grad ind protocol and pharmacology study guide
TRANSCRIPT
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 1 of 41
Student Name: Teagan Rogers Employee No:_60258042
GRAD IND Protocol and Pharmacology Study Guide
2021
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 2 of 41
Dear Graduate P1 Trainee,
This Study Guide is to assist you in your learning of NSW Ambulance Protocols and Pharmacology. Completion is a mandatory part of your training and will be collected at the end of week four (4) of your Induction Course.
To save paper, this document is to be completed electronically and emailed to your Course Coordinator for electronic filing.
The majority of the answers are located within the NSW Ambulance Protocols and Pharmacology book or on the APP. If you have not downloaded the APP yet, it is highly recommend that you do so, as it will give you the latest updates.
Some of the questions will ask you to perform some research to provide an answer. This research does not need referencing and the answer does not need to be exceedingly
detailed, only enough to show your understanding. Completion of this Study Guide will also assist you to study for your Protocol and Pharmacology Quiz.
The quiz will consist of 20 multiple choice questions to be completed in thirty (30) minutes. Students may use their Protocols and Pharmacology Booklets if required to
complete the exam. The pass mark is 100%. Scores greater than or equal to 85% will require written resubmission of incorrect answers. Scores less than 85% will incur a supplementary assessment.
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 3 of 41
AMBULANCE PARAMEDIC PROTOCOL AND PHARMACOLOGY QUESTIONS WORK BOOK
NB: These scenarios ask questions covering multiple protocols in the Ambulance Foundation, Reference and Pharmacology section of your protocols. Your partner
is a P1 paramedic Scenario 1
You and your partner are dispatched on a lights and sirens case to the local football field for a 38 year old male complaining of shortness of breath.
On arrival, you see a middle-aged male sitting on a lawn mower holding his chest in obvious distress. The patient is in the middle of the field.
1. On reaching the patient, they have irregular breathing, and are able to talk in full
sentences. What must be determined and gained by you and your partner before
commencing any treatment or transport? Define each of these three concepts.
Before any treatment can begin, the paramedics must need to assess the patient
or person responsible for the patient has the capacity and competency to give
consent to treatment. If they do have these three concepts, the paramedics can
begin treatment. Consent is fluid however and can be revoked or reassessed at
any time and should be reassessed before transport.
Consent must be given by someone who has capacity, given freely, sufficiently
specific to the procedure or treatment proposed and must be informed. There is
expressed and implied consent and the person responsible for the patient can
also give consent.
Capacity is based on the patient being able to understand the facts involved,
weigh up the consequences and communicate their decision. Competency refers to the patient’s status under the law to able to make the decision
about their healthcare and well-being. Competency is demonstrated in patients without
chronic
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 4 of 41
compromise of cognitive function.
2. The patient gives you their consent to assess and treat them. Your partner instructs
you to assess the patient. What are the two assessments that you need to initially
perform. How do these assist you in your initial treatment of the patient?
The first is the primary survey – consisting of danger, response, airway, breathing,
circulation and the patient disability. This should be repeated after the first
intervention as it is the best indication of patients response to treatment.
Secondary survey is the next step of this and includes a full head to toe and
focused assessments dependent on how the patient presents.
On doing your initial survey you find:
Airway Currently patent, though is complaining of airway swelling
Breathing Irregular due to anxiety, able to
talk in full sentences, wheezing audible
Circulation Pulses: Present, rapid, thready Skin: Pale, cool, clammy
Disability Level of Consciousness is Alert
Exposure Hives on chest and throat, there is a welt on the left shoulder.
Initial Observations Blood Pressure – 90/40 Respiratory Rate – 22/per minute Heart Rate – 124 Pupils – Equal and reactive
Oxygen Saturations on room air – 92%,
3. Your partner and you decide that the patient needs oxygen. Explain why oxygen
is required for this patient according to the Oxygen Pharmacology 221.
Oxygen is indicated as the patient has a Sp02 of less than 92% on room air.
Given this patients hypoxic presentation, the targeted outcome is maintain Sp02
of >94-98%.
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 5 of 41
4. Both paramedics decide due to the patient’s signs and symptoms to administer the
medication Adrenaline. Explain the process that you and your partner must do
when selecting and confirming to administer a medication.
1. Confirm diagnosis and establish the need to administer medication
2. Check for any contraindications to administration
3. Select medication to be administered and confirm with partner
- The correct medication is selected (look alike/sound alike
medications) - The medication is within expiry date - The medication does not appear to be damaged or unusable
4. Draw up or prepare medication to be administered. Medications must not be mixed or administered together unless authorized by protocol or pharmacology
5. Confirm the “5 Rights” of medication administration with your partner
- Right patient
- Right medication - Right dose - Right route - Right time
6. Administer medication and repeat doses. Continue to monitor patient and
above process for each new medication
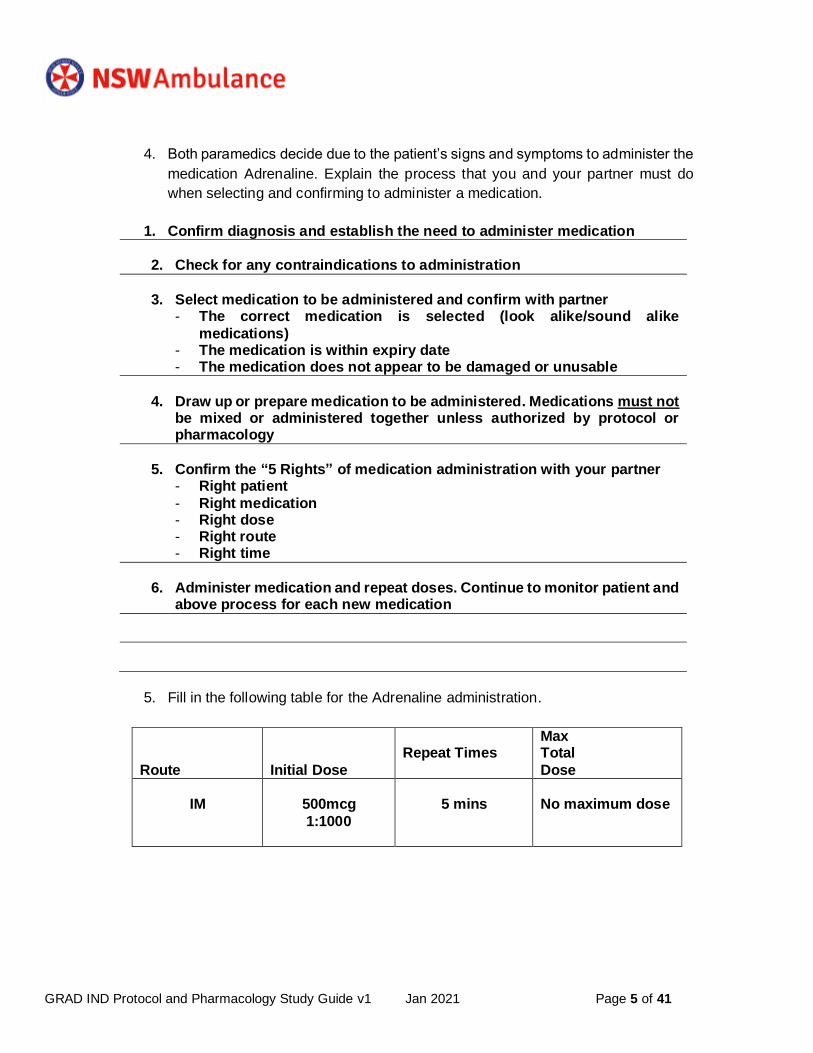
5. Fill in the following table for the Adrenaline administration.
Route Initial Dose
Repeat Times
Max Total
Dose
IM
500mcg
1:1000
5 mins
No maximum dose
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 6 of 41
6. What could be any possible adverse effects that your patient could experience post
your administration of Adrenaline?
Adverse effects can include tachycardia, dysrhythmias (ventricular
fibrillation), hypertension, pupillary dilation, anxiety, and nausea with or
without vomiting.
7. The patient’s condition is slow to respond to your treatment regime. You decide
that the patient needs urgent transport. Why do you and your partner make this
decision and under what category would you put this decision? (A8)
The patient is experiencing a distribution and relative hypovolemic shock with due
profound reduction in venous tone and fluid extravasation causing
reduced venous return cause decreased myocardial function.
8. Your transport time to hospital is 20 minutes with lights and sirens. How often are
you required to take the patient’s observations? What system dictates this?
(Reference 28)
According to R28 (Adult observation range guides), the patient meets the Red Zone
Criteria with a systolic blood pressure of 90. This requires repeat observations
every 5 minutes.
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 7 of 41
Scenario 2
You are called to a 10-year-old riding an ATV was thrown off at about 30kmh, when they
hit a log in tall grass. The patient’s caregivers are present on scene and are very
concerned about their child’s well-being.
Airway Protecting airway, crying, breathing spontaneously
Breathing Clear lungs bilaterally, oxygen saturations 98% on room air
Circulation Capillary refill intact, colour slightly pale skin, heart sounds normal, peripheral pulses palpable
Disability Awake, alert, anxious and crying, moving all extremities, pupils normal
Exposure Deformity and laceration to R mid forearm noted.
Initial Observations Blood Pressure – 100/70 Respiratory Rate – 16/per minute Heart Rate – 128
Pupils – Equal and reactive Oxygen Saturations on room air – 98%,
1. You and your partner have assessed the scene and are with the patient and
caregivers. Whose consent do you need to start assessing and treating this patient?
What determines this decision? (A3)
As per A3 (informed consent, capacity, and competency), there is no set age for
when a minor can independently consent or refuse treatment. Given the
nature of this specific case, the child is anxious and crying. While consent can
be sought by the patient, the caregivers are on scene and will be able to give
consent of behalf of the child/patient.
2. What are two key points that could help you recognize that this 10-year child is sicker
than they could possibly appear? (A5) By having a structured assessment and repeated observations it will assist
in detecting subtle signs or cues or illness. As noted in A5, parental anxiety
should not be discounted even if the child does not seem unwell.
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 8 of 41
3. The caregivers agree with you and your partner’s decision to try to ease the patient’s
pain. As the patient is 10-years old what is the preferred route of administration of
medications for this child’s complaint? (A6)
As per A6 (Pain Management), consideration should be given to the route for
children <14 years or under (as this patient is) with inhalational/intranasal
administration as the preferred route.
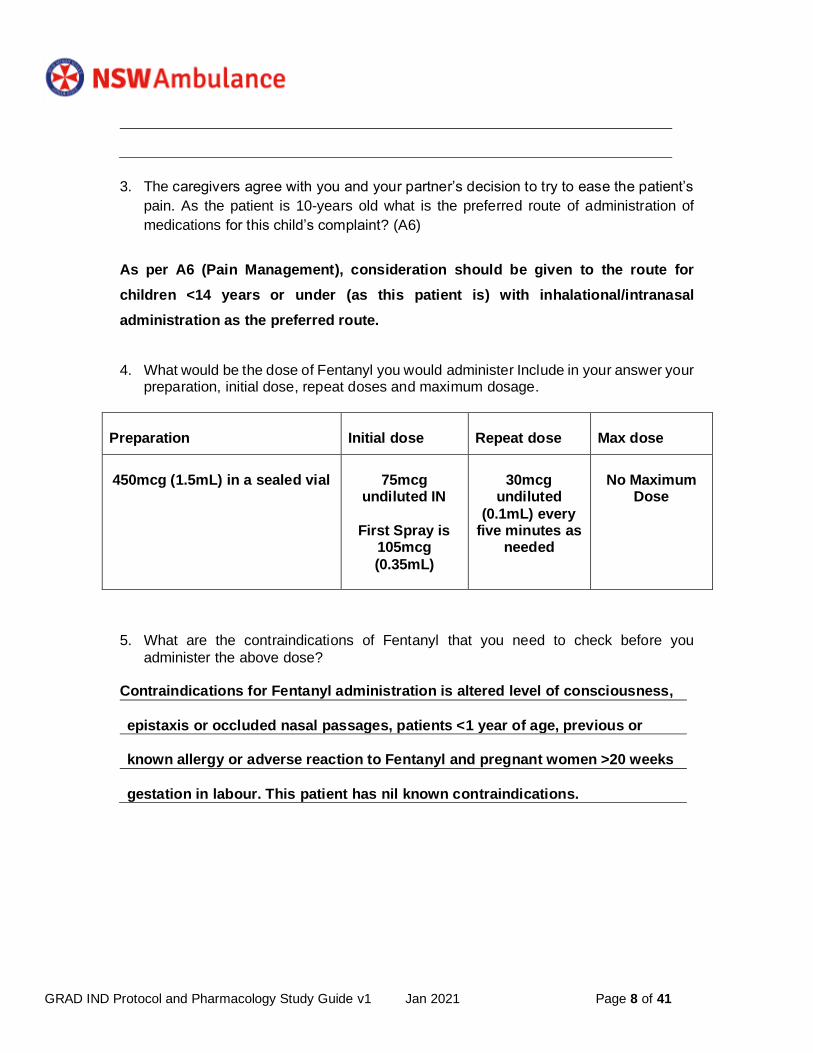
4. What would be the dose of Fentanyl you would administer Include in your answer your preparation, initial dose, repeat doses and maximum dosage.
Preparation
Initial dose
Repeat dose
Max dose
450mcg (1.5mL) in a sealed vial
75mcg
undiluted IN
First Spray is
105mcg
(0.35mL)
30mcg
undiluted
(0.1mL) every five minutes as
needed
No Maximum
Dose
5. What are the contraindications of Fentanyl that you need to check before you
administer the above dose? Contraindications for Fentanyl administration is altered level of consciousness,
epistaxis or occluded nasal passages, patients <1 year of age, previous or
known allergy or adverse reaction to Fentanyl and pregnant women >20 weeks
gestation in labour. This patient has nil known contraindications.
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 9 of 41
Medical Protocol Questions
These scenarios ask questions covering the Medical/Surgical Protocols and Pharmacology sections of your protocols. Your partner is a P1 Paramedic.
Scenario 1
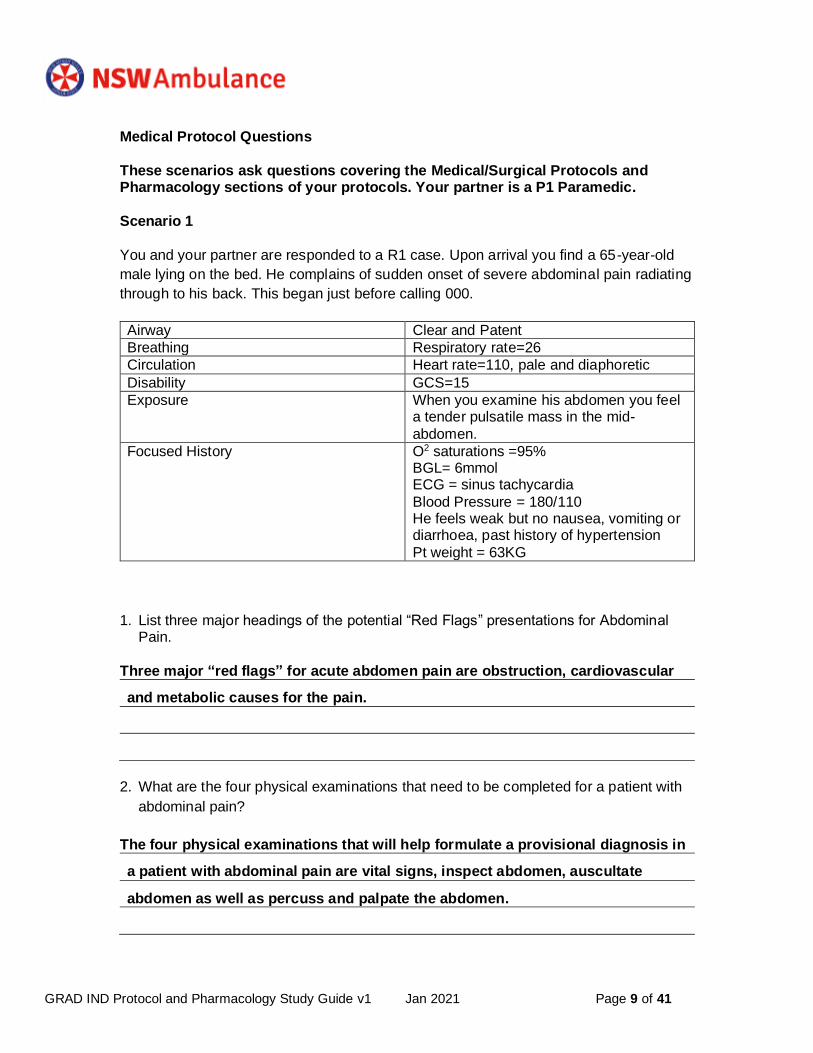
You and your partner are responded to a R1 case. Upon arrival you find a 65-year-old
male lying on the bed. He complains of sudden onset of severe abdominal pain radiating
through to his back. This began just before calling 000.
Airway Clear and Patent
Breathing Respiratory rate=26
Circulation Heart rate=110, pale and diaphoretic
Disability GCS=15
Exposure When you examine his abdomen you feel a tender pulsatile mass in the mid-
abdomen.
Focused History O2 saturations =95% BGL= 6mmol ECG = sinus tachycardia
Blood Pressure = 180/110 He feels weak but no nausea, vomiting or diarrhoea, past history of hypertension
Pt weight = 63KG
1. List three major headings of the potential “Red Flags” presentations for Abdominal
Pain.
Three major “red flags” for acute abdomen pain are obstruction, cardiovascular
and metabolic causes for the pain.
2. What are the four physical examinations that need to be completed for a patient with
abdominal pain?
The four physical examinations that will help formulate a provisional diagnosis in
a patient with abdominal pain are vital signs, inspect abdomen, auscultate
abdomen as well as percuss and palpate the abdomen.
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 10 of 41
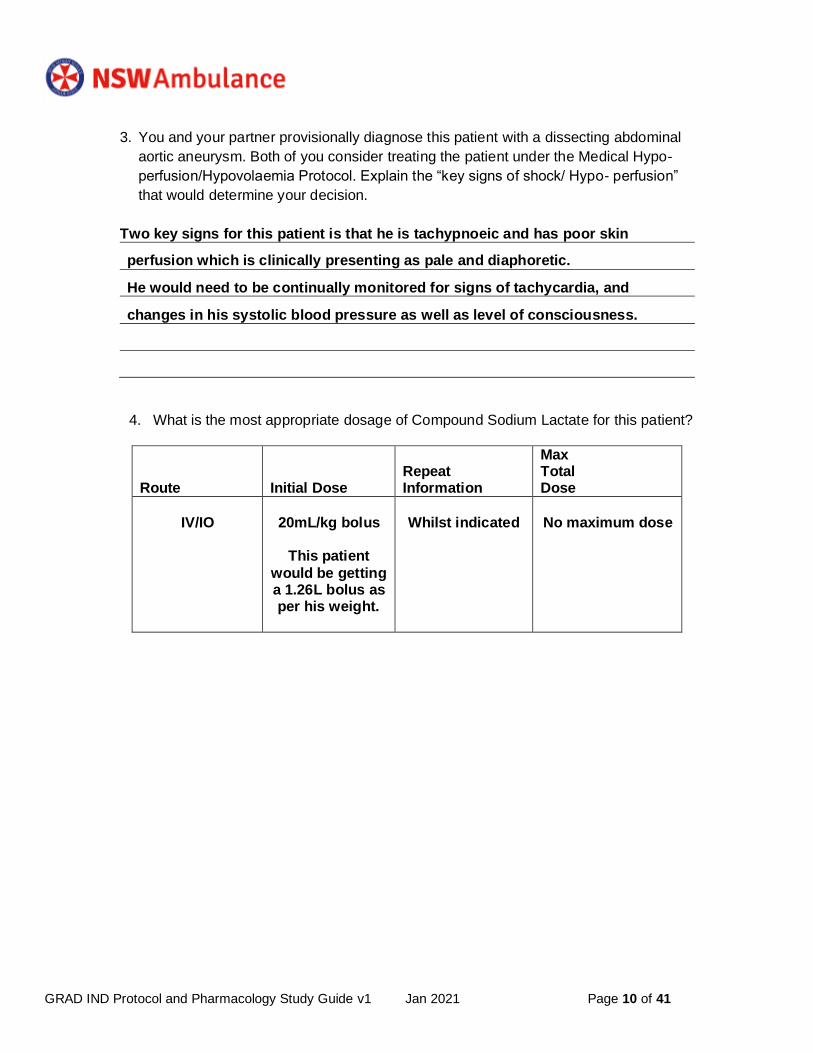
3. You and your partner provisionally diagnose this patient with a dissecting abdominal
aortic aneurysm. Both of you consider treating the patient under the Medical Hypo-
perfusion/Hypovolaemia Protocol. Explain the “key signs of shock/ Hypo- perfusion”
that would determine your decision.
Two key signs for this patient is that he is tachypnoeic and has poor skin
perfusion which is clinically presenting as pale and diaphoretic.
He would need to be continually monitored for signs of tachycardia, and
changes in his systolic blood pressure as well as level of consciousness.
4. What is the most appropriate dosage of Compound Sodium Lactate for this patient?
Route Initial Dose
Repeat Information
Max Total Dose
IV/IO
20mL/kg bolus
This patient
would be getting a 1.26L bolus as per his weight.
Whilst indicated
No maximum dose
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 11 of 41
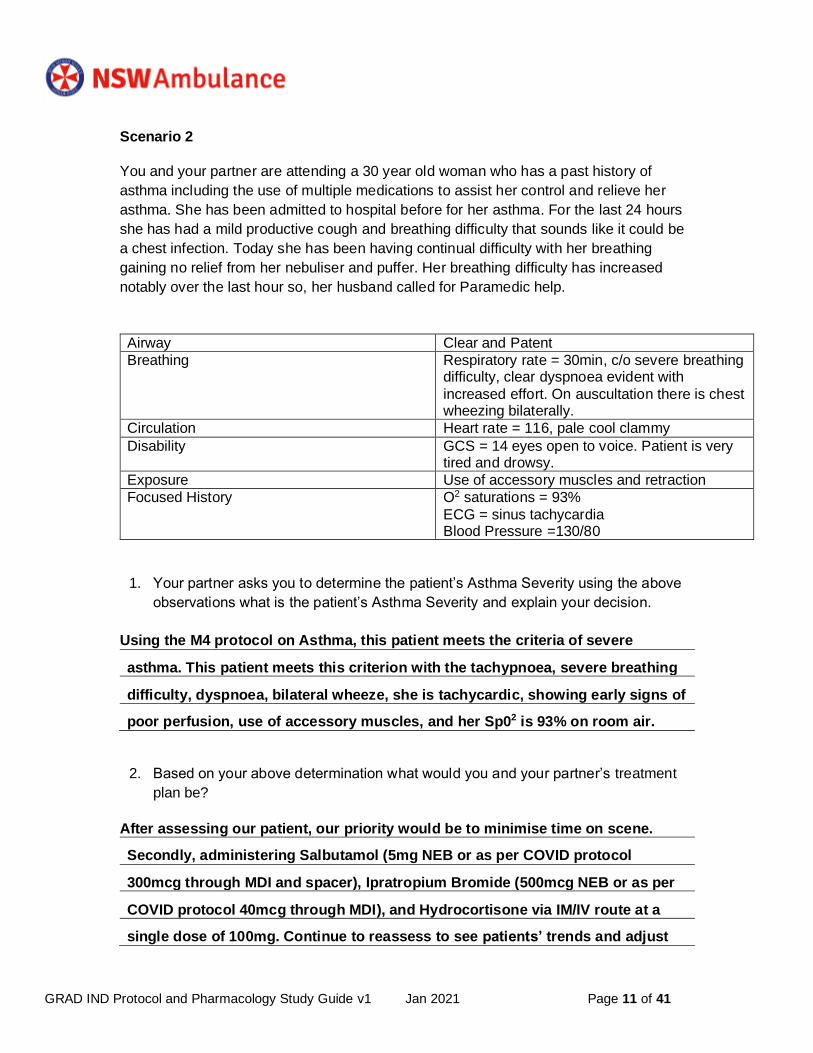
Scenario 2
You and your partner are attending a 30 year old woman who has a past history of
asthma including the use of multiple medications to assist her control and relieve her
asthma. She has been admitted to hospital before for her asthma. For the last 24 hours
she has had a mild productive cough and breathing difficulty that sounds like it could be
a chest infection. Today she has been having continual difficulty with her breathing
gaining no relief from her nebuliser and puffer. Her breathing difficulty has increased
notably over the last hour so, her husband called for Paramedic help.
Airway Clear and Patent
Breathing Respiratory rate = 30min, c/o severe breathing difficulty, clear dyspnoea evident with
increased effort. On auscultation there is chest wheezing bilaterally.
Circulation Heart rate = 116, pale cool clammy
Disability GCS = 14 eyes open to voice. Patient is very tired and drowsy.
Exposure Use of accessory muscles and retraction
Focused History O2 saturations = 93%
ECG = sinus tachycardia Blood Pressure =130/80
1. Your partner asks you to determine the patient’s Asthma Severity using the above
observations what is the patient’s Asthma Severity and explain your decision.
Using the M4 protocol on Asthma, this patient meets the criteria of severe
asthma. This patient meets this criterion with the tachypnoea, severe breathing
difficulty, dyspnoea, bilateral wheeze, she is tachycardic, showing early signs of
poor perfusion, use of accessory muscles, and her Sp02 is 93% on room air.
2. Based on your above determination what would you and your partner’s treatment
plan be?
After assessing our patient, our priority would be to minimise time on scene.
Secondly, administering Salbutamol (5mg NEB or as per COVID protocol
300mcg through MDI and spacer), Ipratropium Bromide (500mcg NEB or as per
COVID protocol 40mcg through MDI), and Hydrocortisone via IM/IV route at a
single dose of 100mg. Continue to reassess to see patients’ trends and adjust
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 12 of 41
accordingly. If she begins to trend negatively or there is no improvement call
control for ICP backup for potential IV adrenaline.
3. Your partner asks you to obtain out of the medication kit the correct Salbutamol and
Ipratropium Bromide dose. What are the correct doses of both medications for this
patient?
Secondly, administering Salbutamol 5mg NEB (or as per COVID protocol 300mcg
through MDI and spacer), and Ipratropium Bromide 500mcg NEB (or as per
COVID protocol 40mcg through MDI).
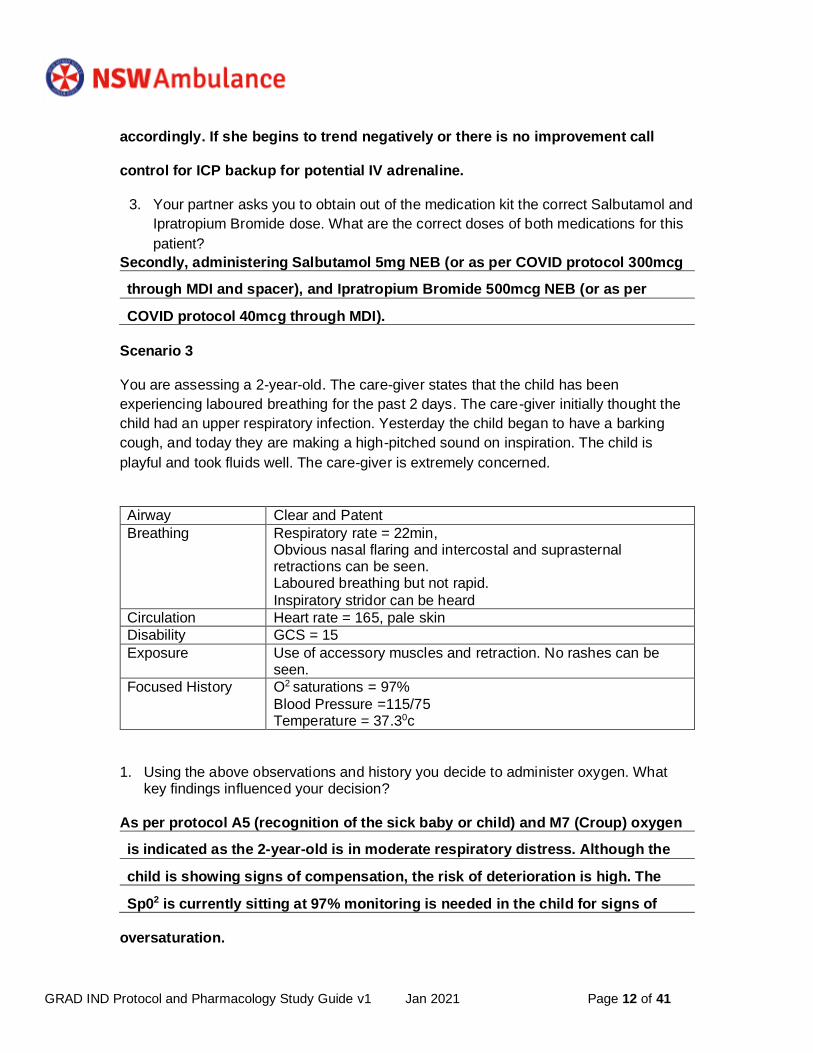
Scenario 3
You are assessing a 2-year-old. The care-giver states that the child has been
experiencing laboured breathing for the past 2 days. The care-giver initially thought the
child had an upper respiratory infection. Yesterday the child began to have a barking
cough, and today they are making a high-pitched sound on inspiration. The child is
playful and took fluids well. The care-giver is extremely concerned.
Airway Clear and Patent
Breathing Respiratory rate = 22min, Obvious nasal flaring and intercostal and suprasternal retractions can be seen. Laboured breathing but not rapid.
Inspiratory stridor can be heard
Circulation Heart rate = 165, pale skin
Disability GCS = 15
Exposure Use of accessory muscles and retraction. No rashes can be seen.
Focused History O2 saturations = 97%
Blood Pressure =115/75 Temperature = 37.30c
1. Using the above observations and history you decide to administer oxygen. What key findings influenced your decision?
As per protocol A5 (recognition of the sick baby or child) and M7 (Croup) oxygen
is indicated as the 2-year-old is in moderate respiratory distress. Although the
child is showing signs of compensation, the risk of deterioration is high. The
Sp02 is currently sitting at 97% monitoring is needed in the child for signs of
oversaturation.
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 13 of 41
2. Does this patient fall within or outside the Paediatric White zone criteria of Between
the Flags? If they do, what are you required to do?
They are outside of the Paediatric White Zone Criteria in the criteria of systolic
blood pressure and pulse rate. She is hypertensive and tachycardic. As per
these guidelines paramedics are required to increase frequency in
observations and consider urgent transport with treatment commencing
en-route.
Scenario 4
You and your partner are responded to a person unwell. Upon arrival you find a young
man who is confused. His family states he is a diabetic and took his insulin today but has
not eaten. They noticed he was confused about 20 minutes ago. They have given him
some candy but it has not helped. He is unable to answer questions due to confusion.
You are 30 minutes from the hospital.
Airway Clear and Patent
Breathing Respiratory rate = 20
Circulation Heart rate= 80
Disability GCS= 13
Exposure Nil
Focused History O2 saturations =98% Blood Pressure=120/80 Temperature=36.30c
1. Discuss the clinical significance of hypoglycaemia in the elderly.
Hypoglycaemia in the elderly has a large and potentially catastrophic outcomes.
Hypoglycaemic elderly patients are more likely to have falls, fractures, injuries
arrhythmias and in severe cases, death. Symptoms may go unrecognised
or can be misdiagnosed as other neurological conditions (i.e TIA or stroke).
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 14 of 41
2. Referring to the Glucose Gel Pharmacology is Glucose Gel able to be administered to this patient? Explain your answer.
No, due to his GCS of 13 he is unable to self-administer glucose gel. It would
be a choking risk to allow him to swallow the gel.
Scenario 5
You have been responded to a 4-year-old female feeling unwell. The mother states that
the child has a history of increasing lethargy, fever, dizziness when she tries to stand up.
There is no history of vomiting or diarrhoea. Her food and fluid intake has decreased
over the last 12 hours. Typical chicken pox lesions developed 5 days ago. Over the last
18 hours or so several lesions on her abdomen have become red, tender and swollen.
On your arrival the patient is postured supine and listless.
Airway Clear and Patent
Breathing Respiratory rate = 60, Rapid
Circulation Heart rate= 165 Peripherally pulse is weak and thready.
Disability GCS= 13
Exposure Extremities are warm and bright red. Skin is mottled
Skin is warm to mid forearms and mid calves.
Focused History O2 saturations = 96% Blood Pressure = 90/30
Temperature = 39.40c
1. List the three areas of focus for a patient you suspect has Sepsis.
1. Recognise the risk factors, signs and symptoms of sepsis
2. Resuscitate with IV fluids and antibiotics if indicated for interventions
3. Transport to ED and identify sepsis risk factors during clinical handover
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 15 of 41
2. What are the Sepsis risk factors for this particular patient?
The risk factors for this child are deterioration despite previous treatment and
high level of parental concern. Given the child has been sick for an extended
period of time they may be considered immunocompromised.
3. According to the Medical Hypoperfusion/Hypovolaemia Protocol what category of
hypovolaemia does Sepsis fall into? Explain this type of hypovolaemia.
According to the M5 protocol sepsis falls into the relative hypovolaemia category.
This is the due to the fact that patients in septic shock have increased size in
the vascular bed due to vasodilation.
4. You and your partner want to ensure that you have made the right diagnosis, so you
look at the Acute Rheumatic Fever Protocol. Explain why it is important to recognise
Acute Rheumatic Fever and report it.
It is important to recognise and report acute rheumatic fever due to the fact it is
caused by the streptococcal bacterium and there may be an increased risk of
the patient developing Rheumatic Heart Disease, resulting in valvular disease or
stroke later in life. In addition, it is a mandatory reportable disease under the
NSW Health policy.
5. Does this patient fit into any of the high risk groups for Acute Rheumatic Fever and
have any signs and symptoms? If so what are these? She fits the high-risk group as she is female.
While this case doesn’t discuss her ethnicity or housing conditions, she may
also fit those groups.
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 16 of 41
Cardiac/Cardiovascular Protocol Questions
NB: These scenarios ask questions covering the Cardiac/Cardiovascular
Protocols and Pharmacology sections of your protocols.
Your partner is a P1 Paramedic.
Scenario 1
You and your partner are dispatched to a 50-year-old male unwell. Upon arrival, you find
the 50-year-old male sitting on the couch. He complains of mid-sternal chest pain that
began 30 minutes ago. He has also developed nausea, sweating, and dyspnoea. He has
a history of angina but has never had a heart attack. He has taken two nitro-glycerine
tabs (which have expired) with no change in the pain. He also states that he has already
taken his aspirin today about three hours before you arrived. He has a history of angina
and hypertension. He is still a smoker.
Airway Clear and Patent
Breathing Respiratory rate=20, slight wheeze like sound heard bilaterally.
Circulation Heart rate=92, pale and diaphoretic
Disability GCS=15
Exposure Nil findings
Focused History O2 saturations = 95%, BGL= 6mmol, ECG= Sinus Rhythm and
Meets ST elevation MI Criteria Blood Pressure =146/90
1. What is your understanding of the term Acute Coronary Syndrome? (A1)
The term ACS encompasses a spectrum of conditions that affect the
cardiovascular system. It spans from angina to acute myocardial infarctions and
is associated with atherosclerosis in the arteries. It can be something that
patients have well managed and live with or it can be something that can lead to
death, dependent on the severity.
2. List the medications that are required to be administered to a patient with chest pain if
they meet the indications for them.
If patients are indicated, they can receive Aspirin, Glycerol Trinitrate, and oxygen
and pain management – preferably morphine.
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 17 of 41
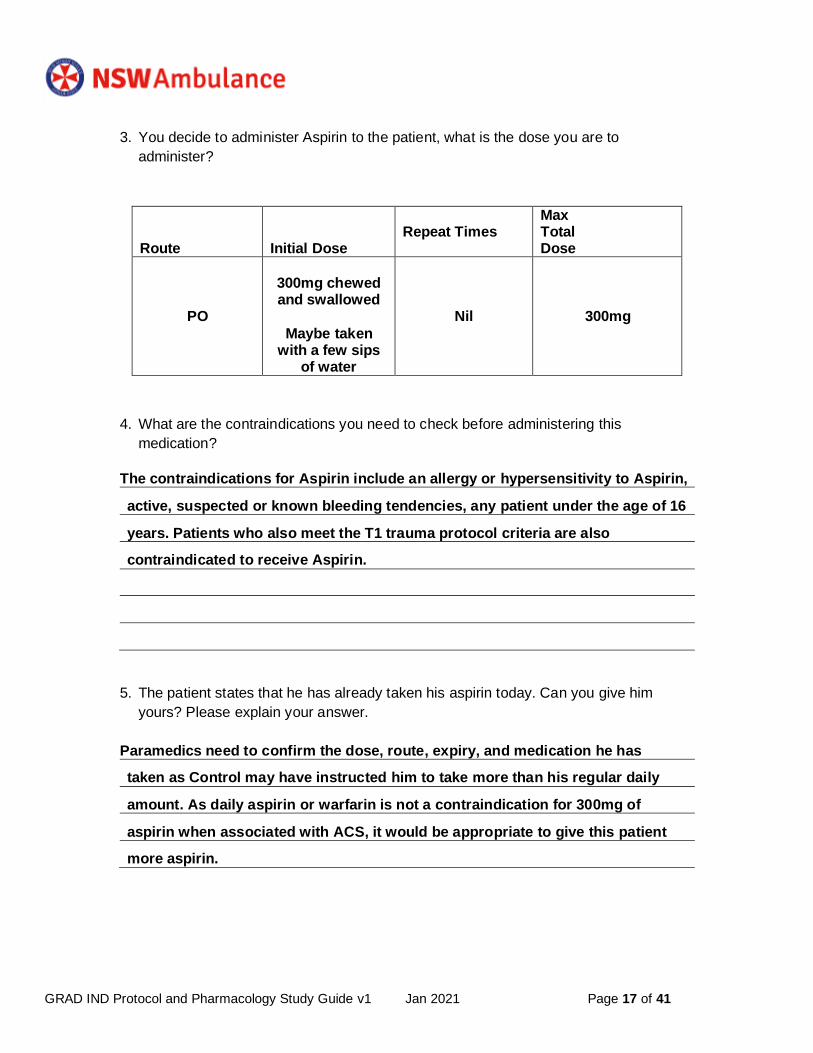
3. You decide to administer Aspirin to the patient, what is the dose you are to
administer?
Route Initial Dose
Repeat Times
Max Total Dose
PO
300mg chewed and swallowed
Maybe taken with a few sips
of water
Nil
300mg
4. What are the contraindications you need to check before administering this
medication?
The contraindications for Aspirin include an allergy or hypersensitivity to Aspirin,
active, suspected or known bleeding tendencies, any patient under the age of 16
years. Patients who also meet the T1 trauma protocol criteria are also
contraindicated to receive Aspirin.
5. The patient states that he has already taken his aspirin today. Can you give him
yours? Please explain your answer.
Paramedics need to confirm the dose, route, expiry, and medication he has
taken as Control may have instructed him to take more than his regular daily
amount. As daily aspirin or warfarin is not a contraindication for 300mg of
aspirin when associated with ACS, it would be appropriate to give this patient
more aspirin.
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 18 of 41
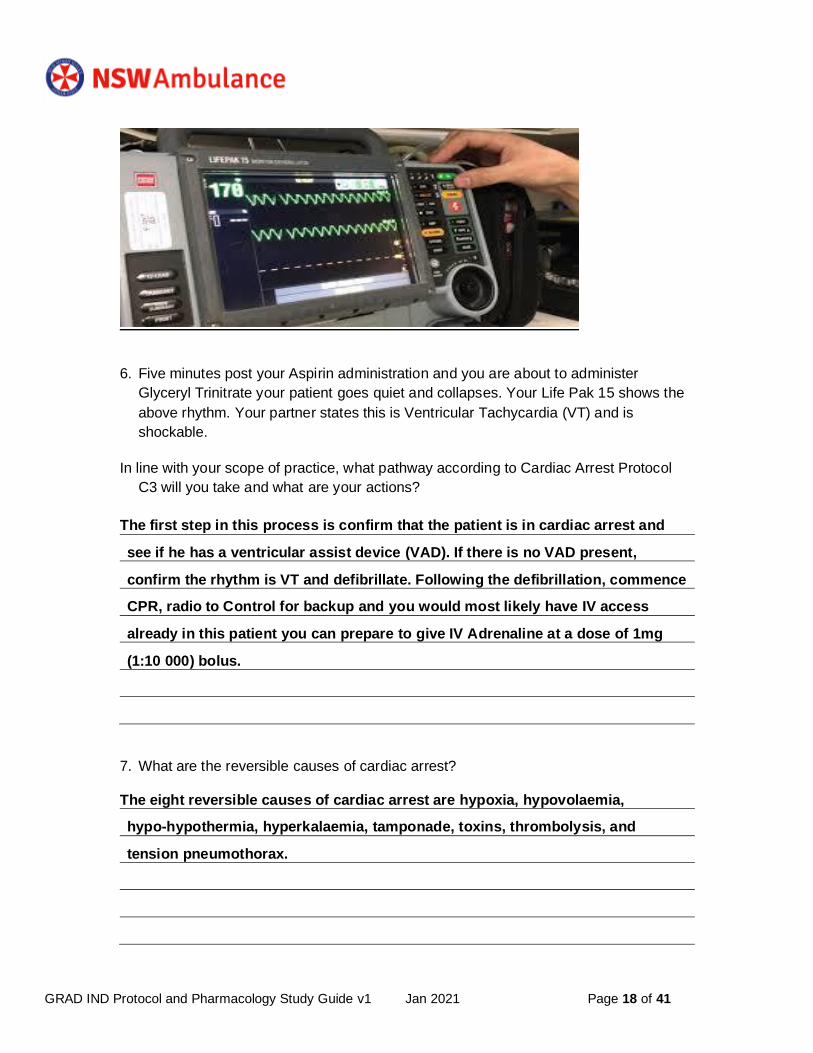
6. Five minutes post your Aspirin administration and you are about to administer
Glyceryl Trinitrate your patient goes quiet and collapses. Your Life Pak 15 shows the
above rhythm. Your partner states this is Ventricular Tachycardia (VT) and is
shockable.
In line with your scope of practice, what pathway according to Cardiac Arrest Protocol
C3 will you take and what are your actions?
The first step in this process is confirm that the patient is in cardiac arrest and
see if he has a ventricular assist device (VAD). If there is no VAD present,
confirm the rhythm is VT and defibrillate. Following the defibrillation, commence
CPR, radio to Control for backup and you would most likely have IV access
already in this patient you can prepare to give IV Adrenaline at a dose of 1mg
(1:10 000) bolus.
7. What are the reversible causes of cardiac arrest?
The eight reversible causes of cardiac arrest are hypoxia, hypovolaemia,
hypo-hypothermia, hyperkalaemia, tamponade, toxins, thrombolysis, and
tension pneumothorax.
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 19 of 41
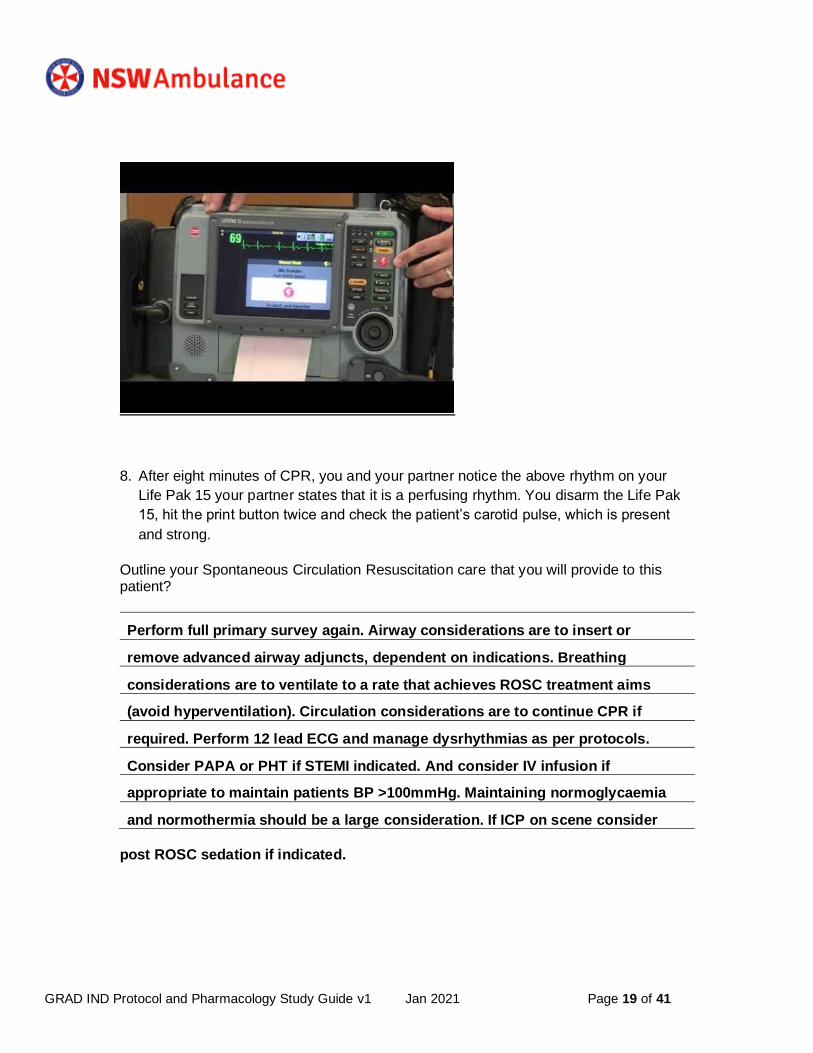
8. After eight minutes of CPR, you and your partner notice the above rhythm on your
Life Pak 15 your partner states that it is a perfusing rhythm. You disarm the Life Pak
15, hit the print button twice and check the patient’s carotid pulse, which is present
and strong.
Outline your Spontaneous Circulation Resuscitation care that you will provide to this patient?
Perform full primary survey again. Airway considerations are to insert or
remove advanced airway adjuncts, dependent on indications. Breathing
considerations are to ventilate to a rate that achieves ROSC treatment aims
(avoid hyperventilation). Circulation considerations are to continue CPR if
required. Perform 12 lead ECG and manage dysrhythmias as per protocols.
Consider PAPA or PHT if STEMI indicated. And consider IV infusion if
appropriate to maintain patients BP >100mmHg. Maintaining normoglycaemia
and normothermia should be a large consideration. If ICP on scene consider
post ROSC sedation if indicated.
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 20 of 41
Scenario 2
You and your partner are dispatched to a 77-year-old female with a suspected Stroke. The husband of a 77-year-old female has called because his wife has slurred speech and left sided weakness. Husband states the symptoms started 30 minutes prior to your
arrival. You are 30 minutes from the hospital.
Airway Clear and Patent
Breathing Respiratory rate=12, Chest is clear
Circulation Heart rate=60, pale and diaphoretic
Disability GCS=15
Exposure Nil findings
Focused History O2 saturations =93%, BGL= 5.3 mmol ECG = Sinus Rhythm.
Blood Pressure= 140/90 The patient is a type II diabetic.
1. What are the signs and symptoms of a stroke and define the F.A.S.T mnemonic? Signs of symptoms of stroke can include sudden onset of numbness or
altered sensations in the limbs, sudden onset of memory loss, confusion,
difficulty speaking or swallowing. In addition, a sudden onset of ataxic gait.
F.A.S.T stands for:
F – facial palsy?, A- any weakness present?, S- is any speech impaired/slurring,
T- confirming time around when the signs/symptoms began. 2. List the Hyper Acute Stroke Mandatory criteria.
The Hyperacute stroke criteria is a positive response to any of the F.A.S.T criteria,
AND estimated arrival to ED is <4.5 hours from onset of signs and symptoms or
last time the patient was seen well AND patient is >18 years of age AND BGL is
>4mmol.

GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 21 of 41
3. You decide that the patient is Hyper Acute Stroke Mandatory Criteria positive, outline your treatment and transport requirements. Treatment and transport plans should include gaining IV access using an 18G
cannular in the ACF, pre-notify receiving hospital via the Control centre of
hyperacute stroke mandatory criteria positive patient. If the patient is
unaccompanied during transport obtain a contact name/number of carer or
relative to the patient.
Transport without delay to ED following the transport destination cascade.
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 22 of 41
Trauma Protocol Questions
NB: These scenarios ask questions covering multiple protocols in the Trauma and
Pharmacology section of your protocols.
Your partner is a P1 Paramedic.
Scenario 1
You and your partner respond to a person fallen > 3meters. Upon arrival, you find a
young man who was putting up a TV antenna and fell off the roof. Family states he has
been unconscious since falling. The family states the patient has no allergies; the patient
fell from the top of the roof approximately 15m. The patient landed onto a concrete
driveway.
Airway Clear and Patent There is no gag reflex
Breathing Respiratory rate=8 Decreased breath sounds on the right side
Circulation Heart rate=65 Pale and diaphoretic
Disability GCS= 6
Eyes – 1 Verbal – 1 Motor – 4
The pupils are medium sized and react sluggishly.
Exposure There is a large hematoma in the occipital area. There is bloody fluid coming from the right ear.
Focused History O2 saturations = 93%,
BGL= 6mmol, ECG=Sinus Rhythm Blood Pressure=170/80
1. Discuss why airway management is extremely important for patient with a head injury
Given the nature of brain injuries, a secondary brain injury can occur due to
hypoxia and hypotension. Airway management that focuses on ventilation and
oxygenation as well as treatment for hypotension is important as neglecting
these factors are associated with poor outcomes.
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 23 of 41
2. What are the clinical prompts that this patient has that assists your diagnosis that the
patient has a head injury?
Clinical prompts that may suggest the patient has a head injury is GCS>14,
visual deformity of the skull or face, cerebrospinal fluid present from ears or
nose, a systolic BP <90mmHg, a history of LOC or trauma of any kind,
ecchymosis around ears or eyes, with or reduced pupil reactions.
3. According the Head Injury protocol how should this patient be postured during
transport to ED and what should be maintained?
Patients should be transported with considerations to their positioning.
If they are being transported via stretcher, they should be positioned with their
head up at a 30-degree angle where possible, spinal precautions must be
maintained.
4. Examining the Spinal Injuries Protocol and the above observations discuss why you
would apply a cervical collar to this patient.
Due to the high mechanism of injury this patient meets the criteria for a cervical
collar.
5. Pelvic fractures should be considered in patients whose mechanism of injury may
have resulted in a large inertia change on impact. List the high risk mechanisms for a
pelvic fracture. Does your patient fit into any of these?
Pelvic fractures should be considered in all patients with a large inertia change
on impact. High mechanism for these injuries include vehicle vs pedestrian,
motorbike crash, side impact vehicle collisions, crush injuries, falls from or
trampling by livestock. This patient fits the high-risk mechanism criteria of a fall
from height.
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 24 of 41
6. If you suspect a patient has a pelvic injury what must you not do?
Paramedics should not spring the pelvis or log roll the patient in any
circumstances. Extrication devices should be utilized to facilitate extrication.
7. Using the Trauma Triage Tool-Major Trauma Criteria (MIST) what Mechanisms,
Injuries, Signs and Symptoms, does your patient have to meet the Major Trauma
Criteria?
This patient meets the MIST criteria in multiple sections. M – fall greater than 3m,
rapid deceleration injury. I – head injury with LOC, potential ecchymosis. S-
reduced RR (8), increased BP (170/80), reduced GCS (6). This patient meets the
MIST criteria.
8. From your previous answer, you determine that your patient meets the Major Trauma
Criteria. What does this authorise you to do?
By meeting the criteria, paramedics are authorized to transport up to 60 mins
(metropolitan) or 90 mins (regional) from scene to reach the appropriate
trauma facility.
9. Your partner asks you to provide a full MIST Report to pass a “CODE 3” to the
Control Center who will then pass it to the receiving hospital. Use the above history and observations.
Male patient of unknown age. Mechanism of injury is a fall of 15m onto concrete
driveway, his injuries are periorbital ecchymosis, and fluid coming from right
ear, and ? tension pneumothorax with decreased breath sounds on the right
side. He is GCS 6, E=1, V=1, M=6. HR is 65 (and strong/weak/thready/etc). Pupils
are medium sized and sluggish. ECG shows sinus rhythm, and he is currently
hypertensive at 170/80. We are enroute and “X” minutes away.
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 25 of 41
10. Enroute to hospital, you reassess the patient’s observation and discover that the
patient has rapidly deteriorated. According to the deteriorating trauma patient protocol,
list the core physiological observations used to identify the deteriorating trauma patient.
The physiological observations used to identify a deteriorating trauma patient
are respiratory rate, LOC, pulse rate, blood pressure (systolic and diastolic),
temperature and oxygen saturation. Being able to identify these negatively
trending observations is important to support positive outcomes for the patients.
11. Under what indication would you administer Compound Sodium Lactate to this patient
and what would your dose be?
Compound sodium lactate would be given to this patient if their systolic
blood pressure dropped <100mmHg as we are treating this patient as if they
they have a head injury.
Route Initial Dose
Repeat Times
Max Total
Dose
IV
250mL bolus
Repeat until BP
>100mmHg
No maximum dose
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 26 of 41
Scenario 2
You are responded to a fire. Upon arrival, you find a 25-year-old male complaining of
severe pain. The patient was burned when he put gasoline on some rubbish he was trying
to burn. He has Dermal and full thickness burns of his face, neck, anterior chest (he was
not wearing a shirt), and both arms. His nasal hairs are burned but he has no burns in his
mouth. He has no history of any medical problems, takes no medications, and has a known
allergy to opiate medications (Anaphylactic reaction). His last meal was 4 hours ago. You
are 30 minutes from the hospital.
Airway Clear and Patent
Breathing Respiratory rate=20
Circulation Heart rate=100
Disability GCS= 15
Exposure Dermal and full thickness burns of his whole face, anterior neck,
anterior chest (he was not wearing a shirt), and both arms to the
elbows.
Focused History O2 saturations = 98%,
BGL= 4.6mmol,
ECG= Sinus Rhythm
Blood Pressure =120/70
1. Using the Rules of 9’s, calculate the Total body Surface Area burnt.
His total body surface area is 22.5%. This is made up of head (4.5%), anterior chest
(9%), and both arms (9% - 4.5% each arm).
2. This case is located in the Sydney Metropolitan Area, where should you transport this
patient. Will you transport lights and sirens or normal speed? Why?
This patient should be transported to either Concord Repatriation General Hospital
or Royal North Shore Hospital as they are both trauma facilities and with
specialized burns units and will be able to appropriately care for this patient.
The transport would be a lights and sirens response and would include a Code 3
through Control.
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 27 of 41
3. Choose one cooling option available for treating this particular patient? Once you have
cooled the burn site your partner asks you to apply clear plastic to the site, how is this
to be done?
The cooling options available for this patient are normal saline or compound
sodium lactate directly to the burned area. Once cooled, apply clear plastic
film longitudinally over the burn as not inhibit swelling of the burned surface
area and surrounding tissues.
4. The patient is complaining of pain, whist you are cooling them your partner states for
you to administer Methoxyflurane. Before you administer the medication, you need to
check for any contraindications. What are the contraindications of Methoxyflurane?
The contraindications for methoxyflurane are malignant hyperthermia, altered or
decreased level of consciousness, pre-eclampsia or eclampsia, untreated renal
failure, patients under the age of 1, acute behaviorally disturbed patients, and
any patient currently on tetracycline use.
5. What is the initial dose and repeat dose of Methoxyflurane?
Route Initial Dose
Repeat Times
Max Total
Dose
INH
3mL delivered by
penthrox inhaler
You may only repeat once as
indicated. As they last
approx. 30 mins,
the second administration would happen
after this.
6mL in 24 hours 15mL in 7 days
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 28 of 41
6. Examining the history and assessment of your patient, refer to the Inhalation Injuries
Protocol. What category of inhalation injury do you consider your patient may have
experienced? Explain your answer.
This patient has a direct thermal injury. Given that it was a fire, the dry air holds
little heat and therefore dissipates quickly. The clinical observations of singed
nasal hair suggests this as he has no burns to his airway or mouth. This patient
is still at risk for oedema and potential upper airway compromise.
7. List the questions you need to consider to determine the potential severity of exposure.
To determine the potential severity of the burns, the paramedics need to determine
the history and mechanism of injury, the type and duration of exposure, the
physical signs and symptoms, and the patients clinical observations.
8. List the signs of smoke inhalation.
The pneumonic to remember this is HISSCA. It stands for:
H - hoarse voice
I-inspiratory stridor
S- see-saw breathing
S-singed facial and/or nasal hair
C- Carbonaceous material around the mouth, nose or in the sputum
A-anterior burns to the neck
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 29 of 41
Other Protocol Questions
NB: These scenarios ask questions covering multiple protocols not previously specified and Pharmacology section of your protocols. Your partner is a P1 Paramedic.
Your ambulance has responded to a football field where a player has collapsed at the end
of a 3-hour practice in 36-degree heat. Upon arrival, you find a 17-year-old male who is
unresponsive. He is very flushed. The coach has had him taken to the shower and has
cool water spraying on him. The trainer is getting bags of ice to place under his arms and
in his groin. The patient responds only to pain. You are 30 minutes from the hospital.
Airway Clear and Patent
Breathing Respiratory rate=24.
Circulation Heart rate=160, pale and diaphoretic
Disability GCS=5
Exposure Nil findings
Focused History O2 saturations =99%,
BGL=6mmol,
ECG=Sinus Tachycardia Rhythm
Blood Pressure=90/60
Temperature= 42.50
1. Discuss the difference between heat stroke and heat exhaustion including some examples
of the various clinical features.
Heat stroke is hyperthermia in the setting of CNS dysfunction. Heat exhaustion
is a milder form of heat illness and the profound CNS dysfunction is absent.
Heat stroke should be suspected in this patients case as it is often associated
with high heat stress through exertion or environmental factors.
This patients clinical features of ALOC, collapse, and core body temp >40°
suggest he is suffering from heat stroke.
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 30 of 41
2. According to the Hyperthermia Protocol what is going to be your treatment regime for
your scope of practice.
The treatment process for this patient is to remove any clothing, place ice packs
to the patients neck, armpits and groin. Continually reassessing for hypothermia
Treat any associated conditions such as dehydration, medical hypoperfusion,
seizures, nausea and vomiting, and hypoglycemia.
Scenario 2
It is winter and you are working at the bottom of the Blue Mountains and you have
responded to a call of a homeless man found passed out in the cold. Upon arrival, you
find a disheveled man who appears to be in his 40s. He is shivering, and states he drank
too much wine during the night and passed out without any cover. There is no history of
trauma.
Airway Clear and Patent
Breathing Respiratory rate=12.
Circulation Heart rate=80
Disability GCS=15
Exposure He is very cold with mottled skin and unable to walk on his own.
Focused History O2 saturations = 94%,
BGL=6mmol,
ECG=Sinus Rhythm
Blood Pressure=110/70
Temperature= 330
1. Reviewing the above patient’s history and observations what will be your treatment
regime.
As his temperature is <35° the patient needs to be removed from the cold
environment into the warm ambulance, remove any wet clothing and dry him,
Warm the patient by wrapping him in a dry blanket followed by a space blanket.
Assess the patient for any cold injuries.

GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 31 of 41
2. What must not be done as part of your treatment regime?
According to E4, do not rub any frozen tissue, use any radiant heat to rewarm the
affected part, do not break any blisters that have formed, rewarm any part of the
body if there is a chance of refreezing. It is also important in this patient’s case
to inspect all limbs and not let or make him walk.
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 32 of 41
Scenario 3
The police have called you. Upon arrival, you find a young man handcuffed, and being
held on the ground by five police officers. He is screaming curses and continues to struggle
in spite of all of the officers holding him down. The police state that they were called
because he was running naked in the traffic. When the police arrived, he became
aggressive and pushed an officer who hit her head and lost consciousness. A paramedic
team is caring for her. The police used their Taser (CEW) in order to subdue him but he
continues to fight in spite of several shocks. He is known to be a methamphetamine (ICE)
addict and has a history of Bipolar Disorder.
Airway Clear and Patent
Breathing Respiratory rate=36.
Circulation Heart rate=180
Diaphoretic
Disability GCS=15.
Dilated pupils and does not seem to focus when he looks at you.
Exposure Patient is covered with bruises and abrasions.
He continues to scream and struggle.
The two Taser darts are still in the skin of his chest.
Focused History O2 saturations =95%,
BGL=4.4mmol,
ECG=Sinus Tachycardia Rhythm
Blood Pressure=190/100
Temperature= 370
1. What do the initials CEW stand for? Explain what this devise does to a person.
A CEW is a form of taser known as a conducted electrical weapon. A CEW is a
battery operated hand-held device which can deliver up to 50 000 volts of
electricity, in rapid pulses, via two barbed electrodes or direct contact. CEW’s
produce pain and a loss of voluntary control of muscles.
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 33 of 41
2. Discuss the treatment regime of a patient sprayed with OC spray. Why is shampoo
and soap no longer required?
A patient who has been sprayed with OC spray should have their face, eyes and
eyelids irrigated with copious amounts of cold water (running where possible).
After irrigation, ice packs may be applied to the area to reduce burning sensation.
Considerations should be applied to prevent hypothermia and removal of the
patients decontaminated clothing.
Shampoo and conditioner is no longer required as NSW police no longer deploy
oil based OC spray, it is water based and can be rinsed with water.
3. Refer to the Delirium Protocol, could the above patient be experiencing delirium.
Explain your answer.
Yes, this patient could be experiencing an excited delirium due to the known
methamphetamine addiction as drugs can be a potential cause of an excited
delirium. Although, given his history of biopolar disorder, he also may be in a
manic phase and may be having an acute psychosis that can sometimes be
misdiagnosed as excited delirium.
4. Your partner states to you that this patient is undergoing a mental health emergency.
How can you establish a rapport with this patient?
To establish a rapport with the patient it is important that the paramedics calmly
identify themselves to the patient, they ask the patients name and main concerns,
it is important to reassure your patients and effectively communicate with
simple words and sentences.
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 34 of 41
5. As the patient was playing in the traffic, you consider that he may have been trying to
end his life. What Acronym can assist you in assessing this and what does it mean?
It would be appropriate to assess the patients risk of suicide with the THREAT
acronym. It stands for:
T- thinking of suicide
H-history of previous suicide attempts
R-reasons and circumstances
E-emotionally depressed
A-access to lethal means
T-tactics and plans
6. You and your partner assess that the patient is mentally unwell and is having suicidal
thoughts. The patient is unwilling to come to hospital with you voluntarily. Discuss what
actions you and your partner are allowed to do, to take this patient to hospital.
It can be determined by the patients actions and behavior that they do not have
the competency and capacity to adequately keep themselves safe. Under this,
this patient has met the criteria to be sectioned, and as a result the paramedics
will enact an S20. To facilitate safe transport for all involved, the patient should
be considered for sedation, restraint, a search and for police escort to hospital.
7. You and your partner decide to administer Droperidol to this patient, fill in the
following table.
Route Initial Dose
Repeat Times
Max Total
Dose
IV/IM
10mg bolus
Once after 15
minutes if
indicated
20mg
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 35 of 41
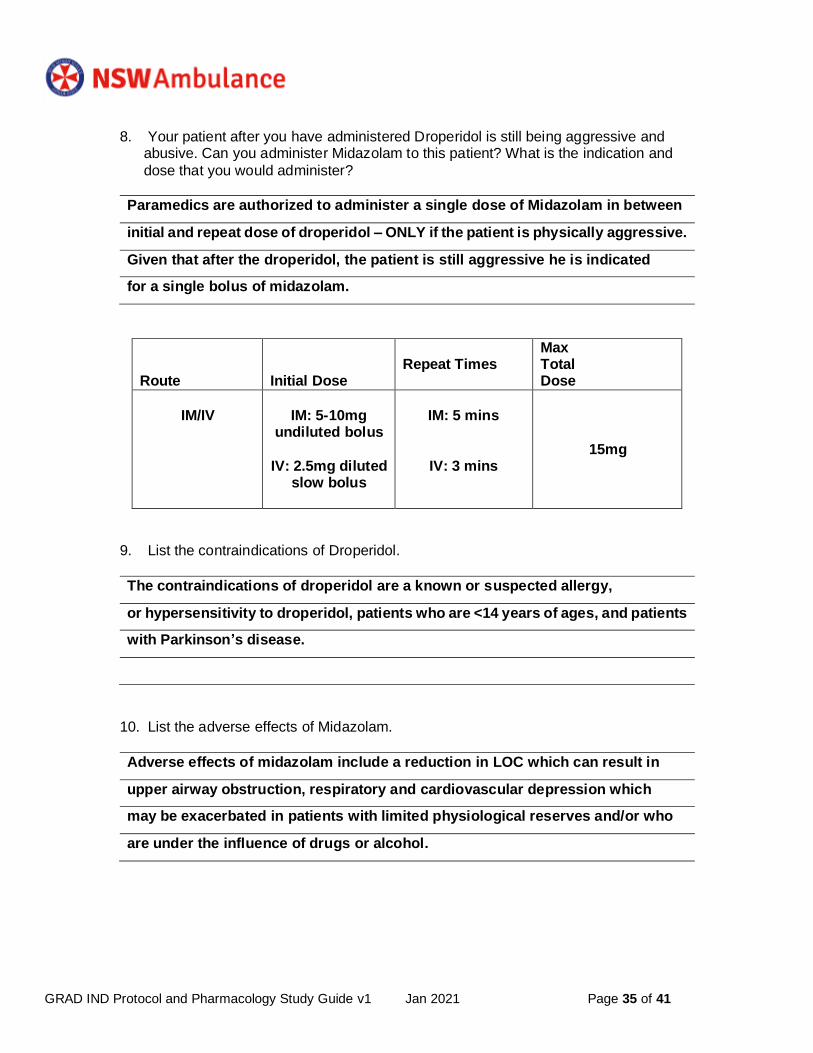
8. Your patient after you have administered Droperidol is still being aggressive and abusive. Can you administer Midazolam to this patient? What is the indication and
dose that you would administer?
Paramedics are authorized to administer a single dose of Midazolam in between
initial and repeat dose of droperidol – ONLY if the patient is physically aggressive.
Given that after the droperidol, the patient is still aggressive he is indicated
for a single bolus of midazolam.
Route Initial Dose
Repeat Times
Max Total Dose
IM/IV
IM: 5-10mg
undiluted bolus
IV: 2.5mg diluted
slow bolus
IM: 5 mins
IV: 3 mins
15mg
9. List the contraindications of Droperidol.
The contraindications of droperidol are a known or suspected allergy,
or hypersensitivity to droperidol, patients who are <14 years of ages, and patients
with Parkinson’s disease.
10. List the adverse effects of Midazolam.
Adverse effects of midazolam include a reduction in LOC which can result in
upper airway obstruction, respiratory and cardiovascular depression which
may be exacerbated in patients with limited physiological reserves and/or who
are under the influence of drugs or alcohol.
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 36 of 41
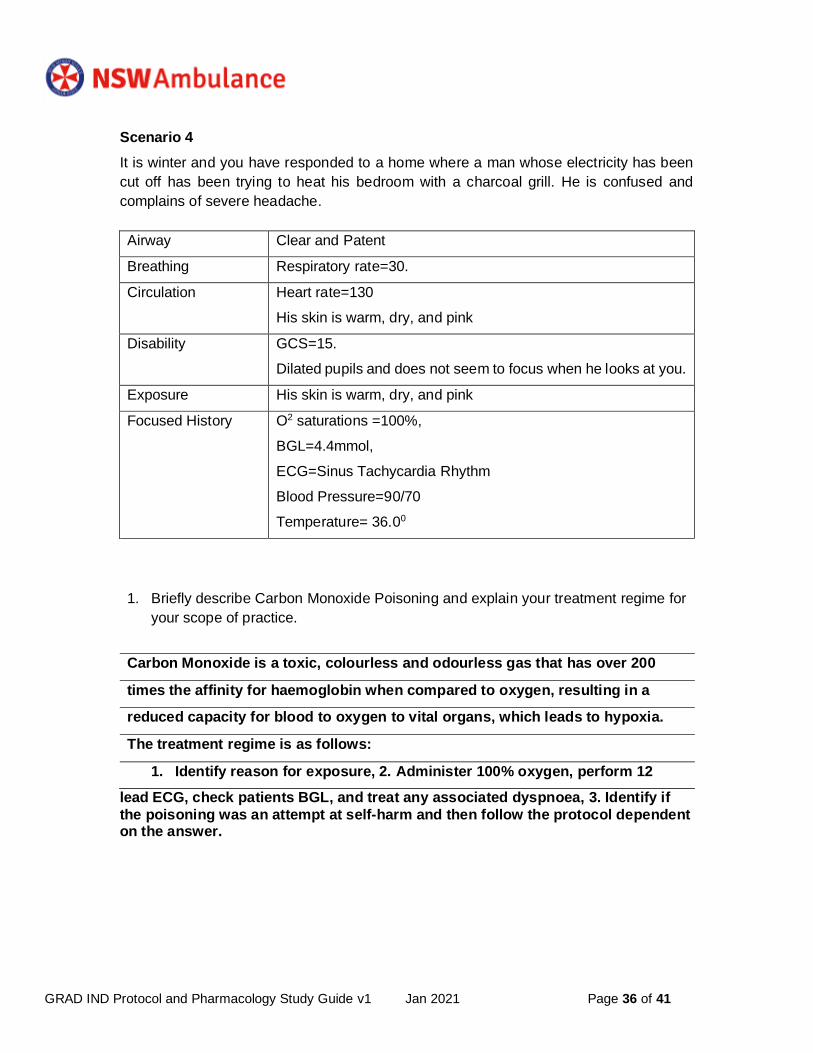
Scenario 4
It is winter and you have responded to a home where a man whose electricity has been
cut off has been trying to heat his bedroom with a charcoal grill. He is confused and
complains of severe headache.
Airway Clear and Patent
Breathing Respiratory rate=30.
Circulation Heart rate=130
His skin is warm, dry, and pink
Disability GCS=15.
Dilated pupils and does not seem to focus when he looks at you.
Exposure His skin is warm, dry, and pink
Focused History O2 saturations =100%,
BGL=4.4mmol,
ECG=Sinus Tachycardia Rhythm
Blood Pressure=90/70
Temperature= 36.00
1. Briefly describe Carbon Monoxide Poisoning and explain your treatment regime for
your scope of practice.
Carbon Monoxide is a toxic, colourless and odourless gas that has over 200
times the affinity for haemoglobin when compared to oxygen, resulting in a
reduced capacity for blood to oxygen to vital organs, which leads to hypoxia.
The treatment regime is as follows:
1. Identify reason for exposure, 2. Administer 100% oxygen, perform 12
lead ECG, check patients BGL, and treat any associated dyspnoea, 3. Identify if
the poisoning was an attempt at self-harm and then follow the protocol dependent on the answer.
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 37 of 41
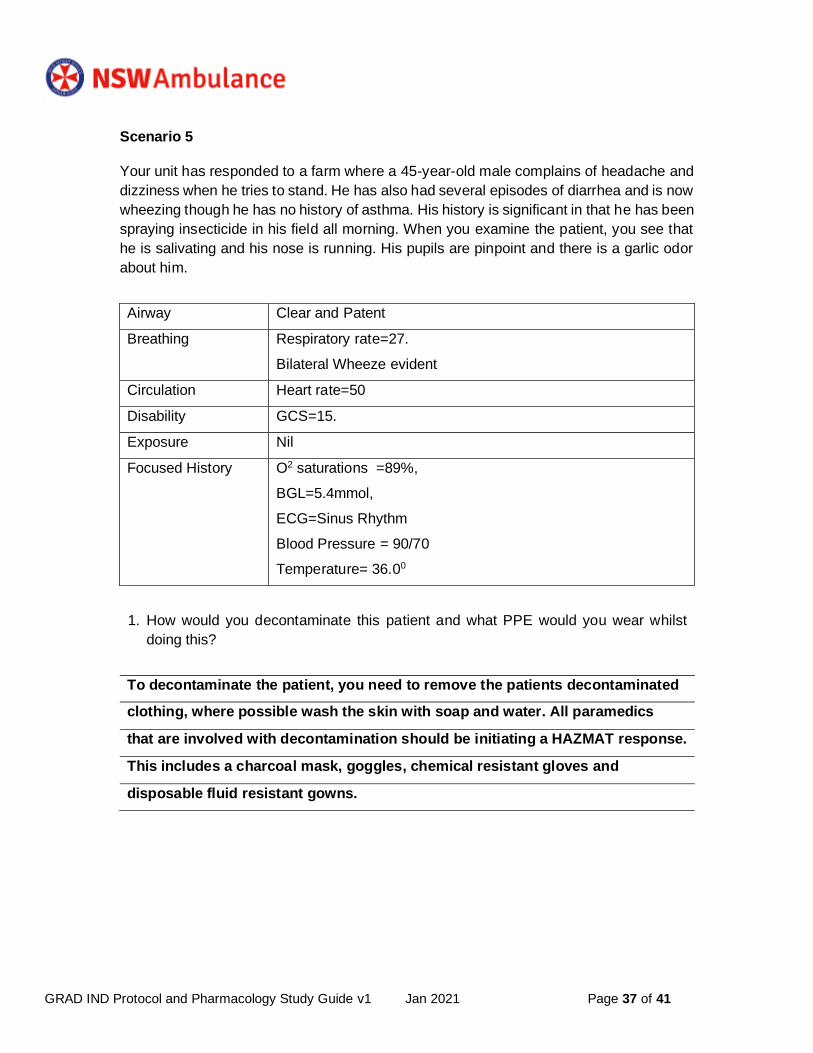
Scenario 5
Your unit has responded to a farm where a 45-year-old male complains of headache and
dizziness when he tries to stand. He has also had several episodes of diarrhea and is now
wheezing though he has no history of asthma. His history is significant in that he has been
spraying insecticide in his field all morning. When you examine the patient, you see that
he is salivating and his nose is running. His pupils are pinpoint and there is a garlic odor
about him.
Airway Clear and Patent
Breathing Respiratory rate=27.
Bilateral Wheeze evident
Circulation Heart rate=50
Disability GCS=15.
Exposure Nil
Focused History O2 saturations =89%,
BGL=5.4mmol,
ECG=Sinus Rhythm
Blood Pressure = 90/70
Temperature= 36.00
1. How would you decontaminate this patient and what PPE would you wear whilst
doing this?
To decontaminate the patient, you need to remove the patients decontaminated
clothing, where possible wash the skin with soap and water. All paramedics
that are involved with decontamination should be initiating a HAZMAT response.
This includes a charcoal mask, goggles, chemical resistant gloves and
disposable fluid resistant gowns.
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 38 of 41
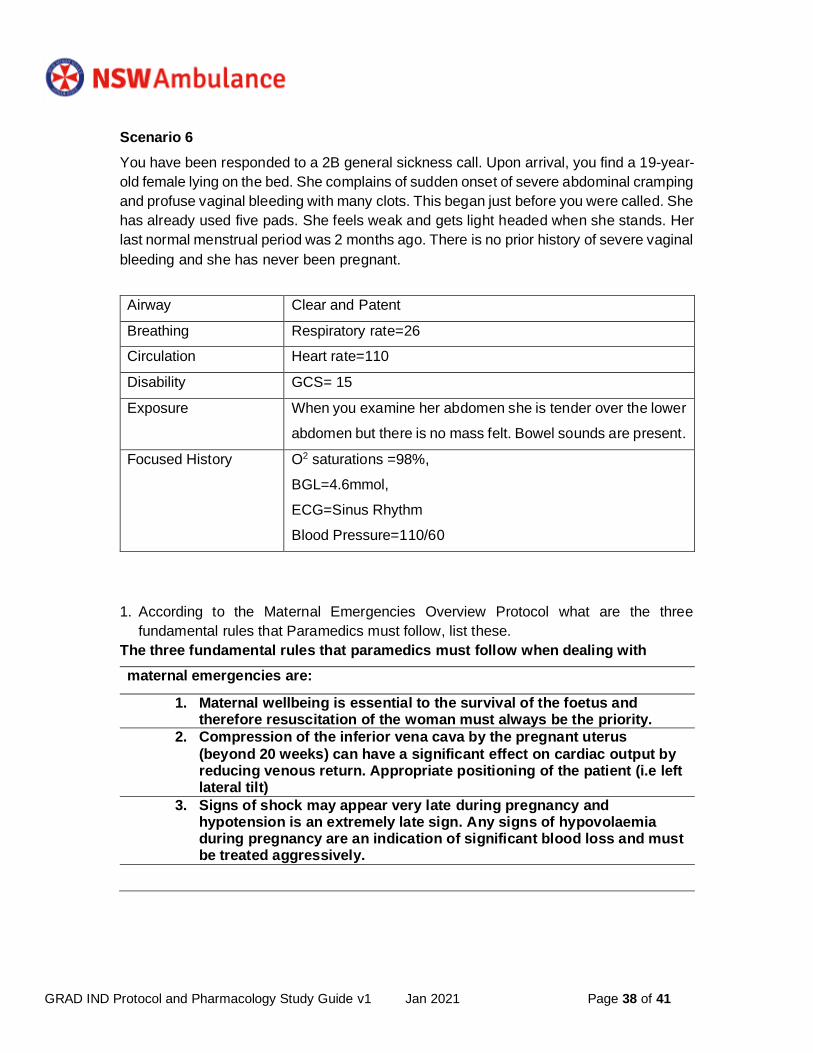
Scenario 6
You have been responded to a 2B general sickness call. Upon arrival, you find a 19-year-
old female lying on the bed. She complains of sudden onset of severe abdominal cramping
and profuse vaginal bleeding with many clots. This began just before you were called. She
has already used five pads. She feels weak and gets light headed when she stands. Her
last normal menstrual period was 2 months ago. There is no prior history of severe vaginal
bleeding and she has never been pregnant.
Airway Clear and Patent
Breathing Respiratory rate=26
Circulation Heart rate=110
Disability GCS= 15
Exposure When you examine her abdomen she is tender over the lower
abdomen but there is no mass felt. Bowel sounds are present.
Focused History O2 saturations =98%,
BGL=4.6mmol,
ECG=Sinus Rhythm
Blood Pressure=110/60
1. According to the Maternal Emergencies Overview Protocol what are the three
fundamental rules that Paramedics must follow, list these.
The three fundamental rules that paramedics must follow when dealing with
maternal emergencies are:
1. Maternal wellbeing is essential to the survival of the foetus and therefore resuscitation of the woman must always be the priority.
2. Compression of the inferior vena cava by the pregnant uterus
(beyond 20 weeks) can have a significant effect on cardiac output by reducing venous return. Appropriate positioning of the patient (i.e left lateral tilt)
3. Signs of shock may appear very late during pregnancy and hypotension is an extremely late sign. Any signs of hypovolaemia during pregnancy are an indication of significant blood loss and must be treated aggressively.
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 39 of 41
2. Your 19-year-old patient is suffering from severe abdominal cramping and profuse
vaginal bleeding with many clots. According to “Bleeding in Pregnancy” Protocol, what
are the general questions that you should ask to assist you in assessing the patient’s
problem.
Bleeding da uring pregnancy can be caused by several conditions, some of which
can be life-threatening to both the woman and the foetus. There are clinical
prompts those paramedics can use to help shape the clinical picture. These
include:
- “Are you or could you be pregnant?” If yes, how many weeks/months do you think you are?
- “When did the bleeding start? What were you doing?” - “What is the blood loss like? How much are you bleeding and are you
still bleeding?” - “Has this happened before or in any other pregnancies?” - “Do you have any pain? When does the pain start? What does it feel
like?”
Given that she is most likely less than 20 weeks pregnant, the focused questions
for this patient would be:
- “Do you have any history of tubal infection, surgery or previous ectopic
pregnancy?”
- “Are you using contraception with progesterone only pills or do you have
an IUD?”
3. What are to be your actions in assessing this patient and what must not be conducted?
While assessing this patient, there should be focused and general questions
around the nature of the bleeding as discussed above. Under no circumstances
should the paramedics conduct a pelvic exam or place anything into the vagina
to control blood loss as life threatening haemorrhage may occur but will not be
evident.
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 40 of 41
You and your partner have responded to R1 medical call. Upon arrival, you find a 30-year-
old female lying on the bed. She says that she is pregnant at term (40 weeks) and the
baby is coming. This is her fourth pregnancy and she has had no problems with any of her
other pregnancies. She receives her prenatal care at the local hospital. When you examine
her perineum, you see that the baby’s head is crowning.
Airway Clear and Patent
Breathing Respiratory rate=22
Circulation Heart rate=110
Disability GCS= 15
Exposure When you examine her abdomen she is tender over the lower
abdomen but there is no mass felt. Bowel sounds are present.
Focused History O2 saturations =98%,
BGL=4.8mmol,
ECG=Sinus Rhythm
Blood Pressure=110/70
1. Discuss the stages of labour. What stage of labour is your patient in?
There are four stages of labour. This patient is in the second stage of labour.
First stage: The longest stage of labour and is from the time of onset of regular
contractions until complete cervical dilation (10cm).
Second stage: The time from complete cervical dilation until delivery of the
foetus. In the out of hospital setting this is when the woman has the urge to push
or the presenting part of the foetus becomes visible.
Third stage: Time from delivery of the foetus until delivery of the placenta and
membranes.
Fourth stage: The first hour after delivery of the placenta.
GRAD IND Protocol and Pharmacology Study Guide v1 Jan 2021 Page 41 of 41
2. What are five questions that you can ask your patient using the Clinical history prompts
to determine the stage of labour?
1. When did the pain commence? Where is the pain? Is the pain constant or
intermittent? How often does the pain occur? How long does the pain last? Is the
pain mild, moderate of severe?
2. Has there been any vaginal discharge or bleeding? What does the
discharge look like?
3. What is the consistency of the discharge?
4. Has the woman had a spontaneous rupture of membranes? If so, what time
did they occur?
5. Does the woman have an urge to push?
6. You deliver a female infant almost immediately. Explain your actions in the care of the
infant.
Post birth, place the newborn on the mothers chest/abdomen with minimal tension
on the umbilical cord and note time of birth. Given this newborn is full term, dry
the newborn whilst maintaining skin to skin with the mother. Perform rapid
assessment of the newborn looking for HR, RR and tone. If the newborn is
positive to the rapid assessment, perform newborn resuscitation. If the newborn is
negative, place newborn lateral or prone on mothers chest, dry the infant and place
a clean, dry wrap around and beanie on the head. Perform APGAR at 1 and 5 minute
mark. Encourage mother to breastfeed.
7. Calculate the APGAR score for your infant patient. The infant is all pink, Pulse= 98, is
coughing and crying, is very active and is breathing fast and regular.
The APGAR of this newborn is a 9. Given this APGAR, once the cord has gone white
(approximately 3-5 minutes after birth) consider cutting the cord in consultation
with the parents wishes.