYP IAPT funding £28k and GP Repatriation Funding £2k. 7. Capital Resource
The CCG has not received any capital funding in 2016/17. 8. Other Key Financial Targets Below is a summary table outlining all the key financial targets for the CCG, the current performance and the forecast, there are no areas of concern to be noted.
Key Duty Target Actual
Surplus Achieve annual target of £7,722k
£12,580
BPPC
95% + invoices paid within 30 days (NHS)
97.37%
95% + invoices paid within 30 days (non NHS)
98.62%
95% + invoice values paid within 30 days (NHS)
99.92%
95% + invoice values paid within 30 days (Non NHS)
98.56%
Cash Drawdown
1.25% of monthly drawdown remaining at period end
1.11%
Running Costs
Maintain spend within annual target of £6,962k
£6,138k
Capital Resources
Expenditure not to exceed allocation (N/A)
N/A
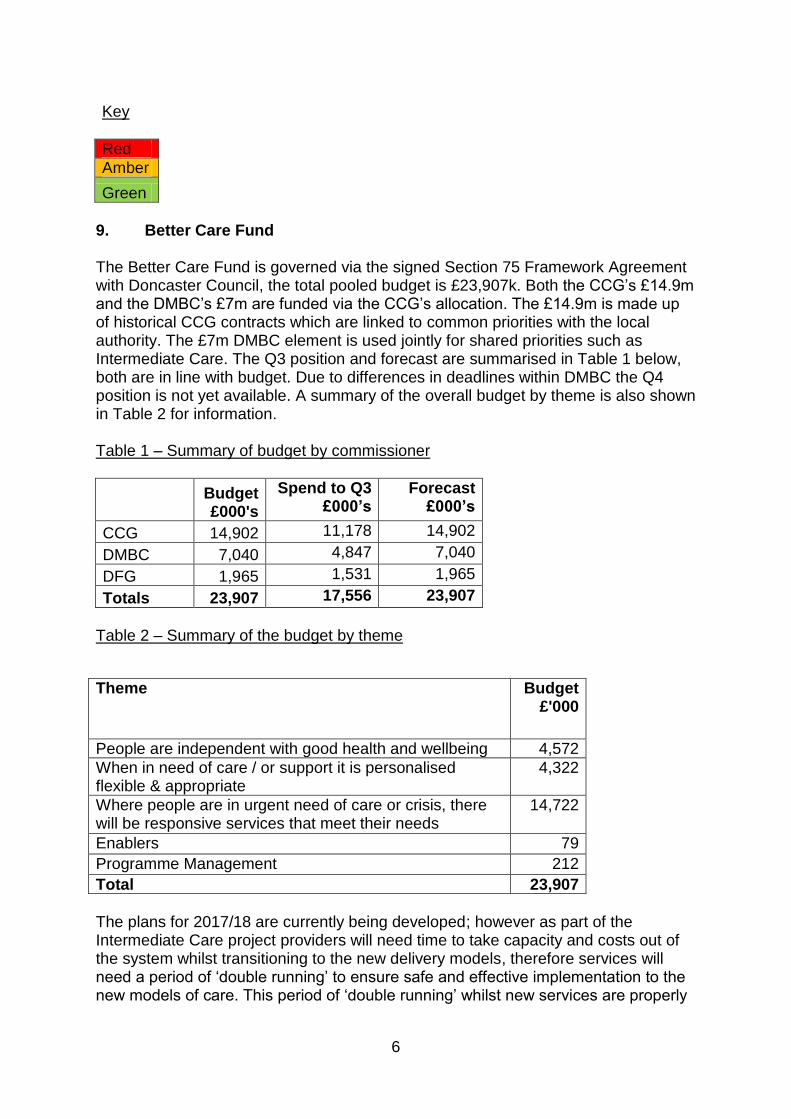
6
Key
Red
Amber
Green
9. Better Care Fund The Better Care Fund is governed via the signed Section 75 Framework Agreement with Doncaster Council, the total pooled budget is £23,907k. Both the CCG’s £14.9m and the DMBC’s £7m are funded via the CCG’s allocation. The £14.9m is made up of historical CCG contracts which are linked to common priorities with the local authority. The £7m DMBC element is used jointly for shared priorities such as Intermediate Care. The Q3 position and forecast are summarised in Table 1 below, both are in line with budget. Due to differences in deadlines within DMBC the Q4 position is not yet available. A summary of the overall budget by theme is also shown in Table 2 for information. Table 1 – Summary of budget by commissioner
Budget £000's
Spend to Q3 £000’s
Forecast £000’s
CCG 14,902 11,178 14,902
DMBC 7,040 4,847 7,040
DFG 1,965 1,531 1,965
Totals 23,907 17,556 23,907
Table 2 – Summary of the budget by theme
Theme Budget £'000
People are independent with good health and wellbeing 4,572
When in need of care / or support it is personalised flexible & appropriate
4,322
Where people are in urgent need of care or crisis, there will be responsive services that meet their needs
14,722
Enablers 79
Programme Management 212
Total 23,907
The plans for 2017/18 are currently being developed; however as part of the Intermediate Care project providers will need time to take capacity and costs out of the system whilst transitioning to the new delivery models, therefore services will need a period of ‘double running’ to ensure safe and effective implementation to the new models of care. This period of ‘double running’ whilst new services are properly
7
established and appropriately staffed is critical to the success of the transformation programme and the BCF will be used to support this. 10. Primary Medical Care Delegated Commissioning The CCG assumed devolved responsibility for Primary Medical Care commissioning with effect from April 2016. The total allocation devolved from NHS England was £41m and expenditure is currently forecast to be contained within this budget. The financial position will be discussed regularly at the Primary Care Committee including developments for 2017/18 and implementation of the Primary Care Forward View. The CCG is currently developing an offer of a non-financial support package for vulnerable practices to enable them to become sustainable for the future. This will be taken forward through the Primary Care Committee. 11. Conclusion and Recommendations Members are asked to: Receive and note the Finance Report for March 2017 (Month 12).

8
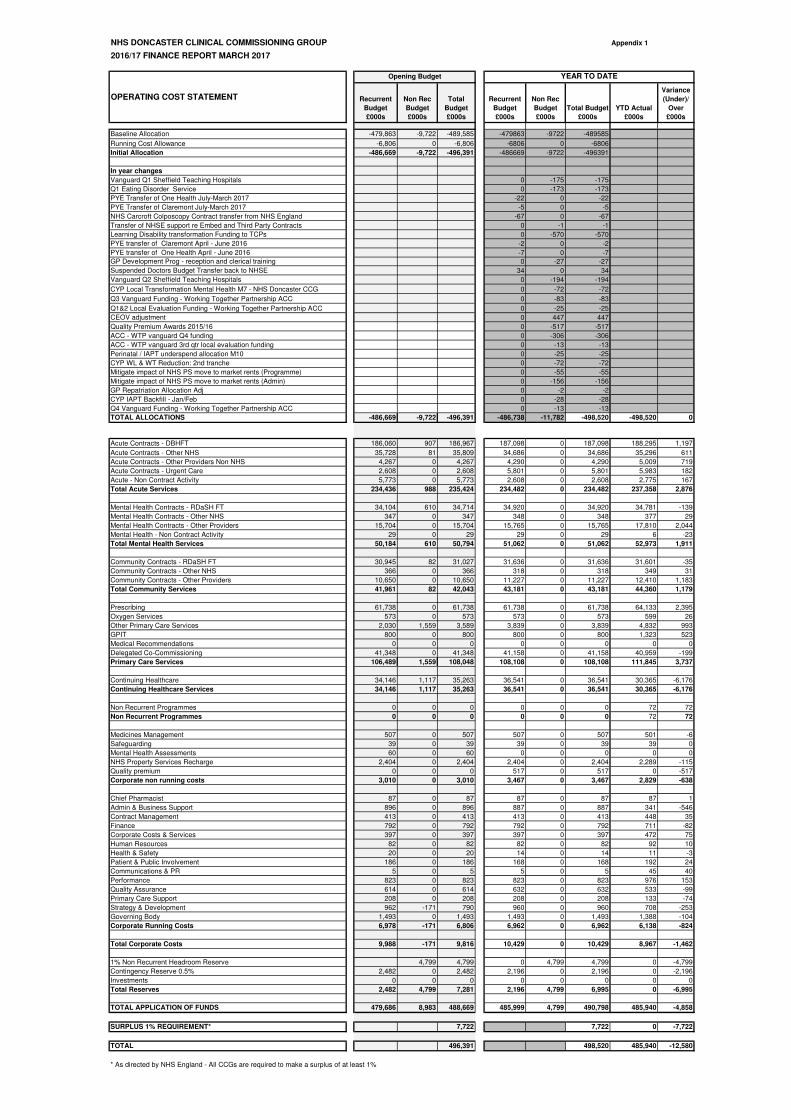
NHS DONCASTER CLINICAL COMMISSIONING GROUP Appendix 1
2016/17 FINANCE REPORT MARCH 2017
Recurrent
Budget
£000s
Non Rec
Budget
£000s
Total
Budget
£000s
Recurrent
Budget
£000s
Non Rec
Budget
£000s
Total Budget
£000s
YTD Actual
£000s
Variance
(Under)/
Over
£000s
Baseline Allocation -479,863 -9,722 -489,585 -479863 -9722 -489585
Running Cost Allowance -6,806 0 -6,806 -6806 0 -6806
Initial Allocation -486,669 -9,722 -496,391 -486669 -9722 -496391
In year changes
Vanguard Q1 Sheffield Teaching Hospitals 0 -175 -175
Q1 Eating Disorder Service 0 -173 -173
PYE Transfer of One Health July-March 2017 -22 0 -22
PYE Transfer of Claremont July-March 2017 -5 0 -5
NHS Carcroft Colposcopy Contract transfer from NHS England -67 0 -67
Transfer of NHSE support re Embed and Third Party Contracts 0 -1 -1
Learning Disability transformation Funding to TCPs 0 -570 -570
PYE transfer of Claremont April - June 2016 -2 0 -2
PYE transfer of One Health April - June 2016 -7 0 -7
GP Development Prog - reception and clerical training 0 -27 -27
Suspended Doctors Budget Transfer back to NHSE 34 0 34
Vanguard Q2 Sheffield Teaching Hospitals 0 -194 -194
CYP Local Transformation Mental Health M7 - NHS Doncaster CCG 0 -72 -72
Q3 Vanguard Funding - Working Together Partnership ACC 0 -83 -83
Q1&2 Local Evaluation Funding - Working Together Partnership ACC 0 -25 -25
CEOV adjustment 0 447 447
Quality Premium Awards 2015/16 0 -517 -517
ACC - WTP vanguard Q4 funding 0 -306 -306
ACC - WTP vanguard 3rd qtr local evaluation funding 0 -13 -13
Perinatal / IAPT underspend allocation M10 0 -25 -25
CYP WL & WT Reduction: 2nd tranche 0 -72 -72
Mitigate impact of NHS PS move to market rents (Programme) 0 -55 -55
Mitigate impact of NHS PS move to market rents (Admin) 0 -156 -156
GP Repatriation Allocation Adj 0 -2 -2
CYP IAPT Backfill - Jan/Feb 0 -28 -28
Q4 Vanguard Funding - Working Together Partnership ACC 0 -13 -13
TOTAL ALLOCATIONS -486,669 -9,722 -496,391 -486,738 -11,782 -498,520 -498,520 0
Acute Contracts - DBHFT 186,060 907 186,967 187,098 0 187,098 188,295 1,197
Acute Contracts - Other NHS 35,728 81 35,809 34,686 0 34,686 35,296 611
Acute Contracts - Other Providers Non NHS 4,267 0 4,267 4,290 0 4,290 5,009 719
Acute Contracts - Urgent Care 2,608 0 2,608 5,801 0 5,801 5,983 182
Acute - Non Contract Activity 5,773 0 5,773 2,608 0 2,608 2,775 167
Total Acute Services 234,436 988 235,424 234,482 0 234,482 237,358 2,876
Mental Health Contracts - RDaSH FT 34,104 610 34,714 34,920 0 34,920 34,781 -139
Mental Health Contracts - Other NHS 347 0 347 348 0 348 377 29
Mental Health Contracts - Other Providers 15,704 0 15,704 15,765 0 15,765 17,810 2,044
Mental Health - Non Contract Activity 29 0 29 29 0 29 6 -23
Total Mental Health Services 50,184 610 50,794 51,062 0 51,062 52,973 1,911
Community Contracts - RDaSH FT 30,945 82 31,027 31,636 0 31,636 31,601 -35
Community Contracts - Other NHS 366 0 366 318 0 318 349 31
Community Contracts - Other Providers 10,650 0 10,650 11,227 0 11,227 12,410 1,183
Total Community Services 41,961 82 42,043 43,181 0 43,181 44,360 1,179
Prescribing 61,738 0 61,738 61,738 0 61,738 64,133 2,395
Oxygen Services 573 0 573 573 0 573 599 26
Other Primary Care Services 2,030 1,559 3,589 3,839 0 3,839 4,832 993
GPIT 800 0 800 800 0 800 1,323 523
Medical Recommendations 0 0 0 0 0 0 0 0
Delegated Co-Commissioning 41,348 0 41,348 41,158 0 41,158 40,959 -199
Primary Care Services 106,489 1,559 108,048 108,108 0 108,108 111,845 3,737
Continuing Healthcare 34,146 1,117 35,263 36,541 0 36,541 30,365 -6,176
Continuing Healthcare Services 34,146 1,117 35,263 36,541 0 36,541 30,365 -6,176
Non Recurrent Programmes 0 0 0 0 0 0 72 72
Non Recurrent Programmes 0 0 0 0 0 0 72 72
Medicines Management 507 0 507 507 0 507 501 -6
Safeguarding 39 0 39 39 0 39 39 0
Mental Health Assessments 60 0 60 0 0 0 0 0
NHS Property Services Recharge 2,404 0 2,404 2,404 0 2,404 2,289 -115
Quality premium 0 0 0 517 0 517 0 -517
Corporate non running costs 3,010 0 3,010 3,467 0 3,467 2,829 -638
Chief Pharmacist 87 0 87 87 0 87 87 1
Admin & Business Support 896 0 896 887 0 887 341 -546
Contract Management 413 0 413 413 0 413 448 35
Finance 792 0 792 792 0 792 711 -82
Corporate Costs & Services 397 0 397 397 0 397 472 75
Human Resources 82 0 82 82 0 82 92 10
Health & Safety 20 0 20 14 0 14 11 -3
Patient & Public Involvement 186 0 186 168 0 168 192 24
Communications & PR 5 0 5 5 0 5 45 40
Performance 823 0 823 823 0 823 976 153
Quality Assurance 614 0 614 632 0 632 533 -99
Primary Care Support 208 0 208 208 0 208 133 -74
Strategy & Development 962 -171 790 960 0 960 708 -253
Governing Body 1,493 0 1,493 1,493 0 1,493 1,388 -104
Corporate Running Costs 6,978 -171 6,806 6,962 0 6,962 6,138 -824
Total Corporate Costs 9,988 -171 9,816 10,429 0 10,429 8,967 -1,462
1% Non Recurrent Headroom Reserve 4,799 4,799 0 4,799 4,799 0 -4,799
Contingency Reserve 0.5% 2,482 0 2,482 2,196 0 2,196 0 -2,196
Investments 0 0 0 0 0 0 0 0
Total Reserves 2,482 4,799 7,281 2,196 4,799 6,995 0 -6,995
TOTAL APPLICATION OF FUNDS 479,686 8,983 488,669 485,999 4,799 490,798 485,940 -4,858
SURPLUS 1% REQUIREMENT* 7,722 7,722 0 -7,722
TOTAL 496,391 498,520 485,940 -12,580
* As directed by NHS England - All CCGs are required to make a surplus of at least 1%
OPERATING COST STATEMENT
Opening Budget YEAR TO DATE
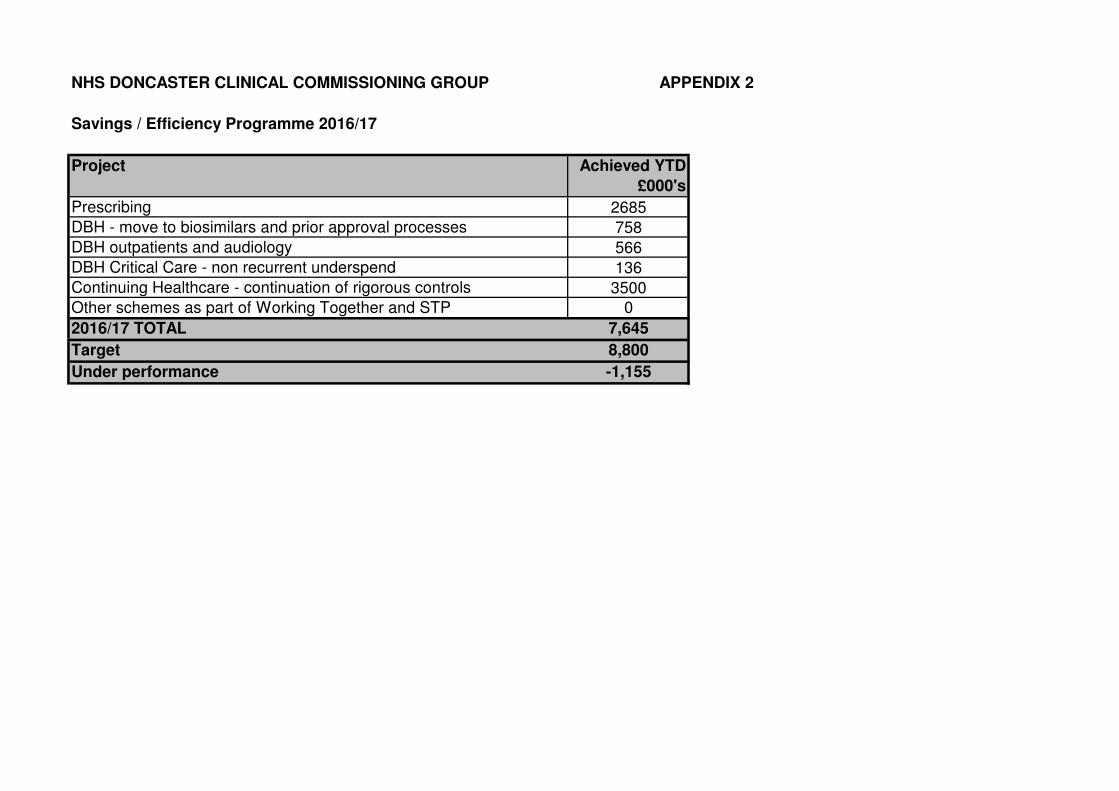
NHS DONCASTER CLINICAL COMMISSIONING GROUP APPENDIX 2
Savings / Efficiency Programme 2016/17
Project Achieved YTD
£000's
Prescribing 2685
DBH - move to biosimilars and prior approval processes 758
DBH outpatients and audiology 566
DBH Critical Care - non recurrent underspend 136
Continuing Healthcare - continuation of rigorous controls 3500
Other schemes as part of Working Together and STP 0
2016/17 TOTAL 7,645
Target 8,800
Under performance -1,155
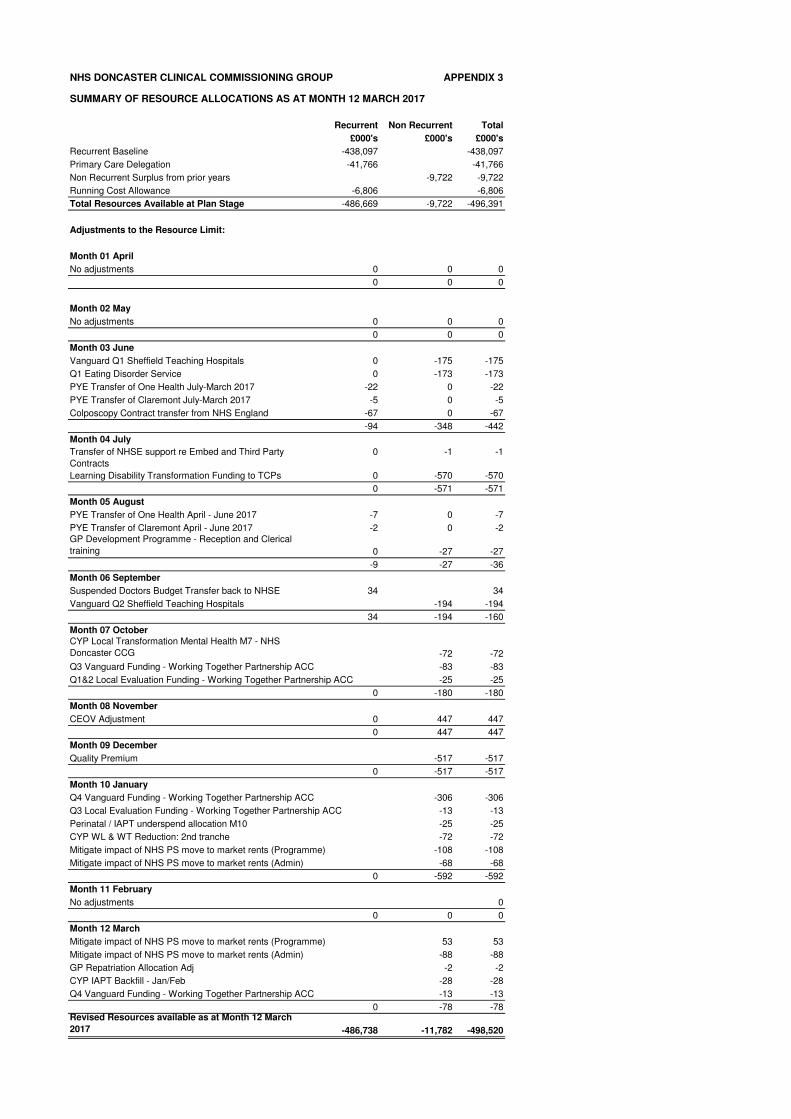
NHS DONCASTER CLINICAL COMMISSIONING GROUP APPENDIX 3
SUMMARY OF RESOURCE ALLOCATIONS AS AT MONTH 12 MARCH 2017
Recurrent Non Recurrent Total
£000's £000's £000's
Recurrent Baseline -438,097 -438,097
Primary Care Delegation -41,766 -41,766
Non Recurrent Surplus from prior years -9,722 -9,722
Running Cost Allowance -6,806 -6,806
Total Resources Available at Plan Stage -486,669 -9,722 -496,391
Adjustments to the Resource Limit:
Month 01 April
No adjustments 0 0 0
0 0 0
Month 02 May
No adjustments 0 0 0
0 0 0
Month 03 June
Vanguard Q1 Sheffield Teaching Hospitals 0 -175 -175
Q1 Eating Disorder Service 0 -173 -173
PYE Transfer of One Health July-March 2017 -22 0 -22
PYE Transfer of Claremont July-March 2017 -5 0 -5
Colposcopy Contract transfer from NHS England -67 0 -67
-94 -348 -442
Month 04 July
Transfer of NHSE support re Embed and Third Party
Contracts
0 -1 -1
Learning Disability Transformation Funding to TCPs 0 -570 -570
0 -571 -571
Month 05 August
PYE Transfer of One Health April - June 2017 -7 0 -7
PYE Transfer of Claremont April - June 2017 -2 0 -2
GP Development Programme - Reception and Clerical
training 0 -27 -27
-9 -27 -36
Month 06 September
Suspended Doctors Budget Transfer back to NHSE 34 34
Vanguard Q2 Sheffield Teaching Hospitals -194 -194
34 -194 -160
Month 07 October
CYP Local Transformation Mental Health M7 - NHS
Doncaster CCG -72 -72
Q3 Vanguard Funding - Working Together Partnership ACC -83 -83
Q1&2 Local Evaluation Funding - Working Together Partnership ACC -25 -25
0 -180 -180
Month 08 November
CEOV Adjustment 0 447 447
0 447 447
Month 09 December
Quality Premium -517 -517
0 -517 -517
Month 10 January
Q4 Vanguard Funding - Working Together Partnership ACC -306 -306
Q3 Local Evaluation Funding - Working Together Partnership ACC -13 -13
Perinatal / IAPT underspend allocation M10 -25 -25
CYP WL & WT Reduction: 2nd tranche -72 -72
Mitigate impact of NHS PS move to market rents (Programme) -108 -108
Mitigate impact of NHS PS move to market rents (Admin) -68 -68
0 -592 -592
Month 11 February
No adjustments 0
0 0 0
Month 12 March
Mitigate impact of NHS PS move to market rents (Programme) 53 53
Mitigate impact of NHS PS move to market rents (Admin) -88 -88
GP Repatriation Allocation Adj -2 -2
CYP IAPT Backfill - Jan/Feb -28 -28
Q4 Vanguard Funding - Working Together Partnership ACC -13 -13
0 -78 -78Revised Resources available as at Month 12 March
2017 -486,738 -11,782 -498,520
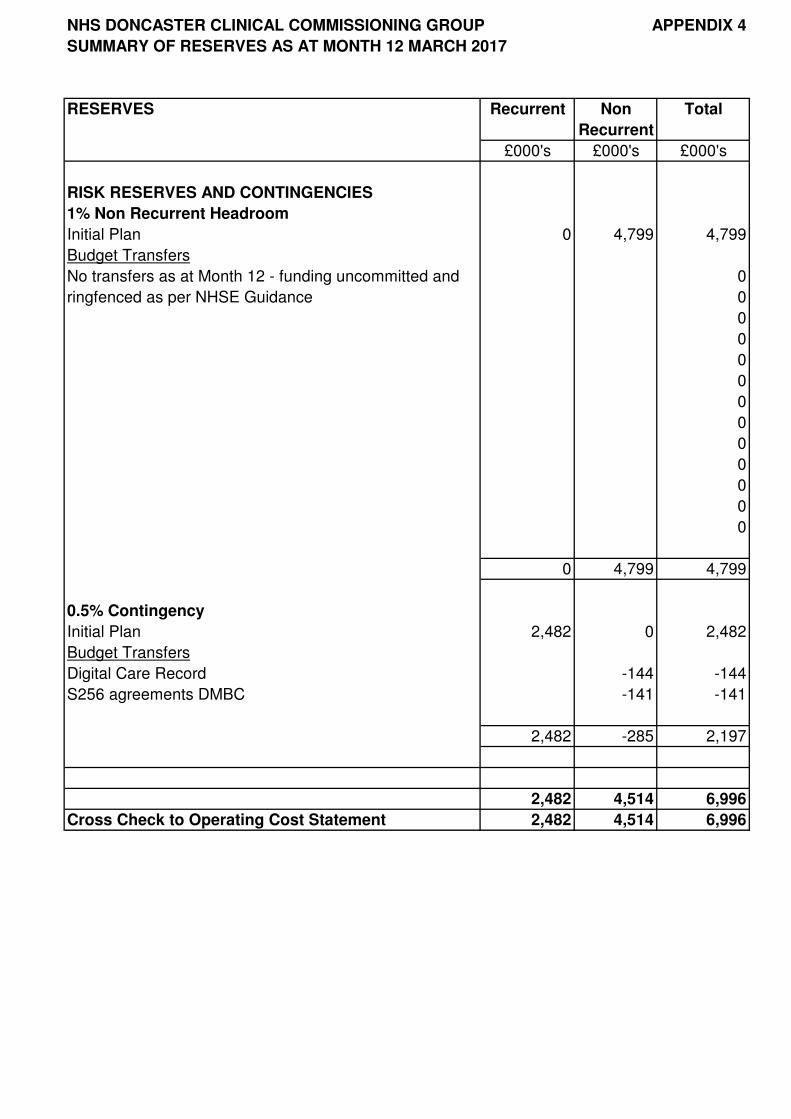
NHS DONCASTER CLINICAL COMMISSIONING GROUP APPENDIX 4
SUMMARY OF RESERVES AS AT MONTH 12 MARCH 2017
RESERVES Recurrent Non Total
Recurrent
£000's £000's £000's
RISK RESERVES AND CONTINGENCIES
1% Non Recurrent Headroom
Initial Plan 0 4,799 4,799
Budget Transfers
No transfers as at Month 12 - funding uncommitted and 0
ringfenced as per NHSE Guidance 0
0
0
0
0
0
0
0
0
0
0
0
0 4,799 4,799
0.5% Contingency
Initial Plan 2,482 0 2,482
Budget Transfers
Digital Care Record -144 -144
S256 agreements DMBC -141 -141
2,482 -285 2,197
2,482 4,514 6,996
Cross Check to Operating Cost Statement 2,482 4,514 6,996
Enc D
Item 9
Corporate Assurance Report Quarter 4 2016/2017

Meeting name Governing Body
Meeting date 18 May 2017
Title of paper
Corporate Assurance Report – Quarter 4 2016/17
Executive / Clinical Lead(s)
Mrs Sarah Atkins Whatley, Chief of Corporate Services
Author(s) Mrs Sarah Atkins Whatley, Chief of Corporate Services Corporate Services Team
Purpose of Paper - Executive Summary The key points from this report to which the organisation’s attention is particularly drawn are:
• Risk: Following a Governing Body Assurance Framework Timeout session in January 2017 we revised our corporate objectives against which the Governing Body Assurance Framework is mapped, and we developed a refreshed list of current and emerging strategic risks to the achievement of these objectives. A new Governing Body Assurance Framework template has been developed and is being used from 1 April 2017.
• External assessments: The CCG has been assessed as “compliant” for Conflicts of Interest in all 5 areas in the NHS England mandated review by our Internal Auditors. The Section 117 Internal Audit Report noted the significant amount of work which had been completed since the CCG took over responsibility for Section 117s, but noted that the work was not formally captured and therefore a limited opinion was issued in respect of governance arrangements and the quality review of Section 117 care. The Internal Audit of our Budgetary Control & Key Financial Systems resulted in significant assurance.
• Constitution & governance structure: From 1 April 2017 we have entered into a Joint Committee with other CCGs for the Commissioners Working Together programme. The associated constitutional update required to capture this change has been supported by our Members and approved by NHS England. A consultation with Member Practices is taking place recommending the removal of Terms of Reference from the Constitution to reduce the bureaucratic burden on Member Practices to approve minor changes.
• Procedural documents: Our Human Resources Policies have reached their 3-year review period and any changes are being consulted upon with the Joint Negotiation & Consultative Forum with Staff Side colleagues prior to Committee approval.
• Emergency Preparedness, Resilience & Response (EPRR): In the last Quarter we have provided assurance to NHS England on our commissioning arrangements to support treatment associated with avian influenza. The learning from the national Exercise Cygnus to exercise plans for pandemic influenza has
been shared, and is being embedded within participating organisations. All CCG team business continuity plans have been reviewed in the last Quarter and updated to reflect any developments.
• Sustainability: We have reported a full 6-month progress update on our Sustainability Action Plan within our Sustainability Strategy; sustainability actions are embedded throughout our organisational activities.
• Information Governance: On 27 March 2017 we published our 2016/17 Information Governance (IG) Toolkit. We attained an overall IG Toolkit score of 77%, improving on the score achieved for 2015/16 by 1% and achieving a minimum score of 2 across all the standards, meaning that our Toolkit outcome is “satisfactory”. The Toolkit was also subject to Internal Audit review in the last Quarter, which resulted in an outcome of significant assurance. Work is underway to develop an IG Workplan for 2017/18, which will be largely dictated by an expected national refresh of the Toolkit to take into account the new General Data Protection Regulation which we are preparing for and comes into legislative effect from May 2018.
• Counter Fraud: In the last Quarter a Counter Fraud update and a Counter Fraud Work Plan for 2017/18 were received. The Counter Fraud Self-Review Tool (SRT) was also completed and submitted by 31 March 2017 with a “Green” rating. The Fraud, Corruption & Bribery Policy has been refreshed and approved by Audit Committee.
• Mandatory & statutory training: There is a generally a deteriorating picture, and action is being taken through line managers to address the compliance rate.
Recommendation(s) It is recommended that the meeting considers and notes the information provided.
Impact analysis Quality impact Nil
Equality impact
Neutral
Sustainability impact
Sustainability impacts are listed in the report
Financial implications
Nil
Legal implications
Nil
Management of Conflicts of
Interest None identified
Consultation / Engagement
(internal departments,
clinical, stakeholder & public/patient)
N/A
Report previously
presented at
Information which fed the report has previously been received by the Corporate Governance Management Group and a range of
other CCG meetings / Committees. Risk
analysis Risks are highlighted throughout the report.
Assurance Framework
1.1

1
CORPORATE ASSURANCE
REPORT
Quarter 4 2016/17
(1 January – 31 March 2017)
2
Contents ______________________________________________________
Section Sub-Section Page Executive Summary
3
Section 1 Risk Management 1.1. Assurance Framework 1.2. Risk Register 1.3. Internal Incident Reporting 1.4. Claims & Legal Issues
4 4 6 7 8
Section 2 External Assessments
9
Section 3 Committee Activity
10
Section 4 Corporate Governance 4.1. Constitution & Establishment 4.2. Governance Structure 4.3. Statutory roles 4.4. Procedural Document Management 4.5. Health & Safety, Fire Safety & Security 4.6. Emergency Resilience & Business Continuity 4.7. Sustainability 4.8. Complaints Management 4.9. Whistleblowing
12 12 12 14 14 15 15 16 17 18
Section 5 Information Governance 5.1. The protection and use of personal confidential data 5.2. Information Governance Toolkit 5.3. Freedom of Information Act Requests 5.4. Data Protection Subject Access Requests 5.5. Information Management & Technology
19 19 19 19 20 20
Section 6 Financial Governance
21
Section 7 Organisational Development & Staffing Governance 7.1. Organisational Development 7.2. Staffing Governance
22 22 22
3
Executive Summary _________________________________________________________ The key points from this report to which the organisation’s attention is particularly drawn are:
Risk: Following a Governing Body Assurance Framework Timeout session in January 2017 we revised our corporate objectives against which the Governing Body Assurance Framework is mapped, and we developed a refreshed list of current and emerging strategic risks to the achievement of these objectives. A new Governing Body Assurance Framework template has been developed and is being used from 1 April 2017.
External assessments: The CCG has been assessed as “compliant” for Conflicts of Interest in all 5 areas in the NHS England mandated review by our Internal Auditors. The Section 117 Internal Audit Report noted the significant amount of work which had been completed since the CCG took over responsibility for Section 117s, but noted that the work was not formally captured and therefore a limited opinion was issued in respect of governance arrangements and the quality review of Section 117 care. The Internal Audit of our Budgetary Control & Key Financial Systems resulted in significant assurance.
Constitution & governance structure: From 1 April 2017 we have entered into a Joint Committee with other CCGs for the Commissioners Working Together programme. The associated constitutional update required to capture this change has been supported by our Members and approved by NHS England. A consultation with Member Practices is taking place recommending the removal of Terms of Reference from the Constitution to reduce the bureaucratic burden on Member Practices to approve minor changes.
Procedural documents: Our Human Resources Policies have reached their 3-year review period and any changes are being consulted upon with the Joint Negotiation & Consultative Forum with Staff Side colleagues prior to Committee approval.
Emergency Preparedness, Resilience & Response (EPRR): In the last Quarter we have provided assurance to NHS England on our commissioning arrangements to support treatment associated with avian influenza. The learning from the national Exercise Cygnus to exercise plans for pandemic influenza has been shared, and is being embedded within participating organisations. All CCG team business continuity plans have been reviewed in the last Quarter and updated to reflect any developments.
Sustainability: We have reported a full 6-month progress update on our Sustainability Action Plan within our Sustainability Strategy; sustainability actions are embedded throughout our organisational activities.
Information Governance: On 27 March 2017 we published our 2016/17 Information Governance (IG) Toolkit. We attained an overall IG Toolkit score of 77%, improving on the score achieved for 2015/16 by 1% and achieving a minimum score of 2 across all the standards, meaning that our Toolkit outcome is “satisfactory”. The Toolkit was also subject to Internal Audit review in the last Quarter, which resulted in an outcome of significant assurance. Work is underway to develop an IG Workplan for 2017/18, which will be largely dictated by an expected national refresh of the Toolkit to take into account the new General Data Protection Regulation in May 2018 for which we are preparing.
Counter Fraud: In the last Quarter a Counter Fraud update and a Counter Fraud Work Plan for 2017/18 were received. The Counter Fraud Self-Review Tool (SRT) was also completed and submitted by 31 March 2017 with a “Green” rating. The Fraud, Corruption & Bribery Policy has been refreshed and approved by Audit Committee.
Mandatory & statutory training: There is a generally a deteriorating picture, and action is being taken through line managers to address the compliance rate.
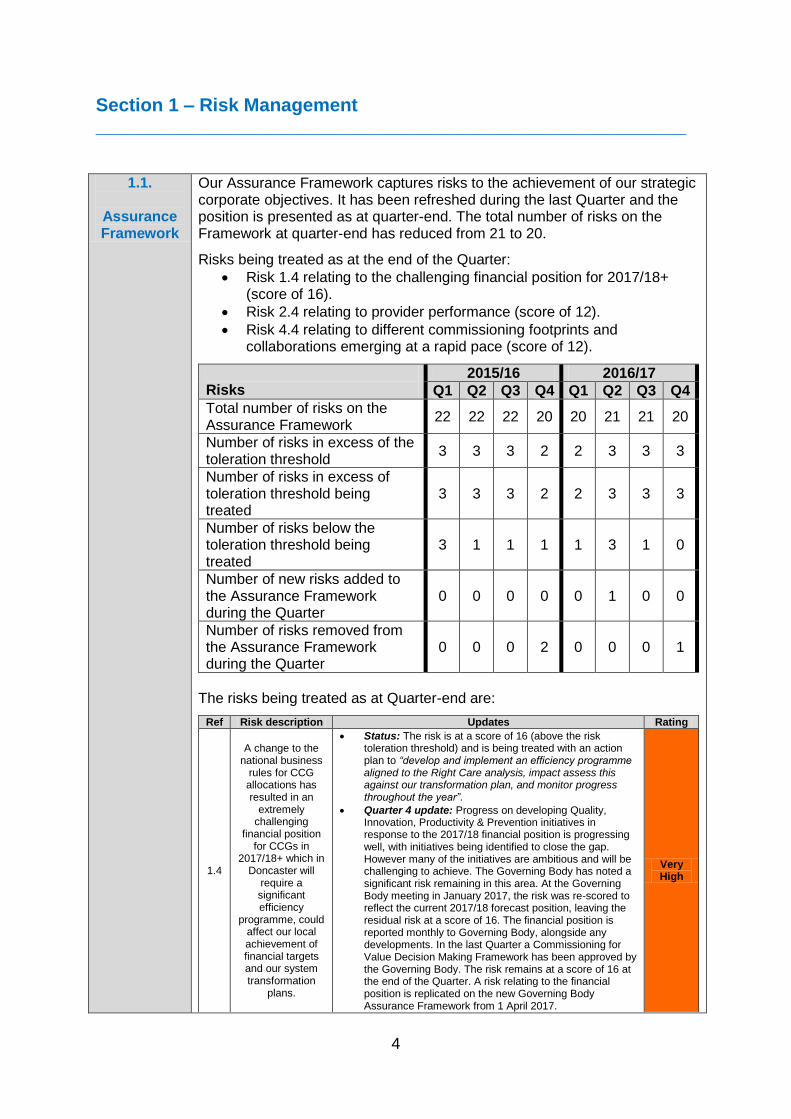
4
Section 1 – Risk Management _________________________________________________________
1.1.
Assurance Framework
Our Assurance Framework captures risks to the achievement of our strategic corporate objectives. It has been refreshed during the last Quarter and the position is presented as at quarter-end. The total number of risks on the Framework at quarter-end has reduced from 21 to 20.
Risks being treated as at the end of the Quarter:
Risk 1.4 relating to the challenging financial position for 2017/18+ (score of 16).
Risk 2.4 relating to provider performance (score of 12).
Risk 4.4 relating to different commissioning footprints and collaborations emerging at a rapid pace (score of 12).
Risks
2015/16 2016/17
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
Total number of risks on the Assurance Framework
22 22 22 20 20 21 21 20
Number of risks in excess of the toleration threshold
3 3 3 2 2 3 3 3
Number of risks in excess of toleration threshold being treated
3 3 3 2 2 3 3 3
Number of risks below the toleration threshold being treated
3 1 1 1 1 3 1 0
Number of new risks added to the Assurance Framework during the Quarter
0 0 0 0 0 1 0 0
Number of risks removed from the Assurance Framework during the Quarter
0 0 0 2 0 0 0 1
The risks being treated as at Quarter-end are:
Ref Risk description Updates Rating
1.4
A change to the national business
rules for CCG allocations has resulted in an
extremely challenging
financial position for CCGs in
2017/18+ which in Doncaster will
require a significant efficiency
programme, could affect our local achievement of financial targets and our system transformation
plans.
Status: The risk is at a score of 16 (above the risk toleration threshold) and is being treated with an action plan to “develop and implement an efficiency programme aligned to the Right Care analysis, impact assess this against our transformation plan, and monitor progress throughout the year”.
Quarter 4 update: Progress on developing Quality, Innovation, Productivity & Prevention initiatives in response to the 2017/18 financial position is progressing well, with initiatives being identified to close the gap. However many of the initiatives are ambitious and will be challenging to achieve. The Governing Body has noted a significant risk remaining in this area. At the Governing Body meeting in January 2017, the risk was re-scored to reflect the current 2017/18 forecast position, leaving the residual risk at a score of 16. The financial position is reported monthly to Governing Body, alongside any developments. In the last Quarter a Commissioning for Value Decision Making Framework has been approved by the Governing Body. The risk remains at a score of 16 at the end of the Quarter. A risk relating to the financial position is replicated on the new Governing Body Assurance Framework from 1 April 2017.
Very High
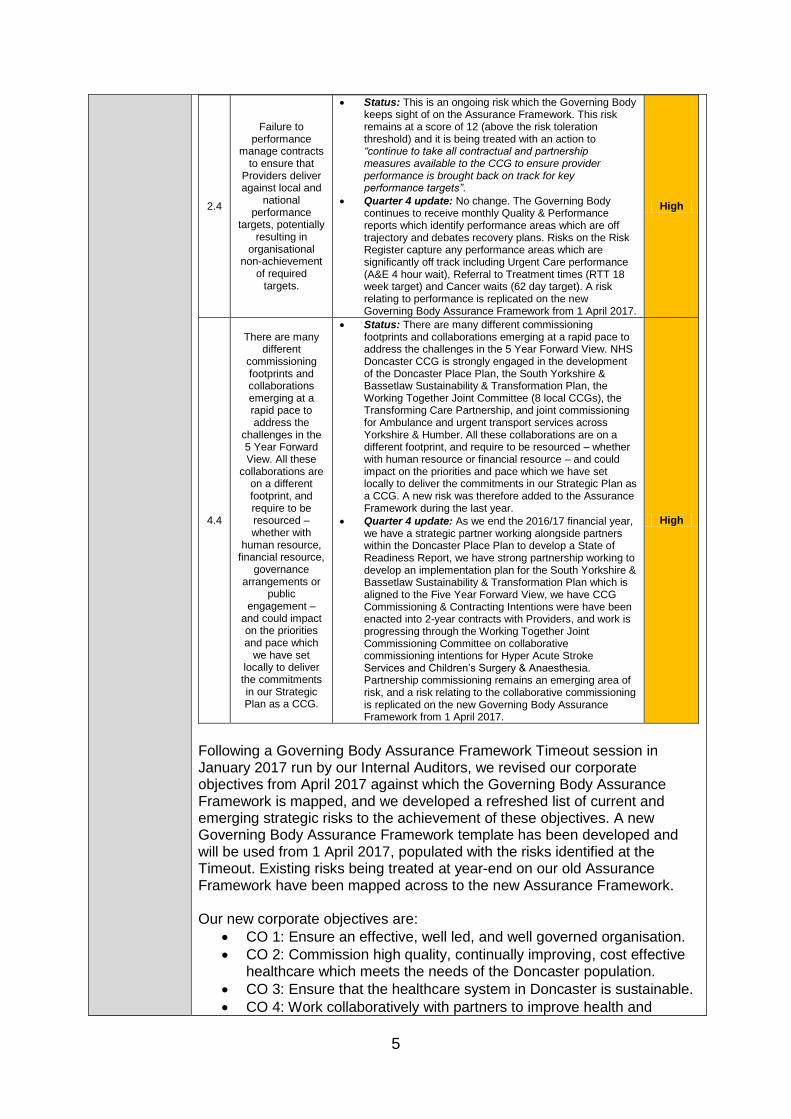
5
2.4
Failure to performance
manage contracts to ensure that
Providers deliver against local and
national performance
targets, potentially resulting in
organisational non-achievement
of required targets.
Status: This is an ongoing risk which the Governing Body keeps sight of on the Assurance Framework. This risk remains at a score of 12 (above the risk toleration threshold) and it is being treated with an action to “continue to take all contractual and partnership measures available to the CCG to ensure provider performance is brought back on track for key performance targets”.
Quarter 4 update: No change. The Governing Body continues to receive monthly Quality & Performance reports which identify performance areas which are off trajectory and debates recovery plans. Risks on the Risk Register capture any performance areas which are significantly off track including Urgent Care performance (A&E 4 hour wait), Referral to Treatment times (RTT 18 week target) and Cancer waits (62 day target). A risk relating to performance is replicated on the new Governing Body Assurance Framework from 1 April 2017.
High
4.4
There are many different
commissioning footprints and collaborations emerging at a rapid pace to address the
challenges in the 5 Year Forward View. All these
collaborations are on a different footprint, and require to be resourced – whether with
human resource, financial resource,
governance arrangements or
public engagement –
and could impact on the priorities and pace which
we have set locally to deliver the commitments in our Strategic Plan as a CCG.
Status: There are many different commissioning footprints and collaborations emerging at a rapid pace to address the challenges in the 5 Year Forward View. NHS Doncaster CCG is strongly engaged in the development of the Doncaster Place Plan, the South Yorkshire & Bassetlaw Sustainability & Transformation Plan, the Working Together Joint Committee (8 local CCGs), the Transforming Care Partnership, and joint commissioning for Ambulance and urgent transport services across Yorkshire & Humber. All these collaborations are on a different footprint, and require to be resourced – whether with human resource or financial resource – and could impact on the priorities and pace which we have set locally to deliver the commitments in our Strategic Plan as a CCG. A new risk was therefore added to the Assurance Framework during the last year.
Quarter 4 update: As we end the 2016/17 financial year, we have a strategic partner working alongside partners within the Doncaster Place Plan to develop a State of Readiness Report, we have strong partnership working to develop an implementation plan for the South Yorkshire & Bassetlaw Sustainability & Transformation Plan which is aligned to the Five Year Forward View, we have CCG Commissioning & Contracting Intentions were have been enacted into 2-year contracts with Providers, and work is progressing through the Working Together Joint Commissioning Committee on collaborative commissioning intentions for Hyper Acute Stroke Services and Children’s Surgery & Anaesthesia. Partnership commissioning remains an emerging area of risk, and a risk relating to the collaborative commissioning is replicated on the new Governing Body Assurance Framework from 1 April 2017.
High
Following a Governing Body Assurance Framework Timeout session in January 2017 run by our Internal Auditors, we revised our corporate objectives from April 2017 against which the Governing Body Assurance Framework is mapped, and we developed a refreshed list of current and emerging strategic risks to the achievement of these objectives. A new Governing Body Assurance Framework template has been developed and will be used from 1 April 2017, populated with the risks identified at the Timeout. Existing risks being treated at year-end on our old Assurance Framework have been mapped across to the new Assurance Framework. Our new corporate objectives are:
CO 1: Ensure an effective, well led, and well governed organisation.
CO 2: Commission high quality, continually improving, cost effective healthcare which meets the needs of the Doncaster population.
CO 3: Ensure that the healthcare system in Doncaster is sustainable.
CO 4: Work collaboratively with partners to improve health and
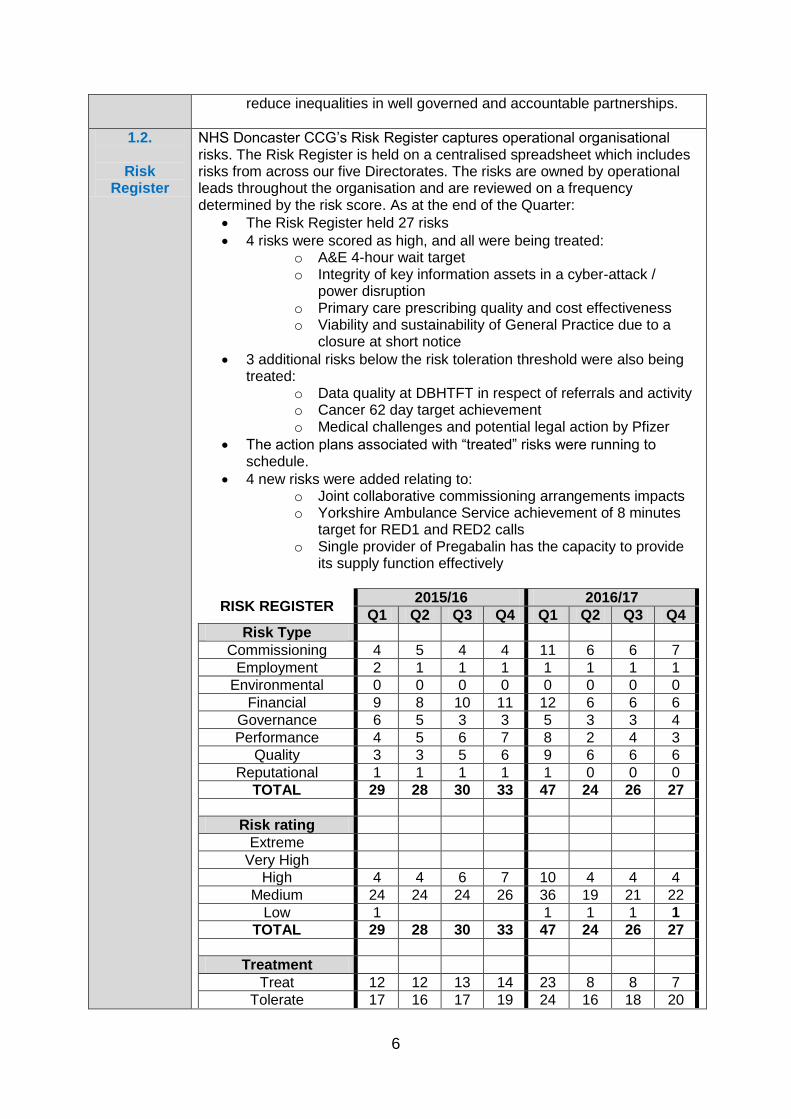
6
reduce inequalities in well governed and accountable partnerships.
1.2.
Risk Register
NHS Doncaster CCG’s Risk Register captures operational organisational risks. The Risk Register is held on a centralised spreadsheet which includes risks from across our five Directorates. The risks are owned by operational leads throughout the organisation and are reviewed on a frequency determined by the risk score. As at the end of the Quarter:
The Risk Register held 27 risks
4 risks were scored as high, and all were being treated: o A&E 4-hour wait target o Integrity of key information assets in a cyber-attack /
power disruption o Primary care prescribing quality and cost effectiveness o Viability and sustainability of General Practice due to a
closure at short notice
3 additional risks below the risk toleration threshold were also being treated:
o Data quality at DBHTFT in respect of referrals and activity o Cancer 62 day target achievement o Medical challenges and potential legal action by Pfizer
The action plans associated with “treated” risks were running to schedule.
4 new risks were added relating to: o Joint collaborative commissioning arrangements impacts o Yorkshire Ambulance Service achievement of 8 minutes
target for RED1 and RED2 calls o Single provider of Pregabalin has the capacity to provide
its supply function effectively
RISK REGISTER 2015/16 2016/17
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
Risk Type
Commissioning 4 5 4 4 11 6 6 7
Employment 2 1 1 1 1 1 1 1
Environmental 0 0 0 0 0 0 0 0
Financial 9 8 10 11 12 6 6 6
Governance 6 5 3 3 5 3 3 4
Performance 4 5 6 7 8 2 4 3
Quality 3 3 5 6 9 6 6 6
Reputational 1 1 1 1 1 0 0 0
TOTAL 29 28 30 33 47 24 26 27
Risk rating
Extreme
Very High
High 4 4 6 7 10 4 4 4
Medium 24 24 24 26 36 19 21 22
Low 1 1 1 1 1
TOTAL 29 28 30 33 47 24 26 27
Treatment
Treat 12 12 13 14 23 8 8 7
Tolerate 17 16 17 19 24 16 18 20

7
Terminate
Transfer
TOTAL 29 28 30 33 47 24 26 27
1.3.
Internal Incident
Reporting
The following table shows the number and category of internal incidents reported during the last quarter, and the severity. There have been nine incidents reported in the last Quarter. Seven of the incidents were information governance issues, and two were estates/facilities issues. Three of the information governance incidents originated from outside the CCG and were not breaches by our team members or for our organisation. The remaining four were all breaches by CCG staff, three within the Previously Unassessed Periods of Care team, and one within the Commissioning team. All were assessed using the Information Commissioner’s Information Governance Serious Incident Requiring Investigation Framework, and were classed as minor incidents which were not externally reportable. The estates/facilities incidents relate to an unauthorised visitor in Reception which has resulted in a secure MagLock being requested from NHS Property Services for the door of Reception, and a minor car bump in the carpark for which no further action was required.
INCIDENT MANAGEMENT 2015/16 2016/17
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
Category
Accident / Injury 4 1
Communication
Confidentiality / Information Governance
1 4 2 5 5 11 5 7
Disruptive or Violent behaviour / Assault
Estates/Facilities/Security/Health & Safety
3 5 1 2 1 2
Financial loss
Patient Safety 1
Other
Total 5 7 7 6 8 12 6
Impact
1 - Low (No Harm) 1 7 7 6 8 12 6 9
2 - Medium (Minor treatment only)
3
3 - High (Significant, not permanent harm)
1
4 - Very High (Permanent harm / damage)
5 - Extreme (death)
Total 5 7 7 6 8 12 6 9
Reporting
National Patient Safety Agency (NPSA)
0 0 0 0 0 0 0 0
Counter Fraud and Security Management Service SIRS
0 0 0 0 0 0 0 0
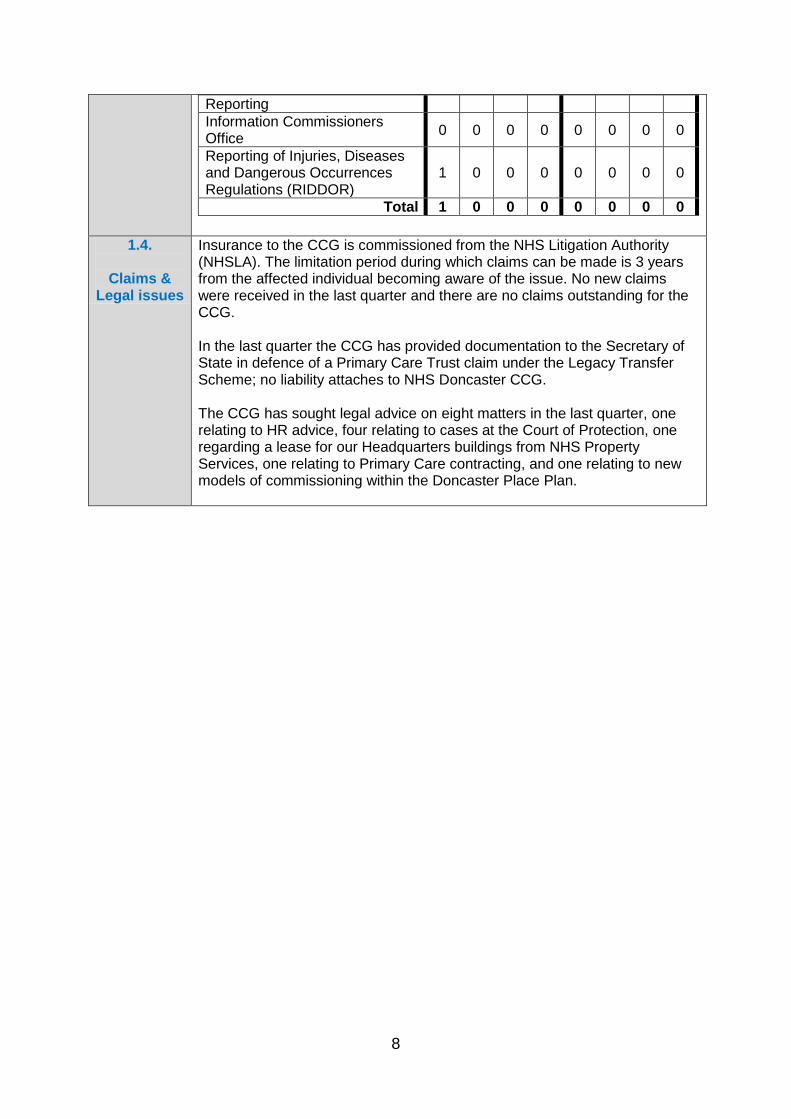
8
Reporting
Information Commissioners Office
0 0 0 0 0 0 0 0
Reporting of Injuries, Diseases and Dangerous Occurrences Regulations (RIDDOR)
1 0 0 0 0 0 0 0
Total 1 0 0 0 0 0 0 0
1.4.
Claims & Legal issues
Insurance to the CCG is commissioned from the NHS Litigation Authority (NHSLA). The limitation period during which claims can be made is 3 years from the affected individual becoming aware of the issue. No new claims were received in the last quarter and there are no claims outstanding for the CCG. In the last quarter the CCG has provided documentation to the Secretary of State in defence of a Primary Care Trust claim under the Legacy Transfer Scheme; no liability attaches to NHS Doncaster CCG. The CCG has sought legal advice on eight matters in the last quarter, one relating to HR advice, four relating to cases at the Court of Protection, one regarding a lease for our Headquarters buildings from NHS Property Services, one relating to Primary Care contracting, and one relating to new models of commissioning within the Doncaster Place Plan.
9
Section 2 – External Assessments _________________________________________________________
NHS Doncaster CCG is subject to a number of external assessments / inspections in order to provide assurance on the quality of services commissioned and our systems of internal
control. The following reports have been received in the last Quarter.
Internal Audit
(Service commissioned
from 360 Assurance)
Section 117 (Mental Health Act Aftercare) Report: The review noted the significant amount of work which had been completed since the CCG took over responsibility for Section 117s from Doncaster PCT, but noted that the work was not formally captured and therefore a limited opinion was issued in respect of governance arrangements and the quality review of Section 117 care.
Conflicts of Interest: The CCG has been assessed as “compliant” in all 5 areas which 360 Assurance were required to examine in the NHS England mandated review.
Budgetary Control & Key Financial Systems: The audit reviews areas on a cyclical programme in addition to general areas reviewed annually. A significant assurance has been issued. Recommendations have been made around Governing Body challenge of the finances, traffic light reporting, Journals, and information to the Governing Body prior to the start of the financial year.
Information Governance IIG) Toolkit: The audit is mandated, and standards are reviewed on a cyclical basis. A significant assurance has been issued. A medium risk has been identified in IG training compliance.
Governing Body Development Session Output: A report has been developed to show the actions that were agreed at the session in respect of revising the CCG’s Strategic Objectives and identifying principal risks for inclusion on the 2017/18 Assurance Framework.
Review of Internal Audit Service Level Agreement 2017/18: The Audit Committee reviewed the position.
Draft Head of Internal Audit Opinion: The Audit Committee has noted the draft Opinion of Significant Assurance.
Strategic Internal Audit Plan 2017-2020: The Audit Committee approved the 2017/18 plan, noting that it will be subject to change in line with future challenges.
External Audit
(Service
commissioned from KPMG)
External Audit Plan: The outline of the External Audit Strategy for the 2016/17 year-end audit was received by the Audit Committee in January 2017. The approach has a greater focus on sustainability and aims to provide an audit opinion on two significant risks areas across all CCGs: the potential for fraudulent recognition of income, and the potential for management override of controls. As a CCGs with delegated responsibility for primary medical care commissioning, the audit also focusses on accounting for co-commissioning.
We also receive Service Auditor Reports from Shared Business Services (Finance & Payroll), and NHS England (primary care payments).
Other inspections
External inspections of the CCG’s arrangements for Health & Safety, Fire Safety, or Information Governance can take place on an ad hoc basis. No inspections have taken place and no reports are expected.
10
Section 3 – Committee Activity _________________________________________________________
Audit Committee
At the 2 meetings held in the last Quarter the Committee considered and noted assurance on:
External Audit technical update and external audit year-end plan, and noting the re-appointment of KPMG as our External Auditors.
A range of Internal Audit reports as detailed in Section 2 of this report, and a review of the Internal Audit Service Level Agreement.
Internal Audit Plan 2017/18 to 2020.
Counter Fraud progress report, and Counter Fraud Work Plan 2017/18.
Financial exceptions, the timetable for the Annual Accounts and our banking arrangements.
Corporate Governance assurance including a review of the Assurance Framework Quarter 3 position, the Corporate Assurance Quarter 3 Report, and a review of audit recommendations.
Approval of the following policies: Fraud, Corruption & Bribery Policy, Whistleblowing Policy, Freedom of Information Policy, Information Governance Policy.
Minutes from the Corporate Governance Management Group.
Remuneration Committee
The Remuneration Committee meets as required. One meeting was held in the last Quarter to consider the potential redundancy of a member of staff. The Committee will meet in April 2017 for the regular review of remuneration for Governing Body members.
Quality & Patient Safety
Committee
At the two meetings held in the last Quarter, the Committee discussed the following areas:
Overview Quality Reports for each of our main providers – acute, mental health / community, urgent care, care homes, individual placements and primary care.
A Medicines Management Report.
The recent Internal Audit in relation to Section 117 Aftercare responsibilities which resulted in a ‘Limited Assurance’ opinion.
A Previously Un-assessed Periods of Care benchmarking report.
Assurance reports on Safeguarding (including a Looked After Children mid-year report), Infection Prevention & Control, and Transforming Care (Learning Disability).
A Serious Incident Report, a Complaints Report and receipt of the Caldicott Workplan and Log.
Considered papers on Learning Candour and Accountability.
Received minutes from Sub Groups including Medicines Management, Incident Management, Area Prescribing and Safeguarding Assurance.
Engagement & Experience Committee
Three meetings were held in the last Quarter where the following areas were discussed:
Engagement planning for the Doncaster Place Plan & the South Yorkshire & Bassetlaw Sustainability & Transformation Plan.
Meeting our Public Sector Equality Duties by publishing our Equality Delivery System (EDS) self-assessment by 31 January 2017, and refreshing our Equality Objectives.
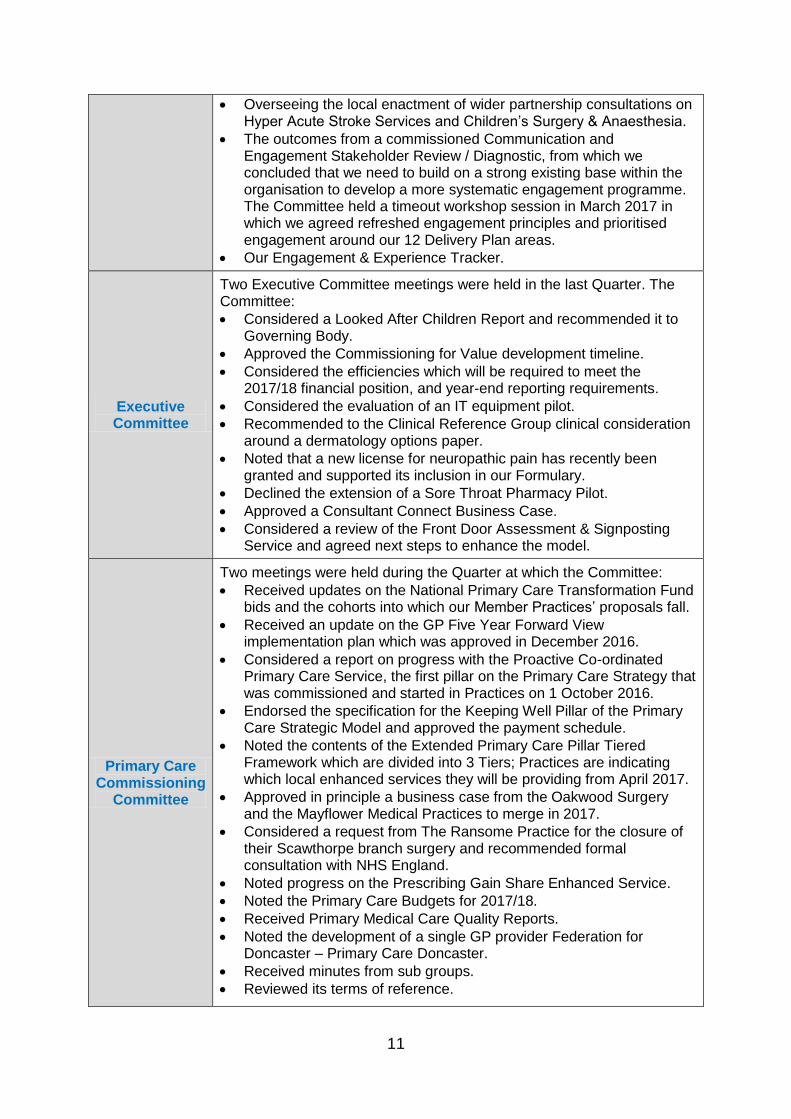
11
Overseeing the local enactment of wider partnership consultations on Hyper Acute Stroke Services and Children’s Surgery & Anaesthesia.
The outcomes from a commissioned Communication and Engagement Stakeholder Review / Diagnostic, from which we concluded that we need to build on a strong existing base within the organisation to develop a more systematic engagement programme. The Committee held a timeout workshop session in March 2017 in which we agreed refreshed engagement principles and prioritised engagement around our 12 Delivery Plan areas.
Our Engagement & Experience Tracker.
Executive Committee
Two Executive Committee meetings were held in the last Quarter. The Committee:
Considered a Looked After Children Report and recommended it to Governing Body.
Approved the Commissioning for Value development timeline.
Considered the efficiencies which will be required to meet the 2017/18 financial position, and year-end reporting requirements.
Considered the evaluation of an IT equipment pilot.
Recommended to the Clinical Reference Group clinical consideration around a dermatology options paper.
Noted that a new license for neuropathic pain has recently been granted and supported its inclusion in our Formulary.
Declined the extension of a Sore Throat Pharmacy Pilot.
Approved a Consultant Connect Business Case.
Considered a review of the Front Door Assessment & Signposting Service and agreed next steps to enhance the model.
Primary Care Commissioning
Committee
Two meetings were held during the Quarter at which the Committee:
Received updates on the National Primary Care Transformation Fund bids and the cohorts into which our Member Practices’ proposals fall.
Received an update on the GP Five Year Forward View implementation plan which was approved in December 2016.
Considered a report on progress with the Proactive Co-ordinated Primary Care Service, the first pillar on the Primary Care Strategy that was commissioned and started in Practices on 1 October 2016.
Endorsed the specification for the Keeping Well Pillar of the Primary Care Strategic Model and approved the payment schedule.
Noted the contents of the Extended Primary Care Pillar Tiered Framework which are divided into 3 Tiers; Practices are indicating which local enhanced services they will be providing from April 2017.
Approved in principle a business case from the Oakwood Surgery and the Mayflower Medical Practices to merge in 2017.
Considered a request from The Ransome Practice for the closure of their Scawthorpe branch surgery and recommended formal consultation with NHS England.
Noted progress on the Prescribing Gain Share Enhanced Service.
Noted the Primary Care Budgets for 2017/18.
Received Primary Medical Care Quality Reports.
Noted the development of a single GP provider Federation for Doncaster – Primary Care Doncaster.
Received minutes from sub groups.
Reviewed its terms of reference.
12
Section 4 – Corporate Governance _________________________________________________________
4.1.
Constitution and
Establishment
As a Membership organisation comprising 43 Member Practices, NHS Doncaster CCG remains fully authorised by NHS England. The Governing Body, under delegated authority from Member Practices, agreed to enter into a Joint Committee with other CCGs for the Commissioners Working Together programme. The associated constitutional update required to capture this change was supported by our Members during Quarter 4, and was submitted to NHS England for approval, which has been received. The Joint Committee commenced from 1 April 2017 and is reflected in our governance meeting structure overleaf. A current consultation with Member Practices is underway recommending the removal of Terms of Reference from the Constitution in order to reduce the bureaucratic burden on Member Practices to approve minor changes every time a set of Terms of Reference is updated. The Locality Lead election schedule resulted in the re-appointment of Dr Nick Tupper to the Central Locality and Dr Marco Pieri to the North West Locality in January 2017.
4.2.
Governance Structure
Our meeting governance structure is detailed overleaf. Activity flowing through each formal Committee of the Governing Body is captured in Section 3 of this report.
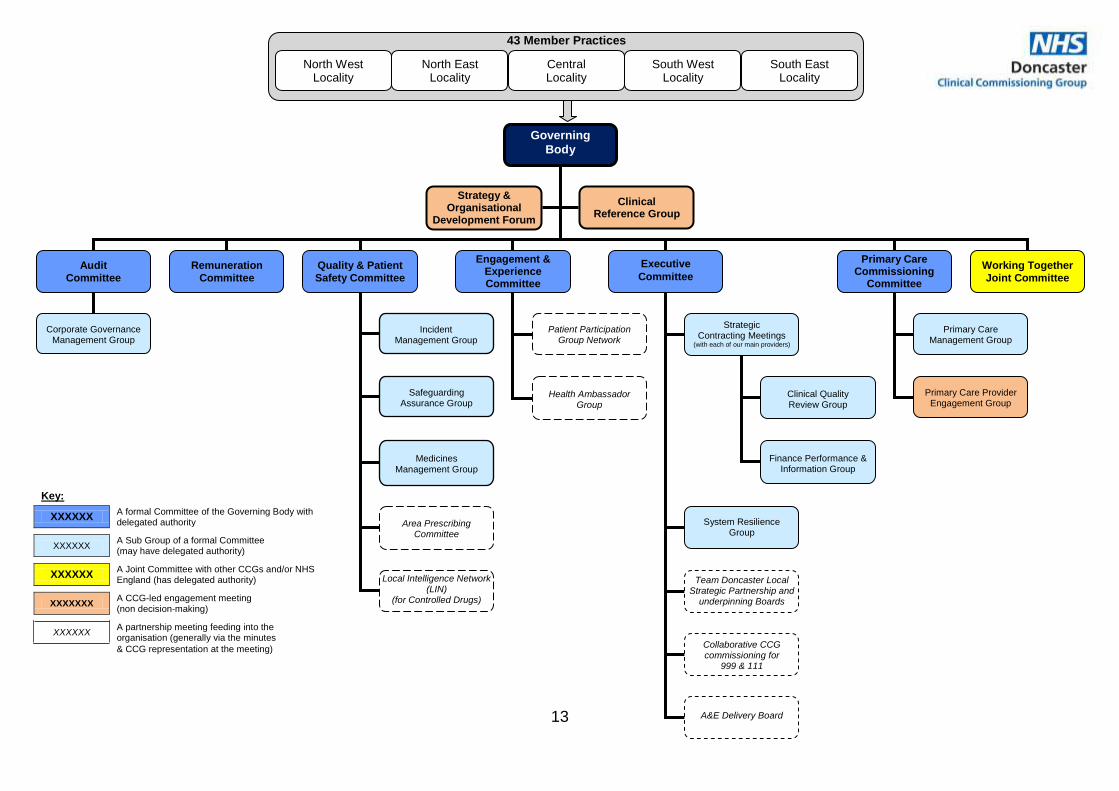
13
Governing
Body
Incident Management Group
Safeguarding Assurance Group
Medicines Management Group
Corporate Governance Management Group
Strategy & Organisational
Development Forum
Primary Care Management Group
Primary Care Provider Engagement Group
Area Prescribing Committee
Local Intelligence Network (LIN)
(for Controlled Drugs)
Patient Participation Group Network
Health Ambassador Group
Clinical Reference Group
Audit
Committee
Remuneration
Committee
Quality & Patient
Safety Committee
Engagement & Experience Committee
Executive
Committee
Primary Care Commissioning
Committee
Working Together
Joint Committee
Strategic Contracting Meetings
(with each of our main providers)
System Resilience Group
Team Doncaster Local Strategic Partnership and
underpinning Boards
Collaborative CCG commissioning for
999 & 111
A&E Delivery Board
Clinical Quality Review Group
Finance Performance & Information Group
Key:
XXXXXX A formal Committee of the Governing Body with delegated authority
XXXXXX A Sub Group of a formal Committee (may have delegated authority)
XXXXXX A Joint Committee with other CCGs and/or NHS England (has delegated authority)
XXXXXXX A CCG-led engagement meeting (non decision-making)
XXXXXX A partnership meeting feeding into the organisation (generally via the minutes
& CCG representation at the meeting)
North West Locality
North East Locality
Central Locality
South West Locality
South East Locality
43 Member Practices
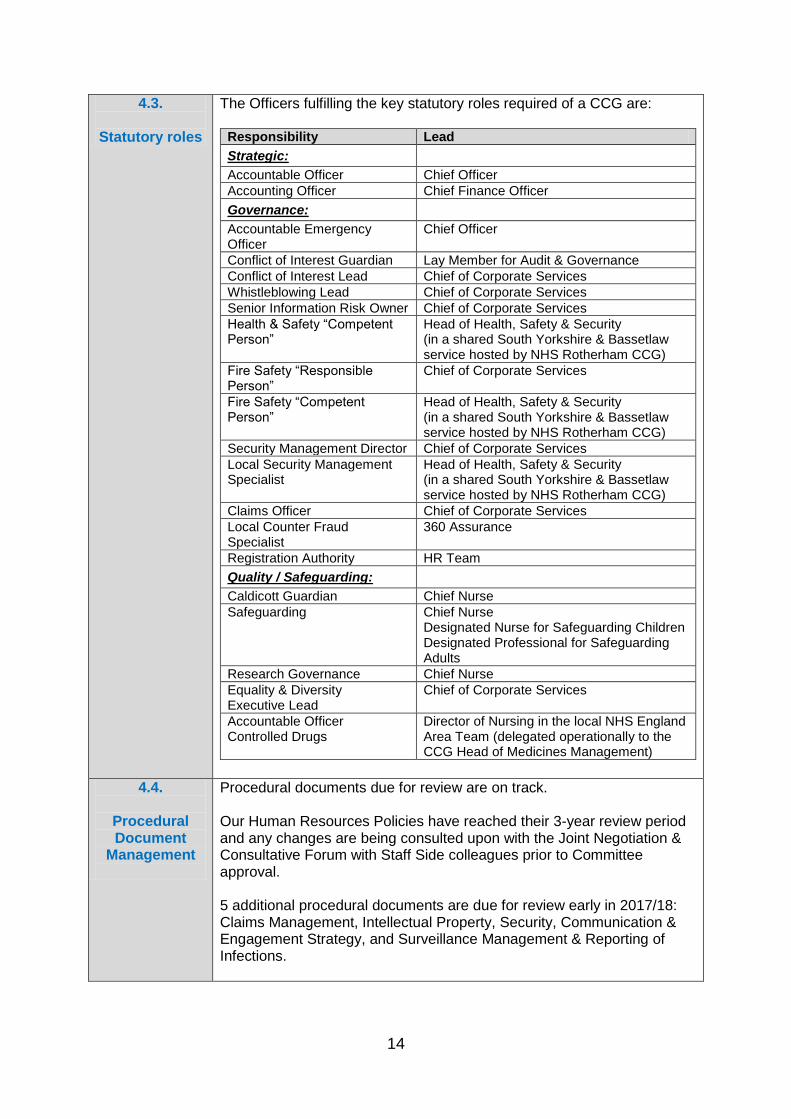
14
4.3.
Statutory roles
The Officers fulfilling the key statutory roles required of a CCG are:
Responsibility Lead
Strategic:
Accountable Officer Chief Officer
Accounting Officer Chief Finance Officer
Governance:
Accountable Emergency Officer
Chief Officer
Conflict of Interest Guardian Lay Member for Audit & Governance
Conflict of Interest Lead Chief of Corporate Services
Whistleblowing Lead Chief of Corporate Services
Senior Information Risk Owner Chief of Corporate Services
Health & Safety “Competent Person”
Head of Health, Safety & Security (in a shared South Yorkshire & Bassetlaw service hosted by NHS Rotherham CCG)
Fire Safety “Responsible Person”
Chief of Corporate Services
Fire Safety “Competent Person”
Head of Health, Safety & Security (in a shared South Yorkshire & Bassetlaw service hosted by NHS Rotherham CCG)
Security Management Director Chief of Corporate Services
Local Security Management Specialist
Head of Health, Safety & Security (in a shared South Yorkshire & Bassetlaw service hosted by NHS Rotherham CCG)
Claims Officer Chief of Corporate Services
Local Counter Fraud Specialist
360 Assurance
Registration Authority HR Team
Quality / Safeguarding:
Caldicott Guardian Chief Nurse
Safeguarding Chief Nurse Designated Nurse for Safeguarding Children Designated Professional for Safeguarding Adults
Research Governance Chief Nurse
Equality & Diversity Executive Lead
Chief of Corporate Services
Accountable Officer Controlled Drugs
Director of Nursing in the local NHS England Area Team (delegated operationally to the CCG Head of Medicines Management)
4.4.
Procedural Document
Management
Procedural documents due for review are on track. Our Human Resources Policies have reached their 3-year review period and any changes are being consulted upon with the Joint Negotiation & Consultative Forum with Staff Side colleagues prior to Committee approval. 5 additional procedural documents are due for review early in 2017/18: Claims Management, Intellectual Property, Security, Communication & Engagement Strategy, and Surveillance Management & Reporting of Infections.
15
4.5.
Health & Safety, Fire
Safety & Security
Health & Safety:
The Competent Person for Health & Safety has confirmed to the Corporate Governance Management Group that the CCG remains compliant with health & safety legislation.
The Health & Safety Executive publication of revised legislation has been reviewed, and none impacts upon the CCG’s duties.
All health & safety internal inspections are in date. Fire:
The annual fire risk assessment is in date.
Fire Marshalls are running weekly fire alarm tests. Security:
There are national plans for the creation of a new Special Health Authority dedicated to counter fraud work. The new organisation will be called the NHS Counter Fraud Authority (NHSCFA) and exists in shadow form from 1 April 2017. The transfer of staff and the creation of the NHSCFA will take place during the first quarter of 2017/18, with the new organisation being launched on 3 July 2017. At this point NHS Protect will cease to exist. Services provided by NHS Protect’s Local Support and Development and Training teams will cease on 31 March 2017. The remaining NHS Protect security management functions will also be decommissioned at this time as part of the transition leading to the establishment of the NHSCFA.
NHS Doncaster CCG is part of a partnership arrangement with the South Yorkshire & Bassetlaw CCGs for Health, Safety & Security hosted by NHS Rotherham CCG. As part of this service we have access to advice and support from an experienced and accredited NHS security management professional.
4.6.
Emergency Resilience and
Business Continuity
Emergency Preparedness, Resilience & Response:
In the last Quarter we have provided assurance to NHS England on our commissioning arrangements to support treatment associated with avian influenza.
The learning from the national Exercise Cygnus to exercise plans for pandemic influenza has been shared, and is being embedded within participating organisations.
Business Continuity:
All CCG team business continuity plans have been reviewed in the last Quarter and updated to reflect any developments within the team. Team contact lists have also been verified and a cascade test has been undertaken.
16
4.7.
Sustainability
The action plan is on track and work is on-going around this. A full 6-month update is reported at the end of Quarter’s 2 and 4. The Quarter 4 update is detailed below.
Area of focus Development Plan Updates
Leadership, engagement
and workforce development
Regularly review our Sustainable Development Management Plan for approval by our Governing Body at least every 3 years.
The strategy was last refreshed and approved by Governing Body in January 2016. The strategy remains in date.
Continue to engage with and empower communities through enacting our Communication, Engagement & Experience Strategy, reporting progress to our Engagement & Experience Committee.
Our Engagement & Experience Committee oversees progress, and in the last 6 months has refreshed our CCG engagement principles and priorities. We have developed a strong partnership with Healthwatch Doncaster, including seconding a team member to work on the partnership Health Ambassadors project.
Continue to support our team members through enacting our Organisational Development Strategy, reporting progress through our Corporate Assurance Reports.
Our commissioned Organisational Development (OD) Diagnostic took place in Quarters 2 and 3 of 2016/17, and resulted in a refreshed OD Strategy & Action Plan which was approved by the Governing Body in December 2016. Governing Body “Sponsors” for each of the 6 areas in the OD Strategy have been identified, and work is ongoing to deliver the action plan.
Carbon hotspots
Continue to engage with and empower our team members to save carbon through initiatives such as recycling, saving energy and reducing unnecessary travel.
Our Colleague Engagement Group (CEG) regularly review initiatives, which in the past 6 months have included Healthy Workplaces and the Staff Survey results.
Commissioning and
procurement
Regularly review procurement documentation to ensure that economic, environmental and social sustainability remain intrinsic to the process.
Our Procurement Strategy was updated to reflect the new 2015 regulations, was approved by the Governing Body, and remains in date.
Sustainable clinical and care models
Continue to focus on system transformation within our Strategic Plan, reporting progress to our Governing Body.
Our organisational focus very much remains on system transformation, and the last 6 months has seen the approval of the South Yorkshire & Bassetlaw Sustainability & Transformation Plan, and the Doncaster Place Plan, in both of which we are a key partner. We have been focusing on transformational change in intermediate care, starting with a Falls Pathway integrated pilot with Doncaster Council.
Healthy, sustainable and resilient communities
Work in partnership to support delivery of the Health & Wellbeing Board Strategy, monitoring progress through the Health & Wellbeing Board.
Our Chair has now been nominated as the Vice Chair of the Health & Wellbeing Board. We are working in partnership with the Public Health team in Doncaster Council on a Health Inequalities Group in support of the Health & Wellbeing Strategy. Our transformation and clinical priority areas very much map to the Health & Wellbeing Board Strategy which was refreshed and approved in December 2015.
Metrics
Use core indicators to assess our own and our providers’ sustainability performance, reporting our progress through our Annual Report.
Our Annual Report has been drafted, and will be approved by the Governing Body in May 2017, and it contains the required sustainability commentary and metrics.
17
Innovation, Technology
and Research & Development
Implement our Information Technology Strategy, reporting progress annually to the Governing Body.
We have published a Local Digital Roadmap which builds upon our Information Technology (IT) Strategy. We Chair a partnership Health & Social Care Interoperability Group to oversee implementation of the Local Digital Roadmap, and are currently procuring for a partner to develop a “proof of concept” for an electronic Doncaster Integrated Care Record.
Creating social value
Continue to consider all aspects of sustainability when reviewing business cases and taking commissioning decisions.
We last refreshed our Standards of Business Conduct & Conflicts of Interest Policy in August 2016, and this includes a Business Case Template which considers matters of sustainability. Sustainability is also built into our Procurement Strategy.
4.8.
Complaints management
Below is a summary of complaints data for NHS Doncaster CCG for the last quarter which has been reported to NHS Digital.
Total Upheld Partially upheld
Not upheld
2015/16 Annual Total
56 6 16 30
Quarter 1 15 1 6 7
Quarter 2 21 1 4 10
Quarter 3 14 1 1 5
Quarter 4 20 1 4 13
2016/17 Annual Total
70 10 31 65
7 complaints opened in Quarter 3 2016/17 were resolved in Q4 2016/17. 1 multi-agency complaint opened in Q3 remains open. 1 complaint (currently closed) is awaiting the outcome of the Independent Review. 2 complaints opened in Quarter 4 are carried forward to Quarter 1 of 2017-18.
Themes and trends from complaints are reported through the Committee structure of the organisation. Of the 20 complaints received and investigated during the quarter (6 were received as MP letters):
7 complaints related to current Continuing Healthcare (CHC) – relating to the decision-making process and the decisions
5 related to Previously Un-assessed Periods of Care (PUPoC) claims – the time taken, the process and the decisions
3 related to commissioning
2 related to Individual Funding Requests – non-eligibility
2 complaints relate to the CHC Appeals – the time taken, and the decisions.
1 related to Children’s CHC. The complaint which was upheld was from a solicitor. It related to a PUPoC Team error where information was sent out to the claimant rather than the solicitor handling the claim. The complaints which was partially upheld related to:
PUPoC process - documents sent to claimant before all the evidence had been received.
18
Complex Assessment Process (CAP) bed provider complained of poor communication.
CHC current – letter not received which requested a meeting, and Health & Social Care limited support for adults with Autism.
4.9.
Whistleblowing
Whistleblowing may relate to financial, employment or clinical care.
Category
2015/16 2016/17
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
Whistleblowing disclosures 0 0 0 0 1 0 0 0
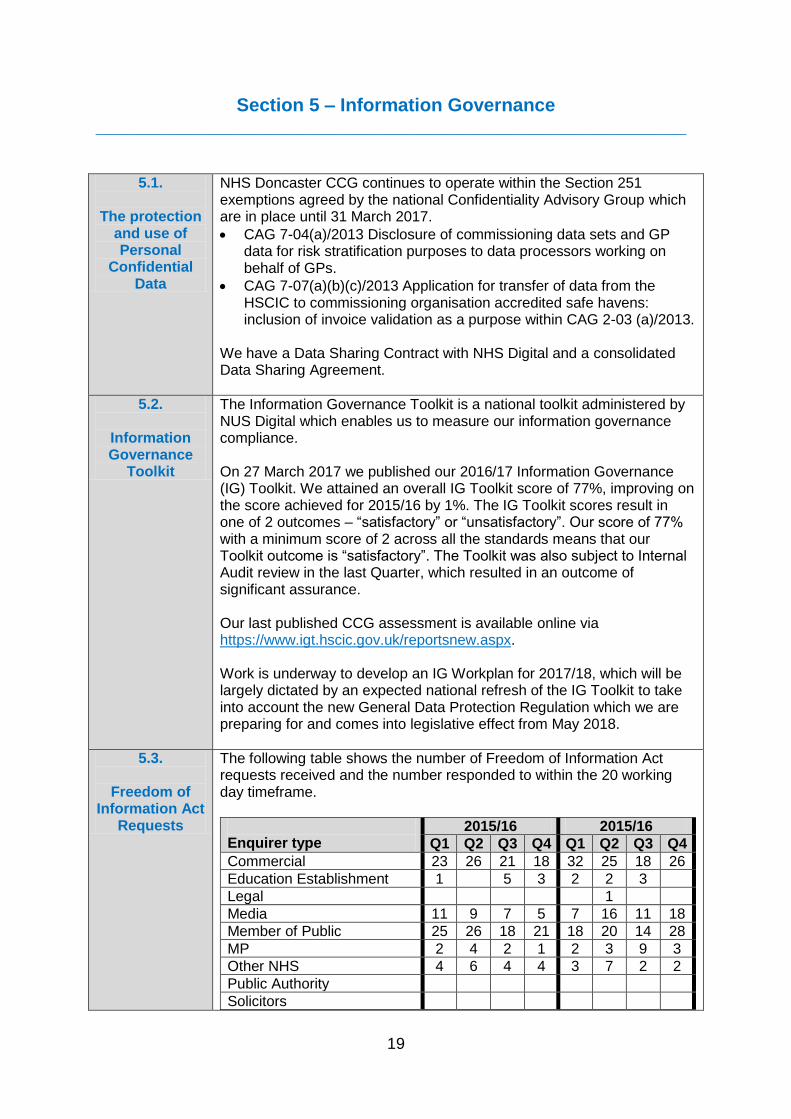
19
Section 5 – Information Governance _________________________________________________________
5.1.
The protection and use of Personal
Confidential Data
NHS Doncaster CCG continues to operate within the Section 251 exemptions agreed by the national Confidentiality Advisory Group which are in place until 31 March 2017.
CAG 7-04(a)/2013 Disclosure of commissioning data sets and GP data for risk stratification purposes to data processors working on behalf of GPs.
CAG 7-07(a)(b)(c)/2013 Application for transfer of data from the HSCIC to commissioning organisation accredited safe havens: inclusion of invoice validation as a purpose within CAG 2-03 (a)/2013.
We have a Data Sharing Contract with NHS Digital and a consolidated Data Sharing Agreement.
5.2.
Information Governance
Toolkit
The Information Governance Toolkit is a national toolkit administered by NUS Digital which enables us to measure our information governance compliance. On 27 March 2017 we published our 2016/17 Information Governance (IG) Toolkit. We attained an overall IG Toolkit score of 77%, improving on the score achieved for 2015/16 by 1%. The IG Toolkit scores result in one of 2 outcomes – “satisfactory” or “unsatisfactory”. Our score of 77% with a minimum score of 2 across all the standards means that our Toolkit outcome is “satisfactory”. The Toolkit was also subject to Internal Audit review in the last Quarter, which resulted in an outcome of significant assurance. Our last published CCG assessment is available online via https://www.igt.hscic.gov.uk/reportsnew.aspx. Work is underway to develop an IG Workplan for 2017/18, which will be largely dictated by an expected national refresh of the IG Toolkit to take into account the new General Data Protection Regulation which we are preparing for and comes into legislative effect from May 2018.
5.3.
Freedom of Information Act
Requests
The following table shows the number of Freedom of Information Act requests received and the number responded to within the 20 working day timeframe.
Enquirer type
2015/16 2015/16
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
Commercial 23 26 21 18 32 25 18 26
Education Establishment 1 5 3 2 2 3
Legal 1
Media 11 9 7 5 7 16 11 18
Member of Public 25 26 18 21 18 20 14 28
MP 2 4 2 1 2 3 9 3
Other NHS 4 6 4 4 3 7 2 2
Public Authority
Solicitors
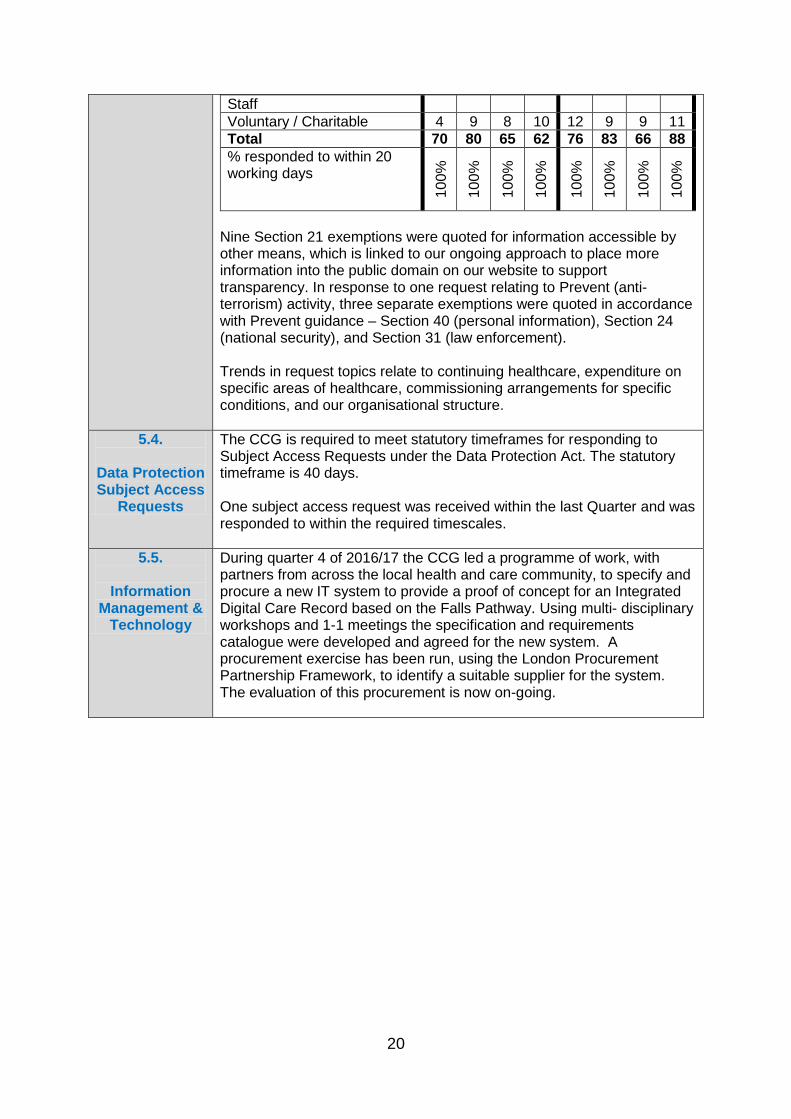
20
Staff
Voluntary / Charitable 4 9 8 10 12 9 9 11
Total 70 80 65 62 76 83 66 88
% responded to within 20 working days
100%
100%
100%
100%
100%
100%
100%
100%
Nine Section 21 exemptions were quoted for information accessible by other means, which is linked to our ongoing approach to place more information into the public domain on our website to support transparency. In response to one request relating to Prevent (anti-terrorism) activity, three separate exemptions were quoted in accordance with Prevent guidance – Section 40 (personal information), Section 24 (national security), and Section 31 (law enforcement). Trends in request topics relate to continuing healthcare, expenditure on specific areas of healthcare, commissioning arrangements for specific conditions, and our organisational structure.
5.4.
Data Protection Subject Access
Requests
The CCG is required to meet statutory timeframes for responding to Subject Access Requests under the Data Protection Act. The statutory timeframe is 40 days. One subject access request was received within the last Quarter and was responded to within the required timescales.
5.5.
Information Management &
Technology
During quarter 4 of 2016/17 the CCG led a programme of work, with partners from across the local health and care community, to specify and procure a new IT system to provide a proof of concept for an Integrated Digital Care Record based on the Falls Pathway. Using multi- disciplinary workshops and 1-1 meetings the specification and requirements catalogue were developed and agreed for the new system. A procurement exercise has been run, using the London Procurement Partnership Framework, to identify a suitable supplier for the system. The evaluation of this procurement is now on-going.
21
Section 6 – Financial Governance _________________________________________________________
Financial procedures and
systems
The Standing Financial Instructions, Standing Orders and Scheme of Delegation are in date, having been updated in March 2016 to mirror our Constitutional changes.
Financial Governance
Losses and Special Payments: Following a break-in at a General Practice, the CCG replaced two stolen PCs from the stocks held by the CCG. The cost of the replacement PCs was estimated at £1,377.43. The incident was reported to the police. Waivers for SFIs: No new applications to waive the tenders and quotes procedures have been processed during the Quarter. Debtors/Creditors: As at quarter-end there were a minimum number of outstanding Debtor and Creditor balances. Declarations of Interest: The NHS Doncaster CCG Declarations of Interests Register was being actively updated from September 2016 in accordance with the new definitions of interests in the revised NHS England statutory guidance for CCGs. Training has also been held to brief staff on the key policy changes. Disclosure of Gifts and Hospitalities: There have been no gifts or hospitality accepted by the organisation in line with the Standards of Business Conduct & Conflicts of Interest Policy during the Quarter.
Counter Fraud The CCG’s Counter Fraud Specialist (CFS) is commissioned via 360 Assurance. The Audit Committee receives assurance via Counter Fraud reports which cover the areas of contract performance, strategic governance, inform and involve, and prevent and deter. In the last Quarter a Counter Fraud update and a Counter Fraud Work Plan for 2017/18 were received. The Counter Fraud Self-Review Tool (SRT) was also completed and submitted by 31 March 2017 with a “Green” rating. The Fraud, Corruption & Bribery Policy was refreshed and approved by Audit Committee.
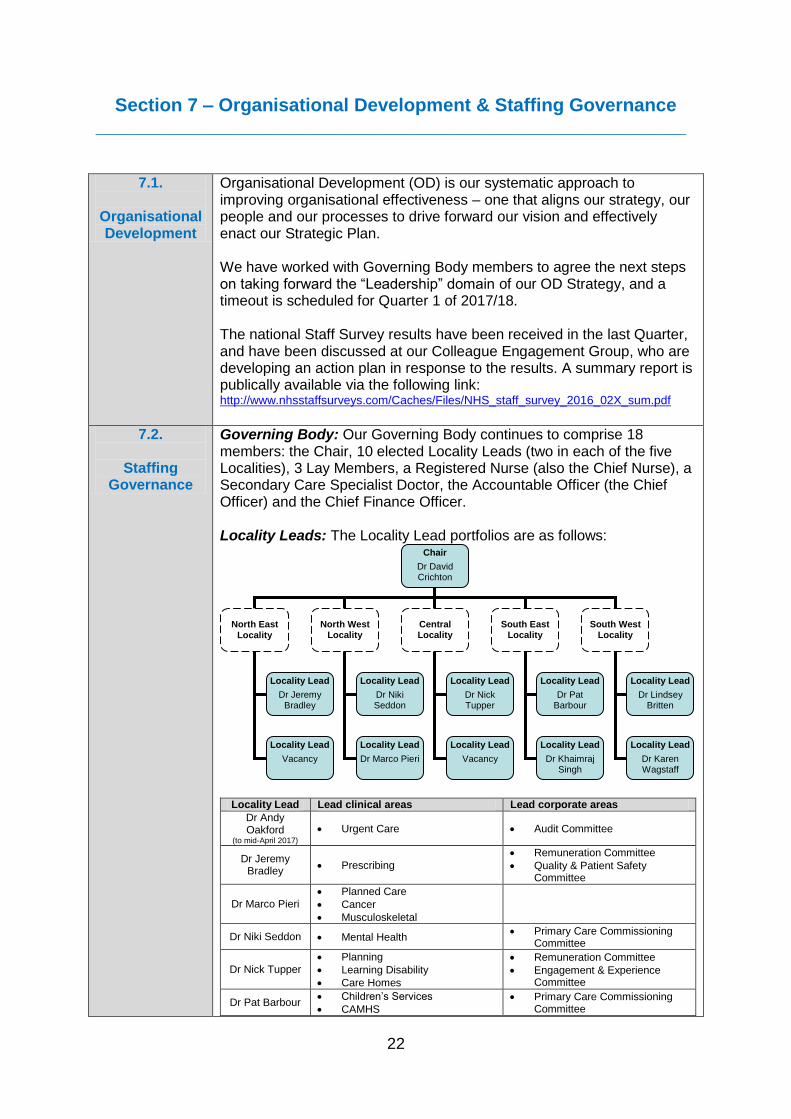
22
Section 7 – Organisational Development & Staffing Governance _________________________________________________________
7.1.
Organisational Development
Organisational Development (OD) is our systematic approach to improving organisational effectiveness – one that aligns our strategy, our people and our processes to drive forward our vision and effectively enact our Strategic Plan. We have worked with Governing Body members to agree the next steps on taking forward the “Leadership” domain of our OD Strategy, and a timeout is scheduled for Quarter 1 of 2017/18. The national Staff Survey results have been received in the last Quarter, and have been discussed at our Colleague Engagement Group, who are developing an action plan in response to the results. A summary report is publically available via the following link: http://www.nhsstaffsurveys.com/Caches/Files/NHS_staff_survey_2016_02X_sum.pdf
7.2.
Staffing Governance
Governing Body: Our Governing Body continues to comprise 18 members: the Chair, 10 elected Locality Leads (two in each of the five Localities), 3 Lay Members, a Registered Nurse (also the Chief Nurse), a Secondary Care Specialist Doctor, the Accountable Officer (the Chief Officer) and the Chief Finance Officer. Locality Leads: The Locality Lead portfolios are as follows:
Locality Lead Lead clinical areas Lead corporate areas
Dr Andy Oakford
(to mid-April 2017) Urgent Care Audit Committee
Dr Jeremy Bradley
Prescribing
Remuneration Committee
Quality & Patient Safety Committee
Dr Marco Pieri Planned Care
Cancer
Musculoskeletal
Dr Niki Seddon Mental Health Primary Care Commissioning
Committee
Dr Nick Tupper Planning
Learning Disability
Care Homes
Remuneration Committee
Engagement & Experience Committee
Dr Pat Barbour Children’s Services
CAMHS
Primary Care Commissioning Committee
Chair
Dr David Crichton
North East Locality
North West Locality
Central Locality
South East Locality
South West Locality
Locality Lead
Dr Jeremy Bradley
Locality Lead
Vacancy
Locality Lead
Dr Niki Seddon
Locality Lead
Dr Marco Pieri
Locality Lead
Dr Nick Tupper
Locality Lead
Vacancy
Locality Lead
Dr Pat Barbour
Locality Lead
Dr Khaimraj Singh
Locality Lead
Dr Lindsey Britten
Locality Lead
Dr Karen Wagstaff
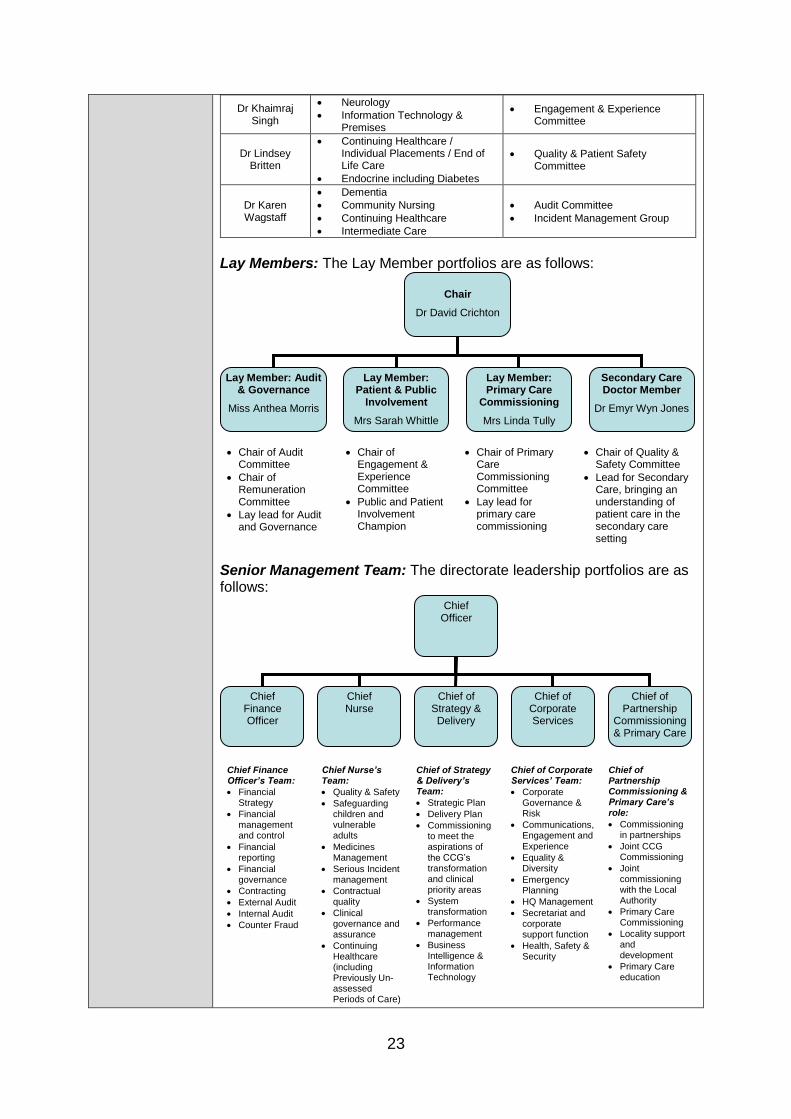
23
Dr Khaimraj Singh
Neurology
Information Technology & Premises
Engagement & Experience Committee
Dr Lindsey Britten
Continuing Healthcare / Individual Placements / End of Life Care
Endocrine including Diabetes
Quality & Patient Safety Committee
Dr Karen Wagstaff
Dementia
Community Nursing
Continuing Healthcare
Intermediate Care
Audit Committee
Incident Management Group
Lay Members: The Lay Member portfolios are as follows:
Chair of Audit Committee
Chair of Remuneration Committee
Lay lead for Audit and Governance
Chair of Engagement & Experience Committee
Public and Patient Involvement Champion
Chair of Primary Care Commissioning Committee
Lay lead for primary care commissioning
Chair of Quality & Safety Committee
Lead for Secondary Care, bringing an understanding of patient care in the secondary care setting
Senior Management Team: The directorate leadership portfolios are as follows:
Chief Finance Officer’s Team:
Financial Strategy
Financial management and control
Financial reporting
Financial governance
Contracting
External Audit
Internal Audit
Counter Fraud
Chief Nurse’s Team:
Quality & Safety
Safeguarding children and vulnerable adults
Medicines Management
Serious Incident management
Contractual quality
Clinical governance and assurance
Continuing Healthcare (including Previously Un-assessed Periods of Care)
Chief of Strategy & Delivery’s Team:
Strategic Plan
Delivery Plan
Commissioning to meet the aspirations of the CCG’s transformation and clinical priority areas
System transformation
Performance management
Business Intelligence & Information Technology
Chief of Corporate Services’ Team:
Corporate Governance & Risk
Communications, Engagement and Experience
Equality & Diversity
Emergency Planning
HQ Management
Secretariat and corporate support function
Health, Safety & Security
Chief of Partnership Commissioning & Primary Care’s role:
Commissioning in partnerships
Joint CCG Commissioning
Joint commissioning with the Local Authority
Primary Care Commissioning
Locality support and development
Primary Care education
Chief Officer
Chief Finance Officer
Chief Nurse
Chief of Strategy & Delivery
Chief of Corporate Services
Chief of Partnership
Commissioning & Primary Care
Chair
Dr David Crichton
Lay Member: Audit & Governance
Miss Anthea Morris
Lay Member: Patient & Public
Involvement
Mrs Sarah Whittle
Lay Member: Primary Care
Commissioning
Mrs Linda Tully
Secondary Care Doctor Member
Dr Emyr Wyn Jones
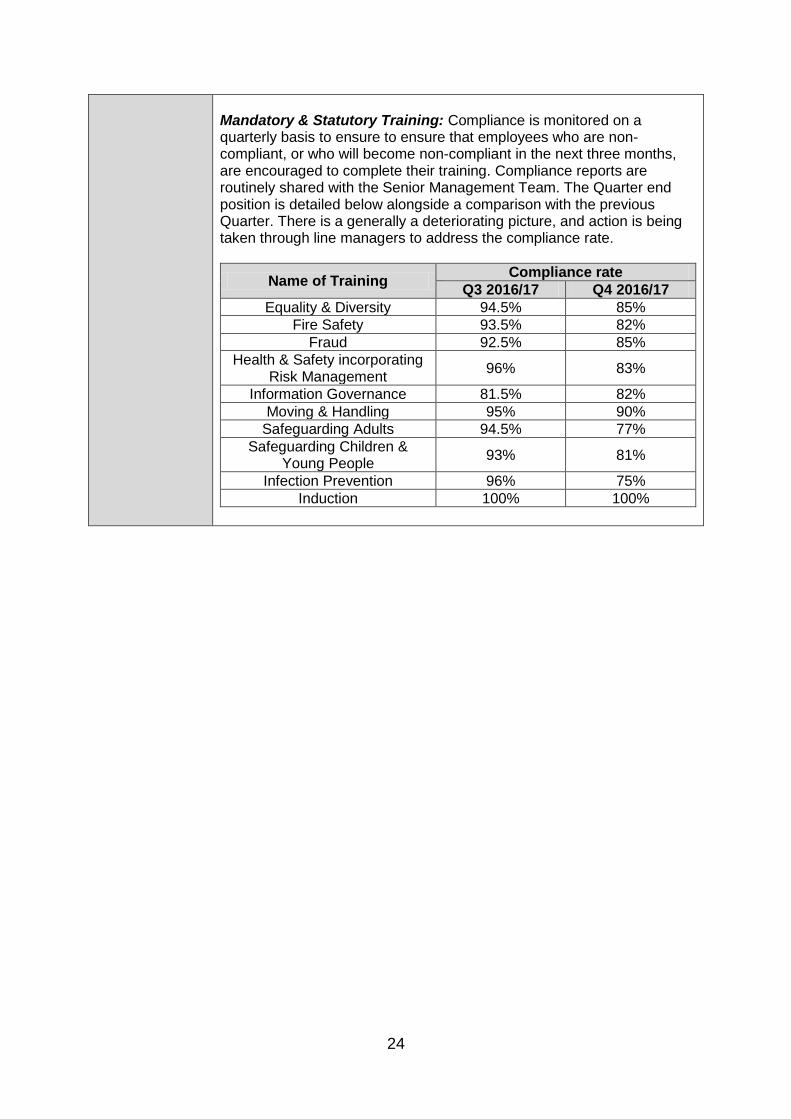
24
Mandatory & Statutory Training: Compliance is monitored on a quarterly basis to ensure to ensure that employees who are non-compliant, or who will become non-compliant in the next three months, are encouraged to complete their training. Compliance reports are routinely shared with the Senior Management Team. The Quarter end position is detailed below alongside a comparison with the previous Quarter. There is a generally a deteriorating picture, and action is being taken through line managers to address the compliance rate.
Name of Training Compliance rate
Q3 2016/17 Q4 2016/17
Equality & Diversity 94.5% 85%
Fire Safety 93.5% 82%
Fraud 92.5% 85%
Health & Safety incorporating Risk Management
96% 83%
Information Governance 81.5% 82%
Moving & Handling 95% 90%
Safeguarding Adults 94.5% 77%
Safeguarding Children & Young People
93% 81%
Infection Prevention 96% 75%
Induction 100% 100%
Enc E
Item 10
Chair & Chief Officer Report

1
Meeting name Governing Body
Meeting date 18 May 2017
Title of paper
Chair and Chief Officer Report
Executive / Clinical Lead(s)
Dr David Crichton, Clinical Chair Mrs Jackie Pederson, Chief Officer
Author(s) Mrs Sarah Atkins Whatley, Chief of Corporate Services
Purpose of Paper - Executive Summary
The purpose of this report is to update the Governing Body on issues relating to the activity of the CCG of which the Governing Body needs to be aware, but which do not themselves warrant a full Governing Body paper. This month the paper includes updates on the following areas:
• Doncaster Place Plan update
• Patient Transport Services Contract Award
• Involving people in health and care
• Workplace Wellbeing Charter
• Annual Review letter from NHS England
• Pre-Election Period
Recommendation(s)
The Governing Body is asked to:
• Note the report.
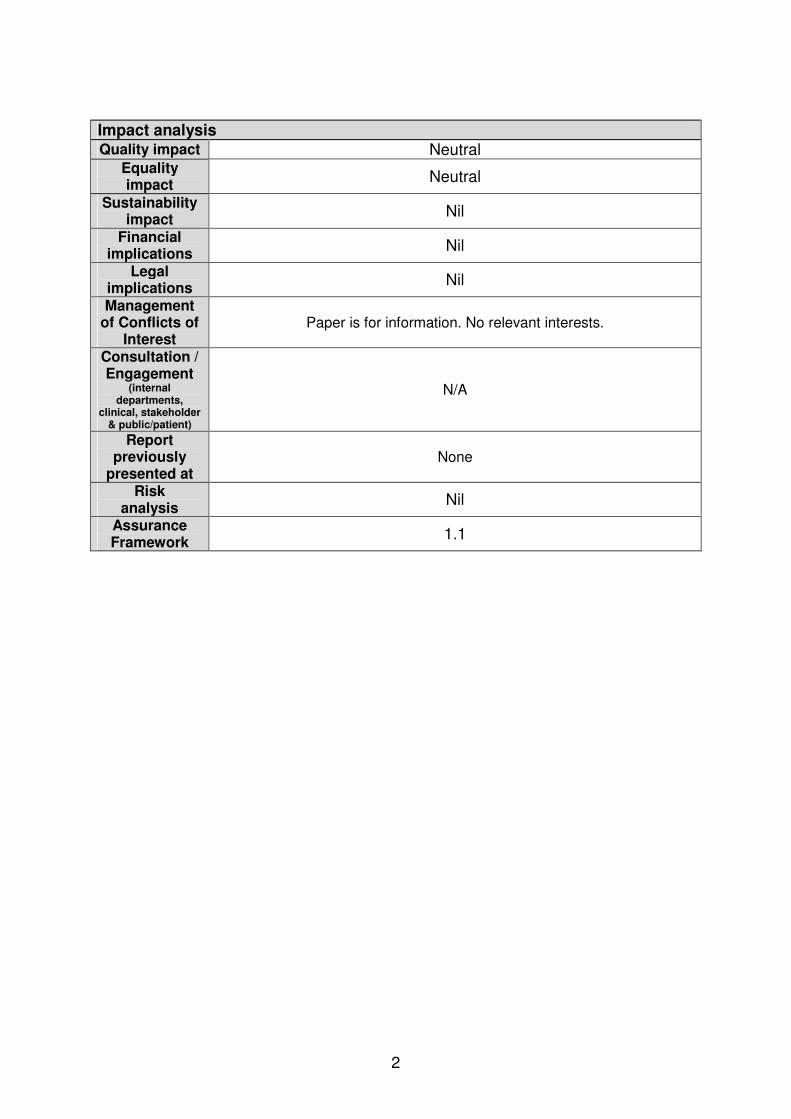
2
Impact analysis Quality impact Neutral
Equality impact
Neutral
Sustainability impact
Nil
Financial implications
Nil
Legal implications
Nil
Management of Conflicts of
Interest Paper is for information. No relevant interests.
Consultation / Engagement
(internal departments,
clinical, stakeholder & public/patient)
N/A
Report previously
presented at None
Risk analysis
Nil
Assurance Framework
1.1
3
Chair and Chief Officer Report
May 2017 1. Doncaster Place Plan update Our Doncaster Place Plan strategic partner, EY, have concluded a Phase 1 State of Readiness Report on the Doncaster Place Plan. The report highlights the significant amount of work undertaken to date and shared commitment across the partners to the aspirations in the published Place Plan. 5 workstreams have been identified for the next phase of implementation:
1. Programme set-up: programme management. 2. System and Service Design: defining the outcomes, specification and service
model to deliver improved health and care in Doncaster. 3. Leadership Development: to support system leadership. 4. Operating Framework Development: providers considering how they may
want to organise themselves to deliver the outcomes specified. 5. Communication & Engagement: a continuous process.
2. Patient Transport Services Contract Award A joint procurement process for the provision of a non-emergency patient transport service (NEPTS) for the patients of Barnsley, Doncaster, Rotherham and Sheffield has been undertaken. The NEPTS was divided into ‘Lots’ based on activity type and bidders competed for each lot. The multi stage process resulted in two bidders being awarded the following contracts:
• The Thames Ambulance Service was awarded the contract for Lot 1A “On day discharges”.
• The remaining lots were awarded to the Yorkshire Ambulance Service: o Lot 1 Core PTS o Lot 3 Ad-hoc transport o Lot 4 GP Urgents (Sheffield)
The contracts are expected to start on 1st September 2017 and have been awarded for the duration of 5 years. Contract award was made and publically announced prior to the commencement of the Pre-Election Period.
4
3. Involving people in health and care Working with CCGs and a range of other stakeholders, NHS England has developed refreshed statutory guidance on involvement. The guidance highlights the benefits of involving people in their own health and care and involving communities in commissioning decisions. It reflects the new commissioning landscape and sets out the context and principles of involvement. The guidance is made up of two documents, “Involving people in their own health and care” and “Patient and public participation in commissioning health and care”. https://www.england.nhs.uk/participation/involvementguidance/ Team members across all Directorates in the CCG have been briefed on the new guidance, and the principles in the guidance are reflected in the newly refreshed engagement principles of the CCG:
• Lived experience is vital in commissioning healthcare services effectively.
• Engage together in partnership across Doncaster health and social care services wherever possible, avoiding duplication of engagement activity.
• Centralise feedback wherever possible through the local statutory voice of the users of health and social care services – Healthwatch Doncaster.
• Focus CCG engagement activity on the priority areas of the CCG, identifying the best engagement option for each priority area using the Ladder of Engagement.
• Engagement should be:
• Planned (with a clear purpose, scope, limitations and outcomes)
• Productive (with a focus on improving health outcomes)
• Undertaken early (before decisions are made)
• Open, transparent & empowering (clear on what can be influenced)
• Ongoing (proactive conversations rather than reactive to changes)
• Inclusive (including targeting more seldom heard groups)
• Accessible (times, places, methodologies)
• Sustainable (with adequate time and resources)
• Take the time to feed back to contributors on the outcome of engagement activity, and celebrate engagement successes.
Our Communication & Engagement Strategy is now being refreshed to reflect these engagement principles.
5
4. Workplace Wellbeing Charter The Workplace Wellbeing Charter is an organisational statement of intent, showing organisational commitment to the health of employees. NHS Doncaster CCG is currently working towards achieving the Charter. Benefits of adopting the Charter include:
• The ability to audit and benchmark against an established and independent set of standards – identifying what the organisation already has in place and what gaps there may be in the health, safety and wellbeing of our employees.
• Developing strategies and plans – the Charter provides a clear structure that organisations can use to develop health, safety & wellbeing strategies and plans.
• National recognition – The Charter award process is robust and evidence based. Over 1,000 organisations across England hold the award. The Workplace Wellbeing Charter is widely recognised as the business standard for health, safety & wellbeing across England. As a Health organisation it is good to achieve and lead by example.
Recent CCG Workplace Wellbeing initiatives have included:
• A monthly organisational news round-up emails to keep all team members up to date with CCG news
• A new Joint Negotiation & Consultative Forum with Staff Side colleagues
• Lunchtime “Mindfulness” sessions
• On-site Health Checks
• After-work Yoga sessions run by a staff member
• Employee-funded stress/sports massage sessions outside of work time
• Blood pressure checks
• Cycle to work scheme As part of the Occupational Health service, team members also have access to an Employee Assistance Programme to help them deal with personal problems that might adversely impact their work performance, health, and wellbeing. The service provides access to:
• Stress helpline
• Structured telephone counselling
• Referral to face to face counselling via a network of over 600 British Association of Counsellors and Psychotherapist (BACP) across the UK
• Referral to serious illness and accident support
• A range of engaging and useful online tools including: o Emotional support o Fitness advice (including video demonstrations) o Personal coaching tool o Health assessment
6
5. Annual Review letter from NHS England Following our CCG Annual Review with NHS England in April 2017, the formal feedback letter from NHS England has been received and is attached to this report as Appendix A. 6. Pre-Election Period We have now entered the pre-election period. As usual, the Cabinet Office has published General Election guidance for the civil service; NHS England has summarised how the guidance applies to the NHS. Until after a new Government has been formed, there should be:
• No new decisions or announcements of policy or strategy;
• No decisions on large and/or contentious procurement contracts;
• No participation by NHS its representatives in debates and events which may be politically controversial.
The guidance applies to all communications, including social media. Locally we were already in a pre-election period because of the local elections and mayoral elections which took place in early May 2017. The new restrictions run through to the General Election on 8 June 2017. 7. Recommendations The Governing Body is asked to:
• Note the report.
Dr David Crichton, Chair Jackie Pederson, Accountable Officer Doncaster CCG
Dear David and Jackie, RE: CCG 2016/17 ANNUAL REVIEW Thank you for meeting with us on 12 April 2017 for your Annual Review Meeting. The purpose of this letter is to provide feedback on the key issues we discussed, and to confirm next steps for the publication of the 2016/17 Annual Performance Assessment.
As you will be aware, NHS England has a statutory duty to conduct an annual performance assessment of each CCG. The Government’s Mandate to NHS England specifies the four ‘Ofsted-style’ headline categories to be used: Outstanding; Good; Requires Improvement and Inadequate.
Whilst the methodology for the calculation of the 2016/17 Annual Performance Assessment has not yet been published, it is likely that the Quality of Leadership (QoL) indicator will be significantly weighted, and will account for 30% of the overall judgement alongside the two finance indicators accounting for 20%. The remaining 50% will be made up of the rating against the six clinical priority areas. Each of the six clinical priority areas has an independent national panel that will make an assessment; in June 2017 you will be given a rating on each of these six clinical areas using Ofsted terminology which will then contribute to the overall rating.
Reflections on 16/17
We discussed the CCG’s key achievements in 2016/17 and particularly the focus the CCG has on improving outcomes for the population of Doncaster. We celebrated the success of your relatively new leadership team, which presents a coherent plan for the CCG, but also undertakes a significant leadership role across Doncaster at place, and across the wider SYB STP footprint. We discussed the significant strides made in developing relationships across the system, enabling partnership working.
I commended you on the leadership role you undertake in relation to Transforming Care, and thanked you for the work you have led on behalf of 9 CCGs across Yorkshire & Humber on PUPoC. We acknowledged the challenge ahead in terms of
Direct 0113 82 47511 Date: 8 May 2017
NHS England – North (Yorkshire & the Humber)
3 Leeds City Office Park Meadow Lane
Leeds LS11 5BD
the clarity regarding the second wave, and I confirmed that we will continue to push for clarity.
We discussed the recent RTT performance at DBH, and acknowledged that the Trust has an RTT recovery plan in place which is not directly aligned to the commissioner’s plans to deliver 92% throughout 2017/18. We noted your positive engagement in the regional demand management work and that you have a number of schemes in place to manage referral demand. You have also refreshed the governance arrangements around elective care, and have established a Planned Care Board constituted of all partners to oversee planned care.
We discussed the A&E performance at DBHFT and the executive level focus on urgent and emergency care, achieved through the A&E Delivery Board which spans Bassetlaw and Doncaster and the role of local SRGs which continue, focusing on local system delivery.
Performance against the cancer 62 day urgent standard has been a challenge throughout the year. This is attributed largely to tertiary referrals rather than performance at the DGH and it is expected that the work of the Cancer Alliance board in re-defining cancer pathways and agreeing inter-provider transfer protocols will have a positive impact on performance.
Operational and Financial Plans for 2017-19
The CCG’s operational and financial plans have been submitted and approved locally for 2017-19. The financial plan achieves all business rules and includes challenging, but realistic efficiency savings. We acknowledged that there is limited mitigation in plans and that pressures continue to emerge and so there will be a continuous programme of review throughout 2017 – 19.
All contracts were agreed by the December 2016 deadline and activity trajectories are agreed, and in the main are aligned to contracts.
You described the robust approach undertaken to QIPP planning, and your QIPP is fully aligned to delivery plans.
Finally, we congratulated you on collectively agreeing the SYB financial control total.
CCG “Place Strategy”
We discussed the CCG strategy to move to an Accountable Care Partnership (ACP) model. We discussed the future contracting model, and you described a number of mechanisms to test out different models, including testing a capitated budget within intermediate care services and an alliance contract for urgent and emergency care service. You have external support in reviewing the various contracting options from Ernst and Young (EY) and will continue to utilise this to support commissioning decisions. We acknowledged that whilst place is where the majority of the required
transformation will occur, the development of effective system wide commissioning across the STP for hospital services will be essential for the health and care of Doncaster residents. As with other CCGs you will have to balance place and wider STP commissioning appropriately to ensure you get the best outcomes for health.
Wider STP Implementation
We discussed the wider STP implementation and in particular, the Sustainable Hospitals Review. We discussed the importance of commissioner leadership in reviewing services to ensure the best possible outcomes for our patients across South Yorkshire & Bassetlaw, and I encouraged you to continue to ensure that the Doncaster voice is heard.
It is clear from our discussions that the CCG is working at a very high level of performance delivering well through your leadership and the hard work of the organisation. Thank you.
I will write to you again in June / July with your finalised Annual Assessment Results. In the meantime, please do not hesitate to contact Alison Knowles or Mark Janvier should you require any further information.
Yours sincerely
Moira Dumma
Director of Commissioning Operations

Verbal
Item 11
Locality Feedback
Enc F
Item 12
Receipt of Minutes

1
Minutes of the Audit Committee Held on Thursday 9th March 2017 at 9:00-11:30am
Meeting Room 3, Sovereign House, Heavens Walk, Doncaster, DN4 5HZ Committee Members Present
Miss Anthea Morris (Chair) Lay Member Dr Andrew Oakford Locality Lead Dr Karen Wagstaff Locality Lead Mrs Sarah Whittle Lay Member Dr Emyr Wyn Jones Secondary Care Doctor Lead
Formal Committee Members Present:
Mrs Sarah Atkins Whatley Chief of Corporate Services Mrs Hayley Tingle Chief Finance Officer Mrs Annette Tudor Internal Audit – 360 Assurance Mrs Tracy Wyatt Deputy Chief Finance Officer
Mr James Boyle External Auditor, KPMG Mrs Amanda Smith Counter Fraud Specialist In attendance: Miss Lindsay Moore Senior Corporate Services
Support Officer (taking Notes) Mrs Claire Burns Head of Procurement and
Business Support (for item 8.5) Mr Gareth Jones Corporate Governance Manager
(observing)
Action 1 Apologies for Absence
Apologies were received from:
Mrs Claire Partridge, External Auditor, KPMG
2 Declarations of Interest The Chair reminded committee members of their obligation to declare any interest they may have on any issues arising at committee meetings which might conflict with the business of NHS Doncaster Clinical Commissioning Group (CCG). Declarations declared by members of the committee are listed in the CCG’s Register of Interests. The Register is available either via the secretary to the Governing Body or the CCG website at the following link: www.doncasterccg.nhs.uk The meeting was noted as quorate. Declarations of interest from sub committees / working groups: None declared.
2
Declarations of interest from today’s meeting: None Declared.
3 Minutes of the meeting held on 12th January 2017 The minutes of the meeting held on 12 January 2017 were agreed as an accurate record.
4 Matters Arising via Action Tracker The actions within the tracker were noted as complete.
5 External Audit 5.1 External Audit Technical Update Mr Boyle advised that the Internal Audit has been completed and there have been no issues found which are foreseen to alter the year end Audits. The knowledge and understanding of key risks has been updated and there are no key risks identified. Mr Boyle presented the External Audit Technical Update to the Committee for noting and information purposes and advised that the Audit Deliverables are outlined on page 5. Mr Boyle advised that one key change to the update is the addition of KPMGCentral which is a web based, secure online collaboration space that connects you and your team to KPMG’s global network of member firms. Once registered, you can use it to access engagement documents, monitor engagement milestones and pose questions to your KPMG engagement team through any web browser. Mr Boyle agreed to send information to Mrs Atkins Whatley regarding the encryption of the Information Governance Toolkit if this is to be used with KPMGCentral. Mrs Atkins Whatley advised that discussions have been held around this and the use of the system is recommended to Audit Committee to be used for the final Audit. The committee noted that NHSE have advised us to continue to use the CCG guidance around conflicts of interest for the present time. Dr Wagstaff noted that there may be a lack of awareness that we have to declare ‘declined’ offers of gifts and hospitality if they are over the value of £10. Mrs Smith said that this could be a training
3
issue to be looked at. Mrs Tingle joined the meeting 5.2 Appointment of External Auditors Mrs Tingle advised that Governing Body have approved the re -appointment of KPMG and official notice has been given of the appointment.
6 Internal Audit 6.1 Internal Audit Progress Report and Technical Update Mrs Tudor informed the Committee that Delivery of work from the 2016/17 Internal Audit Plan is progressing and that four reports have been issued since the last Audit Committee meeting:
Conflicts of Interest. The CCG has been assessed as ‘compliant’ in all 5 areas 360 Assurance were required to examine in the NHSE mandated review. This is an excellent performance and compares favourably with our findings elsewhere;
Budgetary Control & Key Financial Systems. A significant assurance has been issued in respect of the overall control environment examined.
Information Governance Toolkit. A significant assurance has been issued in respect of the overall control environment examined.
Governing Body Development Session Output. A report has been developed to show the actions that were agreed at the session in respect of revising the CCG’s Strategic Objectives and identifying principal risks for inclusion on the 2017/18 Assurance Framework
Mrs Tudor advised that the Primary Care Quality benchmark work is on-going and conversations are being held with the CCG to identify processes and direction of travel, follow up activity and implementation of recommendations are also being looked at. The Audit Committee noted the report and the assurances contained within it. 6.2 Review of Internal Audit SLA 2017/18 Mrs Tingle informed the committee that the SLA for 2016/17 is in place and there is no end date in the contract for 2017/18 however
4
this is being looked at. No change in the KPI is envisaged and it is currently at 90% compliance. Mrs Tingle raised the issue of attendance at the 360 Consortium Boards, these often clash with other meetings which means it is difficult for Mrs Tingle or a suitable representative to attend. Mrs Tudor agreed to look at the meeting schedule to establish if any changes can be made and also informed the committee that if difficulties continue to arise Tim Thomas is happy to meet with CFO’s individually. 6.3 Draft Head of Internal Audit Opinion Work is on-going in respect of Stage 4 of the Head of Internal Audit Opinion, including the completion of some follow-ups to ensure clearance of recommended actions. The draft Opinion should be issued by the required deadline of the 17th of March 2017 and at this stage are expecting to be issued a Significant Assurance. 6.4 Strategic Internal Audit Plan 2017-2020 As a result of the planning meeting held Audit Committee and members of the CCG’s Senior Management Team, a Strategic Internal Audit Plan for 2017-2020 has been prepared. The Plan has been predicated on the basis of 120 days being delivered during the year, in line with the discussions that have taken place with the Senior Management Team in relation to the availability of CCG resources for the completion of internal audit reviews. The Committee approved the Strategic Internal Audit Plan 2017-2020 6.5 Review of Counter Fraud Progress Report Mrs Smith informed the Committee that this report outlines the work completed to date in respect of the DCCG 2016/17 Counter Fraud, Bribery and Corruption Operational Plan. The following key points were highlighted:
NHS Protect issued a circular in November 2016 which advised that a new submission deadline of 1 April 2017 (previously 31 May) will apply to fraud, bribery and corruption SRT submissions.
NHS Protect Standards 1.8-1.9. The CFS has issued a draft procedural document to the CCG to outline the actions needed to comply with two standards which relate to the CCG’s responsibility to ensure that the providers it contracts with to deliver NHS services comply with Service Condition 24 of the NHS Standard Contact. There has currently only been one provider that has been unwilling to share the information with 360 assurance. Mrs Atkins Whatley confirmed that she is aware of this and the matter is being dealt with.
Mrs Tudor
5
Risk Assessment. The CFS has prepared the CCG’s local fraud risk assessment for 2017/18 in accordance with updated standards as advised by NHS Protect.
National Conferences. Since the previous reporting period, 360 Assurance CFS have attended two national conferences of relevance to our roles and of benefit to our client organisations. The first was run by the Chartered Institute of Internal Auditors and the Fraud Advisory Panel and concerned fighting fraud with proactive tools
Cyber Crime Event. Following a recent successful cyber-attack at a local Foundation Trust, CFS staff attended a training event hosted by the Yorkshire & Humber Regional Cyber Crime Unit. The seminar highlighted current and emerging cyber threats and the key actions health bodies should take to ensure they are addressed. Staff awareness of cyber-crime risks is a key factor in fighting this emerging threat and the CFS has published an article in the latest CCG’s Counter Fraud newsletter.
Scam Warnings. The CFS has provided staff with warnings regarding locally identified scams and instances of sharp practice by forwarding details to the Chief Finance Officer and, where appropriate, the Communications Team for dissemination to staff. Details of local concerns have also been included within the Fraudulent Times newsletter.
There has been 2 scam alerts issued during this reporting period;
Warning of fake UKPC parking ticket email loaded with malware;
Email to Audit Committee members containing malicious software and viruses.
The committee noted the report and the information contained within. 6.6 Approval of Counter Fraud Work-Plan 2017/18 Mrs Smith advised that the work-plan has been agreed with Mrs Tingle and highlights the CCG’s local fraud, bribery and corruption risk assessment and related proposals for anti-fraud, bribery and corruption activity in 2017/18. There have been no individual areas of extreme fraud risk h highlighted, it has been shown that fraud revelation is often the result of a significant number of low and medium impact risks, rather than a single significant impact event. This means that the amount and variety of fraud, bribery and corruption risks identified suggests that the likelihood of fraud, bribery and corruption being perpetrated against the CCG continues to be substantial.
6
The Committee noted the report and assurances contained within it.
7 Financial Reporting 7.1 Finance Exception Reports Mrs Wyatt presented the report to the committee and the following points were noted;
Following a break-in at the Burns Practice, the CCG replaced two stolen PCs from the stocks held by the CCG. The cost of the replacement PCs was estimated at £1,377.43. The incident was reported to the police.
The Audit Committee is required to approve the writing off of all losses and special payments made up to £10,000 in value
No new applications to waive the tenders and quotes procedures have been processed since the last meeting.
There are four outstanding Debtors over six months old and over £5,000:
o First Care Ltd (The Hollies) £75,440.95 – This is in relation to an overpayment on a schedule payment which is being recouped by withholding future CHC payments. So far £34k has been withheld and the net balance is therefore £41k.
o DMBC two invoices (£16,606.91 & £7,011.05) relating to recharges of Children’s CHC cases. DMBC need to provide a PO number in order for these to be released. This is being actively chased with DMBC
o PHB patient £5,901.54 – instalment terms being discussed with the patient
There are currently 27 outstanding Creditors over six months old totalling £1,520,967. The two key suppliers are DMBC £766,829 and Property Services £395,822.
The Committee noted the report and approved the write off of the loss of the 2 PCs. 7.2 Agreement of Final Accounts timetable and plans/progress The SBS deadlines were incorporated into the timetable before it was circulated to the Finance Team, a meeting has been arranged to discuss the timetable although there are no issues anticipated. Finance staff have attended the Annual Accounts workshops run by NHS England and KPMG. The committee agreed that the following meetings will be needed to discuss the financial accounts and the following dates are to be
7
added to diaries;
11th May 2017 – Formal Audit Committee minus the reports from External Audit.
18th May 2017 – Extra Ordinary Audit Committee – for Audit Committee Members and External Audit Members.
4th May 2017 – Informal Audit Committee for Audit Committee Members only.
25th May -Extra Ordinary Governing Body Meeting to discuss the Draft ISA 260.
7.3 Review of Banking arrangements Mrs Tingle informed the committee that the arrangements are mandated by NHSE and we have 1 bank account that is managed by the finance team and reviewed annually. All requirements are currently being met.
8 Integrated Governance, Risk Management and Internal Control. 8.1 Quarter 3 Corporate Assurance Report Mrs Atkins Whatley informed the Committee that the report has been presented to Governing Body and the following point were noted;
The Assurance Framework retains the same 21 risks as in Quarter 2 and a deep dive review of the Framework is scheduled for Quarter 4. As at the end of the Quarter, the Risk Register held 26 risks. 8 of these risks were being treated: A&E 4-hour wait, e-cigarettes prescribing position (new risk), completion of PUPOC reviews by the required deadline, primary care prescribing quality & cost effectiveness, data quality in respect of referrals and activity, ambulance handover times (new risk), cancer 62 day target achievement (new risk), and implementation of the Section 117 “Who Pays” guidance. The action plans were all running to schedule.
There have been six incidents reported in the last Quarter. Five of the incidents were information governance issues, and all originated from outside the CCG and were not breaches by our team members or for our organisation.
The Governing Body, under delegated authority from Member Practices, agreed to enter into a Joint Committee with other CCGs and NHS England for the Commissioners Working Together programme; this was formerly a collaborative partnership arrangement as referenced in our Constitution.
We participated in Exercise Cygnus during October 2016,
8
exercising the country’s plans for responding to a flu pandemic. The exercise was run from COBR downwards, and NHS Doncaster CCG participated at a South Yorkshire Health Tactical level. The learning will be fed back into the CCG.
Work is progressing well on collating evidence for the 2016/17 Information Governance Toolkit self-assessment, and an Internal Audit is scheduled for February 2017.
The Local Digital Roadmap plan has now achieved final approval from NHS England and has been published on our website.
NHS Protect have brought forward the deadline for the 2017 Counter Fraud Self-Assessment Tool. The standards are expected to be released in January 2017 for self-assessment and reporting by 31 March 2017.
This quarter the Organisational Development Strategy and underpinning action plan were refreshed and have since been approved by the Governing Body. The Strategy is broken down into six areas with a sponsor for each area. Our Colleague Engagement Group is working towards the Healthy Workplaces Award Scheme, looking at a range of different potential initiatives.
The committee noted the report and the information contained within it. 8.2 Risk Register Annual Report Mrs Atkins Whatley presented the report to the committee and the following points were noted; The Risk Register is held on a centralised spread sheet which includes risks from across the five CCG Directorates. The risks are owned by operational leads throughout the CCG. The Corporate Governance Manager meets with risk owners to review and update their risk, and also works with risk leads to add new risks to the Risk Register as and when they are identified. The entire Risk Register is presented annually to the Audit Committee. As at the end of Quarter 3:
The Risk Register held 26 risks
4 risks were scored as high, and all were being treated: o A&E 4-hour wait o E-cigarettes prescribing position o Completion of PUPOC reviews by the required
deadline o Primary care prescribing quality and cost
effectiveness
4 additional risks below the risk toleration threshold were
9
also being treated: o Data quality at DBH in respect of referrals and
activity o Ambulance handover times o Cancer 62 day target achievement o Implementation of the Section 117 “Who Pays”
guidance
The action plans associated with “treated” risks were running to schedule.
3 new risks were added relating to: o E-cigarette prescribing o Ambulance handovers o Cancer 62 day target achievement
2 risks which both related to prescribing were merged, and the risk score increased.
The Committee agreed that it would be useful to add information around the data quality in relation to Dementia to the risk register. Mrs Atkins Whatley agreed to speak to Mr Goddard around this. Audit Committee noted the report. 8.3 Probity Risk Register Report Mrs Atkins Whatley informed the Committee that the Probity Register consists of two different registers,
a. Register of Interests b. Register of Gifts, Hospitality & Sponsorship
Both of the registers are published on our website and are prepared, populated and published in accordance with NHS England’s statutory guidance. The NHS England guidance around managing Conflicts of Interest was revised and issued in late June 2016. All CCG employees, governing body and committee members, and practice staff with involvement in CCG business, are required to complete mandatory online conflicts of interest training which will be provided by NHS England once it is released. Register of Interests From September 2016, declarations were sought on a new Declarations of Interest Form which was aligned to the new descriptions of types of conflict:
Financial interests: This is where an individual may get direct financial benefits from the consequences of a commissioning decision.
Non-financial professional interests: This is where an
Mrs Atkins Whatley
10
individual may obtain a non-financial professional benefit from the consequences of a commissioning decision, such as increasing their professional reputation or status or promoting their professional career.
Non-financial personal interests: This is where an individual may benefit personally in ways which are not directly linked to their professional career and do not give rise to a direct financial benefit.
Indirect interests: This is where an individual has a close association with an individual who has a financial interest, a non-financial professional interest or a non-financial personal interest in a commissioning decision.
A completed Declaration form is required from all CCG employees, Governing Body and Committee Members, Members of the CCG (e.g. member practices). Conflict of interest forms are also issued to new employees, are required to be noted within minutes of meetings, upon a change of job role. The information is requested and reviewed on a 6 monthly basis. The Register of Interests was published on the CCG website in October 2016. A refreshed copy of the Register of Interests with updated interests was uploaded in January 2017. The register is available to members of the public and includes positive declarations for all staff, and all declarations (positive or nil) for Governing Body members and Member Practices. The full un-redacted register is held by the Corporate Governance Team. Register of Gifts, Hospitality & Sponsorship The Register of Gifts, Hospitality & Sponsorship was published on our website in October 2016. Two declarations have been made in 2016/17:
Commercial sponsorship of our GP Education Programme, TARGET. This was accepted in accordance with the separate TARGET procedure within our Standards of Business Conduct & Conflicts of Interest Policy.
Invitation from our External Audit provider to a Christmas Party: Declined.
The Committee noted the report 8.4 Implementation of Audit Committee Recommendations Mrs Wyatt presented the report to the committee and the recommendations within the report to close 7 actions and carry forward 12 was approved. Printed copies are to be provided to future Audit Committee Meetings. 8.5 Standing Orders, Standing Financial Instructions and
Miss Moore
11
Scheme of Delegation Mrs Atkins Whatley and Mrs Tingle informed the Committee that The document has been reviewed and the following amendments are recommended:
Change Quality & Safety Committee to Quality & Patient Safety Committee.
Change Delivery & Performance Committee to Executive Committee and amend the delegated roles.
Add reference within the Standing Orders and Scheme of Delegation to the Joint Committee of CCGs which has been established for the Working Together programme.
Remove reference to the obsolete NHS England definition of relevant and material interests, and replace with reference to the CCG’s Standards of Business Conduct & Conflicts of Interest Policy.
Add reference to the role of the Conflict of Interest Guardian.
Remove references to the Audit Commission.
Updating of Section 17 on Tendering and Contracting in line with the latest national guidance.
The Committee noted the document and recommended the amendments to the Governing Body for approval. Tendering Limits Mrs Burns and Mrs Tingle advised the committee that consideration is being given to increasing the tendering limits based on the consistency of our providers whilst still maintaining our responsibility for Value for Money. One quote would be required for amounts up to £5’000 3 Quotes would be required for amounts from £5’000 - £25’000 The E – Tendering process will be used for amounts in excess of £25’000 and anything over £164’000 will go via the formal procurement processes. The Committee approved the proposal in principle and requested that a full options paper be presented to Audit Committee in July 2017. 8.6 Integrated Risks arising from other Committee’s Remuneration Committee: There has been no meeting held since the April 2016 meeting, however the new Terms of Reference have been agreed virtually and will be presented to Governing Body on 16th March for approval. Engagement & Experience Committee: No risks to report, however a recent workshop was held to develop the engagement
Mrs Burns / Mrs
Tingle
12
principles and test them against the Dementia Strategy. These will also link to our priority areas. Executive Committee: No risks to report. Discussions were held at the 2nd March meeting around changing the Pregabalin from Lyrica to Alzain which would make savings of around £1million. Executive committee also recommended that the Sore Throat Test and Treat (STTT) Service is tested out in pharmacies. Quality & Patient Safety Committee: This Committee is monitoring A&E performance, Care Home Performance and s117 /CHC performance. A recent ‘Never Event’ was highlighted in the press and raised at Governing Body. Primary Care Commissioning Committee: No risks to report. Clinical Reference Group: There are no risks arising from this Group. A Dermatology Update discussion will be held at the meeting on 23rd March alongside further discussions relating to procedures of limited clinical value. Strategy and Organisational Development Forum A potential increase in Ambulance Discharge and A&E Attendance was highlighted.
9 Administration Arrangements 9.1 Review of Audit Committee Forward Planner The Committee reviewed and noted the Audit Committee forward planner and requested that Q1 performance report is added to the July 2017 schedule and also the SBS Audit report be added to the May Audit Committee. The committee also requested that the ‘Ad Hoc’ item column is removed. 9.2 Minutes of the Corporate Governance Management Group Meeting held on 15 February 2017. The Committee noted the minutes
Miss Moore
Miss Moore
10 Any Other Business There were no items raised.
11 Date and Time of Next Meeting Thursday 11 May 2017 at 9:00am – 12noon in Meeting Room 3, Sovereign House, Heavens Walk, Doncaster, DN4 5HZ
Page 1 of 12
Minutes of the Quality & Patient Safety Committee Held on Thursday 2nd March 2017 at 9.30am
Boardroom, White Rose House
Formal Committee Members Present:
Committee Members Present Dr Emyr Jones (Chair) Secondary Care Doctor Member Mr Andrew Russell Chief Nurse Mrs Suzannah Cookson Deputy Chief Nurse, Designated Nurse
Safeguarding Children & LAC Mr Ian Boldy Designated Nurse Safeguarding Adults,
DCCG Dr Jeremy Bradley GP Representative, DCCG Mrs Wendy Feirn Senior Nurse, Quality & Patient Safety Mrs Chris Quinn Patient Experience Manager Mr Mark Randerson Head of Medicines Management Mrs Jenny Rayner Senior Officer for Quality Mrs Zara Head Primary Care Quality Nurse Mrs Andrea Stothard Quality & Patient Safety Manager
Mrs Leah Denman Named Nurse for Safeguarding Adults. Dr Lindsay Britten GP Representative, DCCG Mrs Katie Fenn Children’s Team Leader, DCCG
Formal Committee Members in Attendance:
None
In attendance: Mrs Lesley Twigg Minutes
Action
1. Welcome and Apologies Dr Jones welcomed everyone to the meeting. Apologies for absence were received from:
• Mrs Andrea lbbeson, Named Nurse for Children's Safeguarding
2. Declarations of Interest
The Chair reminded committee members of their obligation to declare any interest they may have on any issues arising at committee meetings which might conflict with the business of NHS Doncaster Clinical Commissioning Group (CCG). Declarations declared by members of the committee are listed in the CCG’s
Page 2 of 12
Register of Interests. The Register is available either via the secretary to the Governing Body or the CCG website at the following link: www.doncasterccg.nhs.uk The meeting was noted as quorate. Declarations of interest from today’s meeting: No Declarations were received.
3. Minutes and Actions of the Previous Meeting – Enclosure A & B The minutes of the meeting held on 19th January 2017 were approved as a true record with the following amendments:
• Replace Named with Designated on Mrs Cookson’s job title
• Page 3, first paragraph, line: Replace ‘being done’ with ‘underway’
• Page 6. Paragraph 3, last line: Replace “Mr Boldy adding that Brian Jacobson are auditing CHC in May 2017” with “Mr Boldy adding that CHC will be audited in May 2017 with the re-audit being based on the original Browne Jacobson audit”.
• Page 8, Agenda Item 5.9, line 1: Replace ‘last week’ with ‘at the Primary Care event’.
• Page 9, Agenda Item 6.2, line 1: Replace ‘ has gone live’ with ‘Children’s Trust has gone live’.
4. Matters Arising not on the Agenda The Committee went through the action log for the meeting. All updates will be recorded on the action log. There were no other matters arising raised by Committee members.
5. QUALITY
5.1 DBHfT Quality Report – Verbal
Mr Russell updated the committee that the ACQRG planned for 14th February 2017 had been cancelled as Mrs Cookson was on annual leave, the meeting was cancelled by mutual consent with the Trust as there were no immediate quality concerns to discuss or escalate.
Mr Russell informed the committee that there had not been any quality concerns raised at the last Strategic Contract meeting but that Q3 CQUIN evidence is still outstanding and the Q4 projected outcomes. There have been some issues with ED performance but that this has recently improved with ED achieving 95% for a couple of days; Mrs Cookson added that ED waiting times
Page 3 of 12
during winter had been a national concern with most acute Trusts not achieving the 95%.
Dr Jones asked the committee if they had any further questions for Mr Russell, nothing further asked.
5.2 FCMS Quality Update – Enclosure C
Mr Russell updated that the FCMS Quality meeting had been held last week and that this is a very positive meeting with attendees from FCMS being open and transparent; Mr Russell added that the core focus of the meeting was to go through their Quality report in detail and challenging where necessary. Dr Britten added that she had attended the meeting last week for the first time and that it had been useful to start discussing more integrated ways of working e.g. inviting an FCMS representative to attend EoL meetings.
Dr Jones asked about the data relating to Serious Incidents (SI’s) in the report; Mr Russell responded that previously FCMS had used a paper based system but are now recording all SI’s on Datix and are training all staff at present on using the system; Dr Jones asked that Mr Russell keep an eye on this as the numbers are very low.
Mr Russell highlighted to the committee that FCMS are doing a lot of good work on audits and have recently moved to using a system for audits called Clinical Guardian and that across the organisation they have only identified two cases that were classed as unsafe.
Dr Jones asked about the Frequent Fliers data on the report and Mr Russell responded that a meeting is being organised to discuss these patients and to try and identify if the patients are a frequent flier when accessing other health care e.g. GP’s.
Dr Jones queried the work being done by FCMS on Summary Care Records with Mr Russell explaining to the committee that this is a technical issue and that FCMS are hopeful that this will be resolved quickly and that if not resolved this will be picked up as part of the contract and finance discussions with the provider. Dr Jones asked that Mr Russell contact the provider to get assurance that the technical issue has been fixed and to report back at the next committee meeting.
Mr Russell asked the committee if they wanted to see the full quality report provided by FCMS at this meeting or would they rather have a paper which details the highs and lows from the report; following discussion the committee agreed that they would prefer to receive a report which contained the key elements from the quality report.
Dr Jones asked the committee if they had any further questions for Mr Russell,
Page 4 of 12
nothing further asked.
Action 11/2017: Mr Russell to find out if the technical issues regarding Summary Care Records has been resolved.
AR
5.3 RDaSH Quality Report – Enclosure D
Mr Russell updated that Q3 CQUINs have been achieved; this has not gone to the RDaSH CQRG as yet. Mrs Stothard added that she had received the Q4 Forecast and this looks like it will be achieved. Mr Russell said that he and Mrs Cookson were meeting with Mrs Wildgoose next week and would be discussing the Trust’s Quality Impact Assessment and the Transformation Plan changes as we do not fully understand how this pulls into the Quality Framework; Mr Russell added that he would provide an update on this issue at the next meeting in May 2017.
Dr Jones asked the committee if they had any further questions for Mrs Cookson, nothing further asked.
Action 12/2017: Mr Russell to update Q & PSC following his discussion with Mrs Wildgoose regarding the Trust’s Quality Impact Assessment and the Transformation changes and how this feeds into the Quality Framework.
AR
5.4 Care Home Report – Enclosure E
Mrs Denman gave a brief update on the Care Home Report.
CAP Pathway: Mrs Denman updated that there is a procurement process underway in relation to the CAP beds that are commissioned from Care Homes. Dr Jones asked if there were resource implications and Mr Russell responded that a Paper had been submitted through SMT and that the Executive committee would be asked to approve the resources required. Mr Russell added that an effective Discharge to Assess process is a mandate from NHS England.
Quality Monitoring: Mrs Denman updated that feedback in relation to the quality monitoring process has been very positive; Dr Jones asked if this would be evaluated. Mr Boldy said that data streams were being looked at and the impact on other services e.g. DRI, GP’s etc.
Quality Monitoring of Out of Area Placements: Mrs Denman updated that as part of this work we also consider CQC reports and check if we have any patients placed in that facility and take appropriate action if we do.
The Committee discussed the Care Home Quality report and a number of specific care homes including those that had been inspected by CQC and those identified through quality monitoring processes where improvements
Page 5 of 12
were required.
The committee was informed of the actions that were being undertaken.
The Committee was informed of one out of area care home where CQC had significant concerns in relation to quality and were minded to take immediate action. The home moved to close requiring all residents to be moved to alternative accommodation. As of the 3rd March all residents will have been moved into another facility including 5 Doncaster residents.
Mrs Denman updated that Dr Tupper will take over as chair of the Care Home Implementation Board with Mr Boldy adding that Mrs Tooley will take up post in the CCG in a few weeks to drive this work forward. Dr Jones asked if this work had lost momentum and Mr Boldy said that it had and it was now time to refocus which is why Dr Tupper and Mrs Tooley would take this forward for the CCG.
Dr Jones said that the positive impact on use of healthcare resources was reassuring and asked the committee if they had any further questions for Mrs Denman or Mr Boldy, nothing further asked.
5.5 Individual Placements Report – Enclosure F
Mr Boldy updated that this is the first formal report and he had reviewed the work of the CHC teams and identified that there was a severe imbalance of workload and responsibilities. Highlights from the report are detailed below:
Fast Tracks: Review has highlighted a lack of process and that the 12 week assessment has not been timely. The Adult Team Leaders have also worked through and updated all policies and procedures; these will now be shared with DMBC.
FNC Reviews: There is a lot of work to be done to bring this back on line. There is a clear understanding of the reviews required and a plan is in place to move towards all reviews being done in a timely fashion.
Current Challenge: There are 443 outstanding reviews and we have identified what staff should be doing and will allocate a number of reviews to each staff. Dr Britten asked if this would increase and Mr Boldy confirmed that it would with staff being expected to complete 10 assessments each month but that this needs to be managed well. Mr Russell added that a lot of work has been done to review all processes and to make these more efficient. Dr Jones said that there had been poor leadership and management in the past in this area. Mr Boldy added that the relationship with the Local Authority has also been a challenge and this has resulted in staff working under pressure. Dr Jones said that this has been a really good piece of work and was reassured that plans were now in place to address issues identified.
Page 6 of 12
Quarter 3 Data and Report: Dr Jones queried the increase from joint funded cases to fully funded cases; Mr Boldy said that this was partly down to the inexperience of staff involved but these cases are now being reviewed and that we were an outlier for joint funded cases but we now understand the scale of the problem.
Children’s CHC: Dr Jones asked if there were any issues; Mr Boldy responded that this is a new team and there are not as many children’s cases but that the team would learn lessons from the work done on adult’s CHC.
Mr Russell informed the committee that we had come a long way in 3 years and that there have been challenges in the team moving back to the CCG from CSU and that significant improvement in governance had been made and that last year’s review by Browne Jacobson had said that there had been significant progress. Mr Boldy added that Woodfield 24 packages are prioritised and reviewed and there have not been any outstanding since Christmas.
Dr Jones asked regarding the format of this report to come to future Q & PSC and asked that it not include a lot of graphs or tables. Mr Russell said that the work that Mrs Quinn does will also feed into future reports and that this will be included in the Quality Work Plan and this will come to this meeting and exceptions will be highlighted; Dr Jones agreed that this approach sounds right.
Dr Jones asked the committee if they had any further questions for Mr Boldy or Mr Russell, nothing further asked. Dr Jones asked that the minutes reflect that this work is a priority and that it is supported across the CCG and that Governing Body are mindful of all the work being undertaken.
5.6 Section 117 Exception Reporting & Work Plan – Enclosure G
Mr Russell updated that the plan will go to the Individual Placement Steering group this month for sign off and that any exceptions will be reported to this committee and concerns raised to the Audit Committee.
Dr Jones said that there were a lot of actions that were amber on the plan but is reassured that they all have actions to address the issue and asked that this committee were kept in touch with progress.
Mr Russell asked about the format for future reports; following discussion the committee agreed that Mr Russell would condense into one side of A4 for future reports.
Dr Jones asked the committee if they had any further questions for Mr Russell, nothing further asked.
Action 013/2017: Mr Russell to provide future Section 117 reports in a
Page 7 of 12
condensed one side of A4.
5.7 Medicines Management Report – Enclosure H
Mr Randerson introduced this report and highlighted the following:
Specialist Infant Formulae Guidance: Work has been done to develop guidance for general practice, in collaboration with other local paediatric dieticians. The guidance will be launched formally at the GP TARGET session planned for May 2017.
CAMHs Audit: Significant deficiencies identified in the management of depression, Mr Golze the Children’s Commissioner has been involved and an action plan is being developed. Dr Jones asked about the deficiencies and Mr Randerson responded that the Trust have an extensive audit programme, this issue was identified during an audit but it now needs to be addressed in a timely manner. Dr Jones asked that the minutes reflect the concerns that the Quality & Patient Safety Committee have regarding this issue and asked that this was also discussed at the next RDaSH CQRG meeting.
Diabetic Network: Mr Randerson said that this was a good news story regarding the switch policy and plan for strips and needles.
Prescribing for Protected Groups – LD: Mr Randerson described that as an LD Call to Action to not overprescribe to this client group. As soon as patients are identified as LD there a review will be undertaken. Mr Randerson added that other areas and Trusts have also struggled in this area in the past.
Action 014/2017: Mrs Cookson to raise the CAMHs issue at the next RDaSH CQRG.
Dr Jones asked the committee if they had any further questions for Mr Randerson or Dr Bradley, nothing further asked.
SC
5.8 Q3 PUPoC Benchmarking Report – Enclosure I
Mr Russell informed the committee that the paper showed where we sit and that there were no surprises and that eligibility is interesting as we are quite low and that other areas have a higher conversion rate for PUPoC. Dr Britten asked when the appeals would be cleared and whether the funding was protected; Mr Russell responded that the appeals can take a very long time and that the funding is protected and that there is no financial risk to the CCG. Dr Britten asked what would happen to any potential underspend; Mr Russell replied that this would a decision made by NHS England. Dr Jones said that the paper was reassuring adding that this is discussed regularly at the Strategy and Governing Body meetings.
Dr Jones asked the committee if they had any further questions for Mr Russell,
Page 8 of 12
nothing further asked.
5.9 Primary Care Quality Report – Enclosure J
Mrs Head introduced the report and highlighted the following to the committee:
Mrs Head has now visited a total of 34 GP Practices and has made an additional 7 appointments. There are now only 3 practices where she has not visited or has an appointment in place to visit.
The visits are identifying quality issues and Mrs Head is working with those practices to address and implement improvements. Mrs Cookson added that the practices are seeing this as a positive and appreciate the support.
Mrs Head updated that practices are now seeing how simple the Primary Care Matrix is to use with Dr Britten adding that the Scott Practice use the system and it has had a positive impact, Mrs Head said that overcoming barriers was the hardest part.
Mrs Head said that work was on-going regarding nurse training to bring this to the same level as the TARGET training that the GP’s receive.
Dr Jones asked that the Primary Care Matrix is brought to the next committee meeting for a demonstration. Mrs Head said she would be happy to do this.
Mr Russell enquired regarding the reporting for child protection case conference given this was a statutory requirement, Mrs Cookson responded that work is ongoing with the DCST to ensure robust processes are in place to notify practices. The intention was that this would be raised again with practices at the March Safeguarding TARGET. Dr Jones queried the Female Genital Mutilation update as some practices are yet to register in accordance with the national requirement. Mrs Head updated that Dr Kelly is speaking to and working with those GP Practices. Mr Russell said that if this needs to be escalated it should be escalated to this committee and also the Primary Care Strategy Group.
Dr Jones asked the committee if they had any further questions for Mrs Head, nothing further asked.
Action 015/17: Mrs Twigg to add the Primary Care Matrix to the agenda for the May 2017 meeting for Mrs Head to demonstrate it to the committee.
LT / ZH
5.10 Q3 RDaSH CQUIN Attainment (To Note) – Enclosure K
Mrs Stothard asked that the committee note that the Q3 attainment had not yet gone to the RDaSH CQRG and that this will go to the April 2017 meeting.
Dr Jones asked that the minutes reflect our appreciation for the hard work that
Page 9 of 12
the Trust have done with CQUINs; Mrs Stothard said that the Trust had invested to put in place a CQUIN team and that they are very dedicated.
6. PATIENT SAFETY
6.1 IPC Update – Enclosure L
Mrs Feirn introduced the report and highlighted the following:
MRSA: If there are no cases in March 2017 this will be a full 3 years where there has not been a case in Doncaster.
CDI: Mrs Feirn updated that there had been a slight spike in the date for August 2016 but of the 3 cases there were 2 patients who then went on to have a faecal transplant. Dr Jones commented that the data is very positive with Mr Russell and Dr Jones both asked that the minutes reflect how far below the trajectory the data is.
React to Red: Mrs Feirn updated that there is a Care Home event at the end of March 2017. The analysis from this project will be out late summer 2017; Dr Jones asked if the project had been positively received; Mrs Feirn said that it had and both Trusts have done a lot of good work but that her concern is after the project ends that the work needs to be maintained, adding that Sheffield CCG are including this in the contracts with their providers and that this may be something that Doncaster CCG may wish to consider.
Mr Russell said that in the past this had been discussed and the decision made not to pay a Quality Premium specifically as the view was that agreed quality standards should be inherent in the contract rather than an additional stretch. Mr Russell added that Bassetlaw had done the original pilot for React to Red but they only have 12 care homes so it was much easier to do, adding that once the evaluation data is received we should consider what mechanism we use to maintain the standard and quality and using the Care Home Implementation Board may well be an option.
Dr Jones asked the committee if they had any further questions for Mrs Feirn, nothing further asked.
6.2 Safeguarding Adults and Children’s Update – Verbal
Safeguarding Adults
Mr Boldy updated that there had been an Adult’s Safeguarding Time Out to identify key priorities. There is a board meeting next week and there are two reviews outstanding, there is nothing further to update the committee on at present.
Page 10 of 12
Safeguarding Children
Mrs Cookson updated that the Children’s Safeguarding Board time out had been held in January 2017 to develop the 2017-18 business objectives. Mrs Cookson also highlighted that the Children’s Safeguarding Board had been highlighted nationally in the media as a good safeguarding board. Mr Russell asked if an inspection would include the Children’s Board; Mrs Cookson said it would and the inspection is undertaken by Ofsted.
Mrs Cookson informed the committee that the GP TARGET for March 2017 will have sessions on Signs of Safety and Looked after Children (LAC) Voice of the Child.
The CCG/Designated Nurse has been requested to hold health strategy meetings for 2 possible Fabricated and Factious Illness (FII) cases, these will be investigated and managed as appropriate.
Dr Jones asked if there was anything to update the committee on regarding Child Sexual Exploitation (CSE); Mrs Cookson said that the Trust has a tight grip on this area and are working with taxi companies, hotels etc and have a work plan that they are working through. Mr Russell added that the Trust work well with the local authority; Mrs Cookson said that the service is now commissioned by Public Health.
Dr Jones asked the committee if they had any further questions for Mrs Cookson or Mr Boldy, nothing further asked.
6.3 Caldicott Log – Verbal
Mr Russell updated that one enquiry had been received but was not added to the log as it was asking for advice.
Dr Jones asked the committee if they had any further questions for Mr Russell, nothing further asked.
6.4 CQC Update – Verbal
Mr Russell updated that there was nothing new regarding CQC Inspections to update the committee.
Dr Jones asked the committee if they had any further questions for Mr Russell, nothing further asked.
6.5 Quality & Safety 2017-18 Work Plan - Verbal
Mr Russell updated that the Quality Team time out is planned for 5th April 2017
Page 11 of 12
and this will be used to develop the plan.
Dr Jones asked the committee if they had any further questions for Mr Russell, nothing further asked.
7. Any Other Business
Terms of Reference
Dr Jones asked the group for their thoughts regarding the Terms of Reference; following discussion it was agreed to make the following amendments:
• The Membership and Attendance sections would be merged into Attendance as they are the same thing.
• Mrs Feirn to be added to the Attendance list.
• A deputy chair is to be identified.
• Section 5 Quorum: Amend that one of the quorum members must be a GP.
• Quality of Primary Medical Services: Mrs Cookson and Mrs Head to look at this section and provide an update to Mrs Twigg.
• Section 7.3 is to be removed as a separate section within the ToR and that both paragraphs should be added to section 7.1 as bullets.
Following much discussion regarding research Dr Jones suggested asking 360 Assurance if this should fall into this Committee’s remit; once we have a response it will either be removed or a separate mechanism put in place to ensure governance of research. Action 016/2017: Mr Russell to speak with Assurance 360 about research in ToR. Action 017/2017: Mrs Cookson and Mrs Head to look at section7.2 and provide an update to Mrs Twigg. Action 018/2017: Mrs Twigg to update the ToR as detailed in the minutes and send out with the minutes and actions of the meeting. Action 019/2017: A deputy chair is to be identified – Mr Russell
AR
SC / ZH
LT
AR
8. Minutes and Information
• Medicines Management Group – Enc N
• Incident Management Group – Enc O & P
• Area Prescribing Committee – Enc Q
• Safeguarding Assurance Group – Enc R
Page 12 of 12
9. Date and Time of Next Meeting Thursday 4th May 2017 at 09.30 - 11.30 in the Boardroom, Sovereign House
FUTURE MEETING DATES
DATE TIME VENUE
Thursday 6th July 2017 0930 - 1130 Boardroom, Sovereign House
Thursday 7th September 2017 0930 - 1130 Boardroom, Sovereign House
Thursday 2nd November 2017 0930 - 1130 Boardroom, Sovereign House
1
Paper A
Joint Committee of Clinical Commissioning Groups
Meeting held 21 March 2017, 9:30 – 11:30 am, at Sheffield CCG
Decision Summary for CCG Boards
1 Decision making business case – children’s surgery and anaestheia
13/17 (a) that the presentation developed for the Sustainability and Transformation Plan Collaborative Partnership board (STP CPB) would be shared with the Joint Committee of Clinical Commissioning Groups (JCCC)
HELEN STEVENS
(b) that full public consultation report would be shared also when finalised
HELEN STEVENS
(c) that full assurance would be given to JCCC that each of the seven acute units met the national standards to enable the full decision on 24 May and any issues would be brought to the attention of the JCCC
WILL CLEARY-GRAY
2 Matters Arising from the previous meeting
15/17 (a) discussions were still ongoing with NHS Hardwick Clinical Commissioning Group (CCG) to support collective decision making approach and the Chair would write to the NHS Hardwick CCG Chief Officer
TIM MOORHEAD
2
Minutes of the meeting of Joint Committee of the Clinical Commissioning Group, held 21 March 2017, 9:30 – 11:30, Sheffield CCG
Present:
Dr Tim Moorhead, Clinical Chair, NHS Sheffield CCG (Chair) Dr Andrew Perkins, Clinical Chair, NHS Bassetlaw CCG (Chair)
Will Cleary-Gray, Director of Sustainability and Transformation, South Yorkshire and Bassetlaw
Sustainability and Transformation Partnership
Chris Edwards, Accountable Officer, NHS Rotherham CCG
Idris Griffiths, Interim Accountable Officer, NHS Bassetlaw CCG
Debbie Hilditch, Healthwatch Representative
Pat Keane, Interim Chief Operating Officer, NHS Wakefield CCG
Alison Knowles, Locality Director – North, NHS England Dr Ben Milton, Clinical Chair, NHS North Derbyshire CCG
Julia Newton, Director of Finance, NHS Sheffield CCG Jackie Pederson, Accountable Officer, NHS Doncaster CCG Matt Powls, Interim Director of Commissioning and Performance, NHS Sheffield CCG (Deputy for Maddy Ruff, Accountable Officer)
Lesley Smith, Accountable Officer, NHS Barnsley CCG
Apologies: Steve Allinson, Accountable Officer, NHS North Derbyshire CCG
John Boyington, Lay Member
Sir Andrew Cash, Chief Executive, Sheffield Teaching Hospitals NHS Foundation Trust/South
Yorkshire and Bassetlaw Sustainability and Transformation Partnership Lead
Dr David Crichton, Clinical Chair, NHS Doncaster CCG
Dr Phillip Earnshaw, Clinical Chair, NHS Wakefield CCG
Andy Gregory, Accountable Officer, NHS Hardwick CCG
Steve Hardy, Lay Member Dr Julie Kitlowski, Clinical Chair, NHS Rotherham CCG Dr Steve Lloyd, Clinical Chair, NHS Hardwick CCG
Maddy Ruff, Accountable Officer, NHS Sheffield CCG
Jo Webster, Accountable Officer, NHS Wakefield CCG In attendance:
Kate Woods, Programme Office Manager, Commissioners Working Together
Rachel Gillott, Deputy Director of Transformation, South Yorkshire and Bassetlaw Sustainability and
Transformation Partnership
Helen Stevens, Associate Director of Communications and Engagement, Commissioners Working
Together
Diane Jordan, Senior Finance Manager, Commissioners Working Together
Dr Peter Anderton, Clinical Lead for Stroke, Commissioners Working Together
James Scott, Project Lead Childrens, Working Together Partnership Vanguard Linda Daniel, Project manager – Childrens, Commissioners Working Together
3
Minute reference
Item
ACTION
12/17 Welcome, introduction and apologies The meeting was opened with an outline of the approach for the session, which would be to work through the next eight weeks to the point of decision on the proposed service changes for Children’s Surgery and Anaesthesia and Hyper Acute Stroke Services on 24 May 2017. The JCCC would address:
- The current clinical case for change - The engagement and consultation section of the business case - The financial elements of the business cases
The outstanding issues and next steps would be considered by JCCC and the proposals to work through these over the coming weeks. The JCCC was asked to note that the financial detail was still being developed and the level of risk needed to be noted by the group to be able to make a decision on the proposed configuration of the service.
13/17 Decision making business case update – Children’s Surgery and Anaesthesia The JCCC was presented with an update, covering the work to date, the clinical case for change, the proposed reconfiguration, options on this proposal, the public and stakeholder feedback, impact on pathways of care, the financial funding impact and an assessment of next steps. A query was raised around the standards from 2013/14/15 and assurance around whether there remained a clinical case for change. It was confirmed that a peer review would take place using a designation toolkit. The focus of the work would be on out of hours evenings and weekends and there was variation across the patch within the case for change, and standardisation and consistency must be reached across the patch. It was confirmed that there remained a clinical case for change for this work. The interdependencies on maternity, neonates and acutely ill child and the point at which these interdependencies needed to be addressed. The JCCC noted that the position had progressed for this work, with changes in provider practice, resulting in smaller numbers of children impacted. This helped to understand the impact on pathways. The outcome of the consultation exercise was reflected on. It was agreed that the presentation developed for the STP CPB would be shared with the JCCC. The full report would be shared also when finalised. This would be presented to the Joint Overview and Scrutiny Committee on 3 April 2017. The methodology behind the consultation was outlined to JCCC. It was noted that where the public and stakeholders agreed to the proposed changes, the views of the case for change were around better care, equal access, better use of allocation of resources, and that people trust the NHS to make decision on their behalf. Where there was
HELEN STEVENS HELEN STEVENS
4
disagreement with the proposed changes, concerns were expressed around not being able to access care close to home, concerns around a possible adverse impact on safety, and skepticism about the motivation for the work. Alternative suggestions were requested from the public and the responses to this were to keep services as is. The themes outlined above remained the same throughout public meetings and discussion groups also. The JCCC were updated on the numbers being impacted by this work noting they were lower than initial projections. A query was raised as to why the Barnsley figure was higher than for other areas. JS confirmed that this was due to clinical coding and the inclusion of undifferentiated abdominal pain diagnosis. In response to a query raised, it was confirmed that detail behind the lower figures being looked at than initially projected, was also being shared with provider organisations. The numbers had changed due to change in the commissioning specification. This is due to i) revised assumptions suggesting that only out-of-hours non-elective work would be affected, rather than all non-day case works, and ii) clinical discussions leading to clarity on diagnoses which would require urgent surgery and those which could be managed locally. A discussion took place around the governance processes for this work, and it was confirmed that the consultation documentation had stated that based on review of current numbers, the figure of patients affected was small, and therefore the fundamental principles of the consultation had not changed and the process was robust. The JCCC discussed assurance around the proposal being based on all providers meeting and maintaining national standards given the trends in workforce development. It was confirmed that this was a standards driven approach. It was confirmed that an initial baseline/peer review had been carried out, and a formal annual review would take place against standards. This would be undertaken by the managed clinical network (MCN). One of the roles of the MCN was to ensure decision points in the pathways of care were correct. It was noted that the proposed change was the result of work with clinicians in local hospitals as well as consultation with public should be made explicit. How clinicians supported the clinical case for change would be crucial. JCCC were presented with a summary and next steps:
• Ongoing development of decision-making business case – Financial model – Commissioning approach and contract award – system
wide • Quality Reviews - peer review visits via MCN, for baseline
assessment against service specification, May - summer • Further refinement of clinical pathways, leading to standardised
protocol via MCN, May • Move to implementation phase (if decision proceeds) – further
engagement of COOs and Trust operational teams. To be finalised in line with mobilisation schedule.
5
• Formal review via MCN, built into implementation schedule A discussion took place around the principles for undertaking this work, given the low numbers involved and the wider issues around quality standards and staffing and how the wider services would be addressed. It was agreed that this work was being undertaken on the clinical consensus being development through the network that changes were required. As this was being worked through, it was clear that a significant change in terms of the impact of people was not at the scale originally envisaged. The current journey had highlighted major concerns around out of hours services and this is why this was being addressed. This should be made explicit as part of the narrative of this work. A further comment on the interdependencies with paediatrics aligning with acute medical pediatrics was made, noting as possible impact on surgery as the Acutely Ill Child progressed. It was confirmed that the analysis of the consultation would be fully fed back to all stakeholders and to the public. JCCC requested full assurance that each of the seven acute units met the national standards to enable the full decision on 24 May.
WILL CLEARY-GRAY
14/17 Decision making business case update – Hyper Acute Stroke Services JCCC were presented with an overview of the work on Hyper Acute Stroke Services to date, noting that this work predated the work of the Sustainability and Transformation Plan. The presentation covered the clinical case for change, options, considered, the proposed reconfiguration, public and stakeholder feedback, the financial and funding implications and a summary of next steps. The JCCC were updated on the consultation elements, noting that where respondents agreed with the proposals the key themes were being able to access better quality of care with improved outcomes and a more effective allocation of resources. Where the public and stakeholders disagreed with the proposals, key themes were around not being able to access care closer to home, the social impact of the need for further travel, (this did not show through on the children’s survey, and a comment was made that this suggested a misunderstanding about the way that the changes were presented to the public), and concerns around the pressure on the ambulance service. The ambulance concerns had also been a theme from the Joint Overview and Scrutiny Committee who had requested reassurance on ambulance services. The mixed responses from the public were noted. Financial initial summary was presented to the JCCC. It was noted that a finance working group was formed in September 2016, led by DJ with representation from each provider organsiation and supported by deputy CFOs as part of this process. This group had addressed activity data, stroke best practice tariffs, implications of a service change for providers, transportation funding, and looked at potentials around introducing local funding model versus national tariff. A summary of the issues were presented to the JCCC. Figures were indicative and based
6
on business cases. A discussion took place around national staffing standards to improve quality indicators and concerns were noted around money assumptions to recruit staff. DJ confirmed that this was aspirational. It was noted that the tariff implications from the provider business cases would be helpful. It was confirmed that no assumptions were made on mortality implications at this point. Length of Stay would not affect the tariff. The impact of excess bed days and social care would not be factored into this business case at the present time. The work around excess bed days was crucial and work on HASU should not be seen in isolation. Next steps were outlined to the JCCC:
• Share very early draft Decision Business Case (DBC) with commissioners
• Transport cost and modelling finalised • Revisit provider financial issues/risks • Agree financial principles • Commissioning Approach agreed • Finalise DBC • Joint Committee Decision
A comment was made that the whole pathway needed to be addressed to secure flow through the system to optimise any changes to HASU. Capacity to deal with the changes should be addressed. It was noted that positive engagement with providers was taking place, looking at the implications of centralising HASU and looking at the interface with other parts of system. It was noted that a stroke clinical network to support mobilisation of work around standardisation and consistency of services would be established. In response to a query it was confirmed that a decision would be taken in May based on all of the information presented to them, including the clinical case for change as well as the views of the public. A discussion took place around telemedicine and it was confirmed that this technology was being utilised currently for out of hours and this had been in place since 2012. The JCCC noted that there remained a strong clinical case for change, noting further work needed to be done on financials and affordability noting that long term, the affordability for this work must be sustainable. The financial business case to move to the next stage of the process needed reconsidering with different approach. It was noted that having the draft business cases to consider prior to the meeting would have helped discussions and this was acknowledged.
15/17 The minutes of previous meeting The minutes of the meeting held 21 February were accepted as a true and accurate record subject to a change to the discussion on the Joint Committee.
16/17 Matters arising
7
NHS Hardwick CCG JCCC were updated on the position of NHS Hardwick Clinical Commissioning Group (CCG) with regards to formal delegation to the JCCC for decisions on stroke and Children’s Surgery and Anaethesia. An early discussion had taken place with NHS Hardwick CCG which was helpful in providing clarification and also NHS England. The JCCC supported a recommendation for the Chair to write to NHS Hardwick CCG to summarise shared understanding to agree a supportive collective decision making approach for the current proposals. Lay membership HS advised the group that discussions with interested parties had taken place around the role. AP, MR and HS would be undertaking the interviews for the position.
TIM MOORHEAD
17/17 Any other business The JCCC were asked to note that all organisations must engage and consider how to work differently, as transformation funding would not necessarily be available for future pieces of work. Careful consideration was required to ensure that a culture and context of working where any small system change was made would be supported by transformation funding. This formed part of a wider discussions on commissioners and providers working as a system.

Verbal
Item 13
Any Other Business

Verbal
Item 14
Date & Time of Next Meeting
Thursday 15 June 2017 at 1pm in the Boardroom, Sovereign House, Heavens
Walk, Doncaster, DN4 5HZ
