group.bmj - british journal of ophthalmologybjo.bmj.com/content/bjophthalmol/64/3/164.full.pdf ·...
TRANSCRIPT
British Journal of Ophthalmology, 1980, 64, 164-169
Corneal endothelial changes under inducedintraocular pressure elevation: a scanning andtransmission electron microscopic study in rabbitsS. MELAMED,' I. BEN-SIRA,l AND Y. BEN-SHAUL2
From the "Department of Ophthalmology, Beilinson Medical Center, Tel-Aviv University,Petah-Tikva, Israel, and the 2Department of Microbiology, the George S. Wise Faculty ofLife Sciences, Tel-Aviv University, Tel-Aviv, Israel
SUMMARY Intraocular pressure was artificially raised to 60-70 mmHg in 7 albino rabbits for periodsof 15 minutes to 4 hours. The corneal endothelium of these eyes was studied by transmission andscanning electron microscopy. A correletion between exposure time to elevated IOP, clinical signsobserved by slit-lamp examination, and extent of morphological damage is clearly shown. In eyesexposed to high pressure for 15 and 30 minutes corneas remained transparent and only minimalchanges could be detected by SEM, which consisted of small areas of cells with unevenness of theirsurface, occasional cellular ruptures, and diminution of cilia and microvilli. After 1-2 hours ofexposure small, solitary corneal opacifications appeared. In these eyes more severe morphologicalchanges affecting larger areas were observed, with additional cellular blebbing, excariocytosis,cellular rupture, disintegration, and disappearance seen in SEM. Thin sections revealed swelling ofmitochondria, disorganisation of endoplasmic reticulum, and the existence of myelin bodies. Ineyes exposed for 3 and 4 hours to high IOP diffuse corneal haziness, implying stromal oedema,appeared. In these eyes the areas affected were larger, the extent of damage being more severe. Manyareas were bare of endothelium, surrounded by scattered cellular debris, and showed cells withballooning surfaces and multiple ruptures. Even in severe cellular damage cellular junctions ap-peared intact. It is assumed that endothelial cells are more sensitive to IOP elevation than thecellular junctions and that injury to the active pump system due to morphological damage is res-
ponsible for the resultant corneal oedema.
It is widely accepted that endothelial integrity andmetabolic activity are essential for continuousmaintenance of corneal dehydration and trans-parency. On the one hand the endothelium is thesite of a metabolically dependent fluid pump thatcounteracts fluid leakage, while on the other it actsas a barrier to solutes from the anterior chamber.--5Corneal oedema accompanying acute glaucomawas shown to result from noncompensated cornealendothelium.1 2 4-6 This noncompensation, whichallows excessive flow of fluid to the corneal stroma,might be explained by two mechanisms: (1) Highintraocular pressure (IOP) affects the metabolicactive-pumping mechanism without any morpho-logical changes, thus reducing resistance to aqueousflow to the stroma with resultant stromal oedema.5(2) Elevated IOP causes morphological cellular
Correspondence to Dr S. Melamed.
damage, thus reducing anatomically and func-tionally the barrier to flow of fluid into the stroma.In 47 eyes with chronic glaucoma decreased con-centration of endothelial cells along with progres-sive atrophy and degeneration were described.6More recently other investigators using scanning
electron microscopy (SEM) and transmissionelectron microscopy (TEM)7-10 have shown variousmorphological changes which could be attributed tothe nonfunctioning endothelium. Among thesechanges were flattening of cells, blebbing of cellularsurface, intracellular vacuolisations, nuclear expul-sion (excaryocytosis), and complete endothelialdisorganisation or disappearance.
All these morphological changes were clearlyshown by Svedbergh10 in monkey eyes exposed tomoderate IOP (33-44 mmHg) for 3-7 hours.However, in that study the IOP was elevated byadjusting the height of a reservoir containing mock
164
on 15 May 2018 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.64.3.164 on 1 M
arch 1980. Dow
nloaded from
Corneal endothelial changes under induced intraocular pressure elevation
aqueous humor connected to the anterior chamber.Although it is acceptable that high IOP was themain cause for the morphological changes described,some additional damage could be attributed to theperfusion of the anterior chamber. Perfusion of thecornea in vitro with Ringer bicarbonate withoutapplication of high pressure resulted in variableultrastructural changes such as vacuolisation,mitochondrial and endoplasmic reticulum swelling,and complete intracellular disorganisation."1The purpose of the present study was to investi-
gate the extent and chatacter of endothelial ultra-structural changes in relation to different exposureperiods of elevated lOP and the extent of theresulting stromal oedema. In order to minimisepossible damage due to perfusion and turbulencenear the endothelium the LOP was artificially ele-vated by connecting a reservoir of normal saline tothe vitreous through the pars plana.
Materials and methods
Seven albino rabbits of 2-5-3-5 kg body weightwere anaesthetised by injection of pentobarbitonesodium (30 mg/kg) intravenously. After deepanaesthesia was achieved the IOP was artificiallyelevated in the right eye, the left eye serving as acontrol. IOP elevation was carried out by connectinga reservoir of normal saline through the pars planato the vitreous. The height of the reservoir wasadjusted between 81 and 95 cm, creating an IOP of60-70 mmHg. The rate of IOP elevation wasverified by measurement with hand-held applanationtonometer (Perkins).To eliminate the possible effect of saline perfusion
2 control eyes were connected to the reservoiradjusted to a height of 10 cm, keeping IOP withinnormal limits. During the period of IOP elevationwe carried out slit-lamp examination, looking forsigns of comeal oedema, ciliary congestion, flat-tening of the anterior chamber, pupillary diameter,and its reaction to light. Eyes examined wereexposed to different period of IOP elevation,lasting 15 minutes, 30 minutes, 1 hour, 90 minutes,and 2, 3, and 4 hours.At the end of the exposure time both eyes were
enucleated and buttons of cornea were immediatelycut from the globe. The corneas were immersed in2% glutaraldehyde in 0-1 M cacodylate buffer, pH7-4, and fixed at 4°C overnight. For thin sectioningand TEM the tissue was postfixed in 2% OSO4 inthe same buffer and embedded in Epon. Thinsections on grids were stained with uranyl acetateand lead citrate. Preparations were examined andphotographed in a Jeol-100B electron microscopeat 80 kV. For SEM fixed pieces of cornea were
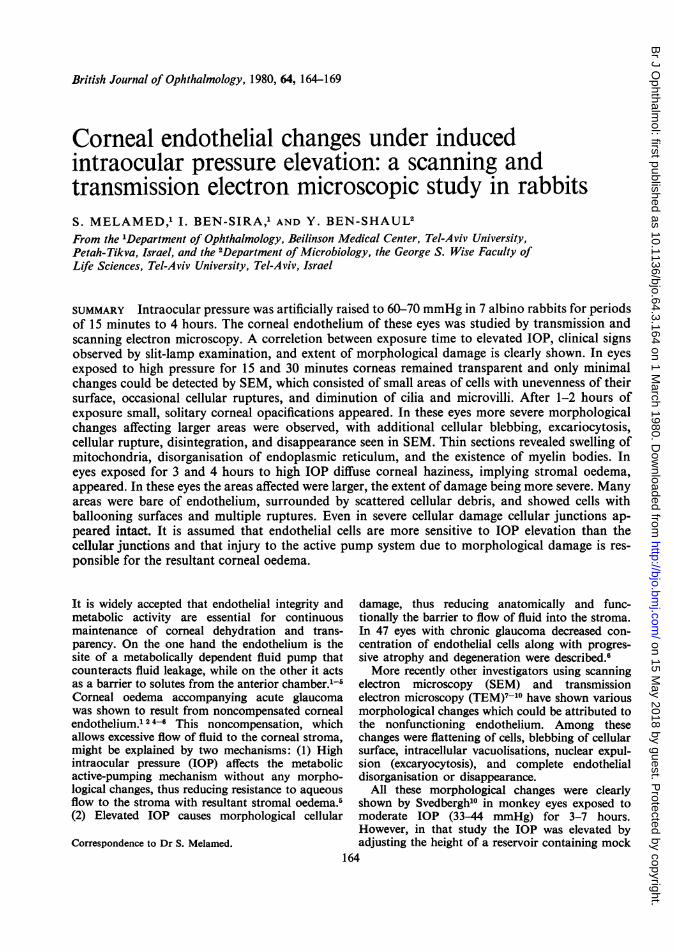
Fig. 1 Normal corneal endothelium (SEM). Cellsare flat, hexagonal in shape, with randomly distributedmicrovilli (M) and cilia (C). Note the sharply demarcatedintercellular borders. x 3000.
postfixed with OSO4 as above, washed and dehy-drated in a series of ethyl alcohols. Drying wascarried out from liquid CO2 by the critical pointmethod. After drying, preparation were coated witheither gold or gold-paladium (60-40%) by sputteringand photographed in a Jeol-S35 scanning electronmicroscope at 20-25 kV.
Results
On slit-lamp examination slight corneal opacifica-tion could be detected after 1-2 hours of exposureto high IOP. Diffuse stromal oedema appearedonly after 3-4 hours of exposure. Ciliary congestioncould be observed after 30 minutes, while pupillarymid-dilatation and nonreaction to light could bedetected only after 1 hour. Flattening of the anteriorchamber was noticed immediately.
In the control eyes (including the 2 eyes perfusedwith saline) the endothelial appearance resembledpreviously reported descriptions.'2'6 In TEM thecells appeared flat, with numerous mitochondriaand organised rough endoplasmic reticulum. Apicaltight junctions were observed between cells withoccasional pinocytotic vesicles and cilia on the cellsurface. In SEM endothelial cells appeared flat,hexagonal in shape, with randomly distributedmicrovilli and cilia on the cell surface. Sharplydemarcated, interdigitating cellular borders werealso observed (Fig. 1). In eyes exposed for 15 and
165
on 15 May 2018 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.64.3.164 on 1 M
arch 1980. Dow
nloaded from
S. Melamed, I Ben-Sira, and Y. Ben-Shaul
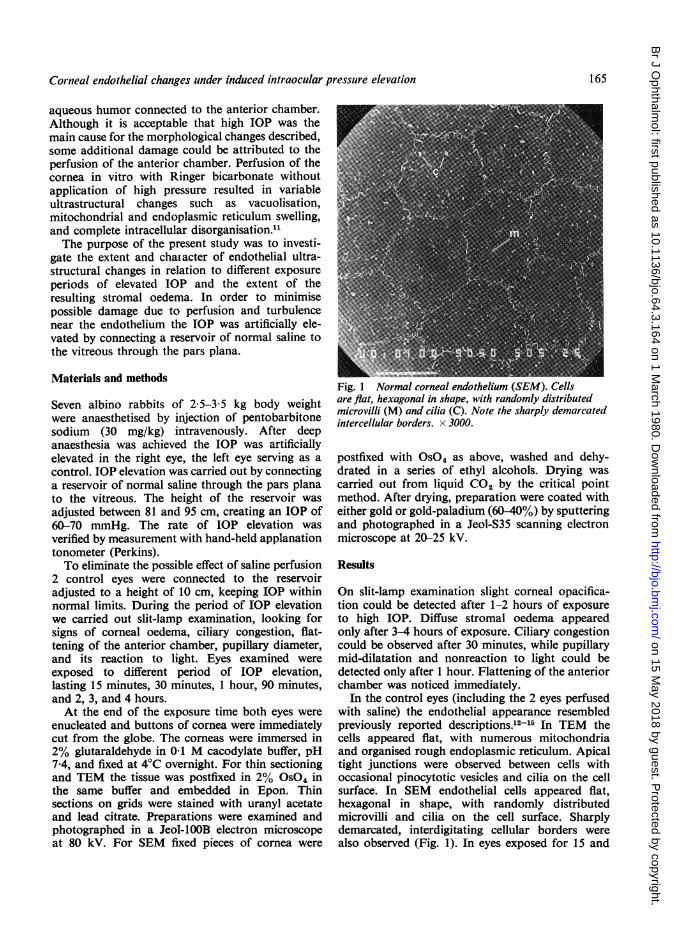
Fig. 2 Border area between nonaffected endothelium Fig. 3 Minimal damage to endothelium after 30 minutes(bottom) and minimally damaged cells after 15 minutes of elevated IOP. Normally appeared endothelium (right)of exposure to elevated IOP. Note unevenness of cellular is adjacent to cells with attenuated cell surface,surface and diminution of microvilli and cilia. x 3000. blebbing (b), and cellular ruptures (arrows). x 3000.... ~~~~~~~~~~~~~~~~~~~~~~~~~~- ,,-----.---.......................A---E--
Fig. 4 Endothelial cell after exposure of I hour to high pressure. Distention and swelling of mitochondria (M)and endoplasmic reticulum (ER) is evident. Note vacuolisations (V) and myelin body (MB). x 18 000.
166
on 15 May 2018 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.64.3.164 on 1 M
arch 1980. Dow
nloaded from
Corneal endothelial changes under induced intraocular pressutre elevatioln
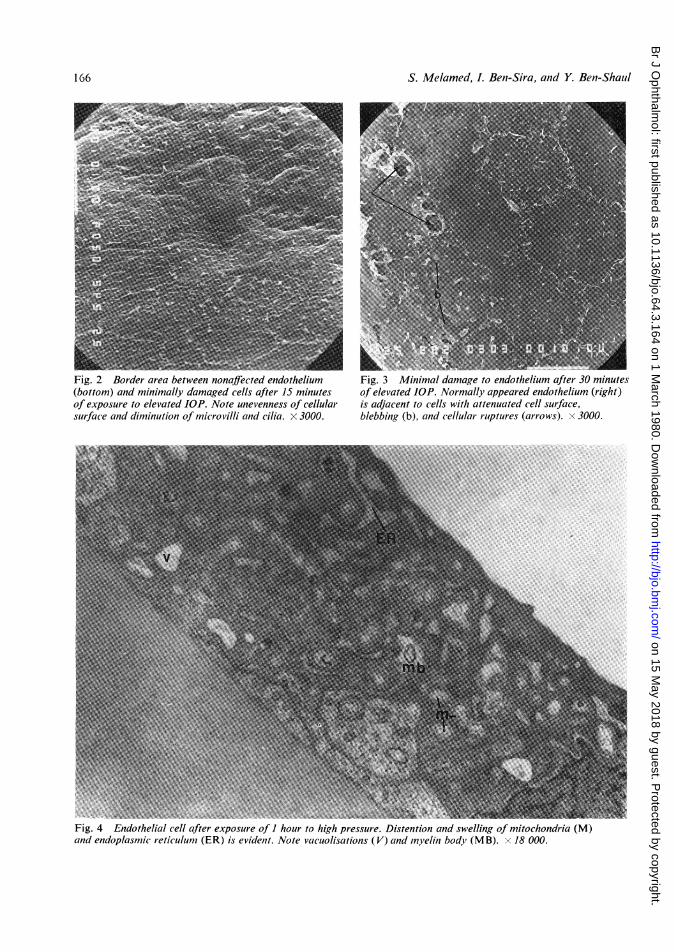
Fig. 5 An area of severely damaged endothelium afterexposure of 4 hours to elevated IOP. The centre ofinsulated area is devoid of endothelium (D),surrounded by ruptures cells and cellular debris.At right normal endothelium (E) is seen and at leftminimally damaged cells are shown. x 750.
30 minutes to elevated IOP only anterior chamberflattening and ciliary congestion were observed byslit-lamp examination. No signs of corneal oedemaor regional opacification were detected. Thinsections of the endothelial cells in these eyes werecompletely normal. In SEM only minimal changescould be seen. Most of the cells appeared normal,but in small, scattered areas unevenness of cellularsurface along with slight swelling of cellular contentwere evident. Occasional ruptured cell surfaceswere encountered. Cilia and microvilli were obser% edless frequently (Figs. 2, 3).
In eyes exposed for 1-2 hours to high pressure,small solitary corneal opacifications could be seenon slit-lamp examination, along with pupillarymid-dilatation and nonreaction to light. Increasedciliary congestion and anterior chamber flatteningwere also observed. Eyes exposed to high IOP for3 and 4 hours showed further deterioration ofcorneal opacification to more diffuse haziness,indicating progression of corneal oedema.
In thin sections affected cells showed disorgani-sation and swelling of endoplasmic reticulum andmitochondria along with vacuolisations and myelinbodies (probably evidence of cellular destruction)(Fig. 4). Despite intracellular damage junctionalcomplexes appeared intact, unaffected by acutelyelevated IOP.
Fig. 6 Severely damaged endothelium. Ruptured cellcontaining empty crater after nuclear expulsion. x 6000.
Fig. 7 Severely damaged endothelium. Bare area(Descemet's membrane) surrounded by ruptureddisintegrated cells. x 3000.
SEM, enabling the observation of large areas ofthe affected endothelium, disclosed different typesof cellular damage. It was evident that larger areasof the endothelium were damaged when the eyeswere exposed to elevated IOP for 3-4 h. Moreover,it was possible to monitor different types of mor.
167
on 15 May 2018 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.64.3.164 on 1 M
arch 1980. Dow
nloaded from
S. Melamed, L. Beni-Sira, anid Y. Ben-Shaiil
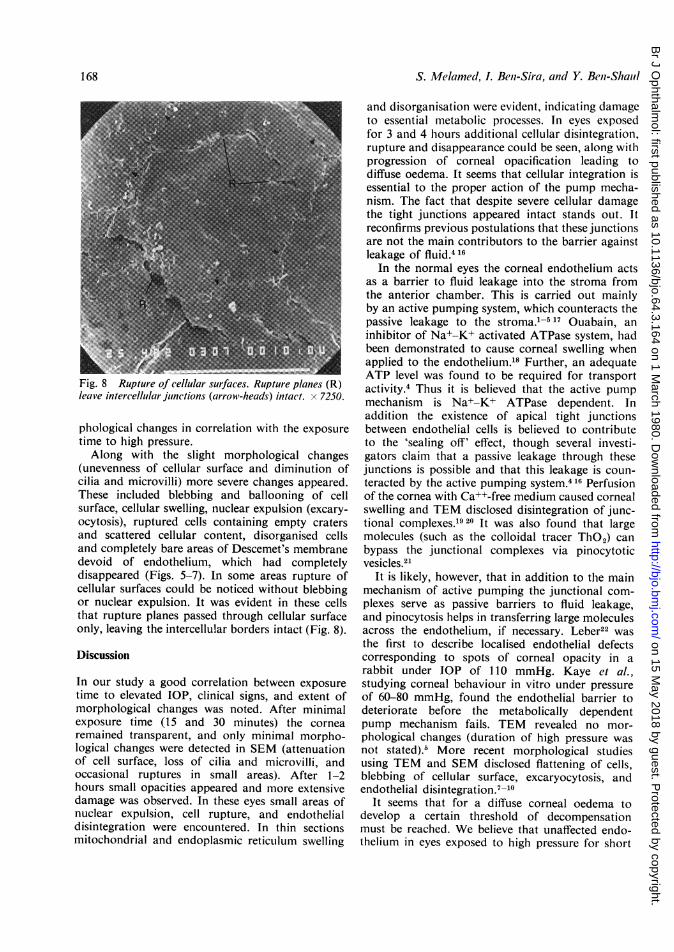
Fig. 8 Rupture of cellular surfaces. Rupture planes (R)leave intercellular junctions (arrow-heads) intact. x 7250.
phological changes in correlation with the exposuretime to high pressure.Along with the slight morphological changes
(unevenness of cellular surface and diminution ofcilia and microvilli) more severe changes appeared.These included blebbing and ballooning of cellsurface, cellular swelling, nuclear expulsion (excary-ocytosis), ruptured cells containing empty cratersand scattered cellular content, disorganised cellsand completely bare areas of Descemet's membranedevoid of endothelium, which had completelydisappeared (Figs. 5-7). In some areas rupture ofcellular surfaces could be noticed without blebbingor nuclear expulsion. It was evident in these cellsthat rupture planes passed through cellular surfaceonly, leaving the intercellular borders intact (Fig. 8).
Discussion
In our study a good correlation between exposuretime to elevated IOP, clinical signs, and extent ofmorphological changes was noted. After minimalexposure time (15 and 30 minutes) the cornearemained transparent, and only minimal morpho-logical changes were detected in SEM (attenuationof cell surface, loss of cilia and microvilli, andoccasional ruptures in small areas). After 1-2hours small opacities appeared and more extensivedamage was observed. In these eyes small areas ofnuclear expulsion, cell rupture, and endothelialdisintegration were encountered. In thin sectionsmitochondrial and endoplasmic reticulum swelling
and disorganisation were evident, indicating damageto essential metabolic processes. In eyes exposedfor 3 and 4 hours additional cellular disintegration,rupture and disappearance could be seen, along withprogression of corneal opacification leading todiffuse oedema. It seems that cellular integration isessential to the proper action of the pump mecha-nism. The fact that despite severe cellular damagethe tight junctions appeared intact stands out. Itreconfirms previous postulations that these junctionsare not the main contributors to the barrier againstleakage of fluid.4 16
In the normal eyes the corneal endothelium actsas a barrier to fluid leakage into the stroma fromthe anterior chamber. This is carried out mainlyby an active pumping system, which counteracts thepassive leakage to the stroma.1-5 17 Ouabain, aninhibitor of Na+-K+ activated ATPase system, hadbeen demonstrated to cause corneal swelling whenapplied to the endothelium.18 Further, an adequateATP level was found to be required for transportactivity.4 Thus it is believed that the active pumpmechanism is Na+-K+ ATPase dependent. Inaddition the existence of apical tight junctionsbetween endothelial cells is believed to contributeto the 'sealing off' effect, though several investi-gators claim that a passive leakage through thesejunctions is possible and that this leakage is coun-teracted by the active pumping system.416 Perfusionof the cornea with Ca++-free medium caused cornealswelling and TEM disclosed disintegration of junc-tional complexes.'920 It was also found that largemolecules (such as the colloidal tracer ThO2) canbypass the junctional complexes via pinocytoticvesicles.21
It is likely, however, that in addition to thie mainmechanism of active pumping the junctional com-plexes serve as passive barriers to fluid leakage,and pinocytosis helps in transferring large moleculesacross the endothelium, if necessary. Leber22 wasthe first to describe localised endothelial defectscorresponding to spots of corneal opacity in arabbit under IOP of 110 mmHg. Kaye et al.,studying corneal behaviour in vitro under pressureof 60-80 mmHg, found the endothelial barrier todeteriorate before the metabolically dependentpump mechanism fails. TEM revealed no mor-phological changes (duration of high pressure wasnot stated).5 More recent morphological studiesusing TEM and SEM disclosed flattening of cells,blebbing of cellular surface, excaryocytosis, andendothelial disintegration.'-10
It seems that for a diffuse corneal oedema todevelop a certain threshold of decompensationmust be reached. We believe that unaffected endo-thelium in eyes exposed to high pressure for short
168
on 15 May 2018 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.64.3.164 on 1 M
arch 1980. Dow
nloaded from
Corneal endothelial changes under induced intraocular pressure elevation
periods can compensate for the rather small dam-aged and leaky areas, thus keeping corneal stromadehydrated and transparent. However, if the extentof damage is more severe, as seen in eyes exposedfor longer periods, the remaining functioningendothelium loses its ability to compensate for thelarger leaking areas, and a diffuse corneal oedemaresults. In the rabbit cornea under IOP of 60-70mmHg this decompensation appears after 3 to 4hours of exposure.This work was made possible by a grant from the IsraeliMinistry of Health.
References
'Ytteborg J, Dohlman CH. Corneal edema and intraocularpressure. (1). Animal experiments. Arch Ophthalmol 1965;74: 375-81.2Ytteborg J, Dohlman CH. Corneal edema and intraocularpressure. (2). Clinical results. Arch Ophthalmol 1965; 74:477-84.3Donn A. Cornea and sciera. Arch Ophthalmol 1966; 75:261-88.4Fischbarg J. Active and passive properties of the cornealendothelium. Exp Eye Res 1973; 15: 615-38.5Kaye GI, Sibley RC, Hoefle FB. Recent studies on thenature and function of the corneal endothelial barrier.Exp Eye Res 1973; 15: 585-613.6lrvine AR. The role of the endothelium in bullous kera-topathy. Arch Ophthalmol 1956; 56: 338-51.7Hervouet F, George Y, Tusques J, Ertus M. Aspect dedifferentes structures oculaires humaines en microscope abalayage. Bull Soc Ophtalmol Fr 1972; 84: 603-20.8Hervouet F, Ertus M. Scanning Electron MicroscopicStudies of the Eye Structures. Paris: Masson, 1973; 12-13.9Renard G, Galle P. Etude en microccopie a balayage del'endothelium corn6en humain. Ann Oculist 1973; 206:835-49.
°0Svedbergh B. Effects of artificial intraocular pressureelevation on the corneal endothelium in the vervet monkey.Acta Ophthalmol 1975; 53: 839-55.
"Mccarey BE, Edelhauser HF, Van-Horn DL. Functionaland structural changes in the corneal endothelium duringin-vitro perfusion. Invest Ophthalmol 1973; 12: 410-17.
"Blumcke S, Morgenroth K. The stereo ultrastructure ofthe external and internal surface of the cornea. J UltrastructRes 1967; 18: 502-18.
"Hogan H, Alvarado J, Weddel J. Histology of the HumanEye. Philadelphia: Saunders, 1971; 102-11 and 171-8.
14Svedbergh B, Bill A. Scanning electron microscopic studiesof the corneal endothelium in man and monkeys. ActaOphthalmol 1972; 50: 321-36.
15Doughman DJ, Van-Horn D, Harris JE, Miller GE,Lindstrom R, Good RA. The ultrastructure of humanorgan cultured cornea. Arch Ophthalmol 1974; 92: 516-23.
'6Mishima S, Kaye GI, Takahashi GH, Kudo T, TrenberthSM. In: Langham M, ed. The Cornea. MacromolecularOrganization of a Connective Tissue. Baltimore: JohnsHopkins Press, 1969; 207.
"Maurice DM. The cornea and sclera. In: Davson H, ed.The Eye. London and New York: Academic Press, 1969;1: 489-600.
18Trenberth SM, Mishima S. The effect of ouabain on therabbit corneal endothelium. Invest Ophthalmol 1968; 7:44-52.
19Kaye GI, Mishima S, Cole DJ, Kaye NW. Studies on thecornea: VII. Effects of perfusion with a Ca++-free mediumon the corneal endothelium. Invest Ophthalmol 1968; 7:53-66.
20Kaye GI, Hoefle FB, Donn A. Studies on the cornea:VIII. Reversibility of the effects of in-vitro perfusion ofthe rabbit corneal endothelium with calcium-free medium.Invest Ophthalmol 1973; 12: 98-113.
2'Kaye GI, Pappas GP, Donn A, Mallet N. Studies on thecornea: II. The uptake and transport of colloidal particlesby the living rabbit cornea in-vitro. J Cell Biol 1962; 12:481-501.
22Leber T. Studies uber den flussigkeitswechsel. Albrecht vonGraeffes Arch Klin Ophthalmol 1873; 19: 87-185.
169
on 15 May 2018 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.64.3.164 on 1 M
arch 1980. Dow
nloaded from