hand infection: discussion
TRANSCRIPT

Thorsang Chayovan5th year medical student

ผูป่้วยหญงิไทย อาย ุ23 ปี
Chief Complaint :เจบ็ปวดที่ น้ิวนางมือซา้ย มา 2 วนั
Present History : ปฏเิสธอบุตัเิหต ุขยบัน้ิวนางปวดมาก ไม่มีไข ้
ตรวจร่างกาย น้ิวนางบวมแดง เจบ็เม่ือมีการขยบั


Pain Stiffness Fever Previous history Underlying disease Systemic inflammatory disease manifestation
(RA, SLE, gout) Trauma history Lifestyle Family history
Inspection Signs of Inflammation
Deformities
Evidence of trauma
Palpation Stepping and crepitus
Range of motion
Neurovascular function
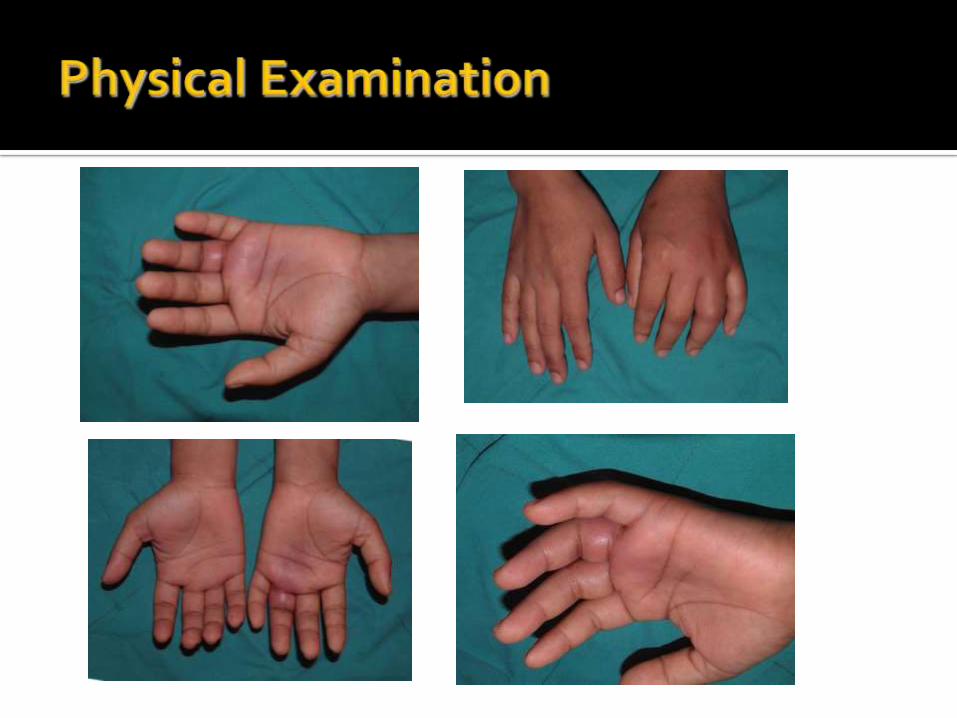

Pain on active motion for 2 days
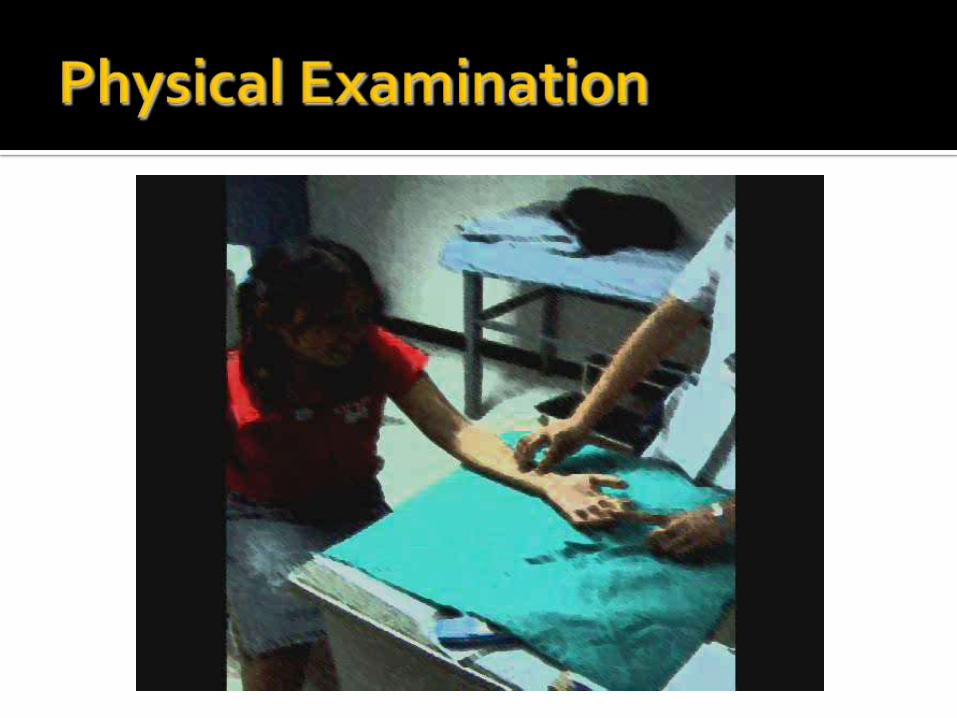
Erythema and swelling Flexion deformity Severe pain on passive extension


Infection Pyogenic Flexor Tenosynovitis Acute osteomyelitis Cellulitis Septic arthritis
Inflammation Systemic lupus erythematosus Rheumatoid Arthritis Gouty arthritis
Trauma Fracture Dislocation
X-rays: AP and lat. to rule out bony involvement or foreign body
MRI: Flexor tenosynovitis diagnosed by MRI of the hand is a strong predictor of early RA

Synovial Fluid Aspiration suppurative synovial fluid: culture
nonsuppurative conditions: synovial fluid may show ▪ nonbirefringent crystals (gout)
▪ birefringent crystals (calcium pyrophosphate deposition disease [CPPD] or pseudogout)
CBC WBC count not elevated in nonsuppurative
conditions
left shift is frequently present in acute processes

ESR elevated in acute or chronic infections and may serve
as a marker to follow resolution of an infection not elevated in nonsuppurative conditions.
Coagulation studies in anticoagulated patients or in patients with known
or suspected bleeding diathesis DIC:rare
rheumatologic factor : rule out RA
acid-fast bacilli and fungal cultures in patients with chronic or atypical presentation.

pathophysiologic state causing disruption of normal flexor tendon function
Cause Infection* secondary to acute or chronic inflammation as a result of
diabetes, overuse, or arthritis
Septic FT : the 4 Kanavel signs1) finger held in slight flexion2) fusiform swelling3) tenderness along the flexor tendon sheath4) pain with passive extension of the digit

orthopedic emergency closed-space infection increased pressure inhibits blood flow tendon ischemia tendon necrosis and rupture
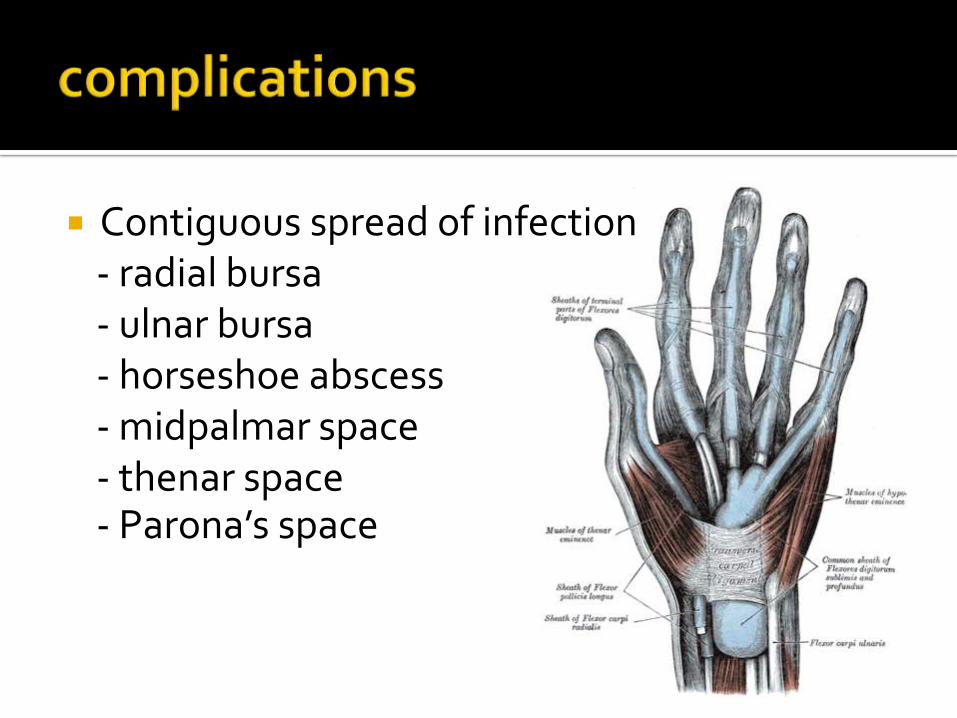
Contiguous spread of infection- radial bursa- ulnar bursa- horseshoe abscess- midpalmar space- thenar space- Parona’s space
Finger stiffness Vascular occlusion Tendon necrosis and function loss Median nerve compression

Principles Antibiotics Rest, splint and elevation Drainage Rehabilitation

Conservative treatment- within 24-48 hours after onset- admission for empiric antibiotics and observation
- splint (position of safe immobilization)
- elevation
Surgical treatment- late presentation ( > 48 hours)- conservative treatment failure- abscess suspected : marked tenderness- immunocompromised

Incision and drainage with postoperative closed irrigation
modified Neviaser technique
postoperative closed irrigation- 30 ml of isotonic solution q 2 hours for 48
hours - re-examine : off or continue?

Rehabilitation- ASAP (alleviation of inflammation)- re-apply splint between exercise sessions
(for the first few days)

Incision hereor more!
Open drainage : advanced infection and necrosis that require debridement