grampian primary care atrial fibrillation guidelines 2010
TRANSCRIPT
1-18
Grampian Primary Care Atrial Fibrillation Guidelines 2010
Grampian Primary
Care Atrial Fibrillation
Guidelines 2010
2-18
Grampian Primary Care Atrial Fibrillation Guidelines 2010
Contents
A INTRODUCTION …………………………………………………………............................................................ 3
B INVESTIGATIONS USED IN ATRIAL FIBRILLATION …………………………………………………………………. 4
C CLASSIFICATION OF AF ; The 3 P’s …………………………………………………………………………………… 4
D TREATMENT OF ATRIAL FIBRILLATION ………………………………………………………………………………….
1. MANAGING THE HEART RATE + / OR RHYTHM ……………………………………………………….
(a) Rate Control ……………………………………………………………………………………………………..
(b) Rhythm Control …………………………………………………………………………………………………
2. REDUCING THE THROMBOEMBOLIC RISK ……………………………………………………………….
3. ESTIMATING THE BLEEDING RISK …………………………………….........…………………………….
4. IDENTIFYING AND TREATING THE UNDERLYING CAUSE…………………………………………..
5
5
6
7
8
10
11
E SUMMARY AND TABLES ……………………………………………………………………………………………….. . 12

3-18
Grampian Primary Care Atrial Fibrillation Guidelines 2010
4-18
Grampian Primary Care Atrial Fibrillation Guidelines 2010
A. INTRODUCTION
Atrial Fibrillation (AF) represents an epidemic of a disease which causes strokes, with a current prevalence of 1.2% of the total population, rising to 4% in the over 65’s, with 10% or more of the over 80 year old population being affected.
The vast majority of patients with Atrial Fibrillation can be managed within Primary Care.
Atrial Fibrillation can lead to considerable morbidity and mortality and cause:
Breathlessness / Heart Failure
Chest Pains / Angina
Palpitations
Dizziness / Syncope
Impaired cognitive Function (repetitive micro emboli and Alzheimer’s Disease)
Tiredness
Stroke / TIA / Systemic Embolism
.
Treatment is aimed at
1. Managing the: a) heart rate (and / or) b) rhythm
2. Reducing the thrombo-embolic risk
3. Identifying and managing the underlying cause
5-18
Grampian Primary Care Atrial Fibrillation Guidelines 2010
B. INVESTIGATIONS USED IN ATRIAL FIBRILLATION
The Heart Charity: Arrhythmia Alliance recommends pulse screening for possible AF. (If pulse is found to be irregular, an ECG should be performed)
The possible aetiological factors for the Atrial Fibrillation should be considered in all
patients.
The following investigations should be performed in Primary Care in all patients with Atrial
Fibrillation:
ECG
Blood tests : FBC TFT’s U+E’s LFT’s (INR if anticoagulation being considered)
ECHOCARDIOGRAM (Direct Access ECHO if patient not being referred to
cardiologist:- try to control the ventricular rate at least before referral as LV
dysfunction may be exaggerated at rapid rates)
If patients are suspected of having Paroxysmal Atrial Fibrillation (PAF) either a Holter
Monitor or Event Recorder (if attacks > 24-48 hours apart) should be performed. A 12 lead
ECG during episode of symptoms would be even better.
C. CLASSIFICATION OF AF : The 3 P’s
TYPE DESCRIPTION TREATMENT
First attack No previous AF None (but should still
have echo performed and
thromboembolic risk assessed)
Self limiting

6-18
Grampian Primary Care Atrial Fibrillation Guidelines 2010
RECURRENT AF
Paroxysmal Spontaneous termination Rate or Rhythm
within 1-2 days (seldom control
attacks > 7 days)
Persistent Non-self terminating Rate or Rhythm
Intervention needed to control
stop AF
Permanent AF Dominant rhythm Rate control
Conversion not needed
or not attempted
D. TREATMENT OF ATRIAL FIBRILLATION
After managing any underlying cause (eg. thyrotoxicosis, infection) decisions need to be
made regarding:
1. MANAGING THE HEART RATE + / 0R RHYTHM
Ideally all patients would be restored to sinus rhythm but in practice this is difficult to
maintain and therefore a rate approach is usually recommended with only a minority of
patients requiring cardiology (or GPwSI) referral for consideration of cardio-version for
rhythm control.
QIS (Quality Improvement Scotland) recommend that rate versus rhythm options should be
discussed with all patients and recorded in their medical records.

7-18
Grampian Primary Care Atrial Fibrillation Guidelines 2010
a) RATE CONTROL
The following factors would guide one more towards RATE CONTROL:
Age > 65 years
Long duration of AF > 1 year
Contraindication to anti-arryhthmics
Severe structural heart disease
Significant left atrial enlargement
Traditionally the aim of rate control was to reduce the heart rate to 60 – 80 bpm at rest
(and 90 – 115 bpm during moderate exercise), although recent research suggests that
this may not always be necessary, providing that patients remain asymptomatic if their
ventricular rate (on ECG, not pulse) is less than 110 bpm at rest. This approach of LENIENT
rate control only applies to ENTIRELY ASYMPTOMATIC patients.
Should they become symptomatic, re-evaluation of LV Function by ECHO and stricter rate
control should then be achieved.
The following drugs are used to control heart rate
(None may be required if rate well controlled)
β-Blockers (eg. Atenolol, Bisporolol) ↓ resting and exercise HR
Rate- Limiting Calcium Channel Blocker :
(non-hydropyridine) ↓ resting and exercise HR
eg. Diltiazem or Verapamil Must NOT be used along with β-Blocker unless pacemaker
implanted or under specialist advice.
Digoxin weak A-V blocker, NOT first-line
may be used as adjuvant therapy
Others (eg. Amiodarone) Where conventional drugs unsuccessful
Amiodarone is rarely used to control the ventricular
rate and should only be commenced by a SPECIALIST
because of its potential side-effects.

8-18
Grampian Primary Care Atrial Fibrillation Guidelines 2010
OTHER TREATMENTS:
Other treatments which might be considered by a specialist include: pacemaker insertion,
hybrid therapy (pacemaker plus drugs), catheter ablation (A-V junction: ablate and pace)
b) RHYTHM CONTROL
The following factors would guide one more towards RHYTHM CONTROL:
Symptomatic patients (despite adequate rate control)
Inability to adequately control rate (with associated symptoms)
Younger patients
Presenting first time with absence of major structural heart disease
Secondary to treated or corrected precipitant
Congestive Heart Failure
Patients being considered for RHYTHM CONTROL require FULL anti-coagulation for 3 to 4
weeks prior to cardio-version (whether electrical or pharmacological) unless the onset AF
duration is less than 48 hours. Anti-coagulation is required for at least 4 weeks after
successful cardio-version to sinus rhythm.
A high proportion of patients who are cardio-verted from AF to sinus rhythm will relapse
back into AF and may require further cardio-version with concomitant use of anti-
arrhythmic drugs if not used previously.
UNSUITABLE FOR CARDIO-VERSION:
Contra-indication to anti-coagulation
Structural Heart Disease (mitral stenosis, large left atrium > 5.5cm)
History of multiple failed attempts at cardio-version +/or relapses (even with
concomitant use of anti-arryhthmics)
Ongoing but reversible cause of AF (eg. Untreated thyrotoxicosis)
9-18
Grampian Primary Care Atrial Fibrillation Guidelines 2010
PAROXYSMAL ATRIAL FIBRILLATION:
Anti-arrhythmic drugs for RHYTHM control should be tried prior to consideration of
ablation.
Start off with a beta blocker then if ineffective refer to secondary care for consideration of a
class 1c drug eg Flecainide, possibly Sotalol, Dronedarone or Amiodarone.
Ablation may be performed by catheter (or rarely surgical) ablation procedure and can be
particularly useful in troublesome, drug refractory Paroxysmal (or occasionally persistent)
Atrial Fibrillation.
2. REDUCING THE THROMBOEMBOLIC RISK
Epidemiological studies consistently point to AF being the cause of between 15% and 20% of all thrombo-embolic strokes. There is also strong evidence suggesting that AF is associated with some of the worst
strokes in terms of subsequent morbidity and mortality.
Certain co-morbid factors have been reliably identified as particular high-risk factors for
stroke in patients with Atrial Fibrillation. Stroke risk in AF is not homogenous however, and
depends on an individual patient’s profile of stroke risk co-factors: many patients face an
annual stroke risk of between 4% up to 35%.
Because this risk of stroke / TIA or systemic embolism increases when certain risk factors are
present, it is recommended that all patients have a risk assessment as to whether they
require anti-coagulation.
Patients with valvular heart disease (moderate or severe valvular stenosis or regurgitation)
require warfarin therapy (unless contraindicated) regardless of additional risk factors.
Patients with non-valvular AF should have a CHA2DS2-VASc (or similar) risk assessment
performed (a QIS standard).
10-18
Grampian Primary Care Atrial Fibrillation Guidelines 2010
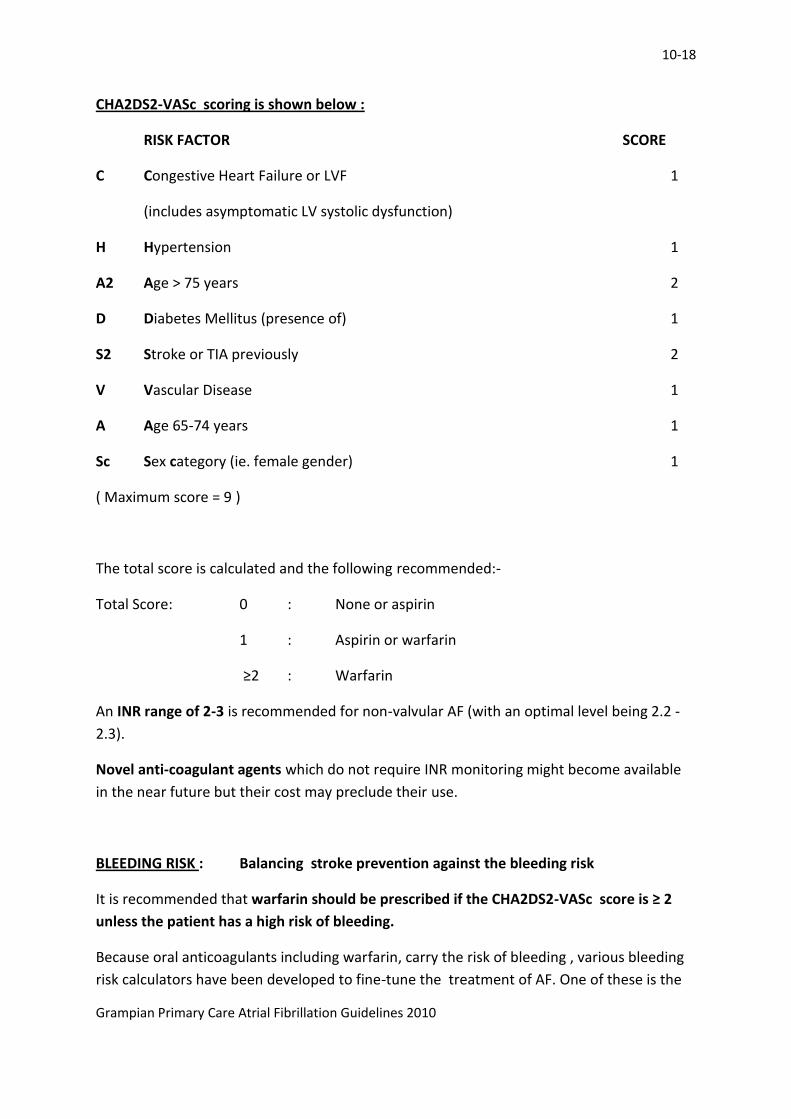
CHA2DS2-VASc scoring is shown below :
RISK FACTOR SCORE
C Congestive Heart Failure or LVF 1
(includes asymptomatic LV systolic dysfunction)
H Hypertension 1
A2 Age > 75 years 2
D Diabetes Mellitus (presence of) 1
S2 Stroke or TIA previously 2
V Vascular Disease 1
A Age 65-74 years 1
Sc Sex category (ie. female gender) 1
( Maximum score = 9 )
The total score is calculated and the following recommended:-
Total Score: 0 : None or aspirin
1 : Aspirin or warfarin
≥2 : Warfarin
An INR range of 2-3 is recommended for non-valvular AF (with an optimal level being 2.2 -
2.3).
Novel anti-coagulant agents which do not require INR monitoring might become available
in the near future but their cost may preclude their use.
BLEEDING RISK : Balancing stroke prevention against the bleeding risk
It is recommended that warfarin should be prescribed if the CHA2DS2-VASc score is ≥ 2
unless the patient has a high risk of bleeding.
Because oral anticoagulants including warfarin, carry the risk of bleeding , various bleeding
risk calculators have been developed to fine-tune the treatment of AF. One of these is the
11-18
Grampian Primary Care Atrial Fibrillation Guidelines 2010
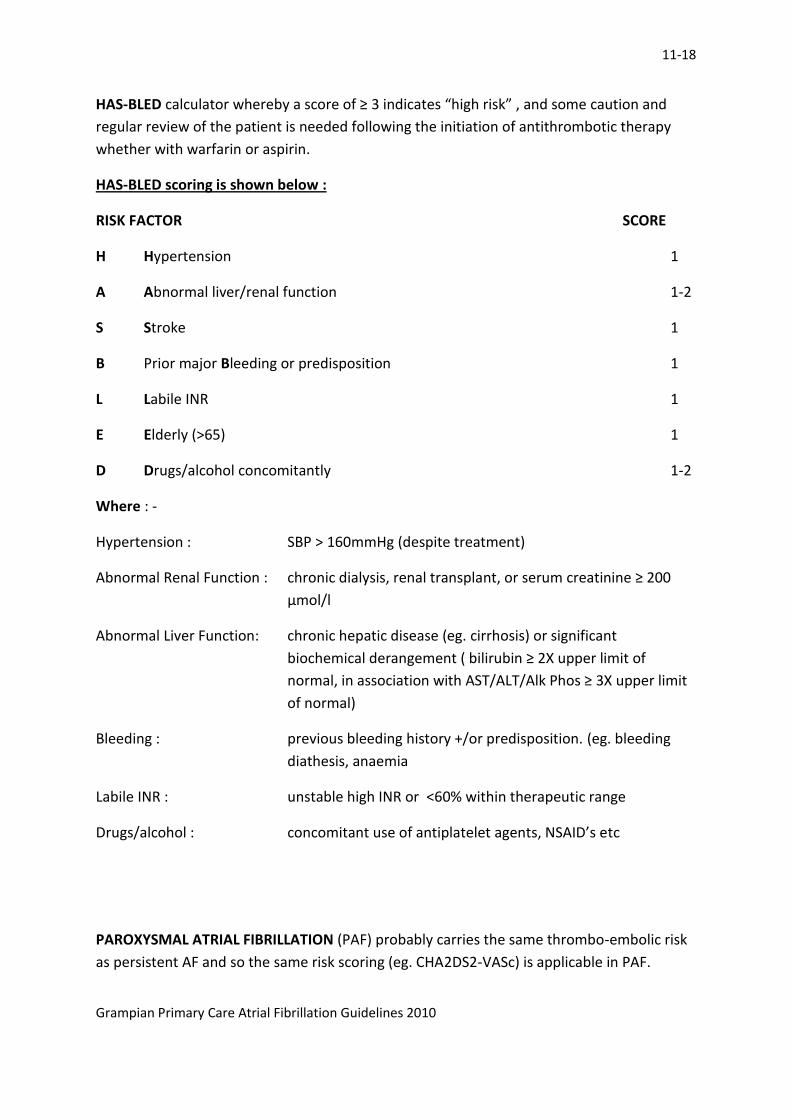
HAS-BLED calculator whereby a score of ≥ 3 indicates “high risk” , and some caution and
regular review of the patient is needed following the initiation of antithrombotic therapy
whether with warfarin or aspirin.
HAS-BLED scoring is shown below :
RISK FACTOR SCORE
H Hypertension 1
A Abnormal liver/renal function 1-2
S Stroke 1
B Prior major Bleeding or predisposition 1
L Labile INR 1
E Elderly (>65) 1
D Drugs/alcohol concomitantly 1-2
Where : -
Hypertension : SBP > 160mmHg (despite treatment)
Abnormal Renal Function : chronic dialysis, renal transplant, or serum creatinine ≥ 200
µmol/l
Abnormal Liver Function: chronic hepatic disease (eg. cirrhosis) or significant
biochemical derangement ( bilirubin ≥ 2X upper limit of
normal, in association with AST/ALT/Alk Phos ≥ 3X upper limit
of normal)
Bleeding : previous bleeding history +/or predisposition. (eg. bleeding
diathesis, anaemia
Labile INR : unstable high INR or <60% within therapeutic range
Drugs/alcohol : concomitant use of antiplatelet agents, NSAID’s etc
PAROXYSMAL ATRIAL FIBRILLATION (PAF) probably carries the same thrombo-embolic risk
as persistent AF and so the same risk scoring (eg. CHA2DS2-VASc) is applicable in PAF.
12-18
Grampian Primary Care Atrial Fibrillation Guidelines 2010
Performing a DCCV does not reduce future thromboembolic risk even if apparently
successful in restoring long-term SR. Indication for warfarin will still be based on overall
thromboembolic risk. (ie cardioversion does not remove the need for anticoagulation long-
term)
3. IDENTIFYING AND TREATING THE UNDERLYING CAUSE
The causes of the Atrial Fibrillation (eg. Hypertension, Ischaemic Heart Disease, Heart
Failure, Valvular heart disease, thyrotoxicosis, etc) should always be considered and
addressed where appropriate.
E. SUMMARY
AF is a common condition and can largely be managed in primary care. When certain clinical
circumstances prevail (eg. younger patients, haemodynamically challenged, heart failure,
refractory symptoms) secondary referral should be considered for possible cardio-version,
advice re potent antiarrhythmic drug treatment or interventional EP procedures.

13-18
Grampian Primary Care Atrial Fibrillation Guidelines 2010
SUMMARY AND TABLES
TYPE DESCRIPTION TREATMENT
First Attack Self limiting
No previous AF
None
RECURRENT AF
Paroxysmal Spontaneous termination
within 1-2 days ( seldom
attacks > 7 days )
Rate or Rhythm
control
Persistent Spontaneous termination
within 1-2 days ( seldom attacks
> 7 days )
Rate or Rhythm
control
Permanent AF Dominant rhythm Conversion not neededor not attempted
Rate control
THE 3 P CLASSIFICATION OF ATRIAL
FIBRILLATION

14-18
Grampian Primary Care Atrial Fibrillation Guidelines 2010
Confirmed diagnosis of AF
Paroxysmal AF Persistent AF Permanent AF
Rhythm
control
Remains symptomatic * Rate
controlFailure of rhythm control
or
* The vast majority of patients will be managed by rate control, with or without anticoagulation
depending upon their RISK
15-18
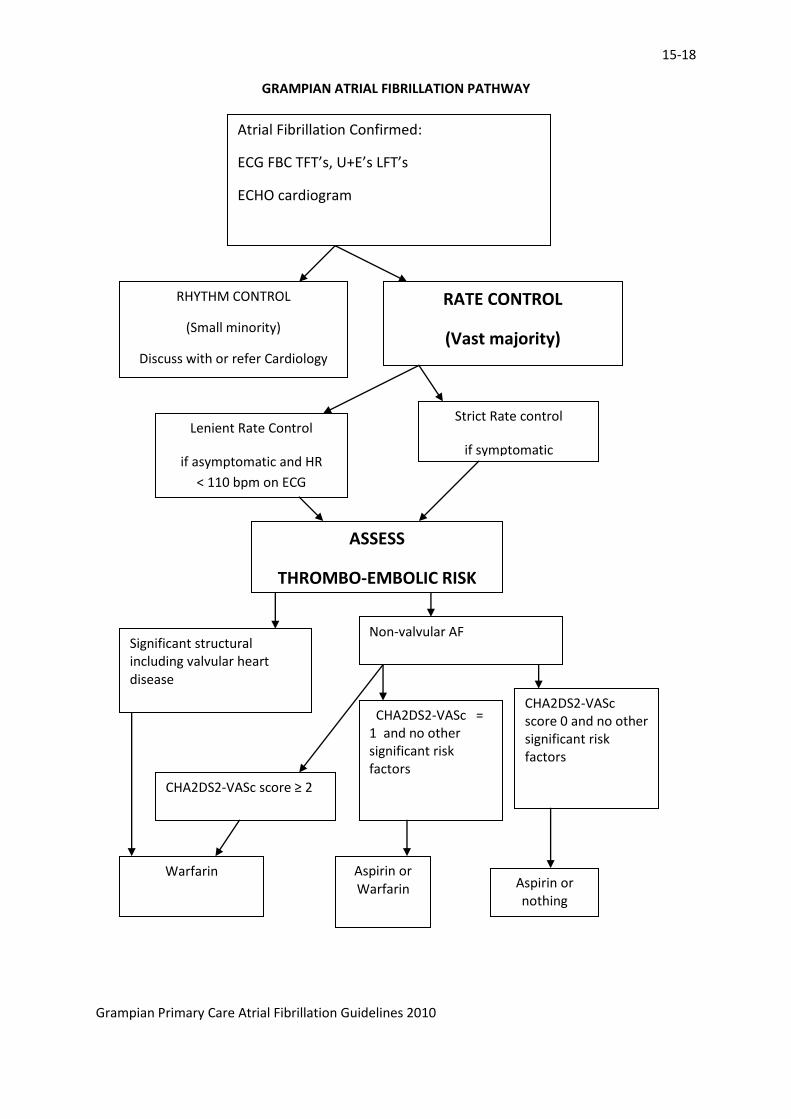
GRAMPIAN ATRIAL FIBRILLATION PATHWAY
Grampian Primary Care Atrial Fibrillation Guidelines 2010
Atrial Fibrillation Confirmed:
ECG FBC TFT’s, U+E’s LFT’s
ECHO cardiogram
RHYTHM CONTROL
(Small minority)
Discuss with or refer Cardiology
RATE CONTROL
(Vast majority)
Lenient Rate Control
if asymptomatic and HR
< 110 bpm on ECG
Strict Rate control
if symptomatic
ASSESS
THROMBO-EMBOLIC RISK
Significant structural including valvular heart disease
Non-valvular AF
CHA2DS2-VASc score ≥ 2
CHA2DS2-VASc = 1 and no other significant risk factors
CHA2DS2-VASc score 0 and no other significant risk factors
Warfarin Aspirin or Warfarin Aspirin or
nothing
16-18
GRAMPIAN ATRIAL FIBRILLATION PATHWAY
Grampian Primary Care Atrial Fibrillation Guidelines 2010
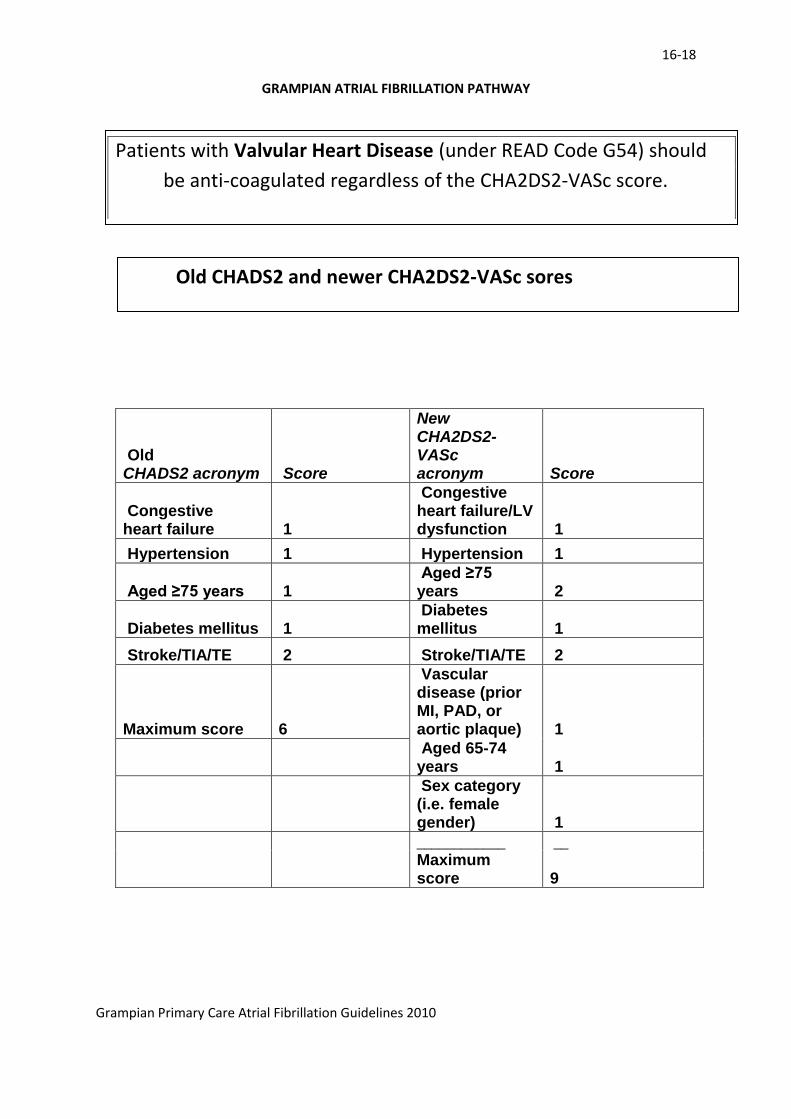
Old CHADS2 acronym Score
New CHA2DS2-VASc acronym Score
Congestive heart failure 1
Congestive heart failure/LV dysfunction 1
Hypertension 1 Hypertension 1
Aged ≥75 years 1 Aged ≥75 years 2
Diabetes mellitus 1 Diabetes mellitus 1
Stroke/TIA/TE 2 Stroke/TIA/TE 2
Maximum score 6
Vascular disease (prior MI, PAD, or aortic plaque) 1
Aged 65-74 years 1
Sex category (i.e. female gender) 1
____________ __
Maximum score 9
Patients with Valvular Heart Disease (under READ Code G54) should
be anti-coagulated regardless of the CHA2DS2-VASc score.
New CHA2DS2-VASc and older CHADS2 scores Old CHADS2 and newer CHA2DS2-VASc sores
17-18
GRAMPIAN ATRIAL FIBRILLATION PATHWAY
Grampian Primary Care Atrial Fibrillation Guidelines 2010
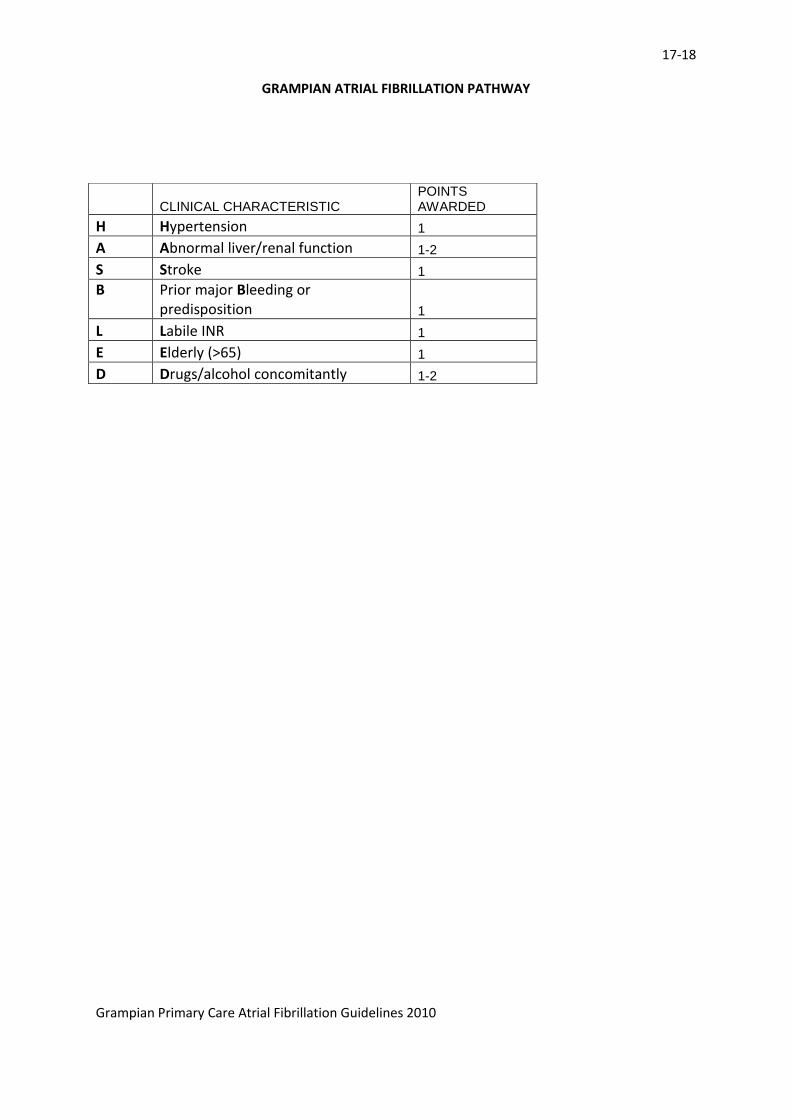
CLINICAL CHARACTERISTIC POINTS AWARDED
H Hypertension 1
A Abnormal liver/renal function 1-2
S Stroke 1
B Prior major Bleeding or predisposition 1
L Labile INR 1
E Elderly (>65) 1
D Drugs/alcohol concomitantly 1-2
18-18
GRAMPIAN ATRIAL FIBRILLATION PATHWAY
Grampian Primary Care Atrial Fibrillation Guidelines 2010
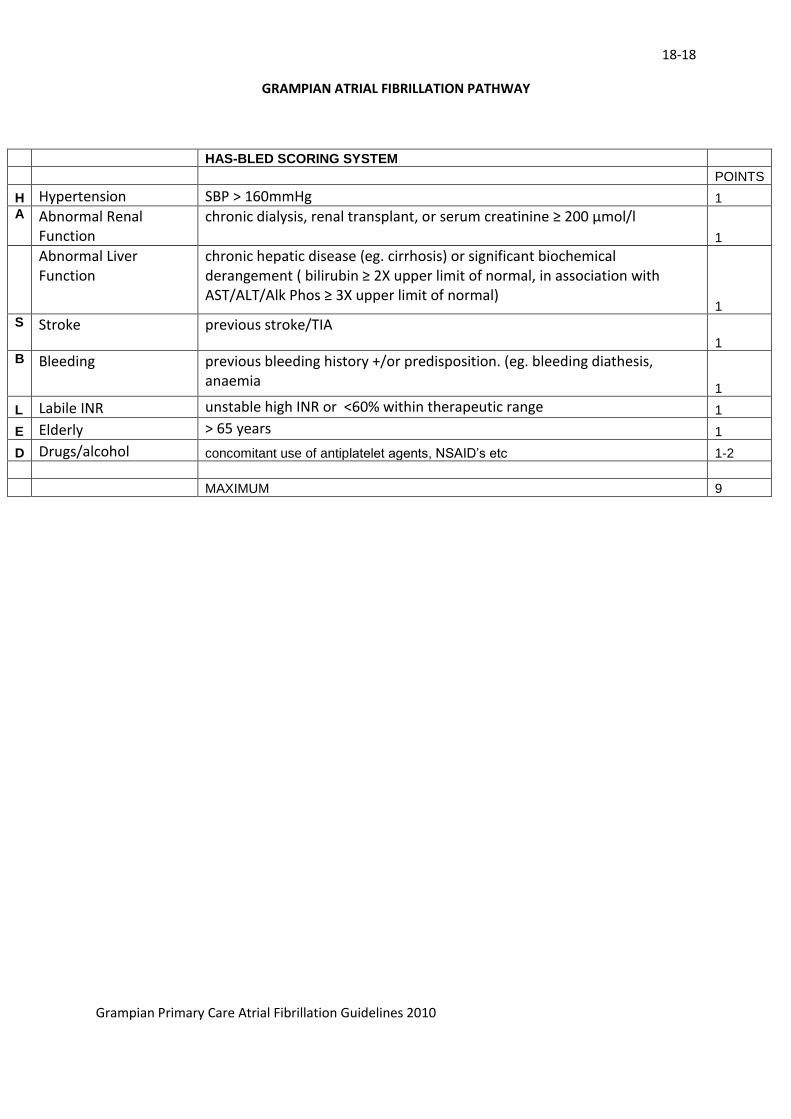
HAS-BLED SCORING SYSTEM
POINTS
H Hypertension SBP > 160mmHg 1
A Abnormal Renal Function
chronic dialysis, renal transplant, or serum creatinine ≥ 200 µmol/l
1
Abnormal Liver Function
chronic hepatic disease (eg. cirrhosis) or significant biochemical derangement ( bilirubin ≥ 2X upper limit of normal, in association with AST/ALT/Alk Phos ≥ 3X upper limit of normal)
1
S Stroke previous stroke/TIA 1
B Bleeding previous bleeding history +/or predisposition. (eg. bleeding diathesis, anaemia
1
L Labile INR unstable high INR or <60% within therapeutic range 1
E Elderly > 65 years 1
D Drugs/alcohol concomitant use of antiplatelet agents, NSAID’s etc 1-2
MAXIMUM 9