graphical methods for turning data into information martin utley clinical operational research unit...
Post on 21-Dec-2015
217 views
TRANSCRIPT

Graphical methods for turning data into information
Martin Utley
Clinical Operational Research Unit (CORU)University College London
www.ucl.ac.uk/operational-research

Monitoring outcomes to improve outcomes
Care process
Data
Information system
Analysis of data
Feedback
Need to get every step right

Care process
Data
Information system
Analysis of data
Feedback
Steps discussed in this talk

Case study 1: monitoring outcomes of cardiac surgery
Work done by:
Steve GallivanChris Sherlaw-JohnsonJocelyn Lovegrove
Tom TreasureOswaldo Valencia
CORU
St Georges / Guy’s

Mortality data for cardiac surgery
0000000000000000100000000
0000000000000000000000000
0000000000000100000000000
0000000100000000000000000
0000000000000000000100000
0000000000000000000001010

Mortality data for cardiac surgery
0000000000000000100000000
0000000000000000000000000
0000000000000100000000000
0000000100000000000000000
0000000000000000000100000
0000000000000000000001010
6 perioperative deaths in 150 cases

0 20 40 60 80 100 120 140
Operation number
0
2
4
6
8
10
Cumulative deaths
Graphical presentation of data
First used in the context of surgery by DeLeval

0 20 40 60 80 100 120 140
Operation number
0
2
4
6
8
10
Cumulative deaths
Graphical presentation of data
Is this series of outcomes good or bad?

Co-morbidity
Emergency status
Repeat operation
LV function
Age
Risk of perioperative
death
Risk of perioperative
death
Patient factors that contribute to risk of death
To be fair, assessment of outcomes should account for case-mix

0 20 40 60 80 100 120 140
Operation number
0
2
4
6
8
10
Cumulative deaths
Expected mortality (from risk model)
Actual mortality
Net lifegain
Par for the course
Compare outcomes to expectations

Variable Life Adjusted Display (VLAD)
0 20 40 60 80 100 120 140
Operation number
0
1
2
3
4
5Net life gain
VLAD plot for a single surgeon

0 20 40 60 80 100 120 140Operation number
012345
-1-2-3-4
Net life gain
Vlad the impaler
The venerable bleed
Hawkeye Pierce
Comparing three fictitious surgeons
Unexpecteddeath
Survivoragainst
the odds

Comparing surgeons within a unit
Net life gain
Operation number
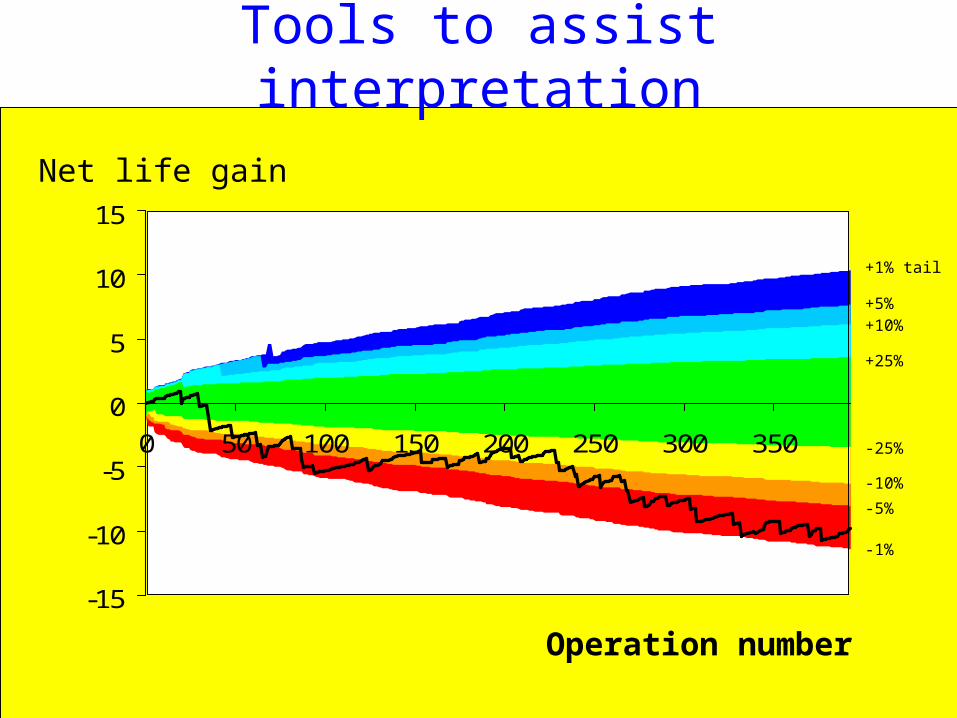
-15
-10
-5
0
5
10
15
0 50 100 150 200 250 300 350
Operation number
Net
lif
e g
ain
-1%
-5%
-10%
-25%
+25%
+10%+5%
+1% tail
Tools to assist interpretation
Net life gain
Operation number

Keys to success
• Surgeons say that visual display is intuitive
• Can be used to identify possible problems in real time
• Monitoring tool “rewards” good outcomes rather than just punish bad outcomes
• Clinical champion
VLAD adopted worldwide

Case study 2:
monitoring prescription errorsCollaborators:
Steve GallivanChristos Paschalides
Bryony Dean Franklin Ann JacklinKara O’Grady
Nick Barber
CORU
Hammersmith
London School of Pharmacy
Funded by the Trustees of Hammersmith Hospitals NHS Trust

Monitoring the prescribing process
Care process
Data
Information system
Analysis of data
Feedback
Junior doctor writes prescription
Ward pharmacist corrects any errors that he or she
identifies

Care process
Data
Information system
Analysis of data
Feedback
Prescription errors deemed sufficiently serious by
pharmacist are logged asincidents
Monitoring the prescribing process

Care process
Data
Information system
Analysis of data
Feedback
Extensive research on nature and rates of reported
prescription errors
Monitoring the prescribing process

Care process
Data
Information system
Analysis of data
No systematic feedback to prescribers
With no feedback, how can we expect prescribing practice to improve?
The problem

Feasibility study
Ward pharmacistchecks new medication orders...
...& records consultant team, number of new orders and all
errors identifiedData entered onto
spreadsheetJunior doctors write prescriptions
Graphical summaries prepared
Feedback sentto head of specialty
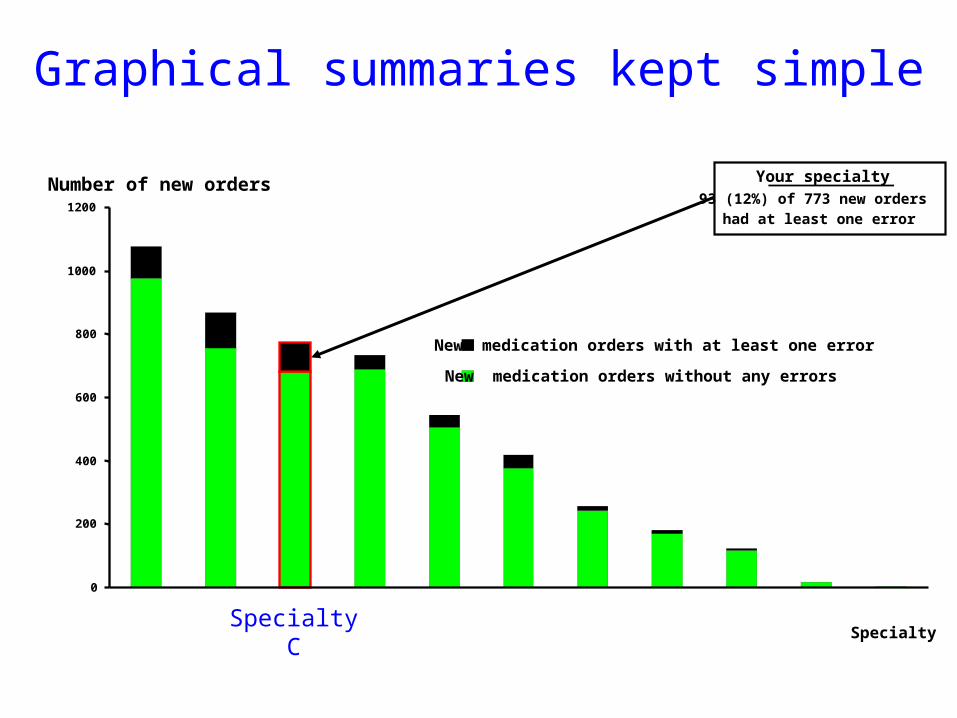
0
200
400
600
800
1000
1200
SpecialtyC
Specialty
New medication orders with at least one error
New medication orders without any errors
Number of new orders Your specialty93 (12%) of 773 new orders
had at least one error
Graphical summaries kept simple

0%
2%
4%
6%
8%
10%
12%
14%
16%
AMUC All other specialties
Specialty
Proportion of new orders w ith an
error
Proportion for whole directorate
Proportion of new orders with an error
Proportion for whole directorate
AdmissionsCXH
All other specialties
How much statistics?
95% confidenceinterval
SpecialtyC

16/02/0502/03/05
16/03/05
30/03/05
11/04/05
25/04/05
09/05/05
23/05/05
0
10
20
30
40
50
60
70
80
90
100
0 200 400 600 800 1000
Cumulative number of orders with an error
Cumulative number of new medication orders
Other specialties
AMUC
16/02/0502/03/05
16/03/05
30/03/05
11/04/05
25/04/05
09/05/05
23/05/05
0
10
20
30
40
50
60
70
80
90
100
0 200 400 600 800 1000
Cumulative number of orders with an error
Cumulative number of new medication orders
Other specialties
AMUCAdmissions
CXH
Performance over time
SpecialtyC

Prototype feedback pages 1 and 2
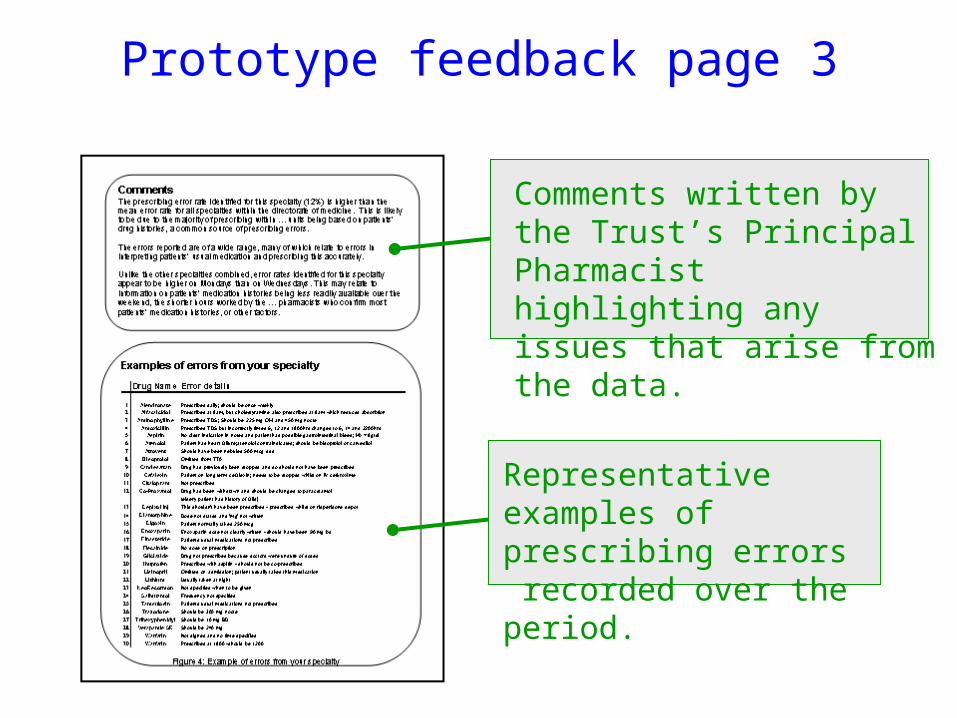
Prototype feedback page 3
Comments written by the Trust’s Principal Pharmacist highlighting any issues that arise from the data.
Representative examples of prescribing errors recorded over the period.

...does this process leadto improvement?
Care
process
Data
Information
system
Analysis of
dataFeedback
Care
process
Data
Information
system
Analysis of
dataFeedback
Hang on...
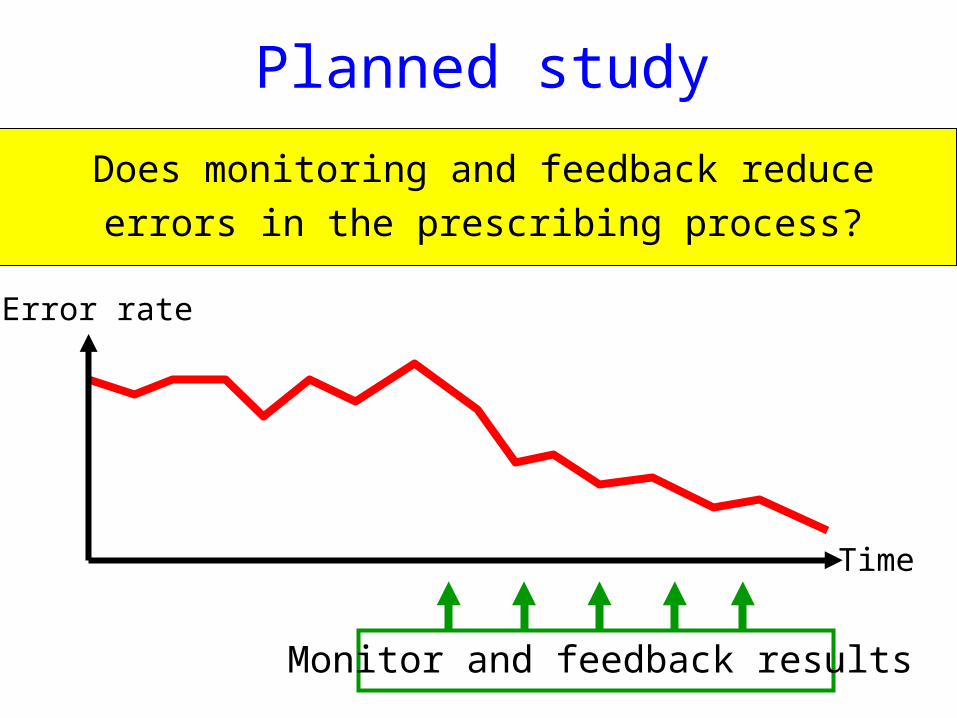
Planned study
Does monitoring and feedback reduce
errors in the prescribing process?
Time
Error rate
Monitor and feedback results
Summary
• Succinct graphical methods can be very useful in the analysis of clinical data and in feeding back information to clinical teams.
• Appropriate feedback cannot do any harm, can it?
• Evaluation of monitoring systems in terms of clinical improvement is desirable.