grad. program lecture #1 notes biochem and physiol of ... 2017... · biochem and physiol of cornea...
TRANSCRIPT
1
Grad. Program lecture #1 NOTES
Biochem and physiol of cornea
Fall 2017
Pic of cornea
- The cornea is the transparent covering of the eye
- the anterior surface is exposed to the external environment while the posterior is
exposed to the aqueous humour
- the cornea is continuous with the sclera and conj.
- and the region between the cornea and sclera is known as the limbus
List of dimensions etc..
- Basic dimensions and properties of the human cornea, please note that some of these
numbers vary depending upon which text you read, so they are just a guideline.
- the human cornea has an area of about 1.3cm2, and takes up about 1/6 circumference of
eye ball
- horizontal diameter is 11-12mm while vertical diameter is typically 9-11mm
- in centre the cornea is about 0.5mm thick
- but it increases in thickness in the periphery to 0.7-1mm
- the cornea is steepest in the centre and flatter in the periphery
- the Radius of curvature is (a) anterior 7.8mm; (b) posterior 6.2-6.8 mm
- the cornea has a refractive power of 40D, which is approx 2/3 of the total refractive
power of the eye
- the overall refractive index of the cornea is 1.376
- and the water content is 78%
(refractive index is ability to bend light…RF of air is 1, bigger difference between RF in
air and of material means more ability to bend light)
Corneal function
list of corneal functions
- The cornea has two primary functions
- the first is to refract light
- how good the cornea is at doing this is dependent upon the transparency, smoothness,
shape and refractive index of the cornea
- maintaining transparency is the most important
- as we’ll discuss in detail later a major factor dictating transparency is the level of
hydration of the cornea
- if there is too much water in the cornea, in other words edema, then the cornea scatters
a great deal of light and so becomes opaque
- the second function is to give protection to the underlying ocular structures
2
- the thick collagen layers of the stroma form a tough covering that is difficult to
penetrate
- and as we’ll talk about in a little while the outer epithelium creates a barrier to
penetration by noxious chemicals and secretes peptides that help protect from infection
(strength from stroma, mechanical barrier and chemical components)
Corneal structure
pic of section through cornea
- the word cornea derives from the Latin word corneus meaning horny
- it consists of 5 distinct layers
- there is the outermost stratified epithelium which itself is composed of several layers of
cells
- beneath the epithelium is the acellular anterior limiting lamina (ALL) originally named
Bowman’s layer after English ophthalmologist Sir William Bowman.
- Dr. Bergmanson who you come across at some point always uses ALL and he will take
great pleasure in correcting you if you say Bowman's.
- what is not acceptable is the term Bowman's membrane, as this is simply not correct
- then comes the stroma which forms the bulk of the cornea
- this is composed of layers of collagen with cells called keratocytes sandwiched between
them
- then there is the posterior limiting lamina (PLL) originally called Descemets membrane,
named after French physiologist Jean Descemet
- Descemets membrane is actually the basement membrane of the final layer known as
the endothelium, which is a single layer of cells
Corneal Innervation
Text slide
- Under normal conditions the cornea is avascular, i.e. no blood vessels, this of course is
to help with transparency
- does however have prominent nerve supply
- paper by Marfurt et al. published in Experimental Eye Research 90(4): 478-492, 2010
that describes the detailed innervation of the human cornea. There was also a nice, but
slightly older review by Muller et al. in Experimental Eye Research 76(5): 521-542,
2003 that reviews the structure, neurochemicals and function of the corneal nerves.
- our current understanding is that the human cornea has two types of nerve fibers
- it is very highly innervated by sensory fibers and also has sparse (adrenergic)
sympathetic fibers
- the sensory fibers are branches of the Ciliary nerves which originate from the
ophthalmic branch of trigeminal nerve (fifth cranial nerve)
- and the sympathetic fibers arise from the superior cervical ganglion
3
- other species such as rat and cat also have parasympathetic innervation (from ciliary
ganglion) but this has not been proven in humans.
Pic of innervation
- the fibers exist as a ring around the cornea which penetrate in to the stroma
- the fibers enter and penetrate the anterior 2/3 of the cornea so they are not found in the
posterior regions around the endothelium
- they course forwards and at the interface of ALL and the stroma form the subepithelial
plexus
- Many fibers from this plexus project up in to the epithelium forming a second plexus,
the "subbasal epithelial plexus" from here the fibers spread between the layers of
epithelial cells and terminate
repeat Text slide
- the fibers have a myelin sheath as they enter the cornea but they rapidly lose this within
about 1 to 1.5 mm after entering (other wise may compromise the transparency of the
stroma) but they do keep a sheath of Schwann cells.
Various nerve Images
This is the cornea of a mouse that has been genetically modified to express a protein that
fluoresces yellow in its sensory nerves….you can see the yellow nerves coursing through
the cornea.
- As the nerves pass through the stroma you'll often find that they are in close proximity
to keratocytes and sometimes cytoplasmic projections from the keratocytes can be seen
encircling the nerve fibers
- this is suggestive of interactions between keratocytes and neurons
(contact between keratocytes and neurons occurs more often in patients with keratoconus,
although it is unclear if this is cause or effect)
- the nerves retain a coat of Schwann cells until they get to the epithelium
- here the coat is lost and the nerves end as “naked” terminals in between the epi cells
- in effect the epithelial cells serve as the Schwann cell coat
here is a schematic from Muller review article showing an artists impression of nerves
terminating in the epithelium, and here is actual staining for the nerves, using b-tubulin,
can see them going all the way up through the epithelium.
Confocal images
It is also possible to visualize the nerves in the living human eye using an instrument
called the confoscan…this is an in vivo confocal microscope. The patient sits in a head
4
rest and the objective is brought up to the eye, a blob of gel is used to couple the corneal
surface to the objective.
Then can capture images through the whole thickness of the cornea from epithelium to
endothelium. See those images on the screen, then machine has various programs to
allow e.g. to count density of cells.
This is what the corneal nerves can look like….currently most imaging for nerves is for
research studies for example this equipment has been used to show loss of nerve density
with contact lens wear.
The college also has several Heidelburg retinal tomographers for research use and both of
these come with whats called a cornea module which allows visualization of the cornea
very similar to that seen with the Confoscan.
Text of nerves - sensory
- Studies have shown that the sensory nerve endings in the cornea contain several
neuropeptides
- the major ones are SP, CGRP, PACAP (pituitary adenylyl cyclase activating peptide),
and Galanin
- SP and CGRP containing fibers are most abundant
- nerve fibers may contain either or both of these neuropeptides
- the exact roles of each of these neuropeptides is uncertain
- loss of the most superficial cell layers of the epithelium exposes the sensory nerve
endings and is very very painful
- largely because of the very high density of terminals in the cornea…something like an
average of 2500 terminals/mm2, about 5 times that of skin
- central cornea has highest density of fibers so is very sensitive whereas
- peripheral cornea has less fibers and is less sensitive
- corneal sensitivity also varies diurnally, so the cornea is more sensitive in the morning
(important to consider when doing clinical studies)
- sensory fibers are most sensitive to touch i.e. mechanical pressure which produces a
sensation of pain
- also believed to sense temperature and some say pH, again response to both of these
stimuli is manifest as pain
- having this exquisite sensitivity is essential to the well being of the cornea
- stimulation of the sensory nerve fibers is a clear indication that something is wrong
- and through central mechanisms and local release of neuropeptides from the nerve
endings, leads to reflex blinking and tearing which are protective mechanisms to wipe or
wash away anything irritating the corneal surface
5
- SP and CGRP are released after an injury and in part mediate the ocular response to
injury (involves lacrimation, vasodilation of limbal vessels, protein extravasation,
increased IOP, modulating macrophage and leucocyte function)
- in addition to the perception of pain, the sensory nerves are believed to have a trophic
effect on the corneal epithelium, in other words they provide soluble substances essential
to the health and well being of the epithelium.
- we know this because destruction of the sensory input, weather by experimental surgical
means or infections such as Herpes, results in a condition called neurotrophic (or
neuroparalytic) keratitis where there is rounding up of the epithelial cells, breakdown of
complexes that hold the cells together, increased epithelial permeability, and impaired
wound healing after an injury
- it is presumed then that neuropeptides released by sensory nerve endings are responsible
for the trophic effect in other words they regulate the normal growth and normal function
of the corneal epithelial cells.
- this has yet to be successfully proved in vivo (knockouts) but is supported by studies in
vitro which for example have shown that both SP and CGRP can under certain conditions
(+ IGF-1 or EGF) stimulate epithelial cell division and migration. (both of which are
required for normal corneal healing)
More nerve text - sympathetic
- The precise role of the (adrenergic) sympathetic nerves that are scattered through the
cornea is unclear
- the major neurochemicals present in these nerves are norepinephrine, serotonin and
neuropeptide Y
- thought that they are involved in modulating ion transport in the epithelium
- also appear to stimulate corneal epithelial cell proliferation under normal physiologic
conditions and during corneal wound healing (via action of NA, independent of peptides),
so again likely have a trophic role in maintaining the health of the epithelium.
- so to summarize
- the cornea has mostly sensory fibers but also a few sympathetic fibers
- the sensory fibers are there to detect pain, which triggers reflex blinking and tearing to
protect the cornea
- they also provide a nurturing environment to maintain a healthy epithelium
- the sympathetic fibers likely help regulate epithelial ion transport and also may
be required for regulating epithelial cell proliferation
There is still a lot to learn about corneal nerves but more people are starting to study them
so hopefully we’ll have a clearer picture of precisely what they do over the next few
years.

6
Corneal nutrition and metabolism
text slide of nutrition
- OK so lets talk a little about how the cells of the cornea get the nutrients they need to
stay healthy
- corneal cells primarily use glucose to produce energy
- and let me remind you that that the major form of energy used by cells is ATP
- adenosine triphosphate
pic of ATP
ATP is a nucleotide consisting of an adenine ring, a sugar called a ribose, and three
phosphate groups
The last two phosphate groups are each joined to the rest of the molecule by a high
energy bond.
Hydrolysis of ATP, in other words breaking of the high energy bond and removal of one
of the phosphates leaves adenosine diphosphate, and removal of the second leaves
adenosine monophosphate.
When each bond is hydrolysed 12kcal of energy is released that can be harnessed to drive
reactions that require energy for example synthesising macromolecules such as proteins
and nucleic acids, moving things around inside of the cell or across the plasma
membrane
- so the glucose that is taken up by the cells is used to make ATP
rpt of nutrition text
- most of the glucose used by the corneal cells comes by diffusion from the aqueous
humour where the level of glucose is roughly equivalent to that of blood i.e. about 5mM
under basal conditions
- up to about 10% may come from limbal blood supply and tears
- so even the epithelium gets most of its glucose from AH
- also the epithelium has large stores of glucose in the form of glycogen this ensures that
even if the supply of glucose from the AH is reduced then the cells have enough to
survive
- glucose is taken up by corneal cells using specific transporters called GLUTs. Once
inside the cell it can be metabolized by several pathways but the primary way is by
glycolysis followed by the Krebs cycle followed by oxidative phosphorylation.

7
We are not going to go in to this in great detail, but if you want to remind your selves of
biochemistry etc that like me you probably did many years ago you can look up the
details in texts such as Molecular Biology of the Cell or Biochemistry by Stryer.
pic glycolysis
- glycolysis is a metabolic pathway that occurs in the cytoplasm of the cell
- it begins with the phosphorylation of glucose, which is then gradually converted into
pyruvate by a series of sequential enzymatic reactions.
- in addition to pyruvate the other two important products are ATP and NADH (2 mole of
each from one mole glucose)
- the pyruvate that is generated is then further metabolized in the mitochondria
pic of mitochondrion This is the classic view of what a mitochondrion looks like. Each mitochondrion is bound
by two membranes, referred to as the inner and outer membranes, thus the mitochondrion
has two compartments
There is the inner matrix, which is bound by the inner membrane
Then there is a narrow intermembrane space, before the outer membrane is reached.
The outer membrane contains the protein porin which forms large channels through the
membrane, so this membrane is very leaky and allows for the passage of relatively large
molecules.
(The outer membrane also contains the enzymes necessary for lipid metabolism.)
The inner membrane is folded to form many cristae…this increases the surface area
The inner membrane contains enzymes that carry out oxidative phosphorylation and that
synthesize ATP.
Whereas the matrix contains enzymes required for citric acid cycle and the breaking
down of fatty acids.
The matrix also has copies of all the necessary genes so that the whole mitochondrion can
be rapidly replicated in times when the demand for energy rises
pic of Krebs cycle The pyruvate that is generated by glycolysis (and any from the breakdown of amino
acids) in the cytosol is transported in to the mitochondrion where it is converted to
acetylCo by the action of an enzyme called pyruvate dehydrogenase (also get carbon
dioxide and NADH)
8
The acetyl coA formed from pyruvate (and any derived from fat metabolism) then passes
in to the citric acid cycle (also known as the Krebs or tricarboxylic acid cycle)
The cycle beings when acetyl coA interacts with oxalocetate giving citrate…hence one of
the names for the cycle
So a molecule containing two carbon atoms interacts with another that has 4 carbon
atoms to give a new molecule that has 6 carbon atoms
In the following 7 sequential enzyme mediated reactions two carbon atoms are removed
as CO2 and the oxaloacetate is regenerated and can enter the cycle again
The cycle also produces one GTP that can be readily converted to ATP
In terms of energy production most important molecules generated in the citric acid cycle
are NADH and FADH2
NAD(H) is nicotinamide adenine dinucleotide
FAD(H2) is flavin adenine dinucleotide
These molecules are the means by which high energy electrons are transferred from the
citric acid cycle to the pathway of oxidative phosphorylation by which ATP is generated.
Pic of electron transport chain
Oxidative phosphorylation occurs on the inner mitochondrial membrane.
Embedded in the membrane are a series of metal containing proteins which form the
carriers of the electron transport or respiratory chain.
The electrons being carried by NADH produced during glycolysis and the citric acid
cycle and FADH2 produced by the citric acid cycle
Are transferred to the first carrier group then transferred sequentially between the
carriers.
The first carrier is the NADH dehydrogenase complex, the second cytochrome b-c1 and
the third cytochrome oxidase
And ubiquinone is the go between from 1st to 2
nd and cytochrome c is go between from
2nd
to 3rd
Energy is released as the electrons move from one carrier to the next and this energy is
used to pump hydrogen ions across the inner mitochondrial membrane, out of the matrix.
9
This concept was first proposed by Mitchell in 1961 and was called the chemiosmotic
hypothesis. (The term chemiosmotic describes the linking of a chemical reaction , i.e. the
transport of electrons, with movement, or osmosis which is Greek for “to push”.)
The energy that is released as the electrons are transferred down the respiratory chain is
used to pump hydrogen ions across the inner mitochondrial membrane, out of the matrix.
The pumping of hydrogen ions creates both a pH and a voltage gradient…such that the
pH is higher in the matrix and the matrix side of the inner membrane is -ve (whereas have
low pH and positive charge in intermembrane space)
These gradients create the proton motive force that drives the hydrogen ions back across
the inner membrane.
(the pH gradient tends to drive H+ back across the membrane, whereas the voltage
gradient attracts positive ions in to the matrix and pushes negative ones out)
As the hydrogen ions are driven back across the membrane, the enzyme ATP synthase is
activated and catalyses the addition of an inorganic phosphate group to ADP so making
ATP
For every two electrons that pass down the respiratory chain 2-3 ATP are generated.
(ATP synthase is clever enzyme - a reverse coupling device- that can either make ATP or
hydrolyse it…normally proton motive force favours synthesis. The number of hydrogen
ions that are required to flow through the enzyme in order to make one ATP is unknown)
Calc of ATP from glucose (So for the metabolism of glucose, for every glucose metabolised by glycolysis you
generate 2 ATP, 2 NADH and 2 pyruvate.
Then in converting the 2 pyruvate to 2 acetyl coA, 2 more NADH are generated.
Then via the citric acid cycle, the metabolism of the two acetyl coA, gives 2 GTP which
become 2 ATP, 6 NADH and 2 FADH2.
So that’s 4 ATP, 10 NADH and 2 FADH2
Each NADH carries one pair of electrons, which enters the respiratory chain. For each
pair of electrons that passes down the chain, 3 ATP are generated. 10 NADH so get total
of 30ATP.
Each FADH2 carries one pair of electrons, which enters the respiratory chain but at a
later stage than the electrons from NADH so only get 2 ATP per FADH2….so have total
of 4 ATP.) Over all get 38 moles of ATP from one mole of glucose.
- what we have just described is aerobic metabolism and can only occur if there are
adequate levels of oxygen for oxidative phosphorylation.
However there are instances when there is not enough oxygen around e.g. overnight
while lids are closed or with some contact lenses, in which case oxidative
10
phosphorylation cannot occur so anaerobic metabolism predominates particularly in
corneal epithelial cells.
Anaerobic metabolism
In anaerobic metabolism glucose is metabolised by the glycolytic pathway generating 2
ATP for each mole of glucose.
However, the pyruvate formed cannot enter the citric acid cycle because there is not
enough oxygen for oxidative phosphorylation to occur, but it must go some where,
otherwise it would accumulate and by a negative feed back effect, inhibit the glycolytic
pathway.
So the pyruvate formed is converted in to lactic acid by a reaction involving NADH,
hydrogen ions and the enzyme lactate dehydrogenase.
The lactic acid then diffuses out of the cells.
When oxygen becomes available again the lactic acid can be converted back to pyruvate
which can then enter the citric acid cycle and undergo oxidative phosphorylation. Or the
pyruvate can be converted back to glucose and then into glycogen for storage.
Also some of the lactate produced will diffuse through the corneal stroma and into the
aqueous humour and so is eliminated.
So metabolism of glucose under anaerobic conditions produces only 2 ATP, but this is
better than nothing.
- the lactate that forms cannot normally be eliminated via the tear film because it cannot
pass the barrier formed by the superficial epithelial cells.
- if however the epi barrier is compromised the lactate can pass in to the tear film…in
fact the presence of significant amounts of lactate in the tear film is used as an indicator
of epithelial damage.
- excessive production or failure to remove lactate leads to sustained elevated levels in
the cells and the intercellular spaces which alters the osmotic balance (causes hypertonia)
in the cornea and causes oedema both in the epithelial layer and in the stroma which
compromises vision
- some glucose is also metabolised by a pathway called the hexose monophosphate shunt
pic HMP Shunt
this is an off-shoot of glycolytic pathway in which glucose-6-phosphate (6C sugar) is
converted in to ribose 5 phosphate (5C sugar) for use in nucleic acid synthesis, and
11
produces NADPH required for variety of biosynthetic reactions e.g. fatty acid synthesis
and provides “reducing” power to help protect against oxidative damage.
- finally glucose can also be metabolized via the sorbitol pathway (also known as polyol
pathway) in which glucose is converted in to sorbitol and fructose by an enzyme called
aldose reductase
- thought that in diabetes where have raised levels of glucose that more glucose than
normal is metabolised via the sorbitol pathway
- this leads to the accumulation of sorbitol which alters the osmotic balance of the corneal
cells, leading to cell swelling and cell damage
- may be responsible for some of the corneal changes seen in diabetics
- the cornea obtains oxygen from atmosphere via the tears when eye open
- when the eyes are closed may still have enough in tears to supply needs (switch from
aerobic to anaerobic metabolism)
- if required can also obtain small amount from vessels in limbal area or from AH, or
from conjunctival vessels when the eye is closed
- but in general all oxygen even that for the endothelium comes from tears (more oxygen
in tears than AH)
- pretty much all other nutrients….amino acids, vitamins, ions etc..are supplied via the
AH
GLYCOCALYX and TEARFILM
pic of glycocalyx
here a cell has been stained to show the glycocalyx which is this very dark material
coating the surface
glycocalyx cartoon
and this is a depiction of the actual components..
so black is the lipid bilayer i.e. the plasma membrane, green are proteins and blue are
carbohydrate i.e., sugar groupings.
many proteins traverse the plasma membrane of the epithelial cells and project out into
the extracellular environment.
These proteins are covered in a layer of carbohydrate.
Also there are glycolipids embedded in the plasma membrane that are oriented so that the
carbohydrate groups project outwards
12
Together the layer of carbohydrate over the proteins along with the sugar residues present
on glycolipids constitute the glycocalyx.
(also includes proteins with carbohydrate chains that have been absorbed on to the
surface)
A variety of roles have been suggested for the glycocalyx..including that it is a protective
layer, protecting the membrane from mechanical and chemical damage
It may also help to keep foreign objects and other cells at a safe distance also mediate
cell-cell adhesion processes and at the ocular surface helps mediate interaction between
corneal epithelial cells and the tear film.
OK so the glycocalyx is formed by carbohydrate groups that are attached to proteins in
the plasma membrane and of proteins and material that has been absorbed on to the cell
surface
- the glycocalyx on the plasma membrane of the superficial corneal cells interacts with
molecules called mucins of tear film
pic of tear film
the tear film coats the ocular surface,
we won’t talk much about the tear film
there are literature reports on its thickness vary greatly ranging from 1-2um to 50um, an
average number of 7-10um.
- classically the tear film is described as being composed of three layers…..an outermost
lipid layer that prevents evaporation of the other layers.
Then there is the inner aqueous layer, which is produced by lacrimal and accessory
lacrimal glands.
Then a mucin layer in direct apposition to the corneal surface.
- recently there has been a shift in thinking about the tear film, and rather than forming
three distinct layers more and more people are beginning to think that all the three major
components interact to form a more gel like layer with a gradient of lipid with
concentration being higher concentration further away from the ocular surface and a
gradient of mucin with the concentration being highest at the ocular surface.
The lipid components are secreted by the meibomian glands that line the lids and their
function is to help prevent evaporation of the tears. As we age we gradually lose
meibomian glands which may contribute to accelerated tear evaporation and the dry eye
typically seen at older ages.

13
The aqueous component contributes ions, enzymes, etc….
The mucins are proteins, abbreviated to MUC, the major one is Muc5ac which is a
soluble mucin secreted by the goblet cells of the conjunctiva in to the tear film.
Recent evidence also suggests that both conjunctival and corneal epithelial cells produce
some of the mucin components in particular MUC 1, 4 and 16. These mucins are bound
to the plasma membrane of the epithelial cells.
- the mucins essentially become part of the glycocalyx. The soluble mucins in the tear
film are absorbed by the glycocalyx where they interact with glycoproteins. Whereas the
membrane bound mucins project from the cell surface and interact with the tear film.
These interactions basically helps hold the tear film on to the ocular surface.
- together the mucins and other glycoproteins decrease the surface tension of the
hydrophobic (water hating) plasma membrane of the cell making the surface wettable by
the aqueous tears
- so this allows tears to be evenly spread over the cornea
- the microvilli project out about 500nm (?) for the surface of the cell, the tears fill the
gaps between the projections and so you get a nice smooth optical surface for refracting
light
( Plasma membrane of cells is lipid bilayer that is hydrophobic so if unaltered would
cause aqueous tears to bead up)
- in addition this surface also resists attachment of bacteria
- most microorganisms have to attach to the surface of a cell before they can penetrate
and infect it
- an intact smooth ocular surface appears to help prevent attachment
EPITHELIUM
pic of epi.
- the epithelium contributes to both the refractive and protective functions of the cornea
- through interacting with the tear film it provides a nice smooth surface for the refraction
of light
- it forms a barrier to prevent entry of fluid and noxious substances and produces
antimicrobial substances
- the epithelium is described histologically as a stratified squamous nonkeritinized
epithelium
- about 50um thick over the whole length of epi.
- typically is 5 to 7 cell layers thick
- cells are tightly packed with no intercellular spaces, fit tightly together rather like pieces
of a jigsaw
- there are usually 2-3 outer layers of flattened cells called superficial cells
14
- then there are 2-3 middle layers of wing cells, some people call these umbrella cells
- and there is a single inner layer of basal cells which sit on a basement membrane that
they secrete, this separates them from ALL
- the basement membrane, also known as the basal lamina, is about 50-100nm wide and
can be divided in to two layers according to its appearance in the electron microscope
- the most anterior layer appears light and is the lamina lucida, it is approx 24nm wide
and its major component is laminin
- the posterior layer appears darker and is the lamina densa, it is 30-60nm wide and its
major component is collagen type IV. This layer increases in thickness with age and
becomes particularly thick in people who are diabetic
- other components of the basal lamina include fibronectin, collagen XII and perlecan
- the cells represent different stages of differentiation of same cell type
- so a basal cell divides and differentiates in to a wing cell which then undergoes terminal
differentiation to become a superficial cell which is eventually sloughed off in to tear film
- if you look at the superficial cells with an electron microscope can see some appear
darker than others..its believed that these are cells that are about to be shed
- the sloughing cells are thought to die by apoptosis
- an even closer look under the electron microscope reveals that the outer most layer of
superficial cells have hundreds of tiny finger-like projections, these are called microvilli
- also some areas appear to have ridges or folds, these are called microplicae
Cell-cell, cell-stroma interactions texts
- The cells of the epithelium are held tightly and very closely together and through the
basal layer they are attached very very firmly to the underlying anterior limiting lamina
and the stroma so they form a very effective barrier
- each of the cell layers of the epithelium is particularly rich in junctions suited to its
position and function
- the superficial cells have many tight junctions holding them together.
schematic of tight junction, pic of tight junction EM - The particular type of tight junction they have is called the zonula occludens.
- this type of junction effectively binds two neighbouring cells together creating a barrier
that is effectively impermeable to water and other aqueous molecules
- even when look at junction under an electron microscope no visible gap between the
two parts of the plasma membrane
- in the zonula occludens junction the interaction of transmembrane proteins from each
cell forms a belt that completely encircles the cell, joining it to its different neighbours
and forming a barrier completely impenetrable to all but the tiniest molecules
15
- the barrier created by the tight junctions resists entry of fluid from the tear film
- therefore the epithelium helps prevent corneal oedema
- this can be readily demonstrated by scraping off the epithelium, then measuring corneal
thickness, find that increases steadily with time, causing up to 0.2mm increase in
thickness
- several proteins have been identified as components of the zonula occludens
- these include claudins and occludins which are transmembrane proteins which interact
with peripheral membrane proteins (on inside of cell) ZO-1 and –2 which in turn link to
the actin cytoskeleton. are but precise roles for each have yet to be assigned
- tight junctions occasionally found in wing cell or basal cell layer but by far most
common junction in superficial layer
- wing cells are particularly rich in junctions called desmosomes or macula adherens
- these are located on the lateral cell surfaces, and essentially rivet adjacent cells together
at intervals down the sides of the cells
- the desmosome has an electron dense region or plaque on the inside of the membrane
which is composed of a complex of proteins (such as plakoglobin and desmoplakins)
responsible for connecting to the intermediate filaments of the cell cytoskeleton
- then projecting from the plaque across the plasma membrane and in to the intercellular
space are proteins called cadherins
- the cadherins interact with cadherins coming from the adjacent cell (literature
conflicting as to which cadherin in corneal epi..some say E is present some say its not 20
or so cadherins, E cadherin typically in epithelia and it interacts with beta-catenin and
p120 catenin, weak beta-catenin staining reported throughout epi..)
- these connections help make the epithelium mechanically strong and capable of
resisting significant shearing forces caused by rubbing the eye
- also find desmosomes between wing cells and superficial cells between basal cells and
wing cells and between basal cells and basal cells but not as numerous as in wing cell
layer
- Basal cells have most important attachment because they are the means through which
the whole epithelium is anchored down firmly on to the remainder of the cornea
- basal cells are attached to each other by desmosomes and are firmly attached to the
basement membrane and the underlying stroma by structures called adhesion complexes
- the major components of these adhesion complexes are a type of cell-cell junction
called a hemidesmosome, and also anchoring fibrils and anchoring plaques
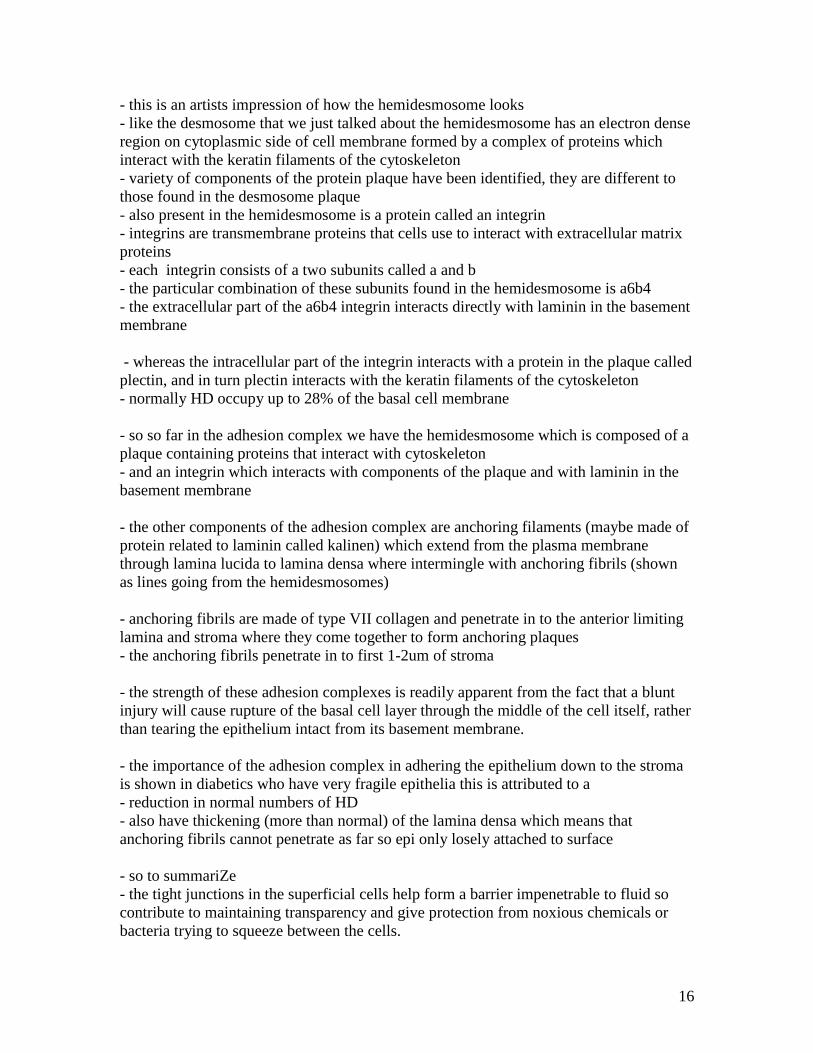
Pic Schematics of hemidesmosomes
- as its name suggests the hemidesmosome looks like half of a desmosome
16
- this is an artists impression of how the hemidesmosome looks
- like the desmosome that we just talked about the hemidesmosome has an electron dense
region on cytoplasmic side of cell membrane formed by a complex of proteins which
interact with the keratin filaments of the cytoskeleton
- variety of components of the protein plaque have been identified, they are different to
those found in the desmosome plaque
- also present in the hemidesmosome is a protein called an integrin
- integrins are transmembrane proteins that cells use to interact with extracellular matrix
proteins
- each integrin consists of a two subunits called a and b
- the particular combination of these subunits found in the hemidesmosome is a6b4
- the extracellular part of the a6b4 integrin interacts directly with laminin in the basement
membrane
- whereas the intracellular part of the integrin interacts with a protein in the plaque called
plectin, and in turn plectin interacts with the keratin filaments of the cytoskeleton
- normally HD occupy up to 28% of the basal cell membrane
- so so far in the adhesion complex we have the hemidesmosome which is composed of a
plaque containing proteins that interact with cytoskeleton
- and an integrin which interacts with components of the plaque and with laminin in the
basement membrane
- the other components of the adhesion complex are anchoring filaments (maybe made of
protein related to laminin called kalinen) which extend from the plasma membrane
through lamina lucida to lamina densa where intermingle with anchoring fibrils (shown
as lines going from the hemidesmosomes)
- anchoring fibrils are made of type VII collagen and penetrate in to the anterior limiting
lamina and stroma where they come together to form anchoring plaques
- the anchoring fibrils penetrate in to first 1-2um of stroma
- the strength of these adhesion complexes is readily apparent from the fact that a blunt
injury will cause rupture of the basal cell layer through the middle of the cell itself, rather
than tearing the epithelium intact from its basement membrane.
- the importance of the adhesion complex in adhering the epithelium down to the stroma
is shown in diabetics who have very fragile epithelia this is attributed to a
- reduction in normal numbers of HD
- also have thickening (more than normal) of the lamina densa which means that
anchoring fibrils cannot penetrate as far so epi only losely attached to surface
- so to summariZe
- the tight junctions in the superficial cells help form a barrier impenetrable to fluid so
contribute to maintaining transparency and give protection from noxious chemicals or
bacteria trying to squeeze between the cells.
17
- the desmosomes between the wing cells give strength to the epithelial layer helping it to
resist mechanical force
- whereas adhesion complexes of the basal cells anchor the whole epithelium to the
underlying stroma again helping it to resist mechanical force
- another type of junction found in the epithelium are gap junctions which allow the cells
to communicate with one another
- gap junctions are formed by proteins called connexins that are embedded in the cell
membrane
- when 6 of these connexins associate they form a little channel through the membrane
called a connexon
- when the connexons from two adjacent cells are in direct alignment to each other they
form a gap junction which allows for the passage of inorganic ions and small molecules
between cells
- in the epithelium gap junctions in basal cells are composed of connexin 26, 30, 31, 43.
43 and 30 found in all layers, 26 only in “lower supra basal layers…presume they mean
wing), 31 only in apical surface of basal cells.
(from Shurman et al. IOVS 2005 46(6) 1957-65)
- most of the spread of information occurs basal cell to basal cell, wing cell to wing cell
and basal-wing cell, there is minimal communication form the cells of the lower layers
and the superficial cells.
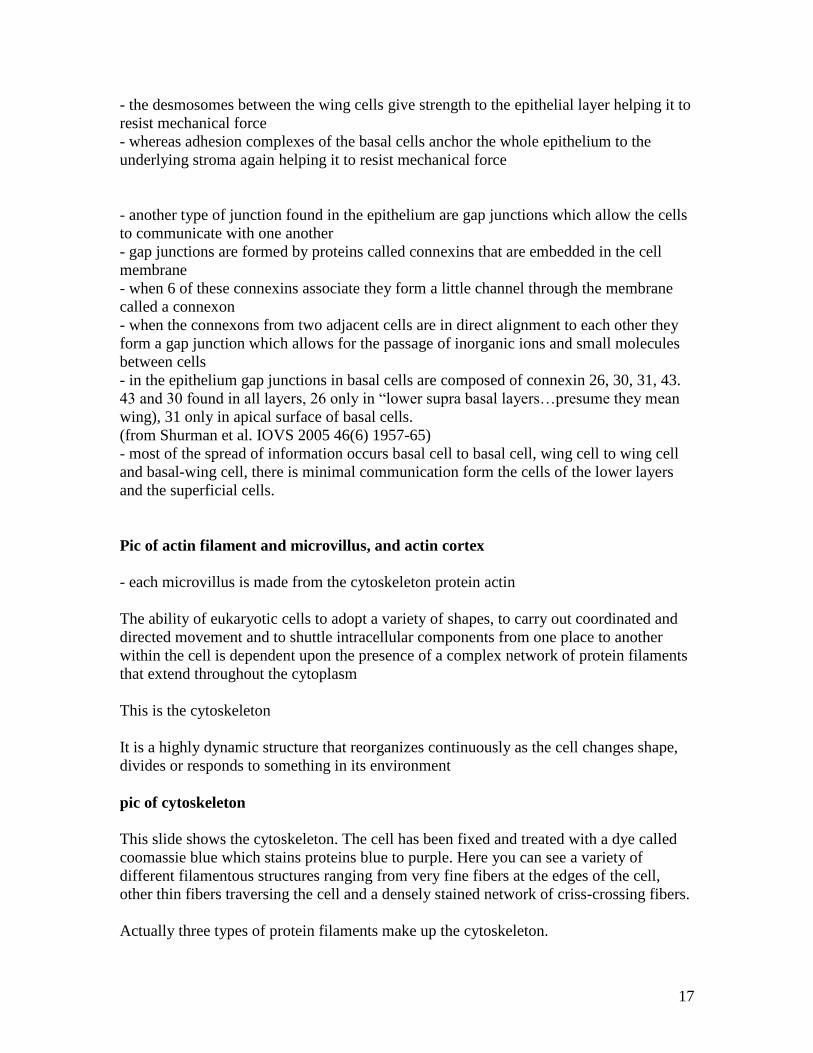
Pic of actin filament and microvillus, and actin cortex
- each microvillus is made from the cytoskeleton protein actin
The ability of eukaryotic cells to adopt a variety of shapes, to carry out coordinated and
directed movement and to shuttle intracellular components from one place to another
within the cell is dependent upon the presence of a complex network of protein filaments
that extend throughout the cytoplasm
This is the cytoskeleton
It is a highly dynamic structure that reorganizes continuously as the cell changes shape,
divides or responds to something in its environment
pic of cytoskeleton
This slide shows the cytoskeleton. The cell has been fixed and treated with a dye called
coomassie blue which stains proteins blue to purple. Here you can see a variety of
different filamentous structures ranging from very fine fibers at the edges of the cell,
other thin fibers traversing the cell and a densely stained network of criss-crossing fibers.
Actually three types of protein filaments make up the cytoskeleton.

18
list of filament types
Actin or microfilaments – cell shape & movement
Microtubules – transport and cell division
and intermediate filaments – mechanical support
Each filament is composed of thousands of protein molecules joined together to form a
structure that may stretch from one side of the cell to the other
(The filaments are responsible for changing cell shape, for allowing movement, some
connect protein complexes and organelles in different regions of the cell and serve as
tracks to facilitate transport between them while others provide mechanical support.)
pic actin filaments The actin filaments which go in to making the microvilli are found throughout the
cytoplasm but as shown in this figure are concentrated in the cell cortex, in other words
the area immediately below the plasma membrane.
To make the filament many molecules of the protein G-actin (G for globular) polymerize
(requires ATP) together to form long chains, then two chains intertwine to form a helix.
A variety of different proteins can associate with the actin filaments and help organize the
actin either into bundles or a web/gel like network.
For example Fimbirn and a-actinin are called actin-bundling proteins. Fimbrin helps pack
actin filaments very close together to help form thin projections called filopodia.
a- Actinin on the other hand holds the actin filaments further apart, and gives enough
room between filaments for another protein called myosin to bind so forming what is
known as a stress fiber.
Myosin allows the actin filaments to be pulled over each other, hence produces a
contraction. This allows a cell to make small changes in shape and so mould itself to the
shape of for example the basement membrane it rests on.
Yet another actin binding protein called filamin, cross links two actin filaments together
so forming a loose gel like net work (involved in lamelipodia formation).
Pic of lamellipodia
So the various different actin binding proteins give actin different properties so allowing
actin to participate in short lived and dynamic structures that are produced when the cell
needs them such as the lamellipodia a corneal epithelial cell uses to migrate across the
corneal surface. It also participates in the formation of stable structures such as the
microvilli that project from the surface of superficial cells at the corneal surface
19
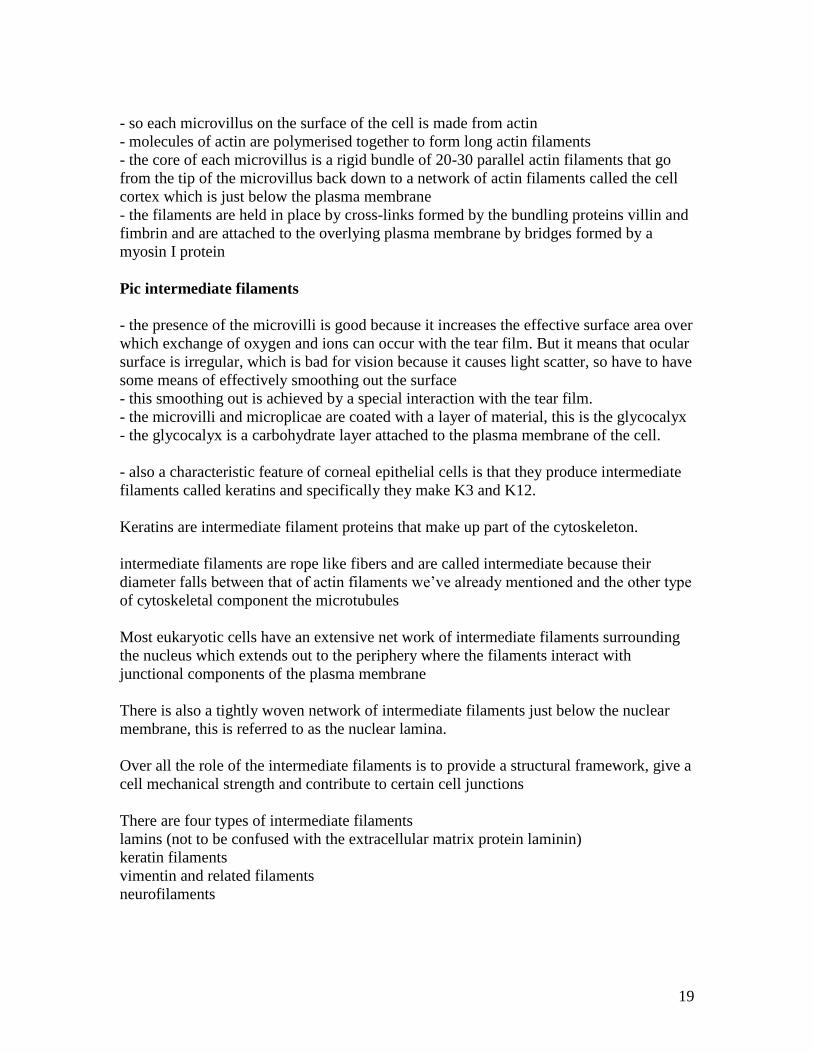
- so each microvillus on the surface of the cell is made from actin
- molecules of actin are polymerised together to form long actin filaments
- the core of each microvillus is a rigid bundle of 20-30 parallel actin filaments that go
from the tip of the microvillus back down to a network of actin filaments called the cell
cortex which is just below the plasma membrane
- the filaments are held in place by cross-links formed by the bundling proteins villin and
fimbrin and are attached to the overlying plasma membrane by bridges formed by a
myosin I protein
Pic intermediate filaments
- the presence of the microvilli is good because it increases the effective surface area over
which exchange of oxygen and ions can occur with the tear film. But it means that ocular
surface is irregular, which is bad for vision because it causes light scatter, so have to have
some means of effectively smoothing out the surface
- this smoothing out is achieved by a special interaction with the tear film.
- the microvilli and microplicae are coated with a layer of material, this is the glycocalyx
- the glycocalyx is a carbohydrate layer attached to the plasma membrane of the cell.
- also a characteristic feature of corneal epithelial cells is that they produce intermediate
filaments called keratins and specifically they make K3 and K12.
Keratins are intermediate filament proteins that make up part of the cytoskeleton.
intermediate filaments are rope like fibers and are called intermediate because their
diameter falls between that of actin filaments we’ve already mentioned and the other type
of cytoskeletal component the microtubules
Most eukaryotic cells have an extensive net work of intermediate filaments surrounding
the nucleus which extends out to the periphery where the filaments interact with
junctional components of the plasma membrane
There is also a tightly woven network of intermediate filaments just below the nuclear
membrane, this is referred to as the nuclear lamina.
Over all the role of the intermediate filaments is to provide a structural framework, give a
cell mechanical strength and contribute to certain cell junctions
There are four types of intermediate filaments
lamins (not to be confused with the extracellular matrix protein laminin)
keratin filaments
vimentin and related filaments
neurofilaments
20
The lamins form the network of filaments lining the inside of the nuclear membrane
which is called the nuclear lamina
Vimentin is found in many cell types, and other related proteins are found in specific
cells
Desmin is found in muscle cells and GFAP is found in glial cells
Keratins or cytokeratins as they are often called are found in epithelial cells
There are over 20 different types of keratin which based on their amino acid sequence
can be divided in to acidic or basic or type I and type II.
Neuronal intermediate filaments as their name suggests are found in neurones and are
also known as neurofilaments.
They are found in both the cell body of the neuron and in the axon and come in three
forms, called NF-L, M and H have been identified so far (L, M, H refers to molecular
weight, usually the neurofilament contains all of the three forms)
Despite the many different proteins the basic structure of the intermediate filament is the
same.
First two protein molecules come together to form a dimer, then two dimers form a
tetramer, then the tetramers join up end to end. Then several strands of tetramer are
packed together to form a circular filament.
For a vimentin filament all the basic protein units are the same, whereas for a keratin
filament, one acidic keratin protein comes together with one basic protein to form the
dimer which is then known as a keratin pair.
As said the major function of intermediate filaments is to provide support and help the
cell resist mechanical stress
As you can see the components in the filaments are arranged so that there is much
overlapping of the peptide chains which makes them able to with stand a great amount of
force (much more than actin or the microtubules) before they rupture.
So the intermediate filaments in epithelial cells are called keratins and the specific keratin
pair present in corneal epithelial cells is unique to those cells and is composed of acidic
K12 (55kDa) and the basic K3 (64 kDa)
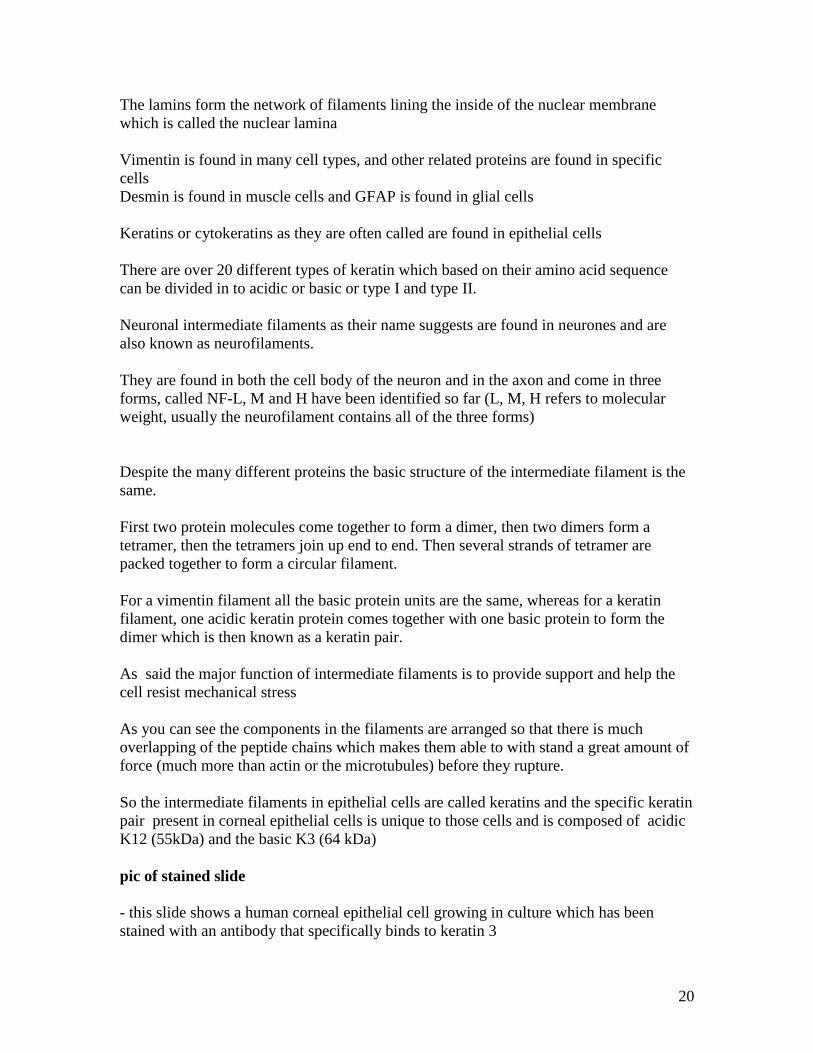
pic of stained slide
- this slide shows a human corneal epithelial cell growing in culture which has been
stained with an antibody that specifically binds to keratin 3

21
- knockout mice who have had the K12 gene inactivated have a very fragile corneal
epithelium. Also Meesman's corneal dystrophy patients have mutations in K3 or K12
genes and they too have fragile epithelia. Showing the importance of the keratins for
maintaining cell integrity.
Specific Epithelial biochemistry/physiology
- high levels of acetylcholine, choline acetylase and cholinesterase in epi.
- also cornea has muscarinic receptors, i.e. receptors for acetylcholine
- why this cholinergic system exists and what is does no one really knows…suggested
role in pain transmission after injury, that it is involved in regulating transport process or
that it regulates cell proliferation and so promotes corneal wound healing.
- other epithelial tissue elsewhere in body also have high levels of acetylcholine and
associated enzymes but again a specific role has yet to be elucidated
- has enzyme systems for detoxification and drug metabolism
- e.g. catalase, glutathione peroxidase and superoxide dismutase scavenge superoxide free
radical) and H2O2 to provide protection from oxidative damage
Slide = pic of pump system
- Like all cells corneal epithelial cells possess a variety of transport systems for moving
ions in and out which maintains the appropriate conditions, such as pH, for optimal cell
performance.
We do not know all of the players or what their specific roles are.
- Things that we are certain of are that the over all effect of the systems are the transport
of sodium from the tears to the stroma and the transport of chloride in the reverse
direction
- sodium enters mainly through channels in the superficial epithelial cells then is
transported out in to the stroma by a ouabain-sensitive NaK ATPase in basal membrane
- with 3 sodium being transported out for 2 potassium coming in
- have an electrochemical gradient for sodium
- so to counter act this a sodium chloride co-transporter also located in the basal
membrane brings in Na and Cl
- the Cl then diffuse out of channels in apical membrane
- thought that the sympathetic nerves that innervate the epithelium may help to regulate
the chloride channels
- they release the neurotransmitter norepinephrine which acts on specific receptors on the
epithelial cell membrane resulting in an increase in intracellular cAMP which promotes
diffusion of chloride out of the channels and in to tears
22
- in addition to transport systems for sodium and chloride the epithelial cells also have a
sodium hydrogen exchanger and a lactate and hydrogen cotransporter.
- These help regulate intracellular pH, and remove lactate produced by anaerobic
metabolism which would otherwise cause the cells to swell.
- the movement of ions across the epithelial cells could promote osmotic transport of
water out of the stroma and in to the tear film… and so could potentially promote,
deturgescence, i.e. dehydration of swollen cornea although contribution of this to in vivo
situations is controversial and is suggested to be minimal
- The epithelial cells also have very high levels of the enzymes aldehyde dehydrogenase 3
and transketolase
- both of these enzymes are found in many other cell types
- ALDHs catalyse the oxidation of cellular aldehydes to carboxylic acids and are
involved in reactions such as the metabolism of neurotransmitters, and detoxification of
drugs
- TKT is an enzyme that participates in the pentose-phosphate pathway, which among
other things converts glucose in to ribose which is then used to make nucleotides for
making DNA and RNA
- in the cornea it has been suggested that ALDH3 through its detoxifying activities and
TKT through its metabolic effects protect the epithelial cells against lipid peroxidation
and free radical formation particularly that caused by UV irradiation.
- however in the cornea the concentrations of these proteins in the cells is to too high for
them simply to function as enzymes
- been suggested that they are "corneal crystallins"..ie. do the same job in the cornea as
crystallins do in the lens
- which is to contribute to refractive index and minimise light scatter within the cell
- so these "corneal crystallins" may help to maintain the transparency of the epithelial
cells
- but has yet to be definitively proven
- also recently suggested that ALDH3 helps regulate the cell cycle i.e. proliferation of
corneal epithelial cells….
OK couple of other characteristics of the epithelium…
- by comparison to many cells, corneal epi cells have relatively few organelles, which is
in keeping with maintaining corneal transparency
- also as progress through the different stages of differentiation can see decreases in
levels of organelles
- e.g. basal cells have the most mitochondria, wing cells have less and superficial cells
have even fewer
23
text epi turnover and XYZ (PP)
- as we have previously said the epithelium is a self renewing tissue
- cells in the basal layer divide, giving rise to daughter cells that differentiate in to wing
cells, then finally superficial cells which are terminally differentiated and are shed in to
the tear film
- this turnover of cells is very important as it ensures that the epithelial barrier is
maintained in good condition and it helps the cornea to resist infection
- since in the normal undamaged cornea the first site of attack by micro-organisms will be
the outer layers
- constant shedding of these layers prevents the spread of infection to underlying layers
- the cells of the basal layer proliferate
- been estimated that at any one time about 5% of cells in basal layer are undergoing
division
- to the best of our knowledge it takes approximately 7 days for basal cell in basal layer
having undergone its final round of cell division, to differentiate in to a wing cell, then a
superficial cell then to be sloughed off in to the tear film
- however in addition to mitosis in the basal layer the epithelium is maintained by
migration of new basal cells from limbus
- there are stem cells in limbus, which divide continuously but slowly to provide new
basal cells
- which migrate centripetally (i.e. towards the centre) on to the cornea at the rate of about
120um/week, that means that it takes several months for the cells to get from the limbus
to the central cornea
- once on the cornea the cells are believed to stay and proliferate in the basal layer for 1-2
weeks then start on their process of differentiation to become wing then superficial cells.
- this process of epithelial renewal was first proposed in 1983 by Thoft and Friend as
their X, Y Z hypothesis of corneal epithelial maintenance
- where X is the proliferation of basal cells, Y the migration of cells and Z the cell loss
from the surface
- so put simply to maintain a normal epithelial surface the sum of X the proliferation and
Y the migration must be equal to Z the loss of cells from the surface
Pic of schematic of limbal area
- the stem cells that give rise to the corneal cells have been found in basal epithelium of
the limbus
- as we said at the beginning the limbus is the zone between cornea and conj/sclera
- it is about 1mm wide
- and represents the region where the cornea gradually develops in to sclera and conj.
- at the limbus the epithelium becomes thicker, 10 or more cells thick and less regular
24
- also basal cells are smaller and less columnar than in the cornea
- the basement membrane starts to undulate
- the anterior limiting lamina is not present, it stops at the end of the cornea
- the stroma is continuous with corneal stroma but much more irregular, collagen fibers
are a variety of sizes and have different spacing
- also no descemets which again stops at the edge of the cornea (the ring that forms
around the cornea that corresponds to the edge of Descemets is called Schwalbe’s ring or
line)
- endothelium is continuous with corneal endo but lots of modifications because it is the
site of drainage of AH
- also have the appearance of blood vessels
text of stem cell characteristics & epi stem cell
- a stem cell is a cell that has a high capacity for self-renewal which lasts for life of the
individual
- all epithelial tissues have a set of stem cells as do the red and white blood cells
- In addition to having high proliferative capacity i.e. ability to divide repeatedly
stem cells also are characterised by having a long cell cycle and the capacity to undergo
asymmetric cells division
- in other words when they divide one of the daughter cells remains as a stem cell
whereas the other is a little more differentiated and is called a transient amplifying cell
- these transient amplifying cells have limited proliferative potential and are considered to
be the first step on the way to terminal differentiation
- different levels of stem cells exist classed according to how many cell types they may
differentiate in to. So embryonic stem cells are, totipotent, they can become any cell type,
hematipoetic stem cells are multipotent as they can be come one of several different types
of blood cells.
The limbal stem cells were initially suggested to be unipotent, i.e. they would only
differentiate in to corneal epithelial cells. However it has been shown in cell culture that
given the correct conditions it is possible to get corneal cells to become skin cells…so
further study of proliferation potential of limbal cells is needed.
- several lines of evidence support the hypothesis that the limbal basal cells are the stem
cells for the corneal epithelium
- the limbal basal cells have a long cell cycle time (i.e. slow rate of mitosis)
- they have a higher proliferative potential than central corneal epithelial cells
- if the limbus is surgically removed then healing of the corneal surface occurs by
migration of conjunctival cells on to the cornea rather than epithelial cells
- however if the limbus is transplanted back then healing of the corneal surface occurs by
regeneration of a corneal epithelium
- the limbal basal cells do not express the corneal epithelial specific keratin K3 K12 pair
indicating that they are less well differentiated than the corneal epithelial cells.
(suprabasal limbal epi cells do have K3/K12..ie are more differentiated)

25
- also variety of biochemical differences between limbal basal cells and corneal epithelial
basal cells, such as differential expression of proteins called cyclins that regulate the cell
cycle, and of protein kinase C and EGF receptor (more in limbal)
- believed that fewer than 10% of limbal basal cells are actually stem cells with the
remainder being transient amplifying cells…reasonable number is that that there are
probably a few 1000 of stem cells, vs millions of TAs
- so why are the stem cells in the limbus and not in the cornea itself
- the main reason is that in order to maintain the characteristics of a stem cell, the cells
have to have their own microenvironment or niche, otherwise they would just
differentiate in to TA cells
- the limbus can provide such a microenvironment
- if look closely at structure of the limbus find its is very undulating
- small pegs of stroma project upwards between the cells of the epithelium
- this arrangement of cells is called the Palisades of Vogt
- believed that the stem cells reside in the bottom of the crypts
- this both protects them from injury and also means that they are in close proximity to
the limbal vessels
- this puts the cells in an environment very different from the avascular cornea
- therefore very likely that factors carried in the blood are responsible, at least in part, for
maintaining the specific characteristics of the stem cells and that some regulate stem cell
differentiation in to TA cells
- one proposed regulatory factor which promotes stem cell differentiation is retinoic acid
- also the basal cells of the limbus are heavily pigmented which affords extra protection
to the limbal area from uv light
- also anchoring fibrils that extend through the stromal pegs and potentially may promote
the adherence of the stem cells, so preventing movement from correct environment
- so the limbus provides an appropriate environment for the stem cells to maintain their
stemness and most people accept that the stem cells for the corneal epithelium are housed
there
- so to re-cap on the life cycle of a corneal epithelial cell
pic of limbal location of stem cells
- to maintain the normal cornea
- stem cells in the limbus regularly divide to form a new stem cell and a transient
amplifying cell
- the transient amplifying cell slowly migrates in to the cornea, and so becomes a basal
cell of the corneal epithelium migration takes weeks to months
- once in the cornea the transient amplifying cell has the capacity to undergo several
rounds of cell division each giving rise to new basal cells that stay in the basal layer
26
- at its last round of cell division the transient amplifying cell/basal cell divides to give
two daughter cells which simultaneously differentiate to become wing cells which are
also referred to as post mitotic cells
- then ultimately they become the terminally differentiated superficial cells which die by
apoptosis and are sloughed off
pic alt stem cell paper
so having just told you that corneal epi stem cells are located in a niche in the limbus a
paper came out a couple of years ago that caused a bit of a stir
heres the title….which as you can see suggests that contrary to what I have just told you
that the stem cells are located across the cornea and not just at the limbus.
This results of this paper are still being debated but it seems that the general consensus
from the researchers who work specifically in the corneal stem cell field is that the
findings may apply to small mammals such as the mice but not to human.
This paper is on the intranet along with a review on corneal epithelial stem cells should
you want to read more.
- The epithelium consists mostly of epithelial cells
- but there are a few cells from the immune system, specifically called antigen presenting
cells
antigen presenting cells are cells which screen the local environment for the presence of
infecting organisms then if they find any they convey that information to the immune
system which is then activated and lots of cells enter the cornea to help get rid of the
infection.
HRT pic This is how they look by confocal microscopy….so this is a living patient, the image is
taken at the level of the basal epithelial cells, these bright cells are the antigen presenting
cells.
Only a few are found at the central cornea, many more are at the periphery. Also they
have different activation states, so those in the central cornea tend to be immature,
whereas those in the peripheral cornea are more mature, ready to respond immediately to
an invading pathogen.
- most of the antigen presenting cells are Langerhans cells…which specifically express a
protein called langerin
and there are some dendritic cells
27
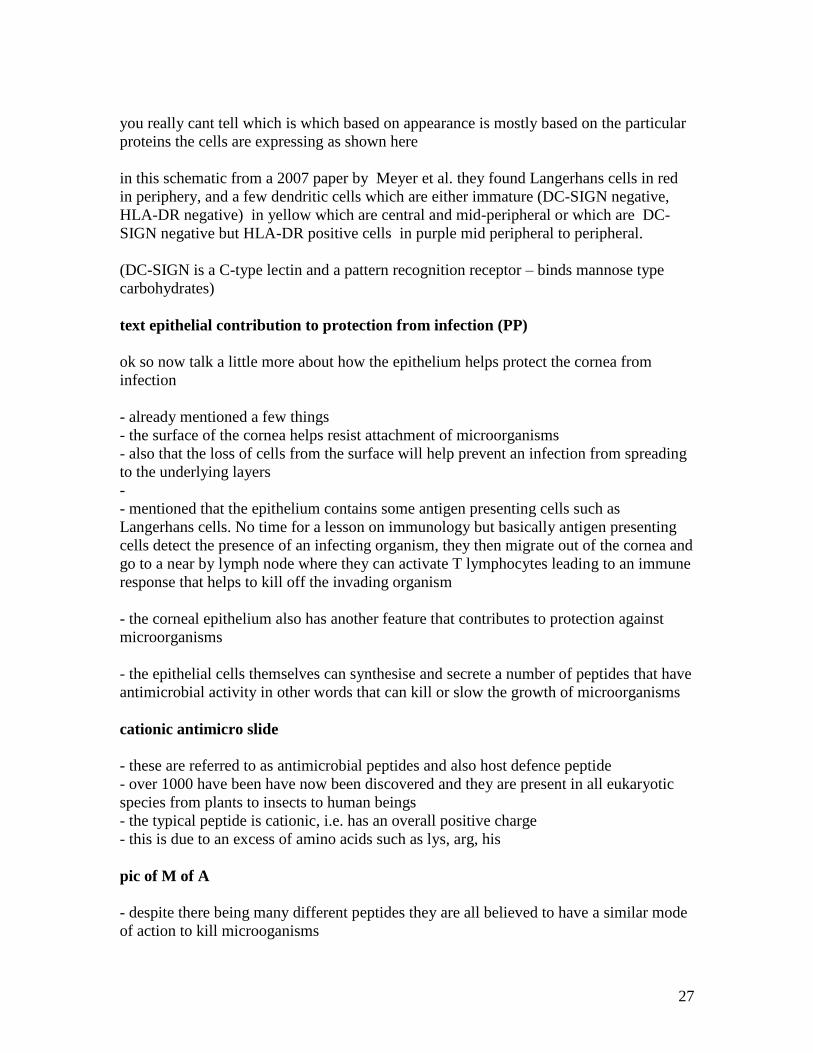
you really cant tell which is which based on appearance is mostly based on the particular
proteins the cells are expressing as shown here
in this schematic from a 2007 paper by Meyer et al. they found Langerhans cells in red
in periphery, and a few dendritic cells which are either immature (DC-SIGN negative,
HLA-DR negative) in yellow which are central and mid-peripheral or which are DC-
SIGN negative but HLA-DR positive cells in purple mid peripheral to peripheral.
(DC-SIGN is a C-type lectin and a pattern recognition receptor – binds mannose type
carbohydrates)
text epithelial contribution to protection from infection (PP)
ok so now talk a little more about how the epithelium helps protect the cornea from
infection
- already mentioned a few things
- the surface of the cornea helps resist attachment of microorganisms
- also that the loss of cells from the surface will help prevent an infection from spreading
to the underlying layers
-
- mentioned that the epithelium contains some antigen presenting cells such as
Langerhans cells. No time for a lesson on immunology but basically antigen presenting
cells detect the presence of an infecting organism, they then migrate out of the cornea and
go to a near by lymph node where they can activate T lymphocytes leading to an immune
response that helps to kill off the invading organism
- the corneal epithelium also has another feature that contributes to protection against
microorganisms
- the epithelial cells themselves can synthesise and secrete a number of peptides that have
antimicrobial activity in other words that can kill or slow the growth of microorganisms
cationic antimicro slide
- these are referred to as antimicrobial peptides and also host defence peptide
- over 1000 have been have now been discovered and they are present in all eukaryotic
species from plants to insects to human beings
- the typical peptide is cationic, i.e. has an overall positive charge
- this is due to an excess of amino acids such as lys, arg, his
pic of M of A
- despite there being many different peptides they are all believed to have a similar mode
of action to kill microoganisms
28
- the most popular model is that the positively charged peptide interacts with the
negatively charged microbial cell membrane
- several of the peptides come together to for a pore
- the presence of the pore allows ions and small molecules that should be inside the
organism out, and things that should be outside in
- this disturbs metabolism so protein and DNA synthesis stops, respiration stops and the
organism dies
- in some case so many pores form that this disturbs the osmotic balance and the
organism bursts
- also recently been shown that these peptides are also active against viruses. It appears
that they can prevent viruses from attaching to the surface of the cells they are trying to
infect.
CAPs produced by epi/at ocular surface
- so what antimicrobial peptides are produced by epithelial cells
- we and others have shown that corneal epithelial cells can make 3 human b-defensins,
that is hBD-1, -2, -3. Under normal circumstances it seems that the cells make 1 and 3
and that they also make 2 during inflammation or when challenged by certain bacteria
such as pseudomonas
- we have also detected a peptide from the cathelicidin family called LL-37
- there are others too.such as LEAP and no doubt others will be found
but defensins and cathelicidin are the most well studied
- together these peptides help protect the cornea from a wide range of organisms, for
example hBD-3 is particularly effective against staph aureus
- hBD-2 is very effective against pseudomonas
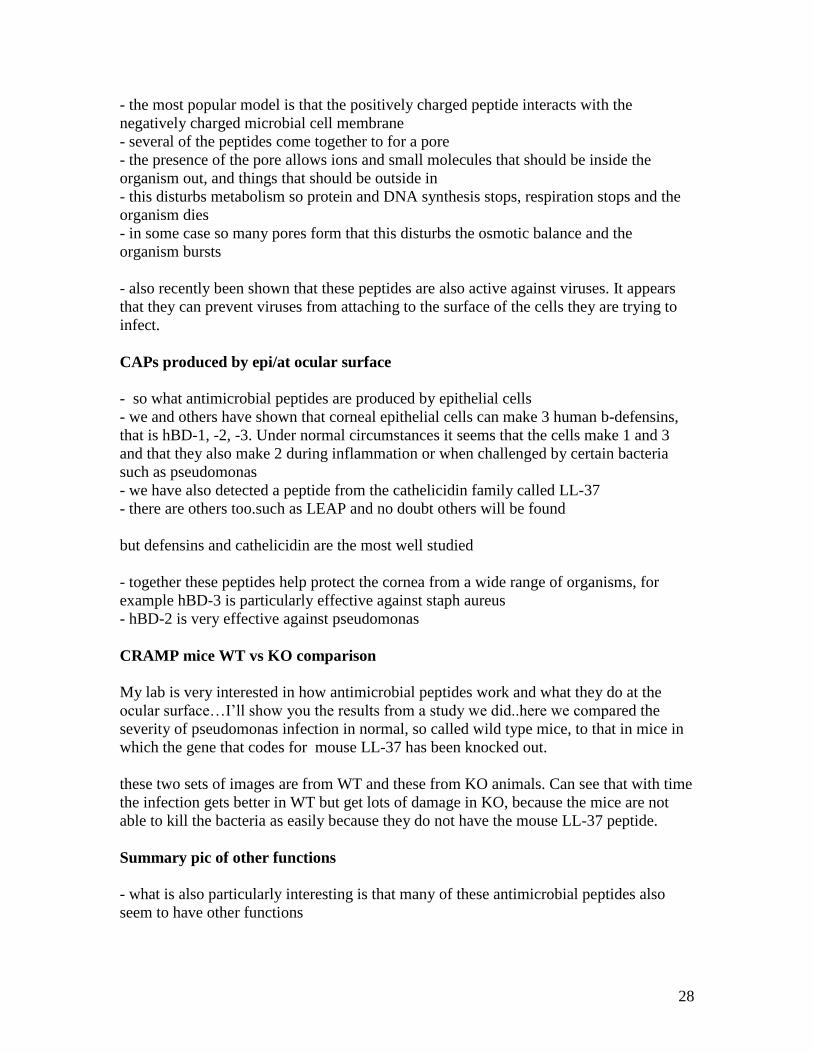
CRAMP mice WT vs KO comparison
My lab is very interested in how antimicrobial peptides work and what they do at the
ocular surface…I’ll show you the results from a study we did..here we compared the
severity of pseudomonas infection in normal, so called wild type mice, to that in mice in
which the gene that codes for mouse LL-37 has been knocked out.
these two sets of images are from WT and these from KO animals. Can see that with time
the infection gets better in WT but get lots of damage in KO, because the mice are not
able to kill the bacteria as easily because they do not have the mouse LL-37 peptide.
Summary pic of other functions
- what is also particularly interesting is that many of these antimicrobial peptides also
seem to have other functions

29
- and in particular it seems that they can serve as regulators of the immune response and
will attract other cells such as T-cells which can mediate killing of a specific organism to
a site of infection
- so not only do they protect the cornea but in addition they recruit backup just in case
they cant deal with the organism themselves.
- hope by this point all appreciate the importance of having an intact epithelium
- if the epithelium is damaged then no longer have smooth surface so have disruption of
optical function also have lost barrier so have some degree of oedema and have exposed
underlying stroma predisposing the cornea to infection
- in order to restore all of these functions it is essential that the epithelium can be rapidly
repaired after an injury
text of wound healing
- this brings us to the subject of corneal epithelial wound healing
- healing of a corneal epithelial wound such as that created by scraping off the full
thickness of the epithelium in the central part of the cornea can be divided in to two
phases
- a lag phase
- and a healing phase
- in the few hours immediately after a corneal epithelial wound not much seems to
happen
- in fact wound may get larger due to sloughing off of dead cells
- these first few hours are called the lag phase
- during this time the intact cells around the wounded area are actually very busy gearing
up metabolism and intracellular pathways
- also during the lag phase neutrophils arrive at the injured area, most carried in the tear
film and attracted by cytokines (IL-8) produced by dying/healthy cells, to phagocytose
any debris
- also fibronectin, again present in the tear film is deposited on the exposed stromal
surface
- so towards end of the lag phase, which lasts about 6 hours, can actually see visible
changes in the arrangement of cells
- basal cells lose their columnar appearance and start to flatten out such that the
epithelium closest to the injured area is only one cell thick
- these changes are achieved by rearrangement of the actin in the cytoskeleton of the cells
30
- the flattened single layer of cells is called the leading edge
- look at the cells under a microscope can see that they have narrow projections, these are
called filopodia (involves fimbrin bundling protein) and thicker projections which are
called lamellipodia (filamin gel forming)which project out on to the wound surface
- again these structures are formed by re-arrangement of actin filaments
- also been noted that hemidesmosomes disappear from the first 50-100um or so back
from wound edge
- and that their numbers are significantly reduced in the 200um further back
- this is some work published by MA Stepp..a corneal researcher based in Washington
DC
- this was a study where they specifically stained rat corneal epithelium before and after
wounding to look at the distribution of components of the hemidesmosome
- panel A - here is a section through a normal rat cornea that has been stained with an
antibody that specifically recognises the b4 subunit of the integrin found in the
hemidesmosome
- can see that staining, the bright parts, is pretty much restricted to basal surface of the
basal cells as you would expect
- this is staining 4 hours after wounding
- here is the leading edge of the wound
- now can see rather than forming nice line, staining is very diffuse indicating that the
hemidesmosomes have been disassembled and the components have been redistributed
around the cell, no longer concentrated at basal surface
- ok that was the latent phase which basically prepares the ground for the next phase, the
healing phase
- this involves three processes
- cell migration
- cell proliferation
- and cell adhesion
- during this phase the cells migrate towards each other until the whole area of the defect
is covered with at least a single layer of cells
- cell migration is made possible by the fact that the cells closest to the wound have lost
their hemidesmosomes so are no longer firmly attached to the underlying layers
- however it is important that these cells maintain some sort of contact with the
underlying layers other wise they would simply be swept away by blinking
- so during wound healing the cells form what are known as focal contacts which allow
them to adhere loosely to the surface but also to move across it.
pic of focal contact
- this is an artists impression of a focal contact
31
- in this adhesion structure components of the cell cytoskeleton interact directly with the
cytoplasmic domain of an integrin
- in turn the extracellular domain of the integrin interacts with an extracellular matrix
protein
- so an actin filament binds to the protein vinculin, which in turn binds to talin and this
protein directly interacts with the integrin
- during corneal wound healing the major integrin involved is a5b1
- and this interacts directly with the fibronectin that was deposited on the exposed corneal
surface by the tear film
- actual migration is also made possible by the redistribution of actin filaments
- and the large stores of glycogen that can be broken down in to glucose and utilised to
make ATP to provide energy for the migratory process
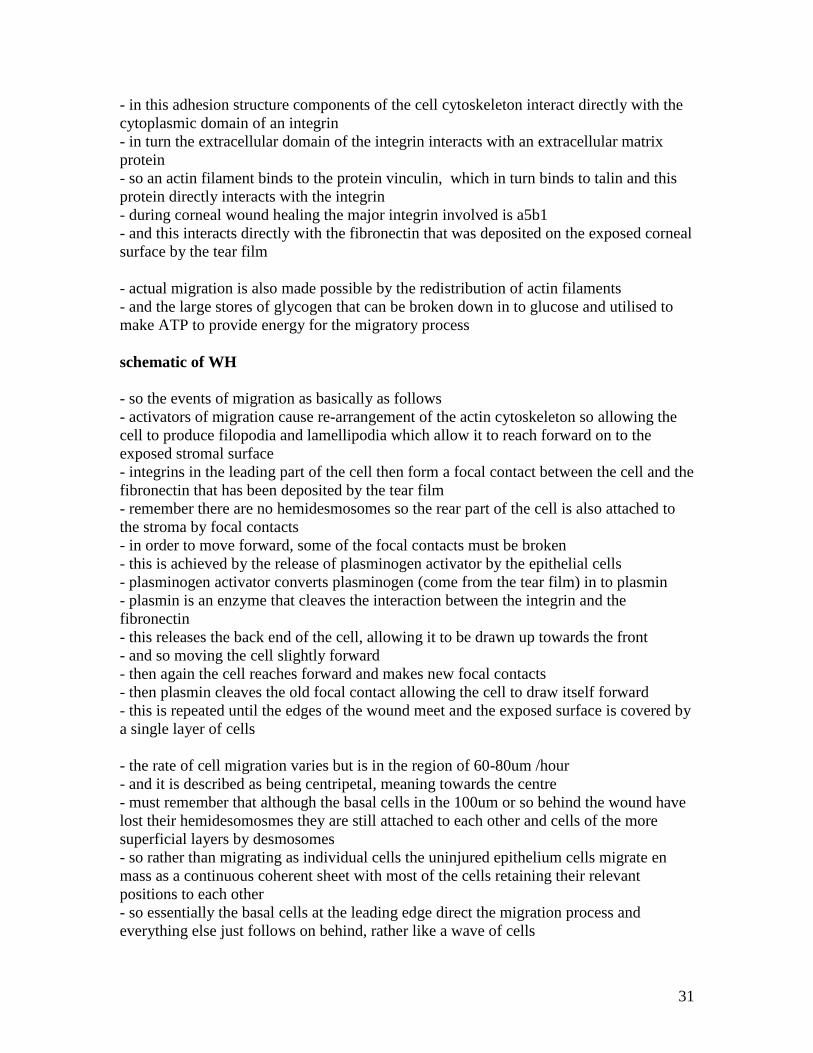
schematic of WH
- so the events of migration as basically as follows
- activators of migration cause re-arrangement of the actin cytoskeleton so allowing the
cell to produce filopodia and lamellipodia which allow it to reach forward on to the
exposed stromal surface
- integrins in the leading part of the cell then form a focal contact between the cell and the
fibronectin that has been deposited by the tear film
- remember there are no hemidesmosomes so the rear part of the cell is also attached to
the stroma by focal contacts
- in order to move forward, some of the focal contacts must be broken
- this is achieved by the release of plasminogen activator by the epithelial cells
- plasminogen activator converts plasminogen (come from the tear film) in to plasmin
- plasmin is an enzyme that cleaves the interaction between the integrin and the
fibronectin
- this releases the back end of the cell, allowing it to be drawn up towards the front
- and so moving the cell slightly forward
- then again the cell reaches forward and makes new focal contacts
- then plasmin cleaves the old focal contact allowing the cell to draw itself forward
- this is repeated until the edges of the wound meet and the exposed surface is covered by
a single layer of cells
- the rate of cell migration varies but is in the region of 60-80um /hour
- and it is described as being centripetal, meaning towards the centre
- must remember that although the basal cells in the 100um or so behind the wound have
lost their hemidesomosmes they are still attached to each other and cells of the more
superficial layers by desmosomes
- so rather than migrating as individual cells the uninjured epithelium cells migrate en
mass as a continuous coherent sheet with most of the cells retaining their relevant
positions to each other
- so essentially the basal cells at the leading edge direct the migration process and
everything else just follows on behind, rather like a wave of cells
32
- obviously with the loss of cells due to injury then there will not be sufficient existing
basal cells to cover the wounded area so even as migration is occurring at the edges of the
wound, basal cells a few hundred um back from the leading edge are dividing to provide
new basal cells
- so these are then available to join the ranks of cells migrating to fill the wounded area
- also to compensate for the basal cells having to divide and thus come closer to their
finite capacity for division, the stem cells in the limbus also start to divide
- division of stem cells is particularly prominent if the wounded area is very large
- once the cells at the leading edge have met and thus the defect has been covered with a
single layer of cells those cell too divide so that the normal multilayered structure of the
epithelium can be reformed and the barrier function of the epithelium restored
- while basal cells are busy proliferating to restore the epithelial structure they also must
reform their firm attachments to the underlying layers..in other words they must re-form
the hemidesmosomes, otherwise the newly regenerated epithelium which is only loosely
attached to the surface is in danger of being swept away
- how fast the adhesion complexes re-form depends on whether or not the basement
membrane of the epithelial cells was damaged
- if the basement membrane is not damaged then it is simply a matter of the cell
redistributing the hemidesmosomal components to appropriate places on the plasma
membrane
- and these components then take up their normal interaction, so the a6b4 integrin
interacts with laminin, while the anchoring filaments and fibrils which have been left
intact in the basement membrane simply re-associate
- so in this case it only takes a matter of days for the epithelium to be firmly attached to
the underlying layers
- if however the basement membrane is damaged then several weeks may pass before the
adhesion complexes reform as new basement membrane must be layed down and new
anchoring fibrils produced
- if the injury includes the limbus and destroys the stem cells then the wound will be
resurfaced by conjunctival cells that migrate on to the cornea
- providing vascularisation does not occur then the cells undergo transdifferentiation to
become more corneal epithelial like than conjunctival like
- never become true corneal epithelium and do not express classic corneal K3/K12 pair
- if vascularisation does occur then cells remain as conjunctival cells so a stem cell
transplant becomes necessary.
- so what do we know about how the events that occur during wound healing are
regulated
33
- well the important processes in wound healing are migration, proliferation and we know
that cell behaviours such as those are regulate by peptide growth factors and cytokines
which activate intracellular signalling pathways inside the cell
- know from personal experience that the cornea itself can produce all the chemical
regulatory factors it needs to cause resurfacing of an epithelial defect
- in my lab we regularly take human, monkey or bovine corneas scrape off the epithelium
leaving just ring of intact cells around the limbus then put the whole cornea in to culture
- we add only a few drops of tissue culture media every few hours to keep the surface
moist
- the tissue culture media contains only glucose, amino acids and salts,
- within 48 to 72 hours of putting the human/monkey (5-6 days for bovine, cos larger) the
wounded area will be resurfaced with new epithelial cells
- thats not to say that factors from the tear film or from corneal nerves do not play a role
in influencing corneal epithelial wound healing in vivo
- through a variety of mainly in vitro studies performed in labs across the world we are
slowly beginning to identify factors that have the potential to regulate corneal epithelial
wound healing in vivo
as can see from this summary picture many of them come from tear film, some from epi
and some from keratocytes and nerves
also evidence that some helpful factors come from neutrophils and also platelets that
invaded the cornea after injury, as healing is delayed if this influx of cells is prohibited.
likely to find no single master factor involved in vivo, but several can have same function
so even if one removed another is there to take over….this would make sense considering
how dependent vision is on the existence of a smooth, intact epithelial surface
summarize functions
- so to summarise the epithelium contributes to both refractive and protective function of
the cornea
- by interacting with the tear film it helps provide a smooth surface for the refraction of
light which also resists bacterial attachment
- junctions between the cells contribute to the formation of a barrier to prevent flow of
water from tear film in to stroma which otherwise would cause stromal edema and loss of
transparency
- the barrier also prevents passage of noxious substances in to underlying layers and is
resistant to abrasion

34
-the epithelium also produces antimicrobial peptides which help eliminate
microorganisms
- the constant renewal of the epithelium ensures all cells in good condition and able to
maintain adequate interaction with tear film and helps remove any invading organisms
- also the renewal process ensures that following an injury defects are repaired rapidly
this restores the barrier and helps prevent infection