h fes– ehabilita echnolog: evie , tua, ontr ategies · 2 f. anaya e al. 1 3...
TRANSCRIPT

Vol.:(0123456789)1 3
International Journal of Intelligent Robotics and Applications (2018) 2:1–28 https://doi.org/10.1007/s41315-017-0042-6
REGULAR PAPER
Hybrid FES–robotic gait rehabilitation technologies: a review on mechanical design, actuation, and control strategies
Francisco Anaya1 · Pavithra Thangavel1 · Haoyong Yu1
Received: 19 September 2017 / Accepted: 27 December 2017 / Published online: 17 January 2018 © Springer Nature Singapore Pte Ltd. 2018
AbstractGait disorders in neurologically disabled people can be treated by various techniques available today which include passive orthoses, functional electrical stimulation (FES) and robot assisted gait training devices (RAGT). However, each system has its own drawback. For example, gait rehabilitation with orthosis is physically taxing for the patient with no significant functional improvement. FES uses muscle powers as physiological actuators to promote balance and improve gait but leads to fatigue, along with poor control of joint trajectories. RAGT devices including powered exoskeletons, gait rehabilitation systems employing programmable footplates and mobile training platforms, have shown significant advantages but the devices are not yet mature due to numerous drawbacks associated with physical and cognitive interaction, energy-management and portability issues. The combination of FES technology and RAGT devices, often named hybrid FES–robot technologies, has arisen as a promising approach to aid in gait restoration. This work reports a comprehensive review on the hybrid FES–robot technologies over the last decades, focusing on different mechanical structures, actuator designs, sensing technologies, and control approaches. The hybrid robotic structures are classified into two categories: (i) orthotic-based hybrid systems, where (a) FES is used to stimulate the muscles and produce joint torque while the robotic system acts as energy dissipating device, and (b) FES and robotic systems are both torque-generating devices; and (ii) non-orthotic based hybrid systems. The review compiles a variety of sources and illustrates the technology’s most important challenges in the fields of hybrid rehabilitation robotics which may contribute towards further development of hybrid robot systems.
Keywords Functional electrical stimulation · FES · Neuroprosthesis · Robotic assisted gait · Robot control · Muscle fatigue · Rehabilitation · Gait · Hybrid control
AbbreviationsFES Functional electrical stimulationRAGT Robot assisted gait trainingCBO Controlled-brake orthosisSBO Spring-brake orthosisGBO Gravity balanced orthosisJCO Joint-coupled orthosisESO Energy storing orthosisVCHM Variable constraint hip mechanismSEAHO Semi-active hybrid orthosisIMU Inertial measurement unitsHyPO Hybrid powered orthosisFES-IM Intramuscular functional electrical stimulation
BWS Body weight supportPID Proportional-integral-derivativeVIKM Variable impedance knee mechanismHNP Hybrid neuroprosthesisGT-FES Gait trainer with functional electrical
stimulationCT Conventional therapyAFO Ankle-foot orthosisLEE Lower-extremity exoskeletonBLERE Bionic lower extremity rehabilitation
exoskeleton
1 Background
According to the World Health Organization, around 15 mil-lion people fall victim to stroke every year around the world, and this number is estimated to grow by 3.4 million people by 2030 (Mackay et al. 2004). The most important body
* Haoyong Yu [email protected]
1 Department of Biomedical Engineering, National University of Singapore, 9 Engineering Drive 1, Singapore 117575, Singapore

2 F. Anaya et al.
1 3
function disability related to stroke is the inability to produce controlled movement. This motor impairment has a major impact on the stroke survivor’s quality of life. Stroke patients undergo rehabilitation therapy in the hope of recovering their lost neuromuscular functions and to regain control over their body movement. However, even after completing conventional therapy only 40–50% of stroke patients benefit from this intensive therapy (Schaechter 2004). In particular, stroke patients who had a unilateral paralysis rarely regain walking function to the point of effective ambulation (Hara 2013).
Many methods of training are available for gait recovery in persons with motor impairment. However, these numer-ous approaches have their own limitation which calls for the need to improve the available rehabilitation interven-tions that aim to recover the walking capability. Functional electrical stimulation (FES) and robotic rehabilitation ther-apy targeting motor function recovery have been gaining attention over the past decade. FES-based approach aims to deliver low intensity electrical stimulation to promote muscle contraction and produce flexion, extension of joints needed for ambulation. In comparison with conventional treatment, FES is reported to produce better results by not only promoting motor improvements but also by inducing changes in motor cortex excitability and functional corti-cal reorganization (Maffiuletti et al. 2011; Popović 2014). However, the high degree of complexity and non-linearity involved in controlling joint movement during the swing phase of FES-induced gait prevents its widespread adop-tion in lower limb rehabilitation. Also, the high metabolic and performance costs of activity caused by the induced recruitment of motor unit results in fast and abrupt incidence of muscle fatigue, which consequently foils proper progres-sion of the treatment (Lynch and Popovic 2008; Zhang et al. 2007; Popovic 2003).
Rehabilitation robots are supposed to be a promising therapy approach that can deliver longer duration of therapy with adjustable training intensity and customized treatment for individual patient’s needs and problems. As the robotic technology can provide accurate kinetic and kinematic measurements, it is easier to quantify a person’s functional improvement with the treatment (Lum et al. 2002; Huang and Krakauer 2009). Nonetheless, robot-assisted training is susceptible to limited effect, where patient’s compliance is restricted, resulting in no functional improvements. Regard-less of the developments in sophisticated systems focused at enhancing rehabilitation outcomes, the use of robotics is still controversial due to the lack of evidence supporting superiority of robotic therapy restoring motor function over standard health care.
To overcome the drawbacks of each individual approach, the combination of FES with robotic devices was proposed; which aims to provide more effective, safe, and robust
rehabilitation therapy. These combined technologies are con-ventionally termed Hybrid Robotic Rehabilitation Systems and are defined as systems that aim to achieve motor recov-ery or compensate motor function by combining electrically stimulated muscle action and torque provision to the joints (del-Ama et al. 2014). A previous review has identified and discussed the key technological aspects concerning hybrid exoskeletons (del-Alma et al. 2012). However, a review not only focusing on the application of this technology to pow-ered exoskeletons but also to robotic footplates systems, mobile platforms and cycling systems is still not recorded in literature. In this paper, we also discuss the limitations of the currently developed systems and future research and development directions of hybrid robotic technologies. We provide detailed comparison for the exoskeleton bio-inspired joint design and highlight the rising hybrid robotic technolo-gies, with focus on their mechanical design, actuator system, and sensing and control strategy.
Our analysis follows two classifications: (i) orthotic-based hybrid systems, where (a) FES is used to stimulate the mus-cles and produce joint torque while the robotic system acts as energy dissipating device, and (b) FES and robotic systems are both torque-generating devices; and (ii) non-orthotic based hybrid systems which include robotic footplates sys-tems, mobile platforms and cycling systems. The analysis is addressed from a technological and a clinical perspective where their main challenges for consolidation is discussed. This may contribute towards further development of hybrid robotic rehabilitation systems.
2 Results
From the search results, 55 papers were selected for the review. This amounted to 28 different hybrid robotic system which were then classified into two groups: orthotic-based hybrid systems (23), and non-orthotic based hybrid systems (5), including robotic footplates systems, mobile platforms and cycling systems.
Relevant and referenced publications were included in the survey if they: (i) Fit into the definition of hybrid rehabilita-tion systems (presented a shared use of robotics with passive or active actuation and functional electrical stimulation), (ii) focused on lower limb rehabilitation and (iii) considered at least one gait outcome measure such as kinematic data, elec-tromyography signal analysis, force measurements, clinical scales, or functional evaluation in either healthy subjects or stroke survivors. Works in which the robotic treatment and FES were prescribed separately were excluded from this review. The sequence of the reviewed technologies follows a time order and the invention year of the robot is added in each summary table.

3Hybrid FES–robotic gait rehabilitation technologies: a review on mechanical design, actuation,…
1 3
2.1 Technical overview of orthosis‑based hybrid systems
In the context of this review, we define FES Hybrid-Robotic gait rehabilitation technologies as those systems that aim to achieve motor recovery or compensate motor function in patients with neurological challenges by combining the effects of functional electrical stimulation and torque pro-vision at joint level. The combination of FES and robotic control is not a new concept. Hybrid robotic systems were introduced for the first time in 1972 by Tomovic R. (1973) after which several hybrid technologies have been intro-duced with varied mechanical designs, actuation, and con-trol approaches. However, a two-fold classification could be identified: (1) Hybrid systems where FES is used to stimulate the muscles and produce joint torque while the robotic system acts as energy dissipating device, and (2) Active hybrid systems where FES and robotic system are both torque generating devices.
2.1.1 FES is used to stimulate the muscles and produce joint torque while the robotic system acts as energy dissipating device
We identified eight main hybrid systems for the recovery of gait related functions in patients with motor impairments where FES is used to stimulate the muscles and produce joint torque while the orthotic robot acts as energy dissi-pating device. Hybrid systems with energy dissipation are built on the bases of systems where FES is used to actively stimulate the muscles of the limb while the robotic systems are mostly passive gait orthosis. Here, the former hybrid system provides joint trajectory control and reduces muscle fatigue with the help of elastic elements and joints brakes. Table 1 shows a summary of the reported orthotic-based hybrid systems where the robotic systems have been mostly used as energy dissipation devices.
2.1.1.1 Hybrid orthosis controlled by joint brakes Durfee and Hausdorff were the first to propose the concept of joint brakes to control joint movements generated by FES in 1990 (Durfee and Hausdorff 1990), by presenting three controllers for position tracking of the free-swinging shank in hybrid FES gait. To build on this concept, the authors introduced the 8 DOFs controlled-brake orthosis (CBO) with four FES channels (Fig. 1) (Durfee et al. 1992; Goldfarb and Durfee 1996; Goldfarb et al. 2003). CBO is a long leg brace with friction controllable brakes at the hip and knee joints. It uses the muscle stimulation as a power source to produce desired joint trajectories while the friction controllable brakes reg-ulate the power generated by the electrical stimulation at each joint. The muscle fatigue was decreased by locking the brakes throughout the entire stance phase and by stopping
stimulation to the quadriceps. The laboratory CBO weighs 6 kg and refers to a two-sided device which interfaces with the hip, knee and ankle joints. The CBO completely relies on the robotic structure to provide support to the axial load-ing of joint movement at the hip. Experiments were per-formed for the evaluation of CBO on SCI patients wearing the device and their ambulation performance was accessed. The results of these experiments showed that the CBO was capable of providing better control over the joint trajecto-ries and significantly reduce muscle fatigue as compared to FES-only gait.
A second solution, named Sensor Walk, was presented by Sharma et al. (2014). This system consists of a novel KAFO with FES programmed to couple hip and knee flexion (Fig. 2). A spring clutch mechanism is built into the system for locking and unlocking of the joints during the stance phase of gait. The KAFO system locks the knee joint just before stance phase and remains locked until early swing phase. Similar to previously reported system (Goldfarb et al. 2003), the KAFO locks the knee joint of both legs during double support phase and unlock the knee joint when swing phase is initiated. The KAFO is completely passive, with the only purpose of providing additional stability and support to the individual’s body weight by unlocking and locking the knee joint while hip flexors/extensors contract to produce hip torque during the swing phase. However, no clinical tests have been done for this technology.
A similar solution to manage muscle fatigue and joint trajectory was introduced by Chang et al. (2016, 2017). The Stimulation-driven exoskeleton system was designed to restore the loss of motor function caused by varying types of paralysis from spinal cord trauma. The hybrid neuro-prosthesis consists of the combination of a passive variable-constraint exoskeleton to provide better support and stability with FES (Fig. 3). The overall control of the sys-tem governed the locking and unlocking of the lower limb exoskeleton’s hip and knee joints as well as the stimulation designs triggering hip and knee flexors and extensors mus-cles across different phases of gait. Attaching controllable brakes to passive gait orthosis during FES-assisted walk-ing aimed to solve the drawbacks of joint trajectory control generated by FES. Unlike other hybrid neuro-prosthesis, the Stimulation-driven exoskeleton, followed the “muscle-first” approach where the stimulated contraction of the muscles produced the joint movements rather than using motor driv-ers to produce these motions.
The stimulation-driven exoskeleton developed was tested on an individual with paraplegic gait to (1) evaluate the functional electrical stimulation approach required to induce the desired limb motions and (2) assess the control design by means of gait event detection algorithm for stepping with a finite-state automaton controller. The high-level control of the controller defined the states of the hydraulics and was

4 F. Anaya et al.
1 3
Tabl
e 1
Iden
tified
orth
oses
-bas
ed h
ybrid
syste
ms f
or g
ait f
unct
ion
whe
re F
ES is
use
d to
stim
ulat
e th
e m
uscl
es a
nd p
rodu
ce jo
int t
orqu
e w
hile
the
robo
tic sy
stem
act
s as e
nerg
y di
ssip
atin
g de
vice
Dev
ice
nam
e/gr
oup
Wea
rabl
e ro
bot
Mot
or-n
euro
pros
thes
isC
linic
al e
valu
atio
nD
raw
back
Hyb
rid o
rthos
is c
ontro
lled
by jo
int b
rake
s C
ontro
lled-
brak
e or
thos
is C
BO
(199
2) (D
urfe
e et
al.
1992
; Gol
d-fa
rb a
nd D
urfe
e 19
96; G
oldf
arb
et a
l. 20
03)
Pass
ive
Hip
and
Kne
e: b
rake
. Ank
le:
elas
tic.
Orth
osis
wei
ght:
6 kg
.8
DO
FsRo
M: H
ip -1
0-25
°, K
nee
0–60
°.B
rake
torq
ue: H
ip 3
0 N
m, K
nee
50 N
m
4 FE
S-C
hann
els
Feed
back
con
trol:
mus
cula
r fat
igue
m
onito
ring.
Per
onea
l ner
ve st
imu-
latio
n fo
r hip
and
kne
e fle
xion
. Q
uadr
icep
sG
ait p
hase
con
trol:
pero
neal
ner
ve
stim
ulat
ed d
urin
g sw
ing
phas
e to
fle
x hi
p, k
nee,
and
ank
le; q
uadr
i-ce
ps st
imul
ated
bef
ore
doub
le
supp
ort (
stan
ce) t
o pr
epar
e fo
r leg
ex
tens
ion
1 Su
bjec
t:co
mpl
ete
T6 (G
oldf
arb
and
Dur
fee
1996
)4
subj
ects
: 3 c
ompl
ete
T6-T
7, 1
in
com
plet
e T8
(Gol
dfar
b et
al.
2003
)
Use
of w
ithdr
awal
refle
x
Otto
bock
Sen
sor W
alk
(201
4)
(Sha
rma
et a
l. 20
14)
Pass
ive
Kne
e, A
nkle
and
Foo
t: El
ec-
trom
agne
tic u
nloc
king
mec
hani
sm.
Orth
osis
wei
ght:
3.41
kg
3DO
Fs
4 FE
S-ch
anne
ls.
Hip
flex
ors a
nd e
xten
sors
.G
ait p
hase
con
trol:
stim
ulat
ion
initi
-at
ed d
urin
g sw
ing
phas
e
Not
teste
dEv
alua
tion
of sa
fety
and
usa
bilit
y ha
ve n
ot y
et b
een
repo
rted
Stim
ulat
ion-
driv
en e
xosk
elet
on
(201
6) (C
hang
et a
l.201
6; C
hang
et
al.
2017
)
Pass
ive
Hip
and
Kne
e: c
ontro
llabl
e hy
drau
lic L
ower
ext
rem
ity jo
int
cons
train
ts
12 F
ES-c
hann
els:
hip
flex
ors,
hip
exte
nsor
s, kn
ee fl
exor
s, kn
ee
exte
nsor
s and
ank
le d
orsi
flexo
rsO
pen
loop
/On–
off fe
edfo
rwar
d co
ntro
l.G
ait p
hase
con
trol:
stim
ulat
ion
initi
-at
ed d
urin
g ea
rly sw
ing
1 su
bjec
t:C
ompl
ete
T4 (C
hang
et a
l. 20
16)
Trig
ger b
utto
n.Pr
epro
gram
ed F
ES p
aram
eter
s
Sprin
g-br
ake
orth
osis
Spr
ing-
Bra
ke O
rthos
is S
BO (2
000)
(G
haro
oni e
t al.
2001
; Gha
roon
i et
al.
2000
; Jai
lani
et a
l. 20
11)
Pass
ive
Hip
and
Kne
e: b
rake
and
el
astic
-mec
hani
cal c
oupl
ing
2 FE
S-ch
anne
ls.
Feed
back
con
trol.
Ener
gy st
orag
e fro
m q
uadr
icep
s ele
ctro
stim
ula-
tion.
Gai
t pha
se c
ontro
l: sti
mul
atio
n in
itiat
ed d
urin
g st
ance
pha
se to
aid
kn
ee e
xten
sion
Not
teste
dEv
alua
tion
of sa
fety
and
usa
bilit
y ha
ve n
ot y
et b
een
repo
rted
Gra
vity
Bal
ance
d O
rthos
is G
BO
(200
6) (K
rishn
amoo
rthy
et a
l. 20
08; B
anal
a et
al.
2006
; A
graw
al e
t al.
2007
)
Pass
ive
Hip
, Kne
e &
Ank
le.
Sprin
gs to
bal
ance
gra
vity
effe
ct o
n lim
bs. T
read
mill
-bas
ed.
7 D
OFs
4 FE
S-ch
anne
ls.
Ank
le d
orsi
flexo
r and
pla
ntar
flexo
r m
uscl
es.
Ope
n-lo
op c
ontro
lG
ait p
hase
con
trol:
ankl
e do
rsifl
ex-
ors s
timul
ated
dur
ing
swin
g ph
ase
and
plan
tar fl
exor
s to
aid
knee
fle
xion
1 Su
bjec
t: str
oke
(Kris
hnam
oorth
y et
al.
2008
)Pr
epro
gram
ed F
ES p
aram
eter
s.To
o bu
lky:
onl
y fo
r clin
ic u
se. S
ta-
tiona
ry tr
aini
ng sy
stem

5Hybrid FES–robotic gait rehabilitation technologies: a review on mechanical design, actuation,…
1 3
Tabl
e 1
(con
tinue
d)
Dev
ice
nam
e/gr
oup
Wea
rabl
e ro
bot
Mot
or-n
euro
pros
thes
isC
linic
al e
valu
atio
nD
raw
back
Join
t-cou
pled
orth
osis
Ene
rgy
storin
g or
thos
is E
SO
(200
5) (K
angu
de e
t al.
2009
; D
urfe
e an
d R
ivar
d 20
05; K
an-
gude
et a
l. 20
10)
Pass
ive
Hip
and
Kne
e: b
rake
and
el
astic
and
pne
umat
ic c
oupl
ing.
Orth
osis
wei
ght:
16.8
2 kg
.Ro
M: H
ip -1
0-25
°, K
nee
-5-6
0°.
Bra
ke to
rque
: Hip
17
Nm
, Kne
e 34
Nm
2 FE
S-ch
anne
ls.
Ope
n-lo
op c
ontro
lQ
uadr
icep
s mus
cles
. Use
stim
u-la
ted
mus
cle
ener
gy to
driv
e hi
p ac
tuat
or.
Gai
t pha
se c
ontro
l: sti
mul
atio
n in
itiat
ed d
urin
g st
ance
pha
se to
aid
kn
ee e
xten
sion
1 Su
bjec
t:In
com
plet
e T1
2 (K
angu
de e
t al.
2010
)
Wei
ght a
nd si
ze o
f the
syste
m.
Prep
rogr
amed
FES
par
amet
ers
Hyb
rid jo
int-c
oupl
ed c
ontro
lled
brak
e or
thos
is (2
009)
(Far
ris
et a
l. 20
09; F
arris
et a
l. 20
09)
Pass
ive
Hip
and
Kne
e: b
rake
and
el
astic
-mec
hani
cal u
nidi
rect
iona
l co
uplin
g.O
rthos
is w
eigh
t: 6
kgB
rake
torq
ue: 5
0.7
Nm
max
. 6 D
OFs
2 FE
S-ch
anne
lsO
pen-
loop
con
trol
Ener
gy st
orag
e fro
m q
uadr
icep
s el
ectro
stim
ulat
ion
Gai
t pha
se c
ontro
l: sti
mul
atio
n in
itiat
ed d
urin
g st
ance
pha
se to
aid
kn
ee e
xten
sion
Not
teste
dPr
epro
gram
ed F
ES p
aram
eter
s.Ev
alua
tion
of sa
fety
and
usa
bilit
y ha
ve n
ot y
et b
een
repo
rted
Varia
ble
hip
cons
train
t mec
hani
sms
Var
iabl
e co
nstra
in h
ip m
echa
nism
V
CH
M (2
008)
(Aud
u et
al.
2010
; K
obet
ic e
t al.
2009
; To
et a
l. 20
08)
Pass
ive
Hip
: Con
strai
nt O
rthos
isO
rthos
is w
eigh
t: 22
kg
4 FE
S-ch
anne
ls: h
ip fl
exor
s and
ex
tens
ors
Ope
n-lo
op c
ontro
lG
ait p
hase
con
trol:
stim
ulat
ion
initi
-at
ed d
urin
g sw
ing
phas
e
Not
teste
dW
eigh
t and
size
of t
he sy
stem
.Pr
epro
gram
ed F
ES p
aram
eter
s.Ev
alua
tion
of sa
fety
and
usa
bilit
y ha
ve n
ot y
et b
een
repo
rted
DO
Fs d
egre
es o
f fre
edom
, RoM
rang
e of
mot
ion,
FES
func
tiona
l ele
ctric
al st
imul
atio
n, T
thor
acic

6 F. Anaya et al.
1 3
coded with the sit-to-stand, standing, steeping, and stand to sit stimulation patterns. For the steeping state, the gait event detector determined transitions between early swing, double stance, late swing, and weight acceptance gait phases. At early swing phase, the contralateral knee joint was locked and the ipsilateral knee was unlocked. During double stance, all valves remained in their default state by locking the knees joints. Once the subject pressed the “go” button, the finite automaton shifted to early swing phase where muscle stimu-lation for the ipsilateral leg was initiated. At this point, while the ipsilateral knee mechanics was unlocked to allow the knee to swing freely, the contralateral knee remained locked. During late swing phase, and after an extension threshold was surpassed by the ipsilateral leg, the knee was locked for weight acceptance in stance phase. In this way, the weight acceptance phase ensure that weight was fully accepted prior
to initiating a new step. The individual then initiated the fol-lowing step for the contralateral leg by pressing the “go” but-ton again. Although during testing, the finite automaton con-troller successfully moved through the different states and the subjects showed sufficient joint angles and foot–ground clearance, this hybrid system has been reported to result in high energy cost of gait (del-Alma et al. 2012).
2.1.1.2 Spring‑brake orthosis Unlike those aforementioned technologies, Gharonni et al. (2000, 2001) presented a hybrid orthosis with energy storage (SBO). Here, stimula-tion is provided to the paralyzed muscles while a spring-loaded orthosis store and transfer the energy to produce joint flexion. Therefore, knee flexion during swing phase is achieved by means of the energy stored by stretching a spring which is released from rest whereas hip flexion is achieved by the gravitational force acting upon the system. Consequently, Gharonni et al.’s hybrid orthosis produces maximum possible torque through the stimulated quadri-ceps during knee extension. When excess stimulation is pro-vided to the quadriceps muscles, the spring resists the knee extension and the remaining quadriceps torque is stored in the spring to be discharged later. A break can then contract the spring, discharging its stored energy resulting in knee flexion. A single test on a non-disabled subject was reported using the spring-break orthosis which addresses the knee and hip joint kinematics.
Krishnamoorthy et al. (2008) tested a passive robotic sys-tem and FES on one patient with post stroke hemiparesis.
Fig. 1 Controlled-brake orthosis (CBO). Retrieved from (Goldfarb et al. 2003)
Fig. 2 Ottobock Sensor Walk with surface FES electrodes. Retrieved from (Sharma et al. 2014)
Fig. 3 Overview of the Self-contained exoskeleton. Retrieved from (Chang et al. 2017)

7Hybrid FES–robotic gait rehabilitation technologies: a review on mechanical design, actuation,…
1 3
The robotic orthosis employed is known as Gravity Balanced Orthosis (GBO). GBO is a treadmill-based device which allows intension based ambulation of the patient and opti-mizes the effects of gravity on their limbs (Fig. 4). It also assists knee and hip joint movements with specially designed springs that compensate for the limb segment weights. The springs were mounted at a convenient location on the ortho-sis which was found by calculating the center of mass of the user to fully or partially balance gravity effects throughout the joint motion. The level of gravity balance can be adjusted depending on the user’s need. Since it did not have any actu-ators to generate joint motion it worked as a passive device.
This system used FES to stimulate ankle dorsiflexor muscles during swing phase and plantarflexion muscles to assist knee flexion. Foot switches were used to determine gait phases during treadmill walking. Initial test on the subject was performed to determine the stimulation inten-sity required to produce knee flexion\extension and ankle plantar\dorsiflexion. The results of the preliminary study showed an increase in the patient’s gait parameters such as walking speed, weight bearing capacity of the paretic leg, knee and hip joint angles. And the positive changes were still retained during the 1 month follow up evaluation. The researchers also added that the combination GBO and FES can benefit patients with inadequate hip–knee flexion during swing phase from GBO support and electrical stimulation
can compensate for the inadequate muscle strength to gener-ate plantar-dorsiflexion.
2.1.1.3 Joint‑coupled orthosis On top of the spring-break orthosis, the joint coupled orthosis concept was developed based on the elastic-storage principle, but in this case, the elastic element acts across two joints. Durfee et al. (Kangude et al. 2009, 2010; Durfee and Rivard 2005), developed an energy storing orthosis (ESO) that elicits the hip motion by means of a pneumatically driven actuator which stores and transfers energy from knee extension caused by quadriceps stimulation. Thus, the robotic structure not only governs the locking and unlocking of the exoskeletal joints, but also employs the induced quadriceps muscle power to “push on the orthosis” while storing energy in the process. The power transmission systems are added on commercial orthotics, the Newport 4 Hip System belt, and the Donjoy Legend knee brace. The total weight of the system is 16.82 kg. The system description is as follows: The knee and hip joints are held in flexed positions by the elastic energy storage actua-tors. FES generates energy for knee extension by stimulat-ing the quadriceps and the excess energy generated is stored in the spring and the energy transfer element. This stored energy is then transferred and discharged at the hip joint causing hip extension and enabling forward progression. Lastly, release of the hip and knee joints from the straight-leg position to the initial flexed equilibrium position initi-ates a new step. Pre-clinical evaluation on a single 51 year old male with T12 spinal cord injury was performed during fit and standing tasks. Nevertheless, the outcomes of this test were restricted to those of safety and fitting functions of the orthosis, with no major results on functionality.
A similar approach to Durfee’s Energy Storing Ortho-sis was presented by Farris et al. (2009), where a hybrid FES–robot cooperative control system incorporated two FES-channels with a microprocessor-controlled orthosis for gait rehabilitation. In this orthosis, the flexion of the knee leads to hip flexion as both joints were unidirectionally cou-pled. Additionally, the hybrid orthosis included sensors and modulated friction brakes which worked in combination with FES to provide feedback control of joint trajectories. Quadri-ceps muscles were stimulated by two FES channels due to their easy accessibility and strong contraction. The control-lable friction brakes on the orthosis lock the knee joint dur-ing stance and when the knee joint is unlocked during swing, it also releases the stored energy from the biasing spring which causes the knee to flex; and due to the joint coupling effect, the hip joint also flexes. During the late swing phase, the hip brakes lock the hip joint while the quadriceps mus-cles are stimulated causing knee extension. Once the knee is fully extended, it remains locked during the stance phase of the gait. A simulation of the joint-coupled controlled brake orthosis was conducted on ten healthy subjects to determine
Fig. 4 Gravity Balanced Orthosis (GBO) with FES. Retrieved from (Krishnamoorthy et al. 2008)

8 F. Anaya et al.
1 3
the efficiency of spring and joint coupling to generate hip\knee flexion and if quadriceps stimulation generated suf-ficient power without causing muscle fatigue. The results reported that the knee flexion amplitude stabilized at 85% of the mean amplitude which led to the conclusion that this energy storing method might slow down the onset of muscle fatigue. However, experiments were conducted in healthy individuals only and clinical data on neurologically injured patients has not yet been reported.
2.1.1.4 Variable hip constraint mechanism Audu et al. (2010) introduced a variable constraint hip mechanism (VCHM) intended to be worn in combination with FES. The VCHM consists on a hydraulic mechanism in which double acting hydraulic cylinders were connected to the hip joints via custom rack-and-pinion transmissions (Fig. 5). The hip constrain states are achieved by activating specific valve(s) which lock the hips of the VCHM depending on the phase of gait, therefore allowing free movement when the hips are being stimulated by the FES while restricting the joints movement when support is required. In such manner, the hip joints are coupled during double stance phase and locked against flexion during single stance to prevent undesirable anterior trunk tilt. During swing phase, the hip joints are released to move, allowing the leg to swing passively or be
powered by FES, while producing forward progression. The effect of the hip mechanism was studied in five able-bodied subjects with no history of orthopedic illness or any other ailment that would prejudice their walking abilities. Results showed a reduced normalized hip movement suggesting that the VCHM allows for improved unconstrained hip motion. However, future testing with individuals with paraplegia may produce dissimilar results.
2.1.2 FES and robotic system are both torque generating devices
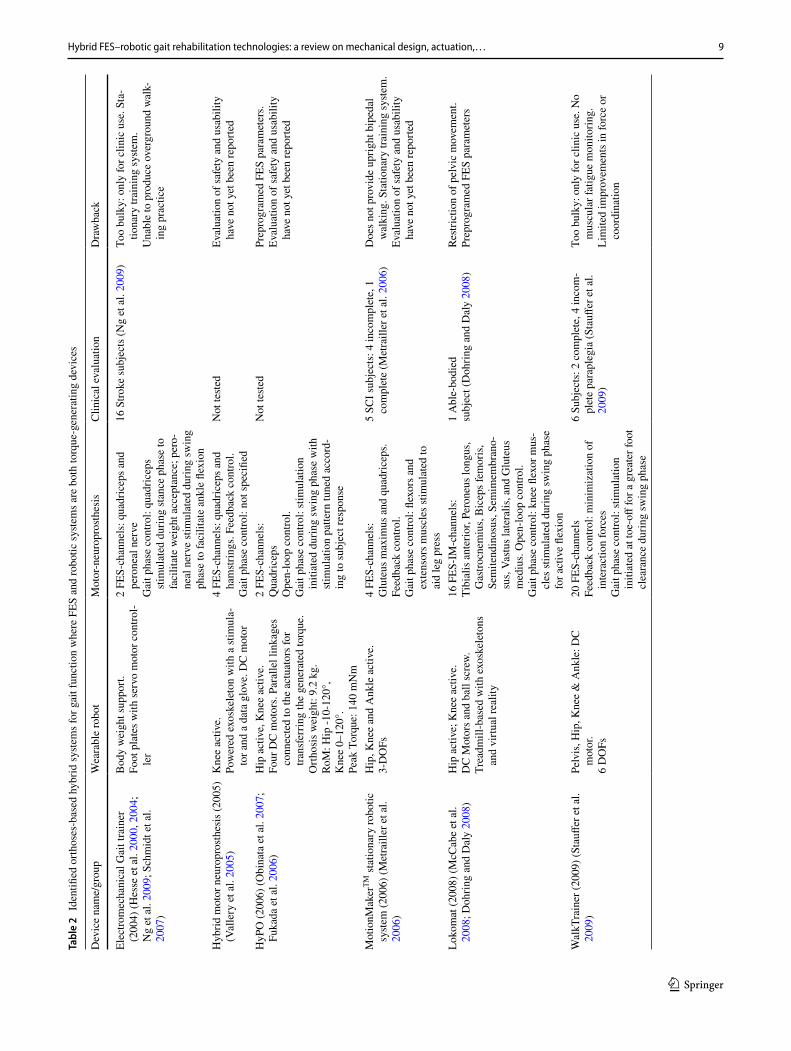
We identified 15 main orthotic-based hybrid technologies for the restoration and support of gait functions where FES and the robotic system are both torque-generating devices (Table 2). With regard to the actuation principle of the wear-able robot joints, hybrid powered wearable robots are clas-sified as either semi-active or fully active (del-Ama et al. 2016). Powered robotic systems for gait rehabilitation often follow the following concept: (1) applying power to the hip, (2) dissipating power at the knee and (3) storing and releas-ing energy at the ankle trough elastic components (Pons et al. 2013). In most existing robotic system designs, electric direct drivers and brushless DC-motor-gearbox combina-tions are mainly employed (Pons et al. 2013).
An electromechanical gait trainer GT II (RehaStim) was developed by Hesse et al. (2000; Hesse 2004). It consists of a BWS system and two-foot plates driven by servo motor controller whose movements simulate symmetric stance and swing (Fig. 6). Ng et al. (2009) tested this device with func-tional electrical stimulation (GT-FES) on 16 stroke patients and compared the results to conventional physiotherapy (CT). The protocol involved 20 min of gait training with GT II and FES was provided simultaneously. Two Chan-nel FES stimulator was linked to the gait trainer control-ler which synchronized the gait phase and the stimulation timings. Subjects received standardized stimulation to the quadriceps during stance phase to facilitate weight accept-ance and the peroneal nerve during swing phase to facili-tate ankle dorsiflexion and knee flexion. The results proved that the GT-FES group showed significant improvement in lower limb strength, mobility, ambulation ability and walk-ing speed as compared to that of CT group.
Vallery et al. (2005) introduced a hybrid motor neuropro-sthesis composed of three parts: an exoskeleton, a stimula-tor, and a data glove for the user interface. The exoskeleton consists of a knee orthosis driven by a DC-motor in combi-nation with a gear box to exert torque on the patient’s knee. The knee angles and angular velocities are fed back to the system for control purposes and the lower thigh is modeled as a pendulum. The control approach proposed is based on a cooperative control, where the low frequency components are given to the motor-neuroprosthesis controller, while the
Fig. 5 Hybrid neuroprosthesis with variable-constraint hip mecha-nism. Retrieved from (Kobetic et al. 2009)
9Hybrid FES–robotic gait rehabilitation technologies: a review on mechanical design, actuation,…
1 3
Tabl
e 2
Iden
tified
orth
oses
-bas
ed h
ybrid
syste
ms f
or g
ait f
unct
ion
whe
re F
ES a
nd ro
botic
syste
ms a
re b
oth
torq
ue-g
ener
atin
g de
vice
s
Dev
ice
nam
e/gr
oup
Wea
rabl
e ro
bot
Mot
or-n
euro
pros
thes
isC
linic
al e
valu
atio
nD
raw
back
Elec
trom
echa
nica
l Gai
t tra
iner
(2
004)
(Hes
se e
t al.
2000
, 200
4;
Ng
et a
l. 20
09; S
chm
idt e
t al.
2007
)
Bod
y w
eigh
t sup
port.
Foot
pla
tes w
ith se
rvo
mot
or c
ontro
l-le
r
2 FE
S-ch
anne
ls: q
uadr
icep
s and
pe
rone
al n
erve
Gai
t pha
se c
ontro
l: qu
adric
eps
stim
ulat
ed d
urin
g st
ance
pha
se to
fa
cilit
ate
wei
ght a
ccep
tanc
e; p
ero-
neal
ner
ve st
imul
ated
dur
ing
swin
g ph
ase
to fa
cilit
ate
ankl
e fle
xion
16 S
troke
subj
ects
(Ng
et a
l. 20
09)
Too
bulk
y: o
nly
for c
linic
use
. Sta
-tio
nary
trai
ning
syste
m.
Una
ble
to p
rodu
ce o
verg
roun
d w
alk-
ing
prac
tice
Hyb
rid m
otor
neu
ropr
osth
esis
(200
5)
(Val
lery
et a
l. 20
05)
Kne
e ac
tive.
Pow
ered
exo
skel
eton
with
a st
imul
a-to
r and
a d
ata
glov
e. D
C m
otor
4 FE
S-ch
anne
ls: q
uadr
icep
s and
ha
mstr
ings
. Fee
dbac
k co
ntro
l.G
ait p
hase
con
trol:
not s
peci
fied
Not
teste
dEv
alua
tion
of sa
fety
and
usa
bilit
y ha
ve n
ot y
et b
een
repo
rted
HyP
O (2
006)
(Obi
nata
et a
l. 20
07;
Fuka
da e
t al.
2006
)H
ip a
ctiv
e, K
nee
activ
e.Fo
ur D
C m
otor
s. Pa
ralle
l lin
kage
s co
nnec
ted
to th
e ac
tuat
ors f
or
trans
ferr
ing
the
gene
rate
d to
rque
.O
rthos
is w
eigh
t: 9.
2 kg
.Ro
M: H
ip -1
0-12
0°,
Kne
e 0–
120°
.Pe
ak T
orqu
e: 1
40 m
Nm
2 FE
S-ch
anne
ls:
Qua
dric
eps
Ope
n-lo
op c
ontro
l.G
ait p
hase
con
trol:
stim
ulat
ion
initi
ated
dur
ing
swin
g ph
ase
with
sti
mul
atio
n pa
ttern
tune
d ac
cord
-in
g to
subj
ect r
espo
nse
Not
teste
dPr
epro
gram
ed F
ES p
aram
eter
s.Ev
alua
tion
of sa
fety
and
usa
bilit
y ha
ve n
ot y
et b
een
repo
rted
Mot
ionM
aker
TM st
atio
nary
robo
tic
syste
m (2
006)
(Met
raill
er e
t al.
2006
)
Hip
, Kne
e an
d A
nkle
act
ive.
3-D
OFs
4 FE
S-ch
anne
ls:
Glu
teus
max
imus
and
qua
dric
eps.
Feed
back
con
trol.
Gai
t pha
se c
ontro
l: fle
xors
and
ex
tens
ors m
uscl
es st
imul
ated
to
aid
leg
pres
s
5 SC
I sub
ject
s: 4
inco
mpl
ete,
1
com
plet
e (M
etra
iller
et a
l. 20
06)
Doe
s not
pro
vide
upr
ight
bip
edal
w
alki
ng. S
tatio
nary
trai
ning
syste
m.
Eval
uatio
n of
safe
ty a
nd u
sabi
lity
have
not
yet
bee
n re
porte
d
Loko
mat
(200
8) (M
cCab
e et
al.
2008
; Doh
ring
and
Dal
y 20
08)
Hip
act
ive;
Kne
e ac
tive.
DC
Mot
ors a
nd b
all s
crew
.Tr
eadm
ill-b
ased
with
exo
skel
eton
s an
d vi
rtual
real
ity
16 F
ES-I
M-c
hann
els:
Tibi
alis
ant
erio
r, Pe
rone
us lo
ngus
, G
astro
cnem
ius,
Bic
eps f
emor
is,
Sem
itend
inos
us, S
emim
embr
ano-
sus,
Vastu
s lat
eral
is, a
nd G
lute
us
med
ius.
Ope
n-lo
op c
ontro
l.G
ait p
hase
con
trol:
knee
flex
or m
us-
cles
stim
ulat
ed d
urin
g sw
ing
phas
e fo
r act
ive
flexi
on
1 A
ble-
bodi
edsu
bjec
t (D
ohrin
g an
d D
aly
2008
)Re
stric
tion
of p
elvi
c m
ovem
ent.
Prep
rogr
amed
FES
par
amet
ers
Wal
kTra
iner
(200
9) (S
tauff
er e
t al.
2009
)Pe
lvis
, Hip
, Kne
e &
Ank
le: D
C
mot
or.
6 D
OFs
20 F
ES-c
hann
els
Feed
back
con
trol:
min
imiz
atio
n of
in
tera
ctio
n fo
rces
Gai
t pha
se c
ontro
l: sti
mul
atio
n in
itiat
ed a
t toe
-off
for a
gre
ater
foot
cl
eara
nce
durin
g sw
ing
phas
e
6 Su
bjec
ts: 2
com
plet
e, 4
inco
m-
plet
e pa
rapl
egia
(Sta
uffer
et a
l. 20
09)
Too
bulk
y: o
nly
for c
linic
use
. No
mus
cula
r fat
igue
mon
itorin
g.Li
mite
d im
prov
emen
ts in
forc
e or
co
ordi
natio
n

10 F. Anaya et al.
1 3
Tabl
e 2
(con
tinue
d)
Dev
ice
nam
e/gr
oup
Wea
rabl
e ro
bot
Mot
or-n
euro
pros
thes
isC
linic
al e
valu
atio
nD
raw
back
Mec
hatro
nic
low
er li
mb
(200
9)
(Pob
oron
iuc
et a
l. 20
09)
Bru
shle
ss D
C se
rvom
otor
.R
ated
torq
ue: 0
.637
Nm
4 D
OFs
6 FE
S-ch
anne
ls:
Qua
dric
eps,
ham
strin
gs a
nd g
lute
al
mus
cles
Ope
n-lo
op c
ontro
l: m
axim
um p
ulse
w
idth
.G
ait p
hase
con
trol:
not s
peci
fied
Not
teste
dFo
r sta
ndin
g-up
, sta
ndin
g an
d si
tting
-do
wn
exer
cise
s onl
y.Pr
epro
gram
ed F
ES p
aram
eter
s.Ev
alua
tion
of sa
fety
and
usa
bilit
y ha
ve n
ot y
et b
een
repo
rted
Vand
erbi
lt In
dego
(201
1) (Q
uint
ero
et a
l. 20
11; H
a et
al.
2016
; Far
ris
et a
l. 20
11; H
a et
al.
2012
)
Hip
& K
nee
activ
e; A
nkle
pas
sive
.Po
wer
ed e
xosk
elet
on w
ith b
rush
less
D
C m
otor
s at b
oth
hip
and
knee
jo
ints
, and
nor
mal
ly-lo
cked
bra
kes
Orth
osis
wei
ght:
12 k
g.Ro
M: H
ip -3
0-10
5°,
Kne
e -1
0-10
5°.
Peak
Tor
que:
40
Nm
4 FE
S-ch
anne
ls:
Qua
dric
eps a
nd h
amstr
ings
Feed
back
con
trol.
Gai
t pha
se c
ontro
l: ha
mstr
ings
sti
mul
ated
to a
id h
ip e
xten
sion
, qu
adric
eps s
timul
ated
to a
id k
nee
exte
nsio
n (s
tanc
e)
3 Su
bjec
tsM
otor
com
plet
e T6
-T10
(Ha
et a
l. 20
16)
Prep
rogr
amed
FES
par
amet
ers
Varia
ble
impe
danc
e kn
ee m
echa
nism
V
IKM
-HN
P (2
011)
(Bul
ea e
t al.
2011
, 201
3a, b
, 201
4)
Kne
e ac
tive.
Line
ar M
R fl
uid
dam
per w
ith fo
ur-
bar l
inka
ge tr
ansm
issi
onO
rthos
is w
eigh
t: 11
.1 k
g.Ro
M: K
nee
-10-
90°,
Peak
Tor
que:
65
Nm
4 FE
S-ch
anne
ls:
Hip
& K
nee
exte
nsor
s.O
pen-
loop
con
trol.
Gai
t pha
se c
ontro
l: no
t spe
cifie
d
1 Su
bjec
t: M
otor
com
plet
e T7
(B
ulea
et a
l. 20
13a,
b)
Prep
rogr
amed
FES
par
amet
ers.
Trig
ger b
utto
n
Hyb
rid-m
ultic
hann
el F
ES W
alki
ng
Ass
istiv
e D
evic
e (2
012)
(Kur
ok-
awa
et a
l. 20
12)
Hip
act
ive,
act
uate
d w
ith c
om-
pres
sed
air a
ctua
tor
8 FE
S-ch
anne
ls:
Gas
trocn
emiu
s, so
leus
, tib
ialis
ant
e-rio
r and
qua
dric
eps.
Ope
n-lo
op c
ontro
l.G
ait p
hase
con
trol:
gastr
ocne
-m
ius,
sole
us, a
nd ti
bial
is a
nter
ior
stim
ulat
ed d
urin
g in
itial
swin
g to
aid
kne
e fle
xion
; qua
dric
eps
stim
ulat
ed d
urin
g st
ance
pha
se to
st
abili
ze k
nee
join
t
7 H
ealth
y su
bjec
ts2
SCI p
atie
nts
Inco
mpl
ete
C5
(Kur
okaw
a et
al.
2012
)
Prep
rogr
amed
FES
par
amet
ers
Lim
ited
impr
ovem
ents
in h
ip a
nd
ankl
e jo
int k
inem
atic
s.
iLeg
low
er li
mb
reha
bilit
atio
n ro
bot
(201
3) (C
hen
et a
l. 20
13)
Hip
act
ive;
Kne
e ac
tive
Leg
robo
t sys
tem
2-D
OFs
4 FE
S-ch
anne
ls:
Glu
teus
max
imus
& q
uadr
icep
s fe
mor
is.
Feed
back
con
trol.
Gai
t pha
se c
ontro
l: no
t spe
cifie
d
Not
teste
dD
oes n
ot p
rovi
de u
prig
ht b
iped
al
wal
king
. Sta
tiona
ry tr
aini
ng sy
stem
.Ev
alua
tion
of sa
fety
and
usa
bilit
y ha
ve n
ot y
et b
een
repo
rted

11Hybrid FES–robotic gait rehabilitation technologies: a review on mechanical design, actuation,…
1 3
Tabl
e 2
(con
tinue
d)
Dev
ice
nam
e/gr
oup
Wea
rabl
e ro
bot
Mot
or-n
euro
pros
thes
isC
linic
al e
valu
atio
nD
raw
back
Sem
i-act
ive
hybr
id o
rthos
isSE
AH
O (2
014)
(Kirs
ch, e
t al.
2014
)H
ip a
ctiv
e; K
nee
sem
i-act
ive;
Ank
le
pass
ive
Elec
tric
mot
ors l
ocat
ed
at th
e hi
p jo
ints
, and
wra
p sp
ring
clut
ches
atta
ched
at t
he k
nee
join
ts.
Peak
Tor
que:
40
Nm
.2D
OFs
6 FE
S-ch
anne
ls:
Gas
trocn
emiu
s, qu
adric
eps,
and
ham
strin
gs.
Ope
n lo
op –
Ban
g-ba
ng c
ontro
l (o
nly
on–o
ff st
ates
).G
ait p
hase
con
trol:
gastr
ocne
miu
s sti
mul
ated
dur
ing
stan
ce p
hase
to
aid
kne
e ex
tens
ion;
qua
dric
eps
and
ham
strin
gs st
imul
ated
dur
ing
swin
g ph
ase
to a
id k
nee
flexi
on
Not
teste
dPr
epro
gram
ed F
ES p
aram
eter
s. St
imul
atio
n am
plitu
de e
qual
s to
max
imum
con
tract
ion
stim
ulat
ion.
Eval
uatio
n of
safe
ty a
nd u
sabi
lity
have
not
yet
bee
n re
porte
d
Kin
esis
(201
4) (d
el-A
ma
et a
l. 20
14,
2015
)K
nee
activ
e; A
nkle
pas
sive
Con
trolle
r- 4
mai
n co
mpo
nent
s: (1
) a
robo
tic o
r joi
nt ro
botic
, (2)
a F
ES
cont
rolle
r, (3
) a m
uscl
e fa
tigue
es
timat
or (M
FE) a
nd (4
) a fi
nite
-st
ate
mac
hine
(FSM
).D
C fl
at m
otor
s.Ro
M: K
nee
5-12
0°.
1 D
OFs
4 FE
S-ch
anne
ls:
Qua
dric
eps a
nd h
amstr
ings
Feed
back
con
trol.
PID
con
trol o
f kn
ee e
xten
sors
mus
cles
. ILC
for
the
knee
flex
or m
uscl
es.
Gai
t pha
se c
ontro
l: no
t spe
cifie
d
4 H
ealth
y su
bjec
ts (d
el-A
ma
et a
l. 20
14).
3 M
otor
inco
mpl
ete
SCI (
del-A
ma
et a
l. 20
14, 2
015)
PID
con
trolle
r dec
reas
es st
imul
atio
n pe
rform
ance
and
inte
rfere
with
the
ILC
con
trol t
ask
FEX
O K
nee
(201
4) (R
en e
t al.
2014
)K
nee
Act
ive.
DC
Mot
or, P
ID c
ontro
ller.
Nom
inal
torq
ue o
f 0.4
Nm
.Ro
M: K
nee
-80-
80°.
1-D
OFs
4 FE
S-ch
anne
ls:
Vasti
and
Ham
strin
gs.
Feed
forw
ard
-loop
con
trol.
Gai
t pha
se c
ontro
l: no
t spe
cifie
d
Not
teste
dSy
stem
eva
luat
ed o
nly
in si
tting
po
sitio
n.Ev
alua
tion
of sa
fety
and
usa
bilit
y ha
ve n
ot y
et b
een
repo
rted
Hip
-Kne
e ex
oske
leto
n an
d A
nkle
m
otio
n in
duce
d by
FES
syste
m
(201
6) (T
u et
al.
2016
)
Hip
act
ive;
Kne
e ac
tive.
Pneu
mat
ic m
uscl
e co
ntro
lled
by u
se
of a
pro
porti
onal
val
ve w
ith a
pre
s-su
re se
nsor
.Ro
M: H
ip -2
5-40
°,K
nee
-85-
0°.
Peak
Tor
que:
Hip
60N
m, K
nee
40N
m.
2 D
OFs
3 FE
S-ch
anne
lsTi
bial
is a
nter
ior,
sole
us, g
astro
cne-
miu
s.Fe
edba
ck c
ontro
l.G
ait p
hase
con
trol:
not s
peci
fied
Not
teste
dTo
o bu
lky:
onl
y fo
r clin
ic u
se.
Lim
ited
impr
ovem
ents
in h
ip a
nd
knee
join
t kin
emat
ics.
Eval
uatio
n of
safe
ty a
nd u
sabi
lity
have
not
yet
bee
n re
porte
d
DO
Fs d
egre
es o
f fre
edom
, RoM
rang
e of
mot
ion,
FES
func
tiona
l ele
ctric
al s
timul
atio
n, T
thor
acic
, C c
ervi
cal,
DC
dire
ct c
urre
nt, S
CI s
pina
l cor
d in
jury
, MR
mag
neto
rheo
logi
cal,
ILC
iter
ativ
e le
arni
ng c
ontro
l, PI
D p
ropo
rtion
al–i
nteg
ral–
deriv
ativ
e
12 F. Anaya et al.
1 3
high frequencies are directed to the motor controller (Fig. 7). In this way, each actuator is exploited individually regarding its own requirements, resulting in improvements in perfor-mance, energy consumption and muscle fatigue. However, validation results have not yet been published.
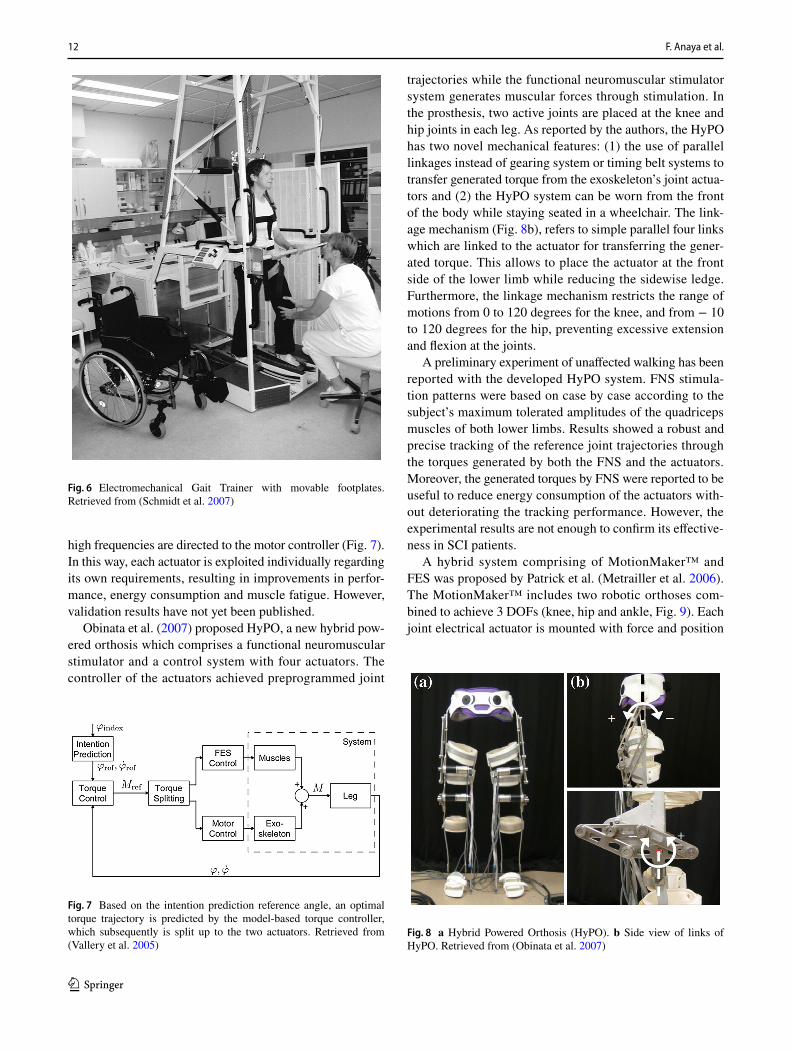
Obinata et al. (2007) proposed HyPO, a new hybrid pow-ered orthosis which comprises a functional neuromuscular stimulator and a control system with four actuators. The controller of the actuators achieved preprogrammed joint
trajectories while the functional neuromuscular stimulator system generates muscular forces through stimulation. In the prosthesis, two active joints are placed at the knee and hip joints in each leg. As reported by the authors, the HyPO has two novel mechanical features: (1) the use of parallel linkages instead of gearing system or timing belt systems to transfer generated torque from the exoskeleton’s joint actua-tors and (2) the HyPO system can be worn from the front of the body while staying seated in a wheelchair. The link-age mechanism (Fig. 8b), refers to simple parallel four links which are linked to the actuator for transferring the gener-ated torque. This allows to place the actuator at the front side of the lower limb while reducing the sidewise ledge. Furthermore, the linkage mechanism restricts the range of motions from 0 to 120 degrees for the knee, and from − 10 to 120 degrees for the hip, preventing excessive extension and flexion at the joints.
A preliminary experiment of unaffected walking has been reported with the developed HyPO system. FNS stimula-tion patterns were based on case by case according to the subject’s maximum tolerated amplitudes of the quadriceps muscles of both lower limbs. Results showed a robust and precise tracking of the reference joint trajectories through the torques generated by both the FNS and the actuators. Moreover, the generated torques by FNS were reported to be useful to reduce energy consumption of the actuators with-out deteriorating the tracking performance. However, the experimental results are not enough to confirm its effective-ness in SCI patients.
A hybrid system comprising of MotionMaker™ and FES was proposed by Patrick et al. (Metrailler et al. 2006). The MotionMaker™ includes two robotic orthoses com-bined to achieve 3 DOFs (knee, hip and ankle, Fig. 9). Each joint electrical actuator is mounted with force and position
Fig. 6 Electromechanical Gait Trainer with movable footplates. Retrieved from (Schmidt et al. 2007)
Fig. 7 Based on the intention prediction reference angle, an optimal torque trajectory is predicted by the model-based torque controller, which subsequently is split up to the two actuators. Retrieved from (Vallery et al. 2005)
Fig. 8 a Hybrid Powered Orthosis (HyPO). b Side view of links of HyPO. Retrieved from (Obinata et al. 2007)

13Hybrid FES–robotic gait rehabilitation technologies: a review on mechanical design, actuation,…
1 3
sensor for the control of FES. 20-channel self-designed FES stimulator called “StimWave2” with closed loop control is employed in this system. The hybrid system was evaluated on five SCI patients who underwent 2 months training with the system. The training program included 1 h of leg press exercise once in 2 days. The FES stimulated the extensor and flexor muscles in the leg to aid leg press. The targeted muscles were gluteus maximus, quadriceps and gastrocne-mius, hamstrings and tibialis anterior. The results showed to increase the muscle strength of the patients. After the train-ing, three of the participants were able to voluntarily exert 150 N of force during leg press which they were unable to do earlier. Though the FES displayed positive results, there were no clear benefits of the robotic system mentioned in the paper.
Two attempts to synchronize the Lokomat gait robot system with a multichannel functional electrical stimulator were also found. Firstly, McCabe et al. (2008) combined the Lokomat gait robot system (Hocoma Inc.) with a multichan-nel functional electrical simulator using intramuscular elec-trodes (FES-IM) to provide a more coordinated gait training (Fig. 10). Lokomat system comprised of a robotic orthosis, body weight support (BWS) system and a treadmill which provides the subjects with knee joint, hip joint and sagittal plane motion. The FES-IM system comprised of eight intra-muscular electrodes placed on tibialis anterior, semimem-branosus, peroneus longus, vastus lateralis, gastrocnemius, biceps femoris, gluteus medius, and semitendinosus, in both legs. Custom FES-IM patterns were generated for each sub-ject to eliminate deficient components of stance and swing phases of gait and keep the gait pattern as close to normal as possible. Six Ischemic stroke subjects participated in the evaluation of the system. During the initial session, each subject was trained with the Lokomat alone to record the swing and stance durations for the customization of FES-IM stimulation patterns. During the next session, the Lokomat
and FES-IM were tested together. The results proved the fea-sibility of delivering FES-IM patterns simultaneously with Lokomat assistance. The Lokomat provided close to normal movements during the swing phase knee flexion while FES-IM stimulated the knee flexor muscles for active flexion of the knee joint. The same combined effect was also noted during the stance phase.
Secondly, Dohring and Daly (2008) reported the auto-matic synchronization of the Lokomat robotic gait orthosis and functional electrical stimulation using intramuscular electrodes (FES-IM). In this study, the Lokomat was syn-chronized with the stimulation of eight targeted muscles during the gait pattern by making use of the pulse produced by the Lokomat at each right heel strike. Results from two 30-min test trails in one able-bodied subject revealed a more feasible, accurate and repeatable synchronization of the FES gait patterns than manually delivered FES during Lokomat training.
Despite the recent achievements in integrating the Lokomat system with FES control, earlier studies (Hidler et al. 2009; Regnaux et al. 2008) have shown that Lokomat restricts the pelvic rotation and weight shifting between legs, which results in abnormal acceleration and deacceleration during the swing phase. Furthermore, due to the linkages in the Lokomat, the upper extremity motion is also restricted, which makes it difficult to swing the arms while walking.
Stauffer et al. (2009) developed the WalkTrainer as a hybrid orthosis with feedback FES control based on the Cyberthosis concept, which relies on the active participation of the subject’s muscles while the motions applied by the orthoses must closely mimic natural movements (Fig. 11). With this purpose, the Walk trainer consists of leg and pelvic
Fig. 9 MotionMakerTM prototype with an able-bodied subject. Retrieved from (Metrailler et al. 2006)
Fig. 10 Combination of Lokomat and multichannel FES with intra-muscular electrodes. Retrieved from (Schuck et al. 2012) and (Querry et al. 2008)

14 F. Anaya et al.
1 3
orthosis, an active BWS system and motorized wheels for over ground ambulation. The leg orthosis is designed with the idea of having a parallel mechanical leg that is placed just behind the human leg. Linkages connect the powered leg to the device and modified shoes interface the feet with the motor driver. The linear axis unit control the flexion and extension of the hip joint while the knee joint is actuated by a two-stage crank and connecting rod systems. Utilizing the same actuation strategy as the knee, the movement of ankle joint is powered by parallelogram.
The principal benefit of this leg orthosis consists of hav-ing the mechanical parts, cables and motors at the back of the machine, allowing the arms to swing freely. Six subjects with paraplegia participated in the preliminary evaluation of the WalkTrainer. The experiments consisted of short term preliminary clinical trial of 60 min a week training over 3 months which resulted in a drop in the Ashworth Spasticity Scale but with no significant increases in force or coordination.
Poboroniuc et al. (2009) designed a mechatronic lower limb to replicate the lower limbs of the human body, espe-cially the sitting and standing motions (Fig. 12). It consists of five lower limb joints which are actuated by a brushless servomotor driven by servo drivers providing position, velocity and torque control modes. The robotic structure also includes a functional electrical stimulator module to provide active joint movements. The electrical stimulations to the muscles are given in increasing and decreasing pulse widths to gluteal, quadriceps and hamstrings depending on the sitting or standing task. However, this system has not been tested on human subjects.
Vanderbilt exoskeleton, developed by Quintero et al. in 2011, is a power exoskeleton for gait rehabilitation in per-sons with paraplegia (Quintero et al. 2011). It consists of hip and knee joint actuators and weighs around 12kgs. The prototype of the powered orthosis is shown in Fig. 13, which
intends to deliver power-driven support in the sagittal plane at the hip and knee joints. Individual joints are driven by a brushless DC motor which provides a maximum continu-ous torque around 12 Nm. The knee actuators additionally
Fig. 11 The CAD model of the active bodyweight support system and the prototype of the WalkTrainer. Retrieved from (Stauffer et al. 2009)
Fig. 12 The schematic structure of a mechatronic lower limb. Retrieved from (Poboroniuc et al. 2009)
Fig. 13 Powered orthosis prototype. Retrieved from (Quintero et al. 2011)
15Hybrid FES–robotic gait rehabilitation technologies: a review on mechanical design, actuation,…
1 3
employ electrically driven locked brakes, such that the joints continue to be locked in case of power failure and during the stance phase of gait, and are freed during the swing phase of gait. The hip joint presents a range of motion of 105° in flexion and 30° in extension, while the knee joint presents a range of motion of 105° in flexion and 10° in extension. The proposed orthosis is aimed to be worn in combination with a passive ankle foot orthosis, to provide stability to the ankle and to correct foot drop during the swing phase of gait.
The orthosis controller consists of state-flow system with the following four states: (1) right step forward, (2) double-support with right foot forward, (3) left step forward and 4) double-support with left foot forward. The cooperative controller combining FES with the exoskeleton is based on the idea that the hamstring should assist the exoskeleton to extend the hip when extension torques are required while not disturbing the system when flexion torques are desired. Additionally, quadriceps generate extension torques about the knee. To achieve this, the controller employs a constant activation level and varies the timing based on the finite-state machine and the torques on the hip and knee joints from previous steps. The hamstrings are stimulated in their corresponding stance phases and during double support due to the significant amount of hip extension required by the exoskeleton to maintain torso stability while the quadriceps are stimulated during the swing phase. Experiments were performed on 3 SCI patients to evaluate the performance of the controller. Results showed good trajectory tracking and considerable reduction of 20% on the motor power require-ments in both the knee and hip joints (Ha et al. 2016).
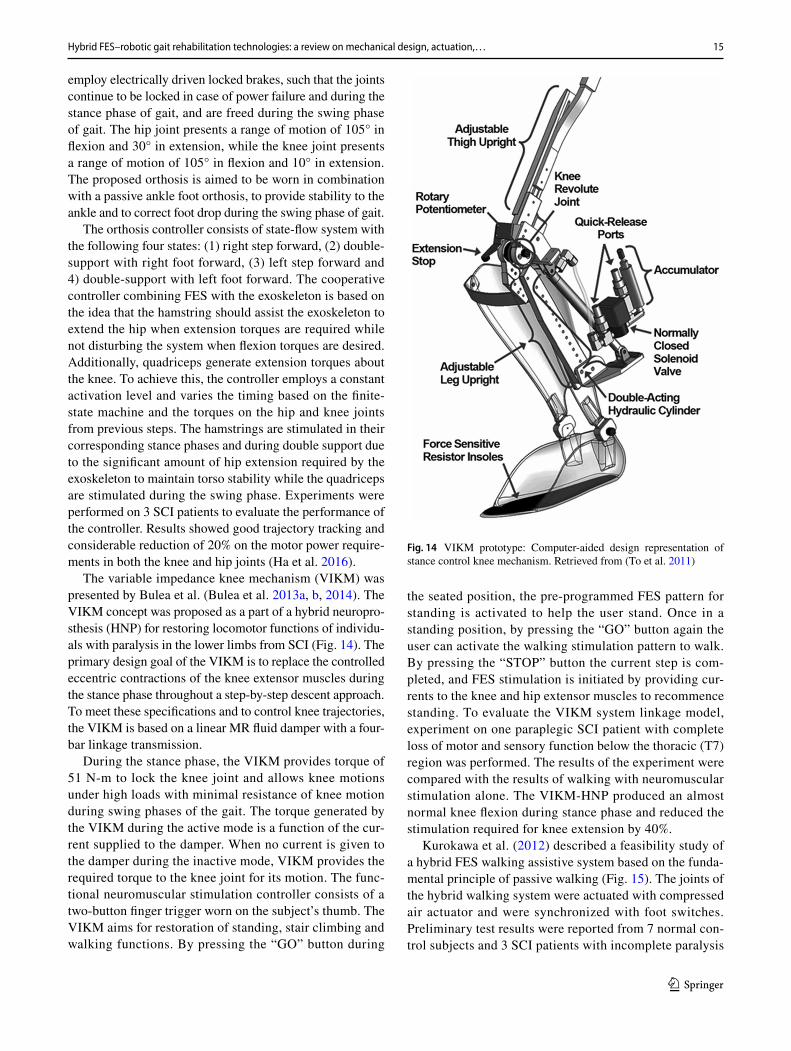
The variable impedance knee mechanism (VIKM) was presented by Bulea et al. (Bulea et al. 2013a, b, 2014). The VIKM concept was proposed as a part of a hybrid neuropro-sthesis (HNP) for restoring locomotor functions of individu-als with paralysis in the lower limbs from SCI (Fig. 14). The primary design goal of the VIKM is to replace the controlled eccentric contractions of the knee extensor muscles during the stance phase throughout a step-by-step descent approach. To meet these specifications and to control knee trajectories, the VIKM is based on a linear MR fluid damper with a four-bar linkage transmission.
During the stance phase, the VIKM provides torque of 51 N-m to lock the knee joint and allows knee motions under high loads with minimal resistance of knee motion during swing phases of the gait. The torque generated by the VIKM during the active mode is a function of the cur-rent supplied to the damper. When no current is given to the damper during the inactive mode, VIKM provides the required torque to the knee joint for its motion. The func-tional neuromuscular stimulation controller consists of a two-button finger trigger worn on the subject’s thumb. The VIKM aims for restoration of standing, stair climbing and walking functions. By pressing the “GO” button during
the seated position, the pre-programmed FES pattern for standing is activated to help the user stand. Once in a standing position, by pressing the “GO” button again the user can activate the walking stimulation pattern to walk. By pressing the “STOP” button the current step is com-pleted, and FES stimulation is initiated by providing cur-rents to the knee and hip extensor muscles to recommence standing. To evaluate the VIKM system linkage model, experiment on one paraplegic SCI patient with complete loss of motor and sensory function below the thoracic (T7) region was performed. The results of the experiment were compared with the results of walking with neuromuscular stimulation alone. The VIKM-HNP produced an almost normal knee flexion during stance phase and reduced the stimulation required for knee extension by 40%.
Kurokawa et al. (2012) described a feasibility study of a hybrid FES walking assistive system based on the funda-mental principle of passive walking (Fig. 15). The joints of the hybrid walking system were actuated with compressed air actuator and were synchronized with foot switches. Preliminary test results were reported from 7 normal con-trol subjects and 3 SCI patients with incomplete paralysis
Fig. 14 VIKM prototype: Computer-aided design representation of stance control knee mechanism. Retrieved from (To et al. 2011)

16 F. Anaya et al.
1 3
at C5 level. Electrical stimulations were delivered to the gastrocnemius, soleus, and tibialis anterior for stiffness control of the ankle joint and for assisting the knee flexion in the initial swing. Quadriceps were stimulated for sta-bilizing the knee joint during stance phase. M-wave was monitored for control and fatigue monitoring purposes. However, results of this approach were controversial, as only certain improvements were reported in ankle and hip kinematics.
Chen et al. (2013) proposed a 2 DOF (hip, knee) self-developed exoskeleton for lower limb rehabilitation. The joints of the exoskeleton were equipped with DC motors, encoders, and torque sensors to drive the joints. The leg-robot system is simplified as shown in Fig. 16. The EMG measurements detect the voluntary movement intensions of the patients, depending on which the FES module generates the stimulation pattern for contracting the gluteous maxi-mums and quadriceps femoris to produce torque at the hip and knee joints, respectively. The control approach of this hybrid robot was split into two components, the impedance control, and the FES control. The mass-damper-spring rela-tionship between force and position, determined during leg
press exercises, helps the impedance controller to produce the desired active compliance on the robot. The FES control-ler generates the desired torque at the joints and controls the intensity of stimulation depending on the need. Although the authors make a promising research on FES-assisted strategy combined with impedance control for conducting leg press exercise, validation results of this interesting approach have not yet been presented.
A semi-active hybrid orthosis (SEAHO) was presented by Kirsch et al. (2014). SEAHO, shown in Fig. 17, consists of three main components: electric motors, FES and wrap spring clutches. The DC-motors, which are placed at the hip joints, can discharge up to 40Nm to produce hip flex-ion while plantar flexion of the foot, knee extension and knee flexion which is produced by electrically stimulating the gastrocnemius, quadriceps muscle and the hamstrings, respectively. The stimulation parameters used for each muscle are preprogrammed as a function of the maximum tolerated intensity, which may lead to fatigue. The relative triggering of the stimulation for the three muscle groups is strictly defined by the hip angles. The final components of the SEAHO refers to the wrap spring clutches attached at the knee joints. With the goal to prevent knee flexion when locked, while still allowing a certain amount of extension, the wrap spring clutch is only unlocked when knee flexors are stimulated. This feature reduces the energy demand of the user to maintain standing position between steps or to maintain the stance leg extension during the step. For the initial device testing, only three states were explored in an able-bodied subject. Since the subject started the experiment in standing position with both feet together, the first state was a half-step. The other two states were defined for both
Fig. 15 Hybrid multichannel electrical stimulator. Retrieved from (Kurokawa et al. 2012)
Fig. 16 Photograph of the prototype of the rehabilitation robot and the simplified model, where qii s the angle for joint i; mr
i , mh
i and li
represent the mass of the robot, the mass of the leg and the length for link i, respectively. Fr2h and Fh2r represent the interaction forces between the robot and the human leg. Retrieved from (Chen et al. 2013)
Fig. 17 A semi-active hybrid orthosis (SEAHO). Retrieved from (Kirsch et al. 2014)

17Hybrid FES–robotic gait rehabilitation technologies: a review on mechanical design, actuation,…
1 3
left and right step. The results of the initial testing suggested that the device is ready for testing in paraplegic subjects with the addition of inertial measurements units (IMU) for the implementation of feedback control of the electrical stimu-lation based on the knee angles. However, to the best of our knowledge, such a protocol has not been developed yet.
Another hybrid wearable robot reported in 2014 is Kinesis, a knee–ankle–foot exoskeleton consisting of an active actuator at the knee and a passive elastic actuator at the ankle, which prevents drop-foot during swing phase (Fig. 18). The system also interfaces with a PC-controlled stimulator (Rehastim, Hasomed GmbH) for biphasic cur-rent controlled stimulation to knee extensors (rectus femoris and vastus lateralis) and flexors (semitendinosus and biceps femoris) muscles. The kinesis controller consists of electri-cal muscle stimulator and the robotic controller. The FES control is achieved by means of an iterative learning con-trol algorithm for knee flexor muscles and a PID controller for knee extensor muscles, which allows customizing FES parameters through a closed-loop control of stimulation. The robotic joints controller corresponds to an admittance con-troller, which permits the regulation of robotic assistance to the joints during gait. The Kinesis was evaluated on three SCI patients, in which improvements in gait profiles were reported during treatment and follow-up (del-Ama et al. 2014). Despite evaluation of the Kinesis showing good patients acceptance with a good perception over the device, it was reported that the PID controller decreased the stimula-tion performance by interfering with the iterative learning control of the FES parameters.
FEXO Knee proposed by Ren et al. is a powered hybrid exoskeleton which targets single joint rehabilitation for the right knee (Ren et al. 2014). It has a self-developed knee exoskeleton and a commercial functional electrical stimu-lator- RehaStim 2 (Hasomed, Germany). The system also consists of a central pattern generator which predicts the phases by eliminating phase conflicts between the human
shank and exoskeleton to generate the reference trajectories and provide FES at the right phases (Fig. 19).
To provide active torque for the knee joint, two muscle groups- Vasti and Hamstring, are stimulated by FES. The exoskeleton uses DC servo motor to generate torque for knee flexion and extension. A model-based feedforward controller was designed to control the FES parameters (pulse width), whereas the control of the knee joint trajectory of the exo-skeleton was achieved by a proportional-integral-derivative (PID) controller. Preliminary tests were performed on four healthy subjects where the results showed that the phase regulation based on a biologically inspired control strat-egy, maintains the synchronization between the FES refer-ence trajectory and the actual knee angle trajectory. There were unexpected torque conflictions when the FEXO knee exceeded the desired maximum trajectory. The mutual
Fig. 18 Kinesis hybrid exoskel-eton and cooperative control approach. Retrieved from (del-Ama et al. 2014)
Fig. 19 Schematic of the exoskeleton in FEXO Knee. Eight main components are displayed: (1) DC servo motor, (2) driven pulleys, (3) Bowden cables, (4) encoder, (5) shank wraps, (6) interactive force sensors, (7) linear springs, and (8) tension sensors. Retrieved from (Ren et al. 2014)

18 F. Anaya et al.
1 3
torque in flexion and extension of the knee varied in each trial due to different stimulation response of the two muscle groups. As the experiments were performed in a sitting posi-tion the results and parameters may vary drastically with over ground walking experiments. Further trials with para-plegic subjects need to be performed for proper evaluation of the system.
Lastly, Tu et al. (1759; 2016) proposed a lower limb exo-skeleton system with a treadmill and BWS system (Fig. 20). Each pneumatic limb has two degrees of freedom allow-ing flexion and extension of knee and hip joints. A pair of pneumatic muscle (Festo, MAS-40) actuate the joints where inflation/deflation is controlled by a proportional valve with pressure sensor. The CVRC algorithm was employed to con-trol the hip and knee trajectories for treadmill-based gait training, whereas FES stimulation signals control ankle movement. Electrical stimulation was delivered to the tibi-alis anterior, soleus, and gastrocnemius under closed-loop control. One single healthy subject participated in the test-ing of the model-based hybrid cooperative control. The trajectory tracking errors did not show obvious differences between 2 phases of training of 0–5 s and 50–55 s, respec-tively at the hip, knee and ankle joints. The results of this study suggest that pneumatic muscle is a feasible approach in developing lower limb rehabilitation robots as it is light-weight and a low-cost actuator. However, future research in this approach is sorely needed.
2.2 Technical overview of non‑orthosis based hybrid systems, including robotic footplates systems, mobile platforms, cycling wheelchairs and related technologies
Apart from those orthotic-based technologies, technologies such as robotic footplates systems, pelvic-supporting robots,
treadmill based rehabilitation technologies and cycling wheelchairs have also been reported. We identified 5 main robots which incorporate FES for lower limb rehabilitation (Table 3).
A passive therapeutic arm to support the pelvis dur-ing treadmill training of gait with FES was introduced by Cikajlo et al. (2007) in 2007. The passive therapeutic arm was intended to regulate and stabilize the pelvis move-ments during walking in a treadmill. It consists of a steel cylinder, a vertical rod, two hinge joints and a pelvic belt fixed to a horizontal rod (Fig. 21). The pelvic belt was designed to provide balancing force when subjects deviate vertically in sagittal and frontal planes, depending on the adjusted stiffness, allowing physiological rotation of the pelvis. Both hinge joints were passive and permit vertical support.
The FES gait pattern was determined via a shank accel-eration sensor. At the end of terminal swing, the stored accelerations were recorded and compared with a reference physiological acceleration. Based on the comparison output, FES intensity was decreased with a minimal FES intensity of 50%, or increased up to 10%. The FES stimulation was then applied to the peroneal nerve and stopped at the end of the swing phase. An initial clinical assessment of the passive therapeutic arm was completed on a single subject with chronic incomplete SCI (T10). The experimental trial resulted in moderate improvements of gait performance in the studied subject. However, the training period was short-ened because of the appearance of muscle fatigue induced by FES stimulation. The subject was unable to complete the expected gait exercises during walking on the treadmill and the experiment was interrupted.
Kuznetsov et al. (2013) tested a Robotic Tilt Table Sys-tem (Erigo, Hocoma AG, Switzerland) with FES, naming it ROBO-FES. The system consists of a tilting stretcher which can be tiltled between 0° and 80° and foot plates with springs to perform stepping motions. This device is used for mobilization out of bed, body verticalization, and rhythmic motions with cyclic loading of the leg.
A six-channel FES stimulator (Motionstim 8, Medel GmbH, Germany) was incorporated with the robotic system. Biceps femoris and quadriceps femoris of both legs were stimulated during leg flexion and gastrocnemius muscles of both legs were stimulated during leg extension. Intensity of the stimulation was maintained in a range between 5 and 100 mA. This system was tested on 73 hemiparetic ischemic stroke survivors where 38 were treated with ROBO-FES (Fig. 22) and 35 with ROBO and no FES. The study showed training with ROBO-FES may increase leg strength, cerebral blood flow and blood pressures as compared to the training without FES.
Ye et al. (2014) introduced a rehabilitation system for hemiplegic patients based on a pelvis-supporting robotic
Fig. 20 Hip-Knee exoskeleton system concept diagram. Retrieved from (Tu et al. 2016)

19Hybrid FES–robotic gait rehabilitation technologies: a review on mechanical design, actuation,…
1 3
Tabl
e 3
Iden
tified
robo
tic fo
otpl
ates
syste
ms,
mob
ile p
latfo
rms,
and
cycl
ing
syste
ms f
or g
ait f
unct
ion
with
FES
FES
func
tiona
l ele
ctric
al st
imul
atio
n, T
thor
acic
, VD
C v
olts
of d
irect
cur
rent
Dev
ice
nam
e/gr
oup
Wea
rabl
e ro
bot
Mot
or-n
euro
pros
thes
isC
linic
al e
valu
atio
nD
raw
back
Pass
ive
ther
apeu
tic a
rm fo
r pel
vis
supp
ort (
2007
) (C
ikaj
lo e
t al.
2007
)St
eel c
ylin
der w
ith a
djus
tabl
e sti
ff-ne
ss h
elic
alsp
ring,
ver
tical
rod,
two
hing
e jo
ints
an
d pe
lvic
bel
t
2 FE
S-ch
anne
ls: P
eron
eal n
erve
Feed
back
con
trol.
Gai
t pha
se c
ontro
l: pe
rone
al n
erve
sti
mul
ated
dur
ing
the
swin
g ph
ase
1 Su
bjec
t: T1
0 (C
ikaj
lo e
t al.
2007
)D
oes n
ot p
rovi
de p
ower
to jo
ints
.Li
mite
d to
the
pelv
is su
ppor
t
ROBO
-FES
(201
3) (K
uzne
tsov
et a
l. 20
13)
Foot
plat
es w
ith sp
rings
.M
obili
zatio
n, b
ody
verti
caliz
atio
n,
cycl
ic lo
adin
g of
leg
6 FE
S-ch
anne
ls: B
icep
s fem
o-ris
, gas
trocn
emiu
s. St
imul
atio
n be
twee
n 5
and
100
mA
.O
pen-
loop
con
trol.
Gai
t pha
se c
ontro
l: bi
ceps
fem
oris
an
d qu
adric
eps f
emor
is st
imul
ated
du
ring
leg
flexi
on; g
astro
cnem
ius
stim
ulat
ed d
urin
g le
g ex
tens
ion
38 h
emip
aret
ic is
chem
ic st
roke
su
bjec
ts (K
uzne
tsov
et a
l. 20
13)
Prep
rogr
amed
FES
par
amet
ers.
Doe
s not
pro
vide
upr
ight
bip
edal
w
alki
ng
Pelv
is su
ppor
t rob
ot (2
013)
(Ye
et a
l. 20
13, 2
014;
)Ro
bot b
ase
and
a pe
lvic
supp
ort
mec
hani
sm4
FES-
chan
nels
:Q
uadr
icep
s and
tibi
alis
ant
erio
r.O
pen-
loop
con
trol.
Gai
t pha
se c
ontro
l: qu
adric
eps a
nd
tibia
lis a
nter
ior s
timul
ated
dur
ing
swin
g ph
ase
Not
teste
dD
oes n
ot p
rovi
de p
ower
to k
nee
and
ankl
e jo
ints
.Pr
epro
gram
ed F
ES p
aram
eter
s.Ev
alua
tion
of sa
fety
and
usa
bilit
y ha
ve
not y
et b
een
repo
rted
Prof
hand
(201
3) (W
atan
abe
et a
l. 20
13; W
atan
abe
and
Kar
asaw
a 20
16)
Peda
led
whe
elch
air p
rope
lled
by th
e lo
wer
lim
bs4
FES-
chan
nels
.O
pen-
loop
con
trol.
Gai
t pha
se c
ontro
l: qu
adric
eps
fem
oris
stim
ulat
ed d
urin
g sw
ing
phas
e to
geth
er w
ith h
amstr
ings
of
the
cont
rala
tera
l sid
e to
aid
kne
e ex
tens
ion
and
cont
rala
tera
l kne
e fle
xion
Not
teste
dD
oes n
ot p
rovi
de p
ower
to jo
ints
.C
anno
t giv
e ph
ysic
al su
ppor
t to
knee
an
d hi
p jo
ints
.Pr
epro
gram
ed F
ES p
aram
eter
s.D
oes n
ot p
rovi
de u
prig
ht b
iped
al
wal
king
.Ev
alua
tion
of sa
fety
and
usa
bilit
y ha
ve
not y
et b
een
repo
rted
Mot
oriz
ed F
ES-c
yclin
g te
st be
d (2
017)
(Bel
lman
et a
l. 20
17)
Ank
le a
ctiv
e.C
omm
erci
ally
avai
labl
e re
cum
-be
nt tr
icyc
le (T
erra
Trik
e Ro
ver)
m
odifi
ed w
ith a
24
VD
C m
otor
and
or
thot
ic p
edal
s
4 FE
S-ch
anne
ls:
Qua
dric
eps a
nd h
amstr
ings
Ope
n-lo
op c
ontro
l.G
ait p
hase
con
trol:
not s
peci
fied
Not
teste
d.D
oes n
ot p
rovi
de u
prig
ht b
iped
al
wal
king
.Pr
epro
gram
ed F
ES p
aram
eter
s. St
a-tio
nary
trai
ning
syste
m.
Eval
uatio
n of
safe
ty a
nd u
sabi
lity
have
no
t yet
bee
n re
porte
d

20 F. Anaya et al.
1 3
system with functional electrical stimulation (Fig. 23). The pelvis support robot combines a pelvic support mechanism and a robot base integrated with a treadmill. The vertical and lateral motions of the pelvis are actively supported by the pelvic support brace which is attached to a motor actu-ated device. The vertical unloading and lateral motion forces exerted by the user during walking are detected by two load cells employed by the system. For natural walking, the pelvic support brace provides three passive rotational degrees of freedom at the pelvis.
Electrical stimulations were delivered to the quadriceps and tibialis anterior muscles, to assist and stimulate the leg swing. A preliminary evaluation was reported for two healthy subjects wearing an ankle–foot orthosis (AFO) to simulate hemiplegic gait. However, further evaluation with patient data is required.
Targeting the hemiplegic patients, a lower limb reha-bilitation cycling wheelchair “Profhand” for rehabilitation and locomotion was developed in Japan (Watanabe et al. 2013). The Profhand is a pedaled wheelchair propelled by the lower limbs. The stimulation timings are estimated by crank angle recordings obtained from a wireless iner-tial measurement unit (WAA-010) attached centrally in the crankshaft. Electrical stimulations are provided to the quadriceps (for knee extension) and medial hamstrings or the gluteus maximus with two different patterns. For the first pattern, the quadriceps femoris muscle is stimulated together with hamstrings of the contralateral side caus-ing knee extension and contralateral knee flexion. For the second pattern, the quadriceps femoris is stimulated in conjunction with gluteus maximum of the ipsilateral side causing knee and hip extension of the lower limb. By recording the crank angle θ, the configuration of stimu-lated muscles is adjusted. The electrical stimulation to the right and left quadriceps femoris are switched at the crank angle θR and θL, respectively, where θL was set as θL = θR + 180°. Experimental tests were performed on 3 healthy subjects which proved that the Profhand provided effective propulsion by stimulating the quadriceps femoris and the gluteus maximus of the same limb. However, the cycling speeds were reported to be smaller than that of voluntary cycling.
Lastly, in (Bellman et al. 2017), Bellman et al. introduced a motorized FES-cycling test bed which incorporates func-tional electrical stimulation with switched control input. In the switching strategy applied here, the electric motors pro-vide assistance during crank cycle only when the effective-ness of the kinematics due to the rider’s muscle activity is low. A modified recumbent tricycle (TerraTrike Rover) with 24 VDC electric motor (Unite Motor Co. Ltd. MY1016Z2) coupled to the drive chain mounted at the mechanical frame
Fig. 21 Passive therapeutic arm based on a belt for supporting the subject’s pelvis to increase stability during treadmill walking. Retrieved from (Cikajlo et al. 2007)
Fig. 22 The ROBO-FES System. Retrieved from (Hacoma 2017)
Fig. 23 Motions of pelvis support robot. Retrieved from (Ye et al. 2014)

21Hybrid FES–robotic gait rehabilitation technologies: a review on mechanical design, actuation,…
1 3
(Fig. 24) was used for the FES trials. The orthotics pedals were affixed to the custom pedals to fix the riders pedals by preventing dorsi/plantar flexion of the ankles and to ensure proper sagittal alignment of the lower limbs. A current-controlled stimulator delivered biphasic, rectangular, sym-metric pulses to the subject’s muscle groups. The stimula-tion frequency was stablished at 60 Hz with amplitude fixed at 90 mA for the quadriceps and 80 mA for the hamstring muscles. Experimental results from five able-bodied subjects successfully validated the ability of the controller with an average cadence tracking error of 0.00 ± 5.82%.
3 Discussion
To the best of our knowledge, the twenty-eight hybrid robotic systems reviewed in this paper describe the state of the art systems that combines rehabilitation robotics with FES for lower limb rehabilitation. The hybrid robotic sys-tems reviewed here demonstrated the viability of combining FES with a wearable robotic device.
Hybrid robotic systems integrate two technologies, that complement each other, onto one platform so they can over-come the drawbacks of individual approaches. In such sce-nario, FES and gait rehabilitation robots promises to provide more safe, robust, and efficient neurological rehabilitation. To achieve this, it is important to determine the contribu-tion of each individual system and establish the impact it will have on the results of rehabilitation. While the wear-able robotic devices are designed to assist movement during the swing phase of the gait and to prevent joint movement during the stance phase, the FES takes benefit of the mus-cle power produced to reduce energy demand of the robotic device. This reduces the need for more powerful and bulky joints actuators, resulting in lighter systems. Moreover, such hybrid systems claim to promote more efficient motor learning as compared to other conventional practices such as
treadmill walking, due to the high demanding, community-based locomotion practice involved.
Over the years, hybrid wearable robots have proven themselves as a promising rehabilitation method by aiding affected individuals to regain their lost functional mobility and improving their quality of life. Regarding the imple-mentation of the motor neuroprosthesis, hybrid wearable robots were classified into either open or closed loop and regarding their actuation principle, they were classified into purely dissipating, semi-active or fully active, depending on the actuator’s ability to add or dissipate energy to the joint.
3.1 Orthotic robot‑based hybrid systems
A number of approaches for hybrid robotic gait restoration are currently available; however, the most widely developed hybrid robotic systems combined an exoskeletal robot and an FES device. Exoskeletal robots are worn by the patients to enhance the motor function of a limb or to fully substitute it while the FES targets the person’s paralyzed muscles to evoke actions that would not be possible otherwise. Differ-ent approaches were proposed to combine FES and lower limb exoskeletons, where the FES system reviewed were as complex as intramuscular systems with up to 8 stimulated muscles (McCabe et al. 2008), and as simple as systems incorporating surface stimulation of a single muscle (Kan-gude et al. 2009).
3.1.1 Hybrid exoskeletons where FES is used to stimulate the muscles and produce joint torque while the robotic system acts as energy dissipating device
Hybrid exoskeletons under control of joint brakes (Goldfarb and Durfee 1996; Chang et al. 2016) employ FES for deriv-ing the power to generate locomotion, by attaching brakes to the passive orthosis joints. The control strategy is based on employing joint brakes to delimit position and movement speed of joints produced by FES. Furthermore, the addi-tion of controllable brakes prevents the need to stimulate the muscle groups during the stance phases of gait, which results in a delayed musculature fatigue onset. As conse-quence, this combined approach acts as an FES regulator for the following step.
Efforts towards a hybrid orthosis with energy storage has also been proposed in (Gharooni et al. 2000, 2001; Sharma et al. 2014), where a spring-loaded mechanism stores and transfers energy from the stimulated paralyzed muscles to the corresponding joint, resulting in joint flexion. On top of the spring-break energy storing orthosis, joint-coupled orthosis has also been reported. These systems are similar to the spring-loaded mechanism orthoses, which are based on what is called the elastic-storage principle, but here the
Fig. 24 Model of the motorized FES cycle-rider system. a Electric motor. b Stimulator. c Orthotic pedals. Retrieved from (Bellman et al. 2017)

22 F. Anaya et al.
1 3
elastic element was employed across two joints (hip and knee joints). Examples of the joint-coupled orthosis were presented by Farris et al. in (2009) and by Durfee WK in (Kangude et al. 2009), where hip motion was driven by the energy generated at the knee joint. Even though this may seem to be an energy efficient method, it may not be an effective rehabilitation method as it considers only an individual muscle in the leg and the stimulation pattern is nowhere close to the normal activation pattern.
Despite the decent evidence reported in literature on hybrid exoskeletons controlled by joint brakes, there are some drawbacks that prevents the widespread adoption of such technologies: hybrid exoskeletons controlled by brakes are unable to fully control the joint trajectories due to the inability of joint brakes to deliver torque. Therefore, limb movement is achieved entirely by the contraction of the stimulated muscles. Here, FES systems are considered to be robust and reliable to generate lower limb movements effi-ciently. However, as stimulation approaches corresponds to a majority of systems performing open-loop FES control, the quality of the motion generated was deemed poor in terms of joint trajectories and velocities. Also, the control system results in inadequacy due to the insufficient torque power produced. This control strategy reports no information about joint movements exerted by FES being fed back into the FES controller showing lack of direct control over muscle stimulation. Furthermore, due to the low joint power exerted and the poor control of joint trajectory, it is difficult to man-age the early appearance of muscle fatigue caused by FES. Consequently, a robust FES controller would play an impor-tant role in successfully deploying a hybrid exoskeleton con-trolled by joint brakes. Though the adequate administration of FES relies on the control strategy (preferably closed-loop control), the number of stimulating channels and the pre-cise electrode placement; the controller approach should also be able to compensate the null joint power exerted by the exoskeleton. FES-control strategies such as open-loop and linear feedback controllers, are mostly insufficient for controlling the limb excursion, mainly because of the high muscle response variability (Lynch and Popovic 2008).
Unlike hybrid exoskeletons employing joint brakes, active hybrid exoskeletons permit better control over the amount of power being added to the joint, which establishes an effec-tive feedback control of limb motions between the combined end-effector and the FES device.
3.1.2 Hybrid exoskeletons where FES and robotic systems are both torque‑generating devices
Two conditions essential for gait restoration are: joint stabil-ity and their control. Here, fully powered exoskeletons that combines the control of an end-effector and a FES device seems to give an alternative to the previously reviewed
hybrid systems with energy dissipating orthoses. The imple-mentation of active actuators on the exoskeleton joints does not only have the advantage of increasing joint power but also to assist the joint trajectory when the muscle is not capable of generating enough torque for the joint move-ment. Consequently, active actuator implementation on the exoskeleton joints has been reported as an effective strategy to reduce muscle fatigue caused by continuous exaggerated muscle stimulation.
Considering the fully active hybrid exoskeletons, mechanical design of the exoskeleton includes treadmill based exoskeletons and over-ground exoskeletons with DC motors as it produces controllable output with quick response time. The treadmill based exoskeletons widely employ the BWS system that provides uplifting force to maintain balance and suspension to the subject walking on the treadmill. Lokomat (McCabe et al. 2008) is a nota-ble system reviewed in this paper that uses the BWS sys-tem with the treadmill. Moreover, WalkTrainer (Stauffer et al. 2009) also employs BWS with motorized wheels for over ground movement and the Electromechanical Gait Trainer (Hesse 2004) employs BWS with movable foot-plates. Other exoskeletons systems include the portable over ground exoskeletons that provide more freedom of motion as compared to the treadmill based systems.
In addition to the aforementioned capability of fully powered exoskeletons to compensate joint trajectory, handling early muscle fatigue is also an aspect of impor-tance to design a fully powered hybrid exoskeleton due to the alteration in muscular activation with current FES systems. Following the principle in which the active exoskeleton can provides torque to the joints and where the FES intensity and duration can be adjusted with the proper control to allow time for muscle relaxation, vari-ous approaches have been proposed. Comparable to the joint brakes based exoskeletons, fully powered exoskeleton have been developed with open-loop control (Hesse 2004; Obinata et al. 2007; McCabe et al. 2008; Poboroniuc et al. 2009; Kurokawa et al. 2012; Kirsch et al. 2014; Bulea et al. 2011) and closed-loop control (Vallery et al. 2005; Stauffer et al. 2009; Chen et al. 2013; Tu et al. 2016; del-Ama et al. 2015; Quintero et al. 2012) of the FES param-eters. However, pre-programmed FES systems result in delivering of excessive electrical stimulation to the mus-cles causing either early fatigue or exaggerated gait pat-tern. Whereas in closed-loop control systems the residual physical abilities of the patients are yet to be implemented in the feed control of the hybrid exoskeletons.
Alternatively, learning feedforward loop controllers considered in (Ren et al. 2014) characterizes an interesting method that feats the cyclical ability of robotic rehabilitation to learn from deviations of preceding trials. This learning competence offers an alternative to assist and adjust to the

23Hybrid FES–robotic gait rehabilitation technologies: a review on mechanical design, actuation,…
1 3
physiological changes of the patients (i.e. Muscle activation variance due to muscle spasticity or fatigue) by integrating the residual physical abilities of the patients to the controller. Therefore, the main challenge for the full spread of hybrid fully powered exoskeletons is developing an optimally shared control by integrating the FES system, the exoskel-eton, and the patient’s residual movement capacity, in order to produce limb movement of enough range and adequate joint trajectory.
3.2 Non‑orthotic robot‑based hybrid systems
Although FES-based technologies have been mostly devel-oped in the field of hybrid exoskeletons, technologies includ-ing robotic footplate systems, mobile platforms and cycling systems have also been proposed. However, a number of drawbacks arise from such systems, such as the inability to add power at the joint level (Cikajlo et al. 2007; Ye et al. 2013, 2014) or to provide upright bipedal walking (Kuznet-sov et al. 2013; Watanabe et al. 2013; Bellman et al. 2017).
Wheelchairs continue to be employed as a mobility option for people with high levels of motor disability. However, they remain as the less desirable options due to the lack of upright bipedal walking. It has been suggested that standing itself has physical and psychological benefits that are not replicated by wheelchairs (Esquenazi et al. 2017).
3.3 Future research and development directions of hybrid robot assistive devices
The following subsections briefly discuss some non-exhaus-tive potential future research directions and challenges in hybrid robot assistive devices.
3.3.1 Understanding biological joint kinematics: compliant joint mechanisms for lower limb exoskeletons
The progressive developments in robotic exoskeletons have resulted from advances in sensors, actuators, and processors. However, there still exists a substantial gap in our understanding of the physiology and biomechanics of human movement (Ferris et al. 2007). This lack of knowl-edge impediments our ability to estimate how exoskeletons will impact the locomotion of cognitively impaired patients (Cenciarini et al. 2011).
Regardless of different design approaches, orthotic robot-based technologies share a main objective, that is, to transfer power to the user’s limb. Moreover, the robots must guar-antee its wearer’s safety, while maintaining or improving its own efficiency. In such a context, the robot must provide mechanical support so that the added loads do not affect the user’s condition. It also must adjust to the wearer’s anatomy. All of this while maintaining a relatively diminutive size.
Thus, there is one main concern that rises when designing the physical part of an exoskeleton: there is a kinematic incompatibility caused by the mismatch between the human and the robotic joints.
Taking into consideration the diversity of morphology among individuals and the inherent complexity of the human joints, it is unreasonable to try to determine a general design that maximizes performance while reducing the mechanical interference for each user (Cenciarini et al. 2011). There-fore, it is commonly accepted to simplify the wearer’s joint kinematics by employing simple robotic elements such as revolute or spherical joints to model the human anatomy, which translates not only into obtaining the mechanical sim-plicity, but also into achieving simpler actuation, controllers, and subsequently cheaper prototypes. However, revolute or spherical joints only reflects the dominant rotations and neglects the small dose of concealed translations (Vukobra-tovic 2007), making it impossible to properly comply with the user (Scott and Winter 1993).
While walking, the whole body participates, including toes and arms. Nevertheless, the hip, knee and ankle joints have been recognized to be more relevant than any other joint, as they produce the greater motions and torques. As an example, the knee joint, is defined as a condyloid joint (Hamill and Knutzen 2009) formed by the proximal portion of the tibia and the distal end of the femur. It performs flex-ion and extension, and internal or external rotations; none-theless, when loaded under body weight or during full exten-sion, internal and external rotations are greatly constrained (Celebi et al. 2013). When knee flexes or extends, tibia rolls and slides on femur causing the instant center of rotation to be displaced up to 3 cm (Lee and Guo 2010). Convention-ally, the knee joint is merely modeled as a revolute joint, as reported in (Sharma et al. 2014; Farris et al. 2009; Pons et al. 2013; Schuck et al. 2012; Querry et al. 2008; Quintero et al. 2011). This estimation significantly simplifies the mechani-cal and kinematic considerations during exoskeletal design but sacrifices the ergonomics and mechanical compliance with the wearer’s anatomy. However, according to (Wang et al. 2014), this oversimplification results in “parasitic” forces and torques which may lead to prolonged discomfort or risk of injury over time.
To avoid the above-mentioned problems and to give bet-ter user experience, numerous scientists are proposing new mechanisms that comply with the users’ anatomy. One of the pioneer designs to do so are those presented by Wang et al. (2014). They proposed five exoskeleton designs to investigate the internal forces and torque generated in the knee with combinations of adaptive kinematic components: pin and fixed end, pin and slider, cam and slider, pin and pinned slider, and cam and pinned slider. They used an arti-ficial model of the knee (A82 Functional Knee Joint Model, 3B Scientific GmbH, Germany) to emulate the knee joint

24 F. Anaya et al.
1 3
mechanics in experiments. Experimental results suggest that the implementation of a pin slider/cam can effectively reduce internal joint forces and torque during the human–robot interaction.
To build on this concept and trying to reduce pain for people with knee osteoarthritis, Lee and Wang (Lee et al. 2015) (Wang et al. 2016) expanded their work by building a weight-support lower-extremity-exoskeleton (LEE) with a compliant joint to release the high-load during gait to the knee while supporting human bodyweight during walking. Unlike prior designs in which it is almost impossible to pro-vide body weight support due to the use of passive DOFs, the design of this compliant joint uses deformable rings to perform compliant coupling (θ > 20°) for adjusting mis-alignments of the rotating centers of the human–machine knee joint. Testing results showed a reduced plantar force by 27 and 21% at the 1st and 2nd peak forces, respectively; thus, showing its effectiveness in supporting the human weight by 20% during level walking.
Parallel to Lee and Wang et al.’ work, different compli-ance solutions to the ankle and hip joints have also been proposed. However, according to Gálvez-Zúñiga and Ace-ves-López in their review on compliant joint mechanisms for lower limb exoskeletons (Gálvez-Zúñiga and Aceves-López 2016), only one lower limb exoskeleton with more than one active complaint joint has been reported: the prototype of Yang et al. (2014) known as Bionic Lower Extremity Reha-bilitation Exoskeleton (BLERE). Their design consists of a novel exoskeleton with compatible hip and knee joints that aid patients to perform level ambulation. They used a pinned slider alongside cam and a curved slider, and two revolute joints for the knee and hip joint, respectively; allowing free movement in all the 3 DOFs mechanisms. The analytical results showed good compliance of the design.
To the best of our knowledge, despite the good perfor-mance reported on compliant joint mechanisms for lower limb exoskeletons, no system has integrated compliant joints with FES for restoration and rehabilitation of motor func-tion. Thus, we believe further efforts should be made to incorporate compliant joint mechanisms into the mechanical design of hybrid robotic systems. In the foreseeable future, it is expected to advance towards the development of tech-nologies in this area as a way to reduce the misalignment between the human and robot joint axes which can cause undesired interaction forces.
3.3.2 Improving functional outcomes in physical rehabilitation
It is common knowledge that countless patients with neu-rological disorders, including stroke and SCI, experience significant continuous improvement of motor, language, and cognitive function. The residual physical abilities of
the patient (i.e. voluntary muscle contraction, range of joint motion, bioelectrical residual activity) and adapta-tion, urge us to vouch for long-term rehabilitation in place of, or at least in conjunction with, motor substitution. This suggests the inclusion of principles in motor reha-bilitation, including “assist-as-needed” (Cai et al. 2006) and “challenged-based” in the development of hybrid robotic systems.
To enhance the welfares of FES-aided gait in functional motor recovery, the stimulation approach must modulate stimulation considering user intent, active participation (e.g., to start the gait) and adaptation, including changes in spasticity and muscle fatigue, while preserving a significant challenge. If insight into the functional movement disorders is fully understood, the design of the robot controller can effectively imitate the actions of a particular patient, thus the robotic controllers (FES and robot) can be personalized to the user impairments. We therefore advocate the inclusion of the principles of “assist-as-needed” and “challenge-based” to the customization of the motor control scheme from the very beginning, in the field of hybrid robotics for lower limb rehabilitation.
3.3.3 Clinical challenges and the relevance of feedback
Research on hybrid robot assistive devices still has to prove its effectiveness when they are used in the rehabilitation of motor function. The upcoming research requires enhanced clinical evidence to support not only effectiveness but to address issues like safety, acceptability, interaction between the wearer and the device and its social constraints. Most of the hybrid robotic devices studied in this article have pre-sented initial evaluation based on safety and energy perfor-mance. However, although these systems have proved to be functional, no evidence supporting major influence of the hybrid systems on the rehabilitation of lower limb impaired individuals has been reported.
Furthermore, having in mind the idea of considering functional active participation of the patient as a com-ponent to motor recovery, feedback provision results in essential component of motor rehabilitation. Today, there is vivid discussion on future research on the way to most effectively provide augmented feedback to better improve motor skills in patients with neurological disorders. The pace of technological development in augmented feedback seems to accelerate more every year, and the last dec-ade saw its share of major studies focused to investigate not only visual, but also auditory, haptic or multimodal augmented feedback. It may be interesting to investigate whether hybrid systems with the more complex, realistic motor tasks of augmented feedback enhances relearning of motor skills in recovery motor function after neurological injury such as stroke.

25Hybrid FES–robotic gait rehabilitation technologies: a review on mechanical design, actuation,…
1 3
3.3.4 Major technical challenges
Reduced metabolic cost along with reduced muscular fatigue while using hybrid robots is one of the key areas to improve. For this to become reality, closed-loop based FES controllers must be exploited. The investigation of new user-based con-trol strategies may give solutions to some of the challenges associated with early fatigue or exaggerated gait pattern.
Likewise, the investigation of modular architectures of mechanisms for rehabilitation robots may address some of the issues associated with increased metabolic costs. Modular robots aim to actuate singular joints like the hip, knee, or ankle; thus, resulting in light weight robots which allows the users to direct physical efforts towards the motor mechanisms that are impaired. Also “soft robotics” that are fabricated with polymeric elastomers and claims to be portable, self-directed, lightweight and with sufficient torque-generating capability to apply biologically relevant forces to the lower limb joints of the wearer (Asbeck et al. 2015), may give a solution. In this review paper, only two modular robotic systems (for the knee joint) were reported in (Bulea et al. 2013a, b; Ren et al. 2014), and none of the cited articles reported the use of any sort of soft robot. In the near future, lightweight rehabilitation robots in which the natural passive dynamics of human gait is preserved need to be developed. Given the current drawbacks in actuator technologies and control approaches, the concept of func-tional ambulation seems fundamental for reduction of the high metabolic energy expenditure required of users. It is projected future research in this area as a way of improving both mechanically and neuronal human–robot interaction.
4 Conclusion
This paper presents the overview of Hybrid Robotic systems which combines FES with lower limb rehabilitation devices for motor recovery. It is a unique approach which aims to enhance the effectiveness of the currents capabilities of these individual techniques.
The systems reviewed in this paper show the feasibility of this technology to provide good control over joint move-ment by minimizing the system’s energy demands. The inclusion of active actuators on the exoskeletons manages the muscle fatigue by optimizing the electrical stimulation needed to produce a joint motion and enables a more natural movement. The three major concepts implemented by these hybrid technologies to produce the desired joint motion are stimulating the gastrocnemius muscles to assist in push-off, locking of the knee joint during stance phase and by provid-ing external energy to the hip joints. However, only few of the systems reported in this review were evaluated with non- disables subjects. The potential of novel hybrid approaches
to rehabilitate motor functions with repeatability and flexi-bility (adaptation), makes them an attractive area of research and development; however, based on an insufficient amount of evidence supporting function recovery after brain injury, the hybrid robotic systems are not yet at a level to be listed as a solution for functional rehabilitation in motor disorders.
Lastly, this paper identifies not only the future research directions but also the scientific, technological, and clinical challenges involved with these hybrid technologies. Also, a new concept including hybrid bio-inspired joint exoskel-etons and FES for motor rehabilitation has been proposed. A better understanding of how humans performs motion would be able to better support this concept. Then technologies can be analogously designed and concepts such as augmented feedback and “assist-as-needed” revisited.
Funding The work was funded in part by the FRC Tier 1 Grant R-397-000-218-112, Faculty of Engineering, National University of Singapore, and in part by the NMRC B&B Grant No. NMRC/BnB/0019b/2015, Ministry of Health, Singapore.
Compliance with ethical standards
Conflict of interest The authors declare that they have no conflict of interest.
References
Agrawal, S.K., Banala, S.K., Fattah, A., Sangwan, V., Krishnamoorthy, V., Scholz, J.P., Hsu, W.-L.: Assessment of motion of a swing leg and gait rehabilitation with a gravity balancing exoskeleton. IEEE Trans. Neural Syst. Rehabil. Eng. 15(3), 410–420 (2007)
Asbeck, A.T., De Rossi, S.M., Holt, K.G., Walsh, C.J.: A biologically inspired soft exosuit for walking assistance. Int. J. Robot. Res. 34(6), 744–762 (2015)
Audu, M.L., To, C.S., Kobetic, R., Triolo, R.J.: Gait evaluation of a novel hip constraint orthosis with implication for walking in para-plegia. IEEE Trans. Neural Syst. Rehabil. Eng. 18(6), 610–618 (2010)
Banala, S.K., Agrawal, S.K., Fattah, A., Krishnamoorthy, V., Hsu, W.-L., Scholz, J., Rudolph, K.: Gravity-balancing leg orthosis and its performance evaluation. IEEE Trans. Rob. 22(6), 1228–1239 (2006)
Bellman, M.J., Downey, R.J., Parikh, A., Dixon, W.E.: Automatic con-trol of cycling induced by functional electrical stimulation with electric motor assistance. IEEE Trans. Autom. Sci. Eng. 14(2), 1225–1234 (2017)
Bulea, T. C., Kobetic, R., Triolo, R. J.: Restoration of stance phase knee flexion during walking after spinal cord injury using a variable impedance orthosis. In: 33rd Annual international conference of the IEEE EMBS, Boston, Massachusetts USA (2011)
Bulea, T.C., Kobetic, R., To, C.S., Audu, M.L., Schnellenberger, J.R., Triolo, R.J.: A variable impedance knee mechanism for controlled stance flexion during pathological gait. IEEE/ASME Trans. Mechatron. 17(5), 822–832 (2012)
Bulea, T.C., Kobetic, R., Audu, M.L., Triolo, R.J.: Stance controlled knee flexion improves stimulation driven walking after spinal cord injury. J. Neuroeng. Rehabil. 10(1), 68 (2013a)

26 F. Anaya et al.
1 3
Bulea, T.C., Kobetic, R., Audu, M.L., Schnellenberger, J.R., Triolo, R.J.: Finite state control of a variable impedance hybrid neuropro-sthesis for locomotion after paralysis. IEEE Trans. Neural Syst. Rehabil. Eng. 21(1), 141–151 (2013b)
Bulea, T.C., et al.: Forward stair descent with hybrid neuroprosthe-sis after paralysis: single case study demonstrating feasibility. J. Rehabil. Res. Dev. 51(7), 1077 (2014)
Cai, L. L., Fong, A. J., Liang, Y., Burdick, J. Edgerton,V. R.: Assist-as-needed training paradigms for robotic rehabilitation of spinal cord injuries. In: Proceedings 2006 IEEE international conference on robotics and automation, Orlando, Florida (2006)
Celebi, B., Yalcin, M., Patoglu, V.: AssistOn-Knee: a self-aligning knee exoskeleton. In: Proceedings of the 26th IEEE/RSJ international conference on intelligent robots and systems (IROS ‘13), Tokyo, Japan (2013)
Cenciarini, M., Dollar, A. M.: Biomechanical considerations in the design of lower limb exoskeletons. In: Proceedings of the IEEE international conference on rehabilitation robotics (ICORR ‘11), Zurich, Switzerland (2011)
Chang, S. R., Nandor, M. J., Li, L., Foglyano, K. M., Schnellen-berger, J. R., Kobetic, R., Quinn, R. D. Triolo, R. J.: A stim-ulation-driven exoskeleton for walking after paraplegia. In: 2016 IEEE 38th Annual international conference of the IEEE Engineering in Medicine and Biology Society (EMBC) (2016)
Chang, S.R., Nandor, M.J., Li, L., Kobetic, R., Foglyano, K.M., Schnellenberger, J.R., Audu, M.L., Pinault, G., Quinn, R.D., Triolo, R.J.: A muscle-driven approach to restore stepping with an exoskeleton for individuals with paraplegia. J. Neuroeng. Rehabil. 14(1), 48 (2017)
Chen, Y., Hu, J., Wang, W., Peng, L., Peng, L., Hou, Z.-G.: An FES-assisted training strategy combined with impedance control for a lower limb rehabilitation robot. In: IEEE international conference on robotics and biomimetics (ROBIO), Shenzhen, China (2013)
Cikajlo, I., Obreza, P., Savrin, R., Matjacic, Z.: Passive therapeutic arm for pelvis support during FES supported gait treadmill training—a case study. In: IEEE 10th International conference on rehabilita-tion robotics, Noordwijk, The Netherlands (2007)
del-Alma, A.J., Koutsou, A.D., Moreno, J.C., de-los-Reyes, A., Gil-Agudo, A., Pons, J.L.: Review of hybrid exoskeletons to restore gait following spinal cord injury. J. Rehabil. Res. Dev. 49(4), 497–514 (2012)
del-Ama, A. J., Agudo, Á. G., Pons, J. L., Moreno, J. C.: Hybrid gait training with an overground robot for people with incomplete spi-nal cord injury: a pilot study. Front. Human Neurosci. 8 (2014)
del-Ama, A.J., Gil-Agudo, A., Pons, J.L., Moreno, J.C.: Hybrid FES–robot cooperative control of ambulatory gait rehabilitation exo-skeleton. J. Neuroeng. Rehabil. 11(1), 27 (2014)
del-Ama, A.J., Agudo, Á.G., Bravo-Esteban, E., Perez-Nombela, S., Pons, J.L., Moreno, J.C.: Hybrid therapy of walking with Kinesis overground robot for persons with incomplete spinal cord injury: a feasibility study. Robot. Auton. Syst. 73, 44–58 (2015)
del-Ama, A. J., Gil-Agudo, Á., Pérez-Nombela, S., Piñuela-Martín, E., Pons, J. L., Moreno, J. C.: Recent advances on lower limb hybrid wearable robots. In: IFESS 2016, La Grande Motte, France (2016)
Dohring, M.E., Daly, J.J.: Automatic synchronization of functional electrical stimulation and robotic assisted treadmill training. IEEE Trans. Neural Syst. Rehabil. Eng. 16(3), 310–314 (2008)
Durfee, W.K., Hausdorff, J.M.: Regulating knee joint position by com-bining electrical stimulation with a controllable friction brake. Ann. Biomed. Eng. 18(6), 575–596 (1990)
Durfee, W.K., Rivard, A.: Design and simulation of a pneumatic, stored-energy, hybrid orthosis for gait restoration. J. Biomech. Eng. 127(6), 1014–1019 (2005)
Durfee, W. K., Goldfarb, M.: Design of a controlled-brake orthosis for regulating FES-aided gait. In: 14th Annual international
conference of the IEEE Engineering in Medicine and Biology Society, Paris, France (1992)
Esquenazi, A., Talaty, M., Jayaraman, A.: Powered exoskeletons for walking assistance in persons with central nervous system inju-ries: a narrative review. PM&R 9(1), 46–62 (2017)
Farris, R. J., Quintero, H. A., Withrow, T. J., Goldfarb, M.: Design of a joint-coupled orthosis for FES-aided gait. In: IEEE 11th Interna-tional conference on rehabilitation robotics, Kyoto International Conference Center, Japan (2009)
Farris, R. J., Quintero, H. A., Withrow, T. J., Goldfarb, M.: Design and simulation of a joint-coupled orthosis for regulating FES-aided gait. In: IEEE international conference on robotics and automa-tion, Kobe, Japan (2009)
Farris, R.J., Quintero, H.A., Goldfarb, M.: Preliminary evaluation of a powered lower limb orthosis to aid walking in paraplegic individu-als. IEEE Trans. Neural Syst. Rehabil. Eng. 19(6), 652–659 (2011)
Ferris, D.P., Sawicki, G.S., Daley, M.A.: A physiologist’s perspective on robotic exoskeletons for human locomotion. Int. J. Humanoid Rob. 4(3), 507–528 (2007)
Fukada, S., Obinata, G., Hase, K., Nakayama, A., Shimada, Y., Matsu-naga, T., Iwami, T., Miyawaki, K., Tsunetou, M.: Development of a hybrid power assist orthosis with FES. In: 11th Annual confer-ence of the International FES Society, Zao, Japan (2006)
Gálvez-Zúñiga, M.A., Aceves-López, A.: A review on compliant joint mechanisms for lower limb exoskeletons. J. Robot. 2016, 9 (2016)
Gharooni, S., Tokhi, M. O., Heller, B.: The use of elastic element in a hybrid orthosis for swing phase generation in orthotic gait. In: Proceedings of the 5th annual conference of the International Functional Electrical Stimulation Society, Aalborg, (2000)
Gharooni, S., Heller, B., Tokhi, M.O.: A new hybrid spring brake orthosis for controlling hip and knee flexion in the swing phase. IEEE Trans. Neural Syst. Rehabil. Eng. 9(1), 106–107 (2001)
Goldfarb, M., Durfee, W.: Design of a controlled-brake orthosis for FES-aided gait. IEEE Trans. Rehabil. Eng. 4(1), 13–24 (1996)
Goldfarb, M., Korkowski, K., Harrold, B., Durfee, W.: Preliminary evaluation of a controlled-brake orthosis for FES-aided gait. IEEE Trans. Neural Syst. Rehabil. Eng. 11(3), 241–248 (2003)
Ha, K. H., Quintero, H. A., Farris, R. J., Goldfarb, M.: Enhancing stance phase propulsion during level walking by combining FES with a powered exoskeleton for persons with paraplegia. In: 34th Annual international conference of the IEEE EMBS, San Diego, California USA (2012)
Ha, K.H., Murray, S.A., Goldfarb, M.: An approach for the cooperative control of FES with a powered exoskeleton during level walking for persons with paraplegia. IEEE Trans. Neural Syst. Rehabil. Eng. 24(4), 455–466 (2016)
Hacoma: Erigo Hacoma (online). http s://www.hoco ma.com/us/solu tion s/erig o/. Accessed 18 Sep 2017
Hamill, J., Knutzen, M.: Biomechanical Basis of Human Movement, 3rd edn. Lippincott Williams & Wilkins, Philadelphia (2009)
Hara, Y.: Rehabilitation with functional electrical stimulation in stroke patients. Int. J. Phys. Med. Rehabil. 1(147), 2 (2013)
Hesse, S.: Recovery of gait and other motor functions after stroke: novel physical and pharmacological treatment strategies. Restor. Neurol. Neurosci. 22(3–5), 359–369 (2004)
Hesse, S., Uhlenbrock, D., Werner, C., Bardeleben, A.: A mechanized gait trainer for restoring gait in nonambulatory subjects. Arch. Phys. Med. Rehabil. 81(9), 1158–1161 (2000)
Hidler, J., Nichols, D., Pelliccio, M., Brady, K., Campbell, D.D., Kah, J.H., Hornby, T.G.: Multicenter randomized clinical trial evaluat-ing the effectiveness of the Lokomat in subacute stroke. Neurore-habil. Neural Repair 23(1), 5–13 (2009)
Huang, V., Krakauer, J.: Robotic neurorehabilitation: a computational motor learning perspective. J. Neuroeng. Rehabil. 6(1), 5 (2009)

27Hybrid FES–robotic gait rehabilitation technologies: a review on mechanical design, actuation,…
1 3
Jailani,R., Tokhi, M., Gharooni, S., Jogtaei, M.: Finite state control of FES-assisted walking with spring brake orthosis. In: UKSim 13th International conference on modelling and simulation (2011)
Kangude, A., Burgstahler, B., Durfee, W.: Engineering evaluation of the energy-storing orthosis FES gait system. In: 32nd Annual international conference of the IEEE EMBS, Buenos Aires, Argentina (2010)
Kangude, A., Burgstahler, B., Kakastys, J., Durfee, W.: Single channel hybrid FES gait system using an energy storing orthosis: prelimi-nary design. In: 31st Annual international conference of the IEEE EMBS, Minneapolis, Minnesota, USA (2009)
Kirsch, N., Alibeji, N., Fisher, L., Gregory, C., Sharma, N.: A semi-active hybrid neuroprosthesis for restoring lower limb function in paraplegics. In: Engineering in medicine and biology society (EMBC), 2014 36th Annual international conference of the IEEE, pp. 2557–2560 (2014)
Kobetic, R., To, C.S., Schnellenberger, J.R., Audu, M., Bulea, T.C., Gaudio, R., Pinault, G., Tashman, S., Triolo, R.J.: Development of hybrid orthosis for standing, walking and stair climbing after spinal cord injury. J. Rehabil. Res. Dev. 46(3), 447–462 (2009)
Krishnamoorthy, V., Hsu, W.-L., Benoit, D.L., Banala, S.K., Peru-mal, R., Sangwan, V., Binder-Macleod, S.A., Agrawal, S.K., Scholz, J.P.: Gait training after stroke: a pilot study combining a gravity-balanced orthosis, functional electrical stimulation and visual feedback. J. Neurol. Phys. Ther. 32(4), 192–202 (2008)
Kurokawa, N., Yamamoto, N. Tagawa, Y., Yamamoto, T., Kuno, H.: Development of hybrid FES walking assistive system—feasibil-ity study. In: International conference on advanced mechatronic systems, Tokyo, Japan (2012)
Kuznetsov, A.N., Rybalko, N.V., Daminov, V.D., Luft, A.R.: Early poststroke rehabilitation using a robotic tilt-table stepper and functional electrical stimulation. Stroke Res. Treat. 2013, 9 (2013)
Lee, K.-M., Guo, J.: Kinematic and dynamic analysis of an anatomi-cally based knee joint. J. Biomech. 43(7), 1231–1236 (2010)
Lee, K.-M., Wang, D.: Design analysis of a passive weight-support lower-extremity-exoskeleton with compliant knee-joint. In: 2015 IEEE international conference on robotics and automa-tion (ICRA), Seattle, Washington (2015)
Lum, P., Reinkensmeyer, D., Mahoney, R., Rymer, W., Burgar, C.: Robotic devices for movement therapy after stroke: current sta-tus and challenges to clinical acceptance. Top. Stroke Rehabil. 8(4), 40–53 (2002)
Lynch, C., Popovic, M.: Functional electrical stimulation. IEEE Con-trol Syst. 28(2), 40–50 (2008)
Mackay, J., Mensah, G., Mendis, S., Greenlund, K.: The Atlas of Heart Disease and Stroke. World Health Organization, Geneva (2004)
Maffiuletti, N., Minetto, M., Farina, D., Bottinelli, R.: Electrical stimu-lation for neuromuscular testing and training: state-of-the art and unresolved issues. Eur. J. Appl. Physiol. 111, 2391–2397 (2011)
McCabe, J.P., Dohring, M.E., Marsolais, E.B., Rogers, J., Burdsall, R., Roenigk, K., Pundik, S., Daly, J.J.: Feasibility of combining gait robot and multichannel functional electrical stimulation with intramuscular electrodes. J. Rehabil. Res. Dev. 45(7), 997–1006 (2008)
Metrailler, P., Blanchard, V., Perrin, I., Brodard, R., Frischknecht, R., Schmitt, C., Fournier, J., Bouri, M., Clavel, R.: Improvement of rehabilitation possibilities with the MotionMaker TM. In: The first IEEE/RAS-EMBS international conference on biomedical robotics and biomechatronics (2006)
Ng, M., Tong, R., Li, L.: A pilot study of randomized clinical con-trolled trial of gait training in subacute stroke patients with partial body-weight support electromechanical gait trainer and functional electrical stimulation. Stroke 39(1), 154–160 (2009)
Obinata, G., Fukada, S., Matsunaga, T., Iwami, T., Shimada, Y.: Hybrid control of powered orthosis and functional neuromuscular stimu-lation for restoring gait. In: Cité Internationale, Lyon, France, 2007, 29th Annual international conference of the IEEE EMBS (2007)
Poboroniuc, M.S., Stefan, C.M., Livint, G., Irimia, D.C.: Issues on mechatronic devices aiming to test neuroprothesis. In: Advanced Technologies for Enhanced Quality of Life, AT-EQUAL ’09, pp. 23–27 (2009)
Pons, J. L., Moreno, J. C., Rocon, E.: Exoskeletal robotics for func-tional substitution. Introduction to Neural Engineering for Motor Rehabilitation, pp. 327–348. Wiley (2013)
Popovic, M.: Control of neural prostheses for grasping and reaching. Med. Eng. Phys. 25(1), 41–50 (2003)
Popović, D.: Advances in functional electrical stimulation (FES). J. Electromyogr. Kinesiol. 24(6), 795–802 (2014)
Querry, R.G., Pacheco, F., Annaswamy, T., Goetz, L., Winchester, P.K., Tansey, K.E.: Synchronous stimulation and monitoring of soleus H reflex during robotic body weight-supported ambulation in subjects with spinal cord injury. J. Rehabil. Res. Dev. 45(1), 175–186 (2008)
Quintero, H. A., Farris, R. J., Goldfarb, M.: Control and implementa-tion of a powered lower limb orthosis to aid walking in paraplegic individuals. In: 2011 IEEE international conference on rehabilita-tion robotics, Switzerland (2011)
Quintero, H. A., Farris, R. J., Ha, K., Goldfarb, M.: Preliminary assess-ment of the efficacy of supplementing knee extension capability in a lower limb exoskeleton with FES. In: 34th Annual international conference of the IEEE EMBS, San Diego, California, USA (2012)
Regnaux, J.-P., Kaveh, S., Marehbian, J., Bussel, B., Dobkin, B.H.: An accelerometry-based comparison of 2 robotic assistive devices for treadmill training of gait. Neurorehabil. Neural Repair 22(4), 348–354 (2008)
Ren, Y., Zhang, D.: FEXO Knee: a rehabilitation device for knee joint combining functional electrical stimulation with a compli-ant exoskeleton. In: São Paulo, Brazil, 2014, 5th IEEE RAS & EMBS international conference on biomedical robotics and bio-mechatronics (BioRob), pp. 683–688 (2014)
Schaechter, J.: Motor rehabilitation and brain plasticity after hemipa-retic stroke. Prog. Neurobiol. 73(1), 61–72 (2004)
Schmidt, H., Werner, C., Bernhar, R., Hesse, S., Krüger, J.: Gait reha-bilitation machines based on programmable footplates. J. Neuro-eng. Rehabil. 4(1), 2 (2007)
Schuck, A., Labruyere, R., Vallery, H., Riener, R., Duschau-Wicke, A.: Feasibility and effects of patient-cooperative robot-aided gait training applied in a 4-week pilot trial. J. Neuroeng. Rehabil. 9(1), 31 (2012)
Scott, S.H., Winter, D.A.: Biomechanical model of the human foot: kinematics and kinetics during the stance phase of walking. J. Biomech. 26(9), 1091–1104 (1993)
Sharma, N., Mushahwar, V., Stein, R.: Dynamic optimization of FES and orthosis-based walking using simple models. IEEE Trans. Neural Syst. Rehabil. Eng. 22(1), 114–126 (2014)
Stauffer, Y., Allemand, Y., Bouri, M., Fournier, J., Clavel, R., Metrailler, P., Brodard, R., Reyna, F.: The WalkTrainer—a new generation of walking reeducation device combining orthoses and muscle stimu-lation. IEEE Trans. Neural Syst. Rehabil. Eng. 17(1), 38–45 (2009)
To, C.S., Kobetic, R., Schnellenberger, J.R., Audu, M.L., Triolo, R.J.: Design of a variable constraint hip mechanism for a hybrid neu-roprosthesis to restore gait after spinal cord injury. IEEE/ASME Trans. Mechatron. 13(2), 197–205 (2008)
To, C.S., Kobetic, R., Bulea, T.C., Audu, M.L., Schnellenberger, J.R., Pinault, G., Triolo, R.J.: Stance control knee mechanism for lower-limb support in hybrid neuroprosthesis. J. Rehabil. Res. Dev. 48(7), 839 (2011)

28 F. Anaya et al.
1 3
Tomovic, R., Vukobrativic, M., Vodovnik, L.: Hybrid actuators for orthotic systems: hybrid assistive systems. In: Tomovic, R. (ed.) Advances in External Control of Human Extremities, pp. 73–80 (1973)
Tu, X., Huang, J., He, J.: Leg hybrid rehabilitation based on hip-knee exoskeleton and ankle motion induced by FES. In: International Conference on Advanced Robotics and Mechatronics (ICARM) (2016)
Tu, X., Jiaxin, L., Chen, S., Zhang, S., Li, H., Cao, J., He, J.: Model-based hybrid cooperative control of hip-knee exoskeleton and FES induced ankle muscles for gait rehabilitation. Int. J. Pattern Recognit. Artif. Intell. 31(9), 1759019 (2017)
Vallery, H., Stutzle, T., Buss, M., Abel, D.: Control of a hybrid motor prosthesis for the knee joint, in IFAC Proceedings Volumes. Czech Republic, Prague (2005)
Vukobratovic, M.K.: When were active exoskeletons actually born? Int. J. Humanoid Rob. 4(3), 459–486 (2007)
Wang, D., Lee, K.-M., Guo, J., Yang, C.-J.: Adaptive knee joint exo-skeleton based on biological geometries. IEEE/ASME Trans. Mechatron. 19(4), 1268–1278 (2014)
Wang, D., Lee, K.-M., Ji, J.: A passive gait-based weight-support lower extremity exoskeleton with compliant joints. IEEE Trans. Rob. 32(4), 933–942 (2016)
Watanabe, T., Karasawa, Y.: Comparison of muscle stimulation groups for simplified practical FES cycling control with cycling wheel-chair: an experimental test with healthy subjects. IEICE Trans. Inf. Syst. 99(5), 1345–1352 (2016)
Watanabe, T., Murakami, T., Handa, Y.: Preliminary tests of a proto-type FES control system for cycling wheelchair rehabilitation. In: 2013 IEEE International conference on rehabilitation robotics, Seattle, Washington USA (2013)
Yang, W., Yang, C.-J., Wei, Q.-X.: Design of an anthropomorphic lower extremity exoskeleton with compatible joints. In: Proceed-ings of the IEEE International Conference on Robotics and Bio-mimetics (IEEE ROBIO ‘14), Bali, Indonesia, (2014)
Ye, J., Nakashima, Y., Zhang, B., Kobayash, Y., Fujie, M. G.: Func-tional electrical stimulation based on a pelvis support robot for gait rehabilitation of hemiplegic patients after stroke. In: 36th Annual international conference of the IEEE engineering in medi-cine and biology society, Chicago, IL, USA (2014)
Ye, J., Watanabe, T., Seki, M., Zhang, B., Liu, Q., Yokoo, Y., Kobayashi, Y., Cao, Q., Fujie, M. G.: Development of a novel gait rehabilitation system based on FES and treadmill-walk for convalescent hémi-plégie stroke survivors. In: IEEE/RSJ international conference on intelligent robots and systems (IROS), Tokyo, Japan (2013)
Zhang, D., Guan, T., Widjaja, F., Ang,W.: Functional electrical stimu-lation in rehabilitation engineering: a survey.In: Proceedings of the 1st international convention on Rehabilitation engineering and assistive technology: in conjunction with 1st Tan Tock Seng Hospi-tal Neurorehabilitation Meeting (CREATe’07), pp. 221–226 (2007)
Francisco Anaya received the B.S. degree in Biomedical Engineer-ing from Monterrey Institute of Technology and Higher Educa-tion, Mexico, in 2014. He is cur-rently working towards his Ph.D. at National University of Singa-pore, with research interests relating to biomechanics and muscle coordination of human walking, functional electrical stimulation (FES) and lower-limb robotic rehabilitation. He completed internships with the Center for Technology and
Research in Biomedicine, in Mexico and Holland Bloorview Kids Rehabilitation Hospital, in Toronto ON, Canada, prior to joining the Biorobotics lab at National University of Singapore. He is currently engaged in the development of systems to improve walking and mobil-ity for people with musculoskeletal and neuromuscular conditions by integrating FES with a novel robotic platform that enables patients post stroke to perform over-ground gait training at home or community rehab centers.
Pavithra Thangavel received the B.S. degree in Biomedical Engi-neering in 2013 from SRM Uni-versity, India, and the Master’s degree in Biomedical Engineer-ing in 2016 from VIT University, India. She is a Research Engi-neer in the Biorobotics Lab at National University of Singa-pore. Her current research is focused on the biomechanical study and evaluation of the lower limb powered exoskeleton.
Haoyong Yu received the B.S. and M.S. degrees in Mechanical Engineering from Shanghai Jiao Tong University, Shanghai, China, in 1988 and 1991, respec-tively. He received the Ph.D. degree in Mechanical Engineer-ing from Massachusetts Institute of Technology, Cambridge, Mas-sachusetts, USA, in 2002. He was a Principal Member of Tech-nical Staff at DSO National Lab-oratories, Singapore, until 2010. His research areas in DSO included exoskeleton and humanoid robots, intelligent
ground and aerial robots, and bio-inspired robots. Dr. Yu joined the Department of Biomedical Engineering in 2010. He is also a Principal Investigator of the Singapore Institute of Neurotechnology (SINAPSE), and the Advanced Robotic Centre at the National University of Singapore.