hay fever - pharmaceutical society of australia september... · facts behind the fact card hay...
TRANSCRIPT

september 2015Professional develoPment and Practice suPPort for the self care Program
Vol.16 number 8
Print Post aPProved 100019799
Hay fever

2 inPHARMation September 2015 I © Pharmaceutical Society of Australia Ltd.
John bell says
Vol.16 number 8
september 2015
This publication is supplied to subscribers of the Self Care program. For information on the program, contact PSA at the address below.
Advertising policy: inPHARMation will carry only messages that are likely to be of interest to members and which do not reflect unfavourably, directly or by implication, on the pharmacy profession or the professional practice of pharmacy. Messages that do not comply with this policy will be refused.
Views expressed by authors of articles in inPHARMation are their own and not necessarily those of PSA, nor PSA editorial staff, and must not be quoted as such.
The information contained in this material is derived from a critical analysis of a wide range of authoritative evidence. Any treatment decisions based on this information should be made in the context of the clinical circumstances of each patient.
PSA4618
ISSN: 2201-3911
Photographs in non-news articles in inPHARMation are for illustrative purposes only and the models appearing in these photographs should not be presumed to endorse any product mentioned in the article or suffer from any condition mentioned in the article.
Pharmaceutical Society of auStralia ltd. abn 49 008 532 072
Po box 42, deakin West act 2600
p: 1800 303 270 or 1300 369 772 e: [email protected]
www.psa.org.au© Pharmaceutical Society of Australia Ltd., 2015
This magazine contains material that has been provided by the Pharmaceutical Society of Australia (PSA), and may contain material provided by the Commonwealth and third parties. Copyright in material provided by the Commonwealth or third parties belong to them. PSA owns the copyright in the magazine as a whole and all material in the magazine that has been developed by PSA. In relation to PSA owned material, no part may be reproduced by any process except in accordance with the provisions of the Copyright Act 1968 (Cth), or the written permission of PSA. Requests and inquiries regarding permission to use PSA material should be addressed to: Pharmaceutical Society of Australia, PO Box 42, Deakin West ACT 2600. Where you would like to use material that has been provided by the Commonwealth or third parties, contact them directly.
self care fact cards
Keep your Fact Cards up-to-date. Re-order any title at any time at www.psa.org.au/selfcare
efactcards
Self Care Fact Cards are now available online. To gain access contact [email protected]
counter connection certificates
You can now print a certificate upon successful completion of Counter Connection modules and include in your training records for QCPP. Available at: www.psa.org.au/selfcareeducation
display units
Self Care display units can be ordered at: www.psa.org.au/services. Product category is Self Care display options.
sponsorship
For sponsorship and advertising enquiries contact:
Joey Calandra PSA Corporate Relations Manager p: 03 9389 4021 e: [email protected]
production coordinator Simon Carroll
Contributor Sarah Gray
peer review Maureen Narayan-Ram
Layout Hiba Attar
Contents
pHarmaCist CpD 4 facts behind the fact card: Hay fever
pHarmaCy assistant’s eDuCation10 counter connection: Hay fever
reguLars3 health column
16 noticeboard
Hay fever occurs in response to allergens including pollens, house dust mites, moulds and animal dander.
See page 4, Facts Behind the Fact Card: Hay fever

3inPHARMation September 2015 I © Pharmaceutical Society of Australia Ltd.
hay feverby sarah gray
Health column
many people suffer from allergic rhinitis or as it is commonly known, hay fever. about 15% of australians have experienced hay fever symptoms; rhinorrhoea (sneezing, itching of eyes, throat and nose, red and watery eyes) and nasal congestion.
hay fever is defined based on the timing and duration of a person’s symptoms. intermittent allergic rhinitis (previously known as seasonal rhinitis) refers to symptoms occurring on less than 4 days a week or for less than 4 weeks at a time. Persistent allergic rhinitis refers to symptoms that occur for more than 4 days a week and continue for more than 4 weeks.
symptoms of allergic rhinitis are often triggered by airborne allergens such as pollens and grass seeds. these triggers often appear at certain times of the year such as spring and early summer when the
pollen count is high. however, dust mites, moulds and animal dander that occur all-year-round also trigger allergic rhinitis. other triggers include chemical irritants such as cigarette smoke.
allergic rhinitis is often under-diagnosed and under-treated. Yet it can have a significant impact on a person’s quality of life, ability to sleep and work. managing allergic rhinitis involves minimising exposure to allergens, pharmacotherapy and immunotherapy. it is often difficult to minimise allergen exposure, particularly if the allergen is airborne such as pollen. remaining indoors or wearing masks or glasses are strategies that may be beneficial, if somewhat impractical.
medicines used to treat allergic rhinitis include antihistamines, intranasal corticosteroids and decongestants.
the selection of medicines is based on the duration and severity of the person’s symptoms and the impact on the person’s lifestyle. immunotherapy may be recommended when symptoms are severe and avoidance strategies and medicines have been ineffective or inappropriate. it is used mainly for patients with moderate-to-severe symptoms.
this issue of inPharmation magazine reviews the causes and triggers of intermittent and persistent allergic rhinitis. the common symptoms are described as well as how to differentiate between the allergic and non-allergic condition by reviewing characteristic symptoms. management options, including pharmacotherapy, are reviewed.
PSA offers professional development
anywhere, anytime with
online CPD
P: 1300 369 772 » [email protected] » www.psa.org.au/short-courses
PSA
4830
AACP-approved No. 2- 15-198
The PSA MMR Stage 1 course is now available online
» Start anytime and work at your own pace
» Receive instant feedback as you progress
» Complete this first step to being renumerated for conducting HMRs and RMMRs
Enrol now www.psa.org.au/short-courses
Take the first step to become a consultant pharmacist

4 inPHARMation September 2015 I © Pharmaceutical Society of Australia Ltd.
John bell says
Hay feverby sarah gray
learning objectivesafter reading this article, pharmacists should be able to:
• identify the causes and triggers of hay fever
• describe the common signs and symptoms of hay fever
• discuss the pharmacological and non-pharmacological management options for hay fever.
Competencies addressed: 3.1, 3.2, 6.1, 6.2.
This education module is independently researched and compiled by PSA-commissioned authors and peer reviewed.
allergic rhinitis (commonly known as hay fever) is a non‑infectious form of rhinitis.1 it is characterised by rhinorrhoea (sneezing, itching of eyes, throat and nose, red and watery eyes) and nasal congestion.2 Hay fever occurs in response to allergens including pollens, house dust mites, moulds and animal dander.3,4 it is one of the most common chronic respiratory conditions in australia, affecting around 15% of australians, and can significantly impact a patient’s quality of life.5,6
Facts behind the Fact Card hay fever Pharmacist cPd module number 263
Michaela, aged 27 years, comes into the pharmacy with rhinorrhoea, itchy eyes and sneezing. She works as a landscape gardener. When these symptoms occur, she takes one telfast (fexofenadine) 120 mg tablet in the morning for two weeks. Previously, the antihistamine relieved her symptoms but this year it did not.
Pathogenesisallergic rhinitis is associated with an immunoglobulin e (ige)-mediated immune response after exposure to allergens.1 following exposure, chemical mediators, such as histamine, are released from mast cells in the nasal mucosa. this causes epithelial permeability to increase, resulting in movement of inflammatory cells to the area and an allergic response. sneezing occurs within minutes of exposure to the allergen. nasal secretions increase within 15–20 minutes. nasal obstruction may also occur about 6–12 hours later.7
triggerstriggers for hay fever include allergens such as grass, weed and tree pollens. these triggers tend to appear at certain times of the year, often in spring, and are known as intermittent triggers. other triggers, such as dust mites, cat and dog dander, persist all year round. most people are sensitised to both intermittent and persistent triggers through repeated exposure.1,4 once an individual is sensitised, even non-specific triggers or small amounts of an allergen can cause a rapid allergic response and severe symptoms.4 hay fever can also be aggravated by chemical irritants such as cigarette smoke and chemicals and irritants associated with the workplace (e.g. in manufacturing processes, hairdressing and nail salon chemicals).1,8
Symptomsthe duration of symptoms is used to classify hay fever.2 if the symptoms occur intermittently (lasting for less than 4 days a week or for less than 4 weeks) the condition is known as intermittent allergic rhinitis. however, if the symptoms persist for more
1 75GrouP 2
up
to
cPd creditS

5inPHARMation September 2015 I © Pharmaceutical Society of Australia Ltd.
Practice point 1
patient symptom‑based questionsuse symptom-based questions to gather information6:
• What are your main symptoms (e.g. rhinorrhoea, sneezing, itchy nose, nasal congestion)?
• do you have eye symptoms (e.g. itchy or watery eyes)?
• have you ever had hay fever, or asthma diagnosed by a doctor (asthma and allergic rhinitis often co-exist)?
• do you have a family member with allergies or asthma?
• how long have you had the symptoms?
• do the symptoms occur all year round or at a particular time of the year?
• are you aware of anything that seems to trigger the symptoms (e.g. being outdoors or around animals, doing a particular activity at work or at home)?
• is your nasal discharge clear and watery (purulent discharge suggests infection)?
• are you experiencing any wheezing or shortness of breath (may indicate asthma)?
• do you have earache (may indicate otitis media)?
• do you have facial pain (may indicate sinusitis)?
• What medicines have you already tried for these symptoms? Were they effective? ask if the patient is using a nasal decongestant)
• do you have any other medical conditions and are you taking any other medicines?
• are you pregnant (may indicate rhinitis of pregnancy)?
Facts behind the Fact Cardhay fever Pharmacist cPd module number 263
than 4 days a week and last for more than 4 weeks, the condition is then classified as persistent allergic rhinitis.2
hay fever can be further classified based on the severity of symptoms. symptoms are classified as either mild or moderate-to-severe based on the impact they have on sleep, activities of daily living, work and school performance, and sporting and leisure activities as well as the degree to which they are troublesome.1
symptoms associated with hay fever may vary among patients and include3,6,9:
• nasal symptoms such as itching, sneezing, rhinorrhoea
• sinus-related congestion, postnasal drainage, headache
• itchy, red or teary eyes
• wheezing, cough and shortness of breath
• itchy ears, throat and voice
• sleep disturbances and lethargy.
risk factorsthere are both genetic and environmental risk factors that influence the development of allergic rhinitis.10
genetic factors – if a child has one parent with atopy (allergies), he or she has a 30% risk of developing allergic rhinitis. if both parents are atopic this risk increases to 50–70%. having other allergic conditions also predisposes a person to allergic rhinitis. allergic rhinitis and asthma frequently co-exist and allergic rhinitis has been identified as an independent risk factor for asthma. a person with concurrent asthma has an 80% chance of developing allergic rhinitis.6,11
age – the median onset age for intermittent allergic rhinitis is 15 years compared with 20 years for persistent allergic rhinitis.4
environmental and occupational exposure – in susceptible people (e.g. with a personal or family history of atopy) exposure to allergens in their living, school, work or recreational environment may produce sensitisation and increase the risk of developing intermittent allergic rhinitis.4,12
Diagnosishay fever is frequently trivialised, under-diagnosed and under-treated. however, it can have a substantial impact on a person’s quality of life and performance at home, school or work.3,7 accurate diagnosis will direct treatment.
initially, establish if the patient has an allergic or non-allergic condition by reviewing the patient’s symptoms. Patients presenting with symptoms of sneezing, rhinorrhoea, nasal itching and conjunctivitis, which may be worse in the morning and evening, usually have allergic rhinitis. non-allergic rhinitis may be caused by hot, spicy foods (gustatory rhinitis), certain medicines, alcoholic drinks, sudden changes in temperature, cold, dry air, inhaled irritants (e.g. tobacco smoke, chemicals) and emotional stress.13
overuse of intranasal decongestants (rhinitis medicamentosa) is also associated with nasal blockade.1 see table 1 for a differential diagnosis.
determine the severity (mild or moderate-to-severe) and frequency (intermittent or persistent) of the condition.8 if the patient does not provide sufficient information about their symptoms, use structured questioning to obtain more information6 (see Practice point 1).
if the diagnosis is in doubt, the patient should be referred to a doctor for further investigation (see Practice point 2).
managementthe management of hay fever involves three main strategies6:
• allergen minimisation• treatment• immunotherapy.
hay fever is associated with other inflammatory conditions (e.g. asthma, conjunctivitis, sinusitis) and, if left untreated, these conditions may worsen in hay fever sufferers.6 before offering treatment options, consider the patient’s age, pregnancy and breastfeeding status and medical and hypersensitivity history.2
Allergen minimisation
minimising exposure to allergens is an important strategy in the management of hay fever and is most feasible if the allergen associated with producing the allergic reaction has been identified (see Immunotherapy).1
6 inPHARMation September 2015 I © Pharmaceutical Society of Australia Ltd.
John bell says
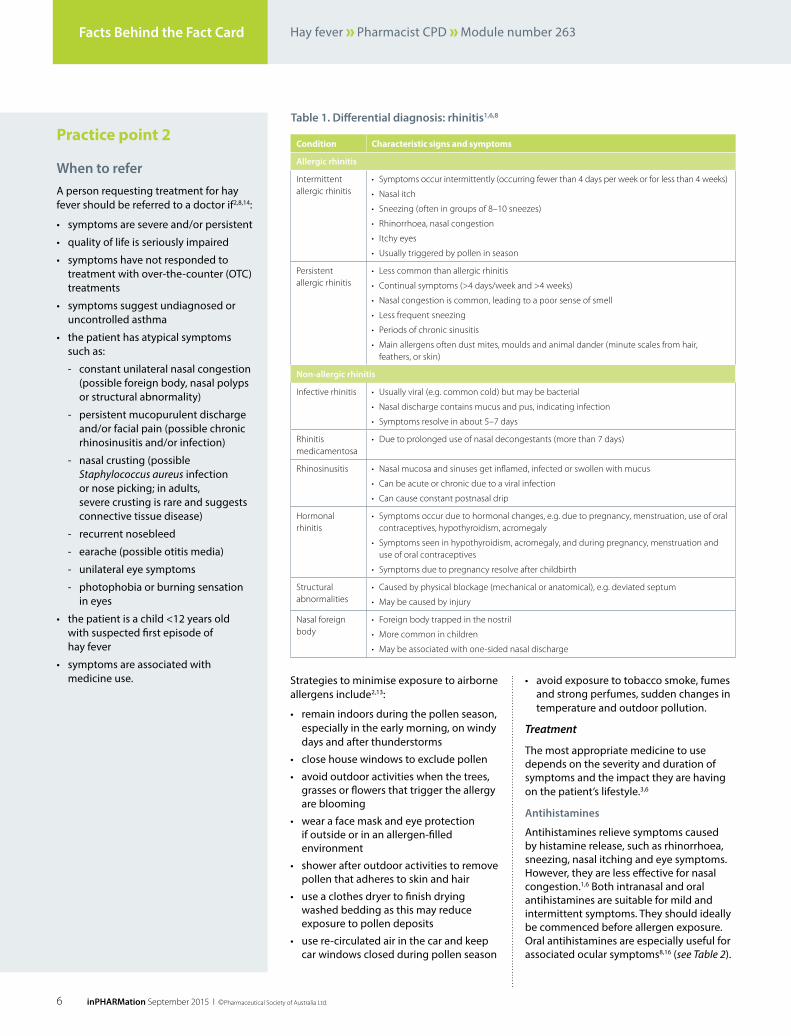
Practice point 2
When to refera person requesting treatment for hay fever should be referred to a doctor if2,8,14:
• symptoms are severe and/or persistent
• quality of life is seriously impaired
• symptoms have not responded to treatment with over-the-counter (otc) treatments
• symptoms suggest undiagnosed or uncontrolled asthma
• the patient has atypical symptoms such as:
- constant unilateral nasal congestion (possible foreign body, nasal polyps or structural abnormality)
- persistent mucopurulent discharge and/or facial pain (possible chronic rhinosinusitis and/or infection)
- nasal crusting (possible Staphylococcus aureus infection or nose picking; in adults, severe crusting is rare and suggests connective tissue disease)
- recurrent nosebleed
- earache (possible otitis media)
- unilateral eye symptoms
- photophobia or burning sensation in eyes
• the patient is a child <12 years old with suspected first episode of hay fever
• symptoms are associated with medicine use.
Facts behind the Fact Card hay fever Pharmacist cPd module number 263
strategies to minimise exposure to airborne allergens include2,13:
• remain indoors during the pollen season, especially in the early morning, on windy days and after thunderstorms
• close house windows to exclude pollen
• avoid outdoor activities when the trees, grasses or flowers that trigger the allergy are blooming
• wear a face mask and eye protection if outside or in an allergen-filled environment
• shower after outdoor activities to remove pollen that adheres to skin and hair
• use a clothes dryer to finish drying washed bedding as this may reduce exposure to pollen deposits
• use re-circulated air in the car and keep car windows closed during pollen season
• avoid exposure to tobacco smoke, fumes and strong perfumes, sudden changes in temperature and outdoor pollution.
Treatment
the most appropriate medicine to use depends on the severity and duration of symptoms and the impact they are having on the patient’s lifestyle.3,6
antihistamines
antihistamines relieve symptoms caused by histamine release, such as rhinorrhoea, sneezing, nasal itching and eye symptoms. however, they are less effective for nasal congestion.1,6 both intranasal and oral antihistamines are suitable for mild and intermittent symptoms. they should ideally be commenced before allergen exposure. oral antihistamines are especially useful for associated ocular symptoms8,16 (see Table 2).
table 1. Differential diagnosis: rhinitis1,6,8
condition characteristic signs and symptoms
allergic rhinitis
Intermittent allergic rhinitis
• Symptoms occur intermittently (occurring fewer than 4 days per week or for less than 4 weeks)
• Nasal itch
• Sneezing (often in groups of 8–10 sneezes)
• Rhinorrhoea, nasal congestion
• Itchy eyes
• Usually triggered by pollen in season
Persistent allergic rhinitis
• Less common than allergic rhinitis
• Continual symptoms (>4 days/week and >4 weeks)
• Nasal congestion is common, leading to a poor sense of smell
• Less frequent sneezing
• Periods of chronic sinusitis
• Main allergens often dust mites, moulds and animal dander (minute scales from hair, feathers, or skin)
non‑allergic rhinitis
Infective rhinitis • Usually viral (e.g. common cold) but may be bacterial
• Nasal discharge contains mucus and pus, indicating infection
• Symptoms resolve in about 5–7 days
Rhinitis medicamentosa
• Due to prolonged use of nasal decongestants (more than 7 days)
Rhinosinusitis • Nasal mucosa and sinuses get inflamed, infected or swollen with mucus
• Can be acute or chronic due to a viral infection
• Can cause constant postnasal drip
Hormonal rhinitis
• Symptoms occur due to hormonal changes, e.g. due to pregnancy, menstruation, use of oral contraceptives, hypothyroidism, acromegaly
• Symptoms seen in hypothyroidism, acromegaly, and during pregnancy, menstruation and use of oral contraceptives
• Symptoms due to pregnancy resolve after childbirth
Structural abnormalities
• Caused by physical blockage (mechanical or anatomical), e.g. deviated septum
• May be caused by injury
Nasal foreign body
• Foreign body trapped in the nostril
• More common in children
• May be associated with one-sided nasal discharge

7inPHARMation September 2015 I © Pharmaceutical Society of Australia Ltd.
Practice point 3
Correct use of nasal spraysthe correct use of nasal sprays will deliver a dose throughout the lining of the nasal cavity, including the side wall, rather than to the front part of the nose and nasopharynx.1,6,8
correct technique for using a nasal spray effectively and safely1:
• clear the nasal passages first; using a saline nasal spray may be helpful.
• shake the bottle and follow the manufacturer’s advice (package insert) about priming if needed.
• bend your neck forward and look down.
• for intranasal corticosteroids (incs), use your right hand for the left nostril and vice versa. Put the nozzle just inside the nose, aiming towards the outer wall.
• change hands and repeat for the other side.
• avoid sniffing too hard or the liquid is likely to go straight down the throat.
remind patients to:
• prime the spray device before use
• tilt their heads forward rather than back
• not use saline drops or other nasal irrigations immediately after using an incs device
• avoid blowing the nose soon after using the spray device as this could dislodge the medicine.
related fact cards Hay fever
Sinus problems
Facts behind the Fact Cardhay fever Pharmacist cPd module number 263
oral antihistamines are classified as1,2,6,14:
• less-sedating (e.g. cetirizine, desloratadine, fexofenadine, levocetirizine, loratadine). they are less likely to cause sedation and have little or no anticholinergic effects (cetirizine and levocetirizine are more likely to cause sedation). they rapidly relieve symptoms of sneezing and rhinorrhoea and may also ease ocular symptoms
• sedating (e.g. dexchlorpheniramine, promethazine). they are not recommended for the treatment of rhinitis but can be used if sedation is required. they can cause anticholinergic side effects (e.g. dry mouth and eyes, urinary retention and worsening of glaucoma).
there is little difference in efficacy between antihistamines, and patient choice often guides treatment selection.1,14 less-sedating antihistamines are often preferred due to their longer duration of action, allowing once-daily dosing.1,6 less-sedating antihistamines can be used by adults and children.1
intranasal antihistamines (e.g. levocabastine, azelastine) are as effective as oral antihistamines but have a faster onset of action.1 twice-daily dosing is required.1,6,14 refer to Practice point 3 for administration technique.
ocular antihistamines (e.g. azelastine, levocabastine) may be required to treat allergic conjunctivitis associated with hay fever.1
intranasal corticosteroids (inCs)
intranasal corticosteroids (incs) are used to both relieve and prevent the development of hay fever symptoms.2 they produce local anti-inflammatory effects and vasoconstriction as well as decreasing capillary permeability and mucus production.1,14 incs are more effective than antihistamines in the treatment of nasal symptoms (especially congestion and impaired sense of smell).6
incs are recommended as first-line therapy for moderate-to-severe hay fever associated with frequent symptoms and nasal congestion. they have a slow onset of action and usually start relieving symptoms within a few days, but need to be trialled for a month to gauge efficacy.1 they can be used prophylactically in patients with more severe symptoms. for seasonal hay fever caused by pollen exposure, they should be commenced two weeks before the start of the pollen season. incs can also
be used ‘as required’ for nasal symptoms. they have similar or better efficacy than oral antihistamines. however, ‘as required’ use is less effective than continuous treatment.6 the initial incs dose, for both symptom relief and prevention, should be continued for one month then reduced to a maintenance dose (see Table 2).1
incs can be recommended for both adults and children with moderate-to-severe hay fever (even if the patient is already using inhaled corticosteroids for asthma). for those with troublesome symptoms, an agent with a more rapid onset of action (e.g. oral h1-antihistamine or short-term intranasal decongestant) can be added to therapy.9
a combination of an intranasal antihistamine with a corticosteroid (azelastine and fluticasone propionate) can be used to provide rapid relief of symptoms as well as an anti-inflammatory effect. it is effective in the treatment of hay fever.1
incs are well tolerated, with crusting, dryness and minor epistaxis (nosebleed) occuring in about 5% of patients.6 if nosebleeds do occur, refer the patient for further medical review.6 there are no side effects associated with long-term use of incs in the recommended dose range. long-term use of incs in children should be at the lowest effective dose.7
the correct administration of incs and consumer adherence are vital for treatment success. regularly advise consumers on the correct use of incs, demonstrating the most effective technique.3 for videos demonstrating administration, see the national asthma council website at: www.nationalasthma.org.au/how‑to‑videos/using‑your‑nasal‑spray (see Practice point 3).
Decongestants
decongestants may be used short-term to relieve nasal congestion associated with hay fever.1 topical nasal decongestants may be useful at the start of treatment to open nasal passages.7 if antihistamines and intranasal corticosteroids have not relieved nasal congestion, oral decongestants often provide rapid relief.1
decongestants are sympathomimetics that produce vasoconstriction of dilated nasal vessels, reducing tissue swelling and nasal congestion. they have no effect on other symptoms of hay fever. they are not recommended for use in children under six years of age and should be used cautiously in children between six and twelve years of age.1,14

8 inPHARMation September 2015 I © Pharmaceutical Society of Australia Ltd.
John bell saysFacts behind the Fact Card hay fever Pharmacist cPd module number 263
Immunotherapy
allergen immunotherapy (i.e. desensitisation) is used to treat moderate-to-severe hay fever when there has been poor response to other management options (such as allergen avoidance strategies and drug treatments)1 and in the presence of comorbid conditions or complications.15
before treatment is started, the allergen must be defined by the presence of specific ige and confirmed by either skin prick test and/or radioallergosorbent test (rast). treatment with either subcutaneous or sublingual immunotherapy continues for between 3–5 years and symptom improvement may be delayed for 6–12 months.1,16
subcutaneous immunotherapy must be given under medical supervision due to the risk of immediate- or slower-onset systemic reactions (e.g. mild urticaria and rhinitis, through to angioedema, severe asthma and anaphylactic shock).1 sublingual immunotherapy is safer and effective in both adults and children with grass pollen and dust mite allergy, but is more expensive than subcutaneous immunotherapy.1 immunotherapy is often combined with pharmacotherapy and avoidance of allergens.15
ipratropiumipratropium is an anticholinergic medicine with a rapid onset of action and a prolonged effect (4–12 hours).1 it can be used with incs or an antihistamine if rhinorrhoea is severe.1 adverse effects include nasal dryness, nosebleed, dry mouth and taste disturbance.14 there have been rare reports of urinary retention and allergic reactions (urticaria, angioedema, rash, bronchospasm).14
saline nasal drops/spraysodium chloride 0.9% solution (nose drops, irrigation or spray) may help to thin nasal secretions and relieve nasal congestion. saline can be used before an incs to clear mucus and improve mucosal contact with the corticosteroid, potentially reducing the dose of incs required to be effective.2 in children, it should be used in preference to an intranasal sympathomimetic as it is safe and inexpensive.14 saline eye drops may be adequate to reduce ocular symptoms associated with allergic conjunctivitis, which can be a predominant symptom of allergic rhinitis.2
oral decongestants (e.g. phenylephrine, pseudoephedrine)14:
• can cause systemic adverse effects, including central nervous system (cns) stimulation, insomnia, irritability, dizziness, headache, tremor, palpitations, tachycardia and hypertension
• are contraindicated in severe coronary artery disease and in severe or uncontrolled hypertension.
intranasal decongestants (e.g. oxymetazoline, phenylephrine, tramazoline, xylometazoline)1,6:
• are more effective than oral decongestants if nasal congestion is a problem
• should not be used for more than 3 days in any age group, as prolonged use causes rebound congestion (rhinitis medicamentosa)
• have significant adverse effects (including somnolence, convulsions, bradycardia, hypoventilation and hypothermia). these have been reported after use of nasal or oral decongestants in children under 6 years of age.
other therapies
montelukastmontelukast is a leukotriene receptor antagonist that reduces inflammation.6 it is as effective as an oral antihistamine, but less effective than incs for treating hay fever.1 in children, it is used to treat hay fever and asthma when they co-exist. it can be used if a child cannot tolerate an intranasal preparation.2
sodium cromoglycatesodium cromoglycate nasal spray is used prophylactically to treat mild-to-moderate allergic rhinitis.14 it is less effective than antihistamines and incs.7 intranasal cromoglycate may be preferred to incs in children.14 even though it has a good safety profile, the requirement for frequent dosing (up to five times daily) can compromise adherence.7
table 2. over‑the‑counter (otC) treatment options for allergic rhinitis2
intermittent Persistent
mild moderate‑to‑severe mild moderate‑to‑severe
Oral or intranasal antihistamine and/or decongestant
INCS and/or oral or intranasal antihistamine
INCS and/or oral or intranasal antihistamine
INCS and oral or intranasal antihistamine
if rhinorrhea – add ipratropium
if congestion – add short-term decongestant
Review after 2–4 weeks
If symptoms have improved continue treatment for 1 month
If symptoms have improved continue treatment as for persistent mild allergic rhinitis
If no improvement, treat as for moderate-to-severe persistent allergic rhinitis
If symptoms do not improve refer to a medical practitioner
antihistamines relieve symptoms caused by histamine release, such as rhinorrhoea, sneezing, nasal itching and eye symptoms.
“ “

9inPHARMation September 2015 I © Pharmaceutical Society of Australia Ltd.
Facts behind the Fact Cardhay fever Pharmacist cPd module number 263
case studyMichaela has characteristic signs and symptoms of moderate‑to‑severe hay fever. Apart from the fexofenadine, she confirms that she is not using any other medicines.
To make the correct diagnosis, you question Michaela about her symptoms. She says that they usually occur in springtime and involve itchy, watery eyes and a runny nose. During spring, these symptoms occur daily with episodes of repeated sneezing and intermittent nasal congestion. She has had these symptoms since childhood, but over the last 2–3 years the intensity of the symptoms has become more severe.
You recommend the use of an intranasal corticosteroid spray. You tell Michaela that the nasal spray may take several days to reach full effect and it should be used daily to maintain effectiveness. It is important to tell Michaela how to correctly use the nasal spray to maximise its effectiveness and avoid damage to the nasal passages. You demonstrate the correct use of the spray to her.
You also suggest the use of a saline nasal spray to clear the nasal passages before using the INCS. You instruct Michaela to use this spray before the INCS spray.
references1. Allergic rhinitis. In: eTG complete [online]. Melbourne:
Therapeutic Guidelines Limited; Feb 2015. At: http://online.tg.org.au/complete/tgc.htm#
2. Hay fever. In: Sansom LN, ed. Australian pharmaceutical formulary and handbook. 23rd edn. Canberra: Pharmaceutical Society of Australia; 2015. p. 538–41.
3. Sussman G, Sussman D, Sussman A. Intermittent allergic rhinitis. CMAJ 2010;182(9):935–7. At: www.ncbi.nlm.nih.gov/pmc/articles/PMC2882453/
4. Rutter P, Newby D. Rhinitis. In: Community Pharmacy: symptoms, diagnosis and treatment. Australia: Elsevier; 2009. p. 19–27.
5. Australian Institute of Health and Welfare. Allergic rhinitis (‘hay fever’) in Australia. Canberra: AIHW; 2011. At: www.aihw.gov.au/publication-detail/?id=10737420595
6. Allergic Rhinitis and its Impact on Asthma (ARIA) in collaboration with the World Health Organisation. ARIA in the pharmacy: management of allergic rhinitis symptoms in the pharmacy; 2003. At: www.whiar.org/docs/ARIA_Pharm_PG.pdf
7. Patient: allergic rhinitis. 2012. At: www.patient.co.uk/doctor/allergic-rhinitis
8. Hu W, Katelaris CH, Kemp AS. Allergic rhinitis: practical management strategies. Aust Fam Phys April 2008;37(4):214–20. At: www.racgp.org.au/%20afp/200804/200804hu.pdf
9. National Asthma Council Australia. Managing people with allergic rhinitis and asthma: information paper for health professionals; 2012. At: www.nationalasthma.org.au/uploads/publication/allergic-rhinitis-asthma-hp.pdf
10. Wang D. Risk factors of allergic rhinitis: genetic or environmental? Ther Clin Risk Manag 2005;1(2):115–23. At: www.ncbi.nlm.nih.gov/pmc/articles/PMC1661616/
11. National Asthma Council Australia. Allergic rhinitis (hay fever) and your asthma. 2015. At: www.nationalasthma.org.au/publication/allergic-rhinitis-hay-fever-and-your-asthma
12. Bousquet J, Khaltaev N, Cruz AA, et al. Allergic Rhinitis and its Impact on asthma (ARIA) 2008. Allergy: European Journal of Allergy and Clinical Immunology 2008:63(s.86):8–160. At: www.onlinelibrary.wiley.com/doi/10.1111/j.1398-9995.2007.01620.x/full
13. The Australasian Society of Clinical Immunology and Allergy (ASCIA). Allergen minimisation. 2010. At: www.allergy.org.au/patients/allergy-treatment/allergen-minimisation
14. Drugs for rhinitis and sinusitis. In: Rossi S, ed. Australian medicines handbook. Adelaide: Australian Medicines Handbook; 2015 At: https://amhonline.amh.net.au
15. Sheikh J. Allergic rhinitis. In: Kaliner M, ed. Medscape. 2015. At: www.emedicine.medscape.com/article/134825-overview#aw2aab6b2b2
Avoiding exposure to allergens such as pollens and grass seeds would also help Michaela. However, this is difficult for her as she usually works outside. You suggest she wear a face mask when outside and shower afterwards to remove allergens from her hair, skin and clothes. You give her the Hay fever Self Care Fact Card which lists some self‑care strategies to reduce allergens in the home.
You invite Michaela to return to the pharmacy if her symptoms do not improve. You advise Michaela that if she begins to experience facial pain and thick, coloured nasal discharge to return to the pharmacy or go to the doctor, as this could be a sign of an intranasal infection.

10 inPHARMation September 2015 I © Pharmaceutical Society of Australia Ltd.
John bell says
Circle one correct answer from each of the following questions
before undertaking this assessment, you need to have read the facts behind the fact card article and the associated fact cards. this activity has been accredited by Psa as a group 2 activity. 1.75 cPd credits (group 2) will be awarded to pharmacists with four out of five questions correct. Psa is accredited by the australian Pharmacy council to accredit providers of cPd activities for pharmacists that may be used as supporting evidence of continuing competence.
please submit your assessment by 31 october 2015
submit answers
submit online at www.psa.org.au/selfcare
fax: 02 6285 2869
mail: self care answers Pharmaceutical society of australia Po box 42 deakin West act 2600
accreditation number: cs150009
this activity has been accredited for 1.75 group 2 cPd credits suitable for inclusion in an individual pharmacist’s cPd plan.
— — — — — —Personal id number:
full name: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Pharmacy: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
address: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
suburb: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . state: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Postcode: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Hay feverassessment questions for the pharmacist
Please retain a copy for your own purposes. Photocopy if you require extra copies.
Facts behind the Fact Card hay fever Pharmacist cPd module number 263
1. triggers of hay fever include:
a) allergens.
b) Pathogens.
c) nasal blockage.
d) none of the above.
2. Which one of the following is a common symptom of hay fever?
a) cough.
b) sneezing.
c) sore throat.
d) none of the above.
3. risk factors that may influence the development of hay fever include:
a) family history of hay fever.
b) mould spores.
c) concomitant asthma.
d) all of the above.
4. Which one of the following statements about hay fever treatment is CorreCt?
a) intranasal sodium cromoglycate may be preferred to incs in children.
b) ipratropium nasal spray requires frequent dosing as its effect lasts for less than two hours.
c) montelukast is less effective than oral antihistamines and incs.
d) ipratropium nasal spray relieves rhinorrhoea, sneezing and nasal congestion.
5. Which one of the following symptoms of allergic rhinitis would necessitate referral to a doctor?
a) itchy, watery eyes.
b) shortness of breath and wheezing on exertion.
c) Watery, clear nasal discharge.
d) bilateral nasal blockage.

Hay fever is the common name for allergic rhinitis. It is an allergic reaction in the nose, throat and eyes. Hay fever often occurs in spring and summer, when it is caused by airborne pollens from trees, plants and grasses. Medicines can relieve and prevent symptoms of hay fever.
• reducedsenseofsmellandtaste
• snoring
• feelingtired,run-down,irritable.
Hayfeversymptomsareoftenworseinthemornings,onwindydaysandafterthunderstorms(whentheamountofpollenintheairishighest).
Hay fever(Allergic rhinitis)
EAR,NOSE&THROAT
Hayfever,orallergicrhinitis,isusuallycausedbyinhalingpollensthatarepresentintheairatcertaintimesoftheyear.Somepeoplehavesymptomsofallergicrhinitisallyearround.Constantsymptomscanbecausedbyallergenssuchasanimalhair,moulds,housedustmitesandcockroaches.Adoctorcanarrange‘allergyskintests’tohelpfindthecauseofallergicrhinitis.
Signs and symptomsSymptomsofallergicrhinitisinclude:
• sneezing
• runnynose
• blockednose(congestion)
• itchingnose,ears,mouthorthroat
• puffy,itchy,wateryandredeyes
• headaches
• post-nasaldrip(mucusfromthenoseandsinusesrunsdownthebackofthethroat),whichcancausecoughing
P: 1300 369 772 » [email protected] » www.psa.org.au/selfcare PSA is pharmacy.
Self Care health promotion resources
Order yours today at www.psa.org.au/selfcare/health-promotion-resources
‘Self Care – There’s nothing else in community pharmacy that o� ers such a complete, cost-e� ective, sta� friendly training program and resources to improve customer service and business results.’
– Samantha Kourtis, Pharmacy owner, PSA member and Self Care subscriber
ORDER YOUR
POSTERS TODAY!FREE

12 inPHARMation September 2015 I © Pharmaceutical Society of Australia Ltd.
John bell says
Sinuses are air-filled spaces within the bones around the nose. They are connected to each other, the nose and the throat. Sinuses can become inflamed and blocked, usually due to allergy, irritation or infection. Sinus problems can often be successfully treated with medicines available from a pharmacist.
• headache• tiredness• badbreath,badtasteinmouth• afeelingofpressureorfullnessin
the ears• toothache• sorethroat• nausea• fever.
Causes of sinus problemsSinusproblemsoccurwhentheliningofasinusbecomesinflamedandswollen,orwhennormalmucusdrainagefromasinusisblocked.
Thingsthatcancauseinflammationandswellingoftheliningofthesinusesinclude:
• infection–maybeviral(e.g.thecommoncold)orbacterial
• allergy(e.g.topollens,dustmites,moulds,animals)
Sinus problems
EAR,NOSE&THROAT
Inflammationofasinusiscalledsinusitis.Sinusitismaybeanacute(shortterm)conditionlastingafewdaysorweeks,orachronic(longterm)conditionlastingmanymonthsor years.
Signs and symptomsSymptomsofsinusproblemsinclude:
• blockednoseandsinuses(congestion)
• pain,discomfortorpressureovertheareaoftheaffectedsinus.Lyingdownorbendingforwardsoftenworsensthediscomfort
• post-nasaldrip(mucusfromthesinusesandnoserunsdownthebackofthethroat),whichcancausecoughing
• yelloworgreenmucusinthenoseor throat
• lossofsenseofsmellortaste
Hay fever is an allergic condition causing a runny, itchy nose, sneezing and itchy eyes. it is not contagious (cannot be caught from someone) and can occur at any time of the year. pollens as well as dust mites, mould and animal fur are all triggers for hay fever. Hay fever occurs commonly. about one‑fifth of the australian population is affected. it is most common in people aged between 25–44 years, but can be seen in younger or older people.
Hay feverby sarah gray This education module is independently researched and compiled by PSA-commissioned authors and peer reviewed.
Erica, 32 years of age, comes into the pharmacy sneezing and with a runny nose. She would like something to stop these symptoms. She is part of a morning walking group and is finding it hard to participate.
What causes hay fever?hay fever (also called allergic rhinitis) is caused by an allergic reaction to certain particles called allergens in the air. these allergens can be grass, weed or tree pollens, dust mites or animal fur. in spring there are a lot of grass and plant pollen particles in the air. People who get symptoms around this time are said to have intermittent or seasonal allergic rhinitis. People who get hay fever throughout the year are said to have persistent hay fever caused by dust mites, mould and animal fur or hair.
the allergic reaction in hay fever usually occurs in the lining of the nasal passages when the particles are inhaled (breathed in). the nasal passages become irritated, swollen and very sensitive (inflamed). the particles can also get trapped in the eyes causing increased watering and itchiness.
People with a family history of asthma or eczema are more likely to get hay fever. hay fever can’t be spread from person-to-person, unlike conditions such as the common cold which are caused by a virus.
SymptomsPeople with hay fever commonly experience a combination of the following symptoms:
• runny nose – usually clear and watery
• sneezing
• itchy nose
• red, puffy, watery, itchy eyes
• headaches.
hay fever symptoms are often worse in the mornings, on windy days and after thunderstorms (when the amount of pollen in the air is highest). ask customers about the symptoms they are experiencing, when they usually get them and if they know what might be causing them. the answers will guide your recommendation for treatment. by asking symptom-based questions, you can offer the most appropriate treatment or refer them to the pharmacist if necessary (see Box 1).
Counter Connection hay fever Pharmacy assistant’s education module 263
Hay fever is the common name for allergic rhinitis. It is an allergic reaction in the nose, throat and eyes. Hay fever often occurs in spring and summer, when it is caused by airborne pollens from trees, plants and grasses. Medicines can relieve and prevent symptoms of hay fever.
• reducedsenseofsmellandtaste
• snoring
• feelingtired,run-down,irritable.
Hayfeversymptomsareoftenworseinthemornings,onwindydaysandafterthunderstorms(whentheamountofpollenintheairishighest).
Hay fever(allergic rhinitis)
EAR,NOSE&THROAT
Hayfever,orallergicrhinitis,isusuallycausedbyinhalingpollensthatarepresentintheairatcertaintimesoftheyear.Somepeoplehavesymptomsofallergicrhinitisallyearround.Constantsymptomscanbecausedbyallergenssuchasanimalhair,moulds,housedustmitesandcockroaches.Adoctorcanarrange‘allergyskintests’tohelpfindthecauseofallergicrhinitis.
Signs and symptomsSymptomsofallergicrhinitisinclude:
• sneezing
• runnynose
• blockednose(congestion)
• itchingnose,ears,mouthorthroat
• puffy,itchy,wateryandredeyes
• headaches
• post-nasaldrip(mucusfromthenoseandsinusesrunsdownthebackofthethroat),whichcancausecoughing

13inPHARMation September 2015 I © Pharmaceutical Society of Australia Ltd.
advise customers that they can limit symptoms of hay fever by:
• checking the daily pollen count forecast on television or in the newspaper (over 50 is high) and staying indoors if the count is high
• remaining inside as much as possible in spring, on windy days or after thunderstorms
• wearing a face mask or glasses when outside if the pollen count is high
• dusting with a damp cloth to collect dust and pollen
• showering after being outside to remove any pollen in their hair or eyes.
treatmenthay fever treatment is based on how severe the symptoms are and how long the customer has had the symptoms. antihistamines, decongestants and intranasal corticosteroids (incs) are commonly-used medicines.
antihistaminesantihistamines act quickly and relieve mild hay fever symptoms such as a runny nose, nasal itching and sneezing. they may not be as effective in relieving symptoms of nasal congestion (blocked nose). either antihistamine nasal sprays or oral antihistamine tablets can be used to treat symptoms of hay fever. they are equally effective, but nasal sprays act faster than tablets.
People respond differently to different antihistamines, and a customer may need to try several before finding one that is most effective for them. there are two groups of antihistamines – less-sedating and sedating (see Table 1).
intranasal corticosteroids (inCs)intranasal corticosteroids (incs) can relieve and prevent symptoms of hay fever. they treat the same symptoms as antihistamines but are particularly effective for relieving nasal congestion. for adults and children over 12 years, the usual dose is two sprays in each nostril twice daily. examples of incs sprays include Beconase Allergy and Hayfever 12 hour, Rhinocort Hayfever, Telnase.
incs do not work immediately. some relief of symptoms may be felt within a few hours of starting treatment, but up to 2 weeks of regular use may be required before maximum effectiveness is reached. they must be used every day to continue working. When incs are first used, they may cause nasal stinging and itching, sneezing, sore throat, dry mouth, cough and, occasionally, nosebleed.
saline nasal spray or drops can be used to clear thick mucus from the nasal passages before using incs and this may improve their effectiveness. saline nasal drops and spray may also be useful to moisten nasal passages that have become dry from using incs. saline nasal spray or drops can be recommended for babies, children and pregnant women as a safe alternative to incs.
always show customers the correct method for using nasal sprays (see Practice point 3 in Facts Behind the Fact Card). a consumer leaflet on how to use nasal sprays is found at: www.nationalasthma.org.au/uploads/publication/intranasal‑corticosteroid‑spray‑technique.pdf
Decongestantsnasal decongestants are effective in relieving nasal congestion (blockage) but have no effect on other hay fever symptoms. they are available as oral tablets or nasal sprays. the nasal sprays are fast-acting and more effective than the tablets. customers may want to use them for a short-term period until their incs or antihistamines take full effect.
decongestant nasal sprays should only be used for 3 days. any longer use can cause rebound nasal congestion (blockage). the oral tablets do not produce rebound congestion, but may cause insomnia, dizziness, nervousness and heart palpitations. nasal decongestants are not recommended for children.
Counter Connectionhay fever Pharmacy assistant’s education module 263
table 1. types of antihistamines
less-sedating Sedating
• Used for treating sneezing and itching
• Pharmacy Only (Schedule 2) – can be supplied by a pharmacy assistant
• Less likely to cause drowsiness
• Examples: cetirizine (e.g Zyrtec, Alzene), loratadine (e.g. Allerdyne, Claratyne), fexofenadine (e.g. Telfast, Xergic)
• Cause sedation and drowsiness
• Useful if taken at night to help sleeping
• Pharmacist Only (Schedule 3) – must be supplied by a pharmacist
• Examples: cyproheptadine (e.g. Periactin), promethazine (e.g. Phenergan), dexchlorpheniramine (e.g. Polaramine)
• Please describe your symptoms
• When do the symptoms occur? do they occur all year round or at a particular time of the year?
• how long have you had the symptoms?
• are you aware of anything that seems to trigger the symptoms (e.g. being outdoors, around animals, playing sport, doing a particular activity at work or at home)?
• do your hobbies or occupation bring you into contact with any potential triggers for hay fever (e.g. smoke, fumes)?
• do you suffer from asthma, eczema or any other allergies?
• do you have a family member with allergies or asthma?
• What medicines have you already tried for these symptoms? Were they effective?
• do you have any other medical conditions and are you taking any other medicines?
box 1. ask customers symptom‑based questions about hay fever
Hay fever (also called allergic rhinitis) is caused by an allergic reaction to certain particles called allergens in the air.
“ “
14 inPHARMation September 2015 I © Pharmaceutical Society of Australia Ltd.
John bell says
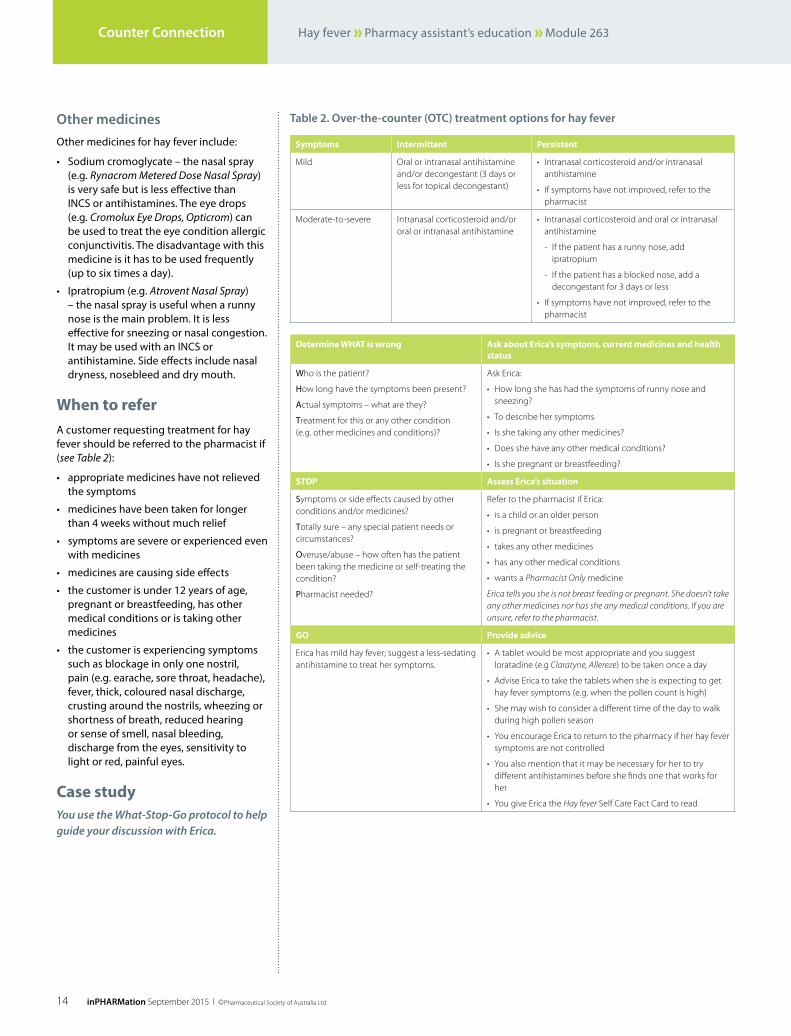
other medicinesother medicines for hay fever include:
• sodium cromoglycate – the nasal spray (e.g. Rynacrom Metered Dose Nasal Spray) is very safe but is less effective than incs or antihistamines. the eye drops (e.g. Cromolux Eye Drops, Opticrom) can be used to treat the eye condition allergic conjunctivitis. the disadvantage with this medicine is it has to be used frequently (up to six times a day).
• ipratropium (e.g. Atrovent Nasal Spray) – the nasal spray is useful when a runny nose is the main problem. it is less effective for sneezing or nasal congestion. it may be used with an incs or antihistamine. side effects include nasal dryness, nosebleed and dry mouth.
When to refera customer requesting treatment for hay fever should be referred to the pharmacist if (see Table 2):
• appropriate medicines have not relieved the symptoms
• medicines have been taken for longer than 4 weeks without much relief
• symptoms are severe or experienced even with medicines
• medicines are causing side effects
• the customer is under 12 years of age, pregnant or breastfeeding, has other medical conditions or is taking other medicines
• the customer is experiencing symptoms such as blockage in only one nostril, pain (e.g. earache, sore throat, headache), fever, thick, coloured nasal discharge, crusting around the nostrils, wheezing or shortness of breath, reduced hearing or sense of smell, nasal bleeding, discharge from the eyes, sensitivity to light or red, painful eyes.
case studyYou use the What‑Stop‑Go protocol to help guide your discussion with Erica.
Counter Connection hay fever Pharmacy assistant’s education module 263
determine What is wrong ask about erica’s symptoms, current medicines and health status
Who is the patient?
how long have the symptoms been present?
actual symptoms – what are they?
treatment for this or any other condition (e.g. other medicines and conditions)?
Ask Erica:
• How long she has had the symptoms of runny nose and sneezing?
• To describe her symptoms
• Is she taking any other medicines?
• Does she have any other medical conditions?
• Is she pregnant or breastfeeding?
StoP assess erica’s situation
symptoms or side effects caused by other conditions and/or medicines?
totally sure – any special patient needs or circumstances?
overuse/abuse – how often has the patient been taking the medicine or self-treating the condition?
Pharmacist needed?
Refer to the pharmacist if Erica:
• is a child or an older person
• is pregnant or breastfeeding
• takes any other medicines
• has any other medical conditions
• wants a Pharmacist Only medicine
Erica tells you she is not breast feeding or pregnant. She doesn’t take any other medicines nor has she any medical conditions. If you are unsure, refer to the pharmacist.
Go Provide advice
Erica has mild hay fever; suggest a less-sedating antihistamine to treat her symptoms.
• A tablet would be most appropriate and you suggest loratadine (e.g Claratyne, Allereze) to be taken once a day
• Advise Erica to take the tablets when she is expecting to get hay fever symptoms (e.g. when the pollen count is high)
• She may wish to consider a different time of the day to walk during high pollen season
• You encourage Erica to return to the pharmacy if her hay fever symptoms are not controlled
• You also mention that it may be necessary for her to try different antihistamines before she finds one that works for her
• You give Erica the Hay fever Self Care Fact Card to read
table 2. over‑the‑counter (otC) treatment options for hay fever
Symptoms intermittent Persistent
Mild Oral or intranasal antihistamine and/or decongestant (3 days or less for topical decongestant)
• Intranasal corticosteroid and/or intranasal antihistamine
• If symptoms have not improved, refer to the pharmacist
Moderate-to-severe Intranasal corticosteroid and/or oral or intranasal antihistamine
• Intranasal corticosteroid and oral or intranasal antihistamine
- If the patient has a runny nose, add ipratropium
- If the patient has a blocked nose, add a decongestant for 3 days or less
• If symptoms have not improved, refer to the pharmacist
15inPHARMation September 2015 I © Pharmaceutical Society of Australia Ltd.
Counter Connectionhay fever Pharmacy assistant’s education module 263
— — — — — —Personal id number:
full name: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Pharmacy: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
address: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
suburb: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . state: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Postcode: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
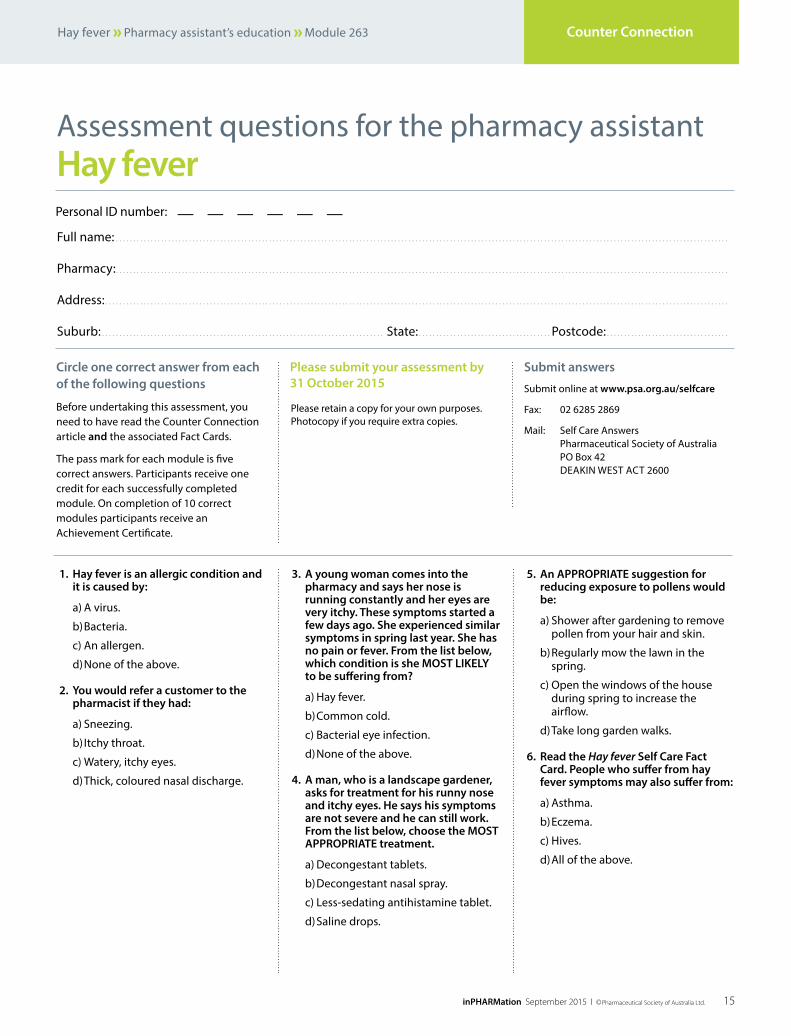
Circle one correct answer from each of the following questions
before undertaking this assessment, you need to have read the counter connection article and the associated fact cards.
the pass mark for each module is five correct answers. Participants receive one credit for each successfully completed module. on completion of 10 correct modules participants receive an achievement certificate.
please submit your assessment by 31 october 2015
Please retain a copy for your own purposes. Photocopy if you require extra copies.
Hay feverassessment questions for the pharmacy assistant
submit answers
submit online at www.psa.org.au/selfcare
fax: 02 6285 2869
mail: self care answers Pharmaceutical society of australia Po box 42 deakin West act 2600
1. Hay fever is an allergic condition and it is caused by:
a) a virus.
b) bacteria.
c) an allergen.
d) none of the above.
2. you would refer a customer to the pharmacist if they had:
a) sneezing.
b) itchy throat.
c) Watery, itchy eyes.
d) thick, coloured nasal discharge.
3. a young woman comes into the pharmacy and says her nose is running constantly and her eyes are very itchy. these symptoms started a few days ago. she experienced similar symptoms in spring last year. she has no pain or fever. From the list below, which condition is she most LiKeLy to be suffering from?
a) hay fever.
b) common cold.
c) bacterial eye infection.
d) none of the above.
4. a man, who is a landscape gardener, asks for treatment for his runny nose and itchy eyes. He says his symptoms are not severe and he can still work. From the list below, choose the most appropriate treatment.
a) decongestant tablets.
b) decongestant nasal spray.
c) less-sedating antihistamine tablet.
d) saline drops.
5. an appropriate suggestion for reducing exposure to pollens would be:
a) shower after gardening to remove pollen from your hair and skin.
b) regularly mow the lawn in the spring.
c) open the windows of the house during spring to increase the airflow.
d) take long garden walks.
6. read the Hay fever self Care Fact Card. people who suffer from hay fever symptoms may also suffer from:
a) asthma.
b) eczema.
c) hives.
d) all of the above.

16 inPHARMation September 2015 I © Pharmaceutical Society of Australia Ltd.
John bell says
What’s coming up in inPHARMation?next month’s inPHARMation will focus on foot care.
foot care is important because it can be a good reflection of a person’s health in general. untreated foot conditions can affect a person’s quality of life.
Pharmacists and pharmacy assistants can assist customers to maintain good foot health and provide appropriate advice on how to manage some common foot health problems. the october issue of inPHARMation discusses some of the common foot conditions often seen in pharmacy. facts behind the fact card outlines the common causes and management of foot conditions such as warts, corns and calluses, bunions and blisters. counter connection describes how foot conditions occur and what products are available to help treat them. it also has information on what advice to provide customers enquiring about foot care.
self care achievers Self Care presents certificates to staff who successfully complete a year of Counter Connection modules. We would like to congratulate the following people:
conferences
noticeboard
Conferencesblackmore’s institute 2nd annual symposiumtranslating research into practice23–24 OctoberPullman Melbourne, Albert Parkwww.ivvy.com/event/BIS15
11th national allied Health Conference9–11 NovemberCrown Convention Centre, Melbournewww.nahc.com.au
innovating to a self‑Care Future2015 asmi conference 11 NovemberWaterview Convention Centre, Homebush, Sydney Contact: [email protected].
australian pharmacy professional Conference 2016 17–20 MarchGold Coast Convention & Exhibition Centre, Queenslandhttp://appconference.com
national health calendar dates
september
1–30 prostate Cancer awareness monthwww.prostate.org.au
14–21 national stroke Weekndis.cerebralpalsy.org.au
october
19–25 sock it to suicide Weekwww.whitewreath.com
20 World osteoporosis Daywww.worldosteoporosisday.org
31 national bandana Daywww.canteen.org
november
14 World Diabetes Daywww.idf.org
15–21 national skin Cancer action Weekwww.cancer.org.au
year 16Chris Stevenson
year 12Carrie Goodman
Sandra Hope-Johnstone
year 11Sandra Crispin
year 10Assia Baban
Debbie Kolbig
Karen Oldano
Kerry Dwyer
Sandie Finlay
year 9Carissa Callen
Christine Harris
Helen Campbell
Lisa Wiseman
Magdalena Lioi
Sharon Wigham
Shirley MacPherson
year 8Athena Tselonis
Huriye Irfanli
Joanne Johns
Julie Veitch
Kim Case
Sharon Larsen
year 7Dianne Fullarton
Jean Burke
Jeannie Race
Julie Killen
Kathryn Blackstock
Melissa Starkey
Sandra Lane
year 6Ange Bottcher
Anne Kay
Christine Davies
Debbie Needs
Felicity Barone
Gai Booth
Helen Hogan
Kelly Holmes
Kristine Taylor
Marian Inglis
Pam Biddle
year 5Dianne Brierley
Eleanor Barillas
Jane Campbell
Karen Read
Kirsty Wright
Lena McGuinness
Matthew Brown
Megan Collins
Noryati Jamal
Sandra Murphy
Sharon Wilkinson
Sue Heinrich
Val Downes
year 4Amanda Hill
Angela Ayuob
Ashleigh Bailey
Debbie Heinrich
Fay Welber
Jacki Perrett
Jenny Adams
Jenny McKenna
Krystal Evans
Kylie Richardson
Kym Allen
Nataly Spaseska
Sarah Clark
Sarah Fitzpatrick
Trista Gumburd
Zoee Bishop
year 3Cath Semmler
Clare Fisher
Jessica Foster
Jessica Lew
Jo-Anne Digney
Jordan Fisher
Karina Maronian
Kay Sloan
Kim Kirkpatrick
Leana Barker
Lyn Horne
Maria Farquhar
Narelle Boxhall
Nicole Williams
Rosie Brenton
Sue Loip
Suzanne Farnham
Tracey Gaynor
Zivka Vergara
year 2Ben Sharman
Carmelina Bachiller
Cindy Costelloe
Daiana Carulli
Demi Schreiber
Elizabeth Hagley
Elma Brkic
Elsa Keep
Elyse Burdak
Emily Roberts
Georgie Mathewson
Hannah Plozza
Jacinta Johnson
Jane Bailey
Jess Newman
Jessica Avery
Jessica Burton
Jessica Threadgate
Jodie Taggart
Kaitlan Smith
Katelyn Frost
Katrina Howell
Kirstie Marshall
Kurt Williams
Lauren Jackson
Madeline Gaiter
Mary-Lyn Keogh
Meagan Taylor
Melissa Lyfield
Michelle Karangoda
Pauline Jackson
Rochelle Fields
Sarah McConnon
Sharon Baillie
Shellie Wells
Shinae Milligan
Shona Thornton
year 1Abi Jamal
Adrian Cooney
Alicia Wilson
Allison O’Driscoll
Ambrose Yuen
Amy Phillips
Ashlyn Lee
Ben Sharman
Bernie Peterson
Brooke Kimmitt
Brooke O’Brien
Lenny Lay
Cheryl Pearce
Christine Phillips
Cody Marshall
Deb Hales
Denise Felsman
Dione Okmazic
Eileen Roberts
Elisa Buczko
Emily Pinnney
Gabby Tomkins
Gabriella Cicchini
Genevieve Lavis
Gillian Barrett
Glenda Jones
Isabelle Cooney
Jacki Wedding
JC Citizen
Jessica Bird
Jessie Gray
Joyce Upson
Kayleen Thomson
Kaylin Skipper
Kerry West
Kevin Foo
Kiani Prior
Kylie Douglas
Melissa Paull
Michelle O’Donnell
Naomi Charlton
Nicola Brown
Nicole Smith
Rebecca Cross
Rebecca Green
Renee Agar
Rhonda Cute
Sally Bellette
Sarah Andrews
Sarah Asher
Sheryl Lampard
Sonia Pryor
Sophia Gordon
Tahlia Watson
Tara Coyne
Teagan Doyle
Tia Reeve
Trudi Sauerbier
Vanessa Emmerton
Wendy McCarthy
Xuan Dao Nguyen