harvey newnham - alfred health
TRANSCRIPT

Targeting Zero Harm in Victorian Hospitals – A Physician’s View
of the Key Implications from the Review of Hospital Safety and
Quality Assurance in Victoria
Medico-Legal Congress, Thursday 9th March 2017
Harvey Newnham MBBS, FRACP, PhD, GAICD Clinical Program Director Emergency and Acute Medicine, Alfred Health

HN Conflict of interest declaration
• Employee of Alfred Health,
– funded by Victorian Department of Health and Human Services
• Board member of Better Care Victoria
– Ministerial board of Victorian DHHS
• Other advisory roles to Victorian DHHS
• Honorary Chair of Board of Health Education Australia Limited (HEAL)

Synopsis
• Why was it done?
• Key findings
• Implications for clinicians
• Medico-legal implications
Commissioned by: • Victorian Minister of Health, The Hon Jill
Hennessy Grattan Institute Review Panel: • Stephen Duckett (Health Program Dir) • Marie Cuddihy (CEO, Kyneton Health) • Harvey Newnham (Clinician, Alfred Health) Writing team: • Danielle Romans, senior associate Grattan
Institute, writing research and project coordination
• Jonathan Prescott, Acting manager Safety Program with VicDHHS, consultation and logistic support,
• Elsa Lapiz – VicDHHS system Intelligence and Analytics branch
Stephen Duckett

309 pages 179 Recommendations
50h of interviews - government, hospitals, NFPs, private and academia; variety of disciplines Five workshops
320 consumers, board members, CEOs, clinician leaders, DON, DMS Australian and International leaders in patient safety (many commented on report) MJA Insight article and discussion paper on DHHS website 91 public submissions shaped recommendations


Brent James Intermountain ATP course 2014
Base Jumping
Brent James, Intermountain APT course 2014

7
Total incidence of CHADx by major class (Source: VAED
for FY 2014-15)
Major class All Public
Hospitals All Private
Hospitals All Victorian
Hospitals
01: Post-procedural complications 34,106 17,808 51,914 02: Adverse drug events 14,858 6,402 21,260
03: Accidental injuries 6,078 2,179 8,257 04: Infections 12,846 2,694 15,540
05: Cardiovascular complications 47,304 17,984 65,288
06: Respiratory complications 23,499 8,737 32,236
07: Gastrointestinal complications 36,815 19,118 55,933 08: Skin conditions 18,196 7,509 25,705
09: Genitourinary complications 27,575 9,753 37,328 10: Hospital-acquired psychiatric
states 16,959 5,934 22,893
11: Early pregnancy complications 2,710 757 3,467
12: Labour & delivery complications 76,050 20,600 96,650
13: Perinatal complications 40,458 4,424 44,882
14: Haematological complications 12,994 3,970 16,964 15: Metabolic complications 45,536 10,743 56,279
16: Nervous system complications 4,245 1,429 5,674 17: Other complications 40,535 17,563 58,098 Total 460,764 157,604 618,368
ACSQHC ‘Priority
complications’
Public
Hospitals Private
Hospitals
Pressure injury 5,356 1,605
Falls with Fracture or ICI 362 127
Healthcare Assoc
Infection 16,597 5,587
Surgical complications 2,563 1,099
Respiratory
complications 2,846 554
Venous
Thromboembolism 1,098 429
Renal failure 309 52
GI bleeding 2,099 617
Medication
complications 2,017 455
Delirium 7,116 2,588
Incontinence 1,246 415
Malnutrition 1,564 482
Cardiac complications 9,843 4,194
Iatrogenic
pneumothorax requiring
intercostal catherer 230 74
Total count for all major
categories 53,246 18,278
Courtesy S. Duckett

Physician autonomy Is like a Limber pine on the edge of Bryce Canyon
Eddy: “The complexity of modern medicine exceeds the capacity of the unaided human mind”

What doctors consider “real research”: Clinical and biomedical research
Education and Training
Gap needing to be filled: • Systems & Processes for
Delivering Safe High Quality Care
• Clinical Governance • Improvement science • Leadership and
teamwork skills
What Doctors know
What doctors teach their
students

Healthcare Harm
• Major issues:
– Inherent patient risk and care complexity
– Clinical autonomy
– Process variability
– Imperfect communication
• World wide trend for system managers to partner with clinicians to improve safety and quality
• Is the Victorian DHHS appropriately setup to provide best practice support and oversight to achieve best possible patient outcomes?
• Several prior reports have not led to substantial change:
– A “tick and flick” approach is unlikely to achieve required change
• Safety and quality as first priority – Jill Hennessy Victorian health minister

Australian Hospital Care is State-based Queensland, Post Patel Centralised, devolving.
Clinical Senate Centralised recruitment
and services
NSW, Post Garling Centralised, devolving.
Major investment in governance:
4 Pillars ACI, BHI, CEC, HETI
Adapted from Grant Phelps Deakin Leadership seminar Feb 2017
South Australia, Post NHRA Small, central department
control. Organisational CEOs not recognised in legislation.
Tasmania, Post NHRA Department monitors responds and funds as
system manager
Victoria, Post Djerriwarrh Devolved, increasing central
accountability. Safer Care Victoria, BCV, VAHI,
Boards commission, Clinical Council

Key functions to be strengthened
Devolved governance
Democratic accountability
System leadership
Kings Fund Report: Chris Hamm, Nicholas Timmins Oct 2015

Courtesy Stephen Duckett
7 avoidable deaths 2013-4 notified CCOPM March 2015 – reviewed by Euan Wallace
response mostly appropriate, but processes were not able to detect deficiencies in clinical governance and “lacked robust capacity” for routine surveillance of serious clinical events
Scope (Expansive!)
• Does Department have adequate systems for safety and quality assurance?
– How can they be improved?
• Inclusion of mental health care, public and private sectors

Scope 2 • Governance
– Board capability – especially rural and regional (all honorary boards)
– Monitoring of clinical governance at Dept, health service and hospital level
• Especially challenging for rural and regional
– Use of information gained
• Information flow
– Availability of Q&S information to boards and CEOs
– Improved incident management implementation
– Flow of information between monitoring bodies (AHPRA etc)
• Clinical Engagement and Leadership
– Best approach to providing this to support CMO and dept. oversight of Q&S
– Strategy for promoting an improvement culture among management and clinicians
– How can the department lead Q&S agenda and engage clinicians?
• Patient experience of care
– What can the DHHS do to at system level to strengthen this?

Our aim is to recommend changes so that:
1. The department ensures hospitals are monitoring and improving the quality of care they provide
2. The department strengthens its own oversight of hospital safety and
quality in order to detect and investigate early warning signs suggesting potential failures of clinical governance
3. The community can verify that system and hospital governance
arrangements identify and rectify defects in care, and continuously improve the processes and outcomes of care
4. Health workers welcome the department as a partner in
improving quality and safety of care
5. The culture of the department and health services will prioritise patient safety and continuous improvement of care.


18
Culture
‘the only thing of real importance
that leaders do is to create and
manage culture’
Schein, E.H. (1992) Organizational culture and leadership, Jossey Bass, San Francisco.
Courtesy S Duckett
Key Findings - 1
1. Knowledge is not being shared and implemented widely
2. Costs of poor care often hidden within hospitals and from patients
1:10 patients suffers complication of hospitalisation
50% of these “avoidable”
3. Hospitals need strong oversight and support by system managers.
System managers should use economies of scale to coordinate, encourage and facilitate improvement
4. Department is struggling to oversee and support Q&S care.
Insufficient information to ensure minister and public re Q&S
Incident management system not up to the task
Focus has tended to be on performance/access KPIs
Over reliance on accreditation
Expert committees are fragmented and sometimes poorly resourced with information

Key Findings cont….
5. Governance of hospitals inadequate Responsibility devolved to boards which may lack resources/information/expertise
6. Support for Q&S improvement variable with duplication and variation in quality.
7. Limited response to previous reports: X3 VAGO 2005-2016
8. DHHS has lost some internal capacity and widely uses consultants to manage Q&S initiatives

Targeting Zero Recommendations: Major Themes n 1 Safety and quality improvement must be a core goal of the department and system 21
2 All boards must be highly skilled, independent and effective 19
3 All hospitals should be held to account for improving safety and quality of care,
regardless of their size or sector 0
4 The flow of information in the health system must ensure deficiencies of care are
identified and focus attention on opportunities for improvement 58
5 All hospitals should have access to independent clinical expertise to help identify
deficiencies in care and focus attention on opportunities for improvement 7
6 Risk should be managed across the system so that hospitals only offer care that is
within their capabilities, with high-risk care concentrated in the centres where it is
safest
8
7 There must be robust assessment of clinical governance and hospital safety and
quality performance in the department 30
8 Mental health services must be adequately funded to allow delivery of timely, safe
and high-quality care 3
9 Clinical leaders must be engaged to strengthen, direct and lead efforts to improve
safety and quality of care 29
10 The system must have a stronger focus on improving patients' experiences of care 10
Total (some overlap) 179

22 Copyright © 2016 Wolters Kluwer Health, Inc. All rights reserved. Published by Lippincott Williams & Wilkins, Inc.
2
Effect of Hospital Volume on Surgical Outcomes After Pancreaticoduodenectomy: A Systematic Review and Meta-analysis. Hata, Tatsuo; Motoi, Fuyuhiko; MD, PhD; Ishida, Masaharu; MD, PhD; Naitoh, Takeshi; MD, PhD; Katayose, Yu; MD, PhD; Egawa, Shinichi; MD, PhD; Unno, Michiaki; MD, PhD Annals of Surgery. 263(4):664-672, April 2016. DOI: 10.1097/SLA.0000000000001437
FIGURE 3. Scatter plot of hospitals according to the median values of each included hospital group and postoperative mortality rates. PD indicates pancreaticoduodenectomy.
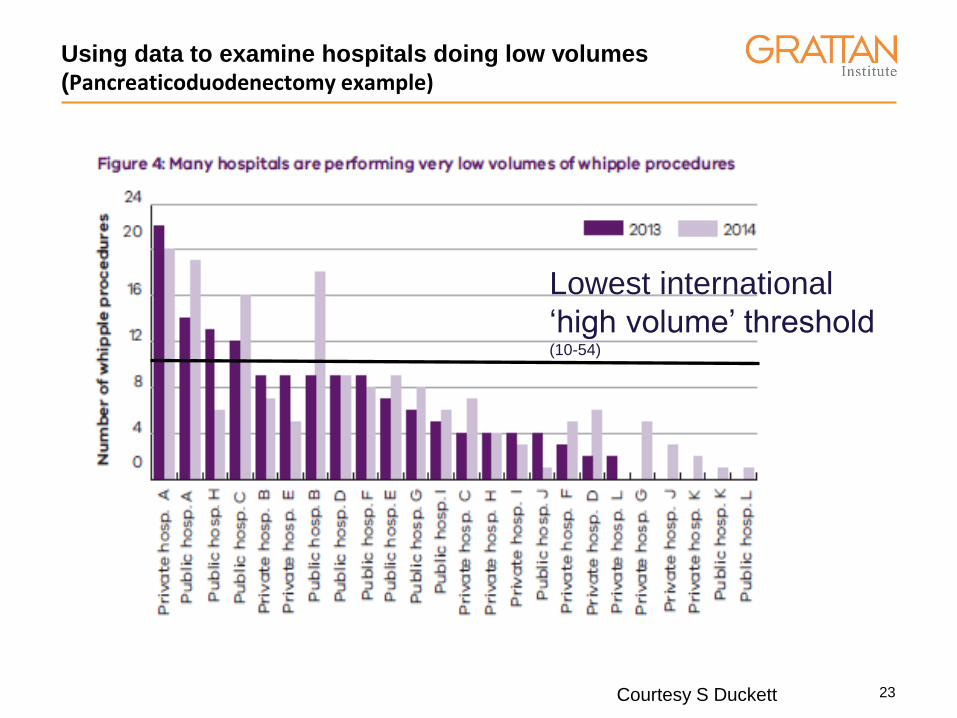
Things MACI might be interested in – 2 low volume Issue of low volume
Courtesy S Duckett
23
Using data to examine hospitals doing low volumes
(Pancreaticoduodenectomy example)
Lowest international
‘high volume’ threshold (10-54)
Courtesy S Duckett

24
Key themes for safety and quality
reform
1. Fostering a culture of continuous improvement and clinical
excellence in the health sector, including by engaging and
empowering clinicians in reform.
2. Strengthening oversight of both safety issues and clinical
governance by the Department, so that warning signs are detected
and acted upon in a timely manner.
3. Improving governance of hospitals, so that the public can be
confident that all hospitals - big and small, public and private - are
delivering safe care.
4. Advancing transparency within the health sector, so that
communities can verify that their local hospital is rapidly identifying
and rectifying important defects in care when they arise.
https://www2.health.vic.gov.au/hospitals-and-health-services/quality-safety-service/hospital-
safety-and-quality-review
Courtesy S Duckett

The Department’s Response: Overview of Better, Safer Care reforms
1. Enhance system leadership and strengthening clinical engagement
Support Safer Care Victoria (SCV) to lead quality and safety improvement across Victorian health services by providing support via a range of new quality and safety programs and utilising the experiences of frontline clinicians through revitalised clinical networks and establishment of the Victorian Clinical Council (VCC). Strengthened Clinical Networks. Alignment with Better Care Victoria (BCV), DHHS innovation and improvement arm
2. Make better use of information and data
Support the Victorian Agency for Health Information (VAHI), and a range of initiatives to provide timely, high quality information that ensures the health sector and community are better informed about health services; and that health services have access to better information about their performance.
3. Improve sector governance
Lead a range of new governance initiatives to support the work of the Boards Ministerial Advisory Committee (BMAC), to ensure that boards are independent, skilled and effective.
4. Strengthen departmental oversight
Initiate new programs to enhance the role of the department as system manager in oversighting hospital patient safety and quality performance and seek funding for a range of initiatives to better support smaller rural hospitals.
Introduce a new Quality and Safety Bill into Parliament in 2017 to address a number of Targeting zero’s recommendations that require a legislative response with a major review of the Health Service Act 1988 to follow.
Adapted from Better, Safer Care Victorian DHHS 2016

Philosophical Changes
• Onus on clinicians at all levels to step up and hold themselves accountable for quality and safety in the system (rather than just the patient in front of them, their practice or unit). – No longer good enough to “leave it to the quality unit or DHHS”.
– Supports required to help clinicians get requisite skills and experience
• Fit for purpose – volume issues, capability matching, governance and improvement support where it is needed
• Transparency to assist the public in knowing how the health service is performing.
• Linking incident reports directly to quality outcomes (ie its about improving the system rather than apportioning blame)

Opportunities for clinicians
• Local improvement opportunities • Victorian Clinical Council • Clinical Networks • DHHS advisory committees • Emerging leaders group • BCV project funding • Hospital board membership • Clinical governance training/engagement • Hospital/Health service board roles

“The standard you walk past is the standard you are prepared to accept”
David Hurley
(former Chief of Defence and Governor of NSW)


The role of boards in
clinical governance:
activities and attitudes
among members of
public health service
boards in Victoria
Bismark MM, Simon J.
Walter SJ and
Studdert DM Australian Health Review, 2013, 37, 682–687
Strengthened democratic accountability (Avoiding the Lake Wobegon effect*)
Unskilled and unaware
of it: how difficulties in
recognizing one's own
incompetence lead to
inflated self-
assessments.
Kruger J, Dunning D, J
Pers Soc Psychol 1999
*Garrison Keiller

Board skills rubric for clinical governance competency

PRONE Score
The PRONE score: an algorithm for predicting doctors’ risks of
formal patient complaints using routinely collected administrative
data
Spittal MJ, Bismark MM, Studdert D
PRONE score as a leading indicator

Courtesy S Duckett

Legal issues from a clinicians perspective
• New expectations for board members – Skills and information
• Shared responsibility for hospital oversight in Health Services Act
• Improved transparency of outcomes for public
• Whistleblower protection
• Sharing of complaints data with AHPRA/HCEs/VMIA
• Extension of most implications to private hospitals
• No fault compensation for medical injuries

• Victoria has the building blocks to provide care as good as anywhere in the world.
• We have some of the most competent practitioners – we need to support them to work in a team environment geared towards continuous improvement of safer care, accountable always to the community we serve.
• Clinician engagement is the key: • at the bedside but also • at hospital management, • executive board and • DHHS levels.
New reality for clinicians
“How wonderful it is that nobody need wait a single moment before starting to improve the world.”
Anne Frank

Thank you to the hundreds of people who contributed data, advice, commentary and support for
this review and
to all those who work tirelessly every day to care for us when we are sick and to keep
us well the rest of the time
[email protected] Stephen Duckett